Page 1 : Progress in Pediatric Cardiology 58 (2020) 101258, , Contents lists available at ScienceDirect, , Progress in Pediatric Cardiology, journal homepage: www.elsevier.com/locate/ppedcard, , Review, , Intraoperative echocardiography in congenital heart surgery: What the, surgeon wants to know, , T, , ⁎, , Jennifer S. Nelsona,b, , Amr Matoqc, Gul Dadlania, Peter D. Weardena, Karen Bendera, a, , Department of Cardiovascular Services, Nemours Children's Hospital, Orlando, FL 32827; USA, Department of Surgery, University of Central Florida College of Medicine, Orlando, FL 32827; USA, c, Nemours Cardiac Center, Alfred I. DuPont Hospital for Children, Wilmington, DE 19803; USA, b, , A R T I C LE I N FO, , A B S T R A C T, , Keywords:, Congenital heart surgery, Cardiac imaging, Transesophageal echocardiography, Communication in the operating room, , Intraoperative transesophageal echocardiography (TEE) plays an integral role in the modern era of congenital, heart surgery. Pre- and post-repair imaging obtained in the operating room by a pediatric cardiologist is now, routine for most cardiac operations. This intraoperative collaboration is unique among the subspecialties, and, in, many cases, influences the next step of the operation. Although TEE is an invaluable tool for providing detailed, anatomical information, the surgical decisions based on that information are a reflection of the working relationship between the surgeon and the echocardiographer. As equally-invested stakeholders, pediatric cardiologists and surgeons share the responsibility for outcomes in congenital heart surgery. Optimizing communication in the operating room between surgeons and physicians performing echocardiograms is critical to, providing the best possible outcomes for patients. Although published guidelines describe the technical conduct, of TEE, they fail to describe what the surgeon is looking for and why. Just as surgeons may be unfamiliar with, the technical aspects of echocardiography, cardiologists may be unfamiliar with the technical aspects of certain, cardiac surgery procedures, and generally do not observe the entire operation. Because the surgeon looks at the, echocardiogram from the unique perspective of having recently handled the involved structures, he or she will, place priority on some aspects over others. Common priorities can be described by operation type. Herein, we, provide an overview of intraoperative TEE for six benchmark operations, from the perspective of the surgeon., , 1. Introduction, In the modern era of congenital heart surgery, intraoperative, transesophageal echocardiography (TEE) has become routine. A critical, evaluation of the surgical repair in collaboration with a pediatric cardiologist is now a standard part of most cardiac operations. For congenital heart surgeons, this examination of the result before the completion of the operation invites the opportunity for immediate feedback, and affords the opportunity for improvement in outcomes. TEE has, been shown to reduce morbidity, mortality, and cost in congenital, cardiac surgery [1–3]. What remains unmeasured is the necessary, teamwork component of this process. Although operative decisions are, ultimately made by the attending surgeon, these decisions are influenced by the intraoperative TEE expertise of our cardiology colleagues., As equally invested stakeholders in surgical outcomes, cardiologists, care for the patients long after they leave the operating room, sometimes for many decades. The working relationship and communication, in the operating room between the surgeon and the physician, , ⁎, , performing the echocardiogram is critical to providing the best possible, surgical outcomes for patients in any congenital heart program. Herein,, we provide an overview of intraoperative TEE for six benchmark operations from the perspective of the surgeon. The operations discussed, include: 1) complete repair of tetralogy of Fallot (TOF), 2) ventricular, septal defect closure (VSD), 3) repair of complete atrioventricular canal, (AVC), 4) arterial switch operation (ASO +/− VSD), 5) Fontan operation, and 6) repair of truncus arteriosus [4]. Because these operations frequently utilize TEE, and are typically included in quality reports for public reporting of congenital heart surgery outcomes, we aim, to improve communication in the operating room by explaining the, surgical implications of relevant TEE views. Sharing the surgical perspective is intended to increase efficiency in the operating room and, help optimize decision-making that may lead to improved outcomes for, patients., , Corresponding author at: Nemours Children's Hospital, 6535 Nemours Parkway, Orlando, FL 32827, USA., E-mail address:
[email protected] (J.S. Nelson)., , https://doi.org/10.1016/j.ppedcard.2020.101258, Received 24 May 2020; Accepted 10 June 2020, Available online 13 June 2020, 1058-9813/ © 2020 Elsevier B.V. All rights reserved., , Downloaded for Abhishek Srivastava (
[email protected]) at Fortis Escorts Heart Institute and Research Centre from ClinicalKey.com by, Elsevier on November 03, 2021. For personal use only. No other uses without permission. Copyright ©2021. Elsevier Inc. All rights reserved.
Page 2 : Progress in Pediatric Cardiology 58 (2020) 101258, , J.S. Nelson, et al., , Table 1, Common surgeon questions, implications, and favorite TEE views., Surgeon question, , Implication, , Our favorite TEE views, , General, “Is there a patent ductus arteriosus?”, , Should I plan to look for and ligate this fragile structure?, , Level: Upper esophagus, Transducer angel: 0–30 degrees, View will show the mid ascending aorta, main pulmonary artery, and proximal right pulmonary artery. A patent ductus arteriosus is, confirmed by seeing continuous flow into the main pulmonary, artery., View 1, Level: Mid esophagus, Transducer angel: 0–30°, View: Start in a four-chamber view with the coronary sinus, visualized and color box placed across the atrial septum. Pull the, probe up to sweep the entire atrial septum. This will ensure that, coronary sinus, sinus venosus and superiorly located atrial septal, defects are seen., View 2, Level: mid-esophagus, Transducer angel: 90–110°, View: This will create a bicaval view of the atrial septum with the, superior vena cava and inferior vena cava., View 3, Bubble study (if needed) in mid esophageal four-chamber view, View 1, Level: Mid esophagus, Transducer angel: 0–30°, View: Four-chamber view looks for air in all chambers, “echobright densities”, View 2, Level: mid-esophagus, Transducer angel: 120–140°, View: Long axis view demonstrates the left ventricle, left, ventricular outflow tract, aortic valve and proximal ascending, aorta. Air in the left ventricle rises anteriorly and will usually be, positioned along the ventricular septum and will show as an, “echobright density”., Level: Mid esophagus, Transducer angel: 0–30°, View: The four-chamber view allows the person performing the, TEE to communicate the filling of the various chambers after, bypass with the surgeon and can be correlated with the pressure, transduced lines in the right atrium and left atrium when, available., View 1, Level: Mid esophagus, Transducer angel: 0–30°, View Four-chamber chamber view will demonstrate the right and, left ventricular size and function well., View 2:, Level: transgastric, Transducer angel: 0–20°, View: Transgastric short axis view (at the level of papillary, muscle) will give a good assessment of the right and left, ventricular systolic function., , “Are there any atrial level shunts?”, , Do I need to change my cannulation strategy to prevent air, embolus? Will I need to arrest the heart?, , “Do you see any air?”, , Is there air in the systemic circulation? Do I need to further de-air, the heart to prevent air embolus before I let the heart eject?, , “How does the filling look?”, , Does my inspection of the outside of the heart and the, hemodynamics on the monitor match the TEE information, regarding filling? Should I fill the heart more before coming off, pump?, , “How's the function?”, , Does my knowledge of the clamp time and operative course fit, with the TEE information regarding systolic function?, Does the combination of all available data change my, management strategy with regard to inotropic support?, , Tetralogy of Fallot repair, “What is the location and degree of right, ventricular outflow tract, obstruction?”, , Can I do a valve-sparing repair? What do I need to patch? Where, is the muscle that needs resecting?, , View 1:, Level: Upper esophagus, Transducer angel: 0–30°, View will show the mid ascending aorta, main pulmonary artery, and proximal right pulmonary artery. This view will assess the, branched pulmonary arteries and main pulmonary artery., View 2:, Level: mid esophagus, Transducer angel: 50–70°, View: Right ventricular inflow and outflow view. This will show, the aortic valve in center with the right atrium, tricuspid valve,, body of the right ventricle, right ventricular outflow tract and, pulmonary valve spanning across the aortic valve., Very good for complete assessment of the entire right ventricular, outflow tract and relationship of the VSD to the tricuspid and, pulmonary valves., View 3, Level: transgastric, Transducer angel: 0–20°, View: Right ventricle inflow to outflow view. The right atrium,, , (continued on next page), 2, , Downloaded for Abhishek Srivastava (
[email protected]) at Fortis Escorts Heart Institute and Research Centre from ClinicalKey.com by, Elsevier on November 03, 2021. For personal use only. No other uses without permission. Copyright ©2021. Elsevier Inc. All rights reserved.
Page 3 : Progress in Pediatric Cardiology 58 (2020) 101258, , J.S. Nelson, et al., , Table 1 (continued), Surgeon question, , Implication, , Our favorite TEE views, tricuspid valve, body of the right ventricle, right ventricular, outflow tract and pulmonary valve can all be imaged. May be, difficult to achieve this image in some patients., , VSD repair, “What is the location of the VSD?”, , “Any new aortic regurgitation?”, , How will I plan to approach this VSD? Transatrially,, transpulmonary, or via right ventriculotomy?, , Did I cause any distortion or injury to the aortic, pulmonary or, tricuspid valve while suturing the VSD patch?, , View 1, Level: mid-esophagus, Transducer angel: 0–30°, View: Start in a four-chamber view posteriorly with the coronary, sinus seen and place the color box across the entire ventricular, septum including the apex. Then pull the probe up, performing a, sweep of the septum posteriorly to anteriorly to the pulmonary, valve. All types of VSD's should be able to be seen as well as the, tricuspid valve., View 2, Level: mid esophagus, Transducer angel: 50–70°, View: Right ventricular inflow and outflow view. This will show, the aortic valve in center with the right atrium, tricuspid valve,, body of the right ventricle and pulmonary valve spanning across, the aortic valve., Very good for detecting perimembranous, muscular, and, supracristal ventricular septal defects as well as excluding doublechambered right ventricle. The tricuspid and pulmonary valves, should be inspected in this plane., View 3, Level: mid-esophagus, Transducer angel: 120–140°, View: Long axis view demonstrates the left ventricle, left, ventricular outflow tract, aortic valve and proximal ascending, aorta. This will demonstrate the relationship of the VSD to the, aortic valve and exclude a subaortic membrane. Perimembranous, and muscular VSD's are well seen., , TEE = transesophageal echocardiogram; VSD = ventricular septal defect., , 2. General information – preoperative exam, , 3. General information - postoperative exam, , 2.1. Is the diagnosis the same? Anything else I need to plan for? Reasons I, would cannulate differently?, , 3.1. “Do you see any air? How's the function? Did we achieve the goals of, the operation?”, , After safe probe placement, a systematic TEE examination is conducted using the most recent guidelines of the American Society of, Echocardiography [5]. In addition to evaluating the right and left heart, function, the surgeon will be most interested in confirming the diagnosis, and knowing if there are any previously unrecognized anatomical, details that would alter the operative plan (Table 1). For example, a, child brought to the operating room for closure of a VSD may be found, to have a subaortic membrane, or a double-chambered right ventricle, previously unrecognized on the preoperative transthoracic echocardiogram. Because time is of the essence when the aorta is crossclamped, anything that helps the surgeon plan ahead and avoid being, surprised by the intra-cardiac anatomy is helpful., A common finding on preoperative TEE is a patent ductus arteriosus, that was not previously noted. After initiating cardiopulmonary bypass,, the presence of a patent ductus arteriosus can result in low perfusion, pressure, requiring prompt ligation. Therefore, it is preferable to know, about a patent ductus arteriosus preoperatively. Also, the identification, of intracardiac shunts not recognized on prior transthoracic studies may, require a different cannulation strategy than was planned, and the, surgeon, perfusionist, and operative team will need to adjust accordingly. A bubble study with agitated saline should be completed if there, is a question of an intracardiac shunt. This is particularly important in a, redo sternotomy because alternate cannulation strategies may need to, be applied in case of inadvertent cardiac injury during the sternotomy, or dissection., , Before weaning from cardiopulmonary bypass, the surgeon wants to, know if there is intracavitary air, particularly in the systemic circulation, that needs to be evacuated prior to allowing the heart to eject., During weaning from bypass, he or she will want to know information, about ventricular filling and contractility in order to guide volume, administration and titration of inotropes. After separation from bypass,, the surgeon wants to know if the repair is adequate, or if further revisions are necessary. Operation-specific details are provided below., 4. Complete repair of tetralogy of Fallot, 4.1. Background, TOF describes a spectrum of disease states across a range of anatomical variants. The most frequently diagnosed form is TOF with, pulmonary stenosis. Other variants include TOF with pulmonary atresia, with or without major aortopulmonary collaterals, and TOF with absent, pulmonary valve. Special considerations for the intraoperative TEE, examination of these other types will not be covered in this review., TOF with pulmonary stenosis is characterized by a VSD, right ventricular outflow tract obstruction, an overriding aorta, and right ventricular hypertrophy. The goals of surgery are to close the VSD and, relieve the right ventricular outflow tract obstruction. Today, intraoperative TEE, and the surgical decision-making that follows it, are, both valuable contributors to a successful outcome [6]. In addition, TEE, information obtained regarding the volume status and contractility of, the right ventricle can help the anesthesiologist manage intravascular, fluid administration and depth of anesthesia to prevent a hypercyanotic, 3, , Downloaded for Abhishek Srivastava (
[email protected]) at Fortis Escorts Heart Institute and Research Centre from ClinicalKey.com by, Elsevier on November 03, 2021. For personal use only. No other uses without permission. Copyright ©2021. Elsevier Inc. All rights reserved.
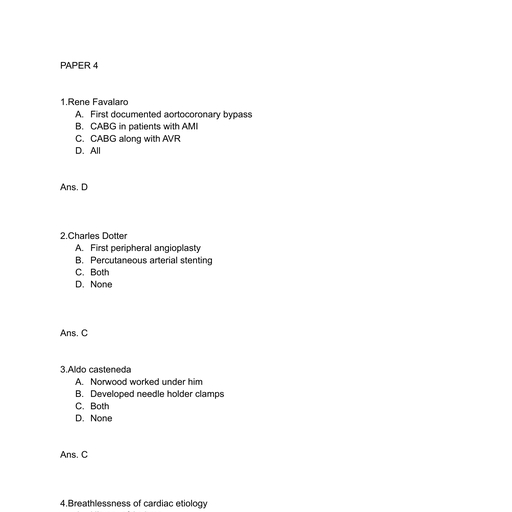
Page 4 : Progress in Pediatric Cardiology 58 (2020) 101258, , J.S. Nelson, et al., , for the individual patient., , spell in the operating room prior to the initiation of cardiopulmonary, bypass., , 4.2.5. Is there a left superior vena cava?, Ten percent of TOF patients have a persistent left superior vena, cava. Often it drains to the coronary sinus, and, in the absence of a, bridging vein, a third venous cannula for cardiopulmonary bypass may, be needed. A dilated coronary sinus is a frequent clue to the presence of, a left superior vena cava but it may not appear dilated in the setting of, systemic right ventricular pressure., , 4.2. Pre-repair, 4.2.1. “Is the VSD ‘typical’ for TOF?”, The preliminary TEE study should assess the size, location and, number of ventricular septal defects. The typical ventricular septal, defect in TOF is perimembranous, large and unrestrictive. The direction, of flow through the ventricular septal defect is determined by the degree of right ventricular outflow tract obstruction and may vary dramatically as the dynamic component of the outflow tract obstruction, changes. Occasionally, the ventricular septal defect is juxtaarterial or, doubly committed, and this information can influence the surgical approach., , 4.3. Post-repair, 4.3.1. “Is there a significant residual ventricular septal defect?”, The same views used during the initial TEE are used for detecting a, residual VSD. It is important to look closely at the margins of the VSD, patch for a residual shunt but these should not be confused with an, eccentric tricuspid regurgitation jet. A residual VSD < 3 mm is likely, hemodynamically insignificant, and usually does not need to be addressed. At the time of hospital discharge, it is non-detectable in twothirds of the patients in whom it was noted [7]. On the other hand, a, residual defect > 4–5 mm warrants attention before leaving the operating room. For residual defects between 3 and 5 mm, hemodynamic, calculations can be done by sampling blood and measuring the oxygen, saturation from the superior vena cava, pulmonary artery, and aorta. If, the residual defect results in a pulmonary blood flow to systemic blood, flow ratio (Qp:Qs) > 1.5 to 1, the residual defect should be repaired., Muscular VSDs not apparent pre-repair when flow through the large, perimembranous VSD is non-restrictive may be apparent by color flow, Doppler on the post-repair study. These ventricular muscular septal, defects are seldom large enough to warrant re-arresting the heart for, repair., , 4.2.2. “What is the location and severity of right ventricular outflow tract, obstruction?”, Right ventricular outflow tract obstruction in TOF can occur at, multiple levels. It typically involves the subvalvular region, characterized by a narrow infundibulum and the presence of obstructive, hypertrophied right ventricular muscle bundles. It frequently includes, valvular components such as a small pulmonary valve annulus and a, dysplastic pulmonary valve (often bileaflet) and supravalvular components such as discrete stenosis and/or diffuse hypoplasia of the main, and/or branch pulmonary arteries. For several decades, the pulmonary, valve was routinely sacrificed during repair to alleviate all right ventricular outflow tract obstruction leaving the patient with unrestricted, pulmonary regurgitation and the likely need for future reintervention., More recent efforts have focused on saving the pulmonary valve and the, anatomical detail obtained during the initial TEE examination can influence the decision concerning the appropriateness of a valve-sparing, procedure (Table 1)., A pulmonary valve annulus with a Z-score larger than −3 may be, amenable to a valve-sparing procedure. In that case, the surgeon will, initially limit his or her incision in the main pulmonary artery, infundibulum, or both, so that it does not cross the annulus. The valve, may then be grossly examined and a decision made. If a transannular, patch is required, the surgeon may create a monocusp valve. A monocusp valve can reduce the amount of pulmonary insufficiency and right, ventricular dysfunction in the immediate post-operative period., Discrete focal stenoses of the main and/or branch pulmonary arteries, are amenable to patch angioplasty and pulse wave, continuous wave,, and color Doppler provide important information regarding pressure, gradients at these locations. Diminutive, diffusely hypoplastic branch, pulmonary arteries might steer the surgeon to a two-staged repair- a, modified Blalock-Taussig shunt followed by a complete repair in several, months when the pulmonary arteries demonstrate flow-related growth., , 4.3.2. “Is there excessive residual right ventricular outflow tract, obstruction?”, It is seldom possible to reduce the right ventricular outflow tract, gradient to zero. Therefore, after most TOF repairs, there is a mild, degree of RVOT obstruction remaining. The surgeon will want to know, what the degree of residual obstruction is, where it is located, and, whether it appears to be fixed or dynamic (Fig. 1). In cases where a, valve-sparing repair was performed, he or she will want to focus on the, pulmonary valve in particular, to try to decide expeditiously whether, return to bypass is needed. Regardless of the type of repair, direct, pressure measurements to assess post-operative hemodynamics are, , 4.2.3. Is there a coronary artery crossing the RVOT?, Five to 10% of patients with TOF have a surgically relevant, anomalous coronary artery, and coronary artery anatomy should be, clarified on the preoperative TEE examination. The anatomy is also, verified on direct visualization during the operation. The most common, coronary anomaly is a left anterior descending artery (LAD) originating, from the right coronary artery which crosses the right ventricular, outflow tract. Because this location would be incised for a transannular, patch, an alternative surgical strategy such as a right ventricle to pulmonary artery conduit or transatrial repair can be used to relieve the, right ventricular outflow tract obstruction and avoid injury to the LAD., 4.2.4. Is there an atrial septal defect or PFO?, A small PFO is often desirable after a TOF repair. Thirty percent of, patients with TOF will already have an atrial septal defect or PFO. If the, surgeon has planned to close the VSD through a right ventriculotomy,, he or she may not need to open the right atrium, depending on the goals, , Fig. 1. TEE Mid-Esophageal RV in-out (50–80°) view showing residual obstruction in the right ventricular outflow tract (arrow) following repair of tetralogy of Fallot., 4, , Downloaded for Abhishek Srivastava (
[email protected]) at Fortis Escorts Heart Institute and Research Centre from ClinicalKey.com by, Elsevier on November 03, 2021. For personal use only. No other uses without permission. Copyright ©2021. Elsevier Inc. All rights reserved.
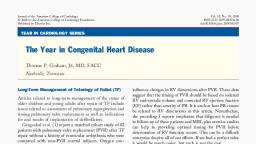
Page 5 : Progress in Pediatric Cardiology 58 (2020) 101258, , J.S. Nelson, et al., , are the most common type of VSD seen by surgeons, but they frequently, extend into adjacent parts of the ventricular septum. Inlet defects, often, called “canal” type defects, are located behind the septal leaflet of the, tricuspid valve. Outlet defects are also known as supracristal, conal,, infundibular or juxtaarterial. Muscular defects can be single or multiple., , typically obtained by the surgeon to corroborate the echo-based information. When the right ventricular pressure is > 70–80% systemic,, or if the RVOT gradient is > 30 mmHg, additional efforts to reduce the, RVOT obstruction are generally undertaken. An assessment of the severity of tricuspid regurgitation may also give the surgeon a better, understanding of the degree to which the residual obstruction is problematic. If the right ventricular hypertension is thought due to a diffusely hypoplastic pulmonary bed, re-arresting the heart may still be, required to fenestrate the VSD patch., , 5.2. Pre-repair, 5.2.1. “Where is the VSD?”, The surgeon wants to know the location of the VSD, and if there are, other lesions that need to be addressed at the time of surgery. The location of the VSD determines the operative approach. For example, a, perimembranous VSD is closed transatrially, through the tricuspid, valve, while a supracristal VSD may be better approached through the, pulmonary valve, via an incision in the main pulmonary artery, (Table 1)., , 4.3.3. “Which direction is blood shunting across the PFO?”, The stiff hypertrophied right ventricle of TOF demonstrates worsened restrictive physiology after cardiopulmonary bypass. To preserve, cardiac output, many surgeons leave a small atrial septal defect or PFO, as a “pop-off”. Until the right ventricular diastolic compliance improves, the flow will be predominately right to left and the patient may, experience some mild to moderate arterial oxygen desaturation., 4.3.4. “Is there new aortic regurgitation?”, The post-repair TEE examination may demonstrate aortic insufficiency if the aortic valve is injured or distorted during repair of the, ventricular septal defect (Table 1). New aortic regurgitation generally, warrants re-arresting the heart to inspect for VSD patch sutures involving the aortic valve. If identified, that portion of the patch suture line, must be revised. Additional tips for TEE imaging following repair of, TOF are shown in Text Box 1., , 5.3. Post-repair, 5.3.1. “Is the VSD closed? Is there new aortic valve insufficiency or severe, tricuspid regurgitation?”, The TEE evaluation of a repaired perimembranous VSD is also discussed in the TOF repair section. Following patch closure of a supracristal VSD, the TEE view is different (Fig. 2), but the surgeon's questions are similar: is there are residual shunt, and what is the estimated, size and specific location? Most surgeons would consider re-arresting, the heart and re-attempting to close the VSD if the residual shunt is, hemodynamically significant (Qp: Qs post-repair of 1.5:1 or greater), or, if the size of the residual shunt is > 3 mm. Because there are other, factors to consider (LV systolic function, bypass time, other co-morbidities), the decision to “go back” for a residual VSD is made on a caseby-case basis, often involving a conversation with the surgeon and the, cardiologist performing the TEE. Because the residual VSD may be, difficult to see, as much information as possible about its location is, helpful., New aortic regurgitation is discussed in the TOF repair section., Tricuspid regurgitation is also of interest. Approaching a VSD transatrially requires retraction of the tricuspid valve to expose the VSD., Tricuspid regurgitation may be the result of a retraction-related injury, to the valve or due to distortion caused by the VSD patch situated beneath its anteroseptal commissure. For this reason, some surgeons, perform a commissuroplasty at this location to prevent tricuspid regurgitation. The tricuspid regurgitation jet may also be used to estimate, right ventricular pressure., , 5. Ventricular septal defect repair, 5.1. Background, A VSD is the second most common congenital heart anomaly. A, bicuspid aortic valve is the most common but rarely requires surgery in, childhood. The VSD can be anywhere in the ventricular septum –, perimembranous, inlet, outlet, or muscular. Perimembranous defects, Box 1, Echocardiographer tips – repair of Tetralogy of Fallot., Pre-repair, Additional muscular VSDs may be present although they are frequently, • VSD:, undetected by color flow imaging until the larger primary VSD has been repaired., Right ventricular outflow tract: The deep transgastric right ventricular outflow view, • will, define the entire RVOT including the pulmonary valve and supravalvular area., pulmonary arteries: The mid-esophageal 5-chamber view with the probe, • Branch, rotated to the left brings the branch pulmonary arteries into view. The air-filled left, , •, •, •, •, , bronchus lies between the left pulmonary artery and the esophagus making, visualization of this branch pulmonary artery challenging and frequently, unsuccessful., Coronary anatomy: Dual left anterior descending coronary arteries may be present, and the presence of a left anterior descending artery in the normal position does not, rule out an aberrant additional left anterior descending. A prominent conal branch, can be confused with an anomalous left anterior descending artery but it will, terminate in the infundibulum rather than course down the interventricular grove., ASD: An ASD is best seen from the following views: mid-esophageal 4-chamber,, mid-esophageal aortic valve short-axis, mid-esophageal right ventricular inflowoutflow, mid-esophageal bicaval, and deep transgastric atrial septal., Left superior vena cava: The left superior vena cava lies anterior to the pulmonary, artery on TEE., Additional sources of pulmonary artery blood flow: Inspect for more than one, ductus arteriosus and/or major aortopulmonary collateral arteries. In the presence, of a large patent ductus arteriosus, the right ventricular outflow tract gradient may, be underestimated., , 6. Repair of complete atrioventricular canal, 6.1. Background, Atrioventricular canal defects, also referred to as atrioventricular, septal defects, or endocardial cushion defects, represents 4–7% of, congenital heart defects and are often associated with Down syndrome, [8]. There are many variations of AVC, but they all share the following, features: AV valve leaflet insertion at the same level; a deficiency of the, atrioventricular septum (e.g. ostium primum ASD, inlet VSD); anterior, and superior displacement of the aortic valve (unwedged); elongation, of the left ventricular outflow tract (gooseneck deformity); rotation of, the left ventricular papillary muscles; and, a cleft in the left AV valve., , Post-repair, Right ventricular outflow tract: Evaluate the RVOT for persistent obstruction at, the subvalvular, valvular, and supravalvular areas including the branch, pulmonary arteries. There may be dynamic as well as fixed obstruction. Use, continuous-wave Doppler to measure peak and mean gradients at each location., Right ventricular systolic pressure: May be estimated by continuous-wave Doppler, interrogation of the tricuspid regurgitation., , •, , 6.2. Pre-repair, , •, , 6.2.1. “How much is the left AV valve leaking?”, The TEE evaluation of an AVC should include an assessment of the, valve apparatus and the valve competency pre-repair. Valvar regurgitation may appear less severe under general anesthesia, but the valve, 5, , Downloaded for Abhishek Srivastava (
[email protected]) at Fortis Escorts Heart Institute and Research Centre from ClinicalKey.com by, Elsevier on November 03, 2021. For personal use only. No other uses without permission. Copyright ©2021. Elsevier Inc. All rights reserved.
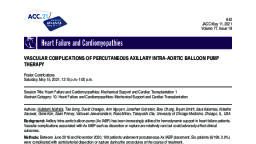
Page 6 : Progress in Pediatric Cardiology 58 (2020) 101258, , J.S. Nelson, et al., , Fig. 2. TEE with color Doppler mid-esophageal aortic valve short axis view (25–45°) A) pre-operative imaging of supracristal VSD and B) post-repair image showing, no residual VSD., , Fig. 3. Mid esophageal four chamber views of a complete atrioventricular canal. A) Preoperative 2D image showing large VSD and ASD with atrioventricular valves, at same level. B) Preoperative image with color Doppler showing trivial regurgitation of the left atrioventricular valve. C) Post-repair 2D image showing VSD and ASD, patches. D) Post-repair image with color Doppler showing no residual VSD and trivial left atrioventricular valve regurgitation., , apparatus can often be better seen in TEE, compared to a transthoracic, study (Fig. 3A,B). Also of interest to the surgeon is an assessment of any, subvalvar attachments to or across the interventricular septum. Preoperative evaluation of the left ventricular outflow tract for the “gooseneck deformity” commonly seen in AVC is also useful in predicting, postoperative left ventricular outflow tract obstruction. These anatomic, details can help the surgeon gauge the complexity of the repair, and, estimate the cross-clamp time that will be involved., , cardiac shunts, and how much the left atrioventricular valve is leaking,, as recurrent left atrioventricular valve regurgitation is the most, common reason patients require repeat intervention in the future, (Fig. 3C-D). Following “cleft closure” of the left atrioventricular valve,, the surgeon will want to know the inflow gradient, to assess for stenosis. Lastly, avoidance of left ventricular outflow tract obstruction is, another surgical consideration, and an evaluation for flow acceleration, at that location is standard for repair of AVC., , 6.3. Post-repair, , 7. Truncus arteriosus repair, , 6.3.1. “How much is the left AV valve leaking?”, The goals of surgical repair of AVC are to close the VSD and ASD and, to divide the atrioventricular valves without leaving the patient with, significant valvular stenosis or regurgitation. There are two main, techniques for repair of AVC involving either one or two patches to, separate the valves and reconstruct the septum. Regardless of the, technique used, the surgeon wants to know if there are residual intra-, , 7.1. Background, Truncus arteriosus (TA) is a rare anomaly and represents only 1–2%, of congenital heart anomalies but must be repaired in the neonatal, period to avoid irreversible pulmonary vascular obstructive disease. A, single arterial trunk provides the origins of the coronary arteries, ascending aorta, and pulmonary artery. The pulmonary artery may arise, 6, , Downloaded for Abhishek Srivastava (
[email protected]) at Fortis Escorts Heart Institute and Research Centre from ClinicalKey.com by, Elsevier on November 03, 2021. For personal use only. No other uses without permission. Copyright ©2021. Elsevier Inc. All rights reserved.
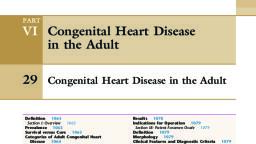
Page 7 : Progress in Pediatric Cardiology 58 (2020) 101258, , J.S. Nelson, et al., , of life [12]. In d-TGV, ventriculoarterial discordance results in the aorta, arising from the right ventricle and the pulmonary artery from the left, ventricle. The atrioventricular connections are concordant. In 80% of, patients with d-TGV the aorta is to the right and anterior to the pulmonary artery, and 40% have a VSD as an additional source of mixing, [13]. However, a VSD may not be an efficient site of mixing due to, preferential streaming of blood into the respective great artery. The, VSD is usually perimembranous but can be found anywhere along the, ventricular septum and can vary in size from very large to small and, restrictive. Left ventricular outflow tract obstruction occurs in 5–10% of, cases and correction requires a much more extensive operation than the, standard arterial switch operation and will not be discussed in this, review., Survival after birth is not possible without mixing of the two parallel, circulations. In the setting of the most common form of d-TGV- an intact, ventricular septum and no other defects- the foramen ovale and ductus, arteriosus play key roles in maintaining adequate systemic oxygenation., The severity of cyanosis varies with the adequacy of mixing at the atrial, septum and the flow through the ductus arteriosus. A prostaglandin E1, infusion is started immediately after birth to preserve patency of the, ductus arteriosus and a balloon atrial septostomy may be needed if, there is inadequate mixing at the atrial level and severe hypoxemia, persists., The goals of surgery are: 1) to restore ventriculoarterial concordance and 2) and close the patent ductus arteriosus (PDA), PFO, (typically large following balloon atrial septostomy), and VSD (if one is, present). To accomplish the arterial switch portion, the aorta and pulmonary artery are divided just below the level of the pulmonary bifurcation. The branch pulmonary arteries are transposed to a position, anterior to the aorta (LeCompte maneuver). The coronary arteries are, harvested from the native aortic root, taking a variable amount of sinus, tissue with them as a ‘button’. The distal aorta is reanastomosed to the, native pulmonary root to form a neoaortic root either before (closed, technique) or after coronary reimplantation (open technique)., Regardless of the technique, the coronary arteries are mobilized and, reimplanted into the neoaortic root, taking great care not to cause, distortion by stretching or kinking these small vessels. The neopulmonary artery is then reconstructed with patch material to close the, defects left behind from the harvest of the coronary buttons. Ultimately,, the reconstructed pulmonary root is reanastomosed to the pulmonary, bifurcation, taking care to avoid undue tension, as the branch pulmonary arteries can become stenotic as they drape over the ascending, aorta., , from the common trunk as a single main pulmonary artery or separate, right and left branch pulmonary arteries. The ductus arteriosus is not, needed to support the fetal circulation and is often absent. The truncal, valve is most often tricuspid (70%) but can be quadricuspid (20%),, pentacuspid or unicuspid and is often dysplastic, regurgitant or stenotic., 8. Pre-repair, In truncus arteriosus, preoperative evaluation with transthoracic, echocardiography is usually sufficient to gather the information needed, to plan surgical intervention. This includes, mainly, the type/classification of truncus arteriosus, morphology and competence of the truncal, valve, the ventricular septal defect size and margins, pulmonary artery, branches takeoff and size, biventricular size and systolic function and, the presence of any arch anomalies., 8.1. Post-repair, 8.1.1. “Is there conduit obstruction? Is there good flow in the branch PAs?”, In complete repair, the surgeon's priorities when looking at the, echocardiogram are to identify any significant residual VSD and to, verify unobstructed blood flow from the right ventricle to pulmonary, artery conduit into the branch pulmonary arteries, as these are the, aspects that are most likely to necessitate resuming bypass and potentially re-arresting the heart. A right ventricular pressure estimate and, direction of shunt flow may influence medical management when, weaning from bypass, such as the decision to utilize inhaled nitric, oxide. The site of the aortic repair (or reconstruction, depending on the, type) is also an area of interest to rule out distortion of the valve or flow, acceleration. Intraoperative echocardiography should also evaluate the, truncal valve for stenosis and/or regurgitation and the left ventricular, outflow tract for obstruction. If the initial palliation is bilateral PA, banding, the intraoperative echocardiography evaluation should include measuring bilateral PA band gradient, which is often easier to do, with epicardial echocardiogram (Fig. 4) [9–11]., 9. Arterial Switch Operation for d-Transposition of the Great, Vessels ( ± VSD), 9.1. Background, Dextro-transposition of the great vessels (d-TGV) presents at birth, with cyanosis and without surgical repair carries a 90% mortality in the, first year of life. For the last three decades, the arterial switch operation, which replaced the original surgical approach of redirecting blood, flow by atrial baffling (Mustard or Senning procedure), has resulted in, long term survival rates of 96–99% when performed in the first 2 weeks, , 9.2. Pre-repair, 9.2.1. “Is there any outflow tract obstruction? Is the coronary anatomy as, anticipated on TTE?”, On the preoperative TEE, the surgeon wants to know if there is any, previously undetected outflow tract obstruction, and if present, the, severity of it. The presence of left ventricular outflow tract obstruction, can significantly change the surgical approach to a Nakaidoh or Rastelli, procedure., The other preoperative focus is on understanding the coronary, anatomy. Coronary artery variations are common in d-TGV, such as the, circumflex arising from the right coronary artery, a single right coronary artery, an intramural course, or separate ostia in one sinus. The, coronary anatomy can influence the operative plan with regard to, harvesting and reimplanting the coronary arteries. Some variations,, inverted and intramural coronaries in particular, can make coronary, artery translocation more challenging. Difficulty with coronary artery, re-implantation accounts for the majority of perioperative deaths, so, anatomical detail about the coronaries is helpful to know preoperatively [14]., Other preoperative details to note include the morphology of the, semilunar valves and the presence or absence of a VSD. Confirm the, , Fig. 4. – Epicardial echocardiogram image showing the pulmonary arteries, originating from the aorta in a patient with truncus arteriosus who has undergone bilateral pulmonary artery banding., 7, , Downloaded for Abhishek Srivastava (
[email protected]) at Fortis Escorts Heart Institute and Research Centre from ClinicalKey.com by, Elsevier on November 03, 2021. For personal use only. No other uses without permission. Copyright ©2021. Elsevier Inc. All rights reserved.
Page 8 : Progress in Pediatric Cardiology 58 (2020) 101258, , J.S. Nelson, et al., , Fig. 6. TEE Upper esophageal PA view (0–30°) showing color Doppler imaging, of pulmonary arteries after LeCompte maneuver (arrow). The pulmonary bifurcation has been surgically repositioned anterior to the aorta., , Fig. 5. TEE Mid-Esophageal Aortic valve short axis view (25–45°) with color, flow showing flow in right (arrow) and left (double arrow) coronary arteries., , annulus size, number of leaflets, and presence of regurgitation and/or, stenosis of the semilunar valves. Close attention should be paid to the, pulmonary valve, as it will remain the semilunar valve for the systemic, circulation. Early operation is important in transposition of the great, vessels. Left ventricle mass regresses steadily and results in the inability, of the left ventricle to support the systemic circulation. The presence of, a VSD, although not always helpful with maintaining systemic oxygenation, does shunt right to left in d-TGV and may delay left ventricular, regression. More than one ventricular septal defect is uncommon. If a, ventricular septal defect is present, its size, location, proximity to the, semilunar or atrioventricular valves should be carefully defined., , Box 2, Echocardiographer Tips – Arterial Switch Operation., Pre-repair, tract obstruction: Views that can be helpful include the mid-esophageal, • Outflow, long-axis, mid-esophageal right ventricular inflow-outflow, transgastric and deep, transgastric., , Evaluate the ventricular septum with the following views to confirm the, • VSD:, transthoracic echocardiographic findings: mid-esophageal 4-chamber view, mid-, , •, , 9.3. Post-repair, , •, , 9.3.1. “Do you see antegrade flow in the coronaries? How's the function? Is, there narrowing at the pulmonary artery anastomosis?, Color flow mapping and Doppler of the coronary arteries is essential. Kinking, tension, and extrinsic compression on a translocated, coronary artery by the neopulmonary artery can all cause post-repair, coronary insufficiency. The surgeon will want to know if flow is seen in, the coronaries (Fig. 5) and if ventricular function is concerning on TEE,, although it is generally obvious on direct visual inspection of the heart, if there is a regional perfusion defect and accompanying acute ischemia, with poor function., Both outflow tracts need to be carefully evaluated for obstruction., After the coronary arteries are mobilized and reimplanted, the reconstructed pulmonary root is reanastomosed to the pulmonary bifurcation. Increased flow velocity often seen in branch pulmonary arteries after the LeCompte maneuver due to the new anterior position of, the PAs that drape over the aorta. Ideally, the branch PAs will have, been adequately mobilized prior to the LeCompte maneuver, in order to, prevent undue tension at the time they are reanastomosed to the newly, reconstructed pulmonary artery (Fig. 6). Because supravalvar pulmonary artery stenosis is a common long-term complication after the, arterial switch operation [15], the surgeon will want to know if there is, flow acceleration seen at this site., Other areas of particular interest to the surgeon on the post-repair, TEE include an assessment of the function of each semilunar valve, (looking particularly for regurgitation), and an inspection for residual, intracardiac shunting. The same views used during the initial TEE examination are used for detecting a residual PFO/ASD and VSD., Echocardiographer tips for imaging in the arterial switch operation are, shown in Box 2., , esophageal 5-chamber with a probe angle of 0°; mid-esophageal right ventricular, inflow-outflow with the probe angle between 40 and 60°; mid-esophageal aortic, valve long-axis with the probe angle between 90 and 120°; and a deep gastric 5chamber with the probe angle between 0 and 20°., Semilunar valves: Views for examining the semilunar valves include midesophageal long-axis, mid-esophageal aortic valve short-axis and mid-esophageal, aortic valve long-axis., Left ventricular mass and function: The left ventricle should appear circular in, shape with the interventricular septum convex towards the right ventricle. Left, ventricle imaging is best using the mid-esophageal 4-chamber, mid-esophageal 2chamber and transgastric short-axis views. The size and function of the mitral valve, should also be re-assessed., , Post-repair, Coronary artery flow: The mid-esophageal aortic valve short axis view (25–45°), with color flow can show flow in the proximal coronary arteries., Supravalvar pulmonary stenosis: The mid-esophageal ascending aortic short-axis, view can be used to assess the main pulmonary artery and the mid-esophageal 5chamber view with the probe rotated to the left to image the branch pulmonary, arteries., Atrial septal defect: Will be closed as part of the surgical repair and is best examined, for residual shunting with mid-esophageal 4-chamber, mid-esophageal aortic valve, short-axis, mid-esophageal right ventricular inflow-outflow, mid-esophageal, bicaval, and deep transgastric imaging., , •, •, •, , 10. Fontan operation, 10.1. Background, The goal of the Fontan operation is to establish a complete cavopulmonary connection. Usually, the Fontan operation represents the, third stage of palliation for patients with single-ventricle physiology., Therefore, in most cases the patient has already undergone a bi-directional Glenn or hemiFontan procedure. At the time of the Fontan, the, patient undergoes a redo sternotomy and the inferior vena cava is, connected to the pulmonary arteries and their existing connection to, the superior vena cava. This connection may be accomplished with an, extra-cardiac conduit (commonly follows a bi-directional Glenn), or a, lateral tunnel (commonly follows a hemiFontan procedure). A fenestration connecting the Fontan pathway with the common atrium, , 8, , Downloaded for Abhishek Srivastava (
[email protected]) at Fortis Escorts Heart Institute and Research Centre from ClinicalKey.com by, Elsevier on November 03, 2021. For personal use only. No other uses without permission. Copyright ©2021. Elsevier Inc. All rights reserved.
Page 9 : Progress in Pediatric Cardiology 58 (2020) 101258, , J.S. Nelson, et al., , compromise [17,18]. The use of epicardial echocardiography as an, adjunct to TEE provides additional value especially in vascular structures such as pulmonary artery branches (Fig. 4) [10]. The degree to, which epicardial echocardiography is utilized is very center-specific,, but surgeons and cardiologists should have a basic familiarity with the, process of working together to obtain and interpret the images. An, obscured view of the probe due to surgical drapes can be disorienting, for the cardiologist who is analyzing the images (and often helping to, direct the surgeon who is holding the probe). Clear communication is, critical to acquiring useful images efficiently and avoiding errors in, interpretation., 11. Summary, Fig. 7. TEE Mid-esophageal bicaval view with color flow showing a lateral, tunnel Fontan conduit and flow across the open fenestration. The direction of, flow is from the Fontan circulation into the adjacent common atrium., , Intraoperative TEE is routine in modern congenital heart surgery, programs. Most congenital heart centers utilize intraoperative TEE to, confirm preoperative diagnoses and alter surgical plans if additional, lesions are noted, ensure cardiac de-airing prior to separation from, cardiopulmonary bypass, identify new and residual problems prior to, removal of cardiopulmonary bypass cannulae, and evaluate ventricular, filling and function to help guide fluid and inotropic support [5]., Understanding the surgical perspective is paramount to performing, an efficient TEE. Effective communication between the echocardiographer and the surgeon is a key element in the conduct of modern, congenital cardiac surgery. Improving this collaboration will help, provide the best possible outcomes for our patients., , (containing the pulmonary venous return) is frequently performed and, has been associated with shorter hospitalizations, lower volume of chest, tube drainage, and fewer additional procedures postoperatively, compared to the Fontan procedure without a fenestration [16]., 10.2. Pre-repair, 10.2.1. “Is there an issue with the Glenn or hemi-Fontan pathway that I, need to address?”, Before the operation begins, the surgeon wants to know if there is, any obstruction to systemic venous return reaching the distal pulmonary arteries. A stenotic anastomosis of the superior vena cava to the, pulmonary artery should be addressed at the Fontan. If there are branch, pulmonary artery stenoses, these should also be addressed at the time of, surgery., , CRediT authorship contribution statement, Jennifer S. Nelson:Conceptualization, Writing - original draft,, Writing - review & editing, Validation.Amr Matoq:Writing - original, draft, Writing - review & editing.Gul Dadlani:Writing - review &, editing, Validation.Peter D. Wearden:Writing - review & editing,, Validation.Karen Bender:Conceptualization, Writing - original draft,, Writing - review & editing, Validation., , 10.3. Post-repair, , Declaration of competing interest, , 10.3.1. “Is there any obstruction in the Fontan pathway and is the, fenestration open?”, The post-repair TEE should demonstrate the Fontan pathway as best, as possible. At this point the surgeon wants to know if there is any, obstruction within the pathway that would require immediate revision., Pulmonary artery flow and Doppler patterns should also be evaluated., Direct pressure measurements taken by the surgeon at the field will, contribute to the hemodynamic assessment., In a fenestrated Fontan, it is comforting to visualize flow across the, fenestration (Fig. 7), as creating a fenestration in an extra-cardiac, Fontan can be complicated by kinking, narrowing, or other distortion, when the heart is filled, depending on the technique used to construct, it. Regardless, establishing the patency of the fenestration, and the flow, direction will help determine if the physiology is acceptable and the, operation may be concluded, or if further revisions are necessary prior, to leaving the operating room. This information also helps guide postoperative medical management., , The authors have no relevant conflicts of interest to disclose.,This, research did not receive any specific grant from funding agencies in the, public, commercial or not-for-profit sectors., References, [1] Bettex DA, Pretre R, Jenni R and Schmid ER. Cost-effectiveness of routine intraoperative transesophageal echocardiography in pediatric cardiac surgery: a 10year experience. Anesth Analg. 2005;100:1271–5, table of contents., [2] Randolph GR, Hagler DJ, Connolly HM, Dearani JA, Puga FJ, Danielson GK, et al., Intraoperative transesophageal echocardiography during surgery for congenital, heart defects. J Thorac Cardiovasc Surg 2002;124:1176–82., [3] Siwik ES, Spector ML, Patel CR, Zahka KG. Costs and cost-effectiveness of routine, transesophageal echocardiography in congenital heart surgery. Am Heart J, 1999;138:771–6., [4] Jacobs JP, O’Brien SM, Pasquali SK, Jacobs ML, Lacour-Gayet FG, Tchervenkov CI,, et al. Variation in outcomes for benchmark operations: an analysis of the Society of, Thoracic Surgeons congenital heart surgery database. Ann Thorac Surg, 2011;92:2184–91. [discussion 2191-2]., [5] Puchalski MD, Lui GK, Miller-Hance WC, Brook MM, Young LT, Bhat A, et al., Guidelines for performing a comprehensive transesophageal echocardiographic:, examination in children and all patients with congenital heart disease: recommendations from the American Society of Echocardiography. J Am Soc, Echocardiogr 2019;32:173–215., [6] Smith CA, McCracken C, Thomas AS, Spector LG, St Louis JD, Oster ME, et al. Longterm outcomes of tetralogy of Fallot: a study from the pediatric cardiac care consortium. JAMA Cardiol 2019;4:34–41., [7] Dodge-Khatami A, Knirsch W, Tomaske M, Pretre R, Bettex D, Rousson V, et al., Spontaneous closure of small residual ventricular septal defects after surgical repair., Ann Thorac Surg 2007;83:902–5., [8] Hoffman JI, Kaplan S, Liberthson RR. Prevalence of congenital heart disease. Am, Heart J 2004;147:425–39., [9] Stern KWD, Emani SM, Peek GJ, Geva T, Kutty S. Epicardial echocardiography in, pediatric and congenital heart surgery. World J Pediatr Congenit Heart Surg, , 10.4. Epicardial echo, 10.4.1. “How do I work this thing?”, Epicardial echocardiogram plays a vital role in intraoperative imaging, particularly in smaller patients, and when TEE is contraindicated., It has also been shown to be superior to TEE in extracardiac and vascular structures like pulmonary artery branches, aortic arch, BT shunt,, coronary arteries, pulmonary veins, and cavo-pulmonary anastomosis, [10,11,17]. On the other hand, epicardial echocardiography interrupts, the surgical procedure and cannot be utilized for continuous monitoring. It also can rarely cause arrhythmia or hemodynamic, 9, , Downloaded for Abhishek Srivastava (
[email protected]) at Fortis Escorts Heart Institute and Research Centre from ClinicalKey.com by, Elsevier on November 03, 2021. For personal use only. No other uses without permission. Copyright ©2021. Elsevier Inc. All rights reserved.