Page 1 :
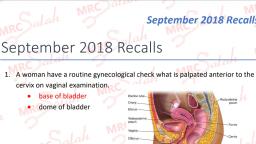
Which of the following drugs increases the rate of gastric emptying in the vagotomised stomach?, , Ondansetron, , Metoclopramide, , Cyclizine, , Erythromycin, , Chloramphenicol, Vagotomy seriously compromises gastric emptying which is why either a pyloroplasty or gastroenterostomy is routinely performed at the same time., Chloramphenicol has no effect on gastric emptying. Ondansetron slows gastric emptying slightly., Metoclopramide increases the rate of gastric emptying but its effects are mediated via the vagus, nerve. Erythromycin enhances gastric emptying by acting via the motilin receptor in the gut., Please rate this question:, , Discuss and give feedback, , Next question, , Gastric emptying, , , , , The stomach serves both a mechanical and immunological function. Solid and liquid are, retained in the stomach during which time repeated peristaltic activity against a closed, pyloric sphincter will cause fragmentation of food bolus material. Contact with gastric acid will, help to neutralise any pathogens present., The amount of time material spends in the stomach is related to its composition and volume., For example a glass of water will empty more quickly than a large meal. The presence of, amino acids and fat will all serve to delay gastric emptying., , Controlling factors, Neuronal stimulation of the stomach is mediated via the vagus and the parasympathetic nervous, system will tend to favor an increase in gastric motility. It is for this reason that individuals who have, undergone truncal vagotomy will tend to routinely require either a pyloroplasty or gastro-enterostomy, as they would otherwise have delayed gastric emptying., The following hormonal factors are all involved:
Page 2 :
Delay emptying, , Increase emptying, , Gastric inhibitory peptide, , Gastrin, , Cholecystokinin, , Enteroglucagon, , Diseases affecting gastric emptying, All diseases that affect gastric emptying may result in bacterial overgrowth, retained food and, eventually the formation of bezoars that may occlude the pylorus and make gastric emptying even, worse. Fermentation of food may cause dyspepsia, reflux and foul smelling belches of gas., Iatrogenic, Gastric surgery can have profound effects on gastric emptying. As stated above any procedure that, disrupts the vagus can cause delayed emptying. Whilst this is particularly true of vagotomy, this, operation is now rarely performed. Surgeons are divided on the importance of vagal disruption that, occurs during an oesophagectomy, some will routinely perform a pyloroplasty and others will not., When a distal gastrectomy is performed, the type of anastomosis performed will impact on emptying., When a gastro-enterostomy is constructed, a posterior, retrocolic gastroenterostomy will empty, better than an anterior one., Diabetic gastroparesis, This is predominantly due to neuropathy affecting the vagus nerve. The stomach empties poorly and, patients may have episodes of repeated and protracted vomiting. Diagnosis is made by upper GI, endoscopy and contrast studies, in some cases a radio nucleotide scan is needed to demonstrate, the abnormality more clearly. In treating these conditions, drugs such as metoclopramide will be less, effective as they exert their effect via the vagus nerve. One of the few prokinetic drugs that do not, work in this way is the antibiotic erythromycin., Malignancies, Obviously a distal gastric cancer may obstruct the pylorus and delay emptying. In addition,, malignancies of the pancreas may cause extrinsic compression of the duodenum and delay, emptying. Treatment in these cases is by gastric decompression using a wide bore nasogastric tube, and insertion of a stent or, if that is not possible, by a surgical gastroenterostomy. As a general rule, gastroenterostomies constructed for bypass of malignancy are usually placed on the anterior wall of, the stomach (in spite of the fact that they empty less well). A Roux en Y bypass may also be, undertaken, but the increased number of anastomoses for this, in malignant disease that is being, palliated, is probably not justified., Congenital Hypertrophic Pyloric Stenosis, This is typically a disease of infancy. Most babies will present around 6 weeks of age with projectile, non bile stained vomiting. It has an incidence of 2.4 per 1000 live births and is more common in, males. Diagnosis is usually made by careful history and examination and a mass may be palpable in
Page 3 :
the epigastrium (often cited seldom felt!). The most important diagnostic test is an ultrasound that, usually demonstrates the hypertrophied pylorus. Blood tests may reveal a hypochloraemic metabolic, alkalosis if the vomiting is long standing. Once the diagnosis is made the infant is resuscitated and a, pyloromyotomy is performed (either open or laparoscopically). Once treated there are no long term, sequelae., Next question
Page 4 :
Which of the following is not secreted by the parietal cells?, , Hydrochloric acid, , Mucus, , Magnesium, , Intrinsic factor, , Calcium, Chief of Pepsi cola = Chief cells secrete PEPSInogen, Parietal cells: secrete HCl, Ca, Na, Mg and intrinsic factor, Chief cells: secrete pepsinogen, Surface mucosal cells: secrete mucus and bicarbonate, Please rate this question:, , Discuss and give feedback, , Next question, , Gastric secretions, A working knowledge of gastric secretions is important for surgery because peptic ulcers are, common, surgeons frequently prescribe anti secretory drugs and because there are still patients, around who will have undergone acid lowering procedures (Vagotomy) in the past., Gastric acid, , , , , , Is produced by the parietal cells in the stomach, pH of gastric acid is around 2 with acidity being maintained by the H+/K+ ATP ase pump. As, part of the process bicarbonate ions will be secreted into the surrounding vessels., Sodium and chloride ions are actively secreted from the parietal cell into the canaliculus., This sets up a negative potential across the membrane and as a result sodium and, potassium ions diffuse across into the canaliculus., Carbonic anhydrase forms carbonic acid which dissociates and the hydrogen ions formed by, dissociation leave the cell via the H+/K+ antiporter pump. At the same time sodium ions are, actively absorbed. This leaves hydrogen and chloride ions in the canaliculus these mix and, are secreted into the lumen of the oxyntic gland.
Page 5 :
This is illustrated diagrammatically below:, , Image sourced from Wikipedia, , Phases of gastric acid secretion, There are 3 phases of gastric secretion:, 1. Cephalic phase (smell / taste of food), , , , 30% acid produced, Vagal cholinergic stimulation causing secretion of HCL and gastrin release from G cells, , 2. Gastric phase (distension of stomach ), , , , 60% acid produced, Stomach distension/low H+/peptides causes Gastrin release
Page 6 :
3. Intestinal phase (food in duodenum), , , , 10% acid produced, High acidity/distension/hypertonic solutions in the duodenum inhibits gastric acid secretion, via enterogastrones (CCK, secretin) and neural reflexes., , Regulation of gastric acid production, Factors increasing production include:, , , , , Vagal nerve stimulation, Gastrin release, Histamine release (indirectly following gastrin release) from enterchromaffin like cells, , Factors decreasing production include:, , , , , Somatostatin (inhibits histamine release), Cholecystokinin, Secretin, , The diagram below illustrates some of the factors involved in regulating gastric acid secretion and, the relevant associated pharmacology, , Image sourced from Wikipedia, , Below is a brief summary of the major hormones involved in food digestion:
Page 7 :
Source, , Stimulus, , Actions, , Gastrin, , G cells in, antrum of the, stomach, , Distension of, stomach, extrinsic, nerves, Inhibited by: low, antral pH,, somatostatin, , Increase HCL, pepsinogen and IF secretion,, increases gastric motility, trophic effect on, gastric mucosa, , CCK, , I cells in, upper small, intestine, , Partially digested, proteins and, triglycerides, , Increases secretion of enzyme-rich fluid, from pancreas, contraction of gallbladder, and relaxation of sphincter of Oddi,, decreases gastric emptying, trophic effect on, pancreatic acinar cells, induces satiety, , Secretin, , S cells in, upper small, intestine, , Acidic chyme,, fatty acids, , Increases secretion of bicarbonate-rich fluid, from pancreas and hepatic duct cells,, decreases gastric acid secretion, trophic, effect on pancreatic acinar cells, , VIP, , Small, intestine,, pancreas, , Neural, , Stimulates secretion by pancreas and, intestines, inhibits acid and pepsinogen, secretion, , Somatostatin, , D cells in the, pancreas and, stomach, , Fat, bile salts and, glucose in the, intestinal lumen, , Decreases acid and pepsin secretion,, decreases gastrin secretion, decreases, pancreatic enzyme secretion, decreases, insulin and glucagon secretion, inhibits trophic effects of gastrin, stimulates, gastric mucous production, Next question
Page 8 :
A 65 year old man is admitted for a below knee amputation. He is taking digoxin. Clinically the, patient has an irregularly irregular pulse. What would you expect to see when you examine the, jugular venous pressure?, , Absent y waves, , Slow y descent, , Cannon waves, , Steep y descent, , Absent a waves, Jugular venous pressure, Absent a waves = Atrial fibrillation, Large a waves = Any cause of right ventricular hypertrophy, tricuspid stenosis, Cannon waves (extra large a waves) = Complete heart block, Prominent v waves = Tricuspid regurgitation, Slow y descent = Tricuspid stenosis, right atrial myxoma, Steep y descent = Right ventricular failure, constrictive pericarditis, tricuspid regurgitation, Theme from January 2013 exam, This patient has atrial fibrillation and is most likely to have absent a waves., Please rate this question:, , Discuss and give feedback, , Next question, , Jugular venous pressure, As well as providing information on right atrial pressure, the jugular vein waveform may provide, clues to underlying valvular disease. A non-pulsatile JVP is seen in superior vena caval obstruction., Kussmaul's sign describes a paradoxical rise in JVP during inspiration seen in constrictive, pericarditis, 'a' wave = atrial contraction, , , large if atrial pressure e.g. tricuspid stenosis, pulmonary stenosis, pulmonary hypertension
Page 9 :
, , absent if in atrial fibrillation, , Cannon 'a' waves, , , , caused by atrial contractions against a closed tricuspid valve, are seen in complete heart block, ventricular tachycardia/ectopics, nodal rhythm, single, chamber ventricular pacing, , 'c' wave, , , , closure of tricuspid valve, not normally visible, , 'v' wave, , , , due to passive filling of blood into the atrium against a closed tricuspid valve, giant v waves in tricuspid regurgitation, , 'x' descent = fall in atrial pressure during ventricular systole, 'y' descent = opening of tricuspid valve, , Image sourced from Wikipedia, , Next question
Page 10 :
Which part of the ECG represents atrial depolarization?, , P wave, , Q wave, , T wave, , QRS complex, , P-R interval, , Theme from April 2013 exam, Theme from April 2014 exam, The P wave represents atrial depolarization. Note that atrial repolarization is obscured within the, QRS complex., Please rate this question:, , Discuss and give feedback, , Next question, , The normal ECG
Page 11 :
Image sourced from Wikipedia, , P wave, , , , , Represents the wave of depolarization that spreads from the SA node throughout the atria, Lasts 0.08 to 0.1 seconds (80-100 ms), The isoelectric period after the P wave represents the time in which the impulse is traveling, within the AV node, , P-R interval, , , , , Time from the onset of the P wave to the beginning of the QRS complex, Ranges from 0.12 to 0.20 seconds in duration, Represents the time between the onset of atrial depolarization and the onset of ventricular, depolarization, , QRS complex, , , , Represents ventricular depolarization, Duration of the QRS complex is normally 0.06 to 0.1 seconds
Page 12 :
ST segment, , , , Isoelectric period following the QRS, Represents period which the entire ventricle is depolarized and roughly corresponds to the, plateau phase of the ventricular action potential, , T wave, , , , Represents ventricular repolarization and is longer in duration than depolarization, A small positive U wave may follow the T wave which represents the last remnants of, ventricular repolarization., , Q-T interval, , , , , , , Represents the time for both ventricular depolarization and repolarization to occur, and, therefore roughly estimates the duration of an average ventricular action potential., Interval ranges from 0.2 to 0.4 seconds depending upon heart rate., At high heart rates, ventricular action potentials shorten in duration, which decreases the Q-T, interval. Therefore the Q-T interval is expressed as a "corrected Q-T (QTc)" by taking the QT interval and dividing it by the square root of the R-R interval (interval between ventricular, depolarizations). This allows an assessment of the Q-T interval that is independent of heart, rate., Normal corrected Q-Tc interval is less than 0.44 seconds., Next question
Page 13 :
A 45 year old male has alcoholic cirrhosis and decompensated liver failure, which of the following, clotting factors is least likely to be affected?, , Factor V, , Factor VII, , Factor IX, , Factor VIII, , Factor XI, , Factor VIII is synthesised in the endothelial cells of the liver rather than the liver itself and therefore, is less prone to the effects of hepatic dysfunction., Please rate this question:, , Discuss and give feedback, , Next question, , Abnormal coagulation, Cause, , Factors affected, , Heparin, , Prevents activation factors 2,9,10,11, , Warfarin, , Affects synthesis of factors 2,7,9,10
Page 14 :
Cause, , Factors affected, , DIC, , Factors 1,2,5,8,11, , Liver disease, , Factors 1,2,5,7,9,10,11, , Interpretation blood clotting test results, , Disorder, , APTT, , PT, , Bleeding time, , Haemophilia, , Increased, , Normal, , Normal, , von Willebrand's disease, , Increased, , Normal, , Increased, , Vitamin K deficiency, , Increased, , Increased, , Normal, Next question
Page 15 :
A 23 year old is stabbed in the groin and develops hypovolaemic shock. What is the most likely, finding on analysis of his urine?, , Decreased specific gravity, , Increased specific gravity, , Increased urinary glucose, , Increased urinary protein, , Increased red blood cells in the urine, , Theme from April 2013 Exam, Hypovolaemic shock is likely to compromise renal blood flow especially if blood pressure falls below, the range at which the kidney is able to autoregulate its blood flow. The result of this will be an, increase of the specific gravity as water retention occurs in an attempt to maintain circulating, volume., Please rate this question:, , Discuss and give feedback, , Next question, , Renal Physiology, Overview, , , , , Each nephron is supplied with blood from an afferent arteriole that opens onto the glomerular, capillary bed., Blood then flows to an efferent arteriole, supplying the peritubular capillaries and medullary, vasa recta., The kidney receives up to 25% of resting cardiac output., , Control of blood flow, , , , The kidney is able to autoregulate its blood flow between systolic pressures of 80- 180mmHg, so there is little variation in renal blood flow., This is achieved by myogenic control of arteriolar tone, both sympathetic input and hormonal, signals (e.g. renin) are responsible.
Page 16 :
Glomerular structure and function, , , , , , , , , Blood inside the glomerulus has considerable hydrostatic pressure., The basement membrane has pores that will allow free diffusion of smaller solutes, larger, negatively charged molecules such as albumin are unable to cross., The glomerular filtration rate (GFR) is equal to the concentration of a solute in the urine,, times the volume of urine produced per minute, divided by the plasma concentration, (assuming that the solute is freely diffused e.g. inulin)., In clinical practice creatinine is used because it is subjected to very little proximal tubular, secretion., Although subject to variability, the typical GFR is 125ml per minute., Glomerular filtration rate = Total volume of plasma per unit time leaving the capillaries and, entering the bowman's capsule, Renal clearance = volume plasma from which a substance is removed per minute by the, kidneys, , Substances used to measure GFR have the following features:, 1. Inert, 2. Free filtration from the plasma at the glomerulus (not protein bound), 3. Not absorbed or secreted at the tubules, 4. Plasma concentration constant during urine collection, Examples: inulin, creatinine, GFR = urine concentration (mmol/l) x urine volume (ml/min), -------------------------------------------------------------------------plasma concentration (mmol/l), , , , , The clearance of a substance is dependent not only on its diffusivity across the basement, membrane but also subsequent tubular secretion and / or reabsorption., So glucose which is freely filtered across the basement membrane is usually reabsorbed, from tubules giving a clearance of zero., , Tubular function, , , , , , , Reabsorption and secretion of substances occurs in the tubules., In the proximal tubule substrates such as glucose, amino acids and phosphate are cotransported with sodium across the semi permeable membrane., Up to two thirds of filtered water is reabsorbed in the proximal tubules., This will lead to increase in urea concentration in the distal tubule allowing for its increased, diffusion., Substances to be secreted into the tubules are taken up from the peritubular blood by tubular, cells.
Page 17 :
, , , Solutes such as paraaminohippuric acid are cleared with a single passage through the, kidneys and this is why it is used to measure renal plasma flow. Ions such as calcium and, phosphate will have a tubular reabsorption that is influenced by plasma PTH levels., Potassium may be both secreted and re-absorbed and is co-exchanged with sodium., , Loop of Henle, , , , , , , , , , Approximately 60 litres of water containing 9000mmol sodium enters the descending limb of, the loop of Henle in 24 hours., Loops from the juxtamedullary nephrons run deep into the medulla., The osmolarity of fluid changes and is greatest at the tip of the papilla., The thin ascending limb is impermeable to water, but highly permeable to sodium and, chloride ions., This loss means that at the beginning of the thick ascending limb the fluid is hypo osmotic, compared with adjacent interstitial fluid., In the thick ascending limb the reabsorption of sodium and chloride ions occurs by both, facilitated and passive diffusion pathways., The loops of Henle are co-located with vasa recta, these will have similar solute, compositions to the surrounding extracellular fluid so preventing the diffusion and, subsequent removal of this hypertonic fluid., The energy dependent reabsorption of sodium and chloride in the thick ascending limb helps, to maintain this osmotic gradient., , Next question
Page 18 :
A healthy man has a blood pressure of 120/80 mmHg and an intra cranial pressure of 17 mmHg., What is the approximate cerebral perfusion pressure?, , 103 mmHg, , 63 mmHg, , 83 mmHg, , 91 mmHg, , 76 mmHg, Cerebral perfusion pressure= Mean arterial pressure - intra cranial pressure, , Theme from September 2015 Exam, The mean arterial pressure can be calculated as:, MAP= Diastolic pressure+ 0.333(Systolic pressure- Diastolic pressure), In this situation the MAP = 93., The ICP is subtracted from this value; 93 - 17 = 76, Please rate this question:, , Discuss and give feedback, , Next question, , Cerebral perfusion pressure, The cerebral perfusion pressure (CPP) is defined as being the net pressure gradient causing blood, flow to the brain. The CPP is tightly autoregulated to maximise cerebral perfusion. A sharp rise in, CPP may result in a rising ICP, a fall in CPP may result in cerebral ischaemia. It may be calculated, by the following equation:, CPP= Mean arterial pressure - Intra cranial pressure
Page 19 :
Following trauma, the CPP has to be carefully controlled and the may require invasive monitoring of, the ICP and MAP., Next question
Page 20 :
There is decreased secretion of which one of the following hormones in response to major surgery:, , Insulin, , Cortisol, , Renin, , Anti diuretic hormone, , Prolactin, Endocrine parameters reduced in stress response:, , , , , Insulin, Testosterone, Oestrogen, , Insulin is often released in decreased quantities following surgery., Please rate this question:, , Discuss and give feedback, , Next question, , Stress response: Endocrine and metabolic changes, , , , , Surgery precipitates hormonal and metabolic changes causing the stress response., Stress response is associated with: substrate mobilization, muscle protein loss, sodium and, water retention, suppression of anabolic hormone secretion, activation of the sympathetic, nervous system, immunological and haematological changes., The hypothalamic-pituitary axis and the sympathetic nervous systems are activated and, there is a failure of the normal feedback mechanisms of control of hormone secretion., , A summary of the hormonal changes associated with the stress response:, , Increased, , Decreased, , No Change
Page 22 :
, , ACTH stimulates cortisol production within a few minutes of the start of surgery. More ACTH, is produced than needed to produce a maximum adrenocortical response., , Cortisol, , , , , , Significant increases within 4-6 hours of surgery (>1000 nmol litre-1)., The usual negative feedback mechanism fails and concentrations of ACTH and cortisol, remain persistently increased., The magnitude and duration of the increase correlate with the severity of stress and the, response is not abolished by the administration of corticosteroids., The metabolic effects of cortisol are enhanced:, , Skeletal muscle protein breakdown to provide gluconeogenic precursors and amino acids for protein, synthesis in the liver, Stimulation of lipolysis, 'Anti-insulin effect', Mineralocorticoid effects, Anti-inflammatory effects, Growth hormone, , , , Increased secretion after surgery has a minor role, Most important for preventing muscle protein breakdown and promote tissue repair by insulin, growth factors, , Alpha Endorphin, , , Increased, , Antidiuretic hormone, , , , , An important vasopressor and enhances haemostasis, Renin is released causing the conversion of angiotensinogen to angiotensin I, Angiotensin II formed by ACE on angiotensin 1, which causes the secretion of aldosterone, from the adrenal cortex. This increases sodium reabsorption at the distal convoluted tubule, , Insulin, , , Release inhibited by stress
Page 23 :
, , , , Occurs via the inhibition of the beta cells in the pancreas by the α2-adrenergic inhibitory, effects of catecholamines, Insulin resistance by target cells occurs later, The perioperative period is characterized by a state of functional insulin deficiency, , Thyroxine (T4) and tri-iodothyronine (T3), , , Circulating concentrations are inversely correlated with sympathetic activity and after surgery, there is a reduction in thyroid hormone production, which normalises over a few days., , Metabolic effect of endocrine response, Carbohydrate metabolism, , , , , , , , Hyperglycaemia is a main feature of the metabolic response to surgery, Due to increase in glucose production and a reduction in glucose utilization, Catecholamines and cortisol promote glycogenolysis and gluconeogenesis, Initial failure of insulin secretion followed by insulin resistance affects the normal responses, The proportion of the hyperglycaemic response reflects the severity of surgery, Hyperglycaemia impairs wound healing and increase infection rates, , Protein metabolism, , , , , , , Initially there is inhibition of protein anabolism, followed later, if the stress response is, severe, by enhanced catabolism, The amount of protein degradation is influenced by the type of surgery and also by the, nutritional status of the patient, Mainly skeletal muscle protein is affected, The amino acids released form acute phase proteins (fibrinogen, C reactive protein,, complement proteins, a2-macroglobulin, amyloid A and ceruloplasmin) and are used for, gluconeogenesis, Nutritional support has little effect on preventing catabolism, , Lipid metabolism, Increased catecholamine, cortisol and glucagon secretion, and insulin deficiency, promotes lipolysis, and ketone body production., Salt and water metabolism, , , , ADH causes water retention, concentrated urine, and potassium loss and may continue for 3, to 5 days after surgery, Renin causes sodium and water retention
Page 24 :
Cytokines, , , , , , Glycoproteins, Interleukins (IL) 1 to 17, interferons, and tumour necrosis factor, Synthesized by activated macrophages, fibroblasts, endothelial and glial cells in response to, tissue injury from surgery or trauma, IL-6 main cytokine associated with surgery. Peak 12 to 24 h after surgery and increase by, the degree of tissue damage Other effects of cytokines include fever, granulocytosis,, haemostasis, tissue damage limitation and promotion of healing., , Modifying the response, , , , , , , , , Opioids suppress hypothalamic and pituitary hormone secretion, At high doses the hormonal response to pelvic and abdominal surgery is abolished., However, such doses prolong recovery and increase the need for postoperative ventilatory, support, Spinal anaesthesia can reduce the glucose, ACTH, cortisol, GH and epinephrine changes,, although cytokine responses are unaltered, Cytokine release is reduced in less invasive surgery, Nutrition prevents the adverse effects of the stress response. Enteral feeding improves, recovery, Growth hormone and anabolic steroids may improve outcome, Normothermia decreases the metabolic response, , References, Deborah Burton, Grainne Nicholson, and George Hall, Endocrine and metabolic response to surgery ., Contin Educ Anaesth Crit Care Pain (2004) 4(5): 144-147 doi:10.1093/bjaceaccp/mkh040, Next question
Page 25 :
A 28 year old man undergoes an ileocaecal resection to treat terminal ileal Crohns disease. Post, operatively he attends the clinic and complains of diarrhoea. His CRP is within normal limits and, small bowel enteroclysis shows no focal changes. Which of the following interventions is most likely, to be beneficial?, , 5 ASA drugs, , Azathioprine, , Pulsed methylprednisolone, , Infliximab, , Oral cholestyramine, , Malabsorption of bile salts is a common cause of diarrhoea following ileal resection. A normal small, bowel study and CRP effectively excludes active Crohns disease and therefore immunomodulator, drugs are not appropriate., Please rate this question:, , Discuss and give feedback, , Next question, , Ileum, Anatomical overview, The terminal ileum comprises two fifths of the small intestine and has a diameter that is smaller than, that of the jejunum (typically 2cm at the ileocaecal valve). The ileum is attached to the abdominal, wall by a mesentery that contains more fat than that of the jejunum. The blood supply of the ileum is, derived from branches of the superior mesenteric artery, the vascular arcades of the ileum are more, densely packed than those of the jejunum. The wall of the ileum contains Peyers patches which are, aggregations of lymphoid tissue.
Page 26 :
Function, The main function of the terminal ileum is absorption of vitamin B12 and bile salts. The, neuroendocrine cells in the wall of the ileum may secrete hormones. In surgical patients, resection of, the terminal ileum is a common procedure for conditions such as terminal ileal Crohns disease., Where a significant proportion of the ileum is removed, patients are at increased risk of bile salt, malabsorption with the development of bile salt diarrhoea and increased risk of gallstones. The lack, of vitamin B12 may pre-dispose to macrocytic anaemia., Next question
Page 27 :
Which of the following statements related to the coagulation cascade is true?, , The intrinsic pathway is the main pathway in coagulation, , Heparin inhibits the activation of Factor 8, , The activation of factor 8 is the point when the intrinsic and the extrinsic pathways meet, , Tissue factor released by damaged tissue initiates the extrinsic pathway, , Thrombin converts plasminogen to plasmin, , Theme from April 2015 Exam, The extrinsic pathway is the main path of coagulation. Heparin inhibits the activation of factors, 2,9,10,11. The activation of factor 10 is when both pathways meet. Thrombin converts fibrinogen to, fibrin. During fibrinolysis plasminogen is converted to plasmin to break down fibrin., Please rate this question:, , Discuss and give feedback, , Next question, , Coagulation cascade, Two pathways lead to fibrin formation, Intrinsic pathway (components already present in the blood), , , , , , , , Minor role in clotting, Subendothelial damage e.g. collagen, Formation of the primary complex on collagen by high-molecular-weight kininogen (HMWK),, prekallikrein, and Factor 12, Prekallikrein is converted to kallikrein and Factor 12 becomes activated, Factor 12 activates Factor 11, Factor 11 activates Factor 9, which with its co-factor Factor 8a form the tenase complex, which activates Factor 10, , Extrinsic pathway (needs tissue factor released by damaged tissue), , , Tissue damage
Page 28 :
, , , , Factor 7 binds to Tissue factor, This complex activates Factor 9, Activated Factor 9 works with Factor 8 to activate Factor 10, , Common pathway, , , , Activated Factor 10 causes the conversion of prothrombin to thrombin, Thrombin hydrolyses fibrinogen peptide bonds to form fibrin and also activates factor 8 to, form links between fibrin molecules, , Fibrinolysis, Plasminogen is converted to plasmin to facilitate clot resorption, , Image sourced from Wikipedia, , Intrinsic pathway, , Increased APTT, , Factors 8,9,11,12, , Extrinsic pathway, , Increased PT, , Factor 7, , Common pathway, , Increased APTT & PT, , Factors 2,5,10, , Vitamin K dependent, , Factors 2,7,9,10
Page 29 :
A 34 year old man receives morphine following an appendicectomy. He develops constipation as a, result. Which of the following best accounts for this process?, , Stimulation of DOPA receptors, , Inhibition of DOPA receptors, , Stimulation of µ receptors, , Stimulation of serotonin release, , Inhibition of serotonin release, 4 Types of opioid receptor:, , , , , , δ (located in CNS)- Accounts for analgesic and antidepressant effects, k (mainly CNS)- analgesic and dissociative effects, µ (central and peripheral) - causes analgesia, miosis, decreased gut motility, Nociceptin receptor (CNS)- Affect of appetite and tolerance to µ agonists., , Theme from April 2013 Exam, Constipation is a common side effect of morphine treatment and stimulation of µ receptors accounts, for this process., Please rate this question:, , Discuss and give feedback, , Next question, , Morphine, Strong opiate analgesic. It is a pro- type narcotic drug and its effects mediated via the 4 types of, opioid receptor. Its clinical effects stem from binding to these receptor sites within the CNS and, gastrointestinal tract. Unwanted side effects include nausea, constipation, respiratory depression, and, if used long term, addiction ., It may be administered orally or intravenously. It can be reversed with naloxone., Next question
Page 30 :
Which of the following is not well absorbed following a gastrectomy?, , Vitamin c, , Zinc, , Vitamin B12, , Copper, , Molybdenum, , Vitamin B12. The others are unaffected, Post gastrectomy syndrome, , , , , Rapid emptying of food from stomach into the duodenum: diarrhoea, abdominal pain,, hypoglycaemia, Complications: Vitamin B12 and iron malabsorption, osteoporosis, Treatment: High protein, low carbohydrate diet. Replace B12/Fe/Ca, , Please rate this question:, , Discuss and give feedback, , Next question, , Gastric emptying, , , , , The stomach serves both a mechanical and immunological function. Solid and liquid are, retained in the stomach during which time repeated peristaltic activity against a closed, pyloric sphincter will cause fragmentation of food bolus material. Contact with gastric acid will, help to neutralise any pathogens present., The amount of time material spends in the stomach is related to its composition and volume., For example a glass of water will empty more quickly than a large meal. The presence of, amino acids and fat will all serve to delay gastric emptying., , Controlling factors, Neuronal stimulation of the stomach is mediated via the vagus and the parasympathetic nervous, system will tend to favor an increase in gastric motility. It is for this reason that individuals who have, undergone truncal vagotomy will tend to routinely require either a pyloroplasty or gastro-enterostomy
Page 31 :
as they would otherwise have delayed gastric emptying., The following hormonal factors are all involved:, , Delay emptying, , Increase emptying, , Gastric inhibitory peptide, , Gastrin, , Cholecystokinin, , Enteroglucagon, , Diseases affecting gastric emptying, All diseases that affect gastric emptying may result in bacterial overgrowth, retained food and, eventually the formation of bezoars that may occlude the pylorus and make gastric emptying even, worse. Fermentation of food may cause dyspepsia, reflux and foul smelling belches of gas., Iatrogenic, Gastric surgery can have profound effects on gastric emptying. As stated above any procedure that, disrupts the vagus can cause delayed emptying. Whilst this is particularly true of vagotomy, this, operation is now rarely performed. Surgeons are divided on the importance of vagal disruption that, occurs during an oesophagectomy, some will routinely perform a pyloroplasty and others will not., When a distal gastrectomy is performed, the type of anastomosis performed will impact on emptying., When a gastro-enterostomy is constructed, a posterior, retrocolic gastroenterostomy will empty, better than an anterior one., Diabetic gastroparesis, This is predominantly due to neuropathy affecting the vagus nerve. The stomach empties poorly and, patients may have episodes of repeated and protracted vomiting. Diagnosis is made by upper GI, endoscopy and contrast studies, in some cases a radio nucleotide scan is needed to demonstrate, the abnormality more clearly. In treating these conditions, drugs such as metoclopramide will be less, effective as they exert their effect via the vagus nerve. One of the few prokinetic drugs that do not, work in this way is the antibiotic erythromycin., Malignancies, Obviously a distal gastric cancer may obstruct the pylorus and delay emptying. In addition,, malignancies of the pancreas may cause extrinsic compression of the duodenum and delay, emptying. Treatment in these cases is by gastric decompression using a wide bore nasogastric tube, and insertion of a stent or, if that is not possible, by a surgical gastroenterostomy. As a general rule, gastroenterostomies constructed for bypass of malignancy are usually placed on the anterior wall of, the stomach (in spite of the fact that they empty less well). A Roux en Y bypass may also be, undertaken, but the increased number of anastomoses for this, in malignant disease that is being, palliated, is probably not justified.
Page 32 :
Congenital Hypertrophic Pyloric Stenosis, This is typically a disease of infancy. Most babies will present around 6 weeks of age with projectile, non bile stained vomiting. It has an incidence of 2.4 per 1000 live births and is more common in, males. Diagnosis is usually made by careful history and examination and a mass may be palpable in, the epigastrium (often cited seldom felt!). The most important diagnostic test is an ultrasound that, usually demonstrates the hypertrophied pylorus. Blood tests may reveal a hypochloraemic metabolic, alkalosis if the vomiting is long standing. Once the diagnosis is made the infant is resuscitated and a, pyloromyotomy is performed (either open or laparoscopically). Once treated there are no long term, sequelae., Next question
Page 33 :
Which vitamin is involved in the formation of collagen?, , Vitamin A, , Vitamin B, , Vitamin C, , Vitamin D, , Vitamin E, , Theme from September 2015 Exam, Vitamin C is needed for the hydroxylation of proline during collagen synthesis., Please rate this question:, , Discuss and give feedback, , Next question, , Collagen, Collagen is one of the most important structural proteins within the extracellular matrix, collagen, together with components such as elastin and glycosaminoglycans determine the properties of all, tissues., , , , , , , Composed of 3 polypeptide strands that are woven into a helix, usually a combination of, glycine with either proline or hydroxyproline plus another amino acid, Numerous hydrogen bonds exist within molecule to provide additional strength, Many sub types but commonest sub type is I (90% of bodily collagen), tissues with increased, levels of flexibility have increased levels of type III collagen, Vitamin c is important in establishing cross links, Synthesised by fibroblasts, , Collagen Diseases, Disorders of collagen range from relatively common, acquired defects (typically aging), through to, rarer congenital disorders. The latter are exemplified by conditions such as osteogenesis imperfecta, and Ehlers Danlos syndromes., Osteogenesis imperfecta:, -8 Subtypes
Page 34 :
-Defect of type I collagen, -In type I the collagen is normal quality but insufficient quantity, -Type II- poor quantity and quality, -Type III- Collagen poorly formed, normal quantity, -Type IV- Sufficient quantity but poor quality, Patients have bones which fracture easily, loose joint and multiple other defects depending upon, which sub type they suffer from., Ehlers Danlos:, -Multiple sub types, -Abnormality of types 1 and 3 collagen, -Patients have features of hypermobility., -Individuals are prone to joint dislocations and pelvic organ prolapse. In addition to many other, diseases related to connective tissue defects., Next question
Page 35 :
A 56 year old man has long standing chronic pancreatitis and develops pancreatic insufficiency., Which of the following will be absorbed normally?, , Fat, , Protein, , Folic acid, , Vitamin B12, , None of the above, , Pancreatic lipase is required for digestion of fat, Proteases facilitate protein and B12 absorption., Folate digestion is independent of the pancreas., Please rate this question:, , Discuss and give feedback, , Next question, , Pancreas exocrine physiology, Composition of pancreatic secretions, Pancreatic secretions are usually 1000-1500ml per 24 hours and have a pH of 8., Secretion, , Enzymic, , Source, , Substances secreted, , Acinar cells, , Trypsinogen, Procarboxylase, Amylase, Elastase
Page 36 :
Aqueous, , Ductal and, Centroacinar cells, , Sodium, Bicarbonate, Water, Potassium, Chloride, NB: Sodium and potassium reflect their plasma levels; chloride, and bicarbonate vary with flow rate, , Regulation, The cephalic and gastric phases (neuronal and physical) are less important in regulating the, pancreatic secretions. The effect of digested material in the small bowel stimulates CCK release and, ACh which stimulate acinar and ductal cells. Of these CCK is the most potent stimulus. In the case, of the ductal cells these are potently stimulated by secretin which is released by the S cells of the, duodenum. This results in an increase in bicarbonate., Enzyme activation, Trypsinogen is converted via enterokinase to active trypsin in the duodenum. Trypsin then activates, the other inactive enzymes, Next question
Page 37 :
A 56 year old male presents to the acute surgical take with severe abdominal pain. He is normally fit, and well. He has no malignancy. The biochemistry laboratory contacts the ward urgently, his, corrected calcium result is 3.6 mmol/l. What is the medication of choice to treat this abnormality?, , IV Pamidronate, , Oral Alendronate, , Dexamethasone, , Vitamin D, , Resonium salts, , Theme from January 2012 exam, IV Pamidronate is the drug of choice as it most effective and has long lasting effects. Calcitonin, would need to be given with another agent, to ensure that the hypercalcaemia is treated once its, short term effects wear off. IV zoledronate is preferred in scenarios associated with malignancy., Please rate this question:, , Discuss and give feedback, , Next question, , Management of hypercalcaemia, , , , , Free Ca is affected by pH (increased in acidosis) and plasma albumin concentration, ECG changes include: Shortening of QTc interval, Urgent management is indicated if:, , Calcium > 3.5 mmol/l, Reduced consciousness, Severe abdominal pain, Pre renal failure
Page 38 :
Management:, , , , , , Airway Breathing Circulation, Intravenous fluid resuscitation with 3-6L of 0.9% Normal saline in 24 hours, Concurrent administration of calcitonin will also help lower calcium levels, Medical therapy (usually if Corrected calcium >3.0mmol/l), , Bisphosphonates, , , , , Analogues of pryrophosphate, Prevent osteoclast attachment to bone matrix and interfere with osteoclast activity, Inhibit bone resorption., , Agents, Drug, , Side effects, , Notes, , IV Pamidronate, , pyrexia, leucopaenia, , Most potent agent, , IV Zoledronate, , response lasts 30 days, , Used for malignancy associated hypercalcaemia, , Calcitonin, , , Quickest onset of action however short duration (tachyphylaxis) therefore only given with a, second agent., , Prednisolone, , , May be given in hypercalcaemia related to sarcoidosis, myeloma or vitamin D intoxication., Next question
Page 39 :
An over enthusiastic medical student decides to ask you questions about ECGs. Rather than, admitting your dwindling knowledge on this topic, you bravely attempt to answer her questions! One, question is what segment of the ECG represents ventricular repolarization?, , QRS complex, , Q-T interval, , P wave, , T wave, , S-T segment, , Theme from January 2012 exam, The T wave represents ventricular repolarization. The common sense approach to remembering, this, is to acknowledge that ventricular repolarization is the last phase of cardiac contraction and, should therefore correspond the the last part of the QRS complex., Please rate this question:, , Discuss and give feedback, , Next question, , The normal ECG
Page 40 :
Image sourced from Wikipedia, , P wave, , , , , Represents the wave of depolarization that spreads from the SA node throughout the atria, Lasts 0.08 to 0.1 seconds (80-100 ms), The isoelectric period after the P wave represents the time in which the impulse is traveling, within the AV node, , P-R interval, , , , , Time from the onset of the P wave to the beginning of the QRS complex, Ranges from 0.12 to 0.20 seconds in duration, Represents the time between the onset of atrial depolarization and the onset of ventricular, depolarization, , QRS complex, , , , Represents ventricular depolarization, Duration of the QRS complex is normally 0.06 to 0.1 seconds
Page 41 :
ST segment, , , , Isoelectric period following the QRS, Represents period which the entire ventricle is depolarized and roughly corresponds to the, plateau phase of the ventricular action potential, , T wave, , , , Represents ventricular repolarization and is longer in duration than depolarization, A small positive U wave may follow the T wave which represents the last remnants of, ventricular repolarization., , Q-T interval, , , , , , , Represents the time for both ventricular depolarization and repolarization to occur, and, therefore roughly estimates the duration of an average ventricular action potential., Interval ranges from 0.2 to 0.4 seconds depending upon heart rate., At high heart rates, ventricular action potentials shorten in duration, which decreases the Q-T, interval. Therefore the Q-T interval is expressed as a "corrected Q-T (QTc)" by taking the QT interval and dividing it by the square root of the R-R interval (interval between ventricular, depolarizations). This allows an assessment of the Q-T interval that is independent of heart, rate., Normal corrected Q-Tc interval is less than 0.44 seconds., Next question
Page 42 :
The oxygen-haemoglobin dissociation curve is shifted to the right in which of the following, scenarios?, , Hypothermia, , Respiratory alkalosis, , Low altitude, , Decreased 2,3-DPG in transfused red cells, , Chronic iron deficiency anaemia, Mnemonic to remember causes of right shift of the oxygen dissociation curve:, CADET face RIGHT, C O2, A cidosis, 2,3-DPG, E xercise, T emperature, The curve is shifted to the right when there is an increased oxygen requirement by the tissue. This, includes:, , , , , Increased temperature, Acidosis, Increased DPG:, , DPG is found in erythrocytes and is increased during glycolysis. It binds to the Hb molecule, thereby, releasing oxygen to tissues. DPG is increased in conditions associated with poor oxygen delivery to, tissues, such as anaemia and high altitude., Please rate this question:, , Discuss and give feedback, , Next question, , Oxygen Transport
Page 43 :
Oxygen transport, Almost all oxygen is transported within erythrocytes. It has limited solubility and only 1% is carried as, solution. Therefore the amount of oxygen transported will depend upon haemoglobin concentration, and its degree of saturation., Haemoglobin, Globular protein composed of 4 subunits. Haem consists of a protoporphyrin ring surrounding an, iron atom in its ferrous state. The iron can form two additional bonds; one with oxygen and the other, with a polypeptide chain. There are two alpha and two beta subunits to this polypeptide chain in an, adult and together these form globin. Globin cannot bind oxygen but is able to bind to carbon dioxide, and hydrogen ions, the beta chains are able to bind to 2,3 diphosphoglycerate. The oxygenation of, haemoglobin is a reversible reaction. The molecular shape of haemoglobin is such that binding of, one oxygen molecule facilitates the binding of subsequent molecules., Oxygen dissociation curve, , , , The oxygen dissociation curve describes the relationship between the percentage of, saturated haemoglobin and partial pressure of oxygen in the blood. It is not affected by, haemoglobin concentration., Chronic anaemia causes 2, 3 DPG levels to increase, hence shifting the curve to the right, , Haldane effect, , , Shifts to left = for given oxygen tension there is increased saturation of Hb with oxygen i.e., Decreased oxygen delivery to tissues, , Bohr effect, , , Shifts to right = for given oxygen tension there is reduced saturation of Hb with oxygen i.e., Enhanced oxygen delivery to tissues
Page 44 :
Image sourced from Wikipedia, , Shifts to Left = Lower oxygen delivery, , , , , , , HbF, methaemoglobin, carboxyhaemoglobin, low [H+] (alkali), low pCO2, low 2,3-DPG, low temperature, , Shifts to Right = Raised oxygen, delivery, , , , , , raised [H+] (acidic), raised pCO2, raised 2,3-DPG*, raised temperature, , *2,3-diphosphoglycerate, Next question
Page 45 :
A 45 year old man undergoes a sub total colectomy and formation of end ileostomy. What is the, most likely sodium content per litre of ileostomy fluid?, , 120 mmol, , 60 mmol, , 20 mmol, , 210 mmol, , 180 mmol, , Investigators in the 1960's dehydrated and measured the sodium content of ileostomy effluent and, determined this concentration. Not an experiment many would care to repeat!, Please rate this question:, , Discuss and give feedback, , Next question, , Gastrointestinal secretions, Up to 7 litres of gastrointestinal secretions enter the lumen of the GI tract in a 24 hour period. The, absorptive function of the small bowel is such that by the time a formed stool is created, it will, contain, on average 200ml water., The common secretions together with their approximate volumes are demonstrated below:, , Origin of secretion, , Volume in ml / 24 hour period, , Na +mmol/L, , K+mmol/L, , Cl-mmol/L, , HCO3
Page 46 :
Origin of secretion, , Volume in ml / 24 hour period, , Na +mmol/L, , K+mmol/L, , Cl-mmol/L, , HCO3, , Salivary glands, , 1500, , 10, , 26, , 10, , 30, , Stomach, , 1500, , 60, , 10, , 130, , Duodenum, , 100-2000, , 140, , 80, , 80, , Pancreas, , 1000, , 140, , 5, , 70, , 115, , Bile, , 50-800, , 145, , 50, , 100, , 35, , Jejunum/ileum, , 3000, , 140, , 50, , 104, , 30, , Colon, , 100, , 60, , 30, , 40, , The regulation of these secretions is dependent upon location. In the salivary glands a complex, interaction of flow rate governed by the autonomic nervous system. The exact composition of, sodium and potassium is regulated by aldosterone. In the stomach hormones such as gastrin play a, role and feedback is both endocrine and neurologically mediated (vagus). In the duodenum CCK is, released in response to duodenal distension and this causes contraction of the gallbladder and, release of bile., Pancreatic secretions are affected by somatostatin. The secretions in the small bowel are affected, by the osmolality of the lumenal contents. This is in part due to the tightness of cellular junctions and, in this regard the jejunum is more permeable than the ileum. The practical implication of this is that if, an individual has an extensive intestinal resection and a high output, proximally sited stoma then, administration of hypotonic rather than isotonic solutions will result in worsening of electrolyte, disturbances as electrolyte rich secretions will enter the jejunum., In some individuals a colectomy or similar procedure results in formation of an end or loop ileostomy., Ileostomies typically lose between 500 and 1000ml over a 24 hour period and patients with high, output ileostomies can rapidly become dehydrated. Ileostomy effluent typically contains 126mmol/L, of sodium and 22mmol/L of potassium. Knowledge of this fluid composition should guide fluid, prescribing in replacing losses., Next question
Page 47 :
A 73 year old lady is admitted for a laparoscopic cholecystectomy. During her pre-operative, assessment it is noted that she is receiving furosemide for the treatment of hypertension. Where is, the site of action of this diuretic?, , Proximal convoluted tubule, , Descending limb of the loop of Henle, , Ascending limb of the loop of Henle, , Distal convoluted tubule, , Collecting ducts, Action of furosemide = ascending limb of the loop of Henle, , Furosemide and bumetanide are loop diuretics that act by inhibiting the Na-K-Cl cotransporter in the, thick ascending limb of the loop of Henle, reducing the absorption of NaCl., Please rate this question:, , Discuss and give feedback, , Next question, , Diuretic agents, The diuretic drugs are divided into three major classes, which are distinguished according to the site, at which they impair sodium reabsorption: loop diuretics in the thick ascending loop of Henle,, thiazide type diuretics in the distal tubule and connecting segment; and potassium sparing diuretics, in the aldosterone - sensitive principal cells in the cortical collecting tubule., In the kidney, sodium is reabsorbed through Na+/ K+ ATPase pumps located on the basolateral, membrane. These pumps return reabsorbed sodium to the circulation and maintain low intracellular, sodium levels. This latter effect ensures a constant concentration gradient.
Page 48 :
Physiological effects of commonly used diuretics, , Site of action, , Diuretic, , Carrier or channel, inhibited, , Percentage of filtered sodium, excreted, , Ascending limb of loop of, Henle, , Frusemide, , Na+/K+ 2Cl - carrier, , Up to 25%, , Distal tubule and connecting, segment, , Thiazides, , Na+Cl- carrier, , Between 3 and 5%, , Cortical collecting tubule, , Spironolactone, , Na+/K+ ATP ase pump, , Between 1 and 2%, Next question
Page 49 :
Which of the following physiological changes do not occur following tracheostomy?, , Alveolar ventilation is increased., , Anatomical dead space is reduced by 50%., , Work of breathing is increased., , Proportion of ciliated epithelial cells in the trachea may decrease., , Splinting of the larynx may lead to swallowing difficulties., , Work of breathing is decreased which is one reasons it is popular option for weaning ventilated, patients. Humidified air in this setting helps to reduce the viscosity of mucous that forms., Please rate this question:, , Discuss and give feedback, , Next question, , Trachea, Trachea, , Location, , C6 vertebra to the upper border of T5 vertebra (bifurcation), , Arterial and venous supply, , Inferior thyroid arteries and the thyroid venous plexus., , Nerve, , Branches of vagus, sympathetic and the recurrent nerves, , Relations in the neck, , Anterior(Superior to, inferior), , , , , , , , , Isthmus of the thyroid gland, Inferior thyroid veins, Arteria thyroidea ima (when that vessel exists), Sternothyroid, Sternohyoid, Cervical fascia
Page 50 :
, , Posterior, Laterally, , Anastomosing branches between the anterior jugular, veins, , Oesophagus., , , , , , Common carotid arteries, Right and left lobes of the thyroid gland, Inferior thyroid arteries, Recurrent laryngeal nerves, , Relations in the thorax, Anterior, , , Manubrium, the remains of the thymus, the aortic arch, left common carotid arteries, and the, deep cardiac plexus, , Lateral, , , In the superior mediastinum, on the right side is the pleura and right vagus; on its left side, are the left recurrent nerve, the aortic arch, and the left common carotid and subclavian, arteries., Next question
Page 52 :
Image sourced from Wikipedia, , Please rate this question:, , Discuss and give feedback, , Next question, , Renin, Renin is secreted by juxtaglomerular cells and hydrolyses angiotensinogen to produce angiotensin I
Page 54 :
A 28 year old man is shot in the abdomen and haemorrhages. Which of the following substances will, produce vasoconstriction in response to this process?, , Renin, , Angiotensin I, , Angiotensin II, , Aldosterone, , None of the above, , Theme from April 2014 exam, Renin does not cause vasoconstriction. Angiotensin I is biologically inactive. Aldosterone will, increase blood pressure but does not have direct vasospastic effects., Please rate this question:, , Discuss and give feedback, , Next question, , Shock, , , , , , , , , Shock occurs when there is insufficient tissue perfusion., The pathophysiology of shock is an important surgical topic and may be divided into the, following aetiological groups:, Septic, Haemorrhagic, Neurogenic, Cardiogenic, Anaphylactic, , Septic shock, Septic shock is a major problem and those patients with severe sepsis have a mortality rate in, excess of 40%. In those who are admitted to intensive care mortality ranges from 6% with no organ, failure to 65% in those with 4 organ failure., Sepsis is defined as an infection that triggers a particular Systemic Inflammatory Response, Syndrome (SIRS). This is characterised by body temperature outside 36 oC - 38 o C, HR >90, beats/min, respiratory rate >20/min, WBC count >12,000/mm 3 or < 4,000/mm 3, altered mental state, or hyperglycaemia (in absence of diabetes).
Page 55 :
Patients with infections and two or more elements of SIRS meet the diagnostic criteria for sepsis., Those with organ failure have severe sepsis and those with refractory hypotension -septic shock., During the septic process there is marked activation of the immune system with extensive cytokine, release. This may be coupled with or triggered by systemic circulation of bacterial toxins. These all, cause endothelial cell damage and neutrophil adhesion. The overall hallmarks are thus those, ofexcessive inflammation, coagulation and fibrinolytic suppression., The surviving sepsis campaign (2012) highlights the following key areas for attention:, , , , , Prompt administration of antibiotics to cover all likely pathogens coupled with a rigorous, search for the source of infection., Haemodynamic stabilisation. Many patients are hypovolaemic and require aggressive fluid, administration. Aim for CVP 8-12 cm H2O, MAP >65mmHg., Modulation of the septic response. This includes manoeuvres to counteract the changes and, includes measures such as tight glycaemic control. The routine use of steroids is not, advised., , In surgical patients, the main groups with septic shock include those with anastomotic leaks,, abscesses and extensive superficial infections such as necrotising fasciitis. When performing, surgery the aim should be to undertake the minimum necessary to restore physiology. These, patients do not fare well with prolonged surgery. Definitive surgery can be more safely undertaken, when physiology is restored and clotting in particular has been normalised., Haemorrhagic shock, The average adult blood volume comprises 7% of body weight. Thus in the 70 Kg adult this will, equate to 5 litres. This changes in children (8-9% body weight) and is slightly lower in the elderly., The table below outlines the 4 major classes of haemorrhagic shock and their associated, physiological sequelae:, , Parameter, , Class I, , Class II, , Class III, , Class IV, , Blood loss ml, , <750ml, , 750-1500ml, , 1500-2000ml, , >2000ml, , Blood loss %, , <15%, , 15-30%, , 30-40%, , >40%, , Pulse rate, , <100, , >100, , >120, , >140, , Blood pressure, , Normal, , Normal, , Decreased, , Decreased
Page 56 :
Parameter, , Class I, , Class II, , Class III, , Class IV, , Respiratory rate, , 14-20, , 20-30, , 30-40, , >35, , Urine output, , >30ml, , 20-30ml, , 5-15ml, , <5ml, , Symptoms, , Normal, , Anxious, , Confused, , Lethargic, , Decreasing blood pressure during haemorrhagic shock causes organ hypoperfusion and relative, myocardial ischaemia. The cardiac index gives a numerical value for tissue oxygen delivery and is, given by the equation: Cardiac index= Cardiac output/ body surface area. Where Hb is, haemoglobin concentration in blood and SaO2 the saturation and PaO2 the partial pressure of, oxygen. Detailed knowledge of this equation is required for the MRCS Viva but not for part A,, although you should understand the principle., In patients suffering from trauma the most likely cause of shock is haemorrhage. However, the, following may also be the cause or occur concomitantly:, , , , , , , Tension pneumothorax, Spinal cord injury, Myocardial contusion, Cardiac tamponade, , When assessing trauma patients it is worth remembering that in order to generate a palpable, femoral pulse an arterial pressure of >65mmHg is required., Once bleeding is controlled and circulating volume normalised the levels of transfusion should be to, maintain a Hb of 7-8 in those with no risk factors for tissue hypoxia and Hb 10 for those who have, such risk factors., Neurogenic shock, This occurs most often following a spinal cord transection, usually at a high level. There is, resultant interruption of the autonomic nervous system. The result is either decreased sympathetic, tone or increased parasympathetic tone, the effect of which is a decrease in peripheral vascular, resistance mediated by marked vasodilation., This results in decreased preload and thus decreased cardiac output (Starlings law). There is, decreased peripheral tissue perfusion and shock is thus produced. In contrast with many other types, of shock peripheral vasoconstrictors are used to return vascular tone to normal., Cardiogenic shock, In medical patients the main cause is ischaemic heart disease. In the traumatic setting direct, myocardial trauma or contusion is more likely. Evidence of ECG changes and overlying sternal
Page 57 :
fractures or contusions should raise the suspicion of injury. Treatment is largely supportive and, transthoracic echocardiography should be used to determine evidence of pericardial fluid or direct, myocardial injury. The measurement of troponin levels in trauma patients may be undertaken but, they are less useful in delineating the extent of myocardial trauma than following MI., When cardiac injury is of a blunt nature and is associated with cardiogenic shock the right side of the, heart is the most likely site of injury with chamber and or valve rupture. These patients require, surgery to repair these defects and will require cardiopulmonary bypass to achieve this. Some may, require intra aortic balloon pump as a bridge to surgery., Anaphylactic shock, Anaphylaxis may be defined as a severe, life-threatening, generalised or systemic, hypersensitivity reaction., Anaphylaxis is one of the few times when you would not have time to look up the dose of a, medication. The Resuscitation Council guidelines on anaphylaxis have recently been updated., Adrenaline is by far the most important drug in anaphylaxis and should be given as soon as, possible. The recommended doses for adrenaline, hydrocortisone and chlorpheniramine are as, follows:, , Adrenaline, , Hydrocortisone, , Chlorpheniramine, , < 6 months, , 150 mcg (0.15ml 1 in 1,000), , 25 mg, , 250 mcg/kg, , 6 months - 6 years, , 150 mcg (0.15ml 1 in 1,000), , 50 mg, , 2.5 mg, , 6-12 years, , 300 mcg (0.3ml 1 in 1,000), , 100 mg, , 5 mg, , Adult and child 12 years, , 500 mcg (0.5ml 1 in 1,000), , 200 mg, , 10 mg, , Adrenaline can be repeated every 5 minutes if necessary. The best site for IM injection is the, anterolateral aspect of the middle third of the thigh., Common identified causes of anaphylaxis, , , , , food (e.g. Nuts) - the most common cause in children, drugs, venom (e.g. Wasp sting), Next question
Page 58 :
A 43 year old lady is recovering on the intensive care unit following a Whipples procedure. She has, a central venous line in situ. Which of the following will lead to the "y" descent on the waveform, trace?, , Ventricular contraction, , Emptying of the right atrium, , Emptying of the right ventricle, , Opening of the pulmonary valve, , Cardiac tamponade, JVP, 3 Upward deflections and 2 downward deflections, Upward deflections, , , , , a wave = atrial contraction, c wave = ventricular contraction, v wave = atrial venous filling, , Downward deflections, , , , x wave = atrium relaxes and tricuspid valve moves down, y wave = ventricular filling, , Theme from January 2012, The 'y' descent represents the emptying of the atrium and the filling of the right ventricle., Please rate this question:, , Discuss and give feedback, , Next question, , Cardiac physiology
Page 59 :
, , , , , The heart has four chambers ejecting blood into both low pressure and high pressure, systems., The pumps generate pressures of between 0-25mmHg on the right side and 0-120 mmHg on, the left., At rest diastole comprises 2/3 of the cardiac cycle., The product of the frequency of heart rate and stroke volume combine to give the cardiac, output which is typically 5-6L per minute., , Detailed descriptions of the various waveforms are often not a feature of MRCS A (although they are, on the syllabus). However, they are a very popular topic for surgical physiology in the MRCS B, exam., Electrical properties, , , , , , , Intrinsic myogenic rhythm within cardiac myocytes means that even the denervated heart is, capable of contraction., In the normal situation the cardiac impulse is generated in the sino atrial node in the right, atrium and conveyed to the ventricles via the atrioventricular node., The sino atrial node is also capable of spontaneous discharge and in the absence of, background vagal tone will typically discharge around 100x per minute. Hence the higher, resting heart rate found in cardiac transplant cases. In the SA and AV nodes the resting, membrane potential is lower than in surrounding cardiac cells and will slowly depolarise from, -70mV to around -50mV at which point an action potential is generated., Differences in the depolarisation slopes between SA and AV nodes help to explain why the, SA node will depolarise first. The cells have a refractory period during which they cannot be, re-stimulated and this period allows for adequate ventricular filling. In pathological, tachycardic states this time period is overridden and inadequate ventricular filling may then, occur, cardiac output falls and syncope may ensue., , Parasympathetic fibres project to the heart via the vagus and will release acetylcholine. Sympathetic, fibres release nor adrenaline and circulating adrenaline comes from the adrenal medulla., Noradrenaline binds to β 1 receptors in the SA node and increases the rate of pacemaker potential, depolarisation., Cardiac cycle
Page 60 :
Image sourced from Wikipedia, , , , Mid diastole: AV valves open. Ventricles hold 80% of final volume. Outflow valves shut., Aortic pressure is high., , , , Late diastole: Atria contract. Ventricles receive 20% to complete filling. Typical end diastolic, volume 130-160ml., , , , Early systole: AV valves shut. Ventricular pressure rises. Isovolumetric ventricular, contraction. AV Valves bulge into atria (c-wave). Aortic and pulmonary pressure exceededblood is ejected. Shortening of ventricles pulls atria downwards and drops intra atrial, pressure (x-descent)., , , , Late systole: Ventricular muscles relax and ventricular pressures drop. Although ventricular, pressure drops the aortic pressure remains constant owing to peripheral vascular resistance, and elastic property of the aorta. Brief period of retrograde flow that occurs in aortic recoil, shuts the aortic valve. Ventricles will contain 60ml end systolic volume. The average stroke, volume is 70ml (i.e. Volume ejected).
Page 61 :
, , Early diastole: All valves are closed. Isovolumetric ventricular relaxation occurs. Pressure, wave associated with closure of the aortic valve increases aortic pressure. The pressure dip, before this rise can be seen on arterial waveforms and is called the incisura. During systole, the atrial pressure increases such that it is now above zero (v- wave). Eventually atrial, pressure exceed ventricular pressure and AV valves open - atria empty passively into, ventricles and atrial pressure falls (y -descent ), , The negative atrial pressures are of clinical importance as they can allow air embolization to occur if, the neck veins are exposed to air. This patient positioning is important in head and neck surgery to, avoid this occurrence if veins are inadvertently cut, or during CVP line insertion., Mechanical properties, , , , Preload = end diastolic volume, Afterload = aortic pressure, , It is important to understand the principles of Laplace's law in surgery., , , , , It states that for hollow organs with a circular cross section, the total circumferential wall, tension depends upon the circumference of the wall, multiplied by the thickness of the wall, and on the wall tension., The total luminal pressure depends upon the cross sectional area of the lumen and the, transmural pressure. Transmural pressure is the internal pressure minus external pressure, and at equilibrium the total pressure must counterbalance each other., In terms of cardiac physiology the law explains that the rise in ventricular pressure that, occurs during the ejection phase is due to physical change in heart size. It also explains why, a dilated diseased heart will have impaired systolic function., , Starlings law, , , , Increase in end diastolic volume will produce larger stroke volume., This occurs up to a point beyond which cardiac fibres are excessively stretched and stroke, volume will fall once more. It is important for the regulation of cardiac output in cardiac, transplant patients who need to increase their cardiac output., , Baroreceptor reflexes, , , , , , , Baroreceptors located in aortic arch and carotid sinus., Aortic baroreceptor impulses travel via the vagus and from the carotid via the, glossopharyngeal nerve., They are stimulated by arterial stretch., Even at normal blood pressures they are tonically active., Increase in baroreceptor discharge causes:
Page 62 :
*Increased parasympathetic discharge to the SA node., *Decreased sympathetic discharge to ventricular muscle causing decreased contractility and fall in, stroke volume., *Decreased sympathetic discharge to venous system causing increased compliance., *Decreased peripheral arterial vascular resistance, Atrial stretch receptors, , , , , , , , Located in atria at junction between pulmonary veins and vena cava., Stimulated by atrial stretch and are thus low pressure sensors., Increased blood volume will cause increased parasympathetic activity., Very rapid infusion of blood will result in increase in heart rate mediated via atrial receptors:, theBainbridge reflex., Decreases in receptor stimulation results in increased sympathetic activity this will decrease, renal blood flow-decreases GFR-decreases urinary sodium excretion-renin secretion by, juxtaglomerular apparatus-Increase in angiotensin II., Increased atrial stretch will also result in increased release of atrial natriuretic peptide., Next question
Page 63 :
Which of the following are not characteristic features of central chemoreceptors in the control of, ventilation?, , They are located in the medulla oblongata, , They are stimulated primarily by venous hypercapnia, , They are relatively insensitive to hypoxia, , They may be affected by changes in the pH of CSF, , During acute hypercapnia the carotid receptors will be stimulated first, , Theme from April 2014 exam, They are stimulated by arterial carbon dioxide. It takes longer to equilibrate than the peripheral, chemoreceptors located in the carotid. They are less sensitive to acidity due to the blood brain, barrier., Please rate this question:, , Discuss and give feedback, , Next question, , Control of ventilation, , , , , Control of ventilation is coordinated by the respiratory centres, chemoreceptors, lung, receptors and muscles., Automatic, involuntary control of respiration occurs from the medulla., The respiratory centres control the respiratory rate and the depth of respiration., , Respiratory centres, , Medullary, respiratory centre, , Inspiratory and expiratory neurones. Has ventral group which controls, forced voluntary expiration and the dorsal group controls inspiration., Depressed by opiates., , Apneustic centre, , Lower pons, Stimulates inspiration - activates and prolongs inhalation
Page 64 :
Overridden by pneumotaxic control to end inspiration, , Pneumotaxic centre, , Upper pons, inhibits inspiration at a certain point. Fine tunes the, respiratory rate., , Ventillatory variables, , , , , , Levels of pCO2 most important in ventilation control, Levels of O2 are less important., Peripheral chemoreceptors: located in the bifurcation of carotid arteries and arch of the, aorta. They respond to changes in reduced pO2, increased H+ and increased pCO2 in, ARTERIAL BLOOD., Central chemoreceptors: located in the medulla. Respond to increased H+ in BRAIN, INTERSTITIAL FLUID to increase ventilation. NB the central receptors are NOT influenced, by O2levels., , Lung receptors include:, , , , , Stretch receptors: respond to lung stretching causing a reduced respiratory rate, Irritant receptors: respond to smoke etc causing bronchospasm, J (juxtacapillary) receptors, Next question
Page 65 :
A 32 year old man has a glomerular filtration rate of 110ml / minute at a systolic blood pressure of, 120/80. If his blood pressure were to fall to 100/70 what would glomerular filtration rate be?, , 110ml / minute, , 100ml/ minute, , 55ml/ minute, , 25ml/ minute, , 75ml/ minute, , Theme from April 2014 exam, The proposed drop in blood pressure falls within the range within which the kidney autoregulates its, blood supply. GFR will therefore remain unchanged., Please rate this question:, , Discuss and give feedback, , Next question, , Renal Physiology, Overview, , , , , Each nephron is supplied with blood from an afferent arteriole that opens onto the glomerular, capillary bed., Blood then flows to an efferent arteriole, supplying the peritubular capillaries and medullary, vasa recta., The kidney receives up to 25% of resting cardiac output., , Control of blood flow, , , , The kidney is able to autoregulate its blood flow between systolic pressures of 80- 180mmHg, so there is little variation in renal blood flow., This is achieved by myogenic control of arteriolar tone, both sympathetic input and hormonal, signals (e.g. renin) are responsible.
Page 66 :
Glomerular structure and function, , , , , , , , , Blood inside the glomerulus has considerable hydrostatic pressure., The basement membrane has pores that will allow free diffusion of smaller solutes, larger, negatively charged molecules such as albumin are unable to cross., The glomerular filtration rate (GFR) is equal to the concentration of a solute in the urine,, times the volume of urine produced per minute, divided by the plasma concentration, (assuming that the solute is freely diffused e.g. inulin)., In clinical practice creatinine is used because it is subjected to very little proximal tubular, secretion., Although subject to variability, the typical GFR is 125ml per minute., Glomerular filtration rate = Total volume of plasma per unit time leaving the capillaries and, entering the bowman's capsule, Renal clearance = volume plasma from which a substance is removed per minute by the, kidneys, , Substances used to measure GFR have the following features:, 1. Inert, 2. Free filtration from the plasma at the glomerulus (not protein bound), 3. Not absorbed or secreted at the tubules, 4. Plasma concentration constant during urine collection, Examples: inulin, creatinine, GFR = urine concentration (mmol/l) x urine volume (ml/min), -------------------------------------------------------------------------plasma concentration (mmol/l), , , , , The clearance of a substance is dependent not only on its diffusivity across the basement, membrane but also subsequent tubular secretion and / or reabsorption., So glucose which is freely filtered across the basement membrane is usually reabsorbed, from tubules giving a clearance of zero., , Tubular function, , , , , , , Reabsorption and secretion of substances occurs in the tubules., In the proximal tubule substrates such as glucose, amino acids and phosphate are cotransported with sodium across the semi permeable membrane., Up to two thirds of filtered water is reabsorbed in the proximal tubules., This will lead to increase in urea concentration in the distal tubule allowing for its increased, diffusion., Substances to be secreted into the tubules are taken up from the peritubular blood by tubular, cells.
Page 67 :
, , , Solutes such as paraaminohippuric acid are cleared with a single passage through the, kidneys and this is why it is used to measure renal plasma flow. Ions such as calcium and, phosphate will have a tubular reabsorption that is influenced by plasma PTH levels., Potassium may be both secreted and re-absorbed and is co-exchanged with sodium., , Loop of Henle, , , , , , , , , , Approximately 60 litres of water containing 9000mmol sodium enters the descending limb of, the loop of Henle in 24 hours., Loops from the juxtamedullary nephrons run deep into the medulla., The osmolarity of fluid changes and is greatest at the tip of the papilla., The thin ascending limb is impermeable to water, but highly permeable to sodium and, chloride ions., This loss means that at the beginning of the thick ascending limb the fluid is hypo osmotic, compared with adjacent interstitial fluid., In the thick ascending limb the reabsorption of sodium and chloride ions occurs by both, facilitated and passive diffusion pathways., The loops of Henle are co-located with vasa recta, these will have similar solute, compositions to the surrounding extracellular fluid so preventing the diffusion and, subsequent removal of this hypertonic fluid., The energy dependent reabsorption of sodium and chloride in the thick ascending limb helps, to maintain this osmotic gradient., , Next question
Page 68 :
Which of the following does not stimulate insulin release?, , Gastrin, , Atenolol, , Protein, , Secretin, , Vagal cholinergic action, , Beta blockers inhibit the release of insulin., Stimulation of insulin release:, , , , , , , , , Glucose, Amino acid, Vagal cholinergic, Secretin/Gastrin/CCK, Fatty acids, Beta adrenergic drugs, , Please rate this question:, , Discuss and give feedback, , Next question, , Insulin, Insulin is a peptide hormone, produced by beta cells of the pancreas, and is central to regulating, carbohydrate and fat metabolism in the body. Insulin causes cells in the liver, skeletal muscles, and, fat tissue to absorb glucose from the blood. In the liver and skeletal muscles, glucose is stored as, glycogen, and in fat cells (adipocytes) it is stored as triglycerides., Structure, The human insulin protein is composed of 51 amino acids, and has a molecular weight of 5808 Da. It, is a dimer of an A-chain and a B-chain, which are linked together by disulfide bonds., Synthesis
Page 69 :
Pro-insulin is formed by the rough endoplasmic reticulum in pancreatic beta cells. Then pro-insulin is, cleaved to form insulin and C-peptide. Insulin is stored in secretory granules and released in, response to Ca2+., Function, , , , , , Secreted in response to hyperglycaemia, Glucose utilisation and glycogen synthesis, Inhibits lipolysis, Reduces muscle protein loss, Next question
Page 70 :
A 63 year old female is referred to the surgical clinic with an iron deficiency anaemia. Her past, medical history includes a left hemi colectomy but no other co-morbidities. At what site is most, dietary iron absorbed?, , Stomach, , Duodenum, , Proximal ileum, , Distal ileum, , Colon, , Theme from April 2014 exam, Iron is best absorbed from the proximal small bowel (duodenum and jejunum) in the Fe 2+ state. Iron, is transported across the small bowel mucosa by a divalent membrane transporter protein (hence, the improved absorption of Fe 2+). The intestinal cells typically store the bound iron as ferritin. Cells, requiring iron will typically then absorb the complex as needed., Please rate this question:, , Discuss and give feedback, , Next question, , Iron metabolism, Absorption, , , , , , , , , , Transport, , Duodenum and upper jejunum, About 10% of dietary iron absorbed, Fe2+ (ferrous iron) much better absorbed than Fe3+ (ferric iron), Ferrous iron is oxidized to form ferric iron, which is combined with, apoferritin to form ferritin, Absorption is regulated according to body's need, Increased by vitamin C, gastric acid, Decreased by proton pump inhibitors, tetracycline, gastric achlorhydria,, tannin (found in tea), , In plasma as Fe3+ bound to transferrin
Page 72 :
Which of the following haemodynamic changes is not seen in hypovolaemic shock?, , Decreased cardiac output, , Increased heart rate, , Reduced left ventricle filling pressures, , Reduced blood pressure, , Reduced systemic vascular resistance, Cardiogenic Shock:, e.g. MI, valve abnormality, increased SVR (vasoconstriction in response to low BP), increased HR (sympathetic response), decreased cardiac output, decreased blood pressure, Hypovolaemic shock:, blood volume depletion, e.g. haemorrhage, vomiting, diarrhoea, dehydration, third-space losses during major operations, increased SVR, increased HR, decreased cardiac output, decreased blood pressure, Septic shock:, occurs when the peripheral vascular dilatation causes a fall in SVR, similar response may occur in anaphylactic shock, neurogenic shock, reduced SVR, increased HR, normal/increased cardiac output, decreased blood pressure, SVR will typically increase, Please rate this question:, , Discuss and give feedback, , Next question
Page 73 :
Shock, , , , , , , , , Shock occurs when there is insufficient tissue perfusion., The pathophysiology of shock is an important surgical topic and may be divided into the, following aetiological groups:, Septic, Haemorrhagic, Neurogenic, Cardiogenic, Anaphylactic, , Septic shock, Septic shock is a major problem and those patients with severe sepsis have a mortality rate in, excess of 40%. In those who are admitted to intensive care mortality ranges from 6% with no organ, failure to 65% in those with 4 organ failure., Sepsis is defined as an infection that triggers a particular Systemic Inflammatory Response, Syndrome (SIRS). This is characterised by body temperature outside 36 oC - 38 o C, HR >90, beats/min, respiratory rate >20/min, WBC count >12,000/mm 3 or < 4,000/mm 3, altered mental state, or hyperglycaemia (in absence of diabetes)., Patients with infections and two or more elements of SIRS meet the diagnostic criteria for sepsis., Those with organ failure have severe sepsis and those with refractory hypotension -septic shock., During the septic process there is marked activation of the immune system with extensive cytokine, release. This may be coupled with or triggered by systemic circulation of bacterial toxins. These all, cause endothelial cell damage and neutrophil adhesion. The overall hallmarks are thus those, ofexcessive inflammation, coagulation and fibrinolytic suppression., The surviving sepsis campaign (2012) highlights the following key areas for attention:, , , , , Prompt administration of antibiotics to cover all likely pathogens coupled with a rigorous, search for the source of infection., Haemodynamic stabilisation. Many patients are hypovolaemic and require aggressive fluid, administration. Aim for CVP 8-12 cm H2O, MAP >65mmHg., Modulation of the septic response. This includes manoeuvres to counteract the changes and, includes measures such as tight glycaemic control. The routine use of steroids is not, advised., , In surgical patients, the main groups with septic shock include those with anastomotic leaks,, abscesses and extensive superficial infections such as necrotising fasciitis. When performing, surgery the aim should be to undertake the minimum necessary to restore physiology. These, patients do not fare well with prolonged surgery. Definitive surgery can be more safely undertaken, when physiology is restored and clotting in particular has been normalised., Haemorrhagic shock, The average adult blood volume comprises 7% of body weight. Thus in the 70 Kg adult this will, equate to 5 litres. This changes in children (8-9% body weight) and is slightly lower in the elderly.
Page 74 :
The table below outlines the 4 major classes of haemorrhagic shock and their associated, physiological sequelae:, , Parameter, , Class I, , Class II, , Class III, , Class IV, , Blood loss ml, , <750ml, , 750-1500ml, , 1500-2000ml, , >2000ml, , Blood loss %, , <15%, , 15-30%, , 30-40%, , >40%, , Pulse rate, , <100, , >100, , >120, , >140, , Blood pressure, , Normal, , Normal, , Decreased, , Decreased, , Respiratory rate, , 14-20, , 20-30, , 30-40, , >35, , Urine output, , >30ml, , 20-30ml, , 5-15ml, , <5ml, , Symptoms, , Normal, , Anxious, , Confused, , Lethargic, , Decreasing blood pressure during haemorrhagic shock causes organ hypoperfusion and relative, myocardial ischaemia. The cardiac index gives a numerical value for tissue oxygen delivery and is, given by the equation: Cardiac index= Cardiac output/ body surface area. Where Hb is, haemoglobin concentration in blood and SaO2 the saturation and PaO2 the partial pressure of, oxygen. Detailed knowledge of this equation is required for the MRCS Viva but not for part A,, although you should understand the principle., In patients suffering from trauma the most likely cause of shock is haemorrhage. However, the, following may also be the cause or occur concomitantly:, , , , , , , Tension pneumothorax, Spinal cord injury, Myocardial contusion, Cardiac tamponade, , When assessing trauma patients it is worth remembering that in order to generate a palpable, femoral pulse an arterial pressure of >65mmHg is required.
Page 75 :
Once bleeding is controlled and circulating volume normalised the levels of transfusion should be to, maintain a Hb of 7-8 in those with no risk factors for tissue hypoxia and Hb 10 for those who have, such risk factors., Neurogenic shock, This occurs most often following a spinal cord transection, usually at a high level. There is, resultant interruption of the autonomic nervous system. The result is either decreased sympathetic, tone or increased parasympathetic tone, the effect of which is a decrease in peripheral vascular, resistance mediated by marked vasodilation., This results in decreased preload and thus decreased cardiac output (Starlings law). There is, decreased peripheral tissue perfusion and shock is thus produced. In contrast with many other types, of shock peripheral vasoconstrictors are used to return vascular tone to normal., Cardiogenic shock, In medical patients the main cause is ischaemic heart disease. In the traumatic setting direct, myocardial trauma or contusion is more likely. Evidence of ECG changes and overlying sternal, fractures or contusions should raise the suspicion of injury. Treatment is largely supportive and, transthoracic echocardiography should be used to determine evidence of pericardial fluid or direct, myocardial injury. The measurement of troponin levels in trauma patients may be undertaken but, they are less useful in delineating the extent of myocardial trauma than following MI., When cardiac injury is of a blunt nature and is associated with cardiogenic shock the right side of the, heart is the most likely site of injury with chamber and or valve rupture. These patients require, surgery to repair these defects and will require cardiopulmonary bypass to achieve this. Some may, require intra aortic balloon pump as a bridge to surgery., Anaphylactic shock, Anaphylaxis may be defined as a severe, life-threatening, generalised or systemic, hypersensitivity reaction., Anaphylaxis is one of the few times when you would not have time to look up the dose of a, medication. The Resuscitation Council guidelines on anaphylaxis have recently been updated., Adrenaline is by far the most important drug in anaphylaxis and should be given as soon as, possible. The recommended doses for adrenaline, hydrocortisone and chlorpheniramine are as, follows:, , Adrenaline, , Hydrocortisone, , Chlorpheniramine, , < 6 months, , 150 mcg (0.15ml 1 in 1,000), , 25 mg, , 250 mcg/kg, , 6 months - 6 years, , 150 mcg (0.15ml 1 in 1,000), , 50 mg, , 2.5 mg, , 6-12 years, , 300 mcg (0.3ml 1 in 1,000), , 100 mg, , 5 mg
Page 76 :
Adult and child 12 years, , 500 mcg (0.5ml 1 in 1,000), , 200 mg, , 10 mg, , Adrenaline can be repeated every 5 minutes if necessary. The best site for IM injection is the, anterolateral aspect of the middle third of the thigh., Common identified causes of anaphylaxis, , , , , food (e.g. Nuts) - the most common cause in children, drugs, venom (e.g. Wasp sting), Next question
Page 77 :
An otherwise fit 30 year old male donates 500ml of blood. Which of the processes outlined below is, most likely to occur?, , Reduction of urine output, , Activation of the renin angiotensin system, , Sweating, , Fall in mean arterial pressure, , Tachypnoea, , Theme from 2011 Exam, The loss of 500ml (assuming a 70 Kg male) will usually be sufficient to activate the renin angiotensin, system. It is unlikely that it would cause any other physiological disturbance., Please rate this question:, , Discuss and give feedback, , Next question, , Bleeding, The initial response to bleeding, even if of relatively small volume is generalised splanchnic, vasoconstriction mediated by activation of the sympathetic nervous system. This process of, vasoconstriction is usually sufficient to maintain renal perfusion and cardiac output if the volume of, blood lost is small. Over the following hours the circulating fluid volume is restored and normal, haemodynamics resume. Loss of greater volumes of blood will typically result in activation in the, renin angiotensin system (see diagram below).
Page 78 :
Image sourced from Wikipedia, , Where the source of bleeding ceases these physiological measures will restore circulating volume., Ongoing bleeding will result in haemorrhagic shock., Blood loss is typically quantified by the degree of shock produced as outlined below:, , Parameter, , Class I, , Class II, , Class III, , Class IV, , Blood loss ml, , <750ml, , 750-1500ml, , 1500-2000ml, , >2000ml, , Blood loss %, , <15%, , 15-30%, , 30-40%, , >40%, , Pulse rate, , <100, , >100, , >120, , >140, , Blood pressure, , Normal, , Normal, , Decreased, , Decreased, , Respiratory rate, , 14-20, , 20-30, , 30-40, , >35, , Urine output, , >30ml, , 20-30ml, , 5-15ml, , <5ml, , Symptoms, , Normal, , Anxious, , Confused, , Lethargic, Next question
Page 79 :
A 25 year old man is undergoing respiratory spirometry. He takes a maximal inspiration and, maximally exhales. Which of the following measurements will best illustrate this process?, , Functional residual capacity, , Vital capacity, , Inspiratory capacity, , Maximum voluntary ventilation, , Tidal volume, , Theme from April 2012 exam, Theme from April 2014 exam, The maximum voluntary ventilation is the maximal ventilation over the course of 1 minute., Please rate this question:, , Discuss and give feedback, , Next question, , Lung volumes, The diagram demonstrates lung volumes and capacities
Page 80 :
Image sourced from Wikipedia, , Definitions, , Tidal volume (TV), , , , , Is the volume of air inspired and expired during each, ventilatory cycle at rest., It is normally 500mls in males and 340mls in females., , Inspiratory reserve, volume (IRV), , , , Is the maximum volume of air that can be forcibly inhaled, following a normal inspiration. 3000mls., , Expiratory reserve, volume (ERV), , , , Is the maximum volume of air that can be forcibly exhaled, following a normal expiration. 1000mls., , Residual volume (RV), , , , Is that volume of air remaining in the lungs after a maximal, expiration., RV = FRC - ERV. 1500mls., , , , Functional residual, capacity (FRC), , , , , Vital capacity (VC), , , , , Total lung capacity, (TLC), , Forced vital capacity, (FVC), , , , Is the volume of air remaining in the lungs at the end of a, normal expiration., FRC = RV + ERV. 2500mls., Is the maximal volume of air that can be forcibly exhaled after, a maximal inspiration., VC = TV + IRV + ERV. 4500mls in males, 3500mls in, females., , , , Is the volume of air in the lungs at the end of a maximal, inspiration., TLC = FRC + TV + IRV = VC + RV. 5500-6000mls., , , , The volume of air that can be maximally forcefully exhaled., Next question
Page 81 :
Which of the following does not decrease the functional residual capacity?, , Obesity, , Pulmonary fibrosis, , Muscle relaxants, , Laparoscopic surgery, , Upright position, Increased FRC:, , , , , Erect position, Emphysema, Asthma, , Decreased FRC:, , , , , , , Pulmonary fibrosis, Laparoscopic surgery, Obesity, Abdominal swelling, Muscle relaxants, , When the patient is upright the diaphragm and abdominal organs put less pressure on the lung, bases, allowing for an increase in the functional residual capacity (FRC). Other causes of increased, FRC include:, , , , Emphysema, Asthma, , In addition to those listed above, causes of reduced FRC include:, , , , Abdominal swelling, Pulmonary oedema
Page 82 :
, , , Reduced muscle tone of the diaphragm, Age, , Please rate this question:, , Discuss and give feedback, , Next question, , Lung volumes, The diagram demonstrates lung volumes and capacities, , Image sourced from Wikipedia, , Definitions, , Tidal volume (TV), , , , , Is the volume of air inspired and expired during each, ventilatory cycle at rest., It is normally 500mls in males and 340mls in females., , Inspiratory reserve, volume (IRV), , , , Is the maximum volume of air that can be forcibly inhaled, following a normal inspiration. 3000mls., , Expiratory reserve, volume (ERV), , , , Is the maximum volume of air that can be forcibly exhaled, following a normal expiration. 1000mls., , Residual volume (RV), , , , Is that volume of air remaining in the lungs after a maximal, expiration.
Page 83 :
Functional residual, capacity (FRC), , , , RV = FRC - ERV. 1500mls., , , , Is the volume of air remaining in the lungs at the end of a, normal expiration., FRC = RV + ERV. 2500mls., , , , Vital capacity (VC), , , , , Total lung capacity, (TLC), , Forced vital capacity, (FVC), , , , Is the maximal volume of air that can be forcibly exhaled after, a maximal inspiration., VC = TV + IRV + ERV. 4500mls in males, 3500mls in, females., , , , Is the volume of air in the lungs at the end of a maximal, inspiration., TLC = FRC + TV + IRV = VC + RV. 5500-6000mls., , , , The volume of air that can be maximally forcefully exhaled., Next question
Page 85 :
, , , , , , Low BP, Hyponatraemia, Sympathetic nerve stimulation, Catecholamines, Erect posture, , Angiotensin, , , , , , ACE in lung converts angiotensin I → angiotensin II, Vasoconstriction leads to raised BP, Stimulates thirst, Stimulates aldosterone and ADH release, , Aldosterone, , , , Released by the zona glomerulosa in response to raised angiotensin II, potassium, and, ACTH levels, Causes retention of Na+ in exchange for K+/H+ in distal tubule, , Image sourced from Wikipedia, , Next question
Page 86 :
Secretions from which of the following will contain the highest levels of potassium?, , Rectum, , Small bowel, , Gallbladder, , Pancreas, , Stomach, , Theme from April 2014 Exam, The rectum has the potential to generate secretions rich in potassium. This is the rationale behind, administration of resins for hyperkalaemia and the development of hypokalaemia in patients with, villous adenoma of the rectum., Please rate this question:, , Discuss and give feedback, , Next question, , Potassium secretion -GI tract, Potassium secretions, , Salivary glands, , Variable may be up to 60mmol/L, , Stomach, , 10 mmol/L
Page 87 :
Bile, , 5 mmol/L, , Pancreas, , 4-5 mmol/L, , Small bowel, , 10 mmol/L, , Rectum, , 30 mmol/L, , The above table provides average figures only and the exact composition varies depending upon the, existence of disease, serum aldosterone levels and serum pH., A key point to remember for the exam is that gastric potassium secretions are low. Hypokalaemia, may occur in vomiting, usually as a result of renal wasting of potassium, not because of potassium, loss in vomit., Next question
Page 88 :
What is the typical stroke volume in a resting 70 Kg man?, , 10ml, , 150ml, , 125ml, , 45ml, , 70ml, , Theme from April 2014 Exam, Theme from September 2013 Exam, Stroke volumes range from 55-100ml., Please rate this question:, , Discuss and give feedback, , Next question, , Stroke volume-Cardiac physiology, The stroke volume equates to the volume of blood ejected from the ventricle during each cycle of, cardiac contraction. The volumes for both ventricles are typically equal and equate roughly to 70ml, for a 70Kg man. It is calculated by subtracting the end systolic volume from the end diastolic, volume., Factors affecting stroke volume, , , , , , Cardiac size, Contractility, Preload, Afterload, Next question
Page 89 :
A patient loses 1.6L of fresh blood from their abdominal drain. Which of the following will not, decrease?, , Cardiac output, , Renin secretion, , Firing of carotid baroreceptors, , Firing of aortic baroreceptors, , Blood pressure, , Renin secretion will increase as systemic hypotension will cause impairment of renal blood flow., Although the kidney can autoregulate its own blood flow over a range of systemic blood pressures a, loss of 1.6 L will usually produce an increase in renin secretion., Please rate this question:, , Discuss and give feedback, , Next question, , Shock, , , , , , , , , Shock occurs when there is insufficient tissue perfusion., The pathophysiology of shock is an important surgical topic and may be divided into the, following aetiological groups:, Septic, Haemorrhagic, Neurogenic, Cardiogenic, Anaphylactic, , Septic shock, Septic shock is a major problem and those patients with severe sepsis have a mortality rate in, excess of 40%. In those who are admitted to intensive care mortality ranges from 6% with no organ, failure to 65% in those with 4 organ failure., Sepsis is defined as an infection that triggers a particular Systemic Inflammatory Response, Syndrome (SIRS). This is characterised by body temperature outside 36 oC - 38 o C, HR >90, beats/min, respiratory rate >20/min, WBC count >12,000/mm 3 or < 4,000/mm 3, altered mental state, or hyperglycaemia (in absence of diabetes).
Page 90 :
Patients with infections and two or more elements of SIRS meet the diagnostic criteria for sepsis., Those with organ failure have severe sepsis and those with refractory hypotension -septic shock., During the septic process there is marked activation of the immune system with extensive cytokine, release. This may be coupled with or triggered by systemic circulation of bacterial toxins. These all, cause endothelial cell damage and neutrophil adhesion. The overall hallmarks are thus those, ofexcessive inflammation, coagulation and fibrinolytic suppression., The surviving sepsis campaign (2012) highlights the following key areas for attention:, , , , , Prompt administration of antibiotics to cover all likely pathogens coupled with a rigorous, search for the source of infection., Haemodynamic stabilisation. Many patients are hypovolaemic and require aggressive fluid, administration. Aim for CVP 8-12 cm H2O, MAP >65mmHg., Modulation of the septic response. This includes manoeuvres to counteract the changes and, includes measures such as tight glycaemic control. The routine use of steroids is not, advised., , In surgical patients, the main groups with septic shock include those with anastomotic leaks,, abscesses and extensive superficial infections such as necrotising fasciitis. When performing, surgery the aim should be to undertake the minimum necessary to restore physiology. These, patients do not fare well with prolonged surgery. Definitive surgery can be more safely undertaken, when physiology is restored and clotting in particular has been normalised., Haemorrhagic shock, The average adult blood volume comprises 7% of body weight. Thus in the 70 Kg adult this will, equate to 5 litres. This changes in children (8-9% body weight) and is slightly lower in the elderly., The table below outlines the 4 major classes of haemorrhagic shock and their associated, physiological sequelae:, , Parameter, , Class I, , Class II, , Class III, , Class IV, , Blood loss ml, , <750ml, , 750-1500ml, , 1500-2000ml, , >2000ml, , Blood loss %, , <15%, , 15-30%, , 30-40%, , >40%, , Pulse rate, , <100, , >100, , >120, , >140, , Blood pressure, , Normal, , Normal, , Decreased, , Decreased
Page 91 :
Parameter, , Class I, , Class II, , Class III, , Class IV, , Respiratory rate, , 14-20, , 20-30, , 30-40, , >35, , Urine output, , >30ml, , 20-30ml, , 5-15ml, , <5ml, , Symptoms, , Normal, , Anxious, , Confused, , Lethargic, , Decreasing blood pressure during haemorrhagic shock causes organ hypoperfusion and relative, myocardial ischaemia. The cardiac index gives a numerical value for tissue oxygen delivery and is, given by the equation: Cardiac index= Cardiac output/ body surface area. Where Hb is, haemoglobin concentration in blood and SaO2 the saturation and PaO2 the partial pressure of, oxygen. Detailed knowledge of this equation is required for the MRCS Viva but not for part A,, although you should understand the principle., In patients suffering from trauma the most likely cause of shock is haemorrhage. However, the, following may also be the cause or occur concomitantly:, , , , , , , Tension pneumothorax, Spinal cord injury, Myocardial contusion, Cardiac tamponade, , When assessing trauma patients it is worth remembering that in order to generate a palpable, femoral pulse an arterial pressure of >65mmHg is required., Once bleeding is controlled and circulating volume normalised the levels of transfusion should be to, maintain a Hb of 7-8 in those with no risk factors for tissue hypoxia and Hb 10 for those who have, such risk factors., Neurogenic shock, This occurs most often following a spinal cord transection, usually at a high level. There is, resultant interruption of the autonomic nervous system. The result is either decreased sympathetic, tone or increased parasympathetic tone, the effect of which is a decrease in peripheral vascular, resistance mediated by marked vasodilation., This results in decreased preload and thus decreased cardiac output (Starlings law). There is, decreased peripheral tissue perfusion and shock is thus produced. In contrast with many other types, of shock peripheral vasoconstrictors are used to return vascular tone to normal., Cardiogenic shock, In medical patients the main cause is ischaemic heart disease. In the traumatic setting direct, myocardial trauma or contusion is more likely. Evidence of ECG changes and overlying sternal
Page 92 :
fractures or contusions should raise the suspicion of injury. Treatment is largely supportive and, transthoracic echocardiography should be used to determine evidence of pericardial fluid or direct, myocardial injury. The measurement of troponin levels in trauma patients may be undertaken but, they are less useful in delineating the extent of myocardial trauma than following MI., When cardiac injury is of a blunt nature and is associated with cardiogenic shock the right side of the, heart is the most likely site of injury with chamber and or valve rupture. These patients require, surgery to repair these defects and will require cardiopulmonary bypass to achieve this. Some may, require intra aortic balloon pump as a bridge to surgery., Anaphylactic shock, Anaphylaxis may be defined as a severe, life-threatening, generalised or systemic, hypersensitivity reaction., Anaphylaxis is one of the few times when you would not have time to look up the dose of a, medication. The Resuscitation Council guidelines on anaphylaxis have recently been updated., Adrenaline is by far the most important drug in anaphylaxis and should be given as soon as, possible. The recommended doses for adrenaline, hydrocortisone and chlorpheniramine are as, follows:, , Adrenaline, , Hydrocortisone, , Chlorpheniramine, , < 6 months, , 150 mcg (0.15ml 1 in 1,000), , 25 mg, , 250 mcg/kg, , 6 months - 6 years, , 150 mcg (0.15ml 1 in 1,000), , 50 mg, , 2.5 mg, , 6-12 years, , 300 mcg (0.3ml 1 in 1,000), , 100 mg, , 5 mg, , Adult and child 12 years, , 500 mcg (0.5ml 1 in 1,000), , 200 mg, , 10 mg, , Adrenaline can be repeated every 5 minutes if necessary. The best site for IM injection is the, anterolateral aspect of the middle third of the thigh., Common identified causes of anaphylaxis, , , , , food (e.g. Nuts) - the most common cause in children, drugs, venom (e.g. Wasp sting), Next question
Page 93 :
What are the most likely effects of the release of vasopressin from the pituitary?, , Vasoconstriction of the afferent glomerular arteriole, , Increased permeability of the mesangial cells to glucose, , Reduced permeability of the inner medullary portion of the collecting duct to urea, , Increased secretion of aldosterone from the macula densa, , Increased water permeability of the distal tubule cells of the kidney, , ADH (vasopressin) results in the insertion of aquaporin channels in apical membrane of the distal, tubule and collecting ducts., Please rate this question:, , Discuss and give feedback, , Next question, , Renal Physiology, Overview, , , , , Each nephron is supplied with blood from an afferent arteriole that opens onto the glomerular, capillary bed., Blood then flows to an efferent arteriole, supplying the peritubular capillaries and medullary, vasa recta., The kidney receives up to 25% of resting cardiac output., , Control of blood flow, , , , The kidney is able to autoregulate its blood flow between systolic pressures of 80- 180mmHg, so there is little variation in renal blood flow., This is achieved by myogenic control of arteriolar tone, both sympathetic input and hormonal, signals (e.g. renin) are responsible., , Glomerular structure and function
Page 94 :
, , , , , , , , Blood inside the glomerulus has considerable hydrostatic pressure., The basement membrane has pores that will allow free diffusion of smaller solutes, larger, negatively charged molecules such as albumin are unable to cross., The glomerular filtration rate (GFR) is equal to the concentration of a solute in the urine,, times the volume of urine produced per minute, divided by the plasma concentration, (assuming that the solute is freely diffused e.g. inulin)., In clinical practice creatinine is used because it is subjected to very little proximal tubular, secretion., Although subject to variability, the typical GFR is 125ml per minute., Glomerular filtration rate = Total volume of plasma per unit time leaving the capillaries and, entering the bowman's capsule, Renal clearance = volume plasma from which a substance is removed per minute by the, kidneys, , Substances used to measure GFR have the following features:, 1. Inert, 2. Free filtration from the plasma at the glomerulus (not protein bound), 3. Not absorbed or secreted at the tubules, 4. Plasma concentration constant during urine collection, Examples: inulin, creatinine, GFR = urine concentration (mmol/l) x urine volume (ml/min), -------------------------------------------------------------------------plasma concentration (mmol/l), , , , , The clearance of a substance is dependent not only on its diffusivity across the basement, membrane but also subsequent tubular secretion and / or reabsorption., So glucose which is freely filtered across the basement membrane is usually reabsorbed, from tubules giving a clearance of zero., , Tubular function, , , , , , , , , Reabsorption and secretion of substances occurs in the tubules., In the proximal tubule substrates such as glucose, amino acids and phosphate are cotransported with sodium across the semi permeable membrane., Up to two thirds of filtered water is reabsorbed in the proximal tubules., This will lead to increase in urea concentration in the distal tubule allowing for its increased, diffusion., Substances to be secreted into the tubules are taken up from the peritubular blood by tubular, cells., Solutes such as paraaminohippuric acid are cleared with a single passage through the, kidneys and this is why it is used to measure renal plasma flow. Ions such as calcium and, phosphate will have a tubular reabsorption that is influenced by plasma PTH levels., Potassium may be both secreted and re-absorbed and is co-exchanged with sodium.
Page 95 :
Loop of Henle, , , , , , , , , , Approximately 60 litres of water containing 9000mmol sodium enters the descending limb of, the loop of Henle in 24 hours., Loops from the juxtamedullary nephrons run deep into the medulla., The osmolarity of fluid changes and is greatest at the tip of the papilla., The thin ascending limb is impermeable to water, but highly permeable to sodium and, chloride ions., This loss means that at the beginning of the thick ascending limb the fluid is hypo osmotic, compared with adjacent interstitial fluid., In the thick ascending limb the reabsorption of sodium and chloride ions occurs by both, facilitated and passive diffusion pathways., The loops of Henle are co-located with vasa recta, these will have similar solute, compositions to the surrounding extracellular fluid so preventing the diffusion and, subsequent removal of this hypertonic fluid., The energy dependent reabsorption of sodium and chloride in the thick ascending limb helps, to maintain this osmotic gradient., , Next question
Page 96 :
Which of the following hormones is mainly responsible for sodium - potassium exchange in the, salivary ducts?, , Vasopressin, , Angiotensin I, , Aldosterone, , Somatostatin, , Cholecystokinin, , Aldosterone is responsible for regulating ion exchange in salivary glands. It acts on a sodium /, potassium ion exchange pump.It is a mineralocorticoid hormone derived from the zona glomerulosa, of the adrenal gland., Please rate this question:, , Discuss and give feedback, , Next question, , Parotid gland, Anatomy of the parotid gland, , Location, , Overlying the mandibular ramus; anterior and inferior to the ear., , Salivary duct, , Crosses the masseter, pierces the buccinator and drains adjacent to the, 2nd upper molar tooth (Stensen's duct)., , Structures passing, through the gland, , Relations, , , , , , , Facial nerve (Mnemonic: The Zebra Buggered My Cat; Temporal, Zygomatic, Buccal, Mandibular, Cervical), External carotid artery, Retromandibular vein, Auriculotemporal nerve, , , , Anterior: masseter, medial pterygoid, superficial temporal and
Page 97 :
, , maxillary artery, facial nerve, stylomandibular ligament, Posterior: posterior belly digastric muscle, sternocleidomastoid,, stylohyoid, internal carotid artery, mastoid process, styloid, process, , Arterial supply, , Branches of external carotid artery, , Venous drainage, , Retromandibular vein, , Lymphatic drainage, , Deep cervical nodes, , Nerve innervation, , , , , , Parasympathetic-Secretomotor, Sympathetic-Superior cervical ganglion, Sensory- Greater auricular nerve, , Parasympathetic stimulation produces a water rich, serous saliva. Sympathetic stimulation leads to, the production of a low volume, enzyme-rich saliva., Next question
Page 98 :
In a 70 Kg male, what proportion of total body fluid will be contributed by plasma?, , 50%, , 5%, , 35%, , 65%, , 25%, 70 Kg male = 42 L water (60% of total body weight), , Please rate this question:, , Discuss and give feedback, , Next question, , Fluid compartment physiology, Body fluid compartments comprise intracellular and extracellular compartments. The latter includes, interstitial fluid, plasma and transcellular fluid., Typical figures are based on the 70 Kg male., Body fluid volumes, , Compartment, , Volume in litres, , Percentage of total volume, , Intracellular, , 28 L, , 60-65%
Page 99 :
Compartment, , Volume in litres, , Percentage of total volume, , Extracellular, , 14 L, , 35-40%, , Plasma, , 3L, , 5%, , Interstitial, , 10 L, , 24%, , Transcellular, , 1L, , 3%, , Figures are approximate, Next question
Page 100 :
A 23 year old man is undergoing an inguinal hernia repair under local anaesthesia. The surgeon, encounters a bleeding site which he manages with diathermy. About a minute or so later the patient, complains that he is able to feel the burning pain of the heat at the operative site. Which of the, following nerve fibres is responsible for the transmission of this signal?, , A α fibres, A β fibres, , B fibres, , C fibres, , None of the above, , Slow transmission of mechanothermal stimuli is transmitted via C fibres., A α fibres transmit information relating to motor proprioception, A β fibres transmit touch and, pressure and B fibres are autonomic fibres., Please rate this question:, , Discuss and give feedback, , Next question, , Pain - neuronal transmission, Somatic pain, , , , Peripheral nociceptors are innervated by either small myelinated fibres (A-gamma) fibres or, by unmyelinated C fibres., The A gamma fibres register high intensity mechanical stimuli. The C fibres usually register, high intensity mechanothermal stimuli., Next question
Page 101 :
What is the approximate volume of pancreatic secretions in a 24 hour period?, , 100ml, , 200ml, , 500ml, , 1500ml, , 3000ml, , Typically the pancreas secretes between 1000 and 1500ml per day., Please rate this question:, , Discuss and give feedback, , Next question, , Pancreas exocrine physiology, Composition of pancreatic secretions, Pancreatic secretions are usually 1000-1500ml per 24 hours and have a pH of 8., Secretion, , Enzymic, , Aqueous, , Source, , Substances secreted, , Acinar cells, , Trypsinogen, Procarboxylase, Amylase, Elastase, , Ductal and, , Sodium, Bicarbonate
Page 102 :
Centroacinar cells, , Water, Potassium, Chloride, NB: Sodium and potassium reflect their plasma levels; chloride, and bicarbonate vary with flow rate, , Regulation, The cephalic and gastric phases (neuronal and physical) are less important in regulating the, pancreatic secretions. The effect of digested material in the small bowel stimulates CCK release and, ACh which stimulate acinar and ductal cells. Of these CCK is the most potent stimulus. In the case, of the ductal cells these are potently stimulated by secretin which is released by the S cells of the, duodenum. This results in an increase in bicarbonate., Enzyme activation, Trypsinogen is converted via enterokinase to active trypsin in the duodenum. Trypsin then activates, the other inactive enzymes, Next question
Page 103 :
A 34 year old lady has just undergone a parathyroidectomy for primary hyperparathyroidism. The, operation is difficult and all 4 glands were explored. The wound was clean and dry at the conclusion, of the procedure and a suction drain inserted. On the ward she becomes irritable and develops, stridor. On examination, her neck is soft and the drain empty. Which of the following treatments, should be tried initially?, , Administration of intravenous calcium gluconate, , Administration of intravenous lorazepam, , Removal of the skin closure on the ward, , Direct laryngoscopy, , Administration of calcichew D3 orally, , Exploration of the parathyroid glands may result in impairment of the blood supply. Serum PTH, levels can fall quickly and features of hypocalcaemia may ensue, these include neuromuscular, irritability and laryngospasm. Prompt administration of intravenous calcium gluconate can be, lifesaving. The absence of any neck swelling and no blood in the drain would go against a contained, haematoma in the neck (which should be managed by removal of skin closure)., Please rate this question:, , Discuss and give feedback, , Next question, , Calcium homeostasis, Calcium ions are linked to a wide range of physiological processes. The largest store of bodily, calcium is contained within the skeleton. Calcium levels are primarily controlled by parathyroid, hormone, vitamin D and calcitonin., Hormonal regulation of calcium, , Hormone, , Parathyroid hormone (PTH), , Actions, , , , , Increase calcium levels and decrease phosphate, levels, Increases bone resorption, Immediate action on osteoblasts to increase ca2+ in
Page 104 :
Hormone, , Actions, , , , , , , , , 1,25-dihydroxycholecalciferol (the, active form of vitamin D), , Calcitonin, , , , , extracellular fluid, Osteoblasts produce a protein signaling molecule, that activate osteoclasts which cause bone, resorption, Increases renal tubular reabsorption of calcium, Increases synthesis of 1,25(OH)2D (active form, of vitamin D) in the kidney which increases, bowel absorption of Ca2+, Decreases renal phosphate reabsorption, , , , , Increases plasma calcium and plasma phosphate, Increases renal tubular reabsorption and gut, absorption of calcium, Increases osteoclastic activity, Increases renal phosphate reabsorption, , , , , , , Secreted by C cells of thyroid, Inhibits intestinal calcium absorption, Inhibits osteoclast activity, Inhibits renal tubular absorption of calcium, , Both growth hormone and thyroxine also play a small role in calcium metabolism., Next question
Page 105 :
Theme: Interpretation of aterial blood gas results, , A. pH 7.19, pCO2 10.2, pO2 16 (FiO2 85%), Bicarbonate 23.8, Base excess -2.2, mmol, B. pH 7.57, PaCO2 3.5, Pa O2 24.5 (FiO2 85%), Bicarbonate 23.5, Base excess, +1.8 mmol, C. pH 7.14, PaCO2 7.4, PaO2 8.9 (FiO2 40%), Bicarbonate 14 mmol, Base excess, -10.6, D. pH 7.36, PaCO2 7.3, PO2 8.9 (FiO2 40%), Bicarbonate 30.2, Base excess 5.3, E. pH 7.32, PCO2 3.8, PaO2 22.2 (FiO2 40%), Bicarbonate 19.1, Base excess -7.9, , Which of the following arterial blood gases fit with the description below?, , 42., , Acute respiratory acidosis, pH 7.19, pCO2 10.2, pO2 16 (FiO2 85%), Bicarbonate 23.8, Base excess -2.2 mmol, , 43., , Metabolic acidosis with a compensatory respiratory alkalosis, You answered pH 7.19, pCO2 10.2, pO2 16 (FiO2 85%), Bicarbonate 23.8, Base excess -2.2 mmol, The correct answer is pH 7.32, PCO2 3.8, PaO2 22.2 (FiO2 40%), Bicarbonate 19.1, Base excess -7.9, , 44., , Chronic respiratory acidosis with a compensatory metabolic alkalosis, You answered pH 7.19, pCO2 10.2, pO2 16 (FiO2 85%), Bicarbonate 23.8, Base excess -2.2 mmol, The correct answer is pH 7.36, PaCO2 7.3, PO2 8.9 (FiO2 40%), Bicarbonate 30.2, Base excess 5.3
Page 106 :
Please rate this question:, , Discuss and give feedback, , Next question, , Arterial blood gas interpretation, In advanced life support training, a 5 step approach to arterial blood gas interpretation is advocated., 1. How is the patient?, 2. Is the patient hypoxaemic?, The Pa02 on air should be 10.0-13.0 kPa, 3. Is the patient acidaemic (pH <7.35) or alkalaemic (pH >7.45), 4. What has happened to the PaCO2?, If there is acidaemia, an elevated PaCO2 will account for this, 5. What is the bicarbonate level or base excess?, A metabolic acidosis will have a low bicarbonate level and a low base excess (< -2 mmol), A metabolic alkalosis will have a high bicarbonate and a high base excess (> +2 mmol), , Next question
Page 107 :
A 23 year old man presents with blunt abdominal trauma and a splenic bleed is suspected. He is, commenced on an infusion of tranexamic acid. Which of the following best describes its mechanism, of action?, , Inhibition of plasmin, , Inhibition of thrombin, , Inhibition of factor II, , Inhibition of factor Xa, , Activation of factor VIII, , Tranexamic acid inhibits plasmin and this prevents fibrin degradation., Please rate this question:, , Discuss and give feedback, , Next question, , Tranexamic acid, Tranexamic acid is a synthetic derivative of lysine. Its primary mode of action is as an anti fibrinolytic, that competitively inhibits the conversion of plasminogen to plasmin. Plasmin degrades fibrin and, therefore rendering plasmin inactive slows this process., The role of tranexamic acid in trauma was investigated in the CRASH 2 trial and has been shown to, be of benefit in bleeding trauma when administered in the first 3 hours., Next question
Page 108 :
A 34 year old male donates a unit of blood. It is stored at 4 oC. After 72 hours which of the following, clotting factors will be most affected?, , Factor V, , Factor II, , Factor VII, , Factor IX, , Factor XI, , Factors V and VIII are sensitive to temperature which is the reason why FFP is frozen soon after, collection., Please rate this question:, , Discuss and give feedback, , Next question, , Blood products, Whole blood fractions, , Fraction, , Key points, , Packed red cells, , Used for transfusion in chronic anaemia and cases where infusion of large, volumes of fluid may result in cardiovascular compromise. Product obtained, by centrifugation of whole blood., , Platelet rich, plasma, , Usually administered to patients who are thrombocytopaenic and are bleeding, or require surgery. It is obtained by low speed centrifugation., , Platelet, concentrate, , Prepared by high speed centrifugation and administered to patients with, thrombocytopaenia.
Page 109 :
Fresh frozen, plasma, , , , , , , , , Cryoprecipitate, , SAG-Mannitol, Blood, , , , , , Prepared from single units of blood., Contains clotting factors, albumin and immunoglobulin., Unit is usually 200 to 250ml., Usually used in correcting clotting deficiencies in patients with hepatic, synthetic failure who are due to undergo surgery., Usual dose is 12-15ml/Kg-1., It should not be used as first line therapy for hypovolaemia., Formed from supernatant of FFP., Rich source of Factor VIII and fibrinogen., Allows large concentration of factor VIII to be administered in small, volume., , Removal of all plasma from a blood unit and substitution with:, , , , , , Sodium chloride, Adenine, Anhydrous glucose, Mannitol, , Up to 4 units of SAG M Blood may be administered. Thereafter whole blood, is preferred. After 8 units, clotting factors and platelets should be considered., Cell saver devices, These collect patients own blood lost during surgery and then re-infuse it. There are two main types:, , , , Those which wash the blood cells prior to re-infusion. These are more expensive to purchase, and more complicated to operate. However, they reduce the risk of re-infusing contaminated, blood back into the patient., Those which do not wash the blood prior to re-infusion., , Their main advantage is that they avoid the use of infusion of blood from donors into patients and, this may reduce risk of blood borne infection. It may be acceptable to Jehovah's witnesses. It is, contraindicated in malignant disease for risk of facilitating disease dissemination., Blood products used in warfarin reversal, In some surgical patients the use of warfarin can pose specific problems and may require the use of, specialised blood products, Immediate or urgent surgery in patients taking warfarin(1) (2):, 1. Stop warfarin, 2. Vitamin K (reversal within 4-24 hours)
Page 110 :
-IV takes 4-6h to work (at least 5mg), -Oral can take 24 hours to be clinically effective, 3. Fresh frozen plasma, Used less commonly now as 1st line warfarin reversal, -30ml/kg-1, -Need to give at least 1L fluid in 70kg person (therefore not appropriate in fluid overload), -Need blood group, -Only use if human prothrombin complex is not available, 4. Human Prothrombin Complex (reversal within 1 hour), -Bereplex 50 u/kg, -Rapid action but factor 6 short half life, therefore give with vitamin K, References, 1. Dentali, F., C. Marchesi, et al. (2011). "Safety of prothrombin complex concentrates for rapid, anticoagulation reversal of vitamin K antagonists. A meta-analysis." Thromb Haemost 106(3): 429438., 2. http://www.transfusionguidelines.org/docs/pdfs/bbt-03warfarin-reversal-flowchart-2006.pdf, Next question
Page 111 :
Cortisol is predominantly produced by which of the following?, , Zona fasciculata of the adrenal, , Zona glomerulosa of the adrenal, , Zona reticularis of the adrenal, , Adrenal medulla, , Posterior lobe of the pituitary, Relative Glucocorticoid activity:, Hydrocortisone = 1, Prednisolone = 4, Dexamethasone = 25, Cortisol is produced by the zona fasciculata of the adrenal gland., Please rate this question:, , Discuss and give feedback, , Next question, , Cortisol, , , , , , , Glucocorticoid, Released by zona fasiculata of the adrenal gland, 90% protein bound; 10% active, Circadian rhythm: High in the mornings, Negative feedback via ACTH, , Actions, , , , , , , , Glycogenolysis, Gluconeogenesis, Protein catabolism, Lipolysis, Stress response, Anti-inflammatory
Page 112 :
, , , , , Decrease protein in bones, Increase gastric acid, Increases neutrophils/platelets/red blood cells, Inhibits fibroblastic activity, , Next question
Page 113 :
Which of the following is not an intravenous colloid?, , Gelofusine, , Dextran 40, , Human albumin solution, , Hydroxyethyl starch, , Bicarbonate 8.4%, , Bicarbonate is a crystalloid., Please rate this question:, , Discuss and give feedback, , Next question, , Pre operative fluid management, Fluid management has been described in the British Consensus guidelines on IV fluid, therapy for Adult Surgical patients (GIFTASUP) and by NICE (CG174 December 2013), The Recommendations include:, , , , , , , , , , Use Ringer's lactate or Hartmann's when a crystalloid is needed for resuscitation or, replacement of fluids. Avoid 0.9% N. Saline (due to risk of hyperchloraemic acidosis) unless, patient vomiting or has gastric drainage., Use 4%/0.18% dextrose saline or 5% dextrose in maintenance fluids. It should not be used, in resuscitation or as replacement fluids., Adult maintenance fluid requirements are: Na 50-100 mmol/day and K 40-80 mmol/day in, 1.5-2.5L fluid per day., Patients for elective surgery should NOT be nil by mouth for >2 hours (unless has disorder of, gastric emptying)., Patients for elective surgery should be given carbohydrate rich drinks 2-3h before. Ideally, this should form part of a normal pre op plan to facilitate recovery., Avoid mechanical bowel preparation., If bowel prep is used, simultaneous administration of Hartmann's or Ringer's lactate should, be considered., Excessive fluid losses from vomiting should be treated with a crystalloid with potassium, replacement. 0.9% N. Saline should be given if there is hypochloraemia. Otherwise
Page 114 :
, , , , , , Hartmann's or Ringer lactate should be given for diarrhoea/ileostomy/ileus/obstruction., Hartmann's should also be given in sodium losses secondary to diuretics., High risk patients should receive fluids and inotropes., An attempt should be made to detect pre or operative hypovolaemia using flow based, measurements. If this is not available, then clinical evaluation is needed i.e. JVP, pulse, volume etc., In Blood loss or infection causing hypovolaemia should be treated with a balanced crystalloid, or colloid (or until blood available in blood loss). A critically ill patient is unable to excrete Na, or H20 leading to a 5% risk of interstitial oedema. Therefore 5% dextrose as well as colloid, should be given., If patients need IV fluid resuscitation, use crystalloids that contain sodium in the range 130154 mmol/l, with a bolus of 500 ml over less than 15 minutes (NICE Guidance CG 174)., Next question
Page 115 :
Theme: Electrolyte disorders, , A., B., C., D., E., F., , Hypotonic hypovolaemic hyponatraemia, Hypotonic hypervolaemic hyponatraemia, Pseudohyponatraemia, Syndrome of inappropriate ADH secretion (SIADH), Hypertonic hyponatraemia, Over administration 5% dextrose, , Please select the most likely reason for hyponatraemia for each scenario given. Each option may be, used once, more than once or not at all., , 49., , A 73 year old man presents to pre operative clinic for an elective total hip replacement. He, is on frusemide for hypertension. He is found to have the following blood results:, Na 120, Urine Na 10 (low), Serum osmolality 280 (normal), Hypotonic hypovolaemic hyponatraemia, The blood results reflect extra-renal sodium loss. The body is trying to preserve the, sodium by not allowing any sodium into the urine (hence the low Na in the urine). Note, with renal sodium loss the Urinary sodium is high., , 50., , A 67 year old man presents to pre operative clinic for an elective hernia repair. He is on, frusemide for heart failure. He is found to have the following blood results:, Na 120, Urine Na 35 (high), Urine osmolality 520 (high), Serum osmolality 265 (low), You answered Hypotonic hypovolaemic hyponatraemia, The correct answer is Syndrome of inappropriate ADH secretion (SIADH), This blood picture fits with SIADH. SIADH causes retention of fluid from the urine, (concentrated urine) into the blood vessels, therefore diluting the fluid in the blood vessels, (low osmolality). Management involves removing the cause and fluid restriction., , 51., , A 77 year old man presents to pre operative clinic for a total knee replacement. He is on, frusemide for hypertension. He is known to have multiple myeloma. He is found to have, the following blood results:, Na 120, Serum osmolality 280 (normal)
Page 116 :
Urine osmolality normal, Urine Na normal, You answered Hypotonic hypovolaemic hyponatraemia, The correct answer is Pseudohyponatraemia, Hyperlipidaemia and multiple myeloma are known to cause a pseudohyponatraemia., SIADH:, , , , , Low serum osmolality, High/Normal urine osmolality, , Please rate this question:, , Discuss and give feedback, , Next question, , Hyponatraemia, This is commonly tested in the MRCS (despite most surgeons automatically seeking medical advice, if this occurs!). The most common cause in surgery is the over administration of 5% dextrose., Hyponatraemia may be caused by water excess or sodium depletion. Causes of, pseudohyponatraemia include hyperlipidaemia (increase in serum volume) or a taking blood from a, drip arm. Urinary sodium and osmolarity levels aid making a diagnosis., Classification, , Urinary sodium > 20, mmol/l, , Sodium depletion, renal loss, , , , , , , , , , Patient often hypovolaemic, Diuretics (thiazides), Addison's, Diuretic stage of renal failure, SIADH (serum osmolality, low, urine osmolality high,, urine Na high), Patient often euvolaemic, , Mnemonic: Syndrome of, INAPPropriate AntiDiuretic Hormone:, In creased, Na (sodium), PP (urine)
Page 117 :
Urinary sodium < 20, mmol/l, , Sodium depletion, extra-renal loss, , , , Water excess (patient, often hypervolaemic and, oedematous), , , , , , , Diarrhoea, vomiting,, sweating, Burns, adenoma of rectum (if, villous lesion and large), Secondary, hyperaldosteronism: CCF,, cirrhosis, Reduced GFR: renal failure, IV dextrose, psychogenic, polydipsia, , Management, Symptomatic Hyponatremia :, Acute hyponatraemia with Na <120: immediate therapy. Central Pontine Myelinolisis, may occur, from overly rapid correction of serum sodium. Aim to correct until the Na is > 125 at a rate of 1, mEq/h. Normal saline with frusemide is an alternative method., The sodium requirement can be calculated as follows :, (125 - serum sodium) x 0.6 x body weight = required mEq of sodium, Next question
Page 118 :
A 25 year old man undergoes an appendicetomy for appendicitis. The appendix is submitted for, histopathological evaluation. Which of the following is most likely to be identified microscopically?, , Macrophages, , Neutrophils, , Fibroblasts, , Lymphocytes, , Stem cells, , Theme from April 2015 Exam, Theme from January 2015 Exam, Neutrophil polymorphs are the cell type most commonly encountered in acute inflammation., Please rate this question:, , Discuss and give feedback, , Next question, , Acute inflammation, Inflammation is the reaction of the tissue elements to injury. Vascular changes occur, resulting in the, generation of a protein rich exudate. So long as the injury does not totally destroy the existing tissue, architecture, the episode may resolve with restoration of original tissue architecture., Vascular changes, , , , , , Vasodilation occurs and persists throughout the inflammatory phase., Inflammatory cells exit the circulation at the site of injury., The equilibrium that balances Starlings forces within capillary beds is disrupted and a protein, rich exudate will form as the vessel walls also become more permeable to proteins., The high fibrinogen content of the fluid may form a fibrin clot. This has several important, immunomodulatory functions., , Sequelae
Page 119 :
Resolution, , , , , Typically occurs with minimal initial injury, Stimulus removed and normal tissue architecture results, , Organisation, , , , , Delayed removal of exudate, Tissues undergo organisation and usually fibrosis, , Suppuration, , , , , Typically formation of an abscess or an empyema, Sequestration of large quantities of dead neutrophils, , Progression to chronic, inflammation, , , , , Coupled inflammatory and reparative activities, Usually occurs when initial infection or suppuration has, been inadequately managed, , Causes, , , , , , , Infections e.g. Viruses, exotoxins or endotoxins released by bacteria, Chemical agents, Physical agents e.g. Trauma, Hypersensitivity reactions, Tissue necrosis, , Presence of neutrophil polymorphs is a histological diagnostic feature of acute inflammation, Next question
Page 120 :
A 53 year old man is on the intensive care unit following an emergency abdominal aortic aneurysm, repair. He develops abdominal pain and diarrhoea and is profoundly unwell. His abdomen has no, features of peritonism. Which of the following arterial blood gas pictures is most likely to be present?, , pH 7.45, pO2 10.1, pCO2 3.2, Base excess 0, Lactate 0, , pH 7.35, pO2 8.0, pCO2 5.2, Base excess 2, Lactate 1, , pH 7.20, pO2 9.0, pCO2 3.5, Base excess -10, Lactate 8, , pH 7.29, pO2 8.9, pCO2 5.9, Base excess -4, Lactate 3, , pH 7.30, pO2 9.2 pCO2 4.8, Base excess -2, lactate 1, , This man is likely to have a metabolic acidosis secondary to a mesenteric infarct., Please rate this question:, , Discuss and give feedback, , Next question, , Disorders of acid - base balance, Disorders of acid- base balance are often covered in the MRCS part A, both in the SBA and EMQ, sections., The acid-base normogram below shows how the various disorders may be categorised
Page 121 :
Image sourced from Wikipedia, , Metabolic acidosis, , , , , This is the most common surgical acid - base disorder., Reduction in plasma bicarbonate levels., Two mechanisms:, , 1. Gain of strong acid (e.g. diabetic ketoacidosis), 2. Loss of base (e.g. from bowel in diarrhoea), - Classified according to the anion gap, this can be calculated by:, (Na+ + K+) - (Cl- + HCO3-)., - If a question supplies the chloride level then this is often a clue that the anion gap should be, calculated. The normal range = 10-18 mmol/L, Normal anion gap ( = hyperchloraemic metabolic acidosis), , , , , , , Gastrointestinal bicarbonate loss: diarrhoea, ureterosigmoidostomy, fistula, Renal tubular acidosis, Drugs: e.g. acetazolamide, Ammonium chloride injection, Addison's disease, , Raised anion gap
Page 122 :
, , , , , Lactate: shock, hypoxia, Ketones: diabetic ketoacidosis, alcohol, Urate: renal failure, Acid poisoning: salicylates, methanol, , Metabolic acidosis secondary to high lactate levels may be subdivided into two types:, , , , Lactic acidosis type A: (Perfusion disorders e.g.shock, hypoxia, burns), Lactic acidosis type B: (Metabolic e.g. metformin toxicity), , Metabolic alkalosis, , , , , Usually caused by a rise in plasma bicarbonate levels., Rise of bicarbonate above 24 mmol/L will typically result in renal excretion of excess, bicarbonate., Caused by a loss of hydrogen ions or a gain of bicarbonate. It is due mainly to problems of, the kidney or gastrointestinal tract, , Causes, , , , , , , , , , Vomiting / aspiration (e.g. Peptic ulcer leading to pyloric stenosis, nasogastric suction), Diuretics, Liquorice, carbenoxolone, Hypokalaemia, Primary hyperaldosteronism, Cushing's syndrome, Bartter's syndrome, Congenital adrenal hyperplasia, , Mechanism of metabolic alkalosis, , , , , , Activation of renin-angiotensin II-aldosterone (RAA) system is a key factor, Aldosterone causes reabsorption of Na+ in exchange for H+ in the distal convoluted tubule, ECF depletion (vomiting, diuretics) → Na+ and Cl- loss → activation of RAA system → raised, aldosterone levels, In hypokalaemia, K+ shift from cells → ECF, alkalosis is caused by shift of H + into cells to, maintain neutrality
Page 123 :
Respiratory acidosis, , , , Rise in carbon dioxide levels usually as a result of alveolar hypoventilation, Renal compensation may occur leading to Compensated respiratory acidosis, , Causes, , , , , COPD, Decompensation in other respiratory conditions e.g. Life-threatening asthma / pulmonary, oedema, Sedative drugs: benzodiazepines, opiate overdose, , Respiratory alkalosis, , , , Hyperventilation resulting in excess loss of carbon dioxide, This will result in increasing pH, , Causes, , , , , , , Psychogenic: anxiety leading to hyperventilation, Hypoxia causing a subsequent hyperventilation: pulmonary embolism, high altitude, Early salicylate poisoning*, CNS stimulation: stroke, subarachnoid haemorrhage, encephalitis, Pregnancy, , *Salicylate overdose leads to a mixed respiratory alkalosis and metabolic acidosis. Early stimulation, of the respiratory centre leads to a respiratory alkalosis whilst later the direct acid effects of, salicylates (combined with acute renal failure) may lead to an acidosis, Next question
Page 124 :
A 48 year old women suffers blunt trauma to the head and develops respiratory compromise. As a, result she develops hypercapnia. Which of the following effects is most likely to ensue?, , Cerebral vasoconstriction, , Cerebral vasodilation, , Cerebral blood flow will remain unchanged, , Shunting of blood to peripheral tissues will occur in preference to CNS perfusion, , None of the above, , Hypercapnia will tend to produce cerebral vasodilation. This is of considerable importance in patients, with cranial trauma as it may increase intracranial pressure., Please rate this question:, , Discuss and give feedback, , Next question, , Applied neurophysiology, , , , , , , Pressure within the cranium is governed by the Monroe-Kelly doctrine. This considers the, skull as a closed box. Increases in mass can be accommodated by loss of CSF. Once a, critical point is reached (usually 100- 120ml of CSF lost) there can be no further, compensation and ICP rises sharply. The next step is that pressure will begin to equate with, MAP and neuronal death will occur. Herniation will also accompany this process., The CNS can autoregulate its own blood supply. Vaso constriction and dilatation of the, cerebral blood vessels is the primary method by which this occurs. Extremes of blood, pressure can exceed this capacity resulting in risk of stroke. Other metabolic factors such as, hypercapnia will also cause vasodilation, which is of importance in ventilating head injured, patients., The brain can only metabolise glucose, when glucose levels fall, consciousness will be, impaired., Next question
Page 125 :
A patient is seen in clinic complaining of abdominal pain. Routine bloods show:, Na+, , 142 mmol/l, , K+, , 4.0 mmol/l, , Chloride, , 104 mmol/l, , Bicarbonate, , 19 mmol/l, , Urea, , 7.0 mmol/l, , Creatinine, , 112 µmol/l, , What is the anion gap?, , 4 mmol/L, , 14 mmol/L, , 20 mmol/L, , 21 mmol/L, , 23 mmol/L, , The anion gap may be calculated by using (sodium + potassium) - (bicarbonate + chloride), = (142 + 4.0) - (104 + 19) = 23 mmol/L, Please rate this question:, , Discuss and give feedback, , Next question, , Anion gap, The anion gap is calculated by:, (sodium + potassium) - (bicarbonate + chloride), A normal anion gap is 8-14 mmol/L
Page 126 :
It is useful to consider in patients with a metabolic acidosis:, Causes of a normal anion gap or hyperchloraemic metabolic acidosis, , , , , , , gastrointestinal bicarbonate loss: diarrhoea, ureterosigmoidostomy, fistula, renal tubular acidosis, drugs: e.g. acetazolamide, ammonium chloride injection, Addison's disease, , Causes of a raised anion gap metabolic acidosis, , , , , , lactate: shock, hypoxia, ketones: diabetic ketoacidosis, alcohol, urate: renal failure, acid poisoning: salicylates, methanol, Next question
Page 127 :
A 73 year old man has an arterial line in situ. On studying the trace the incisura can be seen. What is, the physiological event which accounts for this process?, , Atrial repolarisation, , Mitral valve closure, , Ventricular repolarisation, , Elastic recoil of the aorta, , Tricuspid valve closure, , Theme from 2010 Exam, It is the temporary rise in aortic pressure occurring as a result of elastic recoil., Please rate this question:, , Discuss and give feedback, , Next question, , Cardiac physiology, , , , , , The heart has four chambers ejecting blood into both low pressure and high pressure, systems., The pumps generate pressures of between 0-25mmHg on the right side and 0-120 mmHg on, the left., At rest diastole comprises 2/3 of the cardiac cycle., The product of the frequency of heart rate and stroke volume combine to give the cardiac, output which is typically 5-6L per minute., , Detailed descriptions of the various waveforms are often not a feature of MRCS A (although they are, on the syllabus). However, they are a very popular topic for surgical physiology in the MRCS B, exam., Electrical properties, , , Intrinsic myogenic rhythm within cardiac myocytes means that even the denervated heart is, capable of contraction.
Page 128 :
, , , , , In the normal situation the cardiac impulse is generated in the sino atrial node in the right, atrium and conveyed to the ventricles via the atrioventricular node., The sino atrial node is also capable of spontaneous discharge and in the absence of, background vagal tone will typically discharge around 100x per minute. Hence the higher, resting heart rate found in cardiac transplant cases. In the SA and AV nodes the resting, membrane potential is lower than in surrounding cardiac cells and will slowly depolarise from, -70mV to around -50mV at which point an action potential is generated., Differences in the depolarisation slopes between SA and AV nodes help to explain why the, SA node will depolarise first. The cells have a refractory period during which they cannot be, re-stimulated and this period allows for adequate ventricular filling. In pathological, tachycardic states this time period is overridden and inadequate ventricular filling may then, occur, cardiac output falls and syncope may ensue., , Parasympathetic fibres project to the heart via the vagus and will release acetylcholine. Sympathetic, fibres release nor adrenaline and circulating adrenaline comes from the adrenal medulla., Noradrenaline binds to β 1 receptors in the SA node and increases the rate of pacemaker potential, depolarisation., Cardiac cycle, , Image sourced from Wikipedia, , , , Mid diastole: AV valves open. Ventricles hold 80% of final volume. Outflow valves shut., Aortic pressure is high., , , , Late diastole: Atria contract. Ventricles receive 20% to complete filling. Typical end diastolic, volume 130-160ml.
Page 129 :
, , Early systole: AV valves shut. Ventricular pressure rises. Isovolumetric ventricular, contraction. AV Valves bulge into atria (c-wave). Aortic and pulmonary pressure exceededblood is ejected. Shortening of ventricles pulls atria downwards and drops intra atrial, pressure (x-descent)., , , , Late systole: Ventricular muscles relax and ventricular pressures drop. Although ventricular, pressure drops the aortic pressure remains constant owing to peripheral vascular resistance, and elastic property of the aorta. Brief period of retrograde flow that occurs in aortic recoil, shuts the aortic valve. Ventricles will contain 60ml end systolic volume. The average stroke, volume is 70ml (i.e. Volume ejected)., , , , Early diastole: All valves are closed. Isovolumetric ventricular relaxation occurs. Pressure, wave associated with closure of the aortic valve increases aortic pressure. The pressure dip, before this rise can be seen on arterial waveforms and is called the incisura. During systole, the atrial pressure increases such that it is now above zero (v- wave). Eventually atrial, pressure exceed ventricular pressure and AV valves open - atria empty passively into, ventricles and atrial pressure falls (y -descent ), , The negative atrial pressures are of clinical importance as they can allow air embolization to occur if, the neck veins are exposed to air. This patient positioning is important in head and neck surgery to, avoid this occurrence if veins are inadvertently cut, or during CVP line insertion., Mechanical properties, , , , Preload = end diastolic volume, Afterload = aortic pressure, , It is important to understand the principles of Laplace's law in surgery., , , , , It states that for hollow organs with a circular cross section, the total circumferential wall, tension depends upon the circumference of the wall, multiplied by the thickness of the wall, and on the wall tension., The total luminal pressure depends upon the cross sectional area of the lumen and the, transmural pressure. Transmural pressure is the internal pressure minus external pressure, and at equilibrium the total pressure must counterbalance each other., In terms of cardiac physiology the law explains that the rise in ventricular pressure that, occurs during the ejection phase is due to physical change in heart size. It also explains why, a dilated diseased heart will have impaired systolic function.
Page 130 :
Starlings law, , , , Increase in end diastolic volume will produce larger stroke volume., This occurs up to a point beyond which cardiac fibres are excessively stretched and stroke, volume will fall once more. It is important for the regulation of cardiac output in cardiac, transplant patients who need to increase their cardiac output., , Baroreceptor reflexes, , , , , , , Baroreceptors located in aortic arch and carotid sinus., Aortic baroreceptor impulses travel via the vagus and from the carotid via the, glossopharyngeal nerve., They are stimulated by arterial stretch., Even at normal blood pressures they are tonically active., Increase in baroreceptor discharge causes:, , *Increased parasympathetic discharge to the SA node., *Decreased sympathetic discharge to ventricular muscle causing decreased contractility and fall in, stroke volume., *Decreased sympathetic discharge to venous system causing increased compliance., *Decreased peripheral arterial vascular resistance, Atrial stretch receptors, , , , , , , , Located in atria at junction between pulmonary veins and vena cava., Stimulated by atrial stretch and are thus low pressure sensors., Increased blood volume will cause increased parasympathetic activity., Very rapid infusion of blood will result in increase in heart rate mediated via atrial receptors:, theBainbridge reflex., Decreases in receptor stimulation results in increased sympathetic activity this will decrease, renal blood flow-decreases GFR-decreases urinary sodium excretion-renin secretion by, juxtaglomerular apparatus-Increase in angiotensin II., Increased atrial stretch will also result in increased release of atrial natriuretic peptide., Next question
Page 131 :
A surgeon is considering using lignocaine as local anasthesia for a minor procedure. Which of the, following best accounts for its actions?, , Blockade of neuronal acetylcholine receptors, , Blockade of neuronal nicotinic receptors, , Blockade of neuronal sodium channels, , Blockade of neuronal potassium channels, , Blockade of neuronal calcium channels, , Lignocaine blocks sodium channels. They will typically be activated first, hence the pain some, patients experience on administration., Please rate this question:, , Discuss and give feedback, , Next question, , Local anaesthetic agents, Lidocaine, , , , , , , , , An amide, Local anaesthetic and a less commonly used antiarrhythmic (affects Na channels in the, axon), Hepatic metabolism, protein bound, renally excreted, Toxicity: due to IV or excess administration. Increased risk if liver dysfunction or low protein, states. Note acidosis causes lidocaine to detach from protein binding., Drug interactions: Beta blockers, ciprofloxacin, phenytoin, Features of toxicity: Initial CNS over activity then depression as lidocaine initially blocks, inhibitory pathways then blocks both inhibitory and activating pathways. Cardiac arrhythmias., Increased doses may be used when combined with adrenaline to limit systemic absorption., , Cocaine, , , Pure cocaine is a salt, usually cocaine hydrochloride. It is supplied for local anaesthetic, purposes as a paste.
Page 132 :
, , , , It is supplied for clinical use in concentrations of 4 and 10%. It may be applied topically to the, nasal mucosa. It has a rapid onset of action and has the additional advantage of causing, marked vasoconstriction., It is lipophillic and will readily cross the blood brain barrier. Its systemic effects also include, cardiac arrhythmias and tachycardia., Apart from its limited use in ENT surgery it is otherwise used rarely in mainstream surgical, practice., , Bupivacaine, , , , , , Bupivacaine binds to the intracellular portion of sodium channels and blocks sodium influx, into nerve cells, which prevents depolarization., It has a much longer duration of action than lignocaine and this is of use in that it may be, used for topical wound infiltration at the conclusion of surgical procedures with long duration, analgesic effect., It is cardiotoxic and is therefore contra indicated in regional blockage in case the tourniquet, fails., Levobupivicaine (Chirocaine) is less cardiotoxic and causes less vasodilation., , Prilocaine, , , Similar mechanism of action to other local anaesthetic agents. However, it is far less, cardiotoxic and is therefore the agent of choice for intravenous regional anaesthesia e.g., Biers Block., , All local anaesthetic agents dissociate in tissues and this contributes to their therapeutic effect. The, dissociation constant shifts in tissues that are acidic e.g. where an abscess is present, and this, reduces the efficacy., Doses of local anaesthetics, , Agent, , Dose plain, , Dose with adrenaline, , Lignocaine, , 3mg/Kg, , 7mg/Kg, , Bupivacaine, , 2mg/Kg, , 2mg/Kg, , Prilocaine, , 6mg/Kg, , 9mg/Kg, , These are a guide only as actual doses depend on site of administration, tissue vascularity and comorbidities.
Page 133 :
Maximum total local anaesthetic doses, , , , , Lignocaine 1% plain - 3mg/ Kg - 200mg (20ml), Lignocaine 1% with 1 in 200,000 adrenaline - 7mg/Kg - 500mg (50ml), Bupivicaine 0.5% - 2mg/kg- 150mg (30ml), , Maximum doses are based on ideal body weight, Effects of adrenaline, Adrenaline may be added to local anaesthetic drugs. It prolongs the duration of action at the site of, injection and permits usage of higher doses (see above). It is contra indicated in patients taking, MAOI's or tricyclic antidepressants. The toxicity of bupivacaine is related to protein binding and, addition of adrenaline to this drug does not permit increases in the total dose of bupivacaine, in, contrast to the situation with lignocaine., References, An excellent review is provided by:, French J and Sharp L. Local Anaesthetics. Ann R Coll Surg Engl 2012; 94: 76-80., Next question
Page 134 :
A 22 year old man suffers a blunt head injury. He is drowsy and has a GCS of 7 on admission., Which of the following is the major determinant of cerebral blood flow in this situation?, , Systemic blood pressure, , Mean arterial pressure, , Intra cranial pressure, , Hypoxaemia, , Acidosis, , Theme from 2009 Exam, Hypoxaemia and acidosis may both affect cerebral blood flow. However, in the traumatic situation, increases in intracranial pressure are far more likely to occur especially when GCS is low. This will, adversely affect cerebral blood flow., Please rate this question:, , Discuss and give feedback, , Next question, , Cerebral blood flow, , , , , , , , CNS autoregulates its own blood supply, Factors affecting the cerebral pressure include; systemic carbon dioxide levels, CNS, metabolism, CNS trauma, CNS pressure, The PaCO2 is the most potent mediator, Acidosis and hypoxaemia will increase cerebral blood flow but to a lesser degree, Intra cranial pressure may increase in patients with head injuries and this can result in, impaired blood flow, Intra cerebral pressure is governed by Monroe-Kelly Doctrine which considers brain as, closed box, changes in pressure are offset by loss of CSF. When this is no longer possible, ICP rises, Next question
Page 135 :
A 43 year old man has recurrent episodes of dyspepsia and treatment is commenced with oral, antacids. Which of the hormones listed below is released in response to increased serum gastrin, levels and decreases intra gastric pH?, , Cholecystokinin, , Histamine, , Somatostatin, , Insulin, , Vasoactive intestinal peptide, , Theme from January 2013 Exam, Histamine is released from enterochromaffin cells in the stomach mucosa which stimulates acid, secretion. It is usually released in response to increased serum gastrin levels. Histamine blockers, (e.g. cimetidine) were extremely popular treatments until the advent of proton pump inhibitors., Please rate this question:, , Discuss and give feedback, , Next question, , Gastric secretions, A working knowledge of gastric secretions is important for surgery because peptic ulcers are, common, surgeons frequently prescribe anti secretory drugs and because there are still patients, around who will have undergone acid lowering procedures (Vagotomy) in the past., Gastric acid, , , , , , Is produced by the parietal cells in the stomach, pH of gastric acid is around 2 with acidity being maintained by the H +/K+ ATP ase pump. As, part of the process bicarbonate ions will be secreted into the surrounding vessels., Sodium and chloride ions are actively secreted from the parietal cell into the canaliculus., This sets up a negative potential across the membrane and as a result sodium and, potassium ions diffuse across into the canaliculus., Carbonic anhydrase forms carbonic acid which dissociates and the hydrogen ions formed by, dissociation leave the cell via the H+/K+ antiporter pump. At the same time sodium ions are, actively absorbed. This leaves hydrogen and chloride ions in the canaliculus these mix and, are secreted into the lumen of the oxyntic gland.
Page 136 :
This is illustrated diagrammatically below:, , Image sourced from Wikipedia, , Phases of gastric acid secretion, There are 3 phases of gastric secretion:, 1. Cephalic phase (smell / taste of food), , , , 30% acid produced, Vagal cholinergic stimulation causing secretion of HCL and gastrin release from G cells, , 2. Gastric phase (distension of stomach ), , , , 60% acid produced, Stomach distension/low H+/peptides causes Gastrin release
Page 137 :
3. Intestinal phase (food in duodenum), , , , 10% acid produced, High acidity/distension/hypertonic solutions in the duodenum inhibits gastric acid secretion, via enterogastrones (CCK, secretin) and neural reflexes., , Regulation of gastric acid production, Factors increasing production include:, , , , , Vagal nerve stimulation, Gastrin release, Histamine release (indirectly following gastrin release) from enterchromaffin like cells, , Factors decreasing production include:, , , , , Somatostatin (inhibits histamine release), Cholecystokinin, Secretin, , The diagram below illustrates some of the factors involved in regulating gastric acid secretion and, the relevant associated pharmacology, , Image sourced from Wikipedia, , Below is a brief summary of the major hormones involved in food digestion:
Page 138 :
Source, , Stimulus, , Actions, , Gastrin, , G cells in, antrum of the, stomach, , Distension of, stomach, extrinsic, nerves, Inhibited by: low, antral pH,, somatostatin, , Increase HCL, pepsinogen and IF secretion,, increases gastric motility, trophic effect on, gastric mucosa, , CCK, , I cells in, upper small, intestine, , Partially digested, proteins and, triglycerides, , Increases secretion of enzyme-rich fluid, from pancreas, contraction of gallbladder, and relaxation of sphincter of Oddi,, decreases gastric emptying, trophic effect on, pancreatic acinar cells, induces satiety, , Secretin, , S cells in, upper small, intestine, , Acidic chyme,, fatty acids, , Increases secretion of bicarbonate-rich fluid, from pancreas and hepatic duct cells,, decreases gastric acid secretion, trophic, effect on pancreatic acinar cells, , VIP, , Small, intestine,, pancreas, , Neural, , Stimulates secretion by pancreas and, intestines, inhibits acid and pepsinogen, secretion, , Somatostatin, , D cells in the, pancreas and, stomach, , Fat, bile salts and, glucose in the, intestinal lumen, , Decreases acid and pepsin secretion,, decreases gastrin secretion, decreases, pancreatic enzyme secretion, decreases, insulin and glucagon secretion, inhibits trophic effects of gastrin, stimulates, gastric mucous production, Next question
Page 139 :
Which main group of receptors does dobutamine bind to?, , α-1, , α-2, , ß-1, , ß-2, , D-1, , Dobutamine is a sympathomimetic with both alpha- and beta-agonist properties; it displays a, considerable selectivity for beta1-cardiac receptors., Please rate this question:, , Discuss and give feedback, , Next question, , Inotropes and cardiovascular receptors, Inotropes are a class of drugs which work primarily by increasing cardiac output. They should be, distinguished from vasoconstrictor drugs which are used specifically when the primary problem is, peripheral vasodilatation., Catecholamine type agents are commonly used and work by increasing cAMP levels by adenylate, cyclase stimulation. This in turn intracellular calcium ion mobilisation and thus the force of, contraction. Adrenaline works as a beta adrenergic receptor agonist at lower doses and an alpha, receptor agonist at higher doses. Dopamine causes dopamine receptor mediated renal and, mesenteric vascular dilatation and beta 1 receptor agonism at higher doses. This results in, increased cardiac output. Since both heart rate and blood pressure are raised, there is less overall, myocardial ischaemia. Dobutamine is a predominantly beta 1 receptor agonist with weak beta 2 and, alpha receptor agonist properties. Noradrenaline is a catecholamine type agent and predominantly
Page 141 :
Which of the following is responsible for the release and synthesis of calcitonin?, , Parathyroid glands, , Anterior pituitary, , Thyroid gland, , Posterior pituitary, , Adrenal glands, , Calcitonin has the opposite effect of PTH and is released from the thyroid gland., Please rate this question:, , Discuss and give feedback, , Next question, , Calcium homeostasis, Calcium ions are linked to a wide range of physiological processes. The largest store of bodily, calcium is contained within the skeleton. Calcium levels are primarily controlled by parathyroid, hormone, vitamin D and calcitonin., Hormonal regulation of calcium, , Hormone, , Parathyroid hormone (PTH), , Actions, , , , , , , , , Increase calcium levels and decrease phosphate, levels, Increases bone resorption, Immediate action on osteoblasts to increase ca2+ in, extracellular fluid, Osteoblasts produce a protein signaling molecule, that activate osteoclasts which cause bone, resorption, Increases renal tubular reabsorption of calcium, Increases synthesis of 1,25(OH)2D (active form, of vitamin D) in the kidney which increases
Page 142 :
Hormone, , Actions, , , , 1,25-dihydroxycholecalciferol (the, active form of vitamin D), , Calcitonin, , , , , bowel absorption of Ca2+, Decreases renal phosphate reabsorption, , , , , Increases plasma calcium and plasma phosphate, Increases renal tubular reabsorption and gut, absorption of calcium, Increases osteoclastic activity, Increases renal phosphate reabsorption, , , , , , , Secreted by C cells of thyroid, Inhibits intestinal calcium absorption, Inhibits osteoclast activity, Inhibits renal tubular absorption of calcium, , Both growth hormone and thyroxine also play a small role in calcium metabolism., Next question
Page 143 :
What is the half life of insulin in the circulation of a normal healthy adult?, , Less than 30 minutes, , Between 1 and 2 hours, , Between 2 and 3 hours, , Between 4 and 5 hours, , Over 6 hours, , Insulin is degraded by enzymes in the circulation. It typically has a half life of less than 30 minutes., Abnormalities of the clearance of insulin may occur in type 2 diabetes., Please rate this question:, , Discuss and give feedback, , Next question, , Insulin, Insulin is a peptide hormone, produced by beta cells of the pancreas, and is central to regulating, carbohydrate and fat metabolism in the body. Insulin causes cells in the liver, skeletal muscles, and, fat tissue to absorb glucose from the blood. In the liver and skeletal muscles, glucose is stored as, glycogen, and in fat cells (adipocytes) it is stored as triglycerides., Structure, The human insulin protein is composed of 51 amino acids, and has a molecular weight of 5808 Da. It, is a dimer of an A-chain and a B-chain, which are linked together by disulfide bonds., Synthesis, Pro-insulin is formed by the rough endoplasmic reticulum in pancreatic beta cells. Then pro-insulin is, cleaved to form insulin and C-peptide. Insulin is stored in secretory granules and released in, response to Ca2+., Function, , , , , , Secreted in response to hyperglycaemia, Glucose utilisation and glycogen synthesis, Inhibits lipolysis, Reduces muscle protein loss
Page 144 :
Which of the following statements about blood clotting is untrue?, , Platelet adhesion to disrupted endothelium is dependent upon von Willebrand factor, , Protein C is a vitamin K dependent substance, , The bleeding time provides an assessment of platelet function, , The prothrombin time tests the extrinsic system, , Administration of aprotinin during liver transplantation surgery prolongs survival, , Although aprotinin reduces fibrinolysis and thus bleeding, it is associated with increased risk of death, and was withdrawn in 2007. Protein C is dependent upon vitamin K and this may paradoxically, increase the risk of thrombosis during the early phases of warfarin treatment., Please rate this question:, , Discuss and give feedback, , Next question, , Coagulation cascade, Two pathways lead to fibrin formation, Intrinsic pathway (components already present in the blood), , , , , , , , Minor role in clotting, Subendothelial damage e.g. collagen, Formation of the primary complex on collagen by high-molecular-weight kininogen (HMWK),, prekallikrein, and Factor 12, Prekallikrein is converted to kallikrein and Factor 12 becomes activated, Factor 12 activates Factor 11, Factor 11 activates Factor 9, which with its co-factor Factor 8a form the tenase complex, which activates Factor 10, , Extrinsic pathway (needs tissue factor released by damaged tissue), , , , Tissue damage, Factor 7 binds to Tissue factor
Page 145 :
, , , This complex activates Factor 9, Activated Factor 9 works with Factor 8 to activate Factor 10, , Common pathway, , , , Activated Factor 10 causes the conversion of prothrombin to thrombin, Thrombin hydrolyses fibrinogen peptide bonds to form fibrin and also activates factor 8 to, form links between fibrin molecules, , Fibrinolysis, Plasminogen is converted to plasmin to facilitate clot resorption, , Image sourced from Wikipedia, , Intrinsic pathway, , Increased APTT, , Factors 8,9,11,12, , Extrinsic pathway, , Increased PT, , Factor 7, , Common pathway, , Increased APTT & PT, , Factors 2,5,10, , Vitamin K dependent, , Factors 2,7,9,10, Next question
Page 146 :
Theme: Management of vomiting, , A., B., C., D., E., F., , Ondansetron, Metoclopramide, Cyclizine, Erythromycin, Cisapride, Haloperidol, , Please select the most appropriate drug for the given scenario. Each option may be used once,, more than once or not at all., , 13., , A 78 year old man with diabetes develops autonomic gastropathy with persistent and, troublesome vomiting., You answered Ondansetron, The correct answer is Erythromycin, Unlike metoclopramide. the effects of erythromycin on gastric emptying are not mediated, via the vagus nerve., , 14., , A drug which blocks the chemoreceptor trigger zone in the area postrema., Ondansetron, 5 HT3 blockers are most effective for many types of nausea for this reason., , 15., , A 48 year old man with oesphageal varices has a profuse haemorrhage on the ward., You answered Ondansetron, The correct answer is Metoclopramide, Intravenous metoclopramide causes increased oesophageal pressure and this may, temporarily slow the rate of haemorrhage whilst more definitive measures are instigated., , Please rate this question:, , Discuss and give feedback, , Next question
Page 147 :
Vomiting, Reflex oral expulsion of gastric (and sometimes intestinal) contents - reverse peristalsis and, abdominal contraction, The vomiting centre is in part of the medulla oblongata and is triggered by receptors in several, locations:, , , , , , , Labyrinthine receptors of ear (motion sickness), Over distention receptors of duodenum and stomach, Trigger zone of CNS - many drugs (e.g., opiates) act here, Touch receptors in throat, Next question
Page 148 :
Which of the following cell types is least likely to be found in a wound 1 week following injury?, , Macrophages, , Fibroblasts, , Myofibroblasts, , Endothelial cells, , Neutrophils, , Theme from April 2012 Exam, Myofibroblasts are differentiated fibroblasts, in which the cytoskeleton contains actin filaments., These cell types facilitate wound contracture and are the hallmark of a mature wound. They are, almost never found in wounds less than 1 month old., Please rate this question:, , Discuss and give feedback, , Next question, , Phases of wound healing, Phase, , Key features, , Cells, , Timeframe, , Haemostasis, , , , , Vasospasm in adjacent vessels, Platelet plug formation and, generation of fibrin rich clot, , Erythrocytes and, platelets, , Seconds/, Minutes, , Inflammation, , , , Neutrophils migrate into wound, (function impaired in diabetes)., Growth factors released, including, basic fibroblast growth factor and, vascular endothelial growth factor., Fibroblasts replicate within the, adjacent matrix and migrate into, wound., , Neutrophils,, fibroblasts and, macrophages, , Days, , , ,
Page 149 :
Regeneration, , , , Macrophages and fibroblasts, couple matrix regeneration and clot, substitution., , , , Platelet derived growth factor and, transformation growth factors, stimulate fibroblasts and epithelial, cells., Fibroblasts produce a collagen, network., Angiogenesis occurs and wound, resembles granulation tissue., , Fibroblasts,, endothelial cells,, macrophages, , Weeks, , Longest phase of the healing, process and may last up to one year, (or longer)., During this phase fibroblasts, become differentiated, (myofibroblasts) and these, facilitate wound contraction., Collagen fibres are remodelled., Microvessels regress leaving a pale, scar., , Myofibroblasts, , 6 weeks to 1, year, , , , , Remodelling, , , , , , , , , Next question
Page 150 :
The blood - brain barrier is not highly permeable to which of the following?, , Carbon dioxide, , Barbituates, , Glucose, , Oxygen, , Hydrogen ions, , The blood brain barrier is relatively impermeable to highly dissociated compounds., Please rate this question:, , Discuss and give feedback, , Next question, , Cerebrospinal fluid, The CSF fills the space between the arachnoid mater and pia mater (covering surface of the brain)., The total volume of CSF in the brain is approximately 150ml. Approximately 500 ml is produced by, the ependymal cells in the choroid plexus (70%), or blood vessels (30%). It is reabsorbed via the, arachnoid granulations which project into the venous sinuses., Circulation, 1. Lateral ventricles (via foramen of Munro), 2. 3rd ventricle, 3. Cerebral aqueduct (aqueduct of Sylvius), 4. 4th ventricle (via foramina of Magendie and Luschka), 5. Subarachnoid space, 6. Reabsorbed into the venous system via arachnoid granulations into superior sagittal sinus, Composition, , , , , , Glucose: 50-80mg/dl, Protein: 15-40 mg/dl, Red blood cells: Nil, White blood cells: 0-3 cells/ mm3, Next question
Page 151 :
A 43 year old presents to the urology clinic complaining of impotence. Which of the following will, occur in response to increased penile parasympathetic stimulation?, , Detumescence, , Ejaculation, , Erection, , Vasospasm of the penile branches of the pudendal artery, , Contraction of the smooth muscle in the epididymis and vas deferens, Memory aid for erection, p=parasympathetic=points, s=sympathetic=shoots, Parasympathetic stimulation causes erection. Sympathetic stimulation will produce ejaculation,, detumescence and vasospasm of the pudendal artery. It will also cause contraction of the smooth, muscle in the epididymis and vas to convey the ejaculate., Please rate this question:, , Discuss and give feedback, , Next question, , Penile erection, Physiology of erection, , Autonomic, , , , , Somatic, nerves, , Sympathetic nerves originate from T11-L2 and parasympathetic nerves, from S2-4 join to form pelvic plexus., Parasympathetic discharge causes erection, sympathetic discharge causes, ejaculation and detumescence., , Supplied by dorsal penile and pudendal nerves. Efferent signals are relayed from, Onufs nucleus (S2-4) to innervate ischiocavernosus and bulbocavernosus muscles., , Autonomic discharge to the penis will trigger the veno-occlusive mechanism which triggers the flow, of arterial blood into the penile sinusoidal spaces. As the inflow increases the increased volume in, this space will secondarily lead to compression of the subtunical venous plexus with reduced venous
Page 152 :
return. During the detumesence phase the arteriolar constriction will reduce arterial inflow and, thereby allow venous return to normalise., Priapism, Prolonged unwanted erection, in the absence of sexual desire, lasting more than 4 hours., Classification of priaprism, , Low flow priaprism, , Due to veno-occlusion (high intracavernosal pressures)., , , , , , , High flow priaprism, , Due to unregulated arterial blood flow., , , Recurrent priaprism, , Most common type, Often painful, Often low cavernosal flow, If present for >4 hours requires emergency treatment, , Usually presents as semi rigid painless erection, , Typically seen in sickle cell disease, most commonly of high flow type., , Causes, , , , , , Intracavernosal drug therapies (e.g. for erectile dysfunction>, Blood disorders such as leukaemia and sickle cell disease, Neurogenic disorders such as spinal cord transection, Trauma to penis resulting in arterio-venous malformations, , Tests, , , , Exclude sickle cell/ leukaemia, Consider blood sampling from cavernosa to determine whether high or low flow (low flow is, often hypoxic), , Management, , , , , Ice packs/ cold showers, If due to low flow then blood may be aspirated from copora or try intracavernosal alpha, adrenergic agonists., Delayed therapy of low flow priaprism may result in erectile dysfunction.
Page 153 :
, , Which of the following best accounts for the action of PTH in increasing serum calcium, levels?, , Activation of vitamin D to increase absorption of calcium from the small intestine., , Direct stimulation of osteoclasts to absorb bone with release of calcium., , Stimulation of phosphate absorption at the distal convoluted tubule of the kidney., , Decreased porosity of the vessels at Bowmans capsule to calcium., , Vasospasm of the afferent renal arteriole thereby reducing GFR and calcium urinary loss., , , , , Theme from April 2012 Exam, PTH increases the activity of 1-α-hydroxylase enzyme, which converts 25hydroxycholecalciferol to 1,25-dihydroxycholecalciferol, the active form of vitamin D., Osteoclasts do not have a PTH receptor and effects are mediated via osteoblasts., Please rate this question:, , , , , , Discuss and give feedback, , , , Next question, , , , Parathyroid hormone, , , , Parathyroid hormone is secreted by the chief cells of the parathyroid glands. It acts to, increase serum calcium concentration by stimulation of the PTH receptors in the kidney and, bone. PTH has a plasma half life of 4 minutes., Effects of PTH, , Bone, , Binds to osteoblasts which signal to osteoclasts to cause resorption of bone and, release calcium.
Page 154 :
Kidney, , Active reabsorption of calcium and magnesium from the distal convoluted tubule., Decreases reabsorption of phosphate., , Intestine via, kidney, , Increases intestinal calcium absorption by increasing activated vitamin D. Activated, vitamin D increases calcium absorption., , , , , Next question
Page 155 :
Which of the following drugs does not cause syndrome of inappropriate anti diuretic hormone, release?, , Haloperidol, , Carbamazepine, , Amitriptylline, , Cyclophosphamide, , Methotrexate, Drugs causing SIADH: ABCD, A nalgesics: opioids, NSAIDs, B arbiturates, C yclophosphamide/ Chlorpromazine/ Carbamazepine, D iuretic (thiazides), Please rate this question:, , Discuss and give feedback, , Next question, , Hyponatraemia, This is commonly tested in the MRCS (despite most surgeons automatically seeking medical advice, if this occurs!). The most common cause in surgery is the over administration of 5% dextrose., Hyponatraemia may be caused by water excess or sodium depletion. Causes of, pseudohyponatraemia include hyperlipidaemia (increase in serum volume) or a taking blood from a, drip arm. Urinary sodium and osmolarity levels aid making a diagnosis., Classification, , Urinary sodium > 20, mmol/l, , Sodium depletion, renal loss, , , Patient often hypovolaemic, , Mnemonic: Syndrome of, INAPPropriate AntiDiuretic Hormone:, In creased, Na (sodium)
Page 156 :
, , , , , , , Urinary sodium < 20, mmol/l, , PP (urine), , Sodium depletion, extra-renal loss, , , , Water excess (patient, often hypervolaemic and, oedematous), , Diuretics (thiazides), Addison's, Diuretic stage of renal failure, SIADH (serum osmolality, low, urine osmolality high,, urine Na high), Patient often euvolaemic, , , , , , , Diarrhoea, vomiting,, sweating, Burns, adenoma of rectum (if, villous lesion and large), Secondary, hyperaldosteronism: CCF,, cirrhosis, Reduced GFR: renal failure, IV dextrose, psychogenic, polydipsia, , Management, Symptomatic Hyponatremia :, Acute hyponatraemia with Na <120: immediate therapy. Central Pontine Myelinolisis, may occur, from overly rapid correction of serum sodium. Aim to correct until the Na is > 125 at a rate of 1, mEq/h. Normal saline with frusemide is an alternative method., The sodium requirement can be calculated as follows :, (125 - serum sodium) x 0.6 x body weight = required mEq of sodium, Next question
Page 157 :
Which of the following changes are not typically seen in established dehydration?, , Rising haematocrit, , Urinary sodium <20mmol/ litre, , Metabolic acidosis, , Decreased serum urea to creatinine ratio, , Hypernatraemia, , Diagnosing dehydration can be complicated, laboratory features include:, , , , , , , , , Hypernatraemia, Rising haematocrit, Metabolic acidosis, Rising lactate, Increased serum urea to creatinine ratio, Urinary sodium <20 mmol/litre, Urine osmolality approaching 1200mosmol/kg, , Please rate this question:, , Discuss and give feedback, , Next question, , Pre operative fluid management, Fluid management has been described in the British Consensus guidelines on IV fluid, therapy for Adult Surgical patients (GIFTASUP) and by NICE (CG174 December 2013), The Recommendations include:, , , , Use Ringer's lactate or Hartmann's when a crystalloid is needed for resuscitation or, replacement of fluids. Avoid 0.9% N. Saline (due to risk of hyperchloraemic acidosis) unless, patient vomiting or has gastric drainage., Use 4%/0.18% dextrose saline or 5% dextrose in maintenance fluids. It should not be used, in resuscitation or as replacement fluids.
Page 158 :
, , , , , , , , , , , , , Adult maintenance fluid requirements are: Na 50-100 mmol/day and K 40-80 mmol/day in, 1.5-2.5L fluid per day., Patients for elective surgery should NOT be nil by mouth for >2 hours (unless has disorder of, gastric emptying)., Patients for elective surgery should be given carbohydrate rich drinks 2-3h before. Ideally, this should form part of a normal pre op plan to facilitate recovery., Avoid mechanical bowel preparation., If bowel prep is used, simultaneous administration of Hartmann's or Ringer's lactate should, be considered., Excessive fluid losses from vomiting should be treated with a crystalloid with potassium, replacement. 0.9% N. Saline should be given if there is hypochloraemia. Otherwise, Hartmann's or Ringer lactate should be given for diarrhoea/ileostomy/ileus/obstruction., Hartmann's should also be given in sodium losses secondary to diuretics., High risk patients should receive fluids and inotropes., An attempt should be made to detect pre or operative hypovolaemia using flow based, measurements. If this is not available, then clinical evaluation is needed i.e. JVP, pulse, volume etc., In Blood loss or infection causing hypovolaemia should be treated with a balanced crystalloid, or colloid (or until blood available in blood loss). A critically ill patient is unable to excrete Na, or H20 leading to a 5% risk of interstitial oedema. Therefore 5% dextrose as well as colloid, should be given., If patients need IV fluid resuscitation, use crystalloids that contain sodium in the range 130154 mmol/l, with a bolus of 500 ml over less than 15 minutes (NICE Guidance CG 174)., Next question
Page 159 :
A 67 year old male is admitted to the surgical unit with acute abdominal pain. He is found to have a, right sided pneumonia. The nursing staff put him onto 15L O 2 via a non rebreathe mask. After 30, minutes the patient is found moribund, sweaty and agitated by the nursing staff. An arterial blood, gas reveals:, , pH, , 7.15, , pCO2, , 10.2, , pO2, , 8, , Bicarbonate, , 32, , Base excess, , - 5.2, , What is the most likely cause for this patients deterioration?, , Acute respiratory alkalosis secondary to hyperventilation, , Over administration of oxygen in a COPD patient, , Metabolic acidosis secondary to severe pancreatitis, , Metabolic alkalosis secondary to hypokalaemia, , Acute respiratory acidosis secondary to pneumonia, , Theme from April 2012 exam, This patient has an acute respiratory acidosis, however this is on a background of chronic, respiratory acidosis (due to COPD) with a compensatory metabolic alkalosis (the elevated, bicarbonate is the main clue to the chronic nature of the respiratory acidosis). This blood gas picture, is typical in a COPD patient who has received too much oxygen; these patients lose their hypoxic
Page 160 :
drive for respiration, therefore retain CO2 and subsequently hypoventilate leading to respiratory, arrest. If the bicarbonate was normal, then the answer would be acute respiratory acidosis, secondary to pneumonia., Please rate this question:, , Discuss and give feedback, , Next question, , Arterial blood gas interpretation, In advanced life support training, a 5 step approach to arterial blood gas interpretation is advocated., 1. How is the patient?, 2. Is the patient hypoxaemic?, The Pa02 on air should be 10.0-13.0 kPa, 3. Is the patient acidaemic (pH <7.35) or alkalaemic (pH >7.45), 4. What has happened to the PaCO2?, If there is acidaemia, an elevated PaCO2 will account for this, 5. What is the bicarbonate level or base excess?, A metabolic acidosis will have a low bicarbonate level and a low base excess (< -2 mmol), A metabolic alkalosis will have a high bicarbonate and a high base excess (> +2 mmol), , Next question
Page 161 :
Which of the following statements relating to the pharmacology of warfarin is untrue?, , Interferes with clotting factors 2,7,9 and 10, , It may not be clinically effective for up to 72 hours, , The half life of warfarin is 40 hours, , Warfarin has a large volume of distribution, , It is metabolized in the liver, Factors 2,7,9,10 affected, Warfarin interferes with fibrin formation by affecting carboxylation of glutamic acid residues in factors, 2,7,9 and 10. Factor 2 has the longest half life of approximately 60 hours, therefore it can take up to, 3 days for warfarin to be fully effective. Warfarin has a small volume of distribution as it is protein, bound., Please rate this question:, , Discuss and give feedback, , Next question, , Warfarin, Warfarin is an oral anticoagulant which inhibits the reduction of vitamin K to its active hydroquinone, form, which in turn acts as a cofactor in the formation of clotting factor II, VII, IX and X (mnemonic =, 1972) and protein C, Factors that may potentiate warfarin, , , , , , , Liver disease, P450 enzyme inhibitors, e.g.: amiodarone, ciprofloxacin, Cranberry juice, Drugs which displace warfarin from plasma albumin, e.g. NSAIDs, Inhibit platelet function: NSAIDs, , Side-effects
Page 162 :
, , , , Haemorrhage, Teratogenic, Skin necrosis: when warfarin is first started biosynthesis of protein C is reduced. This results, in a temporary procoagulant state after initially starting warfarin, normally avoided by, concurrent heparin administration. Thrombosis may occur in venules leading to skin, necrosis., Next question
Page 163 :
Which of the following does not cause an increased anion gap acidosis?, , Uraemia, , Paraldehyde, , Diabetic ketoacidosis, , Ethylene glycol, , Acetazolamide, Causes of increased anion acidosis: MUDPILES, M - Methanol, U - Uraemia, D - DKA/AKA, P - Paraldehyde/phenformin, I - Iron/INH, L - Lactic acidosis, E - Ethylene glycol, S - Salicylates, Please rate this question:, , Discuss and give feedback, , Next question, , Disorders of acid - base balance, Disorders of acid- base balance are often covered in the MRCS part A, both in the SBA and EMQ, sections., The acid-base normogram below shows how the various disorders may be categorised
Page 164 :
Image sourced from Wikipedia, , Metabolic acidosis, , , , , This is the most common surgical acid - base disorder., Reduction in plasma bicarbonate levels., Two mechanisms:, , 1. Gain of strong acid (e.g. diabetic ketoacidosis), 2. Loss of base (e.g. from bowel in diarrhoea), - Classified according to the anion gap, this can be calculated by:, (Na+ + K+) - (Cl- + HCO3-)., - If a question supplies the chloride level then this is often a clue that the anion gap should be, calculated. The normal range = 10-18 mmol/L, Normal anion gap ( = hyperchloraemic metabolic acidosis), , , , , , , Gastrointestinal bicarbonate loss: diarrhoea, ureterosigmoidostomy, fistula, Renal tubular acidosis, Drugs: e.g. acetazolamide, Ammonium chloride injection, Addison's disease, , Raised anion gap
Page 165 :
, , , , , Lactate: shock, hypoxia, Ketones: diabetic ketoacidosis, alcohol, Urate: renal failure, Acid poisoning: salicylates, methanol, , Metabolic acidosis secondary to high lactate levels may be subdivided into two types:, , , , Lactic acidosis type A: (Perfusion disorders e.g.shock, hypoxia, burns), Lactic acidosis type B: (Metabolic e.g. metformin toxicity), , Metabolic alkalosis, , , , , Usually caused by a rise in plasma bicarbonate levels., Rise of bicarbonate above 24 mmol/L will typically result in renal excretion of excess, bicarbonate., Caused by a loss of hydrogen ions or a gain of bicarbonate. It is due mainly to problems of, the kidney or gastrointestinal tract, , Causes, , , , , , , , , , Vomiting / aspiration (e.g. Peptic ulcer leading to pyloric stenosis, nasogastric suction), Diuretics, Liquorice, carbenoxolone, Hypokalaemia, Primary hyperaldosteronism, Cushing's syndrome, Bartter's syndrome, Congenital adrenal hyperplasia, , Mechanism of metabolic alkalosis, , , , , , Activation of renin-angiotensin II-aldosterone (RAA) system is a key factor, Aldosterone causes reabsorption of Na+ in exchange for H+ in the distal convoluted tubule, ECF depletion (vomiting, diuretics) → Na+ and Cl- loss → activation of RAA system → raised, aldosterone levels, In hypokalaemia, K+ shift from cells → ECF, alkalosis is caused by shift of H + into cells to, maintain neutrality
Page 166 :
Respiratory acidosis, , , , Rise in carbon dioxide levels usually as a result of alveolar hypoventilation, Renal compensation may occur leading to Compensated respiratory acidosis, , Causes, , , , , COPD, Decompensation in other respiratory conditions e.g. Life-threatening asthma / pulmonary, oedema, Sedative drugs: benzodiazepines, opiate overdose, , Respiratory alkalosis, , , , Hyperventilation resulting in excess loss of carbon dioxide, This will result in increasing pH, , Causes, , , , , , , Psychogenic: anxiety leading to hyperventilation, Hypoxia causing a subsequent hyperventilation: pulmonary embolism, high altitude, Early salicylate poisoning*, CNS stimulation: stroke, subarachnoid haemorrhage, encephalitis, Pregnancy, , *Salicylate overdose leads to a mixed respiratory alkalosis and metabolic acidosis. Early stimulation, of the respiratory centre leads to a respiratory alkalosis whilst later the direct acid effects of, salicylates (combined with acute renal failure) may lead to an acidosis, Next question
Page 167 :
Which one of the following is least associated with thrombocytopenia?, , Heparin therapy, , Rheumatoid arthritis, , Infectious mononucleosis, , Liver disease, , Pregnancy, , Rheumatoid arthritis, unlike systemic lupus erythematous, is generally associated with a, thrombocytosis. In some cases of Felty's syndrome thrombocytopaenia may be seen secondary to, hypersplenism. This however represents a small percentage of patients with rheumatoid arthritis., Please rate this question:, , Discuss and give feedback, , Next question, , Thrombocytopenia, Causes of severe thrombocytopenia, , , , , , ITP, DIC, TTP, haematological malignancy, , Causes of moderate thrombocytopenia, , , , , , , , , , heparin induced thrombocytopenia (HIT), drug-induced (e.g. quinine, diuretics, sulphonamides, aspirin, thiazides), alcohol, liver disease, hypersplenism, viral infection (EBV, HIV, hepatitis), pregnancy, SLE/antiphospholipid syndrome
Page 169 :
Which of the following will increase the volume of pancreatic exocrine secretions?, , Octreotide, , Cholecystokinin, , Aldosterone, , Adrenaline, , None of the above, , Cholecystokinin will often increase the volume of pancreatic secretions., Please rate this question:, , Discuss and give feedback, , Next question, , Pancreas exocrine physiology, Composition of pancreatic secretions, Pancreatic secretions are usually 1000-1500ml per 24 hours and have a pH of 8., Secretion, , Enzymic, , Aqueous, , Source, , Substances secreted, , Acinar cells, , Trypsinogen, Procarboxylase, Amylase, Elastase, , Ductal and, , Sodium, Bicarbonate
Page 170 :
Centroacinar cells, , Water, Potassium, Chloride, NB: Sodium and potassium reflect their plasma levels; chloride, and bicarbonate vary with flow rate, , Regulation, The cephalic and gastric phases (neuronal and physical) are less important in regulating the, pancreatic secretions. The effect of digested material in the small bowel stimulates CCK release and, ACh which stimulate acinar and ductal cells. Of these CCK is the most potent stimulus. In the case, of the ductal cells these are potently stimulated by secretin which is released by the S cells of the, duodenum. This results in an increase in bicarbonate., Enzyme activation, Trypsinogen is converted via enterokinase to active trypsin in the duodenum. Trypsin then activates, the other inactive enzymes, Next question
Page 171 :
Where is the majority of iron found in the body?, , Bone, , Haemoglobin, , Ferritin and haemosiderin, , Myoglobin, , Plasma iron, , Approximately 70% of body iron is found bound to haemoglobin., Please rate this question:, , Discuss and give feedback, , Next question, , Iron metabolism, Absorption, , , , , , , , , , Duodenum and upper jejunum, About 10% of dietary iron absorbed, Fe2+ (ferrous iron) much better absorbed than Fe3+ (ferric iron), Ferrous iron is oxidized to form ferric iron, which is combined with, apoferritin to form ferritin, Absorption is regulated according to body's need, Increased by vitamin C, gastric acid, Decreased by proton pump inhibitors, tetracycline, gastric achlorhydria,, tannin (found in tea), , Transport, , In plasma as Fe3+ bound to transferrin, , Storage, , Ferritin (or haemosiderin) in bone marrow, , Excretion, , Lost via intestinal tract following desquamation, , Distribution in body
Page 173 :
A 44 year old man recieves a large volume transfusion of whole blood. The whole blood is two, weeks old. Which of the following best describes its handling of oxygen?, , It will have a low affinity for oxygen, , Its affinity for oxygen is unchanged, , It will more readily release oxygen in metabolically active tissues than fresh blood, , The release of oxygen in metabolically active tissues will be the same as fresh blood, , It will have an increased affinity for oxygen, , Stored blood has less 2,3 DPG and therefore has a higher affinity for oxygen, this reduces its ability, to release it at metabolising tissues., Please rate this question:, , Discuss and give feedback, , Next question, , Oxygen Transport, Oxygen transport, Almost all oxygen is transported within erythrocytes. It has limited solubility and only 1% is carried as, solution. Therefore the amount of oxygen transported will depend upon haemoglobin concentration, and its degree of saturation., Haemoglobin, Globular protein composed of 4 subunits. Haem consists of a protoporphyrin ring surrounding an, iron atom in its ferrous state. The iron can form two additional bonds; one with oxygen and the other, with a polypeptide chain. There are two alpha and two beta subunits to this polypeptide chain in an, adult and together these form globin. Globin cannot bind oxygen but is able to bind to carbon dioxide, and hydrogen ions, the beta chains are able to bind to 2,3 diphosphoglycerate. The oxygenation of, haemoglobin is a reversible reaction. The molecular shape of haemoglobin is such that binding of, one oxygen molecule facilitates the binding of subsequent molecules., Oxygen dissociation curve
Page 174 :
, , , The oxygen dissociation curve describes the relationship between the percentage of, saturated haemoglobin and partial pressure of oxygen in the blood. It is not affected by, haemoglobin concentration., Chronic anaemia causes 2, 3 DPG levels to increase, hence shifting the curve to the right, , Haldane effect, , , Shifts to left = for given oxygen tension there is increased saturation of Hb with oxygen i.e., Decreased oxygen delivery to tissues, , Bohr effect, , , Shifts to right = for given oxygen tension there is reduced saturation of Hb with oxygen i.e., Enhanced oxygen delivery to tissues, , Image sourced from Wikipedia, , Shifts to Left = Lower oxygen delivery, , , HbF, methaemoglobin, carboxyhaemoglobin, , Shifts to Right = Raised oxygen, delivery
Page 175 :
, , , , , low [H+] (alkali), low pCO2, low 2,3-DPG, low temperature, , , , , , , raised [H+] (acidic), raised pCO2, raised 2,3-DPG*, raised temperature, , *2,3-diphosphoglycerate, Next question
Page 176 :
A 43 year old lady undergoes a day case laparoscopic cholecystectomy. The operation is more, difficult than anticipated and a drain is placed to the operative site. Whilst in recovery, the patient, loses 1800ml of frank blood into the drain. Which of the following will not occur?, , Release of aldosterone via the Bainbridge reflex, , Reduced urinary sodium excretion, , Increase in sympathetic discharge to ventricular muscle, , Fall in parasympathetic discharge to the sino atrial node, , Decreased stimulation from atrial pressure receptors, , Theme from 2013 Exam, The Bainbridge reflex is the increase in heart rate mediated via atrial stretch receptors that occurs, following a rapid infusion of blood., Please rate this question:, , Discuss and give feedback, , Next question, , Cardiac physiology, , , , , , The heart has four chambers ejecting blood into both low pressure and high pressure, systems., The pumps generate pressures of between 0-25mmHg on the right side and 0-120 mmHg on, the left., At rest diastole comprises 2/3 of the cardiac cycle., The product of the frequency of heart rate and stroke volume combine to give the cardiac, output which is typically 5-6L per minute., , Detailed descriptions of the various waveforms are often not a feature of MRCS A (although they are, on the syllabus). However, they are a very popular topic for surgical physiology in the MRCS B, exam., Electrical properties, , , Intrinsic myogenic rhythm within cardiac myocytes means that even the denervated heart is, capable of contraction.
Page 177 :
, , , , , In the normal situation the cardiac impulse is generated in the sino atrial node in the right, atrium and conveyed to the ventricles via the atrioventricular node., The sino atrial node is also capable of spontaneous discharge and in the absence of, background vagal tone will typically discharge around 100x per minute. Hence the higher, resting heart rate found in cardiac transplant cases. In the SA and AV nodes the resting, membrane potential is lower than in surrounding cardiac cells and will slowly depolarise from, -70mV to around -50mV at which point an action potential is generated., Differences in the depolarisation slopes between SA and AV nodes help to explain why the, SA node will depolarise first. The cells have a refractory period during which they cannot be, re-stimulated and this period allows for adequate ventricular filling. In pathological, tachycardic states this time period is overridden and inadequate ventricular filling may then, occur, cardiac output falls and syncope may ensue., , Parasympathetic fibres project to the heart via the vagus and will release acetylcholine. Sympathetic, fibres release nor adrenaline and circulating adrenaline comes from the adrenal medulla., Noradrenaline binds to β 1 receptors in the SA node and increases the rate of pacemaker potential, depolarisation., Cardiac cycle, , Image sourced from Wikipedia, , , , Mid diastole: AV valves open. Ventricles hold 80% of final volume. Outflow valves shut., Aortic pressure is high., , , , Late diastole: Atria contract. Ventricles receive 20% to complete filling. Typical end diastolic, volume 130-160ml.
Page 178 :
, , Early systole: AV valves shut. Ventricular pressure rises. Isovolumetric ventricular, contraction. AV Valves bulge into atria (c-wave). Aortic and pulmonary pressure exceededblood is ejected. Shortening of ventricles pulls atria downwards and drops intra atrial, pressure (x-descent)., , , , Late systole: Ventricular muscles relax and ventricular pressures drop. Although ventricular, pressure drops the aortic pressure remains constant owing to peripheral vascular resistance, and elastic property of the aorta. Brief period of retrograde flow that occurs in aortic recoil, shuts the aortic valve. Ventricles will contain 60ml end systolic volume. The average stroke, volume is 70ml (i.e. Volume ejected)., , , , Early diastole: All valves are closed. Isovolumetric ventricular relaxation occurs. Pressure, wave associated with closure of the aortic valve increases aortic pressure. The pressure dip, before this rise can be seen on arterial waveforms and is called the incisura. During systole, the atrial pressure increases such that it is now above zero (v- wave). Eventually atrial, pressure exceed ventricular pressure and AV valves open - atria empty passively into, ventricles and atrial pressure falls (y -descent ), , The negative atrial pressures are of clinical importance as they can allow air embolization to occur if, the neck veins are exposed to air. This patient positioning is important in head and neck surgery to, avoid this occurrence if veins are inadvertently cut, or during CVP line insertion., Mechanical properties, , , , Preload = end diastolic volume, Afterload = aortic pressure, , It is important to understand the principles of Laplace's law in surgery., , , , , It states that for hollow organs with a circular cross section, the total circumferential wall, tension depends upon the circumference of the wall, multiplied by the thickness of the wall, and on the wall tension., The total luminal pressure depends upon the cross sectional area of the lumen and the, transmural pressure. Transmural pressure is the internal pressure minus external pressure, and at equilibrium the total pressure must counterbalance each other., In terms of cardiac physiology the law explains that the rise in ventricular pressure that, occurs during the ejection phase is due to physical change in heart size. It also explains why, a dilated diseased heart will have impaired systolic function.
Page 179 :
Starlings law, , , , Increase in end diastolic volume will produce larger stroke volume., This occurs up to a point beyond which cardiac fibres are excessively stretched and stroke, volume will fall once more. It is important for the regulation of cardiac output in cardiac, transplant patients who need to increase their cardiac output., , Baroreceptor reflexes, , , , , , , Baroreceptors located in aortic arch and carotid sinus., Aortic baroreceptor impulses travel via the vagus and from the carotid via the, glossopharyngeal nerve., They are stimulated by arterial stretch., Even at normal blood pressures they are tonically active., Increase in baroreceptor discharge causes:, , *Increased parasympathetic discharge to the SA node., *Decreased sympathetic discharge to ventricular muscle causing decreased contractility and fall in, stroke volume., *Decreased sympathetic discharge to venous system causing increased compliance., *Decreased peripheral arterial vascular resistance, Atrial stretch receptors, , , , , , , , Located in atria at junction between pulmonary veins and vena cava., Stimulated by atrial stretch and are thus low pressure sensors., Increased blood volume will cause increased parasympathetic activity., Very rapid infusion of blood will result in increase in heart rate mediated via atrial receptors:, theBainbridge reflex., Decreases in receptor stimulation results in increased sympathetic activity this will decrease, renal blood flow-decreases GFR-decreases urinary sodium excretion-renin secretion by, juxtaglomerular apparatus-Increase in angiotensin II., Increased atrial stretch will also result in increased release of atrial natriuretic peptide., Next question
Page 180 :
Approximately what proportion of salivary secretions is provided by the submandibular glands?, , 10%, , 70%, , 40%, , 90%, , 20%, , Although they are small, the submandibular glands provide the bulk of salivary secretions and, contribute 70%, the sublingual glands provide 5% and the remainder from the parotid., Please rate this question:, , Discuss and give feedback, , Next question, , Submandibular gland, Relations of the submandibular gland, , Superficial, , Platysma, deep fascia and mandible, Submandibular lymph nodes, Facial vein (facial artery near mandible), Marginal mandibular nerve, Cervical branch of the facial nerve, , Deep, , Facial artery (inferior to the mandible), Mylohoid muscle, Sub mandibular duct, Hyoglossus muscle, Lingual nerve, Submandibular ganglion, Hypoglossal nerve
Page 181 :
Submandibular duct (Wharton's duct), , , , , Opens lateral to the lingual frenulum on the anterior floor of mouth., 5 cm length, Lingual nerve wraps around Wharton's duct. As the duct passes forwards it crosses medial, to the nerve to lie above it and then crosses back, lateral to it, to reach a position below the, nerve., , Innervation, , , , Sympathetic innervation- Derived from superior cervical ganglion, Parasympathetic innervation- Submandibular ganglion via lingual nerve, , Arterial supply, Branch of the facial artery. The facial artery passes through the gland to groove its deep surface. It, then emerges onto the face by passing between the gland and the mandible., Venous drainage, Anterior facial vein (lies deep to the Marginal Mandibular nerve), Lymphatic drainage, Deep cervical and jugular chains of nodes, Next question
Page 182 :
Which is the least likely to cause hyperuricaemia?, , Severe psoriasis, , Lesch-Nyhan syndrome, , Amiodarone, , Diabetic ketoacidosis, , Alcohol, Mnemonic of the drugs causing hyperuricaemia as a result of reduced excretion of urate, 'Can't leap', C iclosporin, A lcohol, N icotinic acid, T hiazides, L oop diuretics, E thambutol, A spirin, P yrazinamide, Decreased tubular secretion of urate occurs in patients with acidosis (eg, diabetic ketoacidosis,, ethanol or salicylate intoxication, starvation ketosis). The organic acids that accumulate in these, conditions compete with urate for tubular secretion., Please rate this question:, , Discuss and give feedback, , Next question, , Hyperuricaemia, , , Increased levels of uric acid may be seen secondary to either increased cell turnover or, reduced renal excretion of uric acid. Hyperuricaemia may be found in asymptomatic patients, who have not experienced attacks of gout
Page 183 :
, , Hyperuricaemia may be associated with hyperlipidaemia and hypertension. It may also be, seen in conjunction with the metabolic syndrome, , Increased synthesis, , , , , , , , Lesch-Nyhan disease, Myeloproliferative disorders, Diet rich in purines, Exercise, Psoriasis, Cytotoxics, , Decreased excretion, , , , , , , Drugs: low-dose aspirin, diuretics, pyrazinamide, Pre-eclampsia, Alcohol, Renal failure, Lead, Next question
Page 184 :
Which of the following statements relating to low molecular weight heparins is false?, , They act via inhibition of Factor Xa, , Large doses may be used prior to commencing cardiopulmonary bypass, , They have a highly predictable pharmacokinetic profile, , They are derivatives of unfractionated heparin, , They have a molecular mass in the range of 3000-10000Da, , As they are not easily reversed they are unsuitable for this purpose., Please rate this question:, , Discuss and give feedback, , Next question, , Heparin, , , Causes the formation of complexes between antithrombin and activated thrombin/factors, 7,9,10,11 & 12, , Advantages of low molecular weight heparin, , , , , , , Better bioavailability, Lower risk of bleeding, Longer half life, Little effect on APTT at prophylactic dosages, Less risk of HIT, , Complications, , , , , , Bleeding, Osteoporosis, Heparin induced thrombocytopenia (HIT): occurs 5-14 days after 1st exposure, Anaphylaxis
Page 185 :
In surgical patients that may need a rapid return to theatre, administration of unfractionated heparin, is preferred; as low molecular weight heparins have a longer duration of action and are harder to, reverse., Next question
Page 186 :
A 43 year old lady presents with urinary incontinence. At which of the following locations is Onufs, nucleus likely to be found?, , Medulla oblongata, , Anterior horn of L5 nerve roots, , Micturition centre in the Pons, , Anterior horn of S2 nerve roots, , None of the above, , Onufs nucleus is located in the anterior horn of S2 and is the origin of neurones to the external, urethral sphincter., Please rate this question:, , Discuss and give feedback, , Next question, , Urinary incontinence, Involuntary passage of urine. Most cases are female (80%). It has a prevalence of 11% in those, aged greater than 65 years. The commonest variants include:, , , , , Stress urinary incontinence (50%), Urge incontinence (15%), Mixed (35%), , Males, Males may also suffer from incontinence although it is a much rarer condition in men. A number of, anatomical factors contribute to this. Males have 2 powerful sphincters; one at the bladder neck and, the other in the urethra. Damage to the bladder neck mechanism is a factor in causing retrograde, ejaculation following prostatectomy. The short segment of urethra passing through the urogenital, diaphragm consists of striated muscle fibres (the external urethral sphincter) and smooth muscle, capable of more sustained contraction. It is the latter mechanism that maintains continence following, prostatectomy., Females, The sphincter complex at the level of bladder neck is poorly developed in females. As a result the
Page 187 :
external sphincter complex is functionally more important, its composition being similar to that of, males. Innervation is via the pudendal nerve and the neuropathy that may accompany obstetric, events may compromise this and lead to stress urinary incontinence., Innervation, Somatic innervation to the bladder is via the pudendal, hypogastric and pelvic nerves. Autonomic, nerves travel in these nerve fibres too. Bladder filling leads to detrusor relaxation (sympathetic), coupled with sphincter contraction. The parasympathetic system causes detrusor contraction and, sphincter relaxation. Overall control of micturition is centrally mediated via centres in the Pons., Stress urinary incontinence, , , , , 50% of cases, especially in females., Damage (often obstetric) to the supporting structures surrounding the bladder may lead to, urethral hypermobility., Other cases due to sphincter dysfunction, usually from neurological disorders (e.g. Pudendal, neuropathy, multiple sclerosis)., , Urethral mobility:, Pressure not transmitted appropriately to the urethra resulting in involuntary passage of urine during, episodes of raised intra-abdominal pressure., Sphincter dysfunction:, Sphincter fails to adapt to compress urethra resulting in involuntary passage of urine. When the, sphincter completely fails there is often to continuous passage of urine., Urge incontinence, In these patients there is sense of urgency followed by incontinence. The detrusor muscle in these, patients is unstable and urodynamic investigation will demonstrate overactivity of the detrusor, muscle at inappropriate times (e.g. Bladder filling). Urgency may be seen in patients with overt, neurological disorders and those without. The pathophysiology is not well understood but poor, central and peripheral co-ordination of the events surrounding bladder filling are the main, processes., Assessment, Careful history and examination including vaginal examination for cystocele., Bladder diary for at least 3 days, Consider flow cystometry if unclear symptomatology or surgery considered and diagnosis is unclear., Exclusion of other organic disease (e.g. Stones, UTI, Cancer), Management, Conservative measures should be tried first; Stress urinary incontinence or mixed symptoms should, undergo 3 months of pelvic floor exercise. Over active bladder should have 6 weeks of bladder, retraining., Drug therapy for women with overactive bladder should be offered oxybutynin (or solifenacin if, elderly) if conservative measures fail., In women with detrusor instability who fail non operative therapy a trial of sacral neuromodulation, may be considered, with conversion to permanent implant if good response. Augmentation, cystoplasty is an alternative but will involve long term intermittent self catheterisation., In women with stress urinary incontinence a urethral sling type procedure may be undertaken., Where cystocele is present in association with incontinence it should be repaired particularly if it lies
Page 188 :
at the introitus., NICE guidelines, , , , , , , , , Initial assessment urinary incontinence should be classified as stress/urge/mixed., At least 3/7 bladder diary if unable to classify easily., Start conservative treatment before urodynamic studies if a diagnosis is obvious from the, history, Urodynamic studies if plans for surgery., Stress incontinence: Pelvic floor exercises 3/12, if fails consider surgery., Urge incontinence: Bladder training >6/52, if fails for oxybutynin (antimuscarinic drugs) then, sacral nerve stimulation., Pelvic floor exercises offered to all women in their 1st pregnancy., Next question
Page 189 :
Which of the following is associated with reduced lung compliance?, , Older age, , Emphysematous type COPD, , Decline in pulmonary blood flow, , Adopting a vertical posture, , Adjusting a ventilator to maintain high lung volumes, Increased lung compliance = Older age, COPD, Lung compliance is a measure of the ease of expansion of the lungs and thorax, determined by, pulmonary volume and elasticity. A high degree of compliance indicates a loss of elastic recoil of the, lungs, as in old age or emphysema. This increased lung compliance is due to loss of supportive, tissue around the airways. While a normal lung has a high passive elastic recoil, the sick lung has a, decreased elasticity (i.e. decreased transpulmonary pressure) which leads to increased lung, compliance., Decreased compliance means that a greater change in pressure is needed for a given change in, volume, as in atelectasis, pulmonary fibrosis, pneumonia, or lack of surfactant., Please rate this question:, , Discuss and give feedback, , Next question, , Lung volumes, The diagram demonstrates lung volumes and capacities
Page 190 :
Image sourced from Wikipedia, , Definitions, , Tidal volume (TV), , , , , Is the volume of air inspired and expired during each, ventilatory cycle at rest., It is normally 500mls in males and 340mls in females., , Inspiratory reserve, volume (IRV), , , , Is the maximum volume of air that can be forcibly inhaled, following a normal inspiration. 3000mls., , Expiratory reserve, volume (ERV), , , , Is the maximum volume of air that can be forcibly exhaled, following a normal expiration. 1000mls., , Residual volume (RV), , , , Is that volume of air remaining in the lungs after a maximal, expiration., RV = FRC - ERV. 1500mls., , , , Functional residual, capacity (FRC), , , , , Vital capacity (VC), , , , , Is the volume of air remaining in the lungs at the end of a, normal expiration., FRC = RV + ERV. 2500mls., Is the maximal volume of air that can be forcibly exhaled after, a maximal inspiration., VC = TV + IRV + ERV. 4500mls in males, 3500mls in, females.
Page 191 :
Total lung capacity, (TLC), , Forced vital capacity, (FVC), , , , , Is the volume of air in the lungs at the end of a maximal, inspiration., TLC = FRC + TV + IRV = VC + RV. 5500-6000mls., , , , The volume of air that can be maximally forcefully exhaled., Next question
Page 192 :
Which of the following statements relating to alveolar ventilation is untrue?, , Anatomical dead space is measured by helium dilution, , Physiological dead space is increased in PE, , Alveolar ventilation is defined as the volume of fresh air entering the alveoli per minute, , Anatomical dead space is increased by adrenaline, , Type 2 pneumocytes in the alveoli secrete surfactant, , Anatomical dead space is measured by Fowlers method., A patient inhales 100% oxygen to empty the conducting zone gases of nitrogen and then exhales, through a mouthpiece which analyses the nitrogen concentration at the mouth. Initially the exhaled, gases contain no nitrogen as this is dead space gas; the nitrogen concentration will increase as the, alveolar gases are exhaled. Nitrogen which is measured following the breath of 100% oxygen must, then have come only from gas exchanging areas of the lung and not dead space., Please rate this question:, , Discuss and give feedback, , Next question, , Alveolar ventilation, , , Minute ventilation is the total volume of gas ventilated per minute., , MV (ml/min)= tidal volume x Respiratory rate (resps/min)., , , , Dead space ventilation describes the volume of gas not involved in exchange in the blood., , There are 2 types:, 1. Anatomical dead space: 150mls
Page 193 :
, , , , , Volume of gas in the respiratory tree not involved in gaseous exchange: mouth, pharynx,, trachea, bronchi up to terminal bronchioles, Measured by Fowlers method, Increased by:, Standing, increased size of person, increased lung volume and drugs causing, bronchodilatation e.g. Adrenaline, , 2. Physiological dead space: normal 150 mls, increases in ventilation/perfusion mismatch e.g. PE,, COPD, hypotension, , , Volume of gas in the alveoli and anatomical dead space not involved in gaseous exchange., , , , Alveolar ventilation is the volume of fresh air entering the alveoli per minute., , Alveolar ventilation = minute ventilation - Dead space volume, Next question
Page 194 :
Which opioid receptor does morphine attach to?, , mu, , alpha, , sigma, , beta, , kappa, , Pethidine and other conventional opioids attach to this receptor., Please rate this question:, , Discuss and give feedback, , Next question, , Opioids, - Combine to specific opiate receptors in the CNS (periaqueductal grey matter, limbic system,, substantia gelatinosa), - Morphine attaches to mu1 receptors, Next question
Page 195 :
Which of the following inhibits the secretion of insulin?, , Adrenaline, , Lipids, , Gastrin, , Arginine, , Vagal cholinergic activity, , Inhibition of insulin release:, , , , , , Alpha adrenergic drugs, Beta blockers, Sympathetic nerves, , Please rate this question:, , Discuss and give feedback, , Next question, , Insulin, Insulin is a peptide hormone, produced by beta cells of the pancreas, and is central to regulating, carbohydrate and fat metabolism in the body. Insulin causes cells in the liver, skeletal muscles, and, fat tissue to absorb glucose from the blood. In the liver and skeletal muscles, glucose is stored as, glycogen, and in fat cells (adipocytes) it is stored as triglycerides., Structure, The human insulin protein is composed of 51 amino acids, and has a molecular weight of 5808 Da. It, is a dimer of an A-chain and a B-chain, which are linked together by disulfide bonds., Synthesis, Pro-insulin is formed by the rough endoplasmic reticulum in pancreatic beta cells. Then pro-insulin is, cleaved to form insulin and C-peptide. Insulin is stored in secretory granules and released in, response to Ca2+.
Page 196 :
Function, , , , , , Secreted in response to hyperglycaemia, Glucose utilisation and glycogen synthesis, Inhibits lipolysis, Reduces muscle protein loss, Next question
Page 197 :
What is measured to obtain renal plasma flow?, , Creatinine, , Para-amino hippuric acid (PAH), , Inulin, , Glucose, , Protein, , Theme from April 2016 Exam, Renal plasma flow = (amount of PAH in urine per unit time) / (difference in PAH concentration in the, renal artery or vein), Normal value = 660ml/min, Please rate this question:, , Discuss and give feedback, , Next question, , Renal Physiology, Overview, , , , , , Each nephron is supplied with blood from an afferent arteriole that opens onto the glomerular, capillary bed., Blood then flows to an efferent arteriole, supplying the peritubular capillaries and medullary, vasa recta., The kidney receives up to 25% of resting cardiac output.
Page 198 :
Control of blood flow, , , , , The kidney is able to autoregulate its blood flow between systolic pressures of 80- 180mmHg, so there is little variation in renal blood flow., This is achieved by myogenic control of arteriolar tone, both sympathetic input and hormonal, signals (e.g. renin) are responsible., , Glomerular structure and function, , , , , , , , , , Blood inside the glomerulus has considerable hydrostatic pressure., The basement membrane has pores that will allow free diffusion of smaller solutes, larger, negatively charged molecules such as albumin are unable to cross., The glomerular filtration rate (GFR) is equal to the concentration of a solute in the urine,, times the volume of urine produced per minute, divided by the plasma concentration, (assuming that the solute is freely diffused e.g. inulin)., In clinical practice creatinine is used because it is subjected to very little proximal tubular, secretion., Although subject to variability, the typical GFR is 125ml per minute., Glomerular filtration rate = Total volume of plasma per unit time leaving the capillaries and, entering the bowman's capsule, Renal clearance = volume plasma from which a substance is removed per minute by the, kidneys, , Substances used to measure GFR have the following features:, 1. Inert, 2. Free filtration from the plasma at the glomerulus (not protein bound), 3. Not absorbed or secreted at the tubules, 4. Plasma concentration constant during urine collection, Examples: inulin, creatinine, GFR = urine concentration (mmol/l) x urine volume (ml/min), -------------------------------------------------------------------------plasma concentration (mmol/l), , , , , The clearance of a substance is dependent not only on its diffusivity across the basement, membrane but also subsequent tubular secretion and / or reabsorption., So glucose which is freely filtered across the basement membrane is usually reabsorbed, from tubules giving a clearance of zero.
Page 199 :
Tubular function, , , , , , , , , , Reabsorption and secretion of substances occurs in the tubules., In the proximal tubule substrates such as glucose, amino acids and phosphate are cotransported with sodium across the semi permeable membrane., Up to two thirds of filtered water is reabsorbed in the proximal tubules., This will lead to increase in urea concentration in the distal tubule allowing for its increased, diffusion., Substances to be secreted into the tubules are taken up from the peritubular blood by tubular, cells., Solutes such as paraaminohippuric acid are cleared with a single passage through the, kidneys and this is why it is used to measure renal plasma flow. Ions such as calcium and, phosphate will have a tubular reabsorption that is influenced by plasma PTH levels., Potassium may be both secreted and re-absorbed and is co-exchanged with sodium., , Loop of Henle, , , , , , , , , , , Approximately 60 litres of water containing 9000mmol sodium enters the descending limb of, the loop of Henle in 24 hours., Loops from the juxtamedullary nephrons run deep into the medulla., The osmolarity of fluid changes and is greatest at the tip of the papilla., The thin ascending limb is impermeable to water, but highly permeable to sodium and, chloride ions., This loss means that at the beginning of the thick ascending limb the fluid is hypo osmotic, compared with adjacent interstitial fluid., In the thick ascending limb the reabsorption of sodium and chloride ions occurs by both, facilitated and passive diffusion pathways., The loops of Henle are co-located with vasa recta, these will have similar solute, compositions to the surrounding extracellular fluid so preventing the diffusion and, subsequent removal of this hypertonic fluid., The energy dependent reabsorption of sodium and chloride in the thick ascending limb helps, to maintain this osmotic gradient., , Next question
Page 200 :
Which of the following surgical procedures will have the greatest long term impact on a patients, calcium metabolism?, , Distal gastrectomy, , Cholecystectomy, , Extensive small bowel resection, , Sub total colectomy, , Gastric banding for obesity, , Calcium is mainly absorbed from the small bowel and this will have a direct long term impact on, calcium metabolism and increase the risk of osteoporosis. Gastric banding and distal gastrectomy, may affect a patients dietary choices but any potential deleterious nutritional intake may be, counteracted by administration of calcium supplements orally. Only 10% of calcium is absorbed from, the colon so that a sub total colectomy will only have a negligible effect., Please rate this question:, , Discuss and give feedback, , Next question, , Calcium homeostasis, Calcium ions are linked to a wide range of physiological processes. The largest store of bodily, calcium is contained within the skeleton. Calcium levels are primarily controlled by parathyroid, hormone, vitamin D and calcitonin., Hormonal regulation of calcium
Page 201 :
Hormone, , Parathyroid hormone (PTH), , Actions, , , , , , , , , , , 1,25-dihydroxycholecalciferol (the, active form of vitamin D), , Calcitonin, , , , , Increase calcium levels and decrease phosphate levels, Increases bone resorption, Immediate action on osteoblasts to increase ca2+ in, extracellular fluid, Osteoblasts produce a protein signaling molecule that, activate osteoclasts which cause bone resorption, Increases renal tubular reabsorption of calcium, Increases synthesis of 1,25(OH)2D (active form of, vitamin D) in the kidney which increases bowel, absorption of Ca2+, Decreases renal phosphate reabsorption, , , , , Increases plasma calcium and plasma phosphate, Increases renal tubular reabsorption and gut absorption, of calcium, Increases osteoclastic activity, Increases renal phosphate reabsorption, , , , , , , Secreted by C cells of thyroid, Inhibits intestinal calcium absorption, Inhibits osteoclast activity, Inhibits renal tubular absorption of calcium, , Both growth hormone and thyroxine also play a small role in calcium metabolism., Next question
Page 202 :
A 52-year-old woman with a history of gastrectomy reports lethargy and a sore tongue. Blood tests, are reported as follows:, , Hb, , 10.7 g/dl, , MCV, , 121 fl, , Plt, , 177 * 10^9/l, , WBC, , 5.4 * 10^9/l, , What is the most likely cause?, , Vitamin B12 deficiency, , Vitamin C deficiency, , Iron deficiency anaemia, , Anaemia of chronic disease, , Vitamin E deficiency, , A history of gastrectomy and a macrocytic anaemia should indicate a diagnosis of B12 deficiency., Please rate this question:, , Discuss and give feedback, , Next question
Page 203 :
Vitamin B12 deficiency, Vitamin B12 is mainly used in the body for red blood cell development and also maintenance of the, nervous system. It is absorbed after binding to intrinsic factor (secreted from parietal cells in the, stomach) and is actively absorbed in the terminal ileum. A small amount of vitamin B12 is passively, absorbed without being bound to intrinsic factor., Causes of vitamin B12 deficiency, , , , , , , pernicious anaemia, post gastrectomy, poor diet, disorders of terminal ileum (site of absorption): Crohn's, blind-loop etc, , Features of vitamin B12 deficiency, , , , , , , macrocytic anaemia, sore tongue and mouth, neurological symptoms: e.g. Ataxia, neuropsychiatric symptoms: e.g. Mood disturbances, , Management, , , , , if no neurological involvement 1 mg of IM hydroxocobalamin 3 times each week for 2 weeks,, then once every 3 months, if a patient is also deficient in folic acid then it is important to treat the B12 deficiency first to, avoid precipitating subacute combined degeneration of the cord, Next question
Page 204 :
A 43 year old lady is diagnosed with primary hyperparathyroidism. Her serum PTH levels are, elevated. An endocrine surgeon performs a parathyroidectomy. How long will it take for the serum, PTH levels to fall if the functioning adenoma has been successfully removed?, , 6 hours, , 24 hours, , 2 hours, , 1 hour, , 10 minutes, , PTH has a very short half life usually less than 10 minutes. Therefore a demonstrable drop in serum, PTH should be identified within 10 minutes of removing the adenoma. This is useful clinically since it, is possible to check the serum PTH intraoperatively prior to skin closure and explore the other, glands if levels fail to fall., Please rate this question:, , Discuss and give feedback, , Next question, , Calcium homeostasis, Calcium ions are linked to a wide range of physiological processes. The largest store of bodily, calcium is contained within the skeleton. Calcium levels are primarily controlled by parathyroid, hormone, vitamin D and calcitonin., Hormonal regulation of calcium
Page 205 :
Hormone, , Parathyroid hormone (PTH), , Actions, , , , , , , , , , , 1,25-dihydroxycholecalciferol (the, active form of vitamin D), , Calcitonin, , , , , Increase calcium levels and decrease phosphate levels, Increases bone resorption, Immediate action on osteoblasts to increase ca2+ in, extracellular fluid, Osteoblasts produce a protein signaling molecule that, activate osteoclasts which cause bone resorption, Increases renal tubular reabsorption of calcium, Increases synthesis of 1,25(OH)2D (active form of, vitamin D) in the kidney which increases bowel, absorption of Ca2+, Decreases renal phosphate reabsorption, , , , , Increases plasma calcium and plasma phosphate, Increases renal tubular reabsorption and gut absorption, of calcium, Increases osteoclastic activity, Increases renal phosphate reabsorption, , , , , , , Secreted by C cells of thyroid, Inhibits intestinal calcium absorption, Inhibits osteoclast activity, Inhibits renal tubular absorption of calcium, , Both growth hormone and thyroxine also play a small role in calcium metabolism., Next question
Page 206 :
Which of the following statements relating to abnormal coagulation is false?, , Warfarin affects the synthesis of factor 2,7,9,10, , The prothrombin time is prolonged in Haemophilia A, , Cholestatic jaundice can cause vitamin K deficiency, , Disseminated intravascular coagulation is associated with thrombocytopenia, , Massive transfusion is associated with reduced levels of factor 5 and 8, , In haemophilia A the APTT is prolonged and there is reduced levels of factor 8:C. The bleeding time, and PT are normal. Cholestatic jaundice prevents the absorption of the fat soluble vitamin K., Massive transfusion (>10u blood or equivalent to the blood volume of a person) puts the patient at, risk of thrombocytopaenia, factor 5 and 8 deficiency., Please rate this question:, , Discuss and give feedback, , Next question, , Abnormal coagulation, Cause, , Factors affected, , Heparin, , Prevents activation factors 2,9,10,11, , Warfarin, , Affects synthesis of factors 2,7,9,10, , DIC, , Factors 1,2,5,8,11, , Liver disease, , Factors 1,2,5,7,9,10,11, , Interpretation blood clotting test results
Page 207 :
Disorder, , APTT, , PT, , Bleeding time, , Haemophilia, , Increased, , Normal, , Normal, , von Willebrand's disease, , Increased, , Normal, , Increased, , Vitamin K deficiency, , Increased, , Increased, , Normal, Next question
Page 208 :
A 34 year old man presents with a peptic ulcer. Which of the following is responsible for the release, of gastric acid?, , Chief cells, , Parietal cells, , Brunners Glands, , G Cells, , None of the above, , Parietal cells are responsible for the release of gastric acid. Brunners glands are found in the, duodenum., Please rate this question:, , Discuss and give feedback, , Next question, , Gastric secretions, A working knowledge of gastric secretions is important for surgery because peptic ulcers are, common, surgeons frequently prescribe anti secretory drugs and because there are still patients, around who will have undergone acid lowering procedures (Vagotomy) in the past., Gastric acid, , , , , Is produced by the parietal cells in the stomach, pH of gastric acid is around 2 with acidity being maintained by the H +/K+ ATP ase pump. As, part of the process bicarbonate ions will be secreted into the surrounding vessels.
Page 209 :
, , , Sodium and chloride ions are actively secreted from the parietal cell into the canaliculus., This sets up a negative potential across the membrane and as a result sodium and, potassium ions diffuse across into the canaliculus., Carbonic anhydrase forms carbonic acid which dissociates and the hydrogen ions formed by, dissociation leave the cell via the H+/K+ antiporter pump. At the same time sodium ions are, actively absorbed. This leaves hydrogen and chloride ions in the canaliculus these mix and, are secreted into the lumen of the oxyntic gland., , This is illustrated diagrammatically below:, , Image sourced from Wikipedia, , Phases of gastric acid secretion, There are 3 phases of gastric secretion:, 1. Cephalic phase (smell / taste of food)
Page 210 :
, , , 30% acid produced, Vagal cholinergic stimulation causing secretion of HCL and gastrin release from G cells, , 2. Gastric phase (distension of stomach ), , , , , 60% acid produced, Stomach distension/low H+/peptides causes Gastrin release, , 3. Intestinal phase (food in duodenum), , , , , 10% acid produced, High acidity/distension/hypertonic solutions in the duodenum inhibits gastric acid secretion, via enterogastrones (CCK, secretin) and neural reflexes., , Regulation of gastric acid production, Factors increasing production include:, , , , , , Vagal nerve stimulation, Gastrin release, Histamine release (indirectly following gastrin release) from enterchromaffin like cells, , Factors decreasing production include:, , , , , , Somatostatin (inhibits histamine release), Cholecystokinin, Secretin, , The diagram below illustrates some of the factors involved in regulating gastric acid secretion and, the relevant associated pharmacology
Page 211 :
Image sourced from Wikipedia, , Below is a brief summary of the major hormones involved in food digestion:, , Source, , Stimulus, , Actions, , Gastrin, , G cells in, antrum of the, stomach, , Distension of, stomach, extrinsic, nerves, Inhibited by: low, antral pH,, somatostatin, , Increase HCL, pepsinogen and IF secretion,, increases gastric motility, trophic effect on gastric, mucosa, , CCK, , I cells in upper, small intestine, , Partially digested, proteins and, triglycerides, , Increases secretion of enzyme-rich fluid from, pancreas, contraction of gallbladder and, relaxation of sphincter of Oddi, decreases gastric, emptying, trophic effect on pancreatic acinar, cells, induces satiety, , Secretin, , S cells in, upper small, , Acidic chyme, fatty, acids, , Increases secretion of bicarbonate-rich fluid from, pancreas and hepatic duct cells, decreases gastric, acid secretion, trophic effect on pancreatic acinar
Page 212 :
intestine, , cells, , VIP, , Small, intestine,, pancreas, , Neural, , Stimulates secretion by pancreas and intestines,, inhibits acid and pepsinogen secretion, , Somatostatin, , D cells in the, pancreas and, stomach, , Fat, bile salts and, glucose in the, intestinal lumen, , Decreases acid and pepsin secretion, decreases, gastrin secretion, decreases pancreatic enzyme, secretion, decreases insulin and glucagon, secretion, inhibits trophic effects of gastrin, stimulates, gastric mucous production, Next question
Page 213 :
Which of the following does not lead to relaxation of the lower oesophageal sphincter?, , Metoclopramide, , Botulinum toxin type A, , Nicotine, , Alcohol, , Theophylline, , Metoclopramide acts directly on the smooth muscle of the LOS to cause it to contract., Theophylline is a phosphodiesterase inhibitor (mimics action of prostaglandin E1) which causes, relaxation of the LOS., Please rate this question:, , Discuss and give feedback, , Next question, , Peristalsis, , , , , , , Circular smooth muscle contracts behind the food bolus and longitudinal smooth muscle, propels the food through the oesophagus, Primary peristalsis spontaneously moves the food from the oesophagus into the stomach (9, seconds), Secondary peristalsis occurs when food, which doesn't enter the stomach, stimulates stretch, receptors to cause peristalsis, In the small intestine each peristalsis waves slows to a few seconds and causes mixture of, chyme, In the colon three main types of peristaltic activity are recognised (see below), , Colonic peristalsis
Page 214 :
Segmentation contractions, , Localised contractions in which the bolus is subjected to local forces to, maximise mucosal absorption, , Antiperistaltic contractions, towards ileum, , Localised reverse peristaltic waves to slow entry into colon and, maximise absorption, , Mass movements, , Waves migratory peristaltic waves along the entire colon to empty the, organ prior to the next ingestion of food bolus, Next question
Page 215 :
Which of the following is not released from the islets of Langerhans?, , Pancreatic polypeptide, , Glucagon, , Secretin, , Somatostatin, , Insulin, , Secretin is released from mucosal cells in the duodenum and jejunum., Please rate this question:, , Discuss and give feedback, , Next question, , Pancreas endocrine physiology, Hormones released from the islets of Langerhans, , Beta cells, , Insulin (70% of total secretions), , Alpha cells, , Glucagon, , Delta cells, , Somatostatin, , F cells, , Pancreatic polypeptide, Next question
Page 216 :
Which of the following is not classically seen in coning resulting from raised intra cranial pressure?, , Coma, , Hypotension, , Unreactive mid sized pupils, , Cheyne Stokes style respiratory efforts, , Bradycardia, Cushings triad, , , , , , Widening of the pulse pressure, Respiratory changes, Bradycardia, , Due to raised ICP systemic hypertension is usually seen. Compression of the respiratory centre will, typically result in Cheyne Stokes style respiration., Please rate this question:, , Discuss and give feedback, , Next question, , Coning, , , , , , The cranial vault is a confined cavity apart from infants with a non fused fontanelle., Rises in ICP may be accommodated by shifts of CSF., Once the CSF shifting has reached its capacity ICP will start to rise briskly., The brain autoregulates its blood supply, as ICP rises the systemic circulation will display, changes to try and meet the perfusion needs of the brain. Usually this will involve, hypertension.
Page 217 :
, , As ICP rises further, the brain will be compressed, cranial nerve palsies may be seen and, compression of essential centres in the brain stem will occur. When the cardiac centre is, involved bradycardia will often develop., Next question
Page 218 :
Control of ventilation. Which statement is false?, , Peripheral chemoreceptors are located in the bifurcation of the carotid arteries and arch of the, aorta, , Central chemoreceptors respond to changes in O2, , The respiratory centres control the rate and depth of respiration, , Involuntary control of respiration is from the medulla and pons, , Irritant receptors cause bronchospasm, - Central chemoreceptors: Respond to increased H+ in BRAIN INTERSTITIAL FLUID to increase, ventilation., , Please rate this question:, , Discuss and give feedback, , Next question, , Control of ventilation, , , , , Control of ventilation is coordinated by the respiratory centres, chemoreceptors, lung, receptors and muscles., Automatic, involuntary control of respiration occurs from the medulla., The respiratory centres control the respiratory rate and the depth of respiration., , Respiratory centres, , Medullary, respiratory centre, , Inspiratory and expiratory neurones. Has ventral group which controls forced, voluntary expiration and the dorsal group controls inspiration. Depressed by
Page 219 :
opiates., , Apneustic centre, , Lower pons, Stimulates inspiration - activates and prolongs inhalation, Overridden by pneumotaxic control to end inspiration, , Pneumotaxic centre, , Upper pons, inhibits inspiration at a certain point. Fine tunes the respiratory rate., , Ventillatory variables, , , , , , , Levels of pCO2 most important in ventilation control, Levels of O2 are less important., Peripheral chemoreceptors: located in the bifurcation of carotid arteries and arch of the, aorta. They respond to changes in reduced pO2, increased H+ and increased pCO2 in, ARTERIAL BLOOD., Central chemoreceptors: located in the medulla. Respond to increased H + in BRAIN, INTERSTITIAL FLUID to increase ventilation. NB the central receptors are NOT influenced, by O2levels., , Lung receptors include:, , , , , , Stretch receptors: respond to lung stretching causing a reduced respiratory rate, Irritant receptors: respond to smoke etc causing bronchospasm, J (juxtacapillary) receptors, Next question
Page 220 :
A 54 year old lady has her serum calcium measured. Assuming her renal function is normal, what, proportion of calcium filtered at the glomerulus will be reabsorbed by the renal tubules?, , 5%, , 15%, , 25%, , 50%, , 95%, , Most filtered calcium is reabsorbed (95%) a rare disorder of familial hypercalcemic calciurea may, affect this proportion., Please rate this question:, , Discuss and give feedback, , Next question, , Calcium homeostasis, Calcium ions are linked to a wide range of physiological processes. The largest store of bodily, calcium is contained within the skeleton. Calcium levels are primarily controlled by parathyroid, hormone, vitamin D and calcitonin., Hormonal regulation of calcium, , Hormone, , Actions
Page 221 :
Hormone, , Parathyroid hormone (PTH), , Actions, , , , , , , , , , , 1,25-dihydroxycholecalciferol (the, active form of vitamin D), , Calcitonin, , , , , Increase calcium levels and decrease phosphate levels, Increases bone resorption, Immediate action on osteoblasts to increase ca2+ in, extracellular fluid, Osteoblasts produce a protein signaling molecule that, activate osteoclasts which cause bone resorption, Increases renal tubular reabsorption of calcium, Increases synthesis of 1,25(OH)2D (active form of, vitamin D) in the kidney which increases bowel, absorption of Ca2+, Decreases renal phosphate reabsorption, , , , , Increases plasma calcium and plasma phosphate, Increases renal tubular reabsorption and gut absorption, of calcium, Increases osteoclastic activity, Increases renal phosphate reabsorption, , , , , , , Secreted by C cells of thyroid, Inhibits intestinal calcium absorption, Inhibits osteoclast activity, Inhibits renal tubular absorption of calcium, , Both growth hormone and thyroxine also play a small role in calcium metabolism., Next question
Page 222 :
Which of the following does not cause hyperkalaemia?, , Haemolysis, , Burns, , Familial periodic paralysis, , Type 4 renal tubular acidosis, , Severe malnutrition, 'Machine' - Causes of Increased Serum K+, M - Medications - ACE inhibitors, NSAIDS, A - Acidosis - Metabolic and respiratory, C - Cellular destruction - Burns, traumatic injury, H - Hypoaldosteronism, haemolysis, I - Intake - Excessive, N - Nephrons, renal failure, E - Excretion - Impaired, , Familial periodic paralysis has subtypes associated with hyper and hypokalaemia., Please rate this question:, , Discuss and give feedback, , Next question, , Hyperkalaemia, , , Plasma potassium levels are regulated by a number of factors including aldosterone, acidbase balance and insulin levels.
Page 223 :
, , , Metabolic acidosis is associated with hyperkalaemia as hydrogen and potassium ions, compete with each other for exchange with sodium ions across cell membranes and in the, distal tubule., ECG changes seen in hyperkalaemia include tall-tented T waves, small P waves, widened, QRS leading to a sinusoidal pattern and asystole, , Causes of hyperkalaemia, , , , , , , , , Acute renal failure, Drugs*: potassium sparing diuretics, ACE inhibitors, angiotensin 2 receptor blockers,, spironolactone, ciclosporin, heparin**, Metabolic acidosis, Addison's, Tissue necrosis/rhabdomylosis: burns, trauma, Massive blood transfusion, , Foods that are high in potassium, , , , , Salt substitutes (i.e. Contain potassium rather than sodium), Bananas, oranges, kiwi fruit, avocado, spinach, tomatoes, , *beta-blockers interfere with potassium transport into cells and can potentially cause hyperkalaemia, in renal failure patients - remember beta-agonists, e.g. Salbutamol, are sometimes used as, emergency treatment, **both unfractionated and low-molecular weight heparin can cause hyperkalaemia. This is thought to, be caused by inhibition of aldosterone secretion, Next question
Page 224 :
Which of the following statements is true of glucagon?, , Produced in response to hyperglycaemia, , Released by beta cells, , Inhibits gluconeogenesis, , Produced in response to an increase of amino acids, , Composed of 2 alpha polypeptide chains linked by hydrogen bonds, , Glucagon is a protein comprised of a single polypeptide chain., Produced by alpha cells of pancreatic islets of Langerhans in response to hypoglycaemia and amino, acids., It increases plasma glucose and ketones., Please rate this question:, , Discuss and give feedback, , Next question, , Glucagon, Glucagon, the hormonal antagonist to insulin, is released from the alpha cells of the Islets of, Langerhans in the pancreas. It will result in an increased plasma glucose level., , Stimulation, , Inhibition, , Decreased plasma glucose, , Somatostatin, , Increased catecholamines, , Insulin, , Increased free fatty acids and keto acids, Increased plasma amino acids
Page 226 :
A 28 year old man undergoes a completion right hemicolectomy for treatment of a 5cm appendiceal, carcinoid. As part of his follow up he is due to undergo 24 hour urine collection for 5-HIAA. Which of, the following causes an elevated 5-HIAA in a 24-hour urine collection?, , Naproxen, , Oranges, , Flucloxacillin, , Amiodarone, , Beef, , It is important to be aware of what can falsely elevate 5-HIAA to avoid diagnosing carcinoid, syndrome incorrectly. These include:, Food: spinach, cheese, wine, caffeine, tomatoes, Drugs: Naproxen, Monoamine oxidase inhibitors, Recent surgery, Please rate this question:, , Discuss and give feedback, , Next question, , Carcinoid syndrome, , , , , , Carcinoid tumours secrete serotonin, Originate in neuroendocrine cells mainly in the intestine (midgut-distal ileum/appendix), Can occur in the rectum, bronchi, Hormonal symptoms mainly occur when disease spreads outside the bowel
Page 227 :
Clinical features, , , , , , , , , Onset: insidious over many years, Flushing face, Palpitations, Pulmonary valve stenosis and tricuspid regurgitation causing dyspnoea, Asthma, Severe diarrhoea (secretory, persists despite fasting), , Investigation, , , , , , , 5-HIAA in a 24-hour urine collection, Somatostatin receptor scintigraphy, CT scan, Blood testing for chromogranin A, , Treatment, , , , , Octreotide, Surgical removal, Next question
Page 228 :
A 52 year old man develops septic shock following a Hartmans procedure for perforated diverticular, disease. He is started on an adrenaline infusion. Which of the following is least likely to occur?, , Peripheral vasoconstriction, , Coronary artery vasospasm, , Gluconeogenesis, , Lipolysis, , Tachycardia, , It's cardiac effects are mediated via β 1 receptors. The coronary arteries which have β 2 receptors, are unaffected., Please rate this question:, , Discuss and give feedback, , Next question, , Adrenaline, , , Fight or Flight response, , - Catecholamine (phenylalanine and tyrosine), - Neurotransmitter and hormone, - Released by the adrenal glands, - Effects on α 1 and 2, β 1 and 2 receptors, - Effect on β 2 receptors in skeletal muscle vessels-causing vasodilation, - Increase cardiac output and total peripheral resistance, - Vasoconstriction in the skin and kidneys causing a narrow pulse pressure, Actions, α adrenergic receptors:, , , , , Inhibits insulin secretion by the pancreas, Stimulates glycogenolysis in the liver and muscle, Stimulates glycolysis in muscle
Page 229 :
β adrenergic receptors:, , , , , Stimulates glucagon secretion in the pancreas, Stimulates ACTH, Stimulates lipolysis by adipose tissue, Next question
Page 230 :
Intra cranial pressure is governed by the principles of the Monroe-Kellie doctrine. To which of the, following does this concept not apply?, , A 2 month old child, , A 2 year old child, , A 5 year old child, , A 10 year old child, , An adult, , The Monroe-Kelly Doctrine assumes that the cranial cavity is a rigid box. In children with non fused, fontanells this is not the case., Please rate this question:, , Discuss and give feedback, , Next question, , Applied neurophysiology, , , , , , , Pressure within the cranium is governed by the Monroe-Kelly doctrine. This considers the, skull as a closed box. Increases in mass can be accommodated by loss of CSF. Once a, critical point is reached (usually 100- 120ml of CSF lost) there can be no further, compensation and ICP rises sharply. The next step is that pressure will begin to equate with, MAP and neuronal death will occur. Herniation will also accompany this process., The CNS can autoregulate its own blood supply. Vaso constriction and dilatation of the, cerebral blood vessels is the primary method by which this occurs. Extremes of blood, pressure can exceed this capacity resulting in risk of stroke. Other metabolic factors such as, hypercapnia will also cause vasodilation, which is of importance in ventilating head injured, patients., The brain can only metabolise glucose, when glucose levels fall, consciousness will be, impaired., Next question
Page 231 :
Which of the following is not caused by cortisol in the stress response?, , Anti-inflammatory effects, , Hypoglycaemia, , Skeletal muscle protein breakdown, , Stimulation of lipolysis, , Mineralocorticoid effects, , An 'anti insulin' effect occurs leading to hyperglycaemia., Please rate this question:, , Discuss and give feedback, , Next question, , Stress response: Endocrine and metabolic changes, , , , , Surgery precipitates hormonal and metabolic changes causing the stress response., Stress response is associated with: substrate mobilization, muscle protein loss, sodium and, water retention, suppression of anabolic hormone secretion, activation of the sympathetic, nervous system, immunological and haematological changes., The hypothalamic-pituitary axis and the sympathetic nervous systems are activated and, there is a failure of the normal feedback mechanisms of control of hormone secretion., , A summary of the hormonal changes associated with the stress response:, , Increased, , Decreased, , No Change, , Growth hormone, , Insulin, , Thyroid stimulating hormone, , Cortisol, , Testosterone, , Luteinizing hormone
Page 232 :
Increased, , Decreased, , No Change, , Renin, , Oestrogen, , Follicle stimulating hormone, , Adrenocorticotrophic hormone (ACTH), , Aldosterone, , Prolactin, , Antidiuretic hormone, , Glucagon, , Sympathetic nervous system, , , , Stimulates catecholamine release, Causes tachycardia and hypertension, , Pituitary gland, , , , , , ACTH and growth hormone (GH) is stimulated by hypothalamic releasing factors,, corticotrophin releasing factor (CRF) and somatotrophin (or growth hormone releasing factor), Perioperative increased prolactin secretion occurs by release of inhibitory control, Secretion of thyroid stimulating hormone (TSH), luteinizing hormone (LH) and follicle, stimulating hormone (FSH) does not change significantly, ACTH stimulates cortisol production within a few minutes of the start of surgery. More ACTH, is produced than needed to produce a maximum adrenocortical response., , Cortisol, , , Significant increases within 4-6 hours of surgery (>1000 nmol litre-1).
Page 233 :
, , , , The usual negative feedback mechanism fails and concentrations of ACTH and cortisol, remain persistently increased., The magnitude and duration of the increase correlate with the severity of stress and the, response is not abolished by the administration of corticosteroids., The metabolic effects of cortisol are enhanced:, , Skeletal muscle protein breakdown to provide gluconeogenic precursors and amino acids for protein, synthesis in the liver, Stimulation of lipolysis, 'Anti-insulin effect', Mineralocorticoid effects, Anti-inflammatory effects, Growth hormone, , , , Increased secretion after surgery has a minor role, Most important for preventing muscle protein breakdown and promote tissue repair by insulin, growth factors, , Alpha Endorphin, , , Increased, , Antidiuretic hormone, , , , , An important vasopressor and enhances haemostasis, Renin is released causing the conversion of angiotensinogen to angiotensin I, Angiotensin II formed by ACE on angiotensin 1, which causes the secretion of aldosterone, from the adrenal cortex. This increases sodium reabsorption at the distal convoluted tubule, , Insulin, , , , , , Release inhibited by stress, Occurs via the inhibition of the beta cells in the pancreas by the α2-adrenergic inhibitory, effects of catecholamines, Insulin resistance by target cells occurs later, The perioperative period is characterized by a state of functional insulin deficiency, , Thyroxine (T4) and tri-iodothyronine (T3)
Page 234 :
, , Circulating concentrations are inversely correlated with sympathetic activity and after surgery, there is a reduction in thyroid hormone production, which normalises over a few days., , Metabolic effect of endocrine response, Carbohydrate metabolism, , , , , , , , Hyperglycaemia is a main feature of the metabolic response to surgery, Due to increase in glucose production and a reduction in glucose utilization, Catecholamines and cortisol promote glycogenolysis and gluconeogenesis, Initial failure of insulin secretion followed by insulin resistance affects the normal responses, The proportion of the hyperglycaemic response reflects the severity of surgery, Hyperglycaemia impairs wound healing and increase infection rates, , Protein metabolism, , , , , , , Initially there is inhibition of protein anabolism, followed later, if the stress response is, severe, by enhanced catabolism, The amount of protein degradation is influenced by the type of surgery and also by the, nutritional status of the patient, Mainly skeletal muscle protein is affected, The amino acids released form acute phase proteins (fibrinogen, C reactive protein,, complement proteins, a2-macroglobulin, amyloid A and ceruloplasmin) and are used for, gluconeogenesis, Nutritional support has little effect on preventing catabolism, , Lipid metabolism, Increased catecholamine, cortisol and glucagon secretion, and insulin deficiency, promotes lipolysis, and ketone body production., Salt and water metabolism, , , , ADH causes water retention, concentrated urine, and potassium loss and may continue for 3, to 5 days after surgery, Renin causes sodium and water retention, , Cytokines, , , , , Glycoproteins, Interleukins (IL) 1 to 17, interferons, and tumour necrosis factor, Synthesized by activated macrophages, fibroblasts, endothelial and glial cells in response to, tissue injury from surgery or trauma
Page 235 :
, , IL-6 main cytokine associated with surgery. Peak 12 to 24 h after surgery and increase by, the degree of tissue damage Other effects of cytokines include fever, granulocytosis,, haemostasis, tissue damage limitation and promotion of healing., , Modifying the response, , , , , , , , , Opioids suppress hypothalamic and pituitary hormone secretion, At high doses the hormonal response to pelvic and abdominal surgery is abolished., However, such doses prolong recovery and increase the need for postoperative ventilatory, support, Spinal anaesthesia can reduce the glucose, ACTH, cortisol, GH and epinephrine changes,, although cytokine responses are unaltered, Cytokine release is reduced in less invasive surgery, Nutrition prevents the adverse effects of the stress response. Enteral feeding improves, recovery, Growth hormone and anabolic steroids may improve outcome, Normothermia decreases the metabolic response, , References, Deborah Burton, Grainne Nicholson, and George Hall, Endocrine and metabolic response to surgery ., Contin Educ Anaesth Crit Care Pain (2004) 4(5): 144-147 doi:10.1093/bjaceaccp/mkh040, Next question
Page 236 :
Which of the following features does not put a patient at risk of refeeding syndrome?, , BMI < 16 kg/m2, , Alcohol abuse, , Thyrotoxicosis, , Chemotherapy, , Diuretics, , Diuretics increase the risk of re-feeding syndrome through a process of increasing the risk of, depletion of key electrolytes., Please rate this question:, , Discuss and give feedback, , Next question, , Nutrition - Refeeding syndrome, Refeeding syndrome describes the metabolic abnormalities which occur on feeding a person, following a period of starvation. The metabolic consequences include:, , , , , , Hypophosphataemia, Hypokalaemia, Hypomagnesaemia, Abnormal fluid balance, , These abnormalities can lead to organ failure., Re-feeding problems, If patient not eaten for > 5 days, aim to re-feed at < 50% energy and protein levels, High risk for re-feeding problems, If one or more of the following:, , , , , BMI < 16 kg/m 2, Unintentional weight loss >15% over 3-6 months, Little nutritional intake > 10 days
Page 237 :
, , Hypokalaemia, Hypophosphataemia or hypomagnesaemia prior to feeding (unless high), , If two or more of the following:, , , , , , BMI < 18.5 kg/m2, Unintentional weight loss > 10% over 3-6 months, Little nutritional intake > 5 days, History of: alcohol abuse, drug therapy including insulin, chemotherapy, diuretics and, antacids, , Prescription, , , , , Start at up to 10 kcal/kg/day increasing to full needs over 4-7 days, Start immediately before and during feeding: oral thiamine 200-300mg/day, vitamin B co, strong 1 tds and supplements, Give K+ (2-4 mmol/kg/day), phosphate (0.3-0.6 mmol/kg/day), magnesium (0.2-0.4, mmol/kg/day), Next question
Page 238 :
Which of the following statements relating to the regulation of renal blood flow is untrue?, , In a healthy 70Kg male, the glomerular filtration rate will be the same at a systolic blood, pressure of 120mmHg as a systolic blood pressure of 95 mmHg, Over 90% of the blood supply to the kidney is distributed to the cortex, , The kidney receives approximately 25% of the total cardiac output at rest, , A decrease in renal perfusion pressure will cause the juxtaglomerular cells to secrete renin, , Systolic blood pressures of less than 65mmHg will cause the mesangial cells to secrete, aldosterone, , The kidney autoregulates its blood supply over a range of systolic blood pressures. Drop in arterial, pressure is sensed by the juxtaglomerular cells and renin is released leading to the activation of the, renin-angiontensin system. Mesangial cells are contractile cells that are located in the tubule and, have no direct endocrine function., Please rate this question:, , Discuss and give feedback, , Next question, , Renal Physiology, Overview, , , , , Each nephron is supplied with blood from an afferent arteriole that opens onto the glomerular, capillary bed., Blood then flows to an efferent arteriole, supplying the peritubular capillaries and medullary, vasa recta., The kidney receives up to 25% of resting cardiac output., , Control of blood flow, , , , The kidney is able to autoregulate its blood flow between systolic pressures of 80- 180mmHg, so there is little variation in renal blood flow., This is achieved by myogenic control of arteriolar tone, both sympathetic input and hormonal, signals (e.g. renin) are responsible.
Page 239 :
Glomerular structure and function, , , , , , , , , Blood inside the glomerulus has considerable hydrostatic pressure., The basement membrane has pores that will allow free diffusion of smaller solutes, larger, negatively charged molecules such as albumin are unable to cross., The glomerular filtration rate (GFR) is equal to the concentration of a solute in the urine,, times the volume of urine produced per minute, divided by the plasma concentration, (assuming that the solute is freely diffused e.g. inulin)., In clinical practice creatinine is used because it is subjected to very little proximal tubular, secretion., Although subject to variability, the typical GFR is 125ml per minute., Glomerular filtration rate = Total volume of plasma per unit time leaving the capillaries and, entering the bowman's capsule, Renal clearance = volume plasma from which a substance is removed per minute by the, kidneys, , Substances used to measure GFR have the following features:, 1. Inert, 2. Free filtration from the plasma at the glomerulus (not protein bound), 3. Not absorbed or secreted at the tubules, 4. Plasma concentration constant during urine collection, Examples: inulin, creatinine, GFR = urine concentration (mmol/l) x urine volume (ml/min), -------------------------------------------------------------------------plasma concentration (mmol/l), , , , , The clearance of a substance is dependent not only on its diffusivity across the basement, membrane but also subsequent tubular secretion and / or reabsorption., So glucose which is freely filtered across the basement membrane is usually reabsorbed, from tubules giving a clearance of zero., , Tubular function, , , , , , , Reabsorption and secretion of substances occurs in the tubules., In the proximal tubule substrates such as glucose, amino acids and phosphate are cotransported with sodium across the semi permeable membrane., Up to two thirds of filtered water is reabsorbed in the proximal tubules., This will lead to increase in urea concentration in the distal tubule allowing for its increased, diffusion., Substances to be secreted into the tubules are taken up from the peritubular blood by tubular, cells.
Page 240 :
, , , Solutes such as paraaminohippuric acid are cleared with a single passage through the, kidneys and this is why it is used to measure renal plasma flow. Ions such as calcium and, phosphate will have a tubular reabsorption that is influenced by plasma PTH levels., Potassium may be both secreted and re-absorbed and is co-exchanged with sodium., , Loop of Henle, , , , , , , , , , Approximately 60 litres of water containing 9000mmol sodium enters the descending limb of, the loop of Henle in 24 hours., Loops from the juxtamedullary nephrons run deep into the medulla., The osmolarity of fluid changes and is greatest at the tip of the papilla., The thin ascending limb is impermeable to water, but highly permeable to sodium and, chloride ions., This loss means that at the beginning of the thick ascending limb the fluid is hypo osmotic, compared with adjacent interstitial fluid., In the thick ascending limb the reabsorption of sodium and chloride ions occurs by both, facilitated and passive diffusion pathways., The loops of Henle are co-located with vasa recta, these will have similar solute, compositions to the surrounding extracellular fluid so preventing the diffusion and, subsequent removal of this hypertonic fluid., The energy dependent reabsorption of sodium and chloride in the thick ascending limb helps, to maintain this osmotic gradient., , Next question
Page 241 :
A 39 year old lady undergoes a laparoscopic cholecystectomy as a daycase. The operation is more, difficult than anticipated and the surgeon places a drain to the liver bed. In recovery 1.5 litres of, blood is seen to enter the drain. Which of the following substances is the first to be released in this, situation?, , Angiotensinogen, , Renin, , Angiotensin I, , Angiotensin II, , Aldosterone, , The decrease in blood pressure will be sensed by the juxtaglomerular cells in the kidney. This will, cause renin secretion., Please rate this question:, , Discuss and give feedback, , Next question, , Shock, , , , , , , , , Shock occurs when there is insufficient tissue perfusion., The pathophysiology of shock is an important surgical topic and may be divided into the, following aetiological groups:, Septic, Haemorrhagic, Neurogenic, Cardiogenic, Anaphylactic, , Septic shock, Septic shock is a major problem and those patients with severe sepsis have a mortality rate in, excess of 40%. In those who are admitted to intensive care mortality ranges from 6% with no organ, failure to 65% in those with 4 organ failure., Sepsis is defined as an infection that triggers a particular Systemic Inflammatory Response, Syndrome (SIRS). This is characterised by body temperature outside 36 oC - 38 o C, HR >90, beats/min, respiratory rate >20/min, WBC count >12,000/mm 3 or < 4,000/mm 3, altered mental state
Page 242 :
or hyperglycaemia (in absence of diabetes)., Patients with infections and two or more elements of SIRS meet the diagnostic criteria for sepsis., Those with organ failure have severe sepsis and those with refractory hypotension -septic shock., During the septic process there is marked activation of the immune system with extensive cytokine, release. This may be coupled with or triggered by systemic circulation of bacterial toxins. These all, cause endothelial cell damage and neutrophil adhesion. The overall hallmarks are thus those, ofexcessive inflammation, coagulation and fibrinolytic suppression., The surviving sepsis campaign (2012) highlights the following key areas for attention:, , , , , Prompt administration of antibiotics to cover all likely pathogens coupled with a rigorous, search for the source of infection., Haemodynamic stabilisation. Many patients are hypovolaemic and require aggressive fluid, administration. Aim for CVP 8-12 cm H2O, MAP >65mmHg., Modulation of the septic response. This includes manoeuvres to counteract the changes and, includes measures such as tight glycaemic control. The routine use of steroids is not, advised., , In surgical patients, the main groups with septic shock include those with anastomotic leaks,, abscesses and extensive superficial infections such as necrotising fasciitis. When performing, surgery the aim should be to undertake the minimum necessary to restore physiology. These, patients do not fare well with prolonged surgery. Definitive surgery can be more safely undertaken, when physiology is restored and clotting in particular has been normalised., Haemorrhagic shock, The average adult blood volume comprises 7% of body weight. Thus in the 70 Kg adult this will, equate to 5 litres. This changes in children (8-9% body weight) and is slightly lower in the elderly., The table below outlines the 4 major classes of haemorrhagic shock and their associated, physiological sequelae:, , Parameter, , Class I, , Class II, , Class III, , Class IV, , Blood loss ml, , <750ml, , 750-1500ml, , 1500-2000ml, , >2000ml, , Blood loss %, , <15%, , 15-30%, , 30-40%, , >40%, , Pulse rate, , <100, , >100, , >120, , >140, , Blood pressure, , Normal, , Normal, , Decreased, , Decreased
Page 243 :
Parameter, , Class I, , Class II, , Class III, , Class IV, , Respiratory rate, , 14-20, , 20-30, , 30-40, , >35, , Urine output, , >30ml, , 20-30ml, , 5-15ml, , <5ml, , Symptoms, , Normal, , Anxious, , Confused, , Lethargic, , Decreasing blood pressure during haemorrhagic shock causes organ hypoperfusion and relative, myocardial ischaemia. The cardiac index gives a numerical value for tissue oxygen delivery and is, given by the equation: Cardiac index= Cardiac output/ body surface area. Where Hb is, haemoglobin concentration in blood and SaO2 the saturation and PaO2 the partial pressure of, oxygen. Detailed knowledge of this equation is required for the MRCS Viva but not for part A,, although you should understand the principle., In patients suffering from trauma the most likely cause of shock is haemorrhage. However, the, following may also be the cause or occur concomitantly:, , , , , , , Tension pneumothorax, Spinal cord injury, Myocardial contusion, Cardiac tamponade, , When assessing trauma patients it is worth remembering that in order to generate a palpable, femoral pulse an arterial pressure of >65mmHg is required., Once bleeding is controlled and circulating volume normalised the levels of transfusion should be to, maintain a Hb of 7-8 in those with no risk factors for tissue hypoxia and Hb 10 for those who have, such risk factors., Neurogenic shock, This occurs most often following a spinal cord transection, usually at a high level. There is, resultant interruption of the autonomic nervous system. The result is either decreased sympathetic, tone or increased parasympathetic tone, the effect of which is a decrease in peripheral vascular, resistance mediated by marked vasodilation., This results in decreased preload and thus decreased cardiac output (Starlings law). There is, decreased peripheral tissue perfusion and shock is thus produced. In contrast with many other types, of shock peripheral vasoconstrictors are used to return vascular tone to normal., Cardiogenic shock, In medical patients the main cause is ischaemic heart disease. In the traumatic setting direct, myocardial trauma or contusion is more likely. Evidence of ECG changes and overlying sternal
Page 244 :
fractures or contusions should raise the suspicion of injury. Treatment is largely supportive and, transthoracic echocardiography should be used to determine evidence of pericardial fluid or direct, myocardial injury. The measurement of troponin levels in trauma patients may be undertaken but, they are less useful in delineating the extent of myocardial trauma than following MI., When cardiac injury is of a blunt nature and is associated with cardiogenic shock the right side of the, heart is the most likely site of injury with chamber and or valve rupture. These patients require, surgery to repair these defects and will require cardiopulmonary bypass to achieve this. Some may, require intra aortic balloon pump as a bridge to surgery., Anaphylactic shock, Anaphylaxis may be defined as a severe, life-threatening, generalised or systemic, hypersensitivity reaction., Anaphylaxis is one of the few times when you would not have time to look up the dose of a, medication. The Resuscitation Council guidelines on anaphylaxis have recently been updated., Adrenaline is by far the most important drug in anaphylaxis and should be given as soon as, possible. The recommended doses for adrenaline, hydrocortisone and chlorpheniramine are as, follows:, , Adrenaline, , Hydrocortisone, , Chlorpheniramine, , < 6 months, , 150 mcg (0.15ml 1 in 1,000), , 25 mg, , 250 mcg/kg, , 6 months - 6 years, , 150 mcg (0.15ml 1 in 1,000), , 50 mg, , 2.5 mg, , 6-12 years, , 300 mcg (0.3ml 1 in 1,000), , 100 mg, , 5 mg, , Adult and child 12 years, , 500 mcg (0.5ml 1 in 1,000), , 200 mg, , 10 mg, , Adrenaline can be repeated every 5 minutes if necessary. The best site for IM injection is the, anterolateral aspect of the middle third of the thigh., Common identified causes of anaphylaxis, , , , , food (e.g. Nuts) - the most common cause in children, drugs, venom (e.g. Wasp sting), Next question
Page 246 :
Which of the following drugs causes hyperkalaemia?, , Heparin, , Ciprofloxacin, , Salbutamol, , Levothyroxine, , Codeine phosphate, , Both unfractionated and low-molecular weight heparin can cause hyperkalaemia. This is thought to, be caused by inhibition of aldosterone secretion. Salbutamol is a recognised treatment for, hyperkalaemia., Please rate this question:, , Discuss and give feedback, , Next question, , Hyperkalaemia, , , , , Plasma potassium levels are regulated by a number of factors including aldosterone, acidbase balance and insulin levels., Metabolic acidosis is associated with hyperkalaemia as hydrogen and potassium ions, compete with each other for exchange with sodium ions across cell membranes and in the, distal tubule., ECG changes seen in hyperkalaemia include tall-tented T waves, small P waves, widened, QRS leading to a sinusoidal pattern and asystole, , Causes of hyperkalaemia, , , , , , , , Acute renal failure, Drugs*: potassium sparing diuretics, ACE inhibitors, angiotensin 2 receptor blockers,, spironolactone, ciclosporin, heparin**, Metabolic acidosis, Addison's, Tissue necrosis/rhabdomylosis: burns, trauma, Massive blood transfusion
Page 247 :
Foods that are high in potassium, , , , Salt substitutes (i.e. Contain potassium rather than sodium), Bananas, oranges, kiwi fruit, avocado, spinach, tomatoes, , *beta-blockers interfere with potassium transport into cells and can potentially cause hyperkalaemia, in renal failure patients - remember beta-agonists, e.g. Salbutamol, are sometimes used as, emergency treatment, **both unfractionated and low-molecular weight heparin can cause hyperkalaemia. This is thought to, be caused by inhibition of aldosterone secretion, Next question
Page 248 :
A 25-year-old man who has been morbidly obese for the past five years is reviewed in the surgical, bariatric clinic. In this patient, release of which of the following hormones would increase appetite?, , Leptin, , Thyroxine, , Adiponectin, , Ghrelin, , Serotonin, Obesity hormones, , , , leptin decreases appetite, ghrelin increases appetite, , Whilst thyroxine can increase appetite it does not fit with the clinical picture being described., Please rate this question:, , Discuss and give feedback, , Next question, , Obesity: physiology, Leptin, Leptin is thought to play a key role in the regulation of body weight. It is produced by adipose tissue, and acts on satiety centres in the hypothalamus and decreases appetite. More adipose tissue (e.g., in obesity) results in high leptin levels., Leptin stimulates the release of melanocyte-stimulating hormone (MSH) and corticotrophin-releasing, hormone (CRH). Low levels of leptin stimulates the release of neuropeptide Y (NPY), Ghrelin, Where as leptin induces satiety, ghrelin stimulates hunger. It is produced mainly by the fundus of the, stomach and the pancreas. Ghrelin levels increase before meals and decrease after meals, Next question
Page 249 :
Which of the following is not linked to excess glucocorticoids?, , Osteonecrosis, , Osteoporosis, , Hypokalaemia, , Hyponatraemia, , Growth retardation in children, , There are many adverse effects associated with excess glucocorticoids. Thinning of the skin,, osteonecrosis and osteoporosis are all common. Steroids are associated with retention of sodium, and water. Potassium loss may occur and hypokalaemic alkalosis has been reported., Please rate this question:, , Discuss and give feedback, , Next question, , Cortisol, , , , , , , Glucocorticoid, Released by zona fasiculata of the adrenal gland, 90% protein bound; 10% active, Circadian rhythm: High in the mornings, Negative feedback via ACTH, , Actions, , , , , , , , , , , , Glycogenolysis, Gluconeogenesis, Protein catabolism, Lipolysis, Stress response, Anti-inflammatory, Decrease protein in bones, Increase gastric acid, Increases neutrophils/platelets/red blood cells, Inhibits fibroblastic activity
Page 250 :
A 54-year-old woman is admitted to the Surgical Admissions Unit with abdominal pain. Blood tests, taken on admission show the following:, Magnesium, , 0.40 mmol/l (normal value 0.7-1.0 mmol/l), , Which one of the following factors is most likely to be responsible for this result?, , Excessive resuscitation with intravenous saline, , Digoxin therapy, , Diarrhoea, , Hypothermia, , Rhabdomyolysis, , Please rate this question:, , Discuss and give feedback, , Next question, , Hypomagnasaemia, Cause of low magnesium, , , , , , , Diuretics, Total parenteral nutrition, Diarrhoea, Alcohol, Hypokalaemia, hypocalcaemia, , Features, , , , , , Paraesthesia, Tetany, Seizures, Arrhythmias
Page 252 :
A 43 year old man has a nasogastric tube inserted. The nurse takes a small aspirate of the fluid from, the stomach and tests the pH of the aspirate. What is the normal intragastric pH?, , 0.5, , 2, , 4, , 5, , 6, , Theme from January 2012 Exam, The intragastric pH is usually 2. Administration of proton pump inhibitors can result in almost, complete abolition of acidity, Please rate this question:, , Discuss and give feedback, , Next question, , Gastric secretions, A working knowledge of gastric secretions is important for surgery because peptic ulcers are, common, surgeons frequently prescribe anti secretory drugs and because there are still patients, around who will have undergone acid lowering procedures (Vagotomy) in the past., Gastric acid, , , , , , Is produced by the parietal cells in the stomach, pH of gastric acid is around 2 with acidity being maintained by the H +/K+ ATP ase pump. As, part of the process bicarbonate ions will be secreted into the surrounding vessels., Sodium and chloride ions are actively secreted from the parietal cell into the canaliculus., This sets up a negative potential across the membrane and as a result sodium and, potassium ions diffuse across into the canaliculus., Carbonic anhydrase forms carbonic acid which dissociates and the hydrogen ions formed by, dissociation leave the cell via the H+/K+ antiporter pump. At the same time sodium ions are, actively absorbed. This leaves hydrogen and chloride ions in the canaliculus these mix and, are secreted into the lumen of the oxyntic gland.
Page 253 :
This is illustrated diagrammatically below:, , Image sourced from Wikipedia, , Phases of gastric acid secretion, There are 3 phases of gastric secretion:, 1. Cephalic phase (smell / taste of food), , , , 30% acid produced, Vagal cholinergic stimulation causing secretion of HCL and gastrin release from G cells, , 2. Gastric phase (distension of stomach ), , , , 60% acid produced, Stomach distension/low H+/peptides causes Gastrin release
Page 254 :
3. Intestinal phase (food in duodenum), , , , 10% acid produced, High acidity/distension/hypertonic solutions in the duodenum inhibits gastric acid secretion, via enterogastrones (CCK, secretin) and neural reflexes., , Regulation of gastric acid production, Factors increasing production include:, , , , , Vagal nerve stimulation, Gastrin release, Histamine release (indirectly following gastrin release) from enterchromaffin like cells, , Factors decreasing production include:, , , , , Somatostatin (inhibits histamine release), Cholecystokinin, Secretin, , The diagram below illustrates some of the factors involved in regulating gastric acid secretion and, the relevant associated pharmacology, , Image sourced from Wikipedia, , Below is a brief summary of the major hormones involved in food digestion:
Page 255 :
Source, , Stimulus, , Actions, , Gastrin, , G cells in, antrum of the, stomach, , Distension of, stomach, extrinsic, nerves, Inhibited by: low, antral pH,, somatostatin, , Increase HCL, pepsinogen and IF secretion,, increases gastric motility, trophic effect on, gastric mucosa, , CCK, , I cells in, upper small, intestine, , Partially digested, proteins and, triglycerides, , Increases secretion of enzyme-rich fluid, from pancreas, contraction of gallbladder, and relaxation of sphincter of Oddi,, decreases gastric emptying, trophic effect on, pancreatic acinar cells, induces satiety, , Secretin, , S cells in, upper small, intestine, , Acidic chyme,, fatty acids, , Increases secretion of bicarbonate-rich fluid, from pancreas and hepatic duct cells,, decreases gastric acid secretion, trophic, effect on pancreatic acinar cells, , VIP, , Small, intestine,, pancreas, , Neural, , Stimulates secretion by pancreas and, intestines, inhibits acid and pepsinogen, secretion, , Somatostatin, , D cells in the, pancreas and, stomach, , Fat, bile salts and, glucose in the, intestinal lumen, , Decreases acid and pepsin secretion,, decreases gastrin secretion, decreases, pancreatic enzyme secretion, decreases, insulin and glucagon secretion, inhibits trophic effects of gastrin, stimulates, gastric mucous production, Next question
Page 256 :
Which of the following is the equivalent of cardiac preload?, , End diastolic volume, , Stroke volume, , Systemic vascular resistance, , Mean arterial pressure, , Peak systolic arterial pressure, , Preload is the same as end diastolic volume. When it is increased slightly there is an associated, increase in cardiac output (Frank Starling principle). When it is markedly increased e.g. over 250ml, then cardiac output falls., Please rate this question:, , Discuss and give feedback, , Next question, , Cardiac physiology, , , , , , The heart has four chambers ejecting blood into both low pressure and high pressure, systems., The pumps generate pressures of between 0-25mmHg on the right side and 0-120 mmHg on, the left., At rest diastole comprises 2/3 of the cardiac cycle., The product of the frequency of heart rate and stroke volume combine to give the cardiac, output which is typically 5-6L per minute., , Detailed descriptions of the various waveforms are often not a feature of MRCS A (although they are, on the syllabus). However, they are a very popular topic for surgical physiology in the MRCS B, exam., Electrical properties, , , , Intrinsic myogenic rhythm within cardiac myocytes means that even the denervated heart is, capable of contraction., In the normal situation the cardiac impulse is generated in the sino atrial node in the right, atrium and conveyed to the ventricles via the atrioventricular node.
Page 257 :
, , , , The sino atrial node is also capable of spontaneous discharge and in the absence of, background vagal tone will typically discharge around 100x per minute. Hence the higher, resting heart rate found in cardiac transplant cases. In the SA and AV nodes the resting, membrane potential is lower than in surrounding cardiac cells and will slowly depolarise from, -70mV to around -50mV at which point an action potential is generated., Differences in the depolarisation slopes between SA and AV nodes help to explain why the, SA node will depolarise first. The cells have a refractory period during which they cannot be, re-stimulated and this period allows for adequate ventricular filling. In pathological, tachycardic states this time period is overridden and inadequate ventricular filling may then, occur, cardiac output falls and syncope may ensue., , Parasympathetic fibres project to the heart via the vagus and will release acetylcholine. Sympathetic, fibres release nor adrenaline and circulating adrenaline comes from the adrenal medulla., Noradrenaline binds to β 1 receptors in the SA node and increases the rate of pacemaker potential, depolarisation., Cardiac cycle, , Image sourced from Wikipedia, , , , Mid diastole: AV valves open. Ventricles hold 80% of final volume. Outflow valves shut., Aortic pressure is high., , , , Late diastole: Atria contract. Ventricles receive 20% to complete filling. Typical end diastolic, volume 130-160ml.
Page 258 :
, , Early systole: AV valves shut. Ventricular pressure rises. Isovolumetric ventricular, contraction. AV Valves bulge into atria (c-wave). Aortic and pulmonary pressure exceededblood is ejected. Shortening of ventricles pulls atria downwards and drops intra atrial, pressure (x-descent)., , , , Late systole: Ventricular muscles relax and ventricular pressures drop. Although ventricular, pressure drops the aortic pressure remains constant owing to peripheral vascular resistance, and elastic property of the aorta. Brief period of retrograde flow that occurs in aortic recoil, shuts the aortic valve. Ventricles will contain 60ml end systolic volume. The average stroke, volume is 70ml (i.e. Volume ejected)., , , , Early diastole: All valves are closed. Isovolumetric ventricular relaxation occurs. Pressure, wave associated with closure of the aortic valve increases aortic pressure. The pressure dip, before this rise can be seen on arterial waveforms and is called the incisura. During systole, the atrial pressure increases such that it is now above zero (v- wave). Eventually atrial, pressure exceed ventricular pressure and AV valves open - atria empty passively into, ventricles and atrial pressure falls (y -descent ), , The negative atrial pressures are of clinical importance as they can allow air embolization to occur if, the neck veins are exposed to air. This patient positioning is important in head and neck surgery to, avoid this occurrence if veins are inadvertently cut, or during CVP line insertion., Mechanical properties, , , , Preload = end diastolic volume, Afterload = aortic pressure, , It is important to understand the principles of Laplace's law in surgery., , , , , It states that for hollow organs with a circular cross section, the total circumferential wall, tension depends upon the circumference of the wall, multiplied by the thickness of the wall, and on the wall tension., The total luminal pressure depends upon the cross sectional area of the lumen and the, transmural pressure. Transmural pressure is the internal pressure minus external pressure, and at equilibrium the total pressure must counterbalance each other., In terms of cardiac physiology the law explains that the rise in ventricular pressure that, occurs during the ejection phase is due to physical change in heart size. It also explains why, a dilated diseased heart will have impaired systolic function.
Page 259 :
Starlings law, , , , Increase in end diastolic volume will produce larger stroke volume., This occurs up to a point beyond which cardiac fibres are excessively stretched and stroke, volume will fall once more. It is important for the regulation of cardiac output in cardiac, transplant patients who need to increase their cardiac output., , Baroreceptor reflexes, , , , , , , Baroreceptors located in aortic arch and carotid sinus., Aortic baroreceptor impulses travel via the vagus and from the carotid via the, glossopharyngeal nerve., They are stimulated by arterial stretch., Even at normal blood pressures they are tonically active., Increase in baroreceptor discharge causes:, , *Increased parasympathetic discharge to the SA node., *Decreased sympathetic discharge to ventricular muscle causing decreased contractility and fall in, stroke volume., *Decreased sympathetic discharge to venous system causing increased compliance., *Decreased peripheral arterial vascular resistance, Atrial stretch receptors, , , , , , , , Located in atria at junction between pulmonary veins and vena cava., Stimulated by atrial stretch and are thus low pressure sensors., Increased blood volume will cause increased parasympathetic activity., Very rapid infusion of blood will result in increase in heart rate mediated via atrial receptors:, theBainbridge reflex., Decreases in receptor stimulation results in increased sympathetic activity this will decrease, renal blood flow-decreases GFR-decreases urinary sodium excretion-renin secretion by, juxtaglomerular apparatus-Increase in angiotensin II., Increased atrial stretch will also result in increased release of atrial natriuretic peptide., Next question
Page 260 :
A 48 year old man undergoes a right hemicolectomy for a large caecal polyp. In the immediate post, operative period which of the physiological processes described below is least likely to occur?, , Glycogenolysis, , Increased production of acute phase proteins, , Increased cortisol production, , Bronchoconstriction, , Release of nitric oxide by vessels, , Please rate this question:, , Discuss and give feedback, , Next question, , Response to surgery, Sympathetic nervous system, , , , , Noradrenaline from sympathetic nerves and adrenaline from adrenal medulla, Blood diverted from skin and visceral organs; bronchodilatation, reduced intestinal motility,, increased glucagon and glycogenolysis, insulin reduced, Heart rate and myocardial contractility are increased, , Acute phase response, , , , , TNF-α, IL-1, IL-2, IL-6, interferon and prostaglandins are released, Excess cytokines may cause SIRS, Cytokines increase the release of acute phase proteins, , Endocrine response, , , Hypothalamus, pituitary, adrenal axis
Page 261 :
, , Increases ACTH and cortisol production:, , increases protein breakdown, increases blood glucose levels, , , , Aldosterone increases sodium re-absorption, Vasopressin increases water re-absorption and causes vasoconstriction, , Vascular endothelium, , , , , Nitric oxide produces vasodilatation, Platelet activating factor enhances the cytokine response, Prostaglandins produce vasodilatation and induce platelet aggregation, Next question
Page 262 :
, , A 73 year old female is referred to the surgical clinic with an iron deficiency anaemia. As part, of the diagnostic work up the doctor requests a serum ferritin level. Which of the conditions, listed is most likely to lead to a falsely elevated result?, , Locally perforated sigmoid colonic adenocarcinoma, , Colonic angiodysplasia, , Dieulafoy lesion of the stomach, , Transitional cell carcinoma of the bladder, , Endometrial adenocarcinoma, , , , , A locally perforated colonic tumour will typically cause an intense inflammatory response and, if peritonitis is not present clinically then at the very least a localised abscess. This, inflammatory process is the most likely (from the list) to falsely raise the serum ferritin level., Angiodysplasia and dieulafoy lesions are mucosal arteriovenous malformations and unlikely, to result in considerable inflammatory activity., Please rate this question:, , , , , , Discuss and give feedback, , , , Next question, , , , Ferritin, , , , Ferritin is an intracellular protein that binds iron and stores it to be released in a controlled, fashion at sites where iron is required. Because iron and ferritin are bound the total body, ferritin levels may be decreased in cases of iron deficiency anaemia. Measurement of serum, ferritin levels can be useful in determining whether an apparently low haemoglobin and, microcytosis is truly caused by an iron deficiency state., Ferritin is an acute phase protein and may be synthesised in increased quantities in, situations where inflammatory activity is ongoing. Falsely elevated results may therefore be, encountered clinically and need to be taken in context of the clinical picture and full blood, count results.
Page 263 :
, , Which of the following is least likely to cause a prolonged prothrombin time?, , Cholestatic jaundice, , Disseminated intravascular coagulation, , Prolonged antibiotic treatment, , Liver disease, , Acquired factor 12 deficiency, , , , , Vitamin K deficiency results from cholestatic jaundice and prolonged antibiotic therapy., Acquired factor 12 deficiency causes prolonged APTT., Please rate this question:, , , , , , Discuss and give feedback, , , , , , Abnormal coagulation, , Cause, , Factors affected, , Heparin, , Prevents activation factors 2,9,10,11, , Warfarin, , Affects synthesis of factors 2,7,9,10, , DIC, , Factors 1,2,5,8,11, , Next question
Page 264 :
Cause, , Factors affected, , Liver disease, , Factors 1,2,5,7,9,10,11, , , , Interpretation blood clotting test results, , Disorder, , APTT, , PT, , Bleeding time, , Haemophilia, , Increased, , Normal, , Normal, , von Willebrand's disease, , Increased, , Normal, , Increased, , Vitamin K deficiency, , Increased, , Increased, , Normal, , , , , Next question
Page 265 :
Which statement about peristalsis is true?, , Longitudinal smooth muscle propels the food bolus through the oesophagus, , Secondary peristalsis occurs when there is no food bolus in the oesophagus, , Food transfer from the oesophagus to the stomach is 4 seconds, , Circular smooth muscle is not involved in peristalsis, , Peristalsis only occurs in the oesophagus, , Please rate this question:, , Discuss and give feedback, , Next question, , Peristalsis, , , , , , , Circular smooth muscle contracts behind the food bolus and longitudinal smooth muscle, propels the food through the oesophagus, Primary peristalsis spontaneously moves the food from the oesophagus into the stomach (9, seconds), Secondary peristalsis occurs when food, which doesn't enter the stomach, stimulates stretch, receptors to cause peristalsis, In the small intestine each peristalsis waves slows to a few seconds and causes mixture of, chyme, In the colon three main types of peristaltic activity are recognised (see below), , Colonic peristalsis, , Segmentation contractions, , Localised contractions in which the bolus is subjected to local, forces to maximise mucosal absorption, , Antiperistaltic contractions, towards ileum, , Localised reverse peristaltic waves to slow entry into colon and, maximise absorption
Page 266 :
Mass movements, , Waves migratory peristaltic waves along the entire colon to, empty the organ prior to the next ingestion of food bolus, Next question
Page 267 :
A 24 year old man is injured in a road traffic accident. He becomes oliguric and his renal function, deteriorates. Which of the options below would favor acute tubular necrosis over pre renal uraemia?, , No response to intravenous fluids, , Urinary sodium < 20mmol/L, , Bland coloured urinary sediment, , Increased urine specific gravity, , None of the above, , In acute tubular necrosis there is no response to intravenous fluids because the damage occurs from, within the renal system rather than as a result of volume depletion., Please rate this question:, , Discuss and give feedback, , Next question, , Acute renal failure: Pre renal failure vs. acute tubular necrosis, Prerenal uraemia - kidneys retain sodium to preserve volume, , Urine sodium, , Pre-renal uraemia, , Acute tubular necrosis, , < 20 mmol/L, , > 30 mmol/L
Page 268 :
Pre-renal uraemia, , Acute tubular necrosis, , Fractional sodium excretion*, , < 1%, , > 1%, , Fractional urea excretion**, , < 35%, , >35%, , Urine:plasma osmolality, , > 1.5, , < 1.1, , Urine:plasma urea, , > 10:1, , < 8:1, , Specific gravity, , > 1020, , < 1010, , Urine, , 'bland' sediment, , brown granular casts, , Response to fluid challenge, , Yes, , No, , *fractional sodium excretion = (urine sodium/plasma sodium) / (urine creatinine/plasma creatinine) x, 100, **fractional urea excretion = (urine urea /blood urea ) / (urine creatinine/plasma creatinine) x 100, Next question
Page 269 :
Which of the following is not an effect of cholecystokinin?, , It causes gallbladder contraction, , It increases the rate of gastric emptying, , It relaxes the sphincter of oddi, , It stimulates pancreatic acinar cells, , It has a trophic effect on pancreatic acinar cells, , It decreases the rate of gastric emptying., Please rate this question:, , Discuss and give feedback, , Next question, , Gastric secretions, A working knowledge of gastric secretions is important for surgery because peptic ulcers are, common, surgeons frequently prescribe anti secretory drugs and because there are still patients, around who will have undergone acid lowering procedures (Vagotomy) in the past., Gastric acid, , , , , , Is produced by the parietal cells in the stomach, pH of gastric acid is around 2 with acidity being maintained by the H +/K+ ATP ase pump. As, part of the process bicarbonate ions will be secreted into the surrounding vessels., Sodium and chloride ions are actively secreted from the parietal cell into the canaliculus., This sets up a negative potential across the membrane and as a result sodium and, potassium ions diffuse across into the canaliculus., Carbonic anhydrase forms carbonic acid which dissociates and the hydrogen ions formed by, dissociation leave the cell via the H+/K+ antiporter pump. At the same time sodium ions are, actively absorbed. This leaves hydrogen and chloride ions in the canaliculus these mix and, are secreted into the lumen of the oxyntic gland., , This is illustrated diagrammatically below:
Page 270 :
Image sourced from Wikipedia, , Phases of gastric acid secretion, There are 3 phases of gastric secretion:, 1. Cephalic phase (smell / taste of food), , , , 30% acid produced, Vagal cholinergic stimulation causing secretion of HCL and gastrin release from G cells, , 2. Gastric phase (distension of stomach ), , , , 60% acid produced, Stomach distension/low H+/peptides causes Gastrin release, , 3. Intestinal phase (food in duodenum)
Page 271 :
, , , 10% acid produced, High acidity/distension/hypertonic solutions in the duodenum inhibits gastric acid secretion, via enterogastrones (CCK, secretin) and neural reflexes., , Regulation of gastric acid production, Factors increasing production include:, , , , , Vagal nerve stimulation, Gastrin release, Histamine release (indirectly following gastrin release) from enterchromaffin like cells, , Factors decreasing production include:, , , , , Somatostatin (inhibits histamine release), Cholecystokinin, Secretin, , The diagram below illustrates some of the factors involved in regulating gastric acid secretion and, the relevant associated pharmacology, , Image sourced from Wikipedia, , Below is a brief summary of the major hormones involved in food digestion:, , Source, , Stimulus, , Actions
Page 272 :
Gastrin, , G cells in, antrum of the, stomach, , Distension of, stomach, extrinsic, nerves, Inhibited by: low, antral pH,, somatostatin, , Increase HCL, pepsinogen and IF secretion,, increases gastric motility, trophic effect on, gastric mucosa, , CCK, , I cells in, upper small, intestine, , Partially digested, proteins and, triglycerides, , Increases secretion of enzyme-rich fluid, from pancreas, contraction of gallbladder, and relaxation of sphincter of Oddi,, decreases gastric emptying, trophic effect on, pancreatic acinar cells, induces satiety, , Secretin, , S cells in, upper small, intestine, , Acidic chyme,, fatty acids, , Increases secretion of bicarbonate-rich fluid, from pancreas and hepatic duct cells,, decreases gastric acid secretion, trophic, effect on pancreatic acinar cells, , VIP, , Small, intestine,, pancreas, , Neural, , Stimulates secretion by pancreas and, intestines, inhibits acid and pepsinogen, secretion, , Somatostatin, , D cells in the, pancreas and, stomach, , Fat, bile salts and, glucose in the, intestinal lumen, , Decreases acid and pepsin secretion,, decreases gastrin secretion, decreases, pancreatic enzyme secretion, decreases, insulin and glucagon secretion, inhibits trophic effects of gastrin, stimulates, gastric mucous production, Next question
Page 273 :
Which part of the jugular venous waveform is associated with the closure of the tricuspid valve?, , a wave, , c wave, , x descent, , y descent, , v wave, JVP: C wave - closure of the tricuspid valve, The c wave of the jugular venous waveform is associated with the closure of the tricuspid valve., Please rate this question:, , Discuss and give feedback, , Next question, , Jugular venous pressure, As well as providing information on right atrial pressure, the jugular vein waveform may provide, clues to underlying valvular disease. A non-pulsatile JVP is seen in superior vena caval obstruction., Kussmaul's sign describes a paradoxical rise in JVP during inspiration seen in constrictive, pericarditis, 'a' wave = atrial contraction, , , , large if atrial pressure e.g. tricuspid stenosis, pulmonary stenosis, pulmonary hypertension, absent if in atrial fibrillation, , Cannon 'a' waves, , , , caused by atrial contractions against a closed tricuspid valve, are seen in complete heart block, ventricular tachycardia/ectopics, nodal rhythm, single, chamber ventricular pacing
Page 274 :
'c' wave, , , , closure of tricuspid valve, not normally visible, , 'v' wave, , , , due to passive filling of blood into the atrium against a closed tricuspid valve, giant v waves in tricuspid regurgitation, , 'x' descent = fall in atrial pressure during ventricular systole, 'y' descent = opening of tricuspid valve, , Image sourced from Wikipedia, , Next question
Page 275 :
Which one of the following serum proteins is most likely to increase in a patient with severe sepsis?, , Transferrin, , Transthyretin, , Ferritin, , Albumin, , Cortisol binding protein, , Ferritin can be markedly increased during acute illness. The other parameters tend to decrease, during an acute phase response., Please rate this question:, , Discuss and give feedback, , Next question, , Acute phase proteins, Acute phase proteins, , , , , , , , , , , CRP, procalcitonin, ferritin, fibrinogen, alpha-1 antitrypsin, caeruloplasmin, serum amyloid A, haptoglobin, complement, , During the acute phase response the liver decreases the production of other proteins (sometimes, referred to as negative acute phase proteins). Examples include:, , , , , albumin, transthyretin (formerly known as prealbumin), transferrin
Page 276 :
, , , retinol binding protein, cortisol binding protein, , Levels of CRP are commonly measured in acutely unwell patients. CRP is a protein synthesised in, the liver and binds to phosphocholine in bacterial cells and on those cells undergoing apoptosis. In, binding to these cells it is then able to activate the complement system. CRP levels are known to, rise in patients following surgery. However, levels of greater than 150 at 48 hours post operatively, are suggestive of evolving complications., Next question
Page 277 :
Theme: Critical care, , A. Hypovolaemia, B. Normal, C. Cardiogenic shock, D. Septic shock, , For each of the scenarios outlined in the tables below, please select the most likely diagnosis from, the list. Each option may be used once, more than once or not at all., , 72., , A 45 year old man is admitted to the intensive care unit following a laparotomy. He has a central, line, pulmonary artery catheter and arterial lines inserted. The following results are obtained:, Pulmonary artery occlusion, pressure, , Cardiac output, , Systemic vascular, resistance, , Low, , Low, , High, , Hypovolaemia, Theme from April 2012 Exam, Cardiac output is lowered in hypovolaemia due to decreased preload., , 73., , A 75 year old man is admitted to the intensive care unit following a laparotomy. He has a central, line, pulmonary artery catheter and arterial lines inserted. The following results are obtained:, Pulmonary artery occlusion, pressure, , Cardiac output, , Systemic vascular, resistance, , High, , Low, , High
Page 278 :
You answered Hypovolaemia, The correct answer is Cardiogenic shock, In cardiogenic shock pulmonary pressures are often high. This is the basis for the use of, venodilators in the treatment of pulmonary oedema., , 74., , A 22 year old lady is admitted to the intensive care unit following a laparotomy. She has a central, line, pulmonary artery catheter and arterial lines inserted. The following results are obtained:, Pulmonary artery occlusion, pressure, , Cardiac output, , Systemic vascular, resistance, , Low, , High, , Low, , You answered Hypovolaemia, The correct answer is Septic shock, Decreased SVR is a major feature of sepsis. A hyperdynamic circulation is often present. This is the, reason for the use of vasoconstrictors., , Please rate this question:, , Discuss and give feedback, , Next question, , Pulmonary artery occlusion pressure monitoring, The pulmonary artery occlusion pressure is an indirect measure of left atrial pressure, and thus filling, pressure of the left heart. The low resistance within the pulmonary venous system allows this useful
Page 279 :
measurement to be made. The most accurate trace is made by inflating the balloon at the catheter, tip and "floating" it so that it occludes the vessel. If it is not possible to occlude the vessel in this way, then the measurement gained will be the pulmonary artery end diastolic pressure., Interpretation of PAOP, , PAOP, , mmHg, , Scenario, , Normal, , 8-12, , Low, , <5, , Hypovolaemia, , Low with pulmonary oedema, , <5, , ARDS, , High, , >18, , Overload, , When combined with measurements of systemic vascular resistance and cardiac output it is possible, to accurately classify patients., Systemic vascular resistance, Derived from aortic pressure, right atrial pressure and cardiac output., SVR=80(mean aortic pressure-mean right atrial pressure)/cardiac output, Next question
Page 280 :
A 23 year old man has a routine ECG performed. Which part of the tracing obtained represents atrial, repolarisation?, , P wave, , T wave, , Q-T Interval, , P-R interval, , None of the above, , The process of atrial repolarisation is generally not visible on the ECG strip. It occurs during the, QRS complex., Please rate this question:, , Discuss and give feedback, , Next question, , The normal ECG
Page 281 :
Image sourced from Wikipedia, , P wave, , , , , Represents the wave of depolarization that spreads from the SA node throughout the atria, Lasts 0.08 to 0.1 seconds (80-100 ms), The isoelectric period after the P wave represents the time in which the impulse is traveling, within the AV node, , P-R interval, , , , , Time from the onset of the P wave to the beginning of the QRS complex, Ranges from 0.12 to 0.20 seconds in duration, Represents the time between the onset of atrial depolarization and the onset of ventricular, depolarization, , QRS complex, , , , Represents ventricular depolarization, Duration of the QRS complex is normally 0.06 to 0.1 seconds
Page 282 :
ST segment, , , , Isoelectric period following the QRS, Represents period which the entire ventricle is depolarized and roughly corresponds to the, plateau phase of the ventricular action potential, , T wave, , , , Represents ventricular repolarization and is longer in duration than depolarization, A small positive U wave may follow the T wave which represents the last remnants of, ventricular repolarization., , Q-T interval, , , , , , , Represents the time for both ventricular depolarization and repolarization to occur, and, therefore roughly estimates the duration of an average ventricular action potential., Interval ranges from 0.2 to 0.4 seconds depending upon heart rate., At high heart rates, ventricular action potentials shorten in duration, which decreases the Q-T, interval. Therefore the Q-T interval is expressed as a "corrected Q-T (QTc)" by taking the QT interval and dividing it by the square root of the R-R interval (interval between ventricular, depolarizations). This allows an assessment of the Q-T interval that is independent of heart, rate., Normal corrected Q-Tc interval is less than 0.44 seconds., Next question
Page 283 :
A 72-year-old woman is admitted to the acute surgical unit with profuse vomiting. Admission bloods, show the following:, Na+, , 131 mmol/l, , K+, , 2.2 mmol/l, , Urea, , 3.1 mmol/l, , Creatinine, , 56 µmol/l, , Glucose, , 4.3 mmol/l, , Which one of the following ECG features is most likely to be seen?, , Short PR interval, , Short QT interval, , Flattened P waves, , J waves, , U waves, Hypokalaemia - U waves on ECG, J waves are seen in hypothermia whilst delta waves are associated with Wolff Parkinson White, syndrome., Please rate this question:, , Discuss and give feedback, , Next question, , ECG features in hypokalemia, , , , , , , U waves, Small or absent T waves (occasionally inversion), Prolonged PR interval, ST depression, Long QT interval
Page 284 :
One registered user suggests the following rhyme!, , , In Hypokalaemia, U have no Pot and no T, but a long PR and a long QT!, , Next question
Page 285 :
The oxygen-haemoglobin dissociation curve is shifted to the left in:, , With decreased 2,3-DPG in transfused red cells, , Respiratory acidosis, , High altitude, , Pyrexia, , Haemolytic anaemia, S shaped curve, The curve is shifted to the left when there is a decreased oxygen requirement by the tissue. This, includes:, 1. Hypothermia, 2. Alkalosis, 3. Reduced levels of DPG:, , , DPG is found in erythrocytes and is reduced in non exercising muscles, i.e. when there is, reduced glycolysis., , 4. Polycythaemia, Please rate this question:, , Discuss and give feedback, , Next question, , Oxygen Transport, Oxygen transport, Almost all oxygen is transported within erythrocytes. It has limited solubility and only 1% is carried as, solution. Therefore the amount of oxygen transported will depend upon haemoglobin concentration, and its degree of saturation., Haemoglobin, Globular protein composed of 4 subunits. Haem consists of a protoporphyrin ring surrounding an, iron atom in its ferrous state. The iron can form two additional bonds; one with oxygen and the other, with a polypeptide chain. There are two alpha and two beta subunits to this polypeptide chain in an, adult and together these form globin. Globin cannot bind oxygen but is able to bind to carbon dioxide
Page 286 :
and hydrogen ions, the beta chains are able to bind to 2,3 diphosphoglycerate. The oxygenation of, haemoglobin is a reversible reaction. The molecular shape of haemoglobin is such that binding of, one oxygen molecule facilitates the binding of subsequent molecules., Oxygen dissociation curve, , , , The oxygen dissociation curve describes the relationship between the percentage of, saturated haemoglobin and partial pressure of oxygen in the blood. It is not affected by, haemoglobin concentration., Chronic anaemia causes 2, 3 DPG levels to increase, hence shifting the curve to the right, , Haldane effect, , , Shifts to left = for given oxygen tension there is increased saturation of Hb with oxygen i.e., Decreased oxygen delivery to tissues, , Bohr effect, , , Shifts to right = for given oxygen tension there is reduced saturation of Hb with oxygen i.e., Enhanced oxygen delivery to tissues
Page 287 :
Image sourced from Wikipedia, , Shifts to Left = Lower oxygen delivery, , , , , , , HbF, methaemoglobin, carboxyhaemoglobin, low [H+] (alkali), low pCO2, low 2,3-DPG, low temperature, , Shifts to Right = Raised oxygen, delivery, , , , , , raised [H+] (acidic), raised pCO2, raised 2,3-DPG*, raised temperature, , *2,3-diphosphoglycerate, Next question
Page 288 :
A homeless 42 year old male had an emergency inguinal hernia repair 24 hours previously. He has, a BMI of 15. He has been put on a feeding regime of 35 kcal/kg/day with no additional medications., The nursing staff contact you as he has become confused and unsteady. On examination the patient, is disorientated to place, has diplopia and nystagmus. What is the most likely diagnosis?, , Cerebellar stroke, , Acute dystonic reaction, , Cerebrovascular accident, , Parkinsonism, , Wernickes encephalopathy, Triad of Wernicke encephalopathy:, , , , , Acute confusion, Ataxia, Opthalmoplegia, , This patient has received a carbohydrate rich diet without any thiamine or vitamin B co strong, replacement. This has led to Wernickes encephalopathy, which classically presents with confusion,, ataxia and opthalmoplegia. Characteristically it is associated with chronic alcoholism, however it is, also known to occur post bariatric surgery., Please rate this question:, , Discuss and give feedback, , Next question, , Nutrition - Refeeding syndrome, Refeeding syndrome describes the metabolic abnormalities which occur on feeding a person, following a period of starvation. The metabolic consequences include:, , , , , , Hypophosphataemia, Hypokalaemia, Hypomagnesaemia, Abnormal fluid balance
Page 289 :
These abnormalities can lead to organ failure., Re-feeding problems, If patient not eaten for > 5 days, aim to re-feed at < 50% energy and protein levels, High risk for re-feeding problems, If one or more of the following:, , , , , , BMI < 16 kg/m 2, Unintentional weight loss >15% over 3-6 months, Little nutritional intake > 10 days, Hypokalaemia, Hypophosphataemia or hypomagnesaemia prior to feeding (unless high), , If two or more of the following:, , , , , , BMI < 18.5 kg/m2, Unintentional weight loss > 10% over 3-6 months, Little nutritional intake > 5 days, History of: alcohol abuse, drug therapy including insulin, chemotherapy, diuretics and, antacids, , Prescription, , , , , Start at up to 10 kcal/kg/day increasing to full needs over 4-7 days, Start immediately before and during feeding: oral thiamine 200-300mg/day, vitamin B co, strong 1 tds and supplements, Give K+ (2-4 mmol/kg/day), phosphate (0.3-0.6 mmol/kg/day), magnesium (0.2-0.4, mmol/kg/day), Next question
Page 290 :
A 22 year old lady receives intravenous morphine for acute abdominal pain. Which of the following, best accounts for its analgesic properties?, , Binding to δ opioid receptors in the brainstem, Binding to δ opioid receptors at peripheral nerve sites, Binding to β opioid receptors within the CNS, Binding to α opioid receptors within the CNS, , Binding to µ opioid receptors within the CNS, 4 Types of opioid receptor:, , , , , , δ (located in CNS)- Accounts for analgesic and antidepressant effects, k (mainly CNS)- analgesic and dissociative effects, µ (central and peripheral) - causes analgesia, miosis, decreased gut motility, Nociceptin receptor (CNS)- Affect of appetite and tolerance to µ agonists., , Theme from April 2012 Exam, Please rate this question:, , Discuss and give feedback, , Next question, , Morphine, Strong opiate analgesic. It is a pro- type narcotic drug and its effects mediated via the 4 types of, opioid receptor. Its clinical effects stem from binding to these receptor sites within the CNS and, gastrointestinal tract. Unwanted side effects include nausea, constipation, respiratory depression, and, if used long term, addiction ., It may be administered orally or intravenously. It can be reversed with naloxone., Next question
Page 292 :
Which of the following stimulates prolactin release?, , Leutinising hormone, , Dopamine, , Thyrotropin releasing hormone, , Oestrogen, , Follicle stimulating hormone, , TRH stimulates prolactin release. Dopamine suppresses the release of prolactin., Please rate this question:, , Discuss and give feedback, , Next question, , Prolactin, Prolactin is a peptide hormone released from the anterior pituitary. It is under tonic dopamine, inhibition, thyrotropin releasing hormone has a stimulatory effect on release. Prolactin release, stimulates milk production but also reduces gonadal activity. It decreases GnRH pulsatility at the, hypothalamic level and to a lesser extent, blocks the action of LH on the ovary or testis., Next question
Page 293 :
Theme: Vitamin deficiency, , A. Vitamin A, B. Vitamin B1, C. Vitamin B12, D. Vitamin B3, E. Vitamin C, F. Vitamin K, G. Vitamin D, , Please select the vitamin deficiency most closely associated with the situation described. Each, option may be used once, more than once or not at all., , 82., , A 3 year old child presents with Rickets, You answered Vitamin A, The correct answer is Vitamin D, Vitamin D is needed to help mineralise bone. When this is deficient, mineralisation is inadequate, and deformities mayt result., , 83., , A 44 year old lady presents with jaundice. Following a minor ward based surgical procedure she, develops troublesome and persistent bleeding., You answered Vitamin A, The correct answer is Vitamin K, Patients who are jaundiced usually have impaired absorption of vitamin K. This can result in loss, of the vitamin K dependent clotting factors and troublesome bleeding.
Page 294 :
84., , A 69 year old man who has been living in sheltered accommodation for many months, with, inadequate nutrition notices that his night vision is becoming impaired., Vitamin A, Loss of vitamin A will result in impair rhodopsin synthesis and poor night vision., , Please rate this question:, , Discuss and give feedback, , Next question, , Vitamin deficiency, Vitamin, , Effect of deficiency, , A, , Night blindness, Epithelial atrophy, Infections, , B1, , Beriberi, , B2, , Dematitis and photosensitivity, , B3, , Pellagra, , B12, , Pernicious anaemia
Page 295 :
C, , Poor wound healing, Impaired collagen synthesis, , D, , Rickets (Children), Osteomalacia (Adults), , K, , Clotting disorders, Next question
Page 296 :
A 55 year old man undergoes a laparotomy and repair of incisional hernia. Which of the following, hormones is least likely to be released in increased quantities following the procedure?, , Insulin, , ACTH, , Glucocorticoids, , Aldosterone, , Growth hormone, , Insulin and thyroxine are often have reduced levels of secretion in the post operative period. This,, coupled with increased glucocorticoid release may cause difficulty in management of diabetes in, individuals with insulin resistance., Please rate this question:, , Discuss and give feedback, , Next question, , Stress response: Endocrine and metabolic changes, , , , , Surgery precipitates hormonal and metabolic changes causing the stress response., Stress response is associated with: substrate mobilization, muscle protein loss, sodium and, water retention, suppression of anabolic hormone secretion, activation of the sympathetic, nervous system, immunological and haematological changes., The hypothalamic-pituitary axis and the sympathetic nervous systems are activated and, there is a failure of the normal feedback mechanisms of control of hormone secretion., , A summary of the hormonal changes associated with the stress response:, , Increased, , Decreased, , No Change, , Growth hormone, , Insulin, , Thyroid stimulating hormone
Page 297 :
Increased, , Decreased, , No Change, , Cortisol, , Testosterone, , Luteinizing hormone, , Renin, , Oestrogen, , Follicle stimulating hormone, , Adrenocorticotrophic hormone (ACTH), , Aldosterone, , Prolactin, , Antidiuretic hormone, , Glucagon, , Sympathetic nervous system, , , , Stimulates catecholamine release, Causes tachycardia and hypertension, , Pituitary gland, , , , , , ACTH and growth hormone (GH) is stimulated by hypothalamic releasing factors,, corticotrophin releasing factor (CRF) and somatotrophin (or growth hormone releasing factor), Perioperative increased prolactin secretion occurs by release of inhibitory control, Secretion of thyroid stimulating hormone (TSH), luteinizing hormone (LH) and follicle, stimulating hormone (FSH) does not change significantly, ACTH stimulates cortisol production within a few minutes of the start of surgery. More ACTH, is produced than needed to produce a maximum adrenocortical response.
Page 298 :
Cortisol, , , , , , Significant increases within 4-6 hours of surgery (>1000 nmol litre-1)., The usual negative feedback mechanism fails and concentrations of ACTH and cortisol, remain persistently increased., The magnitude and duration of the increase correlate with the severity of stress and the, response is not abolished by the administration of corticosteroids., The metabolic effects of cortisol are enhanced:, , Skeletal muscle protein breakdown to provide gluconeogenic precursors and amino acids for protein, synthesis in the liver, Stimulation of lipolysis, 'Anti-insulin effect', Mineralocorticoid effects, Anti-inflammatory effects, Growth hormone, , , , Increased secretion after surgery has a minor role, Most important for preventing muscle protein breakdown and promote tissue repair by insulin, growth factors, , Alpha Endorphin, , , Increased, , Antidiuretic hormone, , , , , An important vasopressor and enhances haemostasis, Renin is released causing the conversion of angiotensinogen to angiotensin I, Angiotensin II formed by ACE on angiotensin 1, which causes the secretion of aldosterone, from the adrenal cortex. This increases sodium reabsorption at the distal convoluted tubule, , Insulin, , , , , , Release inhibited by stress, Occurs via the inhibition of the beta cells in the pancreas by the α2-adrenergic inhibitory, effects of catecholamines, Insulin resistance by target cells occurs later, The perioperative period is characterized by a state of functional insulin deficiency
Page 299 :
Thyroxine (T4) and tri-iodothyronine (T3), , , Circulating concentrations are inversely correlated with sympathetic activity and after surgery, there is a reduction in thyroid hormone production, which normalises over a few days., , Metabolic effect of endocrine response, Carbohydrate metabolism, , , , , , , , Hyperglycaemia is a main feature of the metabolic response to surgery, Due to increase in glucose production and a reduction in glucose utilization, Catecholamines and cortisol promote glycogenolysis and gluconeogenesis, Initial failure of insulin secretion followed by insulin resistance affects the normal responses, The proportion of the hyperglycaemic response reflects the severity of surgery, Hyperglycaemia impairs wound healing and increase infection rates, , Protein metabolism, , , , , , , Initially there is inhibition of protein anabolism, followed later, if the stress response is, severe, by enhanced catabolism, The amount of protein degradation is influenced by the type of surgery and also by the, nutritional status of the patient, Mainly skeletal muscle protein is affected, The amino acids released form acute phase proteins (fibrinogen, C reactive protein,, complement proteins, a2-macroglobulin, amyloid A and ceruloplasmin) and are used for, gluconeogenesis, Nutritional support has little effect on preventing catabolism, , Lipid metabolism, Increased catecholamine, cortisol and glucagon secretion, and insulin deficiency, promotes lipolysis, and ketone body production., Salt and water metabolism, , , , ADH causes water retention, concentrated urine, and potassium loss and may continue for 3, to 5 days after surgery, Renin causes sodium and water retention, , Cytokines, , , Glycoproteins
Page 300 :
, , , , Interleukins (IL) 1 to 17, interferons, and tumour necrosis factor, Synthesized by activated macrophages, fibroblasts, endothelial and glial cells in response to, tissue injury from surgery or trauma, IL-6 main cytokine associated with surgery. Peak 12 to 24 h after surgery and increase by, the degree of tissue damage Other effects of cytokines include fever, granulocytosis,, haemostasis, tissue damage limitation and promotion of healing., , Modifying the response, , , , , , , , , Opioids suppress hypothalamic and pituitary hormone secretion, At high doses the hormonal response to pelvic and abdominal surgery is abolished., However, such doses prolong recovery and increase the need for postoperative ventilatory, support, Spinal anaesthesia can reduce the glucose, ACTH, cortisol, GH and epinephrine changes,, although cytokine responses are unaltered, Cytokine release is reduced in less invasive surgery, Nutrition prevents the adverse effects of the stress response. Enteral feeding improves, recovery, Growth hormone and anabolic steroids may improve outcome, Normothermia decreases the metabolic response, , References, Deborah Burton, Grainne Nicholson, and George Hall, Endocrine and metabolic response to surgery ., Contin Educ Anaesth Crit Care Pain (2004) 4(5): 144-147 doi:10.1093/bjaceaccp/mkh040, Next question
Page 301 :
Which of the following is not a major function of the spleen in adults?, , Iron reutilisation, , Storage of platelets, , Storage of monocytes, , Haematopoeisis in haematological disorders, , Storage red blood cells, , The reservoir function of the spleen is less marked in humans than other animals (e.g. pigs) and in, normal individuals it can sequester between 5 and 10% of the red cell mass. The other stated, processes are major splenic functions and this accounts for the answer provided., Please rate this question:, , Discuss and give feedback, , Next question, , Spleen, The spleen is located in the left upper quadrant of the abdomen and its size can vary depending, upon the amount of blood it contains. The typical adult spleen is 12.5cm long and 7.5cm wide. The, usual weight of the adult spleen is 150g., The exact position of the spleen can vary with respiratory activity, posture and the state of, surrounding viscera. It usually lies obliquely with its long axis aligned to the 9th, 10th and 11th ribs. It, is separated from these ribs by both diaphragm and pleural cavity. The normal spleen is not, palpable., The shape of the spleen is influenced by the state of the colon and stomach. Gastric distension will, cause the spleen to resemble the shape of an orange segment. Colonic distension will cause it to, become more tetrahedral., The spleen is almost entirely covered by peritoneum, which adheres firmly to its capsule. Recesses, of the greater sac separate it from the stomach and kidney. It develops from the upper dorsal, mesogastrium, remaining connected to the posterior abdominal wall and stomach by two folds of, peritoneum; the lienorenal ligament and gastrosplenic ligament. The lienorenal ligament is derived, from peritoneum where the wall of the general peritoneum meets the omental bursa between the left, kidney and spleen; the splenic vessels lie in its layers. The gastrosplenic ligament also has two, layers, formed by the meeting of the walls of the greater sac and omental bursa between spleen and, stomach, the short gastric and left gastroepiploic branches of the splenic artery pass in its layers.
Page 303 :
, , , , , Infection: hepatitis, glandular fever, Infective endocarditis, Sickle-cell*, thalassaemia, Rheumatoid arthritis (Felty's syndrome), , *the majority of adult patients with sickle-cell will have an atrophied spleen due to repeated infarction, Next question
Page 304 :
Which one of the following is associated with increased lung compliance?, , Kyphosis, , Pulmonary oedema, , Emphysema, , Pulmonary fibrosis, , Pneumonectomy, , Please rate this question:, , Discuss and give feedback, , Next question, , Respiratory physiology: lung compliance, Lung compliance is defined as change in lung volume per unit change in airway pressure, Causes of increased compliance, , , , age, emphysema - this is due to loss alveolar walls and associated elastic tissue, , Causes of decreased compliance, , , , , , pulmonary oedema, pulmonary fibrosis, pneumonectomy, kyphosis, Next question
Page 305 :
Which of the following areas is predominantly concerned with thermoregulation?, , Hypothalamus, , Anterior pituitary, , Cerebellum, , Brain stem, , Temporal lobe, , Theme from 2012 Exam, The hypothalamus is primarily concerned with thermoregulation. It may relay to the cerebral cortex, to induce behavioural adaptation to facilitate the thermoregulatory process., Please rate this question:, , Discuss and give feedback, , Next question, , Thermoregulation, , , , , , , , The hypothalamus is the main centre for thermoregulation. Peripheral and central, thermoreceptors relay to this region., Central thermoreceptors play the main role in maintenance of core temperature., Hypothalamus may initiate involuntary motor responses to raise body temperature, (e.g.shivering). It will also stimulate the sympathetic nervous system to produce peripheral, vasoconstriction and release of adrenaline from the adrenal medulla., Heat loss is governed by behavioural responses and by autonomic responses including, peripheral vasodilation., Heat loss can be maintained within the thermoneutral zone (25 to 30 degrees) although the, absolute value depends upon atmospheric humidity., Sepsis results in the release of cytokines that reset the thermoregulatory centre resulting in, fever., Next question
Page 306 :
Theme: Acid - base disorders, , A., B., C., D., E., , pH 7.64 pO2 10.0 kPa pCO2 2.8 kPa HCO3 20, pH 7.25 pO2 8.9 pCO2 3.2 HCO3 10, pH 7.20 pO2 6.2 pCO2 8.2 HCO3 27, pH 7.60 pO2 8.2 pCO2 5.8 HCO3 40, pH 7.45 pO2 7.2 pCO2 2.5 HCO3 24, , Please match the diagnosis with the arterial blood gas result. Each option may be used once, more, than once or not at all., , 89., , Pulmonary embolus, You answered pH 7.64 pO2 10.0 kPa pCO2 2.8 kPa HCO3 20, The correct answer is pH 7.45 pO2 7.2 pCO2 2.5 HCO3 24, A combination of hypoxia and respiratory alkalosis should suggest a pulmonary embolus., The respiratory alkalosis is due to hyperventilation associated with the pulmonary, embolism., , 90., , High output ureterosigmoidostomy, You answered pH 7.64 pO2 10.0 kPa pCO2 2.8 kPa HCO3 20, The correct answer is pH 7.25 pO2 8.9 pCO2 3.2 HCO3 10, There is acidosis. To compensate the patient will attempt to raise the pH level in the blood, by hyperventilating, hence the low CO2 level ., , 91., , Widespread mesenteric infarction, You answered pH 7.64 pO2 10.0 kPa pCO2 2.8 kPa HCO3 20, The correct answer is pH 7.25 pO2 8.9 pCO2 3.2 HCO3 10, This is usually associated with acidosis, hyperventillation and reduction in bicarbonate., , Please rate this question:, , Discuss and give feedback, , Next question
Page 307 :
Disorders of acid - base balance, Disorders of acid- base balance are often covered in the MRCS part A, both in the SBA and EMQ, sections., The acid-base normogram below shows how the various disorders may be categorised, , Image sourced from Wikipedia, , Metabolic acidosis, , , , , This is the most common surgical acid - base disorder., Reduction in plasma bicarbonate levels., Two mechanisms:, , 1. Gain of strong acid (e.g. diabetic ketoacidosis), 2. Loss of base (e.g. from bowel in diarrhoea), - Classified according to the anion gap, this can be calculated by:, (Na+ + K+) - (Cl- + HCO3-)., - If a question supplies the chloride level then this is often a clue that the anion gap should be, calculated. The normal range = 10-18 mmol/L, Normal anion gap ( = hyperchloraemic metabolic acidosis), , , Gastrointestinal bicarbonate loss: diarrhoea, ureterosigmoidostomy, fistula
Page 308 :
, , , , , Renal tubular acidosis, Drugs: e.g. acetazolamide, Ammonium chloride injection, Addison's disease, , Raised anion gap, , , , , , Lactate: shock, hypoxia, Ketones: diabetic ketoacidosis, alcohol, Urate: renal failure, Acid poisoning: salicylates, methanol, , Metabolic acidosis secondary to high lactate levels may be subdivided into two types:, , , , Lactic acidosis type A: (Perfusion disorders e.g.shock, hypoxia, burns), Lactic acidosis type B: (Metabolic e.g. metformin toxicity), , Metabolic alkalosis, , , , , Usually caused by a rise in plasma bicarbonate levels., Rise of bicarbonate above 24 mmol/L will typically result in renal excretion of excess, bicarbonate., Caused by a loss of hydrogen ions or a gain of bicarbonate. It is due mainly to problems of, the kidney or gastrointestinal tract, , Causes, , , , , , , , , , Vomiting / aspiration (e.g. Peptic ulcer leading to pyloric stenosis, nasogastric suction), Diuretics, Liquorice, carbenoxolone, Hypokalaemia, Primary hyperaldosteronism, Cushing's syndrome, Bartter's syndrome, Congenital adrenal hyperplasia, , Mechanism of metabolic alkalosis
Page 309 :
, , , , , Activation of renin-angiotensin II-aldosterone (RAA) system is a key factor, Aldosterone causes reabsorption of Na+ in exchange for H+ in the distal convoluted tubule, ECF depletion (vomiting, diuretics) → Na+ and Cl- loss → activation of RAA system → raised, aldosterone levels, In hypokalaemia, K+ shift from cells → ECF, alkalosis is caused by shift of H + into cells to, maintain neutrality, , Respiratory acidosis, , , , Rise in carbon dioxide levels usually as a result of alveolar hypoventilation, Renal compensation may occur leading to Compensated respiratory acidosis, , Causes, , , , , COPD, Decompensation in other respiratory conditions e.g. Life-threatening asthma / pulmonary, oedema, Sedative drugs: benzodiazepines, opiate overdose, , Respiratory alkalosis, , , , Hyperventilation resulting in excess loss of carbon dioxide, This will result in increasing pH, , Causes, , , , , , , Psychogenic: anxiety leading to hyperventilation, Hypoxia causing a subsequent hyperventilation: pulmonary embolism, high altitude, Early salicylate poisoning*, CNS stimulation: stroke, subarachnoid haemorrhage, encephalitis, Pregnancy, , *Salicylate overdose leads to a mixed respiratory alkalosis and metabolic acidosis. Early stimulation, of the respiratory centre leads to a respiratory alkalosis whilst later the direct acid effects of, salicylates (combined with acute renal failure) may lead to an acidosis, Next question
Page 310 :
A 45 year old male is diagnosed with carcinoma of the head of the pancreas. He reports that his, stool sticks to the commode and will not flush away. Loss of which of the following enzymes is most, likely to be responsible for this problem?, , Lipase, , Amylase, , Trypsin, , Elastase, , None of the above, , Theme from April 2014 Exam, Loss of lipase is one of the key features in the development of steatorrhoea which typically consists, of pale and offensive stools that are difficult to flush away., Please rate this question:, , Discuss and give feedback, , Next question, , Pancreatic cancer, , , , , , , Adenocarcinoma, Risk factors: Smoking, diabetes, adenoma, familial adenomatous polyposis, Mainly occur in the head of the pancreas (70%), Spread locally and metastasizes to the liver, Carcinoma of the pancreas should be differentiated from other periampullary tumours with, better prognosis, , Clinical features, , , , , , , Weight loss, Painless jaundice, Epigastric discomfort (pain usually due to invasion of the coeliac plexus is a late feature), Pancreatitis, Trousseau's sign: migratory superficial thrombophlebitis
Page 311 :
Investigations, , , , , , , USS: May miss small lesions, CT Scanning (pancreatic protocol). If unresectable on CT then no further staging needed, PET/CT for those with operable disease on CT alone, ERCP/ MRI for bile duct assessment, Staging laparoscopy to exclude peritoneal disease, , Management, , , , , , , Head of pancreas: Whipple's resection (SE dumping and ulcers). Newer techniques include, pylorus preservation and SMA/ SMV resection, Carcinoma body and tail: poor prognosis, distal pancreatectomy, if operable, Usually adjuvent chemotherapy for resectable disease, ERCP and stent for jaundice and palliation, Surgical bypass may be needed for duodenal obstruction, , Next question
Page 312 :
Which of the following drugs does not interfere with the laboratory analysis of serum cortisol levels?, , Dexamethasone, , Prednisolone, , Hydrocortisone IV, , Hydrocortisone PO, , Hydrocortisone IM, Prednisolone and it's metabolites can chemically mimic cortisol in radio-immunoassay techniques of, laboratory analysis., Dexamethasone can be given as glucorticoid replacement during testing for addisons or adrenal, insufficiency as it does not interfere with cortisol levels. For example, if you have a patient with, polymyalgia rheumatica and they are on long term prednisolone, you can replace the prednisolone, with dexamethasone to undertake a short synacthen test., Please rate this question:, , Discuss and give feedback, , Next question, , Cortisol, , , , , , , Glucocorticoid, Released by zona fasiculata of the adrenal gland, 90% protein bound; 10% active, Circadian rhythm: High in the mornings, Negative feedback via ACTH, , Actions, , , , , , , , Glycogenolysis, Gluconeogenesis, Protein catabolism, Lipolysis, Stress response, Anti-inflammatory
Page 313 :
, , , , , Decrease protein in bones, Increase gastric acid, Increases neutrophils/platelets/red blood cells, Inhibits fibroblastic activity, , Next question
Page 314 :
An elderly lady who presented with weight loss and malabsorption was found to have amyloid of the, small bowel. On presentation she was found to have osteomalacia and was hypocalcaemic. Over, the past seven days she has received total parenteral nutrition with adequate calcium replacement., Despite this she remained hypocalcaemic. Deficiency of which of the following electrolytes is most, likely to account for this process?, , Magnesium, , Potassium, , Sodium, , Phosphate, , None of the above, , Theme from September 2015 Exam, Patients with malabsorption may develop magnesium deficiency, although her TPN feeds may have, contained magnesium it may not have been sufficient to correct her losses. Sodium, phosphate and, potassium would not have this effect on serum calcium., Please rate this question:, , Discuss and give feedback, , Next question, , Combined deficiency of magnesium and calcium, Magnesium is required for both PTH secretion and its action on target tissues. Hypomagnesaemia, may both cause hypocalcaemia and render patients unresponsive to treatment with calcium and, vitamin D supplementation., Magnesium is the fourth most abundant cation in the body. The body contains 1000mmol, with half, contained in bone and the remainder in muscle, soft tissues and extracellular fluid. There is no one
Page 315 :
specific hormonal control of magnesium and various hormones including PTH and aldosterone affect, the renal handling of magnesium., Magnesium and calcium interact at a cellular level also and as a result decreased magnesium will, tend to affect the permeability of cellular membranes to calcium, resulting in hyperexcitability., Next question
Page 316 :
A 19 year old man is attacked outside a club and beaten with a baseball bat. He sustains a blow to, the right side of his head. He is brought to the emergency department and a policy of observation is, adopted. His glasgow coma score deteriorates and he becomes comatose. Which of the following, haemodynamic parameters is most likely to be present?, , Hypertension and bradycardia, , Hypotension and tachycardia, , Hypotension and bradycardia, , Hypertension and tachycardia, , Normotension and bradycardia, , Theme from April 2013 Exam, Hypertension and bradycardia are seen prior to coning. The brain autoregulates its blood supply by, controlling systemic blood pressure., Please rate this question:, , Discuss and give feedback, , Next question, , Head injury, Patients who suffer head injuries should be managed according to ATLS principles and extra cranial, injuries should be managed alongside cranial trauma. Inadequate cardiac output will compromise, CNS perfusion irrespective of the nature of the cranial injury., Types of traumatic brain injury, Bleeding into the space between the dura mater and the skull. Often results from, acceleration-deceleration trauma or a blow to the side of the head. The majority, of extradural haematomas occur in the temporal region where skull fractures, cause a rupture of the middle meningeal artery., Extradural, haematoma, , Features, , , , , Raised intracranial pressure, Some patients may exhibit a lucid interval
Page 317 :
Bleeding into the outermost meningeal layer. Most commonly occur around the, frontal and parietal lobes. May be either acute or chronic., Subdural, haematoma, , Risk factors include old age and alcoholism., Slower onset of symptoms than a extradural haematoma., , Subarachnoid, haemorrhage, , Usually occurs spontaneously in the context of a ruptured cerebral aneurysm, but, may be seen in association with other injuries when a patient has sustained a, traumatic brain injury., , Pathophysiology, , , , , , , , Primary brain injury may be focal (contusion/ haematoma) or diffuse (diffuse axonal injury), Diffuse axonal injury occurs as a result of mechanical shearing following deceleration,, causing disruption and tearing of axons, Intra-cranial haematomas can be extradural, subdural or intracerebral, while contusions may, occur adjacent to (coup) or contralateral (contre-coup) to the side of impact, Secondary brain injury occurs when cerebral oedema, ischaemia, infection, tonsillar or, tentorial herniation exacerbates the original injury. The normal cerebral auto regulatory, processes are disrupted following trauma rendering the brain more susceptible to blood flow, changes and hypoxia, The Cushings reflex (hypertension and bradycardia) often occurs late and is usually a pre, terminal event, , Management, , , , , , , , , , , Where there is life threatening rising ICP such as in extra dural haematoma and whilst, theatre is prepared or transfer arranged use of IV mannitol/ frusemide may be required., Diffuse cerebral oedema may require decompressive craniotomy, Exploratory Burr Holes have little management in modern practice except where scanning, may be unavailable and to thus facilitate creation of formal craniotomy flap, Depressed skull fractures that are open require formal surgical reduction and debridement,, closed injuries may be managed non operatively if there is minimal displacement., ICP monitoring is appropriate in those who have GCS 3-8 and normal CT scan., ICP monitoring is mandatory in those who have GCS 3-8 and abnormal CT scan., Hyponatraemia is most likely to be due to syndrome of inappropriate ADH secretion., Minimum of cerebral perfusion pressure of 70mmHg in adults., Minimum cerebral perfusion pressure of between 40 and 70 mmHg in children., , Interpretation of pupillary findings in head injuries, , Pupil size, , Light response, , Interpretation
Page 318 :
Pupil size, , Light response, , Interpretation, , Unilaterally dilated, , Sluggish or fixed, , 3rd nerve compression secondary to tentorial, herniation, , Bilaterally dilated, , Sluggish or fixed, , Unilaterally dilated or, equal, , Cross reactive (Marcus Gunn), , Bilaterally constricted, , May be difficult to, assess, , Unilaterally, constricted, , Preserved, , , , , Poor CNS perfusion, Bilateral 3rd nerve palsy, , Optic nerve injury, , , , , Opiates, Pontine lesions, Metabolic encephalopathy, , Sympathetic pathway disruption, Next question
Page 319 :
Which of the following drugs does not cause pseudohaematuria?, , Rifampicin, , Quinine, , Noradrenaline, , Levodopa, , Phenytoin, , Rifampicin, phenytoin, levodopa, methyldopa, and quinine all cause pseudohaematuria., Please rate this question:, , Discuss and give feedback, , Next question, , Haematuria, Causes of haematuria, , Trauma, , , , , , , Injury to renal tract, Renal trauma commonly due to blunt injury (others penetrating, injuries), Ureter trauma rare: iatrogenic, Bladder trauma: due to RTA or pelvic fractures, , Infection, , , , Remember TB, , Malignancy, , , , Renal cell carcinoma (remember paraneoplastic syndromes):, painful or painless, Urothelial malignancies: 90% are transitional cell carcinoma, can, occur anywhere along the urinary tract. Painless haematuria., Squamous cell carcinoma and adenocarcinoma: rare bladder, tumours, Prostate cancer, , , ,
Page 321 :
A 74-year-old woman with thyroid cancer is admitted due to shortness of breath. What is the best, investigation to assess for possible compression of the upper airways?, , Arterial blood gases, , Forced vital capacity, , Transfer factor, , Peak expiratory flow rate, , Flow volume loop, , Flow volume loop is the investigation of choice for upper airway compression., Please rate this question:, , Discuss and give feedback, , Next question, , Flow volume loop, A normal flow volume loop is often described as a 'triangle on top of a semi circle', Flow volume loops are the most suitable way of assessing compression of the upper airway, Next question
Page 322 :
Which of the following statements relating to cerebrospinal fluid is untrue?, , The choroid plexus is only present in the lateral ventricles, , Total CSF volume is 100-150ml, , CSF pressure is usually 10-15mmHg, , The cerebral aqueduct connects the third and fourth ventricles, , The foramen of Luschka are paired and lie laterally in the fourth ventricle, , The choroid plexus lies in all ventricles., Please rate this question:, , Discuss and give feedback, , Next question, , Cerebrospinal fluid, The CSF fills the space between the arachnoid mater and pia mater (covering surface of the brain)., The total volume of CSF in the brain is approximately 150ml. Approximately 500 ml is produced by, the ependymal cells in the choroid plexus (70%), or blood vessels (30%). It is reabsorbed via the, arachnoid granulations which project into the venous sinuses., Circulation, 1. Lateral ventricles (via foramen of Munro), 2. 3rd ventricle, 3. Cerebral aqueduct (aqueduct of Sylvius), 4. 4th ventricle (via foramina of Magendie and Luschka), 5. Subarachnoid space, 6. Reabsorbed into the venous system via arachnoid granulations into superior sagittal sinus, Composition, , , , , , Glucose: 50-80mg/dl, Protein: 15-40 mg/dl, Red blood cells: Nil, White blood cells: 0-3 cells/ mm3, Next question
Page 323 :
Which substance can be used to achieve the most accurate measurement of the glomerular filtration, rate?, , Glucose, , Protein, , Inulin, , Creatinine, , Para-amino hippuric acid, , Theme from April 2016 exam, Creatinine declines with age due to decline in renal function and muscle mass. Glucose, protein, (amino acids) and PAH are reabsorbed by the kidney., Please rate this question:, , Discuss and give feedback, , Next question, , Renal Physiology, Overview, , , , , Each nephron is supplied with blood from an afferent arteriole that opens onto the glomerular, capillary bed., Blood then flows to an efferent arteriole, supplying the peritubular capillaries and medullary, vasa recta., The kidney receives up to 25% of resting cardiac output., , Control of blood flow, , , , The kidney is able to autoregulate its blood flow between systolic pressures of 80- 180mmHg, so there is little variation in renal blood flow., This is achieved by myogenic control of arteriolar tone, both sympathetic input and hormonal, signals (e.g. renin) are responsible.
Page 324 :
Glomerular structure and function, , , , , , , , , Blood inside the glomerulus has considerable hydrostatic pressure., The basement membrane has pores that will allow free diffusion of smaller solutes, larger, negatively charged molecules such as albumin are unable to cross., The glomerular filtration rate (GFR) is equal to the concentration of a solute in the urine,, times the volume of urine produced per minute, divided by the plasma concentration, (assuming that the solute is freely diffused e.g. inulin)., In clinical practice creatinine is used because it is subjected to very little proximal tubular, secretion., Although subject to variability, the typical GFR is 125ml per minute., Glomerular filtration rate = Total volume of plasma per unit time leaving the capillaries and, entering the bowman's capsule, Renal clearance = volume plasma from which a substance is removed per minute by the, kidneys, , Substances used to measure GFR have the following features:, 1. Inert, 2. Free filtration from the plasma at the glomerulus (not protein bound), 3. Not absorbed or secreted at the tubules, 4. Plasma concentration constant during urine collection, Examples: inulin, creatinine, GFR = urine concentration (mmol/l) x urine volume (ml/min), -------------------------------------------------------------------------plasma concentration (mmol/l), , , , , The clearance of a substance is dependent not only on its diffusivity across the basement, membrane but also subsequent tubular secretion and / or reabsorption., So glucose which is freely filtered across the basement membrane is usually reabsorbed, from tubules giving a clearance of zero., , Tubular function, , , , , , , Reabsorption and secretion of substances occurs in the tubules., In the proximal tubule substrates such as glucose, amino acids and phosphate are cotransported with sodium across the semi permeable membrane., Up to two thirds of filtered water is reabsorbed in the proximal tubules., This will lead to increase in urea concentration in the distal tubule allowing for its increased, diffusion., Substances to be secreted into the tubules are taken up from the peritubular blood by tubular, cells.
Page 325 :
, , , Solutes such as paraaminohippuric acid are cleared with a single passage through the, kidneys and this is why it is used to measure renal plasma flow. Ions such as calcium and, phosphate will have a tubular reabsorption that is influenced by plasma PTH levels., Potassium may be both secreted and re-absorbed and is co-exchanged with sodium., , Loop of Henle, , , , , , , , , , Approximately 60 litres of water containing 9000mmol sodium enters the descending limb of, the loop of Henle in 24 hours., Loops from the juxtamedullary nephrons run deep into the medulla., The osmolarity of fluid changes and is greatest at the tip of the papilla., The thin ascending limb is impermeable to water, but highly permeable to sodium and, chloride ions., This loss means that at the beginning of the thick ascending limb the fluid is hypo osmotic, compared with adjacent interstitial fluid., In the thick ascending limb the reabsorption of sodium and chloride ions occurs by both, facilitated and passive diffusion pathways., The loops of Henle are co-located with vasa recta, these will have similar solute, compositions to the surrounding extracellular fluid so preventing the diffusion and, subsequent removal of this hypertonic fluid., The energy dependent reabsorption of sodium and chloride in the thick ascending limb helps, to maintain this osmotic gradient., , Next question
Page 326 :
A 45 year old man sustains a closed head injury. He is initially alert, however, his level of, consciousness deteriorates on arrival at hospital. An intra cranial pressure monitor is inserted. What, is the normal intracranial pressure?, , 35 - 45mm Hg, , 45 - 55mm Hg, , <15mm Hg, , 25 - 35mm Hg, , 25 - 30 mm Hg, , The normal intracranial pressure is between 7 and 15 mm Hg. The brain can accommodate, increases up to 24 mm Hg, thereafter clinical features will become evident., Please rate this question:, , Discuss and give feedback, , Next question, , Applied neurophysiology, , , , , , , Pressure within the cranium is governed by the Monroe-Kelly doctrine. This considers the, skull as a closed box. Increases in mass can be accommodated by loss of CSF. Once a, critical point is reached (usually 100- 120ml of CSF lost) there can be no further, compensation and ICP rises sharply. The next step is that pressure will begin to equate with, MAP and neuronal death will occur. Herniation will also accompany this process., The CNS can autoregulate its own blood supply. Vaso constriction and dilatation of the, cerebral blood vessels is the primary method by which this occurs. Extremes of blood, pressure can exceed this capacity resulting in risk of stroke. Other metabolic factors such as, hypercapnia will also cause vasodilation, which is of importance in ventilating head injured, patients., The brain can only metabolise glucose, when glucose levels fall, consciousness will be, impaired., Next question
Page 327 :
A 55-year-old man with a history of type 2 diabetes mellitus, bipolar disorder and chronic obstructive, pulmonary disease has bloods taken during a pre operative assessment of an inguinal hernia repair:, Na+, , 125 mmol/l, , K+, , 3.8 mmol/l, , Bicarbonate, , 24 mmol/l, , Urea, , 3.7 mmol/l, , Creatinine, , 92 µmol/l, , Due to his smoking history a chest x-ray is ordered which is reported as normal. The Consultant, asks you what is the most likely cause for the hyponatraemia?, , Metformin, , Lithium, , Carbamazepine, , Sodium valproate, , Pioglitazone, SIADH - drug causes: carbamazepine, sulfonylureas, SSRIs, tricyclics, Lithium can cause diabetes insipidus but this is generally associated with a high sodium. Lithium, only tends to cause raised antidiuretic hormone levels following a severe overdosage., Please rate this question:, , Discuss and give feedback, , Next question, , syndrome of inappropriate antidiuretic hormone (SIADH): causes, Malignancy, , , especially small cell lung cancer
Page 329 :
A 24 year old man is involved in a road traffic accident. His right leg is trapped for 6 hours whilst he, is moved. On examination his foot is insensate and a dorsalis pedis pulse is only weakly felt. Which, of the biochemical abnormalities listed below is most likely to be present?, , Alkalosis, , Hypercalcaemia, , Hypocalcaemia, , Hyperkalaemia, , Hyponatraemia, , In this scenario the patient will have a compartment syndrome, delayed diagnosis and muscle death., The effect of muscle death will result in the release of potassium. It is also highly likely that there will, be a degree of renal impairment, the result of which is that the serum potassium is likely to be high., Please rate this question:, , Discuss and give feedback, , Next question, , Hyperkalaemia, , , , , Plasma potassium levels are regulated by a number of factors including aldosterone, acidbase balance and insulin levels., Metabolic acidosis is associated with hyperkalaemia as hydrogen and potassium ions, compete with each other for exchange with sodium ions across cell membranes and in the, distal tubule., ECG changes seen in hyperkalaemia include tall-tented T waves, small P waves, widened, QRS leading to a sinusoidal pattern and asystole, , Causes of hyperkalaemia, , , , , , , Acute renal failure, Drugs*: potassium sparing diuretics, ACE inhibitors, angiotensin 2 receptor blockers,, spironolactone, ciclosporin, heparin**, Metabolic acidosis, Addison's, Tissue necrosis/rhabdomylosis: burns, trauma
Page 330 :
, , Massive blood transfusion, , Foods that are high in potassium, , , , Salt substitutes (i.e. Contain potassium rather than sodium), Bananas, oranges, kiwi fruit, avocado, spinach, tomatoes, , *beta-blockers interfere with potassium transport into cells and can potentially cause hyperkalaemia, in renal failure patients - remember beta-agonists, e.g. Salbutamol, are sometimes used as, emergency treatment, **both unfractionated and low-molecular weight heparin can cause hyperkalaemia. This is thought to, be caused by inhibition of aldosterone secretion, Next question
Page 331 :
A 39 year old lady has recurrent attacks of biliary colic. What is the approximate volume of bile to, enter the duodenum per 24 hours?, , 500 mL, , 50 mL, , 100 mL, , 2000 mL, , 150 mL, , Between 500 mL and 1.5 L of bile enters the small bowel daily. Most bile salts are recycled by the, enterohepatic circulation. When the gallbladder contracts the lumenal pressure is approximately, 25cm water, which is why biliary colic may be so painful., Please rate this question:, , Discuss and give feedback, , Next question, , Bile, Bile is produced at a rate of between 500ml and 1500mL per day. Bile is composed of bile salts,, bicarbonate, cholesterol, steroids and water. There are three main factors regulating bile flow;, hepatic secretion, gall bladder contraction and sphincter of oddi resistance. Bile salts are absorbed, in the terminal ileum (and recycled to the liver). Over 90% of all bile salts are recycled in this way,, such that the total pool of bile salts is recycled up to six times a day., Primary bile salts, Cholate and chenodeoxycholate., Secondary bile salts
Page 332 :
Formed by bacterial action on primary bile salts. These are deoxycholate and lithocholate. Of these, deoxycholate is reabsorbed, whilst lithocholate is insoluble and excreted., Pathophysiology of gallstones, Bile salts have a detergent action. They aggregate to form micelles and these have a lipid centre in, which fats may be transported. Excessive quantities of cholesterol cannot be transported in this way, and will tend to precipitate, resulting in the formation of cholesterol rich gallstones., Next question
Page 333 :
At which of the following sites is the most water absorbed?, , Right colon, , Left colon, , Stomach, , Jejunum, , Duodenum, , Water absorption in the gastrointestinal tract predominantly occurs in the small bowel (jejunum and, ileum). The colon is an important site of water absorption, however, its overall contribution is, relatively small. The importance of the colonic component to water absorption may increase, following extensive small bowel resections., Please rate this question:, , Discuss and give feedback, , Next question, , Water absorption, During a 24 hours period the average person will ingest up to 2000ml of liquid orally. In addition a, further 8000ml of fluid will enter the small bowel as gastrointestinal secretions. Intestinal water, absorption is a passive process and is related to solute load. In the jejunum the active absorption of, glucose and amino acids will create a concentration gradient that water will flow across. In the ileum, most water is absorbed by a process of facilitated diffusion (with sodium)., Approximately 150ml of water enters the colon daily, most is absorbed, the colon can adapt to, and, increase this amount following resection., Next question
Page 334 :
Which of the following is not a characteristic of the proximal convoluted tubule in the kidney?, , Up to 95% of filtered amino acids will be reabsorbed at this site, , It is a risk of damage in a patient with compartment syndrome due to a tibial fracture, , It is responsible for absorbing more than 50% of filtered water, , Its secretory function is most effective at low systolic blood pressures (typically less than, 100mmHg), Glucose is reabsorbed by a process of facilitated diffusion, , The proximal convoluted tubule may undergo necrosis in situations such as compartment syndrome., It is responsible for reabsorbing up to two thirds of filtered water. Low systolic blood pressures, (below the renal autoregulatory range) are a risk factor for acute tubular necrosis. Within the, autoregulatory range the absolute value of systolic BP has little effect., Please rate this question:, , Discuss and give feedback, , Next question, , Renal Physiology, Overview, , , , , Each nephron is supplied with blood from an afferent arteriole that opens onto the glomerular, capillary bed., Blood then flows to an efferent arteriole, supplying the peritubular capillaries and medullary, vasa recta., The kidney receives up to 25% of resting cardiac output., , Control of blood flow, , , , The kidney is able to autoregulate its blood flow between systolic pressures of 80- 180mmHg, so there is little variation in renal blood flow., This is achieved by myogenic control of arteriolar tone, both sympathetic input and hormonal, signals (e.g. renin) are responsible.
Page 335 :
Glomerular structure and function, , , , , , , , , Blood inside the glomerulus has considerable hydrostatic pressure., The basement membrane has pores that will allow free diffusion of smaller solutes, larger, negatively charged molecules such as albumin are unable to cross., The glomerular filtration rate (GFR) is equal to the concentration of a solute in the urine,, times the volume of urine produced per minute, divided by the plasma concentration, (assuming that the solute is freely diffused e.g. inulin)., In clinical practice creatinine is used because it is subjected to very little proximal tubular, secretion., Although subject to variability, the typical GFR is 125ml per minute., Glomerular filtration rate = Total volume of plasma per unit time leaving the capillaries and, entering the bowman's capsule, Renal clearance = volume plasma from which a substance is removed per minute by the, kidneys, , Substances used to measure GFR have the following features:, 1. Inert, 2. Free filtration from the plasma at the glomerulus (not protein bound), 3. Not absorbed or secreted at the tubules, 4. Plasma concentration constant during urine collection, Examples: inulin, creatinine, GFR = urine concentration (mmol/l) x urine volume (ml/min), -------------------------------------------------------------------------plasma concentration (mmol/l), , , , , The clearance of a substance is dependent not only on its diffusivity across the basement, membrane but also subsequent tubular secretion and / or reabsorption., So glucose which is freely filtered across the basement membrane is usually reabsorbed, from tubules giving a clearance of zero., , Tubular function, , , , , , , Reabsorption and secretion of substances occurs in the tubules., In the proximal tubule substrates such as glucose, amino acids and phosphate are cotransported with sodium across the semi permeable membrane., Up to two thirds of filtered water is reabsorbed in the proximal tubules., This will lead to increase in urea concentration in the distal tubule allowing for its increased, diffusion., Substances to be secreted into the tubules are taken up from the peritubular blood by tubular, cells.
Page 336 :
, , , Solutes such as paraaminohippuric acid are cleared with a single passage through the, kidneys and this is why it is used to measure renal plasma flow. Ions such as calcium and, phosphate will have a tubular reabsorption that is influenced by plasma PTH levels., Potassium may be both secreted and re-absorbed and is co-exchanged with sodium., , Loop of Henle, , , , , , , , , , Approximately 60 litres of water containing 9000mmol sodium enters the descending limb of, the loop of Henle in 24 hours., Loops from the juxtamedullary nephrons run deep into the medulla., The osmolarity of fluid changes and is greatest at the tip of the papilla., The thin ascending limb is impermeable to water, but highly permeable to sodium and, chloride ions., This loss means that at the beginning of the thick ascending limb the fluid is hypo osmotic, compared with adjacent interstitial fluid., In the thick ascending limb the reabsorption of sodium and chloride ions occurs by both, facilitated and passive diffusion pathways., The loops of Henle are co-located with vasa recta, these will have similar solute, compositions to the surrounding extracellular fluid so preventing the diffusion and, subsequent removal of this hypertonic fluid., The energy dependent reabsorption of sodium and chloride in the thick ascending limb helps, to maintain this osmotic gradient., , Next question
Page 337 :
An arterial blood gas sample is taken and the following results obtained;, PaO2, , 8kPa, , PaCO2, , 4kPa, , pH, , 7.4, , With which of the following are these values most consistent?, , Compensated metabolic alkalosis, , Pulmonary atelectasis, , Alveolar hypoventilation, , Residing at 4500M for 48 hours, , LAD occlusion, , The patient has low oxygen tension and low carbon dioxide. The pH is normal so there is, compensation for a long standing condition in which oxygenation is reduced. There is neither, alkalosis, nor hypoventilation as the carbon dioxide is low. At very high altitude, the low oxygen, tension can exceed the anaerobic threshold and carbon dioxide levels increase., Please rate this question:, , Discuss and give feedback, , Next question, , Arterial blood gas interpretation
Page 338 :
In advanced life support training, a 5 step approach to arterial blood gas interpretation is advocated., 1. How is the patient?, 2. Is the patient hypoxaemic?, The Pa02 on air should be 10.0-13.0 kPa, 3. Is the patient acidaemic (pH <7.35) or alkalaemic (pH >7.45), 4. What has happened to the PaCO2?, If there is acidaemia, an elevated PaCO2 will account for this, 5. What is the bicarbonate level or base excess?, A metabolic acidosis will have a low bicarbonate level and a low base excess (< -2 mmol), A metabolic alkalosis will have a high bicarbonate and a high base excess (> +2 mmol), , Next question
Page 339 :
Which of the following does not cause a normal anion gap acidosis?, , Pancreatic fistula, , Acetazolamide, , Uraemia, , Ureteric diversion, , Renal tubular acidosis, Normal Gap Acidosis: HARDUP, H - Hyperalimentation/hyperventilation, A - Acetazolamide, R - Renal tubular acidosis, D - Diarrhoea, U - Ureteral diversion, P - Pancreatic fistula/parenteral saline, Uraemia will typically cause a high anion gap acidosis. It is one of the unmeasured anions., Please rate this question:, , Discuss and give feedback, , Next question, , Disorders of acid - base balance, Disorders of acid- base balance are often covered in the MRCS part A, both in the SBA and EMQ, sections., The acid-base normogram below shows how the various disorders may be categorised
Page 340 :
Image sourced from Wikipedia, , Metabolic acidosis, , , , , This is the most common surgical acid - base disorder., Reduction in plasma bicarbonate levels., Two mechanisms:, , 1. Gain of strong acid (e.g. diabetic ketoacidosis), 2. Loss of base (e.g. from bowel in diarrhoea), - Classified according to the anion gap, this can be calculated by:, (Na+ + K+) - (Cl- + HCO3-)., - If a question supplies the chloride level then this is often a clue that the anion gap should be, calculated. The normal range = 10-18 mmol/L, Normal anion gap ( = hyperchloraemic metabolic acidosis), , , , , , , Gastrointestinal bicarbonate loss: diarrhoea, ureterosigmoidostomy, fistula, Renal tubular acidosis, Drugs: e.g. acetazolamide, Ammonium chloride injection, Addison's disease, , Raised anion gap
Page 341 :
, , , , , Lactate: shock, hypoxia, Ketones: diabetic ketoacidosis, alcohol, Urate: renal failure, Acid poisoning: salicylates, methanol, , Metabolic acidosis secondary to high lactate levels may be subdivided into two types:, , , , Lactic acidosis type A: (Perfusion disorders e.g.shock, hypoxia, burns), Lactic acidosis type B: (Metabolic e.g. metformin toxicity), , Metabolic alkalosis, , , , , Usually caused by a rise in plasma bicarbonate levels., Rise of bicarbonate above 24 mmol/L will typically result in renal excretion of excess, bicarbonate., Caused by a loss of hydrogen ions or a gain of bicarbonate. It is due mainly to problems of, the kidney or gastrointestinal tract, , Causes, , , , , , , , , , Vomiting / aspiration (e.g. Peptic ulcer leading to pyloric stenosis, nasogastric suction), Diuretics, Liquorice, carbenoxolone, Hypokalaemia, Primary hyperaldosteronism, Cushing's syndrome, Bartter's syndrome, Congenital adrenal hyperplasia, , Mechanism of metabolic alkalosis, , , , , , Activation of renin-angiotensin II-aldosterone (RAA) system is a key factor, Aldosterone causes reabsorption of Na+ in exchange for H+ in the distal convoluted tubule, ECF depletion (vomiting, diuretics) → Na+ and Cl- loss → activation of RAA system → raised, aldosterone levels, In hypokalaemia, K+ shift from cells → ECF, alkalosis is caused by shift of H + into cells to, maintain neutrality
Page 342 :
Respiratory acidosis, , , , Rise in carbon dioxide levels usually as a result of alveolar hypoventilation, Renal compensation may occur leading to Compensated respiratory acidosis, , Causes, , , , , COPD, Decompensation in other respiratory conditions e.g. Life-threatening asthma / pulmonary, oedema, Sedative drugs: benzodiazepines, opiate overdose, , Respiratory alkalosis, , , , Hyperventilation resulting in excess loss of carbon dioxide, This will result in increasing pH, , Causes, , , , , , , Psychogenic: anxiety leading to hyperventilation, Hypoxia causing a subsequent hyperventilation: pulmonary embolism, high altitude, Early salicylate poisoning*, CNS stimulation: stroke, subarachnoid haemorrhage, encephalitis, Pregnancy, , *Salicylate overdose leads to a mixed respiratory alkalosis and metabolic acidosis. Early stimulation, of the respiratory centre leads to a respiratory alkalosis whilst later the direct acid effects of, salicylates (combined with acute renal failure) may lead to an acidosis, Next question
Page 343 :
Which one of the following would cause a rise in the carbon monoxide transfer factor (TLCO)?, , Emphysema, , Pulmonary embolism, , Pulmonary haemorrhage, , Pneumonia, , Pulmonary fibrosis, Transfer factor, , , , raised: asthma, haemorrhage, left-to-right shunts, polycythaemia, low: everything else, , Where alveolar haemorrhage occurs the TLCO tends to increase due to the enhanced uptake of, carbon monoxide by intra-alveolar haemoglobin., Please rate this question:, , Discuss and give feedback, , Next question, , Transfer factor, The transfer factor describes the rate at which a gas will diffuse from alveoli into blood. Carbon, monoxide is used to test the rate of diffusion. Results may be given as the total gas transfer (TLCO), or that corrected for lung volume (transfer coefficient, KCO), , Causes of a raised TLCO, , , , , , , asthma, pulmonary haemorrhage (Wegener's, Goodpasture's), left-to-right cardiac shunts, polycythaemia, hyperkinetic states, , Causes of a lower TLCO, , , , , , , pulmonary fibrosis, pneumonia, pulmonary emboli, pulmonary oedema, emphysema
Page 345 :
Which of the following is least likely to be associated with hypercalcaemia?, , Thiazides, , Antacids, , Coeliac disease, , Sarcoidosis, , Zolinger-Ellison syndrome, Mnemonic for the causes of hypercalcaemia:, CHIMPANZEES, C alcium supplementation, H yperparathyroidism, I atrogentic (Drugs: Thiazides), M ilk Alkali syndrome, P aget disease of the bone, A cromegaly and Addison's Disease, N eoplasia, Z olinger-Ellison Syndrome (MEN Type I), E xcessive Vitamin D, E xcessive Vitamin A, S arcoidosis, Patients with coeliac disease tend to develop hypocalcaemia due to malabsorption of calcium by the, bowel., Please rate this question:, , Discuss and give feedback, , Next question, , Hypercalcaemia, Main causes, , , , Malignancy (most common cause in hospital in-patients), Primary hyperparathyroidism (commonest cause in non hospitalised patients)
Page 346 :
Less common, , , , , , , , , , Sarcoidosis (extrarenal synthesis of calcitriol ), Thiazides, lithium, Immobilisation, Pagets disease, Vitamin A/D toxicity, Thyrotoxicosis, MEN, Milk alkali syndrome, , Clinical features, Stones, bones, abdominal groans, and psychic moans, High serum calcium levels result in decreased neuronal excitability. Therefore sluggish reflexes,, muscle weakness and constipation may occur., Next question
Page 347 :
Release of somatostatin from the pancreas will result in which of the following?, , Decrease in pancreatic exocrine secretions, , Contraction of the gallbladder, , Increase in the rate of gastric emptying, , Increased synthesis of growth hormone, , Increased insulin release, , Octreotide reduces exocrine pancreatic secretions so is used to treat high output pancreatic fistulae, (though parenteral feeding is most effective). Other uses include variceal bleeding and treatment of, acromegaly., Inhibits growth hormone and insulin release (when released from pancreas)., Somatostatin is also released by the hypothalamus causing a negative feedback response on, growth hormone., Please rate this question:, , Discuss and give feedback, , Next question, , Somatostatin, Somatostatin is produced in the D cells of the pancreatic islets. It is also produced in the gut, (enterochromaffin cells) and is found in brain tissue. Those substances that stimulate insulin release, will also induce somatostatin secretion. It is an inhibitor of growth hormone, it also delays gastric, emptying and reduces gastrin secretion., It reduces pancreatic exocrine secretions and may be used therapeutically to treat pancreatic, fistulae.
Page 348 :
Somatostatinomas are rare pancreatic endocrine tumours and will result in the clinical, manifestations of diabetes mellitus, gallstones and steatorrhoea., Next question
Page 349 :
A 34 year old lady develops septic shock and features of the systemic inflammatory response, syndrome as a complication of cholangitis. Which of the following is not a typical feature of this, condition?, , Body temperature less than 36oC or greater than 38oC, , Respiratory rate >20, , Lactate <4 mmol/L, High levels of tumour necrosis factor α, , WCC >12,000 mm3, , Septic shock will typically result in end organ hypoperfusion and as a result lactate levels will often, be high. In the surviving sepsis campaign it is suggested that elevated lactate levels are an, independent indicator for vasopressor support in patient with sepsis. The WCC may be paradoxically, low in severe sepsis, although it is most often elevated., Please rate this question:, , Discuss and give feedback, , Next question, , Shock, , , , , , , , , Shock occurs when there is insufficient tissue perfusion., The pathophysiology of shock is an important surgical topic and may be divided into the, following aetiological groups:, Septic, Haemorrhagic, Neurogenic, Cardiogenic, Anaphylactic, , Septic shock, Septic shock is a major problem and those patients with severe sepsis have a mortality rate in, excess of 40%. In those who are admitted to intensive care mortality ranges from 6% with no organ, failure to 65% in those with 4 organ failure., Sepsis is defined as an infection that triggers a particular Systemic Inflammatory Response, Syndrome (SIRS). This is characterised by body temperature outside 36 oC - 38 o C, HR >90
Page 350 :
beats/min, respiratory rate >20/min, WBC count >12,000/mm 3 or < 4,000/mm 3, altered mental state, or hyperglycaemia (in absence of diabetes)., Patients with infections and two or more elements of SIRS meet the diagnostic criteria for sepsis., Those with organ failure have severe sepsis and those with refractory hypotension -septic shock., During the septic process there is marked activation of the immune system with extensive cytokine, release. This may be coupled with or triggered by systemic circulation of bacterial toxins. These all, cause endothelial cell damage and neutrophil adhesion. The overall hallmarks are thus those, ofexcessive inflammation, coagulation and fibrinolytic suppression., The surviving sepsis campaign (2012) highlights the following key areas for attention:, , , , , Prompt administration of antibiotics to cover all likely pathogens coupled with a rigorous, search for the source of infection., Haemodynamic stabilisation. Many patients are hypovolaemic and require aggressive fluid, administration. Aim for CVP 8-12 cm H2O, MAP >65mmHg., Modulation of the septic response. This includes manoeuvres to counteract the changes and, includes measures such as tight glycaemic control. The routine use of steroids is not, advised., , In surgical patients, the main groups with septic shock include those with anastomotic leaks,, abscesses and extensive superficial infections such as necrotising fasciitis. When performing, surgery the aim should be to undertake the minimum necessary to restore physiology. These, patients do not fare well with prolonged surgery. Definitive surgery can be more safely undertaken, when physiology is restored and clotting in particular has been normalised., Haemorrhagic shock, The average adult blood volume comprises 7% of body weight. Thus in the 70 Kg adult this will, equate to 5 litres. This changes in children (8-9% body weight) and is slightly lower in the elderly., The table below outlines the 4 major classes of haemorrhagic shock and their associated, physiological sequelae:, , Parameter, , Class I, , Class II, , Class III, , Class IV, , Blood loss ml, , <750ml, , 750-1500ml, , 1500-2000ml, , >2000ml, , Blood loss %, , <15%, , 15-30%, , 30-40%, , >40%, , Pulse rate, , <100, , >100, , >120, , >140
Page 351 :
Parameter, , Class I, , Class II, , Class III, , Class IV, , Blood pressure, , Normal, , Normal, , Decreased, , Decreased, , Respiratory rate, , 14-20, , 20-30, , 30-40, , >35, , Urine output, , >30ml, , 20-30ml, , 5-15ml, , <5ml, , Symptoms, , Normal, , Anxious, , Confused, , Lethargic, , Decreasing blood pressure during haemorrhagic shock causes organ hypoperfusion and relative, myocardial ischaemia. The cardiac index gives a numerical value for tissue oxygen delivery and is, given by the equation: Cardiac index= Cardiac output/ body surface area. Where Hb is, haemoglobin concentration in blood and SaO2 the saturation and PaO2 the partial pressure of, oxygen. Detailed knowledge of this equation is required for the MRCS Viva but not for part A,, although you should understand the principle., In patients suffering from trauma the most likely cause of shock is haemorrhage. However, the, following may also be the cause or occur concomitantly:, , , , , , , Tension pneumothorax, Spinal cord injury, Myocardial contusion, Cardiac tamponade, , When assessing trauma patients it is worth remembering that in order to generate a palpable, femoral pulse an arterial pressure of >65mmHg is required., Once bleeding is controlled and circulating volume normalised the levels of transfusion should be to, maintain a Hb of 7-8 in those with no risk factors for tissue hypoxia and Hb 10 for those who have, such risk factors., Neurogenic shock, This occurs most often following a spinal cord transection, usually at a high level. There is, resultant interruption of the autonomic nervous system. The result is either decreased sympathetic, tone or increased parasympathetic tone, the effect of which is a decrease in peripheral vascular, resistance mediated by marked vasodilation., This results in decreased preload and thus decreased cardiac output (Starlings law). There is, decreased peripheral tissue perfusion and shock is thus produced. In contrast with many other types, of shock peripheral vasoconstrictors are used to return vascular tone to normal.
Page 352 :
Cardiogenic shock, In medical patients the main cause is ischaemic heart disease. In the traumatic setting direct, myocardial trauma or contusion is more likely. Evidence of ECG changes and overlying sternal, fractures or contusions should raise the suspicion of injury. Treatment is largely supportive and, transthoracic echocardiography should be used to determine evidence of pericardial fluid or direct, myocardial injury. The measurement of troponin levels in trauma patients may be undertaken but, they are less useful in delineating the extent of myocardial trauma than following MI., When cardiac injury is of a blunt nature and is associated with cardiogenic shock the right side of the, heart is the most likely site of injury with chamber and or valve rupture. These patients require, surgery to repair these defects and will require cardiopulmonary bypass to achieve this. Some may, require intra aortic balloon pump as a bridge to surgery., Anaphylactic shock, Anaphylaxis may be defined as a severe, life-threatening, generalised or systemic, hypersensitivity reaction., Anaphylaxis is one of the few times when you would not have time to look up the dose of a, medication. The Resuscitation Council guidelines on anaphylaxis have recently been updated., Adrenaline is by far the most important drug in anaphylaxis and should be given as soon as, possible. The recommended doses for adrenaline, hydrocortisone and chlorpheniramine are as, follows:, , Adrenaline, , Hydrocortisone, , Chlorpheniramine, , < 6 months, , 150 mcg (0.15ml 1 in 1,000), , 25 mg, , 250 mcg/kg, , 6 months - 6 years, , 150 mcg (0.15ml 1 in 1,000), , 50 mg, , 2.5 mg, , 6-12 years, , 300 mcg (0.3ml 1 in 1,000), , 100 mg, , 5 mg, , Adult and child 12 years, , 500 mcg (0.5ml 1 in 1,000), , 200 mg, , 10 mg, , Adrenaline can be repeated every 5 minutes if necessary. The best site for IM injection is the, anterolateral aspect of the middle third of the thigh., Common identified causes of anaphylaxis, , , , , food (e.g. Nuts) - the most common cause in children, drugs, venom (e.g. Wasp sting), Next question
Page 353 :
Which of the following stimulates gastric acid secretion?, , Cholecystokinin, , Gastric inhibitory peptide, , Secretin, , Histamine, , Somatostatin, , Gastrin: From G cells: stimulates gastric acid production, Pepsin: Digestion of protein, secretion occurs simultaneously with gastrin, Secretin: From mucosal cells in the duodenum and jejunum: inhibits gastric acid, stimulates bile and, pancreatic juice production, Gastric inhibitory peptide: (produced in response to fatty acids) inhibits gastrin release and acid, secretion from parietal cells, Cholecystokinin: From mucosal cells in the duodenum and jejunum (produced in response to fatty, acids) inhibits acid secretion from parietal cells, causes gallbladder contraction and relaxation of, sphincter of Oddi, Somatostatin: From D cells, Please rate this question:, , Discuss and give feedback, , Next question, , Hormonal control of gastric acid secretion
Page 354 :
Source, , Stimulus, , Actions, , Gastrin, , G cells in, antrum of the, stomach, , Distension of, stomach, extrinsic, nerves, Inhibited by: low, antral pH,, somatostatin, , Increase HCL, pepsinogen and IF secretion,, increases gastric motility, trophic effect on gastric, mucosa, , CCK, , I cells in upper, small intestine, , Partially digested, proteins and, triglycerides, , Increases secretion of enzyme-rich fluid from, pancreas, contraction of gallbladder and, relaxation of sphincter of Oddi, decreases gastric, emptying, trophic effect on pancreatic acinar, cells, induces satiety, , Secretin, , S cells in, upper small, intestine, , Acidic chyme, fatty, acids, , Increases secretion of bicarbonate-rich fluid from, pancreas and hepatic duct cells, decreases gastric, acid secretion, trophic effect on pancreatic acinar, cells, , VIP, , Small, intestine,, pancreas, , Neural, , Stimulates secretion by pancreas and intestines,, inhibits acid and pepsinogen secretion, , Somatostatin, , D cells in the, pancreas and, stomach, , Fat, bile salts and, glucose in the, intestinal lumen, , Decreases acid and pepsin secretion, decreases, gastrin secretion, decreases pancreatic enzyme, secretion, decreases insulin and glucagon, secretion, inhibits trophic effects of gastrin, stimulates, gastric mucous production, Next question
Page 355 :
Which of the following statements relating to gastric acid secretions are untrue?, , In parietal cells carbonic anhydrase generates hydrogen ions which are then actively, secreted, The cephalic phase is abolished following truncal vagotomy, , The intestinal phase accounts for 60% of gastric acid produced, , Histamine acts in a paracrine manner on H2 receptors, , H2 receptor antagonists will not completely abolish gastric acid production, , The intestinal phase of gastric acid secretion accounts for only 10% of gastric acid produced., Please rate this question:, , Discuss and give feedback, , Next question, , Gastric secretions, A working knowledge of gastric secretions is important for surgery because peptic ulcers are, common, surgeons frequently prescribe anti secretory drugs and because there are still patients, around who will have undergone acid lowering procedures (Vagotomy) in the past., Gastric acid, , , , , , Is produced by the parietal cells in the stomach, pH of gastric acid is around 2 with acidity being maintained by the H +/K+ ATP ase pump. As, part of the process bicarbonate ions will be secreted into the surrounding vessels., Sodium and chloride ions are actively secreted from the parietal cell into the canaliculus., This sets up a negative potential across the membrane and as a result sodium and, potassium ions diffuse across into the canaliculus., Carbonic anhydrase forms carbonic acid which dissociates and the hydrogen ions formed by, dissociation leave the cell via the H+/K+ antiporter pump. At the same time sodium ions are, actively absorbed. This leaves hydrogen and chloride ions in the canaliculus these mix and, are secreted into the lumen of the oxyntic gland., , This is illustrated diagrammatically below:
Page 356 :
Image sourced from Wikipedia, , Phases of gastric acid secretion, There are 3 phases of gastric secretion:, 1. Cephalic phase (smell / taste of food), , , , 30% acid produced, Vagal cholinergic stimulation causing secretion of HCL and gastrin release from G cells, , 2. Gastric phase (distension of stomach ), , , , 60% acid produced, Stomach distension/low H+/peptides causes Gastrin release
Page 357 :
3. Intestinal phase (food in duodenum), , , , 10% acid produced, High acidity/distension/hypertonic solutions in the duodenum inhibits gastric acid secretion, via enterogastrones (CCK, secretin) and neural reflexes., , Regulation of gastric acid production, Factors increasing production include:, , , , , Vagal nerve stimulation, Gastrin release, Histamine release (indirectly following gastrin release) from enterchromaffin like cells, , Factors decreasing production include:, , , , , Somatostatin (inhibits histamine release), Cholecystokinin, Secretin, , The diagram below illustrates some of the factors involved in regulating gastric acid secretion and, the relevant associated pharmacology, , Image sourced from Wikipedia, , Below is a brief summary of the major hormones involved in food digestion:
Page 358 :
Source, , Stimulus, , Actions, , Gastrin, , G cells in, antrum of the, stomach, , Distension of, stomach, extrinsic, nerves, Inhibited by: low, antral pH,, somatostatin, , Increase HCL, pepsinogen and IF secretion,, increases gastric motility, trophic effect on, gastric mucosa, , CCK, , I cells in, upper small, intestine, , Partially digested, proteins and, triglycerides, , Increases secretion of enzyme-rich fluid, from pancreas, contraction of gallbladder, and relaxation of sphincter of Oddi,, decreases gastric emptying, trophic effect on, pancreatic acinar cells, induces satiety, , Secretin, , S cells in, upper small, intestine, , Acidic chyme,, fatty acids, , Increases secretion of bicarbonate-rich fluid, from pancreas and hepatic duct cells,, decreases gastric acid secretion, trophic, effect on pancreatic acinar cells, , VIP, , Small, intestine,, pancreas, , Neural, , Stimulates secretion by pancreas and, intestines, inhibits acid and pepsinogen, secretion, , Somatostatin, , D cells in the, pancreas and, stomach, , Fat, bile salts and, glucose in the, intestinal lumen, , Decreases acid and pepsin secretion,, decreases gastrin secretion, decreases, pancreatic enzyme secretion, decreases, insulin and glucagon secretion, inhibits trophic effects of gastrin, stimulates, gastric mucous production, Next question
Page 359 :
A 22 year old man is undergoing a daycase excision of a sebaceous cyst. He is needle phobic and, as the surgeon approaches with the needle the patient begins to hyperventilate. He soon develops, circumoral parasthesia and muscular twitching. Which of the following is the most likely explanation, for this event?, , Temporal lobe epilepsy, , Reduction in ionised calcium levels, , Increase in ionised calcium levels, , Fall in serum PTH levels, , Rise in serum PTH levels, , 50% of plasma calcium is ionised. Hyperventilation will induce a state of alkalosis which will lower, ionised plasma calcium levels., Please rate this question:, , Discuss and give feedback, , Next question, , Calcium homeostasis, Calcium ions are linked to a wide range of physiological processes. The largest store of bodily, calcium is contained within the skeleton. Calcium levels are primarily controlled by parathyroid, hormone, vitamin D and calcitonin., Hormonal regulation of calcium, , Hormone, , Parathyroid hormone (PTH), , Actions, , , , , , Increase calcium levels and decrease phosphate, levels, Increases bone resorption, Immediate action on osteoblasts to increase ca2+ in, extracellular fluid, Osteoblasts produce a protein signaling molecule, that activate osteoclasts which cause bone, resorption
Page 360 :
Hormone, , Actions, , , , , , 1,25-dihydroxycholecalciferol (the, active form of vitamin D), , Calcitonin, , , , , Increases renal tubular reabsorption of calcium, Increases synthesis of 1,25(OH)2D (active form, of vitamin D) in the kidney which increases, bowel absorption of Ca2+, Decreases renal phosphate reabsorption, , , , , Increases plasma calcium and plasma phosphate, Increases renal tubular reabsorption and gut, absorption of calcium, Increases osteoclastic activity, Increases renal phosphate reabsorption, , , , , , , Secreted by C cells of thyroid, Inhibits intestinal calcium absorption, Inhibits osteoclast activity, Inhibits renal tubular absorption of calcium, , Both growth hormone and thyroxine also play a small role in calcium metabolism., Next question
Page 361 :
Which of the following inhibits gastric acid secretion?, , Histamine, , Nausea, , Calcium, , Parasympathetic vagal stimulation, , Gastrin, , Nausea inhibits gastric secretion via higher cerebral activity and sympathetic innervation., Please rate this question:, , Discuss and give feedback, , Next question, , Gastric secretions, A working knowledge of gastric secretions is important for surgery because peptic ulcers are, common, surgeons frequently prescribe anti secretory drugs and because there are still patients, around who will have undergone acid lowering procedures (Vagotomy) in the past., Gastric acid, , , , , , Is produced by the parietal cells in the stomach, pH of gastric acid is around 2 with acidity being maintained by the H +/K+ ATP ase pump. As, part of the process bicarbonate ions will be secreted into the surrounding vessels., Sodium and chloride ions are actively secreted from the parietal cell into the canaliculus., This sets up a negative potential across the membrane and as a result sodium and, potassium ions diffuse across into the canaliculus., Carbonic anhydrase forms carbonic acid which dissociates and the hydrogen ions formed by, dissociation leave the cell via the H+/K+ antiporter pump. At the same time sodium ions are, actively absorbed. This leaves hydrogen and chloride ions in the canaliculus these mix and, are secreted into the lumen of the oxyntic gland., , This is illustrated diagrammatically below:
Page 362 :
Image sourced from Wikipedia, , Phases of gastric acid secretion, There are 3 phases of gastric secretion:, 1. Cephalic phase (smell / taste of food), , , , 30% acid produced, Vagal cholinergic stimulation causing secretion of HCL and gastrin release from G cells, , 2. Gastric phase (distension of stomach ), , , , 60% acid produced, Stomach distension/low H+/peptides causes Gastrin release, , 3. Intestinal phase (food in duodenum)
Page 363 :
, , , 10% acid produced, High acidity/distension/hypertonic solutions in the duodenum inhibits gastric acid secretion, via enterogastrones (CCK, secretin) and neural reflexes., , Regulation of gastric acid production, Factors increasing production include:, , , , , Vagal nerve stimulation, Gastrin release, Histamine release (indirectly following gastrin release) from enterchromaffin like cells, , Factors decreasing production include:, , , , , Somatostatin (inhibits histamine release), Cholecystokinin, Secretin, , The diagram below illustrates some of the factors involved in regulating gastric acid secretion and, the relevant associated pharmacology, , Image sourced from Wikipedia, , Below is a brief summary of the major hormones involved in food digestion:, , Source, , Stimulus, , Actions
Page 364 :
Gastrin, , G cells in, antrum of the, stomach, , Distension of, stomach, extrinsic, nerves, Inhibited by: low, antral pH,, somatostatin, , Increase HCL, pepsinogen and IF secretion,, increases gastric motility, trophic effect on, gastric mucosa, , CCK, , I cells in, upper small, intestine, , Partially digested, proteins and, triglycerides, , Increases secretion of enzyme-rich fluid, from pancreas, contraction of gallbladder, and relaxation of sphincter of Oddi,, decreases gastric emptying, trophic effect on, pancreatic acinar cells, induces satiety, , Secretin, , S cells in, upper small, intestine, , Acidic chyme,, fatty acids, , Increases secretion of bicarbonate-rich fluid, from pancreas and hepatic duct cells,, decreases gastric acid secretion, trophic, effect on pancreatic acinar cells, , VIP, , Small, intestine,, pancreas, , Neural, , Stimulates secretion by pancreas and, intestines, inhibits acid and pepsinogen, secretion, , Somatostatin, , D cells in the, pancreas and, stomach, , Fat, bile salts and, glucose in the, intestinal lumen, , Decreases acid and pepsin secretion,, decreases gastrin secretion, decreases, pancreatic enzyme secretion, decreases, insulin and glucagon secretion, inhibits trophic effects of gastrin, stimulates, gastric mucous production, Next question
Page 365 :
A 73 year old lady is diagnosed with hyperaldosteronism. From which of the following structures is, aldosterone released?, , Zona fasciculata of the adrenal gland, , Juxtaglomerular apparatus of the kidney, , Zona reticularis of the adrenal gland, , Adrenal medulla, , Zona glomerulosa of the adrenal cortex, , Aldosterone serves to conserve sodium and water. It is produced in the zona glomerulosa of the, adrenal cortex., Please rate this question:, , Discuss and give feedback, , Next question, , Aldosterone, Aldosterone is secreted by the zona glomerulosa of the adrenal cortex. It is a mineralocorticoid, hormone. Secretion is regulated by the renin- angiotensin system, and by plasma levels of sodium, and potassium. Aldosterone conserves sodium by stimulating the reabsorption of sodium in the, distal nephron in exchange for potassium. Lack of aldosterone release will result in hyperkalaemia, and hyponatraemia., Next question
Page 366 :
Which of the following hormonal agents will increase secretions of water and electrolytes in, pancreatic juice?, , Secretin, , Aldosterone, , Somatostatin, , Cholecystokinin, , Adrenaline, Secretin causes secretion of water and electrolytes, Cholecystokinin causes enzyme secretion, , While secretin will typically increase electrolyte and water volume of secretions, the enzyme content, in increased by cholecystokinin. Somatostatin will decrease the volume of secretions. Aldosterone, will tend to conserve electrolytes., Please rate this question:, , Discuss and give feedback, , Next question, , Pancreas exocrine physiology, Composition of pancreatic secretions, Pancreatic secretions are usually 1000-1500ml per 24 hours and have a pH of 8., Secretion, , Source, , Enzymic, , Acinar cells, , Substances secreted, , Trypsinogen
Page 367 :
Procarboxylase, Amylase, Elastase, , Aqueous, , Ductal and, Centroacinar cells, , Sodium, Bicarbonate, Water, Potassium, Chloride, NB: Sodium and potassium reflect their plasma levels; chloride, and bicarbonate vary with flow rate, , Regulation, The cephalic and gastric phases (neuronal and physical) are less important in regulating the, pancreatic secretions. The effect of digested material in the small bowel stimulates CCK release and, ACh which stimulate acinar and ductal cells. Of these CCK is the most potent stimulus. In the case, of the ductal cells these are potently stimulated by secretin which is released by the S cells of the, duodenum. This results in an increase in bicarbonate., Enzyme activation, Trypsinogen is converted via enterokinase to active trypsin in the duodenum. Trypsin then activates, the other inactive enzymes, Next question
Page 368 :
A 43 year old lady is admitted with cholestasis secondary to a stone impacted at the level of the, ampulla of vater. Which of the following tests is most likely to be predictive of bleeding diathesis at, the time of ERCP in this particular case?, , Bleeding time, , Prothrombin time, , APTT, , Platelet count, , Factor I levels, PT: Vitamin K dependent factors 2, 7, 9, 10, APTT: Factors 8, 9, 11, 12, , Jaundice will impair the production of vitamin K dependent clotting factors. This is most accurately, tested by measuring the prothrombin time. APTT can be affected by vitamin K deficiency (due to, factor 9 deficiency), however this occurs to a lesser extent and is normally associated with severe, liver disease. The bleeding time is a measure of platelet function., Please rate this question:, , Discuss and give feedback, , Next question, , Abnormal coagulation, Cause, , Factors affected
Page 369 :
Cause, , Factors affected, , Heparin, , Prevents activation factors 2,9,10,11, , Warfarin, , Affects synthesis of factors 2,7,9,10, , DIC, , Factors 1,2,5,8,11, , Liver disease, , Factors 1,2,5,7,9,10,11, , Interpretation blood clotting test results, , Disorder, , APTT, , PT, , Bleeding time, , Haemophilia, , Increased, , Normal, , Normal, , von Willebrand's disease, , Increased, , Normal, , Increased, , Vitamin K deficiency, , Increased, , Increased, , Normal, Next question
Page 370 :
Which of the following mechanisms best accounts for the release of adrenaline?, , Release from the adrenal medulla in response to increased angiotensin 1 levels, , Release from the zona fasiculata from the adrenal gland in response to increased, sympathetic discharge, Release from the adrenal medulla in response to increased noradrenaline levels, , Release from the adrenal medulla in response to sympathetic stimulation from the, splanchnic nerves, None of the above, , The adrenal gland releases adrenaline in response to increased sympathetic discharge from, preganglionic sympathetic fibres of the splanchnic nerves. These cause the chromafin cells of the, medulla to release adrenaline (which is preformed) by exocytosis., Please rate this question:, , Discuss and give feedback, , Next question, , Adrenaline, , , Fight or Flight response, , - Catecholamine (phenylalanine and tyrosine), - Neurotransmitter and hormone, - Released by the adrenal glands, - Effects on α 1 and 2, β 1 and 2 receptors, - Effect on β 2 receptors in skeletal muscle vessels-causing vasodilation, - Increase cardiac output and total peripheral resistance, - Vasoconstriction in the skin and kidneys causing a narrow pulse pressure, Actions, α adrenergic receptors:, , , , , Inhibits insulin secretion by the pancreas, Stimulates glycogenolysis in the liver and muscle, Stimulates glycolysis in muscle
Page 371 :
β adrenergic receptors:, , , , , Stimulates glucagon secretion in the pancreas, Stimulates ACTH, Stimulates lipolysis by adipose tissue, Next question
Page 372 :
The acute phase response to injury does not include:, , Pyrexia, , Decreased albumin, , Hepatic sequestration of cations, , Increased transferrin, , Increased serum amyloid A, , The acute phase response includes:, , , , , , , , , , Acute phase proteins, Reduction of transport proteins (albumin, transferrin), Hepatic sequestration cations, Pyrexia, Neutrophil leucocytosis, Increased muscle proteolysis, Changes in vascular permeability, , Please rate this question:, , Discuss and give feedback, , Next question, , Stress response: Endocrine and metabolic changes, , , , , Surgery precipitates hormonal and metabolic changes causing the stress response., Stress response is associated with: substrate mobilization, muscle protein loss, sodium and, water retention, suppression of anabolic hormone secretion, activation of the sympathetic, nervous system, immunological and haematological changes., The hypothalamic-pituitary axis and the sympathetic nervous systems are activated and, there is a failure of the normal feedback mechanisms of control of hormone secretion., , A summary of the hormonal changes associated with the stress response:
Page 374 :
, , ACTH stimulates cortisol production within a few minutes of the start of surgery. More ACTH, is produced than needed to produce a maximum adrenocortical response., , Cortisol, , , , , , Significant increases within 4-6 hours of surgery (>1000 nmol litre-1)., The usual negative feedback mechanism fails and concentrations of ACTH and cortisol, remain persistently increased., The magnitude and duration of the increase correlate with the severity of stress and the, response is not abolished by the administration of corticosteroids., The metabolic effects of cortisol are enhanced:, , Skeletal muscle protein breakdown to provide gluconeogenic precursors and amino acids for protein, synthesis in the liver, Stimulation of lipolysis, 'Anti-insulin effect', Mineralocorticoid effects, Anti-inflammatory effects, Growth hormone, , , , Increased secretion after surgery has a minor role, Most important for preventing muscle protein breakdown and promote tissue repair by insulin, growth factors, , Alpha Endorphin, , , Increased, , Antidiuretic hormone, , , , , An important vasopressor and enhances haemostasis, Renin is released causing the conversion of angiotensinogen to angiotensin I, Angiotensin II formed by ACE on angiotensin 1, which causes the secretion of aldosterone, from the adrenal cortex. This increases sodium reabsorption at the distal convoluted tubule, , Insulin, , , Release inhibited by stress
Page 375 :
, , , , Occurs via the inhibition of the beta cells in the pancreas by the α2-adrenergic inhibitory, effects of catecholamines, Insulin resistance by target cells occurs later, The perioperative period is characterized by a state of functional insulin deficiency, , Thyroxine (T4) and tri-iodothyronine (T3), , , Circulating concentrations are inversely correlated with sympathetic activity and after surgery, there is a reduction in thyroid hormone production, which normalises over a few days., , Metabolic effect of endocrine response, Carbohydrate metabolism, , , , , , , , Hyperglycaemia is a main feature of the metabolic response to surgery, Due to increase in glucose production and a reduction in glucose utilization, Catecholamines and cortisol promote glycogenolysis and gluconeogenesis, Initial failure of insulin secretion followed by insulin resistance affects the normal responses, The proportion of the hyperglycaemic response reflects the severity of surgery, Hyperglycaemia impairs wound healing and increase infection rates, , Protein metabolism, , , , , , , Initially there is inhibition of protein anabolism, followed later, if the stress response is, severe, by enhanced catabolism, The amount of protein degradation is influenced by the type of surgery and also by the, nutritional status of the patient, Mainly skeletal muscle protein is affected, The amino acids released form acute phase proteins (fibrinogen, C reactive protein,, complement proteins, a2-macroglobulin, amyloid A and ceruloplasmin) and are used for, gluconeogenesis, Nutritional support has little effect on preventing catabolism, , Lipid metabolism, Increased catecholamine, cortisol and glucagon secretion, and insulin deficiency, promotes lipolysis, and ketone body production., Salt and water metabolism, , , , ADH causes water retention, concentrated urine, and potassium loss and may continue for 3, to 5 days after surgery, Renin causes sodium and water retention
Page 376 :
Cytokines, , , , , , Glycoproteins, Interleukins (IL) 1 to 17, interferons, and tumour necrosis factor, Synthesized by activated macrophages, fibroblasts, endothelial and glial cells in response to, tissue injury from surgery or trauma, IL-6 main cytokine associated with surgery. Peak 12 to 24 h after surgery and increase by, the degree of tissue damage Other effects of cytokines include fever, granulocytosis,, haemostasis, tissue damage limitation and promotion of healing., , Modifying the response, , , , , , , , , Opioids suppress hypothalamic and pituitary hormone secretion, At high doses the hormonal response to pelvic and abdominal surgery is abolished., However, such doses prolong recovery and increase the need for postoperative ventilatory, support, Spinal anaesthesia can reduce the glucose, ACTH, cortisol, GH and epinephrine changes,, although cytokine responses are unaltered, Cytokine release is reduced in less invasive surgery, Nutrition prevents the adverse effects of the stress response. Enteral feeding improves, recovery, Growth hormone and anabolic steroids may improve outcome, Normothermia decreases the metabolic response, , References, Deborah Burton, Grainne Nicholson, and George Hall, Endocrine and metabolic response to surgery ., Contin Educ Anaesth Crit Care Pain (2004) 4(5): 144-147 doi:10.1093/bjaceaccp/mkh040, Next question
Page 377 :
Which of the following statements relating to blood transfusions in surgical patients is false?, , Packed red cells typically have a haematocrit of between 55 and 75%, , Clotting factor activity in whole blood decreases in samples stored for longer than 7 days, , After 3 weeks of storage blood has a pH of 6.9, , Gamma irradiated blood products are not required routinely, , Patients should be transfused to achieve a target haemoglobin of 10 g/dl and a haematocrit, of 30%, , Patients can generally be managed without transfusion as long as the Hb is 7 or greater. The exact, level depends upon patient factors such as co-morbidities. Old blood functions less effectively and, should not be used during massive transfusions., Please rate this question:, , Discuss and give feedback, , Next question, , Blood products, Whole blood fractions, , Fraction, , Key points, , Packed red cells, , Used for transfusion in chronic anaemia and cases where infusion of large, volumes of fluid may result in cardiovascular compromise. Product obtained, by centrifugation of whole blood., , Platelet rich, plasma, , Usually administered to patients who are thrombocytopaenic and are bleeding, or require surgery. It is obtained by low speed centrifugation., , Platelet, , Prepared by high speed centrifugation and administered to patients with
Page 378 :
concentrate, , Fresh frozen, plasma, , thrombocytopaenia., , , , , , , , Cryoprecipitate, , SAG-Mannitol, Blood, , , , , , Prepared from single units of blood., Contains clotting factors, albumin and immunoglobulin., Unit is usually 200 to 250ml., Usually used in correcting clotting deficiencies in patients with hepatic, synthetic failure who are due to undergo surgery., Usual dose is 12-15ml/Kg-1., It should not be used as first line therapy for hypovolaemia., Formed from supernatant of FFP., Rich source of Factor VIII and fibrinogen., Allows large concentration of factor VIII to be administered in small, volume., , Removal of all plasma from a blood unit and substitution with:, , , , , , Sodium chloride, Adenine, Anhydrous glucose, Mannitol, , Up to 4 units of SAG M Blood may be administered. Thereafter whole blood, is preferred. After 8 units, clotting factors and platelets should be considered., Cell saver devices, These collect patients own blood lost during surgery and then re-infuse it. There are two main types:, , , , Those which wash the blood cells prior to re-infusion. These are more expensive to purchase, and more complicated to operate. However, they reduce the risk of re-infusing contaminated, blood back into the patient., Those which do not wash the blood prior to re-infusion., , Their main advantage is that they avoid the use of infusion of blood from donors into patients and, this may reduce risk of blood borne infection. It may be acceptable to Jehovah's witnesses. It is, contraindicated in malignant disease for risk of facilitating disease dissemination., Blood products used in warfarin reversal, In some surgical patients the use of warfarin can pose specific problems and may require the use of, specialised blood products, Immediate or urgent surgery in patients taking warfarin(1) (2):
Page 379 :
1. Stop warfarin, 2. Vitamin K (reversal within 4-24 hours), -IV takes 4-6h to work (at least 5mg), -Oral can take 24 hours to be clinically effective, 3. Fresh frozen plasma, Used less commonly now as 1st line warfarin reversal, -30ml/kg-1, -Need to give at least 1L fluid in 70kg person (therefore not appropriate in fluid overload), -Need blood group, -Only use if human prothrombin complex is not available, 4. Human Prothrombin Complex (reversal within 1 hour), -Bereplex 50 u/kg, -Rapid action but factor 6 short half life, therefore give with vitamin K, References, 1. Dentali, F., C. Marchesi, et al. (2011). "Safety of prothrombin complex concentrates for rapid, anticoagulation reversal of vitamin K antagonists. A meta-analysis." Thromb Haemost 106(3): 429438., 2. http://www.transfusionguidelines.org/docs/pdfs/bbt-03warfarin-reversal-flowchart-2006.pdf, Next question
Page 380 :
Which of the following statements relating the fluid physiology of a physiologically normal 70 Kg, adult male is false?, , He will have more water per unit of body weight than a female of similar weight, , Plasma will comprise 25% of his body weight, , Interstitial fluid will account for up to 24% of body weight, , Approximately 65% of total body water is intracellular, , 60% of his body weight is composed of water, The 60-40-20 rule:, 60% total body weight is water, 40% of total body weight is intracellular fluids, 20% of body weight is extracellular fluids, , Plasma typically accounts for 4-6% of body weight in healthy individuals., Males typically have more water per unit weight than females, as females have a higher fat content., Please rate this question:, , Discuss and give feedback, , Next question, , Fluid compartment physiology, Body fluid compartments comprise intracellular and extracellular compartments. The latter includes, interstitial fluid, plasma and transcellular fluid., Typical figures are based on the 70 Kg male., Body fluid volumes
Page 381 :
Compartment, , Volume in litres, , Percentage of total volume, , Intracellular, , 28 L, , 60-65%, , Extracellular, , 14 L, , 35-40%, , Plasma, , 3L, , 5%, , Interstitial, , 10 L, , 24%, , Transcellular, , 1L, , 3%, , Figures are approximate, Next question
Page 382 :
A 17 year old lady with long standing anorexia nervosa is due to undergo excision of a lipoma., Which of the following nutritional deficiencies is most likely to be implicated in poor collagen, formation as the wound heals?, , Deficiency of copper, , Deficiency of iron, , Deficiency of ascorbic acid, , Deficiency of phosphate, , None of the above, , Theme from January 2011, Vitamin C is involved in the cross linkage of collagen and impaired wound healing is well described, in cases of vitamin C deficiency., Please rate this question:, , Discuss and give feedback, , Next question, , Collagen, Collagen is one of the most important structural proteins within the extracellular matrix, collagen, together with components such as elastin and glycosaminoglycans determine the properties of all, tissues., , , , , , , Composed of 3 polypeptide strands that are woven into a helix, usually a combination of, glycine with either proline or hydroxyproline plus another amino acid, Numerous hydrogen bonds exist within molecule to provide additional strength, Many sub types but commonest sub type is I (90% of bodily collagen), tissues with increased, levels of flexibility have increased levels of type III collagen, Vitamin c is important in establishing cross links, Synthesised by fibroblasts, , Collagen Diseases, Disorders of collagen range from relatively common, acquired defects (typically aging), through to, rarer congenital disorders. The latter are exemplified by conditions such as osteogenesis imperfecta
Page 383 :
and Ehlers Danlos syndromes., Osteogenesis imperfecta:, -8 Subtypes, -Defect of type I collagen, -In type I the collagen is normal quality but insufficient quantity, -Type II- poor quantity and quality, -Type III- Collagen poorly formed, normal quantity, -Type IV- Sufficient quantity but poor quality, Patients have bones which fracture easily, loose joint and multiple other defects depending upon, which sub type they suffer from., Ehlers Danlos:, -Multiple sub types, -Abnormality of types 1 and 3 collagen, -Patients have features of hypermobility., -Individuals are prone to joint dislocations and pelvic organ prolapse. In addition to many other, diseases related to connective tissue defects., Next question
Page 384 :
A 45 year old man is undergoing a small bowel resection. The anaesthetist decides to administer an, intravenous fluid which is electrolyte rich. Which of the following most closely matches this, requirement?, , Dextrose / Saline, , Pentastarch, , Gelofusine, , Hartmans, , 5% Dextrose with added potassium 20mmol/ L, , Theme from April 2012 Exam, Hartmans solution is the most electrolyte rich. However, both pentastarch and gelofusine have more, macromolecules., Please rate this question:, , Discuss and give feedback, , Next question, , Intra operative fluid management, Composition of commonly used intravenous fluids mmol-1, , Plasma, , Na, , K, , Cl, , Bicarbonate, , Lactate, , 137-147, , 4-5.5, , 95-105, , 22-25, , -
Page 385 :
0.9% Saline, , 153, , -, , 153, , -, , -, , Dextrose / saline, , 30.6, , -, , 30.6, , -, , -, , Hartmans, , 130, , 4, , 110, , -, , 28, , Recommendations for intra operative fluid management, The latest set of NICE guidelines produced in 2013 relating to intravenous fluids did not specifically, address the requirements of intra operative fluid administration. The reason for this is that, administration of fluids in this specific situation does not lend itself to rigid algorithms., With the introduction of enhanced recovery programmes 10 years ago there was an increasing, emphasis of the concept of fluid restriction. Historically, patients received very large volumes of, saline rich solutions peri-operatively. Clearing the sodium load of a single litre of saline may take up, to 36 hours or more. This can have deleterious effects on the tissues including the development of, oedema. This results in poor perfusion, increased risk of ileus and wound breakdown. A tailored, approach to fluid administration is now practiced and far greater usage is made of cardiac output, monitors in providing goal directed fluid therapy., References, British Consensus Guidelines on Intravenous Fluid Therapy for Adult Surgical Patients, GIFTASUP (2009) Revised May 2011., Frost P. Intravenous fluid therapy in adult inpatients. BMJ 2015 (350): 31-34., Next question
Page 386 :
A 16 year old girl develops pyelonephritis and is admitted in a state of septic shock. Which of the, following is not typically seen in this condition?, , Increased cardiac output, , Increased systemic vascular resistance, , Oliguria may occur, , Systemic cytokine release, , Tachycardia, Cardiogenic Shock:, e.g. MI, valve abnormality, increased SVR (vasoconstriction in response to low BP), increased HR (sympathetic response), decreased cardiac output, decreased blood pressure, Hypovolaemic shock:, blood volume depletion, e.g. haemorrhage, vomiting, diarrhoea, dehydration, third-space losses during major operations, increased SVR, increased HR, decreased cardiac output, decreased blood pressure, Septic shock:, occurs when the peripheral vascular dilatation causes a fall in SVR, similar response may occur in anaphylactic shock, neurogenic shock, reduced SVR, increased HR, normal/increased cardiac output, decreased blood pressure, Theme from January 2012 Exam, The SVR is reduced in sepsis and for this reason a vasopressor such as noradrenaline may be used, if hypotension and oliguria remain a concern despite administration of adequate amounts of, intravenous fluids., Please rate this question:
Page 387 :
Discuss and give feedback, , Next question, , Shock, , , , , , , , , Shock occurs when there is insufficient tissue perfusion., The pathophysiology of shock is an important surgical topic and may be divided into the, following aetiological groups:, Septic, Haemorrhagic, Neurogenic, Cardiogenic, Anaphylactic, , Septic shock, Septic shock is a major problem and those patients with severe sepsis have a mortality rate in, excess of 40%. In those who are admitted to intensive care mortality ranges from 6% with no organ, failure to 65% in those with 4 organ failure., Sepsis is defined as an infection that triggers a particular Systemic Inflammatory Response, Syndrome (SIRS). This is characterised by body temperature outside 36 oC - 38 o C, HR >90, beats/min, respiratory rate >20/min, WBC count >12,000/mm 3 or < 4,000/mm 3, altered mental state, or hyperglycaemia (in absence of diabetes)., Patients with infections and two or more elements of SIRS meet the diagnostic criteria for sepsis., Those with organ failure have severe sepsis and those with refractory hypotension -septic shock., During the septic process there is marked activation of the immune system with extensive cytokine, release. This may be coupled with or triggered by systemic circulation of bacterial toxins. These all, cause endothelial cell damage and neutrophil adhesion. The overall hallmarks are thus those, ofexcessive inflammation, coagulation and fibrinolytic suppression., The surviving sepsis campaign (2012) highlights the following key areas for attention:, , , , , Prompt administration of antibiotics to cover all likely pathogens coupled with a rigorous, search for the source of infection., Haemodynamic stabilisation. Many patients are hypovolaemic and require aggressive fluid, administration. Aim for CVP 8-12 cm H2O, MAP >65mmHg., Modulation of the septic response. This includes manoeuvres to counteract the changes and, includes measures such as tight glycaemic control. The routine use of steroids is not, advised., , In surgical patients, the main groups with septic shock include those with anastomotic leaks,, abscesses and extensive superficial infections such as necrotising fasciitis. When performing, surgery the aim should be to undertake the minimum necessary to restore physiology. These, patients do not fare well with prolonged surgery. Definitive surgery can be more safely undertaken
Page 388 :
when physiology is restored and clotting in particular has been normalised., Haemorrhagic shock, The average adult blood volume comprises 7% of body weight. Thus in the 70 Kg adult this will, equate to 5 litres. This changes in children (8-9% body weight) and is slightly lower in the elderly., The table below outlines the 4 major classes of haemorrhagic shock and their associated, physiological sequelae:, , Parameter, , Class I, , Class II, , Class III, , Class IV, , Blood loss ml, , <750ml, , 750-1500ml, , 1500-2000ml, , >2000ml, , Blood loss %, , <15%, , 15-30%, , 30-40%, , >40%, , Pulse rate, , <100, , >100, , >120, , >140, , Blood pressure, , Normal, , Normal, , Decreased, , Decreased, , Respiratory rate, , 14-20, , 20-30, , 30-40, , >35, , Urine output, , >30ml, , 20-30ml, , 5-15ml, , <5ml, , Symptoms, , Normal, , Anxious, , Confused, , Lethargic, , Decreasing blood pressure during haemorrhagic shock causes organ hypoperfusion and relative, myocardial ischaemia. The cardiac index gives a numerical value for tissue oxygen delivery and is, given by the equation: Cardiac index= Cardiac output/ body surface area. Where Hb is, haemoglobin concentration in blood and SaO2 the saturation and PaO2 the partial pressure of, oxygen. Detailed knowledge of this equation is required for the MRCS Viva but not for part A,, although you should understand the principle., In patients suffering from trauma the most likely cause of shock is haemorrhage. However, the, following may also be the cause or occur concomitantly:, , , , , Tension pneumothorax, Spinal cord injury
Page 389 :
, , , Myocardial contusion, Cardiac tamponade, , When assessing trauma patients it is worth remembering that in order to generate a palpable, femoral pulse an arterial pressure of >65mmHg is required., Once bleeding is controlled and circulating volume normalised the levels of transfusion should be to, maintain a Hb of 7-8 in those with no risk factors for tissue hypoxia and Hb 10 for those who have, such risk factors., Neurogenic shock, This occurs most often following a spinal cord transection, usually at a high level. There is, resultant interruption of the autonomic nervous system. The result is either decreased sympathetic, tone or increased parasympathetic tone, the effect of which is a decrease in peripheral vascular, resistance mediated by marked vasodilation., This results in decreased preload and thus decreased cardiac output (Starlings law). There is, decreased peripheral tissue perfusion and shock is thus produced. In contrast with many other types, of shock peripheral vasoconstrictors are used to return vascular tone to normal., Cardiogenic shock, In medical patients the main cause is ischaemic heart disease. In the traumatic setting direct, myocardial trauma or contusion is more likely. Evidence of ECG changes and overlying sternal, fractures or contusions should raise the suspicion of injury. Treatment is largely supportive and, transthoracic echocardiography should be used to determine evidence of pericardial fluid or direct, myocardial injury. The measurement of troponin levels in trauma patients may be undertaken but, they are less useful in delineating the extent of myocardial trauma than following MI., When cardiac injury is of a blunt nature and is associated with cardiogenic shock the right side of the, heart is the most likely site of injury with chamber and or valve rupture. These patients require, surgery to repair these defects and will require cardiopulmonary bypass to achieve this. Some may, require intra aortic balloon pump as a bridge to surgery., Anaphylactic shock, Anaphylaxis may be defined as a severe, life-threatening, generalised or systemic, hypersensitivity reaction., Anaphylaxis is one of the few times when you would not have time to look up the dose of a, medication. The Resuscitation Council guidelines on anaphylaxis have recently been updated., Adrenaline is by far the most important drug in anaphylaxis and should be given as soon as, possible. The recommended doses for adrenaline, hydrocortisone and chlorpheniramine are as, follows:, , < 6 months, , Adrenaline, , Hydrocortisone, , Chlorpheniramine, , 150 mcg (0.15ml 1 in 1,000), , 25 mg, , 250 mcg/kg
Page 390 :
6 months - 6 years, , 150 mcg (0.15ml 1 in 1,000), , 50 mg, , 2.5 mg, , 6-12 years, , 300 mcg (0.3ml 1 in 1,000), , 100 mg, , 5 mg, , Adult and child 12 years, , 500 mcg (0.5ml 1 in 1,000), , 200 mg, , 10 mg, , Adrenaline can be repeated every 5 minutes if necessary. The best site for IM injection is the, anterolateral aspect of the middle third of the thigh., Common identified causes of anaphylaxis, , , , , food (e.g. Nuts) - the most common cause in children, drugs, venom (e.g. Wasp sting), Next question
Page 391 :
Which of the following statements are not typically true in hypokalaemia?, , It may occur as a result of mechanical bowel preparation, , Chronic vomiting may increase renal potassium losses, , It may be associated with aciduria, , It may cause hyponatraemia, , It often accompanies acidosis, , Potassium depletion occurs either through the gastrointestinal tract or the kidney. Chronic vomiting, in itself is less prone to induce potassium loss than diarrhoea as gastric secretions contain less, potassium than those in the lower GI tract. If vomiting produces a metabolic alkalosis then renal, potassium wasting may occur as potassium is excreted in preference to hydrogen ions. The, converse may occur in potassium depletion resulting in acid urine., Hypokalemia is very commonly associated with metabolic alkalosis. This is due to 2 factors: 1) the, common causes of metabolic alkalosis (vomiting, diuretics) directly induce H+ and K loss (via, aldosterone) and thus also cause hypokalemia and 2) hypokalemia is a very important cause of, metabolic alkalosis by three mechanisms. The initial effect is by causing a transcellular shift in which, K leaves and H+ enters the cells, thereby raising the extracellular pH. The second effect is by, causing a transcellular shift in the cells of the proximal tubules resulting in an intracellular acidosis,, which promotes ammonium production and excretion. Thirdly, in the presence of hypokalemia,, hydrogen secretion in the proximal and distal tubules increases. This leads to further reabsorption of, HCO3-. The net effect is an increase in the net acid excretion., Please rate this question:, , Discuss and give feedback, , Next question, , Hypokalaemia, Potassium and hydrogen can be thought of as competitors. Hyperkalaemia tends to be associated, with acidosis because as potassium levels rise fewer hydrogen ions can enter the cells, Hypokalaemia with alkalosis, , , , Vomiting, Diuretics
Page 393 :
A man is admitted after a period of prolonged self, induced starvation. Naso gastric feeding is, planned. Which of the following is least likely to occur?, , Hypokalaemia, , Increased risk of cardiac arrhythmias, , His haemoglobin will have decreased affinity for oxygen, , Hypophosphataemia, , Hypoalbuminaemia, , The process of starvation may lower DPG levels, in practice this is unlikely to occur early as it is, generated during glycolysis. Altered metabolism in starvation may be more acidotic and this would, also tend to impair oxygen carriage., Please rate this question:, , Discuss and give feedback, , Next question, , Nutrition - Refeeding syndrome, Refeeding syndrome describes the metabolic abnormalities which occur on feeding a person, following a period of starvation. The metabolic consequences include:, , , , , , Hypophosphataemia, Hypokalaemia, Hypomagnesaemia, Abnormal fluid balance, , These abnormalities can lead to organ failure., Re-feeding problems, If patient not eaten for > 5 days, aim to re-feed at < 50% energy and protein levels, High risk for re-feeding problems, If one or more of the following:, , , BMI < 16 kg/m 2
Page 394 :
, , , , Unintentional weight loss >15% over 3-6 months, Little nutritional intake > 10 days, Hypokalaemia, Hypophosphataemia or hypomagnesaemia prior to feeding (unless high), , If two or more of the following:, , , , , , BMI < 18.5 kg/m2, Unintentional weight loss > 10% over 3-6 months, Little nutritional intake > 5 days, History of: alcohol abuse, drug therapy including insulin, chemotherapy, diuretics and, antacids, , Prescription, , , , , Start at up to 10 kcal/kg/day increasing to full needs over 4-7 days, Start immediately before and during feeding: oral thiamine 200-300mg/day, vitamin B co, strong 1 tds and supplements, Give K+ (2-4 mmol/kg/day), phosphate (0.3-0.6 mmol/kg/day), magnesium (0.2-0.4, mmol/kg/day), Next question, , v
Page 395 :
Where does spironolactone act in the kidney?, , Glomerulus, , Proximal convoluted tubule, , Descending limb of the loop of Henle, , Ascending limb of the loop of Henle, , Distal convoluted tubule, , Please rate this question:, , Discuss and give feedback, , Next question, , Potassium sparing diuretics, Potassium-sparing diuretics may be divided into the epithelial sodium channel blockers (amiloride, and triamterene) and aldosterone antagonists (spironolactone and eplerenone)., {Amiloride} is a weak diuretic which blocks the epithelial sodium channel in the distal convoluted, tubule., Usually given with thiazides or loop diuretics as an alternative to potassium supplementation., {Spironolactone} is an aldosterone antagonist which acts act in the distal convoluted tubule., Indications, , , , , , ascites: patients with cirrhosis develop a secondary hyperaldosteronism. Relatively large, doses such as 100 or 200mg are often used, heart failure, nephrotic syndrome, Conn's syndrome, Next question
Page 396 :
Which receptor does noradrenaline mainly bind to?, , α 1 receptors, , α 2 receptors, , β 1 receptors, , β 2 receptors, , G receptors, , Theme from September 2015 Exam, Noradrenaline is the precursor of adrenaline. It is a powerful α 1 stimulant (although it will increase, myocardial contractility). Infusions will produce vasoconstriction and an increase in total peripheral, resistance. It is the inotrope of choice in septic shock., Please rate this question:, , Discuss and give feedback, , Next question, , Inotropes and cardiovascular receptors, Inotropes are a class of drugs which work primarily by increasing cardiac output. They should be, distinguished from vasoconstrictor drugs which are used specifically when the primary problem is, peripheral vasodilatation., Catecholamine type agents are commonly used and work by increasing cAMP levels by adenylate, cyclase stimulation. This in turn intracellular calcium ion mobilisation and thus the force of, contraction. Adrenaline works as a beta adrenergic receptor agonist at lower doses and an alpha, receptor agonist at higher doses. Dopamine causes dopamine receptor mediated renal and, mesenteric vascular dilatation and beta 1 receptor agonism at higher doses. This results in, increased cardiac output. Since both heart rate and blood pressure are raised, there is less overall
Page 398 :
Adult lung volumes. Which statement is false?, , In restrictive lung disease the FEV1/FVC ratio is increased, , Residual volume is increased in emphysema, , Functional residual capacity is measured by helium dilution test, , The tidal volume is approximately 340mls in females, , The vital capacity is increased in Guillain Barre syndrome, , FEV1/FVC is normal or >80% in restrictive lung disease such as pulmonary fibrosis. The ratio is, reduced in obstructive airways disease., The functional residual capacity, residual volume and the total lung capacity cannot be measured, with spirometry. They can only be measured by helium dilution., The vital capacity is reduced in:, 1. Pulmonary fibrosis/infiltration/oedema/effusions, 2. Weak respiratory muscles e.g. MG, GBS, myopathies, 3. Skeletal abnormalities e.g. chest wall abnormalities, Please rate this question:, , Discuss and give feedback, , Next question, , Lung volumes, The diagram demonstrates lung volumes and capacities
Page 399 :
Image sourced from Wikipedia, , Definitions, , Tidal volume (TV), , , , , Is the volume of air inspired and expired during each, ventilatory cycle at rest., It is normally 500mls in males and 340mls in females., , Inspiratory reserve, volume (IRV), , , , Is the maximum volume of air that can be forcibly inhaled, following a normal inspiration. 3000mls., , Expiratory reserve, volume (ERV), , , , Is the maximum volume of air that can be forcibly exhaled, following a normal expiration. 1000mls., , Residual volume (RV), , , , Is that volume of air remaining in the lungs after a maximal, expiration., RV = FRC - ERV. 1500mls., , , , Functional residual, capacity (FRC), , , , , Vital capacity (VC), , , , , Is the volume of air remaining in the lungs at the end of a, normal expiration., FRC = RV + ERV. 2500mls., Is the maximal volume of air that can be forcibly exhaled after, a maximal inspiration., VC = TV + IRV + ERV. 4500mls in males, 3500mls in, females.
Page 400 :
Total lung capacity, (TLC), , Forced vital capacity, (FVC), , , , , Is the volume of air in the lungs at the end of a maximal, inspiration., TLC = FRC + TV + IRV = VC + RV. 5500-6000mls., , , , The volume of air that can be maximally forcefully exhaled., Next question
Page 401 :
A 47 year old lady is diagnosed as suffering from a phaeochromocytoma. From which of the, following amino acids are catecholamines primarily derived?, , Aspartime, , Glutamine, , Arginine, , Tyrosine, , Alanine, , Catecholamine hormones are derived from tyrosine, it is modified by a DOPA decarboxylase, enzyme to become dopamine and thereafter via two further enzymic modifications to noradrenaline, and finally adrenaline., Please rate this question:, , Discuss and give feedback, , Next question, , Adrenal physiology, Adrenal medulla, The chromaffin cells of the adrenal medulla secrete the catecholamines noradrenaline and, adrenaline. The medulla is innervated by the splanchnic nerves; the preganglionic sympathetic fibres, secrete acetylcholine causing the chromaffin cells to secrete their contents by exocytosis., Phaeochromocytomas are derived from these cells and will secrete both adrenaline and nor, adrenaline., Adrenal cortex, Three histologically distinct zones are recognised:
Page 403 :
Theme: Events in wound healing, , A., B., C., D., E., F., , Platelets, Neutrophil polymorphs, Endothelial cells, Lymphocytes, Myofibroblasts, Granulomas, , Please select the dominant cell type present in a wound at the specified timeframe. Each option may, be used once, more than once or not at all., , 132., , 10 weeks following injury, You answered Platelets, The correct answer is Myofibroblasts, These differentiated cell types facilitate wound contraction., , 133., , 25 seconds following injury, You answered Neutrophil polymorphs, The correct answer is Platelets, Platelet degranulation and haemostasis are some of the earliest events in wound healing., , 134., , 7 days following injury, You answered Neutrophil polymorphs, The correct answer is Endothelial cells, Angiogenesis which is characterised by endothelial cell proliferation and microvessel, formation is a key step in successful wound healing. It is maximal between 1 and 2 weeks, following injury and wounds may have a reddish appearance during this time., , Please rate this question:, , Discuss and give feedback, , Next question
Page 404 :
Phases of wound healing, Phase, , Key features, , Cells, , Timeframe, , Haemostasis, , , , , Vasospasm in adjacent vessels, Platelet plug formation and, generation of fibrin rich clot, , Erythrocytes and, platelets, , Seconds/, Minutes, , Inflammation, , , , Neutrophils migrate into wound, (function impaired in diabetes)., Growth factors released, including, basic fibroblast growth factor and, vascular endothelial growth factor., Fibroblasts replicate within the, adjacent matrix and migrate into, wound., Macrophages and fibroblasts, couple matrix regeneration and clot, substitution., , Neutrophils,, fibroblasts and, macrophages, , Days, , Platelet derived growth factor and, transformation growth factors, stimulate fibroblasts and epithelial, cells., Fibroblasts produce a collagen, network., Angiogenesis occurs and wound, resembles granulation tissue., , Fibroblasts,, endothelial cells,, macrophages, , Weeks, , Longest phase of the healing, process and may last up to one year, (or longer)., During this phase fibroblasts, become differentiated, (myofibroblasts) and these, facilitate wound contraction., Collagen fibres are remodelled., Microvessels regress leaving a pale, scar., , Myofibroblasts, , 6 weeks to 1, year, , , , , , , , Regeneration, , , , , , , Remodelling, , , , , , , , , Next question
Page 405 :
Where are the arterial baroreceptors located?, , Carotid sinus and aortic arch, , Carotid sinus only, , Superior vena cava, , External carotid artery, , None of the above, , Theme from September 2015 Exam, They lie in the carotid sinus and aortic arch., Please rate this question:, , Discuss and give feedback, , Next question, , Cardiac physiology, , , , , , The heart has four chambers ejecting blood into both low pressure and high pressure, systems., The pumps generate pressures of between 0-25mmHg on the right side and 0-120 mmHg on, the left., At rest diastole comprises 2/3 of the cardiac cycle., The product of the frequency of heart rate and stroke volume combine to give the cardiac, output which is typically 5-6L per minute., , Detailed descriptions of the various waveforms are often not a feature of MRCS A (although they are, on the syllabus). However, they are a very popular topic for surgical physiology in the MRCS B, exam., Electrical properties, , , , Intrinsic myogenic rhythm within cardiac myocytes means that even the denervated heart is, capable of contraction., In the normal situation the cardiac impulse is generated in the sino atrial node in the right, atrium and conveyed to the ventricles via the atrioventricular node.
Page 406 :
, , , , The sino atrial node is also capable of spontaneous discharge and in the absence of, background vagal tone will typically discharge around 100x per minute. Hence the higher, resting heart rate found in cardiac transplant cases. In the SA and AV nodes the resting, membrane potential is lower than in surrounding cardiac cells and will slowly depolarise from, -70mV to around -50mV at which point an action potential is generated., Differences in the depolarisation slopes between SA and AV nodes help to explain why the, SA node will depolarise first. The cells have a refractory period during which they cannot be, re-stimulated and this period allows for adequate ventricular filling. In pathological, tachycardic states this time period is overridden and inadequate ventricular filling may then, occur, cardiac output falls and syncope may ensue., , Parasympathetic fibres project to the heart via the vagus and will release acetylcholine. Sympathetic, fibres release nor adrenaline and circulating adrenaline comes from the adrenal medulla., Noradrenaline binds to β 1 receptors in the SA node and increases the rate of pacemaker potential, depolarisation., Cardiac cycle, , Image sourced from Wikipedia, , , , Mid diastole: AV valves open. Ventricles hold 80% of final volume. Outflow valves shut., Aortic pressure is high., , , , Late diastole: Atria contract. Ventricles receive 20% to complete filling. Typical end diastolic, volume 130-160ml.
Page 407 :
, , Early systole: AV valves shut. Ventricular pressure rises. Isovolumetric ventricular, contraction. AV Valves bulge into atria (c-wave). Aortic and pulmonary pressure exceededblood is ejected. Shortening of ventricles pulls atria downwards and drops intra atrial, pressure (x-descent)., , , , Late systole: Ventricular muscles relax and ventricular pressures drop. Although ventricular, pressure drops the aortic pressure remains constant owing to peripheral vascular resistance, and elastic property of the aorta. Brief period of retrograde flow that occurs in aortic recoil, shuts the aortic valve. Ventricles will contain 60ml end systolic volume. The average stroke, volume is 70ml (i.e. Volume ejected)., , , , Early diastole: All valves are closed. Isovolumetric ventricular relaxation occurs. Pressure, wave associated with closure of the aortic valve increases aortic pressure. The pressure dip, before this rise can be seen on arterial waveforms and is called the incisura. During systole, the atrial pressure increases such that it is now above zero (v- wave). Eventually atrial, pressure exceed ventricular pressure and AV valves open - atria empty passively into, ventricles and atrial pressure falls (y -descent ), , The negative atrial pressures are of clinical importance as they can allow air embolization to occur if, the neck veins are exposed to air. This patient positioning is important in head and neck surgery to, avoid this occurrence if veins are inadvertently cut, or during CVP line insertion., Mechanical properties, , , , Preload = end diastolic volume, Afterload = aortic pressure, , It is important to understand the principles of Laplace's law in surgery., , , , , It states that for hollow organs with a circular cross section, the total circumferential wall, tension depends upon the circumference of the wall, multiplied by the thickness of the wall, and on the wall tension., The total luminal pressure depends upon the cross sectional area of the lumen and the, transmural pressure. Transmural pressure is the internal pressure minus external pressure, and at equilibrium the total pressure must counterbalance each other., In terms of cardiac physiology the law explains that the rise in ventricular pressure that, occurs during the ejection phase is due to physical change in heart size. It also explains why, a dilated diseased heart will have impaired systolic function.
Page 408 :
Starlings law, , , , Increase in end diastolic volume will produce larger stroke volume., This occurs up to a point beyond which cardiac fibres are excessively stretched and stroke, volume will fall once more. It is important for the regulation of cardiac output in cardiac, transplant patients who need to increase their cardiac output., , Baroreceptor reflexes, , , , , , , Baroreceptors located in aortic arch and carotid sinus., Aortic baroreceptor impulses travel via the vagus and from the carotid via the, glossopharyngeal nerve., They are stimulated by arterial stretch., Even at normal blood pressures they are tonically active., Increase in baroreceptor discharge causes:, , *Increased parasympathetic discharge to the SA node., *Decreased sympathetic discharge to ventricular muscle causing decreased contractility and fall in, stroke volume., *Decreased sympathetic discharge to venous system causing increased compliance., *Decreased peripheral arterial vascular resistance, Atrial stretch receptors, , , , , , , , Located in atria at junction between pulmonary veins and vena cava., Stimulated by atrial stretch and are thus low pressure sensors., Increased blood volume will cause increased parasympathetic activity., Very rapid infusion of blood will result in increase in heart rate mediated via atrial receptors:, theBainbridge reflex., Decreases in receptor stimulation results in increased sympathetic activity this will decrease, renal blood flow-decreases GFR-decreases urinary sodium excretion-renin secretion by, juxtaglomerular apparatus-Increase in angiotensin II., Increased atrial stretch will also result in increased release of atrial natriuretic peptide., Next question
Page 409 :
Which one of the following cells secretes the majority of tumour necrosis factor in humans?, , Neutrophils, , Macrophages, , Natural killer cells, , Killer-T cells, , Helper-T cells, , Please rate this question:, , Discuss and give feedback, , Next question, , Tumour necrosis factor, Tumour necrosis factor (TNF) is a pro-inflammatory cytokine with multiple roles in the immune, system, TNF is secreted mainly by macrophages and has a number of effects on the immune system, acting, mainly in a paracrine fashion:, , , , , , , activates macrophages and neutrophils, acts as costimulator for T cell activation, key mediator of bodies response to Gram negative septicaemia, similar properties to IL-1, anti-tumour effect (e.g. phospholipase activation), , TNF-alpha binds to both the p55 and p75 receptor. These receptors can induce apoptosis. It also, cause activation of NFkB, Endothelial effects include increase expression of selectins and increased production of platelet, activating factor, IL-1 and prostaglandins, TNF promotes the proliferation of fibroblasts and their production of protease and collagenase. It is, thought fragments of receptors act as binding points in serum
Page 410 :
Systemic effects include pyrexia, increased acute phase proteins and disordered metabolism leading, to cachexia, TNF is important in the pathogenesis of rheumatoid arthritis - TNF blockers (e.g. infliximab,, etanercept) are now licensed for treatment of severe rheumatoid, Next question
Page 411 :
Which of the following is responsible for the rapid depolarisation phase of the myocardial action, potential?, , Rapid sodium influx, , Rapid sodium efflux, , Slow efflux of calcium, , Efflux of potassium, , Rapid calcium influx, , Please rate this question:, , Discuss and give feedback, , Next question, , Electrical activity of the heart, Myocardial action potential, , Phase, , Description, , Mechanism, , 0, , Rapid depolarisation, , Rapid sodium influx, These channels automatically deactivate after a few ms, , 1, , Early repolarisation, , Efflux of potassium
Page 412 :
Phase, , Description, , Mechanism, , 2, , Plateau, , Slow influx of calcium, , 3, , Final repolarisation, , Efflux of potassium, , 4, , Restoration of ionic, concentrations, , Resting potential is restored by Na+/K+ ATPase, There is slow entry of Na+ into the cell decreasing the potential, difference until the threshold potential is reached, triggering a new, action potential, , NB cardiac muscle remains contracted 10-15 times longer than skeletal muscle, Conduction velocity, , Atrial conduction, , Spreads along ordinary atrial myocardial fibres at 1 m/sec, , AV node, conduction, , 0.05 m/sec, , Ventricular, conduction, , Purkinje fibres are of large diameter and achieve velocities of 2-4 m/sec (this allows a, rapid and coordinated contraction of the ventricles, Next question
Page 413 :
Which of the following is not a feature of normal cerebrospinal fluid?, , It has a pressure of between 10 and 15 mmHg., , It usually contains a small amount of glucose., , It may normally contain up to 5 red blood cells per mm3., , It may normally contain up to 3 white blood cells per mm3., , None of the above, , It should not contain red blood cells., Please rate this question:, , Discuss and give feedback, , Next question, , Cerebrospinal fluid, The CSF fills the space between the arachnoid mater and pia mater (covering surface of the brain)., The total volume of CSF in the brain is approximately 150ml. Approximately 500 ml is produced by, the ependymal cells in the choroid plexus (70%), or blood vessels (30%). It is reabsorbed via the, arachnoid granulations which project into the venous sinuses., Circulation, 1. Lateral ventricles (via foramen of Munro), 2. 3rd ventricle, 3. Cerebral aqueduct (aqueduct of Sylvius), 4. 4th ventricle (via foramina of Magendie and Luschka), 5. Subarachnoid space, 6. Reabsorbed into the venous system via arachnoid granulations into superior sagittal sinus, Composition, , , , , , Glucose: 50-80mg/dl, Protein: 15-40 mg/dl, Red blood cells: Nil, White blood cells: 0-3 cells/ mm3, Next question
Page 414 :
Which of the following is not an effect of somatostatin?, , It stimulates pancreatic acinar cells to release lipase, , It decreases gastric acid secretion, , It deceases gastrin release, , It decreases pepsin secretion, , It decreases glucagon release, , It inhibits pancreatic enzyme secretion., Please rate this question:, , Discuss and give feedback, , Gastric secretions, A working knowledge of gastric secretions is important for surgery because peptic ulcers are, common, surgeons frequently prescribe anti secretory drugs and because there are still patients, around who will have undergone acid lowering procedures (Vagotomy) in the past., Gastric acid, , , , , , Is produced by the parietal cells in the stomach, pH of gastric acid is around 2 with acidity being maintained by the H +/K+ ATP ase pump. As, part of the process bicarbonate ions will be secreted into the surrounding vessels., Sodium and chloride ions are actively secreted from the parietal cell into the canaliculus., This sets up a negative potential across the membrane and as a result sodium and, potassium ions diffuse across into the canaliculus., Carbonic anhydrase forms carbonic acid which dissociates and the hydrogen ions formed by, dissociation leave the cell via the H+/K+ antiporter pump. At the same time sodium ions are, actively absorbed. This leaves hydrogen and chloride ions in the canaliculus these mix and, are secreted into the lumen of the oxyntic gland., , This is illustrated diagrammatically below:
Page 415 :
Image sourced from Wikipedia, , Phases of gastric acid secretion, There are 3 phases of gastric secretion:, 1. Cephalic phase (smell / taste of food), , , , 30% acid produced, Vagal cholinergic stimulation causing secretion of HCL and gastrin release from G cells, , 2. Gastric phase (distension of stomach ), , , , 60% acid produced, Stomach distension/low H+/peptides causes Gastrin release, , 3. Intestinal phase (food in duodenum)
Page 416 :
, , , 10% acid produced, High acidity/distension/hypertonic solutions in the duodenum inhibits gastric acid secretion, via enterogastrones (CCK, secretin) and neural reflexes., , Regulation of gastric acid production, Factors increasing production include:, , , , , Vagal nerve stimulation, Gastrin release, Histamine release (indirectly following gastrin release) from enterchromaffin like cells, , Factors decreasing production include:, , , , , Somatostatin (inhibits histamine release), Cholecystokinin, Secretin, , The diagram below illustrates some of the factors involved in regulating gastric acid secretion and, the relevant associated pharmacology, , Image sourced from Wikipedia, , Below is a brief summary of the major hormones involved in food digestion:, , Source, , Stimulus, , Actions
Page 417 :
Gastrin, , G cells in, antrum of the, stomach, , Distension of, stomach, extrinsic, nerves, Inhibited by: low, antral pH,, somatostatin, , Increase HCL, pepsinogen and IF secretion,, increases gastric motility, trophic effect on, gastric mucosa, , CCK, , I cells in, upper small, intestine, , Partially digested, proteins and, triglycerides, , Increases secretion of enzyme-rich fluid, from pancreas, contraction of gallbladder, and relaxation of sphincter of Oddi,, decreases gastric emptying, trophic effect on, pancreatic acinar cells, induces satiety, , Secretin, , S cells in, upper small, intestine, , Acidic chyme,, fatty acids, , Increases secretion of bicarbonate-rich fluid, from pancreas and hepatic duct cells,, decreases gastric acid secretion, trophic, effect on pancreatic acinar cells, , VIP, , Small, intestine,, pancreas, , Neural, , Stimulates secretion by pancreas and, intestines, inhibits acid and pepsinogen, secretion, , Somatostatin, , D cells in the, pancreas and, stomach, , Fat, bile salts and, glucose in the, intestinal lumen, , Decreases acid and pepsin secretion,, decreases gastrin secretion, decreases, pancreatic enzyme secretion, decreases, insulin and glucagon secretion, inhibits trophic effects of gastrin, stimulates, gastric mucous production
Page 419 :
Question 1 of 347, A 40 year old women presented with a mass on her forehead. On examination, she had a fluctuant, pulsatile mass on her head. Examination of her neck revealed a mass inferior to the hyoid with a, positive Berry's sign. What is the most likely underlying diagnosis?, , Follicular thyroid cancer, , Medullary thyroid cancer, , Papillary thyroid cancer, , Anaplastic thyroid cancer, , Parathyroid gland cancer, Berrys sign= Absence of carotid pulse due to malignant thyromegaly., Theme from April 2013 Exam, Papillary thyroid cancers will tend to spread via lymphatics and present with disease that is nearly, always confined to the neck. Follicular carcinomas may metastasise haematogenously and the skull, may be the presenting site of disease in between 2 and 8% of patients., Please rate this question:, , Discuss and give feedback, , Next question, , Thyroid malignancy, Papillary carcinoma, , , , , , Commonest sub-type, Accurately diagnosed on fine needle aspiration cytology, Histologically, they may demonstrate psammoma bodies (areas of calcification) and so, called 'orphan Annie' nuclei, They typically metastasise via the lymphatics and thus laterally located apparently ectopic, thyroid tissue is usually a metastasis from a well differentiated papillary carcinoma
Page 420 :
Follicular carcinoma, , , , , , Are less common than papillary lesions, Like papillary tumours, they may present as a discrete nodule. Although they appear to be, well encapsulated macroscopically there is invasion on microscopic evaluation, Lymph node metastases are uncommon and these tumours tend to spread, haematogenously. This translates into a higher mortality rate, Follicular lesions cannot be accurately diagnosed on fine needle aspiration cytology and thus, all follicular FNA's (THY 3f) will require at least a hemi thyroidectomy, , Anaplastic carcinoma, , , , Less common and tend to occur in elderly females, Disease is usually advanced at presentation and often only palliative decompression and, radiotherapy can be offered., , Medullary carcinoma, , , , , , These are tumours of the parafollicular cells ( C Cells) and are of neural crest origin., The serum calcitonin may be elevated which is of use when monitoring for recurrence., They may be familial and occur as part of the MEN -2A disease spectrum., Spread may be either lymphatic or haematogenous and as these tumours are not derived, primarily from thyroid cells they are not responsive to radioiodine., , Lymphoma, , , , These respond well to radiotherapy, Radical surgery is unnecessary once the disease has been diagnosed on biopsy material., Such biopsy material is not generated by an FNA and thus a core biopsy has to be obtained, (with care!)., Next question
Page 421 :
Question 2 of 347, What is the most common cause of mesenteric infarction?, , Mesenteric vein thrombosis, , Acute embolism affecting the superior mesenteric artery, , Acute on chronic thrombus of the superior mesenteric artery, , Sub intimal dissection of the superior mesenteric artery, , Proximal migration of abdominal aortic aneurysm, , Theme from January 2013 Exam, Acute embolic events account for up to 50% of cases of mesenteric infarcts. These may occur as a, result of long standing atrial fibrillation, ventricular anuerysms and post myocardial infarction., Please rate this question:, , Discuss and give feedback, , Next question, , Mesenteric vessel disease, Mesenteric ischaemia accounts for 1 in 1000 acute surgical admissions. It is primarily caused by, arterial embolism resulting in infarction of the colon. It is more likely to occur in areas such as the, splenic flexure that are located at the borders of the territory supplied by the superior and inferior, mesenteric arteries., Types, , Acute mesenteric, embolus, (commonest 50%), , , , , , , Sudden onset abdominal pain followed by profuse diarrhoea., May be associated with vomiting., Rapid clinical deterioration., Serological tests: WCC, lactate, amylase may all be abnormal, particularly in established disease. These can be normal in the early, phases., , Acute on chronic, , , , Usually longer prodromal history.
Page 422 :
mesenteric, ischaemia, , , , , , Mesenteric vein, thrombosis, , , , , , Low flow, mesenteric, infarction, , , , , , Post prandial abdominal discomfort and weight loss are dominant, features. Patients will usually present with an acute on chronic, event, but otherwise will tend not to present until mesenteric flow is, reduced by greater than 80%., When acute thrombosis occurs presentation may be as above. In the, chronic setting the symptoms will often be those of ischaemic, colitis (mucosa is the most sensitive area to this insult)., Usually a history over weeks., Overt abdominal signs and symptoms will not occur until venous, thrombosis has reached a stage to compromise arterial inflow., Thrombophilia accounts for 60% of cases., This occurs in patients with multiple co morbidities in whom, mesenteric perfusion is significantly compromised by overuse of, inotropes or background cardiovascular compromise., The end result is that the bowel is not adequately perfused and, infarcts occur from the mucosa outwards., , Diagnosis, , , , , , Serological tests: WCC, lactate, CRP, amylase (can be normal in early disease)., Cornerstone for diagnosis of arterial AND venous mesenteric disease is CT angiography, scanning in the arterial phase with thin slices (<5mm). Venous phase contrast is not helpful., SMA duplex USS is useful in the evaluation of proximal SMA disease in patients with chronic, mesenteric ischaemia., MRI is of limited use due to gut peristalsis and movement artefact., , Management, , , , , Overt signs of peritonism: Laparotomy, Mesenteric vein thrombosis: If no peritonism: Medical management with IV heparin, At operation limited resection of frankly necrotic bowel with view to relook laparotomy at 2448h. In the interim urgent bowel revascularisation via endovascular (preferred) or surgery., , Prognosis, Overall poor. Best outlook is from an acute ischaemia from an embolic event where surgery occurs, within 12h. Survival may be 50%. This falls to 30% with treatment delay. The other conditions carry, worse survival figures., Next question, Question 3 of 347
Page 423 :
Which of the following events is most classically seen in the arterioles of patients with malignant, hypertension?, , Caseous necrosis, , Coagulative necrosis, , Fibrinoid necrosis, , Apoptosis, , Colliquative necrosis, Fibrinoid necrosis is seen in the arterioles of patients with malignant hypertension., Please rate this question:, , Discuss and give feedback, , Next question, , Cell death, Cells can die via two mechanisms; necrosis and apoptosis. These are outlined below:, Necrosis, Necrosis is characterised by bioenergetics failure. Loss of tissue perfusion results in hypoxia and an, inability to generate ATP. The integrity of the cellular membrane is lost and the loss of ATP results in, loss of energy dependent cellular transport mechanisms. There is an influx of water, ionic instability, and cellular lysis. The release of intracellular contents may stimulate an inflammatory response., Several types of necrosis are recognised; coagulative, colliquative, caseous, gangrene, fibrinoid and, fat necrosis. The type of tissue and the underlying cause determine the predominant necrosis, pattern., Coagulative necrosis, , , , , , The commonest type, occurs in most organs, Tissue is initially firm, later becomes soft as tissue is digested by macrophages, In the early phases the histological appearances may demonstrate little change, In later stages cellular outlines are seen with loss of intracellular detail
Page 424 :
Colliquative necrosis, , , , , Occurs in tissues with no supporting stroma, Dominant necrosis pattern in the CNS, Necrotic site may eventually become encysted, , Caseous necrosis, , , , , No definable structure seen in the necrotic tissue, Amorphous eosinophilic tissue may be seen histologically, Classically seen in tuberculosis, , Gangrene, , , , , , Necrosis with putrefaction of tissue, May complicate ischaemia, Haemoglobin degenerates and results in the deposition of iron sulphide (which is why the, tissue is black), Both wet and dry gangrene may occur, in wet gangrene there is often a liquefactive, component and super-added infection (which usually smells!), , Fibrinoid necrosis, , , , Classically seen in arterioles in patients with hypertension (malignant type), Necrosis of the smooth muscle wall occurs and plasma may extravasate into the media with, fibrin deposition, , Fat necrosis, , , , , Direct trauma to fat can result in rupture of adipocytes, Lipids incite a local inflammatory reaction, Inflammatory cells phagocytose the lipid with eventual fibrosis, , Apoptosis, , , , Also known as programmed cell death, Energy dependent pathways are activated via a number of intracellular signalling, mechanisms
Page 425 :
, , , , It is the result of the activation of caspases triggered by the bcl-2 family or the binding of the, FAS ligand to its receptor, DNA fragments, mitochondrial function ceases, nuclear and cellular shrinkage occurs, Phagocytosis of the cell does not occur, instead the cell degenerates into apoptotic bodies, Next question
Page 426 :
Question 4 of 347, A 38 year old lady presents with a recent episode of renal colic. As part of her investigations the, following results are obtained:, Corrected Calcium, , 3.84 mmol/l, , PTH, , 88pg/ml (increased), , Her serum urea and electrolytes are normal., What is the most likely diagnosis?, , Carcinoma of the bronchus, , Secondary hyperparathyroidism, , Primary hyperparathyroidism, , Tertiary hyperparathyroidism, , Carcinoma of the breast, , Theme from September 2012 exam, Theme from September 2011 exam, In this situation the most likely diagnosis is primary hyperparathyroidism. The question mentions that, serum urea and electrolytes are normal, which makes tertiary hyperparathyroidism unlikely., Please rate this question:, , Discuss and give feedback, , Next question, , Primary hyperparathyroidism, In exams, primary hyperparathyroidism is stereotypically seen in elderly females with an, unquenchable thirst and an inappropriately normal or raised parathyroid hormone level. It is most, commonly due to a solitary adenoma, Causes of primary hyperparathyroidism, , , , 80%: solitary adenoma, 15%: hyperplasia
Page 427 :
, , , 4%: multiple adenoma, 1%: carcinoma, , Features - 'bones, stones, abdominal groans and psychic moans', , , , , , , , Polydipsia, polyuria, Peptic ulceration/constipation/pancreatitis, Bone pain/fracture, Renal stones, Depression, Hypertension, , Associations, , , , Hypertension, Multiple endocrine neoplasia: MEN I and II, , Investigations, , , , , Raised calcium, low phosphate, PTH may be raised or normal, Technetium-MIBI subtraction scan, , Treatment, , , Parathyroidectomy, if imaging suggests target gland then a focused approach may be used, Next question
Page 428 :
Question 5 of 347, A 24 year old man is diagnosed as having Hodgkins lymphoma. Which subtype is associated with, the most favorable prognosis?, , Nodular sclerosing, , Lymphocyte depleted, , Nodular lymphocyte predominant, , Classical lymphocyte predominant, , Mixed cellularity, , Theme from September 2014 Exam, The classical lymphocyte predominant variant has the most favorable prognosis. Nodular, lymphocyte predominant disease is a very different disease entity and does not have the same, favorable prognosis., Please rate this question:, , Discuss and give feedback, , Next question, , Hodgkins lymphoma, Presenting features, , , , , Asymptomatic lympadenopathy, Cough, Pel Ebstein fever, haemoptysis, dyspnoea, B Symptoms - 10% weight loss, fever, night sweats, , Staging, All patients are staged with CT scanning of the chest, abdomen and pelvis, The Ann Arbor staging system is commonly used, , Stage, , Features
Page 429 :
Stage, , Features, , I, , Single lymph node region, , II, , Two or more regions on the same side of the diaphragm, , III, , Involvement of lymph node regions on both sides of the diaphragm, , IV, , Involvement of extra nodal sites, , Sub types, Classical Hodgkin lymphoma is classified into the following 4 types:, Nodular sclerosing Hodgkin lymphoma (NSHL), Mixed-cellularity Hodgkin lymphoma (MCHL), Lymphocyte-depleted Hodgkin lymphoma (LDHL), Lymphocyte-rich classical Hodgkin lymphoma (LRHL), A Reed Sternberg cell may be identified histologically., A fifth sub type, Nodular lymphocyte-predominant Hodgkin lymphoma, is characterised by a different, cell type Reed- Sternberg cells are rarely seen., Treatment, This may be multimodal and both chemo and radiotherapy are used., Diagnosis, This is made by excision of a complete lymph node that is then submitted for detailed histological, evaluation., Pathogenesis, Infection with Ebstein Barr virus is linked to the condition (particularly mixed cellularity lymphoma)., Prognosis, Stage I disease is associated with survival figures of up to 85% at 5 years. The lymphocyte rich, classical lymphoma has the best prognosis. Lymphocyte depleted Hodgkins lymphoma, advancing, age, male sex and stage IV disease are all associated with a worsening of prognosis., Next question
Page 430 :
Question 6-8 of 347, , Theme: Head and neck lumps, , A. Branchial cyst, B. Cystic hygroma, C. Carotid body tumour, D. Lymphadenopathy, E. Adenolymphoma of the parotid, F. Pleomorphic adenoma of the parotid, G. Submandibular tumour, H. Thyroglossal cyst, I. Thoracic outlet syndrome, J. Submandibular gland calculus, , Please select the most likely lesion to account for the clinical scenario given. Each option may be, used once, more than once or not at all., , 6., , A 60 year old Tibetan immigrant is referred to the surgical clinic with a painless neck swelling. On, examination, it is located on the left side immediately anterior to the sternocleidomastoid muscle., There are no other abnormalities to find., You answered Branchial cyst, The correct answer is Carotid body tumour, Carotid body tumours typically present as painless masses. They may compress the vagus or, hypoglossal nerves with symptoms attributable to these structures. Over 90% occur spontaneously, and are more common in people living at high altitude. In familial cases up to 30% may be bilateral., Treatment is with excision.
Page 431 :
7., , A 40 year old women presents as an emergency with a painful mass underneath her right, mandible. The mass has appeared over the previous week with the pain worsening as the lump has, increased in size. On examination, there is a 4cm mass underneath her mandible, there is no, associated lymphadenopathy., You answered Branchial cyst, The correct answer is Submandibular gland calculus, The sub mandibular gland is the most common site for salivary calculi. Patients will usually, complain of pain, which is worse on eating. When the lesion is located distally the duct may be laid, open and the stone excised. Otherwise the gland will require removal., , 8., , A 73 year old male smoker is referred to the clinic by his GP. On examination he has a 3cm soft, mass immediately anterior to his ear. It has been present for the past five years and is otherwise, associated with no symptoms., You answered Branchial cyst, The correct answer is Adenolymphoma of the parotid, Warthins tumours (a.k.a. adenolymphoma) are commoner in older men (especially smokers). They, are the second commonest benign tumour of the parotid gland, they may be bilateral. They are, soft and slow growing and relatively easy to excise. Pleomorphic adenomas typically present in, females aged between 40 - 60 years., , Please rate this question:, , Discuss and give feedback, , Next question, , Neck lumps
Page 432 :
The table below gives characteristic exam question features for conditions causing neck lumps:, , Reactive, lymphadenopathy, , By far the most common cause of neck swellings. There may be a history of, local infection or a generalised viral illness, , Lymphoma, , Rubbery, painless lymphadenopathy, The phenomenon of pain whilst drinking alcohol is very uncommon, There may be associated night sweats and splenomegaly, , Thyroid swelling, , May be hypo-, eu- or hyperthyroid symptomatically, Moves upwards on swallowing, , Thyroglossal cyst, , More common in patients < 20 years old, Usually midline, between the isthmus of the thyroid and the hyoid bone, Moves upwards with protrusion of the tongue, May be painful if infected, , Pharyngeal pouch, , More common in older men, Represents a posteromedial herniation between thyropharyngeus and, cricopharyngeus muscles, Usually not seen, but if large then a midline lump in the neck that gurgles on, palpation, Typical symptoms are dysphagia, regurgitation, aspiration and chronic cough, , Cystic hygroma, , A congenital lymphatic lesion (lymphangioma) typically found in the neck,, classically on the left side, Most are evident at birth, around 90% present before 2 years of age, , Branchial cyst, , An oval, mobile cystic mass that develops between the sternocleidomastoid, muscle and the pharynx, Develop due to failure of obliteration of the second branchial cleft in, embryonic development, Usually present in early adulthood
Page 433 :
Cervical rib, , More common in adult females, Around 10% develop thoracic outlet syndrome, , Carotid aneurysm, , Pulsatile lateral neck mass which doesn't move on swallowing, Next question
Page 434 :
Question 9 of 347, , A 12 year old child is admitted with a 12 hour history of colicky right upper quadrant pain. On, examination the child is afebrile and is jaundiced. The abdomen is soft and non tender at the time of, examination. What is the most likely cause?, , Infectious hepatitis, , Acute cholecystitis, , Cholangitis, , Hereditary spherocytosis, , Gilberts syndrome, Cholecystitis is unlikely in the absence of focal tenderness, , Theme from September 2012 Exam, The child is most likely to have hereditary spherocytosis. In these individuals there may be disease, flares precipitated by acute illness. They form small pigment stones. These may cause biliary colic, and some may require cholecystectomy., Gilbert's syndrome is an inherited condition causing unconjugated hyperbilirubinaemia. Patients may, have jaundice or be asymptomatic. The other LFTs are normal and Gilbert's may be confirmed with, a fasting test or Nicotinic acid test. There is no need for treatment as it is a benign condition., Please rate this question:, , Discuss and give feedback, , Next question, , Hereditary Spherocytosis
Page 435 :
Most common disorder of the red cell membrane, it has an incidence of 1 in 5000. The abnormally, shaped erythrocytes are prone to splenic sequestration and destruction. This can result in, hyperbilirubinaemia, jaundice and splenomegaly. In older patients an intercurrent illness may, increase the rate of red cell destruction resulting in more acute symptoms., Severe cases may benefit from splenectomy., Next question
Page 436 :
Question 10 of 347, A 28 year old man has a carcinoid tumour identified in his appendix. Blood testing for which of the, substances listed below is likely to be helpful during follow up?, , CA19-9, , Alkaline phosphatase, , AFP, , CEA, , Chromogranin A, , Theme from September 2013 Exam, It is important to distinguish between blood and urine tests for carcinoid syndrome. Blood tests, usually measure chromogranin A,neuron-specific enolase (NSE), substance P, and gastrin. Urine, tests usually measure 5 HIAA, which is a metabolite of serotonin. Sometimes blood tests for 5, hydroxytryptamine (serotonin) are also performed., Please rate this question:, , Discuss and give feedback, , Next question, , Carcinoid syndrome, , , , , , Carcinoid tumours secrete serotonin, Originate in neuroendocrine cells mainly in the intestine (midgut-distal ileum/appendix), Can occur in the rectum, bronchi, Hormonal symptoms mainly occur when disease spreads outside the bowel, , Clinical features, , , , , , , Onset: insidious over many years, Flushing face, Palpitations, Pulmonary valve stenosis and tricuspid regurgitation causing dyspnoea, Asthma
Page 437 :
, , Severe diarrhoea (secretory, persists despite fasting), , Investigation, , , , , , 5-HIAA in a 24-hour urine collection, Somatostatin receptor scintigraphy, CT scan, Blood testing for chromogranin A, , Treatment, , , , Octreotide, Surgical removal, Next question
Page 438 :
Question 11 of 347, , A 40 year old man presents with obstructive jaundice and dysphagia. Twenty years previously he, underwent a right hemicolectomy for a mucinous right sided colonic carcinoma. He was, subsequently diagnosed as having Lynch syndrome. A recent colonoscopy was normal. What is the, most likely cause of his jaundice?, , Hepatocellular carcinoma, , Liver metastasis from colonic cancer, , Pancreatic carcinoma, , Duodenal carcinoma, , Gastric carcinoma, , Theme from April 2013, Lynch syndrome usually results in colonic cancer which is right sided and mucinous. The next most, common site to be affected is the uterus. The stomach is at particular risk and this risk is up to 10, times greater in HNPCC (Lynch) patients than the general population. Duodenal adenomas (and, rarely carcinoma) are usually seen in association with FAP. Whilst pancreatic carcinoma is, associated with HNPCC it is far less likely to occur than gastric cancer., Please rate this question:, , Discuss and give feedback, , Next question, , Genetics of colorectal cancer, The lifetime risk of colorectal cancer in the UK population is 5%. Up to 5% of newly diagnosed bowel, cancers will be in those individuals who have a high genetically acquired risk of bowel cancer.
Page 440 :
functions, the best-established role for APC in the cancer process is as a major binding partner and, regulator of the β- catenin protein in the so-called canonical or β- catenin dependent Wnt signaling, pathway., HNPCC (Lynch syndrome), HNPCC cancers differ from conventional tumours in a number of respects. In the colon the tumours, are more likely to be right sided, histologically they are more likely to be mucinous and have dense, lymphocytic infiltrates. To be diagnosed as having HNPCC individuals must show typically HNPCC, tumours in at least three individuals, (one of whom must be a first degree relative to the other two)., In at least two successive generations. At least one cancer must be diagnosed under the age of 50., FAP must be excluded and tumours should be verified by pathological identification (Amsterdam, criteria). The genetic changes in HNPCC stem primarily from microsatellite instability affecting DNA, mismatch repair genes. In HNPCC the mismatch repair genes most commonly implicated include;, MSH2 and MLH1 and these occur in up to 70% of people with HNPCC. The finding of microsatellite, instability is unusual in sporadic colorectal cancers. Approximately 60% of individuals who fulfill the, Amsterdam criteria will not be found to have evidence of mismatch repair gene defects on genetic, testing. The risk of developing colorectal cancer in those who have not demonstrated mutation of the, mis match repair genes is increased if they fulfill the Amsterdam criteria, but not, the extent that it is increased in those who fulfill the criteria AND have evidence of mis match repair, gene defects., KRAS Mutations, The RAS family of small G proteins act as molecular switches downstream of growth factor, receptors. KRAS and the other two members of the family; HRAS and NRAS, are the site of, mutation in approximately 40% of colorectal cancers. When adenomas are examined the proportion, of adenomas less than 1cm showing KRAS mutations was only 10% which contrasts with 50% in, those lesions greater than 1cm., p53 mutations, The p53 protein functions as a key transcriptional regulator of genes that encode proteins with, functions in cell-cycle checkpoints at the G1/S and G2/M boundaries, in promoting apoptosis, and in, restricting angiogenesis . As such, selection for p53 defects at the adenoma-carcinoma transition, may reflect the fact that stresses on tumor cells activate cell-cycle arrest, apoptotic, and, antiangiogenic pathways in cells with wild-type p53 function. Many colonic tumours will demonstrate, changes in the p53 gene that may facilitate tumour progression through from adenoma to, carcinoma., Cowden syndrome, Also known as multiple hamartoma syndrome. Rare autosomal dominant condition with incidence of, 1 in 200,000.. It is characterised by multiple mucocutaneous lesions, trichilemmomas, oral, papillomas and acral keratosis. Most often diagnosed in third decade of life. Breast carcinoma may, occur in up to 50% of patients and conditions such as fibrocystic disease of the breast may occur in, 75% of women. Thyroid disease occurs in 75% and may include malignancy. Endoscopic screening, will identify disease in up to 85% although the small bowel is rarely involved. There is a 15-20% risk, of developing colorectal cancer and regular colonoscopic screening from age 45 is recommended.
Page 441 :
Terminology, , Oncogene, , Oncogenes are genes which have the potential to induce cellular proliferation and avoid, apoptosis. Oncogene mutations are general gain of function and are therefore, dominant. Increased expression of oncogenes are found in most tumours, , Tumour, suppressor, gene, , These genes generally inhibit cellular proliferation or induce apoptosis. Mutations in, tumour suppressor genes are generally loss of function mutations, and are therefore, recessive. Mutations in both tumour suppressor gene alleles allow cells to proliferate, without restraint, , References, 1. Fearon, E.R. and B. Vogelstein, A genetic model for colorectal tumorigenesis. Cell, 1990. 61(5): p., 759-67., Next question
Page 442 :
Question 12-14 of 347, Theme: Breast disease, , A., B., C., D., E., F., G., H., , Tuberculosis, Actinomycosis, Duct ectasia, Fibroadenoma, Fat necrosis, Intraductal papilloma, Breast abscess, Breast cancer, , What is the most likely diagnosis for each scenario given? Each diagnosis may be used once, more, than once or not at all., , 12., , A 32 year old woman presents with a tender breast lump. She has a 2 month old child., Clinically there is a tender, fluctuant mass of the breast., You answered Tuberculosis, The correct answer is Breast abscess, Theme from January 2013 Exam, Theme from September 2011 Exam, This lady is likely to be breast feeding and is at risk of mastitis. This may lead to an, abscess if not treated. Staphylococcus aureus is usually the causative organism., , 13., , A 53 year old lady presents with a creamy nipple discharge. On examination she has, discharge originating from multiple ducts and associated nipple inversion., You answered Tuberculosis, The correct answer is Duct ectasia, Duct ectasia is common during the period of breast involution that occurs during the, menopausal period. As the ducts shorten they may contain insipiated material. The, discharge will often discharge from several ducts., , 14., , A 52 year old lady presents with an episode of nipple discharge. It is usually clear in, nature. On examination the discharge is seen to originate from a single duct and although it, appears clear, when the discharge is tested with a labstix it is shown to contain blood., Imaging and examination shows no obvious mass lesion.
Page 443 :
You answered Tuberculosis, The correct answer is Intraductal papilloma, Intraductal papilloma usually cause single duct discharge. The fluid is often clear, although, it may be blood stained. If the fluid is tested with a labstix (little point in routine practice), then it will usually contain small amounts of blood. A microdocechtomy may be, performed., Please rate this question:, , Discuss and give feedback, , Next question, , Non malignant breast disease, Duct ectasia, , , , , , Mammary duct ectasia may be seen in up to 25% of normal female breasts, Patients usually present with nipple discharge, which may be from single or multiple ducts, (usually present age >50 years), The discharge is often thick and green, Duct ectasia is a normal variant of breast involution and is not the same condition as, periductal mastitis, , Periductal mastitis, , , , , , Present at younger age than duct ectasia, May present with features of inflammation, abscess or mammary duct fistula, Strongly associated with smoking, Usually treated with antibiotics, abscess will require drainage, , Intraductal papilloma, , , , , Growth of papilloma in a single duct, Usually presents with clear or blood stained discharge originating from a single duct, No increase in risk of malignancy, , Breast abscess
Page 444 :
, , , , , , Lactational mastitis is common, Infection is usually with Staphylococcus aureus, On examination there is usually a tender fluctuant mass, Treatment is with antibiotics and ultrasound guided aspiration, Overlying skin necrosis is an indication for surgical debridement, which may be complicated, by the development of a subsequent mammary duct fistula., , Tuberculosis, , , , , , Rare in western countries, usually secondary TB, Affects women later in child bearing period, Chronic breast or axillary sinus is present in up to 50% cases, Diagnosis is by biopsy culture and histology, , Next question
Page 445 :
Question 15 of 347, A 34 year old woman who has previously undergone a colectomy for familial adenomatous polyposis, coli presents with a firm lesion at the inferior aspect of her rectus abdominis muscle. Which cell type, is most typically associated with such tumours?, , Myocytes, , Proliferation of apocrine glands, , Chondrocytes, , Lipoblasts, , Myofibroblasts, , Desmoid tumours would be the most likely differential here and consist of a clonal proliferation of, myofibroblasts., Please rate this question:, , Discuss and give feedback, , Next question, , Desmoid tumours, , , , , , , , , , Desmoid tumours are fibrous neoplasms arising from musculoaponeurotic structures. They, are typically contain clonal proliferations of myofibroblasts., They are usually firm overgrowths of tissue with a propensity to local infiltration., They occur in up to 15% of patients with familial adenomatous polyposis coli., Desmoid tumours usually show bi allelic APC mutations, They occur most commonly in women after childbirth in the rectus abdominis muscle., They are usually treated (regardless of site) by radical surgical resection, in some patients, radiotherapy and chemotherapy may be considered. The results of non surgical therapy is, inferior to surgical resection. In selected cases of abdominal desmoids a period of, observation may be preferred as some may spontaneously regress., Desmoids have a high tendency to local recurrence., , Desmoids consist of sheets of differentiated fibroblasts
Page 446 :
Image sourced from Wikipedia, , Next question
Page 447 :
Question 16 of 347, A 2 day old baby is noted to have voiding difficulties and on closer inspection is noted to have, hypospadias. Which of the following abnormalities is most commonly associated with the condition?, , Cryptorchidism, , Diaphragmatic hernia, , Ventricular - septal defect, , Bronchogenic cyst, , Atrial septal defect, , Theme from January 2012 Exam, Hypospadias most commonly occurs as an isolated disorder. Associated urological abnormalities, may be seen in up to 40% of infants, of these cryptorchidism is the most frequent (10%)., Please rate this question:, , Discuss and give feedback, , Next question, , Hypospadias, The urethral meatus opens on the ventral surface of the penis. There is also a ventral deficiency of, the foreskin. The urethral meatus may open more proximally in the more severe variants. However,, 75% of the openings are distally located. The incidence is 1 in 300 male births., Features include:, , , , , , , , Absent frenular artery, Ventrally opened glans, Skin tethering to hypoplastic urethra, Splayed columns of spongiosum tissue distal to the meatus, Deficiency of the foreskin ventrally
Page 448 :
Management:, , , , , , No routine cultural circumcisions, Urethroplasty, Penile reconstruction, , The foreskin is often utilised in the reconstructive process. In boys with very distal disease no, treatment may be needed., Next question
Page 449 :
Question 17-19 of 347, Theme: Liver lesions, , A., B., C., D., E., F., , Cystadenoma, Hydatid cyst, Amoebic abscess, Mesenchymal hamartoma, Liver cell adenoma, Cavernous haemangioma, , Please select the most likely lesion for the scenario given. Each option may be used once, more, than once or not at all., , 17., , A 38 year old lady presents with right upper quadrant pain and nausea. She is otherwise, well and her only medical therapy is the oral contraceptive pill which she has taken for, many years with no ill effects. Her liver function tests are normal. An ultrasound, examination demonstrates a hyperechoic well defined lesion in the left lobe of the liver, which measures 14 cm in diameter., You answered Cystadenoma, The correct answer is Cavernous haemangioma, Cavernous haemangioma often presents with vague symptoms and signs. They may grow, to considerable size. Liver function tests are usually normal. The lesions are typically well, defined and hyperechoic on ultrasound. A causative link between OCP use and, haemangiomata has yet to be established, but is possible., , 18., , A 37 year old lady presents with right upper quadrant pain and nausea. She is otherwise, well and her only medical therapy is the oral contraceptive pill which she has taken for, many years with no ill effects. Her liver function tests and serum alpha feto protein are, normal. An ultrasound examination demonstrates a 4cm non encapsulated lesion in the, right lobe of the liver which has a mixed echoity and heterogeneous texture., You answered Cystadenoma, The correct answer is Liver cell adenoma, Liver cell adenomas are linked to OCP use and 90% of patients with liver cell adenomas, have used the OCP. Liver function tests are often normal. The lesions will typically have a, mixed echoity and heterogeneous texture.
Page 450 :
19., , A 38 year old shepherd presents to the clinic with a 3 month history of malaise and right, upper quadrant pain. On examination he is mildly jaundiced. His liver function tests, demonstrate a mild elevation in bilirubin and transaminases, his full blood count shows an, elevated eosinophil level. An abdominal x-ray is performed by the senior house officer and, demonstrates a calcified lesion in the right upper quadrant of the abdomen., You answered Cystadenoma, The correct answer is Hydatid cyst, Similar theme in September 2011 Exam, Hyatid disease is more common in those who work with sheep or dogs. Liver function, tests may be abnormal and an eosinophilia is often present. Plain radiographs may reveal a, calcified cyst wall., , Please rate this question:, , Discuss and give feedback, , Next question, , Benign liver lesions, Benign liver lesions, , Haemangioma, , , , , , , , , Liver cell, adenoma, , , , , , , , , , Most common benign tumours of mesenchymal origin, Incidence in autopsy series is 8%, Cavernous haemangiomas may be enormous, Clinically they are reddish purple hypervascular lesions, Lesions are normally separated from normal liver by ring of fibrous, tissue, On ultrasound they are typically hyperechoic, 90% develop in women in their third to fifth decade, Linked to use of oral contraceptive pill, Lesions are usually solitary, They are usually sharply demarcated from normal liver although they, usually lack a fibrous capsule, On ultrasound the appearances are of mixed echoity and, heterogeneous texture. On CT most lesions are hypodense when, imaged prior to administration of IV contrast agents, In patients with haemorrhage or symptoms removal of the adenoma
Page 451 :
may be required, Mesenchymal, hamartomas, Liver abscess, , Congential and benign, usually present in infants. May compress normal liver, , , , , , Amoebic abscess, , , , , , , , , Hyatid cysts, , , , , , , , , , , , , Polycystic liver, disease, , , , , Biliary sepsis is a major predisposing factor, Structures drained by the portal venous system form the second largest, source, Common symptoms include fever, right upper quadrant pain. Jaundice, may be seen in 50%, Ultrasound will usually show a fluid filled cavity, hyperechoic walls, may be seen in chronic abscesses, Liver abscess is the most common extra intestinal manifestation of, amoebiasis, Between 75 and 90% lesions occur in the right lobe, Presenting complaints typically include fever and right upper quadrant, pain, Ultrasonography will usually show a fluid filled structure with poorly, defined boundaries, Aspiration yield sterile odourless fluid which has an anchovy paste, consistency, Treatment is with metronidazole, Seen in cases of Echinococcus infection, Typically an intense fibrotic reaction occurs around sites of infection, The cyst has no epithelial lining, Cysts are commonly unilocular and may grow to 20cm in size. The, cyst wall is thick and has an external laminated hilar membrane and an, internal enucleated germinal layer, Typically presents with malaise and right upper quadrant pain., Secondary bacterial infection occurs in 10%., Liver function tests are usually abnormal and eosinophilia is present in, 33% cases, Ultrasound may show septa and hyatid sand or daughter cysts., Percutaneous aspiration is contra indicated, Treatment is by sterilisation of the cyst with mebendazole and may be, followed by surgical resection. Hypertonic swabs are packed around, the cysts during surgery, Usually occurs in association with polycystic kidney disease, Autosomal dominant disorder
Page 452 :
Cystadenoma, , , , Symptoms may occur as a result of capsular stretch, , , , , , , Rare lesions with malignant potential, Usually solitary multiloculated lesions, Liver function tests usually normal, Ultrasonography typically shows a large anechoic, fluid filled area, with irregular margins. Internal echos may result from septa, Surgical resection is indicated in all cases, , , , Next question
Page 453 :
Question 20 of 347, A 5 year old boy presents to the clinic with short stature suggestive of achondroplasia. What is the, genetic basis of this condition?, , X linked defect, , Y linked defect, , YY linked defect, , Autosomal dominant defect, , Autosomal recessive defect, , Theme from April 2013 Exam, Theme from April 2014 exam, Achondroplasia usually occurs as a sporadic mutation. It is then transmitted in an autosomal, dominant fashion., Please rate this question:, , Discuss and give feedback, , Next question, , Achondroplasia, Achondroplasia is a common cause of dwarfism and is caused by defects in the fibroblast growth, factor receptor. In most cases (approximately 70%) it occurs as a sporadic mutation. The main risk, factor is advancing parental age at the time of conception. Once present it is typically inherited in an, autosomal dominant fashion., Radiological features, , , , , , , Large skull with narrow foramen magnum, Short, flattened intervertebral bodies, Narrow spinal canal, Horizontal acetabular roof, Broad, short metacarpals
Page 454 :
Treatment, There is no specific therapy. However, some individuals benefit from limb lengthening procedures., These usually involve application of Ilizarov frames and targeted bone fractures. A clearly defined, need and end point is the cornerstone of achieving success with such procedures., Next question
Page 455 :
Question 21 of 347, A 72 year old man presents with symptoms and signs of benign prostatic hyperplasia. Which of the, following structures is most likely to be enlarged?, , Posterior lobe of the prostate, , Median lobe of the prostate, , Right lateral lobe of the prostate, , Left lateral lobe of the prostate, , Anterior lobe of the prostate, , Carcinoma of the prostate typically occurs in the posterior lobe. The median lobe is usually enlarged, in BPH. The anterior lobe has little in the way of glandular tissue and is seldom enlarged., Please rate this question:, , Discuss and give feedback, , Next question, , Benign Prostatic Hyperplasia, Benign prostatic hyperplasia occurs via an increase in the epithelial and stromal cell numbers in the, peri-urethral zone of the prostate. BPH is very common and 90% of men aged over 80 will have at, least microscopic evidence of benign prostatic hyperplasia. The causes of BPH are still not well, understood, but the importance of androgens remains appreciated even if the exact role by which, they induce BPH is elusive., Presentation, The vast majority of men will present with lower urinary tract symptoms. These will typically be:, , , , , , , , , Poor flow, Nocturia, Hesitancy, Incomplete and double voiding, Terminal dribbling, Urgency
Page 456 :
, , Incontinence, , Investigation, , , , , , , Digital rectal examination to assess prostatic size and morphology., Urine dipstick for infections and haematuria., Uroflowmetry (a flow rate of >15ml/second helps to exclude BOO), Bladder pressure studies may help identify detrusor failure and whilst may not form part of, first line investigations should be included in those with atypical symptoms and prior to redo, surgery., Bladder scanning to demonstrate residual volumes. USS if high pressure chronic retention., , Management, , , , , , Lifestyle changes such as stopping smoking and altering fluid intake may help those with, mild symptoms., Medical therapy includes alpha blockers and 5 α reductase inhibitors. The former work, quickly on receptor zones located at the bladder neck. Cardiovascular side effects are well, documented. The latter work on testosterone metabolising enzymes. Although they have a, slower onset of action, the 5 α reductase inhibitors may prevent acute urinary retention., Surgical therapy includes transurethral resection of the prostate and is the treatment of, choice in those with severe symptoms and those who fail to respond to medical therapy., More tailored bladder neck incision procedures may be considered in those with small, prostates. Retrograde ejaculation may occur following surgery. The change in the type of, irrigation solutions used has helped to minimise the TURP syndrome of electrolyte, disturbances., Next question
Page 457 :
Question 22 of 347, A 38 year old man has been suffering from mechanical back pain for several years. One morning he, awakes from sleep and feels a sudden onset of pain in his back radiating down his left leg. Which of, the following events is most likely to account for his symptoms?, , Prolapse of inner annulus fibrosus, , Prolapse of outer annulus fibrosus, , Prolapse of nucleus pulposus, , Rupture of the ligamentum flavum, , None of the above, , Theme from 2009 Exam, Theme from September 2012 Exam, The symptoms would be most likely the result of intervertebral disk prolapse. In disk prolapse the, nucleus pulposus is the structure which usually herniates., Please rate this question:, , Discuss and give feedback, , Next question, , Intervertebral discs, , , , , , , , Consist of an outer annulus fibrosus and an inner nucleus pulposus., The anulus fibrosus consists of several layers of fibrocartilage., The nucleus pulposus contains loose fibres suspended in a mucoprotein gel with the, consistency of jelly. The nucleus of the disc acts as a shock absorber., Pressure on the disc causes posterior protrusion of the nucleus pulposus. Most commonly in, the lumbrosacral and lower cervical areas., The discs are separated by hyaline cartilage., There is one disc between each pair of vertebrae, except for C1/2 and the sacrococcygeal, vertebrae., Next question
Page 458 :
Question 23-25 of 347, Theme: Paediatric neck masses, , A., B., C., D., E., , Cystic hygroma, Thyroglossal cyst, Rhabdomyosarcoma, Branchial cyst, Dermoid cyst, , Please select the most likely underlying diagnosis for the situation that is described. Each option, may be used once, more than once, or not at all., , 23., , A 2 year old boy is brought to the clinic by his mother who has noticed that he has, developed a small mass. On examination; a small smooth cyst is identified which is, located above the hyoid bone. On ultrasound the lesion appears to be a heterogenous and, multiloculated mass., You answered Cystic hygroma, The correct answer is Dermoid cyst, Theme from September 2015 Exam, Dermoid cysts are usually multiloculated and heterogeneous. Most are located above the, hyoid, and their appearances on imaging differentiate them from thyroglossal cysts., , 24., , A 22 month old baby is brought to the clinic by her mother who is concerned that she has, developed a swelling in her neck. On examination; she has a soft lesion located in the, posterior triangle that transilluminates., Cystic hygroma, Cystic hygromas are soft and transilluminate. Most are located in the posterior triangle., , 25., , A 3 year old boy is brought to the clinic by his mother who has noticed a mass in his neck., On examination; he has a smooth mass located on the lateral aspect of his anterior triangle,, near to the angle of the mandible. On ultrasound; it has a fluid filled, anechoic,, appearance., You answered Cystic hygroma, The correct answer is Branchial cyst
Page 459 :
Branchial cysts are usually located laterally and derived from the second branchial cleft., Unless infection has occurred they will usually have an anechoic appearance on, ultrasound., Please rate this question:, , Discuss and give feedback, , Next question, , Neck Masses in Children, Thyroglossal cyst, , , , , , Branchial cyst, , , , , , , , Dermoids, , , , , , Located in the anterior triangle, usually in the midline and below, the hyoid (65% cases), Derived from remnants of the thyroglossal duct, Thin walled and anechoic on USS (echogenicity suggests, infection of cyst), Six branchial arches separated by branchial clefts, Incomplete obliteration of the branchial apparatus may result in, cysts, sinuses or fistulae, 75% of branchial cysts originate from the second branchial cleft, Usually located anterior to the sternocleidomastoid near the, angle of the mandible, Unless infected the fluid of the cyst has a similar consistency to, water and is anechoic on USS, Derived from pleuripotent stem cells and are located in the, midline, Most commonly in a suprahyoid location, They have heterogeneous appearances on imaging and contain, variable amounts of calcium and fat, , Thyroid gland, , , , True thyroid lesions are rare in children and usually represent, thyroglossal cysts or tumours like lymphoma, , Lymphatic, malformations, , , , , , Usually located posterior to the sternocleidomastoid, Cystic hygroma result from occlusion of lymphatic channels, The painless, fluid filled, lesions usually present prior to the age, of 2, They are often closely linked to surrounding structures and, ,
Page 460 :
, , Infantile, haemangioma, , , , , , , Lymphadenopathy, , , , , , surgical removal is difficult, They are typically hypoechoic on USS, May present in either triangle of the neck, Grow rapidly initially and then will often spontaneously regress, Plain x-rays will show a mass lesion, usually containing, calcified phleboliths, As involution occurs the fat content of the lesions increases, Located in either triangle of the neck, May be reactive or neoplastic, Generalised lymphadenopathy usually secondary to infection in, children (very common), Next question
Page 461 :
Question 26 of 347, A 34 year old man presents to the surgical clinic 8 months following a laparotomy for a ruptured, spleen. He complains of a nodule in the centre of his laparotomy wound. This is explored surgically, and a stitch granuloma is found and excised. From which of the following cell types do granulomata, arise?, , Polymorpho nucleocytes, , Plasma cells, , Reed- Sternberg cells, , Platelets, , Macrophages, Granulomas are organised collections of macrophages, Theme from 2011 Exam, Macrophages give origin to granulomas., Please rate this question:, , Discuss and give feedback, , Next question, , Chronic inflammation, Overview, Chronic inflammation may occur secondary to acute inflammation.In most cases chronic, inflammation occurs as a primary process. These may be broadly viewed as being one of three main, processes:, , , , , Persisting infection with certain organisms such as Mycobacterium tuberculosis which results, in delayed type hypersensitivity reactions and inflammation., Prolonged exposure to non-biodegradable substances such as silica or suture materials, which may induce an inflammatory response., Autoimmune conditions involving antibodies formed against host antigens.
Page 462 :
Acute vs. Chronic inflammation, , Acute inflammation, , Chronic inflammation, , Changes to existing vascular structure and increased, permeability of endothelial cells, , Angiogenesis predominates, , Infiltration of neutrophils, , Macrophages, plasma cells and, lymphocytes predominate, , Process may resolve with:, , Healing by fibrosis is the main result, , , , , , , , Suppuration, Complete resolution, Abscess formation, Progression to chronic inflammation, Healing by fibrosis, , Granulomatous inflammation, A granuloma consists of a microscopic aggregation of macrophages (with epithelial type, arrangement =epitheliod). Large giant cells may be found at the periphery of granulomas., Mediators, Growth factors released by activated macrophages include agents such as interferon and fibroblast, growth factor (plus many more). Some of these such as interferons may have systemic features, resulting in systemic symptoms and signs, which may be present in individuals with long standing, chronic inflammation., The finding of granulomas is pathognomonic of chronic inflammation, as illustrated in this biopsy, from a patient with colonic Crohns disease
Page 463 :
Image sourced from Wikipedia, , Next question
Page 464 :
Question 27 of 347, An unusually tall 43 year old lady presents to the surgical clinic with bilateral inguinal hernias. She, develops chest pain and collapses. As part of her investigations a chest x-ray shows evidence of, mediastinal widening. What is the most likely underlying diagnosis?, , Pulmonary embolus, , Aortic dissection, , Tietze syndrome, , Boerhaaves syndrome, , Myocardial infarct, , Theme from September 2015 Exam, Marfans syndrome may present with a variety of connective tissue disorders such as bilateral, inguinal hernia. They are at high risk of aortic dissection, as in this case., Please rate this question:, , Discuss and give feedback, , Next question, , Aortic dissection, , , , , , , More common than rupture of the abdominal aorta, 33% of patients die within the first 24 hours, and 50% die within 48 hours if no treatment, received, Associated with hypertension, Features of aortic dissection: tear in the intimal layer, followed by formation and propagation, of a subintimal hematoma. Cystic medial necrosis (Marfan's), Most common site of dissection: 90% occurring within 10 centimetres of the aortic valve, , Stanford Classification, , Type, , Location, , Treatment
Page 465 :
Type, , Location, , Treatment, , A, , Ascending aorta/ aortic root, , Surgery- aortic root replacement, , B, , Descending aorta, , Medical therapy with antihypertensives, , DeBakey classification, , Type, , Site affected, , I, , Ascending aorta, aortic arch, descending aorta, , II, , Ascending aorta only, , III, , Descending aorta distal to left subclavian artery, , Clinical features, , , , , , Tearing, sudden onset chest pain (painless 10%), Hypertension or Hypotension, A blood pressure difference (in each arm) greater than 20 mm Hg, Neurologic deficits (20%), , Investigations, , , , , , CXR: widened mediastinum, abnormal aortic knob, ring sign, deviation of the, trachea/oesophagus, CT angiography of the thoracic aorta, MRI angiography, Conventional angiography (now rarely used diagnostically), , Management, , , , , Beta-blockers: aim HR 60-80 bpm and systolic BP 100-120 mm Hg, For type A dissections the standard of care is aortic root replacement, Question 28 of 347
Page 466 :
, , , A 72 year old man has just undergone an emergency repair for a ruptured abdominal aortic, aneurysm. Pre operatively he was taking aspirin, clopidogrel and warfarin. Intra operatively, he received 5000 units of unfractionated heparin prior to application of the aortic cross, clamp. His blood results on admission to the critical care unit are as follows:, Full blood count, , Hb, , 8 g/dl, , Platelets, , 40 * 109/l, , WBC, , 7.1 * 109/l, , , , His fibrin degradation products are measured and found to be markedly elevated. Which of, the following accounts for these results?, , Anastomotic leak, , Disseminated intravascular coagulation, , Heparin induced thrombocytopenia, , Adverse effect of warfarin, , Adverse effects of antiplatelet agents, , , , , Theme from April 2012 Exam, The combination of low platelet counts and raised FDP in this setting make DIC the most, likely diagnosis., Please rate this question:, , , , , , Discuss and give feedback, , , , Next question
Page 467 :
, , Disseminated intravascular coagulation - Diagnosis, , , , Under homeostatic conditions, coagulation and fibrinolysis are coupled. The activation of the, coagulation cascade yields thrombin that converts fibrinogen to fibrin; the stable fibrin clot, being the final product of hemostasis. The fibrinolytic system breaks down fibrinogen and, fibrin. Activation of the fibrinolytic system generates plasmin (in the presence of thrombin),, which is responsible for the lysis of fibrin clots. The breakdown of fibrinogen and fibrin results, in polypeptides (fibrin degradation products). In a state of homeostasis, the presence of, plasmin is critical, as it is the central proteolytic enzyme of coagulation and is also necessary, for fibrinolysis., In DIC, the processes of coagulation and fibrinolysis are dysregulated, and the result is, widespread clotting with resultant bleeding. Regardless of the triggering event of DIC, once, initiated, the pathophysiology of DIC is similar in all conditions. One critical mediator of DIC is, the release of a transmembrane glycoprotein (tissue factor =TF). TF is present on the, surface of many cell types (including endothelial cells, macrophages, and monocytes) and is, not normally in contact with the general circulation, but is exposed to the circulation after, vascular damage. For example, TF is released in response to exposure to cytokines, (particularly interleukin 1), tumor necrosis factor, and endotoxin. This plays a major role in, the development of DIC in septic conditions. TF is also abundant in tissues of the lungs,, brain, and placenta. This helps to explain why DIC readily develops in patients with extensive, trauma. Upon activation, TF binds with coagulation factors that then triggers the extrinsic, pathway (via Factor VII) which subsequently triggers the intrinsic pathway (XII to XI to IX) of, coagulation., Diagnosis, Fibrin degradation products are often raised., , Disorder, , Prothrombin time, , APTT, , Bleeding, time, , Platelet, count, , Warfarin, administration, , Prolonged, , Normal, , Normal, , Normal, , Aspirin administration, , Normal, , Normal, , Prolonged, , Normal, , Heparin, , Often normal (may be, prolonged), , Prolonged, , Normal, , Normal
Page 469 :
Question 29 of 347, A 53 year old man from Hong Kong presents with symptoms of fatigue, weight loss and recurrent, epistaxis. Clinical examination reveals left sided cervical lymphadenopathy and oropharyngeal, examination reveals an ulcerated mass in the naso pharynx. Which of the following viral agents is, most commonly implicated in the development of this condition?, , Cytomegalovirus, , Epstein Barr virus, , Coxsackie virus, , Herpes simplex virus, , None of the above, Trotter's triad (diagnosis of nasopharyngeal carcinoma), , , , , Unilateral conductive hearing loss, Ipsilateral facial & ear pain, Ipsilateral paralysis of soft palate, , The clinical scenario is most typical for nasopharyngeal carcinoma. An association with previous, Epstein Barr Virus is well established. Infection with the other viruses listed is not a recognised risk, factor for the development of the condition., Please rate this question:, , Discuss and give feedback, , Next question, , Nasopharyngeal carcinoma, , , , , Squamous cell carcinoma of the nasopharynx, Rare in most parts of the world, apart from individuals from Southern China, Associated with Epstein Barr virus infection, , Presenting features
Page 470 :
Systemic, , Local, , Cervical lymphadenopathy, , Otalgia, , Unilateral serous otitis media, , Nasal obstruction, discharge and/ or epistaxis, , Cranial nerve palsies e.g. III-VI, , Imaging, Combined CT and MRI., Treatment, Radiotherapy is first line therapy., Next question
Page 471 :
Question 30 of 347, An 18 year old male presents with lethargy, night sweats and on examination is found to have left, supraclavicular lymphadenopathy. A surgical registrar performs a left supraclavicular lymph node, biopsy. The pathologist identifies Reed- Sternberg cells on the subsequent histology sections, what, is the most likely diagnosis?, , Metastatic gastric cancer, , Hodgkins lymphoma, , Non Hodgkins lymphoma, , Tuberculosis, , None of the above, , Reed-Sternberg cells are characteristic histological cell type found in Hodgkins disease., Please rate this question:, , Discuss and give feedback, , Next question, , Lymphadenopathy, , , , Lymphadenopathy in the neck, axillae, groins and abdomen, Need to note: solitary/multiple, defined/indistinct, hard/rubbery/soft, tender/painless, , Causes of lymphadenopathy, Mnemonic: Hodgkins disease, H aematological: Hodgkins lymphoma, NHL, Leukaemia, O ncological: metastases, D ermatopathic lympadenitis, G aucher's disease, K awasaki disease, I nfections: TB, glandular fever, Syphilis, N iemann Pick disease, S erum sickness
Page 473 :
Question 31 of 347, A 28 year old man develops an acute paronychia and subsequent spreading sepsis. The tissue, exudate has a higher protein content than normal tissue because?, , Breakdown of tissue cells release protein, , Capillary walls are more permeable, , Increased blood flow transports more protein into the area, , Intracapillary pressure is raised, , Plasma cells release gamma globulin, , The increased permeability allows the exudation of plasma proteins., Please rate this question:, , Discuss and give feedback, , Next question, , Acute inflammation, Inflammation is the reaction of the tissue elements to injury. Vascular changes occur, resulting in the, generation of a protein rich exudate. So long as the injury does not totally destroy the existing tissue, architecture, the episode may resolve with restoration of original tissue architecture., Vascular changes, , , , , , Vasodilation occurs and persists throughout the inflammatory phase., Inflammatory cells exit the circulation at the site of injury., The equilibrium that balances Starlings forces within capillary beds is disrupted and a protein, rich exudate will form as the vessel walls also become more permeable to proteins., The high fibrinogen content of the fluid may form a fibrin clot. This has several important, immunomodulatory functions., , Sequelae
Page 474 :
Resolution, , , , , Typically occurs with minimal initial injury, Stimulus removed and normal tissue architecture results, , Organisation, , , , , Delayed removal of exudate, Tissues undergo organisation and usually fibrosis, , Suppuration, , , , , Typically formation of an abscess or an empyema, Sequestration of large quantities of dead neutrophils, , Progression to chronic, inflammation, , , , , Coupled inflammatory and reparative activities, Usually occurs when initial infection or suppuration has, been inadequately managed, , Causes, , , , , , , Infections e.g. Viruses, exotoxins or endotoxins released by bacteria, Chemical agents, Physical agents e.g. Trauma, Hypersensitivity reactions, Tissue necrosis, , Presence of neutrophil polymorphs is a histological diagnostic feature of acute inflammation, Next question
Page 475 :
Question 32 of 347, A 40 year old man undergoes a complex appendicectomy and the wound fails to heal satisfactorily., The wound site itself is associated with multiple sinuses and fistulas. Pus is sent for microbiology, and shows gram positive organisms and sulphur granules. What is the most likely underlying, diagnosis?, , Infection with Staphylococcus aureus, , Infection with Bacteroides fragilis, , Actinomycosis, , Crohns disease, , Ulcerative colitis, , Theme from 2014 Exam, The presence of chronic sinuses together with gram positive organisms and sulphur granules is, highly suggestive of Actinomycosis. Crohns disease is associated with multiple fistulae, but not gram, positive organisms with sulphur granules., Please rate this question:, , Discuss and give feedback, , Next question, , Actinomycosis, Chronic, progressive granulomatous disease caused by filamentous gram positive anaerobic, bacteria from the Actinomycetaceae family., Actinomyces are commensal bacteria that become pathogenic when a mucosal barrier is breached., The disease most commonly occurs in the head and neck, although it may also occur in the, abdominal cavity and in the thorax., The mass will often enlarge across tissue planes with the formation of multiple sinus tracts., Abdominopelvic actinomycosis occurs most frequently in individuals that have had appendicitis, (65%) cases.
Page 476 :
Pathology, , , , , On histological examination gram positive organisms and evidence of sulphur granules., Sulphur granules are colonies of organisms that appear as round or oval basophilic masses., They are also seen in other conditions such as nocardiosis., , Treatment, , , , Long term antibiotic therapy usually with penicillin., Surgical resection is indicated for extensive necrotic tissue, non healing sinus tracts,, abscesses or where biopsy is needed to exclude malignancy., , References, Wong V, Turmezei T and Weston V. Actinomycosis. BMJ 2011;343d6099., Next question
Page 477 :
Question 33 of 347, , As a busy surgical trainee on the colorectal unit you are given the unenviable task of reviewing the, unit's histopathology results for colonic polyps. Which of the polyp types described below has the, greatest risk of malignant transformation?, , Hyperplastic polyp, , Tubular adenoma, , Villous adenoma, , Hamartomatous polyp, , Serrated polyp, , Villous adenomas carry the highest risk of malignant transformation. Hyperplastic polyps carry little, in the way of increased risk. Although, patients with hamartomatous polyp syndromes may have a, high risk of malignancy, the polyps themselves have little malignant potential., Please rate this question:, , Discuss and give feedback, , Next question, , Colonic polyps, Colonic Polyps, May occur in isolation, or greater numbers as part of the polyposis syndromes. In FAP greater than, 100 polyps are typically present. The risk of malignancy in association with adenomas is related to, size, and is the order of 10% in a 1cm adenoma. Isolated adenomas seldom give risk of symptoms, (unless large and distal). Distally sited villous lesions may produce mucous and if very large,, electrolyte disturbances may occur.
Page 478 :
Follow up of colonic polyps, , Group, , Features, , Action, , Low risk, , 1 or 2 adenomas less than 1cm, , No follow up or re-colonoscopy, at 5 years, , Moderate, risk, , 3 or 4 small adenomas or 1 adenoma greater than 1cm, , Re-scope at 3 years, , High risk, , More than 5 small adenomas or more than 3 with 1 of, them greater than 1cm, , Re scope at 1 year, , From Atkins and Saunders Gut 2002 51 (suppl V:V6-V9). It is important to stratify patients, appropriately and ensure that a complete colonoscopy with good views was performed., Segmental resection or complete colectomy should be considered when:, 1. Incomplete excision of malignant polyp, 2. Malignant sessile polyp, 3. Malignant pedunculated polyp with submucosal invasion, 4. Polyps with poorly differentiated carcinoma, 5. Familial polyposis coli, -Screening from teenager up to 40 years by 2 yearly sigmoidoscopy/colonoscopy, -Panproctocolectomy and Ileostomy or Restorative Panproctocolectomy., Rectal polypoidal lesions may be amenable to trans anal endoscopic microsurgery., References, Cairns S et al. Guidelines for colorectal cancer screening and surveillance in moderate and high risk, groups (update from 2002). Gut 2010;59:666-690., Next question
Page 479 :
Question 34 of 347, A 23 year old man presents to the surgical clinic with an inguinal hernia. On examination he has a, small direct hernia. However, you also notice that he has pigmented spots around his mouth, on his, palms and soles. In his history he underwent a reduction of an intussusception aged 12 years., Which of the following lesions is most likely to be identified if a colonoscopy were performed?, , Hamartomas, , Tubulovillous adenoma, , Colorectal cancer, , Crohns disease, , Hyperplastic polyps, , Theme from April 2014 Exam, He is most likely to have Peutz-Jeghers syndrome which is associated with Hamartomas., Please rate this question:, , Discuss and give feedback, , Next question, , Peutz-Jeghers syndrome, Peutz-Jeghers syndrome is an autosomal dominant condition characterised by numerous benign, hamartomatous polyps in the gastrointestinal tract. It is also associated with pigmented freckles on, the lips, face, palms and soles. Around 50% of patients will have died from a gastrointestinal tract, cancer by the age of 60 years., Genetics, , , , Autosomal dominant, Responsible gene encodes serine threonine kinase LKB1 or STK11, , Features
Page 480 :
, , , , , Hamartomatous polyps in GI tract (mainly small bowel), Pigmented lesions on lips, oral mucosa, face, palms and soles, Intestinal obstruction e.g. intussusception (which may lead to diagnosis), Gastrointestinal bleeding, , Management, , , Conservative unless complications develop, Next question
Page 481 :
Question 35 of 347, , A 56 year old surgeon has been successfully operating for many years. Over the past few weeks, she has begun to notice that her hands are becoming blistering and weepy. A latex allergy is, diagnosed. Which of the following pathological processes accounts for this scenario?, , Type 1 hypersensitivity reaction, , Type 2 hypersensitivity reaction, , Type 4 hypersensitivity reaction, , Type 3 hypersensitivity reaction, , None of the above, Hypersensitivity reactions: ACID, type 1 --Anaphylactic, type 2 --Cytotoxic, type 3 --Immune complex, type 4 --Delayed hypersensitivity, , Theme from 2012 Exam, Contact dermatitis of a chronic nature is an example of a type 4 hypersensitivity reaction. Type 4, hypersensitivity reactions are cell mediated rather than antibody mediated., Please rate this question:, , Discuss and give feedback, , Next question, , Hypersensitivity reactions
Page 483 :
Question 36 of 347, A 56 year old motorcyclist is involved in a road traffic accident and sustains a displaced femoral, shaft fracture. No other injuries are identified on the primary or secondary surveys. The fracture is, treated with closed, antegrade intramedullary nailing. The following day the patient becomes, increasingly agitated and confused. On examination he is pyrexial, hypoxic SaO 2 90% on 6 litres O2,, tachycardic and normotensive. Systemic examination demonstrates a non blanching petechial rash, present over the torso. What is the most likely explanation for this?, , Pulmonary embolism with paradoxical embolus, , Fat embolism, , Meningococcal sepsis, , Alcohol withdrawl, , Chronic sub dural haematoma, Triad of symptoms:, , , , , Respiratory, Neurological, Petechial rash (tends to occur after the first 2 symptoms), , Theme from April 2014 Exam, Theme from January 2015 Exam, This man has a recent injury and physical signs that would be concordant with fat embolism, syndrome. Meningococcal sepsis is not usually associated with hypoxia initially. Pulmonary emboli, are not typically associated with pyrexia., Please rate this question:, , Discuss and give feedback, , Next question, , Fat embolism, Diagnosis and clinical features
Page 484 :
System, , Feature, , Respiratory, , , , , , Early persistent tachycardia, Tachypnoea, dyspnoea, hypoxia usually 72 hours following injury, Pyrexia, , Dermatological, , , , , Red/ brown impalpable petechial rash (usually only in 25-50%), Subconjunctival and oral haemorrhage/ petechiae, , CNS, , , , , Confusion and agitation, Retinal haemorrhages and intra-arterial fat globules on fundoscopy, , Imaging, , , , May be normal, Fat emboli tend to lodge distally and therefore CTPA may not show any vascular occlusion, a, ground glass appearance may be seen at the periphery, , Treatment, , , , , , Prompt fixation of long bone fractures, Some debate regarding benefit Vs. risk of medullary reaming in femoral shaft/ tibial fractures, in terms of increasing risk (probably does not)., DVT prophylaxis, General supportive care, Next question
Page 485 :
Question 37 of 347, A 45 year old man has widespread metastatic adenocarcinoma of the colon. Which of the following, tumour markers is most likely to be elevated?, , CA19-9, , Carcinoembryonic antigen, , Alpha Feto Protein, , CA 125, , Beta HCG, Screening for colonic cancer using CEA is not justified, Carcinoembryonic antigen is elevated in colonic cancer, typically in relation to disease extent with, highest serum levels noted in metastatic disease. It is falsely elevated in a number of non-malignant, disease states such as cirrhosis and colitis and for this reason it has no role in monitoring colitics for, colonic cancer[1]., Reference, 1. Sturgeon, C.M., L.C. Lai, and M.J. Duffy. Serum tumour markers: how to order and interpret them., BMJ, 2009. 339: p. b3527., Please rate this question:, , Discuss and give feedback, , Next question, , Colorectal cancer screening and diagnosis, Overview, , , , , , Most cancers develop from adenomatous polyps. Screening for colorectal cancer has been, shown to reduce mortality by 16%, The NHS now has a national screening programme offering screening every 2 years to all, men and women aged 60 to 69 years. Patients aged over 70 years may request screening, Eligible patients are sent faecal occult blood (FOB) tests through the post, Patients with abnormal results are offered a colonoscopy
Page 486 :
At colonoscopy, approximately:, , , , , 5 out of 10 patients will have a normal exam, 4 out of 10 patients will be found to have polyps which may be removed due to their, premalignant potential, 1 out of 10 patients will be found to have cancer, , Diagnosis, Essentially the following patients need referral:, - Altered bowel habit for more than six weeks, - New onset of rectal bleeding, - Symptoms of tenesmus, Colonoscopy is the gold standard, provided it is complete and good mucosal visualisation is, achieved. Other options include double contrast barium enema and CT colonography., Staging, Once a malignant diagnosis is made patients with colonic cancer will be staged using chest /, abdomen and pelvic CT. Patients with rectal cancer will also undergo evaluation of the mesorectum, with pelvic MRI scanning., For examination purposes the Dukes and TNM systems are preferred., Tumour markers, Carcinoembryonic antigen (CEA) is the main tumour marker in colorectal cancer. Not all tumours, secrete this, and it may be raised in conditions such as IBD. However, absolute levels do correlate, (roughly) with disease burden and it is once again being used routinely in follow up., Next question
Page 487 :
Question 38 of 347, A 43 year old man presents with haemoptysis and is diagnosed as having tuberculosis. Which of the, cell types listed below will usually internalise the tubercule bacullis?, , Fibroblast, , Neutrophil, , Erythrocyte, , Macrophage, , Eosinophil, , Theme from January 2013 Exam, M. Tuberculosis will reside in macrophages where it will often survive, Please rate this question:, , Discuss and give feedback, , Next question, , Tuberculosis pathology, , , , , , , , Is a form of primary chronic inflammation, caused by the inability of macrophages to kill, theMycobacterium tuberculosis., The macrophages often migrate to regional lymph nodes, the lung lesion plus affected lymph, nodes is referred to as a Ghon complex., This leads to the formation of a granuloma which is a collection of epithelioid histiocytes., There is the presence of caseous necrosis in the centre., The inflammatory response is mediated by a type 4 hypersensitivity reaction., In healthy individuals the disease may be contained, in the immunocompromised, disseminated (miliary TB) may occur., , Diagnosis, , , , Waxy membrane of mycobacteria prevents binding with normal stains. Ziehl - Neelsen, staining is typically used., Culture based methods take far longer.
Page 488 :
Image showing acid- alcohol fast mycobacteria stained using the Ziehl- Neelsen method, , Image sourced from Wikipedia, , Next question
Page 489 :
Question 39 of 347, Which of these tumour markers is most helpful in identifying an individual with hepatocellular, carcinoma?, , Serum AFP, , Serum CA19-9, , CEA, , Beta HCG, , CA125, , Theme from April 2014 Exam, Hepatocellular carcinoma is commonly diagnosed with imaging and an elevated alpha fetoprotein., Biopsy may seed the tumour and should be avoided. Up to 80% of hepatocellular carcinoma arise in, cirrhotic livers., Please rate this question:, , Discuss and give feedback, , Next question, , Liver tumours, Primary liver tumours, The most common primary tumours are cholangiocarcinoma and hepatocellular carcinoma. Overall, metastatic disease accounts for 95% of all liver malignancies making the primary liver tumours, comparatively rare., Primary liver tumours include:, , , , , , , , Cholangiocarcinoma, Hepatocellular carcinoma, Hepatoblastoma, Sarcomas (Rare), Lymphomas, Carcinoids (most often secondary although primary may occur)
Page 490 :
Hepatocellular carcinoma, These account for the bulk of primary liver tumours (75% cases). Its worldwide incidence reflects its, propensity to occur on a background of chronic inflammatory activity. Most cases arise in cirrhotic, livers or those with chronic hepatitis B infection, especially where viral replication is actively, occurring. In the UK it accounts for less than 5% of all cancers, although in parts of Asia its, incidence is 100 per 100,000., The majority of patients (80%) present with existing liver cirrhosis, with a mass discovered on, screening ultrasound., Diagnosis, , , , , , CT/ MRI (usually both) are the imaging modalities of choice, a-fetoprotein is elevated in almost all cases, Biopsy should be avoided as it seeds tumours cells through a resection plane., In cases of diagnostic doubt serial CT and αFP measurements are the preferred strategy., , Treatment, , , , , , , Patients should be staged with liver MRI and chest, abdomen and pelvic CT scan., The testis should be examined in males (testicular tumours may cause raised AFP). PET CT, may be used to identify occult nodal disease., Surgical resection is the mainstay of treatment in operable cases. In patients with a small, primary tumour in a cirrhotic liver whose primary disease process is controlled, consideration, may be given to primary whole liver resection and transplantation., Liver resections are an option but since most cases occur in an already diseased liver the, operative risks and post-operative hepatic dysfunction are far greater than is seen following, metastectomy., These tumours are not particularly chemo or radiosensitive however, both may be used in a, palliative setting. Tumour ablation is a more popular strategy., , Survival, Poor, overall survival is 15% at 5 years., Cholangiocarcinoma, This is the second most common type of primary liver malignancy. As its name suggests these, tumours arise in the bile ducts. Up to 80% of tumours arise in the extra hepatic biliary tree. Most, patients present with jaundice and by this stage the majority will have disease that is not resectable., Primary sclerosing cholangitis is the main risk factor. In deprived countries typhoid and liver flukes, are also major risk factors., Diagnosis, , , , , Patients will typically have an obstructive picture on liver function tests., CA 19-9, CEA and CA 125 are often elevated, CT/ MRI and MRCP are the imaging methods of choice.
Page 491 :
Treatment, , , , Surgical resection offers the best chance of cure. Local invasion of peri hilar tumours is a, particular problem and this coupled with lobar atrophy will often contra indicate surgical, resection., Palliation of jaundice is important, although metallic stents should be avoided in those, considered for resection., , Survival, Is poor, approximately 5-10% 5 year survival., Next question
Page 492 :
Question 40 of 347, A 39 year old man has suffered from terminal ileal Crohns disease for the past 20 years. Which, condition is he least likely to develop?, , Gallstones, , Malabsorption, , Pyoderma gangrenosum, , Amyloidosis, , Feltys syndrome, Felteys syndrome:, , , , , Rheumatoid disease, Splenomegaly, Neutropenia, , Feltys syndrome is associated with rheumatoid disease. Individuals with long standing Crohns, disease are at risk of gallstones because of impairment of the enterohepatic recycling of bile salts., Formation of entero-enteric fistulation may produce malabsorption. Amyloidosis may complicate, chronic inflammatory states., Please rate this question:, , Discuss and give feedback, , Next question, , Crohns disease, Crohns disease is a chronic transmural inflammation of a segment(s) of the gastrointestinal tract and, may be associated with extra intestinal manifestations. Frequent disease patterns observed include, ileal, ileocolic and colonic disease. Peri-anal disease may occur in association with any of these. The, disease is often discontinuous in its distribution. Inflammation may cause ulceration, fissures, fistulas, and fibrosis with stricturing. Histology reveals a chronic inflammatory infiltrate that is usually patchy, and transmural., Ulcerative colitis Vs Crohns
Page 494 :
, , , , , Bile salt diarrhoea secondary to terminal ileal disease, Entero-colic fistula, Short bowel due to multiple resections, Bacterial overgrowth, , Surgical interventions in Crohns disease, The commonest disease pattern in Crohns is stricturing terminal ileal disease and this often, culminates in an ileocaecal resection. Other procedures performed include segmental small bowel, resections and stricturoplasty. Colonic involvement in patients with Crohns is not common and,, where found, distribution is often segmental. However, despite this distribution segmental resections, of the colon in patients with Crohns disease are generally not advocated because the recurrence, rate in the remaining colon is extremely high, as a result the standard options of colonic surgery in, Crohns patients are generally; sub total colectomy, panproctocolectomy and staged sub total, colectomy and proctectomy. Restorative procedures such as ileoanal pouch have no role in therapy., Crohns disease is notorious for the developmental of intestinal fistulae; these may form between the, rectum and skin (peri anal) or the small bowel and skin. Fistulation between loops of bowel may also, occur and result in bacterial overgrowth and malabsorption. Management of enterocutaneous, fistulae involves controlling sepsis, optimising nutrition, imaging the disease and planning definitive, surgical management., Next question
Page 495 :
Question 41 of 347, , A 23 year old women has undergone a pan proctocolectomy and ileoanal pouch because she, suffers from familial adenomatous polyposis coli. What is the commonest extra colonic lesion in this, disorder?, , Gastric fundal polyps, , Trichilemmomas, , Duodenal polyps, , Fibrocystic disease of the breast, , Skull osteomas, Duodenal polyps occur in up to 100% of patients with FAP if follow up is continued for long enough., Duodenal cancer has an incidence of 4-10%., , Theme from April 2014 exam, Duodenal polyps are the commonest extra colonic lesion in FAP. Gastric fundal polyps are seen in, 50% of patients. Skull osteomas are seen in Gardeners syndrome which is a variant of FAP., Please rate this question:, , Discuss and give feedback, , Next question, , Polyposis syndromes
Page 496 :
Screening and, management, , Associated, disorders, , Typically over 100, colonic adenomas, Cancer risk of 100%, 20% are new, mutations, , If known to be at risk, then predictive, genetic testing as, teenager, Annual flexible, sigmoidoscopy from, 15 years, If no polyps found, then 5 yearly, colonoscopy started, at age 20, Polyps found =, resectional surgery, (resection and pouch, Vs sub total, colectomy and IRA), , Gastric fundal, polyps (50%)., Duodenal polyps, 90%., If severe, duodenal, polyposis cancer, risk of 30% at 10, years., Abdominal, desmoid, tumours., , Biallelic mutation, of mut Y human, homologue (MYH), on chromosome, 1p, recessive, , Multiple colonic, polyps, Later onset right, sided cancers more, common than in FAP, 100% cancer risk by, age 60, , Once identified, resection and, ileoanal pouch, reconstruction is, recommended, Attenuated, phenotype - regular, colonoscopy, , Duodenal, polyposis in 30%, Associated with, increased risk of, breast cancer, (self examination), , STK11 (LKB1), mutation on, chromosome 19 in, some (but not all), cases, dominant, , Multiple benign, intestinal, hamartomas, Episodic obstruction, and intussceception, Increased risk of GI, cancers (colorectal, cancer 20%, gastric, 5%), , Annual examination, Pan intestinal, endoscopy every 2-3, years, , Malignancies at, other sites, Classical, pigmentation, pattern, , Syndrome, , Genetic defect, , Features, , Familial, adenomatous, polyposis, , Mutation of APC, gene (80%) cases,, dominant, , MYH, associated, polyposis, , Peutz -Jeghers, syndrome
Page 497 :
Syndrome, , Genetic defect, , Features, , Screening and, management, , Associated, disorders, , Increased risk of, breast, ovarian,, cervical pancreatic, and testicular, cancers, , Cowden, disease, , Mutation of PTEN, gene on, chromosome, 10q22, dominant, , Macrocephaly, Multiple intestinal, hamartomas, Multiple, trichilemmomas, 89% risk of cancer at, any site, 16% risk of colorectal, cancer, , Targeted, individualised, screening, , Breast cancer, (81% risk), Thyroid cancer, and non toxic, goitre, Uterine cancer, , HNPCC (Lynch, syndrome), , Germline, mutations of DNA, mismatch repair, genes, , Colo rectal cancer, 30-70%, Endometrial cancer, 30-70%, Gastric cancer 5-10%, Scanty colonic polyps, may be present, Colonic tumours, likely to be right, sided and mucinous, , Colonoscopy every 12 years from age 25, Consideration of, prophylactic surgery, Extra colonic, surveillance, recommended, , Extra colonic, cancers, , Next question
Page 498 :
Question 42-44 of 347, , Theme: Renal stones, , A. Calcium oxalate, B. Uric acid, C. Cystine, D. Struvite, E. Calcium phosphate, , Please select the most likely stone type for each of the following urinary tract stone scenarios. Each, option may be used once, more than once or not at all., , 42., , A 73 year old lady is undergoing chemotherapy for treatment of acute leukaemia. She develops, symptoms of renal colic. Her urine tests positive for blood. A KUB x-ray shows no evidence of, stones., You answered Calcium oxalate, The correct answer is Uric acid, Chemotherapy and cell death can increase uric acid levels. In this acute setting the uric acid, stones are unlikely to be coated with calcium and will therefore be radiolucent., , 43., , A 16 year old boy presents with renal colic. His parents both have a similar history of the, condition. His urine tests positive for blood. A KUB style x-ray shows a relatively radiodense stone, in the region of the mid ureter., You answered Calcium oxalate, The correct answer is Cystine
Page 499 :
Cystine stones are associated with an inherited metabolic disorder., , 44., , A 43 year old lady with episodes of recurrent urinary tract sepsis presents with a staghorn, calculus of the left kidney. Her urinary pH is 7.3. A KUB x-ray shows a faint outline of the calculus., You answered Calcium oxalate, The correct answer is Struvite, Theme from April 2012 Exam, Chronic infection with urease producing enzymes can produce an alkaline urine with formation of, struvite stone., , Please rate this question:, , Discuss and give feedback, , Next question, , Renal stones, Type of, stones, , Calcium, oxalate, , Features, , Hypercalciuria is a major risk factor (various causes), Hyperoxaluria may also increase risk, Hypocitraturia increases risk because citrate forms complexes with, calcium making it more soluble, Stones are radio-opaque (though less than calcium phosphate stones), Hyperuricosuria may cause uric acid stones to which calcium oxalate, binds, , Percentage of, all calculi, , 85%
Page 500 :
Type of, stones, , Percentage of, all calculi, , Features, , Cystine, , Inherited recessive disorder of transmembrane cystine transport, leading to decreased absorption of cystine from intestine and renal, tubule, Multiple stones may form, Relatively radiodense because they contain sulphur, , 1%, , Uric acid, , Uric acid is a product of purine metabolism, May precipitate when urinary pH low, May be caused by diseases with extensive tissue breakdown e.g., malignancy, More common in children with inborn errors of metabolism, Radiolucent, , 5-10%, , Calcium, phosphate, , May occur in renal tubular acidosis, high urinary pH increases, supersaturation of urine with calcium and phosphate, Renal tubular acidosis types 1 and 3 increase risk of stone formation, (types 2 and 4 do not), Radio-opaque stones (composition similar to bone), , 10%, , Struvite, , Stones formed from magnesium, ammonium and phosphate, Occur as a result of urease producing bacteria (and are thus, associated with chronic infections), Under the alkaline conditions produced, the crystals can precipitate, Slightly radio-opaque, , 2-20%, , Effect of urinary pH on stone formation, Urine pH will show individual variation (from pH 5-7). Post prandially the pH falls as purine, metabolism will produce uric acid. Then the urine becomes more alkaline (alkaline tide). When the, stone is not available for analysis the pH of urine may help to determine which stone was present., , Stone type, , Urine acidity, , Mean urine pH
Page 501 :
Stone type, , Urine acidity, , Mean urine pH, , Calcium phosphate, , Normal- alkaline, , >5.5, , Calcium oxalate, , Variable, , 6, , Uric acid, , Acid, , 5.5, , Struvate, , Alkaline, , >7.2, , Cystine, , Normal, , 6.5, Next question
Page 502 :
Question 45 of 347, , A pathologist is examining a histological section and identifies Hassall's corpuscles. With what are, they most commonly associated?, , Follicular carcinoma of the thyroid, , Medulla of the thymus, , Medulla of the spleen, , Medulla of the kidney, , Fundus of the stomach, , Theme from September 2015 Exam, Hassall's corpuscles are the concentric ring of epithelial cells seen in the medulla of the thymus., Please rate this question:, , Discuss and give feedback, , Next question, , Thymus, The thymus develops from the third and fourth pharyngeal pouches. It descends to lie in the anterior, superior mediastinum. It is encapsulated and is subdivided into lobules, these consist of a cortex and, a medulla. The cortex is composed of tightly packed lymphocytes, the medulla consists largely of, epithelial cells. The medullary epithelial cells are concentrically arranged and may surround a, keratinised centre, known as Hassall's corpuscles., The inferior parathyroid glands also develop from the third pharyngeal pouch and may also be, located with the thymus gland., Its arterial supply is from the internal mammary artery or pericardiophrenic arteries. Venous drainage
Page 503 :
is to the left brachiocephalic vein., Hassall's corpuscles stained with H+E, , Image sourced from Wikipedia, , Next question
Page 504 :
Question 46 of 347, A 64 year old man presents to the clinic with right upper quadrant discomfort. He has never attended, the hospital previously and is usually well. He has just retired from full time employment as a, machinist in a PVC factory. CT scanning shows a large irregular tumour in the right lobe of his liver., Which of the following lesions is the most likely?, , Liposarcoma, , Angiosarcoma, , Hamartoma, , Hyatid liver disease, , Benign angioma, , Angiosarcoma of the liver is a rare tumour. However, it is linked to working with vinyl chloride, as in, this case. Although modern factories minimise the exposure to this agent, this has not always been, the case., Please rate this question:, , Discuss and give feedback, , Next question, , Occupational cancers, Occupational cancers accounted for 5.3% cancer deaths in 2005., In men the main cancers include:, , , , , , , Mesothelioma, Bladder cancer, Non melanoma skin cancer, Lung cancer, Sino nasal cancer, , Occupations with high levels of occupational tumours include:
Page 505 :
, , , , , , , Construction industry, Working with coal tar and pitch, Mining, Metalworkers, Working with asbestos (accounts for 98% of all mesotheliomas), Working in rubber industry, , Shift work has been linked to breast cancer in women (Health and safety executive report RR595)., The latency between exposure and disease is typically 15 years for solid tumours and 20 for, leukaemia., Many occupational cancers are otherwise rare. For example sino nasal cancer is an uncommon, tumour, 50% will be SCC. They are linked to conditions such as wood dust exposure and unlike lung, cancer is not strongly linked to cigarette smoking. Another typical occupational tumour is, angiosarcoma of the liver which is linked to working with vinyl chloride. Again in the non occupational, context this is an extremely rare sporadic tumour., Next question
Page 506 :
Question 47 of 347, A 32 year old man is involved in a house fire and sustains extensive partial thickness burns to his, torso and thigh. Two weeks post operatively he develops oedema of both lower legs. The most likely, cause of this is:, , Iliofemoral deep vein thrombosis, , Venous obstruction due to scarring, , Hypoalbuminaemia, , Excessive administration of intravenous fluids, , None of the above, , Theme from 2009 Exam, Loss of plasma proteins is the most common cause of oedema developing in this time frame., Please rate this question:, , Discuss and give feedback, , Next question, , Burns pathology, Extensive burns, , , , , , , , , , Haemolysis due to damage of erythrocytes by heat and microangiopathy, Loss of capillary membrane integrity causing plasma leakage into interstitial space, Extravasation of fluids from the burn site causing hypovolaemic shock (up to 48h after, injury)- decreased blood volume and increased haematocrit, Protein loss, Secondary infection e.g. Staphylococcus aureus, ARDS, Risk of Curlings ulcer (acute peptic stress ulcers), Danger of full thickness circumferential burns in an extremity as these may develop, compartment syndrome
Page 507 :
Healing, , , , Superficial burns: keratinocytes migrate to form a new layer over the burn site, Full thickness burns: dermal scarring. Usually need keratinocytes from skin grafts to provide, optimal coverage., Next question
Page 508 :
Question 48 of 347, A 42 year old man from Southern India presents with chronic swelling of both lower legs, they are, brawny and indurated with marked skin trophic changes. Which of the following organisms is the, most likely origin of this disease process?, , Loa loa, , Wuchereria bancrofti, , Trypanosoma cruzi, , Trypanosoma gambiense, , None of the above, , W. Bancrofti is the commonest cause of filariasis leading to lymphatic obstruction. Infection with Loa, loatypically occurs in the African sub continent and usually results in generalised sub cutaneous, infections without lymphatic obstruction. Trypanosomal infections would not produce this clinical, picture., Please rate this question:, , Discuss and give feedback, , Next question, , Wuchereria bancrofti, , , , , , , Parasitic filarial nematode, Accounts for 90% of cases of filariasis, Usually diagnosed by blood smears, Usually transmitted by mosquitos, Treatment is with diethylcarbamazine, Next question
Page 509 :
Question 49 of 347, A 45 year old lady has recently undergone a thyroidectomy for treatment of medullary thyroid, cancer. Which of the following tumour markers is used clinically to screen for recurrence?, , Free T3, , Thyroglobulin, , Calcitonin, , Free T4, , Thyroid stimulating hormone, , Theme from 2011 Exam, Calcitonin is clinically utilised to screen for medullary thyroid cancer recurrence. Thyroid function, testing does not form part of either diagnosis or follow up from a malignancy perspective. However,, routine assessment of TSH may be needed in patients on thyroxine., Please rate this question:, , Discuss and give feedback, , Next question, , Thyroid malignancy, Papillary carcinoma, , , , , , Commonest sub-type, Accurately diagnosed on fine needle aspiration cytology, Histologically, they may demonstrate psammoma bodies (areas of calcification) and so, called 'orphan Annie' nuclei, They typically metastasise via the lymphatics and thus laterally located apparently ectopic, thyroid tissue is usually a metastasis from a well differentiated papillary carcinoma, , Follicular carcinoma, , , Are less common than papillary lesions
Page 510 :
, , , , Like papillary tumours, they may present as a discrete nodule. Although they appear to be, well encapsulated macroscopically there is invasion on microscopic evaluation, Lymph node metastases are uncommon and these tumours tend to spread, haematogenously. This translates into a higher mortality rate, Follicular lesions cannot be accurately diagnosed on fine needle aspiration cytology and thus, all follicular FNA's (THY 3f) will require at least a hemi thyroidectomy, , Anaplastic carcinoma, , , , Less common and tend to occur in elderly females, Disease is usually advanced at presentation and often only palliative decompression and, radiotherapy can be offered., , Medullary carcinoma, , , , , , These are tumours of the parafollicular cells ( C Cells) and are of neural crest origin., The serum calcitonin may be elevated which is of use when monitoring for recurrence., They may be familial and occur as part of the MEN -2A disease spectrum., Spread may be either lymphatic or haematogenous and as these tumours are not derived, primarily from thyroid cells they are not responsive to radioiodine., , Lymphoma, , , , These respond well to radiotherapy, Radical surgery is unnecessary once the disease has been diagnosed on biopsy material., Such biopsy material is not generated by an FNA and thus a core biopsy has to be obtained, (with care!)., Next question
Page 511 :
Question 50 of 347, A 22 year old man is kicked in the head during a rugby match. He is temporarily concussed, but then, regains consciousness. Half an hour later he develops slurred speech, ataxia and loses, consciousnesses. On arrival in hospital he is intubated and ventilated. A CT Scan is performed, which shows an extradural haematoma. What is the most likely cause?, , Basilar artery laceration, , Middle meningeal artery laceration, , Laceration of the sigmoid sinus, , Laceration of the anterior cerebral artery, , Laceration of the middle cerebral artery, , Theme from April 2014 Exam, The most likely vessel from those in the list to cause an acute extra dural haemorrhage is the middle, meningeal artery. The anterior and middle cerebral arteries may cause acute sub dural, haemorrhage. Acute sub dural haemorrhages usually take slightly longer to evolve than acute extra, dural haemorrhages., Please rate this question:, , Discuss and give feedback, , Next question, , Middle meningeal artery, , , , , , , Middle meningeal artery is typically the third branch of the first part of the maxillary artery,, one of the two terminal branches of the external carotid artery. After branching off the, maxillary artery in the infratemporal fossa, it runs through the foramen spinosum to supply, the dura mater (the outermost meninges) ., The middle meningeal artery is the largest of the three (paired) arteries which supply the, meninges, the others being the anterior meningeal artery and the posterior meningeal artery., The middle meningeal artery runs beneath the pterion. It is vulnerable to injury at this point,, where the skull is thin. Rupture of the artery may give rise to an extra dural hematoma., In the dry cranium, the middle meningeal, which runs within the dura mater surrounding the, brain, makes a deep indention in the calvarium.
Page 512 :
, , The middle meningeal artery is intimately associated with the auriculotemporal nerve which, wraps around the artery making the two easily identifiable in the dissection of human, cadavers and also easily damaged in surgery., Next question
Page 513 :
Question 51 of 347, Which of the following is not characteristic of a granuloma?, , Altered macrophages, , Fused macrophages, , Epithelioid cells, , Mixture of chronic inflammatory cells, , Polymorphnuclear leucocytes, cellular debris and fibrin, , These are typical components of an abscess cavity. Polymorphonuclear leucocytes may be found in, a granuloma if there is a focus of suppuration., Please rate this question:, , Discuss and give feedback, , Next question, , Chronic inflammation, Overview, Chronic inflammation may occur secondary to acute inflammation.In most cases chronic, inflammation occurs as a primary process. These may be broadly viewed as being one of three main, processes:, , , , , Persisting infection with certain organisms such as Mycobacterium tuberculosis which results, in delayed type hypersensitivity reactions and inflammation., Prolonged exposure to non-biodegradable substances such as silica or suture materials, which may induce an inflammatory response., Autoimmune conditions involving antibodies formed against host antigens., , Acute vs. Chronic inflammation, , Acute inflammation, , Chronic inflammation
Page 514 :
Changes to existing vascular structure and increased, permeability of endothelial cells, , Angiogenesis predominates, , Infiltration of neutrophils, , Macrophages, plasma cells and, lymphocytes predominate, , Process may resolve with:, , Healing by fibrosis is the main result, , , , , , , , Suppuration, Complete resolution, Abscess formation, Progression to chronic inflammation, Healing by fibrosis, , Granulomatous inflammation, A granuloma consists of a microscopic aggregation of macrophages (with epithelial type, arrangement =epitheliod). Large giant cells may be found at the periphery of granulomas., Mediators, Growth factors released by activated macrophages include agents such as interferon and fibroblast, growth factor (plus many more). Some of these such as interferons may have systemic features, resulting in systemic symptoms and signs, which may be present in individuals with long standing, chronic inflammation., The finding of granulomas is pathognomonic of chronic inflammation, as illustrated in this biopsy, from a patient with colonic Crohns disease, , Image sourced from Wikipedia
Page 515 :
Question 52 of 347, A 42 year old man presents with a painless lump in the left testicle that he noticed on self, examination. Clinically there is a firm nodule in the left testicle, ultrasound appearances show an, irregular mass lesion. His serum AFP and HCG levels are both within normal limits. What is the most, likely diagnosis?, , Yolk sack tumour, , Seminoma, , Testicular teratoma, , Epididymo-orchitis, , Adenomatoid tumour, Seminomas typically have normal AFP and HCG. These are usually raised in teratomas and yolk, sac tumours, This man's age, presenting symptoms and normal tumour markers make a seminoma the most, likelydiagnosis. Epididymo-orchitis does not produce irregular mass lesions which are painless., Please rate this question:, , Discuss and give feedback, , Next question, , Testicular disorders, Testicular cancer, Testicular cancer is the most common malignancy in men aged 20-30 years. Around 95% of cases, of testicular cancer are germ-cell tumours. Germ cell tumours may essentially be divided into:, , Tumour type, , Seminoma, , Key features, , , , Commonest, subtype (50%), Average age at, , Tumour, markers, AFP usually, normal, , Pathology, , Sheet like lobular, patterns of cells, with substantial
Page 516 :
Tumour type, , Key features, , , , , , , Teratoma, Yolk sac tumour, Choriocarcinoma, Mixed germ cell, tumours (10%), , Pathology, , diagnosis = 40, Even advanced, disease associated, with 5 year, survival of 73%, , HCG elevated, in 10%, seminomas, Lactate, dehydrogenase;, elevated in 1020% seminomas, (but also in many, other conditions), , fibrous, component., Fibrous septa, contain, lymphocytic, inclusions and, granulomas may, be seen., , Younger age at, presentation =20-30, years, Advanced disease, carries worse prognosis, (48% at 5 years), Retroperitoneal lymph, node dissection may be, needed for residual, disease after, chemotherapy, , AFP elevated, in up to 70% of, cases, HCG elevated, in up to 40% of, cases, Other markers, rarely helpful, , Heterogenous, texture with, occasional ectopic, tissue such as hair, , , , Non seminomatous germ, cell tumours (42%), , Tumour, markers, , Image demonstrating a classical seminoma, these tumours are typically more uniform than, teratomas
Page 517 :
Image sourced from Wikipedia, , Risk factors for testicular cancer, , , , , , , Cryptorchidism, Infertility, Family history, Klinefelter's syndrome, Mumps orchitis, , Features
Page 518 :
, , , , A painless lump is the most common presenting symptom, Pain may also be present in a minority of men, Other possible features include hydrocele, gynaecomastia, , Diagnosis, , , , , Ultrasound is first-line, CT scanning of the chest/ abdomen and pelvis is used for staging, Tumour markers (see above) should be measured, , Management, , , , , Orchidectomy (Inguinal approach), Chemotherapy and radiotherapy may be given depending on staging, Abdominal lesions >1cm following chemotherapy may require retroperitoneal lymph node, dissection., , Prognosis is generally excellent, , , , 5 year survival for seminomas is around 95% if Stage I, 5 year survival for teratomas is around 85% if Stage I, , Benign disease, Epididymo-orchitis, Acute epididymitis is an acute inflammation of the epididymis, often involving the testis and usually, caused by bacterial infection., , , , , Infection spreads from the urethra or bladder. In men <35 years, gonorrhoea or chlamydia, are the usual infections., Amiodarone is a recognised non infective cause of epididymitis, which resolves on stopping, the drug., Tenderness is usually confined to the epididymis, which may facilitate differentiating it from, torsion where pain usually affects the entire testis., , Testicular torsion, , , , , , Twist of the spermatic cord resulting in testicular ischaemia and necrosis., Most common in males aged between 10 and 30 (peak incidence 13-15 years), Pain is usually severe and of sudden onset., Cremasteric reflex is lost and elevation of the testis does not ease the pain.
Page 519 :
, , Treatment is with surgical exploration. If a torted testis is identified then both testis should be, fixed as the condition of bell clapper testis is often bilateral., , Hydrocele, , , , , , , Presents as a mass that transilluminates, usually possible to "get above" it on examination., In younger men it should be investigated with USS to exclude tumour., In children it may occur as a result of a patent processus vaginalis., Treatment in adults is with a Lords or Jabouley procedure., Treatment in children is with trans inguinal ligation of PPV., Next question
Page 520 :
Question 53 of 347, A baby is born by normal vaginal delivery at 39 weeks gestation. Initially all appears well and then, the clinical staff become concerned because the baby develops recurrent episodes of cyanosis., These are worse during feeding and improve dramatically when the baby cries. The most likely, underlying diagnosis is:, , Choanal atresia, , Oesophageal reflux, , Tetralogy of Fallot, , Oesophageal atresia, , Congenital diaphragmatic hernia, , Theme from 2011 exam, Theme from April 2013 Exam, In Choanal atresia the episodes of cyanosis are usually worst during feeding. Improvement may be, seen when the baby cries as the oropharyngeal airway is used., Please rate this question:, , Discuss and give feedback, , Next question, , Choanal atresia, , , , , , , , Congenital disorder with an incidence of 1 in 7000 births., Posterior nasal airway occluded by soft tissue or bone., Associated with other congenital malformations e.g. coloboma, Babies with unilateral disease may go unnoticed., Babies with bilateral disease will present early in life as they are obligate mouth breathers., Treatment is with fenestration procedures designed to restore patency., Next question
Page 521 :
Question 54 of 347, A 28 year old lady presents with a pigmented lesion on her calf. Excisional biopsy confirms a, diagnosis of melanoma measuring 1cm in diameter with a Breslow thickness of 0.1mm. The lesion is, less than 1 mm at all resection margins. Which of the following surgical resection margins is, acceptable for this lesion?, , 5 cm, , 1 cm, , 0.5 cm, , 2 cm, , 3 cm, , Please rate this question:, , Discuss and give feedback, , Next question, , Malignant melanoma, The main diagnostic features (major criteria):, , , , , Change in size, Change in shape, Change in colour, , Secondary features (minor criteria), , , , , , Diameter >6mm, Inflammation, Oozing or bleeding, Altered sensation, , Treatment, , , Suspicious lesions should undergo excision biopsy. The lesion should be removed in, completely as incision biopsy can make subsequent histopathological assessment difficult.
Page 522 :
, , Once the diagnosis is confirmed the pathology report should be reviewed to determine, whether further re-excision of margins is required (see below):, , Margins of excision-Related to Breslow thickness, , Lesions 0-1mm thick, , 1cm, , Lesions 1-2mm thick, , 1- 2cm (Depending upon site and pathological features), , Lesions 2-4mm thick, , 2-3 cm (Depending upon site and pathological features), , Lesions >4 mm thick, , 3cm, , Marsden J et al Revised UK guidelines for management of Melanoma. Br J Dermatol 2010 163:238256., Further treatments such as sentinel lymph node mapping, isolated limb perfusion and block, dissection of regional lymph node groups should be selectively applied., Next question
Page 523 :
Question 55 of 347, A 20 year old man is involved in a road traffic accident. Following the incident he is unable to extend, his wrist. However, this improves over the following weeks. Which type of injury is he most likely to, have sustained?, , Radial nerve neurotmesis, , Radial nerve neuropraxia, , Axillary nerve axonotmesis, , Ulnar nerve neuropraxia, , Ulnar nerve axonotmesis, , Theme from April 2011 Exam, Transient loss of function makes neuropraxia the most likely injury. The wrist extensors are, innervated by the radial nerve making this the most likely site of injury., Please rate this question:, , Discuss and give feedback, , Next question, , Neuropraxia, , , , , , , Nerve intact but electrical conduction is affected, Myelin sheath integrity is preserved, Full recovery, Autonomic function preserved, Wallerian degeneration does not occur, Next question
Page 524 :
Question 56 of 347, , A 53 year old lady has undergone a bilateral breast augmentation procedure many years previously., The implants are tense and uncomfortable and are removed. During their removal the surgeon, encounters a dense membrane surrounding the implants, it has a coarse granular appearance. The, tissue is sent for histology and it demonstrates fibrosis with the presence of calcification. The, underlying process responsible for these changes is:, , Hyperplasia, , Dysplasia, , Metastatic calcification, , Dystrophic calcification, , Necrosis, , Breast implants often become surrounded by a pseudocapsule and this may secondarily then be, subjected to a process of dystrophic calcification., Please rate this question:, , Discuss and give feedback, , Next question, , Pathological calcification, Dystrophic, calcification, , Deposition of calcium deposits in tissues that have undergone degeneration, damage, or disease in the presence of normal serum calcium levels
Page 525 :
Metastatic, calcification, , Deposition of calcium deposits in tissues that are otherwise normal in the presence, of increased serum calcium levels, Next question
Page 526 :
Question 57 of 347, A 4 year old girl presents with symptoms of right sided loin pain, lethargy and haematuria. On, examination she is pyrexial and has a large mass in the right upper quadrant. The most likely, underlying diagnosis is:, , Perinephric abscess, , Nephroblastoma, , Renal cortical adenoma, , Grawitz tumour, , Squamous cell carcinoma of the kidney, , In a child of this age, with the symptoms described a nephroblastoma is the most likely diagnosis. A, perinephric abscess is most unlikely. If an abscess were to occur it would be confined to Gerotas, fascia in the first instance, and hence anterior extension would be unlikely., Please rate this question:, , Discuss and give feedback, , Next question, , Nephroblastoma, Nephroblastoma (Wilms tumours), , , , , , , Usually present in first 4 years of life, May often present as a mass associated with haematuria (pyrexia may occur in 50%), Often metastasise early (usually to lung), Treated by nephrectomy, Younger children have better prognosis (<1 year of age =80% overall 5 year survival), Next question
Page 527 :
Question 58-60 of 347, Theme: Thyroid neoplasms, , A., B., C., D., E., F., G., , Follicular carcinoma, Anaplastic carcinoma, Medullary carcinoma, Papillary carcinoma, Lymphoma, Hashimotos thyroiditis, Graves disease, , For the following histological descriptions please select the most likely underlying thyroid neoplasm., Each option may be used once, more than once or not at all., , 58., , A 22 year old female undergoes a thyroidectomy. The resected specimen shows a non, encapsulated tumour with papillary projections and pale empty nuclei., You answered Follicular carcinoma, The correct answer is Papillary carcinoma, Theme from April 2012, The presence of papillary structures together with the cytoplasmic features described is, strongly suggestive of papillary carcinoma. They are seldom encapsulated., , 59., , A thyroidectomy specimen from a 43 year old lady shows a mass with prominent oxyphil, cells and scanty thyroid colloid., Follicular carcinoma, Hurthle cell tumours are a variant of follicular neoplasms in which oxyphil cells, predominate. They have a poorer prognosis than conventional follicular neoplasms., , 60., , A 32 year old lady undergoes a thyroidectomy for a mild goitre. The resected specimen, shows an intense lymphocytic infiltrate with acinar destruction and fibrosis., You answered Follicular carcinoma, The correct answer is Hashimotos thyroiditis, Lymphocytic infiltrates and fibrosis are typically seen in Hashimotos thyroiditis. In, Lymphoma only dense lymphatic type tissue is usually present.
Page 528 :
Please rate this question:, , Discuss and give feedback, , Next question, , Thyroid neoplasms, Lesion, , Common features, , Follicular, adenoma, , , , , Usually present as a solitary thyroid nodule, Malignancy can only be excluded on formal histological assessment, , Papillary, carcinoma, , , , , , , , , Usually contain a mixture of papillary and colloidal filled follicles, Histologically tumour has papillary projections and pale empty nuclei, Seldom encapsulated, Lymph node metastasis predominate, Haematogenous metastasis rare, Account for 60% of thyroid cancers, , Follicular, carcinoma, , , , May appear macroscopically encapsulated, microscopically capsular, invasion is seen. Without this finding the lesion is a follicular adenoma., Vascular invasion predominates, Multifocal disease rare, Account for 20% of all thyroid cancers, , , , , , Anaplastic, carcinoma, , , , , , , Most common in elderly females, Local invasion is a common feature, Account for 10% of thyroid cancers, Treatment is by resection where possible, palliation may be achieved, through isthmusectomy and radiotherapy. Chemotherapy is ineffective., , Medullary, carcinoma, , , , , , , , Tumours of the parafollicular cells (C Cells), C cells derived from neural crest and not thyroid tissue, Serum calcitonin levels often raised, Familial genetic disease accounts for up to 20% cases, Both lymphatic and haematogenous metastasis are recognised, nodal, disease is associated with a very poor prognosis., Next question
Page 529 :
Question 61 of 347, From which of the following cell types do giant cells most commonly originate?, , Neutrophils, , Myofibroblasts, , Fibroblasts, , Macrophages, , Goblet cells, , Theme from September 2011 and 2009 Exam, Although many cell types may give rise to giant cells, macrophages remain the most common., Please rate this question:, , Discuss and give feedback, , Next question, , Giant cells, , , , , A giant cell is a mass formed by the union of several distinct types of cells, They are most commonly comprised of macrophages, They are different to granulomas although causative agents may overlap, , Section stained using haematoxylin and eosin showing giant cell reaction to suture material
Page 530 :
Image sourced from Wikipedia, , Next question
Page 531 :
Question 62 of 347, A 43 year old lady with hypertension is suspected of having a phaeochromocytoma. Which of the, following investigations is most likely to be beneficial in this situation?, , Dexamethasone suppression test, , Urinary 5-Hydroxyindoleacetic Acid (5-HIAA), , Histamine provocation test, , Tyramine provocation test, , Urinary vanillymandelic acid measurements, , Theme from September 2011 Exam, Theme from September 2012 Exam, Urinary VMA measurements are not completely specific but constitute first line assessment., Stimulation tests of any sort are not justified in first line assessments., Please rate this question:, , Discuss and give feedback, , Next question, , Phaeochromocytoma and adrenal lesions, Phaeochromocytoma, Neuroendocrine tumour of the chromaffin cells of the adrenal medulla. Hypertension and, hyperglycaemia are often found., , , , , , 10% of cases are bilateral., 10% occur in children., 11% are malignant (higher when tumour is located outside the adrenal)., 10% will not be hypertensive., , Familial cases are usually linked to the Multiple endocrine neoplasia syndromes (considered under, its own heading)., Most tumours are unilateral (often right sided) and smaller than 10cm.
Page 532 :
Diagnosis, Urine analysis of vanillymandelic acid (VMA) is often used (false positives may occur e.g. in patients, eating vanilla ice cream!), Blood testing for plasma metanephrine levels., CT and MRI scanning are both used to localise the lesion., Treatment, Patients require medical therapy first. An irreversible alpha adrenoreceptor blocker should be given,, although minority may prefer reversible blockade(1). Labetolol may be co-administered for cardiac, chronotropic control. Isolated beta blockade should not be considered as it will lead to unopposed, alpha activity., These patients are often volume depleted and will often require moderate volumes of intra venous, normal saline perioperatively., Once medically optimised the phaeochromocytoma should be removed. Most adrenalectomies can, now be performed using a laparoscopic approach(2). The adrenals are highly vascular structures, and removal can be complicated by catastrophic haemorrhage in the hands of the inexperienced., This is particularly true of right sided resections where the IVC is perilously close. Should the IVC be, damaged a laparotomy will be necessary and the defect enclosed within a Satinsky style vascular, clamp and the defect closed with prolene sutures. Attempting to interfere with the IVC using any, instruments other than vascular clamps will result in vessel trauma and make a bad situation much, worse., Incidental adrenal lesions, Adrenal lesions may be identified on CT scanning performed for other reasons(3). Factors, suggesting benign disease on CT include(4):, , , , , , Size less than 3cm, Homogeneous texture, Lipid rich tissue, Thin wall to lesion, , All patients with incidental lesions should be managed jointly with an endocrinologist and full work up, as described above. Patients with functioning lesions or those with adverse radiological features, (Particularly size >3cm) should proceed to surgery., References, 1. Weingarten TN, Cata JP, O'Hara JF, Prybilla DJ, Pike TL, Thompson GB, et al. Comparison of, two preoperative medical management strategies for laparoscopic resection of pheochromocytoma., Urology. 2010 Aug;76(2):508 e6-11., 2. Nguyen PH, Keller JE, Novitsky YW, Heniford BT, Kercher KW. Laparoscopic approach to, adrenalectomy: review of perioperative outcomes in a single center. Am Surg. 2011 May;77(5):5926., 3. Ng VW, Ma RC, So WY, Choi KC, Kong AP, Cockram CS, et al. Evaluation of functional and
Page 533 :
malignant adrenal incidentalomas. Arch Intern Med. 2010 Dec 13;170(22):2017-20., 4. Muth A, Hammarstedt L, Hellstrom M, Sigurjonsdottir HA, Almqvist E, Wangberg B. Cohort study, of patients with adrenal lesions discovered incidentally. Br J Surg. 2011 May 27., Next question
Page 534 :
Question 63 of 347, A 46 year old lady presents with symptoms of diarrhoea, weight loss of 10 Kg and a skin rash of, erythematous blisters involving the abdomen and buttocks. The blisters have an irregular border and, both intact and ruptured vesicles. What is the most likely diagnosis?, , Colonic adenocarcinoma, , Pancreatic adenocarcinoma, , Tropical sprue, , Glucagonoma, , Insulinoma, , Theme from September 2011 Exam, Theme from September 2012 Exam, Theme from September 2013 Exam, Glucagonoma is strongly associated with necrolytic migratory erythema., Please rate this question:, , Discuss and give feedback, , Next question, , Glucagonoma, , , , , , , Rare pancreatic tumours arising from the alpha cells of the pancreas., Glucagon levels markedly elevated., Symptoms include diarrhoea, weight loss and necrolytic migratory erythema., A serum level of glucagon >1000pg/ml usually suggests the diagnosis, imaging with CT, scanning is also required., Treatment is with surgical resection. However, careful staging is required for these tumours, are usually malignant and non resectable., Next question
Page 535 :
Question 64 of 347, A 56 year old man presents with symptoms of neuropathic facial pain and some weakness of the, muscles of facial expression on the right side. On examination he has a hard mass approximately, 6cm anterior to the right external auditory meatus. What is the most likely diagnosis?, , Pleomorphic adenoma, , Adenocarcinoma, , Mucoepidermoid carcinoma, , Adenoid cystic carcinoma, , Lymphoma, , Theme from September 2011 Exam, The patient is most likely to have a malignant lesion within the parotid. Of the malignancies listed;, adenoid cystic carcinoma has the greatest tendency to perineural invasion., Please rate this question:, , Discuss and give feedback, , Next question, , Parotid gland malignancy, , , , , , , Most parotid neoplasms (80%) are benign lesions, Most commonly present with painless mass around the mandible, Up to 30% may present with pain, when this is associated with a discrete mass lesion in the, parotid it usually indicates perineural invasion., Perineural invasion is very unlikely to occur in association with benign lesions, 80% of patients with facial nerve weakness caused by parotid malignancies will have nodal, metastasis and a 5 year survival of 25%, , Types of malignancy, , Mucoepidermoid, carcinoma, , 30% of all parotid malignancies, Usually low potential for local invasiveness and metastasis (depends
Page 536 :
mainly on grade), , Adenoid cystic, carcinoma, , Unpredictable growth pattern, Tendency for perineural spread, Nerve growth may display skip lesions resulting in incomplete excision, Distant metastasis more common (visceral rather than nodal spread), 5 year survival 35%, , Mixed tumours, , Often a malignancy occurring in a previously benign parotid lesion, , Acinic cell carcinoma, , Intermediate grade malignancy, May show perineural invasion, Low potential for distant metastasis, 5 year survival 80%, , Adenocarcinoma, , Develops from secretory portion of gland, Risk of regional nodal and distant metastasis, 5 year survival depends upon stage at presentation, may be up to 75%, with small lesions with no nodal involvement, , Lymphoma, , Large rubbery lesion, may occur in association with Warthins tumours, Diagnosis should be based on regional nodal biopsy rather than parotid, resection Treatment is with chemotherapy (and radiotherapy), Next question
Page 537 :
Question 65 of 347, A 20 year old African lady undergoes an open appendicectomy. She is reviewed for an unrelated, problem 8 months later. On abdominal inspection the wound site is covered by shiny dark, protuberant scar tissue that projects beyond the limits of the skin incision. Which of the following is, the most likely underlying process?, , Hypertrophic scar, , Keloid scar, , Marjolins ulcer, , Repeated episodes of wound sepsis, , Mycosis fungoides, , Keloid scars extend beyond the limits of the incision. Mycosis fungoides is a cutaneous T cell, lymphoma., Please rate this question:, , Discuss and give feedback, , Next question, , Wound healing, Surgical wounds are either incisional or excisional and either clean, clean contaminated or dirty., Although the stages of wound healing are broadly similar their contributions will vary according to the, wound type., The main stages of wound healing include:, Haemostasis, , , , Minutes to hours following injury, Vasospasm in adjacent vessels, platelet plug formation and generation of fibrin rich clot., , Inflammation
Page 538 :
, , , , , , Typically days 1-5, Neutrophils migrate into wound (function impaired in diabetes)., Growth factors released, including basic fibroblast growth factor and vascular endothelial, growth factor., Fibroblasts replicate within the adjacent matrix and migrate into wound., Macrophages and fibroblasts couple matrix regeneration and clot substitution., , Regeneration, , , , , , Typically days 7 to 56, Platelet derived growth factor and transformation growth factors stimulate fibroblasts and, epithelial cells., Fibroblasts produce a collagen network., Angiogenesis occurs and wound resembles granulation tissue., , Remodeling, , , , , , , From 6 weeks to 1 year, Longest phase of the healing process and may last up to one year (or longer)., During this phase fibroblasts become differentiated (myofibroblasts) and these facilitate, wound contraction., Collagen fibres are remodeled., Microvessels regress leaving a pale scar., , The above description represents an idealised scenario. A number of diseases may distort this, process. Neovascularisation is an important early process. Endothelial cells may proliferate in the, wound bed and recanalise to form a vessel. Vascular disease, shock and sepsis can all compromise, microvascular flow and impair healing., Conditions such as jaundice will impair fibroblast synthetic function and immunity with a detrimental, effect in most parts of the healing process., Problems with scars:, Hypertrophic scars, Excessive amounts of collagen within a scar. Nodules may be present histologically containing, randomly arranged fibrils within and parallel fibres on the surface. The tissue itself is confined to the, extent of the wound itself and is usually the result of a full thickness dermal injury. They may go on, to develop contractures., Image of hypertrophic scarring. Note that it remains confined to the boundaries of the original, wound:
Page 539 :
Image sourced from Wikipedia, , Keloid scars, Excessive amounts of collagen within a scar. Typically a keloid scar will pass beyond the boundaries, of the original injury. They do not contain nodules and may occur following even trivial injury. They, do not regress over time and may recur following removal., Image of a keloid scar. Note the extension beyond the boundaries of the original incision:, , Image sourced from Wikipedia, , Drugs which impair wound healing:
Page 540 :
, , , , , Non steroidal anti inflammatory drugs, Steroids, Immunosupressive agents, Anti neoplastic drugs, , Closure, Delayed primary closure is the anatomically precise closure that is delayed for a few days but before, granulation tissue becomes macroscopically evident., Secondary closure refers to either spontaneous closure or to surgical closure after granulation tissue, has formed., Next question
Page 541 :
Question 66 of 347, A 28 year old man has a long history of recurrent chest infections. On examination, he is noted to, have no palpable vas deferens. However, both testes are located within the scrotum. What is the, most likely underlying disease association?, , Kleinfelters syndrome, , Kallmann syndrome, , Cystic fibrosis, , Coeliac disease, , Gardners syndrome, 99% of males with cystic fibrosis will have absent vas, Please rate this question:, , Discuss and give feedback, , Next question, , Absence of the vas deferens, , , , , , Absence of the vas may be unilateral or bilateral, Cystic fibrosis CFTR gene mutations are the cause in 40% of cases, Some non CF cases are due to unilateral renal agenesis, Sperm harvesting may allow for assisted conception, Next question
Page 542 :
Question 67 of 347, The pathogenicity of the tubercle bacillus is due to which of the following?, , Necrosis caused by expanding granulomas, , Ability to multiply within fibroblasts, , Delayed hypersensitivity reaction against bacteria, , Effect of antibody response, , Direct toxic effect on host cells, , Mycobacteria stimulate a specific T cell response of cell mediated immunity. This is effective in, reducing the infection, the delayed hypersensitivity also damages tissues. Necrosis occurs in TB but, is usually within the granuloma., Please rate this question:, , Discuss and give feedback, , Next question, , Tuberculosis pathology, , , , , , , , Is a form of primary chronic inflammation, caused by the inability of macrophages to kill, theMycobacterium tuberculosis., The macrophages often migrate to regional lymph nodes, the lung lesion plus affected lymph, nodes is referred to as a Ghon complex., This leads to the formation of a granuloma which is a collection of epithelioid histiocytes., There is the presence of caseous necrosis in the centre., The inflammatory response is mediated by a type 4 hypersensitivity reaction., In healthy individuals the disease may be contained, in the immunocompromised, disseminated (miliary TB) may occur., , Diagnosis, , , , Waxy membrane of mycobacteria prevents binding with normal stains. Ziehl - Neelsen, staining is typically used., Culture based methods take far longer.
Page 543 :
Image showing acid- alcohol fast mycobacteria stained using the Ziehl- Neelsen method, , Image sourced from Wikipedia, , Next question
Page 544 :
Question 68 of 347, A 45 year old women with a thyroid carcinoma undergoes a total thyroidectomy. The post operative, histology report shows a final diagnosis of medullary type thyroid cancer. Which of the tests below is, most likely to be of clinical use in screening for disease recurrence?, , Serum CA 19-9 Levels, , Serum thyroglobulin levels, , Serum PTH levels, , Serum calcitonin levels, , Serum TSH levels, , Theme from September 2012 Exam, Medullary thyroid cancers often secrete calcitonin and monitoring the serum levels of this hormone is, useful in detecting sub clinical recurrence., Please rate this question:, , Discuss and give feedback, , Next question, , Thyroid neoplasms, Lesion, , Common features, , Follicular, adenoma, , , , , Usually present as a solitary thyroid nodule, Malignancy can only be excluded on formal histological assessment, , Papillary, carcinoma, , , , , , , , Usually contain a mixture of papillary and colloidal filled follicles, Histologically tumour has papillary projections and pale empty nuclei, Seldom encapsulated, Lymph node metastasis predominate, Haematogenous metastasis rare
Page 545 :
Lesion, , Follicular, carcinoma, , Common features, , , Account for 60% of thyroid cancers, , , , May appear macroscopically encapsulated, microscopically capsular, invasion is seen. Without this finding the lesion is a follicular adenoma., Vascular invasion predominates, Multifocal disease rare, Account for 20% of all thyroid cancers, , , , , , Anaplastic, carcinoma, , , , , , , Most common in elderly females, Local invasion is a common feature, Account for 10% of thyroid cancers, Treatment is by resection where possible, palliation may be achieved, through isthmusectomy and radiotherapy. Chemotherapy is ineffective., , Medullary, carcinoma, , , , , , , , Tumours of the parafollicular cells (C Cells), C cells derived from neural crest and not thyroid tissue, Serum calcitonin levels often raised, Familial genetic disease accounts for up to 20% cases, Both lymphatic and haematogenous metastasis are recognised, nodal, disease is associated with a very poor prognosis., Next question
Page 546 :
Question 69 of 347, , A 15 year old boy undergoes an emergency splenectomy for trauma. He makes a full recovery and, is discharged home. Eight weeks post operatively the general practitioner performs a full blood count, with a blood film. Which of the following is most likely to be present?, , Myofibroblasts, , Howell-Jolly bodies, , Multinucleate giant cells, , Reed Sternberg Cells, , None of the above, Post splenectomy blood film features:, Howell- Jolly bodies, Pappenheimer bodies, Target cells, Irregular contracted erythrocytes, , As the filtration function is the spleen is no longer present Howell-Jolly bodies are found., Please rate this question:, , Discuss and give feedback, , Next question, , Post splenectomy blood film changes, The loss of splenic tissue results in the inability to readily remove immature or abnormal red blood, cells from the circulation. The red cell count does not alter significantly. However, cytoplasmic
Page 547 :
inclusions may be seen e.g. Howell-Jolly bodies., In the first few days after splenectomy target cells, siderocytes and reticulocytes will appear in the, circulation. Immediately following splenectomy a granulocytosis (mainly composed of neutrophils) is, seen, this is replaced by a lymphocytosis and monocytosis over the following weeks., The platelet count is usually increased and this may be persistent, oral antiplatelet agents may be, needed in some patients., Image showing Howell Jolly bodies (arrowed), , Image sourced from Wikipedia, , Next question
Page 548 :
Question 70 of 347, A 43 year old women is identified as being a carrier of a BRCA 1 mutation. Apart from breast cancer,, which of the following malignancies is she at greatest risk of developing?, , Colonic cancer, , Ovarian cancer, , Follicular carcinoma of the thyroid, , Pituitary adenoma, , Phaeochromocytoma, , BRCA 1 mutation patients are 55% more likely to get ovarian cancer. Those with BRCA 2 are 25%, more likely. The risk of developing other malignancies is slightly increased but not to the same, extent, and not enough to justify screening., Please rate this question:, , Discuss and give feedback, , Next question, , Genetics and surgical disease, Some of the more commonly occurring genetic conditions occurring in surgical patients are, presented here., Li-Fraumeni Syndrome, , , , , , Autosomal dominant, Consists of germline mutations to p53 tumour suppressor gene, High incidence of malignancies particularly sarcomas and leukaemias, Diagnosed when:, , *Individual develops sarcoma under 45 years, *First degree relative diagnosed with any cancer below age 45 years and another family member, develops malignancy under 45 years or sarcoma at any age
Page 549 :
BRCA 1 and 2, , , , , Carried on chromosome 17 (BRCA 1) and Chromosome 13 (BRCA 2), Linked to developing breast cancer (60%) risk., Associated risk of developing ovarian cancer (55% with BRCA 1 and 25% with BRCA 2)., , Lynch Syndrome, , , , , , Autosomal dominant, Develop colonic cancer and endometrial cancer at young age, 80% of affected individuals will get colonic and/ or endometrial cancer, High risk individuals may be identified using the Amsterdam criteria, , Amsterdam criteria, Three or more family members with a confirmed diagnosis of colorectal cancer, one of whom is a, first degree (parent, child, sibling) relative of the other two., Two successive affected generations., One or more colon cancers diagnosed under age 50 years., Familial adenomatous polyposis (FAP) has been excluded., Gardners syndrome, , , , , , , , , Autosomal dominant familial colorectal polyposis, Multiple colonic polyps, Extra colonic diseases include: skull osteoma, thyroid cancer and epidermoid cysts, Desmoid tumours are seen in 15%, Mutation of APC gene located on chromosome 5, Due to colonic polyps most patients will undergo colectomy to reduce risk of colorectal, cancer, Now considered a variant of familial adenomatous polyposis coli, Next question
Page 550 :
Question 71 of 347, , A 53 year old man is due to undergo a splenectomy as a treatment for refractory haemolytic, anaemia. The underlying pathological basis for haemolytic anaemia is thought to be a Type 2, hypersensitivity response. Which of the following mechanisms best describes this process, , Deposition of immune complexes, , Cell mediated immune response, , IgE mediated response, , Formation of autoantibodies against cell surface antigens, , None of the above, Mnemonic for the reactions and the mediators involved, ACID EGG-T, Type 1 Anaphylactic, Type 2 Cytotoxic, Type 3 Immune complex, Type 4 Delayed type, EGG T (mediators), IgE, IgG, IgG, T cells, , Type 2 hypersensitivity reactions (which includes haemolytic anaemia) are associated with formation, of antibody against cell surface antigens., Please rate this question:
Page 552 :
Question 72 of 347, Which of the following is not an oncogene?, , ras, , myc, , sis, , Ki 67, , erb-B, , Ki 67 is a nuclear proliferation marker (used in immunohistochemistry). Although, Ki67 positivity is a, marker of malignancy, it is not itself, an oncogene., Please rate this question:, , Discuss and give feedback, , Next question, , Oncogenes, Oncogenes are cancer promoting genes that are derived from normal genes (proto-oncogenes)., Proto-oncogenes play an important physiological role in cellular growth. They are implicated in the, development of up to 20% of human cancers., Proto-oncogenes may become oncogenes via the following processes:, , , , , Mutation (point mutation), Chromosomal translocation, Increased protein expression, , Only one mutated copy of the gene is needed for cancer to occur - a dominant effect, Classification of oncogenes, , , , Growth factors e.g. Sis, Transcription factors e.g. Myc
Page 553 :
, , , , Receptor tyrosine kinase e.g. RET, Cytoplasmic tyrosine kinase e.g. Src, Regulatory GTPases e.g. Ras, , Tumour suppressor genes, Tumour suppressor genes restrict or repress cellular proliferation in normal cells. Their inactivation, through mutation or germ line incorporation is implicated in renal, colonic, breast, bladder and many, other cancers. One of the best known tumour suppressor genes is p53. p53 gene offers protection, by causing apoptosis of damaged cells. Other well known genes include BRCA 1 and 2., Next question
Page 554 :
Question 73 of 347, A 25 year old man is injured in a road traffic accident. His right tibia is fractured and is managed by, fasciotomies and application of an external fixator. Over the next 48 hours his serum creatinine rises, and urine is sent for microscopy, muddy brown casts are identified. What is the most likely, underlying diagnosis?, , Acute interstitial nephritis, , Acute tubular necrosis, , Glomerulonephritis, , IgA Nephropathy, , Thin basement membrane disease, , This patient is likely to have had compartment syndrome (tibial fracture + fasciotomies) which may, produce myoglobinuria. The presence of worsening renal function, together with muddy brown casts, is strongly suggestive of acute tubular necrosis. Acute interstitial nephritis usually arises from drug, toxicity and does not usually produce urinary muddy brown casts. Thin basement membrane, disease is an autosomal dominant condition that causes persistent microscopic haematuria, but not, worsening renal function., Please rate this question:, , Discuss and give feedback, , Next question, , Acute Renal Failure, , , , , , , , Final pathway is tubular cell death., Renal medulla is a relatively hypoxic environment making it susceptible to renal tubular, hypoxia., Renovascular autoregulation maintains renal blood flow across a range of arterial pressures., Estimates of GFR are best indices of level of renal function. Useful clinical estimates can be, obtained by considering serum creatinine, age, race, gender and body size. eGFR, calculations such as the Cockcroft and Gault equation are less reliable in populations with, high GFR's., Nephrotoxic stimuli such as aminoglycosides and radiological contrast media induce, apoptosis. Myoglobinuria and haemolysis result in necrosis. Overlap exists and, proinflammatory cytokines play and important role in potentiating ongoing damage.
Page 555 :
, , , , Post-operative renal failure is more likely to occur in patients who are elderly, have, peripheral vascular disease, high BMI, have COPD, receive vasopressors, are on, nephrotoxic medication or undergo emergency surgery., Avoiding hypotension will reduce risk of renal tubular damage., There is no evidence that administration of ACE inhibitors or dopamine reduces the, incidence of post-operative renal failure., Next question
Page 556 :
Question 74 of 347, A 56 year old man has undergone a radical nephrectomy. The pathologist bisects the kidney and, identifies a pink fleshy tumour in the renal pelvis. What is the most likely disease?, , Renal cell carcinoma, , Transitional cell carcinoma, , Angiomyolipoma, , Phaeochromocytoma, , Renal adenoma, Most renal tumours are yellow or brown in colour. TCC's are one of the few tumours to appear pink., Theme from April 2012, The finding of a TCC in the renal pelvis mandates a nephroureterectomy., Please rate this question:, , Discuss and give feedback, , Next question, , Renal lesions, Lesion, , Renal cell, carcinoma, , Disease specific features, , , , , , Most present with haematuria, (50%), Common renal tumour (85%, cases), Paraneoplastic features include, hypertension and polycythaemia, Most commonly has, haematogenous mestastasis, , Treatment, , Usually radical or partial, nephrectomy
Page 557 :
Lesion, , Nephroblastoma, , Disease specific features, , , , , , , , Neuroblastoma, , , , , , , , , , Transitional cell, carcinoma, , , , , , , , , , Angiomyolipoma, , , , , , Treatment, , Rare childhood tumour, It accounts for 80% of all, genitourinary malignancies in, those under the age of 15 years, Up to 90% will have a mass, 50% will be hypertensive, Diagnostic work up includes, ultrasound and CT scanning, , Surgical resection combined, with chemotherapy (usually, vincristine, actinomycin D and, doxorubicin), , Most common extracranial, tumour of childhood, 80% occur in those under 4 years, of age, Tumour of neural crest origin (up, to 50% occur in the adrenal, gland), The tumour is usually calcified, and may be diagnosed using, MIBG scanning, Staging is with CT, , Surgical resection, radiotherapy, and chemotherapy, , Accounts for 90% of, lower urinary tract tumours, but, only 10% of renal tumours, Males affected 3x more than, females, Occupational exposure to, industrial dyes and rubber, chemicals may increase risk, Up to 80% present with painless, haematuria, Diagnosis and staging is with CT, IVU, , Radical nephroureterectomy, , 80% of these hamartoma type, lesions occur sporadically, the, remainder are seen in those with, tuberous sclerosis, Tumour is composed of blood, vessels, smooth muscle and fat, , 50% of patients with lesions, >4cm will have symptoms and, will require surgical resection
Page 558 :
Lesion, , Disease specific features, , , Treatment, , Massive bleeding may occur in, 10% of cases, Next question
Page 559 :
Question 75 of 347, , A 65 year old lady presents with a lesion affecting her right breast. On examination she has a, weeping, crusting lesion overlying the right nipple, the areolar region is not involved. There is no, palpable mass lesion in the breast, there is a palpable axillary lymph node. The patient's general, practitioner has tried treating the lesion with 1% hydrocortisone cream, with no success. What is the, most likely diagnosis?, , Infection with Staphylococcus aureus, , Pagets disease of the nipple, , Phylloides tumour, , Nipple eczema, , Basal cell carcinoma, , A weeping, crusty lesion such as this is most likely to represent Pagets disease of the nipple, (especially since the areolar region is spared). Although no mass lesion is palpable, a proportion of, patients will still have an underlying invasive malignancy (hence the lymphadenopathy)., Please rate this question:, , Discuss and give feedback, , Next question, , Pagets disease of the nipple, Pagets disease is an eczematoid change of the nipple associated with an underlying breast, malignancy and it is present in 1-2% of patients with breast cancer. In half of these patients, it is, associated with an underlying mass lesion and 90% of such patients will have an invasive, carcinoma. 30% of patients without a mass lesion will still be found to have an underlying carcinoma.
Page 560 :
The remainder will have carcinoma in situ., Pagets disease differs from eczema of the nipple in that it involves the nipple primarily and only, latterly spreads to the areolar (the opposite occurs in eczema)., Diagnosis is made by punch biopsy, mammography and ultrasound of the breast., Treatment will depend on the underlying lesion., Next question
Page 561 :
Question 76 of 347, A 73 year old man presents with haemoptysis and is suspected of suffering from lung cancer. On, examination he has an enlarged supraclavicular lymph node. Which of the following features is most, likely to be present on histological examination?, , Increased mitoses, , Apoptosis, , Barr Bodies, , Multinucleate giant cells, , Granuloma, , Theme from 2011 Exam, Increased mitoses are commonly seen in association with malignant transformation of cells., Apoptosis is not a common feature of metastatic cancer. Barr Bodies are formed during X, chromosome inactivation in female somatic cells., Please rate this question:, , Discuss and give feedback, , Next question, , Histopathology of malignancy, , , , , , , , , , Abnormal tissue architecture, Coarse chromatin, Invasion of basement membrane*, Abnormal mitoses, Angiogenesis, De-differentiation, Areas of necrosis, Nuclear pleomorphism, , *= Those features that distinguish invasive malignancy from in situ disease, Next question
Page 562 :
Question 77 of 347, , Which of the following pathological explanations best describes the initial pathological processes, occurring in an abdominal aortic aneurysm in an otherwise well 65 year old, hypertensive male?, , Loss of elastic fibres from the adventitia, , Loss of collagen from the adventitia, , Loss of collagen from the media, , Loss of elastic fibres from the media, , Decreased matrix metalloproteinases in the adventitia, , Theme from April 2012 Exam, Theme from April 2013 Exam, In established aneurysmal disease there is dilation of all layers of the arterial wall and loss of both, elastin and collagen. The primary event is loss of elastic fibres with subsequent degradation of, collagen fibres., Please rate this question:, , Discuss and give feedback, , Next question, , Pathology of abdominal aortic aneurysm, Abdominal aortic aneurysms occur primarily as a result of the failure of elastic proteins within the, extracellular matrix. Aneurysms typically represent dilation of all layers of the arterial wall. Most, aneurysms are caused by degenerative disease. After the age of 50 years the normal diameter of, the infrarenal aorta is 1.5cm in females and 1.7cm in males. Diameters of 3cm and greater, are, considered aneurysmal. The pathophysiology involved in the development of aneurysms is complex
Page 563 :
and the primary event is loss of the intima with loss of elastic fibres from the media. This process is, associated with, and potentiated by, increased proteolytic activity and lymphocytic infiltration., Major risk factors for the development of aneurysms include smoking and hypertension. Rare but, important causes include syphilis and connective tissues diseases such as Ehlers Danlos type 1 and, Marfans syndrome., Layers of arterial wall, , Image sourced from Wikipedia, , Next question
Page 564 :
Question 78 of 347, A 28 year old lady has a malignant melanoma removed from her calf. Which of the following, pathological criteria carries the greatest prognostic weighting?, , Vascular invasion, , Abnormal mitoses, , Breslow thickness, , Perineural invasion, , Lymphocytic infiltrates, , Theme from April 2012 exam, Theme from September 2013 exam, The Breslow thickness has considerable prognostic importance. Lymphocytic infiltrates may be, associated with an improved prognosis, but do not carry nearly the same weight as increased, thickness., Please rate this question:, , Discuss and give feedback, , Next question, , Malignant melanoma, The main diagnostic features (major criteria):, , , , , Change in size, Change in shape, Change in colour, , Treatment, , Secondary features (minor criteria), , , , , , Diameter >6mm, Inflammation, Oozing or bleeding, Altered sensation
Page 565 :
, , , Suspicious lesions should undergo excision biopsy. The lesion should be removed in, completely as incision biopsy can make subsequent histopathological assessment difficult., Once the diagnosis is confirmed the pathology report should be reviewed to determine, whether further re-excision of margins is required (see below):, , Margins of excision-Related to Breslow thickness, , Lesions 0-1mm thick, , 1cm, , Lesions 1-2mm thick, , 1- 2cm (Depending upon site and pathological features), , Lesions 2-4mm thick, , 2-3 cm (Depending upon site and pathological features), , Lesions >4 mm thick, , 3cm, , Marsden J et al Revised UK guidelines for management of Melanoma. Br J Dermatol 2010 163:238256., Further treatments such as sentinel lymph node mapping, isolated limb perfusion and block, dissection of regional lymph node groups should be selectively applied., Next question
Page 566 :
Question 79 of 347, A 34 year old lady undergoes an elective cholecystectomy for attacks of recurrent cholecystitis due, to gallstones. Microscopic assessment of the gallbladder is most likely to show which of the, following?, , Dysplasia of the fundus, , Widespread necrosis, , Ashoff-Rokitansky sinuses, , Metaplasia of the fundus, , None of the above, , Aschoff-Rokitansky sinuses are the result of hyperplasia and herniation of epithelial cells through the, fibromuscular layer of the gallbladder wall. They may be macroscopic or microscopic. AshoffRokitansky sinuses may be identified in cases of chronic cholecystitis and gallstones. Although, gallstones may predispose to the development of gallbladder cancer the actual incidence of, dysplasia and metaplastic change is rare. In the elective setting described above necrosis would be, rare., Please rate this question:, , Discuss and give feedback, , Next question, , Gallbladder, , , , Fibromuscular sac with capacity of 50ml, Columnar epithelium, , Relations of the gallbladder, , Anterior, , Posterior, , Liver, , , , Covered by peritoneum, Transverse colon
Page 567 :
, , 1st part of the duodenum, , Laterally, , Right lobe of liver, , Medially, , Quadrate lobe of liver, , Arterial supply, Cystic artery (branch of Right hepatic artery), Venous drainage, Directly to the liver, Nerve supply, Sympathetic- mid thoracic spinal cord, Parasympathetic- anterior vagal trunk, Common bile duct, , Origin, , Confluence of cystic and common hepatic ducts, , Relations at, origin, , , , , Medially - Hepatic artery, Posteriorly- Portal vein, , Relations distally, , , , , , Duodenum - anteriorly, Pancreas - medially and laterally, Right renal vein - posteriorly, , Arterial supply, , Branches of hepatic artery and retroduodenal branches of gastroduodenal, artery, , Hepatobiliary triangle, , Medially, , Common hepatic duct, , Inferiorly, , Cystic duct, , Superiorly, , Inferior edge of liver
Page 568 :
Cystic artery, , Contents, , Relations of the gallbladder, , © Image provided by the University of Sheffield, , Next question
Page 569 :
Question 80 of 347, Which of the following are not true of Li-Fraumeni syndrome?, , It consists of mutations to the p53 tumour suppressor gene, , Is likely to be present in a teenager presenting with a liposarcoma, , It has an autosomal dominant inheritance pattern, , Affected individuals are unlikely to develop acute myeloid leukaemia, , Adrenal malignancies are more common than in normal population, , They are at high risk of developing leukaemia., Please rate this question:, , Discuss and give feedback, , Next question, , Genetics and surgical disease, Some of the more commonly occurring genetic conditions occurring in surgical patients are, presented here., Li-Fraumeni Syndrome, , , , , , Autosomal dominant, Consists of germline mutations to p53 tumour suppressor gene, High incidence of malignancies particularly sarcomas and leukaemias, Diagnosed when:, , *Individual develops sarcoma under 45 years, *First degree relative diagnosed with any cancer below age 45 years and another family member, develops malignancy under 45 years or sarcoma at any age, BRCA 1 and 2
Page 570 :
, , , , Carried on chromosome 17 (BRCA 1) and Chromosome 13 (BRCA 2), Linked to developing breast cancer (60%) risk., Associated risk of developing ovarian cancer (55% with BRCA 1 and 25% with BRCA 2)., , Lynch Syndrome, , , , , , Autosomal dominant, Develop colonic cancer and endometrial cancer at young age, 80% of affected individuals will get colonic and/ or endometrial cancer, High risk individuals may be identified using the Amsterdam criteria, , Amsterdam criteria, Three or more family members with a confirmed diagnosis of colorectal cancer, one of whom is a, first degree (parent, child, sibling) relative of the other two., Two successive affected generations., One or more colon cancers diagnosed under age 50 years., Familial adenomatous polyposis (FAP) has been excluded., Gardners syndrome, , , , , , , , , Autosomal dominant familial colorectal polyposis, Multiple colonic polyps, Extra colonic diseases include: skull osteoma, thyroid cancer and epidermoid cysts, Desmoid tumours are seen in 15%, Mutation of APC gene located on chromosome 5, Due to colonic polyps most patients will undergo colectomy to reduce risk of colorectal, cancer, Now considered a variant of familial adenomatous polyposis coli, Next question
Page 571 :
Question 81 of 347, A 35 year old type 1 diabetic presents with difficulty mobilising and back pain radiating to the thigh., He has a temperature of 39 oC and has pain on extension of the hip. He is diagnosed with an, iliopsoas abscess. Which of the following statements is false in relation to his diagnosis?, , Staphylococcus aureus is the most likely primary cause, , Recurrence occurs in 60% cases, , More common in males, , Crohn's is the most likely secondary cause, , CT guided drainage is preferable first line management, , Classical features include: a limp, back pain and fever. Recurrence rates are about 1520%.Staphylococcus is the commonest primary cause, others include Streptococcus and E.coli., Management is ideally by CT guided drainage., Please rate this question:, , Discuss and give feedback, , Next question, , Iliopsoas abscess, , , , Collection of pus in iliopsoas compartment (iliopsoas and iliacus), Causes:, , Primary, , , , , Haematogenous spread of bacteria, Staphylococcus aureus: most common, , Secondary
Page 572 :
, , , , , , , Crohn's (commonest cause in this category), Diverticulitis, Colorectal cancer, UTI, GU cancers, Vertebral osteomyelitis, Femoral catheter, lithotripsy, Endocarditis, , Note the mortality rate can be up to 19-20% in secondary iliopsoas abscesses compared with 2.4%, in primary abscesses., Clinical features, , , , , , , Fever, Back/flank pain, Limp, Weight loss, , Clinical examination, , , , Patient in the supine position with the knee flexed and the hip mildly externally rotated, , , , Specific tests to diagnose iliopsoas inflammation:, , Place hand proximal to the patient's ipsilateral knee and ask patient to lift thigh against your hand., This will cause pain due to contraction of the psoas muscle., Lie the patient on the normal side and hyperextend the affected hip. In inflammation this should elicit, pain as the psoas muscle is stretched., Investigation, , , , CT is gold standard, , Management, , , , Antibiotics
Page 573 :
, , , Percutaneous drainage, Surgery is indicated if:, , 1. Failure of percutaneous drainage, 2. Presence of an another intra-abdominal pathology which requires surgery, Surgical approach, The authors technique for draining these collections is given here., Review the CT scans and plan surgical approach. An extraperitoneal approach is important., The collection usually extends inferiorly and can be accessed from an incision at a level of L4 on the, affected side., GA, Transverse laterally placed incision., Incise external oblique., Split the subsequent muscle layers., As you approach the peritoneum use blunt dissection to pass laterally around it., Remember the ureter and gonadal veins lie posterior at this level., Eventually you will enter the abscess cavity, a large amount of pus is usually released at this point., Drain the area with suction and washout with saline., Place a corrugated drain well into the abscess cavity., If you have made a small skin incision it is reasonable to bring the drain up through the skin wound., Otherwise place a lateral exit site and close the skin and external oblique. If you do this ensure that, you use interrupted sutures., Anchor the drain with strong securely tied silk sutures (it is extremely tiresome if it falls out!), Reference, Iliopsoas abscesses, I H Mallick, M H Thoufeeq, T P Rajendran, Postgrad Med J 2004;80:459-462, Next question
Page 574 :
Question 82 of 347, Which of the following statements relating to parathyroid neoplasms is incorrect?, , 15% of cases are due to parathyroid carcinoma, , 80% of cases are due to parathyroid adenomas, , Parathyroid adenomas are often encapsulated, , 10% of parathyroid adenomas develop in ectopically located glands, , 85% of cases of primary hyperparathyroidism are due to solitary adenomas, , Parathyroid carcinomas account for up to 5% of tumours. Adenomas are often encapsulated., Lesions that are fibrotic and densely adherent to the gland may be a carcinoma. 85% cases of, primary hyperparathyroidism are due to a single adenoma and this is the reason some surgeons, favour a focused parathyroidectomy., Please rate this question:, , Discuss and give feedback, , Next question, , Parathyroid glands and disorders of calcium metabolism, Hyperparathyroidism, , Disease type, , Primary, hyperparathyroidism, , Hormone profile, , , , , , PTH (Elevated), Ca2+(Elevated), Phosphate (Low), Urine calcium :, creatinine clearance, ratio > 0.01, , Clinical features, , Cause, , May be, asymptomatic if, mild, Recurrent, abdominal pain, (pancreatitis, renal, colic), Changes to, emotional or, , Most cases due to, solitary adenoma, (80%), multifocal, disease occurs in 1015% and parathyroid, carcinoma in 1% or, less
Page 575 :
Disease type, , Hormone profile, , Clinical features, , Cause, , cognitive state, Secondary, hyperparathyroidism, , , , , , , Tertiary, hyperparathyroidism, , , , , , , , , PTH (Elevated), Ca2+ (Low or, normal), Phosphate, (Elevated), Vitamin D levels, (Low), , May have few, symptoms, Eventually may, develop bone, disease, osteitis, fibrosa cystica and, soft tissue, calcifications, , Parathyroid gland, hyperplasia occurs as, a result of low, calcium, almost, always in a setting of, chronic renal failure, , Ca2+(Normal or, high), PTH (Elevated), Phosphate levels, (Decreased or, Normal), Vitamin D (Normal, or decreased), Alkaline, phosphatase, (Elevated), , Metastatic, calcification, Bone pain and /, or fracture, Nephrolithiasis, Pancreatitis, , Occurs as a result of, ongoing hyperplasia, of the parathyroid, glands after, correction of, underlying renal, disorder, hyperplasia, of all 4 glands is, usually the cause, , Differential diagnoses, It is important to consider the rare but relatively benign condition of benign familial hypocalciuric, hypercalcaemia, caused by an autosomal dominant genetic disorder. Diagnosis is usually made by, genetic testing and concordant biochemistry (urine calcium : creatinine clearance ratio <0.01distinguished from primary hyperparathyroidism)., Treatment, Primary hyperparathyroidism, Indications for surgery, , , , , , , , , , Elevated serum Calcium > 1mg/dL above normal, Hypercalciuria > 400mg/day, Creatinine clearance < 30% compared with normal, Episode of life threatening hypercalcaemia, Nephrolithiasis, Age < 50 years, Neuromuscular symptoms, Reduction in bone mineral density of the femoral neck, lumbar spine, or distal radius of more, than 2.5 standard deviations below peak bone mass (T score lower than -2.5)
Page 576 :
Secondary hyperparathyroidism, Usually managed with medical therapy., Indications for surgery in secondary (renal) hyperparathyroidism:, , , , , Bone pain, Persistent pruritus, Soft tissue calcifications, , Tertiary hyperparathyroidism, Allow 12 months to elapse following transplant as many cases will resolve, The presence of an autonomously functioning parathyroid gland may require surgery. If the culprit, gland can be identified then it should be excised. Otherwise total parathyroidectomy and reimplantation of part of the gland may be required., References, 1. Pitt S et al. Secondary and Tertiary Hyperparathyroidism, State of the Art Surgical, Management.Surg Clin North Am 2009 Oct;89(5):1227-39., 2. MacKenzie-Feder J et al. Primary Hyperparathyroidism: An Overview. Int J Endocrinol 2011;, 2011: 251410., Next question
Page 577 :
Question 83 of 347, A 20 year old girl presents with a thyroid cancer, she is otherwise well with no significant family, history. On examination she has a nodule in the left lobe of the thyroid with a small discrete mass, separate from the gland itself. Which of the following is the most likely cause?, , Follicular carcinoma, , Anaplastic carcinoma, , Medullary carcinoma, , Papillary carcinoma, , B Cell Lymphoma, , Theme from September 2011 Exam, Papillary carcinoma is the most common subtype and may cause lymph node metastasis (mass, separate from the gland itself) that is rare with follicular tumours. Anaplastic carcinoma would cause, more local symptoms and would be rare in this age group., Please rate this question:, , Discuss and give feedback, , Next question, , Thyroid malignancy, Papillary carcinoma, , , , , , Commonest sub-type, Accurately diagnosed on fine needle aspiration cytology, Histologically, they may demonstrate psammoma bodies (areas of calcification) and so, called 'orphan Annie' nuclei, They typically metastasise via the lymphatics and thus laterally located apparently ectopic, thyroid tissue is usually a metastasis from a well differentiated papillary carcinoma, , Follicular carcinoma
Page 578 :
, , , , , Are less common than papillary lesions, Like papillary tumours, they may present as a discrete nodule. Although they appear to be, well encapsulated macroscopically there is invasion on microscopic evaluation, Lymph node metastases are uncommon and these tumours tend to spread, haematogenously. This translates into a higher mortality rate, Follicular lesions cannot be accurately diagnosed on fine needle aspiration cytology and thus, all follicular FNA's (THY 3f) will require at least a hemi thyroidectomy, , Anaplastic carcinoma, , , , Less common and tend to occur in elderly females, Disease is usually advanced at presentation and often only palliative decompression and, radiotherapy can be offered., , Medullary carcinoma, , , , , , These are tumours of the parafollicular cells ( C Cells) and are of neural crest origin., The serum calcitonin may be elevated which is of use when monitoring for recurrence., They may be familial and occur as part of the MEN -2A disease spectrum., Spread may be either lymphatic or haematogenous and as these tumours are not derived, primarily from thyroid cells they are not responsive to radioiodine., , Lymphoma, , , , These respond well to radiotherapy, Radical surgery is unnecessary once the disease has been diagnosed on biopsy material., Such biopsy material is not generated by an FNA and thus a core biopsy has to be obtained, (with care!)., Next question
Page 579 :
Question 84 of 347, A 28 year old lady is breast feeding her first child. She presents with discomfort of the right breast., Clinical examination demonstrates erythema and an area that is fluctuant. Aspiration and culture of, the fluid is most likely to demonstrate infection with which of the following organisms?, , Clostridium perfringens, , Staphylococcus aureus, , Streptococcus pyogenes, , Staphylococcus epidermidis, , Actinomycosis, , Theme from April 2014 Exam, Staphylococcus aureus is the commonest cause. The infants mouth is usually the source as it, damages the nipple areolar complex allowing entry of bacteria., Please rate this question:, , Discuss and give feedback, , Next question, , Breast abscess, , , , , , In lactational women Staphylococcus aureus is the most common cause, Typical presentation is with a tender, fluctuant mass in a lactating women, Diagnosis and treatment is performed using USS and associated drainage of the abscess, cavity. Antibiotics should also be administered, Where there is necrotic skin overlying the abscess, the patient should undergo surgery, Next question
Page 580 :
Question 85 of 347, , A 20 year old male presents with a tense, swollen knee joint. There is no history of antecedent, trauma. On examination the joint is tense and swollen but there is no sign of injury. Plain x-rays, show no fracture or arthritis. What is the most likely explanation?, , Rupture of the anterior cruciate ligament, , Rupture of the medial collateral ligament, , Tibial plateau fracture, , Haemophilia A, , von Willebrands disease, Haemarthrosis without trauma is typically a feature of haemophilia A and B, , Theme from 2014 Exam, Without a history of trauma, ligamentous rupture or tibial plateau fractures would be unusual., Please rate this question:, , Discuss and give feedback, , Next question, , Abnormal coagulation, Cause, , Factors affected
Page 581 :
Cause, , Factors affected, , Heparin, , Prevents activation factors 2,9,10,11, , Warfarin, , Affects synthesis of factors 2,7,9,10, , DIC, , Factors 1,2,5,8,11, , Liver disease, , Factors 1,2,5,7,9,10,11, , Interpretation blood clotting test results, , Disorder, , APTT, , PT, , Bleeding time, , Haemophilia, , Increased, , Normal, , Normal, , von Willebrand's disease, , Increased, , Normal, , Increased, , Vitamin K deficiency, , Increased, , Increased, , Normal, Next question
Page 582 :
Question 86 of 347, An 18 year old rock climber falls onto his left arm and sustains a large haematoma of the left upper, arm. Unfortunately the wound associated with the injury is neglected and it becomes infected. Which, of these changes is least likely to occur?, , Axillary lymphadenopathy, , Leucopenia, , Tenderness, , Mild pyrexia, , Local formation of yellow pus, , Leucopenia would be unusual and should prompt a search for another cause., Please rate this question:, , Discuss and give feedback, , Next question, , Acute inflammation, Inflammation is the reaction of the tissue elements to injury. Vascular changes occur, resulting in the, generation of a protein rich exudate. So long as the injury does not totally destroy the existing tissue, architecture, the episode may resolve with restoration of original tissue architecture., Vascular changes, , , , , , Vasodilation occurs and persists throughout the inflammatory phase., Inflammatory cells exit the circulation at the site of injury., The equilibrium that balances Starlings forces within capillary beds is disrupted and a protein, rich exudate will form as the vessel walls also become more permeable to proteins., The high fibrinogen content of the fluid may form a fibrin clot. This has several important, immunomodulatory functions., , Sequelae
Page 583 :
Resolution, , , , , Typically occurs with minimal initial injury, Stimulus removed and normal tissue architecture results, , Organisation, , , , , Delayed removal of exudate, Tissues undergo organisation and usually fibrosis, , Suppuration, , , , , Typically formation of an abscess or an empyema, Sequestration of large quantities of dead neutrophils, , Progression to chronic, inflammation, , , , , Coupled inflammatory and reparative activities, Usually occurs when initial infection or suppuration has, been inadequately managed, , Causes, , , , , , , Infections e.g. Viruses, exotoxins or endotoxins released by bacteria, Chemical agents, Physical agents e.g. Trauma, Hypersensitivity reactions, Tissue necrosis, , Presence of neutrophil polymorphs is a histological diagnostic feature of acute inflammation, Next question
Page 584 :
Question 87-89 of 347, Theme: Tumour markers, , A., B., C., D., E., F., G., H., I., , Invasive ductal carcinoma of the breast, Prostate cancer, Gastric cancer, Ovarian cancer, Colorectal cancer, Pancreatic adenocarcinoma, Seminoma testicular cancer, Non-seminomatous testicular cancer, Hepatocellular carcinoma, , For each tumour marker please select the most likely underlying malignancy. Each option may be, used once, more than once or not at all., , 87., , Raised beta-human chorionic gonadotropin with a raised alpha-feto protein level, You answered Invasive ductal carcinoma of the breast, The correct answer is Non-seminomatous testicular cancer, Theme from April 2012 Exam, A raised alpha-feto protein level excludes a seminoma, , 88., , Elevated CA 19-9, You answered Invasive ductal carcinoma of the breast, The correct answer is Pancreatic adenocarcinoma, , 89., , Raised alpha-feto protein level in a 54-year-old woman, You answered Invasive ductal carcinoma of the breast, The correct answer is Hepatocellular carcinoma, , Please rate this question:
Page 586 :
Question 90-92 of 347, Theme: Benign breast lesions, , A., B., C., D., E., F., G., H., , Fibroadenoma, Breast abscess, Cyst of Montgomery's gland, Galactocele, Lipoma, Duct ectasia, Intraductal papilloma, Fat necrosis, , What is the most likely diagnosis for the scenario given? Each option may be used once, more than, once or not at all., , 90., , A 64 year old obese female presents with a breast lump. She was hit on the breast by a, cricket ball when playing with her grandson., You answered Fibroadenoma, The correct answer is Fat necrosis, An obese, post menopausal woman, with a history of trauma points towards fat necrosis., Trauma causes inflammation of fat cells, leading to formation of a lump. Mammography,, USS and biopsy are usually needed to differentiate it from breast malignancy., , 91., , A 21 year old female notices a bloody discharge from the nipple. She is otherwise well. On, examination there are no discrete lesions to feel and mammography shows dense breast, tissue but no mass lesion., You answered Fibroadenoma, The correct answer is Intraductal papilloma, Intraductal papillomata are the commonest cause of blood stained nipple discharge in, younger women. There is seldom any palpable mass. An ultrasound is required and, possibly a galactogram., , 92., , A 18 year old female notices a non tender mobile breast lump. Clinically there is a smooth, lump which is not tethered to the skin., Fibroadenoma
Page 587 :
Also called a breast 'mouse' due to its mobility. It is a benign condition arising from the, breast lobule. May enlarge in pregnancy., Please rate this question:, , Discuss and give feedback, , Next question, , Benign breast lesions, Lesion, , Fibroadenoma, , Features, , , , , , , Breast cyst, , , , , , , , Sclerosing adenosis,, (radial scars and, complex sclerosing, lesions), , , , , , , , , Treatment, , Develop from a whole lobule, Mobile, firm breast lumps, 12% of all breast masses, Over a 2 year period up to, 30% will get smaller, No increase in risk of, malignancy, , If >3cm surgical excision is usual,, Phyllodes tumours should be, widely excised (mastectomy if the, lesion is large), , 7% of all Western females, will present with a breast, cyst, Usually presents as a smooth, discrete lump (may be, fluctuant), Small increased risk of breast, cancer (especially if, younger), , Cysts should be aspirated, those, which are blood stained or, persistently refill should be, biopsied or excised, , Usually presents as a breast, lump or breast pain, Causes mammographic, changes which may mimic, carcinoma, Cause distortion of the distal, lobular unit, without, hyperplasia (complex lesions, will show hyperplasia), Considered a disorder of, , Lesions should be biopsied,, excision is not mandatory
Page 588 :
Lesion, , Features, , Treatment, , involution, no increase in, malignancy risk, Epithelial hyperplasia, , , , , , , , Fat necrosis, , , , , , Duct papilloma, , , , , , , Variable clinical presentation, ranging from generalised, lumpiness through to discrete, lump, Disorder consists of, increased cellularity of, terminal lobular unit,, atypical features may be, present, Atypical features and family, history of breast cancer, confers greatly increased risk, of malignancy, , If no atypical features then, conservative, those with atypical, features require either close, monitoring or surgical resection, , Up to 40% cases usually, have a traumatic aetiology, Physical features usually, mimic carcinoma, Mass may increase in size, initially, , Imaging and core biopsy, , Usually present with nipple, discharge, Large papillomas may, present with a mass, The discharge usually, originates from a single duct, No increase risk of, malignancy, , Microdochectomy, , Next question
Page 589 :
Question 93 of 347, A 17 year old man is identified as having a Meckels diverticulum. From which of the following, embryological structures is it derived?, , Foregut, , Hindgut, , Urachus, , Cloaca, , Vitello-intestinal duct, Rule of 2's, 2% of population, 2 inches (5cm) long, 2 feet (60 cm) from the ileocaecal valve, 2 x's more common in men, 2 tissue types involved, The Meckels diverticulum is a persistence of the vitello-intestinal duct., Please rate this question:, , Discuss and give feedback, , Next question, , Meckel's diverticulum, , , , , , , , , Congenital abnormality resulting in incomplete obliteration of the vitello-intestinal duct, Normally, in the foetus, there is an attachment between the vitello-intestinal duct and the yolk, sac.This disappears at 6 weeks gestation., The tip is free in majority of cases., Associated with enterocystomas, umbilical sinuses, and omphaloileal fistulas., Arterial supply: omphalomesenteric artery., 2% of population, 2 inches long, 2 feet from the ileocaecal valve., Typically lined by ileal mucosa but ectopic gastric mucosa can occur, with the risk of peptic, ulceration. Pancreatic and jejunal mucosa can also occur.
Page 590 :
Clinical, , , , , Normally asymptomatic and an incidental finding., Complications are the result of obstruction, ectopic tissue, or inflammation., Removal if narrow neck or symptomatic. Options are between wedge excision or formal, small bowel resection and anastomosis., Next question
Page 591 :
Question 94-96 of 347, Theme: Rectal bleeding, , A., B., C., D., E., F., , Solitary rectal ulcer syndrome, Haemorrhoidal disease, Fissure in ano, Fistula in ano, Anal cancer, Ulcerative colitis, , Please select the most likely diagnosis for the scenario given. Each option may be used once, more, than once or not at all., , 94., , A 22 year old man presents with a 6 day history of passage of bloody diarrhoea with, passage of mucous and slime. He is passing an average of 8 to 9 bowel movements per, day. On digital rectal examination there is no discrete abnormality to feel, but there is, some blood stained mucous on the glove., You answered Solitary rectal ulcer syndrome, The correct answer is Ulcerative colitis, The passage of bloody diarrhoea together with mucous and a short history makes this a, likely first presentation of inflammatory bowel disease., , 95., , A 17 year old man presents with a 2 week history of significant pain on defecation, accompanied by the presence of a small amount of blood which is noticed on toilet paper., You answered Solitary rectal ulcer syndrome, The correct answer is Fissure in ano, Young patients with painful rectal bleeding may have a fissure. Treatment is with stool, softeners and either GTN or Diltiazem initially., , 96., , A 24 year old woman presents with a long history of obstructed defecation and chronic, constipation. She often strains to open her bowels for long periods and occasionally, notices that she has passed a small amount of blood. On examination she has an indurated, area located anteriorly approximately 3cm proximal to the anal verge., Solitary rectal ulcer syndrome
Page 592 :
Solitary rectal ulcers are associated with chronic constipation and straining. It will need to, be biopsied to exclude malignancy (the histological appearances are characteristic)., Diagnostic work up should include endoscopy and probably defecating proctogram and, ano-rectal manometry studies., Please rate this question:, , Discuss and give feedback, , Next question, , Rectal bleeding, Rectal bleeding is a common cause for patients to be referred to the surgical clinic. In the clinical, history it is useful to try and localise the anatomical source of the blood. Bright red blood is usually of, rectal anal canal origin, whilst dark red blood is more suggestive of a proximally sited bleeding, source. Blood which has entered the GI tract from a gastro-duodenal source will typically resemble, malaena due to the effects of the digestive enzymes on the blood itself., In the table below we give some typical bleeding scenarios together with physical examination, findings and causation., , Cause, , Type of, bleeding, , Features in history, , Examination findings, , Fissure in, ano, , Bright red, rectal, bleeding, , Painful bleeding that occurs, post defecation in small, volumes. Usually antecedent, features of constipation, , Muco-epithelial defect usually, in the midline posteriorly, (anterior fissures more likely to, be due to underlying disease), , Haemorroids, , Bright red, rectal, bleeding, , Post defecation bleeding noted, both on toilet paper and drips, into pan. May be alteration of, bowel habit and history of, straining. No blood mixed with, stool. No local pain., , Normal colon and rectum., Proctoscopy may show internal, haemorrhoids. Internal, haemorrhoids are usually, impalpable., , Crohns, disease, , Bright red or, mixed blood, , Bleeding that is accompanied, by other symptoms such as, altered bowel habit, malaise,, history of fissures (especially, , Perineal inspection may show, fissures or fistulae. Proctoscopy, may demonstrate indurated, mucosa and possibly strictures., Skip lesions may be noted at
Page 593 :
anterior) and abscesses., , colonoscopy., , Ulcerative, colitis, , Bright red, bleeding, often mixed, with stool, , Diarrhoea, weight loss,, nocturnal incontinence, passage, of mucous PR., , Proctitis is the most marked, finding. Peri anal disease is, usually absent. Colonoscopy, will show continuous mucosal, lesion., , Rectal cancer, , Bright red, blood mixed, volumes, , Alteration of bowel habit., Tenesmus may be present., Symptoms of metastatic, disease., , Usually obvious mucosal, abnormality. Lesion may be, fixed or mobile depending upon, disease extent. Surrounding, mucosa often normal, although, polyps may be present., , Image showing a fissure in ano. Typically these are located posteriorly and in the midline. Fissures, at other sites may be associated with underlying disease., , Image sourced from Wikipedia, , Colonoscopic image of internal haemorroids. Note these may often be impalpable.
Page 594 :
Image sourced from Wikipedia, , Investigation, , , , , , , , , All patients presenting with rectal bleeding require digital rectal examination and proctosigmoidoscopy as a minimal baseline., Remember that haemorrhoids are typically impalpable and to attribute bleeding to these in, the absence of accurate internal inspection is unsatisfactory., In young patients with no other concerning features in the history a carefully performed, sigmoidoscopy that demonstrates clear haemorrhoidal disease may be sufficient. If clear, views cannot be obtained then patients require bowel preparation with an enema and a, flexible sigmoidscopy performed., In those presenting with features of altered bowel habit or suspicion of inflammatory bowel, disease a colonoscopy is the best test., Patients with excessive pain who are suspected of having a fissure may require an, examination under general or local anaesthesia., In young patients with external stigmata of fissure and a compatible history it is acceptable to, treat medically and defer internal examination until the fissure is healed. If the fissure fails to, heal then internal examination becomes necessary along the lines suggested above to, exclude internal disease., , Special tests, , , In patients with a malignancy of the rectum the staging investigations comprise an MRI of the, rectum to identify circumferential resection margin compromise and to identify mesorectal, nodal disease. In addition to this CT scanning of the chest abdomen and pelvis is necessary
Page 595 :
to stage for more distant disease. Some centres will still stage the mesorectum with endo, rectal ultrasound but this is becoming far less common., , , , Patients with fissure in ano who are being considered for surgical sphincterotomy and are, females who have an obstetric history should probably have ano rectal manometry testing, performed together with endo anal ultrasound. As this service is not universally available it is, not mandatory but in the absence of such information there are continence issues that may, arise following sphincterotomy., , Management, , Disease, , Management, , Fissure in ano, , GTN ointment 0.2% or diltiazem cream applied topically is the usual first line, treatment. Botulinum toxin for those who fail to respond. Internal, sphincterotomy for those who fail with botox, can be considered earlier in, males., , Haemorroids, , Lifestyle advice, for small internal haemorrhoids can consider injection, sclerotherapy or rubber band ligation. For external haemorrhoids consider, haemorrhoidectomy. Modern options include HALO procedure and stapled, haemorrhoidectomy., , Inflammatory, bowel disease, , Medical management- although surgery may be needed for fistulating Crohns, (setons)., , Rectal cancer, , Anterior resection or abdomino-perineal excision of the colon and rectum., Total mesorectal excision is now standard of care. Most resections below the, peritoneal reflection will require defunctioning ileostomy. Most patients will, require preoperative radiotherapy., Next question
Page 596 :
Question 97 of 347, Which of the following is the most common childhood brain tumour?, , Glioblastoma multiforme, , Astrocytoma, , Medulloblastoma, , Ependymoma, , Meningioma, , Glioblastoma multiforme is rare in childhood. In contrast, astrocytoma is the commonest brain, tumour in children. Medulloblastoma is no longer the commonest CNS tumour in children (Cancer, research UK), Please rate this question:, , Discuss and give feedback, , Next question, , CNS tumours, , , , , 60% = Glioma and metastatic disease, 20% = Meningioma, 10% = Pituitary lesions, , In paediatric practice medulloblastomas (neuroectodermal tumours) were the commonest lesions,, astrocytomas now account for the majority., Tumours arising in right temporal and frontal lobe may reach considerable size before becoming, symptomatic. Whereas tumours in the speech and visual areas will typically produce early, symptoms., Diagnosis, MRI Scanning provides the best resolution., Treatment, Usually surgery, even if tumour cannot be completely resected conditions such as rising ICP can be, addressed with tumour debulking and survival and quality of life prolonged., Curative surgery can usually be undertaken with lesions such as meningiomas. Gliomas have a
Page 597 :
marked propensity to invade normal brain and resection of these lesions is nearly always, incomplete., Next question
Page 598 :
Question 98 of 347, A keen surgical trainee is about to embark on her first hemi arthroplasty for a fractured neck of, femur. In the anaesthetic room the patient is given 1.2g intravenous co-amoxiclav. There is a, possible history of penicillin allergy but the patient is demented and the history is not checked. The, patient then develops severe respiratory compromise and haemodynamic collapse. Which, pathological process accounts for this event?, , Binding of the drug to circulating IgG class antibodies, , Recognition of the drug by IgE receptors on mast cells, , Drug initiated formation of hapten-protein complexes, , Binding of the drug to circulating IgM class antibodies, , None of the above, Anaphylactic shock:, Antigen recognised by IgE molecules on the surface of mast cells resulting in rapid degranulation, with release of histamine and other inflammatory cytokines., This is a case of anaphylactic shock. In anaphylaxis the mast cells degranulate., Please rate this question:, , Discuss and give feedback, , Next question, , Anaphylactic shock, , , Suspect if there has been exposure to an allergen, , Management, - Remove allergen, - ABCD, - Drugs:, Adrenaline 1:1000 0.5ml INTRAMUSCULARLY (not IV). Repeat after 5 mins if no response., Then Chlorpheniramine 10mg IV, Then Hydrocortisone 100-200mg IV
Page 599 :
Reference, Emergency treatment of anaphylactic reactions. Guidelines for healthcare providers. Working Group, of the Resuscitation Council (UK).2008, Next question
Page 600 :
Question 99 of 347, Which of the following hepatobiliary disorders are most classically associated with ulcerative colitis?, , Gallstones, , Primary sclerosing cholangitis, , Bile duct stones, , Liver hamartomas, , Hepatocellular carcinoma, , Primary sclerosing cholangitis is an idiopathic inflammation of the bile ducts. It may result in, episodes of cholestasis and cholangitis and ultimately result in the need for liver transplantation. It, carries a 10% risk of malignant transformation. Crohns disease is associated with gallstones due to, impaired entero-hepatic circulation. Apart from PSC, ulcerative colitis does not increase the risk of, other liver lesions., Please rate this question:, , Discuss and give feedback, , Next question, , Ulcerative colitis, Ulcerative colitis is a form of inflammatory bowel disease. Inflammation always starts at rectum,, does not spread beyond ileocaecal valve (although backwash ileitis may occur) and is continuous., The peak incidence of ulcerative colitis is in people aged 15-25 years and in those aged 55-65, years. It is less common in smokers., The initial presentation is usually following insidious and intermittent symptoms. Features include:, , , , , , , bloody diarrhoea, urgency, tenesmus, abdominal pain, particularly in the left lower quadrant, extra-intestinal features (see below)
Page 602 :
Management, , , , , Patients with long term disease are at increased risk of development of malignancy, Acute exacerbations are generally managed with steroids, in chronic patients agents such as, azathioprine and infliximab may be used, Individuals with medically unresponsive disease usually require surgery- in the acute phase, a sub total colectomy and end ileostomy. In the longer term a proctectomy will be required., An ileoanal pouch is an option for selected patients, , References, Ford A et al. Ulcerative colitis. BMJ 2013 (346):29-34., Next question
Page 603 :
Question 100 of 347, , Which of the following is least associated with thrombosis?, , Endothelial cell damage, , Use of tourniquets in surgery, , Formation of platelet aggregates, , Thrombocytopenia, , Carcinoma of the stomach, , All the other options either act directly to promote thrombosis e.g. endothelial cell damage or via, changes in consistency or flow of blood., Please rate this question:, , Discuss and give feedback, , Next question, , Abnormal coagulation, Cause, , Factors affected, , Heparin, , Prevents activation factors 2,9,10,11
Page 604 :
Cause, , Factors affected, , Warfarin, , Affects synthesis of factors 2,7,9,10, , DIC, , Factors 1,2,5,8,11, , Liver disease, , Factors 1,2,5,7,9,10,11, , Interpretation blood clotting test results, , Disorder, , APTT, , PT, , Bleeding time, , Haemophilia, , Increased, , Normal, , Normal, , von Willebrand's disease, , Increased, , Normal, , Increased, , Vitamin K deficiency, , Increased, , Increased, , Normal, Next question
Page 605 :
Question 101 of 347, A 16 year old boy develops a painful swelling of his distal femur. An osteoblastic sarcoma is, diagnosed. To which of the following sites is this lesion most likely to metastasise?, , Inguinal lymph nodes, , Common iliac lymph nodes, , Liver, , Brain, , Lung, Sarcomas in which Lymphatic Metastasis is seen:, 'RACE For MS', R: Rhabdomyosarcoma, A: Angiosarcoma, C: Clear cell sarcoma, E: Epithelial cell sarcoma, For: Fibrosarcoma, M: Malignant fibrous histiocytoma, S: Synovial cell sarcoma, Or, 'SCARE', Synovial sarcoma, Clear cell sarcoma, Angiosarcoma, Rhabdomyosarcoma, Epithelioid sarcoma, Sarcomas often metastasise via the haematogenous route and the lung is a common site for, sarcoma metastasis. The liver and brain are often spared (at least initially). A smaller number may, develop lymphatic metastasis (see above)., Please rate this question:
Page 606 :
Discuss and give feedback, , Next question, , Sarcomas, , , Malignant tumours of mesenchymal origin, , Types, May be either bone or soft tissue in origin., Bone sarcoma include:, , , , , Osteosarcoma, Ewings sarcoma (although non bony sites recognised), Chondrosarcoma - originate from Chondrocytes, , Soft tissue sarcoma are a far more heterogeneous group and include:, , , , , , Liposarcoma-adipocytes, Rhabdomyosarcoma-striated muscle, Leiomyosarcoma-smooth muscle, Synovial sarcomas- close to joints (cell of origin not known but not synovium), , Malignant fibrous histiocytoma is a sarcoma that may arise in both soft tissue and bone., Features, Certain features of a mass or swelling should raise suspicion for a sarcoma these include:, , , , , , Large >5cm soft tissue mass, Deep tissue location or intra muscular location, Rapid growth, Painful lump, , Assessment, Imaging of suspicious masses should utilise a combination of MRI, CT and USS. Blind biopsy should, not be performed prior to imaging and where required should be done in such a way that the biopsy, tract can be subsequently included in any resection., Ewings sarcoma, , , , , Commoner in males, Incidence of 0.3 / 1, 000, 000, Onset typically between 10 and 20 years of age
Page 607 :
, , , , Location by femoral diaphysis is commonest site, Histologically it is a small round tumour, Blood borne metastasis is common and chemotherapy is often combined with surgery, , Osteosarcoma, , , , , , , Mesenchymal cells with osteoblastic differentiation, 20% of all primary bone tumours, Incidence of 5 per 1,000,000, Peak age 15-30, commoner in males, Limb preserving surgery may be possible and many patients will receive chemotherapy, , Liposarcoma, , , , , , , , , Malignancy of adipocytes, Rare, approximately 2.5 per 1,000,000. They are the second most common soft tissue, sarcoma, Typically located in deep locations such as retroperitoneum, Affect older age group usually >40 years of age, May be well differentiated and thus slow growing although may undergo de-differentiation, and disease progression, Many tumours will have a pseudocapsule that can misleadingly allow surgeons to feel that, they can 'shell out' these lesions. In reality, tumour may invade at the edge of the, pseudocapsule and result in local recurrence if this strategy is adopted, Usually resistant to radiotherapy, although this is often used in a palliative setting, , Malignant Fibrous Histiocytoma, , , , , , , Tumour with large number of histiocytes, Most common sarcoma in adults, Also described as undifferentiated pleomorphic sarcoma NOS (i.e. Cell of origin is not, known), Four major subtypes are recognised: storiform-pleomorphic (70% cases), myxoid (less, aggressive), giant cell and inflammatory, Treatment is usually with surgical resection and adjuvant radiotherapy as this reduces the, likelihood of local recurrence, Next question
Page 608 :
Question 102 of 347, Infection with which of the following micro-organisms may result in a clinical picture resembling, achalasia of the oesphagus?, , Epstein Barr virus, , Wuchereria Bancrofti, , Candida Spp, , Trypanosoma Cruzi, , Helicobacter Pylori, , Infection with Trypanosoma Cruzi may result in destruction of the ganglion cells of the myenteric, plexus, resulting in a clinical picture similar to achalasia., Please rate this question:, , Discuss and give feedback, , Next question, , Trypanosoma Cruzi, , , , , , , , , Protozoan, Causes Chagas disease, Carried by bugs which infect the skin whilst feeding, Penetrate through open wounds and mucous membranes, Intracellular proliferation, Major infective sites include CNS, intestinal myenteric plexus, spleen, lymph nodes and, cardiac muscle, Chronic disease is irreversible, nifurtimox is used to treat acute infection, Next question
Page 609 :
Question 103 of 347, , A 72 year old man has been unwell for may years and following his death a post mortem is, performed. Tissue is submitted for microscopic evaluation. Evaluation of sections of the myocardium, demonstrates evidence of apple green birefringence with polarised light. What is the most likely, diagnosis?, , Amyloidosis, , SLE, , Tuberculosis, , Disseminated B cell lymphoma, , Systemic sclerosis, Amyloidosis = apple green birefringence with polarised light, , Theme from September 2015 Exam, Please rate this question:, , Discuss and give feedback, , Next question, , Amyloid, Amyloid is an extracellular protein deposit which is insoluble. These deposits disrupt normal tissue, structure and if excessive may affect function. All types of amyloid consist of a major fibrillar protein, that defines the type of amyloid (approximately 90%) plus various minor components., Amyloid is classified with the prefix A (for amyloid) and the suffix depending upon the fibrillary
Page 610 :
protein present. The main clinical types are AA and AL amyloidosis. Systemic AA amyloidosis is a, long-term complication of several chronic inflammatory disorders - e.g. rheumatoid arthritis,, ankylosing spondylitis, Crohn's disease, malignancies and conditions predisposing to recurrent, infections. AL amyloidosis results from extra-cellular deposition of fibril-forming monoclonal, immunoglobulin light chains (most commonly of lambda isotype). Most patients have evidence of, isolated monoclonal gammopathy or asymptomatic myeloma, and the occurrence of AL amyloidosis, in patients with symptomatic multiple myeloma or other B-cell lymphoproliferative disorders is, unusual. AL type amyloidosis is the most common variant. The kidney and heart are two of the most, commonly affected sites. Diagnosis is based on surgical biopsy and characteristic histological, features which consist birefringence under polarised light. Immunohistochemistry is used to, delineate the subtype. Treatment is usually targeted at the underlying cause., Next question
Page 611 :
Question 104 of 347, A 45-year-old man presents to surgical outpatients with a long history of recurrent abdominal pain, and vomiting. He is noted to have a peripheral motor neuropathy on examination. What is the most, likely diagnosis?, , Huntington's disease, , Myeloma, , Acute intermittent porphyria, , Lawrence-Moon-Biedl syndrome, , Friedreich's ataxia, , Neurological signs combined with abdominal pain is acute intermittent porphyria or lead poisoning, until proven otherwise., Please rate this question:, , Discuss and give feedback, , Next question, , Acute intermittent porphyria, Acute intermittent porphyria (AIP) is a rare autosomal dominant condition caused by a defect in, porphobilinogen deaminase, an enzyme involved in the biosynthesis of haem. The results in the, toxic accumulation of delta aminolaevulinic acid and porphobilinogen. It characteristically presents, with abdominal and neuropsychiatric symptoms in 20-40 year olds. AIP is more common in females, (5:1), Features, , , , , , abdominal: abdominal pain, vomiting, neurological: motor neuropathy, psychiatric: e.g. depression, hypertension and tachycardia common
Page 612 :
Diagnosis, , , , , , classically urine turns deep red on standing, raised urinary porphobilinogen (elevated between attacks and to a greater extent during, acute attacks), assay of red cells for porphobilinogen deaminase, raised serum levels of delta aminolaevulinic acid and porphobilinogen, Next question
Page 613 :
Question 105 of 347, A 56 year old man presents with episodic facial pain and discomfort whilst eating. He has suffered, from halitosis recently and he frequently complains of a dry mouth. He has a smooth swelling, underneath his right mandible. What is the most likely underlying diagnosis?, , Stone impacted in Whartons duct, , Stone impacted in Stensens duct, , Benign adenoma of the submandibular gland, , Adenocarcinoma of the submandibular gland, , Squamous cell carcinoma of the submandibular gland, , The symptoms are typical for sialolithiasis. The stones most commonly form in the submandibular, gland and therefore may occlude Whartons duct. Stensens duct drains the parotid gland., Please rate this question:, , Discuss and give feedback, , Next question, , Submandibular glands- disease, Physiology, The submandibular glands secrete approximately 800- 1000ml saliva per day. They typically, produce mixed seromucinous secretions. When parasympathetic activity is dominant; the secretions, will be more serous. The parasympathetic fibres are derived from the chorda tympani nerves and the, submandibular ganglion. Sensory fibres are conveyed by the lingual branch of the mandibular nerve., Sialolithiasis, , , , , , , 80% of all salivary gland calculi occur in the submandibular gland, 70% of the these calculi are radio-opaque, Stones are usually composed of calcium phosphate or calcium carbonate, Patients typically develop colicky pain and post prandial swelling of the gland, Investigation involves sialography to demonstrate the site of obstruction and associated, other stones
Page 614 :
, , Stones impacted in the distal aspect of Whartons duct may be removed orally, other stones, and chronic inflammation will usually require gland excision, , Sialadenitis, , , , , Usually occurs as a result of Staphylococcus aureus infection, Pus may be seen leaking from the duct, erythema may also be noted, Development of a sub mandibular abscess is a serious complication as it may spread, through the other deep fascial spaces and occlude the airway, , Submandibular tumours, , , , , , , Only 8% of salivary gland tumours affect the sub mandibular gland, Of these 50% are malignant (usually adenoid cystic carcinoma), Diagnosis usually involves fine needle aspiration cytology, Imaging is with CT and MRI, In view of the high prevalence of malignancy, all masses of the submandibular glands should, generally be excised., Next question
Page 615 :
Question 106 of 347, Which of the following cellular types or features is not seen in sarcoidosis?, , Reed Sternberg Cells, , T lymphocytes, , Macrophages, , Asteroid bodies, , B lymphocytes, , Reed Sternberg cells are seen in Hodgkins disease. All of the other cell types are seen in sarcoid., Please rate this question:, , Discuss and give feedback, , Next question, , Chronic inflammation, Overview, Chronic inflammation may occur secondary to acute inflammation.In most cases chronic, inflammation occurs as a primary process. These may be broadly viewed as being one of three main, processes:, , , , , Persisting infection with certain organisms such as Mycobacterium tuberculosis which results, in delayed type hypersensitivity reactions and inflammation., Prolonged exposure to non-biodegradable substances such as silica or suture materials, which may induce an inflammatory response., Autoimmune conditions involving antibodies formed against host antigens., , Acute vs. Chronic inflammation, , Acute inflammation, , Chronic inflammation
Page 616 :
Changes to existing vascular structure and increased, permeability of endothelial cells, , Angiogenesis predominates, , Infiltration of neutrophils, , Macrophages, plasma cells and, lymphocytes predominate, , Process may resolve with:, , Healing by fibrosis is the main result, , , , , , , , Suppuration, Complete resolution, Abscess formation, Progression to chronic inflammation, Healing by fibrosis, , Granulomatous inflammation, A granuloma consists of a microscopic aggregation of macrophages (with epithelial type, arrangement =epitheliod). Large giant cells may be found at the periphery of granulomas., Mediators, Growth factors released by activated macrophages include agents such as interferon and fibroblast, growth factor (plus many more). Some of these such as interferons may have systemic features, resulting in systemic symptoms and signs, which may be present in individuals with long standing, chronic inflammation., The finding of granulomas is pathognomonic of chronic inflammation, as illustrated in this biopsy, from a patient with colonic Crohns disease, , Image sourced from Wikipedia
Page 617 :
Question 107 of 347, Which of the following diseases is not considered a risk factor for gastric cancer?, , Polya gastrectomy for antral ulcer, , Atrophic gastritis, , Intestinal metaplasia of columnar type at the gastric cardia, , Patient with polyp showing medium grade dysplasia, , Long term therapy with H2 blockers, , Although some acid lowering procedures increase the risk of gastric cancer the use of H 2 blockers, does not, at the present time, seem to increase the risk., Please rate this question:, , Discuss and give feedback, , Next question, , Gastric cancer, Overview, There are 700,000 new cases of gastric cancer worldwide each year. It is most common in Japan, and less common in western countries. It is more common in men and incidence rises with, increasing age. The exact cause of many sporadic cancer is not known, however, familial cases do, occur in HNPCC families. In addition, smoking and smoked or preserved foods increase the risk., Japanese migrants retain their increased risk (decreased in subsequent generations). The, distribution of the disease in western countries is changing towards a more proximal location, (perhaps due to rising obesity)., Pathology, There is some evidence of support a stepwise progression of the disease through intestinal, metaplasia progressing to atrophic gastritis and subsequent dysplasia, through to cancer. The, favoured staging system is TNM. The risk of lymph node involvement is related to size and depth of, invasion; early cancers confined to submucosa have a 20% incidence of lymph node metastasis., Tumours of the gastro-oesophageal junction are classified as below:
Page 618 :
Type, 1, , True oesophageal cancers and may be associated with Barrett's oesophagus., , Type, 2, , Carcinoma of the cardia, arising from cardiac type epithelium, or short segments with intestinal metaplasia at the oesophagogastric junction., , Type, 3, , Sub cardial cancers that spread across the junction. Involve similar nodal stations to, gastric cancer., , Groups for close endoscopic monitoring, , , , , , Intestinal metaplasia of columnar type, Atrophic gastritis, Low to medium grade dysplasia, Patients who have previously undergone resections for benign peptic ulcer disease (except, highly selective vagotomy)., , Referral to endoscopy, , Patients of any age with, dyspepsia and any of the, following, , Patients without, dyspepsia, , Worsening dyspepsia, , Chronic gastrointestinal bleeding, , Dysphagia, , Barretts oesophagus, , Dysphagia, , Unexplained abdominal, pain or weight loss, , Intestinal metaplasia, , Weight loss, , Vomiting, , Dysplasia, , Iron deficiency anaemia, , Upper abdominal mass, , Atrophic gastritis, , Upper abdominal mass, , Jaundice, , Patient aged over 55 years with, unexplained or persistent, dyspepsia
Page 619 :
Upper GI endoscopy performed for dyspepsia. The addition of dye spraying (as shown in the bottom, right) may facilitate identification of smaller tumours, , Image sourced from Wikipedia, , Staging, , , , , CT scanning of the chest abdomen and pelvis is the routine first line staging investigation in, most centres., Laparoscopy to identify occult peritoneal disease, PET CT (particularly for junctional tumours), , Treatment, , , , , , , Proximally sited disease greater than 5-10cm from the OG junction may be treated by sub, total gastrectomy, Total gastrectomy if tumour is <5cm from OG junction, For type 2 junctional tumours (extending into oesophagus) oesophagogastrectomy is usual, Endoscopic sub mucosal resection may play a role in early gastric cancer confined to the, mucosa and perhaps the sub mucosa (this is debated), Lymphadenectomy should be performed. A D2 lymphadenectomy is widely advocated by the, Japanese, the survival advantages of extended lymphadenectomy have been debated., However, the overall recommendation is that a D2 nodal dissection be undertaken.
Page 620 :
, , Most patients will receive chemotherapy either pre or post operatively., , Prognosis, UK Data, , Disease extent, , Percentage 5 year survival, , All RO resections, , 54%, , Early gastric cancer, , 91%, , Stage 1, , 87%, , Stage 2, , 65%, , Stage 3, , 18%, , Operative procedure, Total Gastrectomy , lymphadenectomy and Roux en Y anastomosis, General anaesthesia, Prophylactic intravenous antibiotics, Incision: Rooftop., Perform a thorough laparotomy to identify any occult disease., Mobilise the left lobe of the liver off the diaphragm and place a large pack over it. Insert a large self, retaining retractor e.g. omnitract or Balfour (take time with this, the set up should be perfect). Pack, the small bowel away., Begin by mobilising the omentum off the transverse colon., Proceed to detach the short gastric vessels., Mobilise the pylorus and divide it at least 2cm distally using a linear cutter stapling device., Continue the dissection into the lesser sac taking the lesser omentum and left gastric artery flush at, its origin., The lymph nodes should be removed en bloc with the specimen where possible., Place 2 stay sutures either side of the distal oesophagus. Ask the anaesthetist to pull back on the, nasogastric tube. Divide the distal oesophagus and remove the stomach., The oesphago jejunal anastomosis should be constructed. Identify the DJ flexure and bring a loop of, jejunum up to the oesophagus (to check it will reach). Divide the jejunum at this point. Bring the, divided jejunum either retrocolic or antecolic to the oesophagus. Anastamose the oesophagus to the, jejunum, using either interrupted 3/0 vicryl or a stapling device. Then create the remainder of the
Page 621 :
Roux en Y reconstruction distally., Place a jejunostomy feeding tube., Wash out the abdomen and insert drains (usually the anastomosis and duodenal stump). Help the, anaesthetist insert the nasogastric tube (carefully!), Close the abdomen and skin., Enteral feeding may commence on the first post-operative day. However, most surgeons will leave, patients on free NG drainage for several days and keep them nil by mouth., Next question
Page 622 :
Question 108 of 347, A 56 year old man is diagnosed as having a glioma. From which of the following cell types do these, tumours usually originate?, , Astrocytes, , Oligodendrocytes, , Ependymal cells, , Squamous cells, , Neuroglial cells, , Theme from January 2012 Exam, Gliomas originate from glial (otherwise known as neuroglial) cells. These serve a structural function, in the CNS. The tumours produced may resemble a number of CNS cell types. Tumours are, therefore named according to the cells they resemble rather than the origin. Where this is not, possible they are termed gliomas., Please rate this question:, , Discuss and give feedback, , Next question, , Glioma, Glioma is a tumour that is typically found in the CNS. These tumours arise from glial cells. They are, sub categorised according to the cell type they most closely resemble., Glioma sub types, , , , , , Ependymomas- Ependymal cells, Astocytomas- Astrocytes (including glioblastoma), Oligodendrogliomas- Oligodendrocytes, Mixed- e.g. oligoastrocytomas, , Gliomas are categorised as being either high or low grade lesions (the former has the worse, prognosis). They may be either supra or infra tentorial. Their symptoms will typically reflect their site
Page 623 :
of origin. Glioblastoma multiforme has the worst prognosis and few patients will survive beyond 12, months., Next question
Page 624 :
Question 109 of 347, A 78 year old man presents with unilateral deafness which has been present for the past 3 months., On examination, Webers test localises to the contralateral side and a CT scan of his head shows a, thickened calvarium with areas of sclerosis and radiolucency. His blood tests show an elevated, alkaline phosphatase, normal serum calcium and normal PTH levels. Which of the following is the, most likely underlying diagnosis?, , Multiple myeloma with skull involvement, , Osteoporosis, , Pagets disease with skull involvement, , Lung cancer with skull metastasis, , Osteopetrosis with skull involvement, , Of the conditions listed Pagets disease is the most likely diagnosis (skull vault expansion and, sensorineural hearing loss). Multiple myeloma would typically result in multiple areas of radiolucency, and usually raised calcium in this setting. Osteopetrosis is a recognised cause of the features, described. However, it is a rare inherited disorder and usually presents in children in young adults., Presentation at this stage with no prior symptoms would be extremely rare and therefore this is not, themost likely diagnosis., Please rate this question:, , Discuss and give feedback, , Next question, , Pagets disease, Paget's disease is a disease of increased but uncontrolled bone turnover and is characterised by, architecturally abnormal bones. It is thought to be primarily a disorder of osteoclasts, with excessive, osteoclastic resorption followed by increased osteoblastic activity causing areas of sclerosis and, deformity. Paget's disease is common (UK prevalence 5%) but symptomatic in only 1 in 20 patients, Predisposing factors, , , , increasing age, male sex
Page 625 :
, , , northern latitude, family history, , Clinical features, , , , , , bone pain (e.g. pelvis, lumbar spine, femur), classical, untreated features: bowing of tibia, bossing of skull, raised alkaline phosphatase (ALP) - calcium* and phosphate are typically normal, skull x-ray: thickened vault, osteoporosis circumscripta, , Indications for treatment include bone pain, skull or long bone deformity, fracture, periarticular, Paget's, , , , bisphosphonate (either oral risedronate or IV zoledronate), calcitonin is less commonly used now, , Complications, , , , , , , deafness (cranial nerve entrapment), bone sarcoma (1% if affected for > 10 years), fractures, skull thickening, high-output cardiac failure, , *usually normal in this condition but hypercalcaemia may occur with prolonged immobilisation, Next question
Page 626 :
Question 110-112 of 347, Theme: Genetic causes of cancer, , A., B., C., D., E., F., , Multiple endocrine neoplasia type I, Multiple endocrine neoplasia type II, Gardner's syndrome, Lynch Syndrome, Kartagener's syndrome, Von Recklinghausen's disease, , Please select the most likely condition for the disease process described. Each option may be used, once, more than once or not at all, , 110., , A 5 year old boy presents with recurrent episodes of sinusitis. The casualty staff are, surprised to find his liver lying in the left upper quadrant of the abdomen., You answered Multiple endocrine neoplasia type I, The correct answer is Kartagener's syndrome, This is a case of Kartagener's syndrome. The primary problem is of immotile cilia, syndrome. When associated with situs inversus Kartagener's syndrome is diagnosed., , 111., , A 22 year old man presents with carcinoma of the caecum. His brother died from, colorectal cancer aged 25 and his mother died from endometrial cancer aged 38., You answered Multiple endocrine neoplasia type I, The correct answer is Lynch Syndrome, This is a case of Lynch syndrome HNPCC. It is transmitted in an autosomal dominant, fashion. Cancer of the uterine body is more common in HNPCC than Gardners syndrome, , 112., , A tall 32 year old lady presents with a diffuse neck swelling a carcinoma of the thyroid, medullary type is diagnosed., You answered Multiple endocrine neoplasia type I, The correct answer is Multiple endocrine neoplasia type II, This is a case MEN type IIb. It is associated with phaeochromocytomas and is, transmitted in an autosomal dominant pattern if inherited. All MEN II tend to have
Page 627 :
medullary carcinoma of the thyroid as a presenting feature, Please rate this question:, , Discuss and give feedback, , Next question, , Genetics and surgical disease, Some of the more commonly occurring genetic conditions occurring in surgical patients are, presented here., Li-Fraumeni Syndrome, , , , , , Autosomal dominant, Consists of germline mutations to p53 tumour suppressor gene, High incidence of malignancies particularly sarcomas and leukaemias, Diagnosed when:, , *Individual develops sarcoma under 45 years, *First degree relative diagnosed with any cancer below age 45 years and another family member, develops malignancy under 45 years or sarcoma at any age, BRCA 1 and 2, , , , , Carried on chromosome 17 (BRCA 1) and Chromosome 13 (BRCA 2), Linked to developing breast cancer (60%) risk., Associated risk of developing ovarian cancer (55% with BRCA 1 and 25% with BRCA 2)., , Lynch Syndrome, , , , , , Autosomal dominant, Develop colonic cancer and endometrial cancer at young age, 80% of affected individuals will get colonic and/ or endometrial cancer, High risk individuals may be identified using the Amsterdam criteria, , Amsterdam criteria, Three or more family members with a confirmed diagnosis of colorectal cancer, one of whom is a, first degree (parent, child, sibling) relative of the other two., Two successive affected generations., One or more colon cancers diagnosed under age 50 years., Familial adenomatous polyposis (FAP) has been excluded.
Page 629 :
Question 113 of 347, A 45 year old man presents with symptoms of urinary colic. In the history he has suffered from, recurrent episodes of frank haematuria over the past week or so. On examination he has a left loin, mass and a varicocele. The most likely diagnosis is:, , Renal adenocarcinoma, , Renal cortical adenoma, , Squamous cell carcinoma of the renal pelvis, , Retroperitoneal fibrosis, , Nephroblastoma, , , , , , , Renal adenocarcinoma are the most common renal malignancy and account for 75% cases., Patients may develop frank haematuria and have episodes of clot colic., A Grawitz tumour is an eponymous name for Renal Adenocarcinoma., May metastasise to bone., , Please rate this question:, , Discuss and give feedback, , Next question, , Renal tumours, Renal cell carcinoma, Renal cell carcinoma is an adenocarcinoma of the renal cortex and is believed to arise from the, proximal convoluted tubule. They are usually solid lesions, up to 20% may be multifocal, 20% may, be calcified and 20% may have either a cystic component or be wholly cystic. They are often, circumscribed by a pseudocapsule of compressed normal renal tissue. Spread may occur either by, direct extension into the adrenal gland, renal vein or surrounding fascia. More distant disease, usually occurs via the haematogenous route to lung, bone or brain., Renal cell carcinoma comprise up to 85% of all renal malignancies. Males are more commonly, affected than females and sporadic tumours typically affect patients in their sixth decade., Patients may present with a variety of symptoms including; haematuria (50%), loin pain (40%), mass, (30%) and up to 25% may have symptoms of metastasis.Less than 10% have the classic triad of
Page 630 :
haematuria, pain and mass., Investigation, Many cases will present as haematuria and be discovered during diagnostic work up. Benign renal, tumours are rare, so renal masses should be investigated with multislice CT scanning. Some units, will add and arterial and venous phase to the scan to demonstrate vascularity and evidence of caval, ingrowth., CT scanning of the chest and abdomen to detect distant disease should also be undertaken., Routine bone scanning is not indicated in the absence of symptoms., Biopsy should not be performed when a nephrectomy is planned but is mandatory before any, ablative therapies are undertaken., Assessment of the functioning of the contra lateral kidney., Management, T1 lesions may be managed by partial nephrectomy and this gives equivalent oncological results to, total radical nephrectomy. Partial nephrectomy may also be performed when there is inadequate, reserve in the remaining kidney., For T2 lesions and above a radical nephrectomy is standard practice and this may be performed via, a laparoscopic or open approach. Preoperative embolisation is not indicated nor is resection of, uninvolved adrenal glands. During surgery early venous control is mandatory to avoid shedding of, tumour cells into the circulation., Patients with completely resected disease do not benefit from adjuvant therapy with either, chemotherapy or biological agents. These should not be administered outside the setting of clinical, trials., Patients with transitional cell cancer will require a nephroureterectomy with disconnection of the, ureter at the bladder., References, Lungberg B et al. EAU guidelines on renal cell carcinoma: The 2010 update. European Urology 2010, (58): 398-406., Next question
Page 631 :
Question 114 of 347, , A 63 year old man finds that he has to stop walking after 100 yards due to bilateral calf pain. He, finds that bending forwards and walking up hill helps. He is able to ride a bike without any pain. What, is the most likely underlying cause?, , Lumbar canal stenosis, , Diabetic neuropathy, , Aorto-iliac occlusion, , Occlusion of the superficial femoral artery, , Pelvic rheumatoid arthritis, , Theme from April 2012 Exam, Theme from April 2013 Exam, The positional nature of the pain and the fact that improves with walking uphill makes an underlying, vascular aetiology far less likely., Please rate this question:, , Discuss and give feedback, , Next question, , Lumbar spinal stenosis, Lumbar spinal stenosis is a condition in which the central canal is narrowed by tumour, disk prolapse, or other similar degenerative changes., Patients may present with a combination of back pain, neuropathic pain and symptoms mimicking, claudication. One of the main features that may help to differentiate it from true claudication in the, history is the positional element to the pain. Sitting is better than standing and patients may find it
Page 632 :
easier to walk uphill rather than downhill. The neurogenic claudication type history makes lumbar, spinal stenosis a likely underlying diagnosis, the absence of such symptoms makes it far less likely., Pathology, Degenerative disease is the commonest underlying cause. Degeneration is believed to begin in the, intervertebral disk where biochemical changes such as cell death and loss of proteoglycan and, water content lead to progressive disk bulging and collapse. This process leads to an increased, stress transfer to the posterior facet joints, which accelerates cartilaginous degeneration,, hypertrophy, and osteophyte formation; this is associated with thickening and distortion of the, ligamentum flavum. The combination of the ventral disk bulging, osteophyte formation at the dorsal, facet, and ligamentum flavum hyptertrophy combine to circumferentially narrow the spinal canal and, the space available for the neural elements. The compression of the nerve roots of the cauda equina, leads to the characteristic clinical signs and symptoms of lumbar spinal stenosis., Diagnosis, MRI scanning is the best modality for demonstrating the canal narrowing. Historically a bicycle test, was used as true vascular claudicants could not complete the test., Treatment, Laminectomy, Next question
Page 633 :
Question 115 of 347, , A 73 year old lady is admitted for a laparoscopic cholecystectomy. During her pre-operative, assessment it is noted that she is receiving furosemide for the treatment of hypertension., Approximately what proportion of the sodium that is filtered at the glomerulus will be subsequently, excreted?, , Up to 25%, , Upt to 75%, , Between 3 and 5%, , <2%, , Between 1 and 2%, , Theme from 2010 Exam, The loop diuretics can lead to marked increases in the amount of sodium excreted. They act in the, medullary and cortical aspects of the thick ascending limb of the loop of Henle. This results in a, decreased medullary osmolal gradient and increases free water excretion (as well as loss of, sodium). Because loop diuretics result in the loss of both sodium and water they are less frequently, associated with hyponatraemia than thiazide diuretics (these latter agents act in the cortex and do, not affect urine concentrating ability)., Please rate this question:, , Discuss and give feedback, , Next question, , Diuretic agents
Page 634 :
The diuretic drugs are divided into three major classes, which are distinguished according to the site, at which they impair sodium reabsorption: loop diuretics in the thick ascending loop of Henle,, thiazide type diuretics in the distal tubule and connecting segment; and potassium sparing diuretics, in the aldosterone - sensitive principal cells in the cortical collecting tubule., In the kidney, sodium is reabsorbed through Na+/ K+ ATPase pumps located on the basolateral, membrane. These pumps return reabsorbed sodium to the circulation and maintain low intracellular, sodium levels. This latter effect ensures a constant concentration gradient., Physiological effects of commonly used diuretics, , Site of action, , Diuretic, , Carrier or channel, inhibited, , Percentage of filtered sodium, excreted, , Ascending limb of loop of, Henle, , Frusemide, , Na+/K+ 2Cl - carrier, , Up to 25%, , Distal tubule and connecting, segment, , Thiazides, , Na+Cl- carrier, , Between 3 and 5%, , Cortical collecting tubule, , Spironolactone, , Na+/K+ ATP ase pump, , Between 1 and 2%, Next question
Page 635 :
Question 116 of 347, A 59 year old man presents with recurrent episodes of urinary sepsis. In his history he mentions that, he has suffered from recurrent attacks of left iliac fossa pain over the past few months. He has also, notices bubbles in his urine. He undergoes a CT scan which shows a large inflammatory mass in the, left iliac fossa. No other abnormality is detected. The most likely diagnosis is:, , Ulcerative colitis, , Crohns disease, , Mesenteric ischaemia, , Diverticular disease, , Rectal cancer, Diverticular disease is one of the commonest causes of colovesical fistula, Theme from April 2016 Exam, Recurrent attacks of diverticulitis may cause the development of local abscesses which may erode, into the bladder resulting in urinary sepsis and pneumaturia. This would be an unusual presentation, from Crohns disease and rectal cancer would be more distally sited and generally evidence of extra, colonic disease would be present if the case were malignant and this advanced., Please rate this question:, , Discuss and give feedback, , Next question, , Diverticular disease, Diverticular disease is a common surgical problem. It consists of herniation of colonic mucosa, through the muscular wall of the colon. The usual site is between the taenia coli where vessels, pierce the muscle to supply the mucosa. For this reason, the rectum, which lacks taenia, is often, spared., Symptoms, , , Altered bowel habit
Page 636 :
, , , Bleeding, Abdominal pain, , Complications, , , , , , , , Diverticulitis, Haemorrhage, Development of fistula, Perforation and faecal peritonitis, Perforation and development of abscess, Development of diverticular phlegmon, , Diagnosis, Patients presenting in clinic will typically undergo either a colonoscopy, CT cologram or barium, enema as part of their diagnostic work up. All tests can identify diverticular disease. It can be far, more difficult to confidently exclude cancer, particularly in diverticular strictures., Acutely unwell surgical patients should be investigated in a systematic way. Plain abdominal films, and an erect chest x-ray will identify perforation. An abdominal CT scan (not a CT cologram) with, oral and intravenous contrast will help to identify whether acute inflammation is present but also the, presence of local complications such as abscess formation., , Severity Classification- Hinchey, , I, , Para-colonic abscess, , II, , Pelvic abscess, , III, , Purulent peritonitis, , IV, , Faecal peritonitis, , Treatment, , , , , , Increase dietary fibre intake., Mild attacks of diverticulitis may be managed conservatively with antibiotics., Peri colonic abscesses should be drained either surgically or radiologically., Recurrent episodes of acute diverticulitis requiring hospitalisation are a relative indication for, a segmental resection.
Page 637 :
, , Hinchey IV perforations (generalised faecal peritonitis) will require a resection and usually a, stoma. This group have a very high risk of post operative complications and usually require, HDU admission. Less severe perforations may be managed by laparoscopic washout and, drain insertion., Next question
Page 638 :
Question 117 of 347, , Which of the following is least likely to occur in association with severe atrophic gastritis?, , Gastric ulcers, , Gastric cancer, , Anaemia, , Duodenal ulcers, , Gastric polyps, Achlorhydria would make the formation of duodenal ulcers unlikely. Note the question states "least, likely"., , Due to the loss of gastric acid a duodenal ulcer is unlikely. Note that gastric polyps may form (see, below)., Please rate this question:, , Discuss and give feedback, , Next question, , Gastritis, Type of gastritis, , Features, , Type A, , Autoimmune
Page 639 :
Type of gastritis, , Features, , Circulating antibodies to parietal cells, causes reduction in cell mass and, hypochlorhydria, Loss of parietal cells = loss of intrinsic factor = B12 malabsorption, Absence of antral involvement, Hypochlorhydria causes elevated gastrin levels- stimulating enterochromaffin cells and, adenomas may form, , Type B, , Antral gastritis, Associated with infection with helicobacter pylori infection, Intestinal metaplasia may occur in stomach and require surveillance endoscopy, Peptic ulceration may occur, , Reflux gastritis, , Bile refluxes into stomach, either post surgical or due to failure of pyloric function, Histologically, evidence of chronic inflammation, and foveolar hyperplasia, May respond to therapy with prokinetics, , Erosive gastritis, , Agents disrupt the gastric mucosal barrier, Most commonly due to NSAIDs and alcohol, With NSAIDs the effects occur secondary to COX 1 inhibition, , Stress ulceration, , This occurs as a result of mucosal ischaemia during hypotension or hypovolaemia, The stomach is the most sensitive organ in the GI tract to ischaemia following, hypovolaemia, Diffuse ulceration may occur, Prophylaxis with acid lowering therapy and sucralfate may minimise complications, , Menetriers, disease, , Gross hypertrophy of the gastric mucosal folds, excessive mucous production and, hypochlorhydria, Pre malignant condition, , References, Whiting J et al. The long term results of endoscopic surveillance of premalignant gastric, lesions. Gut2002; 50 :378381.
Page 641 :
Question 118-120 of 347, Theme: Lung cancer, , A., B., C., D., , Adenocarcinoma, Small cell lung cancer, Large cell lung cancer, Squamous cell carcinoma, , Please select the most likely lung cancer variant for the scenario described. Each option may be, used once, more than once or not at all., , 118., , A 73 year old heavy smoker presents with haemoptysis. On examination he is cachectic, and shows evidence of clubbing. Imaging shows a main bronchial tumour with massive, mediastinal lymphadenopathy together with widespread visceral metastases., You answered Adenocarcinoma, The correct answer is Small cell lung cancer, Theme from April 2012, Small cell carcinoma is associated with disseminated disease at presentation in the, majority of cases. Most cases occur in the main airways and paraneoplastic features are, common., , 119., , A 68 year old female who has never smoked presents with a mass at the periphery of her, right lung., Adenocarcinoma, Adenocarcinomas are the most common tumour type present in never smokers. They are, usually located at the periphery., , 120., , An 85 year old man presents with a cough and haemoptysis. He has a modest smoking, history of 15 pack years. He is found to have a tumour located in the right main bronchus,, with no evidence of metastatic disease. He decides not undergo any treatment and he, remains well for a further 12 months before developing symptomatic metastasis., You answered Adenocarcinoma, The correct answer is Squamous cell carcinoma, Squamous cell carcinomas are reported to be more slow growing and are typically
Page 642 :
centrally located. Small cell carcinomas are usually centrally located. However, small cell, carcinomas would seldom be associated with a survival of a year without treatment., Please rate this question:, , Discuss and give feedback, , Next question, , Lung cancer, Lung cancers may be classified according to histological subtypes. The main distinction is between, small cell and non small cell lung cancer. Non small cell lung cancer is the most common variant and, accounts for 80% of all lung cancers., Non small cell lung cancer, These share common features of prognosis and management. They comprise the following, tumours:, , , , , Squamous cell carcinoma (25% cases), Adenocarcinoma (40% cases), Large cell carcinoma (10% cases), , Paraneoplastic features and early disease dissemination are less likely than with small cell lung, carcinoma. Adenocarcinoma is the most common lung cancer type encountered in never smokers., Small cell lung carcinoma, Small cell lung carcinomas are comprised of cells with a neuro endocrine differentiation. The, neuroendocrine hormones may be released from these cells with a wide range of paraneoplastic, associations. These tumours are strongly associated with smoking and will typically arise in the, larger airways. They disseminate early in the course of the disease and although they are usually, chemosensitive this seldom results in long lasting remissions., Next question
Page 643 :
Question 121 of 347, , Which of the following is not found on a blood film post splenectomy?, , Pappenheimer bodies, , Stipple cells, , Erythrocyte containing siderotic granules, , Howell-Jolly bodies, , Target cells, , Stipple cells are found in lead poisoning/haemoglobinopathies., Blood film in hyposplenism:, Howell-Jolly bodies, Pappenheimer bodies, Poikilocytes (Target cells), Erythrocyte containing siderotic granules, Heinz bodies, Please rate this question:, , Discuss and give feedback, , Next question, , Post splenectomy blood film changes, The loss of splenic tissue results in the inability to readily remove immature or abnormal red blood, cells from the circulation. The red cell count does not alter significantly. However, cytoplasmic
Page 644 :
inclusions may be seen e.g. Howell-Jolly bodies., In the first few days after splenectomy target cells, siderocytes and reticulocytes will appear in the, circulation. Immediately following splenectomy a granulocytosis (mainly composed of neutrophils) is, seen, this is replaced by a lymphocytosis and monocytosis over the following weeks., The platelet count is usually increased and this may be persistent, oral antiplatelet agents may be, needed in some patients., Image showing Howell Jolly bodies (arrowed), , Image sourced from Wikipedia, , Next question
Page 645 :
Question 122 of 347, A 45 year old man with long standing ulcerative colitis and rectal dysplasia presents with a DALM, lesion in the rectum. What is the most appropriate management option?, , Snare polypectomy, , Repeat endoscopy in 2 years, , Discharge, , Anterior resection, , Panproctocolectomy, , DALM lesions complicating ulcerative colitis should be managed with panproctocolectomy. An, anterior resection is inadequate since it will only remove the rectum and ulcerative colitis affects the, entire colon. Since many will be associated with invasion a snare polypectomy is not sufficient either., Please rate this question:, , Discuss and give feedback, , Next question, , Colonic lesions - DALM, , , , , , The term DALM lesion refers to a Dysplasia Associated Lesion or Mass., They may complicate dysplasia occurring in patients with longstanding ulcerative colitis., They have a high incidence of invasive foci., When they complicate longstanding ulcerative colitis, they should be treated by, panproctocolectomy., Next question
Page 646 :
Question 123 of 347, , Which of the metastatic bone tumours described below is at the greatest risk of pathological fracture, ?, , Proximal humeral lesion from a prostate cancer, , Vertebral body lesions from a prostate cancer, , Peritrochanteric lesion from a carcinoma of the breast, , Proximal humeral lesion from a carcinoma of the breast, , Peritrochanteric lesion from a prostate cancer, , Peritrochanteric lesions have the greatest risks of fracture (due to loading). The lesions from breast, cancer are usually lytic and therefore at higher risk rather than the sclerotic lesions from prostate, cancer., Please rate this question:, , Discuss and give feedback, , Next question, , Metastatic bone disease- risk of fracture, Metastatic bone tumours may be described as blastic, lytic or mixed. Osteoblastic metastatic, disease has the lowest risk of spontaneous fracture when compared to osteolytic lesions of a similar, size., Lesions affecting the peritrochanteric region are most prone to spontaneous fracture (because of, loading forces at that site)., The factors are incorporated into the Mirel Scoring system to stratify the risk of spontaneous fracture, for bone metastasis of varying types.
Page 647 :
Mirel Scoring system, , Score, points, , Site, , Radiographic, appearance, , Width of bone, involved, , Pain, , 1, , Upper, extremity, , Blastic, , Less than 1/3, , Mild, , 2, , Lower extremity, , Mixed, , 1/3 to 2/3, , Moderate, , 3, , Peritrochanteric, , Lytic, , More than 2/3, , Aggravated by, function, , Depending upon the score the treatment should be as follows:, , Score, , Risk of fracture, , Treatment, , 9 or greater, , Impending (33%), , Prophylactic fixation, , 8, , Borderline, , Consider fixation, , 7 or less, , Not impending (4%), , Non operative management, Next question
Page 648 :
Question 124 of 347, A 63 year old male presents with several episodes of haematuria. He suffers from COPD secondary, to long term smoking. What is the most likely underlying cause?, , Renal cortical adenoma, , Renal adenocarcinoma, , Nephroblastoma, , Transitional cell carcinoma of the bladder, , Adenocarcinoma of the bladder, , Theme from 2009 Exam, TCC is the most common subtype and is strongly linked to smoking. The important point to note in, this question is the term most likely as renal adenocarcinoma may produce similar symptoms but is, less likely., Please rate this question:, , Discuss and give feedback, , Next question, , Bladder cancer, Bladder cancer is the second most common urological cancer. It most commonly affects males aged, between 50 and 80 years of age. Those who are current, or previous (within 20 years), smokers, have a 2-5 fold increased risk of the disease. Exposure to hydrocarbons such as 2-Naphthylamine, increases the risk. Although rare in the UK, chronic bladder inflammation arising from, Schistosomiasis infection remains a common cause of squamous cell carcinomas, in those countries, where the disease is endemic., Benign tumours, Benign tumours of the bladder including inverted urothelial papilloma and nephrogenic adenoma are, uncommon., Bladder malignancies, , , Transitional cell carcinoma (>90% of cases)
Page 649 :
, , , Squamous cell carcinoma ( 1-7% -except in regions affected by schistosomiasis), Adenocarcinoma (2%), , Transitional cell carcinomas may arise as solitary lesions, or may be multifocal, owing to the effect of, "field change" within the urothelium. Up to 70% of TCC's will have a papillary growth pattern. These, tumours are usually superficial in location and accordingly have a better prognosis. The remaining, tumours show either mixed papillary and solid growth or pure solid growths. These tumours are, typically more prone to local invasion and may be of higher grade, the prognosis is therefore worse., Those with T3 disease or worse have a 30% (or higher) risk of regional or distant lymph node, metastasis., TNM Staging, , Stage, , Description, , T0, , No evidence of tumour, , Ta, , Non invasive papillary carcinoma, , T1, , Tumour invades sub epithelial connective tissue, , T2a, , Tumor invades superficial muscularis propria (inner half), , T2b, , Tumor invades deep muscularis propria (outer half), , T3, , Tumour extends to perivesical fat, , T4, , Tumor invades any of the following: prostatic stroma, seminal vesicles, uterus, vagina, , T4a, , Invasion of uterus, prostate or bowel, , T4b, , Invasion of pelvic sidewall or abdominal wall, , N0, , No nodal disease
Page 650 :
Stage, , Description, , N1, , Single regional lymph node metastasis in the true pelvis (hypogastric, obturator, external, iliac, or presacral lymph node), , N2, , Multiple regional lymph node metastasis in the true pelvis (hypogastric, obturator, external, iliac, or presacral lymph node metastasis), , N3, , Lymph node metastasis to the common iliac lymph nodes, , M0, , No distant metastasis, , M1, , Distant disease, , Presentation, Most patients (85%) will present with painless, macroscopic haematuria. In those patients with, incidental microscopic haematuria, up to 10% of females aged over 50 will be found to have a, malignancy (once infection excluded)., Staging, Most will undergo a cystoscopy and biopsies or TURBT, this provides histological diagnosis and, information relating to depth of invasion. Locoregional spread is best determined using pelvic MRI, and distant disease CT scanning. Nodes of uncertain significance may be investigated using PET, CT., Treatment, Those with superficial lesions may be managed using TURBT in isolation. Those with recurrences or, higher grade/ risk on histology may be offered intravesical chemotherapy. Those with T2 disease are, usually offered either surgery (radical cystectomy and ileal conduit) or radical radiotherapy., Prognosis, , T1, , 90%, , T2, , 60%, , T3, , 35%
Page 652 :
Question 125-127 of 347, , Theme: Neck lumps, , A. Cystic hygroma, B. Bartonella infection, C. Mycobacterium tuberculosis infection, D. Branchial cyst, E. Thyroglossal cyst, F. Pharyngeal pouch, G. Follicular thyroid cyst, H. Parathyroid adenoma, I. None of the above, , Please select the most likely underlying disease process for the scenario given. Each option may be, used once, more than once or not at all., , 125., , A 25 year old cat lover presents with symptoms of abdominal pain, lethargy and sweats. These, have been present for the past two weeks. On examination she has lymphadenopathy in the, posterior triangle., You answered Cystic hygroma, The correct answer is Bartonella infection, Theme from January 2015 Exam, Bartonella infection may occur following a cat scratch. The organism is intracellular. Generalised, systemic symptoms may occur for a week or so prior to clinical presentation., , 126., , A 25 year old lady presents with an swelling located at the anterior border of the, sternocleidomastoid muscle. The swelling is intermittent and on examination it is soft and
Page 653 :
fluctuant., You answered Cystic hygroma, The correct answer is Branchial cyst, Branchial cysts are remnants of the branchial cleft. They may become infected., , 127., , A 38 year old lady presents with a mass in the midline of the neck immediately below the hyoid, bone. It moves upwards on tongue protrusion., You answered Cystic hygroma, The correct answer is Thyroglossal cyst, Thyroglossal cysts are usually located in the midline and are linked to the foramen caecum and, will thus move upwards on tongue protrusion., , Please rate this question:, , Discuss and give feedback, , Next question, , Neck lumps, The table below gives characteristic exam question features for conditions causing neck lumps:, , Reactive, lymphadenopathy, , By far the most common cause of neck swellings. There may be a history of, local infection or a generalised viral illness, , Lymphoma, , Rubbery, painless lymphadenopathy, The phenomenon of pain whilst drinking alcohol is very uncommon
Page 654 :
There may be associated night sweats and splenomegaly, , Thyroid swelling, , May be hypo-, eu- or hyperthyroid symptomatically, Moves upwards on swallowing, , Thyroglossal cyst, , More common in patients < 20 years old, Usually midline, between the isthmus of the thyroid and the hyoid bone, Moves upwards with protrusion of the tongue, May be painful if infected, , Pharyngeal pouch, , More common in older men, Represents a posteromedial herniation between thyropharyngeus and, cricopharyngeus muscles, Usually not seen, but if large then a midline lump in the neck that gurgles on, palpation, Typical symptoms are dysphagia, regurgitation, aspiration and chronic cough, , Cystic hygroma, , A congenital lymphatic lesion (lymphangioma) typically found in the neck,, classically on the left side, Most are evident at birth, around 90% present before 2 years of age, , Branchial cyst, , An oval, mobile cystic mass that develops between the sternocleidomastoid, muscle and the pharynx, Develop due to failure of obliteration of the second branchial cleft in, embryonic development, Usually present in early adulthood, , Cervical rib, , More common in adult females, Around 10% develop thoracic outlet syndrome, , Carotid aneurysm, , Pulsatile lateral neck mass which doesn't move on swallowing, Next question
Page 655 :
Question 128 of 347, A 22 year old man presents with a discharging area on his lower back. On examination there is an, epithelial defect located 6cm proximal to the tip of his coccyx and located in the midline. There are, two further defects located about 2cm superiorly in the same position. He is extremely hirsute. What, is the most likely diagnosis?, , Pre sacral tumour, , Sacrococcygeal teratoma, , Pilonidal sinus, , Fistula in ano, , Occult spina bifida, , Pilonidal sinuses are extremely common in hirsute individuals and typically present as midline, sinuses in the natal cleft., Please rate this question:, , Discuss and give feedback, , Next question, , Pilonidal sinus, , , , , , , , , , Occur as a result of hair debris creating sinuses in the skin (Bascom theory)., Usually in the natal cleft of male patients after puberty., It is more common in Caucasians related to their hair type and growth patterns., The opening of the sinus is lined by squamous epithelium, but most of its wall consists of, granulation tissue. Up to 50 cases of squamous cell carcinoma have been described in, patients with chronic pilonidal sinus disease., Hairs become trapped within the sinus., Clinically the sinus presents when acute inflammation occurs, leading to an abscess., Patients may describe cycles of being asymptomatic and periods of pain and discharge from, the sinus., Treatment is difficult and opinions differ. Definitive treatment should never be undertaken, when acute infection or abscess is present as this will result in failure., Definitive treatments include the Bascom procedure with excision of the pits and obliteration, of the underlying cavity. The Karydakis procedure involves wide excision of the natal cleft
Page 656 :
such that the surface is recontoured once the wound is closed. This avoids the shearing, forces that break off the hairs and has reasonable results., , Pilonidal sinuses are most commonly located in the midline of the natal cleft, as illustrated below, , Image sourced from Wikipedia, , Next question
Page 657 :
Question 129 of 347, A 43 year old man from Greece presents with colicky right upper quadrant pain, jaundice and an, urticarial rash. He is initially treated with ciprofloxacin, but does not improve. What is the most likely, diagnosis?, , Infection with Wucheria bancrofti, , Infection with Echinococcus granulosus, , Type III hypersensitivity reaction, , Allergy to ciprofloxacin, , Common bile duct stones, , Infection with Echinococcus granulosus will typically produce a type I hypersensitivity reaction which, is characterised by an urticarial rash. With biliary rupture a classical triad of biliary colic, jaundice and, urticaria occurs. Whilst jaundice and biliary colic may be a feature of CBD stones they do not, produce an urticarial rash. Antibiotic sensitivity with ciprofloxacin may produce jaundice and a rash,, however it was not present at the outset and does not cause biliary colic., Please rate this question:, , Discuss and give feedback, , Next question, , Hydatid cysts, Hydatid cysts are endemic in Mediterranean and Middle Eastern countries. They are caused by the, tapeworm parasite Echinococcus granulosus. An outer fibrous capsule is formed containing multiple, small daughter cysts. These cysts are allergens which precipitate a type 1 hypersensitivity, reaction., Clinical features are as follows:, , , , , , Up to 90% cysts occur in the liver and lungs, Can be asymtomatic, or symptomatic if cysts > 5cm in diameter, Morbidity caused by cyst bursting, infection and organ dysfunction (biliary, bronchial, renal, and cerebrospinal fluid outflow obstruction), In biliary ruputure there may be the classical triad of; biliary colic, jaundice, and urticaria
Page 658 :
CT is the best investigation to differentiate hydatid cysts from amoebic and pyogenic cysts., Surgery is the mainstay of treatment (the cyst walls must not be ruptured during removal and the, contents sterilised first)., Next question
Page 659 :
Question 130 of 347, A 22 year old lady presents with an episode of renal colic and following investigation is suspected of, suffering from MEN IIa. Which of the following abnormalities of the parathyroid glands are most often, found in this condition?, , Hypertrophy, , Hyperplasia, , Adenoma, , Carcinoma, , Metaplasia, MEN IIa, , , , , Medullary thyroid cancer, Hyperparathyroidism (usually hyperplasia), Phaeochromocytoma, , In MEN IIa the commonest lesion is medullary thyroid cancer, with regards to the parathyroid glands, the most common lesion is hyperplasia. In MEN I a parathyroid adenoma is the most common, lesion., Please rate this question:, , Discuss and give feedback, , Next question, , Multiple Endocrine Neoplasia, Multiple endocrine neoplasia (MEN) is inherited as an autosomal dominant disorder., The table below summarises the three main types of MEN:, , MEN type I, , MEN type IIa, , MEN type IIb
Page 661 :
Question 131 of 347, , A male infant is born prematurely at 34 weeks gestation by emergency cesarean section. He initially, appears to be stable. However, over the ensuing 24 hours he develops worsening neurological, function. Which of the following processes is most likely to have occurred?, , Extra dural haemorrhage, , Sub dural haemorrhage, , Sub arachnoid haemorrhage, , Intraventricular haemorrhage, , Arteriovenous malformation, Premature neonates= Intra ventricular haemorrhage, Non accidental injury= Sub dural bleed, , Theme from April 2012 Exam, Please rate this question:, , Discuss and give feedback, , Next question, , Intraventricular haemorrhage, Intraventricular haemorrhage is a haemorrhage that occurs into the ventricular system of the brain. It, is relatively rare in adult surgical practice and when it does occur, it is typically associated with, severe head injuries. In premature neonates it may occur spontaneously. The blood may clot and, occlude CSF flow, hydrocephalus may result., In neonatal practice the vast majority of IVH occur in the first 72 hours after birth, the aetiology is not
Page 662 :
well understood and it is suggested to occur as a result of birth trauma combined with cellular, hypoxia, together the with the delicate neonatal CNS., Treatment, Is largely supportive, therapies such as intraventricular thrombolysis and prophylactic CSF drainage, have been trialled and not demonstrated to show benefit. Hydrocephalus and rising ICP is an, indication for shunting., Next question
Page 663 :
Question 132 of 347, A 22 year old man is admitted to hospital with a lower respiratory chest infection. He had a, splenectomy after being involved in a car accident. What is the most likely infective organism?, , Haemophilus influenzae, , Staphylococcus aureus, , Rhinovirus, , Mycobacterium tuberculosis, , Moraxella catarrhalis, Organisms causing post splenectomy sepsis:, Streptococcus pneumoniae, Haemophilus influenzae, Meningococci, Encapsulated organisms carry the greatest pathogenic risk following splenectomy. The effects of, sepsis following splenectomy are variable. This may be the result of small isolated fragments of, splenic tissue that retain some function following splenectomy. These may implant spontaneously, following splenic rupture (in trauma) or be surgically implanted at the time of splenectomy., Please rate this question:, , Discuss and give feedback, , Next question, , Post splenectomy sepsis, Hyposplenism may complicate certain medical conditions where splenic atrophy occurs or may be, the result of medical intervention such as splenic artery embolization and splenectomy for trauma., Diagnosis of hyposplenism is difficult and whilst there may be peripheral markers of the, splenectomised state (e.g. Howell Jolly bodies) these are neither 100% sensitive or specific. The, most sensitive test is a radionucleotide labeled red cell scan., Hyposplenism, by whatever mechanism it occurs dramatically increases the risk of post splenectomy, sepsis, particularly with encapsulated organisms. Since these organisms may be opsonised, but this, then goes undetected at an immunological level due to loss of the spleen. For this reason individuals, are recommended to be vaccinated and have antibiotic prophylaxis.
Page 664 :
Key recommendations, , , , , , , , All those with hyposplenism or may become so (such as prior to an elective splenectomy), should receive pneumococcal, haemophilus type b and meningococcal type C vaccines., These should be administered 2 weeks prior to splenectomy or two weeks following, splenectomy. The vaccine schedule for meningococcal disease essentially consists of a, dose of Men C and Hib at 2 weeks and then a dose of the MenACWY vaccine one month, later. Those aged under 2 may require a booster at 2 years. A dose of pneumococcal, polyvalent polysaccharide vaccine (PPV) is given at two weeks. A conjugated vaccine (PCV), is offered to young children. The PCV is more immunogenic but covers fewer serotypes., Boosting PPV is either guided by serological measurements (where available) or by routine, boosting doses at 5 yearly intervals., Annual influenza vaccination is recommended in all cases, Antibiotic prophylaxis is offered to all. The risk of post splenectomy sepsis is greatest, immediately following splenectomy and in those aged less than 16 years or greater than 50, years. Individuals with a poor response to pneumococcal vaccination are another high risk, group. High risk individuals should be counselled to take penicillin or macrolide prophylaxis., Those at low risk may choose to discontinue therapy. All patients should be advised about, taking antibiotics early in the case of intercurrent infections., Asplenic individuals traveling to malaria endemic areas are at high risk and should have both, pharmacological and mechanical protection., , Dosing, Penicillin V 500mg BD or amoxicillin 250mg BD, References, Davies J et al. Review of guidelines for the prevention and treatment of infection in patients with an, absent or dysfunctional spleen: Prepared on behalf of the British Committee for Standards in, Haematology by a Working Party of the Haemato-Oncology Task Force. British Journal of, Haematology2011 (155): 308317., Next question
Page 665 :
Question 133 of 347, A 24 year old man presents with symptoms of malaise, weight loss and lymphadenopathy. A lymph, node biopsy is performed and the subsequent histology report states that there is evidence of, granuloma formation and central necrosis. What is the most likely underlying cause?, , Non Hodgkins lymphoma, , Churg Strauss syndrome, , Epstein Barr Virus infection, , Rheumatoid nodule, , Infection with Mycobacterium tuberculosis, , These histological features are typically seen in TB. Necrosis occurring in granulomas is usually, indicative of an underlying infective cause. Churg Strauss syndrome is a form of vasculitis, which is, the usual histological finding. Granulomas are reported in the condition, but it is rare for them to, demonstrate necrosis., Please rate this question:, , Discuss and give feedback, , Next question, , Tuberculosis pathology, , , , , , , , Is a form of primary chronic inflammation, caused by the inability of macrophages to kill, theMycobacterium tuberculosis., The macrophages often migrate to regional lymph nodes, the lung lesion plus affected lymph, nodes is referred to as a Ghon complex., This leads to the formation of a granuloma which is a collection of epithelioid histiocytes., There is the presence of caseous necrosis in the centre., The inflammatory response is mediated by a type 4 hypersensitivity reaction., In healthy individuals the disease may be contained, in the immunocompromised, disseminated (miliary TB) may occur., , Diagnosis
Page 666 :
, , , Waxy membrane of mycobacteria prevents binding with normal stains. Ziehl - Neelsen, staining is typically used., Culture based methods take far longer., , Image showing acid- alcohol fast mycobacteria stained using the Ziehl- Neelsen method, , Image sourced from Wikipedia, , Next question
Page 667 :
Question 134 of 347, A 20 year old man develops acute appendicitis, his appendix is removed and he makes a full, recovery. Which of the following pathological processes is least likely to be present in the acutely, inflamed tissues?, , Altered Starlings forces., , Seqestration of neutrophils, , Formation of fluid exudate, , Formation of granulomas, , None of the above, Neutrophil polymorphs=Acute inflammation., Granuloma = Chronic inflammation., Acute inflammation:, 3 phases, 1. Changes in blood vessel and flow: flush, flare, wheal, 2. Fluid exudates (rich in protein i.e. Ig, coagulation factors) produced via increased vascular, permeability, 3. Cellular exudates mainly containing neutrophil polymorphs pass into extravascular space., Neutrophils are then transported to tissues via:, a. Margination of neutrophils to the peripheral plasmatic of the vessel rather than the central axial, stream, b. Pavementing: Adhesion of neutrophils to endothelial cells in venules at site of acute inflammation, c. Emigration: neutrophils pass between endothelial cells into the tissue, Please rate this question:, , Discuss and give feedback, , Next question, , Acute inflammation, Inflammation is the reaction of the tissue elements to injury. Vascular changes occur, resulting in the, generation of a protein rich exudate. So long as the injury does not totally destroy the existing tissue, architecture, the episode may resolve with restoration of original tissue architecture.
Page 668 :
Vascular changes, , , , , , Vasodilation occurs and persists throughout the inflammatory phase., Inflammatory cells exit the circulation at the site of injury., The equilibrium that balances Starlings forces within capillary beds is disrupted and a protein, rich exudate will form as the vessel walls also become more permeable to proteins., The high fibrinogen content of the fluid may form a fibrin clot. This has several important, immunomodulatory functions., , Sequelae, , Resolution, , , , , Typically occurs with minimal initial injury, Stimulus removed and normal tissue architecture results, , Organisation, , , , , Delayed removal of exudate, Tissues undergo organisation and usually fibrosis, , Suppuration, , , , , Typically formation of an abscess or an empyema, Sequestration of large quantities of dead neutrophils, , Progression to chronic, inflammation, , , , , Coupled inflammatory and reparative activities, Usually occurs when initial infection or suppuration has, been inadequately managed, , Causes, , , , , , , Infections e.g. Viruses, exotoxins or endotoxins released by bacteria, Chemical agents, Physical agents e.g. Trauma, Hypersensitivity reactions, Tissue necrosis, , Presence of neutrophil polymorphs is a histological diagnostic feature of acute inflammation, Next question
Page 669 :
Question 135-137 of 347, Theme: Liver lesions, , A., B., C., D., E., F., G., H., , Haemangioma, Hepatocellular carcinoma, Hepatic metastasis, Polycystic liver disease, Simple liver cyst, Hyatid cyst, Amoebic abscess, Mesenchymal hamartoma, , Please select the most likely liver lesion for the scenario given. Each option may be used once, more, than once or not at all., , 135., , A 42 year old lady has suffered from hepatitis C for many years and has also developed, cirrhosis. On routine follow up, an ultrasound has demonstrated a 2.5cm lesion in the, right lobe of the liver., You answered Haemangioma, The correct answer is Hepatocellular carcinoma, In patients with cirrhosis the presence of a lesion >2cm is highly suggestive of, malignancy. The diagnosis is virtually confirmed if the AFP is >400ng/mL., , 136., , A 25 year old man from the far east presents with a fever and right upper quadrant pain., As part of his investigations a CT scan shows an ill defined lesion in the right lobe of the, liver., You answered Haemangioma, The correct answer is Amoebic abscess, Amoebic abscesses will tend to present in a similar fashion to other pyogenic liver, abscesses. They should be considered in any individual presenting from a region, whereEntamoeba histiolytica is endemic. Treatment with metronidazole usually produces, a marked clinical response., , 137., , A 42 year old lady presents with right upper quadrant pain and a sensation of abdominal, fullness. An ultrasound scan demonstrates a 6.5 cm hyperechoic lesion in the right lobe of, the liver. Serum AFP is normal.
Page 670 :
Haemangioma, A large hyperechoic lesion in the presence of normal AFP is likely to be a haemangioma., An HCC of equivalent size will almost always result in rise in AFP., Please rate this question:, , Discuss and give feedback, , Next question, , Benign liver lesions, Benign liver lesions, , Haemangioma, , , , , , , , , Liver cell, adenoma, , , , , , , , , , Mesenchymal, hamartomas, Liver abscess, , Most common benign tumours of mesenchymal origin, Incidence in autopsy series is 8%, Cavernous haemangiomas may be enormous, Clinically they are reddish purple hypervascular lesions, Lesions are normally separated from normal liver by ring of fibrous, tissue, On ultrasound they are typically hyperechoic, 90% develop in women in their third to fifth decade, Linked to use of oral contraceptive pill, Lesions are usually solitary, They are usually sharply demarcated from normal liver although they, usually lack a fibrous capsule, On ultrasound the appearances are of mixed echoity and, heterogeneous texture. On CT most lesions are hypodense when, imaged prior to administration of IV contrast agents, In patients with haemorrhage or symptoms removal of the adenoma, may be required, , Congential and benign, usually present in infants. May compress normal liver, , , , , Biliary sepsis is a major predisposing factor, Structures drained by the portal venous system form the second largest, source, Common symptoms include fever, right upper quadrant pain. Jaundice, may be seen in 50%
Page 671 :
Amoebic abscess, , , , Ultrasound will usually show a fluid filled cavity, hyperechoic walls, may be seen in chronic abscesses, , , , Liver abscess is the most common extra intestinal manifestation of, amoebiasis, Between 75 and 90% lesions occur in the right lobe, Presenting complaints typically include fever and right upper quadrant, pain, Ultrasonography will usually show a fluid filled structure with poorly, defined boundaries, Aspiration yield sterile odourless fluid which has an anchovy paste, consistency, Treatment is with metronidazole, , , , , , , , Hyatid cysts, , , , , , , , , , , , , Seen in cases of Echinococcus infection, Typically an intense fibrotic reaction occurs around sites of infection, The cyst has no epithelial lining, Cysts are commonly unilocular and may grow to 20cm in size. The, cyst wall is thick and has an external laminated hilar membrane and an, internal enucleated germinal layer, Typically presents with malaise and right upper quadrant pain., Secondary bacterial infection occurs in 10%., Liver function tests are usually abnormal and eosinophilia is present in, 33% cases, Ultrasound may show septa and hyatid sand or daughter cysts., Percutaneous aspiration is contra indicated, Treatment is by sterilisation of the cyst with mebendazole and may be, followed by surgical resection. Hypertonic swabs are packed around, the cysts during surgery, , Polycystic liver, disease, , , , , , Usually occurs in association with polycystic kidney disease, Autosomal dominant disorder, Symptoms may occur as a result of capsular stretch, , Cystadenoma, , , , , , , Rare lesions with malignant potential, Usually solitary multiloculated lesions, Liver function tests usually normal, Ultrasonography typically shows a large anechoic, fluid filled area, with irregular margins. Internal echos may result from septa, Surgical resection is indicated in all cases, , , , Next question
Page 672 :
Question 138 of 347, Which of the following disorders is associated with massive splenomegaly?, , Acute lymphoblastic leukaemia, , Acute myeloblastic leukaemia, , Acute myelomonocytic leukaemia, , Acute monoblastic leukaemia, , Chronic granulocytic leukaemia, , Chronic leukaemia is more likely to be associated with splenomegaly than acute leukaemia., Please rate this question:, , Discuss and give feedback, , Next question, , Spleen, The spleen is located in the left upper quadrant of the abdomen and its size can vary depending, upon the amount of blood it contains. The typical adult spleen is 12.5cm long and 7.5cm wide. The, usual weight of the adult spleen is 150g., The exact position of the spleen can vary with respiratory activity, posture and the state of, surrounding viscera. It usually lies obliquely with its long axis aligned to the 9th, 10th and 11th ribs. It, is separated from these ribs by both diaphragm and pleural cavity. The normal spleen is not, palpable., The shape of the spleen is influenced by the state of the colon and stomach. Gastric distension will, cause the spleen to resemble the shape of an orange segment. Colonic distension will cause it to, become more tetrahedral., The spleen is almost entirely covered by peritoneum, which adheres firmly to its capsule. Recesses, of the greater sac separate it from the stomach and kidney. It develops from the upper dorsal, mesogastrium, remaining connected to the posterior abdominal wall and stomach by two folds of, peritoneum; the lienorenal ligament and gastrosplenic ligament. The lienorenal ligament is derived, from peritoneum where the wall of the general peritoneum meets the omental bursa between the left, kidney and spleen; the splenic vessels lie in its layers. The gastrosplenic ligament also has two, layers, formed by the meeting of the walls of the greater sac and omental bursa between spleen and
Page 673 :
stomach, the short gastric and left gastroepiploic branches of the splenic artery pass in its layers., Laterally, the spleen is in contact with the phrenicocolic ligament., Relations, Superiorly, , Diaphragm, , Anteriorly, , Gastric impression, , Posteriorly, , Kidney, , Inferiorly, , Colon, , Hilum, , Tail of pancreas and splenic vessels (splenic artery divides here, branches pass to the, white pulp transporting plasma), , Contents, White, pulp, , Immune function. Contains central trabecular artery. The germinal centres are supplied, by arterioles called penicilliary radicles., , Red pulp, , Filters abnormal red blood cells., , Function, , , , , , , , Filtration of abnormal blood cells and foreign bodies such as bacteria., Immunity: IgM. Production of properdin, and tuftsin which help target fungi and bacteria for, phagocytosis., Haematopoiesis: up to 5th month gestation or in haematological disorders., Pooling: storage of 40% platelets., Iron reutilisation, Storage monocytes, , Disorders of the spleen, Massive splenomegaly, , , , , , , Myelofibrosis, Chronic myeloid leukaemia, Visceral leishmaniasis (kala-azar), Malaria, Gaucher's syndrome, , Other causes (as above plus), , , , Portal hypertension e.g. secondary to cirrhosis, Lymphoproliferative disease e.g. CLL, Hodgkin's
Page 674 :
, , , , , , Haemolytic anaemia, Infection: hepatitis, glandular fever, Infective endocarditis, Sickle-cell*, thalassaemia, Rheumatoid arthritis (Felty's syndrome), , *the majority of adult patients with sickle-cell will have an atrophied spleen due to repeated infarction, Next question
Page 675 :
Question 139 of 347, Causes of primary chronic inflammation do not include which of the following?, , Sarcoidosis, , Tuberculosis, , Ulcerative colitis, , Hip prostheses, , Chronic cholecystitis, , Chronic cholecystitis is caused by recurrent episodes of acute inflammation., Prosthetic implants may be the site of primary chronic inflammation. A common example clinically is, breast implants which may become encapsulated. The subsequent fibrosis then results in distortion, and may be painful., Please rate this question:, , Discuss and give feedback, , Next question, , Chronic inflammation, Overview, Chronic inflammation may occur secondary to acute inflammation.In most cases chronic, inflammation occurs as a primary process. These may be broadly viewed as being one of three main, processes:, , , , , Persisting infection with certain organisms such as Mycobacterium tuberculosis which results, in delayed type hypersensitivity reactions and inflammation., Prolonged exposure to non-biodegradable substances such as silica or suture materials, which may induce an inflammatory response., Autoimmune conditions involving antibodies formed against host antigens., , Acute vs. Chronic inflammation
Page 676 :
Acute inflammation, , Chronic inflammation, , Changes to existing vascular structure and increased, permeability of endothelial cells, , Angiogenesis predominates, , Infiltration of neutrophils, , Macrophages, plasma cells and, lymphocytes predominate, , Process may resolve with:, , Healing by fibrosis is the main result, , , , , , , , Suppuration, Complete resolution, Abscess formation, Progression to chronic inflammation, Healing by fibrosis, , Granulomatous inflammation, A granuloma consists of a microscopic aggregation of macrophages (with epithelial type, arrangement =epitheliod). Large giant cells may be found at the periphery of granulomas., Mediators, Growth factors released by activated macrophages include agents such as interferon and fibroblast, growth factor (plus many more). Some of these such as interferons may have systemic features, resulting in systemic symptoms and signs, which may be present in individuals with long standing, chronic inflammation., The finding of granulomas is pathognomonic of chronic inflammation, as illustrated in this biopsy, from a patient with colonic Crohns disease
Page 677 :
Image sourced from Wikipedia, , Next question
Page 678 :
Question 140 of 347, A 30 year old man is trapped in a house fire and sustains 30% partial and full thickness burns to his, torso and limbs. Three days following admission he has a brisk haematemesis. Which of the, following is the most likely explanation for this event?, , Dieulafoy lesion, , Curlings ulcers, , Mallory Weiss tear, , Depletion of platelets, , Depletion of clotting factors, , Curlings ulcers typically occur secondary to thermal injuries and are caused by loss of GI protective, mechanisms. They are at greater risk of perforation than stress ulcers and may also haemorrhage., Please rate this question:, , Discuss and give feedback, , Next question, , Burns, Burns may be thermal, chemical or electrical. In the former category are burns which occur as a, result of heat. Chemical burns occur when the skin is exposed to an extremely caustic or alkaline, substance. Electrical burns occur following exposure to electrical current. The immediate, management includes removal of the burning source which usually includes irrigation of the burned, area. A detailed assessment then needs to be made of the extent of the burns and a number of, charts are available for recording this information. The degree of injury relates to the temperature, and duration of exposure. Most domestic burns are mainly scalds in young children., Following the burn, there is a local response with progressive tissue loss and release of, inflammatory cytokines. Systemically, there are cardiovascular effects resulting from fluid loss and, sequestration of fluid into the third space. There is a marked catabolic response. Immunosupression, is common with large burns and bacterial translocation from the gut lumen is a recognised event., Sepsis is a common cause of death following major burns., Types of burn
Page 679 :
Type of burn, , Skin layers, affected, , Skin, appearance, , Blanching, , Epidermal/Superficial, , Epidermis, , Red, moist, , Yes, , Superficial partial, thickness, , Epidermis and part, of papillary dermis, affected, , Pale, dry, , Yes, , Normally heals, with no, intervention, , Deep partial thickness, , Epidermis, whole, papillary dermis, affected, , Mottled red, colour, , No, , Needs surgical, intervention, (depending on site), , Full thickness, , Whole skin layer, and subcutaneous, tissue affected, , Dry, leathery, hard wound, , No, , Burns centre, , Depth of burn assessment, , , , , , Bleeding on needle prick, Sensation, Appearance, Blanching to pressure, , Percentage burn estimation, Lund Browder chart: most accurate even in children, Wallace rule of nines, Palmar surface: surface area palm = 0.8% burn, >15% body surface area burns in adults needs urgent burn fluid resuscitation, Transfer to burn centre if:, , , , , , Need burn shock resuscitation, Face/hands/genitals affected, Deep partial thickness or full thickness burns, Significant electrical/chemical burns, , Management, , Management
Page 680 :
The initial aim is to stop the burning process and resuscitate the patient. Intravenous fluids will be, required for children with burns greater than 10% of total body surface area. Adults with burns, greater than 15% of total body surface area will also require IV fluids. The fluids are calculated using, the Parkland formula which is; volume of fluid= total body surface area of the burn % x weight (Kg), x4. Half of the fluid is administered in the first 8 hours. A urinary catheter should be inserted., Analgesia should be given. Complex burns, burns involving the hand perineum and face and burns, >10% in adults and >5% in children should be transferred to a burns unit., Circumferential burns affecting a limb or severe torso burns impeding respiration may require, escharotomy to divide the burnt tissue., Conservative management is appropriate for superficial burns and mixed superficial burns that will, heal in 2 weeks. More complex burns may require excision and skin grafting. Excision and primary, closure is not generally practised as there is a high risk of infection., There is no evidence to support the use of anti microbial prophylaxis or topical antibiotics in burn, patients., Escharotomies, , , , Indicated in circumferential full thickness burns to the torso or limbs., Careful division of the encasing band of burn tissue will potentially improve ventilation (if the, burn involves the torso), or relieve compartment syndrome and oedema (where a limb is, involved), , References, www.euroburn.org/e107files/downloads/guidelinesburncare.pdf, Barajas-Nava LA, López-Alcalde J, Roqué i Figuls M, Solà I, Bonfill Cosp X. Antibiotic prophylaxis, for preventing burn wound infection. Cochrane Database of Systematic Reviews 2013, Issue 6. Art., No.: CD008738. DOI: 10.1002/14651858.CD008738.pub2., Hettiaratchy S & Papini R. Initial management of a major burn: assessment and resuscitation. BMJ, 2004;329:101-103, Next question
Page 681 :
Question 141-143 of 347, Theme: Adrenal gland disorders, , A., B., C., D., E., F., G., H., I., , Nelsons syndrome, Conns syndrome, Cushings syndrome, Benign incidental adenoma, Malignant adrenal adenoma, Waterhouse- Friderichsen syndrome, Metastatic lesion, Walker - Warburg syndrome, Phaeochromocytoma, , Please select the most appropriate adrenal disorder for the scenario given. Each disorder may be, selected once, more than once or not at all., , 141., , A 19 year old lady is admitted to ITU with severe meningococcal sepsis. She is on, maximal inotropic support and a CT scan of her chest and abdomen is performed. The, adrenal glands show evidence of diffuse haemorrhage., You answered Nelsons syndrome, The correct answer is Waterhouse- Friderichsen syndrome, WaterhouseFriderichsen syndrome is defined as adrenal gland failure due to bleeding into, the adrenal glands. It is caused by severe bacterial infection (most commonly the, meningococcus Neisseria meningitidis)., The bacterial infection leads to massive hemorrhage into one or (usually) both adrenal, glands. It is characterised by overwhelming bacterial infection meningococcemia leading, to massive blood invasion, organ failure, coma, haemodynamic shock, disseminated, intravascular coagulation with widespread purpura, rapidly developing adrenocortical, insufficiency and death., , 142., , A 34 year old lady is admitted with recurrent episodes of non-specific abdominal pain., On each admission all blood investigations are normal, as are her observations. On this, admission a CT scan was performed. This demonstrates a 1.5cm nodule in the right, adrenal gland. This is associated with a lipid rich core. Urinary VMA is within normal, limits. Other hormonal studies are normal., You answered Nelsons syndrome, The correct answer is Benign incidental adenoma
Page 682 :
This is typical for a benign adenoma. Benign adenomas often have a lipid rich core that is, readily identifiable on CT scanning. In addition the nodules are often well circumscribed., 143., , A 38 year old man is noted to have a blood pressure of 175/110 on routine screening. On, examination there are no physical abnormalities of note. CT scanning shows a left sided, adrenal mass. Plasma metanephrines are elevated., You answered Nelsons syndrome, The correct answer is Phaeochromocytoma, Hypertension in a young patient without any obvious cause should be investigated., Urinary VMA and plasma metanephrines are typically elevated., , Please rate this question:, , Discuss and give feedback, , Next question, , Phaeochromocytoma and adrenal lesions, Phaeochromocytoma, Neuroendocrine tumour of the chromaffin cells of the adrenal medulla. Hypertension and, hyperglycaemia are often found., , , , , , 10% of cases are bilateral., 10% occur in children., 11% are malignant (higher when tumour is located outside the adrenal)., 10% will not be hypertensive., , Familial cases are usually linked to the Multiple endocrine neoplasia syndromes (considered under, its own heading)., Most tumours are unilateral (often right sided) and smaller than 10cm., Diagnosis, Urine analysis of vanillymandelic acid (VMA) is often used (false positives may occur e.g. in patients, eating vanilla ice cream!), Blood testing for plasma metanephrine levels., CT and MRI scanning are both used to localise the lesion.
Page 683 :
Treatment, Patients require medical therapy first. An irreversible alpha adrenoreceptor blocker should be given,, although minority may prefer reversible blockade(1). Labetolol may be co-administered for cardiac, chronotropic control. Isolated beta blockade should not be considered as it will lead to unopposed, alpha activity., These patients are often volume depleted and will often require moderate volumes of intra venous, normal saline perioperatively., Once medically optimised the phaeochromocytoma should be removed. Most adrenalectomies can, now be performed using a laparoscopic approach(2). The adrenals are highly vascular structures, and removal can be complicated by catastrophic haemorrhage in the hands of the inexperienced., This is particularly true of right sided resections where the IVC is perilously close. Should the IVC be, damaged a laparotomy will be necessary and the defect enclosed within a Satinsky style vascular, clamp and the defect closed with prolene sutures. Attempting to interfere with the IVC using any, instruments other than vascular clamps will result in vessel trauma and make a bad situation much, worse., Incidental adrenal lesions, Adrenal lesions may be identified on CT scanning performed for other reasons(3). Factors, suggesting benign disease on CT include(4):, , , , , , Size less than 3cm, Homogeneous texture, Lipid rich tissue, Thin wall to lesion, , All patients with incidental lesions should be managed jointly with an endocrinologist and full work up, as described above. Patients with functioning lesions or those with adverse radiological features, (Particularly size >3cm) should proceed to surgery., References, 1. Weingarten TN, Cata JP, O'Hara JF, Prybilla DJ, Pike TL, Thompson GB, et al. Comparison of, two preoperative medical management strategies for laparoscopic resection of pheochromocytoma., Urology. 2010 Aug;76(2):508 e6-11., 2. Nguyen PH, Keller JE, Novitsky YW, Heniford BT, Kercher KW. Laparoscopic approach to, adrenalectomy: review of perioperative outcomes in a single center. Am Surg. 2011 May;77(5):5926., 3. Ng VW, Ma RC, So WY, Choi KC, Kong AP, Cockram CS, et al. Evaluation of functional and, malignant adrenal incidentalomas. Arch Intern Med. 2010 Dec 13;170(22):2017-20., 4. Muth A, Hammarstedt L, Hellstrom M, Sigurjonsdottir HA, Almqvist E, Wangberg B. Cohort study, of patients with adrenal lesions discovered incidentally. Br J Surg. 2011 May 27., Next question
Page 685 :
Question 144 of 347, , A 43 year old man presents with dyspepsia and undergoes an upper GI endoscopy. During the, procedure diffuse gastric and duodenal ulcers are identified. A Clo test confirms the presence, ofHelicobacter pylori infection. What is the most likely explanation for the ulcers?, , Decreased gastric motility, , Increased urease activity, , Decreased release of mucous and bicarbonate, , Decreased gastrin levels, , Increased acid production, , Theme from April 2011 Exam, H-Pylori has a number of pathological effects. In this question the main issue is by what mechanism, the organism is able to induce both gastric and duodenal ulceration. Without modestly elevated acid, levels, the duodenum would not undergo gastric metaplasia. H-Pylori cannot colonise duodenal, mucosa and therefore the development of ulcers at this site can only occur in those who have, undergone metaplastic transformation (mediated by increased acidity)., Please rate this question:, , Discuss and give feedback, , Next question, , Helicobacter Pylori, Infection with Helicobacter Pylori is implicated in many cases of duodenal ulceration and up to 60%, of patients with gastric ulceration.
Page 686 :
It is a gram negative, helical shaped rod with microaerophillic requirements. It has the ability to, produce a urease enzyme that will hydrolyse urea resulting in the production of ammonia. The effect, of ammonia on antral G cells is to cause release of gastrin via a negative feedback loop., Once infection is established the organism releases enzymes that disrupt the gastric mucous layer., Certain subtypes release cytotoxins cag A and vac A gene products. The organism incites a, classical chronic inflammatory process of the gastric epithelium. This accounts for the development, of gastric ulcers. The mildly increased acidity may induce a process of duodenal gastric metaplasia., Whilst duodenal mucosa cannot be colonised by H-Pylori, mucosa that has undergone metaplastic, change to the gastric epithelial type may be colonised by H- Pylori with subsequent inflammation, and development of duodenitis and ulcers., In patients who are colonised there is a 10-20% risk of peptic ulcer, 1-2% risk gastric cancer and, <1% risk MALT lymphoma., Next question
Page 687 :
Question 145 of 347, A 15 year old boy is admitted with colicky abdominal pain of 6 hours duration. On examination he, has a soft abdomen, on systemic examination he has brownish spots around his mouth, feet and, hands. His mother underwent surgery for intussusception, aged 12, and has similar lesions. What is, the most likely underlying diagnosis?, , Li Fraumeni syndrome, , Peutz-Jeghers syndrome, , Addisons disease, , McCune -Albright syndrome, , Appendicitis, , This is most likely to be Peutz-Jeghers syndrome. Addisons and McCune Albright syndrome may, produce similar skin changes but the intussusception resulting from polyps combined with the, autosomal inheritance pattern makes this the most likely diagnosis., Please rate this question:, , Discuss and give feedback, , Next question, , Peutz-Jeghers syndrome, Peutz-Jeghers syndrome is an autosomal dominant condition characterised by numerous benign, hamartomatous polyps in the gastrointestinal tract. It is also associated with pigmented freckles on, the lips, face, palms and soles. Around 50% of patients will have died from a gastrointestinal tract, cancer by the age of 60 years., Genetics, , , , Autosomal dominant, Responsible gene encodes serine threonine kinase LKB1 or STK11, , Features
Page 688 :
, , , , , Hamartomatous polyps in GI tract (mainly small bowel), Pigmented lesions on lips, oral mucosa, face, palms and soles, Intestinal obstruction e.g. intussusception (which may lead to diagnosis), Gastrointestinal bleeding, , Management, , , Conservative unless complications develop, Next question
Page 689 :
Question 146 of 347, What is the most likely electrolyte abnormality in a patient with diarrhoea and a soft mass felt on, digital rectal examination?, , Hyperkalaemia, , Hypokalaemia, , Hyponatraemia, , Hypernatraemia, , Hypocalcaemia, , Large villous adenomas of the rectum may have marked secretory activity and result in the, development of hypokalaemia as rectal secretions are rich in potassium., Please rate this question:, , Discuss and give feedback, , Next question, , Hypokalaemia, Potassium and hydrogen can be thought of as competitors. Hyperkalaemia tends to be associated, with acidosis because as potassium levels rise fewer hydrogen ions can enter the cells, Hypokalaemia with alkalosis, , , , , , Vomiting, Diuretics, Cushing's syndrome, Conn's syndrome (primary hyperaldosteronism), , Hypokalaemia with acidosis, , , , Diarrhoea, Renal tubular acidosis
Page 693 :
Question 148 of 347, A 25 year old male pedestrian is involved in a road traffic accident. He sustains multiple injuries and, is admitted to the intensive care unit, intubated and ventilated. Over the next week he develops adult, respiratory distress syndrome. What is the main reason for hypoxaemia in this condition?, , Increased lung compliance, , Reduced diffusion, , Reduced surfactant, , Reduced elastase, , Left to right shunt, , Theme from September 2014 Exam, The diffuse lung injury, which is associated with loss of surfactant and increased elastase release, from neutrophils, results in fluid accumulation. This leads to reduced diffusion, which is the main, reason for hypoxaemia., Please rate this question:, , Discuss and give feedback, , Next question, , Adult respiratory distress syndrome, Defined as an acute condition characterized by bilateral pulmonary infiltrates and severe hypoxemia, (PaO2/FiO2 ratio < 200) in the absence of evidence for cardiogenic pulmonary oedema (clinically or, pulmonary capillary wedge pressure of less than 18 mm Hg)., In is subdivided into two stages. Early stages consist of an exudative phase of injury with associated, oedema. The later stage is one of repair and consists of fibroproliferative changes. Subsequent, scarring may result in poor lung function., Causes, , , , , , Sepsis, Direct lung injury, Trauma, Acute pancreatitis
Page 694 :
, , , Long bone fracture or multiple fractures (through fat embolism), Head injury (causes sympathetic nervous stimulation which leads to acute pulmonary, hypertension), , Clinical features, , , , , Acute dyspnoea and hypoxaemia hours/days after event, Multi organ failure, Rising ventilatory pressures, , Management, , , , , , , Treat the underlying cause, Antibiotics (if signs of sepsis), Negative fluid balance i.e. Diuretics, Recruitment manoeuvres such as prone ventilation, use of positive end expiratory pressure, Mechanical ventilation strategy using low tidal volumes, as conventional tidal volumes may, cause lung injury (only treatment found to improve survival rates), Next question
Page 695 :
Question 149 of 347, A 24 year old male was admitted with bloody diarrhea, cramping abdominal pain and weight loss., Colonoscopy revealed a friable, diffusely red mucosa involving the rectum and sigmoid colon. The, mucosa was normal proximal to this. The disease progressed with time to involve most of the entire, colon, but not the ileum. Many years later, a colonic biopsy shows high grade epithelial dysplasia., What is the most likely initial diagnosis?, , Colonic tuberculosis, , Collagenous colitis, , Ulcerative colitis, , Crohns disease, , Ischaemic colitis, , Theme from January 2015 Exam, Ulcerative colitis spreads in a progressive distal to proximal manner. Over time a dysplastic, transformation is recognised. Such endoscopic findings mandate a minimum of close endoscopic, surveillance and if they occur in association with a colonic mass then usually a, pancproctocolectomy., Please rate this question:, , Discuss and give feedback, , Next question, , Ulcerative colitis, Ulcerative colitis is a form of inflammatory bowel disease. Inflammation always starts at rectum,, does not spread beyond ileocaecal valve (although backwash ileitis may occur) and is continuous., The peak incidence of ulcerative colitis is in people aged 15-25 years and in those aged 55-65, years. It is less common in smokers., The initial presentation is usually following insidious and intermittent symptoms. Features include:, , , , , bloody diarrhoea, urgency, tenesmus
Page 697 :
, , , , Superficial inflammation of the colonic and rectal mucosa, Continuous disease from rectum proximally, Superficial ulceration, mucosal islands, loss of vascular definition and continuous ulceration, pattern., , Management, , , , , Patients with long term disease are at increased risk of development of malignancy, Acute exacerbations are generally managed with steroids, in chronic patients agents such as, azathioprine and infliximab may be used, Individuals with medically unresponsive disease usually require surgery- in the acute phase, a sub total colectomy and end ileostomy. In the longer term a proctectomy will be required., An ileoanal pouch is an option for selected patients, , References, Ford A et al. Ulcerative colitis. BMJ 2013 (346):29-34., Next question
Page 698 :
Question 150 of 347, Which virus is associated with Kaposi's sarcoma?, , Human herpes virus 8, , Human papillomavirus 16, , Human T-lymphotropic virus 1, , Epstein-Barr virus, , Human papillomavirus 18, , Please rate this question:, , Discuss and give feedback, , Next question, , Oncoviruses, , , , Viruses which cause cancer, These may be detected on blood test and prevented by vaccine, , These are the main types of oncoviruses and their diseases:, , Oncovirus, , Cancer, , Epstein-Barr virus, , Burkitt's lymphoma, Hodgkin's lymphoma, Post transplant lymphoma, Nasopharyngeal carcinoma, , Human papillomavirus 16/18, , Cervical cancer, Anal cancer
Page 699 :
Penile cancer, Vulval cancer, Oropharyneal cancer, , Human herpes virus 8, , Kaposi's sarcoma, , Hepatitis B virus, , Hepatocellular carcinoma, , Hepatitis C virus, , Hepatocellular carcinoma, , Human T-lymphotropic virus 1, , Tropical spastic paraparesis, Adult T cell leukaemia, Next question
Page 700 :
Question 151 of 347, Which of the following is not a feature of Wallerian Degeneration?, , May result from an axonotmesis, , Typically occurs in the peripheral nervous systems, , The axon remains excitable throughout the whole process, , The distal neuronal stump is affected, , Is a component of the healing process following neuronal injury, , The axon loses its excitability once the process is established., Please rate this question:, , Discuss and give feedback, , Next question, , Wallerian degeneration, - Is the process that occurs when a nerve is cut or crushed., - It occurs when the part of the axon separated from the neuron's cell nucleus degenerates., - It usually begins 24 hours following neuronal injury and the distal axon remains excitable up until, this time., - The degeneration of the axon is following by breakdown of the myelin sheath, a process that, occurs by infiltration of the site with macrophages., - Eventually regeneration of the nerve may occur although recovery will depend on the extent and, manner of injury, Next question
Page 701 :
Question 152 of 347, , A 45 year old woman complains of painful tingling in her fingers. The pain is relieved by hanging the, arm over the side of the bed. She has a positive Tinel's sign at the wrist. Which of the following is, most likely to contribute to her diagnosis?, , Methotrexate use, , Crohn's disease, , Hyperthyroidism, , Tuberculosis, , Rheumatoid arthritis, , This woman has a diagnosis of carpal tunnel syndrome. Rheumatological disorders are a common, cause. Clinical examination should focus on identifying stigmata of rheumatoid arthritis, such as, rheumatoid nodules, vasculitic lesions and metacarpophalangeal joint arthritis., Please rate this question:, , Discuss and give feedback, , Next question, , Carpal tunnel syndome, Carpal tunnel syndrome is caused by compression of median nerve in the carpal tunnel, History, , , , pain/pins and needles in thumb, index, middle finger e.g. at night
Page 702 :
, , patient flicks hand to obtain relief, , Examination, , , , , , , weakness of thumb abduction, wasting of thenar eminence (NOT hypothenar), Tinel's sign: tapping causes paraesthesia, Phalen's sign: flexion of wrist causes symptoms, , Causes of carpal tunnel syndrome, MEDIAN TRAP Mnemonic, , , , , , , , , , , , , Myxoedema, Edema premenstrually, Diabetes, Idiopathic, Acromegaly, Neoplasm, Trauma, Rheumatoid arthritis, Amyloidosis, Pregnancy, , Management, , Non surgical treatment, , Surgery, , May resolve, spontaneously, Avoid precipitants and, reassurance, Night-time splints, Local steroid injections, , Complete division of the flexor retinaculum and decompression of the tunnel, (successful in approximately 80% of patients), , Next question
Page 703 :
Question 153 of 347, A 30 year old male presents with a painless swelling of the testis. Histologically the stroma has a, lymphocytic infiltrate. The most likely diagnosis is :, , Differentiated teratoma, , Malignant undifferentiated teratoma, , Classical seminoma, , Spermatocytic seminoma, , Anaplastic seminoma, , Seminoma is the commonest type of testicular tumour and is more common in males aged between, 30-40 years. Classical seminoma is the commonest subtype and histology shows lymphocytic, stromal infiltrate. Other subtypes include:, 1. Spermatocytic: tumour cells resemble spermatocytes. Excellent prognosis., 2. Anaplastic, 3. Syncytiotrophoblast giant cells: β HCG present in cells, A teratoma is more common in males aged 20-30 years., Please rate this question:, , Discuss and give feedback, , Next question, , Testicular disorders, Testicular cancer, Testicular cancer is the most common malignancy in men aged 20-30 years. Around 95% of cases, of testicular cancer are germ-cell tumours. Germ cell tumours may essentially be divided into:, , Tumour type, , Seminoma, , Key features, , , Commonest, subtype (50%), , Tumour, markers, , Pathology, , AFP usually, normal, , Sheet like lobular, patterns of cells
Page 704 :
Tumour type, , Tumour, markers, , Pathology, , Average age at, diagnosis = 40, Even advanced, disease associated, with 5 year, survival of 73%, , HCG elevated, in 10%, seminomas, Lactate, dehydrogenase;, elevated in 1020% seminomas, (but also in many, other conditions), , with substantial, fibrous, component., Fibrous septa, contain, lymphocytic, inclusions and, granulomas may, be seen., , Younger age at, presentation =20-30, years, Advanced disease, carries worse prognosis, (48% at 5 years), Retroperitoneal lymph, node dissection may be, needed for residual, disease after, chemotherapy, , AFP elevated, in up to 70% of, cases, HCG elevated, in up to 40% of, cases, Other markers, rarely helpful, , Heterogenous, texture with, occasional ectopic, tissue such as hair, , Key features, , , , Non seminomatous germ, cell tumours (42%), , , , , , Teratoma, Yolk sac tumour, Choriocarcinoma, Mixed germ cell, tumours (10%), , Image demonstrating a classical seminoma, these tumours are typically more uniform than, teratomas
Page 705 :
Image sourced from Wikipedia, , Risk factors for testicular cancer, , , , , , , Cryptorchidism, Infertility, Family history, Klinefelter's syndrome, Mumps orchitis, , Features
Page 706 :
, , , , A painless lump is the most common presenting symptom, Pain may also be present in a minority of men, Other possible features include hydrocele, gynaecomastia, , Diagnosis, , , , , Ultrasound is first-line, CT scanning of the chest/ abdomen and pelvis is used for staging, Tumour markers (see above) should be measured, , Management, , , , , Orchidectomy (Inguinal approach), Chemotherapy and radiotherapy may be given depending on staging, Abdominal lesions >1cm following chemotherapy may require retroperitoneal lymph node, dissection., , Prognosis is generally excellent, , , , 5 year survival for seminomas is around 95% if Stage I, 5 year survival for teratomas is around 85% if Stage I, , Benign disease, Epididymo-orchitis, Acute epididymitis is an acute inflammation of the epididymis, often involving the testis and usually, caused by bacterial infection., , , , , Infection spreads from the urethra or bladder. In men <35 years, gonorrhoea or chlamydia, are the usual infections., Amiodarone is a recognised non infective cause of epididymitis, which resolves on stopping, the drug., Tenderness is usually confined to the epididymis, which may facilitate differentiating it from, torsion where pain usually affects the entire testis., , Testicular torsion, , , , , , Twist of the spermatic cord resulting in testicular ischaemia and necrosis., Most common in males aged between 10 and 30 (peak incidence 13-15 years), Pain is usually severe and of sudden onset., Cremasteric reflex is lost and elevation of the testis does not ease the pain.
Page 707 :
, , Treatment is with surgical exploration. If a torted testis is identified then both testis should be, fixed as the condition of bell clapper testis is often bilateral., , Hydrocele, , , , , , , Presents as a mass that transilluminates, usually possible to "get above" it on examination., In younger men it should be investigated with USS to exclude tumour., In children it may occur as a result of a patent processus vaginalis., Treatment in adults is with a Lords or Jabouley procedure., Treatment in children is with trans inguinal ligation of PPV., Next question
Page 708 :
Question 154 of 347, , A 48 year old women presents with recurrent loin pain and fevers. Investigation reveals a staghorn, calculus of the left kidney. Infection with which of the following organisms is most likely?, , Staphylococcus saprophyticus, , Proteus mirabilis, , Klebsiella, , E-Coli, , Staphylococcus epidermidis, , Theme from April 2012 Exam, Infection with Proteus mirabilis accounts for 90% of all proteus infections. It has a urease producing, enzyme. This will tend to favor urinary alkalinisation which is a relative prerequisite for the formation, of staghorn calculi., Please rate this question:, , Discuss and give feedback, , Next question, , Renal stones, Type of, stones, , Features, , Percentage of, all calculi
Page 709 :
Type of, stones, , Features, , Percentage of, all calculi, , Calcium, oxalate, , Hypercalciuria is a major risk factor (various causes), Hyperoxaluria may also increase risk, Hypocitraturia increases risk because citrate forms complexes with, calcium making it more soluble, Stones are radio-opaque (though less than calcium phosphate stones), Hyperuricosuria may cause uric acid stones to which calcium oxalate, binds, , 85%, , Cystine, , Inherited recessive disorder of transmembrane cystine transport, leading to decreased absorption of cystine from intestine and renal, tubule, Multiple stones may form, Relatively radiodense because they contain sulphur, , 1%, , Uric acid, , Uric acid is a product of purine metabolism, May precipitate when urinary pH low, May be caused by diseases with extensive tissue breakdown e.g., malignancy, More common in children with inborn errors of metabolism, Radiolucent, , 5-10%, , Calcium, phosphate, , May occur in renal tubular acidosis, high urinary pH increases, supersaturation of urine with calcium and phosphate, Renal tubular acidosis types 1 and 3 increase risk of stone formation, (types 2 and 4 do not), Radio-opaque stones (composition similar to bone), , 10%, , Struvite, , Stones formed from magnesium, ammonium and phosphate, Occur as a result of urease producing bacteria (and are thus, associated with chronic infections), Under the alkaline conditions produced, the crystals can precipitate, Slightly radio-opaque, , 2-20%
Page 710 :
Effect of urinary pH on stone formation, Urine pH will show individual variation (from pH 5-7). Post prandially the pH falls as purine, metabolism will produce uric acid. Then the urine becomes more alkaline (alkaline tide). When the, stone is not available for analysis the pH of urine may help to determine which stone was present., , Stone type, , Urine acidity, , Mean urine pH, , Calcium phosphate, , Normal- alkaline, , >5.5, , Calcium oxalate, , Variable, , 6, , Uric acid, , Acid, , 5.5, , Struvate, , Alkaline, , >7.2, , Cystine, , Normal, , 6.5, Next question
Page 711 :
Question 155 of 347, Causes of granulomatous disease do not include:, , Amiodarone, , Allopurinol, , Sulphonamides, , Beryllium, , Wegener's granulomatosis, , Allopurinol and sulphonamides cause hepatic granulomas., Please rate this question:, , Discuss and give feedback, , Next question, , Chronic inflammation, Overview, Chronic inflammation may occur secondary to acute inflammation.In most cases chronic, inflammation occurs as a primary process. These may be broadly viewed as being one of three main, processes:, , , , , Persisting infection with certain organisms such as Mycobacterium tuberculosis which results, in delayed type hypersensitivity reactions and inflammation., Prolonged exposure to non-biodegradable substances such as silica or suture materials, which may induce an inflammatory response., Autoimmune conditions involving antibodies formed against host antigens., , Acute vs. Chronic inflammation, , Acute inflammation, , Chronic inflammation
Page 712 :
Changes to existing vascular structure and increased, permeability of endothelial cells, , Angiogenesis predominates, , Infiltration of neutrophils, , Macrophages, plasma cells and, lymphocytes predominate, , Process may resolve with:, , Healing by fibrosis is the main result, , , , , , , , Suppuration, Complete resolution, Abscess formation, Progression to chronic inflammation, Healing by fibrosis, , Granulomatous inflammation, A granuloma consists of a microscopic aggregation of macrophages (with epithelial type, arrangement =epitheliod). Large giant cells may be found at the periphery of granulomas., Mediators, Growth factors released by activated macrophages include agents such as interferon and fibroblast, growth factor (plus many more). Some of these such as interferons may have systemic features, resulting in systemic symptoms and signs, which may be present in individuals with long standing, chronic inflammation., The finding of granulomas is pathognomonic of chronic inflammation, as illustrated in this biopsy, from a patient with colonic Crohns disease, , Image sourced from Wikipedia
Page 713 :
Question 156-158 of 347, , Theme: Facial nerve palsy, , A. Adenoid cystic carcinoma, B. Cerebrovascular accident, C. Petrous temporal fracture, D. Warthins tumour, E. Sarcoidosis, F. Pleomorphic adenoma, G. Cholesteatoma, , Please select the most likely cause of facial nerve palsy for the scenario given. Each option may be, used once, more than once or not at all., , 156., , A 22 year old man presents with symptoms of lethargy and bilateral facial nerve palsy. On, examination he has bilateral parotid gland enlargement., You answered Adenoid cystic carcinoma, The correct answer is Sarcoidosis, Theme from 2011 Exam, Facial nerve palsy is the commonest neurological manifestation of sarcoid. It usually resolves., The absence of ear discharge or discrete lesion on palpation is against the other causes., , 157., , A 21 year old man presents with a unilateral facial nerve palsy after being hit in the head. On, examination he has a right sided facial nerve palsy and a watery discharge from his nose., You answered Adenoid cystic carcinoma
Page 714 :
The correct answer is Petrous temporal fracture, Nasal discharge of clear fluid and recent head injury makes a basal skull fracture the most likely, underlying diagnosis., , 158., , A 43 year old lady presents with symptoms of chronic ear discharge and a right sided facial nerve, palsy. On examination she has foul smelling fluid draining from her right ear and a complete, right sided facial nerve palsy., You answered Adenoid cystic carcinoma, The correct answer is Cholesteatoma, Foul smelling ear discharge and facial nerve weakness is likely to be due to cholesteatoma. The, presence of a neurological deficit is a sinister feature., , Please rate this question:, , Discuss and give feedback, , Next question, , Facial nerve palsy, Sarcoid, , Facial nerve palsy is the most frequent neurological manifestation of sarcoid, Affects right and left side with equal frequency, may be bilateral, Typically resolves in up to 80% of cases, , Cholesteatoma, , Destructive and expanding growth of keratinised squamous epithelium, Patients often complain of chronic ear discharge, Infection with Pseudomonas may occur resulting in foul smell to discharge, Aquired lesions usually arise from the Pars flaccida region of the tympanic, membrane, Surgical removal and mastoidectomy may be needed
Page 715 :
Recurrence rates of 20% may be seen following surgery, , Basal skull, fracture, , History of head injury, Presence of features such as Battles sign on examination, Clinical presence of CSF leak strongly supports diagnosis, Assessment is by CT and MRI scan, Prophylactic antibiotics should be given in cases of CSF leak, , Next question
Page 717 :
, , Whole breast irradiation improves locoregional control when breast conserving surgery is, performed, , Lobular carcinoma in situ, , , , , , , Much rarer than DCIS, Does not form microcalcifications, Usually single growth pattern, When an invasive component is found it is less likely to be associated with axillary nodal, metastasis than with DCIS, Low grade LCIS is usually treated by monitoring rather than excision, Next question
Page 718 :
Question 160 of 347, In patients with an annular pancreas where is the most likely site of obstruction?, , The first part of the duodenum, , The second part of the duodenum, , The fourth part of the duodenum, , The third part of the duodenum, , The duodeno-jejunal flexure, , Theme from September 2014 Exam, The pancreas develops from two foregut outgrowths (ventral and dorsal). During rotation the ventral, bud and adjacent gallbladder and bile duct lie together and fuse. When the pancreas fails to rotate, normally it can compress the duodenum with development of obstruction. Usually occurring as a, result of associated duodenal malformation. The second part of the duodenum is the commonest, site., Please rate this question:, , Discuss and give feedback, , Next question, , Pancreas, The pancreas is a retroperitoneal organ and lies posterior to the stomach. It may be accessed, surgically by dividing the peritoneal reflection that connects the greater omentum to the transverse, colon. The pancreatic head sits in the curvature of the duodenum. Its tail lies close to the hilum of, the spleen, a site of potential injury during splenectomy., Relations, Posterior to the pancreas, , Pancreatic head, , Inferior vena cava, Common bile duct, Right and left renal veins, Superior mesenteric vein and artery
Page 719 :
Pancreatic neck, , Superior mesenteric vein, portal vein, , Pancreatic body-, , Left renal vein, Crus of diaphragm, Psoas muscle, Adrenal gland, Kidney, Aorta, , Pancreatic tail, , Left kidney, , Anterior to the pancreas, , Pancreatic head, , 1st part of the duodenum, Pylorus, Gastroduodenal artery, SMA and SMV(uncinate process), , Pancreatic body, , Stomach, Duodenojejunal flexure, , Pancreatic tail, , Splenic hilum, , Superior to the pancreas, Coeliac trunk and its branches common hepatic artery and splenic artery, Grooves of the head of the pancreas, 2nd and 3rd part of the duodenum, Arterial supply, , , , Head: pancreaticoduodenal artery, Rest: splenic artery, , Venous drainage, , , , Head: superior mesenteric vein, Body and tail: splenic vein
Page 720 :
Ampulla of Vater, , , , Merge of pancreatic duct and common bile duct, Is an important landmark, halfway along the second part of the duodenum, that marks the, anatomical transition from foregut to midgut (also the site of transition between regions, supplied by coeliac trunk and SMA)., , Image sourced from Wikipedia, , Next question
Page 721 :
Question 161-163 of 347, Theme: Chest pain, , A., B., C., D., E., F., G., , Achalasia, Pulmonary embolus, Dissection of thoracic aorta, Boerhaaves syndrome, Gastro-oesophageal reflux, Carcinoma of the oesophagus, Oesophageal candidiasis, , Please select the most likely cause for chest pain for the scenario given. Each option may be used, once, more than once or not at all., , 161., , A 43 year old man who has a long term history of alcohol misuse is admitted with a, history of an attack of vomiting after an episode of binge drinking. After vomiting he, developed sudden onset left sided chest pain, which is pleuritic in nature. On examination, he is profoundly septic and drowsy with severe epigastric tenderness and left sided chest, pain., You answered Achalasia, The correct answer is Boerhaaves syndrome, In patients with Boerhaaves the rupture is often on the left side. The story here is typical., All patients should have a contrast study to confirm the diagnosis and the affected site, prior to thoracotomy., , 162., , A 22 year old man is admitted with severe retrosternal chest pain and recurrent episodes, of dysphagia. These occur sporadically and often resolve spontaneously. On examination, there are no physical abnormalities and the patient seems well., Achalasia, Achalasia may produce severe chest pain and many older patients may undergo cardiac, investigations prior to endoscopy., Endoscopic injection with botulinum toxin is a popular treatment (although the benefit is, not long lasting). Cardiomyotomy together with an antireflux procedure is a more durable, alternative., , 163., , An obese 53 year old man presents with symptoms of recurrent retrosternal discomfort, and dyspepsia. This is typically worse at night after eating a large meal. On examination
Page 722 :
there is no physical abnormality to find., You answered Achalasia, The correct answer is Gastro-oesophageal reflux, Patients with GORD often have symptoms that are worse at night. In this age group an, Upper GI endoscopy should probably be performed., Please rate this question:, , Discuss and give feedback, , Next question, , Surgical chest pain, Dissection of, thoracic aorta, , , , , , Tearing interscapular pain, Discrepancy in arterial blood pressures taken in both arms, May show mediastinal widening on chest x-ray, , Diffuse, oesophageal, spasm, , , , , , , Spectrum of oesophageal motility disorders, Caused by uncoordinated contractions of oesphageal muscles, May show "nutcracker oesophagus" on barium swallow, Symptoms include dysphagia, retrosternal discomfort and dyspepsia, , Gastrooesphageal, reflux, , , , , Common cause of retrosternal discomfort, Usually associated with symptoms of regurgitation, odynophagia and, dyspepsia, Symptoms usually well controlled with PPI therapy, Risk factors include obesity, smoking and excess alcohol consumption, , , , , Boerhaaves, syndrome, , , , , , , , Spontaneous rupture of the oesophagus, Caused by episodes of repeated vomiting often in association with, alcohol excess, Typically there is an episode of repetitive vomiting followed by severe, chest and epigastric pain, Diagnosis is by CT and contrast studies, Treatment is surgical; during first 12 hours primary repair, beyond this, usually creation of controlled fistula with a T Tube, delay beyond 24
Page 723 :
hours is associated with fulminent mediastinitis and is usually fatal., , Achalasia, , , , , , , Difficulty swallowing, dysphagia to both liquids and solids and, sometimes chest pain, Usually caused by failure of distal oesphageal inhibitory neurones, Diagnosis is by pH and manometry studies together with contrast, swallow and endoscopy, Treatment is with either botulinum toxin, pneumatic dilatation or, cardiomyotomy, Next question
Page 724 :
Question 164 of 347, A 32 year old woman presents with an episode of haemoptysis and is found to have metastatic, tumour present within the parenchyma of the lungs. This is biopsied and subsequent histology, shows clear cells. What is the most likely primary site?, , Kidney, , Breast, , Liver, , Adrenal, , Bone, , Clear cell tumours are a sub type of renal cell cancer it is associated with specific genetic changes, localised to chromosome 3., Please rate this question:, , Discuss and give feedback, , Next question, , Renal lesions, Lesion, , Renal cell, carcinoma, , Disease specific features, , , , , , Most present with haematuria, (50%), Common renal tumour (85%, cases), Paraneoplastic features include, hypertension and polycythaemia, Most commonly has, haematogenous mestastasis, , Treatment, , Usually radical or partial, nephrectomy
Page 725 :
Lesion, , Nephroblastoma, , Disease specific features, , , , , , , , Neuroblastoma, , , , , , , , , , Transitional cell, carcinoma, , , , , , , , , , Angiomyolipoma, , , , , , Treatment, , Rare childhood tumour, It accounts for 80% of all, genitourinary malignancies in, those under the age of 15 years, Up to 90% will have a mass, 50% will be hypertensive, Diagnostic work up includes, ultrasound and CT scanning, , Surgical resection combined, with chemotherapy (usually, vincristine, actinomycin D and, doxorubicin), , Most common extracranial, tumour of childhood, 80% occur in those under 4 years, of age, Tumour of neural crest origin (up, to 50% occur in the adrenal, gland), The tumour is usually calcified, and may be diagnosed using, MIBG scanning, Staging is with CT, , Surgical resection, radiotherapy, and chemotherapy, , Accounts for 90% of, lower urinary tract tumours, but, only 10% of renal tumours, Males affected 3x more than, females, Occupational exposure to, industrial dyes and rubber, chemicals may increase risk, Up to 80% present with painless, haematuria, Diagnosis and staging is with CT, IVU, , Radical nephroureterectomy, , 80% of these hamartoma type, lesions occur sporadically, the, remainder are seen in those with, tuberous sclerosis, Tumour is composed of blood, vessels, smooth muscle and fat, , 50% of patients with lesions, >4cm will have symptoms and, will require surgical resection
Page 726 :
Lesion, , Disease specific features, , , Treatment, , Massive bleeding may occur in, 10% of cases, Next question
Page 727 :
Question 165 of 347, A laceration of the wrist produces a median nerve transection. The wound is clean and seen, immediately after injury. Collateral soft tissue damage is absent. The patient asks what the, prognosis is. You indicate that the nerve should regrow at approximately:, , 0.1 mm per day, , 1 mm per day, , 5 mm per day, , 1 cm per day, , None of the above, , Transaction of a peripheral nerve results in hemorrhage and retraction of the severed nerve ends., Almost immediately, degeneration of the axon distal to the injury begins. Degeneration also occurs in, the proximal fragment back to the first node of Ranvier. Phagocytosis of the degenerated axonal, fragments leaves neurilemmal sheath with empty cylindrical spaces where the axons were. Several, days following the injury, axons from the proximal fragment begin to regrow. If they make contact, with the distal neurilemmal sheath, regrowth occurs at about the rate of 1 mm/day. However, if, associated trauma, fracture, infection, or separation of neurilemmal sheath ends precludes contact, between axons, growth is haphazard and a traumatic neuroma is formed. When neural transaction is, associated with widespread soft tissue damage and hemorrhage (with increased probability of, infection), many surgeons choose to delay reapproximation of the severed nerve end for 3 to 4, weeks., Please rate this question:, , Discuss and give feedback, , Next question, , Nerve injury, There are 3 types of nerve injury:, , Neuropraxia, , , , , , , Nerve intact but electrical conduction is affected, Full recovery, Autonomic function preserved, Wallerian degeneration does not occur
Page 728 :
Axonotmesis, , Neurotmesis, , , , , Axon is damaged and the myelin sheath is preserved. The connective tissue, framework is not affected., Wallerian degeneration occurs., , , , , Disruption of the axon, myelin sheath and surrounding connective tissue., Wallerian degeneration occurs., , Wallerian Degeneration, , , , , , Axonal degeneration distal to the site of injury., Typically begins 24-36 hours following injury., Axons are excitable prior to degeneration occurring., Myelin sheath degenerates and is phagocytosed by tissue macrophages., , Nerve repair, , , Neuronal repair may only occur physiologically where nerves are in direct contact. Where a, large defect is present, the process of nerve regeneration is hampered. It may not occur at, all or result in the formation of a neuroma. Where nerve regrowth occurs it is typically at a, rate of 1mm per day., Next question
Page 729 :
Question 166 of 347, Which of the following statements relating to gastric cancer is untrue?, , It is associated with chronic helicobacter pylori infection, , 5% of gastric malignancies are due to lymphoma, , In the Lauren classification the diffuse type of adenocarcinoma typically presents as a, large exophytic growth in the antrum, Smoking is a risk factor, , It is associated with acanthosis nigricans, Barium meal appearances of linitis plastica:, Due to the increased rigidity of the wall, the stomach cannot be adequately distended, with only a, narrow lumen identified. The normal mucosal fold pattern is absent, either distorted, thickened or, nodular., The Lauren classification describes a diffuse type of adenocarcinoma (Linitis plastica type lesion), and an intestinal type. The diffuse type is often deeply infiltrative and may be difficult to detect on, endoscopy. Barium meal appearances can be characteristic., Please rate this question:, , Discuss and give feedback, , Next question, , Gastric cancer, Overview, There are 700,000 new cases of gastric cancer worldwide each year. It is most common in Japan, and less common in western countries. It is more common in men and incidence rises with, increasing age. The exact cause of many sporadic cancer is not known, however, familial cases do, occur in HNPCC families. In addition, smoking and smoked or preserved foods increase the risk., Japanese migrants retain their increased risk (decreased in subsequent generations). The, distribution of the disease in western countries is changing towards a more proximal location, (perhaps due to rising obesity)., Pathology, There is some evidence of support a stepwise progression of the disease through intestinal, metaplasia progressing to atrophic gastritis and subsequent dysplasia, through to cancer. The
Page 730 :
favoured staging system is TNM. The risk of lymph node involvement is related to size and depth of, invasion; early cancers confined to submucosa have a 20% incidence of lymph node metastasis., Tumours of the gastro-oesophageal junction are classified as below:, , Type, 1, , True oesophageal cancers and may be associated with Barrett's oesophagus., , Type, 2, , Carcinoma of the cardia, arising from cardiac type epithelium, or short segments with intestinal metaplasia at the oesophagogastric junction., , Type, 3, , Sub cardial cancers that spread across the junction. Involve similar nodal stations to, gastric cancer., , Groups for close endoscopic monitoring, , , , , , Intestinal metaplasia of columnar type, Atrophic gastritis, Low to medium grade dysplasia, Patients who have previously undergone resections for benign peptic ulcer disease (except, highly selective vagotomy)., , Referral to endoscopy, , Patients of any age with, dyspepsia and any of the, following, , Patients without, dyspepsia, , Worsening dyspepsia, , Chronic gastrointestinal bleeding, , Dysphagia, , Barretts oesophagus, , Dysphagia, , Unexplained abdominal, pain or weight loss, , Intestinal metaplasia, , Weight loss, , Vomiting, , Dysplasia, , Iron deficiency anaemia, , Upper abdominal mass, , Atrophic gastritis
Page 731 :
Upper abdominal mass, , Jaundice, , Patient aged over 55 years with, unexplained or persistent, dyspepsia, , Upper GI endoscopy performed for dyspepsia. The addition of dye spraying (as shown in the bottom, right) may facilitate identification of smaller tumours, , Image sourced from Wikipedia, , Staging, , , , , CT scanning of the chest abdomen and pelvis is the routine first line staging investigation in, most centres., Laparoscopy to identify occult peritoneal disease, PET CT (particularly for junctional tumours), , Treatment, , , , Proximally sited disease greater than 5-10cm from the OG junction may be treated by sub, total gastrectomy, Total gastrectomy if tumour is <5cm from OG junction
Page 732 :
, , , , , For type 2 junctional tumours (extending into oesophagus) oesophagogastrectomy is usual, Endoscopic sub mucosal resection may play a role in early gastric cancer confined to the, mucosa and perhaps the sub mucosa (this is debated), Lymphadenectomy should be performed. A D2 lymphadenectomy is widely advocated by the, Japanese, the survival advantages of extended lymphadenectomy have been debated., However, the overall recommendation is that a D2 nodal dissection be undertaken., Most patients will receive chemotherapy either pre or post operatively., , Prognosis, UK Data, , Disease extent, , Percentage 5 year survival, , All RO resections, , 54%, , Early gastric cancer, , 91%, , Stage 1, , 87%, , Stage 2, , 65%, , Stage 3, , 18%, , Operative procedure, Total Gastrectomy , lymphadenectomy and Roux en Y anastomosis, General anaesthesia, Prophylactic intravenous antibiotics, Incision: Rooftop., Perform a thorough laparotomy to identify any occult disease., Mobilise the left lobe of the liver off the diaphragm and place a large pack over it. Insert a large self, retaining retractor e.g. omnitract or Balfour (take time with this, the set up should be perfect). Pack, the small bowel away., Begin by mobilising the omentum off the transverse colon., Proceed to detach the short gastric vessels., Mobilise the pylorus and divide it at least 2cm distally using a linear cutter stapling device., Continue the dissection into the lesser sac taking the lesser omentum and left gastric artery flush at, its origin., The lymph nodes should be removed en bloc with the specimen where possible.
Page 733 :
Place 2 stay sutures either side of the distal oesophagus. Ask the anaesthetist to pull back on the, nasogastric tube. Divide the distal oesophagus and remove the stomach., The oesphago jejunal anastomosis should be constructed. Identify the DJ flexure and bring a loop of, jejunum up to the oesophagus (to check it will reach). Divide the jejunum at this point. Bring the, divided jejunum either retrocolic or antecolic to the oesophagus. Anastamose the oesophagus to the, jejunum, using either interrupted 3/0 vicryl or a stapling device. Then create the remainder of the, Roux en Y reconstruction distally., Place a jejunostomy feeding tube., Wash out the abdomen and insert drains (usually the anastomosis and duodenal stump). Help the, anaesthetist insert the nasogastric tube (carefully!), Close the abdomen and skin., Enteral feeding may commence on the first post-operative day. However, most surgeons will leave, patients on free NG drainage for several days and keep them nil by mouth., Next question
Page 734 :
Question 167 of 347, Which of the following statements relating to Gardners syndrome variant of familial adenomatous, polyposis coli is false?, , It is an autosomal dominant condition, , Patients may develop retroperitoneal desmoid tumours, , The vast majority of the polyps are benign and thus the risk of colorectal cancer is small, , Patients are at increased risk of thyroid cancer, , It is characterised by a mutation in the APC gene, , The multiple polyps increase the risk of malignancy and most patients should undergo a colectomy., Please rate this question:, , Discuss and give feedback, , Next question, , Genetics and surgical disease, Some of the more commonly occurring genetic conditions occurring in surgical patients are, presented here., Li-Fraumeni Syndrome, , , , , , Autosomal dominant, Consists of germline mutations to p53 tumour suppressor gene, High incidence of malignancies particularly sarcomas and leukaemias, Diagnosed when:, , *Individual develops sarcoma under 45 years, *First degree relative diagnosed with any cancer below age 45 years and another family member, develops malignancy under 45 years or sarcoma at any age, BRCA 1 and 2
Page 735 :
, , , , Carried on chromosome 17 (BRCA 1) and Chromosome 13 (BRCA 2), Linked to developing breast cancer (60%) risk., Associated risk of developing ovarian cancer (55% with BRCA 1 and 25% with BRCA 2)., , Lynch Syndrome, , , , , , Autosomal dominant, Develop colonic cancer and endometrial cancer at young age, 80% of affected individuals will get colonic and/ or endometrial cancer, High risk individuals may be identified using the Amsterdam criteria, , Amsterdam criteria, Three or more family members with a confirmed diagnosis of colorectal cancer, one of whom is a, first degree (parent, child, sibling) relative of the other two., Two successive affected generations., One or more colon cancers diagnosed under age 50 years., Familial adenomatous polyposis (FAP) has been excluded., Gardners syndrome, , , , , , , , , Autosomal dominant familial colorectal polyposis, Multiple colonic polyps, Extra colonic diseases include: skull osteoma, thyroid cancer and epidermoid cysts, Desmoid tumours are seen in 15%, Mutation of APC gene located on chromosome 5, Due to colonic polyps most patients will undergo colectomy to reduce risk of colorectal, cancer, Now considered a variant of familial adenomatous polyposis coli, Next question
Page 736 :
Question 168 of 347, A 60-year-old man presents with lower urinary tract symptoms and is offered a PSA test. Which one, of the following could interfere with the PSA level?, , Vigorous exercise in the past 48 hours, , Poorly controlled diabetes mellitus, , Drinking more than 4 units of alcohol in the past 48 hours, , Smoking, , Recent cholecystectomy, , Please rate this question:, , Discuss and give feedback, , Next question, , PSA testing, Prostate specific antigen (PSA) is a serine protease enzyme produced by normal and malignant, prostate epithelial cells. It has become an important tumour marker but much controversy still exists, regarding its usefulness as a screening tool., The NHS Prostate Cancer Risk Management Programme (PCRMP) has published updated, guidelines in 2009 on how to handle requests for PSA testing in asymptomatic men. A recent, European trial (ERSPC) showed a statistically significant reduction in the rate of death prostate, cancer by 20% in men aged 55 to 69 years but this was associated with a high risk of over-diagnosis, and over-treatment. Having reviewed this and other data the National Screening Committee have, decided not to introduce a prostate cancer screening programme yet but rather allow men to make, an informed choice., Age-adjusted upper limits for PSA were recommended by the PCRMP*:, , {Age}, , {PSA level (ng/ml)}
Page 737 :
50-59 years, , 3.0, , 60-69 years, , 4.0, , > 70 years, , 5.0, , PSA levels may also be raised by**:, , , , , , , , benign prostatic hyperplasia (BPH), prostatitis and urinary tract infection (NICE recommend to postpone the PSA test for at least, 1 month after treatment), ejaculation (ideally not in the previous 48 hours), vigorous exercise (ideally not in the previous 48 hours), urinary retention, instrumentation of the urinary tract, , Poor specificity and sensitivity, , , , , around 33% of men with a PSA of 4-10 ng/ml will be found to have prostate cancer. With a, PSA of 10-20 ng/ml this rises to 60% of men, around 20% with prostate cancer have a normal PSA, various methods are used to try and add greater meaning to a PSA level including ageadjusted upper limits and monitoring change in PSA level with time (PSA velocity or PSA, doubling time), , *aide memoire for upper PSA limit: (age - 20) / 10, **whether digital rectal examination actually causes a rise in PSA levels is a matter of debate, Next question
Page 738 :
Question 169 of 347, Which of the symptoms below is least typical of pancreatic cancer?, , Painless jaundice, , Hyperamylasaemia, , Hyperglycaemia, , Weight loss, , Classical Courvoisier syndrome, , Raised serum amylase is relatively uncommon. The typical Courvoisier syndrome typically occurs in, 20% and hyperglycaemia occurs in 15-20%., Please rate this question:, , Discuss and give feedback, , Next question, , Pancreatic cancer, , , , , , , Adenocarcinoma, Risk factors: Smoking, diabetes, adenoma, familial adenomatous polyposis, Mainly occur in the head of the pancreas (70%), Spread locally and metastasizes to the liver, Carcinoma of the pancreas should be differentiated from other periampullary tumours with, better prognosis, , Clinical features, , , , , , , Weight loss, Painless jaundice, Epigastric discomfort (pain usually due to invasion of the coeliac plexus is a late feature), Pancreatitis, Trousseau's sign: migratory superficial thrombophlebitis
Page 739 :
Investigations, , , , , , , USS: May miss small lesions, CT Scanning (pancreatic protocol). If unresectable on CT then no further staging needed, PET/CT for those with operable disease on CT alone, ERCP/ MRI for bile duct assessment, Staging laparoscopy to exclude peritoneal disease, , Management, , , , , , , Head of pancreas: Whipple's resection (SE dumping and ulcers). Newer techniques include, pylorus preservation and SMA/ SMV resection, Carcinoma body and tail: poor prognosis, distal pancreatectomy, if operable, Usually adjuvent chemotherapy for resectable disease, ERCP and stent for jaundice and palliation, Surgical bypass may be needed for duodenal obstruction, , Next question
Page 740 :
Question 170 of 347, A 53 year old man presents with dyspepsia. An upper GI endoscopy is performed and Helicobacter, pylori is identified. A duodenal ulcer is present in the first part of the duodenum. Duodenal biopsies, are taken and demonstrate epithelium that resembles cells of the gastric antrum. Which of the, following is the most likely explanation for this process?, , Hyperplasia of the crypts of Lieberkhun, , Duodenal metaplasia, , Duodenal dysplasia, , Duodenal carcinoma, , Hyptertrophy of Brunners glands, Metaplasia = cell type conversion, Theme in January 2012 exam, The process involved is metaplasia. During metaplasia there is no direct carcinogenesis, however, the persistent presence of precipitants of metaplasia will lead to malignant changes in cells., Metaplastic changes in the duodenal cap are frequently seen in association with H-Pylori induced, ulcers. It typically resolves after ulcer healing and eradication therapy., Please rate this question:, , Discuss and give feedback, , Next question, , Metaplasia, , , , , , , Definition: reversible change of differentiated cells to another cell type., May represent an adaptive substitution of cells that are sensitive to stress by cell types better, able to withstand the adverse environment., Can be a normal physiological response (ossification of cartilage to form bone), Most common epithelial metaplasia occurs with transformation of columnar cells to, squamous cells (smoking causes ciliated columnar cells to be replaced by squamous, epithelial cells; Schistosomiasis)., Metaplasia from squamous to columnar cells occurs in Barrett oesophagus.
Page 741 :
, , , , If the metaplastic stimulus is removed, the cells will return to their original pattern of, differentiation. However, if the stimulus is not removed then progression to dysplasia may, occur., Not considered directly carcinogenic, however the factors which predispose to metaplasia, if, persistent may induce malignant transformation., The pathogenesis involves a reprogramming of stem cells that are known to exist in normal, tissues, or of undifferentiated mesenchymal cells present in connective tissue. In a, metaplastic change, these precursor cells differentiate along a new pathway., , Next question
Page 742 :
Question 171 of 347, A 22 year old lady presents with symptoms and signs of hyperthyroidism. Her diagnostic work up, results in a diagnosis of Graves disease. Which of the following best describes the pathophysiology, of the condition?, , Formation of IgG antibodies to the TSH receptors on the thyroid gland, , Formation of IgG antibodies to the TRH receptors on the anterior pituitary, , Formation of IgM antibodies to the TSH receptors on the thyroid gland, , Formation of IgA antibodies to the TSH receptors on the thyroid gland, , Formation of IgM antibodies to the TRH receptors on the anterior pituitary, , Usually IgG antibodies are formed against the TSH receptors on the thyroid gland. Which is why the, TSH level is often very low in Graves disease., Please rate this question:, , Discuss and give feedback, , Next question, , Thyroid hormones, Hormones of the thyroid gland, , Triiodothyronine T3, , Major hormone active in target cells, , Thyroxine T4, , Most prevalent form in plasma, less biologically active than T3, , Calcitonin, , Lowers plasma calcium, , Synthesis and secretion of thyroid hormones, , , Thyroid actively concentrates iodide to twenty five times the plasma concentration.
Page 743 :
, , , , , Iodide is oxidised by peroxidase in the follicular cells to atomic iodine which then iodinates, tyrosine residues contained in thyroglobulin., Iodinated tyrosine residues in thyroglobulin undergo coupling to either T3 or T4., Process is stimulated by TSH, which stimulates secretion of thyroid hormones., The normal thyroid has approximately 3 month reserves of thyroid hormones., , LATS and Graves disease, In Graves disease patients develop IgG antibodies to the TSH receptors on the thyroid gland. This, results in chronic and long term stimulation of the gland with release of thyroid hormones. The, typically situation is raised thyroid hormones and low TSH. Thyroid receptor autoantibodies should, be checked in individuals presenting with hyperthyroidism as they are present in up to 85% cases., Next question
Page 744 :
Question 172 of 347, What is the most common cause of hypercalcaemia in the UK in hospitalised patients?, , Thiazide use, , Metastatic malignancy, , Primary hyperparathyroidism, , Osteogenic sarcoma, , Sarcoidosis, , Metastatic cancer accounts for most cases of hypercalcaemia in hospitalised patients. In the, community primary hyperparathyroidism is the commonest cause., Please rate this question:, , Discuss and give feedback, , Next question, , Hypercalcaemia, Main causes, , , , Malignancy (most common cause in hospital in-patients), Primary hyperparathyroidism (commonest cause in non hospitalised patients), , Less common, , , , , , , , , , Sarcoidosis (extrarenal synthesis of calcitriol ), Thiazides, lithium, Immobilisation, Pagets disease, Vitamin A/D toxicity, Thyrotoxicosis, MEN, Milk alkali syndrome
Page 745 :
Clinical features, Stones, bones, abdominal groans, and psychic moans, High serum calcium levels result in decreased neuronal excitability. Therefore sluggish reflexes,, muscle weakness and constipation may occur., Next question
Page 746 :
Question 173-175 of 347, Theme: Diseases affecting the great vessels, , A., B., C., D., E., F., , Aortic coarctation, Cervical rib, Takayasu's arteritis, Subclavian steal syndrome, Patent ductus arteriosus, Aortic dissection, , Please select the most likely underlying cause for the symptoms described. Each option may be, used once, more than once or not at all., , 173., , A 24 year old lady from Western India presents with symptoms of lethargy and dizziness,, worse on turning her head. On examination her systolic blood pressure is 176/128. Her, pulses are impalpable at all peripheral sites. Auscultation of her chest reveals a systolic, heart murmur., You answered Aortic coarctation, The correct answer is Takayasu's arteritis, Takayasu's arteritis most commonly affects young Asian females. Pulseless peripheries, are a classical finding. The CNS symptoms may be variable., , 174., , A 48 year old man notices that he is becoming increasingly dizzy when he plays squash,, in addition he has also developed cramping pain in his left arm. One day he is inflating, his car tyre with a hand held pump, he collapses and is brought to hospital., You answered Aortic coarctation, The correct answer is Subclavian steal syndrome, Subclavian steal syndrome is associated with a stenosis or occlusion of the subclavian, artery, proximal to the origin of the vertebral artery. As a result the increased metabolic, needs of the arm then cause retrograde flow and symptoms of CNS vascular, insufficiency., , 175., , A 25 year old junior doctor has a chest x-ray performed as part of a routine insurance, medical examination. The x-ray shows evidence of rib notching. Auscultation of his chest, reveals a systolic murmur which is loudest at the posterior aspect of the fourth intercostal, space.
Page 747 :
Aortic coarctation, Coarctation of the aorta may occur due to the remnant of the ductus arteriosus acting as a, fibrous constrictive band of the aorta. Weak arm pulses may be seen, radiofemoral delay, is the classical physical finding. Collateral flow through the intercostal vessels may, produce notching of the ribs, if the disease is long standing., Please rate this question:, , Discuss and give feedback, , Next question, , Vascular disease, Aortic dissection, , , , , , , Chest pain (anterior chest pain- ascending aorta, back pain descending aorta), Widening of aorta on chest x-ray, Diagnosis made by CT scanning, Treatment is either medical (Type B disease) or surgical (Type A, disease), , Cervical rib, , , , , , , Supernumery fibrous band arising from seventh cervical vertebra, Incidence of 1 in 500, May cause thoracic outlet syndrome, Treatment involves surgical division of rib, , Subclavian steal, syndrome, , , , , Due to proximal stenotic lesion of the subclavian artery, Results in retrograte flow through vertebral or internal thoracic, arteries, The result is that decrease in cerebral blood flow may occur and, produce syncopal symptoms, A duplex scan and/ or angiogram will delineate the lesion and allow, treatment to be planned, , , , , Takayasu's, arteritis, , , , , , , Large vessel granulomatous vasculitis, Results in intimal narrowing, Most commonly affects young asian females, Patients present with features of mild systemic illness, followed by, pulseless phase with symptoms of vascular insufficiency
Page 748 :
Patent ductus, arteriosus, , , , Treatment is with systemic steroids, , , , Ductus arteriosus is a normal foetal vessel that closes spontaneously, after birth, Results in high pressure, oxygenated blood entering the pulmonary, circuit, Untreated patients develop symptoms of congestive cardiac failure, , , , , Coarctation of the, aorta, , , , , , , , Aortic stenosis at the site of the ductus arteriosus insertion, More prevalent in boys or females with Turners syndrome, Patients may present with symptoms of arterial insufficiency, such, as syncope and claudication, Blood pressure mismatch may be seen, as may mismatch of pulse, pressure in the upper and lower limbs, Treatment is either with angioplasty or surgical resection (the former, is the most common), Next question
Page 749 :
Question 176 of 347, A 25 year old man is found to have carcinoid syndrome. Which of the following hormones is released, by carcinoids?, , Serotonin, , Dopamine, , Nor adrenaline, , Adrenaline, , Aldosterone, Rule of thirds:, 1/3 multiple, 1/3 small bowel, 1/3 metastasize, 1/3 second tumour, Carcinoids secrete serotonin. Carcinoid syndrome will only occur in the presence of liver metastasis, as the hormone released from primary lesions will typically be metabolised by the liver., Please rate this question:, , Discuss and give feedback, , Next question, , Carcinoid syndrome, , , , , , Carcinoid tumours secrete serotonin, Originate in neuroendocrine cells mainly in the intestine (midgut-distal ileum/appendix), Can occur in the rectum, bronchi, Hormonal symptoms mainly occur when disease spreads outside the bowel, , Clinical features, , , Onset: insidious over many years
Page 750 :
, , , , , , Flushing face, Palpitations, Pulmonary valve stenosis and tricuspid regurgitation causing dyspnoea, Asthma, Severe diarrhoea (secretory, persists despite fasting), , Investigation, , , , , , 5-HIAA in a 24-hour urine collection, Somatostatin receptor scintigraphy, CT scan, Blood testing for chromogranin A, , Treatment, , , , Octreotide, Surgical removal, Next question
Page 751 :
Question 177 of 347, Which one of the following genes protects against neoplasms?, , sis, , p53, , ras, , myc, , src, , p53 is a tumour supressor gene and located on chromosome 17. It plays an important role in, causing cells that are undergoing neoplastic changes to enter an apoptotic pathway., Please rate this question:, , Discuss and give feedback, , Next question, , Oncogenes, Oncogenes are cancer promoting genes that are derived from normal genes (proto-oncogenes)., Proto-oncogenes play an important physiological role in cellular growth. They are implicated in the, development of up to 20% of human cancers., Proto-oncogenes may become oncogenes via the following processes:, , , , , Mutation (point mutation), Chromosomal translocation, Increased protein expression, , Only one mutated copy of the gene is needed for cancer to occur - a dominant effect, Classification of oncogenes, , , , Growth factors e.g. Sis, Transcription factors e.g. Myc
Page 752 :
, , , , Receptor tyrosine kinase e.g. RET, Cytoplasmic tyrosine kinase e.g. Src, Regulatory GTPases e.g. Ras, , Tumour suppressor genes, Tumour suppressor genes restrict or repress cellular proliferation in normal cells. Their inactivation, through mutation or germ line incorporation is implicated in renal, colonic, breast, bladder and many, other cancers. One of the best known tumour suppressor genes is p53. p53 gene offers protection, by causing apoptosis of damaged cells. Other well known genes include BRCA 1 and 2., Next question
Page 753 :
Question 178 of 347, A 55 year old man with a long history of achalasia is successfully treated by a Hellers, Cardiomyotomy. Several years later he develops an oesophageal malignancy. Which of the, following lesions is most likely to be present?, , Adenocarcinoma, , Gastrointestinal stromal tumour, , Leiomyosarcoma, , Rhabdomyosarcoma, , Squamous cell carcinoma, , Achalasia is a rare condition. However, even once treated there is an increased risk of malignancy., When it does occur it is most likely to be of squamous cell type., Please rate this question:, , Discuss and give feedback, , Next question, , Oesophageal cancer, , , , , , , Incidence is increasing, In most cases in the Western world this increase is accounted for by a rise in the number of, cases of adenocarcinoma. In the UK adenocarcinomas account for 65% of cases., Barretts oesophagus is a major risk factor for most cases of oesophageal adenocarcinoma., In other regions of the world squamous cancer is more common and is linked to smoking,, alcohol intake, diets rich in nitrosamines and achalasia., Surveillance of Barretts is important, as it imparts a 30 fold increase in cancer risk and if, invasive malignancy is diagnosed early then survival may approach 85% at 5 years., , Diagnosis, , , , Upper GI endoscopy is the first line test, Contrast swallow may be of benefit in classifying benign motility disorders but has no place, in the assessment of tumours
Page 754 :
, , , , Staging is initially undertaken with CT scanning of the chest, abdomen and pelvis. If overt, metastatic disease is identified using this modality then further complex imaging is, unnecessary, If CT does not show metastatic disease, then local stage may be more accurately assessed, by use of endoscopic ultrasound., Staging laparoscopy is performed to detect occult peritoneal disease. PET CT is performed, in those with negative laparoscopy. Thoracoscopy is not routinely performed., , Treatment, Operable disease is best managed by surgical resection. The most standard procedure is an IvorLewis type oesophagectomy. This procedure involves the mobilisation of the stomach and division of, the oesophageal hiatus. The abdomen is closed and a right sided thoracotomy performed. The, stomach is brought into the chest and the oesophagus mobilised further. An intrathoracic, oesophagogastric anastomosis is constructed. Alternative surgical strategies include a transhiatal, resection (for distal lesions), a left thoraco-abdominal resection (difficult access due to thoracic, aorta) and a total oesophagectomy (McKeown) with a cervical oesophagogastric anastomosis., The biggest surgical challenge is that of anastomotic leak, with an intrathoracic anastomosis this will, result in mediastinitis. With high mortality. The McKeown technique has an intrinsically lower, systemic insult in the event of anastomotic leakage., In addition to surgical resection many patients will be treated with adjuvant chemotherapy., Next question
Page 755 :
Question 179 of 347, Which of the following genes is not implicated in the adenoma-carcinoma sequence in colorectal, cancer?, , src, , c-myc, , APC, , p53, , K-ras, , Other genes involved are:, MCC, DCC, c-yes, bcl-2, Please rate this question:, , Discuss and give feedback, , Next question, , Colorectal cancer, , , , , , , , , Annually about 150,000 new cases are diagnosed and 50,000 deaths from the disease, About 75% will have sporadic disease and 25% will have a family history, Colorectal tumours comprise a spectrum of disease ranging from adenomas through to polyp, cancers and frank malignancy., Polyps may be categorised into: neoplastic polyps, adenomatous polyps and non neoplastic, polyps., The majority of adenomas are polypoidal lesions, although flat lesions do occur and may, prove to be dysplastic., Non-neoplastic polyps include hyperplastic, juvenile, hamartomatous, inflammatory, and, lymphoid polyps, which have not generally been thought of as precursors of cancer., Three characteristics of adenomas that correlate with malignant potential have been, characterised. These include increased size, villous architecture and dysplasia. For this, reason most polyps identified at colonoscopy should be removed.
Page 756 :
, , The transformation from polyp to cancer is described by the adenoma - carcinoma sequence, and its principles should be appreciated. Essentially genetic changes accompany the, transition from adenoma to carcinoma; key changes include APC, c-myc, K RAS mutations, and p53 deletions., Next question
Page 757 :
Question 180 of 347, A 63 year old lady is suspected as having sarcoidosis. She is sent to the general surgeons and a, lymph node biopsy is performed. Which histological feature is most likely to be identified in a lymph, node if sarcoid is present?, , Psammoma bodies, , Extensive necrosis, , Dense eosinophillic infiltrates, , Asteroid bodies, , None of the above, , Asteroid bodies are often found in the granulomas of individuals with sarcoid. Unlike the, granulomata associated with tuberculosis the granulomas of sarcoid are rarely associated with, extensive necrosis., An Asteroid body in an individual with sarcoid
Page 758 :
Image sourced from Wikipedia, , Please rate this question:, , Discuss and give feedback, , Next question, , Chronic inflammation, Overview, Chronic inflammation may occur secondary to acute inflammation.In most cases chronic, inflammation occurs as a primary process. These may be broadly viewed as being one of three main, processes:, , , , , Persisting infection with certain organisms such as Mycobacterium tuberculosis which results, in delayed type hypersensitivity reactions and inflammation., Prolonged exposure to non-biodegradable substances such as silica or suture materials, which may induce an inflammatory response., Autoimmune conditions involving antibodies formed against host antigens.
Page 759 :
Acute vs. Chronic inflammation, , Acute inflammation, , Chronic inflammation, , Changes to existing vascular structure and increased, permeability of endothelial cells, , Angiogenesis predominates, , Infiltration of neutrophils, , Macrophages, plasma cells and, lymphocytes predominate, , Process may resolve with:, , Healing by fibrosis is the main result, , , , , , , , Suppuration, Complete resolution, Abscess formation, Progression to chronic inflammation, Healing by fibrosis, , Granulomatous inflammation, A granuloma consists of a microscopic aggregation of macrophages (with epithelial type, arrangement =epitheliod). Large giant cells may be found at the periphery of granulomas., Mediators, Growth factors released by activated macrophages include agents such as interferon and fibroblast, growth factor (plus many more). Some of these such as interferons may have systemic features, resulting in systemic symptoms and signs, which may be present in individuals with long standing, chronic inflammation., The finding of granulomas is pathognomonic of chronic inflammation, as illustrated in this biopsy, from a patient with colonic Crohns disease
Page 760 :
Image sourced from Wikipedia, , Next question
Page 761 :
Question 181 of 347, Brown tumours of bone are associated with which of the following?, , Hyperthyroidism, , Hypothyroidism, , Hyperparathyroidism, , Hypoparathyroidism, , Osteopetrosis, , Brown tumors are tumors of bone that arise in settings of excess osteoclast activity, such as, hyperparathyroidism, and consist of fibrous tissue, woven bone and supporting vasculature, but no, matrix. They are radiolucent on x-ray. The osteoclasts consume the trabecular bone that osteoblasts, lay down and this front of reparative bone deposition followed by additional resorption can expand, beyond the usual shape of the bone, involving the periosteum thus causing bone pain. They appear, brown because haemosiderin is deposited at the site., Please rate this question:, , Discuss and give feedback, , Next question, , Primary hyperparathyroidism, In exams, primary hyperparathyroidism is stereotypically seen in elderly females with an, unquenchable thirst and an inappropriately normal or raised parathyroid hormone level. It is most, commonly due to a solitary adenoma, Causes of primary hyperparathyroidism, , , , , , 80%: solitary adenoma, 15%: hyperplasia, 4%: multiple adenoma, 1%: carcinoma
Page 762 :
Features - 'bones, stones, abdominal groans and psychic moans', , , , , , , , Polydipsia, polyuria, Peptic ulceration/constipation/pancreatitis, Bone pain/fracture, Renal stones, Depression, Hypertension, , Associations, , , , Hypertension, Multiple endocrine neoplasia: MEN I and II, , Investigations, , , , , Raised calcium, low phosphate, PTH may be raised or normal, Technetium-MIBI subtraction scan, , Treatment, , , Parathyroidectomy, if imaging suggests target gland then a focused approach may be used, Next question
Page 763 :
Question 182 of 347, , A 73 year old man is recovering following an emergency Hartmans procedure performed for an, obstructing sigmoid cancer. The pathology report shows a moderately differentiated, adenocarcinoma that invades the muscularis propria, 3 of 15 lymph nodes are involved with, metastatic disease. What is the correct stage for this?, , Astler Coller Stage B2, , Dukes stage A, , Dukes stage B, , Dukes stage C, , Dukes stage D, Remember that the term metastasis simply refers to spread and can include the lymph nodes. In an, examination setting marks can be lost by incorrectly selecting Dukes D (which would be consistent, with liver metastasis) rather than nodal metastasis (Dukes C)., , Theme from September 2011 Exam, The involvement of lymph nodes makes this Dukes C. In the Astler Coller system the B and C, subsets are split to B1 and B2 and C1 and C2. Where C2 denotes involvement of the nodes in, conjunction with penetration of the muscularis propria., Please rate this question:, , Discuss and give feedback, , Next question, , Dukes classification
Page 764 :
Gives the extent of spread of colorectal cancer, , Dukes A, , Tumour confined to the mucosa (95%), , Dukes B, , Tumour invading bowel wall (80%), , Dukes C, , Lymph node metastases (60%), , Dukes D, , Distant metastases (6%)(25% if resectable), , 5 year survival in brackets, Next question
Page 765 :
Question 183 of 347, A 55 year old man presents with a soft, fluctuant lesion overlying his right scapula. The surgeon, suspects the lesion may be a lipoma. Which of the following, if present, may be indicative of an, alternative diagnosis?, , Located in superficial tissues, , Size greater than 5cm, , Presence of multiple similar lesions at other anatomical sites, , Increased mobility of the lesion, , Lobulated appearance during surgical excision
Page 766 :
Question 184 of 347, A 55 year old man with dyspepsia undergoes an upper GI endoscopy. An irregular erythematous, area is seen to protrude proximally from the gastro-oesophageal junction. Apart from specialised, intestinal metaplasia, which of the following cell types should also be present for a diagnosis of, Barretts oesophagus to be made?, , Goblet cell, , Neutrophil, , Lymphocytes, , Epithelial cells, , Macrophages, , Goblet cells need to be present for a diagnosis of Barrett's oesophagus to be made., Please rate this question:, , Discuss and give feedback, , Next question, , Barrett's oesophagus, Barretts oesophagus is a condition characterised by the metaplastic transformation of squamous, oesophageal epithelium to columnar gastric type epithelium. Three types of this metaplastic process, are recognised; intestinal (high risk), cardiac and fundic. The latter two categories may cause, difficulties in diagnosis. The most concrete diagnosis can be made when endoscopic features of, Barretts oesophagus are present together with a deep biopsy that demonstrates not just goblet cell, metaplasia but also oesophageal glands., Barrett's can be sub divided into short (<3cm) and long (>3cm). The length of the affected segment, correlates strongly with the chances of identifying metaplasia. The overall prevalence of Barrett's, oesophagus is difficult to determine but may be in the region of 1 in 20 and is identified in up to 12%, of those undergoing endoscopy for reflux., A proportion of patients with metaplasia will progress to dysplasia and for this reason individuals, identified as having Barrett's should undergo endoscopic surveillance (every 2-5 years). Biopsies, should be quadrantic and taken at 1-2cm intervals. Biopsies need to be adequate. Where mass, lesions are present consideration should be given to endoscopic sub mucosal resection. Up to 40%
Page 767 :
of patients will be upstaged from high grade dysplasia to invasive malignancy with such techniques., Treatment, , , , , , Long term proton pump inhibitor, Consider pH and manometry studies in younger patients who may prefer to consider an anti, reflux procedure, Regular endoscopic monitoring (more frequently if moderate dysplasia). With quadrantic, biopsies every 2-3 cm, If severe dysplasia be very wary of small foci of cancer, , References, A consensus statement of the British approach is provided by:, Bennett C et al Consensus Statements for Management of Barrett's Dysplasia and Early-Stage, Esophageal Adenocarcinoma, Based on a Delphi Process. Gastroenterology Volume 143, Issue 2 ,, Pages 336-346, August 2012., Next question
Page 768 :
Question 185 of 347, Which of the following amino acids is present in all types of collagen?, , Alanine, , Aspartime, , Glycine, , Tyrosine, , Cysteine, , Collagen has a generic structure of Glycine- X- Y, where X and Y are variable sub units. The, relatively small size of the glycine molecule enables collagen to form a tight helical structure., Please rate this question:, , Discuss and give feedback, , Next question, , Collagen, Collagen is one of the most important structural proteins within the extracellular matrix, collagen, together with components such as elastin and glycosaminoglycans determine the properties of all, tissues., , , , , , , Composed of 3 polypeptide strands that are woven into a helix, usually a combination of, glycine with either proline or hydroxyproline plus another amino acid, Numerous hydrogen bonds exist within molecule to provide additional strength, Many sub types but commonest sub type is I (90% of bodily collagen), tissues with increased, levels of flexibility have increased levels of type III collagen, Vitamin c is important in establishing cross links, Synthesised by fibroblasts, , Collagen Diseases, Disorders of collagen range from relatively common, acquired defects (typically aging), through to, rarer congenital disorders. The latter are exemplified by conditions such as osteogenesis imperfecta, and Ehlers Danlos syndromes.
Page 769 :
Osteogenesis imperfecta:, -8 Subtypes, -Defect of type I collagen, -In type I the collagen is normal quality but insufficient quantity, -Type II- poor quantity and quality, -Type III- Collagen poorly formed, normal quantity, -Type IV- Sufficient quantity but poor quality, Patients have bones which fracture easily, loose joint and multiple other defects depending upon, which sub type they suffer from., Ehlers Danlos:, -Multiple sub types, -Abnormality of types 1 and 3 collagen, -Patients have features of hypermobility., -Individuals are prone to joint dislocations and pelvic organ prolapse. In addition to many other, diseases related to connective tissue defects., Next question
Page 770 :
Question 186 of 347, An 8 year old boy presented with a painless swelling on the superotemporal aspect of his orbit. It, was smooth on examination, produced no visual disturbances. Following excision it was found to be, lined by squamous epithelium and hair follicles. Which of the following lesions most closely matches, these findings?, , Dermoid cyst, , Desmoid tumour, , Lipoma, , Sebaceous cyst, , Schwannoma, , Dermoid cysts are embryological remnants and may be lined by hair and squamous epithelium (like, teratomas). They are often located in the midline and may be linked to deeper structures resulting in, a dumbbell shape to the lesion. Complete excision is required as they have a propensity to local, recurrence if not excised., Desmoid tumours are a different entity, they most commonly develop in ligaments and tendons., They are also referred to as aggressive fibromatosis and consist of fibroblast dense lesions, (resembling scar tissue). They should be managed in a similar manner to soft tissue sarcomas., Please rate this question:, , Discuss and give feedback, , Next question, , Skin Diseases, Skin lesions may be referred for surgical assessment, but more commonly will come via a, dermatologist for definitive surgical management., Skin malignancies include basal cell carcinoma, squamous cell carcinoma and malignant melanoma., Basal Cell Carcinoma, , , , Most common form of skin cancer., Commonly occur on sun exposed sites apart from the ear.
Page 771 :
, , , , , Sub types include nodular, morphoeic, superficial and pigmented., Typically slow growing with low metastatic potential., Standard surgical excision, topical chemotherapy and radiotherapy are all successful., As a minimum a diagnostic punch biopsy should be taken if treatment other than standard, surgical excision is planned., , Squamous Cell Carcinoma, , , , , , , Again related to sun exposure., May arise in pre - existing solar keratoses., May metastasize if left., Immunosupression (e.g. following transplant), increases risk., Wide local excision is the treatment of choice and where a diagnostic excision biopsy has, demonstrated SCC, repeat surgery to gain adequate margins may be required., , Malignant Melanoma, , The main diagnostic features (major criteria):, , , , , Secondary features (minor criteria), , , , , , Change in size, Change in shape, Change in colour, , Diameter >6mm, Inflammation, Oozing or bleeding, Altered sensation, , Treatment, , , , Suspicious lesions should undergo excision biopsy. The lesion should be removed in, completely as incision biopsy can make subsequent histopathological assessment difficult., Once the diagnosis is confirmed the pathology report should be reviewed to determine, whether further re-excision of margins is required (see below):, , Margins of excision-Related to Breslow thickness, , Lesions 0-1mm thick, , 1cm, , Lesions 1-2mm thick, , 1- 2cm (Depending upon site and pathological features), , Lesions 2-4mm thick, , 2-3 cm (Depending upon site and pathological features)
Page 772 :
Lesions >4 mm thick, , 3cm, , Marsden J et al. Revised UK guidelines for management of Melanoma. Br J Dermatol 2010 163:238256., Further treatments such as sentinel lymph node mapping, isolated limb perfusion and block, dissection of regional lymph node groups should be selectively applied., Kaposi Sarcoma, , , , , , , Tumour of vascular and lymphatic endothelium., Purple cutaneous nodules., Associated with immuno supression., Classical form affects elderly males and is slow growing., Immunosupression form is much more aggressive and tends to affect those with HIV related, disease., , Non malignant skin disease, Dermatitis Herpetiformis, , , , Chronic itchy clusters of blisters., Linked to underlying gluten enteropathy (coeliac disease)., , Dermatofibroma, , , , , , Benign lesion., Firm elevated nodules., Usually history of trauma., Lesion consists of histiocytes, blood vessels and fibrotic changes., , Pyogenic granuloma, , , , , , Overgrowth of blood vessels., Red nodules., Usually follow trauma., May mimic amelanotic melanoma., , Acanthosis nigricans, , , Brown to black, poorly defined, velvety hyperpigmentation of the skin.
Page 773 :
, , , , Usually found in body folds such as the posterior and lateral folds of the neck, the axilla,, groin, umbilicus, forehead, and other areas., The most common cause of acanthosis nigricans is insulin resistance, which leads to, increased circulating insulin levels. Insulin spillover into the skin results in its abnormal, increase in growth (hyperplasia of the skin)., In the context of a malignant disease, acanthosis nigricans is a paraneoplastic syndrome and, is then commonly referred to as acanthosis nigricans maligna. Involvement of mucous, membranes is rare and suggests a coexisting malignant condition., Next question
Page 774 :
Question 187 of 347, A 55 year old man from Hong Kong presents with left sided otalgia and recurrent episodes of, epistaxis. On examination his pharynx appears normal. Examination of his neck reveals left sided, cervical lymphadenopathy. What is the most likely underlying diagnosis?, , Antrochoanal polyp, , Nasopharyngeal carcinoma, , Adenocarcinoma of the tonsil, , Angiofibroma, , Globus syndrome, , Given this mans ethnic origin and presenting features a nasopharyngeal carcinoma is the most likely, underlying diagnosis., Please rate this question:, , Discuss and give feedback, , Next question, , Nasopharyngeal carcinoma, , , , , Squamous cell carcinoma of the nasopharynx, Rare in most parts of the world, apart from individuals from Southern China, Associated with Epstein Barr virus infection, , Presenting features, , Systemic, , Local, , Cervical lymphadenopathy, , Otalgia, , Unilateral serous otitis media
Page 775 :
Nasal obstruction, discharge and/ or epistaxis, , Cranial nerve palsies e.g. III-VI, , Imaging, Combined CT and MRI., Treatment, Radiotherapy is first line therapy., Next question
Page 776 :
Question 188 of 347, A women is diagnosed as having pernicious anaemia. What is the most likely underlying explanation, for this?, , Autoimmune antibodies to parietal cells, , Autoimmune antibodies to chief cells, , Autoimmune antibodies to goblet cells, , Autoimmune antibodies to Brunners glands, , Autimmune antibodies to fundic cells, , Parietal cell destruction is a major cause of pernicious anaemia and is usually autoimmune, mediated. Other conditions such as bacterial overgrowth may produce mixed patterns and require, more complex diagnostic evaluation., Please rate this question:, , Discuss and give feedback, , Next question, , Pernicious anaemia, , , , , , , , Pernicious anaemia is a chronic illness caused by impaired absorption of vitamin B-12, because of a lack of intrinsic factor (IF) in gastric secretions. It occurs as a relatively common, adult form of anaemia that is associated with gastric atrophy and a loss of IF production and, as a rare congenital autosomal recessive form in which IF production is lacking without, gastric atrophy., Classic pernicious anaemia is caused by the failure of gastric parietal cells to produce, sufficient IF (a gastric protein secreted by parietal cells) to permit the absorption of adequate, quantities of dietary vitamin B-12. Other disorders that interfere with the absorption and, metabolism of vitamin B-12 can produce cobalamin deficiency, with the development of a, macrocytic anaemia and neurologic complications. In many cases the underlying cause is, autoimmune destruction of the parietal cell mass of the gastric antrum., Diagnostic evaluation may include investigations to delineate the precise cause and this may, include Schilling test, trials of B12 and in some cases bone marrow sampling., Treatment of the disorder is with 3 monthly treatment of vitamin B12 injections. Folic acid, supplementation may also be required.
Page 777 :
Question 189 of 347, Patients with suspected temporal arteritis are often sent for temporal artery biopsy. Which statement, is true?, , Temporal artery biopsy is only diagnostic if there is visual loss, , Biopsy is typically taken from the non-symptomatic side to avoid the risk of blindness, , Pre-operative localisation with duplex is mandatory, , Biopsies may be non diagnostic in over 50% of cases, , Biopsies are usually performed under general anaesthesia, , Temporal artery biopsies are frequently non diagnostic. They should be taken from the symptomatic, side and though not mandatory a duplex ultrasound is a helpful investigation, particularly if they mark, the artery. It is usually performed under local anaesthetic., Please rate this question:, , Discuss and give feedback, , Next question, , Temporal artery biopsy, , , Superficial temporal artery is a terminal branch of the external carotid artery, , Main indication, , , Temporal arteritis, , American College of Rheumatology guidelines recommend a temporal artery biopsy if:, , , , , , Age of onset older than 50 years, New-onset headache or localized head pain, Temporal artery tenderness to palpation or reduced pulsation
Page 778 :
, , ESR > 50 mm/h, , Histopathology, , , Vessel wall granulomatous arteritis with mononuclear cell infiltrates and giant cell formation, , Procedure, , , , , , , , , , Position: supine, head 45 degrees, USS doppler to locate the superficial temporal artery or palpate, Local anaesthetic, Artery within temporoparietal fascia, Clamp and ligate the vessel, Cut 3-5cm, Ligate the remaining ends with absorbable suture, Close the skin, , Contraindication, Glucocorticoid therapy > 30 days, Risks, Injury to facial or auriculotemporal nerve, Next question
Page 779 :
Question 190 of 347, , Which of the following best describes the processes underpinning type IV hypersensitivity reactions?, , Deposition of immune complexes of IgG and antigen at the site of inflammation, , Deposition of IgA complexes at the site of inflammation, , Deposition of IgM and IgG complexes at the site of inflammation, , Degranulation of mast cells at the site of inflammation, , T cell mediated response at the site of inflammation, Hypersensitivity reactions: ACID, type 1 --Anaphylactic, type 2 --Cytotoxic, type 3 --Immune complex, type 4 --Delayed hypersensitivity, , T Cells are the mediators of type 4 hypersensitivity reactions which are characterised by the, absence of immune complex deposition., Please rate this question:, , Discuss and give feedback, , Next question, , Hypersensitivity reactions, The Gell and Coombs classification divides hypersensitivity reactions into 4 types
Page 781 :
Question 191-193 of 347, Theme: Bone tumours, , A., B., C., D., E., F., G., H., I., , Osteosarcoma, Fibrosarcoma, Osteoclastoma, Ewings sarcoma, Leiomyosarcoma, Chondrosarcoma, Rhabdomyosarcoma, Osteoid osteoma, Malignant fibrous histiocytoma, , Please select the most appropriate lesion for the clinical scenario given. Each option may be used, once, more than once or not at all., , 191., , A 16 year-old boy presents to his GP with loss of weight, pain and fever. On, examination, a soft tissue mass is palpable over the mid-thigh region, You answered Osteosarcoma, The correct answer is Ewings sarcoma, Ewing's sarcoma is a malignant round cell tumour occurring in the diaphysis of the long, bones in the children. These are not confined to the ends of long bones. x Rays often, show a large soft-tissue mass with concentric layers of new bone formation ( 'onion-peel', sign). The ESR may be elevated, thus suggesting an inflammatory or an infective cause, such as osteomyelitis; although osteomyelitis usually affects the metaphyseal region in, children. Treatment is with chemotherapy and surgical excision, an endoprothesis may be, used to conserve the limb., , 192., , A 75 year old lady presents with weight loss, pain and a swelling over her left knee. She, has been treated for Pagets disease of the bone for some time., Osteosarcoma, Osteosarcoma may complicate Pagets disease of bone in up to 10% cases. Radiological, appearances include bone destruction coupled with new bone formation, periosteal, elevation may also occur. Surgical resection is the main treatment., , 193., , A 17-year-old girl presents with weight loss, fever and a swelling over her right knee., Movements of her knee are restricted. A plain x-ray of the affected site shows multiple
Page 782 :
lytic and lucent lesions with clearly defined borders., You answered Osteosarcoma, The correct answer is Osteoclastoma, Osteoclastoma has a characteristic appearance on x-ray with multple lytic and lucent, areas (Soap bubble) appearances. Pathological fractures may occur. The disease is, usually indolent., Please rate this question:, , Discuss and give feedback, , Next question, , Sarcomas, , , Malignant tumours of mesenchymal origin, , Types, May be either bone or soft tissue in origin., Bone sarcoma include:, , , , , Osteosarcoma, Ewings sarcoma (although non bony sites recognised), Chondrosarcoma - originate from Chondrocytes, , Soft tissue sarcoma are a far more heterogeneous group and include:, , , , , , Liposarcoma-adipocytes, Rhabdomyosarcoma-striated muscle, Leiomyosarcoma-smooth muscle, Synovial sarcomas- close to joints (cell of origin not known but not synovium), , Malignant fibrous histiocytoma is a sarcoma that may arise in both soft tissue and bone., Features, Certain features of a mass or swelling should raise suspicion for a sarcoma these include:, , , , Large >5cm soft tissue mass, Deep tissue location or intra muscular location
Page 783 :
, , , Rapid growth, Painful lump, , Assessment, Imaging of suspicious masses should utilise a combination of MRI, CT and USS. Blind biopsy should, not be performed prior to imaging and where required should be done in such a way that the biopsy, tract can be subsequently included in any resection., Ewings sarcoma, , , , , , , , Commoner in males, Incidence of 0.3 / 1, 000, 000, Onset typically between 10 and 20 years of age, Location by femoral diaphysis is commonest site, Histologically it is a small round tumour, Blood borne metastasis is common and chemotherapy is often combined with surgery, , Osteosarcoma, , , , , , , Mesenchymal cells with osteoblastic differentiation, 20% of all primary bone tumours, Incidence of 5 per 1,000,000, Peak age 15-30, commoner in males, Limb preserving surgery may be possible and many patients will receive chemotherapy, , Liposarcoma, , , , , , , , , Malignancy of adipocytes, Rare, approximately 2.5 per 1,000,000. They are the second most common soft tissue, sarcoma, Typically located in deep locations such as retroperitoneum, Affect older age group usually >40 years of age, May be well differentiated and thus slow growing although may undergo de-differentiation, and disease progression, Many tumours will have a pseudocapsule that can misleadingly allow surgeons to feel that, they can 'shell out' these lesions. In reality, tumour may invade at the edge of the, pseudocapsule and result in local recurrence if this strategy is adopted, Usually resistant to radiotherapy, although this is often used in a palliative setting, , Malignant Fibrous Histiocytoma, , , , Tumour with large number of histiocytes, Most common sarcoma in adults
Page 784 :
, , , , Also described as undifferentiated pleomorphic sarcoma NOS (i.e. Cell of origin is not, known), Four major subtypes are recognised: storiform-pleomorphic (70% cases), myxoid (less, aggressive), giant cell and inflammatory, Treatment is usually with surgical resection and adjuvant radiotherapy as this reduces the, likelihood of local recurrence, Next question
Page 785 :
Question 194 of 347, A 56 year old man is diagnosed with an abdominal aortic aneurysm and undergoes a CT scan to, asses the size of the aorta. During the course of his investigations a lesion of the adrenal gland is, identified. It measures 1.5 cm in diameter and the gland is otherwise normal. What is the most likely, diagnosis?, , Adrenal gland metastasis, , Adrenal gland arterio-venous malformation, , Adrenal cyst, , Phaeochromocytoma, , Adrenal cortical adenoma, 25% of all adrenal lesions >4cm in diameter are malignant, Theme from 2011 Exam, Incidentalomas of the adrenal gland are common and represent the most likely lesion in this, scenario. Clearly the other lesions are all possibilities but are unlikely., Please rate this question:, , Discuss and give feedback, , Next question, , Adrenal lesions- Incidental, Incidentaloma of the adrenal glands have become increasingly common as CT scanning of the, abdomen is widely undertaken. Prevalences range from 1.5-9% in autopsy studies. Overall, 75% will, be non functioning adenomas. However, a thorough diagnostic work up is required to exclude a, more significant lesion., Investigation, , , , , , Morning and midnight plasma cortisol measurements, Dexamethasone suppression test, 24 hour urinary cortisol excretion, 24 hour urinary excretion of catecholamines
Page 786 :
, , Serum potassium, aldosterone and renin levels, , Management, The risk of malignancy is related to the size of the lesion and 25% of all masses greater than 4cm, will be malignant. Such lesions should usually be excised. Where a lesion is a suspected metastatic, deposit a biopsy may be considered. Smaller, innocent lesions are usually followed up by serial CT, scans at 6, 12 and 24 months., Next question
Page 787 :
Question 195 of 347, A 22 year old man is undergoing an abdominal ultrasound scan as part of a series of investigations, for abdominal pain. The radiologist notes that there is evidence of splenic atrophy. What is the most, likely cause?, , Letterer-Siwe disease, , Coeliac disease, , Malaria, , Niemann-Pick disease, , Sarcoidosis, , Splenic atrophy may occur in coeliac disease together with the appearance of Howell-Jolly bodies in, erythrocytes. Letterer - Siwe disease is a form of Histiocytosis X in which macrophages proliferate., Please rate this question:, , Discuss and give feedback, , Next question, , Spleen, The spleen is located in the left upper quadrant of the abdomen and its size can vary depending, upon the amount of blood it contains. The typical adult spleen is 12.5cm long and 7.5cm wide. The, usual weight of the adult spleen is 150g., The exact position of the spleen can vary with respiratory activity, posture and the state of, surrounding viscera. It usually lies obliquely with its long axis aligned to the 9th, 10th and 11th ribs. It, is separated from these ribs by both diaphragm and pleural cavity. The normal spleen is not, palpable., The shape of the spleen is influenced by the state of the colon and stomach. Gastric distension will, cause the spleen to resemble the shape of an orange segment. Colonic distension will cause it to, become more tetrahedral., The spleen is almost entirely covered by peritoneum, which adheres firmly to its capsule. Recesses, of the greater sac separate it from the stomach and kidney. It develops from the upper dorsal, mesogastrium, remaining connected to the posterior abdominal wall and stomach by two folds of, peritoneum; the lienorenal ligament and gastrosplenic ligament. The lienorenal ligament is derived
Page 788 :
from peritoneum where the wall of the general peritoneum meets the omental bursa between the left, kidney and spleen; the splenic vessels lie in its layers. The gastrosplenic ligament also has two, layers, formed by the meeting of the walls of the greater sac and omental bursa between spleen and, stomach, the short gastric and left gastroepiploic branches of the splenic artery pass in its layers., Laterally, the spleen is in contact with the phrenicocolic ligament., Relations, Superiorly, , Diaphragm, , Anteriorly, , Gastric impression, , Posteriorly, , Kidney, , Inferiorly, , Colon, , Hilum, , Tail of pancreas and splenic vessels (splenic artery divides here, branches pass to the, white pulp transporting plasma), , Contents, White, pulp, , Immune function. Contains central trabecular artery. The germinal centres are supplied, by arterioles called penicilliary radicles., , Red pulp, , Filters abnormal red blood cells., , Function, , , , , , , , Filtration of abnormal blood cells and foreign bodies such as bacteria., Immunity: IgM. Production of properdin, and tuftsin which help target fungi and bacteria for, phagocytosis., Haematopoiesis: up to 5th month gestation or in haematological disorders., Pooling: storage of 40% platelets., Iron reutilisation, Storage monocytes, , Disorders of the spleen, Massive splenomegaly, , , , , , , Myelofibrosis, Chronic myeloid leukaemia, Visceral leishmaniasis (kala-azar), Malaria, Gaucher's syndrome, , Other causes (as above plus)
Page 789 :
, , , , , , , , Portal hypertension e.g. secondary to cirrhosis, Lymphoproliferative disease e.g. CLL, Hodgkin's, Haemolytic anaemia, Infection: hepatitis, glandular fever, Infective endocarditis, Sickle-cell*, thalassaemia, Rheumatoid arthritis (Felty's syndrome), , *the majority of adult patients with sickle-cell will have an atrophied spleen due to repeated infarction, Next question
Page 790 :
Question 196 of 347, A patient undergoes excision of a lump and the pathologist then examines a histological section and, identifies a clump of Reed Sternberg cells. What is the most likely diagnosis?, , Thymoma, , Papillary carcinoma of the thyroid, , Hodgkins lymphoma, , Kaposi sarcoma, , Carcinoma of the parathyroid gland, Reed Sternberg cells are diagnostic of Hodgkins lymphoma, Please rate this question:, , Discuss and give feedback, , Next question, , Hodgkins lymphoma, Presenting features, , , , , Asymptomatic lympadenopathy, Cough, Pel Ebstein fever, haemoptysis, dyspnoea, B Symptoms - 10% weight loss, fever, night sweats, , Staging, All patients are staged with CT scanning of the chest, abdomen and pelvis, The Ann Arbor staging system is commonly used, , Stage, , Features
Page 791 :
Stage, , Features, , I, , Single lymph node region, , II, , Two or more regions on the same side of the diaphragm, , III, , Involvement of lymph node regions on both sides of the diaphragm, , IV, , Involvement of extra nodal sites, , Sub types, Classical Hodgkin lymphoma is classified into the following 4 types:, Nodular sclerosing Hodgkin lymphoma (NSHL), Mixed-cellularity Hodgkin lymphoma (MCHL), Lymphocyte-depleted Hodgkin lymphoma (LDHL), Lymphocyte-rich classical Hodgkin lymphoma (LRHL), A Reed Sternberg cell may be identified histologically., A fifth sub type, Nodular lymphocyte-predominant Hodgkin lymphoma, is characterised by a different, cell type Reed- Sternberg cells are rarely seen., Treatment, This may be multimodal and both chemo and radiotherapy are used., Diagnosis, This is made by excision of a complete lymph node that is then submitted for detailed histological, evaluation., Pathogenesis, Infection with Ebstein Barr virus is linked to the condition (particularly mixed cellularity lymphoma)., Prognosis, Stage I disease is associated with survival figures of up to 85% at 5 years. The lymphocyte rich, classical lymphoma has the best prognosis. Lymphocyte depleted Hodgkins lymphoma, advancing, age, male sex and stage IV disease are all associated with a worsening of prognosis., Next question
Page 792 :
Question 197 of 347, Which statement relating to phaeochromocytoma is untrue?, , They are tumours of chromaffin cells in the adrenal medulla., , They are bilateral in 10% of cases., , When located in an extra adrenal location have a higher incidence of malignancy., , May be associated with an elevated urinary VMA., , Up to 40% may have a blood pressure within the normal range., , Normotension is seen in around 10% cases. The remainder show a degree of hypertension., Please rate this question:, , Discuss and give feedback, , Next question, , Phaeochromocytoma and adrenal lesions, Phaeochromocytoma, Neuroendocrine tumour of the chromaffin cells of the adrenal medulla. Hypertension and, hyperglycaemia are often found., , , , , , 10% of cases are bilateral., 10% occur in children., 11% are malignant (higher when tumour is located outside the adrenal)., 10% will not be hypertensive., , Familial cases are usually linked to the Multiple endocrine neoplasia syndromes (considered under, its own heading)., Most tumours are unilateral (often right sided) and smaller than 10cm., Diagnosis, Urine analysis of vanillymandelic acid (VMA) is often used (false positives may occur e.g. in patients, eating vanilla ice cream!)
Page 793 :
Blood testing for plasma metanephrine levels., CT and MRI scanning are both used to localise the lesion., Treatment, Patients require medical therapy first. An irreversible alpha adrenoreceptor blocker should be given,, although minority may prefer reversible blockade(1). Labetolol may be co-administered for cardiac, chronotropic control. Isolated beta blockade should not be considered as it will lead to unopposed, alpha activity., These patients are often volume depleted and will often require moderate volumes of intra venous, normal saline perioperatively., Once medically optimised the phaeochromocytoma should be removed. Most adrenalectomies can, now be performed using a laparoscopic approach(2). The adrenals are highly vascular structures, and removal can be complicated by catastrophic haemorrhage in the hands of the inexperienced., This is particularly true of right sided resections where the IVC is perilously close. Should the IVC be, damaged a laparotomy will be necessary and the defect enclosed within a Satinsky style vascular, clamp and the defect closed with prolene sutures. Attempting to interfere with the IVC using any, instruments other than vascular clamps will result in vessel trauma and make a bad situation much, worse., Incidental adrenal lesions, Adrenal lesions may be identified on CT scanning performed for other reasons(3). Factors, suggesting benign disease on CT include(4):, , , , , , Size less than 3cm, Homogeneous texture, Lipid rich tissue, Thin wall to lesion, , All patients with incidental lesions should be managed jointly with an endocrinologist and full work up, as described above. Patients with functioning lesions or those with adverse radiological features, (Particularly size >3cm) should proceed to surgery., References, 1. Weingarten TN, Cata JP, O'Hara JF, Prybilla DJ, Pike TL, Thompson GB, et al. Comparison of, two preoperative medical management strategies for laparoscopic resection of pheochromocytoma., Urology. 2010 Aug;76(2):508 e6-11., 2. Nguyen PH, Keller JE, Novitsky YW, Heniford BT, Kercher KW. Laparoscopic approach to, adrenalectomy: review of perioperative outcomes in a single center. Am Surg. 2011 May;77(5):5926., 3. Ng VW, Ma RC, So WY, Choi KC, Kong AP, Cockram CS, et al. Evaluation of functional and, malignant adrenal incidentalomas. Arch Intern Med. 2010 Dec 13;170(22):2017-20., 4. Muth A, Hammarstedt L, Hellstrom M, Sigurjonsdottir HA, Almqvist E, Wangberg B. Cohort study, of patients with adrenal lesions discovered incidentally. Br J Surg. 2011 May 27.
Page 794 :
Question 198 of 347, A 69 year old man presents with a purple lesion on his forearm. It is excised and an a 3 cm Merkel, cell tumour is diagnosed. Which of the following statements relating to this diagnosis is false?, , He should undergo a sentinel lymph node biopsy., , Lymphovascular invasion is typically seen histologically, , They are more common in immunosupressed patients, , Histologically they may resemble pyogenic granuloma, , They are associated with visceral metastasis, , Merkel cell tumours are rare cutaneous tumours. Histologically they consist of sheets and nodules of, hyperchromatic epithelial cells, with high rates of mitosis and apoptosis. As such they are relatively, easy to distinguish from pyogenic granuloma which has no features of malignancy and would not, show lymphovascular invasion., Please rate this question:, , Discuss and give feedback, , Next question, , Merkel cell tumours of the skin, , , , , , , Rare but aggressive tumour., Develops from intra epidermal Merkel cells., Usually presents on elderly, sun damaged skin. The periorbital area is the commonest site., Histologically these tumours appear within the dermis and subcutis. The lesions consist of, sheets and nodules of small hyperchromatic epithelial cells with high rates of mitosis and, apoptosis. Lymphovascular invasion is commonly seen., Pre-existing infection with Merkel Cell Polyomavirus is seen in 80% cases., , Treatment, Surgical excision is first line. Margins of 1cm are required. Lesions >10mm in diameter should, undergo sentinel lymph node biopsy. Adjuvant radiotherapy is often given to reduce the risk of local, recurrence.
Page 795 :
Prognosis, , , , With lymph node metastasis 5 year survival is 50% or less., Small lesions without nodal spread are usually associated with a 5 year survival of 80%., , Skin biopsy demonstrating a Merkel Cell cancer. Note the hyperchromatic epithelial cells and high, mitotic rate, , Image sourced from Wikipedia, , Next question
Page 796 :
Question 199 of 347, A 58 year old lady undergoes a screening mammogram and appearances are suspicious for ductal, carcinoma in situ. A stereotactic core biopsy is performed. If ductal carcinoma in situ is to be, diagnosed, which of the following pathological features must not be present?, , Nuclear pleomorphism, , Coarse chromatin, , Abnormal mitoses, , Angiogenesis, , Dysplastic cells infiltrating the suspensory ligaments of the breast, , The presence of invasion is a hallmark of invasive disease and thus would not be a feature of DCIS., Angiogenesis may occur in association with high grade DCIS., Please rate this question:, , Discuss and give feedback, , Next question, , Histopathology of malignancy, , , , , , , , , , Abnormal tissue architecture, Coarse chromatin, Invasion of basement membrane*, Abnormal mitoses, Angiogenesis, De-differentiation, Areas of necrosis, Nuclear pleomorphism, , *= Those features that distinguish invasive malignancy from in situ disease, Next question
Page 797 :
Question 200 of 347, Which of the following does not occur as a pathological response to extensive burns?, , Plasma leakage into interstitial space, , Absolute polycythaemia, , Increased haematocrit, , Keratinocyte migration during healing, , Cardiac output reduction by 50% in first 30 minutes, , Haemolysis is the main pathological response., Please rate this question:, , Discuss and give feedback, , Next question, , Burns pathology, Extensive burns, , , , , , , , , , Haemolysis due to damage of erythrocytes by heat and microangiopathy, Loss of capillary membrane integrity causing plasma leakage into interstitial space, Extravasation of fluids from the burn site causing hypovolaemic shock (up to 48h after, injury)- decreased blood volume and increased haematocrit, Protein loss, Secondary infection e.g. Staphylococcus aureus, ARDS, Risk of Curlings ulcer (acute peptic stress ulcers), Danger of full thickness circumferential burns in an extremity as these may develop, compartment syndrome, , Healing, , , Superficial burns: keratinocytes migrate to form a new layer over the burn site
Page 798 :
, , Full thickness burns: dermal scarring. Usually need keratinocytes from skin grafts to provide, optimal coverage., Next question
Page 799 :
Question 1-3 of 147, Theme: Chest pain, , A., B., C., D., E., F., G., H., I., , Pulmonary embolism, Acute exacerbation asthma, Physiological, Mitral valve stenosis, Aortic dissection, Mitral regurgitation, Bronchopneumonia, Tuberculosis, None of the above, , What is the most likely diagnosis for the scenario given? Each option may be used once, more than, once or not at all., , 1., , A 28 year old Indian woman, who is 18 weeks pregnant, presents with increasing shortness, of breath, chest pain and coughing clear sputum. She is apyrexial, blood pressure is 140/80, mmHg, heart rate 130 bpm and saturations 94% on 15L oxygen. On examination there is a, mid diastolic murmur, there are bibasal crepitations and mild pedal oedema. She suddenly, deteriorates and has a respiratory arrest. Her chest x-ray shows a whiteout of both of her, lungs., You answered Pulmonary embolism, The correct answer is Mitral valve stenosis, Mitral stenosis is the commonest cause of cardiac abnormality occurring in pregnant, women. Mitral stenosis is becoming less common in the UK population, however should be, considered in women from countries where there is a higher incidence of rheumatic heart, disease. Mitral stenosis causes a mid diastolic murmur which may be difficult to auscultate, unless the patient is placed into the left lateral position. These patients are at risk of atrial, fibrillation (up to 40%), which can also contribute to rapid decompensation such as, pulmonary oedema (hence cxr 'whiteout' of lungs). Physiological changes in pregnancy may, cause an otherwise asymptomatic patient to suddenly deteriorate. Balloon valvuloplasty is, the treatment of choice., , 2., , A 28 year old woman, who is 30 weeks pregnant, presents with sudden onset chest pain, associated with loss of consciousness. Her blood pressure is 170/90 mmHg, saturations on, 15L oxygen 93%, heart rate 120 bpm and she is apyrexial. On examination there is an early, diastolic murmur, occasional bibasal creptitations and mild peal oedema. An ECG shows, ST elevation in leads II, III and aVF.
Page 800 :
You answered Pulmonary embolism, The correct answer is Aortic dissection, Aortic dissection is associated with the 3rd trimester of pregnancy, connective tissue, disorders (Marfan's, Ehlers- Danlos) and bicuspid valve. Patients may complain of a tearing, chest pain or syncope. Clinically they may be hypertensive. The right coronary artery may, become involved in the dissection, causing myocardial infarct in up to 2% cases (hence ST, elevation in the inferior leads). An aortic regurgitant murmur may be auscultated., A 28 year old woman, who is 18 weeks pregnant, presents with sudden chest pain. Her, blood pressure is 150/70 mmHg, saturations are 92% on 15L oxygen and her heart rate is, 130 bpm. There are no murmurs and her chest is clear. There is signs of thrombophlebitis in, the left leg., , 3., , Pulmonary embolism, Chest pain, hypoxia and clear chest on auscultation in pregnancy should lead to a high, suspicion of pulmonary embolism., Theme question in September 2011 exam, Pregnant women can decompensate rapidly from cardiac compromise., Please rate this question:, , Discuss and give feedback, , Next question, , Chest pain in pregnancy, Aortic dissection, , , , , , , Predisposing factors in pregnancy are hypertension, congenital heart disease and Marfan's, syndrome, Mainly Stanford type A dissections, Sudden tearing chest pain, transient syncope, Patient may be cold and clammy, hypertensive and have an aortic regurgitation murmur, Involvement of the right coronary artery may cause inferior myocardial infarction, , Surgical management
Page 801 :
Gestational timeframe, , Management, , < 28/40, , Aortic repair with the fetus kept in utero, , 28-32/40, , Dependent on fetal condition, , > 32/40, , Primary Cesarean section followed by aortic repair at the same operation, , Mitral stenosis, , , , , , , Most cases associated with rheumatic heart disease, Becoming less common in British women; suspect in Immigrant women, Commonest cardiac condition in pregnancy, Commonly associated with mortality, Valve surgery; balloon valvuloplasty preferable, , Pulmonary embolism, , , , , , Leading cause of mortality in pregnancy, Half dose scintigraphy; CT chest if underlying lung disease, should aid diagnosis, Treatment with low molecular weight heparin throughout pregnancy and 4-6 weeks after, childbirth, Warfarin is contra indicated in pregnancy (though may be continued in women with, mechanical heart valves due to the significant risk of thromboembolism), , References, 1. Bates S.M. and Ginsberg J.S. How we manage venous thromboembolism during, pregnancy. Blood2002 (100): 3470-3478., 2. Scarsbrook A.Fand Gleeson V. Investigating suspected pulmonary embolism in, pregnancy. BMJ2007 (326) : 1135 doi: 10.1136/bmj.7399.1135., 3. Morley C. A. and Lim B. A. Lesson of the Week: The risks of delay in diagnosis of breathlessness, in pregnancy. BMJ 1995 (311) : 1083., Next question
Page 802 :
Question 4 of 147, A 67 year old man is investigated for biliary colic and a 4.8 cm abdominal aortic aneurysm is, identified. Which of the following statements relating to this condition is untrue?, , The wall will be composed of dense fibrous tissue only, , The majority are located inferior to the renal arteries, , They occur most often in current or former smokers, , He should initially be managed by a process of active surveillance, , Aortoduodenal fistula is a recognised complication following repair., , They are true aneurysms and have all 3 layers of arterial wall., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal aorta aneurysm, , , , , Abdominal aortic aneurysms are a common problem in vascular surgery., They may occur as either true or false aneurysm. With the former all 3 layers of the arterial, wall are involved, in the latter only a single layer of fibrous tissue forms the aneurysm wall., True abdominal aortic aneurysms have an approximate incidence of 0.06 per 1000 people., They are commonest in elderly men and for this reason the UK is now introducing the, aneurysm screening program with the aim of performing an abdominal aortic ultrasound, measurement in all men aged 65 years., , Causes, , , , Several different groups of patients suffer from aneurysmal disease., The commonest group is those who suffer from standard arterial disease, i.e. Those who, arehypertensive, have diabetes and have been or are smokers.
Page 803 :
, , Other patients such as those suffering from connective tissue diseases such as Marfan's, may also develop aneurysms. In patients with abdominal aortic aneurysms the extracellular, matrix becomes disrupted with a change in the balance of collagen and elastic fibres., , Management, , , , , , , , , Most abdominal aortic aneurysms are an incidental finding., Symptoms most often relate to rupture or impending rupture., 20% rupture anteriorly into the peritoneal cavity. Very poor prognosis., 80% rupture posteriorly into the retroperitoneal space, The risk of rupture is related to aneurysm size, only 2% of aneurysms measuring less than, 4cm in diameter will rupture over a 5 year period. This contrasts with 75% of aneurysms, measuring over 7cm in diameter., This is well explained by Laplaces' law which relates size to transmural pressure., For this reason most vascular surgeons will subject patients with an aneurysm size of 5cm or, greater to CT scanning of the chest, abdomen and pelvis with the aim of delineating anatomy, and planning treatment. Depending upon co-morbidities, surgery is generally offered once, the aneurysm is between 5.5cm and 6cm., , A CT reconstruction showing an infrarenal abdominal aortic aneurysm. The walls of the sac are, calcified which may facilitate identification on plain x-rays
Page 804 :
Image sourced from Wikipedia, , Indications for surgery, , , , , Symptomatic aneurysms (80% annual mortality if untreated), Increasing size above 5.5cm if asymptomatic, Rupture (100% mortality without surgery)
Page 805 :
Surgical procedures, Abdominal aortic aneurysm repair, Procedure:, GA, Invasive monitoring (A-line, CVP, catheter), Incision: Midline or transverse, Bowel and distal duodenum mobilised to access aorta., Aneurysm neck and base dissected out and prepared for cross clamp, Systemic heparinisation, Cross clamp (proximal first), Longitudinal aortotomy, Atherectomy, Deal with back bleeding from lumbar vessels and inferior mesenteric artery, Insert graft either tube or bifurcated depending upon anatomy, Suture using Prolene (3/0 for proximal , distal anastomosis suture varies according to site), Clamps off: End tidal CO2 will rise owing to effects of reperfusion, at this point major risk of, myocardial events., Haemostasis, Closure of aneurysm sac to minimise risk of aorto-enteric fistula, Closure: Loop 1 PDS or Prolene to abdominal wall, Skin- surgeons preference, Post operatively:, ITU (Almost all), Greatest risk of complications following emergency repair, Complications: Embolic- gut and foot infarcts, Cardiac - owing to premorbid states, re-perfusion injury and effects of cross clamp, Wound problems, Later risks related to graft- infection and aorto-enteric fistula, Special groups, Supra renal AAA, These patients will require a supra renal clamp and this carries a far higher risk of complications and, risk of renal failure., Ruptured AAA, Pre-operatively the management depends upon haemodynamic instability. In patients with, symptoms of rupture (typical pain, haemodynamic compromise and risk factors) then ideally prompt, laparotomy. In those with vague symptoms and haemodynamic stability the ideal test is CT scan to, determine whether rupture has occurred or not. Most common rupture site is retroperitoneal 80%., These patients will tend to develop retroperitoneal haematoma. This can be disrupted if Bp is, allowed to rise too high so aim for Bp 100mmHg., Operative details are similar to elective repair although surgery should be swift, blind rushing often, makes the situation worse. Plunging vascular clamps blindly into a pool of blood at the aneurysm, neck carries the risk of injury the vena cava that these patients do not withstand. Occasionally a, supracoeliac clamp is needed to effect temporary control, although leaving this applied for more than, 20 minutes tends to carry a dismal outcome.
Page 806 :
EVAR, Increasingly patients are now being offered endovascular aortic aneurysm repair. This is undertaken, by surgeons and radiologists working jointly. The morphology of the aneurysm is important and not, all are suitable. Here is a typical list of those features favoring a suitable aneurysm:, , , , , Long neck, Straight iliac vessels, Healthy groin vessels, , Clearly few AAA patients possess the above and compromise has to be made. The use of, fenestrated grafts can allow supra renal AAA to be treated., Procedure:, GA, Radiology or theatre, Bilateral groin incisions, Common femoral artery dissected out, Heparinisation, Arteriotomy and insertion of guide wire, Dilation of arteriotomy, Insertion of EVAR Device, Once in satisfactory position it is released, Arteriotomy closed once check angiogram shows good position and no endoleak, Complications:, Endoleaks depending upon site are either Type I or 2. These may necessitate re-intervention and all, EVAR patients require follow up . Details are not needed for MRCS., References, A reasonable review is provided by:, Sakalihasan N, Limet R, Defawe O. Abdominal aortic aneurysm. Lancet 2005 (365):1577- 1589, Next question
Page 807 :
Question 5 of 147, Which of the following statements in relation to the p53 tumour suppressor protein is false?, , It may induce necrosis of cells with non repairable DNA damage, , It is affected in Li Fraumeni syndrome, , It can induce DNA repair, , It can halt the cell cycle, , It may inhibit angiogenesis, , When DNA cannot be repaired it will induce cellular apoptosis (not necrosis), Please rate this question:, , Discuss and give feedback, , Next question, , Genetics and surgical disease, Some of the more commonly occurring genetic conditions occurring in surgical patients are, presented here., Li-Fraumeni Syndrome, , , , , , Autosomal dominant, Consists of germline mutations to p53 tumour suppressor gene, High incidence of malignancies particularly sarcomas and leukaemias, Diagnosed when:, , *Individual develops sarcoma under 45 years, *First degree relative diagnosed with any cancer below age 45 years and another family member, develops malignancy under 45 years or sarcoma at any age, BRCA 1 and 2
Page 808 :
, , , , Carried on chromosome 17 (BRCA 1) and Chromosome 13 (BRCA 2), Linked to developing breast cancer (60%) risk., Associated risk of developing ovarian cancer (55% with BRCA 1 and 25% with BRCA 2)., , Lynch Syndrome, , , , , , Autosomal dominant, Develop colonic cancer and endometrial cancer at young age, 80% of affected individuals will get colonic and/ or endometrial cancer, High risk individuals may be identified using the Amsterdam criteria, , Amsterdam criteria, Three or more family members with a confirmed diagnosis of colorectal cancer, one of whom is a, first degree (parent, child, sibling) relative of the other two., Two successive affected generations., One or more colon cancers diagnosed under age 50 years., Familial adenomatous polyposis (FAP) has been excluded., Gardners syndrome, , , , , , , , , Autosomal dominant familial colorectal polyposis, Multiple colonic polyps, Extra colonic diseases include: skull osteoma, thyroid cancer and epidermoid cysts, Desmoid tumours are seen in 15%, Mutation of APC gene located on chromosome 5, Due to colonic polyps most patients will undergo colectomy to reduce risk of colorectal, cancer, Now considered a variant of familial adenomatous polyposis coli, Next question
Page 809 :
Question 6 of 147, Which of the following cell types is most likely to be identified in the wall of a fistula in ano?, , Squamous cells, , Goblet cells, , Columnar cells, , Ciliated columnar cells, , None of the above, , A fistula is an abnormal connection between two epithelial lined surfaces, in the case of a fistula in, ano it will be lined by squamous cells., Please rate this question:, , Discuss and give feedback, , Next question, , Fistulas, , , , , , A fistula is defined as an abnormal connection between two epithelial surfaces., There are many types ranging from Branchial fistulae in the neck to entero-cutaneous, fistulae abdominally., In general surgical practice the abdominal cavity generates the majority and most of these, arise from diverticular disease and Crohn's., As a general rule all fistulae will resolve spontaneously as long as there is no distal, obstruction. This is particularly true of intestinal fistulae., , The four types of fistulae are:, Enterocutaneous, These link the intestine to the skin. They may be high (>500ml) or low output (<250ml) depending, upon source. Duodenal /jejunal fistulae will tend to produce high volume, electrolyte rich secretions, which can lead to severe excoriation of the skin. Colo-cutaneous fistulae will tend to leak faeculent, material. Both fistulae may result from the spontaneous rupture of an abscess cavity onto the skin, (such as following perianal abscess drainage) or may occur as a result of iatrogenic input. In some
Page 810 :
cases it may even be surgically desirable e.g. mucous fistula following sub total colectomy for colitis., Suspect if there is excess fluid in the drain., Enteroenteric or Enterocolic, This is a fistula that involves the large or small intestine. They may originate in a similar manner to, enterocutaneous fistulae. A particular problem with this fistula type is that bacterial overgrowth may, precipitate malabsorption syndromes. This may be particularly serious in inflammatory bowel, disease., Enterovaginal, Aetiology as above., Enterovesicular, This type of fistula goes to the bladder. These fistulas may result in frequent urinary tract infections,, or the passage of gas from the urethra during urination., Management, Some rules relating to fistula management:, , , , , , , , , They will heal provided there is no underlying inflammatory bowel disease and no distal, obstruction, so conservative measures may be the best option, Where there is skin involvement, protect the overlying skin, often using a well fitted stoma, bag- skin damage is difficult to treat, A high output fistula may be rendered more easily managed by the use of octreotide, this will, tend to reduce the volume of pancreatic secretions., Nutritional complications are common especially with high fistula (e.g. high jejunal or, duodenal) these may necessitate the use of TPN to provide nutritional support together with, the concomitant use of octreotide to reduce volume and protect skin., When managing perianal fistulae surgeons should avoid probing the fistula where acute, inflammation is present, this almost always worsens outcomes., When perianal fistulae occur secondary to Crohn's disease the best management option is, often to drain acute sepsis and maintain that drainage through the judicious use of setons, whilst medical management is implemented., Always attempt to delineate the fistula anatomy, for abscesses and fistulae that have an intra, abdominal source the use of barium and CT studies should show a track. For perianal, fistulae surgeons should recall Goodsall's rule in relation to internal and external openings., Next question
Page 811 :
Question 7 of 147, A 22 year old man is referred to the surgical clinic. He has been complaining of varicose veins for, many years. On examination he has extensive varicosities of the right leg, there are areas of marked, port wine staining. The saphenofemoral junction is competent on doppler assessment. The most, likely underlying diagnosis is:, , Deep vein thrombosis, , Klippel-Trenaunay syndrome, , Varicose veins due to sapheno-popliteal junction incompetence, , Sturge - Weber syndrome, , Angiosarcoma, , Sturge - Weber syndrome is a an arteriovenous malformation affecting the face and CNS, the, peripheral vessels are not affected. Simple varicose veins should not typically be associated with, port wine staining, nor should a DVT or angiosarcoma., Please rate this question:, , Discuss and give feedback, , Next question, , Klippel-Trenaunay syndrome, Klippel-Trenaunay-Weber syndrome generally affects a single extremity, although cases of multiple, affected limbs have been reported. The leg is the most common site followed by the arms, the trunk,, and rarely the head and the neck, Signs and symptoms, The birth defect is diagnosed by the presence of a combination of these symptoms:, , , , , , One or more distinctive port-wine stains with sharp borders, Varicose veins, Hypertrophy of bony and soft tissues, that may lead to local gigantism or shrinking., An improperly developed lymphatic system
Page 812 :
In some cases, port-wine stains (capillary port wine type) may be absent. Such cases are very rare, and may be classified as "atypical Klippel-Trenaunay syndrome"., KTS can either affect blood vessels, lymph vessels, or both. The condition most commonly presents, with a mixture of the two. Those with venous involvement experience increased pain and, complications., Next question
Page 813 :
Question 8 of 147, A 68 year old man presents with an ulcerated lesion on his right cheek. It is excised and on, histological assessment a squamous cell carcinoma is diagnosed. It measures 25mm in diameter, and is 4mm deep. Which of the following statements relating to this condition is false?, , In this particular case margins of at least 6mm are required, , Use of cryosurgery to treat this patients lesion would have been unsafe, , Use of radiotherapy to treat this lesion would have been unsafe, , This patients local recurrence rate may approach 15%, , The disease usually spreads via lymphatics, Poor prognostic factors in SCC:, , , , Size >20mm (local recurrence rate of up to 15%), Depth greater than 4mm (risk of metastasis up to 30%), , This man has an SCC with significant risk of metastasis. Although cryotherapy may be used to treat, SCC it would be most unsafe in this setting as the lesion extends deeply. However, radiotherapy is a, safe treatment modality for SCC and may be used in selected cases. It is unwise to use radiotherapy, in areas prone to radionecrosis e.g. the nose., Please rate this question:, , Discuss and give feedback, , Next question, , Squamous cell carcinoma of the skin, , , , , , Second most common skin malignancy, Derived from epidermal keratinocytes, Commonest in fair skinned individuals in sun exposed sites, May occur in perianal and genital skin especially in association with Human Papilloma Virus, 16 and 18 infections.
Page 815 :
Image sourced from Wikipedia, , References, The British Association of Dermatology provides guidelines for the diagnosis and treatment of SCC., http://www. bad.org.uk, Next question
Page 816 :
Question 9 of 147, , A 23 year old man presents with weight loss fatigue and lymphadenopathy. He is diagnosed with, tuberculosis. Which of the following processes most closely matches the underlying pathological, process?, , Type 1 hypersensitivity reaction, , Type 2 hypersensitivity reaction, , Type 3 hypersensitivity reaction, , Type 4 hypersensitivity reaction, , None of the above, , Granulomas (which occur in tuberculosis) are a feature of Type 4 hypersensitivity reactions., Please rate this question:, , Discuss and give feedback, , Next question, , Hypersensitivity reactions, The Gell and Coombs classification divides hypersensitivity reactions into 4 types, , Type I, , Type II, , Type III, , Type IV
Page 818 :
Question 10 of 147, A 73 year old man undergoes an emergency amputation for severe lower limb sepsis and gangrene., Post operatively he develops disseminated intravascular coagulation. Which of the following clotting, factors will be most rapidly consumed in this process?, , Factor V and VIII, , Factor I, , Factor I and III, , Factor III and VII, , Factor VI and VIII, D-I-S-S-E-M-I-N-A-T-E-D, D-Dx: D dimer, I-Immune complexes, S-Snakebite, shock, heatstroke, S-SLE, E-Eclampsia, HELLP syndrome, M-Massive tissue damage, I-Infections: viral and bacterial, N-Neoplasms, A-Acute promyelocytic leukemia, T-Tumor products: Tissue Factor (TF) and TF-like factors released by carcinomas of pancreas,, prostate, lung,, colon, stomach, E-Endotoxins (bacterial), D-Dead fetus (retained), DIC Will tend to consume factors five and eight intially (and platelets)., Please rate this question:, , Discuss and give feedback, , Next question, , Disseminated intravascular coagulation
Page 819 :
Simultaneous coagulation and haemorrhage caused by initially formation of thrombi which consume, clotting factors (factors 5,8) and platelets, ultimately leading to bleeding, Causes include:, , , , , , , Infection, Malignancy, Trauma e.g. major surgery, burns, shock, dissecting aortic aneurysm, Liver disease, Obstetric complications, , Key points, , , , , Clinically bleeding is usually a dominant feature, bruising, ischaemia and organ failure, Blood tests: prolonged clotting times, thrombocytopenia, decreased fibrinogen, increased, fibrinogen degradation products, Treat the underlying cause and supportive management, Next question
Page 820 :
Question 11 of 147, A pregnant women suddenly develops bilateral leg swelling. Her mother and aunt were troubled by, the same problem. What is the most likely underlying abnormality?, , Anti endomysial antibodies, , Anti nuclear antibodies, , Anti cardiolipin antibodies, , Anti thyroid antibodies, , Anti mitochondrial antibodies, Anti phospholipid syndrome= following antibodies, , , , , Lupus anticoagulant, Anti-cardiolipin, Anti-β2-glycoprotein, , Theme from September 2014 Exam, Antiphospholipid syndrome, is an autoimmune, hypercoagulable state caused by antiphospholipid, antibodies. APS provokes blood clots (thrombosis) in both arteries and veins as well as pregnancyrelated complications such as miscarriage, stillbirth, preterm delivery, or severe preeclampsia., The diagnostic criteria requires one clinical event, i.e. thrombosis or pregnancy complication, and, two positive blood tests spaced at least 3 months apart. These antibodies are: lupus anticoagulant,, anti-cardiolipin and anti-β2-glycoprotein., Antiphospholipid syndrome can be primary or secondary. Primary antiphospholipid syndrome occurs, in the absence of any other related disease. Secondary antiphospholipid syndrome occurs with other, autoimmune diseases, such as systemic lupus erythematosus (SLE). In rare cases, APS leads to, rapid organ failure due to generalised thrombosis; this is termed "catastrophic antiphospholipid, syndrome" (CAPS) and is associated with a high risk of death., Antiphospholipid syndrome often requires treatment with anticoagulant medication such as heparin, to reduce the risk of further episodes of thrombosis and improve the prognosis of pregnancy., Warfarin is not used during pregnancy because it can cross the placenta, unlike heparin, and is, teratogenic., Please rate this question:
Page 821 :
Discuss and give feedback, , Next question, , Hypercoagulability, Type of thrombophilia, , Features, , Antithrombin deficiency, , Antithrombin inactivates thrombin and factor XII a, XIa, IXa and Xa, Rare defect, inherited in autosomal dominant fashion, 10x increase in risk of thrombotic events, Heparin may be ineffective because it works via antithrombin, , Protein C and S, deficiency, , These are natural anticoagulants (vitamin K dependent synthesis), Protein C produced by liver, Protein S produced by liver, megakaryocytes, Leydig cells and, endothelial cells, Protein C and S bind to form activated complex which binds to factor, V, Deficiency accounts for up to 5% of thrombotic episodes, , Factor V Leiden, , Resistance to anticoagulant effect of activated protein C, May account for up to 20% or more of thrombotic episodes, Prevalence of 7% in Europe, Most common genetic defect accounting for DVT, , Antiphospholipid, syndrome, , Multi organ disease, Pregnancy involvement common, Arterial and venous thromboses, Either Lupus anticoagulant or Anti cardiolipin antibodies, APTT usually prolonged, Antibodies may be elevated following surgery, drugs or malignancy, Need anticoagulation with INR between 3 and 4, Next question
Page 822 :
Question 12 of 147, A 63 year old Japanese man presents with epigastric discomfort and iron deficiency anaemia. He, undergoes an upper GI endoscopy, where the following appearances are found:, , Image sourced from Wikipedia, , The most likely diagnosis is:, , Squamous cell carcinoma, , Linitis plastica, , Leiomyosarcoma, , Gastric varices, , None of the above, During upper GI endoscopy, a linitis plastica lesion may prevent gastric distension.
Page 823 :
Linitis plastica produces a diffuse infiltrating lesion, the stomach is fibrotic and rigid and will not, typically distend. This may be described as a 'leather bottle stomach'. Diagnosis is made with a, combination of pathology examination with endoscopy, radiological or surgical assessment., Pathologically signet-ring cell proliferation occurs., Please rate this question:, , Discuss and give feedback, , Next question, , Gastric cancer, Overview, There are 700,000 new cases of gastric cancer worldwide each year. It is most common in Japan, and less common in western countries. It is more common in men and incidence rises with, increasing age. The exact cause of many sporadic cancer is not known, however, familial cases do, occur in HNPCC families. In addition, smoking and smoked or preserved foods increase the risk., Japanese migrants retain their increased risk (decreased in subsequent generations). The, distribution of the disease in western countries is changing towards a more proximal location, (perhaps due to rising obesity)., Pathology, There is some evidence of support a stepwise progression of the disease through intestinal, metaplasia progressing to atrophic gastritis and subsequent dysplasia, through to cancer. The, favoured staging system is TNM. The risk of lymph node involvement is related to size and depth of, invasion; early cancers confined to submucosa have a 20% incidence of lymph node metastasis., Tumours of the gastro-oesophageal junction are classified as below:, , Type, 1, , True oesophageal cancers and may be associated with Barrett's oesophagus., , Type, 2, , Carcinoma of the cardia, arising from cardiac type epithelium, or short segments with intestinal metaplasia at the oesophagogastric junction., , Type, 3, , Sub cardial cancers that spread across the junction. Involve similar nodal stations to, gastric cancer., , Groups for close endoscopic monitoring, , , , , , Intestinal metaplasia of columnar type, Atrophic gastritis, Low to medium grade dysplasia, Patients who have previously undergone resections for benign peptic ulcer disease (except, highly selective vagotomy).
Page 824 :
Referral to endoscopy, , Patients of any age with, dyspepsia and any of the, following, , Patients without, dyspepsia, , Worsening dyspepsia, , Chronic gastrointestinal bleeding, , Dysphagia, , Barretts oesophagus, , Dysphagia, , Unexplained abdominal, pain or weight loss, , Intestinal metaplasia, , Weight loss, , Vomiting, , Dysplasia, , Iron deficiency anaemia, , Upper abdominal mass, , Atrophic gastritis, , Upper abdominal mass, , Jaundice, , Patient aged over 55 years with, unexplained or persistent, dyspepsia, , Upper GI endoscopy performed for dyspepsia. The addition of dye spraying (as shown in the bottom, right) may facilitate identification of smaller tumours
Page 825 :
Image sourced from Wikipedia, , Staging, , , , , CT scanning of the chest abdomen and pelvis is the routine first line staging investigation in, most centres., Laparoscopy to identify occult peritoneal disease, PET CT (particularly for junctional tumours), , Treatment, , , , , , , , Proximally sited disease greater than 5-10cm from the OG junction may be treated by sub, total gastrectomy, Total gastrectomy if tumour is <5cm from OG junction, For type 2 junctional tumours (extending into oesophagus) oesophagogastrectomy is usual, Endoscopic sub mucosal resection may play a role in early gastric cancer confined to the, mucosa and perhaps the sub mucosa (this is debated), Lymphadenectomy should be performed. A D2 lymphadenectomy is widely advocated by the, Japanese, the survival advantages of extended lymphadenectomy have been debated., However, the overall recommendation is that a D2 nodal dissection be undertaken., Most patients will receive chemotherapy either pre or post operatively., , Prognosis
Page 826 :
UK Data, , Disease extent, , Percentage 5 year survival, , All RO resections, , 54%, , Early gastric cancer, , 91%, , Stage 1, , 87%, , Stage 2, , 65%, , Stage 3, , 18%, , Operative procedure, Total Gastrectomy , lymphadenectomy and Roux en Y anastomosis, General anaesthesia, Prophylactic intravenous antibiotics, Incision: Rooftop., Perform a thorough laparotomy to identify any occult disease., Mobilise the left lobe of the liver off the diaphragm and place a large pack over it. Insert a large self, retaining retractor e.g. omnitract or Balfour (take time with this, the set up should be perfect). Pack, the small bowel away., Begin by mobilising the omentum off the transverse colon., Proceed to detach the short gastric vessels., Mobilise the pylorus and divide it at least 2cm distally using a linear cutter stapling device., Continue the dissection into the lesser sac taking the lesser omentum and left gastric artery flush at, its origin., The lymph nodes should be removed en bloc with the specimen where possible., Place 2 stay sutures either side of the distal oesophagus. Ask the anaesthetist to pull back on the, nasogastric tube. Divide the distal oesophagus and remove the stomach., The oesphago jejunal anastomosis should be constructed. Identify the DJ flexure and bring a loop of, jejunum up to the oesophagus (to check it will reach). Divide the jejunum at this point. Bring the, divided jejunum either retrocolic or antecolic to the oesophagus. Anastamose the oesophagus to the, jejunum, using either interrupted 3/0 vicryl or a stapling device. Then create the remainder of the, Roux en Y reconstruction distally., Place a jejunostomy feeding tube., Wash out the abdomen and insert drains (usually the anastomosis and duodenal stump). Help the, anaesthetist insert the nasogastric tube (carefully!), Close the abdomen and skin.
Page 827 :
Enteral feeding may commence on the first post-operative day. However, most surgeons will leave, patients on free NG drainage for several days and keep them nil by mouth., Next question
Page 828 :
0/3, Question 13-15 of 147, Theme: Genetics and cancer, , A., B., C., D., E., F., G., , Multiple endocrine neoplasia type I, Multiple endocrine neoplasia type II, Gardner's syndrome, Lynch Syndrome, Kartagener's syndrome, Neurofibromatosis Type I, Neurofibromatosis Type II, , Please select the most likely condition for the disease process described. Each option may be used, once, more than once or not at all., , 13., , A 40 year old male is found to have multiple colonic polyps during a colonoscopy. He, mentions that he has extra teeth., You answered Multiple endocrine neoplasia type I, The correct answer is Gardner's syndrome, Gardner's syndrome is an AD disorder, characterised by: Colonic polyps, supernumerary, teeth, jaw osteomas, congenital hypertrophy of retinal pigment. osteomas of the skull,, thyroid cancer, epidermoid cysts, fibromas and sebaceous cysts., , 14., , A 10 year old boy who has learning difficulties, reports a difference in size between his, two legs., You answered Multiple endocrine neoplasia type I, The correct answer is Neurofibromatosis Type I, Neurofibromatosis type I. A hallmark finding is a plexiform neurofibroma, which is a, sheet of neurofibromatosis tissue which encases major nerves. In children this attracts, extra blood circulation, which can accelerate growth of the affected limb., Other features include:, Schwannoma, > 6, Cafe au lait spots, axillary freckling, Lisch nodules, Optic glioma. Meningiomas, Glioma,, or Schwannoma., , 15., , A 22 year old is found to have bilateral acoustic neuromas.
Page 829 :
You answered Multiple endocrine neoplasia type I, The correct answer is Neurofibromatosis Type II, In NF2 bilateral acoustic neuromas are characteristic with a family history of, Neurofibroma,, Please rate this question:, , Discuss and give feedback, , Next question, , Genetics and surgical disease, Some of the more commonly occurring genetic conditions occurring in surgical patients are, presented here., Li-Fraumeni Syndrome, , , , , , Autosomal dominant, Consists of germline mutations to p53 tumour suppressor gene, High incidence of malignancies particularly sarcomas and leukaemias, Diagnosed when:, , *Individual develops sarcoma under 45 years, *First degree relative diagnosed with any cancer below age 45 years and another family member, develops malignancy under 45 years or sarcoma at any age, BRCA 1 and 2, , , , , Carried on chromosome 17 (BRCA 1) and Chromosome 13 (BRCA 2), Linked to developing breast cancer (60%) risk., Associated risk of developing ovarian cancer (55% with BRCA 1 and 25% with BRCA 2)., , Lynch Syndrome, , , , , , Autosomal dominant, Develop colonic cancer and endometrial cancer at young age, 80% of affected individuals will get colonic and/ or endometrial cancer, High risk individuals may be identified using the Amsterdam criteria
Page 830 :
Amsterdam criteria, Three or more family members with a confirmed diagnosis of colorectal cancer, one of whom is a, first degree (parent, child, sibling) relative of the other two., Two successive affected generations., One or more colon cancers diagnosed under age 50 years., Familial adenomatous polyposis (FAP) has been excluded., Gardners syndrome, , , , , , , , , Autosomal dominant familial colorectal polyposis, Multiple colonic polyps, Extra colonic diseases include: skull osteoma, thyroid cancer and epidermoid cysts, Desmoid tumours are seen in 15%, Mutation of APC gene located on chromosome 5, Due to colonic polyps most patients will undergo colectomy to reduce risk of colorectal, cancer, Now considered a variant of familial adenomatous polyposis coli, Next question
Page 831 :
Question 16 of 147, A 52 year old lady is referred to the breast clinic with symptoms of nipple discharge. The discharge, is usually thick and green. Which of the following statements relating to the most likely underlying, diagnosis is untrue?, , The majority of patients will be smokers, , Typically produces blood stained nipple discharge, , It is not associated with increased risk of breast cancer, , May result in development of mammary duct fistula, , May require total duct excision (Hadfields operation) if it fails to resolve, Blood stained nipple discharge should always be investigated., Nipple fluid cytology is generally unhelpful., Discharge of this type of material is most likely to be due to duct ectasia. Green or brown discharge, is most common. Blood stained discharge should raise concern of intraductal papilloma or cancer., Please rate this question:, , Discuss and give feedback, , Next question, , Nipple discharge, Causes of nipple discharge, , Physiological, , During breast feeding, , Galactorrhoea, , Commonest cause may be response to emotional events, drugs such as, histamine receptor antagonists are also implicated, , Hyperprolactinaemia, , , , , Commonest type of pituitary tumour, Microadenomas <1cm in diameter
Page 832 :
, , , Macroadenomas >1cm in diameter, Pressure on optic chiasm may cause bitemporal hemianopia, , Mammary duct, ectasia, , , , , , , Dilatation breast ducts., Most common in menopausal women, Discharge typically thick and green in colour, Most common in smokers, , Carcinoma, , , , , Often blood stained, May be underlying mass or axillary lymphadenopathy, , Intraductal papilloma, , , , , , Commoner in younger patients, May cause blood stained discharge, There is usually no palpable lump, , Assessment of patients, , , , Examine breast and determine whether there is mass lesion present, All mass lesions should undergo Triple assessment., , Reporting of investigations, Where a mass lesion is suspected or investigations are requested these are prefixed using a system, that denotes the investigation type e.g. M for mammography, followed by a numerical code as, shown below:, , 1, , No abnormality, , 2, , Abnormality with benign features, , 3, , Indeterminate probably benign, , 4, , Indeterminate probably malignant, , 5, , Malignant
Page 833 :
Management of non malignant nipple discharge, , , , , , Exclude endocrine disease, Nipple cytology unhelpful, Smoking cessation advice for duct ectasia, For duct ectasia with severe symptoms, total duct excision may be warranted., Next question
Page 834 :
Question 17 of 147, Which of the following statements relating to gas gangrene is untrue?, , There is necrosis with putrefaction, , The causative pathogens may be detected on normal perineal skin, , Treatment with low dose penicillin is indicated, , Hyperbaric oxygen may be beneficial, , Clostridium perfringens is a recognised cause, , Rapid surgery and high dose antibiotics are indicated in the treatment of gas gangrene., Please rate this question:, , Discuss and give feedback, , Next question, , Meleney's Gangrene and Necrotising Fasciitis, Necrotising fasciitis, , , , , , , Advancing soft tissue infection associated with fascial necrosis, Uncommon, but can be fatal, In many cases there is underlying background immunosuppression e.g. Diabetes, Caused by polymicrobial flora (aerobic and anaerobic) and MRSA is seen increasingly in, cases of necrotising fasciitis, Streptococcus is the commonest organism in isolated pathogen infection (15%), , Meleneys gangrene, , , Meleneys is a similar principle but the infection is more superficially sited than necrotising, fasciitis and often confined to the trunk
Page 835 :
Fournier gangrene, , , , Necrotising fasciitis affecting the perineum, Polymicrobial with E-coli and Bacteroides acting in synergy, , Clinical features, Fever, Pain, Cellulitis, Oedema, Induration, Numbness, Late findings, Purple/black skin discolouration, Blistering, Haemorrhagic bullae, Crepitus, Dirty Dishwater fluid discharge, Septic shock, A typical case of gas gangrene presenting late demonstrating some of the features described above, , Image sourced from Wikipedia, , Diagnosis is mainly clinical, Management
Page 836 :
, , , , Radical surgical debridement forms the cornerstone of management, Sterile dressing is used to dress the wound, Reconstructive surgery is considered once the infection is completely treated, , Reference, Hasham S, Matteucci P, Stanley PR, Hart NB. Necrotising fasciitis. BMJ 2005;330:830-833., Next question
Page 837 :
Question 18 of 147, A 30 year old man presents with abdominal distension, a laparotomy is performed, at operation the, abdomen is filled with a large amount of gelatinous fluid. What is the most likely underlying, diagnosis?, , Infection with entamoeba histolytica, , Pseudomxyoma peritonei, , Metastatic colonic cancer, , Chylous ascites, , None of the above, , Pseudomyxoma is associated with the deposition of large amounts of gelatinous material. The, appendix is the commonest organ or origin., Please rate this question:, , Discuss and give feedback, , Next question, , Pseudomyxoma Peritonei, , , , , , Rare mucinous tumour, Most commonly arising from the appendix (other abdominal viscera are also recognised as, primary sites), Incidence of 1-2/1,000,000 per year, The disease is characterised by the accumulation of large amounts of mucinous material in, the abdominal cavity, , Treatment, Is usually surgical and consists of cytoreductive surgery (and often peritonectomy c.f Sugarbaker, procedure) combined with intra peritoneal chemotherapy with mitomycin C., Survival is related to the quality of primary treatment and in Sugarbakers own centre 5 year survival, rates of 75% have been quoted. Patients with disseminated intraperitoneal malignancy from another
Page 838 :
source fare far worse., In selected patients a second look laparotomy is advocated and some practice this routinely., Next question
Page 839 :
Question 19 of 147, A 30 year old man is suspected of having appendicitis. At operation an inflamed Meckels, diverticulum is found. Which of the following vessels is responsible for the blood supply to a Meckels, diverticulum?, , Right colic artery, , Vitelline artery, , Appendicular artery, , Internal iliac artery, , External iliac artery, , The vitelline arteries supply a Meckels these are usually derived from the ileal arcades., Please rate this question:, , Discuss and give feedback, , Next question, , Meckel's diverticulum, , , , , , , , , Congenital abnormality resulting in incomplete obliteration of the vitello-intestinal duct, Normally, in the foetus, there is an attachment between the vitello-intestinal duct and the yolk, sac.This disappears at 6 weeks gestation., The tip is free in majority of cases., Associated with enterocystomas, umbilical sinuses, and omphaloileal fistulas., Arterial supply: omphalomesenteric artery., 2% of population, 2 inches long, 2 feet from the ileocaecal valve., Typically lined by ileal mucosa but ectopic gastric mucosa can occur, with the risk of peptic, ulceration. Pancreatic and jejunal mucosa can also occur., , Clinical, , , , Normally asymptomatic and an incidental finding., Complications are the result of obstruction, ectopic tissue, or inflammation.
Page 840 :
, , Removal if narrow neck or symptomatic. Options are between wedge excision or formal, small bowel resection and anastomosis., Next question
Page 841 :
Question 20 of 147, Which of the following associations are incorrect?, , Afro-Caribbean skin and keloid scarring, , Extensive third degree burns and wound contraction, , Chemotherapy and dehisence of healed wounds, , Poor healing at the site of previous radiotherapy, , Zinc deficiency and delayed healing, , Please rate this question:, , Discuss and give feedback, , Next question, , Wound healing, Surgical wounds are either incisional or excisional and either clean, clean contaminated or dirty., Although the stages of wound healing are broadly similar their contributions will vary according to the, wound type., The main stages of wound healing include:, Haemostasis, , , , Minutes to hours following injury, Vasospasm in adjacent vessels, platelet plug formation and generation of fibrin rich clot., , Inflammation, , , , Typically days 1-5, Neutrophils migrate into wound (function impaired in diabetes).
Page 842 :
, , , , Growth factors released, including basic fibroblast growth factor and vascular endothelial, growth factor., Fibroblasts replicate within the adjacent matrix and migrate into wound., Macrophages and fibroblasts couple matrix regeneration and clot substitution., , Regeneration, , , , , , Typically days 7 to 56, Platelet derived growth factor and transformation growth factors stimulate fibroblasts and, epithelial cells., Fibroblasts produce a collagen network., Angiogenesis occurs and wound resembles granulation tissue., , Remodeling, , , , , , , From 6 weeks to 1 year, Longest phase of the healing process and may last up to one year (or longer)., During this phase fibroblasts become differentiated (myofibroblasts) and these facilitate, wound contraction., Collagen fibres are remodeled., Microvessels regress leaving a pale scar., , The above description represents an idealised scenario. A number of diseases may distort this, process. Neovascularisation is an important early process. Endothelial cells may proliferate in the, wound bed and recanalise to form a vessel. Vascular disease, shock and sepsis can all compromise, microvascular flow and impair healing., Conditions such as jaundice will impair fibroblast synthetic function and immunity with a detrimental, effect in most parts of the healing process., Problems with scars:, Hypertrophic scars, Excessive amounts of collagen within a scar. Nodules may be present histologically containing, randomly arranged fibrils within and parallel fibres on the surface. The tissue itself is confined to the, extent of the wound itself and is usually the result of a full thickness dermal injury. They may go on, to develop contractures., Image of hypertrophic scarring. Note that it remains confined to the boundaries of the original, wound:
Page 843 :
Image sourced from Wikipedia, , Keloid scars, Excessive amounts of collagen within a scar. Typically a keloid scar will pass beyond the boundaries, of the original injury. They do not contain nodules and may occur following even trivial injury. They, do not regress over time and may recur following removal., Image of a keloid scar. Note the extension beyond the boundaries of the original incision:, , Image sourced from Wikipedia, , Drugs which impair wound healing:
Page 844 :
, , , , , Non steroidal anti inflammatory drugs, Steroids, Immunosupressive agents, Anti neoplastic drugs, , Closure, Delayed primary closure is the anatomically precise closure that is delayed for a few days but before, granulation tissue becomes macroscopically evident., Secondary closure refers to either spontaneous closure or to surgical closure after granulation tissue, has formed., Next question
Page 845 :
Question 21 of 147, , A 45 year old women is identified as having a gastric gastro-intestinal stromal tumour. What is the, usual cell of origin of these lesions?, , Brunners glands, , Interstitial cells of Cajal, , Primitive stem cells of the gut wall, , Fundic glands, , Antral goblet cells, , GIST's are derived from the interstitial pacemaker cells of Cajal. This means that they are often, located extramucosally and macroscopically, demonstrate little mucosal disruption., Please rate this question:, , Discuss and give feedback, , Next question, , Gastrointestinal stromal tumour, GIST's are not common tumours (10 per million) and originate primarily from the interstitial, pacemaker cells (of Cajal). Up to 70% occur in the stomach, the remainder occurring in the small, intestine (20%) and the colon and rectum (5%). Up to 95% are solitary lesions and most are, sporadic. The vast majority express CD117 which is a transmembrane tyrosine kinase receptor and, in these there is a mutation of the c-KIT gene.
Page 846 :
The goal of surgery is resection of the tumour with a 1-2cm margin of normal tissue. As a result, extensive resections are not required. Unfortunately there is a high local recurrence rate, the risk of, which is related to site, incomplete resections and high mitotic count. Salvage surgery for recurrent, disease is associated with a median survival of 15 months., The prognosis in high risk patients is greatly improved through the use of imatinib, which in the, ACOSOG trial (imatinib vs placebo) improved relapse rates from 17% to 2%., In the UK it is advocated by NICE for use in patients with metastatic disease or locally unresectable, disease., Next question
Page 847 :
Question 22 of 147, A 23 year old man fractures his right tibia in a sporting accident. At which point in the healing, process is fracture callus most likely to be visible radiologically?, , 1 day, , 7 days, , 8 weeks, , 6 weeks, , 3 weeks, , Fracture callus is composed of fibroblasts and chondroblasts and the synthesis of fibrocartilage. It is, typically visible on radiographs approximately 3 weeks following injury. If delayed then there may be, risk of non union., Please rate this question:, , Discuss and give feedback, , Next question, , Fracture healing, Bone fracture, - Bleeding vessels in the bone and periosteum, - Clot and haematoma formation, - The clot organises over a week (improved structure and collagen), - The periosteum contains osteoblasts which produce new bone, - Mesenchymal cells produce cartilage (fibrocartilage and hyaline cartilage) in the soft tissue around, the fracture, - Connective tissue + hyaline cartilage = callus, - As the new bone approaches the new cartilage, endochondral ossification occurs to bridge the gap, - Trabecular bone forms, - Trabecular bone is resorbed by osteoclasts and replaced with compact bone, Factors affecting fracture healing
Page 848 :
, , , , , , , , , , , , , Age, Malnutrition, Bone disorders: osteoporosis, Systemic disorders: diabetes, Marfan's syndrome and Ehlers-Danlos syndrome cause, abnormal musculoskeletal healing., Drugs: steroids, non steroidal anti inflammatory agents., Type of bone: Cancellous (spongy) bone fractures are usually more stable, involve greater, surface areas, and have a better blood supply than cortical (compact) bone fractures., Degree of Trauma: The more extensive the injury to bone and surrounding soft tissue, the, poorer the outcome., Vascular Injury: Especially the femoral head, talus, and scaphoid bones., Degree of Immobilization, Intra-articular Fractures: These fractures communicate with synovial fluid, which contains, collagenases that retard bone healing., Separation of Bone Ends: Normal apposition of fracture fragments is needed for union to, occur. Inadequate reduction, excessive traction, or interposition of soft tissue will prevent, healing., Infection, Next question
Page 851 :
Question 24 of 147, A 23 year old man is reviewed on the ward 10 days following a laparotomy. The wound is inspected, and is healing well. Which of the following processes is least likely to be occurring in the wound at, this stage?, , Angiogenesis, , Synthesis of collagen, , Necrosis of fibroblasts, , Secretion of matrix metalloproteinases by fibroblasts, , Proliferation of fibroblasts, Vasculogenesis vs Angiogenesis, Vascu is new. Angi is pre, Vasculogenesis is new vessels developing in situ from existing mesenchyme., Angiogenesis is vessels develop from sprouting off pre-existing arteries., Fibroblasts are an important cell type in healing wounds. They typically proliferate in the early, phases of wound healing. They release matrix metalloproteinases and these facilitate in the, remodelling of the matrix within the healing wound. Necrosis in a healing wound would be unusual, as wounds will tend to show clinical evidence of angiognesis by this time., Please rate this question:, , Discuss and give feedback, , Next question, , Wound healing, Surgical wounds are either incisional or excisional and either clean, clean contaminated or dirty., Although the stages of wound healing are broadly similar their contributions will vary according to the, wound type., The main stages of wound healing include:
Page 852 :
Haemostasis, , , , Minutes to hours following injury, Vasospasm in adjacent vessels, platelet plug formation and generation of fibrin rich clot., , Inflammation, , , , , , , Typically days 1-5, Neutrophils migrate into wound (function impaired in diabetes)., Growth factors released, including basic fibroblast growth factor and vascular endothelial, growth factor., Fibroblasts replicate within the adjacent matrix and migrate into wound., Macrophages and fibroblasts couple matrix regeneration and clot substitution., , Regeneration, , , , , , Typically days 7 to 56, Platelet derived growth factor and transformation growth factors stimulate fibroblasts and, epithelial cells., Fibroblasts produce a collagen network., Angiogenesis occurs and wound resembles granulation tissue., , Remodeling, , , , , , , From 6 weeks to 1 year, Longest phase of the healing process and may last up to one year (or longer)., During this phase fibroblasts become differentiated (myofibroblasts) and these facilitate, wound contraction., Collagen fibres are remodeled., Microvessels regress leaving a pale scar., , The above description represents an idealised scenario. A number of diseases may distort this, process. Neovascularisation is an important early process. Endothelial cells may proliferate in the, wound bed and recanalise to form a vessel. Vascular disease, shock and sepsis can all compromise, microvascular flow and impair healing., Conditions such as jaundice will impair fibroblast synthetic function and immunity with a detrimental, effect in most parts of the healing process., Problems with scars:, Hypertrophic scars, Excessive amounts of collagen within a scar. Nodules may be present histologically containing, randomly arranged fibrils within and parallel fibres on the surface. The tissue itself is confined to the
Page 853 :
extent of the wound itself and is usually the result of a full thickness dermal injury. They may go on, to develop contractures., Image of hypertrophic scarring. Note that it remains confined to the boundaries of the original, wound:, , Image sourced from Wikipedia, , Keloid scars, Excessive amounts of collagen within a scar. Typically a keloid scar will pass beyond the boundaries, of the original injury. They do not contain nodules and may occur following even trivial injury. They, do not regress over time and may recur following removal., Image of a keloid scar. Note the extension beyond the boundaries of the original incision:
Page 854 :
Image sourced from Wikipedia, , Drugs which impair wound healing:, , , , , , Non steroidal anti inflammatory drugs, Steroids, Immunosupressive agents, Anti neoplastic drugs, , Closure, Delayed primary closure is the anatomically precise closure that is delayed for a few days but before, granulation tissue becomes macroscopically evident., Secondary closure refers to either spontaneous closure or to surgical closure after granulation tissue, has formed., Next question
Page 855 :
Question 25 of 147, A 25 year old women presents with a slowly enlarging mass on the side of the face. Clinical, examination demonstrates that the mass is located in the tail of the parotid gland. There is no, evidence of facial nerve involvement. What is the most likely cause?, , Sialolithiasis, , Adenocarcinoma, , Warthins tumour, , Oncocytoma, , Pleomorphic adenoma, , Pleomorphic adenomas are the commonest tumours of the parotid gland and are often slow, growing, smooth and mobile. Warthins tumours are typically found in elderly males and are, composed of multiple cysts and solid components consisting of lymphoid tissue. Warthins tumours, are most often found in the tail of the parotid gland, but not in 25 year old females, where a, pleomorphic adenoma remains the most likely lesion., Please rate this question:, , Discuss and give feedback, , Next question, , Parotid gland clinical, Benign neoplasms, Up to 80% of all salivary gland tumours occur in the parotid gland and up to 80% of these are, benign. There is no consistent correlation between the rate of growth and the malignant potential of, the lesion. However, benign tumours should not invade structures such as the facial nerve., With the exception of Warthins tumours, they are commoner in women than men. The median age of, developing a lesion is in the 5th decade of life., Benign tumour types, , Tumour type, , Features
Page 856 :
Tumour type, , Features, , Benign pleomorphic adenoma or, benign mixed tumor, , Most common parotid neoplasm (80%), Proliferation of epithelial and myoepithelial cells of the ducts, and an increase in stromal components, Slow growing, lobular, and not well encapsulated, Recurrence rate of 1-5% with appropriate excision, (parotidectomy), Recurrence possibly secondary to capsular disruption during, surgery, Malignant degeneration occurring in 2-10% of adenomas, observed for long periods, with carcinoma ex-pleomorphic, adenoma occurring most frequently as adenocarcinoma, , Warthin tumor (papillary, cystadenoma lymphoma or, adenolymphoma), , Second most common benign parotid tumor (5%), Most common bilateral benign neoplasm of the parotid, Marked male as compared to female predominance, Occurs later in life (sixth and seventh decades), Presents as a lymphocytic infiltrate and cystic epithelial, proliferation, May represent heterotopic salivary gland epithelial tissue, trapped within intraparotid lymph nodes, Incidence of bilaterality and multicentricity of 10%, Malignant transformation rare (almost unheard of), , Monomorphic adenoma, , Account for less than 5% of tumours, Slow growing, Consist of only one morphological cell type (hence term, mono), Include; basal cell adenoma, canalicular adenoma,, oncocytoma, myoepitheliomas, , Haemangioma, , Should be considered in the differential of a parotid mass in a, child, Accounts for 90% of parotid tumours in children less than 1, year of age, Hypervascular on imaging, Spontaneous regression may occur and malignant, transformation is almost unheard of, , Malignant salivary gland tumours
Page 857 :
Types of malignancy, , Mucoepidermoid, carcinoma, , 30% of all parotid malignancies, Usually low potential for local invasiveness and metastasis (depends, mainly on grade), , Adenoid cystic, carcinoma, , Unpredictable growth pattern, Tendency for perineural spread, Nerve growth may display skip lesions resulting in incomplete excision, Distant metastasis more common (visceral rather than nodal spread), 5 year survival 35%, , Mixed tumours, , Often a malignancy occurring in a previously benign parotid lesion, , Acinic cell carcinoma, , Intermediate grade malignancy, May show perineural invasion, Low potential for distant metastasis, 5 year survival 80%, , Adenocarcinoma, , Develops from secretory portion of gland, Risk of regional nodal and distant metastasis, 5 year survival depends upon stage at presentation, may be up to 75%, with small lesions with no nodal involvement, , Lymphoma, , Large rubbery lesion, may occur in association with Warthins tumours, Diagnosis should be based on regional nodal biopsy rather than parotid, resection, Treatment is with chemotherapy (and radiotherapy), , Diagnostic evaluation, , , , , , , , Plain x-rays may be used to exclude calculi, Sialography may be used to delineate ductal anatomy, FNAC is used in most cases, Superficial parotidectomy may be either diagnostic of therapeutic depending upon the nature, of the lesion, Where malignancy is suspected the primary approach should be definitive resection rather, than excisional biopsy, CT/ MRI may be used in cases of malignancy for staging primary disease
Page 858 :
Treatment, For nearly all lesions this consists of surgical resection, for benign disease this will usually consist of, a superficial parotidectomy. For malignant disease a radical or extended radical parotidectomy is, performed. The facial nerve is included in the resection if involved. The need for neck dissection is, determined by the potential for nodal involvement., Other parotid disorders, HIV infection, , , , , Lymphoepithelial cysts associated with HIV occur almost exclusively in the parotid, Typically presents as bilateral, multicystic, symmetrical swelling, Risk of malignant transformation is low and management usually conservative, , Sjogren syndrome, , , , , , , , , Autoimmune disorder characterised by parotid enlargement, xerostomia and, keratoconjunctivitis sicca, 90% of cases occur in females, Second most common connective tissue disorder, Bilateral, non tender enlargement of the gland is usual, Histologically, the usual findings are of a lymphocytic infiltrate in acinar units and, epimyoepithelial islands surrounded by lymphoid stroma, Treatment is supportive, There is an increased risk of subsequent lymphoma, , Sarcoid, , , , , , , Parotid involvement occurs in 6% of patients with sarcoid, Bilateral in most cases, Gland is not tender, Xerostomia may occur, Management of isolated parotid disease is usually conservative, Next question
Page 859 :
Question 26 of 147, Beta-naphthalamine is associated with which of the following malignancies?, , Lung cancer, , Bowel cancer, , Bladder cancer, , Liver cancer, , Renal cancer, , Beta-naphthalamine is used in the rubber industry., The following factors are associated with the development of bladder cancer:, , , , , , smoking, occupational: aniline dyes used in printing and textile industry, rubber manufacture, schistosomiasis, drugs: cyclophosphamide, , Please rate this question:, , Discuss and give feedback, , Next question, , Occupational cancers, Occupational cancers accounted for 5.3% cancer deaths in 2005., In men the main cancers include:, , , , , , Mesothelioma, Bladder cancer, Non melanoma skin cancer, Lung cancer
Page 860 :
, , Sino nasal cancer, , Occupations with high levels of occupational tumours include:, , , , , , , , Construction industry, Working with coal tar and pitch, Mining, Metalworkers, Working with asbestos (accounts for 98% of all mesotheliomas), Working in rubber industry, , Shift work has been linked to breast cancer in women (Health and safety executive report RR595)., The latency between exposure and disease is typically 15 years for solid tumours and 20 for, leukaemia., Many occupational cancers are otherwise rare. For example sino nasal cancer is an uncommon, tumour, 50% will be SCC. They are linked to conditions such as wood dust exposure and unlike lung, cancer is not strongly linked to cigarette smoking. Another typical occupational tumour is, angiosarcoma of the liver which is linked to working with vinyl chloride. Again in the non occupational, context this is an extremely rare sporadic tumour., Next question
Page 861 :
Question 27 of 147, A 56 year old man with Wilsons disease presents with right upper quadrant discomfort. An, ultrasound scan is performed and this demonstrates a mass lesion in the right lobe of the liver. What, is the most appropriate method of establishing the underlying diagnosis?, , PET CT scan, , Ultrasound guided biopsy, , Measurement of serum alpha feto protein, , MRI scan of the liver, , CT scan of the liver, High AFP + chronic liver inflammation = Hepatocellular carcinoma., This is likely to be a hepatocellulcar carcinoma. Diagnosis is usually made by AFP measurement, (with further imaging depending on the result). Biopsy should not be performed as it may seed the, tumour. Chronic liver diseases such as Wilsons disease (Hepato-lenticular degeneration) increase, the risk., Please rate this question:, , Discuss and give feedback, , Next question, , Liver tumours, Primary liver tumours, The most common primary tumours are cholangiocarcinoma and hepatocellular carcinoma. Overall, metastatic disease accounts for 95% of all liver malignancies making the primary liver tumours, comparatively rare., Primary liver tumours include:, , , , , Cholangiocarcinoma, Hepatocellular carcinoma, Hepatoblastoma
Page 862 :
, , , , Sarcomas (Rare), Lymphomas, Carcinoids (most often secondary although primary may occur), , Hepatocellular carcinoma, These account for the bulk of primary liver tumours (75% cases). Its worldwide incidence reflects its, propensity to occur on a background of chronic inflammatory activity. Most cases arise in cirrhotic, livers or those with chronic hepatitis B infection, especially where viral replication is actively, occurring. In the UK it accounts for less than 5% of all cancers, although in parts of Asia its, incidence is 100 per 100,000., The majority of patients (80%) present with existing liver cirrhosis, with a mass discovered on, screening ultrasound., Diagnosis, , , , , , CT/ MRI (usually both) are the imaging modalities of choice, a-fetoprotein is elevated in almost all cases, Biopsy should be avoided as it seeds tumours cells through a resection plane., In cases of diagnostic doubt serial CT and αFP measurements are the preferred strategy., , Treatment, , , , , , , Patients should be staged with liver MRI and chest, abdomen and pelvic CT scan., The testis should be examined in males (testicular tumours may cause raised AFP). PET CT, may be used to identify occult nodal disease., Surgical resection is the mainstay of treatment in operable cases. In patients with a small, primary tumour in a cirrhotic liver whose primary disease process is controlled, consideration, may be given to primary whole liver resection and transplantation., Liver resections are an option but since most cases occur in an already diseased liver the, operative risks and post-operative hepatic dysfunction are far greater than is seen following, metastectomy., These tumours are not particularly chemo or radiosensitive however, both may be used in a, palliative setting. Tumour ablation is a more popular strategy., , Survival, Poor, overall survival is 15% at 5 years., Cholangiocarcinoma, This is the second most common type of primary liver malignancy. As its name suggests these, tumours arise in the bile ducts. Up to 80% of tumours arise in the extra hepatic biliary tree. Most, patients present with jaundice and by this stage the majority will have disease that is not resectable., Primary sclerosing cholangitis is the main risk factor. In deprived countries typhoid and liver flukes, are also major risk factors., Diagnosis
Page 863 :
, , , , Patients will typically have an obstructive picture on liver function tests., CA 19-9, CEA and CA 125 are often elevated, CT/ MRI and MRCP are the imaging methods of choice., , Treatment, , , , Surgical resection offers the best chance of cure. Local invasion of peri hilar tumours is a, particular problem and this coupled with lobar atrophy will often contra indicate surgical, resection., Palliation of jaundice is important, although metallic stents should be avoided in those, considered for resection., , Survival, Is poor, approximately 5-10% 5 year survival., Next question
Page 864 :
Question 28 of 147, A 55 year old man has suffered from reflux oesophagitis for many years. During a recent endoscopy, a biopsy is taken from the distal oesophagus. The histopathology report indicates that cells are, identified with features of coarse chromatin and abnormal mitoses. The cells are confined to the, superficial epithelial layer only. Which of the following accounts for this process?, , Metaplasia, , Apoptosis, , Autoimmune oesophagitis, , Dysplasia, , Infection with Helicobacter pylori, Dysplasia = pre cancerous, Dysplasia tends to develop as a result of prolonged stimulation by precipitants. Removal of these, precipitants may possibly reverse these changes. Replacement of differentiated cells with another, cell type describes metaplasia rather than dysplasia. The absence of invasion distinguishes this from, malignancy., Please rate this question:, , Discuss and give feedback, , Next question, , Dysplasia, , , , , , , , , Premalignant condition, Disordered growth and differentiation of cells, Alteration in size, shape, and organization of cells, Features increased abnormal cell growth (increased number of mitoses/abnormal mitoses, and cellular differentiation), Underlying connective tissue is not invaded, Causes include smoking, Helicobacter pylori, Human papilloma virus, Main differences to metaplasia is that dysplasia is considered to be part of carcinogenesis, (pre cancerous) and is associated with a delay in maturation of cells rather than, differentiated cells replacing one another
Page 866 :
Question 29 of 147, Which one of the following confers the least risk of developing osteoporosis?, , Obesity, , Long term unfractionated heparin therapy, , Gastrectomy, , Osteogenesis imperfecta, , Diabetes, , Low body weight is a risk factor for osteoporosis., Please rate this question:, , Discuss and give feedback, , Next question, , Osteoporosis, Risk factors, , , , , , , , , , , Family history, Female sex, Increasing age, Deficient diet, Sedentary lifestyle, Smoking, Premature menopause, Low body weight, Caucasians and Asians, , Diseases which predispose
Page 868 :
Question 30 of 147, , A 63 year old man has a history of claudication that has been present for many years. He is recently, evaluated in the clinic and a duplex scan shows that he has an 85% stenosis of the superficial, femoral artery. Two weeks later he presents with a 1 hour history of severe pain in his leg. On, examination he has absent pulses in the affected limb and it is much cooler than the contra-lateral, limb. Which process best accounts for this presentation?, , Thrombosis, , Embolus, , Atheroma growth, , Sub intimal dissection, , Anaemia, , Theme from April 2012 Exam, In an existing lesion a complication such as thrombosis is more likely than embolus. These patients, should receive heparin and imaging with duplex scanning. Whilst an early surgical bypass or intraarterial thrombolysis may be indicated, an embolectomy should not generally be performed as the, lesion is not an embolus and the operation therefore ineffective., Please rate this question:, , Discuss and give feedback, , Next question, , Claudication
Page 869 :
Claudication is a condition in which patients develop pain in a limb during periods of exercise. The, underlying disorder is usually that of arterial insufficiency. Atheroma develops in the arterial wall and, once this occludes >50-75% of the lumenal diameter the supply to metabolising tissues distally may, become compromised. The typical claudicant complains of calf pain that is worse on exercise and, relieved by rest. This typical description assumes that the SFA is the site of disease, more proximal, disease may present with other symptoms such as buttock claudication and impotence., The history is usually a progressive one, patients presenting as an emergency with severe pain,, diminished sensation, pallor and absent pulses have critical limb ischaemia. This may complicate, claudication and usually indicates a plaque related complication, such as thrombosis., Risk factors, Risk factors for claudication include smoking, diabetes and hyperlipidaemia., Diagnosis, Diagnostic work -up includes measurement of ankle- brachial pressure indices, duplex scanning and, formal angiography., Treatment, Those with long claudication distances, no ulceration or gangrene may be managed conservatively., Patients with rest pain, ulceration or gangrene will almost always require intervention. All patients, should receive an antiplatelet agent and a statin unless there are compelling contra-indications., Next question
Page 870 :
Question 31 of 147, The following are true of carcinoid tumours except:, , When present in the appendix tip and measure less than 2 cm have an excellent prognosis, , Even when metastatic disease is present it tends to follow a protracted course, , When present in the appendix body tend to present with carcinoid syndrome even when, liver metastases are not present, May be imaged using 5 HIAA radionucleotide scanning, , Advanced appendiceal carcinoids may require right hemicolectomy, Rule of thirds:, 1/3 multiple, 1/3 small bowel, 1/3 metastasize, 1/3 second tumour, Liver metastases are necessary for the presence of carcinoid syndrome., Please rate this question:, , Discuss and give feedback, , Next question, , Carcinoid syndrome, , , , , , Carcinoid tumours secrete serotonin, Originate in neuroendocrine cells mainly in the intestine (midgut-distal ileum/appendix), Can occur in the rectum, bronchi, Hormonal symptoms mainly occur when disease spreads outside the bowel, , Clinical features, , , Onset: insidious over many years
Page 871 :
, , , , , , Flushing face, Palpitations, Pulmonary valve stenosis and tricuspid regurgitation causing dyspnoea, Asthma, Severe diarrhoea (secretory, persists despite fasting), , Investigation, , , , , , 5-HIAA in a 24-hour urine collection, Somatostatin receptor scintigraphy, CT scan, Blood testing for chromogranin A, , Treatment, , , , Octreotide, Surgical removal, Next question
Page 872 :
Question 32 of 147, During a difficult femoro-popliteal bypass operation the surgeon inadvertently places a clamp across, the femoral nerve. It remains there for most of the procedure. At the end of the operation the nerve is, inspected, it is in continuity but has evidence of being crushed. Which of the following is most likely, to occur over the following months?, , Wallerian degeneration, , Rapid restoration of neuronal function because the axon itself is intact, , Normal but delayed neuronal transmission due to disruption of the myelin, , Absence of neuroma formation, , None of the above, , A neuronal injury such as this will result in Wallerian degeneration even though the nerve remains in, continuity. Neuromas may well form., Please rate this question:, , Discuss and give feedback, , Next question, , Nerve injury, There are 3 types of nerve injury:, , Neuropraxia, , , , , , , Nerve intact but electrical conduction is affected, Full recovery, Autonomic function preserved, Wallerian degeneration does not occur, , Axonotmesis, , , , Axon is damaged and the myelin sheath is preserved. The connective tissue, framework is not affected., Wallerian degeneration occurs., ,
Page 873 :
Neurotmesis, , , , , Disruption of the axon, myelin sheath and surrounding connective tissue., Wallerian degeneration occurs., , Wallerian Degeneration, , , , , , Axonal degeneration distal to the site of injury., Typically begins 24-36 hours following injury., Axons are excitable prior to degeneration occurring., Myelin sheath degenerates and is phagocytosed by tissue macrophages., , Nerve repair, , , Neuronal repair may only occur physiologically where nerves are in direct contact. Where a, large defect is present, the process of nerve regeneration is hampered. It may not occur at, all or result in the formation of a neuroma. Where nerve regrowth occurs it is typically at a, rate of 1mm per day., Next question
Page 874 :
Question 33 of 147, , A 38 year old lady who smokes heavily presents with recurrent episodes of infection in the right, breast. On examination she has an indurated area at the lateral aspect of the nipple areaolar, complex. Imaging shows no mass lesions. What is the most likely diagnosis?, , Duct ectasia, , Periductal mastitis, , Pagets disease of the nipple, , Mondors disease of the breast, , Radial scar, , Periductal mastitis is common in smokers and may present with recurrent infections. Treatment is, with co-amoxyclav. Mondors disease of the breast is a localised thrombophlebitis of a breast vein., Please rate this question:, , Discuss and give feedback, , Next question, , Duct ectasia, Duct ectasia is a dilatation and shortening of the terminal breast ducts within 3cm of the nipple. It is, common and the incidence increases with age. It typically presents with nipple retraction and, occasionally creamy nipple discharge. It may be confused with periductal mastitis, which presents in, younger women, the vast majority of which are smokers. Periductal mastitis typically presents with, periareolar or sub areolar infections and may be recurrent.
Page 875 :
Patients with troublesome nipple discharge may be treated by microdochectomy (if young) or total, duct excision (if older)., Next question
Page 876 :
Question 34 of 147, Which of the following statements relating to chronic inflammation is true?, , Chronic inflammation is mainly secondary to acute inflammation, , Neutrophils are the predominant cells involved, , Growth factors are not involved in the process, , Appendicitis is mainly a form of chronic inflammation, , Fibrosis is a macroscopic feature, , Macroscopic features include:, , , , , Ulcers, Fibrosis, Granulomatous process, , It most commonly occurs as a primary event rather than as a result of acute inflammation., Please rate this question:, , Discuss and give feedback, , Next question, , Chronic inflammation, Overview, Chronic inflammation may occur secondary to acute inflammation.In most cases chronic, inflammation occurs as a primary process. These may be broadly viewed as being one of three main, processes:, , , , Persisting infection with certain organisms such as Mycobacterium tuberculosis which results, in delayed type hypersensitivity reactions and inflammation., Prolonged exposure to non-biodegradable substances such as silica or suture materials, which may induce an inflammatory response.
Page 877 :
, , Autoimmune conditions involving antibodies formed against host antigens., , Acute vs. Chronic inflammation, , Acute inflammation, , Chronic inflammation, , Changes to existing vascular structure and increased, permeability of endothelial cells, , Angiogenesis predominates, , Infiltration of neutrophils, , Macrophages, plasma cells and, lymphocytes predominate, , Process may resolve with:, , Healing by fibrosis is the main result, , , , , , , , Suppuration, Complete resolution, Abscess formation, Progression to chronic inflammation, Healing by fibrosis, , Granulomatous inflammation, A granuloma consists of a microscopic aggregation of macrophages (with epithelial type, arrangement =epitheliod). Large giant cells may be found at the periphery of granulomas., Mediators, Growth factors released by activated macrophages include agents such as interferon and fibroblast, growth factor (plus many more). Some of these such as interferons may have systemic features, resulting in systemic symptoms and signs, which may be present in individuals with long standing, chronic inflammation., The finding of granulomas is pathognomonic of chronic inflammation, as illustrated in this biopsy, from a patient with colonic Crohns disease
Page 878 :
Image sourced from Wikipedia, , Next question
Page 879 :
1/3, Question 35-37 of 147, , Theme: Paediatric ano-rectal disorders, , A. Ulcerative colitis, B. Juvenile polyps, C. Haemorroids, D. Intussceception, E. Rectal cancer, F. Anal fissure, G. Arteriovenous malformation, , Please select the most likely cause for the condition described. Each option may be used once,, more than once or not at all., , 35., , A 4 year old boy is brought to the clinic. He gives a history of difficult, painful defecation with, bright red rectal bleeding., You answered Ulcerative colitis, The correct answer is Anal fissure, Theme from April 2012 Exam, Painful rectal bleeding in this age group is typically due to a fissure. Treatment should include, stool softeners and lifestyle advice., , 36., , A 2 year old has a history of rectal bleeding. The parents notice that post defecation, a cherry red, lesion is present at the anal verge., You answered Ulcerative colitis
Page 880 :
The correct answer is Juvenile polyps, Theme from September 2012 Exam, These lesions are usually hamartomas and this accounts for the colour of the lesions. Although, the lesions are not themselves malignant they serve as a marker of an underlying polyposis, disorder., , 37., , A 12 year old is brought to the colorectal clinic with a history of rectal bleeding, altered bowel, habit, weight loss and malaise. Abdominal examination is normal., Ulcerative colitis, The systemic features in the history are strongly suggestive of inflammatory bowel disease rather, than the other causes., , Please rate this question:, , Discuss and give feedback, , Next question, , Paediatric proctology, Children may present with altered bowel habit and/ or rectal bleeding. Classical haemorroidal, disease is relatively rare in children. Painful bright red rectal bleeding is much more common since, constipation is a relatively common childhood disorder. The hard stool causes a tear of the anorectal mucosa with subsequent fissure. The pain from the fissure must be addressed promptly or the, child will delay defecation and this fissure will worsen., Inflammatory bowel disease may present in a similar pattern in paediatric practice with altered bowel, habit (usually diarrhoea) and bleeding. Systemic features may be present and investigation with an, endoscopy may be required., Children with intussceception usually present at a relatively young age and the history is usually one, of colicky abdominal pain, together with a mass on clinical examination.The often cited red current, jelly type stool is a rare but classical feature.
Page 881 :
Juvenile polyps may occur as part of the familial polyposis coli syndromes. The lesions, which are, hamartomas, are often cherry red if they protrude externally., Next question
Page 882 :
Question 38 of 147, You review a 42-year-old woman 8 months following a renal transplant for focal segmental, glomerulosclerosis. She is on a combination of tacrolimus, mycophenolate, and prednisolone. She, has now presented with a five day history of feeling generally unwell with jaundice, fatigue and, arthralgia. On examination she has jaundice, widespread lymphadenopathy and hepatomegaly., What is the most likely diagnosis?, , Hepatitis C, , Epstein-Barr virus, , HIV, , Hepatitis B, , Cytomegalovirus, Post transplant complications, CMV: 4 weeks to 6 months post transplant, EBV: post transplant lymphoproliferative disease. > 6 months post transplant, Post transplant lymphoproliferative disorder is most commonly associated with Epstein-Barr virus. It, typically occurs 6 months post transplant and is associated with high dose immunosupressant, therapy. Remember cytomegalovirus presents within the first 4 weeks to 6 months post transplant., Please rate this question:, , Discuss and give feedback, , Next question, , Renal transplant:HLA typing and graft failure, The human leucocyte antigen (HLA) system is the name given to the major histocompatibility, complex (MHC) in humans. It is coded for on chromosome 6., Some basic points on the HLA system
Page 883 :
, , , Class 1 antigens include A, B and C. Class 2 antigens include DP,DQ and DR, When HLA matching for a renal transplant the relative importance of the HLA antigens are as, follows DR > B > A, , Graft survival, , , , 1 year = 90%, 10 years = 60% for cadaveric transplants, 1 year = 95%, 10 years = 70% for living-donor transplants, , Post-op problems, , , , , , ATN of graft, Vascular thrombosis, Urine leakage, UTI, , Hyperacute acute rejection, , , , Due to antibodies against donor HLA type 1 antigens, Rarely seen due to HLA matching, , Acute graft failure (< 6 months), , , , , Usually due to mismatched HLA, Other causes include cytomegalovirus infection, Management: give steroids, if resistant use monoclonal antibodies, , Causes of chronic graft failure (> 6 months), , , , , Chronic allograft nephropathy, Ureteric obstruction, Recurrence of original renal disease (MCGN > IgA > FSGS), Next question
Page 884 :
Question 39 of 147, Which of the following processes facilitates phagocytosis?, , Apoptosis, , Opsonisation, , Proteolysis, , Angiogenesis, , Necrosis, , Theme from September 2014 Exam, Opsonisation will facilitate phagocytosis. The micro-organism becomes coated with antibody, C3b, and certain acute phase proteins. The macrophages and neutrophils have up regulation of, phagocytic cell surface receptors in these circumstances, a process mediated by pro-inflammatory, cytokines. These cells then engulf the micro organism., Please rate this question:, , Discuss and give feedback, , Next question, , Phagocytosis, , , , , , , Ingestion of pathogens or foreign materials by cells, First step is opsonisation whereby the organism is coated by antibody, Second step is adhesion to cell surface, Third step is pseudopodial extension to form a phagocytic vacuole, Lysosomes fuse with vacuole and degrade contents, Next question
Page 885 :
Question 40 of 147, , Features which are evaluated for the grading of breast cancer include all the following, except:, , Tubule formation, , Mitoses, , Nuclear pleomorphism, , Tumour necrosis, , Coarse chromatin, , The necrosis of a tumour may be suggestive of a high grade tumour which has out grown its blood, supply. However, the grading of breast cancer which classically follows the Bloom -Richardson, grading model will tend to favor nuclear appearances (which include mitoses, coarse chromatin and, pleomorphism). Tubule formation is an important marker of the degree of differentiation with, formation of tubular structures being associated with well differentiated tumours., Please rate this question:, , Discuss and give feedback, , Next question, , Tumour grading, Tumours may be graded according to their degree of differentiation, mitotic activity and other, features. Grade 1 tumours are the most differentiated and grade 3 or 4 the least. The assessment is, subjective, in most cases high grade equates to poor prognosis, or at least rapid growth., Tumours of glandular epithelium will tend to arrange themselves into acinar type structures
Page 886 :
containing a central lumen. Well differentiated tumours may show excellent acinar formation and, poorly differentiated tumours simply clumps of cells around a desmoplastic stroma. Sometimes, tumours demonstrate mucous production without evidence of acinar formation. Since mucous, production is evidence of a glandular function such tumours are often termed mucinous, adenocarcinoma., Squamous cell tumours will typically produce structures resembling epithelial cell components. Well, differentiated tumours may also produce keratin (depending upon tissue of origin)., Next question
Page 887 :
Question 41 of 147, , A 34 year old man is diagnosed with an aggressive caecal adenocarcinoma. His sister died from the, same disease at 38 years of age. His mother died from endometrial cancer at the age of 41. What is, the most likely underlying abnormality?, , Familial adenopolypomatosis coli, , Gardeners syndrome, , Mutation of mismatch repair genes, , Deletion of chromosome 6, , MYH gene mutation, , Lynch syndrome which is characterised by aggressive right sided colonic malignancy and, endometrial cancer is caused by microsatellite instability of DNA repair genes., Please rate this question:, , Discuss and give feedback, , Next question, , Genetics of colorectal cancer, The lifetime risk of colorectal cancer in the UK population is 5%. Up to 5% of newly diagnosed bowel, cancers will be in those individuals who have a high genetically acquired risk of bowel cancer., Cancers arising in the low-moderate genetic risk group comprise approximately 30% of newly, diagnosed bowel cancer.
Page 889 :
pathway., HNPCC (Lynch syndrome), HNPCC cancers differ from conventional tumours in a number of respects. In the colon the tumours, are more likely to be right sided, histologically they are more likely to be mucinous and have dense, lymphocytic infiltrates. To be diagnosed as having HNPCC individuals must show typically HNPCC, tumours in at least three individuals, (one of whom must be a first degree relative to the other two)., In at least two successive generations. At least one cancer must be diagnosed under the age of 50., FAP must be excluded and tumours should be verified by pathological identification (Amsterdam, criteria). The genetic changes in HNPCC stem primarily from microsatellite instability affecting DNA, mismatch repair genes. In HNPCC the mismatch repair genes most commonly implicated include;, MSH2 and MLH1 and these occur in up to 70% of people with HNPCC. The finding of microsatellite, instability is unusual in sporadic colorectal cancers. Approximately 60% of individuals who fulfill the, Amsterdam criteria will not be found to have evidence of mismatch repair gene defects on genetic, testing. The risk of developing colorectal cancer in those who have not demonstrated mutation of the, mis match repair genes is increased if they fulfill the Amsterdam criteria, but not, the extent that it is increased in those who fulfill the criteria AND have evidence of mis match repair, gene defects., KRAS Mutations, The RAS family of small G proteins act as molecular switches downstream of growth factor, receptors. KRAS and the other two members of the family; HRAS and NRAS, are the site of, mutation in approximately 40% of colorectal cancers. When adenomas are examined the proportion, of adenomas less than 1cm showing KRAS mutations was only 10% which contrasts with 50% in, those lesions greater than 1cm., p53 mutations, The p53 protein functions as a key transcriptional regulator of genes that encode proteins with, functions in cell-cycle checkpoints at the G1/S and G2/M boundaries, in promoting apoptosis, and in, restricting angiogenesis . As such, selection for p53 defects at the adenoma-carcinoma transition, may reflect the fact that stresses on tumor cells activate cell-cycle arrest, apoptotic, and, antiangiogenic pathways in cells with wild-type p53 function. Many colonic tumours will demonstrate, changes in the p53 gene that may facilitate tumour progression through from adenoma to, carcinoma., Cowden syndrome, Also known as multiple hamartoma syndrome. Rare autosomal dominant condition with incidence of, 1 in 200,000.. It is characterised by multiple mucocutaneous lesions, trichilemmomas, oral, papillomas and acral keratosis. Most often diagnosed in third decade of life. Breast carcinoma may, occur in up to 50% of patients and conditions such as fibrocystic disease of the breast may occur in, 75% of women. Thyroid disease occurs in 75% and may include malignancy. Endoscopic screening, will identify disease in up to 85% although the small bowel is rarely involved. There is a 15-20% risk, of developing colorectal cancer and regular colonoscopic screening from age 45 is recommended., Terminology
Page 890 :
Oncogene, , Oncogenes are genes which have the potential to induce cellular proliferation and avoid, apoptosis. Oncogene mutations are general gain of function and are therefore, dominant. Increased expression of oncogenes are found in most tumours, , Tumour, suppressor, gene, , These genes generally inhibit cellular proliferation or induce apoptosis. Mutations in, tumour suppressor genes are generally loss of function mutations, and are therefore, recessive. Mutations in both tumour suppressor gene alleles allow cells to proliferate, without restraint, , References, 1. Fearon, E.R. and B. Vogelstein, A genetic model for colorectal tumorigenesis. Cell, 1990. 61(5): p., 759-67., Next question
Page 891 :
Question 42 of 147, Which of the following is associated with poor wound healing?, , Jaundice, , Patients taking carbamazepine, , General anaesthesia using thiopentone, , General anaesthesia using ketamine, , Multiple sclerosis, Mnemonic to remember factors affecting wound healing: DID NOT HEAL, D iabetes, I nfection, irradiation, D rugs eg steroids, chemotherapy, N utritional deficiencies (vitamin A, C & zinc, manganese), Neoplasia, O bject (foreign material), T issue necrosis, H ypoxia, E xcess tension on wound, A nother wound, L ow temperature, Liver jaundice, Multiple sclerosis is associated with pressure sores, however the cellular healing process is not, affected., Please rate this question:, , Discuss and give feedback, , Next question, , Wound healing, Surgical wounds are either incisional or excisional and either clean, clean contaminated or dirty., Although the stages of wound healing are broadly similar their contributions will vary according to the
Page 892 :
wound type., The main stages of wound healing include:, Haemostasis, , , , Minutes to hours following injury, Vasospasm in adjacent vessels, platelet plug formation and generation of fibrin rich clot., , Inflammation, , , , , , , Typically days 1-5, Neutrophils migrate into wound (function impaired in diabetes)., Growth factors released, including basic fibroblast growth factor and vascular endothelial, growth factor., Fibroblasts replicate within the adjacent matrix and migrate into wound., Macrophages and fibroblasts couple matrix regeneration and clot substitution., , Regeneration, , , , , , Typically days 7 to 56, Platelet derived growth factor and transformation growth factors stimulate fibroblasts and, epithelial cells., Fibroblasts produce a collagen network., Angiogenesis occurs and wound resembles granulation tissue., , Remodeling, , , , , , , From 6 weeks to 1 year, Longest phase of the healing process and may last up to one year (or longer)., During this phase fibroblasts become differentiated (myofibroblasts) and these facilitate, wound contraction., Collagen fibres are remodeled., Microvessels regress leaving a pale scar., , The above description represents an idealised scenario. A number of diseases may distort this, process. Neovascularisation is an important early process. Endothelial cells may proliferate in the, wound bed and recanalise to form a vessel. Vascular disease, shock and sepsis can all compromise, microvascular flow and impair healing., Conditions such as jaundice will impair fibroblast synthetic function and immunity with a detrimental, effect in most parts of the healing process., Problems with scars:
Page 893 :
Hypertrophic scars, Excessive amounts of collagen within a scar. Nodules may be present histologically containing, randomly arranged fibrils within and parallel fibres on the surface. The tissue itself is confined to the, extent of the wound itself and is usually the result of a full thickness dermal injury. They may go on, to develop contractures., Image of hypertrophic scarring. Note that it remains confined to the boundaries of the original, wound:, , Image sourced from Wikipedia, , Keloid scars, Excessive amounts of collagen within a scar. Typically a keloid scar will pass beyond the boundaries, of the original injury. They do not contain nodules and may occur following even trivial injury. They, do not regress over time and may recur following removal., Image of a keloid scar. Note the extension beyond the boundaries of the original incision:
Page 894 :
Image sourced from Wikipedia, , Drugs which impair wound healing:, , , , , , Non steroidal anti inflammatory drugs, Steroids, Immunosupressive agents, Anti neoplastic drugs, , Closure, Delayed primary closure is the anatomically precise closure that is delayed for a few days but before, granulation tissue becomes macroscopically evident., Secondary closure refers to either spontaneous closure or to surgical closure after granulation tissue, has formed., Next question
Page 895 :
Question 43 of 147, , A 55 year old man undergoes a colonoscopy and a colonic polyp is identified. It has a lobular, appearance and is located on a stalk in the sigmoid colon. Which of the processes below best, accounts for this disease?, , Apoptosis, , Metaplasia, , Dysplasia, , Calcification, , Degeneration, , Theme from April 2012 Exam, Most colonic polyps described above are adenomas. These may have associated dysplasia. The, more high grade the dysplasia the greater the level of clinical concern., Please rate this question:, , Discuss and give feedback, , Next question, , Colonic polyps, Colonic Polyps, May occur in isolation, or greater numbers as part of the polyposis syndromes. In FAP greater than, 100 polyps are typically present. The risk of malignancy in association with adenomas is related to, size, and is the order of 10% in a 1cm adenoma. Isolated adenomas seldom give risk of symptoms
Page 896 :
(unless large and distal). Distally sited villous lesions may produce mucous and if very large,, electrolyte disturbances may occur., Follow up of colonic polyps, , Group, , Features, , Action, , Low risk, , 1 or 2 adenomas less than 1cm, , No follow up or re-colonoscopy, at 5 years, , Moderate, risk, , 3 or 4 small adenomas or 1 adenoma greater than 1cm, , Re-scope at 3 years, , High risk, , More than 5 small adenomas or more than 3 with 1 of, them greater than 1cm, , Re scope at 1 year, , From Atkins and Saunders Gut 2002 51 (suppl V:V6-V9). It is important to stratify patients, appropriately and ensure that a complete colonoscopy with good views was performed., Segmental resection or complete colectomy should be considered when:, 1. Incomplete excision of malignant polyp, 2. Malignant sessile polyp, 3. Malignant pedunculated polyp with submucosal invasion, 4. Polyps with poorly differentiated carcinoma, 5. Familial polyposis coli, -Screening from teenager up to 40 years by 2 yearly sigmoidoscopy/colonoscopy, -Panproctocolectomy and Ileostomy or Restorative Panproctocolectomy., Rectal polypoidal lesions may be amenable to trans anal endoscopic microsurgery., References, Cairns S et al. Guidelines for colorectal cancer screening and surveillance in moderate and high risk, groups (update from 2002). Gut 2010;59:666-690., Next question
Page 897 :
Question 44 of 147, , A 56 year old lady has just undergone a colonoscopy and a 1.5cm lesion was identified in the, caecum. The histology report states that biopsies have been taken from a sessile serrated polyp with, traditional features. What is the best management option?, , Perform a right hemicolectomy, , List the patient for colonoscopic polypectomy, , Discharge the patient, , Re scope the patient in 6 months, , Re scope the patient at 3 years, , These polyps represent an alternative pathway to progression to carcinoma and may be, diagnostically confused with hyperplastic polyps. Hyperplastic polyps are more common in the left, colon and confer no increased risk. SSA's are more common in the right colon and are usually, larger. Those with "traditional features" on histology have dysplasia with increased risk of malignant, transformation., Please rate this question:, , Discuss and give feedback, , Next question, , Colonic polyps, Colonic Polyps, May occur in isolation, or greater numbers as part of the polyposis syndromes. In FAP greater than
Page 898 :
100 polyps are typically present. The risk of malignancy in association with adenomas is related to, size, and is the order of 10% in a 1cm adenoma. Isolated adenomas seldom give risk of symptoms, (unless large and distal). Distally sited villous lesions may produce mucous and if very large,, electrolyte disturbances may occur., Follow up of colonic polyps, , Group, , Features, , Action, , Low risk, , 1 or 2 adenomas less than 1cm, , No follow up or re-colonoscopy, at 5 years, , Moderate, risk, , 3 or 4 small adenomas or 1 adenoma greater than 1cm, , Re-scope at 3 years, , High risk, , More than 5 small adenomas or more than 3 with 1 of, them greater than 1cm, , Re scope at 1 year, , From Atkins and Saunders Gut 2002 51 (suppl V:V6-V9). It is important to stratify patients, appropriately and ensure that a complete colonoscopy with good views was performed., Segmental resection or complete colectomy should be considered when:, 1. Incomplete excision of malignant polyp, 2. Malignant sessile polyp, 3. Malignant pedunculated polyp with submucosal invasion, 4. Polyps with poorly differentiated carcinoma, 5. Familial polyposis coli, -Screening from teenager up to 40 years by 2 yearly sigmoidoscopy/colonoscopy, -Panproctocolectomy and Ileostomy or Restorative Panproctocolectomy., Rectal polypoidal lesions may be amenable to trans anal endoscopic microsurgery., References, Cairns S et al. Guidelines for colorectal cancer screening and surveillance in moderate and high risk, groups (update from 2002). Gut 2010;59:666-690., Next question
Page 899 :
Question 45 of 147, A 30 year old male presents with gynaecomastia. Clinically, he is noted to have a nodule in the left, testis. What is the most likely diagnosis?, , Oestrogen abuse, , Seminoma with syncytiotrophoblast giant cells, , Teratoma, , Choriocarcinoma, , Leydig cell tumour, , Leydig cell tumours are rare testicular sex cord stromal tumours (which also include sertoli cell, tumours) which are associated with hormonal activity., , , , , Patients with Leydig cell tumours may present with gynaecomastia before they notice, testicular enlargement., Majority are benign, Histology: eosinophilic cells in columns, , Please rate this question:, , Discuss and give feedback, , Next question, , Testicular disorders, Testicular cancer, Testicular cancer is the most common malignancy in men aged 20-30 years. Around 95% of cases, of testicular cancer are germ-cell tumours. Germ cell tumours may essentially be divided into:, , Tumour type, , Key features, , Tumour, markers, , Pathology
Page 900 :
Tumour type, , Seminoma, , Tumour, markers, , Pathology, , Commonest, subtype (50%), Average age at, diagnosis = 40, Even advanced, disease associated, with 5 year, survival of 73%, , AFP usually, normal, HCG elevated, in 10%, seminomas, Lactate, dehydrogenase;, elevated in 1020% seminomas, (but also in many, other conditions), , Sheet like lobular, patterns of cells, with substantial, fibrous, component., Fibrous septa, contain, lymphocytic, inclusions and, granulomas may, be seen., , Younger age at, presentation =20-30, years, Advanced disease, carries worse prognosis, (48% at 5 years), Retroperitoneal lymph, node dissection may be, needed for residual, disease after, chemotherapy, , AFP elevated, in up to 70% of, cases, HCG elevated, in up to 40% of, cases, Other markers, rarely helpful, , Heterogenous, texture with, occasional ectopic, tissue such as hair, , Key features, , , , , Non seminomatous germ, cell tumours (42%), , , , , , Teratoma, Yolk sac tumour, Choriocarcinoma, Mixed germ cell, tumours (10%), , Image demonstrating a classical seminoma, these tumours are typically more uniform than, teratomas
Page 901 :
Image sourced from Wikipedia, , Risk factors for testicular cancer, , , , , , , Cryptorchidism, Infertility, Family history, Klinefelter's syndrome, Mumps orchitis, , Features
Page 902 :
, , , , A painless lump is the most common presenting symptom, Pain may also be present in a minority of men, Other possible features include hydrocele, gynaecomastia, , Diagnosis, , , , , Ultrasound is first-line, CT scanning of the chest/ abdomen and pelvis is used for staging, Tumour markers (see above) should be measured, , Management, , , , , Orchidectomy (Inguinal approach), Chemotherapy and radiotherapy may be given depending on staging, Abdominal lesions >1cm following chemotherapy may require retroperitoneal lymph node, dissection., , Prognosis is generally excellent, , , , 5 year survival for seminomas is around 95% if Stage I, 5 year survival for teratomas is around 85% if Stage I, , Benign disease, Epididymo-orchitis, Acute epididymitis is an acute inflammation of the epididymis, often involving the testis and usually, caused by bacterial infection., , , , , Infection spreads from the urethra or bladder. In men <35 years, gonorrhoea or chlamydia, are the usual infections., Amiodarone is a recognised non infective cause of epididymitis, which resolves on stopping, the drug., Tenderness is usually confined to the epididymis, which may facilitate differentiating it from, torsion where pain usually affects the entire testis., , Testicular torsion, , , , , , Twist of the spermatic cord resulting in testicular ischaemia and necrosis., Most common in males aged between 10 and 30 (peak incidence 13-15 years), Pain is usually severe and of sudden onset., Cremasteric reflex is lost and elevation of the testis does not ease the pain.
Page 903 :
, , Treatment is with surgical exploration. If a torted testis is identified then both testis should be, fixed as the condition of bell clapper testis is often bilateral., , Hydrocele, , , , , , , Presents as a mass that transilluminates, usually possible to "get above" it on examination., In younger men it should be investigated with USS to exclude tumour., In children it may occur as a result of a patent processus vaginalis., Treatment in adults is with a Lords or Jabouley procedure., Treatment in children is with trans inguinal ligation of PPV., Next question
Page 904 :
Question 46 of 147, What is the most common cause of osteolytic bone metastasis in children?, , Osteosarcoma, , Neuroblastoma, , Leukaemia, , Rhabdomyosarcoma, , Nephroblastoma, , Neuroblastomas are a relatively common childhood tumour and have a strong tendency to, developing widespread lytic metastasis., Please rate this question:, , Discuss and give feedback, , Next question, , Secondary malignant tumours of bone, Metastatic lesions affecting bone are more common than primary bone tumours., The typical tumours that spread to bone include:, , , , , , , Breast, Bronchus, Renal, Thyroid, Prostate, , 75% cases will affect those over the age of 50, The commonest bone sites affected are:
Page 905 :
, , , , , , , Vertebrae (usually thoracic), Proximal femur, Ribs, Sternum, Pelvis, Skull, , Pathological fracture, Osteolytic lesions are the greatest risk for pathological fracture, The risk and load required to produce fracture varies according to bone site. Bones with lesions that, occupy 50% or less will be prone to fracture under loading (Harrington). When 75% of the bone is, affected the process of torsion about a bony fulcrum may produce a fracture., The Mirel scoring[1] system may be used to help determine the risk of fracture and is more, systematic than the Harrington system described above., Mirel Scoring system, , Score, points, , Site, , Radiographic, appearance, , Width of bone, involved, , Pain, , 1, , Upper extremity, , Blastic, , Less than 1/3, , Mild, , 2, , Lower, extremity, , Mixed, , 1/3 to 2/3, , Moderate, , 3, , Peritrochanteric, , Lytic, , More than 2/3, , Aggravated by, function, , Depending upon the score the treatment should be as follows:, , Score, , Risk of fracture, , Treatment, , 9 or greater, , Impending (33%), , Prophylactic fixation, , 8, , Borderline, , Consider fixation, , 7 or less, , Not impending (4%), , Non operative management
Page 906 :
Where the lesion is an isolated metastatic deposit consideration should be given to excision and, reconstruction as the outcome is better [2]., Non operative treatments, Hypercalcaemia- Treat with re hydration and bisphosphonates., Pain- Opiate analgesics and radiotherapy., Some tumours such as breast and prostate will benefit from chemotherapy and or hormonal agents., References, 1. Mirels, H. Metastatic disease in long bones. A proposed scoring system for diagnosing impending, pathologic fractures. Clin Orthop Relat Res, 1989(249): p. 256-64., 2. Mavrogenis, A.F. et al. Survival analysis of patients with femoral metastases. J Surg Oncol, 2011., Next question
Page 907 :
Question 47 of 147, Which of the following features are not typical of Crohns disease?, , Complex fistula in ano, , Small bowel strictures, , Skip lesions, , 'Rose thorn ulcers' on barium studies, , Pseudopolyps on colonoscopy, , Pseudopolyps are a feature of ulcerative colitis and occur when there is severe mucosal ulceration., The remaining islands of mucosa may then appear to be isolated and almost polypoidal., Please rate this question:, , Discuss and give feedback, , Next question, , Crohns disease, Crohns disease is a chronic transmural inflammation of a segment(s) of the gastrointestinal tract and, may be associated with extra intestinal manifestations. Frequent disease patterns observed include, ileal, ileocolic and colonic disease. Peri-anal disease may occur in association with any of these. The, disease is often discontinuous in its distribution. Inflammation may cause ulceration, fissures, fistulas, and fibrosis with stricturing. Histology reveals a chronic inflammatory infiltrate that is usually patchy, and transmural., Ulcerative colitis Vs Crohns, , Distribution, , Crohn's disease, , Ulcerative colitis, , Mouth to anus, , Rectum and colon
Page 909 :
Surgical interventions in Crohns disease, The commonest disease pattern in Crohns is stricturing terminal ileal disease and this often, culminates in an ileocaecal resection. Other procedures performed include segmental small bowel, resections and stricturoplasty. Colonic involvement in patients with Crohns is not common and,, where found, distribution is often segmental. However, despite this distribution segmental resections, of the colon in patients with Crohns disease are generally not advocated because the recurrence, rate in the remaining colon is extremely high, as a result the standard options of colonic surgery in, Crohns patients are generally; sub total colectomy, panproctocolectomy and staged sub total, colectomy and proctectomy. Restorative procedures such as ileoanal pouch have no role in therapy., Crohns disease is notorious for the developmental of intestinal fistulae; these may form between the, rectum and skin (peri anal) or the small bowel and skin. Fistulation between loops of bowel may also, occur and result in bacterial overgrowth and malabsorption. Management of enterocutaneous, fistulae involves controlling sepsis, optimising nutrition, imaging the disease and planning definitive, surgical management., Next question
Page 910 :
Question 48 of 147, At which of the following sites is the development of diverticulosis least likely?, , Caecum, , Ascending colon, , Transverse colon, , Sigmoid colon, , Rectum, Rectal involvement with diverticular disease almost never occurs., Because the rectum has a circular muscle coat (blending of of the tenia marks the recto-sigmoid, junction), diverticular disease almost never occurs here. Right sided colonic diverticular disease is, well recognised (though less common than left sided)., Please rate this question:, , Discuss and give feedback, , Next question, , Diverticular disease, Diverticular disease is a common surgical problem. It consists of herniation of colonic mucosa, through the muscular wall of the colon. The usual site is between the taenia coli where vessels, pierce the muscle to supply the mucosa. For this reason, the rectum, which lacks taenia, is often, spared., Symptoms, , , , , Altered bowel habit, Bleeding, Abdominal pain
Page 911 :
Complications, , , , , , , , Diverticulitis, Haemorrhage, Development of fistula, Perforation and faecal peritonitis, Perforation and development of abscess, Development of diverticular phlegmon, , Diagnosis, Patients presenting in clinic will typically undergo either a colonoscopy, CT cologram or barium, enema as part of their diagnostic work up. All tests can identify diverticular disease. It can be far, more difficult to confidently exclude cancer, particularly in diverticular strictures., Acutely unwell surgical patients should be investigated in a systematic way. Plain abdominal films, and an erect chest x-ray will identify perforation. An abdominal CT scan (not a CT cologram) with, oral and intravenous contrast will help to identify whether acute inflammation is present but also the, presence of local complications such as abscess formation., , Severity Classification- Hinchey, , I, , Para-colonic abscess, , II, , Pelvic abscess, , III, , Purulent peritonitis, , IV, , Faecal peritonitis, , Treatment, , , , , , , Increase dietary fibre intake., Mild attacks of diverticulitis may be managed conservatively with antibiotics., Peri colonic abscesses should be drained either surgically or radiologically., Recurrent episodes of acute diverticulitis requiring hospitalisation are a relative indication for, a segmental resection., Hinchey IV perforations (generalised faecal peritonitis) will require a resection and usually a, stoma. This group have a very high risk of post operative complications and usually require, HDU admission. Less severe perforations may be managed by laparoscopic washout and, drain insertion.
Page 912 :
Question 49 of 147, A 32 year old lady presents with a 1.5cm pigmented lesion on her back. The surgeon is concerned, that this may be a melanoma. What is the most appropriate course of action?, , 2mm punch biopsy from the centre of the lesion, , 4mm punch biopsy from the centre of the lesion, , Wide excision of the lesion with 3cm margins, , Excisional biopsy of the lesion, , Wide excision of the lesion with 1cm margins, Suspicious naevi should NOT be partially sampled as histological interpretation is severely, compromised. Complete excision is mandatory where lesions fulfil diagnostic criteria. However, wide, excision for margins may be deferred until definitive histology is available., Lesions that are suspicious for melanoma should be excised with complete margins. Radical, excision is not routinely undertaken for diagnostic purposes and therefore if subsequent, histopathological assessment determines that the lesion is a melanoma a re-exicision of margins, may be required. Incisional punch biopsies of potential melanomas makes histological interpretation, difficult and is best avoided., Please rate this question:, , Discuss and give feedback, , Next question, , Malignant melanoma, The main diagnostic features (major criteria):, , , , , Change in size, Change in shape, Change in colour, , Secondary features (minor criteria), , , , , Diameter >6mm, Inflammation, Oozing or bleeding
Page 913 :
, , Altered sensation, , Treatment, , , , Suspicious lesions should undergo excision biopsy. The lesion should be removed in, completely as incision biopsy can make subsequent histopathological assessment difficult., Once the diagnosis is confirmed the pathology report should be reviewed to determine, whether further re-excision of margins is required (see below):, , Margins of excision-Related to Breslow thickness, , Lesions 0-1mm thick, , 1cm, , Lesions 1-2mm thick, , 1- 2cm (Depending upon site and pathological features), , Lesions 2-4mm thick, , 2-3 cm (Depending upon site and pathological features), , Lesions >4 mm thick, , 3cm, , Marsden J et al Revised UK guidelines for management of Melanoma. Br J Dermatol 2010 163:238256., Further treatments such as sentinel lymph node mapping, isolated limb perfusion and block, dissection of regional lymph node groups should be selectively applied., Next question
Page 914 :
Question 50 of 147, A 50 year old male presents with painless frank haematuria. Clinical examination is unremarkable., Routine blood tests reveal a haemoglobin of 18g/dl but are otherwise normal. What is the most likely, underlying diagnosis?, , Squamous cell carcinoma of the bladder, , Adenocarcinoma of the prostate, , Adenocarcinoma of the kidney, , Wilms tumour, , Transitional cell carcinoma of the renal pelvis, , Theme from April 2012 Exam, Polycythaemia is a recognised feature of renal cell carcinoma. Wilms tumours most commonly occur, in children., Please rate this question:, , Discuss and give feedback, , Next question, , Haematuria, Causes of haematuria, , Trauma, , Infection, , , , , , , Injury to renal tract, Renal trauma commonly due to blunt injury (others penetrating, injuries), Ureter trauma rare: iatrogenic, Bladder trauma: due to RTA or pelvic fractures, , , , Remember TB
Page 917 :
1/3, Question 51-53 of 147, Theme: Thyroid neoplasms, , A., B., C., D., E., F., , Follicular carcinoma, Follicular adenoma, Papillary carcinoma, Papillary adenoma, Anaplastic carcinoma, Medullary carcinoma, , Please select the most likely underlying diagnosis for the thyroid masses described. Each option, may be used once, more than once or not at all., , 51., , A 78 year old lady presents to the surgical clinic with symptoms of both dysphagia and, dyspnoea. On examination there is a large mass in the neck that moves on swallowing. CT, scanning of the neck shows a locally infiltrative lesion arising from the thyroid and, invading the strap muscles., You answered Follicular carcinoma, The correct answer is Anaplastic carcinoma, Marked local invasion is a feature of anaplastic carcinoma. These tumours are more, common in elderly females., , 52., , A 25 year old female presents with a lump in her neck. On examination she has a discrete, nodule in the right lobe of the thyroid. A fine needle aspirate shows papillary cells. An, adjacent nodule is also sampled which shows similar well differentiated papillary cells., You answered Follicular adenoma, The correct answer is Papillary carcinoma, Multifocal disease is a recognised feature of papillary lesions. Papillary adenomas are not, really recognised and most well differentiated lesions are papillary carcinomas., , 53., , A 45 year old man presents with a fracture of his right humerus. On examination there is a, lytic lesion of the proximal humerus and a mass in the neck, this moves on swallowing., Follicular carcinoma
Page 918 :
Follicular carcinomas are a recognised source of bone metastasis. Up to 60% will show, vascular invasion histologically., Please rate this question:, , Discuss and give feedback, , Next question, , Thyroid neoplasms, Lesion, , Common features, , Follicular, adenoma, , , , , Usually present as a solitary thyroid nodule, Malignancy can only be excluded on formal histological assessment, , Papillary, carcinoma, , , , , , , , , Usually contain a mixture of papillary and colloidal filled follicles, Histologically tumour has papillary projections and pale empty nuclei, Seldom encapsulated, Lymph node metastasis predominate, Haematogenous metastasis rare, Account for 60% of thyroid cancers, , Follicular, carcinoma, , , , May appear macroscopically encapsulated, microscopically capsular, invasion is seen. Without this finding the lesion is a follicular adenoma., Vascular invasion predominates, Multifocal disease rare, Account for 20% of all thyroid cancers, , , , , , Anaplastic, carcinoma, , , , , , , Most common in elderly females, Local invasion is a common feature, Account for 10% of thyroid cancers, Treatment is by resection where possible, palliation may be achieved, through isthmusectomy and radiotherapy. Chemotherapy is ineffective., , Medullary, carcinoma, , , , , , , , Tumours of the parafollicular cells (C Cells), C cells derived from neural crest and not thyroid tissue, Serum calcitonin levels often raised, Familial genetic disease accounts for up to 20% cases, Both lymphatic and haematogenous metastasis are recognised, nodal
Page 919 :
Lesion, , Common features, , disease is associated with a very poor prognosis., Next question
Page 920 :
Question 54 of 147, Which of these lesions is most closely associated with Barretts oesophagus?, , Squamous cell carcinoma, , Gastro intestinal stromal tumours, , Carcinoid tumours, , Leiomyosarcoma, , Adenocarcinoma, , Theme from September 2014 Exam, Barretts oesophagus is most closely associated with adenocarcinoma, and it confers a 30 fold, increased risk of developing the condition., Please rate this question:, , Discuss and give feedback, , Next question, , Oesophageal cancer, , , , , , , Incidence is increasing, In most cases in the Western world this increase is accounted for by a rise in the number of, cases of adenocarcinoma. In the UK adenocarcinomas account for 65% of cases., Barretts oesophagus is a major risk factor for most cases of oesophageal adenocarcinoma., In other regions of the world squamous cancer is more common and is linked to smoking,, alcohol intake, diets rich in nitrosamines and achalasia., Surveillance of Barretts is important, as it imparts a 30 fold increase in cancer risk and if, invasive malignancy is diagnosed early then survival may approach 85% at 5 years., , Diagnosis, , , , Upper GI endoscopy is the first line test, Contrast swallow may be of benefit in classifying benign motility disorders but has no place, in the assessment of tumours
Page 921 :
, , , , Staging is initially undertaken with CT scanning of the chest, abdomen and pelvis. If overt, metastatic disease is identified using this modality then further complex imaging is, unnecessary, If CT does not show metastatic disease, then local stage may be more accurately assessed, by use of endoscopic ultrasound., Staging laparoscopy is performed to detect occult peritoneal disease. PET CT is performed, in those with negative laparoscopy. Thoracoscopy is not routinely performed., , Treatment, Operable disease is best managed by surgical resection. The most standard procedure is an IvorLewis type oesophagectomy. This procedure involves the mobilisation of the stomach and division of, the oesophageal hiatus. The abdomen is closed and a right sided thoracotomy performed. The, stomach is brought into the chest and the oesophagus mobilised further. An intrathoracic, oesophagogastric anastomosis is constructed. Alternative surgical strategies include a transhiatal, resection (for distal lesions), a left thoraco-abdominal resection (difficult access due to thoracic, aorta) and a total oesophagectomy (McKeown) with a cervical oesophagogastric anastomosis., The biggest surgical challenge is that of anastomotic leak, with an intrathoracic anastomosis this will, result in mediastinitis. With high mortality. The McKeown technique has an intrinsically lower, systemic insult in the event of anastomotic leakage., In addition to surgical resection many patients will be treated with adjuvant chemotherapy., Next question
Page 922 :
Question 55 of 147, A 56 year old man presents with epigastric discomfort and episodes of migratory thrombophlebitis., On examination he is mildly jaundiced. A CT scan shows peri hilar lymphadenopathy and a mass in, the pancreatic head. Which of the following is the most likely underlying diagnosis?, , Squamous cell carcinoma of the pancreas, , Adenocarcinoma of the pancreas, , Insulinoma, , Glucagonoma, , Gastrinoma, , Adenocarcinoma of the pancreas is the most likely diagnosis and migratory thrombophlebitis is, associated with the condition. Squamous cells carcinoma is extremely uncommon in the pancreas., Gastrinoma are extremely rare and thus not the most likely diagnosis., Please rate this question:, , Discuss and give feedback, , Next question, , Pancreatic cancer, , , , , , , Adenocarcinoma, Risk factors: Smoking, diabetes, adenoma, familial adenomatous polyposis, Mainly occur in the head of the pancreas (70%), Spread locally and metastasizes to the liver, Carcinoma of the pancreas should be differentiated from other periampullary tumours with, better prognosis, , Clinical features, , , , , Weight loss, Painless jaundice, Epigastric discomfort (pain usually due to invasion of the coeliac plexus is a late feature)
Page 923 :
, , , Pancreatitis, Trousseau's sign: migratory superficial thrombophlebitis, , Investigations, , , , , , , USS: May miss small lesions, CT Scanning (pancreatic protocol). If unresectable on CT then no further staging needed, PET/CT for those with operable disease on CT alone, ERCP/ MRI for bile duct assessment, Staging laparoscopy to exclude peritoneal disease, , Management, , , , , , , Head of pancreas: Whipple's resection (SE dumping and ulcers). Newer techniques include, pylorus preservation and SMA/ SMV resection, Carcinoma body and tail: poor prognosis, distal pancreatectomy, if operable, Usually adjuvent chemotherapy for resectable disease, ERCP and stent for jaundice and palliation, Surgical bypass may be needed for duodenal obstruction, , Next question
Page 924 :
Question 56 of 147, What is the urinary diagnostic marker for carcinoid syndrome?, , B-HCG, , Histamine, , Chromogranin A, , 5-Hydroxyindoleacetic acid, , 5-Hydroxytryptamine, , Urinary measurement of 5- HIAA is an important part of clinical follow up., Please rate this question:, , Discuss and give feedback, , Next question, , Carcinoid syndrome, , , , , , Carcinoid tumours secrete serotonin, Originate in neuroendocrine cells mainly in the intestine (midgut-distal ileum/appendix), Can occur in the rectum, bronchi, Hormonal symptoms mainly occur when disease spreads outside the bowel, , Clinical features, , , , , , , , Onset: insidious over many years, Flushing face, Palpitations, Pulmonary valve stenosis and tricuspid regurgitation causing dyspnoea, Asthma, Severe diarrhoea (secretory, persists despite fasting)
Page 926 :
Question 57 of 147, A 22 year old man presents with symptoms of headache, lethargy and confusion. On examination he, is febrile and has a right sided weakness. A CT scan shows a ring enhancing lesion affecting the left, motor cortex. Which of the following is the most likely diagnosis?, , Arteriovenous malformation, , Cerebral abscess, , Herpes simplex encephalitis, , Metastatic renal adenocarcinoma, , Glioblastoma multiforme, , The combination of rapidly progressive neurology, fever and headache is highly suggestive of, cerebral abscess. CT scanning will show a ring enhancing lesion because the intravenous contrast, cannot penetrate the centre of the abscess cavity. HSV encephalitis does not produce ring, enhancing lesions., Please rate this question:, , Discuss and give feedback, , Next question, , Brain abscess, , , , , , , CNS abscesses may result from a number of causes including, extension of sepsis from, middle ear or sinuses, trauma or surgery to the scalp, penetrating head injuries and embolic, events from endocarditis., The presenting symptoms will depend upon the site of the abscess (those in critical areas, e.g.motor cortex) will present earlier. Abscesses have a considerable mass effect in the brain, and raised intra cranial pressure is common., Although fever, headache and focal neurology are highly suggestive of a brain abscess the, absence of one or more of these does not exclude the diagnosis, fever may be absent and, even if present, is usually not the swinging pyrexia seen with abscesses at other sites., Assessment of the patient includes imaging with CT scanning., Treatment is usually surgical, a craniotomy is performed and the abscess cavity debrided., The abscess may reform because the head is closed following abscess drainage.
Page 927 :
Question 58 of 147, A 56 year old man from Egypt has suffered from recurrent attacks of haematuria for many years. He, presents with suprapubic discomfort and at cystoscopy is found to have a mass lesion within the, bladder. What is the most likely diagnosis?, , Squamous cell carcinoma, , Transitional cell papilloma, , Adenocarcinoma, , Leiomyosarcoma, , Rhabdomyosarcoma, , Theme from April 2016 exam, In Egypt, Schistosomiasis is more common than in the UK and may cause recurrent episodes of, haematuria. In those affected with the condition who develop a bladder neoplasm, an SCC is the, most common type., Please rate this question:, , Discuss and give feedback, , Next question, , Bladder cancer, Bladder cancer is the second most common urological cancer. It most commonly affects males aged, between 50 and 80 years of age. Those who are current, or previous (within 20 years), smokers, have a 2-5 fold increased risk of the disease. Exposure to hydrocarbons such as 2-Naphthylamine, increases the risk. Although rare in the UK, chronic bladder inflammation arising from, Schistosomiasis infection remains a common cause of squamous cell carcinomas, in those countries, where the disease is endemic., Benign tumours, Benign tumours of the bladder including inverted urothelial papilloma and nephrogenic adenoma are, uncommon., Bladder malignancies
Page 928 :
, , , , Transitional cell carcinoma (>90% of cases), Squamous cell carcinoma ( 1-7% -except in regions affected by schistosomiasis), Adenocarcinoma (2%), , Transitional cell carcinomas may arise as solitary lesions, or may be multifocal, owing to the effect of, "field change" within the urothelium. Up to 70% of TCC's will have a papillary growth pattern. These, tumours are usually superficial in location and accordingly have a better prognosis. The remaining, tumours show either mixed papillary and solid growth or pure solid growths. These tumours are, typically more prone to local invasion and may be of higher grade, the prognosis is therefore worse., Those with T3 disease or worse have a 30% (or higher) risk of regional or distant lymph node, metastasis., TNM Staging, , Stage, , Description, , T0, , No evidence of tumour, , Ta, , Non invasive papillary carcinoma, , T1, , Tumour invades sub epithelial connective tissue, , T2a, , Tumor invades superficial muscularis propria (inner half), , T2b, , Tumor invades deep muscularis propria (outer half), , T3, , Tumour extends to perivesical fat, , T4, , Tumor invades any of the following: prostatic stroma, seminal vesicles, uterus, vagina, , T4a, , Invasion of uterus, prostate or bowel, , T4b, , Invasion of pelvic sidewall or abdominal wall, , N0, , No nodal disease
Page 929 :
Stage, , Description, , N1, , Single regional lymph node metastasis in the true pelvis (hypogastric, obturator, external, iliac, or presacral lymph node), , N2, , Multiple regional lymph node metastasis in the true pelvis (hypogastric, obturator, external, iliac, or presacral lymph node metastasis), , N3, , Lymph node metastasis to the common iliac lymph nodes, , M0, , No distant metastasis, , M1, , Distant disease, , Presentation, Most patients (85%) will present with painless, macroscopic haematuria. In those patients with, incidental microscopic haematuria, up to 10% of females aged over 50 will be found to have a, malignancy (once infection excluded)., Staging, Most will undergo a cystoscopy and biopsies or TURBT, this provides histological diagnosis and, information relating to depth of invasion. Locoregional spread is best determined using pelvic MRI, and distant disease CT scanning. Nodes of uncertain significance may be investigated using PET, CT., Treatment, Those with superficial lesions may be managed using TURBT in isolation. Those with recurrences or, higher grade/ risk on histology may be offered intravesical chemotherapy. Those with T2 disease are, usually offered either surgery (radical cystectomy and ileal conduit) or radical radiotherapy., Prognosis, , T1, , 90%, , T2, , 60%, , T3, , 35%
Page 931 :
Question 59 of 147, A newborn infant is noted to have a unilateral cleft lip only. What is the most likely explanation for, this process?, , Incomplete fusion of the second branchial arch, , Incomplete fusion of the nasolabial muscle rings, , Incomplete fusion of the first branchial arch, , Incomplete fusion of the third branchial arch, , Incomplete fusion of the secondary palate, , Theme from April 2012 Exam, Unilateral isolated cleft lip represents a failure of nasolabial ring fusion. It is not related to branchial, arch fusion. Arch disorders have a far more profound phenotype and malformation sequences., Please rate this question:, , Discuss and give feedback, , Next question, , Cleft lip and palate, Cleft lip and palate are the most common congenital deformity affecting the orofacial structures., Whilst they may be an isolated developmental malformation they are also a recognised component, of more than 200 birth defects. The incidence is as high as 1 in 600 live births. The commonest, variants are:, , , , , Isolated cleft lip (15%), Isolated cleft palate (40%), Combined cleft lip and palate (45%), , The aetiology of the disorder is multifactorial; both genetic (affected first degree relative increases, risk) and environmental factors play a role., Cleft lip, Cleft lip occurs as a result of disruption of the muscles of the upper lip and nasolabial region. These
Page 932 :
muscles comprise a chain of muscles viz; nasolabial, bilabial and labiomental. Defects may be, unilateral or bilateral., Cleft palate, The primary palate consists of all anatomical structures anterior to the incisive foramen. The, secondary palate lies more posteriorly and is sub divided into the hard and soft palate. Cleft palate, occurs as a result of non fusion of the two palatine shelves. Both hard and soft palate may be, involved. Complete cases are associated with complete separation of the nasal septum and vomer, from the palatine processes., Treatment, Surgical reconstruction is the mainstay of management. The procedures are planned according to, the extent of malformation and child age. Simple defects are managed as a single procedure., Complex malformations are usually corrected in stages. Affected individuals have a higher incidence, of hearing and speech problems., Next question
Page 933 :
Question 60 of 147, A 72 year old woman with back pain and chronic renal failure has the following blood test results:, , Reference range, , Ca2+, , 2.03, , 2.15-2.55 mmol/l, , Parathyroid hormone, , 10.4, , 1-6.5 pmol/l, , Phosphate, , 0.80, , 0.6-1.25 mmol/l, , What is the most likely diagnosis?, , Hypoparathyroidism, , Primary hyperparathyroidism, , Secondary hyperparathyroidism, , Tertiary hyperparathyroidism, , Pseudohypoparathyroidism, , In relation to secondary hyperparathyroidism; there is a HIGH PTH and the Ca 2+ is NORMAL or, LOW. In secondary hyperparathyroidism there is hyperplasia of the parathyroid glands in response, to chronic hypocalcaemia (or hyperphosphataemia) and is a normal physiological response. Calcium, is released from bone, kidneys and the gastrointestinal system., Please rate this question:, , Discuss and give feedback, , Next question, , Parathyroid glands and disorders of calcium metabolism
Page 934 :
Hyperparathyroidism, , Disease type, , Hormone profile, , Clinical features, , Cause, , Primary, hyperparathyroidism, , , , , , , PTH (Elevated), Ca2+(Elevated), Phosphate (Low), Urine calcium :, creatinine clearance, ratio > 0.01, , May be, asymptomatic if, mild, Recurrent, abdominal pain, (pancreatitis, renal, colic), Changes to, emotional or, cognitive state, , Most cases due to, solitary adenoma, (80%), multifocal, disease occurs in 1015% and parathyroid, carcinoma in 1% or, less, , Secondary, hyperparathyroidism, , , , , PTH (Elevated), Ca2+ (Low or, normal), Phosphate, (Elevated), Vitamin D levels, (Low), , May have few, symptoms, Eventually may, develop bone, disease, osteitis, fibrosa cystica and, soft tissue, calcifications, , Parathyroid gland, hyperplasia occurs as, a result of low, calcium, almost, always in a setting of, chronic renal failure, , Ca2+(Normal or, high), PTH (Elevated), Phosphate levels, (Decreased or, Normal), Vitamin D (Normal, or decreased), Alkaline, phosphatase, (Elevated), , Metastatic, calcification, Bone pain and /, or fracture, Nephrolithiasis, Pancreatitis, , Occurs as a result of, ongoing hyperplasia, of the parathyroid, glands after, correction of, underlying renal, disorder, hyperplasia, of all 4 glands is, usually the cause, , , , , Tertiary, hyperparathyroidism, , , , , , , , , Differential diagnoses, It is important to consider the rare but relatively benign condition of benign familial hypocalciuric, hypercalcaemia, caused by an autosomal dominant genetic disorder. Diagnosis is usually made by, genetic testing and concordant biochemistry (urine calcium : creatinine clearance ratio <0.01distinguished from primary hyperparathyroidism)., Treatment, Primary hyperparathyroidism
Page 935 :
Indications for surgery, , , , , , , , , , Elevated serum Calcium > 1mg/dL above normal, Hypercalciuria > 400mg/day, Creatinine clearance < 30% compared with normal, Episode of life threatening hypercalcaemia, Nephrolithiasis, Age < 50 years, Neuromuscular symptoms, Reduction in bone mineral density of the femoral neck, lumbar spine, or distal radius of more, than 2.5 standard deviations below peak bone mass (T score lower than -2.5), , Secondary hyperparathyroidism, Usually managed with medical therapy., Indications for surgery in secondary (renal) hyperparathyroidism:, , , , , Bone pain, Persistent pruritus, Soft tissue calcifications, , Tertiary hyperparathyroidism, Allow 12 months to elapse following transplant as many cases will resolve, The presence of an autonomously functioning parathyroid gland may require surgery. If the culprit, gland can be identified then it should be excised. Otherwise total parathyroidectomy and reimplantation of part of the gland may be required., References, 1. Pitt S et al. Secondary and Tertiary Hyperparathyroidism, State of the Art Surgical, Management.Surg Clin North Am 2009 Oct;89(5):1227-39., 2. MacKenzie-Feder J et al. Primary Hyperparathyroidism: An Overview. Int J Endocrinol 2011;, 2011: 251410., Next question
Page 936 :
1/3, Question 61-63 of 147, Theme: Pharyngitis, , A., B., C., D., E., , Infectious mononucleosis, Acute bacterial tonsillitis, Quinsy, Lymphoma, Diptheria, , Please select the most likely underlying cause for the following patients presenting with pharyngitis., Each option may be used once, more than once or not at all., , 61., , An 8 year old child presents with enlarged tonsils that meet in the midline and are covered, with a white film that bleeds when you attempt to remove it. He is pyrexial but otherwise, well., You answered Infectious mononucleosis, The correct answer is Acute bacterial tonsillitis, Theme from April 2012 Exam, In acute tonsillitis the tonsils will often meet in the midline and may be covered with a, membrane. Individuals who are systemically well are unlikely to have diptheria., , 62., , A 10 year old child presents with enlarged tonsils that meet in the midline. Oropharyngeal, examination confirms this finding and you also notice peticheal haemorrhages affecting, the oropharynx. On systemic examination he is noted to have splenomegaly., Infectious mononucleosis, A combination of pharyngitis and tonsillitis is often seen in glandular fever. Antibiotics, containing penicillin may produce a rash when given in this situation, leading to a, mistaken label of allergy., , 63., , A 19 year old man has had a sore throat for the past 5 days. Over the past 24 hours he has, notices increasing and severe throbbing pain in the region of his right tonsil. He is pyrexial, and on examination he is noted to have a swelling of this area., You answered Infectious mononucleosis, The correct answer is Quinsy
Page 937 :
Unilateral swelling and fever is usually indicative of quinsy. Surgical drainage usually, produces prompt resolution of symptoms., Please rate this question:, , Discuss and give feedback, , Next question, , Acute tonsillitis, , , , , , , , Characterised by pharyngitis, fever, malaise and lymphadenopathy., Over half of all cases are bacterial with Streptococcus pyogenes the most common organism, The tonsils are typically oedematous and yellow or white pustules may be present, Infectious mononucleosis may mimic the condition., Treatment with penicillin type antibiotics is indicated for bacterial tonsillitis., Bacterial tonsillitis may result in local abscess formation (quinsy), , Acute streptococcal tonsillitis
Page 938 :
Image sourced from Wikipedia, , Next question
Page 939 :
Question 64 of 147, , A 4 year old boy is brought to the clinic by his mother who has noticed a small lesion at the external, angle of his eye. On examination there is a small cystic structure which has obviously been recently, infected. On removal of the scab, there is hair visible within the lesion. What is the most likely, diagnosis?, , Dermoid cyst, , Desmoid cyst, , Sebaceous cyst, , Epidermoid cyst, , Keratoacanthoma, Dermoid cysts occur at sites of embryonic fusion and may contain multiple cell types. They occur, most often in children., , The lesion is unlikely to be a desmoid cyst as these are seldom located either at this site or in this, age group. In addition they do not contain hair. Sebaceous cysts will usually have a punctum and, contain a cheesy material. Epidermoid cysts contain keratin plugs., Please rate this question:, , Discuss and give feedback, , Next question, , Dermoid cysts
Page 940 :
A cutaneous dermoid cyst may develop at sites of embryonic developmental fusion. They are most, common in the midline of the neck, external angle of the eye and posterior to the pinna of the ear., They typically have multiple inclusions such as hair follicles that bud out from its walls. They may, develop at other sites such as the ovary and in these sites are synonymous with teratomas., A desmoid tumour is a completely different entity and may be classified either as low grade, fibrosarcomas or non aggressive fibrous tumours. They commonly present as large infiltrative, masses. They may be divided into abdominal, extra abdominal and intra abdominal. All types share, the same biological features. Extra abdominal desmoids have an equal sex distribution and primarily, arise in the musculature of the shoulder, chest wall, back and thigh. Abdominal desmoids usually, arise in the musculoaponeurotic structures of the abdominal wall. Intra abdominal desmoids tend to, occur in the mesentery or pelvic side walls and occur most frequently in patients with familial, adenomatous polyposis coli syndrome., Next question
Page 941 :
Question 65 of 147, Which of the following tumours are most likely to give rise to para-aortic nodal metastasis early?, , Ovarian, , Bladder, , Rectal, , Caecal, , Cervical, , Theme from 2009 Exam, Ovarian tumours are supplied by the ovarian vessels, these branch directly from the aorta. The, cervix drains to the internal and external iliac nodes., Please rate this question:, , Discuss and give feedback, , Next question, , Para-aortic lymphadenopathy, Organ sites that may metastasise (early) to the para-aortic lymph nodes:, , , , , Testis, Ovary, Uterine fundus, , Many other organs may result in para-aortic nodal disease. However, these deposits will represent a, much later stage of the disease, since other nodal stations are involved earlier., Next question
Page 942 :
Question 66 of 147, Which of the following statements relating to malignant mesothelioma is false?, , It may be treated by extrapleural pneumonectomy., , It is linked to asbestos exposure., , It is linked to cigarette smoking independent of asbestos exposure., , It may occur intra abdominally., , It is relatively resistant to radiotherapy, , It is not linked to cigarette smoking. When identified at an early stage a radical resection is the, favored option. Radiotherapy is often given perioperatively. However, it is not a particularly, radiosensitive tumour. Combination chemotherapy gives some of the best results and most regimes, are cisplatin based., Please rate this question:, , Discuss and give feedback, , Next question, , Occupational cancers, Occupational cancers accounted for 5.3% cancer deaths in 2005., In men the main cancers include:, , , , , , , Mesothelioma, Bladder cancer, Non melanoma skin cancer, Lung cancer, Sino nasal cancer, , Occupations with high levels of occupational tumours include:
Page 943 :
, , , , , , , Construction industry, Working with coal tar and pitch, Mining, Metalworkers, Working with asbestos (accounts for 98% of all mesotheliomas), Working in rubber industry, , Shift work has been linked to breast cancer in women (Health and safety executive report RR595)., The latency between exposure and disease is typically 15 years for solid tumours and 20 for, leukaemia., Many occupational cancers are otherwise rare. For example sino nasal cancer is an uncommon, tumour, 50% will be SCC. They are linked to conditions such as wood dust exposure and unlike lung, cancer is not strongly linked to cigarette smoking. Another typical occupational tumour is, angiosarcoma of the liver which is linked to working with vinyl chloride. Again in the non occupational, context this is an extremely rare sporadic tumour., Next question
Page 944 :
2/3, Question 67-69 of 147, Theme: Thyroid disorders, , A., B., C., D., E., F., , Sick euthyroid, Hyperthyroidism, Hypothyroidism, Normal euthyroid, Anxiety state, Factitious hyperthyroidism, , For each of the scenarios please match the scenario with the most likely underlying diagnosis. Each, answer may be used once, more than once or not at all., , 67., , A 33 year old man is recovering following a protracted stay on the intensive care unit, recovering from an anastomotic leak following a difficult trans hiatal oesophagectomy. His, progress is slow, and the intensive care doctors receive the following thyroid function test, results:, TSH, , 1.0 u/L, , Free T4, , 8, , T3, , 1.0 (1.2-3.1 normal), , Sick euthyroid, Theme from April 2012 Exam, Sick euthyroid syndrome is caused by systemic illness. With this, the patient may have an, apparently low total and free T4 and T3, with a normal or low TSH. Note that the levels, are only mildly below normal., 68., , A 28 year old female presents to the general practitioner with symptoms of fever and, diarrhoea. As part of her diagnostic evaluation the following thyroid function tests are, obtained:, TSH, , < 0.01, , Free T4, , 30, , T3, , 4.0
Page 945 :
Hyperthyroidism, The symptoms are suggestive of hyperthyroidism. This is supported by the abnormal blood, results; suppressed TSH with an elevated T3 and T4., A 19 year old lady presents with palpitations. The medical officer takes a blood sample for, thyroid function tests. The following results are obtained:, , 69., , TSH, , > 6.0, , Free T4, , 20, , T3, , 2.0, , You answered Sick euthyroid, The correct answer is Hypothyroidism, An elevated TSH with normal T4 indicates partial thyroid failure. This is caused by, Hashimotos, drugs (lithium, antithyroids) and dyshormogenesis., Please rate this question:, , Discuss and give feedback, , Next question, , Hyperthyroidism, Causes of hyperthyroidism include:, , , , , , Diffuse toxic goitre (Graves Disease), Toxic nodular goitre, Toxic nodule, Rare causes, , Graves disease, Graves disease is characterised by a diffuse vascular goitre that appears at the same time as the, clinical manifestations of hyperthyroidism. It is commonest in younger females and may be, associated with eye signs. Thyrotoxic symptoms will predominate. Up to 50% of patients will have a, familial history of autoimmune disorders. The glandular hypertrophy and hyperplasia occur as a, result of the thyroid stimulating effects of the TSH receptor antibodies.
Page 946 :
Toxic nodular goitre, In this disorder the goitre is present for a long period of time prior to the development of clinical, symptoms. In most goitres the nodules are inactive and in some cases it is the internodular tissue, that is responsible for the hyperthyroidism., Toxic nodule, Overactive, autonomously functioning nodule. It may occur as part of generalised nodularity or be a, true toxic adenoma. The TSH levels are usually low as the autonomously functioning thyroid tissue, will exert a negative feedback effect., Signs and symptoms, , Symptoms, , Signs, , Lethargy, , Tachycardia, , Emotionally labile, , Agitation, , Heat intolerance, , Hot, moist palms, , Weight loss, , Exopthalmos, , Excessive appetite, , Thyroid goitre and bruit, , Palpitations, , Lid lag/retraction, , Diagnosis, The most sensitive test for diagnosing hyperthyroidism is plasma T3 (which is raised). Note in, hypothyroidism the plasma T4 and TSH are the most sensitive tests. A TSH level of <0.5U/L, suggests hyperthyroidism. TSH receptor antibodies may be tested for in the diagnosis of Graves., Treatment, First line treatment for Graves disease is usually medical and the block and replace regime is the, favored option. Carbimazole is administered at higher doses and thyroxine is administered orally., Patient are maintained on this regime for between 6 and 12 months. Attempts are then made to, wean off medication. Where relapse then occurs the options are between ongoing medical therapy,, radioiodine or surgery., Next question
Page 948 :
Question 71 of 147, , Which of the tumour types listed below is found most frequently in a person with aggressive, fibromatosis?, , Medullary thyroid cancer, , Basal cell carcinoma of the skin, , Desmoid tumours, , Dermoid tumours, , Malignant melanoma, , Please rate this question:, , Discuss and give feedback, , Next question, , Aggressive fibromatosis, Aggressive fibromatosis is a disorder consisting of desmoid tumours, which behave in a locally, aggressive manner. Desmoid tumours may be identified in both abdominal and extra-abdominal, locations. Metastatic disease is rare. The main risk factor (for abdominal desmoids) is having APC, variant of familial adenomatous polyposis coli. Most cases are sporadic., Treatment is by surgical excision., Next question
Page 949 :
Question 72 of 147, A 20 year old man is suspected of having an inflamed Meckels diverticulum. At which of the, following locations is it most likely to be found?, , Approximately 60 cm distal to the ileo-caecal valve, , Approximately 60 cm proximal to the ileocaecal valve, , Approximately 200cm distal to the ileocaecal valve, , Approximately 200cm proximal to the ileocaecal valve, , 50cm distal to the DJ flexure, Rule of 2's, 2% of population, 2 inches (5cm) long, 2 feet (60 cm) from the ileocaecal valve, 2 x's more common in men, 2 tissue types involved, They are typically found 2 feet proximal to the ileocaecal valve (or approximately 60cm)., Please rate this question:, , Discuss and give feedback, , Next question, , Meckel's diverticulum, , , , , , , , , Congenital abnormality resulting in incomplete obliteration of the vitello-intestinal duct, Normally, in the foetus, there is an attachment between the vitello-intestinal duct and the yolk, sac.This disappears at 6 weeks gestation., The tip is free in majority of cases., Associated with enterocystomas, umbilical sinuses, and omphaloileal fistulas., Arterial supply: omphalomesenteric artery., 2% of population, 2 inches long, 2 feet from the ileocaecal valve., Typically lined by ileal mucosa but ectopic gastric mucosa can occur, with the risk of peptic, ulceration. Pancreatic and jejunal mucosa can also occur.
Page 950 :
Clinical, , , , , Normally asymptomatic and an incidental finding., Complications are the result of obstruction, ectopic tissue, or inflammation., Removal if narrow neck or symptomatic. Options are between wedge excision or formal, small bowel resection and anastomosis., Next question
Page 951 :
Question 73 of 147, A 43 year old lady presents with severe chest pain. Investigations demonstrate a dissecting, aneurysm of the ascending aorta which originates at the aortic valve. What is the optimal long term, treatment?, , Endovascular stent, , Medical therapy with beta blockers, , Medical therapy with ACE inhibitors, , Sutured aortic repair, , Aortic root replacement, , Proximal aortic dissections are generally managed with surgical aortic root replacement. The, proximal origin of the dissection together with chest pain (which may occur in all types of aortic, dissection) raises concerns about the possibility of coronary ostial involvement (which precludes, stenting). There is no role for attempted suture repair in this situation., Please rate this question:, , Discuss and give feedback, , Next question, , Aortic dissection, , , , , , , More common than rupture of the abdominal aorta, 33% of patients die within the first 24 hours, and 50% die within 48 hours if no treatment, received, Associated with hypertension, Features of aortic dissection: tear in the intimal layer, followed by formation and propagation, of a subintimal hematoma. Cystic medial necrosis (Marfan's), Most common site of dissection: 90% occurring within 10 centimetres of the aortic valve, , Stanford Classification, , Type, , Location, , Treatment
Page 952 :
Type, , Location, , Treatment, , A, , Ascending aorta/ aortic root, , Surgery- aortic root replacement, , B, , Descending aorta, , Medical therapy with antihypertensives, , DeBakey classification, , Type, , Site affected, , I, , Ascending aorta, aortic arch, descending aorta, , II, , Ascending aorta only, , III, , Descending aorta distal to left subclavian artery, , Clinical features, , , , , , Tearing, sudden onset chest pain (painless 10%), Hypertension or Hypotension, A blood pressure difference (in each arm) greater than 20 mm Hg, Neurologic deficits (20%), , Investigations, , , , , , CXR: widened mediastinum, abnormal aortic knob, ring sign, deviation of the, trachea/oesophagus, CT angiography of the thoracic aorta, MRI angiography, Conventional angiography (now rarely used diagnostically), , Management, , , , Beta-blockers: aim HR 60-80 bpm and systolic BP 100-120 mm Hg, For type A dissections the standard of care is aortic root replacement
Page 953 :
Question 74 of 147, A 45 year old lady presents with a pathological fracture of her femoral shaft. She is a poor historian,, but it transpires that she underwent a thyroidectomy 1 year previously. She has no other illness or, co-morbidities. What is the most likely underlying diagnosis?, , Hyperparathyroidism, , Metastatic papillary carcinoma of the thyroid, , Metastatic medullary carcinoma of the thyroid, , Metastatic follicular carcinoma of the thyroid, , None of the above, , Follicular carcinomas are a recognised cause of bone metastasis. Papillary lesions typically spread, via the lymphatics., Please rate this question:, , Discuss and give feedback, , Next question, , Thyroid malignancy, Papillary carcinoma, , , , , , Commonest sub-type, Accurately diagnosed on fine needle aspiration cytology, Histologically, they may demonstrate psammoma bodies (areas of calcification) and so, called 'orphan Annie' nuclei, They typically metastasise via the lymphatics and thus laterally located apparently ectopic, thyroid tissue is usually a metastasis from a well differentiated papillary carcinoma, , Follicular carcinoma, , , Are less common than papillary lesions
Page 954 :
, , , , Like papillary tumours, they may present as a discrete nodule. Although they appear to be, well encapsulated macroscopically there is invasion on microscopic evaluation, Lymph node metastases are uncommon and these tumours tend to spread, haematogenously. This translates into a higher mortality rate, Follicular lesions cannot be accurately diagnosed on fine needle aspiration cytology and thus, all follicular FNA's (THY 3f) will require at least a hemi thyroidectomy, , Anaplastic carcinoma, , , , Less common and tend to occur in elderly females, Disease is usually advanced at presentation and often only palliative decompression and, radiotherapy can be offered., , Medullary carcinoma, , , , , , These are tumours of the parafollicular cells ( C Cells) and are of neural crest origin., The serum calcitonin may be elevated which is of use when monitoring for recurrence., They may be familial and occur as part of the MEN -2A disease spectrum., Spread may be either lymphatic or haematogenous and as these tumours are not derived, primarily from thyroid cells they are not responsive to radioiodine., , Lymphoma, , , , These respond well to radiotherapy, Radical surgery is unnecessary once the disease has been diagnosed on biopsy material., Such biopsy material is not generated by an FNA and thus a core biopsy has to be obtained, (with care!)., Next question
Page 955 :
Question 75-77 of 147, , Theme: Cardiac murmurs, , A. Pulmonary stenosis, B. Mitral regurgitation, C. Tricuspid regurgitation, D. Aortic stenosis, E. Mitral stenosis, F. Aortic sclerosis, , What is the most likely cause of the cardiac murmur in the following patients? Each option may be, used once, more than once or not at all., , 75., , A 35 year old Singaporean female attends a varicose vein pre operative clinic. On auscultation a, mid diastolic murmur is noted at the apex. The murmur is enhanced when the patient lies in the, left lateral position., You answered Pulmonary stenosis, The correct answer is Mitral stenosis, Theme from September 2011 exam, A mid diastolic murmur at the apex is a classical description of a mitral stenosis murmur. The, most common cause is rheumatic heart disease. Complications of mitral stenosis include atrial, fibrillation, stroke, myocardial infarction and infective endocarditis., , 76., , A 22 year old intravenous drug user is found to have a femoral abscess. The nursing staff contact, the on call doctor as the patient has a temperature of 39oC. He is found to have a pan systolic, murmur loudest at the left sternal edge at the 4th intercostal space., You answered Pulmonary stenosis
Page 956 :
The correct answer is Tricuspid regurgitation, Intravenous drug users are at high risk of right sided cardiac valvular endocarditis. The character, of the murmur fits with a diagnosis of tricuspid valve endocarditis., , 77., , An 83 year old woman is admitted with a left intertrochanteric neck of femur fracture. On, examination the patient is found to have an ejection systolic murmur loudest in the aortic region., There is no radiation of the murmur to the carotid arteries. Her ECG is normal., You answered Pulmonary stenosis, The correct answer is Aortic sclerosis, The most likely diagnosis is aortic sclerosis. The main differential diagnosis is of aortic stenosis,, however as there is no radiation of the murmur to the carotids and the ECG is normal, this is less, likely., , Please rate this question:, , Discuss and give feedback, , Next question, , Cardiac murmurs, Type of Murmur, , Conditions, , Ejection systolic, , Aortic stenosis, Pulmonary stenosis, HOCM, ASD, Fallot's
Page 957 :
Pan-systolic, , Mitral regurgitation, Tricuspid regurgitation, VSD, , Late systolic, , Mitral valve prolapse, Coarctation of aorta, , Early diastolic, , Aortic regurgitation, Graham-Steel murmur (pulmonary regurgitation), , Mid diastolic, , Mitral stenosis, Austin-Flint murmur (severe aortic regurgitation), Next question
Page 958 :
Question 78 of 147, , A 55 year old lady presents with discomfort in the right breast. On clinical examination a small lesion, is identified and clinical appearances suggest fibroadenoma. Imaging confirms the presence of a, fibroadenoma alone. A core biopsy is taken, this confirms the presence of the fibroadenoma., However, the pathologist notices that a small area of lobular carcinoma in situ is also present in the, biopsy. What is the best management?, , Whole breast irradiation, , Simple mastectomy, , Mastectomy and sentinal lymph node biopsy, , Wide local excision and sentinel lymph node biopsy, , Breast MRI scan, , Lobular carcinoma in situ has a low association with invasive malignancy. It is seldom associated, with microcalcification and therefore MRI is the best tool for determining disease extent. Resection of, in situ disease is not generally recommended and most surgeons would simply pursue a policy of, close clinical and radiological follow up., Please rate this question:, , Discuss and give feedback, , Next question, , Lobular carcinoma of the breast, Lobular breast cancers are less common than their ductal counterparts. They typically present, differently, the mass is usually more diffuse and less obvious on the usual imaging modalities of, ultrasound and mammography. This is significant since the disease may be understaged resulting in
Page 959 :
inadequate treatment when wide local excision is undertaken., In women with invasive lobular carcinoma it is usually safest to perform an MRI scan of the breast, if, breast conserving surgery is planned., Lobular carcinomas are also more likely to be multifocal and metastasise to the contralateral breast., Lobular carcinoma in situ is occasionally diagnosed incidentally on core biopsies. Unlike DCIS,, lobular carcinoma in situ is far less strongly associated with foci of invasion and is usually managed, by close monitoring., Next question
Page 960 :
Question 79 of 147, Which one of the following may be associated with an increased risk of venous thromboembolism?, , Diabetes, , Cannula, , Hyperthyroidism, , Tamoxifen, , Amiodarone, , Consider thromboembolism in breast cancer patients on tamoxifen!, Please rate this question:, , Discuss and give feedback, , Next question, , Venous thromboembolism: risk factors, Common predisposing factors include malignancy, pregnancy and the period following an operation., The comprehensive list below is partly based on the 2010 SIGN venous thromboembolism (VTE), guidelines:, General, , , , , , , , , , increased risk with advancing age, obesity, family history of VTE, pregnancy (especially puerperium), immobility, hospitalisation, anaesthesia, central venous catheter: femoral >> subclavian, , Underlying conditions
Page 961 :
, , , , , , , , , , , , malignancy, thrombophilia: e.g. Activated protein C resistance, protein C and S deficiency, heart failure, antiphospholipid syndrome, Behcet's, polycythaemia, nephrotic syndrome, sickle cell disease, paroxysmal nocturnal haemoglobinuria, hyperviscosity syndrome, homocystinuria, , Medication, , , , , , combined oral contraceptive pill: 3rd generation more than 2nd generation, hormone replacement therapy, raloxifene and tamoxifen, antipsychotics (especially olanzapine) have recently been shown to be a risk factor, , SIGN also state that the following are risk factors for recurrent VTE:, , , , , , previous unprovoked VTE, male sex, obesity, thrombophilias, Next question
Page 962 :
Question 80 of 147, A 42 year old lady is investigated for symptoms of irritability and altered bowel habit. On examination, she is noted to have a smooth enlargement of the thyroid gland. As part of her investigations thyroid, function tests are requested, these are as follows:, , TSH, , 0.1 mug/l, , Free T4, , 35 pmol/l, , The most likely underlying diagnosis is:, , Multinodular goitre, , Follicular carcinoma of the thyroid gland, , Graves disease, , Pregnancy, , None of the above, , TSH receptor antibodies will cause stimulation of the thyroid to synthesise T4. However, this will, have a negative feedback effect on the pituitary causing decrease in TSH levels., Where hyperthyroidism occurs secondary to pregnancy the TSH is typically elevated., Please rate this question:, , Discuss and give feedback, , Next question, , Thyroid disease, Patients may present with a number of different manifestations of thyroid disease. They can be, broadly sub classified according to whether they are euthyroid or have clinical signs of thyroid, dysfunction. In addition it needs to be established whether they have a mass or not., Assessment
Page 963 :
, , , , , History, Examination including USS, If a nodule is identified then it should be sampled ideally via an image guided fine needle, aspiration, Radionucleotide scanning is of limited use, , Thyroid Tumours, , , , , , , Papillary carcinoma, Follicular carcinoma, Anaplastic carcinoma, Medullary carcinoma, Lymphoma's, , Multinodular goitre, , , , , , One of the most common reasons for presentation, Provided the patient is euthyroid and asymptomatic and no discrete nodules are seen, they, can be reassured., In those with compressive symptoms surgery is required and the best operation is a total, thyroidectomy., Sub total resections were practised in the past and simply result in recurrent disease that, requires a difficult revisional resection., , Endocrine dysfunction, , , , , In general these patients are managed by physicians initially., Surgery may be offered alongside radio iodine for patients with Graves disease that fails with, medical management or in patients who would prefer not to be irradiated (e.g. pregnant, women)., Patients with hypothyroidism do not generally get offered a thyroidectomy. Sometimes, people inadvertently get offered resections during the early phase of Hashimotos thyroiditis,, however, with time the toxic phase passes and patients can simply be managed with, thyroxine., , Complications following surgery, , , , , Anatomical such as recurrent laryngeal nerve damage., Bleeding. Owing to the confined space haematoma's may rapidly lead to respiratory, compromise owing to laryngeal oedema., Damage to the parathyroid glands resulting in hypocalcaemia.
Page 965 :
Question 81 of 147, Which of the following is not a risk factor for developing tuberculosis?, , Gastrectomy, , Solid organ transplantation with immunosupression, , Intravenous drug use, , Haematological malignancy, , Amiodarone, , Risk factors for developing active tuberculosis include:, , , , , , , , , , silicosis, chronic renal failure, HIV positive, solid organ transplantation with immunosuppression, intravenous drug use, haematological malignancy, anti-TNF treatment, previous gastrectomy, , Please rate this question:, , Discuss and give feedback, , Next question, , Tuberculosis, Tuberculosis (TB) is an infection caused by Mycobacterium tuberculosis that most commonly affects, the lungs. Understanding the pathophysiology of TB can be difficult - the key is to differentiate, between primary and secondary disease., Primary tuberculosis, A non-immune host who is exposed to M. tuberculosis may develop primary infection of the lungs. A, small lung lesion known as a Ghon focus develops. The Ghon focus is composed of tubercle-laden, macrophages. The combination of a Ghon focus and hilar lymph nodes is known as a Ghon complex
Page 966 :
In immunocompetent people the initial lesion usually heals by fibrosis. Those who are, immunocompromised may develop disseminated disease (miliary tuberculosis)., Secondary (post-primary) tuberculosis, If the host becomes immunocompromised the initial infection may become reactivated. Reactivation, generally occurs in the apex of the lungs and may spread locally or to more distant sites. Possible, causes of immunocomprise include:, , , , , immunosuppressive drugs including steroids, HIV, malnutrition, , The lungs remain the most common site for secondary tuberculosis. Extra-pulmonary infection may, occur in the following areas:, , , , , , , central nervous system (tuberculous meningitis - the most serious complication), vertebral bodies (Pott's disease), cervical lymph nodes (scrofuloderma), renal, gastrointestinal tract, Next question
Page 967 :
Question 82 of 147, Which of the following is not true of gastric cancer?, , There is an association with blood group A, , Adenocarcinoma is the most common subtype, , Individuals with histological evidence of signet ring cells have a lower incidence of, lymph node metastasis, Lymphomas account for 5% cases, , In Western Countries a more proximal disease distribution has been noted, , Signet ring cells are features of poorly differentiated gastric cancer associated with a increased risk, of metastatic disease., Please rate this question:, , Discuss and give feedback, , Next question, , Gastric cancer, Overview, There are 700,000 new cases of gastric cancer worldwide each year. It is most common in Japan, and less common in western countries. It is more common in men and incidence rises with, increasing age. The exact cause of many sporadic cancer is not known, however, familial cases do, occur in HNPCC families. In addition, smoking and smoked or preserved foods increase the risk., Japanese migrants retain their increased risk (decreased in subsequent generations). The, distribution of the disease in western countries is changing towards a more proximal location, (perhaps due to rising obesity)., Pathology, There is some evidence of support a stepwise progression of the disease through intestinal, metaplasia progressing to atrophic gastritis and subsequent dysplasia, through to cancer. The, favoured staging system is TNM. The risk of lymph node involvement is related to size and depth of, invasion; early cancers confined to submucosa have a 20% incidence of lymph node metastasis., Tumours of the gastro-oesophageal junction are classified as below:
Page 968 :
Type, 1, , True oesophageal cancers and may be associated with Barrett's oesophagus., , Type, 2, , Carcinoma of the cardia, arising from cardiac type epithelium, or short segments with intestinal metaplasia at the oesophagogastric junction., , Type, 3, , Sub cardial cancers that spread across the junction. Involve similar nodal stations to, gastric cancer., , Groups for close endoscopic monitoring, , , , , , Intestinal metaplasia of columnar type, Atrophic gastritis, Low to medium grade dysplasia, Patients who have previously undergone resections for benign peptic ulcer disease (except, highly selective vagotomy)., , Referral to endoscopy, , Patients of any age with, dyspepsia and any of the, following, , Patients without, dyspepsia, , Worsening dyspepsia, , Chronic gastrointestinal bleeding, , Dysphagia, , Barretts oesophagus, , Dysphagia, , Unexplained abdominal, pain or weight loss, , Intestinal metaplasia, , Weight loss, , Vomiting, , Dysplasia, , Iron deficiency anaemia, , Upper abdominal mass, , Atrophic gastritis, , Upper abdominal mass, , Jaundice, , Patient aged over 55 years with, unexplained or persistent, dyspepsia
Page 969 :
Upper GI endoscopy performed for dyspepsia. The addition of dye spraying (as shown in the bottom, right) may facilitate identification of smaller tumours, , Image sourced from Wikipedia, , Staging, , , , , CT scanning of the chest abdomen and pelvis is the routine first line staging investigation in, most centres., Laparoscopy to identify occult peritoneal disease, PET CT (particularly for junctional tumours), , Treatment, , , , , , , Proximally sited disease greater than 5-10cm from the OG junction may be treated by sub, total gastrectomy, Total gastrectomy if tumour is <5cm from OG junction, For type 2 junctional tumours (extending into oesophagus) oesophagogastrectomy is usual, Endoscopic sub mucosal resection may play a role in early gastric cancer confined to the, mucosa and perhaps the sub mucosa (this is debated), Lymphadenectomy should be performed. A D2 lymphadenectomy is widely advocated by the, Japanese, the survival advantages of extended lymphadenectomy have been debated., However, the overall recommendation is that a D2 nodal dissection be undertaken.
Page 970 :
, , Most patients will receive chemotherapy either pre or post operatively., , Prognosis, UK Data, , Disease extent, , Percentage 5 year survival, , All RO resections, , 54%, , Early gastric cancer, , 91%, , Stage 1, , 87%, , Stage 2, , 65%, , Stage 3, , 18%, , Operative procedure, Total Gastrectomy , lymphadenectomy and Roux en Y anastomosis, General anaesthesia, Prophylactic intravenous antibiotics, Incision: Rooftop., Perform a thorough laparotomy to identify any occult disease., Mobilise the left lobe of the liver off the diaphragm and place a large pack over it. Insert a large self, retaining retractor e.g. omnitract or Balfour (take time with this, the set up should be perfect). Pack, the small bowel away., Begin by mobilising the omentum off the transverse colon., Proceed to detach the short gastric vessels., Mobilise the pylorus and divide it at least 2cm distally using a linear cutter stapling device., Continue the dissection into the lesser sac taking the lesser omentum and left gastric artery flush at, its origin., The lymph nodes should be removed en bloc with the specimen where possible., Place 2 stay sutures either side of the distal oesophagus. Ask the anaesthetist to pull back on the, nasogastric tube. Divide the distal oesophagus and remove the stomach., The oesphago jejunal anastomosis should be constructed. Identify the DJ flexure and bring a loop of, jejunum up to the oesophagus (to check it will reach). Divide the jejunum at this point. Bring the, divided jejunum either retrocolic or antecolic to the oesophagus. Anastamose the oesophagus to the, jejunum, using either interrupted 3/0 vicryl or a stapling device. Then create the remainder of the
Page 971 :
Roux en Y reconstruction distally., Place a jejunostomy feeding tube., Wash out the abdomen and insert drains (usually the anastomosis and duodenal stump). Help the, anaesthetist insert the nasogastric tube (carefully!), Close the abdomen and skin., Enteral feeding may commence on the first post-operative day. However, most surgeons will leave, patients on free NG drainage for several days and keep them nil by mouth., Next question
Page 972 :
Question 83 of 147, What is the most common presentation of a parotid gland tumour?, , Parapharyngeal mass, , Mass at anterior border of masseter, , Mass inferior to the angle of the mandible, , Mass behind the angle of the mandible, , Mass anterior to the ear, , Parotid tumours may present at any region in the gland. However, most lesions will be located, behind the angle of the mandible, inferior to the ear lobe. Tumours of the deep lobe of the parotid, may present as a parapharyngeal mass and large lesions may displace the tonsil., Please rate this question:, , Discuss and give feedback, , Next question, , Parotid gland malignancy, , , , , , , Most parotid neoplasms (80%) are benign lesions, Most commonly present with painless mass around the mandible, Up to 30% may present with pain, when this is associated with a discrete mass lesion in the, parotid it usually indicates perineural invasion., Perineural invasion is very unlikely to occur in association with benign lesions, 80% of patients with facial nerve weakness caused by parotid malignancies will have nodal, metastasis and a 5 year survival of 25%, , Types of malignancy, , Mucoepidermoid, carcinoma, , 30% of all parotid malignancies, Usually low potential for local invasiveness and metastasis (depends, mainly on grade)
Page 973 :
Adenoid cystic, carcinoma, , Unpredictable growth pattern, Tendency for perineural spread, Nerve growth may display skip lesions resulting in incomplete excision, Distant metastasis more common (visceral rather than nodal spread), 5 year survival 35%, , Mixed tumours, , Often a malignancy occurring in a previously benign parotid lesion, , Acinic cell carcinoma, , Intermediate grade malignancy, May show perineural invasion, Low potential for distant metastasis, 5 year survival 80%, , Adenocarcinoma, , Develops from secretory portion of gland, Risk of regional nodal and distant metastasis, 5 year survival depends upon stage at presentation, may be up to 75%, with small lesions with no nodal involvement, , Lymphoma, , Large rubbery lesion, may occur in association with Warthins tumours, Diagnosis should be based on regional nodal biopsy rather than parotid, resection Treatment is with chemotherapy (and radiotherapy), Next question
Page 974 :
Question 84 of 147, , A 52 year old male is referred to urology clinic with impotence. He is known to have hypertension., He does not have any morning erections. On further questioning the patient reports pain in his, buttocks, this worsens on mobilising. On examination there is some muscle atrophy. The penis and, scrotum are normal. What is the most likely diagnosis?, , Leriche syndrome, , S3-S4 cord lesion, , Pudendal nerve lesion, , Psychological impotence, , Beta blocker induced impotence, Leriche syndrome, Classically, it is described in male patients as a triad of symptoms:, 1. Claudication of the buttocks and thighs, 2. Atrophy of the musculature of the legs, 3. Impotence (due to paralysis of the L1 nerve), , Leriche syndrome, is atherosclerotic occlusive disease involving the abdominal aorta and/or both of, the iliac arteries. Management involves correcting underlying risk factors such as, hypercholesterolaemia and stopping smoking. Investigation is usually with angiography., Please rate this question:, , Discuss and give feedback, , Next question
Page 975 :
Leriche syndrome, Atheromatous disease involving the iliac vessels. Blood flow to the pelvic viscera is compromised., Patients may present with buttock claudication and impotence (in this particular syndrome)., Diagnostic work up will include angiography, where feasible, iliac occlusions are usually treated with, endovascular angioplasty and stent insertion., Next question
Page 976 :
Question 85 of 147, A 23 year old man presents with diarrhoea and passage of mucous. He is suspected of having, ulcerative colitis. Which of the following is least likely to be associated with this condition?, , Superficial mucosal inflammation in the colon, , Significant risk of dysplasia in long standing disease, , Epsiodes of large bowel obstruction during acute attacks, , Haemorrhage, , Disease sparing the anal canal, , Large bowel obstruction is not a feature of UC, patients may develop megacolon. However, this is a, different entity both diagnostically and clinically. Ulcerative colitis does not affect the anal canal and, the anal transitional zone. Inflammation is superficial. Dysplasia can occur in 2% overall, but, increases significantly if disease has been present over 20 years duration. Granulomas are features, of crohn's disease., , Other features:, , , , , Disease maximal in the rectum and may spread proximally, Contact bleeding, Longstanding UC crypt atrophy and metaplasia/dysplasia, , Please rate this question:, , Discuss and give feedback, , Next question, , Ulcerative colitis, Ulcerative colitis is a form of inflammatory bowel disease. Inflammation always starts at rectum,, does not spread beyond ileocaecal valve (although backwash ileitis may occur) and is continuous., The peak incidence of ulcerative colitis is in people aged 15-25 years and in those aged 55-65, years. It is less common in smokers.
Page 977 :
The initial presentation is usually following insidious and intermittent symptoms. Features include:, , , , , , , bloody diarrhoea, urgency, tenesmus, abdominal pain, particularly in the left lower quadrant, extra-intestinal features (see below), , Questions regarding the 'extra-intestinal' features of inflammatory bowel disease are common. Extraintestinal features include sclerosing cholangitis, iritis and ankylosing spondylitis., , Common to both Crohn's disease, (CD) and Ulcerative colitis (UC), , Notes, , Related to, disease activity, , Arthritis: pauciarticular, asymmetric, Erythema nodosum, Episcleritis, Osteoporosis, , Arthritis is the most common extraintestinal feature in both CD and UC, Episcleritis is more common in, Crohns disease, , Unrelated to, disease activity, , Arthritis: polyarticular, symmetric, Uveitis, Pyoderma gangrenosum, Clubbing, Primary sclerosing cholangitis, , Primary sclerosing cholangitis is, much more common in UC, Uveitis is more common in UC, , Pathology, , , , , , , , , Red, raw mucosa, bleeds easily, No inflammation beyond submucosa (unless fulminant disease), Widespread superficial ulceration with preservation of adjacent mucosa which has the, appearance of polyps ('pseudopolyps'), Inflammatory cell infiltrate in lamina propria, Neutrophils migrate through the walls of glands to form crypt abscesses, Depletion of goblet cells and mucin from gland epithelium, Granulomas are infrequent, , Barium enema, , , , , Loss of haustrations, Superficial ulceration, 'pseudopolyps', Long standing disease: colon is narrow and short -'drainpipe colon'
Page 978 :
Endoscopy, , , , , Superficial inflammation of the colonic and rectal mucosa, Continuous disease from rectum proximally, Superficial ulceration, mucosal islands, loss of vascular definition and continuous ulceration, pattern., , Management, , , , , Patients with long term disease are at increased risk of development of malignancy, Acute exacerbations are generally managed with steroids, in chronic patients agents such as, azathioprine and infliximab may be used, Individuals with medically unresponsive disease usually require surgery- in the acute phase, a sub total colectomy and end ileostomy. In the longer term a proctectomy will be required., An ileoanal pouch is an option for selected patients, , References, Ford A et al. Ulcerative colitis. BMJ 2013 (346):29-34., Next question
Page 979 :
Question 86 of 147, A 23 year old lady undergoes a total thyroidectomy as treatment for a papillary carcinoma of the, thyroid. The pathologist examines histological sections of the thyroid gland and identifies a, psammoma body. What are these primarily composed of?, , Clusters of calcification, , Aggregations of neutrophils, , Aggregations of macrophages, , Giant cells surrounding the tumour, , Clusters of oxalate crystals, , Psammoma bodies consist of clusters of microcalcification. They are most commonly seen in, papillary carcinomas., Please rate this question:, , Discuss and give feedback, , Next question, , Thyroid malignancy, Papillary carcinoma, , , , , , Commonest sub-type, Accurately diagnosed on fine needle aspiration cytology, Histologically, they may demonstrate psammoma bodies (areas of calcification) and so, called 'orphan Annie' nuclei, They typically metastasise via the lymphatics and thus laterally located apparently ectopic, thyroid tissue is usually a metastasis from a well differentiated papillary carcinoma, , Follicular carcinoma, , , Are less common than papillary lesions
Page 980 :
, , , , Like papillary tumours, they may present as a discrete nodule. Although they appear to be, well encapsulated macroscopically there is invasion on microscopic evaluation, Lymph node metastases are uncommon and these tumours tend to spread, haematogenously. This translates into a higher mortality rate, Follicular lesions cannot be accurately diagnosed on fine needle aspiration cytology and thus, all follicular FNA's (THY 3f) will require at least a hemi thyroidectomy, , Anaplastic carcinoma, , , , Less common and tend to occur in elderly females, Disease is usually advanced at presentation and often only palliative decompression and, radiotherapy can be offered., , Medullary carcinoma, , , , , , These are tumours of the parafollicular cells ( C Cells) and are of neural crest origin., The serum calcitonin may be elevated which is of use when monitoring for recurrence., They may be familial and occur as part of the MEN -2A disease spectrum., Spread may be either lymphatic or haematogenous and as these tumours are not derived, primarily from thyroid cells they are not responsive to radioiodine., , Lymphoma, , , , These respond well to radiotherapy, Radical surgery is unnecessary once the disease has been diagnosed on biopsy material., Such biopsy material is not generated by an FNA and thus a core biopsy has to be obtained, (with care!)., Next question
Page 981 :
Question 87 of 147, A 52 year old woman attends clinic for investigation of abdominal pain and constipation. On, examination you note blue lines on the gum margin. She mentions that her legs have become weak, in the past few days. What is the most likely diagnosis?, , Acute intermittent porphyria, , Lead poisoning, , Constipation, , Guillan Barre syndrome, , Rectal carcinoma, , This would be an impressive diagnosis to make in the surgical out patient department! The, combination of abdominal pain and a motor periperal neuropathy, should indicate this diagnosis. The, blue line along the gum margin can occur in up to 20% patients with lead poisoning., Please rate this question:, , Discuss and give feedback, , Next question, , Lead poisoning, Along with acute intermittent porphyria, lead poisoning should be considered in questions giving a, combination of abdominal pain and neurological signs, Features, , , , , , , abdominal pain, peripheral neuropathy (mainly motor), fatigue, constipation, blue lines on gum margin (only 20% of adult patients, very rare in children), , Investigations
Page 982 :
, , , , , The blood lead level is usually used for diagnosis. Levels greater than 10 mcg/dl are, considered significant, Full blood count: microcytic anaemia. Blood film shows red cell abnormalities including, basophilic stippling and clover-leaf morphology, Raised serum and urine levels of delta aminolaevulinic acid may be seen making it, sometimes difficult to differentiate from acute intermittent porphyria, Urinary coproporphyrin is also increased (urinary porphobilinogen and uroporphyrin levels, are normal to slightly increased), , Management - various chelating agents are currently used:, , , , , , Dimercaptosuccinic acid (DMSA), D-penicillamine, EDTA, Dimercaprol, Next question
Page 983 :
Question 88-90 of 147, Theme: Vasculitis, , A., B., C., D., E., , Wegeners granulomatosis, Polyarteritis nodosa, Giant cell arteritis, Takayasu's arteritis, Buergers disease, , For each of the scenarios provided please select the most likely underlying diagnosis from the list, below. Each option may be used once, more than once or not at all., , 88., , A 20 year old lady is referred to the vascular clinic. She has been feeling generally unwell, for the past six weeks. She works as a typist and has noticed increasing pain in her, forearms whilst working. On examination she has absent upper limb pulses. Her ESR is, measured and mildly elevated., You answered Wegeners granulomatosis, The correct answer is Takayasu's arteritis, Takayasus arteritis may be divided into acute systemic phases and the chronic pulseless, phase. In the latter part of the disease process the patient may complain of symptoms such, as upper limb claudication. In the later stages of the condition the vessels will typically, show changes of intimal proliferation, together with band fibrosis of the intima and media., , 89., , A 32 year old man presents to the vascular clinic with symptoms of foot pain during, exertion. He is a heavy smoker and has recently tried to stop smoking. On examination he, has normal pulses to the level of the popliteal. However, foot pulses are absent. A, diagnostic angiogram is performed which shows an abrupt cut off at the level of the, anterior tibial artery, together with the formation of corkscrew shaped collateral vessels, distally., You answered Wegeners granulomatosis, The correct answer is Buergers disease, Buergers disease is most common in young male smokers. This demographic is changing, in those areas where young female smokers are more common. In the acute lesion the, internal elastic lamina of the vessels is usually intact. As the disease progresses the, changes progress to hypercellular occlusive thrombus. Tortuous corkscrew collaterals may, reconstitute patent segments of the distal tibial or pedal vessels.
Page 984 :
90., , A 78 year old man presents with symptoms of headaches and deteriorating vision. He, notices that there is marked pain on the right hand side of his face when he combs his hair., You answered Wegeners granulomatosis, The correct answer is Giant cell arteritis, Temporal arteritis may present acutely with symptoms of headache and visual loss, or with, a less acute clinical picture. Sight may be threatened and treatment with, immunosupressants should be started promptly. The often requested temporal artery, biopsy (which can be the bane of many surgeons) is often non diagnostic and unhelpful., , Please rate this question:, , Discuss and give feedback, , Next question, , Vasculitis, The vasculitides are a group of conditions characterised by inflammation of the blood vessel walls., This may, in turn, compromise vessel integrity. Constitutional symptoms may be present. Whilst, certain disease subtypes are reported to affect specific vessels, there is often a degree of overlap, clinically., Vessel diameter and vasculitis classification, , Aorta and branches, , , , , , Takayasu's arteritis, Buergers disease, Giant cell arteritis, , Large and medium sized arteries, , , , , , Buergers disease, Giant cell arteritis, Polyarteritis nodosa, , Medium sized muscular arteries, , , , , Polyarteritis nodosa, Wegeners granulomatosis, , Small muscular arteries, , , , , Wegeners granulomatosis, Rheumatoid vasculitis, , Specific conditions
Page 985 :
Takyasu's arteritis, , , , , , , , Inflammatory, obliterative arteritis affecting aorta and branches, Females> Males, Symptoms may include upper limb claudication, Clinical findings include diminished or absent pulses, ESR often affected during the acute phase, , Buergers disease, , , , Segmental thrombotic occlusions of the small and medium sized, lower limb vessels, Commonest in young male smokers, Proximal pulses usually present, but pedal pulses are lost, An acuter hypercellular occlusive thrombus is often present, Tortuous corkscrew shaped collateral vessels may be seen on, angiography, , , , , , , Giant cell arteritis, , , , , , , Polyarteritis nodosa, , , , , , , Wegeners, granulomatosis, , , , , , , Systemic granulomatous arteritis that usually affects large and, medium sized vessels, Females > Males, Temporal arteritis is commonest type, Granulomatous lesions may be seen on biopsy (although up to, 50% are normal), Systemic necrotising vasculitis affecting small and medium sized, muscular arteries, Most common in populations with high prevalence of hepatitis B, Renal disease is seen in 70% cases, Angiography may show saccular or fusiform aneurysms and, arterial stenoses, Predominantly affects small and medium sized arteries, Systemic necrotising granulomatous vasculitis, Cutaneous vascular lesions may be seen (ulceration, nodules and, purpura), Sinus imaging may show mucosal thickening and air fluid levels, , Treatment, Conditions such as Buergers disease are markedly helped by smoking cessation., Immunosupression is the main treatment for vasculitides., Next question
Page 986 :
Question 91 of 147, A 28 year old man presents with right upper quadrant pain and hydatid disease is suspected. Which, of the following statements relating to the disease is untrue?, , First line treatment is with pentavalent antimony., , Peritoneal contamination with active daughter cysts may complicate surgery., , CT scanning of the liver may show a floating membrane., , Biliary communication with the cysts may occur., , It is caused by Echinococcus granulosus., , Drug treatment is with albendazole or mebendazole. Praziquantzel may be used in the pre operative, stages., Please rate this question:, , Discuss and give feedback, , Next question, , Hydatid cysts, Hydatid cysts are endemic in Mediterranean and Middle Eastern countries. They are caused by the, tapeworm parasite Echinococcus granulosus. An outer fibrous capsule is formed containing multiple, small daughter cysts. These cysts are allergens which precipitate a type 1 hypersensitivity, reaction., Clinical features are as follows:, , , , , , Up to 90% cysts occur in the liver and lungs, Can be asymtomatic, or symptomatic if cysts > 5cm in diameter, Morbidity caused by cyst bursting, infection and organ dysfunction (biliary, bronchial, renal, and cerebrospinal fluid outflow obstruction), In biliary ruputure there may be the classical triad of; biliary colic, jaundice, and urticaria, , CT is the best investigation to differentiate hydatid cysts from amoebic and pyogenic cysts.
Page 987 :
Surgery is the mainstay of treatment (the cyst walls must not be ruptured during removal and the, contents sterilised first)., Next question
Page 988 :
Question 92 of 147, Which of the following statements relating to neutrophil polymorphs is true?, , Produce nitrogen peroxide as a microbicidal agent, , Not involved in opsonisation, , Deficiency leads to AIDS, , Neutrophil disorders always result in chronic granulomatous diseases, , Have a lifespan of 9 hours, , , , , , , , , Neutrophils are the main cells of acute inflammation, important action against gram -ve and, +ve bacteria, Appearance of segmented nucleus and granulated cytoplasm, Have a lifespan of 1-3 days (shorter when consumed during septic process, though 9 hours, is unusual), Actions include: movement, opsonise microorganisms, phagocytosis & intracellular killing of, microorganisms via aerobic (produce HYDROGEN PEROXIDE) & anaerobic mechanisms., Neutrophil disorders include chronic granulomatous diseases: rare, AIDS associated with T cell deficiency, , Please rate this question:, , Discuss and give feedback, , Next question, , Acute inflammation, Inflammation is the reaction of the tissue elements to injury. Vascular changes occur, resulting in the, generation of a protein rich exudate. So long as the injury does not totally destroy the existing tissue, architecture, the episode may resolve with restoration of original tissue architecture., Vascular changes, , , Vasodilation occurs and persists throughout the inflammatory phase.
Page 989 :
, , , , Inflammatory cells exit the circulation at the site of injury., The equilibrium that balances Starlings forces within capillary beds is disrupted and a protein, rich exudate will form as the vessel walls also become more permeable to proteins., The high fibrinogen content of the fluid may form a fibrin clot. This has several important, immunomodulatory functions., , Sequelae, , Resolution, , , , , Typically occurs with minimal initial injury, Stimulus removed and normal tissue architecture results, , Organisation, , , , , Delayed removal of exudate, Tissues undergo organisation and usually fibrosis, , Suppuration, , , , , Typically formation of an abscess or an empyema, Sequestration of large quantities of dead neutrophils, , Progression to chronic, inflammation, , , , , Coupled inflammatory and reparative activities, Usually occurs when initial infection or suppuration has, been inadequately managed, , Causes, , , , , , , Infections e.g. Viruses, exotoxins or endotoxins released by bacteria, Chemical agents, Physical agents e.g. Trauma, Hypersensitivity reactions, Tissue necrosis, , Presence of neutrophil polymorphs is a histological diagnostic feature of acute inflammation, Next question
Page 990 :
Question 93 of 147, , A 33 year old man is involved in a road traffic accident. He is initially stable and transferred to the, accident and emergency department. On arrival he is catheterised. One minute later he becomes, hypotensive, with evidence of angioedema surrounding his penis. What is the most likely explanation, for this event?, , Type V latex hypersensitivity reaction, , Type IV latex hypersensitivity reaction, , Type III latex hypersensitivity reaction, , Type I latex hypersensitivity reaction, , Type II latex hypersensitivity reaction, , Theme from January 2013 exam, Theme from April 2012 Exam, Sudden collapse and angioedema following exposure to latex (of which most urinary catheters are, manufactured) suggests a type I hypersensitivity reaction., Please rate this question:, , Discuss and give feedback, , Next question, , Hypersensitivity reactions, The Gell and Coombs classification divides hypersensitivity reactions into 4 types
Page 992 :
Question 94 of 147, A 43 year old female develops severe chest wall cellulitis following a mastectomy. On examination, the skin is markedly erythematous. Which of the acute inflammatory mediators listed below is least, likely to produce vasodilation?, , Complement component C5a, , Lysosomal compounds, , Histamine, , Serotonin, , Prostaglandins, , Erythema is a classical feature of acute inflammation. Potent mediators of vascular dilatation, include; histamine, prostaglandins, nitric oxide, platelet activating factor, complement C5a (and C3a), and lysosomal compounds. Although serotonin is associated with acute inflammation it is a, vasoconstrictor. The effects of serotonin are dependent upon the state of the vessels in the tissues., Intact and healthy tissues and vessels will respond to a serotonin infusion with vasodilation (hence, the flushing seen in carcinoid syndrome). In contrast it worsens cardiac ischaemia in myocardial, infarcts when released from damaged platelets., Please rate this question:, , Discuss and give feedback, , Next question, , Acute inflammation, Inflammation is the reaction of the tissue elements to injury. Vascular changes occur, resulting in the, generation of a protein rich exudate. So long as the injury does not totally destroy the existing tissue, architecture, the episode may resolve with restoration of original tissue architecture., Vascular changes, , , , , Vasodilation occurs and persists throughout the inflammatory phase., Inflammatory cells exit the circulation at the site of injury., The equilibrium that balances Starlings forces within capillary beds is disrupted and a protein, rich exudate will form as the vessel walls also become more permeable to proteins.
Page 993 :
, , The high fibrinogen content of the fluid may form a fibrin clot. This has several important, immunomodulatory functions., , Sequelae, , Resolution, , , , , Typically occurs with minimal initial injury, Stimulus removed and normal tissue architecture results, , Organisation, , , , , Delayed removal of exudate, Tissues undergo organisation and usually fibrosis, , Suppuration, , , , , Typically formation of an abscess or an empyema, Sequestration of large quantities of dead neutrophils, , Progression to chronic, inflammation, , , , , Coupled inflammatory and reparative activities, Usually occurs when initial infection or suppuration has, been inadequately managed, , Causes, , , , , , , Infections e.g. Viruses, exotoxins or endotoxins released by bacteria, Chemical agents, Physical agents e.g. Trauma, Hypersensitivity reactions, Tissue necrosis, , Presence of neutrophil polymorphs is a histological diagnostic feature of acute inflammation, Next question
Page 994 :
Question 95 of 147, , A 43 year old man presents with a 3 week history of malaise, sore throat, odynophagia and, dysphagia. On examination he is found to have patchy white spots in his oropharynx. An upper GI, endoscopy is performed and similar lesions are identified in the oesophagus. Which investigation is, most likely to identify the underlying pathology in this case?, , Serum urea and electrolytes, , Oesophageal biopsy for culture, , Oesophageal biopsy for histology, , Glucose tolerance testing, , Viral serology, , Oesophageal candidiasis is associated with immunosupression; mainly in patients on chemotherapy,, with haematological malignancy, HIV or inhaled steroids. In patients with HIV, oesophageal, candidiasis is part of the spectrum of AIDS defining illnesses and usually occurs when the CD4, count is less than 200. Others include PCP pneumonia and CMV infections., Please rate this question:, , Discuss and give feedback, , Next question, , Oesophageal candidiasis, Characterised by white spots in the oropharynx with extension into the oesophagus. Associated with, broad spectrum antibiotic usage, immunosupression and immunological disorders., Patients may present with oropharyngeal symptoms, odynophagia and dysphagia.
Page 995 :
Treatment is directed both at the underlying cause (which should be investigated for) and with oral, antifungal agents., Next question
Page 996 :
Question 96-98 of 147, Theme: Colonic obstruction, , A., B., C., D., E., , Malignant obstruction, Ogilvies syndrome, Volvulus, Diverticular stricture, Ischaemic stricture, , Please select the most likely cause of obstruction for the situation described. Each option may be, used once, more than once or not at all., , 96., , A 78 year old man has undergone a hemi-arthroplasty for a intracapsular hip fracture. Post, operatively he develops electrolyte derangement and receives intravenous fluids. Over the, previous 24 hours he develops marked abdominal distension. On examination he has a, tense, tympanic abdomen which is not painful. A contrast enema shows flow of contrast, through to the caecum and through the ileocaecal valve., You answered Malignant obstruction, The correct answer is Ogilvies syndrome, Patients with electrolyte disturbance and previous surgery may develop colonic pseudoobstruction (Ogilvies syndrome). The diagnosis is made using a contrast enema and, treatment is usually directed at the underlying cause with colonic decompression if, indicated., , 97., , A 67 year old man has had multiple episodes with fever and left iliac fossa pain. These, have usually resolved with courses of intravenous antibiotics. He is admitted with a history, of increasing constipation and abdominal distension. A contrast x-ray is performed which, shows flow of contrast to the sigmoid colon, here the contrast flows through a long narrow, segment of colon into dilated proximal bowel., You answered Malignant obstruction, The correct answer is Diverticular stricture, The long history of left iliac fossa pain and development of bowel obstruction suggests a, diverticular stricture. These may contain a malignancy and most will require resection., , 98., , A 78 year old lady from a nursing home is admitted with a 24 hour history of absolute, constipation and abdominal pain. On examination she has a distended abdomen with a soft
Page 997 :
mass in her left iliac fossa. An x-ray is performed which shows a large dilated loop of, bowel in the left iliac fossa which contains a fluid level., You answered Malignant obstruction, The correct answer is Volvulus, Sigmoid volvulus may present with an asymmetrical mass in an elderly patient. It may, contain a fluid level, visible on plain films., Please rate this question:, , Discuss and give feedback, , Next question, , Colonic obstruction, Cause, , Features, , Cancer, , , , , , , , Usually insidious onset, History of progressive constipation, Systemic features (e.g. anaemia), Abdominal distension, Absence of bowel gas distal to site of, obstruction, , Establish diagnosis (e.g., contrast enema/ endoscopy), Laparotomy and resection,, stenting, defunctioning, colostomy or bypass, , Diverticular, stricture, , , , Usually history of previous acute, diverticulitis, Long history of altered bowel habit, Evidence of diverticulosis on imaging or, endoscopy, , Once diagnosis established,, usually surgical resection, Colonic stenting should not, be performed for benign, disease, , Twisting of bowel around its mesentery, Sigmoid colon affected in 76% cases, Patients usually present with abdominal, pain, bloating and constipation, Examination usually shows asymmetrical, distension, Plain X-rays usually show massively, dilated sigmoid colon, loss of haustra and, , Initial treatment is to, untwist the loop, a flexible, sigmoidoscopy may be, needed, Those with clinical, evidence of ischaemia, should undergo surgery, Patient with recurrent, , , , , Volvulus, , , , , , , , Treatment
Page 998 :
Acute colonic, pseudoobstruction, , , , , , , , "U" shape are typical, the loop may, contain fluid levels, , volvulus should undergo, resection, , Symptoms and signs of large bowel, obstruction with no lesion, Usually associated with metabolic, disorders, Usually a cut off in the left colon (82%, cases), Although abdomen tense and distended,, it is usually not painful, All patients should undergo contrast, enema (may be therapeutic!), , Colonoscopic, decompression, Correct metabolic disorders, IV neostigmine, Surgery, , Next question
Page 999 :
Question 99 of 147, , A 52 year old man with dyspepsia is found to have a duodenal ulcer. A CLO test is taken and is, positive. Which statement relating to the likely causative organism is false?, , It is a gram negative organism, , It preferentially colonises gastric type mucosa, , It may occupy areas of ectopic gastric metaplasia, , In patients who are colonised there is commonly evidence of fundal gastritis on endoscopy, , It produces a powerful urease that forms the basis of the Clo test, Helicobacter pylori accounts for >75% cases of duodenal ulceration. It may be diagnosed with either, serology, microbiology, histology or CLO testing., , Theme from January 2011 Exam, Helicobacter pylori rarely produces any typical features on endoscopy. Where infection is suspected, the easiest course of action is to take an antral biopsy for Clo testing in the endoscopy suite., Please rate this question:, , Discuss and give feedback, , Next question, , Helicobacter Pylori, Infection with Helicobacter Pylori is implicated in many cases of duodenal ulceration and up to 60%, of patients with gastric ulceration., It is a gram negative, helical shaped rod with microaerophillic requirements. It has the ability to
Page 1000 :
produce a urease enzyme that will hydrolyse urea resulting in the production of ammonia. The effect, of ammonia on antral G cells is to cause release of gastrin via a negative feedback loop., Once infection is established the organism releases enzymes that disrupt the gastric mucous layer., Certain subtypes release cytotoxins cag A and vac A gene products. The organism incites a, classical chronic inflammatory process of the gastric epithelium. This accounts for the development, of gastric ulcers. The mildly increased acidity may induce a process of duodenal gastric metaplasia., Whilst duodenal mucosa cannot be colonised by H-Pylori, mucosa that has undergone metaplastic, change to the gastric epithelial type may be colonised by H- Pylori with subsequent inflammation, and development of duodenitis and ulcers., In patients who are colonised there is a 10-20% risk of peptic ulcer, 1-2% risk gastric cancer and, <1% risk MALT lymphoma., Next question
Page 1001 :
Question 100 of 147, A 34 year old male presents with painful rectal bleeding and a fissure in ano is suspected. On, examination he has an epithelial defect at the mucocutaenous junction that is located anteriorly., Approximately what proportion of patients with fissure in ano will present with this pattern of, disease?, , 90%, , 10%, , 50%, , 25%, , 100%, , Only a minority of patients with fissure in ano will have an anteriorly sited fissure. They are, particularly rare in males and an anterior fissure in a man should prompt a search for an underlying, cause., Please rate this question:, , Discuss and give feedback, , Next question, , Anal fissure, Anal fissures are a common cause of painful, bright red, rectal bleeding., Most fissures are idiopathic and present as a painful mucocutaneous defect in the posterior midline, (90% cases). Fissures are more likely to be anteriorly located in females, particularly if they are, multiparous. Multiple fissures and those which are located at other sites are more likely to be due to, an underlying cause., Diseases associated with fissure in ano include:, , , , , Crohns disease, Tuberculosis, Internal rectal prolapse, , Diagnosis
Page 1002 :
In most cases the defect can be visualised as a posterior midline epithelial defect. Where symptoms, are highly suggestive of the condition and examination findings are unclear an examination under, anaesthesia may be helpful. Atypical disease presentation should be investigated with colonoscopy, and EUA with biopsies of the area., Treatment, Stool softeners are important as the hard stools may tear the epithelium and result in recurrent, symptoms. The most effective first line agents are topically applied GTN (0.2%) or Diltiazem (2%), paste. Side effects of diltiazem are better tolerated., Resistant cases may benefit from injection of botulinum toxin or lateral internal sphincterotomy, (beware in females). Advancement flaps may be used to treat resistant cases., Sphincterotomy produces the best healing rates. It is associated with incontinence to flatus in up to, 10% of patients in the long term., Next question
Page 1003 :
Question 101 of 147, The pathogenesis of osteopetrosis is best explained by a defect in which of the following?, , Osteoclast function, , PTH receptors, , Osteoblast function, , Calcium resorption in proximal tubule, , Calcium absorption, , Please rate this question:, , Discuss and give feedback, , Next question, , Osteopetrosis, Overview, , , , , Also known as marble bone disease, Rare disorder of defective osteoclast function resulting in failure of normal bone resorption, Stem cell transplant and interferon-gamma have been used for treatment, Next question
Page 1004 :
Question 102 of 147, A 13 month old boy is brought to the surgical clinic by his mother because his left testicle is not, located in the scrotum. At which of the following sites would the testicle be located if it were an, ectopic testis?, , Canalicular, , Inguinal, , External inguinal ring, , Superficial inguinal pouch, , High scrotal, , Theme from September 2013 Exam, Theme from January 2012 Exam, Ectopic testes are those that come to lie outside the normal range of embryological descent (i.e. in, the superficial inguinal pouch). Other sites of ectopic testes include; base of penis, femoral triangle, and perineum., Please rate this question:, , Discuss and give feedback, , Next question, , Testicular disorders-paediatric, Testicular disorders, Testicular disorders are some of the commonest conditions present in paediatric urological practice., Cryptorchidism, , , , The embryological descent of the testicle from within the abdominal cavity may be subject to, a number of variations. Distinctions need to be made clinically from a non descended testis, and a testis that is retractile., Testis that lie outside the normal path of embryological descent are termed ectopic testis., Undescended testis occurs in 1% of male infants. Where the testis does not lie in an intra, scrotal location, its location should be ascertained (by laparoscopy in first instance). Where, both testes are absent, the infant may be intersex.
Page 1005 :
, , , , , MRI scanning may reveal intra-abdominal testes; however a GA is often needed to perform, this investigation in this age group., Testes that are undescended should be placed in the scrotum after 1 year of age, as the, testosterone surge that may facilitate descent occurs at 6 months of age., Where the testes lie distally e.g. Superficial inguinal pouch an open orchidopexy is the, procedure of choice., With abdominal testes a laparoscopy should be performed. The risk of seminoma is, increased in individuals with a non descended testes and this risk is not reduced by, orchidopexy., , Testicular torsion, , , , , , , Typically the patient has severe sudden onset of scrotal pain. The difficulty in paediatric, practice is the lack of clear history., On examination the testis is tender and enlarged., Management is by surgical exploration., Delay beyond 6 hours is associated with low salvage rates., A torted hyatid produces pain that is far more localised and the testis itself should feel, normal. However, diagnostic doubt often exists and in such cases surgical exploration is, warranted., , Hydrocele, , , , , , Occur secondary to patent processus vaginalis, Present as fluid filling in scrotum or as cyst of the spermatic cord, Communicating hydroceles are treated by a trans inguinal ligation of the PPV, Cystic hydroceles in older children may be treated with scrotal exploration, Next question
Page 1006 :
Question 103 of 147, Which of the following is seen more commonly with Crohns disease rather than ulcerative colitis?, , Mucosal islands at endoscopy, , Goblet cell depletion on biopsy, , Fat wrapping of the terminal ileum, , Attenuated symptoms in smokers, , Toxic megacolon, Crohns disease is worse in smokers and smoking is an independent risk factor for disease, recurrence following resection., Fat wrapping of the terminal ileum is commonly seen in patients with ileal disease (the commonest, disease site). The mesenteric fat in patients with IBD is often dense, hard and prone to considerable, haemorrhage during surgery. At endoscopy, the mucosa in patients with Crohns disease is said to, resemble cobblestones, mucosal islands (pseudopolyps) are seen in ulcerative colitis., Please rate this question:, , Discuss and give feedback, , Next question, , Crohns disease, Crohns disease is a chronic transmural inflammation of a segment(s) of the gastrointestinal tract and, may be associated with extra intestinal manifestations. Frequent disease patterns observed include, ileal, ileocolic and colonic disease. Peri-anal disease may occur in association with any of these. The, disease is often discontinuous in its distribution. Inflammation may cause ulceration, fissures, fistulas, and fibrosis with stricturing. Histology reveals a chronic inflammatory infiltrate that is usually patchy, and transmural., Ulcerative colitis Vs Crohns, , Crohn's disease, , Ulcerative colitis
Page 1008 :
, , , , , Bile salt diarrhoea secondary to terminal ileal disease, Entero-colic fistula, Short bowel due to multiple resections, Bacterial overgrowth, , Surgical interventions in Crohns disease, The commonest disease pattern in Crohns is stricturing terminal ileal disease and this often, culminates in an ileocaecal resection. Other procedures performed include segmental small bowel, resections and stricturoplasty. Colonic involvement in patients with Crohns is not common and,, where found, distribution is often segmental. However, despite this distribution segmental resections, of the colon in patients with Crohns disease are generally not advocated because the recurrence, rate in the remaining colon is extremely high, as a result the standard options of colonic surgery in, Crohns patients are generally; sub total colectomy, panproctocolectomy and staged sub total, colectomy and proctectomy. Restorative procedures such as ileoanal pouch have no role in therapy., Crohns disease is notorious for the developmental of intestinal fistulae; these may form between the, rectum and skin (peri anal) or the small bowel and skin. Fistulation between loops of bowel may also, occur and result in bacterial overgrowth and malabsorption. Management of enterocutaneous, fistulae involves controlling sepsis, optimising nutrition, imaging the disease and planning definitive, surgical management., Next question
Page 1009 :
Question 104 of 147, A splenectomy increases the risk of infection from all the following organisms except?, , Pneumococcus, , Klebsiella, , Haemophilus influenzae, , Staphylococcus aureus, , Neisseria meningitidis, , Theme from 2010 Exam, Staphylococcus aureus infection following splenectomy is no more common than in non, splenectomised individuals. The other organisms are encapsulated, which is why they are more, likely to cause overwhelming post splenectomy sepsis., Please rate this question:, , Discuss and give feedback, , Next question, , Post splenectomy sepsis, Hyposplenism may complicate certain medical conditions where splenic atrophy occurs or may be, the result of medical intervention such as splenic artery embolization and splenectomy for trauma., Diagnosis of hyposplenism is difficult and whilst there may be peripheral markers of the, splenectomised state (e.g. Howell Jolly bodies) these are neither 100% sensitive or specific. The, most sensitive test is a radionucleotide labeled red cell scan., Hyposplenism, by whatever mechanism it occurs dramatically increases the risk of post splenectomy, sepsis, particularly with encapsulated organisms. Since these organisms may be opsonised, but this, then goes undetected at an immunological level due to loss of the spleen. For this reason individuals, are recommended to be vaccinated and have antibiotic prophylaxis., Key recommendations, , , All those with hyposplenism or may become so (such as prior to an elective splenectomy), should receive pneumococcal, haemophilus type b and meningococcal type C vaccines.
Page 1010 :
, , , , , These should be administered 2 weeks prior to splenectomy or two weeks following, splenectomy. The vaccine schedule for meningococcal disease essentially consists of a, dose of Men C and Hib at 2 weeks and then a dose of the MenACWY vaccine one month, later. Those aged under 2 may require a booster at 2 years. A dose of pneumococcal, polyvalent polysaccharide vaccine (PPV) is given at two weeks. A conjugated vaccine (PCV), is offered to young children. The PCV is more immunogenic but covers fewer serotypes., Boosting PPV is either guided by serological measurements (where available) or by routine, boosting doses at 5 yearly intervals., Annual influenza vaccination is recommended in all cases, Antibiotic prophylaxis is offered to all. The risk of post splenectomy sepsis is greatest, immediately following splenectomy and in those aged less than 16 years or greater than 50, years. Individuals with a poor response to pneumococcal vaccination are another high risk, group. High risk individuals should be counselled to take penicillin or macrolide prophylaxis., Those at low risk may choose to discontinue therapy. All patients should be advised about, taking antibiotics early in the case of intercurrent infections., Asplenic individuals traveling to malaria endemic areas are at high risk and should have both, pharmacological and mechanical protection., , Dosing, Penicillin V 500mg BD or amoxicillin 250mg BD, References, Davies J et al. Review of guidelines for the prevention and treatment of infection in patients with an, absent or dysfunctional spleen: Prepared on behalf of the British Committee for Standards in, Haematology by a Working Party of the Haemato-Oncology Task Force. British Journal of, Haematology2011 (155): 308317., Next question
Page 1013 :
, , , , , Bile salt diarrhoea secondary to terminal ileal disease, Entero-colic fistula, Short bowel due to multiple resections, Bacterial overgrowth, , Surgical interventions in Crohns disease, The commonest disease pattern in Crohns is stricturing terminal ileal disease and this often, culminates in an ileocaecal resection. Other procedures performed include segmental small bowel, resections and stricturoplasty. Colonic involvement in patients with Crohns is not common and,, where found, distribution is often segmental. However, despite this distribution segmental resections, of the colon in patients with Crohns disease are generally not advocated because the recurrence, rate in the remaining colon is extremely high, as a result the standard options of colonic surgery in, Crohns patients are generally; sub total colectomy, panproctocolectomy and staged sub total, colectomy and proctectomy. Restorative procedures such as ileoanal pouch have no role in therapy., Crohns disease is notorious for the developmental of intestinal fistulae; these may form between the, rectum and skin (peri anal) or the small bowel and skin. Fistulation between loops of bowel may also, occur and result in bacterial overgrowth and malabsorption. Management of enterocutaneous, fistulae involves controlling sepsis, optimising nutrition, imaging the disease and planning definitive, surgical management., Next question
Page 1014 :
Question 106 of 147, Which of the following is not considered a risk factor for the development of oesophageal, malignancy?, , Oesophageal metaplasia, , Smoking, , Excessive intake of alcoholic spirits, , Achalasia, , Blood group O, , Blood group O is not a risk factor for oesophageal cancer. Achalasia is associated with the risk of, developing squamous cell carcinoma of the oesophagus., Please rate this question:, , Discuss and give feedback, , Next question, , Oesophageal cancer, , , , , , , Incidence is increasing, In most cases in the Western world this increase is accounted for by a rise in the number of, cases of adenocarcinoma. In the UK adenocarcinomas account for 65% of cases., Barretts oesophagus is a major risk factor for most cases of oesophageal adenocarcinoma., In other regions of the world squamous cancer is more common and is linked to smoking,, alcohol intake, diets rich in nitrosamines and achalasia., Surveillance of Barretts is important, as it imparts a 30 fold increase in cancer risk and if, invasive malignancy is diagnosed early then survival may approach 85% at 5 years., , Diagnosis, , , , Upper GI endoscopy is the first line test, Contrast swallow may be of benefit in classifying benign motility disorders but has no place, in the assessment of tumours
Page 1015 :
, , , , Staging is initially undertaken with CT scanning of the chest, abdomen and pelvis. If overt, metastatic disease is identified using this modality then further complex imaging is, unnecessary, If CT does not show metastatic disease, then local stage may be more accurately assessed, by use of endoscopic ultrasound., Staging laparoscopy is performed to detect occult peritoneal disease. PET CT is performed, in those with negative laparoscopy. Thoracoscopy is not routinely performed., , Treatment, Operable disease is best managed by surgical resection. The most standard procedure is an IvorLewis type oesophagectomy. This procedure involves the mobilisation of the stomach and division of, the oesophageal hiatus. The abdomen is closed and a right sided thoracotomy performed. The, stomach is brought into the chest and the oesophagus mobilised further. An intrathoracic, oesophagogastric anastomosis is constructed. Alternative surgical strategies include a transhiatal, resection (for distal lesions), a left thoraco-abdominal resection (difficult access due to thoracic, aorta) and a total oesophagectomy (McKeown) with a cervical oesophagogastric anastomosis., The biggest surgical challenge is that of anastomotic leak, with an intrathoracic anastomosis this will, result in mediastinitis. With high mortality. The McKeown technique has an intrinsically lower, systemic insult in the event of anastomotic leakage., In addition to surgical resection many patients will be treated with adjuvant chemotherapy., Next question
Page 1016 :
Question 107-109 of 147, Theme: Thyroid blood testing, , A., B., C., D., , Measurement of antibodies to TSH receptor, Thyroid peroxidase antibodies, Thyroglobulin antibodies, Serum calcitonin, , Please select the blood test most commonly performed for the diagnosis or assessment of the, thyroid disorder described. Each answer may be used once, more than once or not at all., , 107., , A 32 year old lady is diagnosed with Medullary carcinoma of the thyroid and has, undergone resection of the tumour., You answered Measurement of antibodies to TSH receptor, The correct answer is Serum calcitonin, Measurement of basal or stimulated calcitonin concentrations is used to assess the, completeness of surgical resection, and is of use in detecting diseases recurrences during, follow up., , 108., , A 20 year old lady has undergone a total thyroidectomy for a well differentiated papillary, carcinoma. She attends clinic and is well and the surgeon wishes to screen for disease, recurrence., You answered Measurement of antibodies to TSH receptor, The correct answer is Thyroglobulin antibodies, Antibodies to thyroglobulin, the major constituent of colloid and precursor of thyroid, hormones may be elevated in those with metastatic or recurrent thyroid cancer. Results, may be erronoeous in those with other thyroid disorders., , 109., , A 33 year old lady presents with a recently diagnosed goitre and a diagnosis of, Hashimotos thyroiditis is suspected., You answered Measurement of antibodies to TSH receptor, The correct answer is Thyroid peroxidase antibodies, Antibodies to thyroid peroxidase are found in most patients with Graves disease or
Page 1017 :
Hashimotos thyroiditis., Please rate this question:, , Discuss and give feedback, , Next question, , Blood testing in thyroid disease, Assay, , Usage, , Thyroid peroxidase, (microsomal) antibodies, , , , Found in autoimmune disease affecting the thyroid, (Hashimotos 100%) and Graves (70%), , Antibodies to TSH, receptor, , , , Individuals with Graves disease (95%), , Thyroglobulin antibodies, , , , Not useful for clinically distinguishing between different types, of thyroid disease, may be used as part of thyroid cancer, follow up, , Calcitonin, , , , , Released from the parafollicular cells, Usually found in patients with medullary carcinoma of the, thyroid, Next question
Page 1018 :
Question 110 of 147, Which one of the following complications is least associated with ventricular septal defects?, , Right heart failure, , Aortic regurgitation, , Eisenmenger's complex, , Infective endocarditis, , Atrial fibrillation, , Atrial fibrillation is associated more with atrial septal defects, Please rate this question:, , Discuss and give feedback, , Next question, , Ventricular septal defect, Ventricular septal defects are the most common cause of congenital heart disease. They close, spontaneously in around 50% of cases. Non-congenital causes include post myocardial infarction, Features, , , classically a pan-systolic murmur which is louder in smaller defects, , Complications, , , , , , aortic regurgitation*, infective endocarditis, Eisenmenger's complex, right heart failure, , *aortic regurgitation is due to a poorly supported right coronary cusp resulting in cusp prolapse
Page 1019 :
Question 111 of 147, A 24 year old man from Sub Saharan Africa presents with a lymphadenopathy and weight loss. A, diagnosis of tuberculosis is suspected and a lymph node biopsy is performed. Staining with which of, the agents below is most likely to facilitate identification of the causative organism?, , Gram stain, , Ziehl-Neelsen stain, , Von Kossa stain, , Van Gieson stain, , Masson Trichrome stain, , Ziehl-Neelsen stain is typically used to identify mycobacteria. They are not stained in the Gram, staining process. Van Gieson and Masson trichrome are histological staining methods for, identification of connective tissues. The Von Kossa technique is useful for identifying tissue, mineralisation., Please rate this question:, , Discuss and give feedback, , Next question, , Tuberculosis pathology, , , , , , , , Is a form of primary chronic inflammation, caused by the inability of macrophages to kill, theMycobacterium tuberculosis., The macrophages often migrate to regional lymph nodes, the lung lesion plus affected lymph, nodes is referred to as a Ghon complex., This leads to the formation of a granuloma which is a collection of epithelioid histiocytes., There is the presence of caseous necrosis in the centre., The inflammatory response is mediated by a type 4 hypersensitivity reaction., In healthy individuals the disease may be contained, in the immunocompromised, disseminated (miliary TB) may occur., , Diagnosis
Page 1020 :
, , , Waxy membrane of mycobacteria prevents binding with normal stains. Ziehl - Neelsen, staining is typically used., Culture based methods take far longer., , Image showing acid- alcohol fast mycobacteria stained using the Ziehl- Neelsen method, , Image sourced from Wikipedia, , Next question
Page 1021 :
Question 112 of 147, , Which of the following is not a pathological feature of breast cancer?, , Resemblance to ductal epithelial cells, , Angiogenesis, , Nuclear pleomorphism, , Metastatic calcification, , Vascular invasion, , Dystrophic calcification may be present in breast malignancy and is the basis for the breast, screening programme. Metastatic calcification is calcification which occurs in otherwise normal, tissues, usually as a result of hypercalcaemia. Invasive ductal carcinoma is the most common type, of breast cancer, unless the tumour is very poorly differentiated there is usually some resemblance, to ductal epithelial cells., Please rate this question:, , Discuss and give feedback, , Next question, , Breast cancer pathology, The histological features of breast cancer depend upon the underlying diagnosis. The invasive, component is usually comprised of ductal cells (unless it is an invasive lobular cancer). In situ, lesions may co-exist (such as DCIS)., Typical changes seen in conjunction with invasive breast cancer include:, 1. Nuclear pleomorphism
Page 1022 :
2. Coarse chromatin, 3. Angiogenesis, 4. Invasion of the basement membrane, 5. Dystrophic calcification (may be seen on mammography), 6. Abnormal mitoses, 7. Vascular invasion, 8. Lymph node metastasis, The primary tumour is graded on a scale of 1-3 where 1 is the most benign lesion and 3 the most, poorly differentiated., Immunohistochemistry for oestrogen receptor and herceptin status is routinely performed., The grade, lymph node stage and size are combined to provide the Nottingham prognostic index., Next question
Page 1023 :
Question 113-115 of 147, Theme: Renal lesions, , A., B., C., D., E., F., G., , Renal cell carcinoma, Renal transitional cell carcinoma, Nephroblastoma, Neuroblastoma, Angiomyolipoma, Renal squamous cell carcinoma, Retroperitoneal fibrosis, , For each scenario please select the most likely underlying diagnosis. Each option may be used, once, more than once or not at all., , 113., , A 69 year old male presents with haematuria. He worked in the textile industry. He has a, left flank mass. A CT IVU shows a lesion of the left renal pelvis., You answered Renal cell carcinoma, The correct answer is Renal transitional cell carcinoma, TCC is a rare form of renal cancer, accounting for approximately 7% of all renal, tumours. Risk factors include exposure to chemicals in the textile, plastic and rubber, industry., , 114., , A 2 year old boy presents with a right renal mass. On examination he has an irregular, mass arising from the right flank and is hypertensive. A CT scan shows a non calcified, irregular lesion affecting the apex of the right kidney and the right adrenal gland., You answered Renal cell carcinoma, The correct answer is Nephroblastoma, Wilm's tumour of the kidney is the most common renal tumour in children. Both, nephroblastoma and neuroblastoma may occupy the adrenal and apex of the kidney. In, the case of neuroblastoma the lesion will have arisen from the adrenal, in the case of, nephroblastoma the lesion will have arisen from the kidney. Hypertension is more, commonly associated with nephroblastoma. Neuroblastomas are usually calcified,, whereas nephroblastomas are not and this may be of diagnostic usefulness pre, operatively., , 115., , A 35 year old male presents with haematuria. He is found to have bilateral masses in the
Page 1024 :
flanks. He has a history of epilepsy and learning disability., You answered Renal cell carcinoma, The correct answer is Angiomyolipoma, This patient has tuberous sclerosis. This is associated with angiomyolipoma, which is, present in 60-80% patients. It is a benign lesion., Please rate this question:, , Discuss and give feedback, , Next question, , Renal lesions, Lesion, , Renal cell, carcinoma, , Disease specific features, , , , , , Nephroblastoma, , , , , , , , , Neuroblastoma, , , , , Treatment, , Most present with haematuria, (50%), Common renal tumour (85%, cases), Paraneoplastic features include, hypertension and polycythaemia, Most commonly has, haematogenous mestastasis, , Usually radical or partial, nephrectomy, , Rare childhood tumour, It accounts for 80% of all, genitourinary malignancies in, those under the age of 15 years, Up to 90% will have a mass, 50% will be hypertensive, Diagnostic work up includes, ultrasound and CT scanning, , Surgical resection combined, with chemotherapy (usually, vincristine, actinomycin D and, doxorubicin), , Most common extracranial, tumour of childhood, 80% occur in those under 4 years, of age, , Surgical resection, radiotherapy, and chemotherapy
Page 1025 :
Lesion, , Disease specific features, , , , , , , Transitional cell, carcinoma, , , , , , , , , , Angiomyolipoma, , , , , , , Treatment, , Tumour of neural crest origin (up, to 50% occur in the adrenal, gland), The tumour is usually calcified, and may be diagnosed using, MIBG scanning, Staging is with CT, Accounts for 90% of, lower urinary tract tumours, but, only 10% of renal tumours, Males affected 3x more than, females, Occupational exposure to, industrial dyes and rubber, chemicals may increase risk, Up to 80% present with painless, haematuria, Diagnosis and staging is with CT, IVU, , Radical nephroureterectomy, , 80% of these hamartoma type, lesions occur sporadically, the, remainder are seen in those with, tuberous sclerosis, Tumour is composed of blood, vessels, smooth muscle and fat, Massive bleeding may occur in, 10% of cases, , 50% of patients with lesions, >4cm will have symptoms and, will require surgical resection, , Next question
Page 1026 :
Question 116 of 147, , An 18 month old boy presents with recurrent urinary tract infections. As part of the diagnostic workup he is noted to have abnormal renal function. An ultrasound scan is performed and shows bilateral, hydronephrosis. What is the most likely underlying diagnosis?, , Urethral valves, , Meatal stenosis, , Hydronephrosis, , Pelvico-ureteric junction obstruction, , Benign prostatic hyperplasia, , Theme from April 2012 Exam, A posterior urethral valve is an obstructive, developmental uropathy that usually affects male infants, (incidence 1 in 8000). Diagnostic features include bladder wall hypertrophy, hydronephrosis and, bladder diverticula., Please rate this question:, , Discuss and give feedback, , Next question, , Urethral valves, Posterior urethral valves are the commonest cause of infravesical outflow obstruction in males. They, may be diagnosed on ante natal ultrasonography. Because the bladder has to develop high, emptying pressures in utero, the child may develop renal parenchymal damage. This translates to, renal impairment noted in 70% of boys at presentation. Treatment is with bladder catheterisation., Endoscopic valvotomy is the definitive treatment of choice with cystoscopic and renal follow up.
Page 1027 :
Question 117 of 147, At which of the following anatomical sites does dormant tuberculosis most frequently reactivate?, , Apex of the lung, , Base of the lung, , Brain, , Terminal ileum, , Lumbar spine, , TB reactivation most commonly occurs at the lung apex. This site is better oxygenated than, elsewhere allowing the mycobacteria to multiply more rapidly and then spread both locally and, distantly., Please rate this question:, , Discuss and give feedback, , Next question, , Tuberculosis pathology, , , , , , , , Is a form of primary chronic inflammation, caused by the inability of macrophages to kill, theMycobacterium tuberculosis., The macrophages often migrate to regional lymph nodes, the lung lesion plus affected lymph, nodes is referred to as a Ghon complex., This leads to the formation of a granuloma which is a collection of epithelioid histiocytes., There is the presence of caseous necrosis in the centre., The inflammatory response is mediated by a type 4 hypersensitivity reaction., In healthy individuals the disease may be contained, in the immunocompromised, disseminated (miliary TB) may occur., , Diagnosis, , , , Waxy membrane of mycobacteria prevents binding with normal stains. Ziehl - Neelsen, staining is typically used., Culture based methods take far longer.
Page 1028 :
Image showing acid- alcohol fast mycobacteria stained using the Ziehl- Neelsen method, , Image sourced from Wikipedia, , Next question
Page 1029 :
Question 118 of 147, What is the commonest tumour type encountered in the colon?, , Squamous cell carcinoma, , Adenocarcinoma, , Lymphoma, , Anaplastic carcinoma, , Sarcoma, , Adenocarcinoma are the most common and typically arise as a result of the adenoma - carcinoma, sequence., Please rate this question:, , Discuss and give feedback, , Next question, , Colorectal cancer, , , , , , , , , , Annually about 150,000 new cases are diagnosed and 50,000 deaths from the disease, About 75% will have sporadic disease and 25% will have a family history, Colorectal tumours comprise a spectrum of disease ranging from adenomas through to polyp, cancers and frank malignancy., Polyps may be categorised into: neoplastic polyps, adenomatous polyps and non neoplastic, polyps., The majority of adenomas are polypoidal lesions, although flat lesions do occur and may, prove to be dysplastic., Non-neoplastic polyps include hyperplastic, juvenile, hamartomatous, inflammatory, and, lymphoid polyps, which have not generally been thought of as precursors of cancer., Three characteristics of adenomas that correlate with malignant potential have been, characterised. These include increased size, villous architecture and dysplasia. For this, reason most polyps identified at colonoscopy should be removed., The transformation from polyp to cancer is described by the adenoma - carcinoma sequence, and its principles should be appreciated. Essentially genetic changes accompany the, transition from adenoma to carcinoma; key changes include APC, c-myc, K RAS mutations, and p53 deletions.
Page 1030 :
Question 119 of 147, Which of the following changes are most likely to be identified in the aortic wall of a 38 year old lady, with a Marfans syndrome and a dissecting aortic aneurysm?, , Transmural aortitis, , Cystic medial necrosis, , Foamy macrophages, , Dense dystrophic calcification, , None of the above, , Cystic medial necrosis ( or cystic medial degeneration) occurs when basophils and mucoid material, lie in between the intimal elastic fibres of the aorta. It is typically found in the aortic degeneration of, Marfans syndrome, but may also be seen in aortic degeneration in older adults., Please rate this question:, , Discuss and give feedback, , Next question, , Aortic dissection, , , , , , , More common than rupture of the abdominal aorta, 33% of patients die within the first 24 hours, and 50% die within 48 hours if no treatment, received, Associated with hypertension, Features of aortic dissection: tear in the intimal layer, followed by formation and propagation, of a subintimal hematoma. Cystic medial necrosis (Marfan's), Most common site of dissection: 90% occurring within 10 centimetres of the aortic valve, , Stanford Classification, , Type, , Location, , Treatment
Page 1031 :
Type, , Location, , Treatment, , A, , Ascending aorta/ aortic root, , Surgery- aortic root replacement, , B, , Descending aorta, , Medical therapy with antihypertensives, , DeBakey classification, , Type, , Site affected, , I, , Ascending aorta, aortic arch, descending aorta, , II, , Ascending aorta only, , III, , Descending aorta distal to left subclavian artery, , Clinical features, , , , , , Tearing, sudden onset chest pain (painless 10%), Hypertension or Hypotension, A blood pressure difference (in each arm) greater than 20 mm Hg, Neurologic deficits (20%), , Investigations, , , , , , CXR: widened mediastinum, abnormal aortic knob, ring sign, deviation of the, trachea/oesophagus, CT angiography of the thoracic aorta, MRI angiography, Conventional angiography (now rarely used diagnostically), , Management, , , , Beta-blockers: aim HR 60-80 bpm and systolic BP 100-120 mm Hg, For type A dissections the standard of care is aortic root replacement
Page 1032 :
Question 120 of 147, A 58 year old man undergoes an upper GI endoscopy for the investigation of odynophagia. At, endoscopy a reddish area is seen to protrude up into the oesophagus from the gastro-oesophageal, junction. Which of the following pathological events is most likely to explain this process?, , Metaplasia, , Anaplasia, , Dysplasia, , Hypoplasia, , Hyperplasia, , This is most likely to represent Barretts oesphagus and is thus metaplasia. Dysplasia is less likely in, this setting although biopsies are mandatory., Please rate this question:, , Discuss and give feedback, , Next question, , Barrett's oesophagus, Barretts oesophagus is a condition characterised by the metaplastic transformation of squamous, oesophageal epithelium to columnar gastric type epithelium. Three types of this metaplastic process, are recognised; intestinal (high risk), cardiac and fundic. The latter two categories may cause, difficulties in diagnosis. The most concrete diagnosis can be made when endoscopic features of, Barretts oesophagus are present together with a deep biopsy that demonstrates not just goblet cell, metaplasia but also oesophageal glands., Barrett's can be sub divided into short (<3cm) and long (>3cm). The length of the affected segment, correlates strongly with the chances of identifying metaplasia. The overall prevalence of Barrett's, oesophagus is difficult to determine but may be in the region of 1 in 20 and is identified in up to 12%, of those undergoing endoscopy for reflux., A proportion of patients with metaplasia will progress to dysplasia and for this reason individuals, identified as having Barrett's should undergo endoscopic surveillance (every 2-5 years). Biopsies, should be quadrantic and taken at 1-2cm intervals. Biopsies need to be adequate. Where mass, lesions are present consideration should be given to endoscopic sub mucosal resection. Up to 40%
Page 1033 :
of patients will be upstaged from high grade dysplasia to invasive malignancy with such techniques., Treatment, , , , , , Long term proton pump inhibitor, Consider pH and manometry studies in younger patients who may prefer to consider an anti, reflux procedure, Regular endoscopic monitoring (more frequently if moderate dysplasia). With quadrantic, biopsies every 2-3 cm, If severe dysplasia be very wary of small foci of cancer, , References, A consensus statement of the British approach is provided by:, Bennett C et al Consensus Statements for Management of Barrett's Dysplasia and Early-Stage, Esophageal Adenocarcinoma, Based on a Delphi Process. Gastroenterology Volume 143, Issue 2 ,, Pages 336-346, August 2012., Next question
Page 1034 :
Question 121 of 147, A male infant is born by emergency cesarean section at 39 weeks gestation for foetal distress. Soon, after the birth the baby becomes progressively hypoxic and on examination is found to have a, scaphoid abdomen. What is the most likely underlying diagnosis?, , Intestinal malrotation, , Hiatus hernia, , Foramen of Bochdalek hernia, , Foramen of Morgagni hernia, , Tracheo-oesphageal fistula, , The finding of a scaphoid abdomen and respiratory distress suggests extensive intra thoracic, herniation of the abdominal contents. This is seen most frequently with Bochdalek hernias. Morgagni, hernias seldom present in such a dramatic fashion. The other options do not typically present with, the symptoms and signs described., Please rate this question:, , Discuss and give feedback, , Next question, , Embryology of the diaphragm and diaphragmatic hernia, Embryology, The diaphragm is formed between the 5th and 7th weeks of gestation through the progressive fusion, of the septum transversum, pleuroperitoneal folds and via lateral muscular ingrowth. The muscular, origins of the diaphragm are somites located in cervical segments 3 to 5, which accounts for the long, path taken by the phrenic nerve. The components contribute to the following diaphragmatic, segments:, , , , , Septum transversum - Central tendon, Pleuroperitoneal membranes - Parietal membranes surrounding viscera, Cervical somites C5 to C7 - Muscular component of the diaphragm, , Diaphragmatic hernia
Page 1035 :
Type of hernia, , Features, , Morgagni, , Anteriorly located, Minimal compromise on lung development, Minimal signs on antenatal ultrasound, Usually present later, Usually good prognosis, , Bochdalek hernia, , Posteriorly located, Larger defect, Often diagnosed antenatally, Associated with pulmonary hypoplasia, Poor prognosis, , The posterior hernias of Bochdalek are the most common type and if not diagnosed antenatally will, typically present soon after birth with respiratory distress. The classical finding is that of a scaphoid, abdomen on clinical examination because of herniation of the abdominal contents into the chest., Bochdalek hernias are associated with a number of chromosomal abnormalities such as Trisomy 21, and 18. Infants have considerable respiratory distress due to hypoplasia of the developing lung., Historically this was considered to be due to direct compression of the lung by herniated viscera., This view over simplifies the situation and the pulmonary hypoplasia occurs concomitantly with the, hernial development, rather than as a direct result of it. The pulmonary hypoplasia is associated with, pulmonary hypertension and abnormalities of pulmonary vasculature. The pulmonary hypertension, renders infants at risk of right to left shunting (resulting in progressive and worsening hypoxia)., Diagnostic work up of these infants includes chest x-rays/ abdominal ultrasound scans and cardiac, echo., Surgery forms the mainstay of treatment and both thoracic and abdominal approaches may be, utilised. Following reduction of the hernial contents a careful search needs to be made for a hernial, sac as failure to recognise and correct this will result in a high recurrence rate. Smaller defects may, be primarily closed, larger defects may require a patch to close the defect. Malrotation of the viscera, is a recognised association and may require surgical correct at the same procedure (favoring an, abdominal approach)., The mortality rate is 50-75% and is related to the degree of lung compromise and age at, presentation (considerably better in infants >24 hours old)., Next question
Page 1036 :
Question 122 of 147, A 72 year old lady falls and lands on her left hip. She attends the emergency department and is, given some paracetamol by the junior doctor and discharged. Several months later she presents, with ongoing pain and discomfort of the hip. Avascular necrosis of the femoral head is suspected., Which of the following features is least likely to be present?, , Non union of the fracture, , Angiogenesis at the fracture site, , Increased numbers of fibroblasts at the fracture site, , Osteochondritis dissecans, , Apoptosis of osteoblasts, , Apoptosis is not a feature of necrotic cell death. By this stage there would usually be attempted, repair so angiogenesis and proliferation of fibroblasts would be expected. These cells may, differentiate further to become osteoblasts which in turn will lay down new matrix., Please rate this question:, , Discuss and give feedback, , Next question, , Avascular necrosis, , , , , , , Cellular death of bone components due to interruption of the blood supply, causing bone, destruction, Main joints affected are hip, scaphoid, lunate and the talus., It is not the same as non union. The fracture has usually united., Radiological evidence is slow to appear., Vascular ingrowth into the affected bone may occur. However, many joints will develop, secondary osteoarthritis., , Causes, P ancreatitis, L upus, A lcohol, S teroids
Page 1037 :
T rauma, I diopathic, infection, C aisson disease, collagen vascular disease, R adiation, rheumatoid arthritis, A myloid, G aucher disease, S ickle cell disease, Presentation, Usually pain. Often despite apparent fracture union., Investigation, MRI scanning will show changes earlier than plain films., Treatment, In fractures at high risk sites anticipation is key. Early prompt and accurate reduction is essential., Non weight bearing may help to facilitate vascular regeneration., Joint replacement may be necessary, or even the preferred option (e.g. Hip in the elderly)., Next question
Page 1038 :
Question 123 of 147, Which one of the following is least associated with the development of colorectal cancer in patients, with ulcerative colitis?, , Unremitting disease, , Disease duration > 10 years, , Onset before 15 years old, , Poor compliance to treatment, , Disease confined to the rectum, , Please rate this question:, , Discuss and give feedback, , Next question, , Ulcerative colitis and colorectal cancer, Overview, , , , , , risk of colorectal cancer is 10-20 times that of general population, the increased risk is mainly related to chronic inflammation, worse prognosis than patients without ulcerative colitis (partly due to delayed diagnosis), lesions may be multifocal, , Factors increasing risk of cancer, , , , , , , disease duration > 10 years, patients with pancolitis, onset before 15 years old, unremitting disease, poor compliance to treatment, Next question
Page 1039 :
Question 124-126 of 147, Theme: Causes of chest pain, , A., B., C., D., E., F., G., H., , Pulmonary embolism, Anterior myocardial infarction, Inferior myocardial infarction, Proximal aortic dissection, Distal aortic dissection, Boerhaave Syndrome, Mallory weiss tear, Perforated gastric ulcer, , Please select the most likely cause of chest pain for the scenario given. Each option may be used, once, more than once or not at all., , 124., , A 52 year old male presents with tearing central chest pain. On examination, he has an, aortic regurgitation murmur. An ECG shows ST elevation in leads II, III and aVF., You answered Pulmonary embolism, The correct answer is Proximal aortic dissection, Theme from 2011 Exam, An inferior myocardial infarction and AR murmur should raise suspicions of an, ascending aorta dissection rather than an inferior myocardial infarction alone. Also the, history is more suggestive of a dissection. Other features may include pericardial, effusion, carotid dissection and absent subclavian pulse., , 125., , A 52 year old male presents with central chest pain and vomiting. He has drunk a bottle, of vodka. On examination, there is some mild crepitus in the epigastric region., You answered Pulmonary embolism, The correct answer is Boerhaave Syndrome, The Mackler triad for Boerhaave syndrome: vomiting, thoracic pain, subcutaneous, emphysema. It commonly presents in middle aged men with a background of alcohol, abuse., , 126., , A 52 year old male presents with central chest pain. On examination, he has an mitral, regurgitation murmur. An ECG shows ST elevation in leads V1 to V6. There is no ST, elevation in leads II, III and aVF.
Page 1040 :
You answered Pulmonary embolism, The correct answer is Anterior myocardial infarction, The most likely diagnosis is an anterior MI. As there are no ST changes in the inferior, leads, aortic dissection is less likely., Please rate this question:, , Discuss and give feedback, , Next question, , Chest pain, Aortic dissection, , , , , , , , , This occurs when there is a flap or filling defect within the aortic intima. Blood tracks into the, medial layer and splits the tissues with the subsequent creation of a false lumen. It most, commonly occurs in the ascending aorta or just distal to the left subclavian artery (less, common). It is most common in Afro-carribean males aged 50-70 years., Patients usually present with a tearing intrascapular pain, which may be similar to the pain of, a myocardial infarct., The dissection may spread either proximally or distally with subsequent disruption to the, arterial branches that are encountered., In the Stanford classification system the disease is classified into lesions with a proximal, origin (Type A) and those that commence distal to the left subclavian (Type B)., Diagnosis may be suggested by a chest x-ray showing a widened mediastinum. Confirmation, of the diagnosis is usually made by use of CT angiography, Proximal (Type A) lesions are usually treated surgically, type B lesions are usually managed, non operatively., , Pulmonary embolism, , , , , , Typically sudden onset of chest pain, haemoptysis, hypoxia and small pleural effusions may, be present., Most patients will have an underlying deep vein thrombosis, Diagnosis may be suggested by various ECG findings including S waves in lead I, Q waves, in lead III and inverted T waves in lead III. Confirmation of the diagnosis is usually made, through use of CT pulmonary angiography., Treatment is with anticoagulation, in those patients who develop a cardiac arrest or severe, compromise from their PE, consideration may be given to thrombolysis.
Page 1041 :
Myocardial infarction, , , , , , Traditionally described as sudden onset of central, crushing chest pain. It may radiate into, the neck and down the left arm. Signs of autonomic dysfunction may be present. The, presenting features may be atypical in the elderly and those with diabetes., Diagnosis is made through identification of new and usually dynamic ECG changes (and, cardiac enzyme changes). Inferior and anterior infarcts may be distinguished by the, presence of specific ECG changes (usually II, III and aVF for inferior, leads V1-V5 for, anterior)., Treatment is with oral antiplatelet agents, primary coronary angioplasty and/ or thrombolysis., , Perforated peptic ulcer, , , , , , Patients usually develop sudden onset of epigastric abdominal pain, it may be soon followed, by generalised abdominal pain., There may be features of antecendant abdominal discomfort, the pain of gastric ulcer is, typically worse immediately after eating., Diagnosis may be made by erect chest x-ray which may show a small amount of free intraabdominal air (very large amounts of air are more typically associated with colonic, perforation)., Treatment is usually with a laparotomy, small defects may be excised and overlaid with an, omental patch, larger defects are best managed with a partial gastrectomy., , Boerhaaves syndrome, , , , , , , , , Spontaneous rupture of the oesophagus that occurs as a result of repeated episodes of, vomiting., The rupture is usually distally sited and on the left side., Patients usually give a history of sudden onset of severe chest pain that may complicate, severe vomiting., Severe sepsis occurs secondary to mediastinitis., Diagnosis is CT contrast swallow., Treatment is with thoracotomy and lavage, if less than 12 hours after onset then primary, repair is usually feasible, surgery delayed beyond 12 hours is best managed by insertion of a, T tube to create a controlled fistula between oesophagus and skin., Delays beyond 24 hours are associated with a very high mortality rate., Next question
Page 1042 :
Question 127 of 147, A 78 year old lady presents with a tender swelling in her right groin. On examination there is a tender, swelling that lies below and lateral to the pubic tubercle. It has a cough impulse. What is the most, likely underlying diagnosis?, , Thrombophlebitis of the great saphenous vein, , Femoral hernia, , Thrombophlebitis of saphena varix, , Inguinal hernia, , Obturator hernia, , Theme from April 2012 Exam, Whilst a thrombophlebitis of a saphena varix may cause a tender swelling at this site, it would not, usually be associated with a cough impulse., Please rate this question:, , Discuss and give feedback, , Next question, , Femoral canal, The femoral canal lies at the medial aspect of the femoral sheath. The femoral sheath is a fascial, tunnel containing both the femoral artery laterally and femoral vein medially. The canal lies medial to, the vein., Borders of the femoral canal, , Laterally, , Femoral vein, , Medially, , Lacunar ligament, , Anteriorly, , Inguinal ligament
Page 1043 :
Pectineal ligament, , Posteriorly, , Image showing dissection of femoral canal, , Image sourced from Wikipedia, , Contents, , , , Lymphatic vessels, Cloquet's lymph node, , Physiological significance, Allows the femoral vein to expand to allow for increased venous return to the lower limbs., Pathological significance, As a potential space, it is the site of femoral hernias. The relatively tight neck places these at high, risk of strangulation.
Page 1044 :
Question 128 of 147, A 3 month old boy is suspected of having hypospadias. At which of the following locations is the, urethral opening most frequently located in boys suffering from the condition?, , On the distal ventral surface of the penis, , On the proximal ventral surface of the penis, , On the distal dorsal surface of the penis, , On the proximal dorsal surface of the penis, , At the base of the scrotum, , The defect is located ventrally and most often distally. Proximally located urethral openings are well, recognised. Circumcision may compromise reconstruction., Please rate this question:, , Discuss and give feedback, , Next question, , Hypospadias, The urethral meatus opens on the ventral surface of the penis. There is also a ventral deficiency of, the foreskin. The urethral meatus may open more proximally in the more severe variants. However,, 75% of the openings are distally located. The incidence is 1 in 300 male births., Features include:, , , , , , , , Absent frenular artery, Ventrally opened glans, Skin tethering to hypoplastic urethra, Splayed columns of spongiosum tissue distal to the meatus, Deficiency of the foreskin ventrally, , Management:
Page 1045 :
, , , , No routine cultural circumcisions, Urethroplasty, Penile reconstruction, , The foreskin is often utilised in the reconstructive process. In boys with very distal disease no, treatment may be needed., Next question
Page 1046 :
Question 129 of 147, A 52 year old male attends for a preoperative assessment for an inguinal hernia repair. You notice, that the chest x-ray shows a loculated left pleural effusion. On further questioning the patient reports, that he worked as a builder 30 years ago. What is the most likely cause for the effusion?, , Asbestosis, , Pneumonia, , Mesothelioma, , Silicosis, , Left ventricular failure, , This patient has a risk of asbestos exposure through his occupation as a builder. As there a is latent, period of 30 years and a complicated effusion, the most likely cause is mesothelioma., Please rate this question:, , Discuss and give feedback, , Next question, , Mesothelioma, Features, , , , , , , Dyspnoea, weight loss, chest wall pain, Clubbing, 30% present as painless pleural effusion, Only 20% have pre-existing asbestosis, History of asbestos exposure in 85-90%, latent period of 30-40 years, , Basics, , , , , Malignancy of mesothelial cells of pleura, Metastases to contralateral lung and peritoneum, Right lung affected more often than left
Page 1047 :
Management, , , , , , , Investigation: pleural biopsy, CT Scanning, (PET Scanning if surgery considered), Symptomatic, Industrial compensation, Chemotherapy, Surgery if operable, Prognosis poor, median survival 12 months, Next question
Page 1048 :
Question 130 of 147, A 64-year-old woman is reviewed due to multiple non-healing leg ulcers. She reports feeling, generally unwell for many months. Examination findings include a blood pressure of 138/72 mmHg,, pulse 90 bpm, pale conjunctivae and poor dentition associated with bleeding gums. What is the most, likely underlying diagnosis?, , Thyrotoxicosis, , Vitamin B12 deficiency, , Vitamin C deficiency, , Diabetes mellitus, , Sarcoidosis, , Bleeding gums and poor healing are suggestive of vitamin C deficiency., Please rate this question:, , Discuss and give feedback, , Next question, , Vitamin C deficiency, Vitamin C deficiency (scurvy) leads to defective synthesis of collagen resulting in capillary fragility, (bleeding tendency) and poor wound healing, Features, , , , , , gingivitis, loose teeth, poor wound healing, bleeding from gums, haematuria, epistaxis, general malaise, Next question
Page 1049 :
Question 131 of 147, Which of the following is not a typical feature of neuropraxia?, , Transient delay in neuronal transmission, , Axonal degeneration distal to the site of injury, , Absence of neuroma formation, , Preservation of autonomic function, , Absence of axonal degeneration proximal to the site of injury, , Full recovery may occur 6-8 weeks after nerve injury in neuropraxia., Wallerian degeneration does not usually occur in simple neuropraxia., Autonomic function is usually preserved., Please rate this question:, , Discuss and give feedback, , Next question, , Nerve injury, There are 3 types of nerve injury:, , Neuropraxia, , , , , , , Nerve intact but electrical conduction is affected, Full recovery, Autonomic function preserved, Wallerian degeneration does not occur, , Axonotmesis, , , , , Axon is damaged and the myelin sheath is preserved. The connective tissue, framework is not affected., Wallerian degeneration occurs., , , , Disruption of the axon, myelin sheath and surrounding connective tissue., , Neurotmesis
Page 1050 :
, , Wallerian degeneration occurs., , Wallerian Degeneration, , , , , , Axonal degeneration distal to the site of injury., Typically begins 24-36 hours following injury., Axons are excitable prior to degeneration occurring., Myelin sheath degenerates and is phagocytosed by tissue macrophages., , Nerve repair, , , Neuronal repair may only occur physiologically where nerves are in direct contact. Where a, large defect is present, the process of nerve regeneration is hampered. It may not occur at, all or result in the formation of a neuroma. Where nerve regrowth occurs it is typically at a, rate of 1mm per day., Next question
Page 1051 :
Question 132 of 147, A 44 year old lady presents with a pathological fracture of the left femur. She has previously, undergone a renal transplant for end stage renal failure. Her blood test results are as follows:, , Serum Ca2+, , 2.80, , PTH, , 88pg/ml, , Phosphate, , 0.30, , A surgeon decides to perform a parathyroidectomy on the basis of these results. When the glands, are assessed histologically, which of the appearances is most likely to be identified?, , Metaplasia the gland, , Hypertrophy of the gland, , Hyperplasia of the gland, , Parathyroid carcinoma, , Necrosis of the parathyroid gland, , This is likely to be a case of tertiary hyperparathyroidism (high Calcium, high PTH, low phosphate)., Therefore the glands will be hyperplastic. Hypertrophy is not correct as this implies an increase in, size without an increase in cellularity. This mistake has cost many candidates marks in the MRCS, exams over the years!, Please rate this question:, , Discuss and give feedback, , Next question, , Parathyroid glands and disorders of calcium metabolism, Hyperparathyroidism
Page 1052 :
Disease type, , Hormone profile, , Clinical features, , Cause, , Primary, hyperparathyroidism, , , , , , , PTH (Elevated), Ca2+(Elevated), Phosphate (Low), Urine calcium :, creatinine clearance, ratio > 0.01, , May be, asymptomatic if, mild, Recurrent, abdominal pain, (pancreatitis, renal, colic), Changes to, emotional or, cognitive state, , Most cases due to, solitary adenoma, (80%), multifocal, disease occurs in 1015% and parathyroid, carcinoma in 1% or, less, , Secondary, hyperparathyroidism, , , , , PTH (Elevated), Ca2+ (Low or, normal), Phosphate, (Elevated), Vitamin D levels, (Low), , May have few, symptoms, Eventually may, develop bone, disease, osteitis, fibrosa cystica and, soft tissue, calcifications, , Parathyroid gland, hyperplasia occurs as, a result of low, calcium, almost, always in a setting of, chronic renal failure, , Ca2+(Normal or, high), PTH (Elevated), Phosphate levels, (Decreased or, Normal), Vitamin D (Normal, or decreased), Alkaline, phosphatase, (Elevated), , Metastatic, calcification, Bone pain and /, or fracture, Nephrolithiasis, Pancreatitis, , Occurs as a result of, ongoing hyperplasia, of the parathyroid, glands after, correction of, underlying renal, disorder, hyperplasia, of all 4 glands is, usually the cause, , , , , Tertiary, hyperparathyroidism, , , , , , , , , Differential diagnoses, It is important to consider the rare but relatively benign condition of benign familial hypocalciuric, hypercalcaemia, caused by an autosomal dominant genetic disorder. Diagnosis is usually made by, genetic testing and concordant biochemistry (urine calcium : creatinine clearance ratio <0.01distinguished from primary hyperparathyroidism)., Treatment, Primary hyperparathyroidism, Indications for surgery
Page 1053 :
, , , , , , , , , Elevated serum Calcium > 1mg/dL above normal, Hypercalciuria > 400mg/day, Creatinine clearance < 30% compared with normal, Episode of life threatening hypercalcaemia, Nephrolithiasis, Age < 50 years, Neuromuscular symptoms, Reduction in bone mineral density of the femoral neck, lumbar spine, or distal radius of more, than 2.5 standard deviations below peak bone mass (T score lower than -2.5), , Secondary hyperparathyroidism, Usually managed with medical therapy., Indications for surgery in secondary (renal) hyperparathyroidism:, , , , , Bone pain, Persistent pruritus, Soft tissue calcifications, , Tertiary hyperparathyroidism, Allow 12 months to elapse following transplant as many cases will resolve, The presence of an autonomously functioning parathyroid gland may require surgery. If the culprit, gland can be identified then it should be excised. Otherwise total parathyroidectomy and reimplantation of part of the gland may be required., References, 1. Pitt S et al. Secondary and Tertiary Hyperparathyroidism, State of the Art Surgical, Management.Surg Clin North Am 2009 Oct;89(5):1227-39., 2. MacKenzie-Feder J et al. Primary Hyperparathyroidism: An Overview. Int J Endocrinol 2011;, 2011: 251410., Next question
Page 1054 :
Question 133 of 147, A 78 year old man is referred to the clinic by his general practitioner. For many years he noticed a, smooth swelling approximately 5cm anterior to the tragus of his right ear. Apart from being a heavy, smoker he has no co-morbidities. What is the most likely diagnosis?, , Pleomorphic adenoma, , Liposarcoma, , Warthins tumour, , Adenocarcinoma, , None of the above, , Warthins tumours are most common in elderly smokers. They have a relatively benign and indolent, course. They are usually well circumscribed as illustrated below:
Page 1055 :
Image sourced from Wikipedia, , Please rate this question:, , Discuss and give feedback, , Next question, , Parotid gland clinical, Benign neoplasms, Up to 80% of all salivary gland tumours occur in the parotid gland and up to 80% of these are, benign. There is no consistent correlation between the rate of growth and the malignant potential of, the lesion. However, benign tumours should not invade structures such as the facial nerve., With the exception of Warthins tumours, they are commoner in women than men. The median age of, developing a lesion is in the 5th decade of life., Benign tumour types, , Tumour type, , Features, , Benign pleomorphic adenoma or, benign mixed tumor, , Most common parotid neoplasm (80%), Proliferation of epithelial and myoepithelial cells of the ducts, and an increase in stromal components, Slow growing, lobular, and not well encapsulated, Recurrence rate of 1-5% with appropriate excision, (parotidectomy), Recurrence possibly secondary to capsular disruption during, surgery, Malignant degeneration occurring in 2-10% of adenomas, observed for long periods, with carcinoma ex-pleomorphic, adenoma occurring most frequently as adenocarcinoma, , Warthin tumor (papillary, cystadenoma lymphoma or, adenolymphoma), , Second most common benign parotid tumor (5%), Most common bilateral benign neoplasm of the parotid, Marked male as compared to female predominance, Occurs later in life (sixth and seventh decades), Presents as a lymphocytic infiltrate and cystic epithelial, proliferation, May represent heterotopic salivary gland epithelial tissue, trapped within intraparotid lymph nodes, Incidence of bilaterality and multicentricity of 10%, Malignant transformation rare (almost unheard of)
Page 1056 :
Tumour type, , Features, , Monomorphic adenoma, , Account for less than 5% of tumours, Slow growing, Consist of only one morphological cell type (hence term, mono), Include; basal cell adenoma, canalicular adenoma,, oncocytoma, myoepitheliomas, , Haemangioma, , Should be considered in the differential of a parotid mass in a, child, Accounts for 90% of parotid tumours in children less than 1, year of age, Hypervascular on imaging, Spontaneous regression may occur and malignant, transformation is almost unheard of, , Malignant salivary gland tumours, Types of malignancy, , Mucoepidermoid, carcinoma, , 30% of all parotid malignancies, Usually low potential for local invasiveness and metastasis (depends, mainly on grade), , Adenoid cystic, carcinoma, , Unpredictable growth pattern, Tendency for perineural spread, Nerve growth may display skip lesions resulting in incomplete excision, Distant metastasis more common (visceral rather than nodal spread), 5 year survival 35%, , Mixed tumours, , Often a malignancy occurring in a previously benign parotid lesion, , Acinic cell carcinoma, , Intermediate grade malignancy, May show perineural invasion, Low potential for distant metastasis, 5 year survival 80%
Page 1057 :
Adenocarcinoma, , Develops from secretory portion of gland, Risk of regional nodal and distant metastasis, 5 year survival depends upon stage at presentation, may be up to 75%, with small lesions with no nodal involvement, , Lymphoma, , Large rubbery lesion, may occur in association with Warthins tumours, Diagnosis should be based on regional nodal biopsy rather than parotid, resection, Treatment is with chemotherapy (and radiotherapy), , Diagnostic evaluation, , , , , , , , Plain x-rays may be used to exclude calculi, Sialography may be used to delineate ductal anatomy, FNAC is used in most cases, Superficial parotidectomy may be either diagnostic of therapeutic depending upon the nature, of the lesion, Where malignancy is suspected the primary approach should be definitive resection rather, than excisional biopsy, CT/ MRI may be used in cases of malignancy for staging primary disease, , Treatment, For nearly all lesions this consists of surgical resection, for benign disease this will usually consist of, a superficial parotidectomy. For malignant disease a radical or extended radical parotidectomy is, performed. The facial nerve is included in the resection if involved. The need for neck dissection is, determined by the potential for nodal involvement., Other parotid disorders, HIV infection, , , , , Lymphoepithelial cysts associated with HIV occur almost exclusively in the parotid, Typically presents as bilateral, multicystic, symmetrical swelling, Risk of malignant transformation is low and management usually conservative, , Sjogren syndrome, , , , , , Autoimmune disorder characterised by parotid enlargement, xerostomia and, keratoconjunctivitis sicca, 90% of cases occur in females, Second most common connective tissue disorder, Bilateral, non tender enlargement of the gland is usual
Page 1058 :
, , , , Histologically, the usual findings are of a lymphocytic infiltrate in acinar units and, epimyoepithelial islands surrounded by lymphoid stroma, Treatment is supportive, There is an increased risk of subsequent lymphoma, , Sarcoid, , , , , , , Parotid involvement occurs in 6% of patients with sarcoid, Bilateral in most cases, Gland is not tender, Xerostomia may occur, Management of isolated parotid disease is usually conservative, Next question
Page 1059 :
Question 134 of 147, , A 56 year old man presents with lethargy, haematuria and haemoptysis. On examination he is, hypertensive and has a right loin mass. A CT scan shows a lesion affecting the upper pole of the, right kidney, it has a small cystic centre. Which of the options below is the most likely diagnosis?, , Squamous cell carcinoma of the kidney, , Nephroblastoma, , Renal adenocarcinoma, , Transitional cell carcinoma of the kidney, , Polycystic kidney disease, , Renal adenocarcinoma are the most common renal tumours. These will typically affect the renal, parenchyma. Transitional cell carcinoma will usually affect urothelial surfaces. Nephroblastoma, would be very rare in this age group. Renal adenocarcinoma may produce cannon ball metastasis in, the lung which cause haemoptysis, this is not a feature of PKD., Please rate this question:, , Discuss and give feedback, , Next question, , Renal tumours, Renal cell carcinoma, Renal cell carcinoma is an adenocarcinoma of the renal cortex and is believed to arise from the, proximal convoluted tubule. They are usually solid lesions, up to 20% may be multifocal, 20% may, be calcified and 20% may have either a cystic component or be wholly cystic. They are often, circumscribed by a pseudocapsule of compressed normal renal tissue. Spread may occur either by
Page 1060 :
direct extension into the adrenal gland, renal vein or surrounding fascia. More distant disease, usually occurs via the haematogenous route to lung, bone or brain., Renal cell carcinoma comprise up to 85% of all renal malignancies. Males are more commonly, affected than females and sporadic tumours typically affect patients in their sixth decade., Patients may present with a variety of symptoms including; haematuria (50%), loin pain (40%), mass, (30%) and up to 25% may have symptoms of metastasis.Less than 10% have the classic triad of, haematuria, pain and mass., Investigation, Many cases will present as haematuria and be discovered during diagnostic work up. Benign renal, tumours are rare, so renal masses should be investigated with multislice CT scanning. Some units, will add and arterial and venous phase to the scan to demonstrate vascularity and evidence of caval, ingrowth., CT scanning of the chest and abdomen to detect distant disease should also be undertaken., Routine bone scanning is not indicated in the absence of symptoms., Biopsy should not be performed when a nephrectomy is planned but is mandatory before any, ablative therapies are undertaken., Assessment of the functioning of the contra lateral kidney., Management, T1 lesions may be managed by partial nephrectomy and this gives equivalent oncological results to, total radical nephrectomy. Partial nephrectomy may also be performed when there is inadequate, reserve in the remaining kidney., For T2 lesions and above a radical nephrectomy is standard practice and this may be performed via, a laparoscopic or open approach. Preoperative embolisation is not indicated nor is resection of, uninvolved adrenal glands. During surgery early venous control is mandatory to avoid shedding of, tumour cells into the circulation., Patients with completely resected disease do not benefit from adjuvant therapy with either, chemotherapy or biological agents. These should not be administered outside the setting of clinical, trials., Patients with transitional cell cancer will require a nephroureterectomy with disconnection of the, ureter at the bladder., References, Lungberg B et al. EAU guidelines on renal cell carcinoma: The 2010 update. European Urology 2010, (58): 398-406., Next question, Question 135 of 147
Page 1061 :
A 34-year-old man is taken immediately to theatre with aortic dissection. You note he is tall with, pectus excavatum and arachnodactyly. His condition is primarily due to a defect in which one of the, following proteins?, , Polycystin-1, , Fibrillin, , Type IV collagen, , Type I collagen, , Elastin, , Although fibrillin is the primary protein affected (due to a defect in the fibrillin-1 gene) it should be, noted that fibrillin is used as a substrate of elastin., Please rate this question:, , Discuss and give feedback, , Next question, , Marfan's syndrome, Marfan's syndrome is an autosomal dominant connective tissue disorder. It is caused by a defect in, the fibrillin-1 gene on chromosome 15 and affects around 1 in 3,000 people., Features, , , , , , , , , , , , tall stature with arm span to height ratio > 1.05, high-arched palate, arachnodactyly, pectus excavatum, pes planus, scoliosis of > 20 degrees, heart: dilation of the aortic sinuses (seen in 90%) which may lead to aortic aneurysm, aortic, dissection, aortic regurgitation, mitral valve prolapse (75%),, lungs: repeated pneumothoraces, eyes: upwards lens dislocation (superotemporal ectopia lentis), blue sclera, myopia, dural ectasia (ballooning of the dural sac at the lumbosacral level)
Page 1062 :
The life expectancy of patients used to be around 40-50 years. With the advent of regular, echocardiography monitoring and beta-blocker/ACE-inhibitor therapy this has improved significantly, over recent years. Aortic dissection and other cardiovascular problems remain the leading cause of, death however., Next question
Page 1063 :
Question 136 of 147, Which of the following are not typical of Lynch syndrome?, , It is inherited in an autosomal recessive manner, , Affected patients are more likely to develop right colon mucinous tumours than the, general population, Affected individuals have an 80% lifetime risk of colon cancer, , Endometrial cancer is seen in 80% of women, , Gastric cancers are more common, , Lynch syndrome is inherited in an autosomal dominant fashion. It is characterised by microsatellite, instability in the DNA mismatch repair genes. Colonic tumours in patients with Lynch syndrome are, more likely to be right sided tumours and to be poorly differentiated., Please rate this question:, , Discuss and give feedback, , Next question, , Genetics and surgical disease, Some of the more commonly occurring genetic conditions occurring in surgical patients are, presented here., Li-Fraumeni Syndrome, , , , , , Autosomal dominant, Consists of germline mutations to p53 tumour suppressor gene, High incidence of malignancies particularly sarcomas and leukaemias, Diagnosed when:, , *Individual develops sarcoma under 45 years, *First degree relative diagnosed with any cancer below age 45 years and another family member, develops malignancy under 45 years or sarcoma at any age
Page 1064 :
BRCA 1 and 2, , , , , Carried on chromosome 17 (BRCA 1) and Chromosome 13 (BRCA 2), Linked to developing breast cancer (60%) risk., Associated risk of developing ovarian cancer (55% with BRCA 1 and 25% with BRCA 2)., , Lynch Syndrome, , , , , , Autosomal dominant, Develop colonic cancer and endometrial cancer at young age, 80% of affected individuals will get colonic and/ or endometrial cancer, High risk individuals may be identified using the Amsterdam criteria, , Amsterdam criteria, Three or more family members with a confirmed diagnosis of colorectal cancer, one of whom is a, first degree (parent, child, sibling) relative of the other two., Two successive affected generations., One or more colon cancers diagnosed under age 50 years., Familial adenomatous polyposis (FAP) has been excluded., Gardners syndrome, , , , , , , , , Autosomal dominant familial colorectal polyposis, Multiple colonic polyps, Extra colonic diseases include: skull osteoma, thyroid cancer and epidermoid cysts, Desmoid tumours are seen in 15%, Mutation of APC gene located on chromosome 5, Due to colonic polyps most patients will undergo colectomy to reduce risk of colorectal, cancer, Now considered a variant of familial adenomatous polyposis coli, Next question
Page 1065 :
Question 137 of 147, A 23 year old man suffers a thermal injury to his left hand. It becomes red and painful. Which of the, following mediators are not involved in this process?, , Histamine, , Free radicals, , Prostaglandins, , Leukotrienes, , Serotonin, Acute inflammation is not mediated by free radicals, Chemical mediators facilitate the spread of inflammation into normal tissue, Chemical mediators include:, , , , Lysosomal compounds, Chemokines such as serotinin and histamine (released by platelets and mast cells), , Other enzyme cascades producing inflammatory mediators include:, , , Complement, kinin, coagulation system and fibrinolytic system, , Please rate this question:, , Discuss and give feedback, , Next question, , Acute inflammation, Inflammation is the reaction of the tissue elements to injury. Vascular changes occur, resulting in the, generation of a protein rich exudate. So long as the injury does not totally destroy the existing tissue, architecture, the episode may resolve with restoration of original tissue architecture.
Page 1066 :
Vascular changes, , , , , , Vasodilation occurs and persists throughout the inflammatory phase., Inflammatory cells exit the circulation at the site of injury., The equilibrium that balances Starlings forces within capillary beds is disrupted and a protein, rich exudate will form as the vessel walls also become more permeable to proteins., The high fibrinogen content of the fluid may form a fibrin clot. This has several important, immunomodulatory functions., , Sequelae, , Resolution, , , , , Typically occurs with minimal initial injury, Stimulus removed and normal tissue architecture results, , Organisation, , , , , Delayed removal of exudate, Tissues undergo organisation and usually fibrosis, , Suppuration, , , , , Typically formation of an abscess or an empyema, Sequestration of large quantities of dead neutrophils, , Progression to chronic, inflammation, , , , , Coupled inflammatory and reparative activities, Usually occurs when initial infection or suppuration has, been inadequately managed, , Causes, , , , , , , Infections e.g. Viruses, exotoxins or endotoxins released by bacteria, Chemical agents, Physical agents e.g. Trauma, Hypersensitivity reactions, Tissue necrosis, , Presence of neutrophil polymorphs is a histological diagnostic feature of acute inflammation, Next question
Page 1067 :
Question 138 of 147, , An enthusiastic medical student approaches you with a list of questions about blood transfusion, reactions. Which of her following points is incorrect?, , Graft versus host disease involves neutrophil proliferation, , Thrombocytopaenia may occur in women with a prior pregnancy, , IgA antibodies may cause blood pressure compromise during transfusion, , Hypocalcaemia can occur, , Iron overload can be avoided by chelation therapy, Mnemonic for transfusion reactions:, Got a bad unit, G raft vs. Host disease, O verload, T hrombocytopaenia, A lloimmunization, B lood pressure unstable, A cute haemolytic reaction, D elayed haemolytic reaction, U rticaria, N eutrophilia, I nfection, T ransfusion associated lung injury, , GVHD results from lymphocytic proliferation. The patient's own lymphocytes are similar to the, donor's lymphocytes, therefore don't perceive them as being foreign. The donor lymphocytes,, however, sees the recipient lymphocytes as being foreign. Therefore they proliferate causing severe
Page 1068 :
complications., Thrombocytopaenia occurs a few days after transfusion and may resolve spontaneously., Patients with IGA antibodies need IgA deficient blood transfusions., Please rate this question:, , Discuss and give feedback, , Next question, , Blood transfusion reactions, Acute transfusion reactions present as adverse signs or symptoms during or within 24 hours of a, blood transfusion. The most frequent reactions are fever, chills, pruritus, or urticaria, which typically, resolve promptly without specific treatment or complications. Other signs occurring in temporal, relationship with a blood transfusion, such as severe dyspnoea, pyrexia, or loss of consciousness, may be the first indication of a more severe potentially fatal reaction., The causes of adverse reactions are multi-factorial. Immune mediated reactions, some of the most, feared, occur as a result of component mismatch, the commonest cause of which is clerical error., More common, non immune mediated, complications may occur as a result of product, contamination, this may be bacterial or viral., Transfusion related lung injury is well recognised and there are two proposed mechanisms which, underpin this. One involves the sequestration of primed neutrophils within the recipient pulmonary, capillary bed. The other proposed mechanism suggests that HLA mismatches between donor, neutrophils and recipient lung tissue is to blame., The table below summarises the main types of transfusion reaction., , Immune mediated, , Non immune mediated, , Pyrexia, , Hypocalcaemia, , Alloimmunization, , CCF, , Thrombocytopaenia, , Infections
Page 1069 :
Immune mediated, , Non immune mediated, , Transfusion associated lung injury, , Hyperkalaemia, , Graft vs Host disease, , Urticaria, , Acute or delayed haemolysis, , ABO incompatibility, , Rhesus incompatibility, Next question
Page 1070 :
Question 139 of 147, An 82 year old lady presents with a carcinoma of the caecum. Approximately what proportion of, patients presenting with this diagnosis will have synchronous lesions?, , <1%, , 60%, , 50%, , 20%, , 5%, Synchronous colonic tumours are seen in 5% cases and all patients having a flexible sigmoidoscopy, should have completion colonoscopy if tumours or polyps are found, Synchronous lesions may occur in up to 5% of patients with colorectal cancer. A full and complete, lumenal study with either colonoscopy, CT cologram or barium enema is mandatory in all patients, being considered for surgery., Please rate this question:, , Discuss and give feedback, , Next question, , Colorectal cancer, , , , , , , , , Annually about 150,000 new cases are diagnosed and 50,000 deaths from the disease, About 75% will have sporadic disease and 25% will have a family history, Colorectal tumours comprise a spectrum of disease ranging from adenomas through to polyp, cancers and frank malignancy., Polyps may be categorised into: neoplastic polyps, adenomatous polyps and non neoplastic, polyps., The majority of adenomas are polypoidal lesions, although flat lesions do occur and may, prove to be dysplastic., Non-neoplastic polyps include hyperplastic, juvenile, hamartomatous, inflammatory, and, lymphoid polyps, which have not generally been thought of as precursors of cancer., Three characteristics of adenomas that correlate with malignant potential have been, characterised. These include increased size, villous architecture and dysplasia. For this, reason most polyps identified at colonoscopy should be removed.
Page 1071 :
, , The transformation from polyp to cancer is described by the adenoma - carcinoma sequence, and its principles should be appreciated. Essentially genetic changes accompany the, transition from adenoma to carcinoma; key changes include APC, c-myc, K RAS mutations, and p53 deletions., Next question
Page 1072 :
Question 140 of 147, , A 22 year old man undergoes a splenectomy for an iatrogenic splenic injury. On the second post, operative day a full blood count is performed. Which of the following components of the full blood, count is the first to be affected ?, , Erythrocyte count, , Reticulocyte count, , Eosinophil count, , Monocyte count, , Lymphocyte count, , Theme from January 2012 Exam, The granulocyte and platelet count are the first to be affected following splenectomy. Then, reticulocytes increase. Although a lymphocytosis and monocytosis are reported, these take several, weeks to develop., Please rate this question:, , Discuss and give feedback, , Next question, , Post splenectomy blood film changes, The loss of splenic tissue results in the inability to readily remove immature or abnormal red blood, cells from the circulation. The red cell count does not alter significantly. However, cytoplasmic, inclusions may be seen e.g. Howell-Jolly bodies., In the first few days after splenectomy target cells, siderocytes and reticulocytes will appear in the, circulation. Immediately following splenectomy a granulocytosis (mainly composed of neutrophils) is
Page 1073 :
seen, this is replaced by a lymphocytosis and monocytosis over the following weeks., The platelet count is usually increased and this may be persistent, oral antiplatelet agents may be, needed in some patients., Image showing Howell Jolly bodies (arrowed), , Image sourced from Wikipedia, , Next question
Page 1074 :
Question 141 of 147, , A 28 year old lady presents with benign cyclical mastalgia. Which of the following is not a recognised, treatment for the condition?, , Evening primrose oil, , Bromocriptine, , Methotrexate, , Danazol, , Tamoxifen, Surgical excision of tender breast tissue is inappropriate, , Methotrexate is used for the treatment of breast cancer. Whilst the use of tamoxifen is of benefit, other agents such as flaxseed oil or evening primrose oil should be tried first. Danazol is effective,, but many women dislike the side effects., Please rate this question:, , Discuss and give feedback, , Next question, , Benign cyclical mastalgia, Benign cyclical mastalgia is a common cause of breast pain in younger females. It varies in intensity, according to the phase of the menstrual cycle. It is not associated with point tenderness of the chest, wall (more likely to be Tietze's syndrome)., The underlying cause is difficult to pinpoint, examination should focus on identifying focal lesions
Page 1075 :
(such as cysts) that may be treated to provide symptomatic benefit. Women should be advised to, wear a supportive bra. Conservative treatments include flax seed oil and evening primrose oil. There, is slightly more evidence in favor of flax seed oil, though neither has performed much better than, placebo in RCT's., Hormonal agents such as bromocriptine and danazol may be more effective. However, many women, discontinue these therapies due to adverse effects., Next question
Page 1076 :
Question 142 of 147, , A 39 year old lady has undergone surgery for breast cancer. As part of the histopathology report the, pathologist provides the surgeon with a Nottingham Prognostic Index score of 6.4. He also states, that the tumour size is 2cm. Which of the following inferences can be made in relation to this, statement?, , The tumour is likely to be grade 1, , Vascular invasion is present, , Lymph node metastasis are definitely present, , The tumour is oestrogen receptor positive, , None of the above, , A score of this value is unlikely to be reached with a grade 1 tumour and a size of 2cm. Therefore, lymph node metastasis are definitely present. In addition since the maximal score for lymph node, metastasis is 3 the tumour is likely be of a higher grade (see below). The Nottingham Prognostic, Index provides no information about oestrogen receptor status or the presence or absence of, vascular invasion., Please rate this question:, , Discuss and give feedback, , Next question, , Nottingham prognostic index, The Nottingham Prognostic Index can be used to give an indication of survival following breast, cancer surgery. In this system, the tumour size is weighted less heavily than other major prognostic, parameters.
Page 1077 :
Calculation of NPI, Tumour Size x 0.2 + Lymph node score(From table below)+Grade score(From table below)., , Lymph nodes involved, , Grade, , 1, , 0, , 1, , 2, , 1-3, , 2, , 3, , >3, , 3, , Score, , Prognosis, , Score, , Percentage 5 year survival, , 2.0 to 2.4, , 93%, , 2.5 to 3.4, , 85%, , 3.5 to 5.4, , 70%, , >5.4, , 50%, , This data was originally published in 1992. It should be emphasised that other factors such as, vascular invasion and receptor status also impact on survival and are not included in this data and, account for varying prognoses often cited in the literature., Reference, Galea, M.H., et al., The Nottingham Prognostic Index in primary breast cancer. Breast Cancer Res, Treat, 1992. 22(3): p. 207-19.
Page 1078 :
Question 143 of 147, , In patients with multiple endocrine neoplasia type IIb which of the following clinical appearances is, the patient most likely to display?, , Acromegalic facies, , Turners type features, , Profound kyphoscoliosis, , Multiple bony exostoses, , Marfanoid features, , Patients with MEN IIb may display Marfanoid features. It is unclear at the present time whether they, have discrete changes in the microfibrils of elastic fibres that are present in Marfans., Please rate this question:, , Discuss and give feedback, , Next question, , Multiple Endocrine Neoplasia, Multiple endocrine neoplasia (MEN) is inherited as an autosomal dominant disorder., The table below summarises the three main types of MEN:, , MEN type I, , MEN type IIa, , MEN type IIb
Page 1080 :
Question 144 of 147, A 32 year old man undergoes an appendicectomy. A large carcinoid tumour is identified and a, completion right hemicolectomy is performed. He is well for several months and then develops, symptoms of palpitations and facial flushing. Which of the following diagnostic markers should be, requested?, , Alpha feto protein, , Urinary 5-Hydroxyindoleacetic acid measurements, , Urinary catecholamines, , Urinary VMA measurements, , None of the above, , 5 HIAA is the most commonly used diagnostic marker for carcinoid syndrome, it is measured in a 24, hour urine collection., Please rate this question:, , Discuss and give feedback, , Next question, , Carcinoid syndrome, , , , , , Carcinoid tumours secrete serotonin, Originate in neuroendocrine cells mainly in the intestine (midgut-distal ileum/appendix), Can occur in the rectum, bronchi, Hormonal symptoms mainly occur when disease spreads outside the bowel, , Clinical features, , , , , , , , Onset: insidious over many years, Flushing face, Palpitations, Pulmonary valve stenosis and tricuspid regurgitation causing dyspnoea, Asthma, Severe diarrhoea (secretory, persists despite fasting)
Page 1082 :
Question 145 of 147, , A 20 year old male is referred to the clinic. He has undergone genetic testing because his father died, from colorectal cancer at the age of 21. His testing revealed a mutation of the APC gene. A, colonoscopy is proposed. What is the most likely finding?, , Multiple colonic hamartomas, , Carpet villous adenoma of the rectum, , Caecal carcinoma, , Multiple colonic adenomas, , Multiple colonic hyperplastic polyps, , APC mutations are found in familial adenomatous polyposis coli. These have multiple colonic, adenomas., Please rate this question:, , Discuss and give feedback, , Next question, , Polyposis syndromes, , Syndrome, , Genetic defect, , Features, , Screening and, management, , Associated, disorders, , Familial, , Mutation of APC, , Typically over 100, , If known to be at risk, , Gastric fundal
Page 1083 :
Screening and, management, , Associated, disorders, , colonic adenomas, Cancer risk of 100%, 20% are new, mutations, , then predictive, genetic testing as, teenager, Annual flexible, sigmoidoscopy from, 15 years, If no polyps found, then 5 yearly, colonoscopy started, at age 20, Polyps found =, resectional surgery, (resection and pouch, Vs sub total, colectomy and IRA), , polyps (50%)., Duodenal polyps, 90%., If severe, duodenal, polyposis cancer, risk of 30% at 10, years., Abdominal, desmoid, tumours., , Biallelic mutation, of mut Y human, homologue (MYH), on chromosome, 1p, recessive, , Multiple colonic, polyps, Later onset right, sided cancers more, common than in FAP, 100% cancer risk by, age 60, , Once identified, resection and, ileoanal pouch, reconstruction is, recommended, Attenuated, phenotype - regular, colonoscopy, , Duodenal, polyposis in 30%, Associated with, increased risk of, breast cancer, (self examination), , STK11 (LKB1), mutation on, chromosome 19 in, some (but not all), cases, dominant, , Multiple benign, intestinal, hamartomas, Episodic obstruction, and intussceception, Increased risk of GI, cancers (colorectal, cancer 20%, gastric, 5%), Increased risk of, , Annual examination, Pan intestinal, endoscopy every 2-3, years, , Malignancies at, other sites, Classical, pigmentation, pattern, , Syndrome, , Genetic defect, , Features, , adenomatous, polyposis, , gene (80%) cases,, dominant, , MYH, associated, polyposis, , Peutz -Jeghers, syndrome
Page 1084 :
Syndrome, , Genetic defect, , Features, , Screening and, management, , Associated, disorders, , breast, ovarian,, cervical pancreatic, and testicular, cancers, , Cowden, disease, , Mutation of PTEN, gene on, chromosome, 10q22, dominant, , Macrocephaly, Multiple intestinal, hamartomas, Multiple, trichilemmomas, 89% risk of cancer at, any site, 16% risk of colorectal, cancer, , Targeted, individualised, screening, , Breast cancer, (81% risk), Thyroid cancer, and non toxic, goitre, Uterine cancer, , HNPCC (Lynch, syndrome), , Germline, mutations of DNA, mismatch repair, genes, , Colo rectal cancer, 30-70%, Endometrial cancer, 30-70%, Gastric cancer 5-10%, Scanty colonic polyps, may be present, Colonic tumours, likely to be right, sided and mucinous, , Colonoscopy every 12 years from age 25, Consideration of, prophylactic surgery, Extra colonic, surveillance, recommended, , Extra colonic, cancers, , Next question
Page 1085 :
Question 146 of 147, , Which of the following breast tumours is most commonly associated with a risk of metastasis to the, contralateral breast?, , Invasive ductal carcinoma, , Invasive lobular carcinoma, , Phyllodes tumour, , Pagets disease of the breast, , Atypical ductal hyperplasia, , Risk of metastasis to the contralateral breast is a classical feature of invasive lobular carcinoma., Please rate this question:, , Discuss and give feedback, , Next question, , Lobular carcinoma of the breast, Lobular breast cancers are less common than their ductal counterparts. They typically present, differently, the mass is usually more diffuse and less obvious on the usual imaging modalities of, ultrasound and mammography. This is significant since the disease may be understaged resulting in, inadequate treatment when wide local excision is undertaken., In women with invasive lobular carcinoma it is usually safest to perform an MRI scan of the breast, if, breast conserving surgery is planned., Lobular carcinomas are also more likely to be multifocal and metastasise to the contralateral breast., Lobular carcinoma in situ is occasionally diagnosed incidentally on core biopsies. Unlike DCIS,
Page 1086 :
lobular carcinoma in situ is far less strongly associated with foci of invasion and is usually managed, by close monitoring., Next question
Page 1087 :
Question 147 of 147, Which is the characteristic finding on a blood film post splenectomy?, , Stipple cell, , Tear drop cell, , Reticulocytes, , Howell-Jolly bodies, , Schistocyte, , Blood film in hyposplenism:, Howell-Jolly bodies, Pappenheimer bodies, Poikilocytes (Target cells), Erythrocyte containing siderotic granules, Heinz bodies, Please rate this question:, , Discuss and give feedback, , Splenectomy, Indications, , , , , , , Trauma: 1/4 are iatrogenic, Spontaneous rupture: EBV, Hypersplenism: hereditary spherocytosis or elliptocytosis etc, Malignancy: lymphoma or leukaemia, Splenic cysts, hydatid cysts, splenic abscesses, , Splenectomy, Technique, Trauma
Page 1088 :
, , , , , , , , , , , , GA, Long midline incision, If time permits insert a self retaining retractor (e.g. Balfour/ omnitract), Large amount of free blood is usually present. Pack all 4 quadrants of the abdomen. Allow, the anaesthetist to 'catch up', Remove the packs and assess the viability of the spleen. Hilar injuries and extensive, parenchymal lacerations will usually require splenectomy., Divide the short gastric vessels and ligate them., Clamp the splenic artery and vein. Two clamps on the patient side are better and allow for, double ligation and serve as a safety net if your assistant does not release the clamp, smoothly., Be careful not to damage the tail of the pancreas, if you do then this will need to be formally, removed and the pancreatic duct closed., Wash out the abdomen and place a tube drain to the splenic bed., Some surgeons implant a portion of spleen into the omentum, whether you decide to do this, is a matter of personal choice., Post operatively the patient will require prophylactic penicillin V and pneumococcal vaccine., , Elective, Elective splenectomy is a very different operation from that performed in the emergency setting. The, spleen is often large (sometimes massive). Most cases can be performed laparoscopically. The, spleen will often be macerated inside a specimen bag to facilitate extraction., Complications, , , , , , Haemorrhage (may be early and either from short gastrics or splenic hilar vessels, Pancreatic fistula (from iatrogenic damage to pancreatic tail), Thrombocytosis: prophylactic aspirin, Encapsulated bacteria infection e.g. Strep. pneumoniae, Haemophilus, influenzae and Neisseriameningitidis, , Post splenectomy changes, , , , , , Platelets will rise first (therefore in ITP should be given after splenic artery clamped), Blood film will change over following weeks, Howell Jolly bodies will appear, Other blood film changes include target cells and Pappenheimer bodies, Increased risk of post splenectomy sepsis, therefore prophylactic antibiotics and, pneumococcal vaccine should be given., , Post splenectomy sepsis, , , , Typically occurs with encapsulated organisms, Opsonisation occurs but then not recognised
Page 1090 :
Question 1 of 560, Which of the following structures is not transmitted by the jugular foramen?, , Hypoglossal nerve, , Accessory nerve, , Internal jugular vein, , Inferior petrosal sinus, , Vagus nerve, Contents of the jugular foramen:, Anterior: inferior petrosal sinus, Intermediate: glossopharyngeal, vagus, and accessory nerves, Posterior: sigmoid sinus (becoming the internal jugular vein) and some meningeal branches from the, occipital and ascending pharyngeal arteries, Theme from 2009 exam, The jugular foramen may be divided into three compartments:, , , , , Anterior compartment transmits the inferior petrosal sinus, Middle compartment transmits cranial nerves IX, X and XI, Posterior compartment transmits the sigmoid sinus, , Please rate this question:, , Discuss and give feedback, , Next question, , Foramina of the base of the skull, Foramen, , Location, , Contents
Page 1092 :
Foramen, , Location, , Contents, , Abducent nerve (VI), Superior ophthalmic vein, , *= In life the foramen lacerum is occluded by a cartilagenous plug. The ICA initially passes into the, carotid canal which ascends superomedially to enter the cranial cavity through the foramen lacerum., Base of skull anatomical overview, , Image sourced from Wikipedia, , Next question
Page 1093 :
Question 2 of 560, A 19 year old female is admitted with suspected meningitis. The House Officer is due to perform a, lumbar puncture. What is the most likely structure first encountered when the needle is inserted?, , Ligamentum flavum, , Denticulate ligament, , Dural sheath, , Pia Mater, , Supraspinous ligament, , Theme from September 2012 exam, Please rate this question:, , Discuss and give feedback, , Next question, , Lumbar puncture, Lumbar punctures are performed to obtain cerebrospinal fluid. In adults, the procedure is best, performed at the level of L3/L4 or L4/5 interspace. These regions are below the termination of the, spinal cord at L1., During the procedure the needle passes through:, , , , , The supraspinous ligament which connects the tips of spinous processes and the, interspinous ligaments between adjacent borders of spinous processes, Then the needle passes through the ligamentum flavum, which may cause a give as it is, penetrated, A second give represents penetration of the needle through the dura mater into the, subarachnoid space. Clear CSF should be obtained at this point, , References, Boon et al Lumbar Puncture: Anatomical Review of a Clinical Skill. Clinical Anatomy 17:544553, (2004)
Page 1094 :
Question 3 of 560, A 45 year old motor cyclist sustains a tibial fracture and is noted to have anaesthesia of the web, space between his first and second toes. Which of the nerves listed below is most likely to be, compromised?, , Superficial peroneal nerve, , Deep peroneal nerve, , Sural nerve, , Long saphenous nerve, , Tibial nerve, , Theme from September 2014 Exam, The deep peroneal nerve lies in the anterior muscular compartment of the lower leg and can be, compromised by compartment syndrome affecting this area. It provides cutaneous sensation to the, first web space. The superficial peroneal nerve provides more lateral cutaneous innervation., Please rate this question:, , Discuss and give feedback, , Next question, , Deep peroneal nerve, Origin, , From the common peroneal nerve, at the lateral aspect of the fibula, deep to, peroneus longus, , Nerve root values, , L4, L5, S1, S2, , Course and, relation, , , , , Pierces the anterior intermuscular septum to enter the anterior, compartment of the lower leg, Passes anteriorly down to the ankle joint, midway between the two
Page 1096 :
Question 4 of 560, , A patient undergoes a femoral hernia repair and at operation the surgeon decides to enter the, abdominal cavity to resect small bowel. She makes a transverse incision two thirds of the way, between umbilicus and the symphysis pubis. Which of the structures listed below will not be divided?, , Rectus abdominis, , External oblique aponeurosis, , Peritoneum, , Fascia transversalis, , Posterior lamina of the rectus sheath, , An incision at this level lies below the arcuate line and the posterior wall of the rectus sheath is, deficient at this level., Please rate this question:, , Discuss and give feedback, , Next question, , Rectus abdominis muscle, The rectus sheath is formed by the aponeuroses of the lateral abdominal wall muscles. The rectus, sheath has a composition that varies according to anatomical level., 1. Above the costal margin the anterior sheath is composed of external oblique aponeurosis, the, costal cartilages are posterior to it., 2. From the costal margin to the arcuate line, the anterior rectus sheath is composed of external, oblique aponeurosis and the anterior part of the internal oblique aponeurosis. The posterior part of
Page 1098 :
Question 5 of 560, What is the lymphatic drainage of the ovaries?, , Internal iliac nodes, , Common iliac nodes, , Para-aortic nodes, , Para uterine nodes, , Inguinal nodes, , Theme from September 2015 Exam, The lymphatic drainage of the ovary follows the gonadal vessels and drainage is therefore to the, para-aortic nodes., Please rate this question:, , Discuss and give feedback, , Next question, , Lymphatic drainage of the ovaries, uterus and cervix, , , , , , The ovaries drain to the para-aortic lymphatics via the gonadal vessels., The uterine fundus has a lymphatic drainage that runs with the ovarian vessels and may thus, drain to the para-aortic nodes. Some drainage may also pass along the round ligament to the, inguinal nodes., The body of the uterus drains through lymphatics contained within the broad ligament to the, iliac lymph nodes., The cervix drains into three potential nodal stations; laterally through the broad ligament to, the external iliac nodes, along the lymphatics of the uterosacral fold to the presacral nodes, and posterolaterally along lymphatics lying alongside the uterine vessels to the internal iliac, nodes., Next question
Page 1099 :
Question 6-8 of 560, , Theme: Axillary anatomy, , A. Medial pectoral nerve, B. Thoracodorsal nerve, C. Lateral pectoral nerve, D. Intercostobrachial nerve, E. Medial cord of the brachial plexus, F. Long thoracic nerve, G. Axillary nerve, H. Accessory nerve, , Please identify the structure that is most likely to be affected in the scenarios described below. Each, structure may be used once, more than once or not at all., , 6., , A 44 year old lady has undergone a mastectomy and axillary node clearance. Post operatively, she, notices a patch of anaesthesia of her axillary skin when she applies an underarm deodorant., You answered Medial pectoral nerve, The correct answer is Intercostobrachial nerve, The intercostobrachial nerves traverse the axilla and innervate the overlying skin. These can be, injured or divided during axillary surgery and the result is anaesthesia of the overlying skin., , 7., , A 44 year old lady has undergone a mastectomy and axillary node clearance to treat breast cancer., Post operatively, it is noted that she has winging of the scapula., You answered Medial pectoral nerve
Page 1100 :
The correct answer is Long thoracic nerve, Injury to the long thoracic nerve (which innervates the serratus anterior) can occur as it lies at the, medial aspect of the axilla, winging of the scapula will then result., , 8., , A 44 year old lady who works as an interior decorator has undergone a mastectomy and axillary, node clearance to treat breast cancer. Post operatively, she comments that her arm easily, becomes fatigued when she is painting walls., You answered Medial pectoral nerve, The correct answer is Thoracodorsal nerve, The most likely explanation for this is that the thoracodorsal nerve has been injured. This will result, in atrophy of latissimus dorsi and this will become evident with repetitive arm movements where, the arm is elevated and moving up and down (such as in painting). Injury to the pectoral nerves, may produce a similar picture but this pattern of injury is very rare and the pectoral nerves are, seldom injured in breast surgery., , Please rate this question:, , Discuss and give feedback, , Next question, , Axilla, Boundaries of the axilla, , Medially, , Chest wall and Serratus anterior, , Laterally, , Humeral head
Page 1101 :
Floor, , Subscapularis, , Anterior aspect, , Lateral border of Pectoralis major, , Fascia, , Clavipectoral fascia, , Content:, , Long thoracic nerve (of, Bell), , Derived from C5-C7 and passes behind the brachial plexus to enter the axilla., It lies on the medial chest wall and supplies serratus anterior. Its location, puts it at risk during axillary surgery and damage will lead to winging of the, scapula., , Thoracodorsal nerve and, thoracodorsal trunk, , Innervate and vascularise latissimus dorsi., , Axillary vein, , Lies at the apex of the axilla, it is the continuation of the basilic vein., Becomes the subclavian vein at the outer border of the first rib., , Intercostobrachial nerves, , Traverse the axillary lymph nodes and are often divided during axillary, surgery. They provide cutaneous sensation to the axillary skin., , Lymph nodes, , The axilla is the main site of lymphatic drainage for the breast., Next question
Page 1102 :
Question 9 of 560, A 35 year old farm labourer injures the posterior aspect of his hand with a mechanical scythe. He, severs some of his extensor tendons in this injury. How many tunnels lie in the extensor retinaculum, that transmit the tendons of the extensor muscles?, , One, , Three, , Four, , Five, , Six, , There are six tunnels, each lined by its own synovial sheath., Please rate this question:, , Discuss and give feedback, , Next question, , Extensor retinaculum, The extensor rentinaculum is a thickening of the deep fascia that stretches across the back of the, wrist and holds the long extensor tendons in position., Its attachments are:, , , , The pisiform and triquetral medially, The end of the radius laterally, , Structures related to the extensor retinaculum, , Structures superficial to the, retinaculum, , , , , , , Basilic vein, Dorsal cutaneous branch of the ulnar nerve, Cephalic vein, Superficial branch of the radial nerve
Page 1104 :
A 23 year old man undergoes an orchidectomy. The right testicular vein is ligated; into which, structure does it drain?, , Right renal vein, , Inferior vena cava, , Common iliac vein, , Internal iliac vein, , External iliac vein, , Theme from April 2012 exam, Theme from April 2014 exam, The testicular venous drainage begins in the septa and these veins together with those of the tunica, vasculosa converge on the posterior border of the testis as the pampiniform plexus. The, pampiniform plexus drains to the testicular vein. The left testicular vein drains into the left renal vein., The right testicular vein drains into the inferior vena cava., Please rate this question:, , Discuss and give feedback, , Next question, , Scrotal and testicular anatomy, Spermatic cord, Formed by the vas deferens and is covered by the following structures:, , Layer, , Origin, , Internal spermatic fascia, , Transversalis fascia, , Cremasteric fascia, , From the fascial coverings of internal oblique
Page 1105 :
Layer, , Origin, , External spermatic fascia, , External oblique aponeurosis, , Contents of the cord, , Vas deferens, , Transmits sperm and accessory gland secretions, , Testicular artery, , Branch of abdominal aorta supplies testis and, epididymis, , Artery of vas deferens, , Arises from inferior vesical artery, , Cremasteric artery, , Arises from inferior epigastric artery, , Pampiniform plexus, , Venous plexus, drains into right or left testicular vein, , Sympathetic nerve fibres, , Lie on arteries, the parasympathetic fibres lie on the, vas, , Genital branch of the genitofemoral, nerve, , Supplies cremaster, , Lymphatic vessels, , Drain to lumbar and para-aortic nodes, , Scrotum, , , , , , Testes, , Composed of skin and closely attached dartos fascia., Arterial supply from the anterior and posterior scrotal arteries, Lymphatic drainage to the inguinal lymph nodes, Parietal layer of the tunica vaginalis is the innermost layer
Page 1106 :
, , , , , The testes are surrounded by the tunica vaginalis (closed peritoneal sac). The parietal layer, of the tunica vaginalis adjacent to the internal spermatic fascia., The testicular arteries arise from the aorta immediately inferiorly to the renal arteries., The pampiniform plexus drains into the testicular veins, the left drains into the left renal vein, and the right into the inferior vena cava., Lymphatic drainage is to the para-aortic nodes., Next question
Page 1107 :
Question 11 of 560, A 44 year old lady is undergoing an abdominal hysterectomy and the ureter is identified during the, ligation of the uterine artery. At which site does it insert into the bladder?, , Posterior, , Apex, , Anterior, , Base, , Superior aspect of the lateral side, , Theme from September 2012 Exam, The ureters enter the bladder at the upper lateral aspect of the base of the bladder. They are about, 5cm apart from each other in the empty bladder. Internally this aspect is contained within the bladder, trigone., Please rate this question:, , Discuss and give feedback, , Next question, , Ureter, , , , , , , , , 25-35 cm long, Muscular tube lined by transitional epithelium, Surrounded by thick muscular coat. Becomes 3 muscular layers as it crosses the bony pelvis, Retroperitoneal structure overlying transverse processes L2-L5, Lies anterior to bifurcation of iliac vessels, Blood supply is segmental; renal artery, aortic branches, gonadal branches, common iliac, and internal iliac, Lies beneath the uterine artery, Next question
Page 1108 :
Question 12 of 560, , What is the correct embryological origin of the stapes?, , First pharyngeal arch, , Second pharyngeal arch, , Third pharyngeal arch, , Fourth pharyngeal arch, , Fifth pharyngeal arch, Embryological origin stapes = 2nd pharyngeal arch, The ectoderm covering the outer aspect of the second arch originates from a strip of ectoderm, lateral to the metencephalic neural fold. The cartilaginous element to this, eponymously known as, Reicherts cartilage extends from the otic capsule to the midline on each side. Its dorsal end, separates and becomes enclosed in the tympanic cavity as the stapes., , Theme from September 2013 exam, Theme from April 2012 Exam, The dorsal ends of the cartilages of the first and second pharyngeal arches articulate superior to the, tubotympanic recess. These cartilages form the malleus, incus and stapes. At least part of the, malleus is formed from the first arch and the stapes from the second arch. The incus is most likely to, arise from the first arch., Please rate this question:, , Discuss and give feedback, , Next question, , Pharyngeal arches
Page 1109 :
These develop during the fourth week of embryonic growth from a series of mesodermal, outpouchings of the developing pharynx., They develop and fuse in the ventral midline. Pharyngeal pouches form on the endodermal side, between the arches., There are 6 pharyngeal arches, the fifth does not contribute any useful structures and often fuses, with the sixth arch., Pharyngeal arches, , Pharyngeal, arch, , Muscular, contributions, , Skeletal, contributions, , First, , Muscles of, mastication, Anterior belly of, digastric, Mylohyoid, Tensor tympanic, Tensor veli palatini, , Second, , Endocrine, , Artery, , Nerve, , Maxilla, Meckels, cartilage, Incus, Malleus, , n/a, , Maxillary, External, carotid, , Mandibular, , Buccinator, Platysma, Muscles of facial, expression, Stylohyoid, Posterior belly of, digastric, Stapedius, , Stapes, Styloid process, Lesser horn, and upper, body of hyoid, , n/a, , Inferior, branch of, superior, thyroid artery, Stapedial, artery, , Facial, , Third, , Stylopharyngeus, , Greater horn, and lower part, of hyoid, , Thymus, Inferior, parathyroids, , Common and, internal, carotid, , Glossopharyngeal, , Fourth, , Cricothyroid, All intrinsic, muscles of the soft, palate, , Thyroid and, epiglottic, cartilages, , Superior, parathyroids, , Rightsubclavian, artery, Leftaortic arch, , Vagus
Page 1110 :
Pharyngeal, arch, , Muscular, contributions, , Skeletal, contributions, , Sixth, , All intrinsic, muscles of the, larynx (except, cricothyroid), , Cricoid,, arytenoid and, corniculate, cartilages, , Endocrine, , Artery, , Nerve, , n/a, , Right Pulmonary, artery, LeftPulmonary, artery and, ductus, arteriosus, , Vagus and, recurrent, laryngeal nerve, , Next question
Page 1111 :
Question 13 of 560, A 20 year old lady presents with pain on the medial aspect of her thigh. Investigations show a large, ovarian cyst. Compression of which of the nerves listed below is the most likely underlying cause?, , Sciatic, , Genitofemoral, , Obturator, , Ilioinguinal, , Femoral cutaneous, , Theme from April 2012 Exam, The cutaneous branch of the obturator nerve is frequently absent. However, the obturator nerve is a, recognised contributor to innervation of the medial thigh and large pelvic tumours may compress this, nerve with resultant pain radiating distally., Please rate this question:, , Discuss and give feedback, , Next question, , Obturator nerve, The obturator nerve arises from L2, L3 and L4 by branches from the ventral divisions of each of, these nerve roots. L3 forms the main contribution and the second lumbar branch is occasionally, absent. These branches unite in the substance of psoas major, descending vertically in its posterior, part to emerge from its medial border at the lateral margin of the sacrum. It then crosses the, sacroiliac joint to enter the lesser pelvis, it descends on obturator internus to enter the obturator, groove. In the lesser pelvis the nerve lies lateral to the internal iliac vessels and ureter, and is joined, by the obturator vessels lateral to the ovary or ductus deferens., Supplies, , , , Medial compartment of thigh, Muscles supplied: external obturator, adductor longus, adductor brevis, adductor magnus, (not the lower part-sciatic nerve), gracilis
Page 1112 :
, , The cutaneous branch is often absent. When present, it passes between gracilis and, adductor longus near the middle part of the thigh, and supplies the skin and fascia of the, distal two thirds of the medial aspect., , Obturator canal, , , Connects the pelvis and thigh: contains the obturator artery, vein, nerve which divides into, anterior and posterior branches., , Cadaveric cross section demonstrating relationships of the obturator nerve, , Image sourced from Wikipedia, , Next question
Page 1113 :
Question 14 of 560, A 73 year old man presents with a tumour at the central aspect of the posterior third of the tongue., To which of the following lymph node groups is it most likely to metastasise?, , Submental, , Submandibular, , Ipsilateral deep cervical nodes, , Contralateral deep cervical nodes, , Bilateral deep cervical nodes, Posterior third tumours of the tongue commonly metastasise to the bilateral deep cervical lymph, nodes, Tumours of the posterior third of the tongue will typically metastasise early and bilateral nodal, involvement is well recognised, this is most often true of centrally located tumours and those, adjacent to the midline as the lymph vessels may cross the median plane at this location., Please rate this question:, , Discuss and give feedback, , Next question, , Lymphatic drainage of the tongue, , , , , , The lymphatic drainage of the anterior two thirds of the tongue shows only minimal, communication of lymphatics across the midline, so metastasis to the ipsilateral nodes is, usual., The lymphatic drainage of the posterior third of the tongue have communicating networks, as, a result early bilateral nodal metastases are more common in this area., Lymphatics from the tip of the tongue usually pass to the sub mental nodes and from there to, the deep cervical nodes., Lymphatics from the mid portion of the tongue usually drain to the submandibular nodes and, then to the deep cervical nodes. Mid tongue tumours that are laterally located will usually, drain to the ipsilateral deep cervical nodes, those from more central regions may have, bilateral deep cervical nodal involvement., Next question
Page 1114 :
Question 15 of 560, , A 6 month old child is brought to the surgical clinic because of non descended testes. What is the, main structure that determines the descent path of the testicle?, , Processus vaginalis, , Cremaster, , Mesorchium, , Inguinal canal, , Gubernaculum, , Theme from April 2012 exam, Theme from April 2014 exam, The gubernaculum is a ridge of mesenchymal tissue that connects the testis to the inferior aspect of, the scrotum. Early in embryonic development the gubernaculum is long and the testis are located on, the posterior abdominal wall. During foetal growth the body grows relative to the gubernaculum, with, resultant descent of the testis., Please rate this question:, , Discuss and give feedback, , Next question, , Testicular embryology, Until the end of foetal life the testicles are located within the abdominal cavity. They are initially, located on the posterior abdominal wall on a level with the upper lumbar vertebrae (L2). Attached to, the inferior aspect of the testis is the gubernaculum testis which extends caudally to the inguinal, region, through the canal and down to the superficial skin. Both the testis and the gubernaculum are
Page 1115 :
extra-peritoneal., As the foetus grows the gubernaculum becomes progressively shorter. It carries the peritoneum of, the anterior abdominal wall (the processus vaginalis). As the processus vaginalis descends the testis, is guided by the gubernaculum down the posterior abdominal wall and the back of the processus, vaginalis into the scrotum., By the third month of foetal life the testes are located in the iliac fossae, by the seventh they lie at, the level of the deep inguinal ring., The processus vaginalis usually closes after birth, but may persist and be the site of indirect hernias., Part closure may result in development of cysts on the cord., Next question
Page 1116 :
Question 16 of 560, A 21 year old man undergoes surgical removal of an impacted 3rd molar. Post operatively, he is, noted to have anaesthesia on the anterolateral aspect of the tongue. What is the most likely, explanation?, , Injury to the hypoglossal nerve, , Injury to the inferior alveolar nerve, , Injury to the lingual nerve, , Injury to the mandibular branch of the facial nerve, , Injury to the glossopharyngeal nerve, , Theme from September 2014 exam, The lingual nerve is closely related to the third molar and up to 10% of patients undergoing surgical, extraction of these teeth may subsequently develop a lingual neuropraxia. The result is anaesthesia, of the ipsilateral anterior aspect of the tongue. The inferior alveolar nerve innervates the teeth, themselves., Please rate this question:, , Discuss and give feedback, , Next question, , Lingual nerve, , , , , Sensory nerve to the mucosa of the presulcal part of the tongue, floor of mouth and, mandibular lingual gingivae, Arises from posterior trunk of the mandibular nerve, Course runs past tensor veli palatini and lateral pterygoid (where it is joined by the chorda, tympani branch of the facial nerve). Emerging from the cover of the lateral pterygoid it, proceeds antero inferiorly lying on the surface of the medial pterygoid and lies close to the, medial aspect of the mandibular ramus. At the junction of the vertical and horizontal rami of, the mandible it is anterior to the inferior alveolar nerve. It then passes below the mandibular, attachment of the superior pharyngeal constrictor. Eventually, it lies on the periosteum of the, root of the third molar tooth. It then passes medial to the mandibular origin of mylohyoid and, then passes forwards on the inferior surface of this muscle, Next question
Page 1117 :
Question 17 of 560, , What is the most important structure involved in supporting the uterus?, , Round ligament, , Broad ligament, , Uterosacral ligaments, , Cardinal ligaments, , Central perineal tendon, , Theme from April 2016 Exam, The central perineal tendon provides the main structural support to the uterus. Damage to this, structure is commonly associated with the development of pelvic organ prolapse, even when other, structures are intact., Please rate this question:, , Discuss and give feedback, , Next question, , Uterus, The non pregnant uterus resides entirely within the pelvis. The peritoneum invests the uterus and, the structure is contained within the peritoneal cavity. The blood supply to the uterine body is via the, uterine artery (branch of the internal iliac). The uterine artery passes from the inferior aspect of the, uterus (lateral to the cervix) and runs alongside the uterus. It frequently anastomoses with the, ovarian artery superiorly. Inferolaterally the ureter is a close relation and ureteric injuries are a, recognised complication when pathology brings these structures into close proximity.
Page 1118 :
The supports of the uterus include the central perineal tendon (the most important). The lateral, cervical, round and uterosacral ligaments are condensations of the endopelvic fascia and provide, additional structural support., Topography of the uterus, , Image sourced from Wikipedia, , Next question
Page 1119 :
Question 18 of 560, A 34 year old lady suffers from hyperparathyroidism. The right inferior parathyroid is identified as, having an adenoma and is scheduled for resection. From which of the following embryological, structures is it derived?, , Second pharyngeal pouch, , Third pharyngeal pouch, , Fourth pharyngeal pouch, , First pharyngeal pouch, , None of the above, , The inferior parathyroid is a derivative of the third pharyngeal pouch. The superior parathyroid, originates from the fourth pharyngeal pouch., Please rate this question:, , Discuss and give feedback, , Next question, , Parathyroid glands- anatomy, , , , , Four parathyroid glands, Located posterior to the thyroid gland, They lie within the pretracheal fascia, , Embryology, The parathyroids develop from the extremities of the third and fourth pharyngeal pouches. The, parathyroids derived from the fourth pharyngeal pouch are located more superiorly and are, associated with the thyroid gland. Those derived from the third pharyngeal pouch lie more inferiorly, and may become associated with the thymus., Blood supply, The blood supply to the parathyroid glands is derived from the inferior and superior thyroid, arteries[1]. There is a rich anastomosis between the two vessels. Venous drainage is into the thyroid, veins.
Page 1120 :
Relations, , Laterally, , Common carotid, , Medially, , Recurrent laryngeal nerve, trachea, , Anterior, , Thyroid, , Posterior, , Pretracheal fascia, , References, 1.Nobori, M., et al., Blood supply of the parathyroid gland from the superior thyroid artery. Surgery,, 1994. 115(4): p. 417-23., Next question
Page 1121 :
Question 19 of 560, A 23 year old man falls and slips at a nightclub. A shard of glass penetrates the skin at the level of, the medial epicondyle, which of the following sequelae is least likely to occur?, , Atrophy of the first dorsal interosseous muscle, , Difficulty in abduction of the the 2nd, 3rd, 4th and 5th fingers, , Claw like appearance of the hand, , Loss of sensation on the anterior aspect of the 5th finger, , Partial denervation of flexor digitorum profundus, Injury to the ulnar nerve in the mid to distal forearm will typically produce a claw hand. This consists, of flexion of the 4th and 5th interphalangeal joints and extension of the metacarpophalangeal joints., The effects are potentiated when flexor digitorum profundus is not affected, and the clawing is more, pronounced.More proximally sited ulnar nerve lesions produce a milder clinical picture owing to the, simultaneous paralysis of flexor digitorum profundus (ulnar half)., This is the 'ulnar paradox', due to the more proximal level of transection the hand will typically not, have a claw like appearance that may be seen following a more distal injury. The first dorsal, interosseous muscle will be affected as it is supplied by the ulnar nerve., Please rate this question:, , Discuss and give feedback, , Next question, , Ulnar nerve, Origin, , , C8, T1, , Supplies (no muscles in the upper arm), , , Flexor carpi ulnaris
Page 1123 :
Branch, , Supplies, , Muscular branch, , Flexor carpi ulnaris, Medial half of the flexor digitorum profundus, , Palmar cutaneous branch (Arises near the, middle of the forearm), , Skin on the medial part of the palm, , Dorsal cutaneous branch, , Dorsal surface of the medial part of the hand, , Superficial branch, , Cutaneous fibres to the anterior surfaces of the, medial one and one-half digits, , Deep branch, , Hypothenar muscles, All the interosseous muscles, Third and fourth lumbricals, Adductor pollicis, Medial head of the flexor pollicis brevis, , Effects of injury, , Damage at the wrist, , , , , , Wasting and paralysis of intrinsic hand muscles (claw hand), Wasting and paralysis of hypothenar muscles, Loss of sensation medial 1 and half fingers, , Damage at the elbow, , , , , Radial deviation of the wrist, Clawing less in 4th and 5th digits, Next question
Page 1124 :
Question 20 of 560, A 56 year old man is undergoing a superficial parotidectomy for a pleomorphic adenoma. During the, dissection of the parotid, which of the following structures will be encountered lying most, superficially?, , Facial nerve, , External carotid artery, , Occipital artery, , Maxillary artery, , Retromandibular vein, Most superficial structure on the parotid gland = facial nerve, The facial nerve is the most superficial structure in the parotid gland. Slightly deeper to this lies the, retromandibular vein, with the arterial layer lying most deeply., Please rate this question:, , Discuss and give feedback, , Next question, , Parotid gland, Anatomy of the parotid gland, , Location, , Overlying the mandibular ramus; anterior and inferior to the ear., , Salivary duct, , Crosses the masseter, pierces the buccinator and drains adjacent to the, 2nd upper molar tooth (Stensen's duct)., , Structures passing, through the gland, , , , , , Facial nerve (Mnemonic: The Zebra Buggered My Cat; Temporal, Zygomatic, Buccal, Mandibular, Cervical), External carotid artery, Retromandibular vein
Page 1125 :
Relations, , , , Auriculotemporal nerve, , , , Anterior: masseter, medial pterygoid, superficial temporal and, maxillary artery, facial nerve, stylomandibular ligament, Posterior: posterior belly digastric muscle, sternocleidomastoid,, stylohyoid, internal carotid artery, mastoid process, styloid, process, , , , Arterial supply, , Branches of external carotid artery, , Venous drainage, , Retromandibular vein, , Lymphatic drainage, , Deep cervical nodes, , Nerve innervation, , , , , , Parasympathetic-Secretomotor, Sympathetic-Superior cervical ganglion, Sensory- Greater auricular nerve, , Parasympathetic stimulation produces a water rich, serous saliva. Sympathetic stimulation leads to, the production of a low volume, enzyme-rich saliva., Next question
Page 1126 :
Question 21 of 560, A 43 year old man is stabbed outside a nightclub. He suffers a transection of his median nerve just, as it leaves the brachial plexus. Which of the following features is least likely to ensue?, , Ulnar deviation of the wrist, , Complete loss of wrist flexion, , Loss of pronation, , Loss of flexion at the thumb joint, , Inability to oppose the thumb, , Loss of the median nerve will result in loss of function of the flexor muscles. However, flexor carpi, ulnaris will still function and produce ulnar deviation and some residual wrist flexion. High median, nerve lesions result in complete loss of flexion at the thumb joint., Please rate this question:, , Discuss and give feedback, , Next question, , Median nerve, The median nerve is formed by the union of a lateral and medial root respectively from the lateral, (C5,6,7) and medial (C8 and T1) cords of the brachial plexus; the medial root passes anterior to the, third part of the axillary artery. The nerve descends lateral to the brachial artery, crosses to its, medial side (usually passing anterior to the artery). It passes deep to the bicipital aponeurosis and, the median cubital vein at the elbow., It passes between the two heads of the pronator teres muscle, and runs on the deep surface of, flexor digitorum superficialis (within its fascial sheath)., Near the wrist it becomes superficial between the tendons of flexor digitorum superficialis and flexor, carpi radialis, deep to palmaris longus tendon. It passes deep to the flexor retinaculum to enter the, palm, but lies anterior to the long flexor tendons within the carpal tunnel., Branches, , Region, , Branch
Page 1128 :
, , , , unable to pronate forearm, weak wrist flexion, ulnar deviation of wrist, , Anterior interosseous nerve (branch of median nerve), , , , leaves just below the elbow, results in loss of pronation of forearm and weakness of long flexors of thumb and index, finger, , Topography of the median nerve, , Image sourced from Wikipedia, , Next question
Page 1129 :
Question 22 of 560, A 78 year old man is due to undergo an endarterectomy of the internal carotid artery. Which of the, following nervous structures are most at risk during the dissection?, , Recurrent laryngeal nerve, , Sympathetic chain, , Hypoglossal nerve, , Phrenic nerve, , Lingual nerve, Nerves at risk during a carotid endarterectomy:, , , , , Hypoglossal nerve, Greater auricular nerve, Superior laryngeal nerve, , Theme from May 2011 exam, Theme from January 2013 Exam, During a carotid endarterectomy the sternocleidomastoid muscle is dissected, with ligation of the, common facial vein and then the internal jugular is dissected exposing the common and the internal, carotid arteries. The nerves at risk during the operation include:, , , , , Hypoglossal nerve, Greater auricular nerve, Superior laryngeal nerve, , The sympathetic chain lies posteriorly and is less prone to injury in this procedure., Please rate this question:, , Discuss and give feedback, , Next question, , Internal carotid artery
Page 1130 :
The internal carotid artery is formed from the common carotid opposite the upper border of the, thyroid cartilage. It extends superiorly to enter the skull via the carotid canal. From the carotid canal, it then passes through the cavernous sinus, above which it divides into the anterior and middle, cerebral arteries., Relations in the neck, , Posterior, , , , , , , Longus capitis, Pre-vertebral fascia, Sympathetic chain, Superior laryngeal nerve, , Medially, , , , , , External carotid (near origin), Wall of pharynx, Ascending pharyngeal artery, , Laterally, , , , , Internal jugular vein (moves posteriorly at entrance to skull), Vagus nerve (most posterolaterally), , Anteriorly, , , , , , Sternocleidomastoid, Lingual and facial veins, Hypoglossal nerve, , Relations in the carotid canal, , , , , , Internal carotid plexus, Cochlea and middle ear cavity, Trigeminal ganglion (superiorly), Leaves canal lies above the foramen lacerum, , Path and relations in the cranial cavity, The artery bends sharply forwards in the cavernous sinus, the aducens nerve lies close to its, inferolateral aspect. The oculomotor, trochlear, opthalmic and, usually, the maxillary nerves lie in the, lateral wall of the sinus. Near the superior orbital fissure it turns posteriorly and passes posteromedially to pierce the roof of the cavernous sinus inferior to the optic nerve. It then passes between, the optic and oculomotor nerves to terminate below the anterior perforated substance by dividing, into the anterior and middle cerebral arteries., Branches, , , , , Anterior and middle cerebral artery, Ophthalmic artery, Posterior communicating artery
Page 1131 :
, , , , Anterior choroid artery, Meningeal arteries, Hypophyseal arteries, , Image demonstrating the internal carotid artery and its relationship to the external carotid artery, , Image sourced from Wikipedia, , Next question
Page 1132 :
Question 23 of 560, Which of the structures listed below articulates with the head of the radius superiorly?, , Capitulum, , Trochlea, , Lateral epicondyle, , Ulna, , Medial epicondyle, , Theme from September 2016 Exam, The head of the radius articulates with the capitulum of the humerus., Please rate this question:, , Discuss and give feedback, , Next question, , Radius, The radius is one of the two long forearm bones that extends from the lateral side of the elbow to the, thumb side of the wrist. It has two expanded ends, of which the distal end is the larger. Key points, relating to its topography and relations are outlined below;, Upper end, , , , , Articular cartilage- covers medial > lateral side, Articulates with radial notch of the ulna by the annular ligament, Muscle attachment- biceps brachii at the tuberosity, , Shaft, Muscle attachment, , Upper third of the body, , Supinator, Flexor digitorum superficialis
Page 1134 :
Question 24 of 560, Which of the following fascial structures encases the apex of the lungs?, , Waldeyers fascia, , Sibsons fascia, , Pretracheal fascia, , Clavipectoral fascia, , None of the above, Sibson's fascia overlies the apices of both lungs, The suprapleural fascia (Sibson's fascia) runs from C7 to the first rib and overlies the apex of both, lungs.It lies between the parietal pleura and the thoracic cage., Please rate this question:, , Discuss and give feedback, , Next question, , Lung anatomy, The right lung is composed of 3 lobes divided by the oblique and transverse fissures. The left lung, has two lobes divided by the oblique fissure.The apex of both lungs is approximately 4cm superior to, the sterno-costal joint of the first rib. Immediately below this is a sulcus created by the subclavian, artery., Peripheral contact points of the lung, , , , , Base: diaphragm, Costal surface: corresponds to the cavity of the chest, Mediastinal surface: Contacts the mediastinal pleura. Has the cardiac impression. Above and, behind this concavity is a triangular depression named the hilum, where the structures which, form the root of the lung enter and leave the viscus. These structures are invested by pleura,, which, below the hilum and behind the pericardial impression, forms the pulmonary ligament
Page 1135 :
Right lung, Above the hilum is the azygos vein; Superior to this is the groove for the superior vena cava and, right innominate vein; behind this, and nearer the apex, is a furrow for the innominate artery. Behind, the hilum and the attachment of the pulmonary ligament is a vertical groove for the oesophagus; In, front and to the right of the lower part of the oesophageal groove is a deep concavity for the, extrapericardiac portion of the inferior vena cava., The root of the right lung lies behind the superior vena cava and the right atrium, and below the, azygos vein., The right main bronchus is shorter, wider and more vertical than the left main bronchus and, therefore the route taken by most foreign bodies., , Image sourced from Wikipedia, , Left lung, Above the hilum is the furrow produced by the aortic arch, and then superiorly the groove, accommodating the left subclavian artery; Behind the hilum and pulmonary ligament is a vertical, groove produced by the descending aorta, and in front of this, near the base of the lung, is the lower, part of the oesophagus., The root of the left lung passes under the aortic arch and in front of the descending aorta.
Page 1136 :
Image sourced from Wikipedia, , Inferior borders of both lungs, , , , , 6th rib in mid clavicular line, 8th rib in mid axillary line, 10th rib posteriorly, , The pleura runs two ribs lower than the corresponding lung level., Bronchopulmonary segments, , Segment number, , Right lung, , Left lung, , 1, , Apical, , Apical, , 2, , Posterior, , Posterior, , 3, , Anterior, , Anterior, , 4, , Lateral, , Superior lingular, , 5, , Medial, , Inferior lingular, , 6, , Superior (apical), , Superior (apical)
Page 1137 :
Segment number, , Right lung, , Left lung, , 7, , Medial basal, , Medial basal, , 8, , Anterior basal, , Anterior basal, , 9, , Lateral basal, , Lateral basal, , 10, , Posterior basal, , Posterior basal, Next question
Page 1139 :
Discuss and give feedback, , Next question, , Femur, , , , , , , , , , , , , Extends from a rounded head, which articulates with the acetabulum down to the knee joint, where the two large condyles at it's inferior aspect articulate with the tibia., The superior aspect comprises a head and neck which pass inferolaterally to the body and, the two trochanters. These lie at the junction between the neck and the body., The neck meets the body of the femur at an angle of 125o., Developmentally, the neck is part of the body but is demarcated from it by a wide rough, intertrochanteric crest, this continues inferomedially as a spiral line that runs below the lesser, trochanter. Medially, the intertrochanteric line gives attachment to the inferior end of the, iliofemoral ligament. The neck is covered by synovial membrane up to the intertrochanteric, line. The posterior aspect of the neck is demarcated from the shaft by the intertrochanteric, crest and only it's medial aspect is covered by synovium and the joint capsule., The greater trochanter has discernible surfaces that form the site of attachment of the gluteal, muscles.Laterally, the greater trochanter overhangs the body and this forms part of the origin, of vastus lateralis, Viewed anteriorly, the body of the femur appears rounded. Viewed laterally, it has an anterior, concavity which gives fullness to the anterior thigh. Posteriorly, there is a ridge of bone, the, linea aspera. The surface of the anterior aspect of the body forms the origin of the vastus, intermedius. More medially, it forms the origin of vastus medialis., The upper and middle aspects of the linea aspera form part of the origin of the attachments, of the thigh adductors. Inferiorly, it spans out to form the bony floor of the popliteal fossa. At, the inferior aspect of the popliteal surface the surface curves posteriorly to form the femoral, condyles., The structures that are attached to the inferior aspect of the linea aspera split with it as it, approaches the popliteal fossa. Thus the vastus medialis and adductor magnus continue, with the medial split and the biceps femoris and vastus intermedius along the lateral split.
Page 1140 :
© Image provided by the University of Sheffield, , Image demonstrating anterior aspect of femur with muscular attachments, , © Image provided by the University of Sheffield, , Blood supply, The femur has a rich blood supply and numerous vascular foramina exist throughout it's length. The, blood supply to the femoral head is clinically important and is provided by the medial circumflex, femoral and lateral circumflex femoral arteries (Branches of profunda femoris). Also from the inferior, gluteal artery. These form an anastomosis and travel to up the femoral neck to supply the head., Next question
Page 1141 :
Question 26 of 560, , As regards the internal jugular vein, which of the following statements is untrue?, , It lies within the carotid sheath, , It is the continuation of the sigmoid sinus, , The terminal part of the thoracic duct crosses anterior to it to insert into the right subclavian, vein, , The hypoglossal nerve is closely related to it as it passes near the atlas, , The vagus nerve is closely related to it within the carotid sheath, , Theme from April 2013 Exam, Please rate this question:, , Discuss and give feedback, , Next question, , Internal jugular vein, Each jugular vein begins in the jugular foramen, where they are the continuation of the sigmoid, sinus. They terminate at the medial end of the clavicle where they unite with the subclavian vein., The vein lies within the carotid sheath throughout its course. Below the skull the internal carotid, artery and last four cranial nerves are anteromedial to the vein. Thereafter it is in contact medially, with the internal (then common) carotid artery. The vagus lies posteromedially., At its superior aspect, the vein is overlapped by sternocleidomastoid and covered by it at the inferior, aspect of the vein.
Page 1142 :
Below the transverse process of the atlas it is crossed on its lateral side by the accessory nerve. At, its mid point it is crossed by the inferior root of the ansa cervicalis., Posterior to the vein are the transverse processes of the cervical vertebrae, the phenic nerve as it, descends on the scalenus anterior, and the first part of the subclavian artery., On the left side its also related to the thoracic duct., , Image sourced from Wikipedia, , Next question
Page 1143 :
Question 27 of 560, , A 28 year old man requires a urethral catheter to be inserted prior to undergoing a splenectomy., Where is the first site of resistance to be encountered on inserting the catheter?, , Bulbar urethra, , Membranous urethra, , Internal sphincter, , Prostatic urethra, , Bladder neck, , Theme from January 2012 Exam, Theme from April 2014 Exam, The membranous urethra is the least distensible portion of the urethra. This is due to the fact that it, is surrounded by the external sphincter., Please rate this question:, , Discuss and give feedback, , Next question, , Urethral anatomy, Female urethra, The female urethra is shorter and more acutely angulated than the male urethra. It is an extraperitoneal structure and embedded in the endopelvic fascia. The neck of the bladder is subjected to, transmitted intra-abdominal pressure and therefore deficiency in this area may result in stress, urinary incontinence. Between the layers of the urogenital diaphragm the female urethra is, surrounded by the external urethral sphincter, this is innervated by the pudendal nerve. It ultimately
Page 1144 :
lies anterior to the vaginal orifice., Male urethra, In males the urethra is much longer and is divided into four parts., , Pre-prostatic, urethra, , Extremely short and lies between the bladder and prostate gland.It has a stellate lumen, and is between 1 and 1.5cm long.Innervated by sympathetic noradrenergic fibres, as, this region is composed of striated muscles bundles they may contract and prevent, retrograde ejaculation., , Prostatic, urethra, , This segment is wider than the membranous urethra and contains several openings for, the transmission of semen (at the midpoint of the urethral crest)., , Membranous, urethra, , Narrowest part of the urethra and surrounded by external sphincter. It traverses the, perineal membrane 2.5cm postero-inferior to the symphysis pubis., , Penile urethra, , Travels through the corpus spongiosum on the underside of the penis. It is the longest, urethral segment.It is dilated at its origin as the infrabulbar fossa and again in the gland, penis as the navicular fossa. The bulbo-urethral glands open into the spongiose section, of the urethra 2.5cm below the perineal membrane., , The urothelium is transitional in nature near to the bladder and becomes squamous more distally., Next question
Page 1145 :
Question 28 of 560, , Which of the following anatomical structures lies within the spiral groove of the humerus?, , Median nerve, , Radial nerve, , Tendon of triceps, , Musculocutaneous nerve, , Axillary nerve, , Theme from April 2014 Exam, The radial nerve lies in this groove and may be compromised by fractures involving the shaft., Please rate this question:, , Discuss and give feedback, , Next question, , Humerus, The humerus extends from the scapula to the elbow joint. It has a body and two ends. It is almost, completely covered with muscle but can usually be palpated throughout its length. The smooth, rounded surface of the head articulates with the shallow glenoid cavity. The head is connected to the, body of the humerus by the anatomical neck. The surgical neck is the region below the head and, tubercles and where they join the shaft and is the commonest site of fracture. The capsule of the, shoulder joint is attached to the anatomical neck superiorly but extends down to 1.5cm on the, surgical neck., The greater tubercle is the prominence on the lateral side of the upper end of the bone. It merges
Page 1146 :
with the body below and can be felt through the deltoid inferior to the acromion. The tendons of the, supraspinatus and infraspinatus are inserted into impressions on its superior aspect. The lesser, tubercle is a distinct prominence on the front of the upper end of the bone. It can be palpated, through the deltoid just lateral to the tip of the coracoid process., The intertubercular groove passes on the body between the greater and lesser tubercles, continuing, down from the anterior borders of the tubercles to form the edges of the groove. The tendon of, biceps within its synovial sheath passes through this groove, held within it by a transverse ligament., The posterior surface of the body is marked by a spiral groove for the radial nerve which runs, obliquely across the upper half of the body to reach the lateral border below the deltoid tuberosity., Within this groove lie the radial nerve and brachial vessels and both may be affected by fractures, involving the shaft of the humerus., The lower end of the humerus is wide and flattened anteroposteriorly, and inclined anteriorly. The, middle third of the distal edge forms the trochlea. Superior to this are indentations for the coronoid, fossa anteriorly and olecranon fossa posteriorly. Lateral to the trochlea is a rounded capitulum which, articulates with the radius., The medial epicondyle is very prominent with a smooth posterior surface which contains a sulcus for, the ulnar nerve and collateral vessels. It's distal margin gives attachment for the ulnar collateral, ligament and, in front of this, the anterior surface has an impression for the common flexor tendon., Next question
Page 1147 :
Question 29 of 560, , A 24 year old man falls and sustains a fracture through his scaphoid bone. From which of the, following areas does the scaphoid derive the majority of its blood supply?, , From its proximal medial border, , From its proximal lateral border, , From its proximal posterior surface, , From the proximal end, , From the distal end, , Theme from April 2012 Exam, Theme from April 2014 Exam, The blood supply to the scaphoid enters from a small non articular surface near its distal end., Transverse fractures through the scaphoid therefore carry a risk of non union., Please rate this question:, , Discuss and give feedback, , Next question, , Scaphoid bone, The scaphoid has a concave articular surface for the head of the capitate and at the edge of this is a, crescentic surface for the corresponding area on the lunate., Proximally, it has a wide convex articular surface with the radius. It has a distally sited tubercle that, can be palpated. The remaining articular surface is to the lateral side of the tubercle. It faces laterally, and is associated with the trapezium and trapezoid bones.
Page 1148 :
The narrow strip between the radial and trapezial surfaces and the tubercle gives rise to the radial, collateral carpal ligament. The tubercle receives part of the flexor retinaculum. This area is the only, part of the scaphoid that is available for the entry of blood vessels. It is commonly fractured and, avascular necrosis may result., Scaphoid bone, , Image sourced from Wikipedia, , Next question
Page 1149 :
Question 30 of 560, A 21 year old man has an inguinal hernia and is undergoing a surgical repair. As the surgeons, approach the inguinal canal they expose the superficial inguinal ring. Which of the following forms, the lateral edge of this structure?, , Inferior epigastric artery, , Conjoint tendon, , Rectus abdominis muscle, , External oblique aponeurosis, , Transversalis fascia, , The external oblique aponeurosis forms the anterior wall of the inguinal canal and also the lateral, edge of the superficial inguinal ring. The rectus abdominis lies posteromedially and the transversalis, posterior to this., Please rate this question:, , Discuss and give feedback, , Next question, , Inguinal canal, Location, , , , , , Above the inguinal ligament, The inguinal canal is 4cm long, The superficial ring is located anterior to the pubic tubercle, The deep ring is located approximately 1.5-2cm above the half way point between the, anterior superior iliac spine and the pubic tubercle, , Boundaries of the inguinal canal, , Floor, , , , , External oblique aponeurosis, Inguinal ligament
Page 1150 :
Roof, , Anterior wall, , , , Lacunar ligament, , , , , Internal oblique, Transversus abdominis, , External oblique aponeurosis, , Posterior wall, , , , , Transversalis fascia, Conjoint tendon, , Laterally, , , , , Internal ring, Fibres of internal oblique, , Medially, , , , , External ring, Conjoint tendon, , Contents, , Males, , Spermatic cord and ilioinguinal, nerve, , As it passes through the canal the spermatic cord, has 3 coverings:, , , , , Females, , External spermatic fascia from external, oblique aponeurosis, Cremasteric fascia, Internal spermatic fascia, , Round ligament of uterus and, ilioinguinal nerve, , Related anatomy of the inguinal region, The boundaries of Hesselbachs triangle are commonly tested and illustrated below:
Page 1151 :
Image sourced from Wikipedia, , The image below demonstrates the close relationship of the vessels to the lower limb with the, inguinal canal. A fact to be borne in mind when repairing hernial defects in this region., , Image sourced from Wikipedia, , Next question
Page 1152 :
Question 31 of 560, , Which of the following cranial venous sinuses is unpaired?, , Transverse sinus, , Superior sagittal sinus, , Cavernous sinus, , Sigmoid sinus, , Inferior petrosal sinus, The superior sagittal sinus is unpaired, , The superior sagittal sinus is unpaired. It begins at the crista galli, where it may communicate with, the veins of the frontal sinus and sometimes with those of the nasal cavity. It arches backwards in, the falx cerebri to terminate at the internal occipital protuberance (usually into the right transverse, sinus). The parietal emissary veins link the superior sagittal sinus with the veins on the exterior of, the cranium., Please rate this question:, , Discuss and give feedback, , Next question, , Cranial venous sinuses, The cranial venous sinuses are located within the dura mater. They have no valves which is, important in the potential for spreading sepsis. They eventually drain into the internal jugular vein., They are:
Page 1153 :
Superior sagittal sinus, Inferior sagittal sinus, Straight sinus, Transverse sinus, Sigmoid sinus, Confluence of sinuses, Occipital sinus, Cavernous sinus, Topography of cranial venous sinuses, , Image sourced from Wikipedia, , Next question
Page 1154 :
Question 32 of 560, Which of the following laryngeal tumours will not typically metastasise to the cervical lymph nodes?, , Glottic, , Supraglottic, , Subglottic, , Transglottic, , Aryepiglottic fold, , The vocal cords have no lymphatic drainage and therefore this region serves as a lymphatic, watershed. The supraglottic part drains to the upper deep cervical nodes through vessels piercing, the thyrohyoid membrane. The sub glottic part drains to the pre laryngeal, pre tracheal and inferior, deep cervical nodes. The aryepiglottic and vestibular folds have a rich lymphatic drainage and will, metastasise early., Please rate this question:, , Discuss and give feedback, , Next question, , Larynx, The larynx lies in the anterior part of the neck at the levels of C3 to C6 vertebral bodies. The, laryngeal skeleton consists of a number of cartilagenous segments. Three of these are paired;, arytenoid, corniculate and cuneiform. Three are single; thyroid, cricoid and epiglottic. The cricoid, cartilage forms a complete ring (the only one to do so)., The laryngeal cavity extends from the laryngeal inlet to the level of the inferior border of the cricoid, cartilage., Divisions of the laryngeal cavity, , Laryngeal vestibule, , Superior to the vestibular folds, , Laryngeal ventricle, , Lies between vestibular folds and superior to the vocal cords
Page 1155 :
Extends from vocal cords to inferior border of the cricoid cartilage, , Infraglottic cavity, , The vocal folds (true vocal cords) control sound production. The apex of each fold projects medially, into the laryngeal cavity. Each vocal fold includes:, , , , Vocal ligament, Vocalis muscle (most medial part of thyroarytenoid muscle), , The glottis is composed of the vocal folds, processes and rima glottidis. The rima glottidis is the, narrowest potential site within the larynx, as the vocal cords may be completely opposed, forming a, complete barrier., Muscles of the larynx, , Muscle, , Origin, , Insertion, , Innervation, , Action, , Posterior, cricoarytenoid, , Posterior aspect, of lamina of, cricoid, , Muscular process, of arytenoid, , Recurrent, Laryngeal, , Abducts vocal fold, , Lateral, cricoarytenoid, , Arch of cricoid, , Muscular process, of arytenoid, , Recurrent, laryngeal, , Adducts vocal fold, , Thyroarytenoid, , Posterior aspect, of thyroid, cartilage, , Muscular process, of arytenoid, , Recurrent, laryngeal, , Relaxes vocal fold, , Transverse and, oblique, arytenoids, , Arytenoid, cartilage, , Contralateral, arytenoid, , Recurrent, laryngeal, , Closure of, intercartilagenous, part of the rima, glottidis, , Vocalis, , Depression, between lamina, of thyroid, cartilage, , Vocal ligament, and vocal process, of arytenoid, cartilage, , Recurrent, laryngeal, , Relaxes posterior, vocal ligament, tenses, anterior part, , Cricothyroid, , Anterolateral, , Inferior margin, and horn of, , External, , Tenses vocal fold
Page 1156 :
Muscle, , Origin, , Insertion, , Innervation, , part of cricoid, , thyroid cartilage, , laryngeal, , Action, , Blood supply, Arterial supply is via the laryngeal arteries, branches of the superior and inferior thyroid arteries. The, superior laryngeal artery is closely related to the internal laryngeal nerve. The inferior laryngeal, artery is related to the inferior laryngeal nerve. Venous drainage is via superior and inferior laryngeal, veins, the former draining into the superior thyroid vein and the latter draining into the middle thyroid, vein, or thyroid venous plexus., Lymphatic drainage, The vocal cords have no lymphatic drainage and this site acts as a lymphatic watershed., , Supraglottic part, , Upper deep cervical nodes, , Subglottic part, , Prelaryngeal and pretracheal nodes and inferior deep cervical nodes, , The aryepiglottic fold and vestibular folds have a dense plexus of lymphatics associated with them, and malignancies at these sites have a greater propensity for nodal metastasis., , Topography of the larynx, , Image sourced from Wikipedia
Page 1157 :
Question 33 of 560, Which of the following forms the medial wall of the femoral canal?, , Pectineal ligament, , Adductor longus, , Sartorius, , Lacunar ligament, , Inguinal ligament, The femoral canal and the femoral triangle are distinct anatomical structures. Do not confuse them,, especially in the time pressured exam situation., Theme from September 2011 exam, Theme from September 2012 exam, Theme from April 2014 exam, Please rate this question:, , Discuss and give feedback, , Next question, , Femoral canal, The femoral canal lies at the medial aspect of the femoral sheath. The femoral sheath is a fascial, tunnel containing both the femoral artery laterally and femoral vein medially. The canal lies medial to, the vein., Borders of the femoral canal, , Laterally, , Femoral vein, , Medially, , Lacunar ligament
Page 1158 :
Anteriorly, , Inguinal ligament, , Posteriorly, , Pectineal ligament, , Image showing dissection of femoral canal, , Image sourced from Wikipedia, , Contents, , , , Lymphatic vessels, Cloquet's lymph node, , Physiological significance, Allows the femoral vein to expand to allow for increased venous return to the lower limbs.
Page 1159 :
Pathological significance, As a potential space, it is the site of femoral hernias. The relatively tight neck places these at high, risk of strangulation., Next question
Page 1160 :
Question 34 of 560, A 67 year old man is undergoing a transurethral resection of a bladder tumour using diathermy., Suddenly during the procedure the patient's thigh begins to twitch. Stimulation of which of the, following nerves is the most likely cause?, , Femoral, , Pudendal, , Sciatic, , Obturator, , Gluteal, , Theme from January 2011 Exam, Theme from January 2013 Exam, The obturator nerve is most closely related to the bladder (see below)
Page 1161 :
Image sourced from Wikipedia, , Please rate this question:, , Discuss and give feedback, , Next question, , Obturator nerve, The obturator nerve arises from L2, L3 and L4 by branches from the ventral divisions of each of, these nerve roots. L3 forms the main contribution and the second lumbar branch is occasionally, absent. These branches unite in the substance of psoas major, descending vertically in its posterior, part to emerge from its medial border at the lateral margin of the sacrum. It then crosses the, sacroiliac joint to enter the lesser pelvis, it descends on obturator internus to enter the obturator, groove. In the lesser pelvis the nerve lies lateral to the internal iliac vessels and ureter, and is joined, by the obturator vessels lateral to the ovary or ductus deferens., Supplies, , , , , Medial compartment of thigh, Muscles supplied: external obturator, adductor longus, adductor brevis, adductor magnus, (not the lower part-sciatic nerve), gracilis, The cutaneous branch is often absent. When present, it passes between gracilis and, adductor longus near the middle part of the thigh, and supplies the skin and fascia of the, distal two thirds of the medial aspect.
Page 1162 :
Obturator canal, , , Connects the pelvis and thigh: contains the obturator artery, vein, nerve which divides into, anterior and posterior branches., , Cadaveric cross section demonstrating relationships of the obturator nerve, , Image sourced from Wikipedia, , Next question
Page 1163 :
Question 35 of 560, A 5 year old boy is playing with some small ball bearings. Unfortunately he inhales one. To which of, the following lung regions is the ball most likely to settle?, , Right lower lobe, , Left main bronchus, , Right upper lobe, , Left lower lobe, , None of the above, , Theme from September 2011 Exam, Theme from January 2013 Exam, As the most dependent part of the right lung a small object is most likely to lodge here. Most objects, will preferentially enter the right lung owing to the angle the right main bronchus takes from the, trachea., Please rate this question:, , Discuss and give feedback, , Next question, , Lung anatomy, The right lung is composed of 3 lobes divided by the oblique and transverse fissures. The left lung, has two lobes divided by the oblique fissure.The apex of both lungs is approximately 4cm superior to, the sterno-costal joint of the first rib. Immediately below this is a sulcus created by the subclavian, artery., Peripheral contact points of the lung, , , , , Base: diaphragm, Costal surface: corresponds to the cavity of the chest, Mediastinal surface: Contacts the mediastinal pleura. Has the cardiac impression. Above and, behind this concavity is a triangular depression named the hilum, where the structures which, form the root of the lung enter and leave the viscus. These structures are invested by pleura,, which, below the hilum and behind the pericardial impression, forms the pulmonary ligament
Page 1164 :
Right lung, Above the hilum is the azygos vein; Superior to this is the groove for the superior vena cava and, right innominate vein; behind this, and nearer the apex, is a furrow for the innominate artery. Behind, the hilum and the attachment of the pulmonary ligament is a vertical groove for the oesophagus; In, front and to the right of the lower part of the oesophageal groove is a deep concavity for the, extrapericardiac portion of the inferior vena cava., The root of the right lung lies behind the superior vena cava and the right atrium, and below the, azygos vein., The right main bronchus is shorter, wider and more vertical than the left main bronchus and, therefore the route taken by most foreign bodies., , Image sourced from Wikipedia, , Left lung, Above the hilum is the furrow produced by the aortic arch, and then superiorly the groove, accommodating the left subclavian artery; Behind the hilum and pulmonary ligament is a vertical, groove produced by the descending aorta, and in front of this, near the base of the lung, is the lower, part of the oesophagus., The root of the left lung passes under the aortic arch and in front of the descending aorta.
Page 1165 :
Image sourced from Wikipedia, , Inferior borders of both lungs, , , , , 6th rib in mid clavicular line, 8th rib in mid axillary line, 10th rib posteriorly, , The pleura runs two ribs lower than the corresponding lung level., Bronchopulmonary segments, , Segment number, , Right lung, , Left lung, , 1, , Apical, , Apical, , 2, , Posterior, , Posterior, , 3, , Anterior, , Anterior, , 4, , Lateral, , Superior lingular, , 5, , Medial, , Inferior lingular, , 6, , Superior (apical), , Superior (apical)
Page 1166 :
Segment number, , Right lung, , Left lung, , 7, , Medial basal, , Medial basal, , 8, , Anterior basal, , Anterior basal, , 9, , Lateral basal, , Lateral basal, , 10, , Posterior basal, , Posterior basal, Next question
Page 1167 :
Question 36 of 560, A patient presents with superior vena caval obstruction. How many collateral circulations exist as, alternative pathways of venous return?, , None, , One, , Two, , Three, , Four, , There are 4 collateral venous systems:, , , , , Azygos venous system, Internal mammary venous pathway, Long thoracic venous system with connections to the femoral and vertebral veins (2, pathways), , Despite this, venous hypertension still occurs., Please rate this question:, , Discuss and give feedback, , Next question, , Superior vena cava, Drainage, , , , , , Head and neck, Upper limbs, Thorax, Part of abdominal walls
Page 1168 :
Formation, , , , , Subclavian and internal jugular veins unite to form the right and left brachiocephalic veins, These unite to form the SVC, Azygos vein joins the SVC before it enters the right atrium, , Relations, , Anterior, , Anterior margins of the right lung and pleura, , Posteromedial, , Trachea and right vagus nerve, , Posterolateral, , Posterior aspects of right lung and pleura, Pulmonary hilum is posterior, , Right lateral, , Right phrenic nerve and pleura, , Left lateral, , Brachiocephalic artery and ascending aorta, , Developmental variations, Anomalies of the connection of the SVC are recognised. In some individuals a persistent left sided, SVC drains into the right atrium via an enlarged orifice of the coronary sinus. More rarely the left, sided vena cava may connect directly with the superior aspect of the left atrium, usually associated, with an un-roofing of the coronary sinus. The commonest lesion of the IVC is for its abdominal, course to be interrupted, with drainage achieved via the azygos venous system. This may occur in, patients with left sided atrial isomerism., Next question
Page 1169 :
Question 37 of 560, , An 18 year old man is cutting some plants when a small piece of vegetable matter enters his eye., His eye becomes watery. Which of the following is responsible for relaying parasympathetic, neuronal signals to the lacrimal apparatus?, , Pterygopalatine ganglion, , Otic ganglion, , Submandibular ganglion, , Ciliary ganglion, , None of the above, , Theme from January 2013 Exam, The parasympathetic fibres to the lacrimal apparatus transit via the pterygopalatine ganglion., Please rate this question:, , Discuss and give feedback, , Next question, , Lacrimal system, Lacrimal gland, Consists of an orbital part and palpebral part. They are continuous posterolaterally around the, concave lateral edge of the levator palpebrae superioris muscle., The ducts of the lacrimal gland open into the superior fornix. Those from the orbital part penetrate, the aponeurosis of levator palpebrae superioris to join those from the palpebral part. Therefore, excision of the palpebral part is functionally similar to excision of the entire gland.
Page 1170 :
Blood supply, Lacrimal branch of the opthalmic artery. Venous drainage is to the superior opthalmic vein., Innervation, The gland is innervated by the secretomotor parasympathetic fibres from the pterygopalatine, ganglion which in turn may reach the gland via the zygomatic or lacrimal branches of the maxillary, nerve or pass directly to the gland. The preganglionic fibres travel to the ganglion in the greater, petrosal nerve (a branch of the facial nerve at the geniculate ganglion)., Nasolacrimal duct, Descends from the lacrimal sac to open anteriorly in the inferior meatus of the nose., Lacrimation reflex, Occurs in response to conjunctival irritation (or emotional events). The conjunctiva will send signals, via the opthalmic nerve. These then pass to the superior salivary centre. The efferent signals pass, via the greater petrosal nerve (parasympathetic preganglionic fibres) and the deep petrosal nerve, which carries the post ganglionic sympathetic fibres. The parasympathetic fibres will relay in the, pterygopalatine ganglion, the sympathetic fibres do not synapse. They in turn will relay to the, lacrimal apparatus., Next question
Page 1171 :
Question 38 of 560, , Which of the nerves listed below is directly responsible for the innervation of the lateral aspect of, flexor digitorum profundus?, , Ulnar nerve, , Anterior interosseous nerve, , Radial nerve, , Median nerve, , Posterior interosseous nerve, , The anterior interosseous nerve is a branch of the median nerve and is responsible for innervation of, the lateral aspect of the flexor digitorum profundus., Please rate this question:, , Discuss and give feedback, , Next question, , Forearm flexor muscles, Muscle, , Origin, , Insertion, , Nerve supply, , Action, , Flexor carpi, radialis, , Common flexor, origin and, surrounding, , Front of bases of second, and third metacarpals, , Median, , Flexes and abducts the, carpus, part flexes the, elbow and part
Page 1172 :
Muscle, , Origin, , Insertion, , Nerve supply, , fascia, , Action, , pronates forearm, , Palmaris, longus, , Common flexor, origin, , Apex of palmar, aponeurosis, , Median, , Wrist flexor, , Flexor carpi, ulnaris, , Small humeral, head arises from, the common, flexor origin and, adjacent fascia., Ulnar head, comes from, medial border of, olecranon and, posterior border, of ulna, , Pisiform and base of the, fifth metacarpal, , Ulnar nerve, , Flexes and adducts the, carpus, , Flexor, digitorum, superficialis, , Long linear origin, from common, flexor tendon,, adjacent fascia, and septa and, medial border of, the coronoid, process, , Via tendons in the fibrous, flexor sheath. At the level, of the, metacarpophalangeal, joint each tendon split, into two, these bands, pass distally to their, insertions, , Median, , Flexor of, metacarpophalangeal, joint and proximal, interphalangeal joint, , Flexor, digitorum, profundus, , Upper two thirds, of the medial and, anterior surface, of the ulna,, medial side of the, olecranon,, medial half of the, interosseous, , Via tendons that lie deep, to those of flexor, digitorum superficialis to, insert into the distal, phalanx, , Medial part=, ulnar, lateral, part=anterior, interosseous, nerve, , Flexes the distal, interphalangeal joints, and the wrist
Page 1173 :
Muscle, , Origin, , Insertion, , Nerve supply, , Action, , membrane, Next question
Page 1174 :
Question 39 of 560, A 45 year old lady is undergoing a Whipples procedure for carcinoma of the pancreatic head. The, bile duct is transected. Which of the following vessels is mainly responsible for the blood supply to, the bile duct?, , Cystic artery, , Hepatic artery, , Portal vein, , Left gastric artery, , None of the above, Do not confuse the blood supply of the bile duct with that of the cystic duct., Theme from April 2014 exam, The bile duct has an axial blood supply which is derived from the hepatic artery and from, retroduodenal branches of the gastroduodenal artery. Unlike the liver there is no contribution by the, portal vein to the blood supply of the bile duct. Damage to the hepatic artery during a difficult, cholecystectomy is a recognised cause of bile duct strictures., Please rate this question:, , Discuss and give feedback, , Next question, , Gallbladder, , , , Fibromuscular sac with capacity of 50ml, Columnar epithelium, , Relations of the gallbladder, , Anterior, , Liver
Page 1175 :
, , , , Posterior, , Covered by peritoneum, Transverse colon, 1st part of the duodenum, , Laterally, , Right lobe of liver, , Medially, , Quadrate lobe of liver, , Arterial supply, Cystic artery (branch of Right hepatic artery), Venous drainage, Directly to the liver, Nerve supply, Sympathetic- mid thoracic spinal cord, Parasympathetic- anterior vagal trunk, Common bile duct, , Origin, , Confluence of cystic and common hepatic ducts, , Relations at, origin, , , , , Medially - Hepatic artery, Posteriorly- Portal vein, , Relations distally, , , , , , Duodenum - anteriorly, Pancreas - medially and laterally, Right renal vein - posteriorly, , Arterial supply, , Branches of hepatic artery and retroduodenal branches of gastroduodenal, artery, , Hepatobiliary triangle, , Medially, , Common hepatic duct, , Inferiorly, , Cystic duct, , Superiorly, , Inferior edge of liver
Page 1176 :
Cystic artery, , Contents, , Relations of the gallbladder, , © Image provided by the University of Sheffield, , Next question
Page 1177 :
Question 40 of 560, A 43 year old lady is undergoing a total thyroidectomy for an extremely large goitre. The surgeons, decide that access may be improved by division of the infra hyoid strap muscles. At which of the, following sites should they be divided?, , In their upper half, , In their lower half, , In the middle, , At their origin from the hyoid, , At the point of their insertion, , Theme from 2009 Exam, Should the strap muscles require division during surgery they should be divided in their upper half., This is because their nerve supply from the ansa cervicalis enters in their lower half., Please rate this question:, , Discuss and give feedback, , Next question, , Anterior triangle of the neck, Boundaries, , Anterior border of the Sternocleidomastoid, Lower border of mandible, Anterior midline, , Sub triangles (divided by Digastric above and Omohyoid), , , , Muscular triangle: Neck strap muscles, Carotid triangle: Carotid sheath
Page 1178 :
, , Submandibular Triangle (digastric), , Contents of the anterior triangle, , Digastric triangle, , Submandibular gland, Submandibular nodes, Facial vessels, Hypoglossal nerve, , Muscular triangle, , Strap muscles, External jugular vein, , Carotid triangle, , Carotid sheath (Common carotid, vagus and internal jugular vein), Ansa cervicalis, , Nerve supply to digastric muscle, , , , Anterior: Mylohyoid nerve, Posterior: Facial nerve, , Image sourced from Wikipedia, , Next question
Page 1179 :
Question 41 of 560, A 7 year old boy presents with right iliac fossa pain and there is a clinical suspicion that appendicitis, is present. From which of the following embryological structures is the appendix derived?, , Vitello-intestinal duct, , Uranchus, , Foregut, , Hindgut, , Midgut, The appendix is derived from the midgut, Theme from April 2014 exam, It is derived from the midgut which is why early appendicitis may present with periumbilical pain., Please rate this question:, , Discuss and give feedback, , Next question, , Appendix, , , , , , , , Location: Base of caecum., Up to 10cm long., Mainly lymphoid tissue (Hence mesenteric adenitis may mimic appendicitis)., Caecal taenia coli converge at base of appendix and form a longitudinal muscle cover over, the appendix. This convergence should facilitate its identification at surgery if it is retrocaecal, and difficult to find (which it can be when people start doing appendicectomies!), Arterial supply: Appendicular artery (branch of the ileocolic)., It is intra peritoneal., , McBurney's point, , , 1/3 of the way along a line drawn from the Anterior Superior Iliac Spine to the Umbilicus
Page 1181 :
Question 42 of 560, A 22 year old women has recently undergone a surgical excision of the submandibular gland. She, presents to the follow up clinic with a complaint of tongue weakness on the ipsilateral side to her, surgery. Which nerve has been damaged?, , Hypoglossal nerve, , Lingual nerve, , Inferior alveolar nerve, , Facial nerve, , Lesser petrosal nerve, Three cranial nerves may be injured during submandibular gland excision., , , , , Marginal mandibular branch of the facial nerve, Lingual nerve, Hypoglossal nerve, , Theme from April 2012 Exam, Hypoglossal nerve damage may result in paralysis of the ipsilateral aspect of the tongue. The nerve, itself lies deep to the capsule surrounding the gland and should not be injured during an, intracapsular dissection. The lingual nerve is probably at greater risk of injury. However, the effects, of lingual nerve injury are sensory rather than motor.
Page 1182 :
Image sourced from Wikipedia, , Please rate this question:, , Discuss and give feedback, , Next question, , Submandibular gland, Relations of the submandibular gland, , Superficial, , Platysma, deep fascia and mandible, Submandibular lymph nodes, Facial vein (facial artery near mandible), Marginal mandibular nerve, Cervical branch of the facial nerve, , Deep, , Facial artery (inferior to the mandible), Mylohoid muscle, Sub mandibular duct, Hyoglossus muscle, Lingual nerve, Submandibular ganglion, Hypoglossal nerve, , Submandibular duct (Wharton's duct)
Page 1183 :
, , , , Opens lateral to the lingual frenulum on the anterior floor of mouth., 5 cm length, Lingual nerve wraps around Wharton's duct. As the duct passes forwards it crosses medial, to the nerve to lie above it and then crosses back, lateral to it, to reach a position below the, nerve., , Innervation, , , , Sympathetic innervation- Derived from superior cervical ganglion, Parasympathetic innervation- Submandibular ganglion via lingual nerve, , Arterial supply, Branch of the facial artery. The facial artery passes through the gland to groove its deep surface. It, then emerges onto the face by passing between the gland and the mandible., Venous drainage, Anterior facial vein (lies deep to the Marginal Mandibular nerve), Lymphatic drainage, Deep cervical and jugular chains of nodes, Next question
Page 1184 :
Question 43 of 560, You decide to take an arterial blood gas from the femoral artery. Where should the needle be, inserted to gain the sample?, , Mid point of the inguinal ligament, , Mid inguinal point, , 2cm inferomedially to the pubic tubercle, , 2cm superomedially to the pubic tubercle, , 3cm inferolaterally to the deep inguinal ring, The mid inguinal point is midway between the anterior superior iliac spine and the symphysis pubis, Theme from April 2015 Exam, The mid inguinal point in the surface marking for the femoral artery., Please rate this question:, , Discuss and give feedback, , Next question, , Femoral triangle anatomy, Boundaries, , Superiorly, , Inguinal ligament, , Laterally, , Sartorius, , Medially, , Adductor longus, , Floor, , Iliopsoas, adductor longus and pectineus
Page 1185 :
, , , , Roof, , Fascia lata and Superficial fascia, Superficial inguinal lymph nodes (palpable below the inguinal ligament), Long saphenous vein, , Image sourced from Wikipedia, , Contents, , , , , , , , , Femoral vein (medial to lateral), Femoral artery-pulse palpated at the mid inguinal point, Femoral nerve, Deep and superficial inguinal lymph nodes, Lateral cutaneous nerve, Great saphenous vein, Femoral branch of the genitofemoral nerve, Next question
Page 1186 :
Question 44 of 560, , A 67 year old man undergoes a carotid endarterectomy and seems to recover well following surgery., When he is reviewed on the ward post operatively he complains that his voice is hoarse. What is the, most likely cause?, , Damage to the accessory nerve, , Damage to the cervical plexus, , Damage to the glossopharyngeal nerve, , Damage to the hypoglossal nerve, , Damage to the vagus, , Theme from April 2013 Exam, Many of these nerves are at risk of injury during carotid surgery. However, only damage to the vagus, would account for difficulties in speech., Please rate this question:, , Discuss and give feedback, , Next question, , Vagus nerve, The vagus nerve has mixed functions and supplies the structures from the fourth and sixth, pharyngeal arches. It also supplies the fore and midgut sections of the embryonic gut tube. It carries, afferent fibres from these areas (viz; pharynx, larynx, oesophagus, stomach, lungs, heart and great, vessels). The efferent fibres of the vagus are of two main types. The first are preganglionic, parasympathetic fibres distributed to the parasympathetic ganglia that innervate smooth muscle of, the innervated organs (such as gut). The second type of efferent fibres have direct skeletal muscle
Page 1187 :
innervation, these are largely to the muscles of the larynx and pharynx., Origin and course, The vagus arises from the lateral surface of the medulla oblongata by a series of rootlets. It is, related to the glossopharyngeal nerve cranially and the accessory nerve caudally. It exits through, the jugular foramen and is contained within its own dural sheath alongside the accessory nerve. In, the neck it descends vertically in the carotid sheath where it is closely related to the internal and, common carotid arteries. It leaves the neck and enters the mediastinum. On the right it passes, anterior to the first part of the subclavian artery, on the left it lies in the interval between the common, carotid and subclavian arteries., In the mediastinum both nerves pass postero-inferiorly and reach the posterior surface of the, corresponding lung root. These then branch into both lungs. At the inferior end of the mediastinum, these plexuses reunite to form the formal vagal trunks that pass through the oesophageal hiatus and, into the abdomen. The anterior and posterior vagal trunks are formal nerve fibres these then splay, out once again sending fibres over the stomach and posteriorly to the coeliac plexus. Branches pass, to the liver, spleen and kidney., Communications and branches, , Communication, , Details, , Superior, ganglion, , Located in jugular foramen, Communicates with the superior cervical sympathetic ganglion, accessory nerve, Two branches; meningeal and auricular (the latter may give rise to vagal stimulation, following instrumentation of the external auditory meatus), , Inferior ganglion, , Communicates with the superior cervical sympathetic ganglion, hypoglossal nerve and, loop between first and second cervical ventral rami, Two branches; pharyngeal (supplies pharyngeal muscles) and superior laryngeal nerve, (inferomedially- deep to both carotid arteries), , Branches in the neck, , Branch, , Detail, , Superior and inferior, cervical cardiac, branches, , Arise at various points and descend into thorax, On the right these pass posterior to the subclavian artery, On the left the superior branch passes between the arch of the aorta and the, trachea to connect with the deep cardiac plexus. The inferior branch descends
Page 1188 :
Branch, , Detail, , with the vagus itself., , Right recurrent, laryngeal nerve, , Arises from vagus anterior to the first part of the subclavian artery, hooks under, it, and ascends superomedially. It passes close to the common carotid and finally, the inferior thyroid artery to insert into the larynx, , Branches in the thorax, , Branch, , Details, , Left recurrent, laryngeal, nerve, , Arises from the vagus on the aortic arch. It hooks around the inferior surface of the arch,, posterior to the ligamentum arteriosum and passes upwards through the superior, mediastinum and lower part of the neck. It lies in the groove between oesophagus and, trachea (supplies both). It passes with the inferior thyroid artery and inserts into the, larynx., , Thoracic and, cardiac, branches, , There are extensive branches to both the heart and lung roots. These pass throughout, both these viscera. The fibres reunite distally prior to passing into the abdomen., , Abdominal branches, After entry into the abdominal cavity the nerves branch extensively. In previous years the extensive, network of the distal branches (nerves of Laterjet) over the surface of the distal stomach were, important for the operation of highly selective vagotomy. The use of modern PPI's has reduced the, need for such highly selective procedures. Branches pass to the coeliac axis and alongside the, vessels to supply the spleen, liver and kidney., Next question
Page 1189 :
Question 45 of 560, A 25 year old man has an inguinal hernia, which of the following structures must be divided (at open, surgery) to gain access to the inguinal canal?, , Transversalis fascia, , External oblique aponeurosis, , Conjoint tendon, , Rectus abdominis, , Inferior epigastric artery, , Theme from January 2013 Exam, This question is asking what structure forms the anterior wall of the inguinal canal. The anterior wall, is formed by the external oblique aponeurosis. Once this is divided the canal is entered, the cord can, be mobilised and a hernia repair performed. The transversalis fascia and conjoint tendons form the, posterior wall and would not routinely be divided to gain access to the inguinal canal itself., Please rate this question:, , Discuss and give feedback, , Next question, , External oblique muscle, External oblique forms the outermost muscle of the three muscles comprising the anterolateral, aspect of the abdominal wall. Its aponeurosis comprises the anterior wall of the inguinal canal., , Origin, , Insertion, , Nerve, , Outer surfaces of the lowest eight ribs, , , , Anterior two thirds of the outer lip of the iliac crest., The remainder becomes the aponeurosis that fuses with the linea alba in the, midline., , Ventral rami of the lower six thoracic nerves
Page 1190 :
supply, Actions, , Contains the abdominal viscera, may contract to raise intra abdominal pressure., Moves trunk to one side., Next question
Page 1191 :
Question 46 of 560, Which muscle initiates abduction of the shoulder?, , Infraspinatus, , Latissimus dorsi, , Supraspinatus, , Deltoid, , Teres major, , Theme from September 2012 exam, Theme from April 2014 Exam, The intermediate portion of the deltoid muscle is the chief abductor of the humerus. However, it can, only do this after the movement has been initiated by supraspinatus. Damage to the tendon of, supraspinatus is a common form of rotator cuff disease., Please rate this question:, , Discuss and give feedback, , Next question, , Shoulder joint, , , , , Shallow synovial ball and socket type of joint., It is an inherently unstable joint, but is capable to a wide range of movement., Stability is provided by muscles of the rotator cuff that pass from the scapula to insert in the, greater tuberosity (all except sub scapularis-lesser tuberosity)., , Glenoid labrum, , , , , Fibrocartilaginous rim attached to the free edge of the glenoid cavity, Tendon of the long head of biceps arises from within the joint from the supraglenoid tubercle,, and is fused at this point to the labrum., The long head of triceps attaches to the infraglenoid tubercle
Page 1194 :
Question 47 of 560, A 34 year old man is shot in the postero- inferior aspect of his thigh. Which of the following lies at the, most lateral aspect of the popliteal fossa?, , Popliteal artery, , Popliteal vein, , Common peroneal nerve, , Tibial nerve, , Small saphenous vein, , Theme from April 2012 exam, Theme from April 2014 exam, The contents of the popliteal fossa are (from medial to lateral):, Popliteal artery, Popliteal vein, Tibial nerve, Common peroneal nerve, The sural nerve is a branch of the tibial nerve and usually arises at the inferior aspect of the popliteal, fossa. However, its anatomy is variable., Please rate this question:, , Discuss and give feedback, , Next question, , Popliteal fossa, Boundaries of the popliteal fossa, , Laterally, , Biceps femoris above, lateral head of gastrocnemius and plantaris below, , Medially, , Semimembranosus and semitendinosus above, medial head of gastrocnemius below
Page 1195 :
Floor, , Popliteal surface of the femur, posterior ligament of knee joint and popliteus muscle, , Roof, , Superficial and deep fascia, , Image showing the popliteal fossa, , © Image provided by the University of Sheffield, , Contents, , , , , , , , , Popliteal artery and vein, Small saphenous vein, Common peroneal nerve, Tibial nerve, Posterior cutaneous nerve of the thigh, Genicular branch of the obturator nerve, Lymph nodes, Next question
Page 1196 :
Question 48 of 560, , A 67 year old man has an abdominal aortic aneurysm which displaces the left renal vein. Which, branch of the aorta is most likely to affected at this level?, , Inferior mesenteric artery, , Superior mesenteric artery, , Coeliac axis, , Testicular artery, , None of the above, , Theme from April 2013 exam, Theme from April 2014 exam, The left renal vein lies behind of the SMA as it branches off the aorta. Whilst juxtarenal AAA may, sometimes require the division of the left renal vein, direct involvement of the SMA may require a, hybrid surgical bypass and subsequent endovascular occlusion., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal aortic branches, Branches, , Level, , Paired, , Type
Page 1198 :
Question 49 of 560, A 12 year old boy undergoes surgery for recurrent mastoid infections. Post operatively he complains, of an altered taste sensation. Which of the following nerves has been injured?, , Glossopharyngeal, , Greater petrosal, , Olfactory, , Trigeminal, , Chorda tympani, , Theme from April 2012 exam, Theme from April 2014 exam, The chorda tympani branch of the facial nerve passes forwards through itrs canaliculus into the, middle ear, and crosses the medial aspect of the tympanic membrane. It then passes anteroinferiorly in the infratemporal fossa. It distributes taste fibres to the anterior two thirds of the tongue.
Page 1199 :
Image sourced from Wikipedia, , Please rate this question:, , Discuss and give feedback, , Next question, , Facial nerve, The facial nerve is the main nerve supplying the structures of the second embryonic branchial arch., It is predominantly an efferent nerve to the muscles of facial expression, digastric muscle and also to, many glandular structures. It contains a few afferent fibres which originate in the cells of its genicular, ganglion and are concerned with taste., Supply - 'face, ear, taste, tear', , , , , , Face: muscles of facial expression, Ear: nerve to stapedius, Taste: supplies anterior two-thirds of tongue, Tear: parasympathetic fibres to lacrimal glands, also salivary glands, , Path, Subarachnoid path, , , , Origin: motor- pons, sensory- nervus intermedius, Pass through the petrous temporal bone into the internal auditory meatus with the, vestibulocochlear nerve. Here they combine to become the facial nerve., , Facial canal path, , , , The canal passes superior to the vestibule of the inner ear, At the medial aspect of the middle ear, it becomes wider and contains the geniculate, ganglion., , - 3 branches:, 1. greater petrosal nerve, 2. nerve to stapedius, 3. chorda tympani, Stylomastoid foramen, , , , Passes through the stylomastoid foramen (tympanic cavity anterior and mastoid antrum, posteriorly), Posterior auricular nerve and branch to posterior belly of digastric and stylohyoid muscle
Page 1200 :
Face, Enters parotid gland and divides into 5 branches:, , , , , , , Temporal branch, Zygomatic branch, Buccal branch, Marginal mandibular branch, Cervical branch, Next question
Page 1201 :
Question 50 of 560, The first root of the brachial plexus commonly arises at which of the following levels?, , C6, , C5, , C3, , C2, , C8, , It begins at C5 and has 5 roots. It ends with a total of 15 nerves of these 5 are the main nerves to, the upper limb (axillary, radial, ulnar, musculocutaneous and median), Please rate this question:, , Discuss and give feedback, , Next question, , Brachial plexus, Origin, , Anterior rami of C5 to T1, , Sections of the, plexus, , , , , Roots, trunks, divisions, cords, branches, Mnemonic:Real Teenagers Drink Cold Beer, , Roots, , , , , Located in the posterior triangle, Pass between scalenus anterior and medius, , Trunks, , , , , , Located posterior to middle third of clavicle, Upper and middle trunks related superiorly to the subclavian artery, Lower trunk passes over 1st rib posterior to the subclavian artery
Page 1202 :
Divisions, , Apex of axilla, , Cords, , Related to axillary artery, , Diagram illustrating the branches of the brachial plexus, , Image sourced from Wikipedia, , Cutaneous sensation of the upper limb
Page 1203 :
Image sourced from Wikipedia, , Next question
Page 1206 :
, , , A 35 year old man falls and sustains a fracture to the medial third of his clavicle. Which, vessel is at greatest risk of injury?, , Subclavian vein, , Subclavian artery, , External carotid artery, , Internal carotid artery, , Vertebral artery, , , , , Theme from April 2013 exam, Theme from April 2014 exam, The subclavian vein lies behind subclavius and the medial part of the clavicle. It rests on the, first rib, below and in front of the third part of the subclavian artery, and then on scalenus, anterior which separates it from the second part of the artery (posteriorly)., Please rate this question:, , , , , , Discuss and give feedback, , , , Next question, , , , Clavicle, , , , The clavicle extends from the sternum to the acromion and helps prevent the shoulder falling, forwards and downwards., The inferior surface is irregular and strongly marked by ligaments at each end. Laterally, lies, the trapezoid line and this runs anterolaterally. Posteriorly, lies the conoid tubercle. These, give attachment to the conoid and trapezoid parts of the coracoclavicular ligament. The, medial part of the inferior surface has an irregular surface which marks the surface, attachment of the costoclavicular ligament. The intermediate portion is marked by a groove, for the subclavius muscle., Medially, the superior part of the bone has a raised surface which gives attachment to the
Page 1207 :
clavicular head of sternocleidomastoid. Sternohyoid gains attachment to the posterior, surface., Laterally there is an oval articular facet for the acromion and a disk lies between the clavicle, and acromion. The capsule of the joint is attached to the ridge on the margin of the facet., Next question,
Page 1208 :
Question 53 of 560, Where are the greatest proportion of musculi pectinati found?, , Right ventricle, , Left ventricle, , Right atrium, , Pulmonary valve, , Aortic valve, , The musculi pectinati are found in the atria, hence the reason that the atrial walls in the right atrium, are irregular anteriorly., The musculi pectinati of the atria are internal muscular ridges on the anterolateral surface of the, chambers and they are only present in the area derived from the embryological true atrium., Please rate this question:, , Discuss and give feedback, , Next question, , Heart anatomy, The walls of each cardiac chamber comprise:, , , , , Epicardium, Myocardium, Endocardium, , Cardiac muscle is attached to the cardiac fibrous skeleton., Relations, The heart and roots of the great vessels within the pericardial sac are related anteriorly to the, sternum, medial ends of the 3rd to 5th ribs on the left and their associated costal cartilages. The, heart and pericardial sac are situated obliquely two thirds to the left and one third to the right of the, median plane.
Page 1209 :
The pulmonary valve lies at the level of the left third costal cartilage., The mitral valve lies at the level of the fourth costal cartilage., Coronary sinus, This lies in the posterior part of the coronary groove and receives blood from the cardiac veins. The, great cardiac vein lies at its left and the middle and small cardiac veins lie on its right. The smallest, cardiac vein (anterior cardiac vein) drains into the right atrium directly., Aortic sinus, Right coronary artery arises from the right aortic sinus, the left is derived from the left aortic sinus,, which lies posteriorly., Right and left ventricles, , Structure, , Left Ventricle, , A-V Valve, , Mitral (double leaflet), , Walls, , Twice as thick as right, , Trabeculae carnae, , Much thicker and more numerous, , Right coronary artery, The RCA supplies:, , , , , , , Right atrium, Diaphragmatic part of the left ventricle, Usually the posterior third of the interventricular septum, The sino atrial node (60% cases), The atrio ventricular node (80% cases), , Left coronary artery, The LCA supplies:, , , , , , , Left atrium, Most of left ventricle, Part of the right ventricle, Anterior two thirds of the inter ventricular septum, The sino atrial node (remaining 40% cases), , Innervation of the heart, Autonomic nerve fibres from the superficial and deep cardiac plexus. These lie anterior to the
Page 1210 :
bifurcation of the trachea, posterior to the ascending aorta and superior to the bifurcation of the, pulmonary trunk. The parasympathetic supply to the heart is from presynaptic fibres of the vagus, nerves., Valves of the heart, , Mitral valve, , Aortic valve, , Pulmonary valve, , Tricuspid valve, , 2 cusps, , 3 cusps, , 3 cusps, , 3 cusps, , First heart sound, , Second heart, sound, , Second heart, sound, , First heart sound, , 1 anterior cusp, , 2 anterior cusps, , 2 anterior cusps, , 2 anterior cusps, , Attached to chordae, tendinae, , No chordae, , No chordae, , Attached to chordae, tendinae, Next question
Page 1211 :
Question 54 of 560, Which of the following structures separates the subclavian artery and vein?, , Digastric muscle, , Prevertebral fascia, , Anterior scalene muscle, , Middle scalene muscle, , Omohyoid, , The anterior scalene muscle is an important anatomical landmark and separates the subclavian vein, (anterior) from the subclavian artery (posterior)., Please rate this question:, , Discuss and give feedback, , Next question, , Scalene muscles, The 3 paired muscles are:, , , , , Scalenus anterior: Elevate 1st rib and laterally flex the neck to same side, Scalenus medius: Same action as scalenus anterior, Scalenus posterior: Elevate 2nd rib and tilt neck to opposite side, , Innervation, , Spinal nerves C4-6, , Origin, , Transverse processes C2 to C7, , Insertion, , First and second ribs, , Important, relations, , , , , The brachial plexus and subclavian artery pass between the anterior and, middle scalenes through a space called the scalene hiatus/fissure., The subclavian vein and phrenic nerve pass anteriorly to the anterior
Page 1212 :
scalene as it crosses over the first rib., , Image sourced from Wikipedia, , Thoracic outlet syndrome, The scalenes are at risk of adhering to the fascia surrounding the brachial plexus or shortening, causing compression of the brachial plexus when it passes between the clavicle and 1st rib causing, thoracic outlet syndrome., Next question
Page 1213 :
Question 55 of 560, A 33 year old man is stabbed in the right chest and undergoes a thoracotomy. The right lung is, mobilised and the pleural reflection at the lung hilum is opened. Which of the structures listed below, does not lie within this region?, , Pulmonary artery, , Azygos vein, , Pulmonary vein, , Bronchus, , None of the above, , The pleural reflections encase the hilum of the lung and continue inferiorly as the pulmonary, ligament. It encases the pulmonary vessels and bronchus. The azygos vein is not contained within it., Please rate this question:, , Discuss and give feedback, , Next question, , Lung anatomy, The right lung is composed of 3 lobes divided by the oblique and transverse fissures. The left lung, has two lobes divided by the oblique fissure.The apex of both lungs is approximately 4cm superior to, the sterno-costal joint of the first rib. Immediately below this is a sulcus created by the subclavian, artery., Peripheral contact points of the lung, , , , , Base: diaphragm, Costal surface: corresponds to the cavity of the chest, Mediastinal surface: Contacts the mediastinal pleura. Has the cardiac impression. Above and, behind this concavity is a triangular depression named the hilum, where the structures which, form the root of the lung enter and leave the viscus. These structures are invested by pleura,, which, below the hilum and behind the pericardial impression, forms the pulmonary ligament
Page 1214 :
Right lung, Above the hilum is the azygos vein; Superior to this is the groove for the superior vena cava and, right innominate vein; behind this, and nearer the apex, is a furrow for the innominate artery. Behind, the hilum and the attachment of the pulmonary ligament is a vertical groove for the oesophagus; In, front and to the right of the lower part of the oesophageal groove is a deep concavity for the, extrapericardiac portion of the inferior vena cava., The root of the right lung lies behind the superior vena cava and the right atrium, and below the, azygos vein., The right main bronchus is shorter, wider and more vertical than the left main bronchus and, therefore the route taken by most foreign bodies., , Image sourced from Wikipedia, , Left lung, Above the hilum is the furrow produced by the aortic arch, and then superiorly the groove, accommodating the left subclavian artery; Behind the hilum and pulmonary ligament is a vertical, groove produced by the descending aorta, and in front of this, near the base of the lung, is the lower, part of the oesophagus., The root of the left lung passes under the aortic arch and in front of the descending aorta.
Page 1215 :
Image sourced from Wikipedia, , Inferior borders of both lungs, , , , , 6th rib in mid clavicular line, 8th rib in mid axillary line, 10th rib posteriorly, , The pleura runs two ribs lower than the corresponding lung level., Bronchopulmonary segments, , Segment number, , Right lung, , Left lung, , 1, , Apical, , Apical, , 2, , Posterior, , Posterior, , 3, , Anterior, , Anterior, , 4, , Lateral, , Superior lingular, , 5, , Medial, , Inferior lingular, , 6, , Superior (apical), , Superior (apical)
Page 1216 :
Segment number, , Right lung, , Left lung, , 7, , Medial basal, , Medial basal, , 8, , Anterior basal, , Anterior basal, , 9, , Lateral basal, , Lateral basal, , 10, , Posterior basal, , Posterior basal, Next question
Page 1217 :
Question 56 of 560, A 56 year old man requires long term parenteral nutrition and the decision is made to insert a PICC, line for long term venous access. This is inserted into the basilic vein at the region of the elbow. As, the catheter is advanced, into which venous structure is the tip of the catheter most likely to pass, from the basilic vein?, , Subclavian vein, , Axillary vein, , Posterior circumflex humeral vein, , Cephalic vein, , Superior vena cava, , The basilic vein drains into the axillary vein and although PICC lines may end up in a variety of, fascinating locations the axillary vein is usually the commonest site following from the basilic. The, posterior circumflex humeral vein is encountered prior to the axillary vein. However, a PICC line is, unlikely to enter this structure because of its angle of entry into the basilic vein., Please rate this question:, , Discuss and give feedback, , Next question, , Basilic vein, The basilic and cephalic veins both provide the main pathways of venous drainage for the arm and, hand. It is continuous with the palmar venous arch distally and the axillary vein proximally., Path, , , , , , , Originates on the medial side of the dorsal venous network of the hand, and passes up the, forearm and arm., Most of its course is superficial., Near the region anterior to the cubital fossa the vein joins the cephalic vein., Midway up the humerus the basilic vein passes deep under the muscles., At the lower border of the teres major muscle, the anterior and posterior circumflex humeral, veins feed into it.
Page 1218 :
, , It is often joined by the medial brachial vein before draining into the axillary vein., Next question
Page 1219 :
Question 57 of 560, An individual is noted to have a left sided superior vena cava. By which pathway is blood from this, system most likely to enter the heart?, , Via the coronary sinus, , Via the azygos venous system and into the superior vena cava, , Via anomalies in the pumonary vascular bed, , Via the left atrium and persistent foramen ovale, , Directly into the roof of the right atrium, , Theme from September 2013 Exam, Persistent left superior vena cava is the most common anomaly of the thoracic venous system. It is, prevalent in 0.3% of the population and is a benign entity of failed involution during embryogenesis., Please rate this question:, , Discuss and give feedback, , Next question, , Superior vena cava, Drainage, , , , , , Head and neck, Upper limbs, Thorax, Part of abdominal walls, , Formation, , , , , Subclavian and internal jugular veins unite to form the right and left brachiocephalic veins, These unite to form the SVC, Azygos vein joins the SVC before it enters the right atrium
Page 1220 :
Relations, , Anterior, , Anterior margins of the right lung and pleura, , Posteromedial, , Trachea and right vagus nerve, , Posterolateral, , Posterior aspects of right lung and pleura, Pulmonary hilum is posterior, , Right lateral, , Right phrenic nerve and pleura, , Left lateral, , Brachiocephalic artery and ascending aorta, , Developmental variations, Anomalies of the connection of the SVC are recognised. In some individuals a persistent left sided, SVC drains into the right atrium via an enlarged orifice of the coronary sinus. More rarely the left, sided vena cava may connect directly with the superior aspect of the left atrium, usually associated, with an un-roofing of the coronary sinus. The commonest lesion of the IVC is for its abdominal, course to be interrupted, with drainage achieved via the azygos venous system. This may occur in, patients with left sided atrial isomerism., Next question
Page 1221 :
Question 58-60 of 560, Theme: Nerve injury, , A., B., C., D., E., F., , Ulnar nerve, Musculocutaneous nerve, Radial nerve, Median nerve, Axillary nerve, Intercostobrachial nerve, , What is the most likely nerve injury for the scenario given? Each option may be used once, more, than once or not at all., , 58., , A 23 year old man is involved in a fight outside a nightclub and sustains a laceration to his, right arm. On examination he has lost extension of the fingers in his right hand., You answered Ulnar nerve, The correct answer is Radial nerve, The radial nerve supplies the extensor muscle group., , 59., , A 40 year old lady trips and falls through a glass door and sustains a severe laceration to, her left arm. Amongst her injuries it is noticed that she has lost the ability to adduct the, fingers of her left hand., Ulnar nerve, The interossei are supplied by the ulnar nerve., , 60., , A 28 year old rugby player injures his right humerus and on examination is noted to have a, minor sensory deficit overlying the point of deltoid insertion into the humerus., You answered Ulnar nerve, The correct answer is Axillary nerve, This patch of skin is supplied by the axillary nerve, , Theme from April 2014 exam, Please rate this question:
Page 1222 :
Discuss and give feedback, , Next question, , Brachial plexus, Origin, , Anterior rami of C5 to T1, , Sections of the, plexus, , , , , Roots, trunks, divisions, cords, branches, Mnemonic:Real Teenagers Drink Cold Beer, , Roots, , , , , Located in the posterior triangle, Pass between scalenus anterior and medius, , Trunks, , , , , , Located posterior to middle third of clavicle, Upper and middle trunks related superiorly to the subclavian artery, Lower trunk passes over 1st rib posterior to the subclavian artery, , Divisions, , Apex of axilla, , Cords, , Related to axillary artery, , Diagram illustrating the branches of the brachial plexus
Page 1223 :
Image sourced from Wikipedia, , Cutaneous sensation of the upper limb, , Image sourced from Wikipedia, , Next question
Page 1224 :
Question 61 of 560, A 53 year old man is undergoing a radical gastrectomy for carcinoma of the stomach. Which of the, following structures will need to be divided to gain access to the coeliac axis?, , Lesser omentum, , Greater omentum, , Falciform ligament, , Median arcuate ligament, , Gastrosplenic ligament, , The lesser omentum will need to be divided. During a radical gastrectomy this forms one of the, nodal stations that will need to be taken., Please rate this question:, , Discuss and give feedback, , Next question, , Coeliac axis, The coeliac axis has three main branches., , , , , Left gastric, Hepatic: branches-Right Gastric, Gastroduodenal, Right Gastroepiploic, Superior, Pancreaticoduodenal, Cystic (occasionally)., Splenic: branches- Pancreatic, Short Gastric, Left Gastroepiploic, , It occasionally gives off one of the inferior phrenic arteries.
Page 1226 :
Question 62 of 560, A 76 year old man complains of symptoms of claudication. The decision is made to measure his, ankle brachial pressure index. The signal from the dorsalis pedis artery is auscultated with a hand, held doppler device. This vessel is the continuation of which of the following?, , Posterior tibial artery, , Anterior tibial artery, , Peroneal artery, , Popliteal artery, , None of the above, , The dorsalis pedis is a continuation of the anterior tibial artery., Please rate this question:, , Discuss and give feedback, , Next question, , Foot- anatomy, Arches of the foot, The foot is conventionally considered to have two arches., , , , , The longitudinal arch is higher on the medial than on the lateral side. The posterior part of, the calcaneum forms a posterior pillar to support the arch. The lateral part of this structure, passes via the cuboid bone and the lateral two metatarsal bones. The medial part of this, structure is more important. The head of the talus marks the summit of this arch, located, between the sustentaculum tali and the navicular bone. The anterior pillar of the medial arch, is composed of the navicular bone, the three cuneiforms and the medial three metatarsal, bones., The transverse arch is situated on the anterior part of the tarsus and the posterior part of the, metatarsus. The cuneiforms and metatarsal bases narrow inferiorly, which contributes to the, shape of the arch., , Intertarsal joints
Page 1227 :
Sub talar joint, , Formed by the cylindrical facet on the lower surface of the body of the, talus and the posterior facet on the upper surface of the calcaneus. The, facet on the talus is concave anteroposteriorly, the other is convex. The, synovial cavity of this joint does not communicate with any other joint., , Talocalcaneonavicular, joint, , The anterior part of the socket is formed by the concave articular, surface of the navicular bone, posteriorly by the upper surface of the, sustentaculum tali. The talus sits within this socket, , Calcaneocuboid joint, , Highest point in the lateral part of the longitudinal arch. The lower, aspect of this joint is reinforced by the long plantar and plantar, calcaneocuboid ligaments., , Transverse tarsal joint, , The talocalcaneonavicular joint and the calcaneocuboid joint extend, across the tarsus in an irregular transverse plane, between the talus and, calcaneus behind and the navicular and cuboid bones in front. This, plane is termed the transverse tarsal joint., , Cuneonavicular joint, , Formed between the convex anterior surface of the navicular bone and, the concave surface of the the posterior ends of the three cuneiforms., , Intercuneiform joints, , Between the three cuneiform bones., , Cuneocuboid joint, , Between the circular facets on the lateral cuneiform bone and the, cuboid. This joint contributes to the tarsal part of the transverse arch., , A detailed knowledge of the joints is not required for MRCS Part A. However, the contribution they, play to the overall structure of the foot should be appreciated, Ligaments of the ankle joint and foot
Page 1228 :
Image sourced from Wikipedia, , Muscles of the foot, , Muscle, , Origin, , Insertion, , Nerve, supply, , Action, , Abductor, hallucis, , Medial side of the calcaneus,, flexor retinaculum, plantar, aponeurosis, , Medial side of, the base of the, proximal, phalanx, , Medial, plantar, nerve, , Abducts the great toe, , Flexor, digitorum, brevis, , Medial process of the, calcaneus, plantar, eponeurosis., , Via 4 tendons, into the, middle, phalanges of, the lateral 4, toes., , Medial, plantar, nerve, , Flexes all the joints of, the lateral 4 toes except, for the interphalangeal, joint., , Abductor, digit, minimi, , From the tubercle of the, calcaneus and from the, plantar aponeurosis, , Together with, flexor digit, minimi brevis, into the lateral, side of the, , Lateral, plantar, nerve, , Abducts the little toe at, the metatarsophalangeal, joint
Page 1229 :
base of the, proximal, phalanx of the, little toe, , Flexor, hallucis, brevis, , From the medial side of the, plantar surface of the cuboid, bone, from the adjacent part, of the lateral cuneiform bone, and from the tendon of, tibialis posterior., , Into the, proximal, phalanx of the, great toe, the, tendon, contains a, sesamoid bone, , Medial, plantar, nerve, , Flexes the, metatarsophalangeal, joint of the great toe., , Adductor, hallucis, , Arises from two heads. The, oblique head arises from the, sheath of the peroneus longus, tendon, and from the plantar, surfaces of the bases of the, 2nd, 3rd and 4th metatarsal, bones. The transverse head, arises from the plantar, surface of the lateral 4, metatarsophalangeal joints, and from the deep transverse, metatarsal ligament., , Lateral side of, the base of the, proximal, phalanx of the, great toe., , Lateral, plantar, nerve, , Adducts the great toe, towards the second toe., Helps maintain the, transverse arch of the, foot., , Extensor, digitorum, brevis, , On the dorsal surface of the, foot from the upper surface of, the calcaneus and its, associated fascia, , Via four thin, tendons which, run forward, and medially, to be inserted, into the, medial four, toes. The, lateral three, tendons join, with hoods of, extensor, digitorum, longus., , Deep, peroneal, , Extend the, metatarsophalangeal, joint of the medial four, toes. It is unable to, extend the, interphalangeal joint, without the assistance of, the lumbrical muscles., , Nerves in the foot
Page 1230 :
Lateral plantar nerve, Passes anterolaterally towards the base of the 5th metatarsal between flexor digitorum brevis and, flexor accessorius. On the medial aspect of the lateral plantar artery. At the base of the 5th, metatarsal it splits into superficial and deep branches., Medial plantar nerve, Passes forwards with the medial plantar artery under the cover of the flexor retinaculum to the, interval between abductor hallucis and flexor digitorum brevis on the sole of the foot., Plantar arteries, Arise under the cover of the flexor retinaculum, midway between the tip of the medial malleolus and, the most prominent part of the medial side of the heel., , , , , Medial plantar artery. Passes forwards medial to medial plantar nerve in the space between, abductor hallucis and flexor digitorum brevis.Ends by uniting with a branch of the 1st plantar, metatarsal artery., Lateral plantar artery. Runs obliquely across the sole of the foot. It lies lateral to the lateral, plantar nerve. At the base of the 5th metatarsal bone it arches medially across the foot on, the metatarsals, , Dorsalis pedis artery, This vessel is a direct continuation of the anterior tibial artery. It commences on the front of the ankle, joint and runs to the proximal end of the first metatarsal space. Here is gives off the arcuate artery, and continues forwards as the first dorsal metatarsal artery. It is accompanied by two veins, throughout its length. It is crossed by the extensor hallucis brevis, Next question
Page 1231 :
Question 63 of 560, A 67 year old man is due to undergo a revisional total hip replacement using a posterior approach., After dividing gluteus maximus in the line of its fibres there is brisk arterial bleeding. Which of the, following vessels is likely to be responsible?, , Profunda femoris artery, , External iliac artery, , Internal iliac artery, , Obturator artery, , Inferior gluteal artery, , Theme from April 2014 Exam, The inferior gluteal artery runs on the deep surface of the gluteus maximus muscle. It is a branch of, the internal iliac artery. It is commonly divided during the posterior approach to the hip joint., Please rate this question:, , Discuss and give feedback, , Next question, , Hip joint, , , , , , , , Head of femur articulates with acetabulum of the pelvis, Both covered by articular hyaline cartilage, The acetabulum forms at the union of the ilium, pubis, and ischium, The triradiate cartilage (Y-shaped growth plate) separates the pelvic bones, The acetabulum holds the femoral head by the acetabular labrum, Normal angle between femoral head and femoral shaft is 130o, , Ligaments, , , , Transverse ligament: joints anterior and posterior ends of the articular cartilage, Head of femur ligament (ligamentum teres): acetabular notch to the fovea. Contains arterial, supply to head of femur in children.
Page 1233 :
, , Ischiofemoral ligament: posterior support. Ischium to greater trochanter., , Blood supply, Medial circumflex femoral and lateral circumflex femoral arteries (Branches of profunda femoris)., Also from the inferior gluteal artery. These form an anastomosis and travel to up the femoral neck to, supply the head., Next question
Page 1234 :
Question 64 of 560, A 17 year old lady presents with right iliac fossa pain and diagnosed as having acute appendicitis., You take her to theatre to perform a laparoscopic appendicectomy. During the procedure the scrub, nurse distracts you and you inadvertently avulse the appendicular artery. The ensuing haemorrhage, is likely to be supplied directly from which vessel?, , Inferior mesenteric artery, , Superior mesenteric artery, , Ileo-colic artery, , Internal iliac artery, , None of the above, , Theme from April 2014 exam, The appendicular artery is a branch of the ileocolic artery., Please rate this question:, , Discuss and give feedback, , Next question, , Appendix, , , , , , , , Location: Base of caecum., Up to 10cm long., Mainly lymphoid tissue (Hence mesenteric adenitis may mimic appendicitis)., Caecal taenia coli converge at base of appendix and form a longitudinal muscle cover over, the appendix. This convergence should facilitate its identification at surgery if it is retrocaecal, and difficult to find (which it can be when people start doing appendicectomies!), Arterial supply: Appendicular artery (branch of the ileocolic)., It is intra peritoneal., , McBurney's point, , , 1/3 of the way along a line drawn from the Anterior Superior Iliac Spine to the Umbilicus
Page 1236 :
Question 65 of 560, , A 63 year old man who smokes heavily presents with dyspepsia. He is tested and found to be, positive for helicobacter pylori infection. One evening he has an episode of haematemesis and, collapses. What is the most likely vessel to be responsible?, , Portal vein, , Short gastric arteries, , Superior mesenteric artery, , Gastroduodenal artery, , None of the above, , Theme from January 2012 exam, He is most likely to have a posteriorly sited duodenal ulcer. These can invade the gastroduodenal, artery and present with major bleeding. Although gastric ulcers may invade vessels they do not tend, to produce major bleeding of this nature., Please rate this question:, , Discuss and give feedback, , Next question, , Gastroduodenal artery, Supplies, Pylorus, proximal part of the duodenum, and indirectly to the pancreatic head (via the anterior and, posterior superior pancreaticoduodenal arteries)
Page 1237 :
Path, Most commonly arises from the common hepatic artery of the coeliac trunk, Terminates by bifurcating into the right gastroepiploic artery and the superior pancreaticoduodenal, artery, Image showing stomach reflected superiorly to illustrate the relationship of the gastroduodenal artery, to the first part of the duodenum, , Image sourced from Wikipedia, , Next question
Page 1238 :
Question 66 of 560, Which of the following nerves is responsible for the cremasteric reflex?, , Lateral femoral cutaneous nerve, , Femoral nerve, , Obturator nerve, , Genitofemoral nerve, , None of the above, , The motor and sensory fibres of the genitofemoral nerve are tested in the cremasteric reflex. A small, contribution is also played by the ilioinguinal nerve and thus the reflex may be lost following an, inguinal hernia repair., Please rate this question:, , Discuss and give feedback, , Next question, , Genitofemoral nerve, Supplies, Small area of the upper medial thigh., Path, , , , , , , , , Arises from the first and second lumbar nerves., Passes obliquely through psoas major, and emerges from its medial border opposite the, fibrocartilage between the third and fourth lumbar vertebrae., It then descends on the surface of psoas major, under cover of the peritoneum, Divides into genital and femoral branches., The genital branch passes through the inguinal canal, within the spermatic cord, to supply, the skin overlying the skin and fascia of the scrotum. The femoral branch enters the thigh, posterior to the inguinal ligament, lateral to the femoral artery. It supplies an area of skin and, fascia over the femoral triangle., It may be injured during abdominal or pelvic surgery, or during inguinal hernia repairs
Page 1239 :
Question 67 of 560, Which of the structures listed below are not located within the mediastinum?, , Thymus, , Heart, , Great vessels, , Arch of azygos vein, , Vertebral bodies, , The vertebral bodies lie outside of the mediastinum, as do the lungs., Please rate this question:, , Discuss and give feedback, , Next question, , Mediastinum, Region between the pulmonary cavities., It is covered by the mediastinal pleura. It does not contain the lungs., It extends from the thoracic inlet superiorly to the diaphragm inferiorly., Mediastinal regions, , , , , , Region, , Superior mediastinum (between manubriosternal angle and T4/5), Middle mediastinum, Posterior mediastinum, Anterior mediastinum, , Contents
Page 1241 :
Question 68 of 560, A 22 year old man is stabbed in the chest at the level of the junction between the sternum and, manubrium. Which structure is at greatest risk?, , Left atrium, , Oesophagus, , Thyroid gland, , Inferior vena cava, , Aortic arch, , Theme from 2014 Exam, At the level of the Angle of Louis (Manubriosternal angle), is the surface marking for the aortic arch., The oesophagus is posteriorly located and at less risk., Please rate this question:, , Discuss and give feedback, , Next question, , Sternal angle, Anatomical structures at the level of the manubrium and upper sternum, , Upper part of the manubrium, , , , , , , Left brachiocephalic vein, Brachiocephalic artery, Left common carotid, Left subclavian artery, , Lower part of the manubrium/, manubrio-sternal angle, , , , , Costal cartilages of the 2nd ribs, Transition point between superior and inferior, mediastinum, Arch of the aorta, Tracheal bifurcation, Union of the azygos vein and superior vena, , , ,
Page 1243 :
Question 69 of 560, Which of these nerves passes through the greater and lesser sciatic foramina?, , Pudendal nerve, , Sciatic nerve, , Superior gluteal nerve, , Inferior gluteal nerve, , Posterior cutaneous nerve of the thigh, Structures passing through the lesser and greater sciatic foramina (medial to lateral): PIN, , , , , Pudendal nerve, Internal pudendal artery, Nerve to obturator internus, , Theme from 2010 Exam, Theme from January 2013 Exam, Theme from January 2014 Exam, The pudendal nerve originates from the ventral rami of the second, third, and fourth sacral nerves, (S2, S3, S4)., It passes between the piriformis and coccygeus muscles and exits the pelvis through the the greater, sciatic foramen. It crosses the spine of the ischium and reenters the pelvis through the lesser sciatic, foramen. It passes through the pudendal canal., The pudendal nerve gives off the inferior rectal nerves. It terminates into 2 branches: perineal nerve,, and the dorsal nerve of the penis or the dorsal nerve of the clitoris., Please rate this question:, , Discuss and give feedback, , Next question, , Greater sciatic foramen, Contents
Page 1246 :
Question 70 of 560, A cervical rib is due to which of the following?, , Hyperplasia of the annulus fibrosus, , Proliferation of the nucleus pulposus, , Fusion of the transverse processes of the 6th and 7th cervical vertebrae, , An accessory cervical vertebra, , Elongation of the transverse processes of the 7th cervical vertebra, , Cervical ribs occur as a result of the elongation of the transverse process of the 7th cervical, vertebra. It is usually a fibrous band that attaches to the first thoracic rib., Please rate this question:, , Discuss and give feedback, , Next question, , Cervical ribs, , , , , , , , , , 0.2-0.4% incidence, Most cases present with neurological symptoms, Consist of an anomalous fibrous band that often originates from C7 and may arc towards,, but rarely reaches the sternum, Congenital cases may present around the third decade, some cases are reported to occur, following trauma, Bilateral in up to 70%, Compression of the subclavian artery may produce absent radial pulse on clinical, examination and in particular may result in a positive Adsons test (lateral flexion of the neck, towards the symptomatic side and traction of the symptomatic arm- leads to obliteration of, radial pulse), Treatment is most commonly undertaken when there is evidence of neurovascular, compromise. A transaxillary approach is the traditional operative method for excision.
Page 1247 :
Image sourced from Wikipedia, , 3D reconstruction of a left-sided cervical rib, Next question
Page 1248 :
Question 71 of 560, Which of the structures listed below is not a content of the carotid sheath?, , Internal jugular vein, , Internal carotid artery, , Vagus nerve, , Recurrent laryngeal nerve, , Common carotid artery, Contents of carotid sheath:, Common carotid artery, Internal carotid artery, Internal jugular vein, Vagus nerve, Theme from April 2014 exam, Please rate this question:, , Discuss and give feedback, , Next question, , Common carotid artery, The right common carotid artery arises at the bifurcation of the brachiocephalic trunk, the left, common carotid arises from the arch of the aorta. Both terminate at the level of the upper border of, the thyroid cartilage (the lower border of the third cervical vertebra) by dividing into the internal and, external carotid arteries., Left common carotid artery, This vessel arises immediately to the left and slightly behind the origin of the brachiocephalic trunk., Its thoracic portion is 2.5- 3.5 cm in length and runs superolaterally to the sternoclavicular joint., In the thorax, The vessel is in contact, from below upwards, with the trachea, left recurrent laryngeal nerve, left, margin of the oesophagus. Anteriorly the left brachiocephalic vein runs across the artery, and the, cardiac branches from the left vagus descend in front of it. These structures together with the, thymus and the anterior margins of the left lung and pleura separate the artery from the manubrium.
Page 1249 :
In the neck, The artery runs superiorly deep to sternocleidomastoid and then enters the anterior triangle. At this, point it lies within the carotid sheath with the vagus nerve and the internal jugular vein. Posteriorly, the sympathetic trunk lies between the vessel and the prevertebral fascia. At the level of C7 the, vertebral artery and thoracic duct lie behind it. The anterior tubercle of C6 transverse process is, prominent and the artery can be compressed against this structure (it corresponds to the level of the, cricoid)., Anteriorly at C6 the omohyoid muscle passes superficial to the artery., Within the carotid sheath the jugular vein lies lateral to the artery., Right common carotid artery, The right common carotid arises from the brachiocephalic artery. The right common carotid artery, corresponds with the cervical portion of the left common carotid, except that there is no thoracic duct, on the right. The oesophagus is less closely related to the right carotid than the left., Summary points about the carotid anatomy, Path, Passes behind the sternoclavicular joint (12% patients above this level) to the upper border of the, thyroid cartilage, to divide into the external (ECA) and internal carotid arteries (ICA)., Relations, , , , , , , Level of 6th cervical vertebra crossed by omohyoid, Then passes deep to the thyrohyoid, sternohyoid, sternomastoid muscles., Passes anterior to the carotid tubercle (transverse process 6th cervical vertebra)-NB, compression here stops haemorrhage., The inferior thyroid artery passes posterior to the common carotid artery., Then : Left common carotid artery crosses the thoracic duct, Right common carotid artery, crossed by recurrent laryngeal nerve
Page 1250 :
Image sourced from Wikipedia, , Next question
Page 1251 :
Question 72 of 560, , A 22 year old man is undergoing a wedge excision of his great toenail. As the surgeon passes a, needle into the area to administer local anaesthetic, the patient notices a sharp pain. By which, pathway will this sensation be conveyed to the central nervous system?, , Anterior corticospinal tract, , Posterior spinocerebellar tract, , Cuneate fasciculus, , Vestibulospinal tract, , Spinothalamic tract, Spinothalamic tract- Pain and temperature, Vestibulospinal tract- Motor neuronal signals relating to posture, Cuneate fasciculus- Fine touch, pressure and proprioception, Posterior spinocerebellar tract- Proprioceptive signals to cerebellum, Anterior corticospinal tract- Conveys motor signals from precentral gyrus to motor cells within the, cord, , Theme from January 2011 Exam, Pain impulses are transmitted via the spinothalamic tract, Please rate this question:, , Discuss and give feedback, , Next question, , Spinothalamic tract
Page 1252 :
The spinothalamic tract transmits impulses from receptors which measure crude touch, pain and, temperature. The spinothalamic tract comprises the lateral and anterior spinothalamic tracts, the, former typically transmits pain and temperature and the latter crude touch and pressure. Neurones, transmitting these signals will typically ascend by one or two vertebral levels in Lissaurs tract prior to, decussating in the spinal cord itself. Neurones then pass rostrally in the cord to connect at the, thalamus., Next question
Page 1253 :
Question 73 of 560, A 73 year old lady is admitted with brisk rectal bleeding. Despite attempts at resuscitation the, bleeding proceeds to cause haemodynamic compromise. An upper GI endoscopy is normal. A, mesenteric angiogram is performed and a contrast blush is seen in the region of the sigmoid colon., The radiologist decides to embolise the vessel supplying this area. At what spinal level does it leave, the aorta?, , L2, , L1, , L4, , L3, , T10, , Theme from 2009 Exam, The inferior mesenteric artery leaves the aorta at L3. It supplies the left colon and sigmoid. Its, proximal continuation to communicate with the middle colic artery is via the marginal artery., Please rate this question:, , Discuss and give feedback, , Next question, , Levels, Transpyloric plane, Level of the body of L1, , , , , , , , , , Pylorus stomach, Left kidney hilum (L1- left one!), Fundus of the gallbladder, Neck of pancreas, Duodenojejunal flexure, Superior mesenteric artery, Portal vein
Page 1255 :
Question 74 of 560, A 23 year old lady with troublesome axillary hyperhidrosis is undergoing a thorascopic, sympathectomy to treat the condition. Which of the following structures will need to be divided to, access the sympathetic trunk?, , Intercostal vein, , Intercostal artery, , Parietal pleura, , Visceral pleura, , None of the above, , The sympathetic chain lies posterior to the parietal pleura. During a thorascopic sympathetomy this, structure will need to be divided. The intercostal vessels lie posteriorly. They may be damaged with, troublesome bleeding but otherwise are best left alone as deliberate division will not improve surgical, access., Please rate this question:, , Discuss and give feedback, , Next question, , Sympathetic nervous system- anatomy, The cell bodies of the pre-ganglionic efferent neurones lie in the lateral horn of the grey matter of the, spinal cord in the thoraco-lumbar regions., The pre-ganglionic efferents leave the spinal cord at levels T1-L2. These pass to the sympathetic, chain., Lateral branches of the sympathetic chain connect it to every spinal nerve. These post ganglionic, nerves will pass to structures that receive sympathetic innervation at the periphery., Sympathetic chains, These lie on the vertebral column and run from the base of the skull to the coccyx., , Cervical, region, , Lie anterior to the transverse processes of the cervical vertebrae and posterior to, the carotid sheath.
Page 1256 :
Thoracic, region, , Lie anterior to the neck of the upper ribs and and lateral sides of the lower thoracic, vertebrae.They are covered by the parietal pleura, , Lumbar, region, , Enter by passing posterior to the medial arcuate ligament. Lie anteriorly to the, vertebrae and medial to psoas major., , Sympathetic ganglia, , , , , , , Superior cervical ganglion lies anterior to C2 and C3., Middle cervical ganglion (if present) C6, Stellate ganglion- anterior to transverse process of C7, lies posterior to the subclavian artery,, vertebral artery and cervical pleura., Thoracic ganglia are segmentally arranged., There are usually 4 lumbar ganglia., , Clinical importance, , , , , Interruption of the head and neck supply of the sympathetic nerves will result in an ipsilateral, Horners syndrome., For treatment of hyperhidrosis the sympathetic denervation can be achieved by removing the, second and third thoracic ganglia with their rami. Removal of T1 will cause a Horners, syndrome and is therefore not performed., In patients with vascular disease of the lower limbs a lumbar sympathetomy may be, performed, either radiologically or (more rarely now) surgically. The ganglia of L2 and below, are disrupted. If L1 is removed then ejaculation may be compromised (and little additional, benefit conferred as the preganglionic fibres do not arise below L2., Next question
Page 1257 :
Question 75 of 560, In which space is a lumbar puncture performed?, , Subdural space, , Epidural space, , Subarachnoid space, , Extradural space, , Intraventricular space, , Theme from January 2013 exam, Samples of CSF are normally obtained by inserting a needle between the third and fourth lumbar, vertebrae. The tip of the needle lies in the sub arachnoid space, the spinal cord terminates at L1 and, is not at risk of injury. Clinical evidence of raised intracranial pressure is a contraindication to lumbar, puncture., Please rate this question:, , Discuss and give feedback, , Next question, , Cerebrospinal fluid, The CSF fills the space between the arachnoid mater and pia mater (covering surface of the brain)., The total volume of CSF in the brain is approximately 150ml. Approximately 500 ml is produced by, the ependymal cells in the choroid plexus (70%), or blood vessels (30%). It is reabsorbed via the, arachnoid granulations which project into the venous sinuses., Circulation, 1. Lateral ventricles (via foramen of Munro), 2. 3rd ventricle, 3. Cerebral aqueduct (aqueduct of Sylvius), 4. 4th ventricle (via foramina of Magendie and Luschka), 5. Subarachnoid space, 6. Reabsorbed into the venous system via arachnoid granulations into superior sagittal sinus, Composition
Page 1258 :
, , , , , Glucose: 50-80mg/dl, Protein: 15-40 mg/dl, Red blood cells: Nil, White blood cells: 0-3 cells/ mm3, Next question
Page 1259 :
Question 76 of 560, A 21 year old man is stabbed in the antecubital fossa. A decision is made to surgically explore the, wound. At operation the surgeon dissects down onto the brachial artery. A nerve is identified, medially, which nerve is it likely to be?, , Radial, , Recurrent branch of median, , Anterior interosseous, , Ulnar, , Median, , Theme from September 2012 Exam, Please rate this question:, , Discuss and give feedback, , Next question, , Median nerve, The median nerve is formed by the union of a lateral and medial root respectively from the lateral, (C5,6,7) and medial (C8 and T1) cords of the brachial plexus; the medial root passes anterior to the, third part of the axillary artery. The nerve descends lateral to the brachial artery, crosses to its, medial side (usually passing anterior to the artery). It passes deep to the bicipital aponeurosis and, the median cubital vein at the elbow., It passes between the two heads of the pronator teres muscle, and runs on the deep surface of, flexor digitorum superficialis (within its fascial sheath)., Near the wrist it becomes superficial between the tendons of flexor digitorum superficialis and flexor, carpi radialis, deep to palmaris longus tendon. It passes deep to the flexor retinaculum to enter the, palm, but lies anterior to the long flexor tendons within the carpal tunnel., Branches, , Region, , Branch
Page 1261 :
, , , , unable to pronate forearm, weak wrist flexion, ulnar deviation of wrist, , Anterior interosseous nerve (branch of median nerve), , , , leaves just below the elbow, results in loss of pronation of forearm and weakness of long flexors of thumb and index, finger, , Topography of the median nerve, , Image sourced from Wikipedia, , Next question
Page 1262 :
Question 77 of 560, A 65 year old man with long standing atrial fibrillation develops an embolus to the lower leg. The, decision is made to perform an embolectomy, utilising a trans popliteal approach. After incising the, deep fascia, which of the following structures will the surgeons encounter first on exploring the, central region of the popliteal fossa?, , Popliteal vein, , Common peroneal nerve, , Popliteal artery, , Tibial nerve, , None of the above, , Theme from April 2015 Exam, Theme from April 2016 Exam, The tibial nerve lies superior to the vessels in the inferior aspect of the popliteal fossa. In the upper, part of the fossa the tibial nerve lies lateral to the vessels, it then passes superficial to them to lie, medially. The popliteal artery is the deepest structure in the popliteal fossa., Please rate this question:, , Discuss and give feedback, , Next question, , Popliteal fossa, Boundaries of the popliteal fossa, , Laterally, , Biceps femoris above, lateral head of gastrocnemius and plantaris below, , Medially, , Semimembranosus and semitendinosus above, medial head of gastrocnemius below, , Floor, , Popliteal surface of the femur, posterior ligament of knee joint and popliteus muscle
Page 1263 :
Superficial and deep fascia, , Roof, , Image showing the popliteal fossa, , © Image provided by the University of Sheffield, , Contents, , , , , , , , , Popliteal artery and vein, Small saphenous vein, Common peroneal nerve, Tibial nerve, Posterior cutaneous nerve of the thigh, Genicular branch of the obturator nerve, Lymph nodes, Next question
Page 1264 :
Question 78 of 560, , A 43 year old man is undergoing a right hemicolectomy and the ileo-colic artery is ligated. From, which of the following vessels is is derived?, , Inferior mesenteric artery, , Superior mesenteric artery, , Coeliac axis, , Aorta, , None of the above, , The ileocolic artery is a branch of the SMA and supplies the right colon and terminal ileum. The, transverse colon is supplied by the middle colic artery. As veins accompany arteries in the, mesentery and are lined by lymphatics, high ligation is the norm in cancer resections. The ileo-colic, artery branches off the SMA near the duodenum., Please rate this question:, , Discuss and give feedback, , Next question, , Colon anatomy, The colon commences with the caecum. This represents the most dilated segment of the human, colon and its base (which is intraperitoneal) is marked by the convergence of teniae coli. At this point, is located the vermiform appendix. The colon continues as the ascending colon, the posterior aspect, of which is retroperitoneal. The line of demarcation between the intra and retro peritoneal right colon, is visible as a white line, in the living, and forms the line of incision for colonic resections.
Page 1265 :
The ascending colon becomes the transverse colon after passing the hepatic flexure. At this located, the colon becomes wholly intra peritoneal once again. The superior aspect of the transverse colon is, the point of attachment of the transverse colon to the greater omentum. This is an important, anatomical site since division of these attachments permits entry into the lesser sac. Separation of, the greater omentum from the transverse colon is a routine operative step in both gastric and colonic, resections., At the left side of the abdomen the transverse colon passes to the left upper quadrant and makes an, oblique inferior turn at the splenic flexure. Following this, the posterior aspect becomes, retroperitoneal once again., At the level of approximately L4 the descending colon becomes wholly intraperitoneal and becomes, the sigmoid colon. Whilst the sigmoid is wholly intraperitoneal there are usually attachments laterally, between the sigmoid and the lateral pelvic sidewall. These small congenital adhesions are not formal, anatomical attachments but frequently require division during surgical resections., At its distal end the sigmoid passes to the midline and at the region around the sacral promontary it, becomes the upper rectum. This transition is visible macroscopically as the point where the teniae, fuse. More distally the rectum passes through the peritoneum at the region of the peritoneal, reflection and becomes extraperitoneal., Arterial supply, Superior mesenteric artery and inferior mesenteric artery: linked by the marginal artery., Ascending colon: ileocolic and right colic arteries, Transverse colon: middle colic artery, Descending and sigmoid colon: inferior mesenteric artery, Venous drainage, From regional veins (that accompany arteries) to superior and inferior mesenteric vein, Lymphatic drainage, Initially along nodal chains that accompany supplying arteries, then para-aortic nodes., Embryology, Midgut- Second part of duodenum to 2/3 transverse colon, Hindgut- Distal 1/3 transverse colon to anus, Peritoneal location, The right and left colon are part intraperitoneal and part extraperitoneal. The sigmoid and transverse, colon are generally wholly intraperitoneal. This has implications for the sequelae of perforations,, which will tend to result in generalised peritonitis in the wholly intra peritoneal segments., Colonic relations
Page 1266 :
Region of colon, , Relation, , Caecum/ right colon, , Right ureter, gonadal vessels, , Hepatic flexure, , Gallbladder (medially), , Splenic flexure, , Spleen and tail of pancreas, , Distal sigmoid/ upper rectum, , Left ureter, , Rectum, , Ureters, autonomic nerves, seminal vesicles, prostate, urethra (distally), Next question
Page 1267 :
Question 79 of 560, A 53 year old man is undergoing a distal pancreatectomy for trauma. Which of the following vessels, is responsible for the arterial supply to the tail of the pancreas?, , Splenic artery, , Pancreaticoduodenal artery, , Gastric artery, , Hepatic artery, , Superior mesenteric artery, Pancreatic head is supplied by the pancreaticoduodenal artery, Pancreatic tail is supplied by branches of the splenic artery, Theme from April 2014 Exam, There is an arterial "watershed" in the supply between the head and tail of the pancreas. The head is, supplied by the pancreaticoduodenal artery and the tail is supplied by branches of the splenic artery., Please rate this question:, , Discuss and give feedback, , Next question, , Pancreas, The pancreas is a retroperitoneal organ and lies posterior to the stomach. It may be accessed, surgically by dividing the peritoneal reflection that connects the greater omentum to the transverse, colon. The pancreatic head sits in the curvature of the duodenum. Its tail lies close to the hilum of, the spleen, a site of potential injury during splenectomy., Relations, Posterior to the pancreas, , Pancreatic head, , Inferior vena cava, Common bile duct, Right and left renal veins, Superior mesenteric vein and artery
Page 1268 :
Pancreatic neck, , Superior mesenteric vein, portal vein, , Pancreatic body-, , Left renal vein, Crus of diaphragm, Psoas muscle, Adrenal gland, Kidney, Aorta, , Pancreatic tail, , Left kidney, , Anterior to the pancreas, , Pancreatic head, , 1st part of the duodenum, Pylorus, Gastroduodenal artery, SMA and SMV(uncinate process), , Pancreatic body, , Stomach, Duodenojejunal flexure, , Pancreatic tail, , Splenic hilum, , Superior to the pancreas, Coeliac trunk and its branches common hepatic artery and splenic artery, Grooves of the head of the pancreas, 2nd and 3rd part of the duodenum, Arterial supply, , , , Head: pancreaticoduodenal artery, Rest: splenic artery, , Venous drainage, , , , Head: superior mesenteric vein, Body and tail: splenic vein
Page 1269 :
Ampulla of Vater, , , , Merge of pancreatic duct and common bile duct, Is an important landmark, halfway along the second part of the duodenum, that marks the, anatomical transition from foregut to midgut (also the site of transition between regions, supplied by coeliac trunk and SMA)., , Image sourced from Wikipedia, , Next question
Page 1270 :
Question 80 of 560, A 43 year old lady presents with varicose veins and undergoes a saphenofemoral disconnection,, long saphenous vein stripping to the ankle and isolated hook phlebectomies. Post operatively she, notices an area of numbness superior to her ankle. What is the most likely cause for this?, , Sural nerve injury, , Femoral nerve injury, , Saphenous nerve injury, , Common peroneal nerve injury, , Superficial peroneal nerve injury, , The sural nerve is related to the short saphenous vein. The saphenous nerve is related to the long, saphenous vein below the knee and for this reason full length stripping of the vein is no longer, advocated., Please rate this question:, , Discuss and give feedback, , Next question, , Saphenous vein, Long saphenous vein, This vein may be harvested for bypass surgery, or removed as treatment for varicose veins with, saphenofemoral junction incompetence., , , , , , , , Originates at the 1st digit where the dorsal vein merges with the dorsal venous arch of the, foot, Passes anterior to the medial malleolus and runs up the medial side of the leg, At the knee, it runs over the posterior border of the medial epicondyle of the femur bone, Then passes laterally to lie on the anterior surface of the thigh before entering an opening in, the fascia lata called the saphenous opening, It joins with the femoral vein in the region of the femoral triangle at the saphenofemoral, junction
Page 1271 :
Tributaries, , , , , , Medial marginal, Superficial epigastric, Superficial iliac circumflex, Superficial external pudendal veins, , Short saphenous vein, , , , , Originates at the 5th digit where the dorsal vein merges with the dorsal venous arch of the, foot, which attaches to the great saphenous vein., It passes around the lateral aspect of the foot (inferior and posterior to the lateral malleolus), and runs along the posterior aspect of the leg (with the sural nerve), Passes between the heads of the gastrocnemius muscle, and drains into the popliteal vein,, approximately at or above the level of the knee joint., Next question
Page 1272 :
Question 81 of 560, Which of the following muscles does not attach to the radius?, , Pronator quadratus, , Biceps, , Brachioradialis, , Supinator, , Brachialis, , The brachialis muscle inserts into the ulna. The other muscles are all inserted onto the radius., Please rate this question:, , Discuss and give feedback, , Next question, , Radius, The radius is one of the two long forearm bones that extends from the lateral side of the elbow to the, thumb side of the wrist. It has two expanded ends, of which the distal end is the larger. Key points, relating to its topography and relations are outlined below;, Upper end, , , , , Articular cartilage- covers medial > lateral side, Articulates with radial notch of the ulna by the annular ligament, Muscle attachment- biceps brachii at the tuberosity, , Shaft, Muscle attachment, , Upper third of the body, , Supinator, Flexor digitorum superficialis
Page 1274 :
Question 82 of 560, , A 25 year old man is stabbed in the upper arm. The brachial artery is lacerated at the level of the, proximal humerus, and is being repaired. A nerve lying immediately lateral to the brachial artery is, also lacerated. Which of the following is the nerve most likely to be?, , Ulnar nerve, , Median nerve, , Radial nerve, , Intercostobrachial nerve, , Axillary nerve, , Theme from April 2015 exam, The brachial artery begins at the lower border of teres major and terminates in the cubital fossa by, branching into the radial and ulnar arteries. In the upper arm the median nerve lies closest to it in the, lateral position. In the cubital fossa it lies medial to it.
Page 1275 :
Image sourced from Wikipedia, , Please rate this question:, , Discuss and give feedback, , Next question, , Brachial artery, The brachial artery begins at the lower border of teres major as a continuation of the axillary artery. It, terminates in the cubital fossa at the level of the neck of the radius by dividing into the radial and, ulnar arteries., Relations, Posterior relations include the long head of triceps with the radial nerve and profunda vessels, intervening. Anteriorly it is overlapped by the medial border of biceps., It is crossed by the median nerve in the middle of the arm., In the cubital fossa it is separated from the median cubital vein by the bicipital aponeurosis., The basilic vein is in contact at the most proximal aspect of the cubital fossa and lies medially., Next question
Page 1276 :
Question 83 of 560, , What is the course of the median nerve relative to the brachial artery in the upper arm?, , Medial to anterior to lateral, , Lateral to posterior to medial, , Medial to posterior to lateral, , Medial to anterior to medial, , Lateral to anterior to medial, Relations of median nerve to the brachial artery:, Lateral -> Anterior -> Medial, , Theme from 2009, 2012 and 2014 Exams, The median nerve descends lateral to the brachial artery, it usually passes anterior to the artery to, lie on its medial side. It passes deep to the bicipital aponeurosis and the median cubital vein at the, elbow. It enters the forearm between the two heads of the pronator teres muscle., , Image sourced from Wikipedia
Page 1277 :
Please rate this question:, , Discuss and give feedback, , Next question, , Brachial artery, The brachial artery begins at the lower border of teres major as a continuation of the axillary artery. It, terminates in the cubital fossa at the level of the neck of the radius by dividing into the radial and, ulnar arteries., Relations, Posterior relations include the long head of triceps with the radial nerve and profunda vessels, intervening. Anteriorly it is overlapped by the medial border of biceps., It is crossed by the median nerve in the middle of the arm., In the cubital fossa it is separated from the median cubital vein by the bicipital aponeurosis., The basilic vein is in contact at the most proximal aspect of the cubital fossa and lies medially., Next question
Page 1278 :
Question 84 of 560, , Which of the following is not a content of the cavernous sinus?, , Oculomotor nerve, , Internal carotid artery, , Opthalmic nerve, , Abducens nerve, , Optic nerve, Mnemonic for contents of cavernous sinus:, O TOM CAT, Occulomotor nerve (III), Trochlear nerve (IV), Ophthalmic nerve (V1), Maxillary nerve (V2), Carotid artery, Abducent nerve (VI), T, , OTOM=lateral wall components, CA= components within sinus, , The optic nerve lies above and outside the cavernous sinus., Please rate this question:, , Discuss and give feedback
Page 1279 :
Next question, , Cavernous sinus, The cavernous sinuses are paired and are situated on the body of the sphenoid bone. It runs from, the superior orbital fissure to the petrous temporal bone., Relations, Medial, , Lateral, , Pituitary fossa, Sphenoid sinus, , Temporal lobe, , Contents, , Lateral wall components, , (from top to bottom:), Oculomotor nerve, Trochlear nerve, Ophthalmic nerve, Maxillary nerve, , Contents of the sinus, , (from medial to lateral:), Internal carotid artery (and sympathetic plexus), Abducens nerve, , Blood supply, Ophthalmic vein, superficial cortical veins, basilar plexus of veins posteriorly., Drains into the internal jugular vein via: the superior and inferior petrosal sinuses
Page 1280 :
Image sourced from Wikipedia, , Next question
Page 1281 :
Question 85 of 560, Surgical occlusion of which of these structures, will result in the greatest reduction in hepatic blood, flow?, , Portal vein, , Common hepatic artery, , Right hepatic artery, , Coeliac axis, , Left hepatic artery, , The portal vein transports 70% of the blood supply to the liver, while the hepatic artery provides, 30%. The portal vein contains the products of digestion. The arterial and venous blood is dispersed, by sinusoids to the central veins of the liver lobules; these drain into the hepatic veins and then into, the IVC. The caudate lobe drains directly into the IVC rather than into other hepatic veins., Please rate this question:, , Discuss and give feedback, , Next question, , Liver, Structure of the liver, , Right lobe, , , , , Supplied by right hepatic artery, Contains Couinaud segments V to VIII (-/+Sg I), , Left lobe, , , , , Supplied by the left hepatic artery, Contains Couinaud segments II to IV (+/- Sg1), , Quadrate lobe, , , , , , , Part of the right lobe anatomically, functionally is part of the left, Couinaud segment IV, Porta hepatis lies behind, On the right lies the gallbladder fossa
Page 1282 :
Caudate lobe, , , , On the left lies the fossa for the umbilical vein, , , , , , , , Supplied by both right and left hepatic arteries, Couinaud segment I, Lies behind the plane of the porta hepatis, Anterior and lateral to the inferior vena cava, Bile from the caudate lobe drains into both right and left hepatic ducts, , Detailed knowledge of Couinaud segments is not required for MRCS, , , Between the liver lobules are portal canals which contain the portal triad: Hepatic Artery,, Portal Vein, tributary of Bile Duct., , Relations of the liver, , Anterior, , Postero inferiorly, , Diaphragm, , Oesophagus, , Xiphoid process, , Stomach, , Duodenum, , Hepatic flexure of colon, , Right kidney, , Gallbladder, , Inferior vena cava, , Porta hepatis
Page 1283 :
Location, , Postero inferior surface, it joins nearly at right angles with the left sagittal fossa, and, separates the caudate lobe behind from the quadrate lobe in front, , Transmits, , , , , , , , Common hepatic duct, Hepatic artery, Portal vein, Sympathetic and parasympathetic nerve fibres, Lymphatic drainage of the liver (and nodes), , Ligaments, , Falciform ligament, , , , , , 2 layer fold peritoneum from the umbilicus to anterior liver surface, Contains ligamentum teres (remnant umbilical vein), On superior liver surface it splits into the coronary and left, triangular ligaments, , Ligamentum teres, , Joins the left branch of the portal vein in the porta hepatis, , Ligamentum, venosum, , Remnant of ductus venosus, , Arterial supply, , , Hepatic artery, , Venous, , , , Hepatic veins, Portal vein, , Nervous supply, , , Sympathetic and parasympathetic trunks of coeliac plexus, Next question
Page 1284 :
Question 86 of 560, A 43 year old man is due to undergo an excision of the sub mandibular gland. Which of the following, incisions is the most appropriate for this procedure?, , A transversely orientated incision 4cm below the mandible, , A transversely orientated incision immediately inferior to the mandible, , A vertical incision 3 cm anterior to the angle of the mandible and extending inferiorly, , A transversely orientated incision 2cm above the mandible, , A transversely orientated incision 12cm below the mandible, , Theme from 2009 Exam, To access the sub mandibular gland a transverse incision 4cm below the mandible should be made., Incisions located higher than this may damage the marginal mandibular branch of the facial nerve., Please rate this question:, , Discuss and give feedback, , Next question, , Anterior triangle of the neck, Boundaries, , Anterior border of the Sternocleidomastoid, Lower border of mandible, Anterior midline, , Sub triangles (divided by Digastric above and Omohyoid), , , , , Muscular triangle: Neck strap muscles, Carotid triangle: Carotid sheath, Submandibular Triangle (digastric)
Page 1285 :
Contents of the anterior triangle, , Digastric triangle, , Submandibular gland, Submandibular nodes, Facial vessels, Hypoglossal nerve, , Muscular triangle, , Strap muscles, External jugular vein, , Carotid triangle, , Carotid sheath (Common carotid, vagus and internal jugular vein), Ansa cervicalis, , Nerve supply to digastric muscle, , , , Anterior: Mylohyoid nerve, Posterior: Facial nerve, , Image sourced from Wikipedia, , Next question
Page 1286 :
Question 87 of 560, A 5 year old boy presents with recurrent headaches. As part of his assessment he undergoes an, MRI scan of his brain. This demonstrates enlargement of the lateral and third ventricles. Where is, the most likely site of obstruction?, , Foramen of Luschka, , Foramen of Magendie, , Foramen of Munro, , Aqueduct of Sylvius, , None of the above, , Theme from September 2013 Exam, Theme from April 2014 exam, The CSF flows from the 3rd to the 4th ventricle via the Aqueduct of Sylvius., Please rate this question:, , Discuss and give feedback, , Next question, , Cerebrospinal fluid, The CSF fills the space between the arachnoid mater and pia mater (covering surface of the brain)., The total volume of CSF in the brain is approximately 150ml. Approximately 500 ml is produced by, the ependymal cells in the choroid plexus (70%), or blood vessels (30%). It is reabsorbed via the, arachnoid granulations which project into the venous sinuses., Circulation, 1. Lateral ventricles (via foramen of Munro), 2. 3rd ventricle, 3. Cerebral aqueduct (aqueduct of Sylvius), 4. 4th ventricle (via foramina of Magendie and Luschka), 5. Subarachnoid space, 6. Reabsorbed into the venous system via arachnoid granulations into superior sagittal sinus, Composition
Page 1287 :
, , , , , Glucose: 50-80mg/dl, Protein: 15-40 mg/dl, Red blood cells: Nil, White blood cells: 0-3 cells/ mm3, Next question
Page 1288 :
Question 88 of 560, A 23 year old man presents with appendicitis. A decision is made to perform an appendicectomy., The operation commences with a 5cm incision centered on McBurneys point. Which of the following, structures will be encountered first during the dissection?, , External oblique aponeurosis, , Internal oblique muscle, , Transversalis fascia, , Rectus sheath, , Peritoneum, , Theme from April 2014 exam, The external oblique will be encountered first in this location. The rectus sheath lies more medially., The external oblique muscle is the most superficial of the abdominal wall muscles. It originates from, the 5th to 12th ribs and passes inferomedially to insert into the linea alba, pubic tubercle and anterior, half of the iliac crest. It is innervated by the thoracoabdominal nerves (T7-T11) and sub costal, nerves., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal wall, The 2 main muscles of the abdominal wall are the rectus abdominis (anterior) and the quadratus, lumborum (posterior)., The remaining abdominal wall consists of 3 muscular layers. Each muscle passes from the lateral, aspect of the quadratus lumborum posteriorly to the lateral margin of the rectus sheath anteriorly., Each layer is muscular posterolaterally and aponeurotic anteriorly.
Page 1289 :
Image sourced from Wikipedia, , Muscles of abdominal wall, , External, oblique, , , , , , , , , Internal, oblique, , , , , , , Transversus, abdominis, , , , , , , , , , , Lies most superficially, Originates from 5th to 12th ribs, Inserts into the anterior half of the outer aspect of the iliac crest, linea, alba and pubic tubercle, More medially and superiorly to the arcuate line, the aponeurotic layer, overlaps the rectus abdominis muscle, The lower border forms the inguinal ligament, The triangular expansion of the medial end of the inguinal ligament is, the lacunar ligament., Arises from the thoracolumbar fascia, the anterior 2/3 of the iliac crest, and the lateral 2/3 of the inguinal ligament, The muscle sweeps upwards to insert into the cartilages of the lower 3, ribs, The lower fibres form an aponeurosis that runs from the tenth costal, cartilage to the body of the pubis, At its lowermost aspect it joins the fibres of the aponeurosis of, transversus abdominis to form the conjoint tendon., Innermost muscle, Arises from the inner aspect of the costal cartilages of the lower 6 ribs ,, from the anterior 2/3 of the iliac crest and lateral 1/3 of the inguinal, ligament, Its fibres run horizontally around the abdominal wall ending in an, aponeurosis. The upper part runs posterior to the rectus abdominis., Lower down the fibres run anteriorly only., The rectus abdominis lies medially; running from the pubic crest and, symphysis to insert into the xiphoid process and 5th, 6th and 7th costal, cartilages. The muscles lies in a aponeurosis as described above., Nerve supply: anterior primary rami of T7-12, , Surgical notes, During abdominal surgery it is usually necessary to divide either the muscles or their aponeuroses.
Page 1290 :
During a midline laparotomy it is desirable to divide the aponeurosis. This will leave the rectus, sheath intact above the arcuate line and the muscles intact below it. Straying off the midline will, often lead to damage to the rectus muscles, particularly below the arcuate line where they may often, be in close proximity to each other., Next question
Page 1291 :
Question 89 of 560, A 23 year old man is undergoing an inguinal hernia repair. The surgeons mobilise the spermatic cord, and place it in a hernia ring. A small slender nerve is identified superior to the cord. Which nerve is it, most likely to be?, , Iliohypogastric nerve, , Pudendal nerve, , Femoral branch of the genitofemoral nerve, , Ilioinguinal nerve, , Obturator nerve, , Theme from April 2014 exam, The ilioinguinal nerve passes through the inguinal canal and is the nerve most commonly identified, during hernia surgery. The genitofemoral nerve splits into two branches, the genital branch passes, through the inguinal canal within the cord structures. The femoral branch of the genitofemoral nerve, enters the thigh posterior to the inguinal ligament, lateral to the femoral artery. The iliohypogastric, nerve pierces the external oblique aponeurosis above the superficial inguinal ring., Please rate this question:, , Discuss and give feedback, , Next question, , Ilioinguinal nerve, Arises from the first lumbar ventral ramus with the iliohypogastric nerve. It passes inferolaterally, through the substance of psoas major and over the anterior surface of quadratus lumborum. It, pierces the internal oblique muscle and passes deep to the aponeurosis of the external oblique, muscle. It enters the inguinal canal and then passes through the superficial inguinal ring to reach the, skin., Branches, , , , To supply those muscles of the abdominal wall through which it passes., Skin and fascia over the pubic symphysis, superomedial part of the femoral triangle, surface, of the scrotum, root and dorsum of penis or labum majus in females.
Page 1292 :
Question 90 of 560, A 34 year old man undergoes excision of a sarcoma from the right buttock. During the procedure the, sciatic nerve is sacrificed. Which of the following will not occur as a result of this process?, , Loss of extension at the knee joint, , Foot drop, , Inability to extend extensor hallucis longus, , Loss of sensation to the posterior aspect of the thigh, , Loss of sensation to the posterior aspect of the lower leg, , Extension of the knee joint is caused by the obturator and femoral nerves., Please rate this question:, , Discuss and give feedback, , Next question, , Sciatic nerve, The sciatic nerve is formed from the sacral plexus and is the largest nerve in the body. It is the, continuation of the main part of the plexus arising from ventral rami of L4 to S3. These rami, converge at the inferior border of piriformis to form the nerve itself. It passes through the inferior part, of the greater sciatic foramen and emerges beneath piriformis. Medially, lie the inferior gluteal nerve, and vessels and the pudendal nerve and vessels. It runs inferolaterally under the cover of gluteus, maximus midway between the greater trochanter and ischial tuberosity. It receives its blood supply, from the inferior gluteal artery. The nerve provides cutaneous sensation to the skin of the foot and, the leg. It also innervates the posterior thigh muscles and the lower leg and foot muscles. The nerve, splits into the tibial and common peroneal nerves approximately half way down the posterior thigh., The tibial nerve supplies the flexor muscles and the common peroneal nerve supplies the extensor, muscles and the abductor muscles., Summary points, , Origin, , Spinal nerves L4 - S3
Page 1293 :
Articular Branches, , Hip joint, , Muscular branches in, upper leg, , , , , , , Semitendinosus, Semimembranosus, Biceps femoris, Part of adductor magnus, , Cutaneous sensation, , , , , , Posterior aspect of thigh (via cutaneous nerves), Gluteal region, Entire lower leg (except the medial aspect), , Terminates, , , , , At the upper part of the popliteal fossa by dividing into the tibial and, peroneal nerves, , The nerve to the short head of the biceps femoris comes from the common peroneal part of, the sciatic and the other muscular branches arise from the tibial portion., The tibial nerve goes on to innervate all muscles of the foot except the extensor digitorum, brevis (which is innervated by the common peroneal nerve)., Next question
Page 1294 :
Question 91 of 560, Where does the spinal cord terminate in neonates?, , L1, , L2, , L3, , L4, , L5, , Theme from 2009 Exam, Theme from January 2013 Exam, At the 3rd month the foetus's spinal cord occupies the entire length of the vertebral canal. The, vertebral column then grows longer exceeding the growth rate of the spinal cord. This results with, the cord being at L3 at birth and L1-2 by adulthood., Please rate this question:, , Discuss and give feedback, , Next question, , Spinal cord, , , , , Located in a canal within the vertebral column that affords it structural support., Rostrally it continues to the medulla oblongata of the brain and caudally it tapers at a level, corresponding to the L1-2 interspace (in the adult), a central structure, the filum terminale, anchors the cord to the first coccygeal vertebra., The spinal cord is characterised by cervico-lumbar enlargements and these, broadly, speaking, are the sites which correspond to the brachial and lumbar plexuses respectively., , There are some key points to note when considering the surgical anatomy of the spinal cord:, * During foetal growth the spinal cord becomes shorter than the spinal canal, hence the adult site of, cord termination at the L1-2 level., * Due to growth of the vertebral column the spine segmental levels may not always correspond to, bony landmarks as they do in the cervical spine.
Page 1295 :
* The spinal cord is incompletely divided into two symmetrical halves by a dorsal median, sulcus andventral median fissure. Grey matter surrounds a central canal that is continuous, rostrally with the ventricular system of the CNS., * The grey matter is sub divided cytoarchitecturally into Rexeds laminae., * Afferent fibres entering through the dorsal roots usually terminate near their point of entry but may, travel for varying distances in Lissauers tract. In this way they may establish synaptic connections, over several levels, * At the tip of the dorsal horn are afferents associated with nociceptive stimuli. The ventral horn, contains neurones that innervate skeletal muscle., The key point to remember when revising CNS anatomy is to keep a clinical perspective in mind. So, it is worth classifying the ways in which the spinal cord may become injured. These include:, , , , , , , , Trauma either direct or as a result of disc protrusion, Neoplasia either by direct invasion (rare) or as a result of pathological vertebral fracture, Inflammatory diseases such as Rheumatoid disease, or OA (formation of osteophytes, compressing nerve roots etc., Vascular either as a result of stroke (rare in cord) or as complication of aortic dissection, Infection historically diseases such as TB, epidural abscesses., , The anatomy of the cord will, to an extent dictate the clinical presentation. Some points/ conditions to, remember:, , , , , Brown- Sequard syndrome-Hemisection of the cord producing ipsilateral loss of, proprioception and upper motor neurone signs, plus contralateral loss of pain and, temperature sensation. The explanation of this is that the fibres decussate at different levels., Lesions below L1 will tend to present with lower motor neurone signs, Next question
Page 1296 :
Question 92 of 560, A 45 year old man is undergoing a low anterior resection for a carcinoma of the rectum. Which of the, following fascial structures will need to be divided to mobilise the mesorectum from the sacrum and, coccyx?, , Denonvilliers fascia, , Colles fascia, , Sibsons fascia, , Waldeyers fascia, , None of the above, Fascial layers surrounding the rectum:, , , , Anteriorly lies the fascia of Denonvilliers, Posteriorly lies Waldeyers fascia, , Waldeyers fascia separates the mesorectum from the sacrum and will need to be divided., Please rate this question:, , Discuss and give feedback, , Next question, , Rectum, The rectum is approximately 12 cm long. It is a capacitance organ. It has both intra and, extraperitoneal components. The transition between the sigmoid colon is marked by the, disappearance of the tenia coli.The extra peritoneal rectum is surrounded by mesorectal fat that also, contains lymph nodes. This mesorectal fatty layer is removed surgically during rectal cancer surgery, (Total Mesorectal Excision). The fascial layers that surround the rectum are important clinical, landmarks, anteriorly lies the fascia of Denonvilliers. Posteriorly lies Waldeyers fascia., Extra peritoneal rectum, , , Posterior upper third
Page 1297 :
, , , Posterior and lateral middle third, Whole lower third, , Relations, , Anteriorly (Males), , Rectovesical pouch, Bladder, Prostate, Seminal vesicles, , Anteriorly (Females), , Recto-uterine pouch (Douglas), Cervix, Vaginal wall, , Posteriorly, , Sacrum, Coccyx, Middle sacral artery, , Laterally, , Levator ani, Coccygeus, , Arterial supply, Superior rectal artery, Venous drainage, Superior rectal vein, Lymphatic drainage, , , , , Mesorectal lymph nodes (superior to dentate line), Internal iliac and then para-aortic nodes, Inguinal nodes (inferior to dentate line), Next question
Page 1298 :
Question 93 of 560, , What is the nerve supply to the muscle indicated by an X on the prosection below., , © Image provided by the University of Sheffield, , CN XI, , CN IX, , Median pectoral nerve, , Lateral pectoral nerve
Page 1299 :
Suprascapular nerve, Be careful not to confuse CN IX with CN XI, , The muscle indicated is trapezius and it is innervated by the accessory nerve (CN XI), Please rate this question:, , Discuss and give feedback, , Next question, , Trapezius, Origin, , Medial third of the superior nuchal line of the occiput, External occipital protruberance, Ligamentum nuchae, Spines of C7 and all thoracic vertebrae and all intervening interspinous ligaments, , Insertion, , Posterior border of the lateral third of the clavicle, Medial border of the acromion, Upper border of the crest of the spine of the scapula, , Nerve supply, , Spinal portion of the accessory nerve, , Actions, , Elevation of the shoulder girdle, Lateral rotation of the scapula, Next question, , v
Page 1300 :
Question 94 of 560, A 10 year old child has a grommet inserted for a glue ear. What type of epithelium is present on the, external aspect of the tympanic membrane?, , Stratified squamous, , Ciliated columnar, , Non ciliated columnar, , Non stratified squamous, , None of the above, , The external aspect of the tympanic membrane is lined by stratified squamous epithelium. This is, significant clinically in the development of middle ear infections when this type of epithelium may, migrate inside the middle ear., Please rate this question:, , Discuss and give feedback, , Next question, , Ear- anatomy, The ear is composed of three anatomically distinct regions., External ear, Auricle is composed of elastic cartilage covered by skin. The lobule has no cartilage and contains fat, and fibrous tissue., External auditory meatus is approximately 2.5cm long., Lateral third of the external auditory meatus is cartilaginous and the medial two thirds is bony., The region is innervated by the greater auricular nerve. The auriculotemporal branch of the, trigeminal nerve supplies most the of external auditory meatus and the lateral surface of the auricle., Middle ear, Space between the tympanic membrane and cochlea. The aditus leads to the mastoid air cells is the, route through which middle ear infections may cause mastoiditis. Anteriorly the eustacian tube
Page 1301 :
connects the middle ear to the naso pharynx., The tympanic membrane consists of:, , , , , Outer layer of stratified squamous epithelium., Middle layer of fibrous tissue., Inner layer of mucous membrane continuous with the middle ear., , The tympanic membrane is approximately 1cm in diameter., The chorda tympani nerve passes on the medial side of the pars flaccida., The middle ear is innervated by the glossopharyngeal nerve and pain may radiate to the middle ear, following tonsillectomy., Ossicles, Malleus attaches to the tympanic membrane (the Umbo)., Malleus articulates with the incus (synovial joint)., Incus attaches to stapes (another synovial joint)., Internal ear, Cochlea, semi circular canals and vestibule, Organ of corti is the sense organ of hearing and is located on the inside of the cochlear duct on the, basilar membrane., Vestibule accommodates the utricule and the saccule. These structures contain endolymph and are, surrounded by perilymph within the vestibule., The semicircular canals lie at various angles to the petrous temporal bone. All share a common, opening into the vestibule., Next question
Page 1302 :
Question 95 of 560, A 73 year old lady is admitted with acute mesenteric ischaemia. A CT angiogram is performed and a, stenotic lesion is noted at the origin of the superior mesenteric artery. At which of the following levels, does this branch from the aorta?, , L1, , L2, , L3, , L4, , L5, , Theme from January 2012 Exam, Theme from April 2014 exam, The SMA leaves the aorta at L1. It passes under the neck of the pancreas prior to giving its first, branch the inferior pancreatico-duodenal artery., Please rate this question:, , Discuss and give feedback, , Next question, , Superior mesenteric artery, , , , , Branches off aorta at L1, Supplies small bowel from duodenum (distal to ampulla of vater) through to mid transverse, colon, Takes more oblique angle from aorta and thus more likely to recieve emboli than coeliac axis, , Relations of superior mesenteric artery, Superiorly, , Neck of pancreas, , Postero-inferiorly, , Third part of duodenum, Uncinate process, , Posteriorly, , Left renal vein
Page 1303 :
Right, , Superior mesenteric vein, , Branches of the superior mesenteric artery, , , , , , , Inferior pancreatico-duodenal artery, Jejunal and ileal arcades, Ileo-colic artery, Right colic artery, Middle colic artery, , Overview of SMA and branches, , Image sourced from Wikipedia, , Next question
Page 1304 :
Question 96 of 560, The following statements relating to the musculocutaneous nerve are true except?, , It arises from the lateral cord of the brachial plexus, , It provides cutaneous innervation to the lateral side of the forearm, , If damaged, then extension of the elbow joint will be impaired, , It supplies the biceps muscle, , It runs beneath biceps, , It supplies biceps, brachialis and coracobrachialis. If damaged then elbow flexion will be impaired., Please rate this question:, , Discuss and give feedback, , Next question, , Musculocutaneous nerve, , , Branch of lateral cord of brachial plexus, , Path, , , , , , It penetrates the coracobrachialis muscle, Passes obliquely between the biceps brachii and the brachialis to the lateral side of the arm, Above the elbow it pierces the deep fascia lateral to the tendon of the biceps brachii, Continues into the forearm as the lateral cutaneous nerve of the forearm, , Innervates, , , , , , Coracobrachialis, Biceps brachii, Brachialis, Question 97 of 560
Page 1307 :
Foramen, , Location, , Contents, , Superior ophthalmic vein, , , *= In life the foramen lacerum is occluded by a cartilagenous plug. The ICA initially passes, into the carotid canal which ascends superomedially to enter the cranial cavity through the, foramen lacerum., Base of skull anatomical overview, , Image sourced from Wikipedia, , , , , Next question
Page 1308 :
Question 98 of 560, , Which of the cranial nerves listed below is least likely to carry parasympathetic fibres?, , III, , VII, , IX, , X, , II, Cranial nerves carrying parasympathetic fibres, X IX VII III (1973), , The parasympathetic functions served by the cranial nerves include:, III (oculomotor), , Pupillary constriction and accommodation, , VII (facial), , Lacrimal gland, submandibular and sublingual glands, , IX (glossopharyngeal), , Parotid, , X (vagus), , Heart and abdominal viscera, , The optic nerve carries no parasympathetic fibres., The cranial preganglionic parasympathetic nerves arise from specific nuclei in the CNS. These, synapse at one of four parasympathetic ganglia; otic, pterygopalatine, ciliary and submandibular., From these ganglia the parasympathetic nerves complete their journey to their target tissues via CN, V (trigeminal) branches (ophthalmic nerve CNV branch 1, Maxillary nerve CN V branch2, mandibular, nerve CN V branch 3), Please rate this question:
Page 1309 :
Discuss and give feedback, , Next question, , Cranial nerves, Cranial nerve lesions, , Olfactory nerve, , May be injured in basal skull fractures or involved in frontal lobe tumour extension., Loss of olfactory nerve function in relation to major CNS pathology is seldom an, isolated event and thus it is poor localiser of CNS pathology., , Optic nerve, , Problems with visual acuity may result from intra ocular disorders. Problems with, the blood supply such as amaurosis fugax may produce temporary visual distortion., More important surgically is the pupillary response to light. The pupillary size may, be altered in a number of disorders. Nerves involved in the resizing of the pupil, connect to the pretectal nucleus of the high midbrain, bypassing the lateral, geniculate nucleus and the primary visual cortex. From the pretectal nucleus, neurones pass to the Edinger - Westphal nucleus, motor axons from here pass along, with the oculomotor nerve. They synapse with ciliary ganglion neurones; the, parasympathetic axons from this then innervate the iris and produce miosis. The, miotic pupil is seen in disorders such as Horner's syndrome or opiate overdose., Mydriasis is the dilatation of the pupil in response to disease, trauma, drugs (or the, dark!). It is pathological when light fails to induce miosis. The radial muscle is, innervated by the sympathetic nervous system. Because the parasympathetic fibres, travel with the oculomotor nerve they will be damaged by lesions affecting this, nerve (e.g. cranial trauma)., The response to light shone in one eye is usually a constriction of both pupils. This, indicates intact direct and consensual light reflexes. When the optic nerve has an, afferent defect the light shining on the affected eye will produce a diminished, pupillary response in both eyes. Whereas light shone on the unaffected eye will, produce a normal pupillary response in both eyes. This is referred to as the Marcus, Gunn pupil and is seen in conditions such as optic neuritis. In a total CN II lesion, shining the light in the affected eye will produce no response., , Oculomotor nerve, , The pupillary effects are described above. In addition it supplies all ocular muscles, apart from lateral rectus and superior oblique. Thus the affected eye will be
Page 1310 :
deviated inferolaterally. Levator palpebrae superioris may also be impaired resulting, in impaired ability to open the eye., , Trochlear nerve, , The eye will not be able to look down., , Trigeminal nerve, , Largest cranial nerve. Exits the brainstem at the pons. Branches are ophthalmic,, maxillary and mandibular. Only the mandibular branch has both sensory and motor, fibres. Branches converge to form the trigeminal ganglion (located in Meckels cave)., It supplies the muscles of mastication and also tensor veli palatine, mylohyoid,, anterior belly of digastric and tensor tympani. The detailed descriptions of the, various sensory functions are described in other areas of the website. The corneal, reflex is important and is elicited by applying a small tip of cotton wool to the, cornea, a reflex blink should occur if it is intact. It is mediated by: the naso ciliary, branch of the ophthalmic branch of the trigeminal (sensory component) and the, facial nerve producing the motor response. Lesions of the afferent arc will produce, bilateral absent blink and lesions of the efferent arc will result in a unilateral absent, blink., , Abducens nerve, , The affected eye will have a deficit of abduction. This cranial nerve exits the, brainstem between the pons and medulla. It thus has a relatively long intra cranial, course which renders it susceptible to damage in raised intra cranial pressure., , Facial nerve, , Emerges from brainstem between pons and medulla. It controls muscles of facial, expression and taste from the anterior 2/3 of the tongue. The nerve passes into the, petrous temporal bone and into the internal auditory meatus. It then passes, through the facial canal and exits at the stylomastoid foramen. It passes through the, parotid gland and divides at this point. It does not innervate the parotid gland. Its, divisions are considered in other parts of the website. Its motor fibres innervate, orbicularis oculi to produce the efferent arm of the corneal reflex. In surgical, practice it may be injured during parotid gland surgery or invaded by malignancies, of the gland and a lower motor neurone on the ipsilateral side will result., , Vestibulo-cochlear, nerve, , Exits from the pons and then passes through the internal auditory meatus. It is, implicated in sensorineural hearing loss. Individuals with sensorineural hearing loss, will localise the sound in webers test to the normal ear. Rinnes test will be reduced, on the affected side but should still work. These two tests will distinguish, sensorineural hearing loss from conductive deafness. In the latter condition webers
Page 1311 :
test will localise to the affected ear and Rinnes test will be impaired on the affected, side. Surgical lesions affecting this nerve include CNS tumours and basal skull, fractures. It may also be damaged by the administration of ototoxic drugs (of which, gentamicin is the most commonly used in surgical practice)., , Glossopharyngeal, nerve, , Exits the pons just above the vagus. Receives sensory fibres from posterior 1/3, tongue, tonsils, pharynx and middle ear (otalgia may occur following tonsillectomy)., It receives visceral afferents from the carotid bodies. It supplies parasympathetic, fibres to the parotid gland via the otic ganglion and motor function to, stylopharyngeaus muscle. The sensory function of the nerve is tested using the gag, reflex., , Vagus nerve, , Leaves the medulla between the olivary nucleus and the inferior cerebellar, peduncle. Passes through the jugular foramen and into the carotid sheath. Details of, the functions of the vagus nerve are covered in the website under relevant organ, sub headings., , Accessory nerve, , Exists from the caudal aspect of the brainstem (multiple branches) supplies, trapezius and sternocleidomastoid muscles. The distal portion of this nerve is most, prone to injury during surgical procedures., , Hypoglossal nerve, , Emerges from the medulla at the preolivary sulcus, passes through the hypoglossal, canal. It lies on the carotid sheath and passes deep to the posterior belly of digastric, to supply muscles of the tongue (except palatoglossus). Its location near the carotid, sheath makes it vulnerable during carotid endarterectomy surgery and damage will, produce ipsilateral defect in muscle function., Next question
Page 1312 :
Question 99 of 560, , A 72 year old man is undergoing an open abdominal aortic aneurysm repair. The aneurysm is, located in a juxtarenal location and surgical access to the neck of aneurysm is difficult. Which of the, following structures may be divided to improve access?, , Cisterna chyli, , Transverse colon, , Left renal vein, , Superior mesenteric artery, , Coeliac axis, , The left renal vein will be stretched over the neck of the anuerysm in this location and is not, infrequently divided. This adds to the nephrotoxic insult of juxtarenal aortic surgery as a supra renal, clamp is also often applied. Deliberate division of the Cisterna Chyli will not improve access and will, result in a chyle leak. Division of the transverse colon will not help at all and would result in a high, risk of graft infection. Division of the SMA is pointless for a juxtarenal procedure., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal aorta, Abdominal aortic topography
Page 1314 :
Image sourced from Wikipedia, , Next question
Page 1315 :
Question 100 of 560, An occlusion of the anterior cerebral artery may compromise the blood supply to the following, structures except:, , Medial inferior surface of the frontal lobe, , Corpus callosum, , Medial surface of the frontal lobe, , Olfactory bulb, , Brocas area, , Brocas area is usually supplied by branches from the middle cerebral artery., Please rate this question:, , Discuss and give feedback, , Next question, , Circle of Willis, The two internal carotid arteries and two vertebral arteries form an anastomosis known as the Circle, of Willis on the inferior surface of the brain. Each half of the circle is formed by:, 1. Anterior communicating artery, 2. Anterior cerebral artery, 3. Internal carotid artery, 4. Posterior communicating artery, 5. Posterior cerebral arteries and the termination of the basilar artery, The circle and its branches supply; the corpus striatum, internal capsule, diencephalon and, midbrain.
Page 1316 :
Image sourced from Wikipedia, , Vertebral arteries, , , , , , Enter the cranial cavity via foramen magnum, Lie in the subarachnoid space, Ascend on anterior surface of medulla oblongata, Unite to form the basilar artery at the base of the pons, , Branches:, , , , , Posterior spinal artery, Anterior spinal artery, Posterior inferior cerebellar artery, , Basilar artery, Branches:
Page 1317 :
, , , , , , Anterior inferior cerebellar artery, Labyrinthine artery, Pontine arteries, Superior cerebellar artery, Posterior cerebral artery, , Internal carotid arteries, Branches:, , , , , , Posterior communicating artery, Anterior cerebral artery, Middle cerebral artery, Anterior choroid artery, Next question
Page 1319 :
Question 101 of 560, Parasympathetic fibres innervating the parotid gland originate from which of the following?, , Submandibular ganglion, , Otic ganglion, , Ciliary ganglion, , Pterygopalatine ganglion, , None of the above, , Theme from April 2014, Secretion of saliva by the parotid gland is controlled by postsynaptic parasympathetic fibres, originating in the inferior salivatory nucleus; these leave the brain via the tympanic nerve (branch of, glossopharyngeal nerve (CN IX), travel through the tympanic plexus (located in the middle ear), and, then form the lesser petrosal nerve until reaching the otic ganglion. After synapsing in the Otic, ganglion, the postganglionic (postsynaptic) fibres travel as part of the auriculotemporal nerve (a, branch of the mandibular nerve (V3) to reach the parotid gland., Please rate this question:, , Discuss and give feedback, , Next question, , Parotid gland, Anatomy of the parotid gland, , Location, , Overlying the mandibular ramus; anterior and inferior to the ear., , Salivary duct, , Crosses the masseter, pierces the buccinator and drains adjacent to the, 2nd upper molar tooth (Stensen's duct)., , Structures passing, through the gland, , , , , Facial nerve (Mnemonic: The Zebra Buggered My Cat; Temporal, Zygomatic, Buccal, Mandibular, Cervical), External carotid artery
Page 1320 :
Relations, , , , , Retromandibular vein, Auriculotemporal nerve, , , , Anterior: masseter, medial pterygoid, superficial temporal and, maxillary artery, facial nerve, stylomandibular ligament, Posterior: posterior belly digastric muscle, sternocleidomastoid,, stylohyoid, internal carotid artery, mastoid process, styloid, process, , , , Arterial supply, , Branches of external carotid artery, , Venous drainage, , Retromandibular vein, , Lymphatic drainage, , Deep cervical nodes, , Nerve innervation, , , , , , Parasympathetic-Secretomotor, Sympathetic-Superior cervical ganglion, Sensory- Greater auricular nerve, , Parasympathetic stimulation produces a water rich, serous saliva. Sympathetic stimulation leads to, the production of a low volume, enzyme-rich saliva., Next question
Page 1322 :
Arch of the Aorta, , 22.5cm, , Left principal bronchus, , 27cm, , Diaphragmatic hiatus, , 40cm, , Relations, , Anteriorly, , , , , , , Trachea to T4, Recurrent laryngeal nerve, Left bronchus, Left atrium, Diaphragm, , Posteriorly, , , , , , , Thoracic duct to left at T5, Hemiazygos to the left T8, Descending aorta, First 2 intercostal branches of aorta, , Left, , , , , Thoracic duct, Left subclavian artery, , Right, , , , Azygos vein, , Arterial, venous and lymphatic drainage of the oesophagus, , Artery, , Vein, , Lymphatics, , Muscularis externa, , Upper, third, , Inferior, thyroid, , Inferior thyroid, , Deep, cervical, , Striated muscle, , Mid third, , Aortic, branches, , Azygos branches, , Mediastinal, , Smooth & striated, muscle, , Lower, third, , Left gastric, , Posterior mediastinal and, coeliac, , Gastric, , Smooth muscle
Page 1324 :
Question 103 of 560, Which of the following structures suspends the spinal cord in the dural sheath?, , Filum terminale, , Conus medullaris, , Ligamentum flavum, , Denticulate ligaments, , Anterior longitudinal ligament, , The spinal cord is approximately 45cm in men and 43cm in women. The denticulate ligament is a, continuation of the pia mater (innermost covering of the spinal cord) which has intermittent lateral, projections attaching the spinal cord to the dura mater., Please rate this question:, , Discuss and give feedback, , Next question, , Spinal cord, , , , , Located in a canal within the vertebral column that affords it structural support., Rostrally it continues to the medulla oblongata of the brain and caudally it tapers at a level, corresponding to the L1-2 interspace (in the adult), a central structure, the filum terminale, anchors the cord to the first coccygeal vertebra., The spinal cord is characterised by cervico-lumbar enlargements and these, broadly, speaking, are the sites which correspond to the brachial and lumbar plexuses respectively., , There are some key points to note when considering the surgical anatomy of the spinal cord:, * During foetal growth the spinal cord becomes shorter than the spinal canal, hence the adult site of, cord termination at the L1-2 level., * Due to growth of the vertebral column the spine segmental levels may not always correspond to, bony landmarks as they do in the cervical spine., * The spinal cord is incompletely divided into two symmetrical halves by a dorsal median
Page 1325 :
sulcus andventral median fissure. Grey matter surrounds a central canal that is continuous, rostrally with the ventricular system of the CNS., * The grey matter is sub divided cytoarchitecturally into Rexeds laminae., * Afferent fibres entering through the dorsal roots usually terminate near their point of entry but may, travel for varying distances in Lissauers tract. In this way they may establish synaptic connections, over several levels, * At the tip of the dorsal horn are afferents associated with nociceptive stimuli. The ventral horn, contains neurones that innervate skeletal muscle., The key point to remember when revising CNS anatomy is to keep a clinical perspective in mind. So, it is worth classifying the ways in which the spinal cord may become injured. These include:, , , , , , , , Trauma either direct or as a result of disc protrusion, Neoplasia either by direct invasion (rare) or as a result of pathological vertebral fracture, Inflammatory diseases such as Rheumatoid disease, or OA (formation of osteophytes, compressing nerve roots etc., Vascular either as a result of stroke (rare in cord) or as complication of aortic dissection, Infection historically diseases such as TB, epidural abscesses., , The anatomy of the cord will, to an extent dictate the clinical presentation. Some points/ conditions to, remember:, , , , , Brown- Sequard syndrome-Hemisection of the cord producing ipsilateral loss of, proprioception and upper motor neurone signs, plus contralateral loss of pain and, temperature sensation. The explanation of this is that the fibres decussate at different levels., Lesions below L1 will tend to present with lower motor neurone signs, Next question
Page 1326 :
Question 104 of 560, , Where is the 'safe triangle' for chest drain insertion located?, , 4th intercostal space, mid axillary line, , 5th intercostal space, mid axillary line, , 4th intercostal space, mid scapular line, , 5th intercostal space, mid scapular line, , 4th intercostal space, mid clavicular line, 'Safe Triangle' for chest drain insertion:, 5th intercostal space, mid axillary line, , Theme from April 2012 exam, Please rate this question:, , Discuss and give feedback, , Next question, , Chest drains, There are a number of different indications for chest drain insertion. In general terms large bore, chest drains are preferred for trauma and haemothorax drainage. Smaller diameter chest drains can, be used for pneumothorax or pleural effusion drainage., Insertion can be performed either using anatomical guidance or through ultrasound guidance. In the, exam, the anatomical method is usually tested.
Page 1327 :
It is advised that chest drains are placed in the 'safe triangle'. The triangle is located in the mid, axillary line of the 5th intercostal space. It is bordered by:, Anterior edge latissimus dorsi, the lateral border of pectoralis major, a line superior to the horizontal, level of the nipple, and the apex below the axilla., Another triangle is situated behind the scapula. It is bounded above by the trapezius, below by the, latissimus dorsi, and laterally by the vertebral border of the scapula; the floor is partly formed by the, rhomboid major. If the scapula is drawn forward by folding the arms across the chest, and the trunk, bent forward, parts of the sixth and seventh ribs and the interspace between them become, subcutaneous and available for auscultation. The space is therefore known as the triangle of, auscultation., References, Prof Harold Ellis. The applied anatomy of chest drains insertions. British Journal of hospital medicine, 2007; (68): 44-45., Laws D, Neville E, Duffy J. BTS guidelines for insertion of chest drains. Thorax, 2003; (58): 53-59., Next question
Page 1328 :
Question 105 of 560, , Your consultant decides to perform an open inguinal hernia repair under local anaesthesia. Which of, the following dermatomal levels will require blockade?, , T10, , T12, , T11, , S1, , S2, , Theme from April 2012 Exam, Please rate this question:, , Discuss and give feedback, , Next question, , Dermatomes, The common dermatomal levels and cutaneous nerves responsible for them is illustrated below.
Page 1329 :
Image sourced from Wikipedia, , Next question
Page 1330 :
Question 106 of 560, A 44 year old man is undergoing a parotidectomy and the surgeon is carefully preserving the facial, nerve. Unfortunately his trainee then proceeds to divide it. Which of the following will not be affected, as a result?, , Taste sensation from anterior two thirds of the tongue, , Closing the ipsilateral eyelid, , Raising the ipsilateral side of the lip, , Ipsilateral corneal reflex, , None of the above, , Theme from April 2014 exam, The chorda tympani branches inside the facial canal and will therefore be unaffected by this most, unfortunate event! The corneal reflex is mediated by the opthalmic branch of the trigeminal nerve, sensing the stimulus on the cornea, lid or conjunctiva; the facial nerve initiates the motor response of, the reflex., Please rate this question:, , Discuss and give feedback, , Next question, , Facial nerve, The facial nerve is the main nerve supplying the structures of the second embryonic branchial arch., It is predominantly an efferent nerve to the muscles of facial expression, digastric muscle and also to, many glandular structures. It contains a few afferent fibres which originate in the cells of its genicular, ganglion and are concerned with taste., Supply - 'face, ear, taste, tear', , , , , , Face: muscles of facial expression, Ear: nerve to stapedius, Taste: supplies anterior two-thirds of tongue, Tear: parasympathetic fibres to lacrimal glands, also salivary glands
Page 1331 :
Path, Subarachnoid path, , , , Origin: motor- pons, sensory- nervus intermedius, Pass through the petrous temporal bone into the internal auditory meatus with the, vestibulocochlear nerve. Here they combine to become the facial nerve., , Facial canal path, , , , The canal passes superior to the vestibule of the inner ear, At the medial aspect of the middle ear, it becomes wider and contains the geniculate, ganglion., , - 3 branches:, 1. greater petrosal nerve, 2. nerve to stapedius, 3. chorda tympani, Stylomastoid foramen, , , , Passes through the stylomastoid foramen (tympanic cavity anterior and mastoid antrum, posteriorly), Posterior auricular nerve and branch to posterior belly of digastric and stylohyoid muscle, , Face, Enters parotid gland and divides into 5 branches:, , , , , , , Temporal branch, Zygomatic branch, Buccal branch, Marginal mandibular branch, Cervical branch, Next question
Page 1332 :
Question 107 of 560, , A 45 year old lady develops severe back pain and on examination is found to have clinical evidence, of an L5/ S1 radiculopathy. Her symptoms deteriorate and eventually a laminectomy is performed., During a posterior surgical approach the surgeons encounter a tough ligamentous structure lying, anterior to the spinous processes. This structure is most likely to be the, , Transverse spinal ligament, , Supraspinal ligament, , Anterior longitudinal ligament, , Ligamentum flavum, , Posterior longitudinal ligament, , The ligamentum lies in this position, as illustrated below:
Page 1333 :
Image sourced from Wikipedia, , Please rate this question:, , Discuss and give feedback, , Next question, , Vertebral column, , , , There are 7 cervical, 12 thoracic, 5 lumbar, and 5 sacral vertebrae., The spinal cord segmental levels do not necessarily correspond to the vertebral segments., For example, while the C1 cord is located at the C1 vertebra, the C8 cord is situated at the, C7 vertebra. While the T1 cord is situated at the T1 vertebra, the T12 cord is situated at the, T8 vertebra. The lumbar cord is situated between T9 and T11 vertebrae. The sacral cord is, situated between the T12 to L2 vertebrae., , Cervical vertebrae, The interface between the first and second vertebra is called the atlanto-axis junction. The C3 cord, contains the phrenic nucleus., , Muscle, , Nerve root value
Page 1334 :
Muscle, , Nerve root value, , Deltoid, , C5,6, , Biceps, , C5,6, , Wrist extensors, , C6-8, , Triceps, , C6-8, , Wrist flexors, , C6-T1, , Hand muscles, , C8-T1, , Thoracic vertebrae, The thoracic vertebral segments are defined by those that have a rib. The spinal roots form the, intercostal nerves that run on the bottom side of the ribs and these nerves control the intercostal, muscles and associated dermatomes., Lumbosacral vertebrae, Form the remainder of the segments below the vertebrae of the thorax. The lumbosacral spinal cord,, however, starts at about T9 and continues only to L2. It contains most of the segments that innervate, the hip and legs, as well as the buttocks and anal regions., Cauda Equina, The spinal cord ends at L1-L2 vertebral level. The tip of the spinal cord is called the conus. Below, the conus, there is a spray of spinal roots that is called the cauda equina. Injuries below L2, represent injuries to spinal roots rather than the spinal cord proper., Next question
Page 1335 :
Question 108 of 560, Which of the following does not pass through the superior orbital fissure?, , Lacrimal nerve, , Abducens nerve, , Opthalmic artery, , Trochlear nerve, , Superior opthalmic vein, Mnemonic for the nerves passing through the supraorbital fissure:, Live Frankly To See Absolutely No Insult, Lacrimal, Frontal, Trochlear, Superior Division of Oculomotor, Abducens, Nasociliary, Inferior Division of Oculomotor nerve, Theme from September 2015 Exam, Theme from April 2014 exam, The opthalmic artery arises from the internal carotid immediately after it has pierced the dura and, arachnoid. It runs through the optic canal below the optic nerve and within its dural and arachnoid, sheaths. It terminates as the supratrochlear and dorsal nasal arteries., Please rate this question:, , Discuss and give feedback, , Next question, , Foramina of the base of the skull, Foramen, , Location, , Contents
Page 1337 :
Foramen, , Location, , Contents, , Abducent nerve (VI), Superior ophthalmic vein, , *= In life the foramen lacerum is occluded by a cartilagenous plug. The ICA initially passes into the, carotid canal which ascends superomedially to enter the cranial cavity through the foramen lacerum., Base of skull anatomical overview, , Image sourced from Wikipedia, , Next question
Page 1338 :
Question 109 of 560, , An 18 year old man undergoes a tonsillectomy for attacks of recurrent acute tonsillitis. Whilst in, recovery he develops a post operative haemorrhage. Which of the following vessels is the most, likely culprit?, , Facial vein, , External palatine vein, , External carotid artery, , Internal jugular vein, , None of the above, , The external palatine vein lies immediately lateral to the tonsil and if damaged may be a cause of, reactionary haemorrhage following tonsillectomy., Please rate this question:, , Discuss and give feedback, , Next question, , Tonsil, Anatomy, , , , , Each palatine tonsil has two surfaces, a medial surface which projects into the pharynx and a, lateral surface that is embedded in the wall of the pharynx., They are usually 25mm tall by 15mm wide, although this varies according to age and may be, almost completely atrophied in the elderly.
Page 1339 :
, , , , Their arterial supply is from the tonsillar artery, a branch of the facial artery., Its veins pierce the constrictor muscle to join the external palatine or facial veins. The, external palatine vein is immediately lateral to the tonsil, which may result in haemorrhage, during tonsillectomy., Lymphatic drainage is the jugulodigastric node and the deep cervical nodes., , Tonsillitis, , , , , Usually bacterial (50%)- group A Streptococcus. Remainder viral., May be complicated by development of abscess (quinsy). This may distort the uvula., , - Indications for tonsillectomy include recurrent acute tonsillitis, suspected malignancy, enlargement, causing sleep apnoea., - Dissection tonsillectomy is the preferred technique with haemorrhage being the commonest, complication. Delayed otalgia may occur owing to irritation of the glossopharyngeal nerve., Next question
Page 1340 :
Question 110 of 560, A patient is found to have an ischaemic left colon. Which artery arising from the aorta at around the, level of L3 is most likely to account for this situation?, , Superior mesenteric artery, , Inferior mesenteric artery, , Superior rectal artery, , Ileocolic artery, , Middle colic artery, , Theme from January 2013 Exam, Theme from April 2014 exam, Only the IMA is likely to affect the left side of the colon and originate at L3., Please rate this question:, , Discuss and give feedback, , Next question, , Inferior mesenteric artery, The IMA is the main arterial supply of the embryonic hindgut and originates approximately 3-4 cm, superior to the aortic bifurcation. From its aortic origin it passes immediately inferiorly across the, anterior aspect of the aorta to eventually lie on its left hand side. At the level of the left common iliac, artery it becomes the superior rectal artery., Branches, The left colic artery arises from the IMA near its origin. More distally up to three sigmoid arteries will, exit the IMA to supply the sigmoid colon., Next question
Page 1342 :
Question 112 of 560, A 24 year old lady is stabbed in the buttock. Following the injury the wound is sutured in the, emergency department. Eight weeks later she attends the clinic, as she walks into the clinic room, she has a waddling gait and difficulty with thigh abduction. On examination she has buttock muscle, wasting. Which nerve has been injured?, , Superior gluteal nerve, , Obturator nerve, , Sciatic nerve, , Femoral nerve, , Inferior gluteal nerve, , Theme from April 2016 Exam, Damage to the superior gluteal nerve will result in a Trendelenburg gait., Please rate this question:, , Discuss and give feedback, , Next question, , Trendelenburg test, Injury or division of the superior gluteal nerve results in a motor deficit that consists of weakened, abduction of the thigh by gluteus medius, a disabling gluteus medius limp and a compensatory list of, the body to the weakened gluteal side. The compensation results in a gravitational shift so that the, body is supported on the unaffected limb., When a person is asked to stand on one leg, the gluteus medius usually contracts as soon as the, contralateral leg leaves the floor, preventing the pelvis from dipping towards the unsupported side., When a person with paralysis of the superior gluteal nerve is asked to stand on one leg, the pelvis, on the unsupported side descends, indicating that the gluteus medius on the affected side is weak or, non functional ( a positive Trendelenburg test)., This eponymous test also refers to a vascular investigation in which tourniquets are placed around, the upper thigh, these can help determine whether saphenofemoral incompetence is present., Next question, Question 113 of 560
Page 1343 :
At which level is the hilum of the left kidney located?, , L1, , L2, , T12, , T11, , L3, Remember L1 ('left one') is the level of the hilum of the left kidney, Theme from April 2012 exam, Theme from April 2014, Please rate this question:, , Discuss and give feedback, , Next question, , Renal anatomy, Each kidney is about 11cm long, 5cm wide and 3cm thick. They are located in a deep gutter, alongside the projecting vertebral bodies, on the anterior surface of psoas major. In most cases the, left kidney lies approximately 1.5cm higher than the right. The upper pole of both kidneys, approximates with the 11th rib (beware pneumothorax during nephrectomy). On the left hand side, the hilum is located at the L1 vertebral level and the right kidney at level L1-2. The lower border of, the kidneys is usually alongside L3., The table below shows the anatomical relations of the kidneys:, Relations, , Relations, , Right Kidney, , Left Kidney, , Posterior, , Quadratus lumborum, diaphragm, psoas, major, transversus abdominis, , Quadratus lumborum, diaphragm, psoas, major, transversus abdominis
Page 1344 :
Relations, , Right Kidney, , Left Kidney, , Anterior, , Hepatic flexure of colon, , Stomach, Pancreatic tail, , Superior, , Liver, adrenal gland, , Spleen, adrenal gland, , Fascial covering, Each kidney and suprarenal gland is enclosed within a common layer of investing fascia, derived, from the transversalis fascia. It is divided into anterior and posterior layers (Gerotas fascia)., Renal structure, Kidneys are surrounded by an outer cortex and an inner medulla which usually contains between 6, and 10 pyramidal structures. The papilla marks the innermost apex of these. They terminate at the, renal pelvis, into the ureter., Lying in a hollow within the kidney is the renal sinus. This contains:, 1. Branches of the renal artery, 2. Tributaries of the renal vein, 3. Major and minor calyces's, 4. Fat, Structures at the renal hilum, The renal vein lies most anteriorly, then renal artery (it is an end artery) and the ureter lies most, posterior., Next question
Page 1345 :
Question 114 of 560, During a radical neck dissection, division of which of the following fascial layers will expose the ansa, cervicalis?, , Pretracheal fascia, , Carotid sheath, , Prevertebral fascia, , Investing layer of fascia, , Sibsons fascia, , The ansa cervicalis lies anterior to the carotid sheath. It may be exposed by division of the, pretracheal fascia at the posterolateral aspect of the thyroid gland. The pre vertebral fascia lies more, posteriorly and division of the investing layer of fascia will not expose this nerve., Please rate this question:, , Discuss and give feedback, , Next question, , Ansa cervicalis, Superior, root, , Branch of C1 anterolateral to carotid sheath, , Inferior root, , Derived from C2 and C3 roots, passes posterolateral to the internal jugular vein, (may lie either deep or superficial to it), , Innervation, , Sternohyoid, Sternothyroid, Omohyoid
Page 1346 :
The ansa cervicalis lies anterior to the carotid sheath. The nerve supply to the inferior strap muscles, enters at their inferior aspect. Therefore when dividing these muscles to expose a large goitre, the, muscles should be divided in their upper half., , Image sourced from Wikipedia, , Next question
Page 1347 :
Question 115 of 560, , A 73 year old lady presents with symptoms of faecal incontinence. On examination she has weak, anal sphincter muscles. What are the main nerve root values of the nerves supplying the external, anal sphincter?, , S2,3, , L5, S1, , S4,5, , S5, , S2,3,4, S2, 3, 4 Keeps the poo off the floor, , Theme from April 2015Exam, The external anal sphincter is innervated by the inferior rectal branch of the pudendal nerve, this has, root values of S2, 3 and the perineal branch of S4., Please rate this question:, , Discuss and give feedback, , Next question, , Anal sphincter, , , Internal anal sphincter composed of smooth muscle continuous with the circular muscle of, the rectum. It surrounds the upper two- thirds of the anal canal and is supplied by, sympathetic nerves.
Page 1348 :
, , , External anal sphincter is composed of striated muscle which surrounds the internal, sphincter but extends more distally., The nerve supply of the external anal sphincter is from the inferior rectal branch of the, pudendal nerve (S2 and S3) and the perineal branch of the S4 nerve roots., , Image showing relationship of internal and external anal sphincters, , Image sourced from Wikipedia, , Next question
Page 1349 :
Question 116 of 560, , A 22 year old falls over and lands on a shard of glass. It penetrates the palmar aspect of his hand,, immediately lateral to the pisiform bone. Which of the following structures is most likely to be, injured?, , Palmar cutaneous branch of the median nerve, , Lateral tendons of flexor digitorum superficialis, , Ulnar artery, , Flexor carpi radialis tendons, , Lateral tendons of flexor digitorum profundus, , The ulnar nerve and artery are at most immediate risk in this injury. This is illustrated in the image, below:
Page 1350 :
Image sourced from Wikipedia, , Please rate this question:, , Discuss and give feedback, , Next question, , Hand, Anatomy of the hand, , Bones, , , , , 8 Carpal bones, 5 Metacarpals
Page 1352 :
Image sourced from Wikipedia, , Fascia and compartments of the palm, The fascia of the palm is continuous with the antebrachial fascia and the fascia of the dorsum of the, hand. The palmar fascia is thin over the thenar and hypothenar eminences. In contrast the palmar, fascia is relatively thick. The palmar aponeurosis covers the soft tissues and overlies the flexor, tendons. The apex of the palmar aponeurosis is continuous with the flexor retinaculum and the, palmaris longus tendon. Distally, it forms four longitudinal digital bands that attach to the bases of, the proximal phalanges, blending with the fibrous digital sheaths., A medial fibrous septum extends deeply from the medial border of the palmar aponeurosis to the 5th, metacarpal. Lying medial to this are the hypothenar muscles. In a similar fashion, a lateral fibrous, septum extends deeply from the lateral border of the palmar aponeurosis to the 3rd metacarpal. The, thenar compartment lies lateral to this area., Lying between the thenar and hypothenar compartments is the central compartment. It contains the, flexor tendons and their sheaths, the lumbricals, the superficial palmar arterial arch and the digital, vessels and nerves., The deepest muscular plane is the adductor compartment, which contains adductor pollicis., Short muscles of the hand, These comprise the lumbricals and interossei. The four slender lumbrical muscles flex the fingers at, the metacarpophalangeal joints and extend the interphalangeal joint. The four dorsal interossei are, located between the metacarpals and the four palmar interossei lie on the palmar surface of the, metacarpals in the interosseous compartment of the hand.
Page 1353 :
Long flexor tendons and sheaths in the hand, The tendons of FDS and FDP enter the common flexor sheath deep to the flexor retinaculum. The, tendons enter the central compartment of the hand and fan out to their respective digital synovial, sheaths. Near the base of the proximal phalanx, the tendon of FDS splits to permit the passage of, FDP. The FDP tendons are attached to the margins of the anterior aspect of the base of the distal, phalanx., The fibrous digital sheaths contain the flexor tendons and their synovial sheaths. These extend from, the heads of the metacarpals to the base of the distal phalanges., Next question
Page 1354 :
Question 117 of 560, , A 72 year old man has a fall. He is found to have a fractured neck of femur and goes on to have a, left hip hemiarthroplasty. Two months post operatively he is found to have an odd gait. When, standing on his left leg his pelvis dips on the right side. There is no foot drop. What is the cause?, , Sciatic nerve damage, , L5 radiculopathy, , Inferior gluteal nerve damage, , Previous poliomyelitis, , Superior gluteal nerve damage, , Theme from 2010 exam, Theme from April 2014 exam, This patient has a trendelenburg gait caused by damage to the superior gluteal nerve causing, weakness of the abductor muscles. Classically a patient is asked to stand on one leg and the pelvis, dips on the opposite side. The absence of a foot drop excludes the possibility of polio or L5, radiculopathy., Please rate this question:, , Discuss and give feedback, , Next question, , Gluteal region, Gluteal muscles
Page 1356 :
Question 118 of 560, , Which of the following structures lies posterior to the femoral nerve in the femoral triangle?, , Adductor longus, , Pectineus, , Psoas major, , Iliacus, , None of the above, , The iliacus lies posterior to the femoral nerve in the femoral triangle. The femoral sheath lies anterior, to the iliacus and pectineus muscles., Please rate this question:, , Discuss and give feedback, , Next question, , Femoral nerve, Root values, , Innervates, , L2, 3, 4, , , , , , Pectineus, Sartorius, Quadriceps femoris
Page 1357 :
Branches, , , , Vastus lateralis/medialis/intermedius, , , , , , Medial cutaneous nerve of thigh, Saphenous nerve, Intermediate cutaneous nerve of thigh, , Path, Penetrates psoas major and exits the pelvis by passing under the inguinal ligament to enter the, femoral triangle, lateral to the femoral artery and vein., , Image sourced from Wikipedia, , Mnemonic for femoral nerve supply, (don't) M I S V Q Scan for PE
Page 1359 :
Question 119 of 560, You are assisting in an open right adrenalectomy for a large adrenal adenoma. The consultant is, distracted and you helpfully pull the adrenal into the wound to improve the view. Unfortunately this is, followed by brisk bleeding. The vessel responsible for this is most likely to be:, , Portal vein, , Phrenic vein, , Right renal vein, , Superior mesenteric vein, , Inferior vena cava, , Theme from April 2014 exam, It drains directly via a very short vessel. If the sutures are not carefully tied then it may be avulsed off, the IVC. An injury best managed using a Satinsky clamp and a 6/0 prolene suture., Please rate this question:, , Discuss and give feedback, , Next question, , Adrenal gland anatomy, Anatomy, , Location, , Superomedially to the upper pole of each kidney, , Relationships of the, right adrenal, , Diaphragm-Posteriorly, Kidney-Inferiorly, Vena Cava-Medially,, Hepato-renal pouch and bare area of the liver-Anteriorly, , Relationships of the left, adrenal, , Crus of the diaphragm-Postero- medially, Pancreas and splenic, vessels-Inferiorly, Lesser sac and stomach-Anteriorly
Page 1360 :
Arterial supply, , Superior adrenal arteries- from inferior phrenic artery, Middle adrenal, arteries - from aorta, Inferior adrenal arteries -from renal arteries, , Venous drainage of the, right adrenal, , Via one central vein directly into the IVC, , Venous drainage of the, left adrenal, , Via one central vein into the left renal vein, , Next question
Page 1361 :
Question 120 of 560, A 28 year old lady requires an episiotomy for a ventouse vaginal delivery. Which of the nerves listed, below will usually be anaesthetised to allow the episiotomy?, , Femoral, , Ilioinguinal, , Pudendal, , Genitofemoral, , Sacral plexus, , Theme from April 2015 Exam, The pudendal nerve innervates the posterior vulval area and is routinely blocked in procedures such, as episiotomy., Please rate this question:, , Discuss and give feedback, , Next question, , Pudendal nerve, The pudendal nerve arises from nerve roots S2, S3 and S4 and exits the pelvis through the greater, sciatic foramen. It re-enters the perineum through the lesser sciatic foramen. It travels inferior to give, innervation to the anal sphincters and external urethral sphincter. It also provides cutaneous, innervation to the region of perineum surrounding the anus and posterior vulva., Traction and compression of the pudendal nerve by the foetus in late pregnancy may result in late, onset pudendal neuropathy which may be part of the process involved in the development of faecal, incontinence., Next question
Page 1362 :
Question 121 of 560, , A motorcyclist is involved in a road traffic accident. He suffers a complex humeral shaft fracture, which is plated. Post operatively he complains of an inability to extend his fingers. Which of the, following structures is most likely to have been injured?, , Ulnar nerve, , Radial nerve, , Median nerve, , Axillary nerve, , None of the above, Mnemonic for radial nerve muscles: BEST, B rachioradialis, E xtensors, S upinator, T riceps, , The radial nerve is responsible for innervation of the extensor compartment of the forearm., Please rate this question:, , Discuss and give feedback, , Next question, , Radial nerve
Page 1363 :
Continuation of posterior cord of the brachial plexus (root values C5 to T1), Path, , , , , , , , , In the axilla: lies posterior to the axillary artery on subscapularis, latissimus dorsi and teres, major., Enters the arm between the brachial artery and the long head of triceps (medial to humerus)., Spirals around the posterior surface of the humerus in the groove for the radial nerve., At the distal third of the lateral border of the humerus it then pierces the intermuscular, septum and descends in front of the lateral epicondyle., At the lateral epicondyle it lies deeply between brachialis and brachioradialis where it then, divides into a superficial and deep terminal branch., Deep branch crosses the supinator to become the posterior interosseous nerve., , In the image below the relationships of the radial nerve can be appreciated, , Image sourced from Wikipedia, , Regions innervated, , Motor (main nerve), , , , , , Triceps, Anconeus, Brachioradialis
Page 1365 :
Image sourced from Wikipedia, , Next question
Page 1366 :
Question 122 of 560, , An enthusiastic surgical registrar undertakes his first solo splenectomy. The operation is far more, difficult than anticipated and the registrar leaves a tube drain to the splenic bed at the end of the, procedure. Over the following 24 hours approximately 500ml of clear fluid has entered the drain., Biochemical testing of the fluid is most likely to reveal:, , Elevated creatinine, , Elevated triglycerides, , Elevated glucagon, , Elevated amylase, , None of the above, , During splenectomy the tail of the pancreas may be damaged. The pancreatic duct will then drain, into the splenic bed, amylase is the most likely biochemical finding. Glucagon is not secreted into the, pancreatic duct., Please rate this question:, , Discuss and give feedback, , Next question, , Splenic anatomy, The spleen is the largest lymphoid organ in the body. It is an intraperitoneal organ, the peritoneal, attachments condense at the hilum where the vessels enter the spleen. Its blood supply is from the, splenic artery (derived from the coeliac axis) and the splenic vein (which is joined by the IMV and, unites with the SMV).
Page 1367 :
, , , , , Embryology: derived from mesenchymal tissue, Shape: clenched fist, Position: below 9th-12th ribs, Weight: 75-150g, , Relations, , , , , , , , , Superiorly- diaphragm, Anteriorly- gastric impression, Posteriorly- kidney, Inferiorly- colon, Hilum: tail of pancreas and splenic vessels, Forms apex of lesser sac (containing short gastric vessels), Next question
Page 1368 :
Question 123 of 560, A 48 year old lady is undergoing an axillary node clearance for breast cancer. Which of the, structures listed below are most likely to be encountered during the axillary dissection?, , Cords of the brachial plexus, , Thoracodorsal trunk, , Internal mammary artery, , Thoracoacromial artery, , None of the above, Beware of damaging the thoracodorsal trunk if a latissimus dorsi flap reconstruction is planned., Theme from 2009 Exam, Theme from 2014 Exam, The thoracodorsal trunk runs through the nodes in the axilla. If injured it may compromise the, function and blood supply to latissimus dorsi, which is significant if it is to be used as a flap for a, reconstructive procedure., Please rate this question:, , Discuss and give feedback, , Next question, , Axilla, Boundaries of the axilla, , Medially, , Chest wall and Serratus anterior, , Laterally, , Humeral head, , Floor, , Subscapularis
Page 1369 :
Anterior aspect, , Lateral border of Pectoralis major, , Fascia, , Clavipectoral fascia, , Content:, , Long thoracic nerve (of, Bell), , Derived from C5-C7 and passes behind the brachial plexus to enter, the axilla. It lies on the medial chest wall and supplies serratus, anterior. Its location puts it at risk during axillary surgery and, damage will lead to winging of the scapula., , Thoracodorsal nerve and, thoracodorsal trunk, , Innervate and vascularise latissimus dorsi., , Axillary vein, , Lies at the apex of the axilla, it is the continuation of the basilic vein., Becomes the subclavian vein at the outer border of the first rib., , Intercostobrachial, nerves, , Traverse the axillary lymph nodes and are often divided during, axillary surgery. They provide cutaneous sensation to the axillary, skin., , Lymph nodes, , The axilla is the main site of lymphatic drainage for the breast., Next question
Page 1370 :
Question 124 of 560, , A 53 year old lady is recovering following a difficult mastectomy and axillary nodal clearance for, carcinoma of the breast. She complains of shoulder pain and on examination has obvious winging of, the scapula. Loss of innervation to which of the following is the most likely underlying cause?, , Latissimus dorsi, , Serratus anterior, , Pectoralis minor, , Pectoralis major, , Rhomboids, , Theme from April 2012 exam, Theme from April 2014 exam, Winging of the scapula is most commonly the result of long thoracic nerve injury or dysfunction., Iatrogenic damage during the course of the difficult axillary dissection is the most likely cause in this, scenario. Damage to the rhomboids may produce winging of the scapula but would be rare in the, scenario given., Please rate this question:, , Discuss and give feedback, , Next question, , Long thoracic nerve, , , , Derived from ventral rami of C5, C6, and C7 (close to their emergence from intervertebral, foramina), It runs downward and passes either anterior or posterior to the middle scalene muscle
Page 1371 :
, , , It reaches upper tip of serratus anterior muscle and descends on outer surface of this, muscle, giving branches into it, Winging of Scapula occurs in long thoracic nerve injury (most common) or from spinal, accessory nerve injury (which denervates the trapezius) or a dorsal scapular nerve injury, Next question
Page 1372 :
Question 125 of 560, , A 56 year old lady is referred to the colorectal clinic with symptoms of pruritus ani. On examination a, polypoidal mass is identified inferior to the dentate line. A biopsy confirms squamous cell carcinoma., To which of the following lymph node groups will the lesion potentially metastasise?, , Internal iliac, , External iliac, , Mesorectal, , Inguinal, , None of the above, , Theme from September 2011 Exam, Theme from April 2012 Exam, Theme from April 2014 exam, Lesions distal to the dentate line drain to the inguinal nodes. Occasionally this will result in the need, for a block dissection of the groin., Please rate this question:, , Discuss and give feedback, , Next question, , Rectum, The rectum is approximately 12 cm long. It is a capacitance organ. It has both intra and, extraperitoneal components. The transition between the sigmoid colon is marked by the, disappearance of the tenia coli.The extra peritoneal rectum is surrounded by mesorectal fat that also, contains lymph nodes. This mesorectal fatty layer is removed surgically during rectal cancer surgery
Page 1373 :
(Total Mesorectal Excision). The fascial layers that surround the rectum are important clinical, landmarks, anteriorly lies the fascia of Denonvilliers. Posteriorly lies Waldeyers fascia., Extra peritoneal rectum, , , , , , Posterior upper third, Posterior and lateral middle third, Whole lower third, , Relations, , Anteriorly (Males), , Rectovesical pouch, Bladder, Prostate, Seminal vesicles, , Anteriorly (Females), , Recto-uterine pouch (Douglas), Cervix, Vaginal wall, , Posteriorly, , Sacrum, Coccyx, Middle sacral artery, , Laterally, , Levator ani, Coccygeus, , Arterial supply, Superior rectal artery, Venous drainage, Superior rectal vein, Lymphatic drainage, , , , , , Mesorectal lymph nodes (superior to dentate line), Internal iliac and then para-aortic nodes, Inguinal nodes (inferior to dentate line)
Page 1374 :
Question 126 of 560, , A 20 year old man is hit with a hammer on the right side of the head. He dies on arrival in the, emergency department. Which of these features is most likely to be found at post mortem?, , Hydrocephalus, , Supra tentorial herniation, , Laceration of the middle meningeal artery, , Sub dural haematoma, , Posterior fossa haematoma, , Theme based on 2014 exam, This will account for the scenario given where there is a brief delay prior to death. The other options, are less acute and a supratentorial herniation would not occur in this setting., Please rate this question:, , Discuss and give feedback, , Next question, , Head injury, Patients who suffer head injuries should be managed according to ATLS principles and extra cranial, injuries should be managed alongside cranial trauma. Inadequate cardiac output will compromise, CNS perfusion irrespective of the nature of the cranial injury., Types of traumatic brain injury
Page 1375 :
Bleeding into the space between the dura mater and the skull. Often results from, acceleration-deceleration trauma or a blow to the side of the head. The majority, of extradural haematomas occur in the temporal region where skull fractures, cause a rupture of the middle meningeal artery., Extradural, haematoma, , Features, , , , , Raised intracranial pressure, Some patients may exhibit a lucid interval, , Bleeding into the outermost meningeal layer. Most commonly occur around the, frontal and parietal lobes. May be either acute or chronic., Subdural, haematoma, , Risk factors include old age and alcoholism., Slower onset of symptoms than a extradural haematoma., , Subarachnoid, haemorrhage, , Usually occurs spontaneously in the context of a ruptured cerebral aneurysm, but, may be seen in association with other injuries when a patient has sustained a, traumatic brain injury., , Pathophysiology, , , , , , , , , Primary brain injury may be focal (contusion/ haematoma) or diffuse (diffuse axonal injury), Diffuse axonal injury occurs as a result of mechanical shearing following deceleration,, causing disruption and tearing of axons, Intra-cranial haematomas can be extradural, subdural or intracerebral, while contusions may, occur adjacent to (coup) or contralateral (contre-coup) to the side of impact, Secondary brain injury occurs when cerebral oedema, ischaemia, infection, tonsillar or, tentorial herniation exacerbates the original injury. The normal cerebral auto regulatory, processes are disrupted following trauma rendering the brain more susceptible to blood flow, changes and hypoxia, The Cushings reflex (hypertension and bradycardia) often occurs late and is usually a pre, terminal event, , Management, , , , , , Where there is life threatening rising ICP such as in extra dural haematoma and whilst, theatre is prepared or transfer arranged use of IV mannitol/ frusemide may be required., Diffuse cerebral oedema may require decompressive craniotomy, Exploratory Burr Holes have little management in modern practice except where scanning, may be unavailable and to thus facilitate creation of formal craniotomy flap
Page 1376 :
, , , , , , , Depressed skull fractures that are open require formal surgical reduction and debridement,, closed injuries may be managed non operatively if there is minimal displacement., ICP monitoring is appropriate in those who have GCS 3-8 and normal CT scan., ICP monitoring is mandatory in those who have GCS 3-8 and abnormal CT scan., Hyponatraemia is most likely to be due to syndrome of inappropriate ADH secretion., Minimum of cerebral perfusion pressure of 70mmHg in adults., Minimum cerebral perfusion pressure of between 40 and 70 mmHg in children., , Interpretation of pupillary findings in head injuries, , Pupil size, , Light response, , Interpretation, , Unilaterally dilated, , Sluggish or fixed, , 3rd nerve compression secondary to tentorial, herniation, , Bilaterally dilated, , Sluggish or fixed, , Unilaterally dilated or, equal, , Cross reactive (Marcus Gunn), , Bilaterally constricted, , May be difficult to assess, , Unilaterally constricted, , Preserved, , , , , Poor CNS perfusion, Bilateral 3rd nerve palsy, , Optic nerve injury, , , , , , Opiates, Pontine lesions, Metabolic encephalopathy, , Sympathetic pathway disruption, Next question
Page 1377 :
Question 127 of 560, , Which of the following ligaments contains the artery supplying the head of femur in children?, , Transverse ligament, , Ligamentum teres, , Iliofemoral ligament, , Ischiofemoral ligament, , Pubofemoral ligament, , Theme from 2010 Exam, Please rate this question:, , Discuss and give feedback, , Next question, , Hip joint, , , , , , , , Head of femur articulates with acetabulum of the pelvis, Both covered by articular hyaline cartilage, The acetabulum forms at the union of the ilium, pubis, and ischium, The triradiate cartilage (Y-shaped growth plate) separates the pelvic bones, The acetabulum holds the femoral head by the acetabular labrum, Normal angle between femoral head and femoral shaft is 130o, , Ligaments
Page 1378 :
, , , Transverse ligament: joints anterior and posterior ends of the articular cartilage, Head of femur ligament (ligamentum teres): acetabular notch to the fovea. Contains arterial, supply to head of femur in children., , Image sourced from Wikipedia
Page 1380 :
Question 128 of 560, , A 72 year old man develops a hydrocele which is being surgically managed. As part of the, procedure the surgeons divide the tunica vaginalis. From which of the following is this structure, derived?, , Peritoneum, , External oblique aponeurosis, , Internal oblique aponeurosis, , Transversalis fascia, , Rectus sheath, , The tunica vaginalis is derived from peritoneum, it secretes the fluid that fills the hydrocele cavity., Please rate this question:, , Discuss and give feedback, , Next question, , Scrotal and testicular anatomy, Spermatic cord, Formed by the vas deferens and is covered by the following structures:, , Layer, , Origin
Page 1381 :
Layer, , Origin, , Internal spermatic fascia, , Transversalis fascia, , Cremasteric fascia, , From the fascial coverings of internal oblique, , External spermatic fascia, , External oblique aponeurosis, , Contents of the cord, , Vas deferens, , Transmits sperm and accessory gland secretions, , Testicular artery, , Branch of abdominal aorta supplies testis and epididymis, , Artery of vas deferens, , Arises from inferior vesical artery, , Cremasteric artery, , Arises from inferior epigastric artery, , Pampiniform plexus, , Venous plexus, drains into right or left testicular vein, , Sympathetic nerve fibres, , Lie on arteries, the parasympathetic fibres lie on the vas, , Genital branch of the genitofemoral nerve, , Supplies cremaster, , Lymphatic vessels, , Drain to lumbar and para-aortic nodes, , Scrotum, , , , , Composed of skin and closely attached dartos fascia., Arterial supply from the anterior and posterior scrotal arteries
Page 1382 :
, , , Lymphatic drainage to the inguinal lymph nodes, Parietal layer of the tunica vaginalis is the innermost layer, , Testes, , , , , , , The testes are surrounded by the tunica vaginalis (closed peritoneal sac). The parietal layer, of the tunica vaginalis adjacent to the internal spermatic fascia., The testicular arteries arise from the aorta immediately inferiorly to the renal arteries., The pampiniform plexus drains into the testicular veins, the left drains into the left renal vein, and the right into the inferior vena cava., Lymphatic drainage is to the para-aortic nodes., Next question
Page 1383 :
Question 129 of 560, , A 43 year old lady is donating her left kidney to her sister and the surgeons are harvesting the left, kidney. Which of the following structures will lie most anteriorly at the hilum of the left kidney?, , Left renal artery, , Left renal vein, , Left ureter, , Left ovarian vein, , Left ovarian artery, , The renal veins lie most anteriorly, then artery and ureter lies posteriorly., Please rate this question:, , Discuss and give feedback, , Next question, , Renal arteries, , , , The right renal artery is longer than the left renal artery, The renal vein/artery/pelvis enter the kidney at the hilum, , Relations, , Right, , Anterior- IVC, right renal vein, the head of the pancreas, and the descending part of the
Page 1384 :
duodenum, , Left, , Anterior- left renal vein, the tail of the pancreas, , Branches, , , , , , , The renal arteries are direct branches off the aorta (upper border of L2- right side and L1 left side), In 30% there may be accessory arteries (mainly left side). Instead of entering the kidney at, the hilum, they usually pierce the upper or lower part of the organ., Before reaching the hilum of the kidney, each artery divides into four or five segmental, branches (renal vein anterior and ureter posterior); which then divide within the sinus into, lobar arteries supplying each pyramid and cortex., Each vessel gives off some small inferior suprarenal branches to the suprarenal gland, the, ureter, and the surrounding cellular tissue and muscles., Next question
Page 1385 :
Question 130 of 560, , What is the sensory nerve supply to the angle of the jaw?, , Maxillary branch of the trigeminal nerve, , Mandibular branch of the trigeminal nerve, , C3-C4, , Greater auricular nerve (C2-C3), , Buccal branch of the facial nerve, , The trigeminal nerve is the major sensory nerve to the face except over the angle of the jaw. The, angle of the jaw is innervated by the greater auricular nerve., Please rate this question:, , Discuss and give feedback, , Next question, , Trigeminal nerve, The trigeminal nerve is the main sensory nerve of the head. In addition to its major sensory role, it, also innervates the muscles of mastication., Distribution of the trigeminal nerve, , Sensory, , , , , , Scalp, Face, Oral cavity (and teeth)
Page 1386 :
, , , Nose and sinuses, Dura mater, , Motor, , , , , , , , Muscles of mastication, Mylohyoid, Anterior belly of digastric, Tensor tympani, Tensor palati, , Autonomic connections (ganglia), , , , , , , Ciliary, Sphenopalatine, Otic, Submandibular, , Path, , , , , , Originates at the pons, Sensory root forms the large, crescentic trigeminal ganglion within Meckel's cave, and, contains the cell bodies of incoming sensory nerve fibres. Here the 3 branches exit., The motor root cell bodies are in the pons and the motor fibres are distributed via the, mandibular nerve. The motor root is not part of the trigeminal ganglion., , Branches of the trigeminal nerve, , Ophthalmic nerve, , Sensory only, , Maxillary nerve, , Sensory only, , Mandibular nerve, , Sensory and motor, , Sensory, , Ophthalmic, , Exits skull via the superior orbital fissure, Sensation of: scalp and forehead, the upper eyelid, the conjunctiva and cornea of the eye,, the nose (including the tip of the nose, except alae nasi), the nasal mucosa, the frontal
Page 1387 :
sinuses, and parts of the meninges (the dura and blood vessels)., , Maxillary, nerve, , Exit skull via the foramen rotundum, Sensation: lower eyelid and cheek, the nares and upper lip, the upper teeth and gums,, the nasal mucosa, the palate and roof of the pharynx, the maxillary, ethmoid and, sphenoid sinuses, and parts of the meninges., , Mandibular, nerve, , Exit skull via the foramen ovale, Sensation: lower lip, the lower teeth and gums, the chin and jaw (except the angle of the, jaw), parts of the external ear, and parts of the meninges., , Motor, Distributed via the mandibular nerve., The following muscles of mastication are innervated:, , , , , , , Masseter, Temporalis, Medial pterygoid, Lateral pterygoid, , Other muscles innervated include:, , , , , , , Tensor veli palatini, Mylohyoid, Anterior belly of digastric, Tensor tympani, Next question
Page 1388 :
Question 131 of 560, A 63 year old man is undergoing a coronary artery bypass procedure. During the median sternotomy, which structure would routinely require division?, , Parietal pleura, , Interclavicular ligament, , Internal mammary artery, , Brachiocephalic vein, , Left vagus nerve, , Theme from January 2011 Exam, The interclavicular ligament lies at the upper end of a median sternotomy and is routinely divided to, provide access. The pleural reflections are often encountered and should not be intentionally, divided, if they are, then a chest drain will need to be inserted on the affected side as collections, may then accumulate in the pleural cavity. Other structures encountered include the pectoralis major, muscles, again if the incision is truly midline then these should not require formal division. The close, relationship of the brachiocephalic vein should be borne in mind and it should be avoided, iatrogenic, injury to this structure will result in considerable haemorrhage., Please rate this question:, , Discuss and give feedback, , Next question, , Sternotomy, A median sternotomy is the commonest incision utilised to access the heart and great vessels., A midline incision is made from the interclavicular fossa to the xiphoid process and the fat and, subcutaneous tissues are divided to the level of the sternum. The periosteum may be gently, mobilised off the midline, although vigorous periosteal stripping is best avoided. A bone saw is used, to divide the bone itself. Posteriorly the reflections of the parietal pleura should be identified and, avoided (unless surgery to the lung is planned). The fibrous pericardium is incised and the heart, brought into view. Bleeding from the bony edges of the cut sternum is stopped using roller ball, diathermy or bone wax. The left brachiocephalic vein is an important posterior relation at the, superior aspect of the sternotomy incision and should be avoided. More inferior the thymic remnants, may be identified. At the inferior aspect of the incision the abdominal cavity may be entered (though, this is seldom troublesome).
Page 1389 :
Question 132 of 560, , Which of the following structures separates the subclavian artery from the subclavian vein?, , Scalenus anterior, , Scalenus medius, , Sternocleidomastoid, , Pectoralis major, , Pectoralis minor, , The artery and vein are separated by scalenus anterior. This muscle runs from the transverse, processes of C3,4,5 and 6 to insert onto the scalene tubercle of the first rib., Please rate this question:, , Discuss and give feedback, , Next question, , Subclavian artery, Path, , , , , , The left subclavian comes directly off the arch of aorta, The right subclavian arises from the brachiocephalic artery (trunk) when it bifurcates into the, subclavian and the right common carotid artery., From its origin, the subclavian artery travels laterally, passing between anterior and middle, scalene muscles, deep to scalenus anterior and anterior to scalenus medius. As the
Page 1390 :
subclavian artery crosses the lateral border of the first rib, it becomes the axillary artery. At, this point it is superficial and within the subclavian triangle., , Image sourced from Wikipedia, , Branches, , , , , , , , Vertebral artery, Internal thoracic artery, Thyrocervical trunk, Costocervical trunk, Dorsal scapular artery, Next question
Page 1391 :
Question 133 of 560, , A 56 year old lady is due to undergo a left hemicolectomy for carcinoma of the splenic flexure. The, surgeons decide to perform a high ligation of the inferior mesenteric vein. Into which of the following, does this structure usually drain?, , Portal vein, , Inferior vena cava, , Left renal vein, , Left iliac vein, , Splenic vein, Beware of ureteric injury in colonic surgery., , The inferior mesenteric vein drains into the splenic vein, this point of union lies close to the, duodenum and this surgical maneouvre is a recognised cause of ileus., Please rate this question:, , Discuss and give feedback, , Next question, , Left colon, Position
Page 1392 :
, , , , , As the left colon passes inferiorly its posterior aspect becomes extraperitoneal, and the, ureter and gonadal vessels are close posterior relations that may become involved in, disease processes, At a level of L3-4 (variable) the left colon becomes the sigmoid colon and wholly, intraperitoneal once again, The sigmoid colon is a highly mobile structure and may even lie on the right side of the, abdomen, It passes towards the midline, the taenia blend and this marks the transition between sigmoid, colon and upper rectum, , Blood supply, , , , , Inferior mesenteric artery, However, the marginal artery (from the right colon) contributes, this contribution becomes, clinically significant when the IMA is divided surgically (e.g. During AAA repair), Next question
Page 1393 :
Question 134 of 560, A man undergoes a high anterior resection for carcinoma of the upper rectum. Which of the following, vessels will require ligation?, , Superior mesenteric artery, , Inferior mesenteric artery, , Coeliac axis, , Perineal artery, , Middle colic artery, , Theme from April 2013 Exam, Theme from September 2013 Exam, The IMA is usually divided during anterior resection. Not only is this borne out of oncological, necessity but it also permits sufficient colonic mobilisation for anastomosis., Please rate this question:, , Discuss and give feedback, , Next question, , Colon anatomy, The colon commences with the caecum. This represents the most dilated segment of the human, colon and its base (which is intraperitoneal) is marked by the convergence of teniae coli. At this point, is located the vermiform appendix. The colon continues as the ascending colon, the posterior aspect, of which is retroperitoneal. The line of demarcation between the intra and retro peritoneal right colon, is visible as a white line, in the living, and forms the line of incision for colonic resections., The ascending colon becomes the transverse colon after passing the hepatic flexure. At this located, the colon becomes wholly intra peritoneal once again. The superior aspect of the transverse colon is, the point of attachment of the transverse colon to the greater omentum. This is an important, anatomical site since division of these attachments permits entry into the lesser sac. Separation of, the greater omentum from the transverse colon is a routine operative step in both gastric and colonic, resections., At the left side of the abdomen the transverse colon passes to the left upper quadrant and makes an, oblique inferior turn at the splenic flexure. Following this, the posterior aspect becomes
Page 1394 :
retroperitoneal once again., At the level of approximately L4 the descending colon becomes wholly intraperitoneal and becomes, the sigmoid colon. Whilst the sigmoid is wholly intraperitoneal there are usually attachments laterally, between the sigmoid and the lateral pelvic sidewall. These small congenital adhesions are not formal, anatomical attachments but frequently require division during surgical resections., At its distal end the sigmoid passes to the midline and at the region around the sacral promontary it, becomes the upper rectum. This transition is visible macroscopically as the point where the teniae, fuse. More distally the rectum passes through the peritoneum at the region of the peritoneal, reflection and becomes extraperitoneal., Arterial supply, Superior mesenteric artery and inferior mesenteric artery: linked by the marginal artery., Ascending colon: ileocolic and right colic arteries, Transverse colon: middle colic artery, Descending and sigmoid colon: inferior mesenteric artery, Venous drainage, From regional veins (that accompany arteries) to superior and inferior mesenteric vein, Lymphatic drainage, Initially along nodal chains that accompany supplying arteries, then para-aortic nodes., Embryology, Midgut- Second part of duodenum to 2/3 transverse colon, Hindgut- Distal 1/3 transverse colon to anus, Peritoneal location, The right and left colon are part intraperitoneal and part extraperitoneal. The sigmoid and transverse, colon are generally wholly intraperitoneal. This has implications for the sequelae of perforations,, which will tend to result in generalised peritonitis in the wholly intra peritoneal segments., Colonic relations, , Region of colon, , Relation, , Caecum/ right colon, , Right ureter, gonadal vessels, , Hepatic flexure, , Gallbladder (medially), , Splenic flexure, , Spleen and tail of pancreas, , Distal sigmoid/ upper, rectum, , Left ureter
Page 1395 :
Region of colon, , Relation, , Rectum, , Ureters, autonomic nerves, seminal vesicles, prostate, urethra, (distally), Next question
Page 1396 :
Question 135 of 560, A 43 year old lady is due to undergo an axillary node clearance as part of treatment for carcinoma of, the breast. Which of the following fascial layers will be divided during the surgical approach to the, axilla?, , Sibsons fascia, , Pre tracheal fascia, , Waldayers fascia, , Clavipectoral fascia, , None of the above, , The clavipectoral fascia is situated under the clavicular portion of pectoralis major. It protects both, the axillary vessels and nodes. During an axillary node clearance for breast cancer the clavipectoral, fascia is incised and this allows access to the nodal stations. The nodal stations are; level 1 nodes, inferior to pectoralis minor, level 2 lie behind it and level 3 above it. During a Patey Mastectomy, surgeons divide pectoralis minor to gain access to level 3 nodes. The use of sentinel node biopsy, (and stronger assistants!) have made this procedure far less common., Please rate this question:, , Discuss and give feedback, , Next question, , Axilla, Boundaries of the axilla, , Medially, , Chest wall and Serratus anterior, , Laterally, , Humeral head, , Floor, , Subscapularis
Page 1397 :
Anterior aspect, , Lateral border of Pectoralis major, , Fascia, , Clavipectoral fascia, , Content:, , Long thoracic nerve (of, Bell), , Derived from C5-C7 and passes behind the brachial plexus to enter, the axilla. It lies on the medial chest wall and supplies serratus, anterior. Its location puts it at risk during axillary surgery and, damage will lead to winging of the scapula., , Thoracodorsal nerve and, thoracodorsal trunk, , Innervate and vascularise latissimus dorsi., , Axillary vein, , Lies at the apex of the axilla, it is the continuation of the basilic vein., Becomes the subclavian vein at the outer border of the first rib., , Intercostobrachial, nerves, , Traverse the axillary lymph nodes and are often divided during, axillary surgery. They provide cutaneous sensation to the axillary, skin., , Lymph nodes, , The axilla is the main site of lymphatic drainage for the breast., Next question
Page 1398 :
Question 136 of 560, What are the boundaries of the 'safe triangle' for chest drain insertion?, , Bounded by trapezius, latissimus dorsi, and laterally by the vertebral border of the scapula, , Bounded by latissimus dorsi, pectoralis major, line superior to the nipple and apex at the, axilla, Bounded by latissimus dorsi, serratus anterior, line superior to the nipple and apex at the, axilla, Bounded by trapezius, deltoid, rhomboid major and teres minor, , Bounded by trapezius, deltoid and latissimus dorsi, , Theme from April 2012 Exam, Please rate this question:, , Discuss and give feedback, , Next question, , Chest drains, There are a number of different indications for chest drain insertion. In general terms large bore, chest drains are preferred for trauma and haemothorax drainage. Smaller diameter chest drains can, be used for pneumothorax or pleural effusion drainage., Insertion can be performed either using anatomical guidance or through ultrasound guidance. In the, exam, the anatomical method is usually tested., It is advised that chest drains are placed in the 'safe triangle'. The triangle is located in the mid, axillary line of the 5th intercostal space. It is bordered by:, Anterior edge latissimus dorsi, the lateral border of pectoralis major, a line superior to the horizontal, level of the nipple, and the apex below the axilla., Another triangle is situated behind the scapula. It is bounded above by the trapezius, below by the, latissimus dorsi, and laterally by the vertebral border of the scapula; the floor is partly formed by the, rhomboid major. If the scapula is drawn forward by folding the arms across the chest, and the trunk, bent forward, parts of the sixth and seventh ribs and the interspace between them become, subcutaneous and available for auscultation. The space is therefore known as the triangle of, auscultation.
Page 1399 :
References, Prof Harold Ellis. The applied anatomy of chest drains insertions. British Journal of hospital medicine, 2007; (68): 44-45., Laws D, Neville E, Duffy J. BTS guidelines for insertion of chest drains. Thorax, 2003; (58): 53-59., Next question
Page 1400 :
Question 137 of 560, , The vertebral artery traverses all of the following except?, , Transverse process of C6, , Transverse process of the axis, , Vertebral canal, , Foramen magnum, , Intervertebral foramen, , The vertebral artery passes through the foramina which are located in the transverse processes of, the cervical vertebra, it does not traverse the intervertebral foramen., Please rate this question:, , Discuss and give feedback, , Next question, , Vertebral artery, The vertebral artery is the first branch of the subclavian artery. Anatomically it is divisible into 4, regions:, , , , , The first part runs to the foramen in the transverse process of C6. Anterior to this part lies the, vertebral and internal jugular veins. On the left side the thoracic duct is also an anterior, relation., The second part runs superiorly through the foramina of the the transverse processes of the, upper 6 cervical vertebrae. Once it has passed through the transverse process of the axis it
Page 1401 :
, , , then turns superolaterally to the atlas. It is accompanied by a venous plexus and the inferior, cervical sympathetic ganglion., The third part runs posteromedially on the lateral mass of the atlas. It enters the sub occipital, triangle, in the groove of the upper surface of the posterior arch of the atlas. It then passes, anterior to the edge of the posterior atlanto-occipital membrane to enter the vertebral canal., The fourth part passes through the spinal dura and arachnoid, running superiorly and, anteriorly at the lateral aspect of the medulla oblongata. At the lower border of the pons it, unites to form the basilar artery., Next question
Page 1402 :
Question 138 of 560, , A 60 year old female attends the preoperative hernia clinic. She reports some visual difficulty. On, examination she is noted to have a homonymous hemianopia. Where is the lesion most likely to be?, , Frontal lobe, , Pituitary gland, , Parietal lobe, , Optic chiasm, , Optic tract, Lesions before optic chiasm:, Monocular vision loss = Optic nerve lesion, Bitemporal hemianopia = Optic chiasm lesion, Lesions after the optic chiasm:, Homonymous hemianopia = Optic tract lesion, Upper quadranopia = Temporal lobe lesion, Lower quadranopia = Parietal lobe lesion, , Theme from April 2012 exam, Theme from April 2014 exam, Unfortunately we thought as surgeons we could forget about visual field defects! However the, college seem to like them. Remember a homonymous hemianopia is indicative of an optic tract, lesion. Parietal lobe lesions tend to cause inferior quadranopias and there is a bitemporal, hemianopia with optic chiasm lesion or pituitary tumours., , Please rate this question:
Page 1403 :
Discuss and give feedback, , Next question, , Visual field defects, Theme from January 2012 exam, Theme from April 2012 exam, , , , , , left homonymous hemianopia means visual field defect to the left, i.e. Lesion of right optic, tract, homonymous quadrantanopias: PITS (Parietal-Inferior, Temporal-Superior), incongruous defects = optic tract lesion; congruous defects = optic radiation lesion or, occipital cortex, , Homonymous hemianopia, , , , , , Incongruous defects: lesion of optic tract, Congruous defects: lesion of optic radiation or occipital cortex, Macula sparing: lesion of occipital cortex, , Homonymous quadrantanopias, , , , , , Superior: lesion of temporal lobe, Inferior: lesion of parietal lobe, Mnemonic = PITS (Parietal-Inferior, Temporal-Superior), , Bitemporal hemianopia, , , , , , Lesion of optic chiasm, Upper quadrant defect > lower quadrant defect = inferior chiasmal compression, commonly a, pituitary tumour, Lower quadrant defect > upper quadrant defect = superior chiasmal compression, commonly, a craniopharyngioma, Next question
Page 1404 :
Question 139 of 560, A 34 year old male is being examined in the pre-operative assessment clinic. A murmur is identified, in the 4th intercostal space just next to the left side of the sternum. From where is it most likely to, have originated?, , Mitral valve, , Aortic valve, , Pulmonary valve, , Right ventricular aneurysm, , Tricuspid valve, , Theme from September 2012 Exam, The tricuspid valve is generally referred to being best auscultated adjacent to the sternum. The, plane of projected sound from the mitral area is best heard in the region of the cadiac apex., Please rate this question:, , Discuss and give feedback, , Next question, , Heart sounds, Sites of auscultation, , Valve, , Site, , Pulmonary valve, , Left second intercostal space, at the upper sternal border, , Aortic valve, , Right second intercostal space, at the upper sternal border, , Mitral valve, , Left fifth intercostal space, just medial to mid clavicular line
Page 1405 :
Valve, , Site, , Tricuspid valve, , Left fourth intercostal space, at the lower left sternal border, , The diagram below demonstrates where the various cardiac valves are best heard., , Image sourced from Wikipedia, , Next question
Page 1406 :
Question 140 of 560, , During an Ivor Lewis Oesophagectomy for carcinoma of the lower third of the oesophagus which, structure is divided to allow mobilisation of the oesophagus?, , Vagus nerve, , Azygos vein, , Right inferior lobar bronchus, , Phrenic nerve, , Pericardiophrenic artery, , Theme from April 2014 exam, The azygos vein is routinely divided during an oesophagectomy to allow mobilisation. It arches, anteriorly to insert into the SVC on the right hand side., Please rate this question:, , Discuss and give feedback, , Next question, , Treatment of oesophageal cancer, , , , , , , In general resections are not offered to those patients with distant metastasis, and usually, not to those with N2 disease., Local nodal involvement is not in itself a contra indication to resection., Surgical resection is the mainstay of treatment., Neoadjuvent chemotherapy is given in most cases prior to surgery., In situ disease may be managed by endoscopic mucosal resection, although this is still, debated.
Page 1407 :
, , , , , In patients with lower third lesions an Ivor - Lewis type procedure is most commonly, performed. Very distal tumours may be suitable to a transhiatal procedure. Which is an, attractive option as the penetration of two visceral cavities required for an Ivor- Lewis type, procedure increases the morbidity considerably., More proximal lesions will require a total oesphagectomy (Mckeown type) with anastomosis, to the cervical oesophagus., Patients with unresectable disease may derive benefit from local ablative procedures,, palliative chemotherapy or stent insertion., , Operative details of Ivor- Lewis procedure, , , , Combined laparotomy and right thoracotomy, , Indication, , , , Lower and middle third oesophageal tumours, , Preparation, , , , , , Staging with a combination of CT chest abdomen and pelvis- if no metastatic disease, detected then patients will undergo a staging laparoscopy to detect peritoneal disease., If both these modalities are negative then patients will finally undergo a PET CT scan to, detect occult metastatic disease. Only in those whom no evidence of advanced disease is, detected will proceed to resection., Patients receive a GA, double lumen endotracheal tube to allow for lung deflation, CVP and, arterial monitoring., , Procedure, , , , A rooftop incision is made to access the stomach and duodenum., , Laparotomy To mobilize the stomach, , , , , , The greater omentum is incised away from its attachment to the right gastroepiploic vessels, along the greater curvature of the stomach., Then the short gastric vessels are ligated and detached from the greater curvature from the, spleen., The lesser omentum is incised, preserving the right gastric artery.
Page 1408 :
, , , The retroperitoneal attachments of the duodenum in its second and third portions are, incised, allowing the pylorus to reach the oesophageal hiatus. Some surgeons perform a, pyloroplasty at this point to facilitate gastric emptying., The left gastric vessels are then ligated, avoiding any injury to the common hepatic or splenic, arteries. Care must be taken to avoid inadvertently devascularising the liver owing to, variations in anatomy., , Right Thoracotomy Oesophageal resection and oesophagogastric anastomosis, , , , , , , , Through 5th intercostal space, Dissection performed 10cm above the tumour, This may involve transection of the azygos vein., The oesophagus is then removed with the stomach creating a gastric tube., An anastomosis is created., , The chest is closed with underwater seal drainage and tube drains to the abdominal cavity., Post operatively, , , , , , Patients will typically recover in ITU initially., A nasogastric tube will have been inserted intraoperatively and must remain in place during, the early phases of recovery., Post operatively these patients are at relatively high risk of developing complications:, , * Atelectasis- due to the effects of thoracotomy and lung collapse, * Anastomotic leakage. The risk is relatively high owing to the presence of a relatively, devascularised stomach. Often the only blood supply is from the gastroepiploic artery as all others, will have been divided. If a leak does occur then many will attempt to manage conservatively with, prolonged nasogastric tube drainage and TPN. The reality is that up to 50% of patients developing, an anastomotic leak will not survive to discharge., * Delayed gastric emptying (may be avoided by performing a pyloroplasty)., Next question
Page 1409 :
Question 141 of 560, , Which of the following statements relating to quadratus lumborum is false?, , Causes flexion of the thoracic spine, , Causes the rib cage to be pulled down, , Innervated by anterior primary rami of T12 and L1-3, , Attached to the iliac crest, , Inserts into the 12th rib, Quadratus lumborum, Origin: Medial aspect of iliac crest and iliolumbar ligament, Insertion: 12th rib, Action: Pulls the rib cage inferiorly. Lateral flexion., Nerve supply: Anterior primary rami of T12 and L1-3, , The rectus abdominis causes flexion of the thoracic spine and therefore the statement suggesting, that quaratus lumborum does so is incorrect., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal wall, The 2 main muscles of the abdominal wall are the rectus abdominis (anterior) and the quadratus, lumborum (posterior)., The remaining abdominal wall consists of 3 muscular layers. Each muscle passes from the lateral
Page 1410 :
aspect of the quadratus lumborum posteriorly to the lateral margin of the rectus sheath anteriorly., Each layer is muscular posterolaterally and aponeurotic anteriorly., , Image sourced from Wikipedia, , Muscles of abdominal wall, , External, oblique, , , , , , , , , Internal, oblique, , , , , , , Transversus, abdominis, , , , , , , , Lies most superficially, Originates from 5th to 12th ribs, Inserts into the anterior half of the outer aspect of the iliac crest, linea alba and, pubic tubercle, More medially and superiorly to the arcuate line, the aponeurotic layer, overlaps the rectus abdominis muscle, The lower border forms the inguinal ligament, The triangular expansion of the medial end of the inguinal ligament is the, lacunar ligament., , Arises from the thoracolumbar fascia, the anterior 2/3 of the iliac crest and the, lateral 2/3 of the inguinal ligament, The muscle sweeps upwards to insert into the cartilages of the lower 3 ribs, The lower fibres form an aponeurosis that runs from the tenth costal cartilage, to the body of the pubis, At its lowermost aspect it joins the fibres of the aponeurosis of transversus, abdominis to form the conjoint tendon., , Innermost muscle, Arises from the inner aspect of the costal cartilages of the lower 6 ribs , from, the anterior 2/3 of the iliac crest and lateral 1/3 of the inguinal ligament, Its fibres run horizontally around the abdominal wall ending in an aponeurosis., The upper part runs posterior to the rectus abdominis. Lower down the fibres, run anteriorly only., The rectus abdominis lies medially; running from the pubic crest and symphysis, to insert into the xiphoid process and 5th, 6th and 7th costal cartilages. The, muscles lies in a aponeurosis as described above.
Page 1411 :
, , Nerve supply: anterior primary rami of T7-12, , Surgical notes, During abdominal surgery it is usually necessary to divide either the muscles or their aponeuroses., During a midline laparotomy it is desirable to divide the aponeurosis. This will leave the rectus, sheath intact above the arcuate line and the muscles intact below it. Straying off the midline will, often lead to damage to the rectus muscles, particularly below the arcuate line where they may often, be in close proximity to each other., Next question
Page 1412 :
Question 142 of 560, , A 23 year old climber falls and fractures his humerus. The surgeons decide upon a posterior, approach to the middle third of the bone. Which of the following nerves is at greatest risk in this, approach?, , Ulnar, , Antebrachial, , Musculocutaneous, , Radial, , Intercostobrachial, , Theme from April 2012 Exam, The radial nerve wraps around the humerus and may be injured during a posterior approach. An IM, nail may be preferred as it avoids the complex dissection needed for direct bone exposure., Please rate this question:, , Discuss and give feedback, , Next question, , Radial nerve, Continuation of posterior cord of the brachial plexus (root values C5 to T1), Path
Page 1413 :
, , , , , , , In the axilla: lies posterior to the axillary artery on subscapularis, latissimus dorsi and teres, major., Enters the arm between the brachial artery and the long head of triceps (medial to humerus)., Spirals around the posterior surface of the humerus in the groove for the radial nerve., At the distal third of the lateral border of the humerus it then pierces the intermuscular, septum and descends in front of the lateral epicondyle., At the lateral epicondyle it lies deeply between brachialis and brachioradialis where it then, divides into a superficial and deep terminal branch., Deep branch crosses the supinator to become the posterior interosseous nerve., , In the image below the relationships of the radial nerve can be appreciated, , Image sourced from Wikipedia, , Regions innervated, , Motor (main nerve), , Motor (posterior, interosseous branch), , , , , , , Triceps, Anconeus, Brachioradialis, Extensor carpi radialis, , , , , , , Supinator, Extensor carpi ulnaris, Extensor digitorum, Extensor indicis
Page 1414 :
, , , , Sensory, , Extensor digiti minimi, Extensor pollicis longus and brevis, Abductor pollicis longus, , The area of skin supplying the proximal phalanges on the dorsal aspect of the, hand is supplied by the radial nerve (this does not apply to the little finger and, part of the ring finger), , Muscular innervation and effect of denervation, , Anatomical, location, , Muscle affected, , Effect of paralysis, , Shoulder, , Long head of triceps, , Minor effects on shoulder stability in abduction, , Arm, , Triceps, , Loss of elbow extension, , Forearm, , Supinator, Brachioradialis, Extensor carpi radialis longus, and brevis, , Weakening of supination of prone hand and elbow, flexion in mid prone position, , The cutaneous sensation of the upper limb- illustrating the contribution of the radial nerve
Page 1415 :
Image sourced from Wikipedia, , Next question
Page 1416 :
Question 143-145 of 560, , Theme: Nerve injury, , A. Median nerve, B. Ulnar nerve, C. Radial nerve, D. Posterior interosseous nerve, E. Anterior interosseous nerve, F. Musculocutaneous nerve, G. Axillary nerve, H. Brachial Trunks C5-6, I. Brachial trunks C6-7, J. Brachial Trunks C8-T1, , Please select the most likely lesion site for each scenario. Each option may be used once, more, than once or not at all., , 143., , A 42 year old teacher is admitted with a fall. An x-ray confirms a fracture of the surgical neck of, the humerus. Which nerve is at risk?, You answered Median nerve, The correct answer is Axillary nerve, The Axillary nerve winds around the bone at the neck of the humerus. The axillary nerve is also, at risk during shoulder dislocation., , 144., , A 32 year old window cleaner is admitted after falling off the roof. He reports that he had, slipped off the top of the roof and was able to cling onto the gutter for a few seconds. The
Page 1417 :
patient has Horner's syndrome., You answered Median nerve, The correct answer is Brachial Trunks C8-T1, The patient has a Klumpke's paralysis involving brachial trunks C8-T1. Classically there is, weakness of the hand intrinsic muscles. Involvement of T1 may cause a Horner's syndrome. It, occurs as a result of traction injuries or during delivery., , 145., , A 32 year old rugby player is hit hard on the shoulder during a rough tackle. Clinically his arm is, hanging loose on the side. It is pronated and medially rotated., You answered Median nerve, The correct answer is Brachial Trunks C5-6, The patient has an Erb's palsy involving brachial trunks C5-6., , Please rate this question:, , Discuss and give feedback, , Next question, , Brachial plexus, Origin, , Sections of the plexus, , Anterior rami of C5 to T1, , , , , Roots, trunks, divisions, cords, branches, Mnemonic:Real Teenagers Drink Cold Beer
Page 1418 :
Roots, , , , , Located in the posterior triangle, Pass between scalenus anterior and medius, , Trunks, , , , , , Located posterior to middle third of clavicle, Upper and middle trunks related superiorly to the subclavian artery, Lower trunk passes over 1st rib posterior to the subclavian artery, , Divisions, , Apex of axilla, , Cords, , Related to axillary artery, , Diagram illustrating the branches of the brachial plexus, , Image sourced from Wikipedia, , Cutaneous sensation of the upper limb
Page 1419 :
Image sourced from Wikipedia, , Next question
Page 1420 :
Question 146 of 560, , A 68 year old man with critical limb ischaemia is undergoing a femoro-distal bypass graft. During, mobilisation of the proximal part of the posterior tibial artery which of the following is at greatest risk, of injury?, , Tibial nerve, , Sciatic nerve, , Saphenous nerve, , Common peroneal nerve, , Medial superior genicular artery, , The tibial nerve is closely related to the posterior tibial artery. The tibial nerve crosses the vessel, posteriorly approximately 2.5cm distal to its origin. At its origin the nerve lies medial and then lateral, after it crosses the vessel as described., Please rate this question:, , Discuss and give feedback, , Next question, , Posterior tibial artery, , , , , , Larger terminal branch of the popliteal artery, Terminates by dividing into the medial and lateral plantar arteries, Accompanied by two veins throughout its length, Position of the artery corresponds to a line drawn from the lower angle of the popliteal fossa,, at the level of the neck of the fibula, to a point midway between the medial malleolus and the, most prominent part of the heel
Page 1421 :
Relations of the posterior tibial artery, Proximal to distal, , Anteriorly, , Tibialis posterior, Flexor digitorum longus, Posterior surface of tibia and ankle joint, , Posterior, , Tibial nerve 2.5 cm distal to its origin, Fascia overlying the deep muscular layer, Proximal part covered by gastrocnemius and soleus, Distal part covered by skin and fascia, Next question
Page 1422 :
Question 147 of 560, A 67 year old man is undergoing an angiogram for gastro intestinal bleeding. The radiologist, advances the catheter into the coeliac axis. At what spinal level does this vessel typically arise from, the aorta?, , T10, , L3, , L4, , T12, , None of the above, , Theme from April 2014 exam, The coeliac axis lies at T12, it takes an almost horizontal angle off the aorta. It has three major, branches., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal aortic branches, Branches, , Level, , Paired, , Type, , Inferior phrenic, , T12 (Upper border), , Yes, , Parietal, , Coeliac, , T12, , No, , Visceral, , Superior mesenteric, , L1, , No, , Visceral
Page 1426 :
Question 149 of 560, , During a radical gastrectomy for carcinoma of the stomach the surgeons remove the omentum., What is the main source of its blood supply?, , Ileocolic artery, , Superior mesenteric artery, , Gastroepiploic artery, , Middle colic artery, , Inferior mesenteric artery, , The vessels supplying the omentum are the omental branches of the right and left gastro-epiploic, arteries. The colonic vessels are not responsible for the arterial supply to the omentum. The left, gastro-epiploic artery is a branch of the splenic artery and the right gastro-epiploic artery is a, terminal branch of the gastroduodenal artery., Please rate this question:, , Discuss and give feedback, , Next question, , Omentum, , , , The omentum is divided into two parts which invest the stomach. Giving rise to the greater, and lesser omentum. The greater omentum is attached to the inferolateral border of the, stomach and houses the gastro-epiploic arteries., It is of variable size but is less well developed in children. This is important as the omentum, confers protection against visceral perforation (e.g. Appendicitis).
Page 1427 :
, , , Inferiorly between the omentum and transverse colon is one potential entry point into the, lesser sac., Several malignant processes may involve the omentum of which ovarian cancer is the most, notable., Next question
Page 1428 :
Question 150 of 560, , A 38 year old lady is due to undergo a parathyroidectomy for hyperparathyroidism. At operation the, inferior parathyroid gland is identified as being enlarged. A vessel is located adjacent to the gland, laterally. This vessel is most likely to be the:, , External carotid artery, , Common carotid artery, , Internal carotid artery, , External jugular vein, , None of the above, , The common carotid artery is a lateral relation of the inferior parathyroid., Please rate this question:, , Discuss and give feedback, , Next question, , Parathyroid glands- anatomy, , , , , Four parathyroid glands, Located posterior to the thyroid gland, They lie within the pretracheal fascia, , Embryology, The parathyroids develop from the extremities of the third and fourth pharyngeal pouches. The, parathyroids derived from the fourth pharyngeal pouch are located more superiorly and are
Page 1429 :
associated with the thyroid gland. Those derived from the third pharyngeal pouch lie more inferiorly, and may become associated with the thymus., Blood supply, The blood supply to the parathyroid glands is derived from the inferior and superior thyroid, arteries[1]. There is a rich anastomosis between the two vessels. Venous drainage is into the thyroid, veins., Relations, , Laterally, , Common carotid, , Medially, , Recurrent laryngeal nerve, trachea, , Anterior, , Thyroid, , Posterior, , Pretracheal fascia, , References, 1.Nobori, M., et al., Blood supply of the parathyroid gland from the superior thyroid artery. Surgery,, 1994. 115(4): p. 417-23., Next question
Page 1430 :
Question 151 of 560, A 45 year old man has a long femoral line inserted to provide CVP measurements. The catheter, passes from the common iliac vein into the inferior vena cava. At which of the following vertebral, levels will this occur?, , L5, , L4, , S1, , L3, , L2, , The common iliac veins fuse with the IVC at L5., Please rate this question:, , Discuss and give feedback, , Next question, , Inferior vena cava, Origin, , , L5, , Path, , , , , , , , , Left and right common iliac veins merge to form the IVC., Passes right of midline, Paired segmental lumbar veins drain into the IVC throughout its length, The right gonadal vein empties directly into the cava and the left gonadal vein generally, empties into the left renal vein., The next major veins are the renal veins and the hepatic veins, Pierces the central tendon of diaphragm at T8, Right atrium
Page 1431 :
Image sourced from Wikipedia, , Relations, , Anteriorly, , Small bowel, first and third part of duodenum, head of pancreas, liver and bile duct,, right common iliac artery, right gonadal artery, , Posteriorly, , Right renal artery, right psoas, right sympathetic chain, coeliac ganglion, , Levels, , Level, , Vein, , T8, , Hepatic vein, inferior phrenic vein, pierces diaphragm, , L1, , Suprarenal veins, renal vein, , L2, , Gonadal vein, , L1-5, , Lumbar veins
Page 1433 :
Question 152 of 560, Following a carotid endarterectomy a man notices that he has a weakness of his tongue. Damage to, which of the following nerves is the most likely explanation for this process?, , Hypoglossal, , Accessory, , Ansa cervicalis, , Vagus, , Cervical plexus, , Theme from April 2013, The hypoglossal nerve innervates the tongue and is one of the structures more commonly at risk in, carotid surgery., Please rate this question:, , Discuss and give feedback, , Next question, , Internal carotid artery, The internal carotid artery is formed from the common carotid opposite the upper border of the, thyroid cartilage. It extends superiorly to enter the skull via the carotid canal. From the carotid canal, it then passes through the cavernous sinus, above which it divides into the anterior and middle, cerebral arteries., Relations in the neck, , Posterior, , , , , , , Longus capitis, Pre-vertebral fascia, Sympathetic chain, Superior laryngeal nerve, , Medially, , , , , External carotid (near origin), Wall of pharynx
Page 1434 :
, , Ascending pharyngeal artery, , Laterally, , , , , Internal jugular vein (moves posteriorly at entrance to skull), Vagus nerve (most posterolaterally), , Anteriorly, , , , , , Sternocleidomastoid, Lingual and facial veins, Hypoglossal nerve, , Relations in the carotid canal, , , , , , Internal carotid plexus, Cochlea and middle ear cavity, Trigeminal ganglion (superiorly), Leaves canal lies above the foramen lacerum, , Path and relations in the cranial cavity, The artery bends sharply forwards in the cavernous sinus, the aducens nerve lies close to its, inferolateral aspect. The oculomotor, trochlear, opthalmic and, usually, the maxillary nerves lie in the, lateral wall of the sinus. Near the superior orbital fissure it turns posteriorly and passes posteromedially to pierce the roof of the cavernous sinus inferior to the optic nerve. It then passes between, the optic and oculomotor nerves to terminate below the anterior perforated substance by dividing, into the anterior and middle cerebral arteries., Branches, , , , , , , , Anterior and middle cerebral artery, Ophthalmic artery, Posterior communicating artery, Anterior choroid artery, Meningeal arteries, Hypophyseal arteries, , Image demonstrating the internal carotid artery and its relationship to the external carotid artery
Page 1435 :
Image sourced from Wikipedia, , Next question
Page 1436 :
Question 153 of 560, At which of the following levels does the inferior vena cava exit the abdominal cavity?, , T6, , T7, , T10, , T8, , T12, , Theme from April 2012 exam, Theme from April 2014 exam, Please rate this question:, , Discuss and give feedback, , Next question, , Levels, Transpyloric plane, Level of the body of L1, , , , , , , , , , , , , , , Pylorus stomach, Left kidney hilum (L1- left one!), Fundus of the gallbladder, Neck of pancreas, Duodenojejunal flexure, Superior mesenteric artery, Portal vein, Left and right colic flexure, Root of the transverse mesocolon, 2nd part of the duodenum, Upper part of conus medullaris, Spleen
Page 1438 :
Question 154 of 560, Which of the following structures lies deepest in the popliteal fossa?, , Popliteal artery, , Popliteal vein, , Tibial nerve, , Common peroneal nerve, , Popliteal lymph nodes, , Theme from January 2012 exam, Theme from April 2014 exam, From superficial to deep:, The common peroneal nerve exits the popliteal fossa along the medial border of the biceps tendon., Then the tibial nerve lies lateral to the popliteal vessels to pass posteriorly and then medially to, them. The popliteal vein lies superficial to the popliteal artery, which is the deepest structure in the, fossa., Please rate this question:, , Discuss and give feedback, , Next question, , Popliteal fossa, Boundaries of the popliteal fossa, , Laterally, , Biceps femoris above, lateral head of gastrocnemius and plantaris below, , Medially, , Semimembranosus and semitendinosus above, medial head of gastrocnemius below, , Floor, , Popliteal surface of the femur, posterior ligament of knee joint and popliteus muscle
Page 1439 :
Superficial and deep fascia, , Roof, , Image showing the popliteal fossa, , © Image provided by the University of Sheffield, , Contents, , , , , , , , , Popliteal artery and vein, Small saphenous vein, Common peroneal nerve, Tibial nerve, Posterior cutaneous nerve of the thigh, Genicular branch of the obturator nerve, Lymph nodes, Next question
Page 1440 :
Question 155 of 560, Which of the following nerves is responsible for innervation of the triceps muscle?, , Radial, , Ulnar, , Axillary, , Median, , None of the above, To remember nerve roots and their reflexes:, 1-2 Ankle (S1-S2), 3-4 Knee (L3-L4), 5-6 Biceps (C5-C6), 7-8 Triceps (C7-C8), The radial nerve innervates all three heads of triceps, with a separate branch to each head., Please rate this question:, , Discuss and give feedback, , Next question, , Triceps, Origin, , , , , , Insertion, , , , , Long head- infraglenoid tubercle of the scapula., Lateral head- dorsal surface of the humerus, lateral and proximal to the, groove of the radial nerve, Medial head- posterior surface of the humerus on the inferomedial side of, the radial groove and both of the intermuscular septae, Olecranon process of the ulna. Here the olecranon bursa is between the, triceps tendon and olecranon., Some fibres insert to the deep fascia of the forearm, posterior capsule of the
Page 1441 :
elbow (preventing the capsule from being trapped between olecranon and, olecranon fossa during extension), , Innervation, , Radial nerve, , Blood, supply, , Profunda brachii artery, , Action, , Elbow extension. The long head can adduct the humerus and and extend it from a, flexed position, , Relations, , The radial nerve and profunda brachii vessels lie between the lateral and medial, heads, Next question
Page 1442 :
Question 156 of 560, , Which of the positions listed below best describes the location of the coeliac autonomic plexus?, , Anterolateral to the aorta, , Posterolateral to the aorta, , Anterolateral to the sympathetic chain, , Anteromedial to the sympathetic chain, , Posterior to L1, , Please rate this question:, , Discuss and give feedback, , Next question, , Coeliac plexus, The coeliac plexus is the largest of the autonomic plexuses. It is located on a level of the last, thoracic and first lumbar vertebrae. It surrounds the coeliac axis and the SMA. It lies posterior to the, stomach and the lesser sac. It lies anterior to the crura of the diaphragm and the aorta. The plexus, and ganglia are joined are joined by the greater and lesser splanchnic nerves on both sides and, branches from both the vagus and phrenic nerves.
Page 1443 :
Image sourced from Wikipedia, , Next question
Page 1444 :
Question 157 of 560, An intravenous drug user develops a false aneurysm and requires emergency surgery. The, procedure is difficult and the femoral nerve is inadvertently transected. Which of the following, muscles is least likely to be affected as a result?, , Sartorius, , Vastus medialis, , Pectineus, , Quadriceps femoris, , Adductor magnus, Mnemonic for femoral nerve supply, (don't) M I S V Q Scan for PE, M edial cutaneous nerve of the thigh, I ntermediate cutaneous nerve of the thigh, S aphenous nerve, V astus, Q uadriceps femoris, S artorius, PE ectineus, Adductor magnus is innervated by the obturator and sciatic nerve. The pectineus muscle is, sometimes supplied by the obturator nerve but this is variable. Since the question states least likely,, the correct answer is adductor magnus, Please rate this question:, , Discuss and give feedback, , Next question, , Femoral nerve
Page 1445 :
Root values, , L2, 3, 4, , Innervates, , , , , , , Pectineus, Sartorius, Quadriceps femoris, Vastus lateralis/medialis/intermedius, , Branches, , , , , , Medial cutaneous nerve of thigh, Saphenous nerve, Intermediate cutaneous nerve of thigh, , Path, Penetrates psoas major and exits the pelvis by passing under the inguinal ligament to enter the, femoral triangle, lateral to the femoral artery and vein., , Image sourced from Wikipedia
Page 1446 :
Mnemonic for femoral nerve supply, (don't) M I S V Q Scan for PE, M edial cutaneous nerve of the thigh, I ntermediate cutaneous nerve of the thigh, S aphenous nerve, V astus, Q uadriceps femoris, S artorius, PE ectineus, , Next question
Page 1447 :
Question 158 of 560, , What is the nerve root value of the external urethral sphincter?, , S4, , S1, S2, S3, , S2, S3, S4, , L3, L4, L5, , L5, S1, S2, , Theme from April 2012 exam, Theme from April 2013 exam, Theme from April 2014 exam, The external urethral sphincter is innervated by branches of the pudendal nerve, therefore the root, values are S2, S3, S4., Please rate this question:, , Discuss and give feedback, , Next question, , Urethral anatomy, Female urethra, The female urethra is shorter and more acutely angulated than the male urethra. It is an extraperitoneal structure and embedded in the endopelvic fascia. The neck of the bladder is subjected to, transmitted intra-abdominal pressure and therefore deficiency in this area may result in stress, urinary incontinence. Between the layers of the urogenital diaphragm the female urethra is, surrounded by the external urethral sphincter, this is innervated by the pudendal nerve. It ultimately
Page 1448 :
lies anterior to the vaginal orifice., Male urethra, In males the urethra is much longer and is divided into four parts., , Pre-prostatic, urethra, , Extremely short and lies between the bladder and prostate gland.It has a stellate lumen, and is between 1 and 1.5cm long.Innervated by sympathetic noradrenergic fibres, as, this region is composed of striated muscles bundles they may contract and prevent, retrograde ejaculation., , Prostatic, urethra, , This segment is wider than the membranous urethra and contains several openings for, the transmission of semen (at the midpoint of the urethral crest)., , Membranous, urethra, , Narrowest part of the urethra and surrounded by external sphincter. It traverses the, perineal membrane 2.5cm postero-inferior to the symphysis pubis., , Penile urethra, , Travels through the corpus spongiosum on the underside of the penis. It is the longest, urethral segment.It is dilated at its origin as the infrabulbar fossa and again in the gland, penis as the navicular fossa. The bulbo-urethral glands open into the spongiose section, of the urethra 2.5cm below the perineal membrane., , The urothelium is transitional in nature near to the bladder and becomes squamous more distally., Next question
Page 1449 :
Question 159 of 560, A 45 year old man is stabbed in the abdomen and the inferior vena cava is injured. How many, functional valves does this vessel usually have?, , 0, , 1, , 3, , 2, , 4, Mnemonic for the Inferior vena cava tributaries: I Like To Rise So High:, Iliacs, Lumbar, Testicular, Renal, Suprarenal, Hepatic vein, The lack of valves in the IVC is important clinically when it is cannulated during cardiopulmonary, bypass, using separate SVC and IVC catheters, such as when the right atrium is to be opened. Note, that there is a non functional valve between the right atrium and inferior vena cava., Please rate this question:, , Discuss and give feedback, , Next question, , Inferior vena cava, Origin, , , L5
Page 1450 :
Path, , , , , , , , , Left and right common iliac veins merge to form the IVC., Passes right of midline, Paired segmental lumbar veins drain into the IVC throughout its length, The right gonadal vein empties directly into the cava and the left gonadal vein generally, empties into the left renal vein., The next major veins are the renal veins and the hepatic veins, Pierces the central tendon of diaphragm at T8, Right atrium, , Image sourced from Wikipedia, , Relations, , Anteriorly, , Small bowel, first and third part of duodenum, head of pancreas, liver and bile duct,, right common iliac artery, right gonadal artery, , Posteriorly, , Right renal artery, right psoas, right sympathetic chain, coeliac ganglion, , Levels, , Level, , Vein
Page 1453 :
Question 161 of 560, Which of the following statements relating to the root of the neck is false?, , The lung projects into the neck beyond the first rib and is constrained by Sibson's fascia, , The subclavian artery arches over the first rib anterior to scalenus anterior, , The roots and trunks of the Brachial plexus lie posterior to the subclavian artery on the, first rib, The roots and trunks of the Brachial plexus lie between scalenus anterior and scalenus, medius muscles, The thyrocervical trunk is a branch of the subclavian artery, , The subclavian artery lies posterior to scalenus anterior, the vein lies in front. Sibson's fascia is, another name for the suprapleural membrane., Please rate this question:, , Discuss and give feedback, , Next question, , Root of the neck, Thoracic Outlet, , , , , , , , Where the subclavian artery and vein and the brachial plexus exit the thorax and enter the, arm., They pass over the 1st rib and under the clavicle., The subclavian vein is the most anterior structure and is immediately anterior to scalenus, anterior and its attachment to the first rib., Scalenus anterior has 2 parts, the subclavian artery leaves the thorax by passing over the, first rib and between these 2 portions of the muscle., At the level of the first rib, the lower cervical nerve roots combine to form the 3 trunks of the, brachial plexus. The lowest trunk is formed by the union of C8 and T1, and this trunk lies, directly posterior to the artery and is in contact with the superior surface of the first rib.
Page 1454 :
Thoracic outlet obstruction causes neurovascular compromise., Next question
Page 1455 :
Question 162 of 560, , A patient presents to the clinic following a surgical procedure. She complains that she is unable to, shrug her shoulder. What is the most likely underlying nerve injury?, , Accessory nerve, , Cervical plexus, , Ansa cervicalis, , Long thoracic nerve, , Axillary nerve, , Theme from April 2013 exam, Theme from April 2014 exam, The accessory nerve may be injured in operations in the posterior triangle. Injury will affect, trapezius., Please rate this question:, , Discuss and give feedback, , Next question, , Cranial nerves, Cranial nerve lesions, , Olfactory nerve, , May be injured in basal skull fractures or involved in frontal lobe tumour extension., Loss of olfactory nerve function in relation to major CNS pathology is seldom an
Page 1456 :
isolated event and thus it is poor localiser of CNS pathology., , Optic nerve, , Problems with visual acuity may result from intra ocular disorders. Problems with, the blood supply such as amaurosis fugax may produce temporary visual distortion., More important surgically is the pupillary response to light. The pupillary size may, be altered in a number of disorders. Nerves involved in the resizing of the pupil, connect to the pretectal nucleus of the high midbrain, bypassing the lateral, geniculate nucleus and the primary visual cortex. From the pretectal nucleus, neurones pass to the Edinger - Westphal nucleus, motor axons from here pass along, with the oculomotor nerve. They synapse with ciliary ganglion neurones; the, parasympathetic axons from this then innervate the iris and produce miosis. The, miotic pupil is seen in disorders such as Horner's syndrome or opiate overdose., Mydriasis is the dilatation of the pupil in response to disease, trauma, drugs (or the, dark!). It is pathological when light fails to induce miosis. The radial muscle is, innervated by the sympathetic nervous system. Because the parasympathetic fibres, travel with the oculomotor nerve they will be damaged by lesions affecting this, nerve (e.g. cranial trauma)., The response to light shone in one eye is usually a constriction of both pupils. This, indicates intact direct and consensual light reflexes. When the optic nerve has an, afferent defect the light shining on the affected eye will produce a diminished, pupillary response in both eyes. Whereas light shone on the unaffected eye will, produce a normal pupillary response in both eyes. This is referred to as the Marcus, Gunn pupil and is seen in conditions such as optic neuritis. In a total CN II lesion, shining the light in the affected eye will produce no response., , Oculomotor nerve, , The pupillary effects are described above. In addition it supplies all ocular muscles, apart from lateral rectus and superior oblique. Thus the affected eye will be, deviated inferolaterally. Levator palpebrae superioris may also be impaired resulting, in impaired ability to open the eye., , Trochlear nerve, , The eye will not be able to look down., , Trigeminal nerve, , Largest cranial nerve. Exits the brainstem at the pons. Branches are ophthalmic,, maxillary and mandibular. Only the mandibular branch has both sensory and motor, fibres. Branches converge to form the trigeminal ganglion (located in Meckels cave)., It supplies the muscles of mastication and also tensor veli palatine, mylohyoid,, anterior belly of digastric and tensor tympani. The detailed descriptions of the
Page 1457 :
various sensory functions are described in other areas of the website. The corneal, reflex is important and is elicited by applying a small tip of cotton wool to the, cornea, a reflex blink should occur if it is intact. It is mediated by: the naso ciliary, branch of the ophthalmic branch of the trigeminal (sensory component) and the, facial nerve producing the motor response. Lesions of the afferent arc will produce, bilateral absent blink and lesions of the efferent arc will result in a unilateral absent, blink., , Abducens nerve, , The affected eye will have a deficit of abduction. This cranial nerve exits the, brainstem between the pons and medulla. It thus has a relatively long intra cranial, course which renders it susceptible to damage in raised intra cranial pressure., , Facial nerve, , Emerges from brainstem between pons and medulla. It controls muscles of facial, expression and taste from the anterior 2/3 of the tongue. The nerve passes into the, petrous temporal bone and into the internal auditory meatus. It then passes, through the facial canal and exits at the stylomastoid foramen. It passes through the, parotid gland and divides at this point. It does not innervate the parotid gland. Its, divisions are considered in other parts of the website. Its motor fibres innervate, orbicularis oculi to produce the efferent arm of the corneal reflex. In surgical, practice it may be injured during parotid gland surgery or invaded by malignancies, of the gland and a lower motor neurone on the ipsilateral side will result., , Vestibulo-cochlear, nerve, , Exits from the pons and then passes through the internal auditory meatus. It is, implicated in sensorineural hearing loss. Individuals with sensorineural hearing loss, will localise the sound in webers test to the normal ear. Rinnes test will be reduced, on the affected side but should still work. These two tests will distinguish, sensorineural hearing loss from conductive deafness. In the latter condition webers, test will localise to the affected ear and Rinnes test will be impaired on the affected, side. Surgical lesions affecting this nerve include CNS tumours and basal skull, fractures. It may also be damaged by the administration of ototoxic drugs (of which, gentamicin is the most commonly used in surgical practice)., , Glossopharyngeal, nerve, , Exits the pons just above the vagus. Receives sensory fibres from posterior 1/3, tongue, tonsils, pharynx and middle ear (otalgia may occur following tonsillectomy)., It receives visceral afferents from the carotid bodies. It supplies parasympathetic, fibres to the parotid gland via the otic ganglion and motor function to, stylopharyngeaus muscle. The sensory function of the nerve is tested using the gag
Page 1458 :
reflex., , Vagus nerve, , Leaves the medulla between the olivary nucleus and the inferior cerebellar, peduncle. Passes through the jugular foramen and into the carotid sheath. Details of, the functions of the vagus nerve are covered in the website under relevant organ, sub headings., , Accessory nerve, , Exists from the caudal aspect of the brainstem (multiple branches) supplies, trapezius and sternocleidomastoid muscles. The distal portion of this nerve is most, prone to injury during surgical procedures., , Hypoglossal nerve, , Emerges from the medulla at the preolivary sulcus, passes through the hypoglossal, canal. It lies on the carotid sheath and passes deep to the posterior belly of digastric, to supply muscles of the tongue (except palatoglossus). Its location near the carotid, sheath makes it vulnerable during carotid endarterectomy surgery and damage will, produce ipsilateral defect in muscle function., Next question
Page 1459 :
Question 163 of 560, Which of the following are not generally supplied by the right coronary artery?, , The sino atrial node, , The circumflex artery, , The atrioventricular node, , Most of the right ventricle, , The right atrium, , The circumflex artery is generally a branch of the left coronary artery., Please rate this question:, , Discuss and give feedback, , Next question, , Heart anatomy, The walls of each cardiac chamber comprise:, , , , , Epicardium, Myocardium, Endocardium, , Cardiac muscle is attached to the cardiac fibrous skeleton., Relations, The heart and roots of the great vessels within the pericardial sac are related anteriorly to the, sternum, medial ends of the 3rd to 5th ribs on the left and their associated costal cartilages. The, heart and pericardial sac are situated obliquely two thirds to the left and one third to the right of the, median plane., The pulmonary valve lies at the level of the left third costal cartilage., The mitral valve lies at the level of the fourth costal cartilage.
Page 1460 :
Coronary sinus, This lies in the posterior part of the coronary groove and receives blood from the cardiac veins. The, great cardiac vein lies at its left and the middle and small cardiac veins lie on its right. The smallest, cardiac vein (anterior cardiac vein) drains into the right atrium directly., Aortic sinus, Right coronary artery arises from the right aortic sinus, the left is derived from the left aortic sinus,, which lies posteriorly., Right and left ventricles, , Structure, , Left Ventricle, , A-V Valve, , Mitral (double leaflet), , Walls, , Twice as thick as right, , Trabeculae carnae, , Much thicker and more numerous, , Right coronary artery, The RCA supplies:, , , , , , , Right atrium, Diaphragmatic part of the left ventricle, Usually the posterior third of the interventricular septum, The sino atrial node (60% cases), The atrio ventricular node (80% cases), , Left coronary artery, The LCA supplies:, , , , , , , Left atrium, Most of left ventricle, Part of the right ventricle, Anterior two thirds of the inter ventricular septum, The sino atrial node (remaining 40% cases), , Innervation of the heart, Autonomic nerve fibres from the superficial and deep cardiac plexus. These lie anterior to the, bifurcation of the trachea, posterior to the ascending aorta and superior to the bifurcation of the, pulmonary trunk. The parasympathetic supply to the heart is from presynaptic fibres of the vagus, nerves.
Page 1461 :
Valves of the heart, , Mitral valve, , Aortic valve, , Pulmonary valve, , Tricuspid valve, , 2 cusps, , 3 cusps, , 3 cusps, , 3 cusps, , First heart sound, , Second heart, sound, , Second heart, sound, , First heart sound, , 1 anterior cusp, , 2 anterior cusps, , 2 anterior cusps, , 2 anterior cusps, , Attached to chordae, tendinae, , No chordae, , No chordae, , Attached to chordae, tendinae, Next question
Page 1462 :
Question 164 of 560, A 44 year old man has a malignant melanoma and is undergoing a block dissection of the groin. The, femoral triangle is being explored for intra operative bleeding. Which of the following forms the, medial border of the femoral triangle?, , Femoral artery, , Biceps femoris, , Adductor longus, , Sartorius, , Adductor magnus, Vastus medialis forms the lateral border of the adductor canal. The sartorius muscles forms the roof, of the adductor canal., Adductor longus forms the medial boundary of the femoral triangle (see below)., Please rate this question:, , Discuss and give feedback, , Next question, , Femoral triangle anatomy, Boundaries, , Superiorly, , Inguinal ligament, , Laterally, , Sartorius, , Medially, , Adductor longus, , Floor, , Iliopsoas, adductor longus and pectineus
Page 1463 :
, , , , Roof, , Fascia lata and Superficial fascia, Superficial inguinal lymph nodes (palpable below the inguinal ligament), Long saphenous vein, , Image sourced from Wikipedia, , Contents, , , , , , , , , Femoral vein (medial to lateral), Femoral artery-pulse palpated at the mid inguinal point, Femoral nerve, Deep and superficial inguinal lymph nodes, Lateral cutaneous nerve, Great saphenous vein, Femoral branch of the genitofemoral nerve, Next question
Page 1465 :
Borders, , Contents, , Roof Sartorius, , Superficial femoral vein, , In the image below the sartorius muscle is removed to expose the canal contents, , Image sourced from Wikipedia, , Next question
Page 1466 :
Question 166 of 560, , Which of the following is the first vessel to branch from the external carotid artery?, , Superior thyroid artery, , Inferior thyroid artery, , Lingual artery, , Facial artery, , Occipital artery, Mnemonic, (Order in which they branch off)Some (sup thyroid)Attendings (Ascending Pharyngeal)Like, (Lingual)Freaking (Facial)Out (Occipital)Potential (Post auricular)Medical (Maxillary)Students (Sup, temporal), , The first branch of the external carotid artery is the superior thyroid artery. The inferior thyroid artery, is derived from the thyrocervical trunk. The other branches are illustrated below., Please rate this question:, , Discuss and give feedback, , Next question, , External carotid artery, The external carotid commences immediately lateral to the pharyngeal side wall. It ascends and lies, anterior to the internal carotid and posterior to the posterior belly of digastric and stylohyoid. More, inferiorly it is covered by sternocleidomastoid, passed by hypoglossal nerves, lingual and facial, veins.
Page 1467 :
It then pierces the fascia of the parotid gland finally dividing into its terminal branches within the, gland itself., Surface marking of the carotid, This is an imaginary line drawn from the bifurcation of the common carotid passing behind the angle, of the jaw to a point immediately anterior to the tragus of the ear., Branches of the external carotid artery, It has six branches, three in front, two behind and one deep., , Three in front, , Superior thyroid, Lingual, Facial, , Two behind, , Occipital, Posterior auricular, , Deep, , Ascending pharyngeal, , It terminates by dividing into the superficial temporal and maxillary arteries in the parotid gland.
Page 1468 :
Image sourced from Wikipedia, , Next question
Page 1469 :
Question 167 of 560, , A motorcyclist is injured in a road traffic accident and is not wearing a helmet. He suffers a severe, closed head injury and develops raised intracranial pressure. The first cranial nerve to be affected by, this process is likely to be:, , Oculomotor, , Hypoglossal, , Motor branch of the trigeminal, , Abducens, , Sensory branch of the trigeminal, , Theme from April 2014 exam, The abducens nerve (CN VI) has a long intra cranial course and is thus susceptible to raised intra, cranial pressure. It also passes over the petrous temporal bone and 6th nerve palsies are also seen, in mastoiditis., Please rate this question:, , Discuss and give feedback, , Next question, , Cranial nerves, Cranial nerve lesions, , Olfactory nerve, , May be injured in basal skull fractures or involved in frontal lobe tumour extension., Loss of olfactory nerve function in relation to major CNS pathology is seldom an
Page 1470 :
isolated event and thus it is poor localiser of CNS pathology., , Optic nerve, , Problems with visual acuity may result from intra ocular disorders. Problems with, the blood supply such as amaurosis fugax may produce temporary visual distortion., More important surgically is the pupillary response to light. The pupillary size may, be altered in a number of disorders. Nerves involved in the resizing of the pupil, connect to the pretectal nucleus of the high midbrain, bypassing the lateral, geniculate nucleus and the primary visual cortex. From the pretectal nucleus, neurones pass to the Edinger - Westphal nucleus, motor axons from here pass along, with the oculomotor nerve. They synapse with ciliary ganglion neurones; the, parasympathetic axons from this then innervate the iris and produce miosis. The, miotic pupil is seen in disorders such as Horner's syndrome or opiate overdose., Mydriasis is the dilatation of the pupil in response to disease, trauma, drugs (or the, dark!). It is pathological when light fails to induce miosis. The radial muscle is, innervated by the sympathetic nervous system. Because the parasympathetic fibres, travel with the oculomotor nerve they will be damaged by lesions affecting this, nerve (e.g. cranial trauma)., The response to light shone in one eye is usually a constriction of both pupils. This, indicates intact direct and consensual light reflexes. When the optic nerve has an, afferent defect the light shining on the affected eye will produce a diminished, pupillary response in both eyes. Whereas light shone on the unaffected eye will, produce a normal pupillary response in both eyes. This is referred to as the Marcus, Gunn pupil and is seen in conditions such as optic neuritis. In a total CN II lesion, shining the light in the affected eye will produce no response., , Oculomotor nerve, , The pupillary effects are described above. In addition it supplies all ocular muscles, apart from lateral rectus and superior oblique. Thus the affected eye will be, deviated inferolaterally. Levator palpebrae superioris may also be impaired resulting, in impaired ability to open the eye., , Trochlear nerve, , The eye will not be able to look down., , Trigeminal nerve, , Largest cranial nerve. Exits the brainstem at the pons. Branches are ophthalmic,, maxillary and mandibular. Only the mandibular branch has both sensory and motor, fibres. Branches converge to form the trigeminal ganglion (located in Meckels cave)., It supplies the muscles of mastication and also tensor veli palatine, mylohyoid,, anterior belly of digastric and tensor tympani. The detailed descriptions of the
Page 1471 :
various sensory functions are described in other areas of the website. The corneal, reflex is important and is elicited by applying a small tip of cotton wool to the, cornea, a reflex blink should occur if it is intact. It is mediated by: the naso ciliary, branch of the ophthalmic branch of the trigeminal (sensory component) and the, facial nerve producing the motor response. Lesions of the afferent arc will produce, bilateral absent blink and lesions of the efferent arc will result in a unilateral absent, blink., , Abducens nerve, , The affected eye will have a deficit of abduction. This cranial nerve exits the, brainstem between the pons and medulla. It thus has a relatively long intra cranial, course which renders it susceptible to damage in raised intra cranial pressure., , Facial nerve, , Emerges from brainstem between pons and medulla. It controls muscles of facial, expression and taste from the anterior 2/3 of the tongue. The nerve passes into the, petrous temporal bone and into the internal auditory meatus. It then passes, through the facial canal and exits at the stylomastoid foramen. It passes through the, parotid gland and divides at this point. It does not innervate the parotid gland. Its, divisions are considered in other parts of the website. Its motor fibres innervate, orbicularis oculi to produce the efferent arm of the corneal reflex. In surgical, practice it may be injured during parotid gland surgery or invaded by malignancies, of the gland and a lower motor neurone on the ipsilateral side will result., , Vestibulo-cochlear, nerve, , Exits from the pons and then passes through the internal auditory meatus. It is, implicated in sensorineural hearing loss. Individuals with sensorineural hearing loss, will localise the sound in webers test to the normal ear. Rinnes test will be reduced, on the affected side but should still work. These two tests will distinguish, sensorineural hearing loss from conductive deafness. In the latter condition webers, test will localise to the affected ear and Rinnes test will be impaired on the affected, side. Surgical lesions affecting this nerve include CNS tumours and basal skull, fractures. It may also be damaged by the administration of ototoxic drugs (of which, gentamicin is the most commonly used in surgical practice)., , Glossopharyngeal, nerve, , Exits the pons just above the vagus. Receives sensory fibres from posterior 1/3, tongue, tonsils, pharynx and middle ear (otalgia may occur following tonsillectomy)., It receives visceral afferents from the carotid bodies. It supplies parasympathetic, fibres to the parotid gland via the otic ganglion and motor function to, stylopharyngeaus muscle. The sensory function of the nerve is tested using the gag
Page 1472 :
reflex., , Vagus nerve, , Leaves the medulla between the olivary nucleus and the inferior cerebellar, peduncle. Passes through the jugular foramen and into the carotid sheath. Details of, the functions of the vagus nerve are covered in the website under relevant organ, sub headings., , Accessory nerve, , Exists from the caudal aspect of the brainstem (multiple branches) supplies, trapezius and sternocleidomastoid muscles. The distal portion of this nerve is most, prone to injury during surgical procedures., , Hypoglossal nerve, , Emerges from the medulla at the preolivary sulcus, passes through the hypoglossal, canal. It lies on the carotid sheath and passes deep to the posterior belly of digastric, to supply muscles of the tongue (except palatoglossus). Its location near the carotid, sheath makes it vulnerable during carotid endarterectomy surgery and damage will, produce ipsilateral defect in muscle function., Next question
Page 1473 :
Question 168 of 560, A 32 year old man is undergoing a splenectomy. Division of which of the following will be necessary, during the procedure?, , Left crus of diaphragm, , Short gastric vessels, , Gerotas fascia, , Splenic flexure of colon, , Marginal artery, , Theme from 2011 Exam, During a splenectomy the short gastric vessels which lie within the gastrosplenic ligament will need, to be divided. The splenic flexure of the colon may need to be mobilised. However, it will almost, never need to be divided, as this is watershed area that would necessitate a formal colonic resection, in the event of division., Please rate this question:, , Discuss and give feedback, , Next question, , Splenic anatomy, The spleen is the largest lymphoid organ in the body. It is an intraperitoneal organ, the peritoneal, attachments condense at the hilum where the vessels enter the spleen. Its blood supply is from the, splenic artery (derived from the coeliac axis) and the splenic vein (which is joined by the IMV and, unites with the SMV)., , , , , , , Embryology: derived from mesenchymal tissue, Shape: clenched fist, Position: below 9th-12th ribs, Weight: 75-150g
Page 1476 :
© Image provided by the University of Sheffield, , Next question
Page 1477 :
Question 170 of 560, , A 24 year old motor cyclist is involved in a road traffic accident. He suffers a tibial fracture which is, treated with an intra medullary nail. Post operatively he develops a compartment syndrome. Surgical, decompression of the anterior compartment will relieve pressure on all of the following muscles, except?, , Peroneus brevis, , Peroneus tertius, , Extensor digitorum longus, , Tibialis anterior, , None of the above, , The anterior compartment contains:, Tibialis anterior, Extensor digitorum longus, Peroneus tertius, Extensor hallucis longus, Anterior tibial artery, All the muscles are innervated by the deep peroneal nerve., Please rate this question:, , Discuss and give feedback, , Next question, , Lower limb- Muscular compartments, Anterior compartment
Page 1480 :
Question 171 of 560, A 43 year old lady underwent an attempted placement of a central line into the internal jugular vein., Unfortunately, the doctor damaged the carotid artery and this necessitated surgical exploration. As, the surgeons incise the carotid sheath a nerve is identified lying between the internal jugular vein, and the carotid artery. Which of the following is this nerve most likely to be?, , Glossopharyngeal nerve, , Hypoglossal nerve, , Superior laryngeal nerve, , Recurrent laryngeal nerve, , Vagus, , The vagus lies in the carotid sheath. The hypoglossal nerve crosses the sheath, but does not lie, within it., Please rate this question:, , Discuss and give feedback, , Next question, , Common carotid artery, The right common carotid artery arises at the bifurcation of the brachiocephalic trunk, the left, common carotid arises from the arch of the aorta. Both terminate at the level of the upper border of, the thyroid cartilage (the lower border of the third cervical vertebra) by dividing into the internal and, external carotid arteries., Left common carotid artery, This vessel arises immediately to the left and slightly behind the origin of the brachiocephalic trunk., Its thoracic portion is 2.5- 3.5 cm in length and runs superolaterally to the sternoclavicular joint., In the thorax, The vessel is in contact, from below upwards, with the trachea, left recurrent laryngeal nerve, left, margin of the oesophagus. Anteriorly the left brachiocephalic vein runs across the artery, and the, cardiac branches from the left vagus descend in front of it. These structures together with the, thymus and the anterior margins of the left lung and pleura separate the artery from the manubrium.
Page 1481 :
In the neck, The artery runs superiorly deep to sternocleidomastoid and then enters the anterior triangle. At this, point it lies within the carotid sheath with the vagus nerve and the internal jugular vein. Posteriorly, the sympathetic trunk lies between the vessel and the prevertebral fascia. At the level of C7 the, vertebral artery and thoracic duct lie behind it. The anterior tubercle of C6 transverse process is, prominent and the artery can be compressed against this structure (it corresponds to the level of the, cricoid)., Anteriorly at C6 the omohyoid muscle passes superficial to the artery., Within the carotid sheath the jugular vein lies lateral to the artery., Right common carotid artery, The right common carotid arises from the brachiocephalic artery. The right common carotid artery, corresponds with the cervical portion of the left common carotid, except that there is no thoracic duct, on the right. The oesophagus is less closely related to the right carotid than the left., Summary points about the carotid anatomy, Path, Passes behind the sternoclavicular joint (12% patients above this level) to the upper border of the, thyroid cartilage, to divide into the external (ECA) and internal carotid arteries (ICA)., Relations, , , , , , , Level of 6th cervical vertebra crossed by omohyoid, Then passes deep to the thyrohyoid, sternohyoid, sternomastoid muscles., Passes anterior to the carotid tubercle (transverse process 6th cervical vertebra)-NB, compression here stops haemorrhage., The inferior thyroid artery passes posterior to the common carotid artery., Then : Left common carotid artery crosses the thoracic duct, Right common carotid artery, crossed by recurrent laryngeal nerve
Page 1482 :
Image sourced from Wikipedia, , Next question
Page 1483 :
Question 172 of 560, , A patient has a chest drain insertion. There is fresh blood at the chest drain insertion area. Which, vessel has been damaged?, , Pericardiophrenic artery, , Intercostal vein, , Right ventricle, , Vagus artery, , Intercostal artery, The intercostal vein is more superior than the artery and is thus slightly less susceptible to injury., , Theme from 2009 Exam, Within the intercostal spaces there are thin, strong muscles, intercostal vessels, nerves and, lymphatics. There are 3 intercostal muscle layers corresponding to the lateral abdominal wall;, external, internal, innermost intercostals. At the mid axillary line there are thin intracostals which is, an extension of the internal intercostal muscle. In each intercostal space lies the neurovascular, bundle, comprising, from superior to inferiorly; the posterior intercostal vein, artery and nerve, lying, protected in the subcostal groove of the rib above and situated between the second and third layer, of the intercostal muscles. These blood vessels anastomose anteriorly with the anterior intercostal, vessels, which arise from the internal thoracic artery and vein., Please rate this question:, , Discuss and give feedback, , Next question, , Chest drains
Page 1484 :
There are a number of different indications for chest drain insertion. In general terms large bore, chest drains are preferred for trauma and haemothorax drainage. Smaller diameter chest drains can, be used for pneumothorax or pleural effusion drainage., Insertion can be performed either using anatomical guidance or through ultrasound guidance. In the, exam, the anatomical method is usually tested., It is advised that chest drains are placed in the 'safe triangle'. The triangle is located in the mid, axillary line of the 5th intercostal space. It is bordered by:, Anterior edge latissimus dorsi, the lateral border of pectoralis major, a line superior to the horizontal, level of the nipple, and the apex below the axilla., Another triangle is situated behind the scapula. It is bounded above by the trapezius, below by the, latissimus dorsi, and laterally by the vertebral border of the scapula; the floor is partly formed by the, rhomboid major. If the scapula is drawn forward by folding the arms across the chest, and the trunk, bent forward, parts of the sixth and seventh ribs and the interspace between them become, subcutaneous and available for auscultation. The space is therefore known as the triangle of, auscultation., References, Prof Harold Ellis. The applied anatomy of chest drains insertions. British Journal of hospital medicine, 2007; (68): 44-45., Laws D, Neville E, Duffy J. BTS guidelines for insertion of chest drains. Thorax, 2003; (58): 53-59., Next question
Page 1485 :
Question 173 of 560, Two teenagers are playing with an airgun when one accidentally shoots his friend in the abdomen., He is brought to the emergency department. On examination there is a bullet entry point immediately, to the right of the rectus sheath at the level of the 1st lumbar vertebra. Which of the following, structures is most likely to be injured by the bullet?, , Head of pancreas, , Right ureter, , Right adrenal gland, , Fundus of the gallbladder, , Gastric antrum, , Theme from September 2011 Exam, Theme from April 2014 exam, The fundus of the gallbladder lies at this level and is the most superficially located structure., Please rate this question:, , Discuss and give feedback, , Next question, , Levels, Transpyloric plane, Level of the body of L1, , , , , , , , , , , Pylorus stomach, Left kidney hilum (L1- left one!), Fundus of the gallbladder, Neck of pancreas, Duodenojejunal flexure, Superior mesenteric artery, Portal vein, Left and right colic flexure
Page 1487 :
Question 174 of 560, Which of the following muscles inserts onto the lesser tuberostiy of the the humerus?, , Subscapularis, , Deltoid, , Supraspinatus, , Teres minor, , Infraspinatus, , With the exception of subscapularis which inserts into the lesser tuberosity, the muscles of the, rotator cuff insert into the greater tuberosity., Please rate this question:, , Discuss and give feedback, , Next question, , Shoulder joint, , , , , Shallow synovial ball and socket type of joint., It is an inherently unstable joint, but is capable to a wide range of movement., Stability is provided by muscles of the rotator cuff that pass from the scapula to insert in the, greater tuberosity (all except sub scapularis-lesser tuberosity)., , Glenoid labrum, , , , , Fibrocartilaginous rim attached to the free edge of the glenoid cavity, Tendon of the long head of biceps arises from within the joint from the supraglenoid tubercle,, and is fused at this point to the labrum., The long head of triceps attaches to the infraglenoid tubercle, , Fibrous capsule
Page 1490 :
Question 175 of 560, Which of the following nerves is not contained within the posterior triangle of the neck?, , Accessory nerve, , Phrenic nerve, , Greater auricular nerve, , Ansa cervicalis, , Lesser occiptal nerve, , Theme from September 2012 Exam, Ansa cervicalis is a content of the anterior triangle of the neck., Please rate this question:, , Discuss and give feedback, , Next question, , Posterior triangle of the neck, Boundaries, , Apex, , Sternocleidomastoid and the Trapezius muscles at the Occipital bone, , Anterior, , Posterior border of the Sternocleidomastoid, , Posterior, , Anterior border of the Trapezius, , Base, , Middle third of the clavicle
Page 1491 :
Image sourced from Wikipedia, , Contents, , Nerves, , , , , , , Accessory nerve, Phrenic nerve, Three trunks of the brachial plexus, Branches of the cervical plexus: Supraclavicular nerve, transverse cervical, nerve, great auricular nerve, lesser occipital nerve, , Vessels, , , , , External jugular vein, Subclavian artery, , Muscles, , , , , Inferior belly of omohyoid, Scalene, , Lymph, nodes, , , , , Supraclavicular, Occipital, Next question
Page 1492 :
Question 176 of 560, , A 42 year old lady is reviewed in the outpatient clinic following a routine surgical procedure. She, complains of diminished sensation at the dorso-lateral aspect of her foot. Which of the following, nerves is most likely to be affected?, , Sural, , Superficial peroneal, , Deep peroneal, , Medial plantar, , Lateral plantar, , Theme from April 2012 Exam, The sural nerve supplies the lateral aspect of the foot. It runs alongside the short saphenous vein, and may be injured in short saphenous vein surgery., Please rate this question:, , Discuss and give feedback, , Next question, , Foot- Cutaneous sensation, Region, , Nerve
Page 1493 :
Lateral plantar, , Sural, , Dorsum (not 1st web space), , Superficial peroneal, , 1st Web space, , Deep peroneal, , Extremities of toes, , Medial and lateral plantar nerves, , Proximal plantar, , Tibial, , Medial plantar, , Medial plantar nerve, , Lateral plantar, , Lateral plantar nerve
Page 1494 :
Image sourced from Wikipedia, , Next question
Page 1495 :
Question 177 of 560, Which of the following anatomical planes separates the prostate from the rectum?, , Sibsons fascia, , Denonvilliers fascia, , Levator ani muscle, , Waldeyers fascia, , None of the above, , Theme from April 2014 exam, The Denonvilliers fascia separates the rectum from the prostate. Waldeyers fascia separates the, rectum from the sacrum, Please rate this question:, , Discuss and give feedback, , Next question, , Prostate gland, The prostate gland is approximately the shape and size of a walnut and is located inferior to the, bladder. It is separated from the rectum by Denonvilliers fascia and its blood supply is derived from, the internal iliac vessels (via inferior vesical artery). The internal sphincter lies at the apex of the, gland and may be damaged during prostatic surgery, affected individuals may complain of, retrograde ejaculation., Summary of prostate gland, , Arterial supply, , Inferior vesical artery (from internal iliac), , Venous drainage, , Prostatic venous plexus (to paravertebral veins), , Lymphatic, , Internal iliac nodes
Page 1496 :
drainage, , Innervation, , Inferior hypogastric plexus, , Dimensions, , , , , , Transverse diameter (4cm), AP diameter (2cm), Height (3cm), , Lobes, , , , , , , Posterior lobe: posterior to urethra, Median lobe: posterior to urethra, in between ejaculatory ducts, Lateral lobes x 2, Isthmus, , Zones, , , , Peripheral zone: subcapsular portion of posterior prostate. Most, prostate cancers are here, Central zone, Transition zone, Stroma, , , , , , Relations, , Anterior, , Pubic symphysis, Prostatic venous plexus, , Posterior, , Denonvilliers fascia, Rectum, Ejaculatory ducts, , Lateral, , Venous plexus (lies on prostate), Levator ani (immediately below the puboprostatic ligaments)
Page 1497 :
Image sourced from Wikipedia, , Next question
Page 1498 :
Question 178 of 560, , A 56 year old lady is undergoing an adrenalectomy for Conns syndrome. During the operation the, surgeon damages the middle adrenal artery and haemorrhage ensues. From which of the following, structures does this vessel originate?, , Aorta, , Renal artery, , Splenic artery, , Coeliac axis, , Superior mesenteric artery, , The middle adrenal artery is usually a branch of the aorta, the lower adrenal artery typically arises, from the renal vessels., Please rate this question:, , Discuss and give feedback, , Next question, , Adrenal gland anatomy, Anatomy, , Location, , Superomedially to the upper pole of each kidney
Page 1499 :
Relationships of the right, adrenal, , Diaphragm-Posteriorly, Kidney-Inferiorly, Vena Cava-Medially, Hepato-renal, pouch and bare area of the liver-Anteriorly, , Relationships of the left, adrenal, , Crus of the diaphragm-Postero- medially, Pancreas and splenic vesselsInferiorly, Lesser sac and stomach-Anteriorly, , Arterial supply, , Superior adrenal arteries- from inferior phrenic artery, Middle adrenal, arteries - from aorta, Inferior adrenal arteries -from renal arteries, , Venous drainage of the, right adrenal, , Via one central vein directly into the IVC, , Venous drainage of the, left adrenal, , Via one central vein into the left renal vein, , Next question
Page 1500 :
Question 179 of 560, A 73 year old lady suffers a fracture at the surgical neck of the humerus. The decision is made to, operate. There are difficulties in reducing the fracture and a vessel lying posterior to the surgical, neck is injured. Which of the following is this vessel most likely to be?, , Axillary artery, , Brachial artery, , Thoracoacromial artery, , Transverse scapular artery, , Posterior circumflex humeral artery, , The circumflex humeral arteries lie at the surgical neck and is this scenario the posterior circumflex, is likely to be injured. The thoracoacromial and transverse scapular arteries lie more superomedially., The posterior circumflex humeral artery is a branch of the axillary artery., Please rate this question:, , Discuss and give feedback, , Next question, , Shoulder joint, , , , , Shallow synovial ball and socket type of joint., It is an inherently unstable joint, but is capable to a wide range of movement., Stability is provided by muscles of the rotator cuff that pass from the scapula to insert in the, greater tuberosity (all except sub scapularis-lesser tuberosity)., , Glenoid labrum, , , , , Fibrocartilaginous rim attached to the free edge of the glenoid cavity, Tendon of the long head of biceps arises from within the joint from the supraglenoid tubercle,, and is fused at this point to the labrum., The long head of triceps attaches to the infraglenoid tubercle
Page 1503 :
Question 180 of 560, Which of the structures listed below lies posterior to the carotid sheath at the level of the 6th cervical, vertebra?, , Hypoglossal nerve, , Vagus nerve, , Cervical sympathetic chain, , Ansa cervicalis, , Glossopharyngeal nerve, , The carotid sheath is crossed anteriorly by the hypoglossal nerves and the ansa cervicalis. The, vagus lies within it. The cervical sympathetic chain lies posteriorly between the sheath and the, prevertebral fascia., Please rate this question:, , Discuss and give feedback, , Next question, , Common carotid artery, The right common carotid artery arises at the bifurcation of the brachiocephalic trunk, the left, common carotid arises from the arch of the aorta. Both terminate at the level of the upper border of, the thyroid cartilage (the lower border of the third cervical vertebra) by dividing into the internal and, external carotid arteries., Left common carotid artery, This vessel arises immediately to the left and slightly behind the origin of the brachiocephalic trunk., Its thoracic portion is 2.5- 3.5 cm in length and runs superolaterally to the sternoclavicular joint., In the thorax, The vessel is in contact, from below upwards, with the trachea, left recurrent laryngeal nerve, left, margin of the oesophagus. Anteriorly the left brachiocephalic vein runs across the artery, and the, cardiac branches from the left vagus descend in front of it. These structures together with the, thymus and the anterior margins of the left lung and pleura separate the artery from the manubrium., In the neck
Page 1504 :
The artery runs superiorly deep to sternocleidomastoid and then enters the anterior triangle. At this, point it lies within the carotid sheath with the vagus nerve and the internal jugular vein. Posteriorly, the sympathetic trunk lies between the vessel and the prevertebral fascia. At the level of C7 the, vertebral artery and thoracic duct lie behind it. The anterior tubercle of C6 transverse process is, prominent and the artery can be compressed against this structure (it corresponds to the level of the, cricoid)., Anteriorly at C6 the omohyoid muscle passes superficial to the artery., Within the carotid sheath the jugular vein lies lateral to the artery., Right common carotid artery, The right common carotid arises from the brachiocephalic artery. The right common carotid artery, corresponds with the cervical portion of the left common carotid, except that there is no thoracic duct, on the right. The oesophagus is less closely related to the right carotid than the left., Summary points about the carotid anatomy, Path, Passes behind the sternoclavicular joint (12% patients above this level) to the upper border of the, thyroid cartilage, to divide into the external (ECA) and internal carotid arteries (ICA)., Relations, , , , , , , Level of 6th cervical vertebra crossed by omohyoid, Then passes deep to the thyrohyoid, sternohyoid, sternomastoid muscles., Passes anterior to the carotid tubercle (transverse process 6th cervical vertebra)-NB, compression here stops haemorrhage., The inferior thyroid artery passes posterior to the common carotid artery., Then : Left common carotid artery crosses the thoracic duct, Right common carotid artery, crossed by recurrent laryngeal nerve
Page 1505 :
Image sourced from Wikipedia, , Next question
Page 1506 :
Question 181 of 560, , A sprinter attends A&E with severe leg pain. He had forgotten to warm up and ran a 100m sprint, race. Towards the end of the race he experienced pain in the posterior aspect of his thigh. The pain, worsens, localising to the lateral aspect of the knee. The sprinter is unable to flex the knee. What, structure has been injured?, , Anterior cruciate ligament, , Posterior cruciate ligament, , Semimembranosus tendon, , Semitendinosus tendon, , Biceps femoris tendon, , Theme from 2009 Exam, The biceps femoris is commonly injured in sports that require explosive bending of the knee as seen, in sprinting, especially if the athlete has not warmed up first. Avulsion most commonly occurs where, the long head attaches to the ischial tuberosity. Injuries to biceps femoris are more common than to, the other hamstrings., Please rate this question:, , Discuss and give feedback, , Next question, , Biceps femoris, The biceps femoris is one of the hamstring group of muscles located in the posterior upper thigh. It, has two heads.
Page 1507 :
Long head, , Origin, , Ischial tuberosity, , Insertion, , Fibular head, , Action, , Knee flexion, lateral rotation tibia, extension hip, , Innervation, , Tibial division of sciatic nerve (L5, S1, S2), , Arterial, supply, , Profunda femoris artery, inferior gluteal artery, and the superior muscular branches of, popliteal artery, , Image demonstrating the biceps femoris muscle, with the long head outlined, , Image sourced from Wikipedia, , Short head
Page 1509 :
Question 182 of 560, A 24 year old man falls and lands astride a manhole cover. He suffers from an injury to the anterior, bulbar urethra. Where will the extravasated urine tend to collect?, , Lesser pelvis, , Connective tissue of the scrotum, , Deep perineal space, , Ischiorectal fossa, , Posterior abdominal wall, , This portion of the urethra is contained between the perineal membrane and the membranous layer, of the superficial fascia. As these are densely adherent to the ischiopubic rami, extravasated urine, cannot pass posteriorly because the 2 layers are continuous around the superficial transverse, perineal muscles., Please rate this question:, , Discuss and give feedback, , Next question, , Lower genitourinary tract trauma, , , , , , Most bladder injuries occur due to blunt trauma, 85% associated with pelvic fractures, Easily overlooked during assessment in trauma, Up to 10% of male pelvic fractures are associated with urethral or bladder injuries, , Types of injury, , Urethral injury, , , , , , Mainly in males, Blood at the meatus (50% cases), There are 2 types:, , i.Bulbar rupture
Page 1510 :
- most common, - straddle type injury e.g. bicycles, - triad signs: urinary retention, perineal haematoma, blood at the, meatus, ii. Membranous rupture, - can be extra or intraperitoneal, - commonly due to pelvic fracture, - Penile or perineal oedema/ hematoma, - PR: prostate displaced upwards (beware co-existing, retroperitoneal haematomas as they may make examination, difficult), - Investigation: ascending urethrogram, - Management: suprapubic catheter (surgical placement, not, percutaneously), External genitalia injuries, (i.e., the penis and the, scrotum), , , , Secondary to injuries caused by penetration, blunt trauma,, continence- or sexual pleasure-enhancing devices, and, mutilation, , Bladder injury, , , , , , rupture is intra or extraperitoneal, presents with haematuria or suprapubic pain, history of pelvic fracture and inability to void: always, suspect bladder or urethral injury, inability to retrieve all fluid used to irrigate the bladder, through a Foley catheter indicates bladder injury, investigation- IVU or cystogram, management: laparotomy if intraperitoneal, conservative if, extraperitoneal, , , , , , Next question
Page 1511 :
Question 183 of 560, A 73 year old man presents with symptoms of mesenteric ischaemia. As part of his diagnostic work, up a diagnostic angiogram is performed .The radiologist is attempting to cannulate the coeliac axis, from the aorta. At which of the following vertebral levels does this is usually originate?, , T10, , L2, , L3, , T8, , T12, Coeliac trunk branches:, Left Hand Side (LHS), Left gastric, Hepatic, Splenic, The coeliac axis branches off the aorta at T12., Please rate this question:, , Discuss and give feedback, , Next question, , Coeliac axis, The coeliac axis has three main branches., , , , , Left gastric, Hepatic: branches-Right Gastric, Gastroduodenal, Right Gastroepiploic, Superior, Pancreaticoduodenal, Cystic (occasionally)., Splenic: branches- Pancreatic, Short Gastric, Left Gastroepiploic
Page 1512 :
It occasionally gives off one of the inferior phrenic arteries., , Image sourced from Wikipedia, , Relations, , Anteriorly, , Lesser omentum, , Right, , Right coeliac ganglion and caudate process of liver, , Left, , Left coeliac ganglion and gastric cardia, , Inferiorly, , Upper border of pancreas and renal vein, Next question
Page 1513 :
Question 184 of 560, , A 43 year old man is diagnosed as having a malignancy of the right adrenal gland. The decision is, made to resect this via an open anterior approach. Which of the following will be most useful during, the surgery?, , Division of the coronary ligaments of the liver, , Mobilisation of the colonic hepatic flexure, , Division of the right renal vein, , Division of the ligament of Trietz, , Division of the right colic artery, , Mobilisation of the hepatic flexure and right colon are standard steps in open adrenal surgery from, an anterior approach. Mobilisation of the liver is seldom required., Please rate this question:, , Discuss and give feedback, , Next question, , Adrenal gland anatomy, Anatomy, , Location, , Superomedially to the upper pole of each kidney
Page 1514 :
Relationships of the right, adrenal, , Diaphragm-Posteriorly, Kidney-Inferiorly, Vena Cava-Medially, Hepato-renal, pouch and bare area of the liver-Anteriorly, , Relationships of the left, adrenal, , Crus of the diaphragm-Postero- medially, Pancreas and splenic vesselsInferiorly, Lesser sac and stomach-Anteriorly, , Arterial supply, , Superior adrenal arteries- from inferior phrenic artery, Middle adrenal, arteries - from aorta, Inferior adrenal arteries -from renal arteries, , Venous drainage of the, right adrenal, , Via one central vein directly into the IVC, , Venous drainage of the, left adrenal, , Via one central vein into the left renal vein, , Next question
Page 1515 :
Question 185 of 560, A 45 year old man presents with a lipoma located posterior to the posterior border of the, sternocleidomastoid muscle, approximately 4cm superior to the middle third of the clavicle. During, surgical excision of the lesion troublesome bleeding is encountered. Which of the following is the, most likely source?, , Internal jugular vein, , External jugular vein, , Common carotid artery, , Vertebral artery, , Second part of the subclavian artery, , The external jugular vein runs obliquely in the superficial fascia of the posterior triangle. It drains into, the subclavian vein. During surgical exploration of this area the external jugular vein may be injured, and troublesome bleeding may result. The internal jugular vein and carotid arteries are located in the, anterior triangle. The third, and not the second, part of the subclavian artery is also a content of the, posterior triangle, Please rate this question:, , Discuss and give feedback, , Next question, , Posterior triangle of the neck, Boundaries, , Apex, , Sternocleidomastoid and the Trapezius muscles at the Occipital bone, , Anterior, , Posterior border of the Sternocleidomastoid, , Posterior, , Anterior border of the Trapezius
Page 1516 :
Base, , Middle third of the clavicle, , Image sourced from Wikipedia, , Contents, , Nerves, , , , , , , Accessory nerve, Phrenic nerve, Three trunks of the brachial plexus, Branches of the cervical plexus: Supraclavicular nerve, transverse cervical, nerve, great auricular nerve, lesser occipital nerve, , Vessels, , , , , External jugular vein, Subclavian artery, , Muscles, , , , , Inferior belly of omohyoid, Scalene, , Lymph, nodes, , , , , Supraclavicular, Occipital, Next question
Page 1517 :
Question 186-188 of 560, Theme: Levels of spinal injury, , A., B., C., D., E., F., G., H., I., J., , C2, C3, C4, C5, C6, L1, L2, L3, L4, L5, , Please select the most likely spinal level for the injury described. Each option may be used once,, more than once or not at all., , 186., , A 62 year old male complains of back pain. He has had a recent fall. Walking causes pain, of the left lower leg. On examination he is noted to have reduced sensation over the knee., You answered C2, The correct answer is L3, Sensation over the knee is equivalent to the L3 dermatome. The four nerves involved, include the infrapatellar branch of the saphenous nerve, the lateral cutaneous nerve of the, thigh, anterior cutaneous nerve of the thigh (both lateral and medial branches)., , 187., , A 42 year old woman is found to have a burst fracture of the C5 vertebral body. After a, few months where would the level of injury be?, You answered C2, The correct answer is C6, A C5 burst fracture usually injures the C6 spinal cord situated at the C5 vertebrae and, also the C4 spinal roots that exit the spinal column between the C4 and C5 vertebra. Such, an injury should cause a loss of sensations in C4 dermatome and weak deltoids. Due to, oedema , the biceps (C5) may be initially weak but should recover. The wrist extensors, (C6), however, should remain weak and sensation at and below C6 should be severely, compromised. A neurosurgeon would conclude that there is a burst fracture at C5 from, the x-rays, an initial sensory level at C4 (the first abnormal sensory dermatome) and the, partial loss of deltoids and biceps would imply a motor level at C4 (the highest abnormal
Page 1518 :
muscle level). Over time, as the patient recovers the C4 roots and the C5 spinal cord, both, the sensory level and motor level should end up at C6. Such recovery is often attributed, to 'root' recovery., 188., , A 56 year old man suddenly develops severe back pain. His pain has a radicular pattern., On examination he is unable to extend his great toe., You answered C2, The correct answer is L5, Extensor hallucis longus is derived from L5 and loss of EHL function is a useful test to, determine whether this level is involved., , Please rate this question:, , Discuss and give feedback, , Next question, , Spinal disorders, Dorsal column lesion, , , , , Loss vibration and proprioception, Tabes dorsalis, SACD, , Spinothalamic tract, lesion, , , , Loss of pain, sensation and temperature, , Central cord lesion, , , , Flaccid paralysis of the upper limbs, , Osteomyelitis, , , , , , , Normally progressive, Staph aureus in IVDU, normally cervical region affected, Fungal infections in immunocompromised, Thoracic region affected in TB, , Infarction spinal cord, , , , Dorsal column signs (loss of proprioception and fine, discrimination), , Cord compression, , , , , UMN signs, Malignancy
Page 1520 :
Image sourced from Wikipedia
Page 1524 :
Question 189 of 560, The sciatic nerve lies deep to the following structures except:, , Gluteus maximus, , The femoral cutaneous nerve, , Long head of biceps femoris, , Gluteus medius, , Branch of the inferior gluteal artery, , The gluteus medius does not extend around to the sciatic nerve., Please rate this question:, , Discuss and give feedback, , Next question, , Sciatic nerve, The sciatic nerve is formed from the sacral plexus and is the largest nerve in the body. It is the, continuation of the main part of the plexus arising from ventral rami of L4 to S3. These rami, converge at the inferior border of piriformis to form the nerve itself. It passes through the inferior part, of the greater sciatic foramen and emerges beneath piriformis. Medially, lie the inferior gluteal nerve, and vessels and the pudendal nerve and vessels. It runs inferolaterally under the cover of gluteus, maximus midway between the greater trochanter and ischial tuberosity. It receives its blood supply, from the inferior gluteal artery. The nerve provides cutaneous sensation to the skin of the foot and, the leg. It also innervates the posterior thigh muscles and the lower leg and foot muscles. The nerve, splits into the tibial and common peroneal nerves approximately half way down the posterior thigh., The tibial nerve supplies the flexor muscles and the common peroneal nerve supplies the extensor, muscles and the abductor muscles., Summary points, , Origin, , Spinal nerves L4 - S3
Page 1525 :
Articular Branches, , Hip joint, , Muscular branches in, upper leg, , , , , , , Semitendinosus, Semimembranosus, Biceps femoris, Part of adductor magnus, , Cutaneous sensation, , , , , , Posterior aspect of thigh (via cutaneous nerves), Gluteal region, Entire lower leg (except the medial aspect), , Terminates, , , , , At the upper part of the popliteal fossa by dividing into the tibial and, peroneal nerves, , The nerve to the short head of the biceps femoris comes from the common peroneal part of, the sciatic and the other muscular branches arise from the tibial portion., The tibial nerve goes on to innervate all muscles of the foot except the extensor digitorum, brevis (which is innervated by the common peroneal nerve)., Next question
Page 1526 :
Question 190 of 560, Which of the following upper limb muscles is not innervated by the radial nerve?, , Extensor carpi ulnaris, , Abductor digiti minimi, , Anconeus, , Supinator, , Brachioradialis, Mnemonic for radial nerve muscles: BEST, B rachioradialis, E xtensors, S upinator, T riceps, Abductor digiti minimi is innervated by the ulnar nerve., Please rate this question:, , Discuss and give feedback, , Next question, , Radial nerve, Continuation of posterior cord of the brachial plexus (root values C5 to T1), Path, , , , , , In the axilla: lies posterior to the axillary artery on subscapularis, latissimus dorsi and teres, major., Enters the arm between the brachial artery and the long head of triceps (medial to humerus)., Spirals around the posterior surface of the humerus in the groove for the radial nerve., At the distal third of the lateral border of the humerus it then pierces the intermuscular, septum and descends in front of the lateral epicondyle.
Page 1528 :
Muscular innervation and effect of denervation, , Anatomical, location, , Muscle affected, , Effect of paralysis, , Shoulder, , Long head of triceps, , Minor effects on shoulder stability in abduction, , Arm, , Triceps, , Loss of elbow extension, , Forearm, , Supinator, Brachioradialis, Extensor carpi radialis, longus and brevis, , Weakening of supination of prone hand and, elbow flexion in mid prone position, , The cutaneous sensation of the upper limb- illustrating the contribution of the radial nerve, , Image sourced from Wikipedia, , Next question, Question 191 of 560
Page 1529 :
Which of the following forms the floor of the anatomical snuffbox?, , Radial artery, , Cephalic vein, , Extensor pollicis brevis, , Scaphoid bone, , Cutaneous branch of the radial nerve, , Theme from April 2014 exam, The scaphoid bone forms the floor of the anatomical snuffbox. The cutaneous branch of the radial, nerve is much more superficially and proximally located., Please rate this question:, , Discuss and give feedback, , Next question, , Anatomical snuffbox, Posterior border, , Tendon of extensor pollicis longus, , Anterior border, , Tendons of extensor pollicis brevis and abductor pollicis longus, , Proximal border, , Styloid process of the radius
Page 1530 :
Distal border, , Apex of snuffbox triangle, , Floor, , Trapezium and scaphoid, , Content, , Radial artery, , Image showing the anatomical snuffbox, , Image sourced from Wikipedia, , Next question
Page 1531 :
Question 192 of 560, During a liver resection a surgeon performs a pringles manoeuvre to control bleeding. Which of the, following structures will lie posterior to the epiploic foramen at this level?, , Hepatic artery, , Cystic duct, , Greater omentum, , Superior mesenteric artery, , Inferior vena cava, Bleeding from liver trauma or a difficult cholecystectomy can be controlled with a vascular clamp, applied at the epiploic foramen., The epiploic foramen has the following boundaries:, Anteriorly (in the free edge of the lesser omentum): Bile duct to the right, portal vein behind and, hepatic artery to the left., PosteriorlyInferior vena cava, Inferiorly1st part of the duodenum, SuperiorlyCaudate process of the liver, Please rate this question:, , Discuss and give feedback, , Next question, , Liver, Structure of the liver, , Right lobe, , , , , Supplied by right hepatic artery, Contains Couinaud segments V to VIII (-/+Sg I), , Left lobe, , , , , Supplied by the left hepatic artery, Contains Couinaud segments II to IV (+/- Sg1)
Page 1532 :
Quadrate lobe, , , , , , , , Part of the right lobe anatomically, functionally is part of the left, Couinaud segment IV, Porta hepatis lies behind, On the right lies the gallbladder fossa, On the left lies the fossa for the umbilical vein, , Caudate lobe, , , , , , , , Supplied by both right and left hepatic arteries, Couinaud segment I, Lies behind the plane of the porta hepatis, Anterior and lateral to the inferior vena cava, Bile from the caudate lobe drains into both right and left hepatic ducts, , Detailed knowledge of Couinaud segments is not required for MRCS, , , Between the liver lobules are portal canals which contain the portal triad: Hepatic Artery,, Portal Vein, tributary of Bile Duct., , Relations of the liver, , Anterior, , Postero inferiorly, , Diaphragm, , Oesophagus, , Xiphoid process, , Stomach, , Duodenum, , Hepatic flexure of colon, , Right kidney, , Gallbladder
Page 1533 :
Inferior vena cava, , Porta hepatis, , Location, , Postero inferior surface, it joins nearly at right angles with the left sagittal fossa, and, separates the caudate lobe behind from the quadrate lobe in front, , Transmits, , , , , , , , Common hepatic duct, Hepatic artery, Portal vein, Sympathetic and parasympathetic nerve fibres, Lymphatic drainage of the liver (and nodes), , Ligaments, , Falciform ligament, , , , , , 2 layer fold peritoneum from the umbilicus to anterior liver surface, Contains ligamentum teres (remnant umbilical vein), On superior liver surface it splits into the coronary and left, triangular ligaments, , Ligamentum teres, , Joins the left branch of the portal vein in the porta hepatis, , Ligamentum, venosum, , Remnant of ductus venosus, , Arterial supply, , , Hepatic artery, , Venous, , , , Hepatic veins, Portal vein, , Nervous supply, , , Sympathetic and parasympathetic trunks of coeliac plexus, Next question
Page 1534 :
Question 193 of 560, A 72 year old lady is suspected of having a femoral hernia. At which of the following sites is it most, likely to be identifiable clinically?, , Mid inguinal point, , Above and medial to the pubic tubercle, , Below and lateral to the pubic tubercle, , Mid point of the inguinal ligament, , 3 cm superomedially to the superficial inguinal ring, , Femoral hernias exit the femoral canal below and lateral to the pubic tubercle. Femoral hernia occur, mainly in women due to their difference in pelvic anatomy. They are at high risk of strangulation and, therefore should be repaired., Please rate this question:, , Discuss and give feedback, , Next question, , Femoral canal, The femoral canal lies at the medial aspect of the femoral sheath. The femoral sheath is a fascial, tunnel containing both the femoral artery laterally and femoral vein medially. The canal lies medial to, the vein., Borders of the femoral canal, , Laterally, , Femoral vein, , Medially, , Lacunar ligament, , Anteriorly, , Inguinal ligament
Page 1535 :
Pectineal ligament, , Posteriorly, , Image showing dissection of femoral canal, , Image sourced from Wikipedia, , Contents, , , , Lymphatic vessels, Cloquet's lymph node, , Physiological significance, Allows the femoral vein to expand to allow for increased venous return to the lower limbs., Pathological significance, As a potential space, it is the site of femoral hernias. The relatively tight neck places these at high, risk of strangulation.
Page 1538 :
The fascia of the palm is continuous with the antebrachial fascia and the fascia of the dorsum of the, hand. The palmar fascia is thin over the thenar and hypothenar eminences. In contrast the palmar, fascia is relatively thick. The palmar aponeurosis covers the soft tissues and overlies the flexor, tendons. The apex of the palmar aponeurosis is continuous with the flexor retinaculum and the, palmaris longus tendon. Distally, it forms four longitudinal digital bands that attach to the bases of, the proximal phalanges, blending with the fibrous digital sheaths., A medial fibrous septum extends deeply from the medial border of the palmar aponeurosis to the 5th, metacarpal. Lying medial to this are the hypothenar muscles. In a similar fashion, a lateral fibrous, septum extends deeply from the lateral border of the palmar aponeurosis to the 3rd metacarpal. The, thenar compartment lies lateral to this area., Lying between the thenar and hypothenar compartments is the central compartment. It contains the, flexor tendons and their sheaths, the lumbricals, the superficial palmar arterial arch and the digital, vessels and nerves., The deepest muscular plane is the adductor compartment, which contains adductor pollicis., Short muscles of the hand, These comprise the lumbricals and interossei. The four slender lumbrical muscles flex the fingers at, the metacarpophalangeal joints and extend the interphalangeal joint. The four dorsal interossei are, located between the metacarpals and the four palmar interossei lie on the palmar surface of the, metacarpals in the interosseous compartment of the hand., Long flexor tendons and sheaths in the hand, The tendons of FDS and FDP enter the common flexor sheath deep to the flexor retinaculum. The, tendons enter the central compartment of the hand and fan out to their respective digital synovial, sheaths. Near the base of the proximal phalanx, the tendon of FDS splits to permit the passage of, FDP. The FDP tendons are attached to the margins of the anterior aspect of the base of the distal, phalanx., The fibrous digital sheaths contain the flexor tendons and their synovial sheaths. These extend from, the heads of the metacarpals to the base of the distal phalanges., Next question
Page 1539 :
Question 195 of 560, A 34 year old lady undergoes a thyroidectomy for Graves disease. Post operatively she develops a, tense haematoma in the neck. In which of the following fascial planes will it be contained?, , Gerotas fascia, , Waldeyers fascia, , Pretracheal fascia, , Sibsons fascia, , Clavipectoral fascia, , The pretracheal fascia encloses the thyroid and is unyielding. Therefore tense haematomas can, develop., Please rate this question:, , Discuss and give feedback, , Next question, , Thyroid gland, , , , , , , , Right and left lobes connected by isthmus, Surrounded by sheath from pretracheal layer of deep fascia, Apex: Lamina of thyroid cartilage, Base: 4th-5th tracheal ring, Pyramidal lobe: from isthmus, May be attached to foramen caecum at the base of the tongue, , Relations, , Anteromedially, , , , , , , Sternothyroid, Superior belly of omohyoid, Sternohyoid, Anterior aspect of sternocleidomastoid
Page 1540 :
Posterolaterally, , Carotid sheath, , Medially, , , , , , , , , , Larynx, Trachea, Pharynx, Oesophagus, Cricothyroid muscle, External laryngeal nerve (near superior thyroid artery), Recurrent laryngeal nerve (near inferior thyroid artery), , Posterior, , , , , Parathyroid glands, Anastomosis of superior and inferior thyroid arteries, , Isthmus, , , , , Anteriorly: Sternothyroids, sternohyoids, anterior jugular veins, Posteriorly: 2nd, 3rd, 4th tracheal rings (attached via Ligament of, Berry), , Blood Supply, , Arterial, , , , , , Superior thyroid artery (1st branch of external carotid), Inferior thyroid artery (from thyrocervical trunk), Thyroidea ima (in 10% of population -from brachiocephalic artery or aorta), , Venous, , , , , Superior and middle thyroid veins - into the IJV, Inferior thyroid vein - into the brachiocephalic veins, Next question
Page 1541 :
Question 196 of 560, A 32 year old lady complains of carpal tunnel syndrome. The carpal tunnel is explored surgically., Which of the following structures will lie in closest proximity to the hamate bone within the carpal, tunnel?, , The tendon of abductor pollicis longus, , The tendons of flexor digitorum profundus, , The tendons of flexor carpi radialis longus, , Median nerve, , Radial artery, , The carpal tunnel contains nine flexor tendons:, , , , , Flexor digitorum profundus, Flexor digitorum superficialis, Flexor pollicis longus, , The tendon of flexor digitorum profundus lies deepest in the tunnel and will thus lie nearest to the, hamate bone., Please rate this question:, , Discuss and give feedback, , Next question, , Carpal bones, The wrist is comprised of 8 carpal bones, these are arranged in two rows of 4. It is convex from side, to side posteriorly and concave anteriorly., Diagrammatic image of carpal bones
Page 1544 :
Question 197 of 560, , A 45 year old man sustains a significant head injury and a craniotomy is performed. The sigmoid, sinus is bleeding profusely, into which of the following structures does it drain?, , Internal jugular vein, , Straight sinus, , Petrosal sinus, , Inferior sagittal sinus, , External jugular vein, , The sigmoid sinus is joined by the inferior petrosal sinus to drain into the internal jugular vein., Please rate this question:, , Discuss and give feedback, , Next question, , Cranial venous sinuses, The cranial venous sinuses are located within the dura mater. They have no valves which is, important in the potential for spreading sepsis. They eventually drain into the internal jugular vein., They are:, Superior sagittal sinus, Inferior sagittal sinus, Straight sinus, Transverse sinus
Page 1545 :
Sigmoid sinus, Confluence of sinuses, Occipital sinus, Cavernous sinus, Topography of cranial venous sinuses, , Image sourced from Wikipedia, , Next question
Page 1546 :
Question 198 of 560, , Which nerve supplies the interossei of the fourth finger?, , Radial, , Median, , Superficial ulnar, , Deep ulnar, , Posterior interosseous, Mnemonic:, PAD and DAB, Palmer interossei ADduct, Dorsal interossei ABduct, , Theme from April 2013 exam, Theme from April 2014 exam, Please rate this question:, , Discuss and give feedback, , Next question, , Interossei, Origin and insertion, , Nerve supply, , Actions
Page 1547 :
Origin and insertion, , Nerve supply, , Actions, , Three palmar and four dorsal interossei occupy the spaces, between the metacarpal bones. Each palmar interossei, originates from the metacarpal of the digit on which it acts., Each dorsal interossei comes from the surface of the adjacent, metacarpal on which it acts. As a result the dorsal interossei are, twice the size of the palmar ones., The interossei tendons, except the first palmar, pass to one or, other side of the metacarpophalangeal joint posterior to the, deep transverse metacarpal ligament. They become inserted, into the base of the proximal phalanx and partly into the, extensor hood, , They are all, innervated by, the ulnar nerve, , Dorsal interossei, abduct the fingers,, palmar interossei, adduct the fingers, , Clinical notes, Along with the lumbricals the interossei flex the metacarpophalangeal joints and extend the proximal, and distal interphalangeal joints. They are responsible for fine tuning these movements. When the, interossei and lumbricals are paralysed the digits are pulled into hyperextension by extensor, digitorum and a claw hand is seen., Next question
Page 1548 :
Question 199 of 560, , In which of the following cranial bones does the foramen spinosum lie?, , Sphenoid bone, , Frontal bone, , Temporal bone, , Occipital bone, , Parietal bone, , The foramen spinosum (which transmits the middle meningeal artery and vein) lies in the sphenoid, bone., Please rate this question:, , Discuss and give feedback, , Next question, , Foramina of the base of the skull, Foramen, , Location, , Contents, , Foramen ovale, , Sphenoid, bone, , Otic ganglion, V3 (Mandibular nerve:3rd branch of, trigeminal), Accessory meningeal artery
Page 1550 :
Foramen, , Location, , Contents, , Superior ophthalmic vein, , *= In life the foramen lacerum is occluded by a cartilagenous plug. The ICA initially passes into the, carotid canal which ascends superomedially to enter the cranial cavity through the foramen lacerum., Base of skull anatomical overview, , Image sourced from Wikipedia, , Next question
Page 1551 :
Question 200 of 560, Which of the following is not considered a major branch of the descending thoracic aorta?, , Bronchial artery, , Mediastinal artery, , Inferior thyroid artery, , Posterior intercostal artery, , Oesophageal artery, , The inferior thyroid artery is usually derived from the thyrocervical trunk, a branch of the subclavian, artery., Please rate this question:, , Discuss and give feedback, , Next question, , Thoracic aorta, Origin, , T4, , Terminates, , T12, , Relations, , Branches, , , , , , , Anteriorly (from top to bottom)-root of the left lung, the pericardium, the, oesophagus, and the diaphragm, Posteriorly-vertebral column, azygos vein, Right- hemiazygos veins, thoracic duct, Left- left pleura and lung, , , , , Lateral segmental branches: Posterior intercostal arteries, Lateral visceral: Bronchial arteries supply bronchial walls and lung
Page 1553 :
Question 201 of 560, An 18 year old lady with troublesome hyperhidrosis of the hands and arms is due to undergo a, sympathectomy to treat the condition. Which of the following should the surgeons divide to most, effectively treat her condition?, , Sympathetic ganglia at T1, T2 and T3, , Sympathetic ganglia at T2 and T3, , Sympathetic ganglia at T1 and T2, , Stellate ganglion, , Superior cervical ganglion, , To treat hyperhidrosis the sympathetic ganglia at T2 and T3 should be divided. Dividing the other, structures listed would either carry a risk of Horners syndrome or be ineffective., Please rate this question:, , Discuss and give feedback, , Next question, , Sympathetic nervous system- anatomy, The cell bodies of the pre-ganglionic efferent neurones lie in the lateral horn of the grey matter of the, spinal cord in the thoraco-lumbar regions., The pre-ganglionic efferents leave the spinal cord at levels T1-L2. These pass to the sympathetic, chain., Lateral branches of the sympathetic chain connect it to every spinal nerve. These post ganglionic, nerves will pass to structures that receive sympathetic innervation at the periphery., Sympathetic chains, These lie on the vertebral column and run from the base of the skull to the coccyx., , Cervical, region, , Lie anterior to the transverse processes of the cervical vertebrae and posterior to, the carotid sheath., , Thoracic, , Lie anterior to the neck of the upper ribs and and lateral sides of the lower thoracic
Page 1554 :
region, , vertebrae.They are covered by the parietal pleura, , Lumbar, region, , Enter by passing posterior to the medial arcuate ligament. Lie anteriorly to the, vertebrae and medial to psoas major., , Sympathetic ganglia, , , , , , , Superior cervical ganglion lies anterior to C2 and C3., Middle cervical ganglion (if present) C6, Stellate ganglion- anterior to transverse process of C7, lies posterior to the subclavian artery,, vertebral artery and cervical pleura., Thoracic ganglia are segmentally arranged., There are usually 4 lumbar ganglia., , Clinical importance, , , , , Interruption of the head and neck supply of the sympathetic nerves will result in an ipsilateral, Horners syndrome., For treatment of hyperhidrosis the sympathetic denervation can be achieved by removing the, second and third thoracic ganglia with their rami. Removal of T1 will cause a Horners, syndrome and is therefore not performed., In patients with vascular disease of the lower limbs a lumbar sympathetomy may be, performed, either radiologically or (more rarely now) surgically. The ganglia of L2 and below, are disrupted. If L1 is removed then ejaculation may be compromised (and little additional, benefit conferred as the preganglionic fibres do not arise below L2., Next question
Page 1555 :
Question 202 of 560, A 44 year old lady is recovering following a transphenoidal hypophysectomy. Unfortunately there is a, post operative haemorrhage. Which of the following features is most likely to occur initially?, , Cavernous sinus thrombosis, , Abducens nerve palsy, , Bi-temporal hemianopia, , Inferior homonymous hemianopia, , Central retinal vein occlusion, , Theme from April 2014 exam, The pituitary is covered by a sheath of dura and an expanding haematoma at this site may compress, the optic chiasm in the same manner as an expanding pituitary tumour., Please rate this question:, , Discuss and give feedback, , Next question, , Pituitary Gland, The pituitary gland is located within the sella turcica within the sphenoid bone in the middle cranial, fossa. It is covered by a dural fold and weighs around 0.5g. It is attached to the hypothalamus by the, infundibulum. The anterior pituitary receives hormonal stimuli from the hypothalamus by way of the, hypothalamo-pituitary portal system. It develops from a depression in the wall of the pharynx, (Rathkes pouch)., Anterior pituitary hormones, , , , , , , , Growth hormone, Thyroid stimulating hormone, ACTH, Prolactin, LH and FSH, Melanocyte releasing hormone
Page 1556 :
Posterior pituitary hormones, , , , Oxytocin, Anti diuretic hormone, Next question
Page 1557 :
Question 203 of 560, During a right hemicolectomy the caecum is mobilised. As the bowel is retracted medially a vessel is, injured, posterior to the colon. Which of the following is the most likely vessel?, , Right colic artery, , Inferior vena cava, , Aorta, , External iliac artery, , Gonadal vessels, , The gonadal vessels and ureter are important posterior relations that are at risk during a right, hemicolectomy., Please rate this question:, , Discuss and give feedback, , Next question, , Caecum, Location, , , , , Proximal right colon below the ileocaecal valve, Intraperitoneal, , Posterior relations, , , , , , , , Psoas, Iliacus, Femoral nerve, Genitofemoral nerve, Gonadal vessels, , Anterior relations, , Greater omentum, , Arterial supply, , Ileocolic artery
Page 1558 :
Lymphatic drainage, , , , Mesenteric nodes accompany the venous drainage, , The caecum is the most distensible part of the colon and in complete large bowel obstruction, with a competent ileocaecal valve the most likely site of eventual perforation., Next question
Page 1559 :
Question 204 of 560, A 53 year old man with a carcinoma of the lower third of the oesophagus is undergoing an, oesophagogastrectomy. As the surgeons mobilise the lower part of the oesophagus, where are they, most likely to encounter the thoracic duct?, , Anterior to the oesophagus, , On the left side of the oesophagus, , On the right side of the oesophagus, , Immediately anterior to the azygos vein, , Posterior to the oesophagus, , The thoracic duct lies posterior to the oesophagus and passes to the left at the level of the Angle of, Louis. It enters the thorax at T12 together with the aorta., Please rate this question:, , Discuss and give feedback, , Next question, , Thoracic duct, , , , , , , , Continuation of the cisterna chyli in the abdomen., Enters the thorax at T12., Lies posterior to the oesophagus for most of its intrathoracic course. Passes to the left at T5., Lymphatics draining the left side of the head and neck join the thoracic duct prior to its, insertion into the left brachiocephalic vein., Lymphatics draining the right side of the head and neck drain via the subclavian and jugular, trunks into the right lymphatic duct and thence into the mediastinal trunk and eventually the, right brachiocephalic vein., Its location in the thorax makes it prone to injury during oesophageal surgery. Some, surgeons administer cream to patients prior to oesophagectomy so that it is easier to identify, the cut ends of the duct., Next question
Page 1560 :
Question 205 of 560, Which of the following represents the root values of the sciatic nerve?, , L4 to S3, , L1 to L4, , L3 to S1, , S1 to S4, , L5 to S1, , Theme from April 2014 exam, The sciatic nerve most commonly arises from L4 to S3., Please rate this question:, , Discuss and give feedback, , Next question, , Sciatic nerve, The sciatic nerve is formed from the sacral plexus and is the largest nerve in the body. It is the, continuation of the main part of the plexus arising from ventral rami of L4 to S3. These rami, converge at the inferior border of piriformis to form the nerve itself. It passes through the inferior part, of the greater sciatic foramen and emerges beneath piriformis. Medially, lie the inferior gluteal nerve, and vessels and the pudendal nerve and vessels. It runs inferolaterally under the cover of gluteus, maximus midway between the greater trochanter and ischial tuberosity. It receives its blood supply, from the inferior gluteal artery. The nerve provides cutaneous sensation to the skin of the foot and, the leg. It also innervates the posterior thigh muscles and the lower leg and foot muscles. The nerve, splits into the tibial and common peroneal nerves approximately half way down the posterior thigh., The tibial nerve supplies the flexor muscles and the common peroneal nerve supplies the extensor, muscles and the abductor muscles., Summary points, , Origin, , Spinal nerves L4 - S3
Page 1561 :
Articular Branches, , Hip joint, , Muscular branches in, upper leg, , , , , , , Semitendinosus, Semimembranosus, Biceps femoris, Part of adductor magnus, , Cutaneous sensation, , , , , , Posterior aspect of thigh (via cutaneous nerves), Gluteal region, Entire lower leg (except the medial aspect), , Terminates, , , , , At the upper part of the popliteal fossa by dividing into the tibial and, peroneal nerves, , The nerve to the short head of the biceps femoris comes from the common peroneal part of, the sciatic and the other muscular branches arise from the tibial portion., The tibial nerve goes on to innervate all muscles of the foot except the extensor digitorum, brevis (which is innervated by the common peroneal nerve)., Next question
Page 1562 :
Question 206 of 560, , The common peroneal nerve, or its branches, supply the following muscles except:, , Peroneus longus, , Tibialis anterior, , Extensor hallucis longus, , Flexor digitorum brevis, , Extensor digitorum longus, , Flexor digitorum is supplied by the tibial nerve., Please rate this question:, , Discuss and give feedback, , Next question, , Common peroneal nerve, Derived from the dorsal divisions of the sacral plexus (L4, L5, S1 and S2)., This nerve supplies the skin and fascia of the anterolateral surface of the leg and the dorsum of the, foot. It also innervates the muscles of the anterior and peroneal compartments of the leg, extensor, digitorum brevis as well as the knee, ankle and foot joints., It is laterally placed within the sciatic nerve. From the bifurcation of the sciatic nerve it passes, inferolaterally in the lateral and proximal part of the popliteal fossa, under the cover of biceps femoris, and its tendon. To reach the posterior aspect of the fibular head. It ends by dividing into the deep, and superficial peroneal nerves at the point where it winds around the lateral surface of the neck of
Page 1563 :
the fibula in the body of peroneus longus, approximately 2cm distal to the apex of the head of the, fibula. It is palpable posterior to the head of the fibula., Branches, , In the thigh, , Nerve to the short head of biceps, Articular branch (knee), , In the popliteal fossa, , Lateral cutaneous nerve of the calf, , Neck of fibula, , Superficial and deep peroneal nerves, Next question
Page 1564 :
Question 207 of 560, An 83 year old lady presents with a femoral hernia and undergoes a femoral hernia repair. Which of, the following forms the posterior wall of the femoral canal?, , Pectineal ligament, , Lacunar ligament, , Inguinal ligament, , Adductor longus, , Sartorius, , Please rate this question:, , Discuss and give feedback, , Next question, , Femoral canal, The femoral canal lies at the medial aspect of the femoral sheath. The femoral sheath is a fascial, tunnel containing both the femoral artery laterally and femoral vein medially. The canal lies medial to, the vein., Borders of the femoral canal, , Laterally, , Femoral vein, , Medially, , Lacunar ligament, , Anteriorly, , Inguinal ligament, , Posteriorly, , Pectineal ligament
Page 1565 :
Image showing dissection of femoral canal, , Image sourced from Wikipedia, , Contents, , , , Lymphatic vessels, Cloquet's lymph node, , Physiological significance, Allows the femoral vein to expand to allow for increased venous return to the lower limbs., Pathological significance, As a potential space, it is the site of femoral hernias. The relatively tight neck places these at high, risk of strangulation., Next question
Page 1566 :
Question 208 of 560, A 45 year man presents with hand weakness. He is given a piece of paper to hold between his, thumb and index finger. When the paper is pulled, the patient has difficulty maintaining a grip. Grip, pressure is maintained by flexing the thumb at the interphalangeal joint. What is the most likely, nerve lesion?, , Posterior interosseous nerve, , Deep branch of ulnar nerve, , Anterior interosseous nerve, , Superficial branch of the ulnar nerve, , Radial nerve, , Theme from January 2012 exam, This is a description of Froment's sign, which tests for ulnar nerve palsy. It mainly tests for the, function of adductor pollicis. This is supplied by the deep branch of the ulnar nerve. Remember the, anterior interosseous branch (of the median nerve), which innervates the flexor pollicis longus, (hence causing flexion of the thumb IP joint), branches off more proximally to the wrist., Please rate this question:, , Discuss and give feedback, , Next question, , Ulnar nerve, Origin, , , C8, T1, , Supplies (no muscles in the upper arm), , , , Flexor carpi ulnaris, Flexor digitorum profundus
Page 1568 :
Branch, , Supplies, , Muscular branch, , Flexor carpi ulnaris, Medial half of the flexor digitorum profundus, , Palmar cutaneous branch (Arises near the, middle of the forearm), , Skin on the medial part of the palm, , Dorsal cutaneous branch, , Dorsal surface of the medial part of the hand, , Superficial branch, , Cutaneous fibres to the anterior surfaces of the, medial one and one-half digits, , Deep branch, , Hypothenar muscles, All the interosseous muscles, Third and fourth lumbricals, Adductor pollicis, Medial head of the flexor pollicis brevis, , Effects of injury, , Damage at the wrist, , , , , , Wasting and paralysis of intrinsic hand muscles (claw hand), Wasting and paralysis of hypothenar muscles, Loss of sensation medial 1 and half fingers, , Damage at the elbow, , , , , Radial deviation of the wrist, Clawing less in 4th and 5th digits, Next question
Page 1569 :
Question 209 of 560, Which of the following statements relating to the right phrenic nerve is false?, , It lies deep to the prevertebral layer of deep cervical fascia, , Crosses posterior to the 2nd part of the subclavian artery, , It runs on the anterior surface of the scalene muscle, , On the right side it leaves the mediastinum via the vena cava hiatus at a level of T8, , The right phrenic nerve passes over the right atrium, , Please rate this question:, , Discuss and give feedback, , Next question, , Phrenic nerve, Origin, , , C3,4,5, , Supplies, , , Diaphragm, sensation central diaphragm and pericardium, , Path, , , , The phrenic nerve passes with the internal jugular vein across scalenus anterior. It passes, deep to prevertebral fascia of deep cervical fascia., Left: crosses anterior to the 1st part of the subclavian artery.
Page 1570 :
, , , Right: Anterior to scalenus anterior and crosses anterior to the 2nd part of the subclavian, artery., On both sides, the phrenic nerve runs posterior to the subclavian vein and posterior to the, internal thoracic artery as it enters the thorax., , Right phrenic nerve, , , , , In the superior mediastinum: anterior to right vagus and laterally to superior vena cava, Middle mediastinum: right of pericardium, It passes over the right atrium to exit the diaphragm at T8, , Left phrenic nerve, , , , , Passes lateral to the left subclavian artery, aortic arch and left ventricle, Passes anterior to the root of the lung, Pierces the diaphragm alone, , Image showing the passage of the phrenic nerve in the neck, , Image sourced from Wikipedia, , Next question
Page 1571 :
Question 210 of 560, , Which of the following cranial foramina pairings are incorrect?, , Carotid canal and internal carotid artery., , Foramen ovale and mandibular nerve., , Optic canal and ophthalmic artery., , Optic canal and ophthalmic nerve., , Foramen rotundum and maxillary nerve., , Question derived from 2010 and 2011 exams, The optic canal transmits the optic nerve. The ophthalmic nerve traverses the superior orbital, fissure., Please rate this question:, , Discuss and give feedback, , Next question, , Foramina of the base of the skull, Foramen, , Location, , Contents, , Foramen ovale, , Sphenoid, , Otic ganglion, V3 (Mandibular nerve:3rd branch of
Page 1573 :
Foramen, , Location, , Contents, , Abducent nerve (VI), Superior ophthalmic vein, , *= In life the foramen lacerum is occluded by a cartilagenous plug. The ICA initially passes into the, carotid canal which ascends superomedially to enter the cranial cavity through the foramen lacerum., Base of skull anatomical overview, , Image sourced from Wikipedia, , Next question
Page 1574 :
Question 211 of 560, A 22 year old man is involved in a fight and sustains a stab wound in his upper forearm. On, examination there is a small, but deep laceration. There is an obvious loss of pincer movement, involving the thumb and index finger with minimal loss of sensation. The most likely nerve injury is to, the:, , Ulnar nerve, , Radial nerve, , Anterior interosseous nerve, , Axillary nerve, , Median nerve, , The anterior interosseous nerve is a motor branch of the median nerve just below the elbow. When, damaged it classically causes:, , , , , Pain in the forearm, Loss of pincer movement of the thumb and index finger (innervates the long flexor muscles, of flexor pollicis longus & flexor digitorum profundus of the index and middle finger), Minimal loss of sensation due to lack of a cutaneous branch, , Please rate this question:, , Discuss and give feedback, , Next question, , Median nerve, The median nerve is formed by the union of a lateral and medial root respectively from the lateral, (C5,6,7) and medial (C8 and T1) cords of the brachial plexus; the medial root passes anterior to the, third part of the axillary artery. The nerve descends lateral to the brachial artery, crosses to its, medial side (usually passing anterior to the artery). It passes deep to the bicipital aponeurosis and, the median cubital vein at the elbow., It passes between the two heads of the pronator teres muscle, and runs on the deep surface of, flexor digitorum superficialis (within its fascial sheath)., Near the wrist it becomes superficial between the tendons of flexor digitorum superficialis and flexor
Page 1576 :
Damage at elbow, as above plus:, , , , , unable to pronate forearm, weak wrist flexion, ulnar deviation of wrist, , Anterior interosseous nerve (branch of median nerve), , , , leaves just below the elbow, results in loss of pronation of forearm and weakness of long flexors of thumb and index, finger, , Topography of the median nerve, , Image sourced from Wikipedia, , Next question
Page 1577 :
Question 212 of 560, A 66 year old man is undergoing a left nephro-ureterectomy. The surgeons remove the ureter, which, of the following is responsible for the blood supply to the proximal ureter?, , Branches of the renal artery, , External iliac artery, , Internal iliac artery, , Direct branches from the aorta, , Common iliac artery, , Theme from April 2014 exam, The proximal ureter is supplied by branches from the renal artery. For the other feeding vessels see below., Please rate this question:, , Discuss and give feedback, , Next question, , Ureter, , , , , , , , , 25-35 cm long, Muscular tube lined by transitional epithelium, Surrounded by thick muscular coat. Becomes 3 muscular layers as it crosses the bony pelvis, Retroperitoneal structure overlying transverse processes L2-L5, Lies anterior to bifurcation of iliac vessels, Blood supply is segmental; renal artery, aortic branches, gonadal branches, common iliac, and internal iliac, Lies beneath the uterine artery, Next question
Page 1579 :
A 78 year old man presents with symptoms consistent with intermittent claudication. To assess the, severity of his disease you decide to measure his ankle brachial pressure index. To do this you will, identify the dorsalis pedis artery. Which of the following statements relating to this vessel is false?, , It originates from the peroneal artery, , It is crossed by the tendon of extensor hallucis brevis, , Two veins are usually closely related to it, , It passes under the inferior extensor retinaculum, , The tendon of extensor hallucis longus lies medial to it., , The dorsalis pedis artery is a direct continuation of the anterior tibial artery., Please rate this question:, , Discuss and give feedback, , Next question, , Foot- anatomy, Arches of the foot, The foot is conventionally considered to have two arches., , , , , The longitudinal arch is higher on the medial than on the lateral side. The posterior part of, the calcaneum forms a posterior pillar to support the arch. The lateral part of this structure, passes via the cuboid bone and the lateral two metatarsal bones. The medial part of this, structure is more important. The head of the talus marks the summit of this arch, located, between the sustentaculum tali and the navicular bone. The anterior pillar of the medial arch, is composed of the navicular bone, the three cuneiforms and the medial three metatarsal, bones., The transverse arch is situated on the anterior part of the tarsus and the posterior part of the, metatarsus. The cuneiforms and metatarsal bases narrow inferiorly, which contributes to the, shape of the arch., , Intertarsal joints
Page 1580 :
Sub talar joint, , Formed by the cylindrical facet on the lower surface of the body of the, talus and the posterior facet on the upper surface of the calcaneus. The, facet on the talus is concave anteroposteriorly, the other is convex. The, synovial cavity of this joint does not communicate with any other joint., , Talocalcaneonavicular, joint, , The anterior part of the socket is formed by the concave articular, surface of the navicular bone, posteriorly by the upper surface of the, sustentaculum tali. The talus sits within this socket, , Calcaneocuboid joint, , Highest point in the lateral part of the longitudinal arch. The lower, aspect of this joint is reinforced by the long plantar and plantar, calcaneocuboid ligaments., , Transverse tarsal joint, , The talocalcaneonavicular joint and the calcaneocuboid joint extend, across the tarsus in an irregular transverse plane, between the talus and, calcaneus behind and the navicular and cuboid bones in front. This, plane is termed the transverse tarsal joint., , Cuneonavicular joint, , Formed between the convex anterior surface of the navicular bone and, the concave surface of the the posterior ends of the three cuneiforms., , Intercuneiform joints, , Between the three cuneiform bones., , Cuneocuboid joint, , Between the circular facets on the lateral cuneiform bone and the, cuboid. This joint contributes to the tarsal part of the transverse arch., , A detailed knowledge of the joints is not required for MRCS Part A. However, the contribution they, play to the overall structure of the foot should be appreciated, Ligaments of the ankle joint and foot
Page 1581 :
Image sourced from Wikipedia, , Muscles of the foot, , Muscle, , Origin, , Insertion, , Nerve, supply, , Action, , Abductor, hallucis, , Medial side of the calcaneus,, flexor retinaculum, plantar, aponeurosis, , Medial side of, the base of the, proximal, phalanx, , Medial, plantar, nerve, , Abducts the great toe, , Flexor, digitorum, brevis, , Medial process of the, calcaneus, plantar, eponeurosis., , Via 4 tendons, into the, middle, phalanges of, the lateral 4, toes., , Medial, plantar, nerve, , Flexes all the joints of, the lateral 4 toes except, for the interphalangeal, joint., , Abductor, digit, minimi, , From the tubercle of the, calcaneus and from the, plantar aponeurosis, , Together with, flexor digit, minimi brevis, into the lateral, side of the, , Lateral, plantar, nerve, , Abducts the little toe at, the metatarsophalangeal, joint
Page 1582 :
base of the, proximal, phalanx of the, little toe, , Flexor, hallucis, brevis, , From the medial side of the, plantar surface of the cuboid, bone, from the adjacent part, of the lateral cuneiform bone, and from the tendon of, tibialis posterior., , Into the, proximal, phalanx of the, great toe, the, tendon, contains a, sesamoid bone, , Medial, plantar, nerve, , Flexes the, metatarsophalangeal, joint of the great toe., , Adductor, hallucis, , Arises from two heads. The, oblique head arises from the, sheath of the peroneus longus, tendon, and from the plantar, surfaces of the bases of the, 2nd, 3rd and 4th metatarsal, bones. The transverse head, arises from the plantar, surface of the lateral 4, metatarsophalangeal joints, and from the deep transverse, metatarsal ligament., , Lateral side of, the base of the, proximal, phalanx of the, great toe., , Lateral, plantar, nerve, , Adducts the great toe, towards the second toe., Helps maintain the, transverse arch of the, foot., , Extensor, digitorum, brevis, , On the dorsal surface of the, foot from the upper surface of, the calcaneus and its, associated fascia, , Via four thin, tendons which, run forward, and medially, to be inserted, into the, medial four, toes. The, lateral three, tendons join, with hoods of, extensor, digitorum, longus., , Deep, peroneal, , Extend the, metatarsophalangeal, joint of the medial four, toes. It is unable to, extend the, interphalangeal joint, without the assistance of, the lumbrical muscles., , Nerves in the foot
Page 1583 :
Lateral plantar nerve, Passes anterolaterally towards the base of the 5th metatarsal between flexor digitorum brevis and, flexor accessorius. On the medial aspect of the lateral plantar artery. At the base of the 5th, metatarsal it splits into superficial and deep branches., Medial plantar nerve, Passes forwards with the medial plantar artery under the cover of the flexor retinaculum to the, interval between abductor hallucis and flexor digitorum brevis on the sole of the foot., Plantar arteries, Arise under the cover of the flexor retinaculum, midway between the tip of the medial malleolus and, the most prominent part of the medial side of the heel., , , , , Medial plantar artery. Passes forwards medial to medial plantar nerve in the space between, abductor hallucis and flexor digitorum brevis.Ends by uniting with a branch of the 1st plantar, metatarsal artery., Lateral plantar artery. Runs obliquely across the sole of the foot. It lies lateral to the lateral, plantar nerve. At the base of the 5th metatarsal bone it arches medially across the foot on, the metatarsals, , Dorsalis pedis artery, This vessel is a direct continuation of the anterior tibial artery. It commences on the front of the ankle, joint and runs to the proximal end of the first metatarsal space. Here is gives off the arcuate artery, and continues forwards as the first dorsal metatarsal artery. It is accompanied by two veins, throughout its length. It is crossed by the extensor hallucis brevis, Next question
Page 1584 :
Question 215 of 560, Which of the following is not a content of the anterior triangle of the neck?, , Vagus nerve, , Submandibular gland, , Phrenic nerve, , Internal jugular vein, , Hypoglossal nerve, , The phrenic nerve is a content of the posterior triangle. The anterior triangle contains the carotid, sheath and its contents., Please rate this question:, , Discuss and give feedback, , Next question, , Anterior triangle of the neck, Boundaries, , Anterior border of the Sternocleidomastoid, Lower border of mandible, Anterior midline, , Sub triangles (divided by Digastric above and Omohyoid), , , , , Muscular triangle: Neck strap muscles, Carotid triangle: Carotid sheath, Submandibular Triangle (digastric)
Page 1585 :
Contents of the anterior triangle, , Digastric triangle, , Submandibular gland, Submandibular nodes, Facial vessels, Hypoglossal nerve, , Muscular triangle, , Strap muscles, External jugular vein, , Carotid triangle, , Carotid sheath (Common carotid, vagus and internal jugular vein), Ansa cervicalis, , Nerve supply to digastric muscle, , , , Anterior: Mylohyoid nerve, Posterior: Facial nerve, , Image sourced from Wikipedia, , Next question
Page 1586 :
Question 216 of 560, A 32 year old attends neurology clinic complaining of tingling in his hand. He has radial deviation of, his wrist and there is mild clawing of his fingers, with the 4th and 5th digits being relatively spared., What is the most likely lesion?, , Ulnar nerve damage at the wrist, , Ulnar nerve damage at the elbow, , Radial nerve damage at the elbow, , Median nerve damage at the wrist, , Median nerve damage at the elbow, The ulnar paradox- the higher the lesion, the less the clawing of the fingers seen clinically., At the elbow the ulnar nerve lesion affects the flexor carpi ulnaris and flexor digitorum profundus., Please rate this question:, , Discuss and give feedback, , Next question, , Ulnar nerve, Origin, , , C8, T1, , Supplies (no muscles in the upper arm), , , , , , , , Flexor carpi ulnaris, Flexor digitorum profundus, Flexor digiti minimi, Abductor digiti minimi, Opponens digiti minimi, Adductor pollicis
Page 1588 :
Branch, , Supplies, , Muscular branch, , Flexor carpi ulnaris, Medial half of the flexor digitorum profundus, , Palmar cutaneous branch (Arises near the, middle of the forearm), , Skin on the medial part of the palm, , Dorsal cutaneous branch, , Dorsal surface of the medial part of the hand, , Superficial branch, , Cutaneous fibres to the anterior surfaces of the, medial one and one-half digits, , Deep branch, , Hypothenar muscles, All the interosseous muscles, Third and fourth lumbricals, Adductor pollicis, Medial head of the flexor pollicis brevis, , Effects of injury, , Damage at the wrist, , , , , , Wasting and paralysis of intrinsic hand muscles (claw hand), Wasting and paralysis of hypothenar muscles, Loss of sensation medial 1 and half fingers, , Damage at the elbow, , , , , Radial deviation of the wrist, Clawing less in 4th and 5th digits, Next question
Page 1589 :
Question 217 of 560, A 22 year old man is undergoing an endotracheal intubation. Which of the following vertebral levels, is consistent with the origin of the trachea?, , C2, , T1, , C6, , C4, , C3, , The trachea commences at C6. It terminates at the level of T5 (or T6 in tall subjects in deep, inspiration)., Please rate this question:, , Discuss and give feedback, , Next question, , Trachea, Trachea, , Location, , C6 vertebra to the upper border of T5 vertebra (bifurcation), , Arterial and venous supply, , Inferior thyroid arteries and the thyroid venous plexus., , Nerve, , Branches of vagus, sympathetic and the recurrent nerves, , Relations in the neck, , Anterior(Superior to, , , , , Isthmus of the thyroid gland, Inferior thyroid veins
Page 1590 :
inferior), , Posterior, Laterally, , , , , , , , Arteria thyroidea ima (when that vessel exists), Sternothyroid, Sternohyoid, Cervical fascia, Anastomosing branches between the anterior jugular, veins, , Oesophagus., , , , , , Common carotid arteries, Right and left lobes of the thyroid gland, Inferior thyroid arteries, Recurrent laryngeal nerves, , Relations in the thorax, Anterior, , , Manubrium, the remains of the thymus, the aortic arch, left common carotid arteries, and the, deep cardiac plexus, , Lateral, , , In the superior mediastinum, on the right side is the pleura and right vagus; on its left side, are the left recurrent nerve, the aortic arch, and the left common carotid and subclavian, arteries., Next question
Page 1591 :
Question 218 of 560, A young child undergoes a difficult craniotomy for fulminant mastoiditis and associated abscess., During the procedure the trigeminal nerve is severely damaged within Meckels cave. Which deficit is, least likely to be present?, , Anaesthesia over the ipsilateral anterior aspect of the scalp, , Loss of the corneal reflex, , Weakness of the ipsilateral masseter muscle, , Anaesthesia of the anterior aspect of the lip, , Anaesthesia over the entire ipsilateral side of the face, , The angle of the jaw is not innervated by sensory fibres of the trigeminal nerve and is spared in this, type of injury., Remember the trigeminal nerve provides motor innervation to the muscles of mastication. The close, proximity of the site of injury to the motor fibres is likely to result in at least some compromise of, motor muscle function., Please rate this question:, , Discuss and give feedback, , Next question, , Trigeminal nerve, The trigeminal nerve is the main sensory nerve of the head. In addition to its major sensory role, it, also innervates the muscles of mastication., Distribution of the trigeminal nerve, , Sensory, , , , , , , , Scalp, Face, Oral cavity (and teeth), Nose and sinuses, Dura mater
Page 1592 :
Motor, , , , , , , , Muscles of mastication, Mylohyoid, Anterior belly of digastric, Tensor tympani, Tensor palati, , Autonomic connections (ganglia), , , , , , , Ciliary, Sphenopalatine, Otic, Submandibular, , Path, , , , , Originates at the pons, Sensory root forms the large, crescentic trigeminal ganglion within Meckel's cave, and, contains the cell bodies of incoming sensory nerve fibres. Here the 3 branches exit., The motor root cell bodies are in the pons and the motor fibres are distributed via the, mandibular nerve. The motor root is not part of the trigeminal ganglion., , Branches of the trigeminal nerve, , Ophthalmic nerve, , Sensory only, , Maxillary nerve, , Sensory only, , Mandibular nerve, , Sensory and motor, , Sensory, , Ophthalmic, , Exits skull via the superior orbital fissure, Sensation of: scalp and forehead, the upper eyelid, the conjunctiva and cornea of, the eye, the nose (including the tip of the nose, except alae nasi), the nasal, mucosa, the frontal sinuses, and parts of the meninges (the dura and blood, vessels)., , Maxillary, nerve, , Exit skull via the foramen rotundum, Sensation: lower eyelid and cheek, the nares and upper lip, the upper teeth and, gums, the nasal mucosa, the palate and roof of the pharynx, the maxillary,
Page 1593 :
ethmoid and sphenoid sinuses, and parts of the meninges., , Mandibular, nerve, , Exit skull via the foramen ovale, Sensation: lower lip, the lower teeth and gums, the chin and jaw (except the angle, of the jaw), parts of the external ear, and parts of the meninges., , Motor, Distributed via the mandibular nerve., The following muscles of mastication are innervated:, , , , , , Masseter, Temporalis, Medial pterygoid, Lateral pterygoid, , Other muscles innervated include:, , , , , , Tensor veli palatini, Mylohyoid, Anterior belly of digastric, Tensor tympani, Next question
Page 1594 :
Question 219-221 of 560, Theme: Nerve lesions, , A., B., C., D., E., F., , Iliohypogastric nerve, Ilioinguinal nerve, Lateral cutaneous nerve of the thigh, Femoral nerve, Saphenous nerve, Genitofemoral nerve, , Please select the most likely nerve implicated in the situation described. Each option may be used, once, more than once or not at all., , 219., , A 42 year old woman complains of a burning pain of her anterior thigh which worsens on, walking. There is a positive tinel sign over the inguinal ligament., You answered Iliohypogastric nerve, The correct answer is Lateral cutaneous nerve of the thigh, The lateral cutaneous nerve supplies sensation to the anterior and lateral aspect of the, thigh. Entrapment is commonly due to intra and extra pelvic causes. Treatment involves, local anaesthetic injections., , 220., , A 29 year old woman has had a Pfannenstiel incision. She has pain over the inguinal, ligament which radiates to the lower abdomen. There is tenderness when the inguinal, canal is compressed., You answered Iliohypogastric nerve, The correct answer is Ilioinguinal nerve, , 221., , A 22 year man is shot in the groin. On examination he has weak hip flexion, weak knee, extension, and impaired quadriceps tendon reflex, as well as sensory deficit in the, anteromedial aspect of the thigh., You answered Iliohypogastric nerve, The correct answer is Femoral nerve, This is a classical description of a femoral nerve injury.
Page 1595 :
Please rate this question:, , Discuss and give feedback, , Next question, , Nerve lesions during surgery, A variety of different procedures carry the risk of iatrogenic nerve injury. These are important not, only from the patients perspective but also from a medicolegal standpoint., The following operations and their associated nerve lesions are listed here:, , , , , , , , , , , Posterior triangle lymph node biopsy and accessory nerve lesion., Lloyd Davies stirrups and common peroneal nerve., Thyroidectomy and laryngeal nerve., Anterior resection of rectum and hypogastric autonomic nerves., Axillary node clearance; long thoracic nerve, thoracodorsal nerve and intercostobrachial, nerve., Inguinal hernia surgery and ilioinguinal nerve., Varicose vein surgery- sural and saphenous nerves., Posterior approach to the hip and sciatic nerve., Carotid endarterectomy and hypoglossal nerve., , There are many more, with sound anatomical understanding of the commonly performed procedures, the incidence of nerve lesions can be minimised. They commonly occur when surgeons operate in, an unfamiliar tissue plane or by blind placement of haemostats (not recommended)., Next question
Page 1596 :
Question 222 of 560, , Which of the following is not a branch of the external carotid artery?, , Facial artery, , Lingual artery, , Superior thyroid artery, , Mandibular artery, , Maxillary artery, External carotid artery branches mnemonic:, 'Some Angry Lady Figured Out PMS', Superior thyroid (superior laryngeal artery branch), Ascending pharyngeal, Lingual, Facial (tonsillar and labial artery), Occipital, Posterior auricular, Maxillary (inferior alveolar artery, middle meningeal artery), Superficial temporal, , Please rate this question:, , Discuss and give feedback, , Next question
Page 1597 :
External carotid artery, The external carotid commences immediately lateral to the pharyngeal side wall. It ascends and lies, anterior to the internal carotid and posterior to the posterior belly of digastric and stylohyoid. More, inferiorly it is covered by sternocleidomastoid, passed by hypoglossal nerves, lingual and facial, veins., It then pierces the fascia of the parotid gland finally dividing into its terminal branches within the, gland itself., Surface marking of the carotid, This is an imaginary line drawn from the bifurcation of the common carotid passing behind the angle, of the jaw to a point immediately anterior to the tragus of the ear., Branches of the external carotid artery, It has six branches, three in front, two behind and one deep., , Three in front, , Superior thyroid, Lingual, Facial, , Two behind, , Occipital, Posterior auricular, , Deep, , Ascending pharyngeal, , It terminates by dividing into the superficial temporal and maxillary arteries in the parotid gland.
Page 1598 :
Image sourced from Wikipedia, , Next question
Page 1599 :
Question 223 of 560, , A 23 year old man is stabbed in the groin, several structures are injured and the adductor longus, muscle has been lacerated. Which of the following nerves is responsible for the innervation of, adductor longus?, , Femoral nerve, , Obturator nerve, , Sciatic nerve, , Common peroneal nerve, , Ilioinguinal nerve, , The adductors are innervated by the obturator nerve, Please rate this question:, , Discuss and give feedback, , Next question, , Adductor longus, Origin, , Anterior body of pubis, , Insertion, , Middle third of linea aspera
Page 1600 :
Action, , Adducts and flexes the thigh, medially rotate the hip, , Innervation, , Anterior division of obturator nerve (L2, L3, L4), , The schematic image below demonstrates the relationship of the adductor muscles, , Image sourced from Wikipedia, , Next question
Page 1601 :
Question 224 of 560, Which of the following statements relating to the basilar artery and its branches is false?, , The superior cerebellar artery may be decompressed to treat trigeminal neuralgia, , Occlusion of the posterior cerebral artery causes contralateral loss of the visual field, , The oculomotor nerve lies between the superior cerebellar and posterior cerebral arteries, , The posterior inferior cerebellar artery is the largest of the cerebellar arteries arising from, the basilar artery, The labyrinthine branch is accompanied by the facial nerve, , The posterior inferior cerebellar artery is the largest of the cerebellar arteries arising from the, vertebral artery. The labyrinthine artery is long and slender and may arise from the lower part of the, basilar artery. It accompanies the facial and vestibulocochlear nerves into the internal auditory, meatus. The posterior cerebral artery is often larger than the superior cerebellar artery and it is, separated from the vessel, near it's origin, by the oculomotor nerve. Arterial decompression is a well, established therapy for trigeminal neuralgia., Please rate this question:, , Discuss and give feedback, , Next question, , Circle of Willis, The two internal carotid arteries and two vertebral arteries form an anastomosis known as the Circle, of Willis on the inferior surface of the brain. Each half of the circle is formed by:, 1. Anterior communicating artery, 2. Anterior cerebral artery, 3. Internal carotid artery, 4. Posterior communicating artery, 5. Posterior cerebral arteries and the termination of the basilar artery, The circle and its branches supply; the corpus striatum, internal capsule, diencephalon and, midbrain.
Page 1602 :
Image sourced from Wikipedia, , Vertebral arteries, , , , , , Enter the cranial cavity via foramen magnum, Lie in the subarachnoid space, Ascend on anterior surface of medulla oblongata, Unite to form the basilar artery at the base of the pons, , Branches:, , , , , Posterior spinal artery, Anterior spinal artery, Posterior inferior cerebellar artery, , Basilar artery, Branches:
Page 1603 :
, , , , , , Anterior inferior cerebellar artery, Labyrinthine artery, Pontine arteries, Superior cerebellar artery, Posterior cerebral artery, , Internal carotid arteries, Branches:, , , , , , Posterior communicating artery, Anterior cerebral artery, Middle cerebral artery, Anterior choroid artery, Next question
Page 1604 :
Question 225 of 560, Which of the following muscles does not recieve any innervation from the sciatic nerve?, , Semimembranosus, , Quadriceps femoris, , Biceps femoris, , Semitendinosus, , Adductor magnus, , The sciatic nerve is traditionally viewed as being a nerve of the posterior compartment. It is known to, contribute to the innervation of adductor magnus (although the main innervation to this muscle is, from the obturator nerve). The quadriceps femoris is nearly always innervated by the femoral nerve., Please rate this question:, , Discuss and give feedback, , Next question, , Sciatic nerve, The sciatic nerve is formed from the sacral plexus and is the largest nerve in the body. It is the, continuation of the main part of the plexus arising from ventral rami of L4 to S3. These rami, converge at the inferior border of piriformis to form the nerve itself. It passes through the inferior part, of the greater sciatic foramen and emerges beneath piriformis. Medially, lie the inferior gluteal nerve, and vessels and the pudendal nerve and vessels. It runs inferolaterally under the cover of gluteus, maximus midway between the greater trochanter and ischial tuberosity. It receives its blood supply, from the inferior gluteal artery. The nerve provides cutaneous sensation to the skin of the foot and, the leg. It also innervates the posterior thigh muscles and the lower leg and foot muscles. The nerve, splits into the tibial and common peroneal nerves approximately half way down the posterior thigh., The tibial nerve supplies the flexor muscles and the common peroneal nerve supplies the extensor, muscles and the abductor muscles., Summary points, , Origin, , Spinal nerves L4 - S3
Page 1605 :
Articular Branches, , Hip joint, , Muscular branches in, upper leg, , , , , , , Semitendinosus, Semimembranosus, Biceps femoris, Part of adductor magnus, , Cutaneous sensation, , , , , , Posterior aspect of thigh (via cutaneous nerves), Gluteal region, Entire lower leg (except the medial aspect), , Terminates, , , , , At the upper part of the popliteal fossa by dividing into the tibial and, peroneal nerves, , The nerve to the short head of the biceps femoris comes from the common peroneal part of, the sciatic and the other muscular branches arise from the tibial portion., The tibial nerve goes on to innervate all muscles of the foot except the extensor digitorum, brevis (which is innervated by the common peroneal nerve)., Next question
Page 1608 :
Branches, , Branch, , Supplies, , Muscular branch, , Flexor carpi ulnaris, Medial half of the flexor digitorum profundus, , Palmar cutaneous branch (Arises near the, middle of the forearm), , Skin on the medial part of the palm, , Dorsal cutaneous branch, , Dorsal surface of the medial part of the hand, , Superficial branch, , Cutaneous fibres to the anterior surfaces of the, medial one and one-half digits, , Deep branch, , Hypothenar muscles, All the interosseous muscles, Third and fourth lumbricals, Adductor pollicis, Medial head of the flexor pollicis brevis, , Effects of injury, , Damage at the wrist, , , , , , Wasting and paralysis of intrinsic hand muscles (claw hand), Wasting and paralysis of hypothenar muscles, Loss of sensation medial 1 and half fingers, , Damage at the elbow, , , , , Radial deviation of the wrist, Clawing less in 4th and 5th digits, Next question
Page 1609 :
Question 227 of 560, Which of the structures listed below overlies the cephalic vein?, , Extensor retinaculum, , Bicipital aponeurosis, , Biceps muscle, , Antebrachial fascia, , None of the above, , The cephalic vein is superficially located in the upper limb and overlies most the fascial planes. It, pierces the coracoid membrane (continuation of the clavipectoral fascia) to terminate in the axillary, vein. It lies anterolaterally to biceps., Please rate this question:, , Discuss and give feedback, , Next question, , Cephalic vein, Path, , , , , , Dorsal venous arch drains laterally into the cephalic vein, Crosses the anatomical snuffbox and travels laterally up the arm, At the antecubital fossa connected to the basilic vein by the median cubital vein, Pierces deep fascia of deltopectoral groove to join axillary vein, Next question
Page 1612 :
Question 229 of 560, A 22 year old man is involved in a fight. He sustains a laceration to the posterior aspect of his wrist., In the emergency department the wound is explored and the laceration is found to be transversely, orientated and overlies the region of the extensor retinaculum, which is intact. Which of the following, structures is least likely to be injured in this scenario?, , Dorsal cutaneous branch of the ulnar nerve, , Tendon of extensor indicis, , Basilic vein, , Superficial branch of the radial nerve, , Cephalic vein, , The extensor retinaculum attaches to the radius proximal to the styloid, thereafter it runs obliquely, and distally to wind around the ulnar styloid (but does not attach to it). The extensor tendons lie deep, to the extensor retinaculum and would therefore be less susceptible to injury than the superficial, structures., Please rate this question:, , Discuss and give feedback, , Next question, , Extensor retinaculum, The extensor rentinaculum is a thickening of the deep fascia that stretches across the back of the, wrist and holds the long extensor tendons in position., Its attachments are:, , , , The pisiform and triquetral medially, The end of the radius laterally, , Structures related to the extensor retinaculum, , Structures superficial to the, , , , , Basilic vein, Dorsal cutaneous branch of the ulnar nerve
Page 1614 :
Image sourced from Wikipedia, , Next question
Page 1615 :
Question 230 of 560, Which of the following is not a content of the porta hepatis?, , Portal vein, , Hepatic artery, , Cystic duct, , Lymph nodes, , None of the above, , The cystic duct lies outside the porta hepatis and is an important landmark in laparoscopic, cholecystectomy. The structures in the porta hepatis are:, , , , , Portal vein, Hepatic artery, Common hepatic duct, , These structures divide immediately after or within the porta hepatis to supply the functional left and, right lobes of the liver., The porta hepatis is also surrounded by lymph nodes, that may enlarge to produce obstructive, jaundice and parasympathetic nervous fibres that travel along vessels to enter the liver., Please rate this question:, , Discuss and give feedback, , Next question, , Liver, Structure of the liver, , Right lobe, , , , , Supplied by right hepatic artery, Contains Couinaud segments V to VIII (-/+Sg I), , Left lobe, , , , Supplied by the left hepatic artery
Page 1616 :
, , Contains Couinaud segments II to IV (+/- Sg1), , Quadrate lobe, , , , , , , , Part of the right lobe anatomically, functionally is part of the left, Couinaud segment IV, Porta hepatis lies behind, On the right lies the gallbladder fossa, On the left lies the fossa for the umbilical vein, , Caudate lobe, , , , , , , , Supplied by both right and left hepatic arteries, Couinaud segment I, Lies behind the plane of the porta hepatis, Anterior and lateral to the inferior vena cava, Bile from the caudate lobe drains into both right and left hepatic ducts, , Detailed knowledge of Couinaud segments is not required for MRCS, , , Between the liver lobules are portal canals which contain the portal triad: Hepatic Artery,, Portal Vein, tributary of Bile Duct., , Relations of the liver, , Anterior, , Postero inferiorly, , Diaphragm, , Oesophagus, , Xiphoid process, , Stomach, , Duodenum, , Hepatic flexure of colon, , Right kidney
Page 1617 :
Gallbladder, , Inferior vena cava, , Porta hepatis, , Location, , Postero inferior surface, it joins nearly at right angles with the left sagittal fossa, and, separates the caudate lobe behind from the quadrate lobe in front, , Transmits, , , , , , , , Common hepatic duct, Hepatic artery, Portal vein, Sympathetic and parasympathetic nerve fibres, Lymphatic drainage of the liver (and nodes), , Ligaments, , Falciform ligament, , , , , , 2 layer fold peritoneum from the umbilicus to anterior liver surface, Contains ligamentum teres (remnant umbilical vein), On superior liver surface it splits into the coronary and left, triangular ligaments, , Ligamentum teres, , Joins the left branch of the portal vein in the porta hepatis, , Ligamentum, venosum, , Remnant of ductus venosus, , Arterial supply, , , Hepatic artery, , Venous, , , , Hepatic veins, Portal vein, , Nervous supply
Page 1618 :
, , Sympathetic and parasympathetic trunks of coeliac plexus, Next question
Page 1619 :
Question 231 of 560, Which of the following structures is not closely related to the carotid sheath?, , Sternothyroid muscle, , Sternohyoid muscle, , Hypoglossal nerve, , Superior belly of omohyoid muscle, , Anterior belly of digastric muscle, , At its lower end the carotid sheath is related to sternohyoid and sternothyroid. Opposite the cricoid, cartilage the sheath is crossed by the superior belly of omohyoid. Above this level the sheath is, covered by the sternocleidomastoid muscle. Above the level of the hyoid the vessels pass deep to, the posterior belly of digastric and stylohyoid. Opposite the hyoid bone the sheath is crossed, obliquely by the hypoglossal nerve., Please rate this question:, , Discuss and give feedback, , Next question, , Common carotid artery, The right common carotid artery arises at the bifurcation of the brachiocephalic trunk, the left, common carotid arises from the arch of the aorta. Both terminate at the level of the upper border of, the thyroid cartilage (the lower border of the third cervical vertebra) by dividing into the internal and, external carotid arteries., Left common carotid artery, This vessel arises immediately to the left and slightly behind the origin of the brachiocephalic trunk., Its thoracic portion is 2.5- 3.5 cm in length and runs superolaterally to the sternoclavicular joint., In the thorax, The vessel is in contact, from below upwards, with the trachea, left recurrent laryngeal nerve, left, margin of the oesophagus. Anteriorly the left brachiocephalic vein runs across the artery, and the, cardiac branches from the left vagus descend in front of it. These structures together with the, thymus and the anterior margins of the left lung and pleura separate the artery from the manubrium.
Page 1620 :
In the neck, The artery runs superiorly deep to sternocleidomastoid and then enters the anterior triangle. At this, point it lies within the carotid sheath with the vagus nerve and the internal jugular vein. Posteriorly, the sympathetic trunk lies between the vessel and the prevertebral fascia. At the level of C7 the, vertebral artery and thoracic duct lie behind it. The anterior tubercle of C6 transverse process is, prominent and the artery can be compressed against this structure (it corresponds to the level of the, cricoid)., Anteriorly at C6 the omohyoid muscle passes superficial to the artery., Within the carotid sheath the jugular vein lies lateral to the artery., Right common carotid artery, The right common carotid arises from the brachiocephalic artery. The right common carotid artery, corresponds with the cervical portion of the left common carotid, except that there is no thoracic duct, on the right. The oesophagus is less closely related to the right carotid than the left., Summary points about the carotid anatomy, Path, Passes behind the sternoclavicular joint (12% patients above this level) to the upper border of the, thyroid cartilage, to divide into the external (ECA) and internal carotid arteries (ICA)., Relations, , , , , , , Level of 6th cervical vertebra crossed by omohyoid, Then passes deep to the thyrohyoid, sternohyoid, sternomastoid muscles., Passes anterior to the carotid tubercle (transverse process 6th cervical vertebra)-NB, compression here stops haemorrhage., The inferior thyroid artery passes posterior to the common carotid artery., Then : Left common carotid artery crosses the thoracic duct, Right common carotid artery, crossed by recurrent laryngeal nerve
Page 1621 :
Image sourced from Wikipedia, , Next question
Page 1622 :
Question 232 of 560, A 21 year old develops tonsillitis. He is in considerable pain. Which of the following nerves is, responsible for the sensory innervation of the tonsillar fossa?, , Facial nerve, , Trigeminal nerve, , Glossopharyngeal nerve, , Hypoglossal nerve, , Vagus, , The glossopharyngeal nerve is the main sensory nerve for the tonsillar fossa. A lesser contribution is, made by the lesser palatine nerve. Because of this otalgia may occur following tonsillectomy., Please rate this question:, , Discuss and give feedback, , Next question, , Tonsil, Anatomy, , , , , , , Each palatine tonsil has two surfaces, a medial surface which projects into the pharynx and a, lateral surface that is embedded in the wall of the pharynx., They are usually 25mm tall by 15mm wide, although this varies according to age and may be, almost completely atrophied in the elderly., Their arterial supply is from the tonsillar artery, a branch of the facial artery., Its veins pierce the constrictor muscle to join the external palatine or facial veins. The, external palatine vein is immediately lateral to the tonsil, which may result in haemorrhage, during tonsillectomy., Lymphatic drainage is the jugulodigastric node and the deep cervical nodes., , Tonsillitis
Page 1623 :
, , , Usually bacterial (50%)- group A Streptococcus. Remainder viral., May be complicated by development of abscess (quinsy). This may distort the uvula., , - Indications for tonsillectomy include recurrent acute tonsillitis, suspected malignancy, enlargement, causing sleep apnoea., - Dissection tonsillectomy is the preferred technique with haemorrhage being the commonest, complication. Delayed otalgia may occur owing to irritation of the glossopharyngeal nerve., Next question
Page 1624 :
Question 233 of 560, , A man has an incision sited that runs 8cm from the deltopectoral groove to the midline. Which of the, following is not at risk of injury?, , Cephalic vein, , Shoulder joint capsule, , Axillary artery, , Pectoralis major, , Trunk of the brachial plexus, , Theme from April 2012 Exam, This region will typically lie medial to the joint capsule. The diagram below illustrates the plane that, this would transect and as it can be appreciated the other structures are all at risk of injury.
Page 1625 :
Image sourced from Wikipedia, , Please rate this question:, , Discuss and give feedback, , Next question, , Pectoralis major muscle
Page 1626 :
Origin, , From the medial two thirds of the clavicle, manubrium and sternocostal angle, , Insertion, , Lateral edge of the bicipital groove of the humerus, , Nerve supply, , Lateral pectoral nerve, , Actions, , Adductor and medial rotator of the humerus, , Next question
Page 1627 :
Question 234 of 560, A surgeon is due to perform a laparotomy for perforated duodenal ulcer. An upper midline incision is, to be performed. Which of the following structures is the incision most likely to divide?, , Rectus abdominis muscle, , External oblique muscle, , Linea alba, , Internal oblique muscle, , None of the above, , Theme from September 2011 Exam, Upper midline abdominal incisions will involve the division of the linea alba. Division of muscles will, not usually improve access in this approach and they would not be routinely encountered during this, incision., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal incisions, Midline incision, , , , , , Paramedian, incision, , , , , Commonest approach to the abdomen, Structures divided: linea alba, transversalis fascia, extraperitoneal fat,, peritoneum (avoid falciform ligament above the umbilicus), Bladder can be accessed via an extraperitoneal approach through the, space of Retzius, Parallel to the midline (about 3-4cm), Structures divided/retracted: anterior rectus sheath, rectus (retracted),, posterior rectus sheath, transversalis fascia, extraperitoneal fat,, peritoneum
Page 1628 :
Battle, , , , Incision is closed in layers, , , , Similar location to paramedian but rectus displaced medially (and thus, denervated), Now seldom used, , , , Kocher's, , Incision under right subcostal margin e.g. Cholecystectomy (open), , Lanz, , Incision in right iliac fossa e.g. Appendicectomy, , Gridiron, , Oblique incision centered over McBurneys point- usually appendicectomy, (less cosmetically acceptable than Lanz, , Gable, , Rooftop incision, , Pfannenstiel's, , Transverse supra pubic, primarily used to access pelvic organs, , McEvedy's, , Groin incision e.g. Emergency repair strangulated femoral hernia, , Rutherford, Morrison, , Extraperitoneal approach to left or right lower quadrants. Gives excellent, access to iliac vessels and is the approach of choice for first time renal, transplantation., , Image sourced from Wikipedia, , Next question
Page 1629 :
Question 235 of 560, A 59 year old man is undergoing an extended right hemicolectomy for a carcinoma of the splenic, flexure of the colon. The surgeons divide the middle colic vein close to its origin. Into which of the, following structures does this vessel primarily drain?, , Superior mesenteric vein, , Portal vein, , Inferior mesenteric vein, , Inferior vena cava, , Ileocolic vein, , The middle colonic vein drains into the SMV, if avulsed during mobilisation then dramatic, haemorrhage can occur and be difficult to control., Please rate this question:, , Discuss and give feedback, , Next question, , Transverse colon, , , , , , The right colon undergoes a sharp turn at the level of the hepatic flexure to become the, transverse colon., At this point it also becomes intraperitoneal., It is connected to the inferior border of the pancreas by the transverse mesocolon., The greater omentum is attached to the superior aspect of the transverse colon from which it, can easily be separated. The mesentery contains the middle colic artery and vein. The, greater omentum remains attached to the transverse colon up to the splenic flexure. At this, point the colon undergoes another sharp turn., , Relations, Superior, , Liver and gall-bladder, the greater curvature of the stomach, and the lower end of the, spleen, , Inferior, , Small intestine
Page 1630 :
Anterior, , Greater omentum, , Posterior, , From right to left with the descending portion of the duodenum, the head of the pancreas,, convolutions of the jejunum and ileum, spleen, , Next question
Page 1631 :
Question 236-238 of 560, Theme: Nerve Injury, , A., B., C., D., E., F., G., , Median nerve, Ulnar nerve, Radial nerve, Musculocutaneous nerve, Axillary nerve, Anterior interosseous nerve, Posterior interosseous nerve, , For each scenario please select the most likely underlying nerve injury. Each option may be used, once, more than once or not at all., , 236., , A 10 year old boy is admitted to casualty following a fall. On examination there is, deformity and swelling of the upper arm. The ability to flex the fingers of the affected, limb is impaired. However, there is not sensory impairment. Imaging confirms a, displaced supra condylar fracture, You answered Median nerve, The correct answer is Anterior interosseous nerve, Supracondylar fractures may be complicated by neurovascular compromise. The anterior, interosseous nerve is most commonly affected. It has no sensory supply so the defect is, motor alone., , 237., , A well toned weight lifter attends clinic reporting weakness of his left arm. There is, weakness of flexion and supination of the forearm., You answered Median nerve, The correct answer is Musculocutaneous nerve, Musculocutaneous nerve compression due to entrapment of the nerve between biceps and, brachialis. Elbow flexion and supination of the arm are affected. This is a rare isolated, injury., , 238., , An 18 year old girl sustains an Holstein-Lewis fracture. Which nerve is at risk?, You answered Median nerve
Page 1632 :
The correct answer is Radial nerve, Proximal lesions affect the triceps. Also paralysis of wrist extensors and forearm, supinators occur. Reduced sensation of dorsoradial aspect of hand and dorsal 31/2, fingers. Holstein-Lewis fractures are fractures of the distal humerus with radial nerve, entrapment., Please rate this question:, , Discuss and give feedback, , Next question, , Brachial plexus, Origin, , Anterior rami of C5 to T1, , Sections of the, plexus, , , , , Roots, trunks, divisions, cords, branches, Mnemonic:Real Teenagers Drink Cold Beer, , Roots, , , , , Located in the posterior triangle, Pass between scalenus anterior and medius, , Trunks, , , , , , Located posterior to middle third of clavicle, Upper and middle trunks related superiorly to the subclavian artery, Lower trunk passes over 1st rib posterior to the subclavian artery, , Divisions, , Apex of axilla, , Cords, , Related to axillary artery, , Diagram illustrating the branches of the brachial plexus
Page 1633 :
Image sourced from Wikipedia, , Cutaneous sensation of the upper limb, , Image sourced from Wikipedia, , Next question
Page 1634 :
Question 239 of 560, A 23 year old man is stabbed in the chest approximately 10cm below the right nipple. In the, emergency department a abdominal ultrasound scan shows a large amount of intraperitoneal blood., Which of the following statements relating to the likely site of injury is untrue?, , Part of its posterior surface is devoid of peritoneum., , The quadrate lobe is contained within the functional right lobe., , Its nerve supply is from the coeliac plexus., , The hepatic flexure of the colon lies posterio-inferiorly., , The right kidney is closely related posteriorly., , The right lobe of the liver is the most likely site of injury. Therefore the answer is B as the quadrate, lobe is functionally part of the left lobe of the liver. The liver is largely covered in peritoneum., Posteriorly there is an area devoid of peritoneum (the bare area of the liver). The right lobe of the, liver has the largest bare area (and is larger than the left lobe)., Please rate this question:, , Discuss and give feedback, , Next question, , Liver, Structure of the liver, , Right lobe, , , , , Supplied by right hepatic artery, Contains Couinaud segments V to VIII (-/+Sg I), , Left lobe, , , , , Supplied by the left hepatic artery, Contains Couinaud segments II to IV (+/- Sg1), , Quadrate lobe, , , , , , Part of the right lobe anatomically, functionally is part of the left, Couinaud segment IV, Porta hepatis lies behind
Page 1635 :
Caudate lobe, , , , , On the right lies the gallbladder fossa, On the left lies the fossa for the umbilical vein, , , , , , , , Supplied by both right and left hepatic arteries, Couinaud segment I, Lies behind the plane of the porta hepatis, Anterior and lateral to the inferior vena cava, Bile from the caudate lobe drains into both right and left hepatic ducts, , Detailed knowledge of Couinaud segments is not required for MRCS, , , Between the liver lobules are portal canals which contain the portal triad: Hepatic Artery,, Portal Vein, tributary of Bile Duct., , Relations of the liver, , Anterior, , Postero inferiorly, , Diaphragm, , Oesophagus, , Xiphoid process, , Stomach, , Duodenum, , Hepatic flexure of colon, , Right kidney, , Gallbladder, , Inferior vena cava, , Porta hepatis
Page 1636 :
Location, , Postero inferior surface, it joins nearly at right angles with the left sagittal fossa, and, separates the caudate lobe behind from the quadrate lobe in front, , Transmits, , , , , , , , Common hepatic duct, Hepatic artery, Portal vein, Sympathetic and parasympathetic nerve fibres, Lymphatic drainage of the liver (and nodes), , Ligaments, , Falciform ligament, , , , , , 2 layer fold peritoneum from the umbilicus to anterior liver surface, Contains ligamentum teres (remnant umbilical vein), On superior liver surface it splits into the coronary and left, triangular ligaments, , Ligamentum teres, , Joins the left branch of the portal vein in the porta hepatis, , Ligamentum, venosum, , Remnant of ductus venosus, , Arterial supply, , , Hepatic artery, , Venous, , , , Hepatic veins, Portal vein, , Nervous supply, , , Sympathetic and parasympathetic trunks of coeliac plexus, Next question
Page 1637 :
Question 240 of 560, A 22 year old man is involved in a fight and sustains a skull fracture with an injury to the middle, meningeal artery. A craniotomy is performed, and with considerable difficulty the haemorrhage from, the middle meningeal artery is controlled by ligating it close to its origin. What is the most likely, sensory impairment that the patient may notice post operatively?, , Parasthesia of the ipsilateral external ear, , Loss of taste sensation from the anterior two thirds of the tongue, , Parasthesia overlying the angle of the jaw, , Loss of sensation from the ipsilateral side of the tongue, , Loss of taste from the posterior two thirds of the tongue, , The auriculotemporal nerve is closely related to the middle meningeal artery and may be damaged, in this scenario. The nerve supplied sensation to the external ear and outermost part of the tympanic, membrane. The angle of the jaw is innervated by C2,3 roots and would not be affected. The tongue, is supplied by the glossopharyngeal nerve., Please rate this question:, , Discuss and give feedback, , Next question, , Middle meningeal artery, , , , , , , , Middle meningeal artery is typically the third branch of the first part of the maxillary artery,, one of the two terminal branches of the external carotid artery. After branching off the, maxillary artery in the infratemporal fossa, it runs through the foramen spinosum to supply, the dura mater (the outermost meninges) ., The middle meningeal artery is the largest of the three (paired) arteries which supply the, meninges, the others being the anterior meningeal artery and the posterior meningeal artery., The middle meningeal artery runs beneath the pterion. It is vulnerable to injury at this point,, where the skull is thin. Rupture of the artery may give rise to an extra dural hematoma., In the dry cranium, the middle meningeal, which runs within the dura mater surrounding the, brain, makes a deep indention in the calvarium., The middle meningeal artery is intimately associated with the auriculotemporal nerve which, wraps around the artery making the two easily identifiable in the dissection of human, cadavers and also easily damaged in surgery.
Page 1638 :
Question 241 of 560, A 72 year old man presents with haemoptysis and undergoes a bronchoscopy. The carina is noted, to be widened. At which level does the trachea bifurcate?, , T3, , T5, , T7, , T2, , T8, , The trachea bifurcates at the level of the fifth thoracic vertebra. Or the sixth in tall subjects., Please rate this question:, , Discuss and give feedback, , Next question, , Trachea, Trachea, , Location, , C6 vertebra to the upper border of T5 vertebra (bifurcation), , Arterial and venous supply, , Inferior thyroid arteries and the thyroid venous plexus., , Nerve, , Branches of vagus, sympathetic and the recurrent nerves, , Relations in the neck, , Anterior(Superior to, inferior), , , , , , Isthmus of the thyroid gland, Inferior thyroid veins, Arteria thyroidea ima (when that vessel exists)
Page 1639 :
, , , , , Posterior, Laterally, , Sternothyroid, Sternohyoid, Cervical fascia, Anastomosing branches between the anterior jugular, veins, , Oesophagus., , , , , , Common carotid arteries, Right and left lobes of the thyroid gland, Inferior thyroid arteries, Recurrent laryngeal nerves, , Relations in the thorax, Anterior, , , Manubrium, the remains of the thymus, the aortic arch, left common carotid arteries, and the, deep cardiac plexus, , Lateral, , , In the superior mediastinum, on the right side is the pleura and right vagus; on its left side, are the left recurrent nerve, the aortic arch, and the left common carotid and subclavian, arteries., Next question
Page 1640 :
Question 242 of 560, , A 23 year old man is injured during a game of rugby. He suffers a fracture of the distal third of his, clavicle, it is a compound fracture and there is evidence of arterial haemorrhage. Which of the, following vessels is most likely to be encountered first during subsequent surgical exploration?, , Posterior circumflex humeral artery, , Axillary artery, , Thoracoacromial artery, , Sub scapular artery, , Lateral thoracic artery, , Similar theme in September 2011 Exam, The thoracoacromial artery arises from the second part of the axillary artery. It is a short, wide trunk,, which pierces the clavipectoral fascia, and ends, deep to pectoralis major by dividing into four, branches., Please rate this question:, , Discuss and give feedback, , Next question, , Thoracoacromial artery, The thoracoacromial artery (acromiothoracic artery; thoracic axis) is a short trunk, which arises from, the forepart of the axillary artery, its origin being generally overlapped by the upper edge of the, Pectoralis minor., Projecting forward to the upper border of the Pectoralis minor, it pierces the coracoclavicular fascia
Page 1641 :
and divides into four branches: pectoral, acromial, clavicular, and deltoid., , Branch, , Description, , Pectoral, branch, , Descends between the two Pectoral muscles, and is distributed to them and to the breast,, anastomosing with the intercostal branches of the internal thoracic artery and with the, lateral thoracic., , Acromial, branch, , Runs laterally over the coracoid process and under the Deltoid, to which it gives branches; it, then pierces that muscle and ends on the acromion in an arterial network formed by, branches from the suprascapular, thoracoacromial, and posterior humeral circumflex, arteries., , Clavicular, branch, , Runs upwards and medially to the sternoclavicular joint, supplying this articulation, and the, Subclavius., , Deltoid, branch, , Arising with the acromial, it crosses over the Pectoralis minor and passes in the same, groove as the cephalic vein, between the Pectoralis major and Deltoid, and gives branches, to both muscles., Next question
Page 1643 :
femoral triangle, lateral to the femoral artery and vein., , Image sourced from Wikipedia, , Mnemonic for femoral nerve supply, (don't) M I S V Q Scan for PE, M edial cutaneous nerve of the thigh, I ntermediate cutaneous nerve of the thigh, S aphenous nerve, V astus, Q uadriceps femoris, S artorius, PE ectineus, , Next question
Page 1644 :
Question 244 of 560, Where is the vomiting centre located?, , Medulla oblongata, , Substantia nigra, , Antrum of stomach, , Pons, , Midbrain, ABC's of Non- GI causes of vomiting, Acute renal failure, Brain (Increased ICP), Cardiac (Inferior MI), DKA, Ears (labyrinthitis), Foreign substances (Tylenol, theo, etc), Glaucoma, Hyperemesis Gravidarum, Infections (pyelonephritis, meningitis), Please rate this question:, , Discuss and give feedback, , Next question, , Vomiting, Reflex oral expulsion of gastric (and sometimes intestinal) contents - reverse peristalsis and, abdominal contraction, The vomiting centre is in part of the medulla oblongata and is triggered by receptors in several, locations:
Page 1645 :
, , , , , Labyrinthine receptors of ear (motion sickness), Over distention receptors of duodenum and stomach, Trigger zone of CNS - many drugs (e.g., opiates) act here, Touch receptors in throat, Next question
Page 1646 :
Question 245 of 560, Which of the following nerves conveys sensory information from the laryngeal mucosa?, , Glossopharyngeal, , Laryngeal branches of the vagus, , Ansa cervicalis, , Laryngeal branches of the trigeminal, , None of the above, , The laryngeal branches of the vagus supply sensory information from the larynx., Please rate this question:, , Discuss and give feedback, , Next question, , Larynx, The larynx lies in the anterior part of the neck at the levels of C3 to C6 vertebral bodies. The, laryngeal skeleton consists of a number of cartilagenous segments. Three of these are paired;, arytenoid, corniculate and cuneiform. Three are single; thyroid, cricoid and epiglottic. The cricoid, cartilage forms a complete ring (the only one to do so)., The laryngeal cavity extends from the laryngeal inlet to the level of the inferior border of the cricoid, cartilage., Divisions of the laryngeal cavity, , Laryngeal vestibule, , Superior to the vestibular folds, , Laryngeal ventricle, , Lies between vestibular folds and superior to the vocal cords, , Infraglottic cavity, , Extends from vocal cords to inferior border of the cricoid cartilage
Page 1647 :
The vocal folds (true vocal cords) control sound production. The apex of each fold projects medially, into the laryngeal cavity. Each vocal fold includes:, , , , Vocal ligament, Vocalis muscle (most medial part of thyroarytenoid muscle), , The glottis is composed of the vocal folds, processes and rima glottidis. The rima glottidis is the, narrowest potential site within the larynx, as the vocal cords may be completely opposed, forming a, complete barrier., Muscles of the larynx, , Muscle, , Origin, , Insertion, , Innervation, , Action, , Posterior, cricoarytenoid, , Posterior aspect, of lamina of, cricoid, , Muscular process, of arytenoid, , Recurrent, Laryngeal, , Abducts vocal fold, , Lateral, cricoarytenoid, , Arch of cricoid, , Muscular process, of arytenoid, , Recurrent, laryngeal, , Adducts vocal fold, , Thyroarytenoid, , Posterior aspect, of thyroid, cartilage, , Muscular process, of arytenoid, , Recurrent, laryngeal, , Relaxes vocal fold, , Transverse and, oblique, arytenoids, , Arytenoid, cartilage, , Contralateral, arytenoid, , Recurrent, laryngeal, , Closure of, intercartilagenous, part of the rima, glottidis, , Vocalis, , Depression, between lamina, of thyroid, cartilage, , Vocal ligament, and vocal process, of arytenoid, cartilage, , Recurrent, laryngeal, , Relaxes posterior, vocal ligament, tenses, anterior part, , Cricothyroid, , Anterolateral, part of cricoid, , Inferior margin, and horn of, thyroid cartilage, , External, laryngeal, , Tenses vocal fold
Page 1648 :
Blood supply, Arterial supply is via the laryngeal arteries, branches of the superior and inferior thyroid arteries. The, superior laryngeal artery is closely related to the internal laryngeal nerve. The inferior laryngeal, artery is related to the inferior laryngeal nerve. Venous drainage is via superior and inferior laryngeal, veins, the former draining into the superior thyroid vein and the latter draining into the middle thyroid, vein, or thyroid venous plexus., Lymphatic drainage, The vocal cords have no lymphatic drainage and this site acts as a lymphatic watershed., , Supraglottic part, , Upper deep cervical nodes, , Subglottic part, , Prelaryngeal and pretracheal nodes and inferior deep cervical nodes, , The aryepiglottic fold and vestibular folds have a dense plexus of lymphatics associated with them, and malignancies at these sites have a greater propensity for nodal metastasis., , Topography of the larynx, , Image sourced from Wikipedia, , Next question
Page 1649 :
Question 246 of 560, Which of the following nerves passes through the greater sciatic foramen and innervates the, perineum?, , Pudendal, , Sciatic, , Superior gluteal, , Inferior gluteal, , Posterior cutaneous nerve of the thigh, 3 divisions of the pudendal nerve:, , , , , Rectal nerve, Perineal nerve, Dorsal nerve of penis/ clitoris, , All these pass through the greater sciatic foramen., The pudendal nerve innervates the perineum. It passes between piriformis and coccygeus medial to, the sciatic nerve., Please rate this question:, , Discuss and give feedback, , Next question, , Gluteal region, Gluteal muscles, , , , , , Gluteus maximus: inserts to gluteal tuberosity of the femur and iliotibial tract, Gluteus medius: attach to lateral greater trochanter, Gluteus minimis: attach to anterior greater trochanter, All extend and abduct the hip
Page 1651 :
Question 247 of 560, Which of the following is true in relation to the sartorius muscle?, , Innervated by the deep branch of the femoral nerve, , Inserts at the fibula, , It is the shortest muscle in the body, , Forms the Pes anserinus with Gracilis and semitendinous muscle, , Causes extension of the knee, , It is innervated by the superficial branch of the femoral nerve. It is a component of the pes anserinus., Please rate this question:, , Discuss and give feedback, , Next question, , Sartorius, , , , Longest strap muscle in the body, Most superficial muscle in the anterior compartment of the thigh, , Origin, , Anterior superior iliac spine, , Insertion, , Medial surface of the of the body of the tibia (upper part). It inserts anterior to, gracilis and semitendinosus, , Nerve Supply, , Femoral nerve (L2,3), , Action, , , , , Flexor of the hip and knee, slight abducts the thigh and rotates it laterally, It assists with medial rotation of the tibia on the femur. For example it
Page 1652 :
would play a pivotal role in placing the right heel onto the left knee ( and, vice versa), , Important, relations, , The middle third of this muscle, and its strong underlying fascia forms the roof of, the adductor canal , in which lie the femoral vessels, the saphenous nerve and the, nerve to vastus medialis., Next question
Page 1653 :
Question 248-250 of 560, Theme: Nerve lesions, , A., B., C., D., E., F., G., , Sciatic nerve, Peroneal nerve, Tibial Nerve, Obturator nerve, Ilioinguinal nerve, Femoral nerve, None of the above, , Please select the most likely nerve injury for the scenario given. Each option may be used once,, more than once or not at all, , 248., , A 56 year old man undergoes a low anterior resection with legs in the Lloyd-Davies, position. Post operatively he complains of foot drop., You answered Sciatic nerve, The correct answer is Peroneal nerve, Positioning legs in Lloyd- Davies stirrups can carry the risk of peroneal nerve, neuropraxia if not done carefully., , 249., , A 23 year old man complains of severe groin pain several weeks after a difficult inguinal, hernia repair., You answered Sciatic nerve, The correct answer is Ilioinguinal nerve, The ilioinguinal nerve may have been entrapped in the mesh causing a neuroma., , 250., , A 72 year old man develops a foot drop after a revision total hip replacement., Sciatic nerve, This may be done by a number of approaches, in this scenario a posterior approach is the, most likely culprit., , Please rate this question:
Page 1656 :
Question 251 of 560, A 38 year old man falls onto an outstretched hand. Following the accident he is examined in the, emergency department. On palpating his anatomical snuffbox there is tenderness noted in the base., What is the most likely injury in this scenario?, , Rupture of the tendon of flexor pollicis, , Scaphoid fracture, , Distal radius fracture, , Rupture of flexor carpi ulnaris tendon, , None of the above, , A fall onto an outstretched hand is a common mechanism of injury for a scaphoid fracture. This, should be suspected clinically if there is tenderness in the base of the anatomical snuffbox. A tendon, rupture would not result in bony tenderness., Please rate this question:, , Discuss and give feedback, , Next question, , Scaphoid bone, The scaphoid has a concave articular surface for the head of the capitate and at the edge of this is a, crescentic surface for the corresponding area on the lunate., Proximally, it has a wide convex articular surface with the radius. It has a distally sited tubercle that, can be palpated. The remaining articular surface is to the lateral side of the tubercle. It faces laterally, and is associated with the trapezium and trapezoid bones., The narrow strip between the radial and trapezial surfaces and the tubercle gives rise to the radial, collateral carpal ligament. The tubercle receives part of the flexor retinaculum. This area is the only, part of the scaphoid that is available for the entry of blood vessels. It is commonly fractured and, avascular necrosis may result., Scaphoid bone
Page 1657 :
Image sourced from Wikipedia, , Next question
Page 1658 :
Question 252 of 560, A 25 year old man sustains a severe middle cranial fossa basal skull fracture. Once he has, recovered it is noticed that he has impaired tear secretion. This is most likely to be the result of, damage to which of the following?, , Stellate ganglion, , Ciliary ganglion, , Otic ganglion, , Trigeminal nerve, , Greater petrosal nerve, , The greater petrosal nerve may be injured and carries fibres for lacrimation (see below)., Please rate this question:, , Discuss and give feedback, , Next question, , Lacrimal system, Lacrimal gland, Consists of an orbital part and palpebral part. They are continuous posterolaterally around the, concave lateral edge of the levator palpebrae superioris muscle., The ducts of the lacrimal gland open into the superior fornix. Those from the orbital part penetrate, the aponeurosis of levator palpebrae superioris to join those from the palpebral part. Therefore, excision of the palpebral part is functionally similar to excision of the entire gland., Blood supply, Lacrimal branch of the opthalmic artery. Venous drainage is to the superior opthalmic vein., Innervation, The gland is innervated by the secretomotor parasympathetic fibres from the pterygopalatine, ganglion which in turn may reach the gland via the zygomatic or lacrimal branches of the maxillary, nerve or pass directly to the gland. The preganglionic fibres travel to the ganglion in the greater, petrosal nerve (a branch of the facial nerve at the geniculate ganglion)., Nasolacrimal duct
Page 1659 :
Descends from the lacrimal sac to open anteriorly in the inferior meatus of the nose., Lacrimation reflex, Occurs in response to conjunctival irritation (or emotional events). The conjunctiva will send signals, via the opthalmic nerve. These then pass to the superior salivary centre. The efferent signals pass, via the greater petrosal nerve (parasympathetic preganglionic fibres) and the deep petrosal nerve, which carries the post ganglionic sympathetic fibres. The parasympathetic fibres will relay in the, pterygopalatine ganglion, the sympathetic fibres do not synapse. They in turn will relay to the, lacrimal apparatus., Next question
Page 1660 :
Question 253 of 560, , Which of the following structures passes through the quadrangular space near the humeral head?, , Axillary artery, , Radial nerve, , Axillary nerve, , Median nerve, , Transverse scapular artery, , The quadrangular space is bordered by the humerus laterally, subscapularis superiorly, teres major, inferiorly and the long head of triceps medially. It lies lateral to the triangular space. It transmits the, axillary nerve and posterior circumflex humeral artery.
Page 1661 :
Image sourced from Wikipedia, , Please rate this question:, , Discuss and give feedback, , Next question, , Shoulder joint, , , , , Shallow synovial ball and socket type of joint., It is an inherently unstable joint, but is capable to a wide range of movement., Stability is provided by muscles of the rotator cuff that pass from the scapula to insert in the, greater tuberosity (all except sub scapularis-lesser tuberosity)., , Glenoid labrum, , , , , , Fibrocartilaginous rim attached to the free edge of the glenoid cavity, Tendon of the long head of biceps arises from within the joint from the supraglenoid tubercle,, and is fused at this point to the labrum., The long head of triceps attaches to the infraglenoid tubercle, , Fibrous capsule, , , , , , , , Attaches to the scapula external to the glenoid labrum and to the labrum itself (posterosuperiorly), Attaches to the humerus at the level of the anatomical neck superiorly and the surgical neck, inferiorly, Anteriorly the capsule is in contact with the tendon of subscapularis, superiorly with the, supraspinatus tendon, and posteriorly with the tendons of infraspinatus and teres minor. All, these blend with the capsule towards their insertion., Two defects in the fibrous capsule; superiorly for the tendon of biceps. Anteriorly there is a, defect beneath the subscapularis tendon., The inferior extension of the capsule is closely related to the axillary nerve at the surgical, neck and this nerve is at risk in anteroinferior dislocations. It also means that proximally sited, osteomyelitis may progress to septic arthritis., , Movements and muscles
Page 1663 :
Inferior, , Axillary nerve, Circumflex humeral vessels, Next question
Page 1664 :
Question 254 of 560, , Which of the following pairings of foramina and their contents is not correct?, , Superior orbital fissure and the oculomotor nerve, , Foramina rotundum and the maxillary nerve, , Jugular foramen and the hypoglossal nerve, , Foramina spinosum and the middle meningeal artery, , Carotid canal and the internal carotid artery, , The hypoglossal nerve passes through the hypoglossal canal., Please rate this question:, , Discuss and give feedback, , Next question, , Foramina of the base of the skull, Foramen, , Location, , Contents, , Foramen ovale, , Sphenoid, bone, , Otic ganglion, V3 (Mandibular nerve:3rd branch of, trigeminal), Accessory meningeal artery, Lesser petrosal nerve
Page 1666 :
*= In life the foramen lacerum is occluded by a cartilagenous plug. The ICA initially passes into the, carotid canal which ascends superomedially to enter the cranial cavity through the foramen lacerum., Base of skull anatomical overview, , Image sourced from Wikipedia, , Next question
Page 1667 :
Question 255 of 560, A 55 year old man with carcinoma of the larynx is undergoing a difficult laryngectomy. The surgeons, divide the thyrocervical trunk, from which of the following vessels does this structure most commonly, originate?, , Subclavian artery, , Common carotid artery, , Vertebral artery, , External carotid artery, , Internal carotid artery, , The thyrocervical trunk is a branch of the subclavian artery. It arises from the first part between the, subclavian artery and the inner border of scalenus anterior. It branches off the subclavian distal to, the vertebral artery., Please rate this question:, , Discuss and give feedback, , Next question, , Root of the neck, Thoracic Outlet, , , , , , , , Where the subclavian artery and vein and the brachial plexus exit the thorax and enter the, arm., They pass over the 1st rib and under the clavicle., The subclavian vein is the most anterior structure and is immediately anterior to scalenus, anterior and its attachment to the first rib., Scalenus anterior has 2 parts, the subclavian artery leaves the thorax by passing over the, first rib and between these 2 portions of the muscle., At the level of the first rib, the lower cervical nerve roots combine to form the 3 trunks of the, brachial plexus. The lowest trunk is formed by the union of C8 and T1, and this trunk lies, directly posterior to the artery and is in contact with the superior surface of the first rib.
Page 1668 :
Thoracic outlet obstruction causes neurovascular compromise., Next question
Page 1669 :
Question 256 of 560, The following structures are closely related to the brachiocephalic artery except:, , Trachea posteriorly, , Right brachiocephalic vein, , Inferior thyroid vein, , Right recurrent laryngeal nerve, , None of the above, , There is no brachiocephalic artery on the left, however the left brachiocephalic vein lies anteriorly to, the roots of all the 3 great arteries (including the brachiocephalic artery). The right recurrent, laryngeal nerve has no relation to the brachiocephalic artery., Please rate this question:, , Discuss and give feedback, , Next question, , Brachiocephalic artery, The brachiocephalic artery is the largest branch of the aortic arch. From its aortic origin it ascends, superiorly, it initially lies anterior to the trachea and then on its right hand side. It branches into the, common carotid and right subclavian arteries at the level of the sternoclavicular joint., Path, Origin- apex of the midline of the aortic arch, Passes superiorly and posteriorly to the right, Divides into the right subclavian and right common carotid artery, Relations, , Anterior, , , , , , , Sternohyoid, Sternothyroid, Thymic remnants, Left brachiocephalic vein
Page 1670 :
, , Right inferior thyroid veins, , Posterior, , , , , Trachea, Right pleura, , Right lateral, , , , , Right brachiocephalic vein, Superior part of SVC, , Left lateral, , , , , , , Thymic remnants, Origin of left common carotid, Inferior thyroid veins, Trachea (higher level), , Branches, Normally none but may have the thyroidea ima artery, , Image sourced from Wikipedia, , Next question
Page 1671 :
Question 257 of 560, Which of the following structures separates the ulnar artery from the median nerve?, , Brachioradialis, , Pronator teres, , Tendon of biceps brachii, , Flexor carpi ulnaris, , Brachialis, , It lies deep to pronator teres and this separates it from the median nerve., Please rate this question:, , Discuss and give feedback, , Next question, , Ulnar artery, Path, , , , Starts: middle of antecubital fossa, Passes obliquely downward, reaching the ulnar side of the forearm at a point about midway, between the elbow and the wrist. It follows the ulnar border to the wrist, crossing over the, flexor retinaculum. It then divides into the superficial and deep volar arches., , Relations, Deep to- Pronator teres, Flexor carpi radialis, Palmaris longus, Lies on- Brachialis and Flexor digitorum profundus, Superficial to the flexor retinaculum at the wrist, The median nerve is in relation with the medial side of the artery for about 2.5 cm. And then crosses, the vessel, being separated from it by the ulnar head of the Pronator teres, The ulnar nerve lies medially to the lower two-thirds of the artery
Page 1672 :
Branch, , , Anterior interosseous artery, , Image sourced from Wikipedia, , Next question
Page 1673 :
Question 258 of 560, Which muscle is supplied by the superficial peroneal nerve?, , Peroneus tertius, , Sartorius, , Adductor magnus, , Peroneus brevis, , Gracilis, , Please rate this question:, , Discuss and give feedback, , Next question, , Superficial peroneal nerve, Supplies, , , , Lateral compartment of leg: peroneus longus, peroneus brevis (action: eversion and plantar, flexion), Sensation over dorsum of the foot (except the first web space, which is innervated by the, deep peroneal nerve), , Path, , , , , Passes between peroneus longus and peroneus brevis along the length of the proximal one, third of the fibula, 10-12 cm above the tip of the lateral malleolus, the superficial peroneal nerve pierces the, fascia, 6-7 cm distal to the fibula, the superficial peroneal nerve bifurcates into intermediate and, medial dorsal cutaneous nerves, Next question
Page 1674 :
Question 259 of 560, A 32 year old motorcyclist is involved in a road traffic accident. His humerus is fractured and, severely displaced. At the time of surgical repair the surgeon notes that the radial nerve has been, injured. Which of the following muscles is least likely to be affected by an injury at this site?, , Extensor carpi radialis brevis, , Brachioradialis, , Abductor pollicis longus, , Extensor pollicis brevis, , None of the above, Muscles supplied by the radial nerve, BEST, Brachioradialis, Extensors, Supinator, Triceps, The radial nerve supplies the extensor muscles, abductor pollicis longus and extensor pollicis brevis, (the latter two being innervated by the posterior interosseous branch of the radial nerve)., Please rate this question:, , Discuss and give feedback, , Next question, , Radial nerve, Continuation of posterior cord of the brachial plexus (root values C5 to T1), Path, , , , In the axilla: lies posterior to the axillary artery on subscapularis, latissimus dorsi and teres, major., Enters the arm between the brachial artery and the long head of triceps (medial to humerus).
Page 1676 :
hand is supplied by the radial nerve (this does not apply to the little finger and, part of the ring finger), , Muscular innervation and effect of denervation, , Anatomical, location, , Muscle affected, , Effect of paralysis, , Shoulder, , Long head of triceps, , Minor effects on shoulder stability in abduction, , Arm, , Triceps, , Loss of elbow extension, , Forearm, , Supinator, Brachioradialis, Extensor carpi radialis, longus and brevis, , Weakening of supination of prone hand and, elbow flexion in mid prone position, , The cutaneous sensation of the upper limb- illustrating the contribution of the radial nerve, , Image sourced from Wikipedia
Page 1677 :
Question 260 of 560, A man develops an infection in his external auditory meatus. The infection is extremely painful., Which of the following nerves conveys sensation from this region?, , Occipital branch of the trigeminal nerve, , Vestibulocochlear nerve, , Facial nerve, , Auriculotemporal nerve, , Maxillary branch of the trigeminal nerve, Tensor tympania and stapedius are the only two muscles of the middle ear. Contraction of tensor, tympani will tend to dampen the vibrations produced by loud sounds, it is innervated by a branch of, the trigeminal nerve. The stapedius dampens movements of the ossicles in response to loud sounds, and is innervated by a branch of the facial nerve., The auriculotemporal nerve, which is derived from the mandibular branch of the trigeminal nerve, supplies this area., Please rate this question:, , Discuss and give feedback, , Next question, , Ear- anatomy, The ear is composed of three anatomically distinct regions., External ear, Auricle is composed of elastic cartilage covered by skin. The lobule has no cartilage and contains fat, and fibrous tissue., External auditory meatus is approximately 2.5cm long., Lateral third of the external auditory meatus is cartilaginous and the medial two thirds is bony., The region is innervated by the greater auricular nerve. The auriculotemporal branch of the, trigeminal nerve supplies most the of external auditory meatus and the lateral surface of the auricle.
Page 1678 :
Middle ear, Space between the tympanic membrane and cochlea. The aditus leads to the mastoid air cells is the, route through which middle ear infections may cause mastoiditis. Anteriorly the eustacian tube, connects the middle ear to the naso pharynx., The tympanic membrane consists of:, , , , , Outer layer of stratified squamous epithelium., Middle layer of fibrous tissue., Inner layer of mucous membrane continuous with the middle ear., , The tympanic membrane is approximately 1cm in diameter., The chorda tympani nerve passes on the medial side of the pars flaccida., The middle ear is innervated by the glossopharyngeal nerve and pain may radiate to the middle ear, following tonsillectomy., Ossicles, Malleus attaches to the tympanic membrane (the Umbo)., Malleus articulates with the incus (synovial joint)., Incus attaches to stapes (another synovial joint)., Internal ear, Cochlea, semi circular canals and vestibule, Organ of corti is the sense organ of hearing and is located on the inside of the cochlear duct on the, basilar membrane., Vestibule accommodates the utricule and the saccule. These structures contain endolymph and are, surrounded by perilymph within the vestibule., The semicircular canals lie at various angles to the petrous temporal bone. All share a common, opening into the vestibule., Next question
Page 1681 :
Image sourced from Wikipedia, , Fascia and compartments of the palm, The fascia of the palm is continuous with the antebrachial fascia and the fascia of the dorsum of the, hand. The palmar fascia is thin over the thenar and hypothenar eminences. In contrast the palmar, fascia is relatively thick. The palmar aponeurosis covers the soft tissues and overlies the flexor, tendons. The apex of the palmar aponeurosis is continuous with the flexor retinaculum and the, palmaris longus tendon. Distally, it forms four longitudinal digital bands that attach to the bases of, the proximal phalanges, blending with the fibrous digital sheaths., A medial fibrous septum extends deeply from the medial border of the palmar aponeurosis to the 5th, metacarpal. Lying medial to this are the hypothenar muscles. In a similar fashion, a lateral fibrous, septum extends deeply from the lateral border of the palmar aponeurosis to the 3rd metacarpal. The, thenar compartment lies lateral to this area., Lying between the thenar and hypothenar compartments is the central compartment. It contains the, flexor tendons and their sheaths, the lumbricals, the superficial palmar arterial arch and the digital, vessels and nerves., The deepest muscular plane is the adductor compartment, which contains adductor pollicis., Short muscles of the hand, These comprise the lumbricals and interossei. The four slender lumbrical muscles flex the fingers at, the metacarpophalangeal joints and extend the interphalangeal joint. The four dorsal interossei are, located between the metacarpals and the four palmar interossei lie on the palmar surface of the, metacarpals in the interosseous compartment of the hand., Long flexor tendons and sheaths in the hand, The tendons of FDS and FDP enter the common flexor sheath deep to the flexor retinaculum. The, tendons enter the central compartment of the hand and fan out to their respective digital synovial, sheaths. Near the base of the proximal phalanx, the tendon of FDS splits to permit the passage of, FDP. The FDP tendons are attached to the margins of the anterior aspect of the base of the distal, phalanx., The fibrous digital sheaths contain the flexor tendons and their synovial sheaths. These extend from, the heads of the metacarpals to the base of the distal phalanges., Next question
Page 1682 :
Question 262 of 560, Which of the following structures separates the posterior cruciate ligament from the popliteal artery?, , Oblique popliteal ligament, , Transverse ligament, , Popliteus tendon, , Biceps femoris, , Semitendinosus, , The posterior cruciate ligament is separated from the popliteal vessels at its origin by the oblique, popliteal ligament. The transverse ligament is located anteriorly., Please rate this question:, , Discuss and give feedback, , Next question, , Knee joint, The knee joint is a synovial joint, the largest and most complicated. It consists of two condylar joints, between the femur and tibia and a sellar joint between the patella and the femur. The tibiofemoral, articular surfaces are incongruent, however, this is improved by the presence of the menisci. The, degree of congruence is related to the anatomical position of the knee joint and is greatest in full, extension., Knee joint compartments, , Tibiofemoral, , , , Patellofemoral, , , , , Comprised of the patella/femur joint, lateral and medial compartments, (between femur condyles and tibia), Synovial membrane and cruciate ligaments partially separate the medial, and lateral compartments, , Ligamentum patellae, Actions: provides joint stability in full extension
Page 1683 :
Fibrous capsule, The capsule of the knee joint is a complex, composite structure with contributions from adjacent, tendons., Anterior, fibres, , The capsule does not pass proximal to the patella. It blends with the tendinous, expansions of vastus medialis and lateralis, , Posterior, fibres, , These fibres are vertical and run from the posterior surface of the femoral condyles, to the posterior aspect of the tibial condyle, , Medial fibres, , Attach to the femoral and tibial condyles beyond their articular margins, blending, with the tibial collateral ligament, , Lateral, fibres, , Attach to the femur superior to popliteus, pass over its tendon to head of fibula and, tibial condyle, , Bursae, , Anterior, , Laterally, , Medially, , Posterior, , , , , , Subcutaneous prepatellar bursa; between patella and skin, Deep infrapatellar bursa; between tibia and patellar ligament, Subcutaneous infrapatellar bursa; between distal tibial tuberosity and skin, , , , , , Bursa between lateral head of gastrocnemius and joint capsule, Bursa between fibular collateral ligament and tendon of biceps femoris, Bursa between fibular collateral ligament and tendon of popliteus, , , , , Bursa between medial head of gastrocnemius and the fibrous capsule, Bursa between tibial collateral ligament and tendons of sartorius, gracilis and, semitendinosus, Bursa between the tendon of semimembranosus and medial tibial condyle and, medial head of gastrocnemius, , , , Highly variable and inconsistent, , Ligaments, , Medial collateral, ligament, , Medial epicondyle femur to medial tibial condyle: valgus stability, , Lateral collateral, ligament, , Lateral epicondyle femur to fibula head: varus stability, , Anterior cruciate, , Anterior tibia to lateral intercondylar notch femur: prevents tibia sliding
Page 1684 :
ligament, , anteriorly, , Posterior cruciate, ligament, , Posterior tibia to medial intercondylar notch femur: prevents tibia, sliding posteriorly, , Patellar ligament, , Central band of the tendon of quadriceps femoris, extends from patella, to tibial tuberosity, , Image sourced from Wikipedia
Page 1685 :
Image sourced from Wikipedia, , © Image provided by the University of Sheffield, , Menisci, Medial and lateral menisci compensate for the incongruence of the femoral and tibial condyles., Composed of fibrous tissue., Medial meniscus is attached to the tibial collateral ligament., Lateral meniscus is attached to the loose fibres at the lateral edge of the joint and is separate from, the fibular collateral ligament. The lateral meniscus is crossed by the popliteus tendon.
Page 1686 :
Nerve supply, The knee joint is supplied by the femoral, tibial and common peroneal divisions of the sciatic and by, a branch from the obturator nerve. Hip pathology pain may be referred to the knee., Blood supply, Genicular branches of the femoral artery, popliteal and anterior tibial arteries all supply the knee, joint., Next question
Page 1687 :
Question 263 of 560, How many compartments are there in the lower leg?, , 2, , 1, , 3, , 5, , 4, , The posterior compartment of the lower leg has both superficial and deep posterior layers, together, with the anterior and lateral compartments this allows for four compartments. Decompression of the, deep posterior compartment during fasciotomy may be overlooked with significant sequelae., Please rate this question:, , Discuss and give feedback, , Next question, , Fascial compartments of the leg, Compartments of the thigh, Formed by septae passing from the femur to the fascia lata., , Compartment, , Nerve, , Muscles, , Blood supply, , Anterior compartment, , Femoral, , , , , , , Iliacus, Tensor fasciae latae, Sartorius, Quadriceps femoris, , Femoral artery, , Medial compartment, , Obturator, , , , Adductor, longus/magnus/brevis, Gracilis, , Profunda femoris artery, and obturator artery, ,
Page 1689 :
Question 264 of 560, Which structure is least likely to be found at the level of the sternal angle?, , Left brachiocephalic vein, , Intervertebral discs T4-T5, , Start of aortic arch, , 2nd pair of costal cartilages, , Bifurcation of the trachea into left and right bronchi, , The left brachiocephalic vein lies posterior to the manubrium, at the level of its upper border. The, sternal angle refers to the transition between manubrium and sternum and therefore will not include, the left brachiocephalic vein., Please rate this question:, , Discuss and give feedback, , Next question, , Sternal angle, Anatomical structures at the level of the manubrium and upper sternum, , Upper part of the manubrium, , , , , , , Left brachiocephalic vein, Brachiocephalic artery, Left common carotid, Left subclavian artery, , Lower part of the manubrium/, manubrio-sternal angle, , , , , Costal cartilages of the 2nd ribs, Transition point between superior and inferior, mediastinum, Arch of the aorta, Tracheal bifurcation, Union of the azygos vein and superior vena, cava, , , ,
Page 1690 :
, , The thoracic duct crosses to the midline, Next question
Page 1691 :
Question 265 of 560, , A 53 year old man is undergoing a left hemicolectomy for carcinoma of the descending colon. From, which embryological structure is this region of the gastrointestinal tract derived?, , Vitellino-intestinal duct, , Hind gut, , Mid gut, , Fore gut, , Woolffian duct, , The left colon is embryologically part of the hind gut. Which accounts for its separate blood supply, via the IMA., Please rate this question:, , Discuss and give feedback, , Next question, , Colon anatomy, The colon commences with the caecum. This represents the most dilated segment of the human, colon and its base (which is intraperitoneal) is marked by the convergence of teniae coli. At this point, is located the vermiform appendix. The colon continues as the ascending colon, the posterior aspect, of which is retroperitoneal. The line of demarcation between the intra and retro peritoneal right colon, is visible as a white line, in the living, and forms the line of incision for colonic resections., The ascending colon becomes the transverse colon after passing the hepatic flexure. At this located, the colon becomes wholly intra peritoneal once again. The superior aspect of the transverse colon is
Page 1692 :
the point of attachment of the transverse colon to the greater omentum. This is an important, anatomical site since division of these attachments permits entry into the lesser sac. Separation of, the greater omentum from the transverse colon is a routine operative step in both gastric and colonic, resections., At the left side of the abdomen the transverse colon passes to the left upper quadrant and makes an, oblique inferior turn at the splenic flexure. Following this, the posterior aspect becomes, retroperitoneal once again., At the level of approximately L4 the descending colon becomes wholly intraperitoneal and becomes, the sigmoid colon. Whilst the sigmoid is wholly intraperitoneal there are usually attachments laterally, between the sigmoid and the lateral pelvic sidewall. These small congenital adhesions are not formal, anatomical attachments but frequently require division during surgical resections., At its distal end the sigmoid passes to the midline and at the region around the sacral promontary it, becomes the upper rectum. This transition is visible macroscopically as the point where the teniae, fuse. More distally the rectum passes through the peritoneum at the region of the peritoneal, reflection and becomes extraperitoneal., Arterial supply, Superior mesenteric artery and inferior mesenteric artery: linked by the marginal artery., Ascending colon: ileocolic and right colic arteries, Transverse colon: middle colic artery, Descending and sigmoid colon: inferior mesenteric artery, Venous drainage, From regional veins (that accompany arteries) to superior and inferior mesenteric vein, Lymphatic drainage, Initially along nodal chains that accompany supplying arteries, then para-aortic nodes., Embryology, Midgut- Second part of duodenum to 2/3 transverse colon, Hindgut- Distal 1/3 transverse colon to anus, Peritoneal location, The right and left colon are part intraperitoneal and part extraperitoneal. The sigmoid and transverse, colon are generally wholly intraperitoneal. This has implications for the sequelae of perforations,, which will tend to result in generalised peritonitis in the wholly intra peritoneal segments., Colonic relations, , Region of colon, , Relation
Page 1693 :
Region of colon, , Relation, , Caecum/ right colon, , Right ureter, gonadal vessels, , Hepatic flexure, , Gallbladder (medially), , Splenic flexure, , Spleen and tail of pancreas, , Distal sigmoid/ upper rectum, , Left ureter, , Rectum, , Ureters, autonomic nerves, seminal vesicles, prostate, urethra (distally), Next question
Page 1694 :
Question 266 of 560, , What is the most useful test to clinically distinguish between an upper and lower motor neurone, lesion of the facial nerve?, , Blow cheeks out, , Loss of chin reflex, , Close eye, , Raise eyebrow, , Open mouth against resistance, Upper motor neurone lesions of the facial nerve- Paralysis of the lower half of face., Lower motor neurone lesion- Paralysis of the entire ipsilateral face., , Theme from April 2012 Exam, Please rate this question:, , Discuss and give feedback, , Next question, , Upper Vs Lower motor neurone lesions - Facial nerve, The nucleus of the facial nerve is located in the caudal aspect of the ventrolateral pontine, tegmentum. Its axons exit the ventral pons medial to the spinal trigeminal nucleus., Any lesion occurring within or affecting the corticobulbar tract is known as an upper motor neuron, lesion. Any lesion affecting the individual branches (temporal, zygomatic, buccal, mandibular and, cervical) is known as a lower motor neuron lesion.
Page 1695 :
Branches of the facial nerve leaving the facial motor nucleus (FMN) for the muscles do so via both, left and right posterior (dorsal) and anterior (ventral) routes. In other words, this means lower motor, neurons of the facial nerve can leave either from the left anterior, left posterior, right anterior or right, posterior facial motor nucleus. The temporal branch travels out from the left and right posterior, components. The inferior four branches do so via the left and right anterior components. The left and, right branches supply their respective sides of the face (ipsilateral innervation). Accordingly, the, posterior components receive motor input from both hemispheres of the cerebral cortex (bilaterally),, whereas the anterior components receive strictly contra-lateral input. This means that the temporal, branch of the facial nerve receives motor input from both hemispheres of the cerebral cortex, whereas the zygomatic, buccal, mandibular and cervical branches receive information from only, contralateral hemispheres., Now, because the anterior FMN receives only contralateral cortical input whereas the posterior, receives that which is bilateral, a corticobulbar lesion (UMN lesion) occurring in the left hemisphere, would eliminate motor input to the right anterior FMN component, thus removing signaling to the, inferior four facial nerve branches, thereby paralyzing the right mid- and lower-face. The posterior, component, however, although now only receiving input from the right hemisphere, is still able to, allow the temporal branch to sufficiently innervate the entire forehead. This means that the forehead, will not be paralyzed., The same mechanism applies for an upper motor neuron lesion in the right hemisphere. The left, anterior FMN component no longer receives cortical motor input due to its strict contralateral, innervation, whereas the posterior component is still sufficiently supplied by the left hemisphere. The, result is paralysis of the left mid- and lower-face with an unaffected forehead., On the other hand, a lower motor neuron lesion is a bit different., A lesion on either the left or right side would affect both the anterior and posterior routes on that side, because of their close physical proximity to one another. So, a lesion on the left side would inhibit, muscle innervation from both the left posterior and anterior routes, thus paralyzing the whole left side, of the face (Bells Palsy). With this type of lesion, the bilateral and contalateral inputs of the posterior, and anterior routes, respectively, become irrelevant because the lesion is below the level of the, medulla and the facial motor nucleus. Whereas at a level above the medulla a lesion occurring in, one hemisphere would mean that the other hemisphere could still sufficiently innervate the posterior, facial motor nucleus, a lesion affecting a lower motor neuron would eliminate innervation altogether, because the nerves no longer have a means to receive compensatory contralateral input at a, downstream decussation., Next question
Page 1696 :
Question 267 of 560, An 18 year old man is stabbed in the axilla during a fight. His axillary artery is lacerated and, repaired. However, the surgeon neglects to repair an associated injury to the upper trunk of the, brachial plexus. Which of the following muscles is least likely to demonstrate impaired function as a, result?, , Palmar interossei, , Infraspinatus, , Brachialis, , Supinator brevis, , None of the above, , The palmar interossei are supplied by the ulnar nerve. Which lies inferiorly and is therefore less, likely to be injured., Please rate this question:, , Discuss and give feedback, , Next question, , Brachial plexus, Origin, , Anterior rami of C5 to T1, , Sections of the, plexus, , , , , Roots, trunks, divisions, cords, branches, Mnemonic:Real Teenagers Drink Cold Beer, , Roots, , , , , Located in the posterior triangle, Pass between scalenus anterior and medius, , Trunks, , , , Located posterior to middle third of clavicle
Page 1697 :
, , , Upper and middle trunks related superiorly to the subclavian artery, Lower trunk passes over 1st rib posterior to the subclavian artery, , Divisions, , Apex of axilla, , Cords, , Related to axillary artery, , Diagram illustrating the branches of the brachial plexus, , Image sourced from Wikipedia, , Cutaneous sensation of the upper limb
Page 1698 :
Image sourced from Wikipedia, , Next question
Page 1699 :
Question 268 of 560, A 23 year old man is involved in a fight, during the dispute he sustains a laceration to the posterior, aspect of his right arm, approximately 2cm proximal to the olecranon process. On assessment in the, emergency department he is unable to extend his elbow joint. Which of the following tendons is most, likely to have been cut?, , Triceps, , Pronator teres, , Brachioradialis, , Brachialis, , Biceps, , Theme from 2009 Exam, The triceps muscle extends the elbow joint. The other muscles listed all produce flexion of the elbow, joint., Please rate this question:, , Discuss and give feedback, , Next question, , Triceps, Origin, , , , , , Insertion, , , , , Long head- infraglenoid tubercle of the scapula., Lateral head- dorsal surface of the humerus, lateral and proximal to the, groove of the radial nerve, Medial head- posterior surface of the humerus on the inferomedial side of, the radial groove and both of the intermuscular septae, Olecranon process of the ulna. Here the olecranon bursa is between the, triceps tendon and olecranon., Some fibres insert to the deep fascia of the forearm, posterior capsule of the, elbow (preventing the capsule from being trapped between olecranon and
Page 1700 :
olecranon fossa during extension), , Innervation, , Radial nerve, , Blood, supply, , Profunda brachii artery, , Action, , Elbow extension. The long head can adduct the humerus and and extend it from a, flexed position, , Relations, , The radial nerve and profunda brachii vessels lie between the lateral and medial, heads, Next question
Page 1701 :
Question 269 of 560, A 25 year old man undergoes an excision of a pelvic chondrosarcoma, during the operation the, obturator nerve is sacrificed. Which of the following muscles is least likely to be affected as a result?, , Adductor longus, , Pectineus, , Adductor magnus, , Sartorius, , Gracilis, , Sartorius is supplied by the femoral nerve. In approximately 20% of the population, pectineus is, supplied by the accessory obturator nerve., Please rate this question:, , Discuss and give feedback, , Next question, , Obturator nerve, The obturator nerve arises from L2, L3 and L4 by branches from the ventral divisions of each of, these nerve roots. L3 forms the main contribution and the second lumbar branch is occasionally, absent. These branches unite in the substance of psoas major, descending vertically in its posterior, part to emerge from its medial border at the lateral margin of the sacrum. It then crosses the, sacroiliac joint to enter the lesser pelvis, it descends on obturator internus to enter the obturator, groove. In the lesser pelvis the nerve lies lateral to the internal iliac vessels and ureter, and is joined, by the obturator vessels lateral to the ovary or ductus deferens., Supplies, , , , , Medial compartment of thigh, Muscles supplied: external obturator, adductor longus, adductor brevis, adductor magnus, (not the lower part-sciatic nerve), gracilis, The cutaneous branch is often absent. When present, it passes between gracilis and, adductor longus near the middle part of the thigh, and supplies the skin and fascia of the, distal two thirds of the medial aspect.
Page 1702 :
Obturator canal, , , Connects the pelvis and thigh: contains the obturator artery, vein, nerve which divides into, anterior and posterior branches., , Cadaveric cross section demonstrating relationships of the obturator nerve, , Image sourced from Wikipedia, , Next question
Page 1703 :
Question 270 of 560, You excitedly embark on your first laparoscopic cholecystectomy and during the operation the, anatomy of Calots triangle is more hostile than anticipated. Whilst trying to apply a haemostatic clip, you avulse the cystic artery. This is followed by brisk haemorrhage. From which source is this most, likely to originate ?, , Right hepatic artery, , Portal vein, , Gastroduodenal artery, , Liver bed, , Common hepatic artery, , The cystic artery is a branch of the right hepatic artery. There are recognised variations in the, anatomy of the blood supply to the gallbladder. However, the commonest situation is for the cystic, artery to branch from the right hepatic artery., Please rate this question:, , Discuss and give feedback, , Next question, , Gallbladder, , , , Fibromuscular sac with capacity of 50ml, Columnar epithelium, , Relations of the gallbladder, , Anterior, , Posterior, , Liver, , , , , Covered by peritoneum, Transverse colon, 1st part of the duodenum
Page 1704 :
Laterally, , Right lobe of liver, , Medially, , Quadrate lobe of liver, , Arterial supply, Cystic artery (branch of Right hepatic artery), Venous drainage, Directly to the liver, Nerve supply, Sympathetic- mid thoracic spinal cord, Parasympathetic- anterior vagal trunk, Common bile duct, , Origin, , Confluence of cystic and common hepatic ducts, , Relations at, origin, , , , , Medially - Hepatic artery, Posteriorly- Portal vein, , Relations distally, , , , , , Duodenum - anteriorly, Pancreas - medially and laterally, Right renal vein - posteriorly, , Arterial supply, , Branches of hepatic artery and retroduodenal branches of gastroduodenal, artery, , Hepatobiliary triangle, , Medially, , Common hepatic duct, , Inferiorly, , Cystic duct, , Superiorly, , Inferior edge of liver, , Contents, , Cystic artery, , Relations of the gallbladder
Page 1705 :
© Image provided by the University of Sheffield, , Next question
Page 1706 :
Question 271 of 560, A 43 year old man suffers a pelvic fracture which is complicated by an injury to the junction of the, membranous urethra to the bulbar urethra. In which of the following directions is the extravasated, urine most likely to pass?, , Posteriorly into extra peritoneal tissues, , Laterally into the buttocks, , Into the abdomen, , Anteriorly into the connective tissues surrounding the scrotum, , None of the above, , The superficial perineal pouch is a compartment bounded superficially by the superficial perineal, fascia, deep by the perineal membrane (inferior fascia of the urogenital diaphragm), and laterally by, the ischiopubic ramus. It contains the crura of the penis or clitoris, muscles, viscera, blood vessels,, nerves, the proximal part of the spongy urethra in males, and the greater vestibular glands in, females., When urethral rupture occurs as in this case the urine will tend to pass anteriorly because the fascial, condensations will prevent lateral and posterior passage of the urine., Please rate this question:, , Discuss and give feedback, , Next question, , Urogenital triangle, The urogenital triangle is formed by the:, , , , Ischiopubic inferior rami, Ischial tuberosities, , A fascial sheet is attached to the sides, forming the inferior fascia of the urogenital diaphragm., It transmits the urethra in males and both the urethra and vagina in females. The membranous, urethra lies deep to this structure and is surrounded by the external urethral sphincter.
Page 1707 :
Superficial to the urogenital diaphragm lies the superficial perineal pouch. In males this contains:, , , , , , , Bulb of penis, Crura of the penis, Superficial transverse perineal muscle, Posterior scrotal arteries, Posterior scrotal nerves, , In females the internal pudendal artery branches to become the posterior labial arteries in the, superficial perineal pouch., Next question
Page 1708 :
Question 272 of 560, , Which of the following does not pass through the superior orbital fissure?, , Oculomotor nerve, , Abducens nerve, , Ophthalmic artery, , Ophthalmic division of the trigeminal nerve, , Ophthalmic veins, , The ophthalmic artery, a branch of the internal carotid enters the orbit with the optic nerve in the, canal., Please rate this question:, , Discuss and give feedback, , Next question, , Foramina of the base of the skull, Foramen, , Location, , Contents, , Foramen ovale, , Sphenoid, bone, , Otic ganglion, V3 (Mandibular nerve:3rd branch of, trigeminal), Accessory meningeal artery
Page 1710 :
Foramen, , Location, , Contents, , Superior ophthalmic vein, , *= In life the foramen lacerum is occluded by a cartilagenous plug. The ICA initially passes into the, carotid canal which ascends superomedially to enter the cranial cavity through the foramen lacerum., Base of skull anatomical overview, , Image sourced from Wikipedia, , Next question
Page 1711 :
Question 273 of 560, Which nerve supplies the 1st web space of the foot?, , Popliteal nerve, , Superficial peroneal nerve, , Deep peroneal nerve, , Tibial nerve, , Saphenous nerve, , The first web space is innervated by the deep peroneal nerve. See diagram below:
Page 1712 :
Image sourced from Wikipedia, , Please rate this question:, , Discuss and give feedback, , Next question, , Deep peroneal nerve, Origin, , From the common peroneal nerve, at the lateral aspect of the fibula, deep to, peroneus longus
Page 1714 :
Question 274 of 560, , During the course of a radical gastrectomy the surgeons detach the omentum and ligate the right, gastro-epiploic artery. From which vessel does it originate?, , Superior mesenteric artery, , Inferior mesenteric artery, , Coeliac axis, , Common hepatic artery, , Gastroduodenal artery, , Theme from January 2013 Exam, The gastroduodenal artery arises at the superior part of the duodenum and descends behind it to, terminate at its lower border. It terminates by dividing into the right gastro-epiploic artery and the, superior pancreaticoduodenal artery. The right gastro-opiploic artery passes to the left and passes, between the layers of the greater omentum to anastomose with the left gastro-epiploic artery., Please rate this question:, , Discuss and give feedback, , Next question, , Gastroduodenal artery, Supplies, Pylorus, proximal part of the duodenum, and indirectly to the pancreatic head (via the anterior and, posterior superior pancreaticoduodenal arteries), Path
Page 1715 :
Most commonly arises from the common hepatic artery of the coeliac trunk, Terminates by bifurcating into the right gastroepiploic artery and the superior pancreaticoduodenal, artery, Image showing stomach reflected superiorly to illustrate the relationship of the gastroduodenal artery, to the first part of the duodenum, , Image sourced from Wikipedia, , Next question
Page 1718 :
Image sourced from Wikipedia, , Fascia and compartments of the palm, The fascia of the palm is continuous with the antebrachial fascia and the fascia of the dorsum of the, hand. The palmar fascia is thin over the thenar and hypothenar eminences. In contrast the palmar, fascia is relatively thick. The palmar aponeurosis covers the soft tissues and overlies the flexor, tendons. The apex of the palmar aponeurosis is continuous with the flexor retinaculum and the, palmaris longus tendon. Distally, it forms four longitudinal digital bands that attach to the bases of, the proximal phalanges, blending with the fibrous digital sheaths., A medial fibrous septum extends deeply from the medial border of the palmar aponeurosis to the 5th, metacarpal. Lying medial to this are the hypothenar muscles. In a similar fashion, a lateral fibrous, septum extends deeply from the lateral border of the palmar aponeurosis to the 3rd metacarpal. The, thenar compartment lies lateral to this area., Lying between the thenar and hypothenar compartments is the central compartment. It contains the, flexor tendons and their sheaths, the lumbricals, the superficial palmar arterial arch and the digital, vessels and nerves., The deepest muscular plane is the adductor compartment, which contains adductor pollicis., Short muscles of the hand, These comprise the lumbricals and interossei. The four slender lumbrical muscles flex the fingers at, the metacarpophalangeal joints and extend the interphalangeal joint. The four dorsal interossei are, located between the metacarpals and the four palmar interossei lie on the palmar surface of the, metacarpals in the interosseous compartment of the hand., Long flexor tendons and sheaths in the hand, The tendons of FDS and FDP enter the common flexor sheath deep to the flexor retinaculum. The, tendons enter the central compartment of the hand and fan out to their respective digital synovial, sheaths. Near the base of the proximal phalanx, the tendon of FDS splits to permit the passage of
Page 1719 :
FDP. The FDP tendons are attached to the margins of the anterior aspect of the base of the distal, phalanx., The fibrous digital sheaths contain the flexor tendons and their synovial sheaths. These extend from, the heads of the metacarpals to the base of the distal phalanges., Next question
Page 1720 :
Question 276 of 560, A man with lung cancer and bone metastasis in the thoracic spinal vertebral bodies, sustains a, pathological fracture at the level of T4. The fracture is unstable and the spinal cord is severely, compressed at this level. Which of the findings below will not be present 6 weeks after injury?, , Extensor plantar reflexes, , Spasticity of the lower limbs, , Diminished patellar tendon reflex, , Urinary incontinence, , Sensory ataxia, , A thoracic cord lesion causes spastic paraperesis, hyperrflexia and extensor plantar responses, (UMN lesion), incontinence, sensory loss below the lesion and 'sensory' ataxia.These features, typically manifest several weeks later, once spinal shock (in which areflexia predominates) has, resolved., Please rate this question:, , Discuss and give feedback, , Next question, , Spinal cord, , , , , Located in a canal within the vertebral column that affords it structural support., Rostrally it continues to the medulla oblongata of the brain and caudally it tapers at a level, corresponding to the L1-2 interspace (in the adult), a central structure, the filum terminale, anchors the cord to the first coccygeal vertebra., The spinal cord is characterised by cervico-lumbar enlargements and these, broadly, speaking, are the sites which correspond to the brachial and lumbar plexuses respectively., , There are some key points to note when considering the surgical anatomy of the spinal cord:, * During foetal growth the spinal cord becomes shorter than the spinal canal, hence the adult site of, cord termination at the L1-2 level., * Due to growth of the vertebral column the spine segmental levels may not always correspond to
Page 1721 :
bony landmarks as they do in the cervical spine., * The spinal cord is incompletely divided into two symmetrical halves by a dorsal median, sulcus andventral median fissure. Grey matter surrounds a central canal that is continuous, rostrally with the ventricular system of the CNS., * The grey matter is sub divided cytoarchitecturally into Rexeds laminae., * Afferent fibres entering through the dorsal roots usually terminate near their point of entry but may, travel for varying distances in Lissauers tract. In this way they may establish synaptic connections, over several levels, * At the tip of the dorsal horn are afferents associated with nociceptive stimuli. The ventral horn, contains neurones that innervate skeletal muscle., The key point to remember when revising CNS anatomy is to keep a clinical perspective in mind. So, it is worth classifying the ways in which the spinal cord may become injured. These include:, , , , , , , , Trauma either direct or as a result of disc protrusion, Neoplasia either by direct invasion (rare) or as a result of pathological vertebral fracture, Inflammatory diseases such as Rheumatoid disease, or OA (formation of osteophytes, compressing nerve roots etc., Vascular either as a result of stroke (rare in cord) or as complication of aortic dissection, Infection historically diseases such as TB, epidural abscesses., , The anatomy of the cord will, to an extent dictate the clinical presentation. Some points/ conditions to, remember:, , , , , Brown- Sequard syndrome-Hemisection of the cord producing ipsilateral loss of, proprioception and upper motor neurone signs, plus contralateral loss of pain and, temperature sensation. The explanation of this is that the fibres decussate at different levels., Lesions below L1 will tend to present with lower motor neurone signs, Next question
Page 1722 :
Question 277 of 560, Through which of the following foramina does the genital branch of the genitofemoral nerve exit the, abdominal cavity?, , Superficial inguinal ring, , Sciatic notch, , Obturator foramen, , Femoral canal, , Deep inguinal ring, , The genitofemoral nerve divides into two branches as it approaches the inguinal ligament. The, genital branch passes anterior to the external iliac artery through the deep inguinal ring into the, inguinal canal. It communicates with the ilioinguinal nerve in the inguinal canal (though this is seldom, of clinical significance)., Please rate this question:, , Discuss and give feedback, , Next question, , Genitofemoral nerve, Supplies, Small area of the upper medial thigh., Path, , , , , , , Arises from the first and second lumbar nerves., Passes obliquely through psoas major, and emerges from its medial border opposite the, fibrocartilage between the third and fourth lumbar vertebrae., It then descends on the surface of psoas major, under cover of the peritoneum, Divides into genital and femoral branches., The genital branch passes through the inguinal canal, within the spermatic cord, to supply, the skin overlying the skin and fascia of the scrotum. The femoral branch enters the thigh, posterior to the inguinal ligament, lateral to the femoral artery. It supplies an area of skin and, fascia over the femoral triangle.
Page 1723 :
, , It may be injured during abdominal or pelvic surgery, or during inguinal hernia repairs., Next question
Page 1724 :
Question 278 of 560, A 28 year old man lacerates the posterolateral aspect of his wrist with a knife in an attempted, suicide. On arrival in the emergency department the wound is inspected and found to be located, over the lateral aspect of the extensor retinaculum (which is intact). Which of the following structures, is at greatest risk of injury?, , Superficial branch of the radial nerve, , Radial artery, , Dorsal branch of the ulnar nerve, , Tendon of extensor carpi radialis brevis, , Tendon of extensor digiti minimi, , The superficial branch of the radial nerve passes superior to the extensor retinaculum in the position, of this laceration and is at greatest risk of injury. The dorsal branch of the ulnar nerve and artery also, pass superior to the extensor retinaculum n but are located medially., Please rate this question:, , Discuss and give feedback, , Next question, , Extensor retinaculum, The extensor rentinaculum is a thickening of the deep fascia that stretches across the back of the, wrist and holds the long extensor tendons in position., Its attachments are:, , , , The pisiform and triquetral medially, The end of the radius laterally, , Structures related to the extensor retinaculum, , Structures superficial to the, , , , , Basilic vein, Dorsal cutaneous branch of the ulnar nerve
Page 1726 :
Image sourced from Wikipedia, , Next question
Page 1727 :
Question 279 of 560, , A 43 year old man is reviewed in the clinic following a cardiac operation. A chest x-ray is performed, and a circular radio-opaque structure is noted medial to the 4th interspace on the left. Which of the, following procedures is the patient most likely to have undergone?, , Aortic valve replacement with metallic valve, , Tricuspid valve replacement with metallic valve, , Tricuspid valve replacement with porcine valve, , Pulmonary valve replacement with porcine valve, , Mitral valve replacement with metallic valve, , Theme from April 2012 Exam, Please rate this question:, , Discuss and give feedback, , Next question, , Prosthetic heart valves on Chest X-rays, The aortic and mitral valves are most commonly replaced and when a metallic valve is used, can be, most readily identified on plain x-rays., The presence of cardiac disease (such as cardiomegaly) may affect the figures quoted here., Aortic, Usually located medial to the 3rd interspace on the right., Mitral
Page 1728 :
Usually located medial to the 4th interspace on the left., Tricuspid, Usually located medial to the 5th interspace on the right., Please note that these are the sites at which an artificial valve may be located and are NOT the sites, of auscultation., Next question
Page 1729 :
Question 280 of 560, A 63 year old lady is diagnosed as having an endometrial carcinoma arising from the uterine body., To which nodal region will the tumour initially metastasise?, , Para aortic nodes, , Iliac lymph nodes, , Inguinal nodes, , Pre sacral nodes, , Mesorectal lymph nodes, , Theme from 2011 exam, Tumours of the uterine body will tend to spread to the iliac nodes initially. Tumour expansion, crossing different nodal margins this is of considerable clinical significance, if nodal clearance is, performed during a Wertheims type hysterectomy., Please rate this question:, , Discuss and give feedback, , Next question, , Lymphatic drainage of the ovaries, uterus and cervix, , , , , , The ovaries drain to the para-aortic lymphatics via the gonadal vessels., The uterine fundus has a lymphatic drainage that runs with the ovarian vessels and may thus, drain to the para-aortic nodes. Some drainage may also pass along the round ligament to the, inguinal nodes., The body of the uterus drains through lymphatics contained within the broad ligament to the, iliac lymph nodes., The cervix drains into three potential nodal stations; laterally through the broad ligament to, the external iliac nodes, along the lymphatics of the uterosacral fold to the presacral nodes, and posterolaterally along lymphatics lying alongside the uterine vessels to the internal iliac, nodes., Next question
Page 1730 :
Question 281 of 560, Transection of the radial nerve at the level of the axilla will result in all of the following except:, , Loss of elbow extension., , Loss of extension of the interphalangeal joints., , Loss of metacarpophalangeal extension., , Loss of triceps reflex., , Loss of sensation overlying the first dorsal interosseous., , These may still extend by virtue of retained lumbrical muscle function., Please rate this question:, , Discuss and give feedback, , Next question, , Radial nerve, Continuation of posterior cord of the brachial plexus (root values C5 to T1), Path, , , , , , , , In the axilla: lies posterior to the axillary artery on subscapularis, latissimus dorsi and teres, major., Enters the arm between the brachial artery and the long head of triceps (medial to humerus)., Spirals around the posterior surface of the humerus in the groove for the radial nerve., At the distal third of the lateral border of the humerus it then pierces the intermuscular, septum and descends in front of the lateral epicondyle., At the lateral epicondyle it lies deeply between brachialis and brachioradialis where it then, divides into a superficial and deep terminal branch., Deep branch crosses the supinator to become the posterior interosseous nerve., , In the image below the relationships of the radial nerve can be appreciated
Page 1732 :
Anatomical, location, , Muscle affected, , Effect of paralysis, , Shoulder, , Long head of triceps, , Minor effects on shoulder stability in abduction, , Arm, , Triceps, , Loss of elbow extension, , Forearm, , Supinator, Brachioradialis, Extensor carpi radialis, longus and brevis, , Weakening of supination of prone hand and, elbow flexion in mid prone position, , The cutaneous sensation of the upper limb- illustrating the contribution of the radial nerve, , Image sourced from Wikipedia, , Next question
Page 1733 :
Question 282 of 560, Which of the following structures is not located in the superficial perineal space in females?, , Posterior labial arteries, , Pudendal nerve, , Superficial transverse perineal muscle, , Greater vestibular glands, , None of the above, , The pudendal nerve is located in the deep perineal space and then branches to innervate more, superficial structures., Please rate this question:, , Discuss and give feedback, , Next question, , Urogenital triangle, The urogenital triangle is formed by the:, , , , Ischiopubic inferior rami, Ischial tuberosities, , A fascial sheet is attached to the sides, forming the inferior fascia of the urogenital diaphragm., It transmits the urethra in males and both the urethra and vagina in females. The membranous, urethra lies deep to this structure and is surrounded by the external urethral sphincter., Superficial to the urogenital diaphragm lies the superficial perineal pouch. In males this contains:, , , , , , Bulb of penis, Crura of the penis, Superficial transverse perineal muscle, Posterior scrotal arteries
Page 1734 :
, , Posterior scrotal nerves, , In females the internal pudendal artery branches to become the posterior labial arteries in the, superficial perineal pouch., Next question
Page 1735 :
Question 283 of 560, Which of the following is not a branch of the hepatic artery?, , Pancreatic artery, , Cystic artery, , Right gastric artery, , Right hepatic artery, , Gastroduodenal artery, , The pancreatic artery is a branch of the splenic artery., Please rate this question:, , Discuss and give feedback, , Next question, , Coeliac axis, The coeliac axis has three main branches., , , , , Left gastric, Hepatic: branches-Right Gastric, Gastroduodenal, Right Gastroepiploic, Superior, Pancreaticoduodenal, Cystic (occasionally)., Splenic: branches- Pancreatic, Short Gastric, Left Gastroepiploic, , It occasionally gives off one of the inferior phrenic arteries.
Page 1737 :
Question 284 of 560, Which of the following structures does not pass behind the piriformis muscle in the greater sciatic, foramen?, , Sciatic nerve, , Posterior cutaneous nerve of the thigh, , Inferior gluteal artery, , Obturator nerve, , None of the above, , The obturator nerve does not pass through the greater sciatic foramen., Please rate this question:, , Discuss and give feedback, , Next question, , Greater sciatic foramen, Contents, , Nerves, , , , , , , , , Sciatic Nerve, Superior and Inferior Gluteal Nerves, Pudendal Nerve, Posterior Femoral Cutaneous Nerve, Nerve to Quadratus Femoris, Nerve to Obturator internus, , Vessels, , , , , , Superior Gluteal Artery and vein, Inferior Gluteal Artery and vein, Internal Pudendal Artery and vein, , Piriformis
Page 1738 :
The piriformis is a landmark for identifying structures passing out of the sciatic notch, , , , Above piriformis: Superior gluteal vessels, Below piriformis: Inferior gluteal vessels, sciatic nerve (10% pass through it, <1% above it),, posterior cutaneous nerve of the thigh, , Greater sciatic foramen boundaries, , Anterolaterally, , Greater sciatic notch of the ilium, , Posteromedially, , Sacrotuberous ligament, , Inferior, , Sacrospinous ligament and the ischial spine, , Superior, , Anterior sacroiliac ligament, , The greater sciatic foramen
Page 1740 :
Question 285 of 560, A 56 year old man is undergoing a right nephrectomy. The surgeons divide the renal artery. At what, level does this usually branch off the abdominal aorta?, , T9, , L2, , L3, , T10, , L4, , The renal arteries usually branch off the aorta on a level with L2., Please rate this question:, , Discuss and give feedback, , Next question, , Renal arteries, , , , The right renal artery is longer than the left renal artery, The renal vein/artery/pelvis enter the kidney at the hilum, , Relations, , Right, , Anterior- IVC, right renal vein, the head of the pancreas, and the descending part of the, duodenum, , Left, , Anterior- left renal vein, the tail of the pancreas, , Branches
Page 1741 :
, , , , , The renal arteries are direct branches off the aorta (upper border of L2- right side and L1 left side), In 30% there may be accessory arteries (mainly left side). Instead of entering the kidney at, the hilum, they usually pierce the upper or lower part of the organ., Before reaching the hilum of the kidney, each artery divides into four or five segmental, branches (renal vein anterior and ureter posterior); which then divide within the sinus into, lobar arteries supplying each pyramid and cortex., Each vessel gives off some small inferior suprarenal branches to the suprarenal gland, the, ureter, and the surrounding cellular tissue and muscles., Next question
Page 1742 :
Question 286 of 560, A 23 year old man is shot in the chest during a robbery. The left lung is lacerated and is bleeding. An, emergency thoracotomy is performed. The surgeons place a clamp over the hilum of the left lung., Which of the following structures lies most anteriorly at this level?, , Vagus nerve, , Oesophagus, , Descending aorta, , Phrenic nerve, , Azygos vein, , The phrenic nerve lies anteriorly at this point. The vagus passes anteriorly and then arches, backwards immediately superior to the root of the left bronchus, giving off the recurrent laryngeal, nerve as it does so., Please rate this question:, , Discuss and give feedback, , Next question, , Lung anatomy, The right lung is composed of 3 lobes divided by the oblique and transverse fissures. The left lung, has two lobes divided by the oblique fissure.The apex of both lungs is approximately 4cm superior to, the sterno-costal joint of the first rib. Immediately below this is a sulcus created by the subclavian, artery., Peripheral contact points of the lung, , , , , Base: diaphragm, Costal surface: corresponds to the cavity of the chest, Mediastinal surface: Contacts the mediastinal pleura. Has the cardiac impression. Above and, behind this concavity is a triangular depression named the hilum, where the structures which, form the root of the lung enter and leave the viscus. These structures are invested by pleura,, which, below the hilum and behind the pericardial impression, forms the pulmonary ligament
Page 1743 :
Right lung, Above the hilum is the azygos vein; Superior to this is the groove for the superior vena cava and, right innominate vein; behind this, and nearer the apex, is a furrow for the innominate artery. Behind, the hilum and the attachment of the pulmonary ligament is a vertical groove for the oesophagus; In, front and to the right of the lower part of the oesophageal groove is a deep concavity for the, extrapericardiac portion of the inferior vena cava., The root of the right lung lies behind the superior vena cava and the right atrium, and below the, azygos vein., The right main bronchus is shorter, wider and more vertical than the left main bronchus and, therefore the route taken by most foreign bodies., , Image sourced from Wikipedia, , Left lung, Above the hilum is the furrow produced by the aortic arch, and then superiorly the groove, accommodating the left subclavian artery; Behind the hilum and pulmonary ligament is a vertical, groove produced by the descending aorta, and in front of this, near the base of the lung, is the lower, part of the oesophagus., The root of the left lung passes under the aortic arch and in front of the descending aorta.
Page 1744 :
Image sourced from Wikipedia, , Inferior borders of both lungs, , , , , 6th rib in mid clavicular line, 8th rib in mid axillary line, 10th rib posteriorly, , The pleura runs two ribs lower than the corresponding lung level., Bronchopulmonary segments, , Segment number, , Right lung, , Left lung, , 1, , Apical, , Apical, , 2, , Posterior, , Posterior, , 3, , Anterior, , Anterior, , 4, , Lateral, , Superior lingular, , 5, , Medial, , Inferior lingular, , 6, , Superior (apical), , Superior (apical)
Page 1745 :
Segment number, , Right lung, , Left lung, , 7, , Medial basal, , Medial basal, , 8, , Anterior basal, , Anterior basal, , 9, , Lateral basal, , Lateral basal, , 10, , Posterior basal, , Posterior basal, Next question
Page 1746 :
Question 287 of 560, A 22 year old man presents with appendicitis. At operation the appendix is retrocaecal and difficult to, access. Division of which of the following anatomical structures should be undertaken?, , Ileocolic artery, , Mesentery of the caecum, , Gonadal vessels, , Lateral peritoneal attachments of the caecum, , Right colic artery, , The commonest appendiceal location is retrocaecal. Those struggling to find it at operation should, trace the tenia to the caecal pole where the appendix is located. If it cannot be mobilised easily then, division of the lateral caecal peritoneal attachments (as for a right hemicolectomy) will allow caecal, mobilisation and facilitate the procedure., Please rate this question:, , Discuss and give feedback, , Next question, , Appendix, , , , , , , , Location: Base of caecum., Up to 10cm long., Mainly lymphoid tissue (Hence mesenteric adenitis may mimic appendicitis)., Caecal taenia coli converge at base of appendix and form a longitudinal muscle cover over, the appendix. This convergence should facilitate its identification at surgery if it is retrocaecal, and difficult to find (which it can be when people start doing appendicectomies!), Arterial supply: Appendicular artery (branch of the ileocolic)., It is intra peritoneal., , McBurney's point, , , 1/3 of the way along a line drawn from the Anterior Superior Iliac Spine to the Umbilicus
Page 1748 :
Question 288 of 560, Which of the following muscles does not adduct the shoulder?, , Teres major, , Pectoralis major, , Coracobrachialis, , Supraspinatus, , Latissimus dorsi, , Supraspinatus is an abductor of the shoulder., Please rate this question:, , Discuss and give feedback, , Next question, , Shoulder joint, , , , , Shallow synovial ball and socket type of joint., It is an inherently unstable joint, but is capable to a wide range of movement., Stability is provided by muscles of the rotator cuff that pass from the scapula to insert in the, greater tuberosity (all except sub scapularis-lesser tuberosity)., , Glenoid labrum, , , , , Fibrocartilaginous rim attached to the free edge of the glenoid cavity, Tendon of the long head of biceps arises from within the joint from the supraglenoid tubercle,, and is fused at this point to the labrum., The long head of triceps attaches to the infraglenoid tubercle, , Fibrous capsule
Page 1751 :
Question 289 of 560, Which of these muscles is innervated by the cervical branch of the facial nerve?, , Masseter, , Sternocleidomastoid, , Platysma, , Geniohyoid, , Sternothyroid, , The cervical branch of the facial nerve innervates platysma., Please rate this question:, , Discuss and give feedback, , Next question, , Facial nerve, The facial nerve is the main nerve supplying the structures of the second embryonic branchial arch., It is predominantly an efferent nerve to the muscles of facial expression, digastric muscle and also to, many glandular structures. It contains a few afferent fibres which originate in the cells of its genicular, ganglion and are concerned with taste., Supply - 'face, ear, taste, tear', , , , , , Face: muscles of facial expression, Ear: nerve to stapedius, Taste: supplies anterior two-thirds of tongue, Tear: parasympathetic fibres to lacrimal glands, also salivary glands, , Path, Subarachnoid path, , , Origin: motor- pons, sensory- nervus intermedius
Page 1752 :
, , Pass through the petrous temporal bone into the internal auditory meatus with the, vestibulocochlear nerve. Here they combine to become the facial nerve., , Facial canal path, , , , The canal passes superior to the vestibule of the inner ear, At the medial aspect of the middle ear, it becomes wider and contains the geniculate, ganglion., , - 3 branches:, 1. greater petrosal nerve, 2. nerve to stapedius, 3. chorda tympani, Stylomastoid foramen, , , , Passes through the stylomastoid foramen (tympanic cavity anterior and mastoid antrum, posteriorly), Posterior auricular nerve and branch to posterior belly of digastric and stylohyoid muscle, , Face, Enters parotid gland and divides into 5 branches:, , , , , , , Temporal branch, Zygomatic branch, Buccal branch, Marginal mandibular branch, Cervical branch, Next question
Page 1753 :
Question 290 of 560, During a thyroidectomy the surgeons ligate the inferior thyroid artery. From which vessel does this, structure usually originate?, , External carotid artery, , Thyrocervical trunk, , Internal carotid artery, , Subclavian artery, , Vertebral artery, , The inferior thyroid artery originates from the thyrocervical trunk. This is a branch of the subclavian, artery., Please rate this question:, , Discuss and give feedback, , Next question, , Thyroid gland, , , , , , , , Right and left lobes connected by isthmus, Surrounded by sheath from pretracheal layer of deep fascia, Apex: Lamina of thyroid cartilage, Base: 4th-5th tracheal ring, Pyramidal lobe: from isthmus, May be attached to foramen caecum at the base of the tongue, , Relations, , Anteromedially, , , , , , , Sternothyroid, Superior belly of omohyoid, Sternohyoid, Anterior aspect of sternocleidomastoid
Page 1754 :
Posterolaterally, , Carotid sheath, , Medially, , , , , , , , , , Larynx, Trachea, Pharynx, Oesophagus, Cricothyroid muscle, External laryngeal nerve (near superior thyroid artery), Recurrent laryngeal nerve (near inferior thyroid artery), , Posterior, , , , , Parathyroid glands, Anastomosis of superior and inferior thyroid arteries, , Isthmus, , , , , Anteriorly: Sternothyroids, sternohyoids, anterior jugular veins, Posteriorly: 2nd, 3rd, 4th tracheal rings (attached via Ligament of, Berry), , Blood Supply, , Arterial, , , , , , Superior thyroid artery (1st branch of external carotid), Inferior thyroid artery (from thyrocervical trunk), Thyroidea ima (in 10% of population -from brachiocephalic artery or aorta), , Venous, , , , , Superior and middle thyroid veins - into the IJV, Inferior thyroid vein - into the brachiocephalic veins, Next question
Page 1755 :
Question 291 of 560, A 56 year old man is left impotent following an abdomino-perineal excision of the colon and rectum., What is the most likely explanation?, , Psychosexual issues related to an end colostomy, , Damage to the sacral venous plexus during total mesorectal excision, , Damage to the left ureter during sigmoid mobilisation, , Damage to the hypogastric plexus during mobilisation of the inferior mesenteric artery, , Damage to the internal iliac artery during total mesorectal excision, , Autonomic nerve injury is the most common cause., Please rate this question:, , Discuss and give feedback, , Next question, , Nerve lesions during surgery, A variety of different procedures carry the risk of iatrogenic nerve injury. These are important not, only from the patients perspective but also from a medicolegal standpoint., The following operations and their associated nerve lesions are listed here:, , , , , , , , , , , Posterior triangle lymph node biopsy and accessory nerve lesion., Lloyd Davies stirrups and common peroneal nerve., Thyroidectomy and laryngeal nerve., Anterior resection of rectum and hypogastric autonomic nerves., Axillary node clearance; long thoracic nerve, thoracodorsal nerve and intercostobrachial, nerve., Inguinal hernia surgery and ilioinguinal nerve., Varicose vein surgery- sural and saphenous nerves., Posterior approach to the hip and sciatic nerve., Carotid endarterectomy and hypoglossal nerve.
Page 1756 :
There are many more, with sound anatomical understanding of the commonly performed procedures, the incidence of nerve lesions can be minimised. They commonly occur when surgeons operate in, an unfamiliar tissue plane or by blind placement of haemostats (not recommended)., Next question
Page 1757 :
Question 292 of 560, A 73 year old man is due to undergo a radical prostatectomy for carcinoma of the prostate gland. To, which of the following lymph nodes will the tumour drain primarily?, , Para aortic, , Internal iliac, , Superficial inguinal, , Meso rectal, , None of the above, , The prostate lymphatic drainage is primarily to the internal iliac nodes and also the sacral nodes., Although internal iliac is the first site., Please rate this question:, , Discuss and give feedback, , Next question, , Prostate gland, The prostate gland is approximately the shape and size of a walnut and is located inferior to the, bladder. It is separated from the rectum by Denonvilliers fascia and its blood supply is derived from, the internal iliac vessels (via inferior vesical artery). The internal sphincter lies at the apex of the, gland and may be damaged during prostatic surgery, affected individuals may complain of, retrograde ejaculation., Summary of prostate gland, , Arterial supply, , Inferior vesical artery (from internal iliac), , Venous drainage, , Prostatic venous plexus (to paravertebral veins), , Lymphatic, , Internal iliac nodes
Page 1758 :
drainage, , Innervation, , Inferior hypogastric plexus, , Dimensions, , , , , , Transverse diameter (4cm), AP diameter (2cm), Height (3cm), , Lobes, , , , , , , Posterior lobe: posterior to urethra, Median lobe: posterior to urethra, in between ejaculatory ducts, Lateral lobes x 2, Isthmus, , Zones, , , , Peripheral zone: subcapsular portion of posterior prostate. Most, prostate cancers are here, Central zone, Transition zone, Stroma, , , , , , Relations, , Anterior, , Pubic symphysis, Prostatic venous plexus, , Posterior, , Denonvilliers fascia, Rectum, Ejaculatory ducts, , Lateral, , Venous plexus (lies on prostate), Levator ani (immediately below the puboprostatic ligaments)
Page 1759 :
Image sourced from Wikipedia, , Next question
Page 1760 :
Question 293 of 560, Which of the following statements relating to the vertebral column is false?, , There are 7 cervical vertebrae, , The cervical and lumbar lordosis are secondary curves developing after birth due to, change in shape of the intervertebral discs, The lumbar vertebrae do not have a transverse process foramina, , The lumbar vertebrae receive blood directly from the aorta, , The spinous process is formed by the junction of the pedicles posteriorly, , The spinous process is formed by 2 laminae posteriorly., Please rate this question:, , Discuss and give feedback, , Next question, , Vertebral column, , , , There are 7 cervical, 12 thoracic, 5 lumbar, and 5 sacral vertebrae., The spinal cord segmental levels do not necessarily correspond to the vertebral segments., For example, while the C1 cord is located at the C1 vertebra, the C8 cord is situated at the, C7 vertebra. While the T1 cord is situated at the T1 vertebra, the T12 cord is situated at the, T8 vertebra. The lumbar cord is situated between T9 and T11 vertebrae. The sacral cord is, situated between the T12 to L2 vertebrae., , Cervical vertebrae, The interface between the first and second vertebra is called the atlanto-axis junction. The C3 cord, contains the phrenic nucleus., , Muscle, , Nerve root value, , Deltoid, , C5,6
Page 1761 :
Muscle, , Nerve root value, , Biceps, , C5,6, , Wrist extensors, , C6-8, , Triceps, , C6-8, , Wrist flexors, , C6-T1, , Hand muscles, , C8-T1, , Thoracic vertebrae, The thoracic vertebral segments are defined by those that have a rib. The spinal roots form the, intercostal nerves that run on the bottom side of the ribs and these nerves control the intercostal, muscles and associated dermatomes., Lumbosacral vertebrae, Form the remainder of the segments below the vertebrae of the thorax. The lumbosacral spinal cord,, however, starts at about T9 and continues only to L2. It contains most of the segments that innervate, the hip and legs, as well as the buttocks and anal regions., Cauda Equina, The spinal cord ends at L1-L2 vertebral level. The tip of the spinal cord is called the conus. Below, the conus, there is a spray of spinal roots that is called the cauda equina. Injuries below L2, represent injuries to spinal roots rather than the spinal cord proper., Next question
Page 1762 :
Question 294 of 560, A 78 year old lady falls over in her nursing home and sustains a displaced intracapsular fracture of, the femoral neck. A decision is made to perform a hemi arthroplasty through a lateral approach., Which of these vessels will be divided to facilitate access?, , Saphenous vein, , Superior gluteal artery, , Superficial circumflex iliac artery, , Profunda femoris artery, , Transverse branch of the lateral circumflex artery, , During the Hardinge style lateral approach the transverse branch of the lateral circumflex artery is, divided to gain access. The vessels and its branches are illustrated below:
Page 1763 :
Image sourced from Wikipedia, , Please rate this question:, , Discuss and give feedback, , Next question, , Hip joint, , , , , , , Head of femur articulates with acetabulum of the pelvis, Both covered by articular hyaline cartilage, The acetabulum forms at the union of the ilium, pubis, and ischium, The triradiate cartilage (Y-shaped growth plate) separates the pelvic bones, The acetabulum holds the femoral head by the acetabular labrum
Page 1764 :
, , Normal angle between femoral head and femoral shaft is 130o, , Ligaments, , , , Transverse ligament: joints anterior and posterior ends of the articular cartilage, Head of femur ligament (ligamentum teres): acetabular notch to the fovea. Contains arterial, supply to head of femur in children., , Image sourced from Wikipedia
Page 1766 :
Question 295 of 560, A 73 year old man undergoes a sub total oesophagectomy with anastomosis of the stomach to the, cervical oesophagus. Which vessel will be primarily responsible for the arterial supply to the, oesophageal portion of the anastomosis?, , Superior thyroid artery, , Internal carotid artery, , Direct branches from the thoracic aorta, , Inferior thyroid artery, , Subclavian artery, , The cervical oesophagus is supplied by the inferior thyroid artery. The thoracic oesophagus, (removed in this case) is supplied by direct branches from the thoracic aorta., Please rate this question:, , Discuss and give feedback, , Next question, , Oesophagus, , , , , 25cm long, Starts at C6 vertebra, pierces diaphragm at T10 and ends at T11, Squamous epithelium, , Constrictions of the oesophagus, , Structure, , Distance from incisors, , Cricoid cartilage, , 15cm, , Arch of the Aorta, , 22.5cm
Page 1767 :
Left principal bronchus, , 27cm, , Diaphragmatic hiatus, , 40cm, , Relations, , Anteriorly, , , , , , , Trachea to T4, Recurrent laryngeal nerve, Left bronchus, Left atrium, Diaphragm, , Posteriorly, , , , , , , Thoracic duct to left at T5, Hemiazygos to the left T8, Descending aorta, First 2 intercostal branches of aorta, , Left, , , , , Thoracic duct, Left subclavian artery, , Right, , , , Azygos vein, , Arterial, venous and lymphatic drainage of the oesophagus, , Artery, , Vein, , Lymphatics, , Muscularis externa, , Upper, third, , Inferior, thyroid, , Inferior thyroid, , Deep, cervical, , Striated muscle, , Mid third, , Aortic, branches, , Azygos branches, , Mediastinal, , Smooth & striated, muscle, , Lower, third, , Left gastric, , Posterior mediastinal and, coeliac, , Gastric, , Smooth muscle, , Nerve supply
Page 1769 :
Question 296 of 560, , Which of the following structures is not closely related to the brachial artery?, , Ulnar nerve, , Median nerve, , Cephalic vein, , Long head of biceps, , Median cubital vein, , The cephalic vein lies superficially and on the contralateral side of the arm to the brachial artery. The, relation of the ulnar nerves and others are demonstrated in the image below:, , Image sourced from Wikipedia, , Please rate this question:
Page 1770 :
Discuss and give feedback, , Next question, , Brachial artery, The brachial artery begins at the lower border of teres major as a continuation of the axillary artery. It, terminates in the cubital fossa at the level of the neck of the radius by dividing into the radial and, ulnar arteries., Relations, Posterior relations include the long head of triceps with the radial nerve and profunda vessels, intervening. Anteriorly it is overlapped by the medial border of biceps., It is crossed by the median nerve in the middle of the arm., In the cubital fossa it is separated from the median cubital vein by the bicipital aponeurosis., The basilic vein is in contact at the most proximal aspect of the cubital fossa and lies medially., Next question
Page 1771 :
Question 297-299 of 560, , Theme: Anatomy of the abdominal aorta, , A. Common iliac artery, B. Median sacral artery, C. Left renal artery, D. Right renal artery, E. Inferior mesenteric artery, F. Superior mesenteric artery, G. Coeliac axis, H. Lumbar arteries, , Please select the branch of the abdominal aorta that most closely matches the description provided., Each option may be used once, more than once or not at all., , 297., , An aortic branch that leaves the aorta approximately 1cm below the coeliac axis., You answered Common iliac artery, The correct answer is Superior mesenteric artery, The SMA leaves the aorta approximately 1cm below the coeliac axis. This is usually a level of L1, to L 2. It's crossed anteriorly by the splenic vein and the body of the pancreas. It runs, downwards and forwards anterior to the uncinate process., , 298., , The most inferior single branch of the aorta., You answered Common iliac artery, The correct answer is Median sacral artery
Page 1772 :
The median sacral artery leaves the aorta a little above its bifurcation. It descends in the midline, anterior to L4 and L5., , 299., , The most inferior anterior branch of the aorta., You answered Common iliac artery, The correct answer is Inferior mesenteric artery, The IMA leaves the front of of the aorta usually about 3 to 4cm superior to its bifurcation., , Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal aortic branches, Branches, , Level, , Paired, , Type, , Inferior phrenic, , T12 (Upper border), , Yes, , Parietal, , Coeliac, , T12, , No, , Visceral, , Superior mesenteric, , L1, , No, , Visceral, , Middle suprarenal, , L1, , Yes, , Visceral
Page 1774 :
Question 300 of 560, Which ligament keeps the head of the radius connected to the radial notch of the ulna?, , Annular (orbicular) ligament, , Quadrate ligament, , Radial collateral ligament of the elbow, , Ulnar collateral ligament, , Radial collateral ligament, , Theme from September 2013, The annular ligament connects the radial head to the radial notch of the ulna. This is illustrated, below:, , Image sourced from Wikipedia
Page 1775 :
Please rate this question:, , Discuss and give feedback, , Next question, , Radius, The radius is one of the two long forearm bones that extends from the lateral side of the elbow to the, thumb side of the wrist. It has two expanded ends, of which the distal end is the larger. Key points, relating to its topography and relations are outlined below;, Upper end, , , , , Articular cartilage- covers medial > lateral side, Articulates with radial notch of the ulna by the annular ligament, Muscle attachment- biceps brachii at the tuberosity, , Shaft, Muscle attachment, , Upper third of the body, , Supinator, Flexor digitorum superficialis, Flexor pollicis longus, , Middle third of the body, , Pronator teres, , Lower quarter of the body, , Pronator quadratus, Tendon of supinator longus, , Lower end, , , , , , , Quadrilateral, Anterior surface- capsule of wrist joint, Medial surface- head of ulna, Lateral surface- ends in the styloid process, Posterior surface: 3 grooves containing:, , 1. Tendons of extensor carpi radialis longus and brevis, 2. Tendon of extensor pollicis longus, 3. Tendon of extensor indicis
Page 1776 :
Image sourced from Wikipedia, , Next question
Page 1777 :
Question 301 of 560, A 38 year old man presents to the clinic with shoulder weakness. On examination he has an inability, to initiate shoulder abduction. Which of the nerves listed below is least likely to be functioning, normally?, , Suprascapular nerve, , Medial pectoral nerve, , Axillary nerve, , Median nerve, , Radial nerve, , Theme from April 2012 Exam, Please rate this question:, , Discuss and give feedback, , Next question, , Suprascapular nerve, The suprascapular nerve arises from the upper trunk of the brachial plexus. It lies superior to the, trunks of the brachial plexus and passes inferolaterally parallel to them. It passes through the, scapular notch, deep to trapezius. It innervates both supraspinatus and infraspinatus and initiates, abduction of the shoulder. If damaged, patients may be able to abduct the shoulder by leaning over, the affected side and deltoid can then continue to abduct the shoulder.
Page 1778 :
Image sourced from Wikipedia, , Next question
Page 1779 :
Question 302 of 560, Which of the following statements relating to the Cavernous Sinus is false?, , The pituitary gland lies medially, , The internal carotid artery passes through it, , The temporal lobe of the brain is a lateral relation, , The mandibular branch of the trigeminal and optic nerve lie on the lateral wall, , The ophthalmic veins drain into the anterior aspect of the sinus, , The veins that drain into the sinus are important as sepsis can cause cavernous sinus thrombosis., The maxillary branch of the trigeminal and not the mandibular branches pass through the sinus, Please rate this question:, , Discuss and give feedback, , Next question, , Cavernous sinus, The cavernous sinuses are paired and are situated on the body of the sphenoid bone. It runs from, the superior orbital fissure to the petrous temporal bone., Relations, Medial, , Lateral, , Pituitary fossa, Sphenoid sinus, , Temporal lobe, , Contents, , Lateral wall components, , (from top to bottom:), Oculomotor nerve, Trochlear nerve, Ophthalmic nerve
Page 1780 :
Maxillary nerve, , Contents of the sinus, , (from medial to lateral:), Internal carotid artery (and sympathetic plexus), Abducens nerve, , Blood supply, Ophthalmic vein, superficial cortical veins, basilar plexus of veins posteriorly., Drains into the internal jugular vein via: the superior and inferior petrosal sinuses, , Image sourced from Wikipedia, , Next question
Page 1781 :
Question 303 of 560, , Which of the following is not a branch of the subclavian artery?, , Superior thyroid artery, , Vertebral artery, , Thyrocervical trunk, , Internal thoracic artery, , Dorsal scapular artery, Mnemonic for the branches of the subclavian artery: VIT C & D, V ertebral artery, I nternal thoracic, T hyrocervical trunk, C ostalcervical trunk, D orsal scapular, , Superior thyroid artery is a branch of the external carotid artery., Please rate this question:, , Discuss and give feedback, , Next question, , Subclavian artery
Page 1782 :
Path, , , , , , The left subclavian comes directly off the arch of aorta, The right subclavian arises from the brachiocephalic artery (trunk) when it bifurcates into the, subclavian and the right common carotid artery., From its origin, the subclavian artery travels laterally, passing between anterior and middle, scalene muscles, deep to scalenus anterior and anterior to scalenus medius. As the, subclavian artery crosses the lateral border of the first rib, it becomes the axillary artery. At, this point it is superficial and within the subclavian triangle., , Image sourced from Wikipedia, , Branches, , , , , , , , Vertebral artery, Internal thoracic artery, Thyrocervical trunk, Costocervical trunk, Dorsal scapular artery, Next question
Page 1783 :
Question 304 of 560, During the repair of an atrial septal defect the surgeons note that blood starts to leak from the, coronary sinus. Which structure forms the largest tributary of the coronary sinus?, , Thebesian veins, , Great cardiac vein, , Oblique vein, , Small cardiac veins, , None of the above, , The great cardiac vein runs in the anterior interventricular groove, and is the largest tributary of the, coronary sinus. The thebesian veins drain into the heart directly., Please rate this question:, , Discuss and give feedback, , Next question, , Heart anatomy, The walls of each cardiac chamber comprise:, , , , , Epicardium, Myocardium, Endocardium, , Cardiac muscle is attached to the cardiac fibrous skeleton., Relations, The heart and roots of the great vessels within the pericardial sac are related anteriorly to the, sternum, medial ends of the 3rd to 5th ribs on the left and their associated costal cartilages. The, heart and pericardial sac are situated obliquely two thirds to the left and one third to the right of the, median plane., The pulmonary valve lies at the level of the left third costal cartilage.
Page 1784 :
The mitral valve lies at the level of the fourth costal cartilage., Coronary sinus, This lies in the posterior part of the coronary groove and receives blood from the cardiac veins. The, great cardiac vein lies at its left and the middle and small cardiac veins lie on its right. The smallest, cardiac vein (anterior cardiac vein) drains into the right atrium directly., Aortic sinus, Right coronary artery arises from the right aortic sinus, the left is derived from the left aortic sinus,, which lies posteriorly., Right and left ventricles, , Structure, , Left Ventricle, , A-V Valve, , Mitral (double leaflet), , Walls, , Twice as thick as right, , Trabeculae carnae, , Much thicker and more numerous, , Right coronary artery, The RCA supplies:, , , , , , , Right atrium, Diaphragmatic part of the left ventricle, Usually the posterior third of the interventricular septum, The sino atrial node (60% cases), The atrio ventricular node (80% cases), , Left coronary artery, The LCA supplies:, , , , , , , Left atrium, Most of left ventricle, Part of the right ventricle, Anterior two thirds of the inter ventricular septum, The sino atrial node (remaining 40% cases), , Innervation of the heart, Autonomic nerve fibres from the superficial and deep cardiac plexus. These lie anterior to the, bifurcation of the trachea, posterior to the ascending aorta and superior to the bifurcation of the
Page 1785 :
pulmonary trunk. The parasympathetic supply to the heart is from presynaptic fibres of the vagus, nerves., Valves of the heart, , Mitral valve, , Aortic valve, , Pulmonary valve, , Tricuspid valve, , 2 cusps, , 3 cusps, , 3 cusps, , 3 cusps, , First heart sound, , Second heart, sound, , Second heart, sound, , First heart sound, , 1 anterior cusp, , 2 anterior cusps, , 2 anterior cusps, , 2 anterior cusps, , Attached to chordae, tendinae, , No chordae, , No chordae, , Attached to chordae, tendinae, Next question
Page 1786 :
Question 305 of 560, Which of the following vessels provides the greatest contribution to the arterial supply of the breast?, , External mammary artery, , Thoracoacromial artery, , Internal mammary artery, , Lateral thoracic artery, , Subclavian artery, , 60% of the arterial supply to the breast is derived from the internal mammary artery. The external, mammary and lateral thoracic arteries also make a significant (but lesser) contribution. This is of, importance clinically in performing reduction mammoplasty procedures., Please rate this question:, , Discuss and give feedback, , Next question, , Breast, The breast itself lies on a layer of pectoral fascia and the following muscles:, 1. Pectoralis major, 2. Serratus anterior, 3. External oblique, Image showing the topography of the female breast
Page 1787 :
Image sourced from Wikipedia, , Breast anatomy, , Nerve supply, , Arterial supply, , Venous drainage, Lymphatic, drainage, , Branches of intercostal nerves from T4-T6., , , , , , Internal mammary (thoracic) artery, External mammary artery (laterally), Anterior intercostal arteries, Thoraco-acromial artery, , Superficial venous plexus to subclavian, axillary and intercostal veins., , , , , 70% Axillary nodes, Internal mammary chain, Other lymphatic sites such as deep cervical and supraclavicular fossa, (later in disease), Next question
Page 1788 :
Question 306 of 560, Which of the following muscles is supplied by the external laryngeal nerve?, , Transverse arytenoid, , Cricothyroid, , Thyro-arytenoid, , Posterior crico-arytenoid, , Oblique arytenoid, , The others are all supplied by the recurrent laryngeal nerve., Please rate this question:, , Discuss and give feedback, , Next question, , Larynx, The larynx lies in the anterior part of the neck at the levels of C3 to C6 vertebral bodies. The, laryngeal skeleton consists of a number of cartilagenous segments. Three of these are paired;, arytenoid, corniculate and cuneiform. Three are single; thyroid, cricoid and epiglottic. The cricoid, cartilage forms a complete ring (the only one to do so)., The laryngeal cavity extends from the laryngeal inlet to the level of the inferior border of the cricoid, cartilage., Divisions of the laryngeal cavity, , Laryngeal vestibule, , Superior to the vestibular folds, , Laryngeal ventricle, , Lies between vestibular folds and superior to the vocal cords, , Infraglottic cavity, , Extends from vocal cords to inferior border of the cricoid cartilage
Page 1789 :
The vocal folds (true vocal cords) control sound production. The apex of each fold projects medially, into the laryngeal cavity. Each vocal fold includes:, , , , Vocal ligament, Vocalis muscle (most medial part of thyroarytenoid muscle), , The glottis is composed of the vocal folds, processes and rima glottidis. The rima glottidis is the, narrowest potential site within the larynx, as the vocal cords may be completely opposed, forming a, complete barrier., Muscles of the larynx, , Muscle, , Origin, , Insertion, , Innervation, , Action, , Posterior, cricoarytenoid, , Posterior aspect, of lamina of, cricoid, , Muscular process, of arytenoid, , Recurrent, Laryngeal, , Abducts vocal fold, , Lateral, cricoarytenoid, , Arch of cricoid, , Muscular process, of arytenoid, , Recurrent, laryngeal, , Adducts vocal fold, , Thyroarytenoid, , Posterior aspect, of thyroid, cartilage, , Muscular process, of arytenoid, , Recurrent, laryngeal, , Relaxes vocal fold, , Transverse and, oblique, arytenoids, , Arytenoid, cartilage, , Contralateral, arytenoid, , Recurrent, laryngeal, , Closure of, intercartilagenous, part of the rima, glottidis, , Vocalis, , Depression, between lamina, of thyroid, cartilage, , Vocal ligament, and vocal process, of arytenoid, cartilage, , Recurrent, laryngeal, , Relaxes posterior, vocal ligament, tenses, anterior part, , Cricothyroid, , Anterolateral, part of cricoid, , Inferior margin, and horn of, thyroid cartilage, , External, laryngeal, , Tenses vocal fold
Page 1790 :
Blood supply, Arterial supply is via the laryngeal arteries, branches of the superior and inferior thyroid arteries. The, superior laryngeal artery is closely related to the internal laryngeal nerve. The inferior laryngeal, artery is related to the inferior laryngeal nerve. Venous drainage is via superior and inferior laryngeal, veins, the former draining into the superior thyroid vein and the latter draining into the middle thyroid, vein, or thyroid venous plexus., Lymphatic drainage, The vocal cords have no lymphatic drainage and this site acts as a lymphatic watershed., , Supraglottic part, , Upper deep cervical nodes, , Subglottic part, , Prelaryngeal and pretracheal nodes and inferior deep cervical nodes, , The aryepiglottic fold and vestibular folds have a dense plexus of lymphatics associated with them, and malignancies at these sites have a greater propensity for nodal metastasis., , Topography of the larynx, , Image sourced from Wikipedia, , Next question
Page 1791 :
Question 307 of 560, A 28 year old man has sustained a non salvageable testicular injury to his left testicle. The surgeon, decides to perform an orchidectomy and divides the left testicular artery. From which of the following, does this vessel originate?, , Abdominal aorta, , Internal iliac artery, , Inferior epigastric artery, , Inferior vesical artery, , External iliac artery, , The testicular artery is a branch of the abdominal aorta., Please rate this question:, , Discuss and give feedback, , Next question, , Scrotal and testicular anatomy, Spermatic cord, Formed by the vas deferens and is covered by the following structures:, , Layer, , Origin, , Internal spermatic fascia, , Transversalis fascia, , Cremasteric fascia, , From the fascial coverings of internal oblique, , External spermatic fascia, , External oblique aponeurosis, , Contents of the cord
Page 1792 :
Vas deferens, , Transmits sperm and accessory gland secretions, , Testicular artery, , Branch of abdominal aorta supplies testis and, epididymis, , Artery of vas deferens, , Arises from inferior vesical artery, , Cremasteric artery, , Arises from inferior epigastric artery, , Pampiniform plexus, , Venous plexus, drains into right or left testicular vein, , Sympathetic nerve fibres, , Lie on arteries, the parasympathetic fibres lie on the, vas, , Genital branch of the genitofemoral, nerve, , Supplies cremaster, , Lymphatic vessels, , Drain to lumbar and para-aortic nodes, , Scrotum, , , , , , Composed of skin and closely attached dartos fascia., Arterial supply from the anterior and posterior scrotal arteries, Lymphatic drainage to the inguinal lymph nodes, Parietal layer of the tunica vaginalis is the innermost layer, , Testes, , , , , , The testes are surrounded by the tunica vaginalis (closed peritoneal sac). The parietal layer, of the tunica vaginalis adjacent to the internal spermatic fascia., The testicular arteries arise from the aorta immediately inferiorly to the renal arteries., The pampiniform plexus drains into the testicular veins, the left drains into the left renal vein, and the right into the inferior vena cava., Lymphatic drainage is to the para-aortic nodes., Next question
Page 1793 :
Question 308 of 560, During a carotid endarterectomy the internal carotid artery is cross clamped. Assuming that no shunt, is inserted, which of the following vessels will not have diminished or absent flow as a result?, , Anterior cerebral artery, , Ophthalmic artery, , Middle cerebral artery, , Maxillary artery, , None of the above, Mnemonic for branches of the cerebral portion of the internal carotid artery 'Only Press Carotid, Arteries Momentarily', Only = Opthalmic, Press = Posterior communicating, Carotid = Choroidal, Arteries = Anterior cerebral, Momentarily = Middle cerebral, The maxillary artery is a branch of the external carotid artery., Please rate this question:, , Discuss and give feedback, , Next question, , Internal carotid artery, The internal carotid artery is formed from the common carotid opposite the upper border of the, thyroid cartilage. It extends superiorly to enter the skull via the carotid canal. From the carotid canal, it then passes through the cavernous sinus, above which it divides into the anterior and middle, cerebral arteries., Relations in the neck, , Posterior, , , , , Longus capitis, Pre-vertebral fascia
Page 1794 :
, , , Sympathetic chain, Superior laryngeal nerve, , Medially, , , , , , External carotid (near origin), Wall of pharynx, Ascending pharyngeal artery, , Laterally, , , , , Internal jugular vein (moves posteriorly at entrance to skull), Vagus nerve (most posterolaterally), , Anteriorly, , , , , , Sternocleidomastoid, Lingual and facial veins, Hypoglossal nerve, , Relations in the carotid canal, , , , , , Internal carotid plexus, Cochlea and middle ear cavity, Trigeminal ganglion (superiorly), Leaves canal lies above the foramen lacerum, , Path and relations in the cranial cavity, The artery bends sharply forwards in the cavernous sinus, the aducens nerve lies close to its, inferolateral aspect. The oculomotor, trochlear, opthalmic and, usually, the maxillary nerves lie in the, lateral wall of the sinus. Near the superior orbital fissure it turns posteriorly and passes posteromedially to pierce the roof of the cavernous sinus inferior to the optic nerve. It then passes between, the optic and oculomotor nerves to terminate below the anterior perforated substance by dividing, into the anterior and middle cerebral arteries., Branches, , , , , , , , Anterior and middle cerebral artery, Ophthalmic artery, Posterior communicating artery, Anterior choroid artery, Meningeal arteries, Hypophyseal arteries, , Image demonstrating the internal carotid artery and its relationship to the external carotid artery
Page 1795 :
Image sourced from Wikipedia, , Next question
Page 1796 :
Question 309 of 560, A 72 year old lady with osteoporosis falls and sustains an intracapsular femoral neck fracture. The, fracture is completely displaced. Which of the following vessels is the main contributor to the arterial, supply of the femoral head?, , Deep external pudendal artery, , Superficial femoral artery, , External iliac artery, , Circumflex femoral arteries, , Superficial external pudendal artery, , Theme from 2010 Exam, The vessels which form the anastomoses around the femoral head are derived from the medial and, lateral circumflex femoral arteries. These are usually derived from the profunda femoris artery., Please rate this question:, , Discuss and give feedback, , Next question, , Hip joint, , , , , , , , Head of femur articulates with acetabulum of the pelvis, Both covered by articular hyaline cartilage, The acetabulum forms at the union of the ilium, pubis, and ischium, The triradiate cartilage (Y-shaped growth plate) separates the pelvic bones, The acetabulum holds the femoral head by the acetabular labrum, Normal angle between femoral head and femoral shaft is 130o, , Ligaments, , , , Transverse ligament: joints anterior and posterior ends of the articular cartilage, Head of femur ligament (ligamentum teres): acetabular notch to the fovea. Contains arterial, supply to head of femur in children.
Page 1798 :
, , Ischiofemoral ligament: posterior support. Ischium to greater trochanter., , Blood supply, Medial circumflex femoral and lateral circumflex femoral arteries (Branches of profunda femoris)., Also from the inferior gluteal artery. These form an anastomosis and travel to up the femoral neck to, supply the head., Next question
Page 1799 :
Question 310 of 560, , A 21 year old man is hit with a hammer and sustains a depressed skull fracture at the vertex. Which, of the following sinuses is at risk in this injury?, , Superior sagittal sinus, , Inferior petrosal sinus, , Transverse sinus, , Inferior sagittal sinus, , Straight sinus, , Theme in September 2011 Exam, The superior sagittal sinus is at greatest risk in this pattern of injury. This sinus begins at the front of, the crista galli and courses backwards along the falx cerebri. It becomes continuous with the right, transverse sinus near the internal occipital protuberance., Please rate this question:, , Discuss and give feedback, , Next question, , Cranial venous sinuses, The cranial venous sinuses are located within the dura mater. They have no valves which is, important in the potential for spreading sepsis. They eventually drain into the internal jugular vein., They are:
Page 1800 :
Superior sagittal sinus, Inferior sagittal sinus, Straight sinus, Transverse sinus, Sigmoid sinus, Confluence of sinuses, Occipital sinus, Cavernous sinus, Topography of cranial venous sinuses, , Image sourced from Wikipedia, , Next question
Page 1801 :
Question 311 of 560, , A 44 year old man is stabbed in the back and the left kidney is injured. A haematoma forms, which of, the following fascial structures will contain the haematoma?, , Waldeyers fascia, , Sibsons fascia, , Bucks fascia, , Gerotas fascia, , Denonvilliers fascia, , Waldeyers fascia- Posterior ano-rectum, Sibsons fascia- Lung apex, Bucks fascia- Base of penis, Gerotas fascia- Surrounding kidney, Denonvilliers fascia- Between rectum and prostate, Please rate this question:, , Discuss and give feedback, , Next question, , Renal anatomy, Each kidney is about 11cm long, 5cm wide and 3cm thick. They are located in a deep gutter, alongside the projecting vertebral bodies, on the anterior surface of psoas major. In most cases the, left kidney lies approximately 1.5cm higher than the right. The upper pole of both kidneys, approximates with the 11th rib (beware pneumothorax during nephrectomy). On the left hand side, the hilum is located at the L1 vertebral level and the right kidney at level L1-2. The lower border of
Page 1802 :
the kidneys is usually alongside L3., The table below shows the anatomical relations of the kidneys:, Relations, , Relations, , Right Kidney, , Left Kidney, , Posterior, , Quadratus lumborum, diaphragm, psoas, major, transversus abdominis, , Quadratus lumborum, diaphragm, psoas, major, transversus abdominis, , Anterior, , Hepatic flexure of colon, , Stomach, Pancreatic tail, , Superior, , Liver, adrenal gland, , Spleen, adrenal gland, , Fascial covering, Each kidney and suprarenal gland is enclosed within a common layer of investing fascia, derived, from the transversalis fascia. It is divided into anterior and posterior layers (Gerotas fascia)., Renal structure, Kidneys are surrounded by an outer cortex and an inner medulla which usually contains between 6, and 10 pyramidal structures. The papilla marks the innermost apex of these. They terminate at the, renal pelvis, into the ureter., Lying in a hollow within the kidney is the renal sinus. This contains:, 1. Branches of the renal artery, 2. Tributaries of the renal vein, 3. Major and minor calyces's, 4. Fat, Structures at the renal hilum, The renal vein lies most anteriorly, then renal artery (it is an end artery) and the ureter lies most, posterior., Next question
Page 1803 :
Question 312 of 560, A baby is found to have a Klumpke's palsy post delivery. Which of the following is most likely to be, present?, , Loss of flexors of the wrist, , Weak elbow flexion, , Pronation of the forearm, , Adducted shoulder, , Shoulder medially rotated, Features of Klumpkes Paralysis, , , , , , Claw hand (MCP joints extended and IP joints flexed), Loss of sensation over medial aspect of forearm and hand, Horner's syndrome, Loss of flexors of the wrist, , A C8, T1 root lesion is called Klumpke's paralysis and is caused by delivery with the arm extended., Please rate this question:, , Discuss and give feedback, , Next question, , Brachial plexus, Origin, , Anterior rami of C5 to T1, , Sections of the, plexus, , , , , Roots, trunks, divisions, cords, branches, Mnemonic:Real Teenagers Drink Cold Beer, , Roots, , , , Located in the posterior triangle
Page 1804 :
Trunks, , , , Pass between scalenus anterior and medius, , , , , , Located posterior to middle third of clavicle, Upper and middle trunks related superiorly to the subclavian artery, Lower trunk passes over 1st rib posterior to the subclavian artery, , Divisions, , Apex of axilla, , Cords, , Related to axillary artery, , Diagram illustrating the branches of the brachial plexus, , Image sourced from Wikipedia, , Cutaneous sensation of the upper limb
Page 1805 :
Image sourced from Wikipedia, , Next question
Page 1806 :
Question 313 of 560, A 22 year old man undergoes a superficial parotidectomy for a pleomorphic adenoma. The operation, does not proceed well and a diathermy malfunction results in division of the buccal branch of the, facial nerve. Which of the following muscles will not demonstrate impaired function as a result?, , Zygomaticus minor, , Mentalis, , Buccinator, , Levator anguli oris, , Risorius, , Buccal branch supplies, , Zygomaticus minor, , Elevates upper lip, , Risorius, , Aids smile, , Pulls corner of mouth backward and compresses cheek, Buccinator, , Levator anguli oris, , Pulls angles of mouth upward and toward midline, , Orbicularis, , Closes and tightens lips together, , Nasalis, , Flares nostrils and compresses nostrils, , Please rate this question:, , Discuss and give feedback
Page 1807 :
Next question, , Facial nerve, The facial nerve is the main nerve supplying the structures of the second embryonic branchial arch., It is predominantly an efferent nerve to the muscles of facial expression, digastric muscle and also to, many glandular structures. It contains a few afferent fibres which originate in the cells of its genicular, ganglion and are concerned with taste., Supply - 'face, ear, taste, tear', , , , , , Face: muscles of facial expression, Ear: nerve to stapedius, Taste: supplies anterior two-thirds of tongue, Tear: parasympathetic fibres to lacrimal glands, also salivary glands, , Path, Subarachnoid path, , , , Origin: motor- pons, sensory- nervus intermedius, Pass through the petrous temporal bone into the internal auditory meatus with the, vestibulocochlear nerve. Here they combine to become the facial nerve., , Facial canal path, , , , The canal passes superior to the vestibule of the inner ear, At the medial aspect of the middle ear, it becomes wider and contains the geniculate, ganglion., , - 3 branches:, 1. greater petrosal nerve, 2. nerve to stapedius, 3. chorda tympani, Stylomastoid foramen, , , , Passes through the stylomastoid foramen (tympanic cavity anterior and mastoid antrum, posteriorly), Posterior auricular nerve and branch to posterior belly of digastric and stylohyoid muscle, , Face, Enters parotid gland and divides into 5 branches:
Page 1808 :
, , , , , , Temporal branch, Zygomatic branch, Buccal branch, Marginal mandibular branch, Cervical branch, Next question
Page 1809 :
Question 314 of 560, At which of the following vertebral body levels does the common carotid artery typically bifurcate into, the external and internal carotid arteries?, , C4, , C2, , C1, , C6, , C7, , It terminates at the upper border of the thyroid cartilege, Which is usually located at C4., Please rate this question:, , Discuss and give feedback, , Next question, , Common carotid artery, The right common carotid artery arises at the bifurcation of the brachiocephalic trunk, the left, common carotid arises from the arch of the aorta. Both terminate at the level of the upper border of, the thyroid cartilage (the lower border of the third cervical vertebra) by dividing into the internal and, external carotid arteries., Left common carotid artery, This vessel arises immediately to the left and slightly behind the origin of the brachiocephalic trunk., Its thoracic portion is 2.5- 3.5 cm in length and runs superolaterally to the sternoclavicular joint., In the thorax, The vessel is in contact, from below upwards, with the trachea, left recurrent laryngeal nerve, left, margin of the oesophagus. Anteriorly the left brachiocephalic vein runs across the artery, and the, cardiac branches from the left vagus descend in front of it. These structures together with the, thymus and the anterior margins of the left lung and pleura separate the artery from the manubrium., In the neck, The artery runs superiorly deep to sternocleidomastoid and then enters the anterior triangle. At this, point it lies within the carotid sheath with the vagus nerve and the internal jugular vein. Posteriorly
Page 1810 :
the sympathetic trunk lies between the vessel and the prevertebral fascia. At the level of C7 the, vertebral artery and thoracic duct lie behind it. The anterior tubercle of C6 transverse process is, prominent and the artery can be compressed against this structure (it corresponds to the level of the, cricoid)., Anteriorly at C6 the omohyoid muscle passes superficial to the artery., Within the carotid sheath the jugular vein lies lateral to the artery., Right common carotid artery, The right common carotid arises from the brachiocephalic artery. The right common carotid artery, corresponds with the cervical portion of the left common carotid, except that there is no thoracic duct, on the right. The oesophagus is less closely related to the right carotid than the left., Summary points about the carotid anatomy, Path, Passes behind the sternoclavicular joint (12% patients above this level) to the upper border of the, thyroid cartilage, to divide into the external (ECA) and internal carotid arteries (ICA)., Relations, , , , , , , Level of 6th cervical vertebra crossed by omohyoid, Then passes deep to the thyrohyoid, sternohyoid, sternomastoid muscles., Passes anterior to the carotid tubercle (transverse process 6th cervical vertebra)-NB, compression here stops haemorrhage., The inferior thyroid artery passes posterior to the common carotid artery., Then : Left common carotid artery crosses the thoracic duct, Right common carotid artery, crossed by recurrent laryngeal nerve
Page 1811 :
Image sourced from Wikipedia, , Next question
Page 1812 :
Question 315 of 560, A man is stabbed in the chest to the right of the manubriosternal angle. Which structure is least likely, to be injured in this case?, , Right pleura, , The trachea, , Right phrenic nerve, , Right recurrent laryngeal nerve, , Brachiocephalic vein, , The right recurrent laryngeal nerve branches off the right vagus more proximally and arches, posteriorly round the subclavian artery. So of the structures given it is the least likely to be injured., Please rate this question:, , Discuss and give feedback, , Next question, , Mediastinum, Region between the pulmonary cavities., It is covered by the mediastinal pleura. It does not contain the lungs., It extends from the thoracic inlet superiorly to the diaphragm inferiorly., Mediastinal regions, , , , , , Region, , Superior mediastinum (between manubriosternal angle and T4/5), Middle mediastinum, Posterior mediastinum, Anterior mediastinum, , Contents
Page 1814 :
Question 316 of 560, An 18 year old man is stabbed in the neck and has to undergo repair of a laceration to the internal, carotid artery. Post operatively he is noted to have a Horners syndrome. Which of the following will, not be present?, , Apparent enopthalmos, , Loss of sweating on the entire ipsilateral side of the face, , Constricted pupil, , Mild ptosis, , Normal sympathetic activity in the torso, , The anhidrosis will be mild as this is a distal lesion and at worst only a very limited area of the, ipsilateral face will be anhidrotic., Please rate this question:, , Discuss and give feedback, , Next question, , Horners syndrome, Horners syndrome, clinical features:, , , , , , Ptosis, Miosis, Enopthalmos, Anhydrosis, , Primarily a disorder of the sympathetic nervous system. Extent of symptoms depends upon the, anatomical site of the lesion., Proximal lesions occur along the hypothalamospinal tract, Distal lesions are usually post ganglionic e.g. at level of internal carotid artery or beyond., Next question
Page 1815 :
Question 317 of 560, Which of the following types of epithelium lines the lumenal surface of the normal oesophagus?, , Non keratinised stratified squamous epithelium, , Ciliated columnar epithelium, , Keratinised stratified squamous epithelium, , Non ciliated columnar epithelium, , None of the above, , The oesphagus is lined by non keratinised stratified squamous epithelium. Changes to glandular, type epithelium occur as part of metaplastic processes in reflux., Please rate this question:, , Discuss and give feedback, , Next question, , Oesophagus, , , , , 25cm long, Starts at C6 vertebra, pierces diaphragm at T10 and ends at T11, Squamous epithelium, , Constrictions of the oesophagus, , Structure, , Distance from incisors, , Cricoid cartilage, , 15cm, , Arch of the Aorta, , 22.5cm
Page 1816 :
Left principal bronchus, , 27cm, , Diaphragmatic hiatus, , 40cm, , Relations, , Anteriorly, , , , , , , Trachea to T4, Recurrent laryngeal nerve, Left bronchus, Left atrium, Diaphragm, , Posteriorly, , , , , , , Thoracic duct to left at T5, Hemiazygos to the left T8, Descending aorta, First 2 intercostal branches of aorta, , Left, , , , , Thoracic duct, Left subclavian artery, , Right, , , , Azygos vein, , Arterial, venous and lymphatic drainage of the oesophagus, , Artery, , Vein, , Lymphatics, , Muscularis externa, , Upper, third, , Inferior, thyroid, , Inferior thyroid, , Deep, cervical, , Striated muscle, , Mid third, , Aortic, branches, , Azygos branches, , Mediastinal, , Smooth & striated, muscle, , Lower, third, , Left gastric, , Posterior mediastinal and, coeliac, , Gastric, , Smooth muscle, , Nerve supply
Page 1818 :
Question 318 of 560, A 23 year old man is stabbed in the neck, in the region between the omohyoid and digastric, muscles, the injury is explored surgically. At operation a nerve injury is identified immediately, superior to the lingual artery as is branches off the external carotid artery. Which of the following is, the most likely result of this injury?, , Paralysis of the ipsilateral side of the tongue, , Abduction of the ipsilateral vocal cord, , Winging of the scapula, , Paralysis of the ipsilateral hemi diaphragm, , Inability to abduct the shoulder, , The hypoglossal nerve runs anterior to the external carotid, above the lingual arterial branch. If, damaged then ipsilateral paralysis of the genioglossus, hyoglossus and styloglossus muscles will, occur. If the patient is asked to protrude their tongue then it will tend to point to the affected side., Please rate this question:, , Discuss and give feedback, , Next question, , Anterior triangle of the neck, Boundaries, , Anterior border of the Sternocleidomastoid, Lower border of mandible, Anterior midline, , Sub triangles (divided by Digastric above and Omohyoid), , , Muscular triangle: Neck strap muscles
Page 1819 :
, , , Carotid triangle: Carotid sheath, Submandibular Triangle (digastric), , Contents of the anterior triangle, , Digastric triangle, , Submandibular gland, Submandibular nodes, Facial vessels, Hypoglossal nerve, , Muscular triangle, , Strap muscles, External jugular vein, , Carotid triangle, , Carotid sheath (Common carotid, vagus and internal jugular vein), Ansa cervicalis, , Nerve supply to digastric muscle, , , , Anterior: Mylohyoid nerve, Posterior: Facial nerve, , Image sourced from Wikipedia, , Next question
Page 1820 :
Question 319 of 560, , Which of the following structures is not directly related to the right adrenal gland?, , Diaphragm posteriorly, , Bare area of the liver anteriorly, , Right renal vein, , Inferior vena cava, , Hepato-renal pouch, , The right renal vein is very short and lies more inferiorly., Please rate this question:, , Discuss and give feedback, , Next question, , Adrenal gland anatomy, Anatomy, , Location, , Superomedially to the upper pole of each kidney, , Relationships of the right, , Diaphragm-Posteriorly, Kidney-Inferiorly, Vena Cava-Medially, Hepato-renal
Page 1821 :
adrenal, , pouch and bare area of the liver-Anteriorly, , Relationships of the left, adrenal, , Crus of the diaphragm-Postero- medially, Pancreas and splenic vesselsInferiorly, Lesser sac and stomach-Anteriorly, , Arterial supply, , Superior adrenal arteries- from inferior phrenic artery, Middle adrenal, arteries - from aorta, Inferior adrenal arteries -from renal arteries, , Venous drainage of the, right adrenal, , Via one central vein directly into the IVC, , Venous drainage of the, left adrenal, , Via one central vein into the left renal vein, , Next question
Page 1822 :
Question 320 of 560, With respect to the basilic vein, which statement is false?, , Its deep anatomical location makes it unsuitable for use as an arteriovenous access site in, fistula surgery, It originates from the dorsal venous network on the hand, , It travels up the medial aspect of the forearm, , Halfway between the shoulder and the elbow it lies deep to muscle, , It joins the brachial vein to form the axillary vein, , It is used in arteriovenous fistula surgery during a procedure known as a basilic vein transposition., Please rate this question:, , Discuss and give feedback, , Next question, , Basilic vein, The basilic and cephalic veins both provide the main pathways of venous drainage for the arm and, hand. It is continuous with the palmar venous arch distally and the axillary vein proximally., Path, , , , , , , , Originates on the medial side of the dorsal venous network of the hand, and passes up the, forearm and arm., Most of its course is superficial., Near the region anterior to the cubital fossa the vein joins the cephalic vein., Midway up the humerus the basilic vein passes deep under the muscles., At the lower border of the teres major muscle, the anterior and posterior circumflex humeral, veins feed into it., It is often joined by the medial brachial vein before draining into the axillary vein., Next question
Page 1823 :
Question 321 of 560, Mobilisation of the left lobe of the liver will facilitate surgical access to which of the following?, , Abdominal oesophagus, , Duodenum, , Right colic flexure, , Right kidney, , Pylorus of stomach, , The fundus of the stomach is a posterior relation. The pylorus lies more inferolaterally. During a total, gastrectomy division of the ligaments holding the left lobe of the liver will facilitate access to the, proximal stomach and abdominal oesophagus. This manoeuvre is seldom beneficial during a distal, gastrectomy., Please rate this question:, , Discuss and give feedback, , Next question, , Liver, Structure of the liver, , Right lobe, , , , , Supplied by right hepatic artery, Contains Couinaud segments V to VIII (-/+Sg I), , Left lobe, , , , , Supplied by the left hepatic artery, Contains Couinaud segments II to IV (+/- Sg1), , Quadrate lobe, , , , , , , Part of the right lobe anatomically, functionally is part of the left, Couinaud segment IV, Porta hepatis lies behind, On the right lies the gallbladder fossa
Page 1824 :
Caudate lobe, , , , On the left lies the fossa for the umbilical vein, , , , , , , , Supplied by both right and left hepatic arteries, Couinaud segment I, Lies behind the plane of the porta hepatis, Anterior and lateral to the inferior vena cava, Bile from the caudate lobe drains into both right and left hepatic ducts, , Detailed knowledge of Couinaud segments is not required for MRCS, , , Between the liver lobules are portal canals which contain the portal triad: Hepatic Artery,, Portal Vein, tributary of Bile Duct., , Relations of the liver, , Anterior, , Postero inferiorly, , Diaphragm, , Oesophagus, , Xiphoid process, , Stomach, , Duodenum, , Hepatic flexure of colon, , Right kidney, , Gallbladder, , Inferior vena cava, , Porta hepatis
Page 1825 :
Location, , Postero inferior surface, it joins nearly at right angles with the left sagittal fossa, and, separates the caudate lobe behind from the quadrate lobe in front, , Transmits, , , , , , , , Common hepatic duct, Hepatic artery, Portal vein, Sympathetic and parasympathetic nerve fibres, Lymphatic drainage of the liver (and nodes), , Ligaments, , Falciform ligament, , , , , , 2 layer fold peritoneum from the umbilicus to anterior liver surface, Contains ligamentum teres (remnant umbilical vein), On superior liver surface it splits into the coronary and left, triangular ligaments, , Ligamentum teres, , Joins the left branch of the portal vein in the porta hepatis, , Ligamentum, venosum, , Remnant of ductus venosus, , Arterial supply, , , Hepatic artery, , Venous, , , , Hepatic veins, Portal vein, , Nervous supply, , , Sympathetic and parasympathetic trunks of coeliac plexus, Next question
Page 1826 :
Question 322 of 560, The following statements relating to the ankle joint are true except?, , Three groups of ligaments provide mechanical stability, , The sural nerve lies medial to the Achilles tendon at its point of insertion, , Eversion of the foot occurs at the sub talar joint, , The flexor hallucis longus tendon is the most posterior structure at the medial malleolus, , The saphenous nerve crosses the ankle joint., , The sural nerve lies behind the distal fibula. Inversion and eversion are sub talar movements. The, structures passing behind the medial malleolus from anterior to posterior include: tibialis posterior,, flexor digitorum longus, posterior tibia vein, posterior tibial artery, nerve, flexor hallucis longus., Please rate this question:, , Discuss and give feedback, , Next question, , Ankle joint, The ankle joint is a synovial joint composed of the tibia and fibula superiorly and the talus inferiorly., Ligaments of the ankle joint, , , , , Deltoid ligament (medially), Lateral collateral ligament, Talofibular ligaments (both anteriorly and posteriorly), , The calcaneofibular ligament is separate from the fibrous capsule of the joint. The two talofibular, ligaments are fused with it., The components of the syndesmosis are, , , , Antero-inferior tibiofibular ligament, Postero-inferior tibiofibular ligament
Page 1827 :
, , , Inferior transverse tibiofibular ligament, Interosseous ligament, , Movements at the ankle joint, , , , , Plantar flexion (55 degrees), Dorsiflexion (35 degrees), Inversion and eversion movements occur at the level of the sub talar joint, , Nerve supply, Branches of deep peroneal and tibial nerves., References, Golano P et al. Anatomy of the ankle ligaments: a pictorial essay. Knee Surg Sports Traumatol, Arthrosc. 2010 May;18(5):557-69, Next question
Page 1828 :
Question 323 of 560, The oesophagus is constricted at the following levels apart from:, , Cricoid cartilage, , Arch of the aorta, , Lower oesophageal sphincter, , Left main stem bronchus, , Diaphragmatic hiatus, , The oesophagus is not constricted at the level of the lower oesophageal sphincter., Please rate this question:, , Discuss and give feedback, , Next question, , Oesophagus, , , , , 25cm long, Starts at C6 vertebra, pierces diaphragm at T10 and ends at T11, Squamous epithelium, , Constrictions of the oesophagus, , Structure, , Distance from incisors, , Cricoid cartilage, , 15cm, , Arch of the Aorta, , 22.5cm
Page 1829 :
Left principal bronchus, , 27cm, , Diaphragmatic hiatus, , 40cm, , Relations, , Anteriorly, , , , , , , Trachea to T4, Recurrent laryngeal nerve, Left bronchus, Left atrium, Diaphragm, , Posteriorly, , , , , , , Thoracic duct to left at T5, Hemiazygos to the left T8, Descending aorta, First 2 intercostal branches of aorta, , Left, , , , , Thoracic duct, Left subclavian artery, , Right, , , , Azygos vein, , Arterial, venous and lymphatic drainage of the oesophagus, , Artery, , Vein, , Lymphatics, , Muscularis externa, , Upper, third, , Inferior, thyroid, , Inferior thyroid, , Deep, cervical, , Striated muscle, , Mid third, , Aortic, branches, , Azygos branches, , Mediastinal, , Smooth & striated, muscle, , Lower, third, , Left gastric, , Posterior mediastinal and, coeliac, , Gastric, , Smooth muscle, , Nerve supply
Page 1831 :
Question 324 of 560, , A 19 year old man is playing rugby when he suddenly notices a severe pain at the posterolateral, aspect of his right thigh. Which of the following muscle groups is most likely to have been injured?, , Semimembranosus, , Semitendinosus, , Long head of biceps femoris, , Gastrocnemius, , Soleus, , Theme from April 2012 Exam, The biceps femoris is the laterally located hamstring muscle. The semitendinosus and, semimembranosus are located medially. Rupture of gastrocnemius and soleus may occur but is less, common., Please rate this question:, , Discuss and give feedback, , Next question, , Biceps femoris, The biceps femoris is one of the hamstring group of muscles located in the posterior upper thigh. It, has two heads., Long head
Page 1832 :
Origin, , Ischial tuberosity, , Insertion, , Fibular head, , Action, , Knee flexion, lateral rotation tibia, extension hip, , Innervation, , Tibial division of sciatic nerve (L5, S1, S2), , Arterial, supply, , Profunda femoris artery, inferior gluteal artery, and the superior muscular branches of, popliteal artery, , Image demonstrating the biceps femoris muscle, with the long head outlined, , Image sourced from Wikipedia, , Short head, , Origin, , Lateral lip of linea aspera, lateral supracondylar ridge of femur
Page 1834 :
Question 325 of 560, Which of the following is a branch of the third part of the axillary artery?, , Superior thoracic, , Lateral thoracic, , Dorsal scapular, , Thoracoacromial, , Posterior circumflex humeral, , The other branches include:, , , , Subscapular, Anterior circumflex humeral, , Please rate this question:, , Discuss and give feedback, , Next question, , Axilla, Boundaries of the axilla, , Medially, , Chest wall and Serratus anterior, , Laterally, , Humeral head, , Floor, , Subscapularis
Page 1835 :
Anterior aspect, , Lateral border of Pectoralis major, , Fascia, , Clavipectoral fascia, , Content:, , Long thoracic nerve (of, Bell), , Derived from C5-C7 and passes behind the brachial plexus to enter, the axilla. It lies on the medial chest wall and supplies serratus, anterior. Its location puts it at risk during axillary surgery and, damage will lead to winging of the scapula., , Thoracodorsal nerve and, thoracodorsal trunk, , Innervate and vascularise latissimus dorsi., , Axillary vein, , Lies at the apex of the axilla, it is the continuation of the basilic vein., Becomes the subclavian vein at the outer border of the first rib., , Intercostobrachial, nerves, , Traverse the axillary lymph nodes and are often divided during, axillary surgery. They provide cutaneous sensation to the axillary, skin., , Lymph nodes, , The axilla is the main site of lymphatic drainage for the breast., Next question
Page 1836 :
Question 326 of 560, Which of the following structures separates the intervertebral disks from the spinal cord?, , Anterior longitudinal ligament, , Posterior longitudinal ligament, , Supraspinous ligament, , Interspinous ligament, , Ligamentum flavum, , The posterior longitudinal ligament overlies the posterior aspect of the vertebral bodies. It also, overlies the posterior aspect of the intervertebral disks., Please rate this question:, , Discuss and give feedback, , Next question, , Intervertebral discs, , , , , , , , Consist of an outer annulus fibrosus and an inner nucleus pulposus., The anulus fibrosus consists of several layers of fibrocartilage., The nucleus pulposus contains loose fibres suspended in a mucoprotein gel with the, consistency of jelly. The nucleus of the disc acts as a shock absorber., Pressure on the disc causes posterior protrusion of the nucleus pulposus. Most commonly in, the lumbrosacral and lower cervical areas., The discs are separated by hyaline cartilage., There is one disc between each pair of vertebrae, except for C1/2 and the sacrococcygeal, vertebrae., Next question
Page 1837 :
Question 327 of 560, At what level does the aorta bifurcate into the left and right common iliac arteries?, , L1, , L2, , L3, , L4, , L5, , Theme from September 2013 Exam, The aorta typically bifurcates at L4. This level is usually fairly constant and is often tested in the, exam., Please rate this question:, , Discuss and give feedback, , Next question, , Levels, Transpyloric plane, Level of the body of L1, , , , , , , , , , , , , , , Pylorus stomach, Left kidney hilum (L1- left one!), Fundus of the gallbladder, Neck of pancreas, Duodenojejunal flexure, Superior mesenteric artery, Portal vein, Left and right colic flexure, Root of the transverse mesocolon, 2nd part of the duodenum, Upper part of conus medullaris, Spleen
Page 1839 :
Question 328 of 560, A 23 year old man is due to undergo a mitral valve repair for mitral regurgitation. Which of the, following is a feature of the mitral valve?, , Its closure is marked by the first heart sound, , It has two anterior cusps, , The chordae tendinae attach to the anterior cusps only, , The chordae tendinae anchor the valve directly to the wall of the left ventricle, , It is best auscultated in the left third interspace, , The mitral valve is best auscultated over the cardiac apex, where its closure marks the first heart, sound. It has only two cusps. These are attached to chordae tendinae which themselves are linked, to the wall of the ventricle by the papillary muscles., Please rate this question:, , Discuss and give feedback, , Next question, , Heart anatomy, The walls of each cardiac chamber comprise:, , , , , Epicardium, Myocardium, Endocardium, , Cardiac muscle is attached to the cardiac fibrous skeleton., Relations, The heart and roots of the great vessels within the pericardial sac are related anteriorly to the, sternum, medial ends of the 3rd to 5th ribs on the left and their associated costal cartilages. The, heart and pericardial sac are situated obliquely two thirds to the left and one third to the right of the, median plane.
Page 1840 :
The pulmonary valve lies at the level of the left third costal cartilage., The mitral valve lies at the level of the fourth costal cartilage., Coronary sinus, This lies in the posterior part of the coronary groove and receives blood from the cardiac veins. The, great cardiac vein lies at its left and the middle and small cardiac veins lie on its right. The smallest, cardiac vein (anterior cardiac vein) drains into the right atrium directly., Aortic sinus, Right coronary artery arises from the right aortic sinus, the left is derived from the left aortic sinus,, which lies posteriorly., Right and left ventricles, , Structure, , Left Ventricle, , A-V Valve, , Mitral (double leaflet), , Walls, , Twice as thick as right, , Trabeculae carnae, , Much thicker and more numerous, , Right coronary artery, The RCA supplies:, , , , , , , Right atrium, Diaphragmatic part of the left ventricle, Usually the posterior third of the interventricular septum, The sino atrial node (60% cases), The atrio ventricular node (80% cases), , Left coronary artery, The LCA supplies:, , , , , , , Left atrium, Most of left ventricle, Part of the right ventricle, Anterior two thirds of the inter ventricular septum, The sino atrial node (remaining 40% cases), , Innervation of the heart, Autonomic nerve fibres from the superficial and deep cardiac plexus. These lie anterior to the
Page 1841 :
bifurcation of the trachea, posterior to the ascending aorta and superior to the bifurcation of the, pulmonary trunk. The parasympathetic supply to the heart is from presynaptic fibres of the vagus, nerves., Valves of the heart, , Mitral valve, , Aortic valve, , Pulmonary valve, , Tricuspid valve, , 2 cusps, , 3 cusps, , 3 cusps, , 3 cusps, , First heart sound, , Second heart, sound, , Second heart, sound, , First heart sound, , 1 anterior cusp, , 2 anterior cusps, , 2 anterior cusps, , 2 anterior cusps, , Attached to chordae, tendinae, , No chordae, , No chordae, , Attached to chordae, tendinae, Next question
Page 1842 :
Question 329-331 of 560, Theme: Nerve lesions, , A., B., C., D., E., F., G., H., , Intercostobrachial, Median, Axillary, Radial, Ulnar, Musculocutaneous, Brachial plexus upper cord, Brachial plexus lower cord, , Please select the most likely nerve injury for the scenarios given. Each option may be used once,, more than once or not at all., , 329., , A 23 year old rugby player sustains a Smiths Fracture. On examination opposition of the, thumb is markedly weakened., You answered Intercostobrachial, The correct answer is Median, This high velocity injury can often produce significant angulation and displacement. Both, of these may impair the function of the median nerve with loss of function of the muscles, of the thenar eminence, , 330., , A 45 year old lady recovering from a mastectomy and axillary node clearance notices that, sensation in her armpit is impaired., Intercostobrachial, The intercostobrachial nerves are frequently injured during axillary dissection. These, nerves traverse the axilla and supply cutaneous sensation., , 331., , An 8 year old boy falls onto an outstretched hand and sustains a supracondylar fracture., In addition to a weak radial pulse the child is noted to have loss of pronation of the, affected hand., You answered Intercostobrachial, The correct answer is Median
Page 1843 :
This is a common injury in children. In this case the angulation and displacement have, resulted in median nerve injury., Please rate this question:, , Discuss and give feedback, , Next question, , Brachial plexus, Origin, , Anterior rami of C5 to T1, , Sections of the, plexus, , , , , Roots, trunks, divisions, cords, branches, Mnemonic:Real Teenagers Drink Cold Beer, , Roots, , , , , Located in the posterior triangle, Pass between scalenus anterior and medius, , Trunks, , , , , , Located posterior to middle third of clavicle, Upper and middle trunks related superiorly to the subclavian artery, Lower trunk passes over 1st rib posterior to the subclavian artery, , Divisions, , Apex of axilla, , Cords, , Related to axillary artery, , Diagram illustrating the branches of the brachial plexus
Page 1844 :
Image sourced from Wikipedia, , Cutaneous sensation of the upper limb, , Image sourced from Wikipedia, , Next question
Page 1845 :
Question 332 of 560, A 23 year old lady with sialolithiasis of the submandibular gland is undergoing excision of the gland., Which of the following nerves is at risk as the duct is mobilised?, , Lingual nerve, , Buccal nerve, , Facial nerve, , Glossopharyngeal, , Vagus, , The lingual nerve wraps around Whartons duct. The lingual nerve provides sensory supply to the, anterior 2/3 of the tongue., Please rate this question:, , Discuss and give feedback, , Next question, , Submandibular gland, Relations of the submandibular gland, , Superficial, , Platysma, deep fascia and mandible, Submandibular lymph nodes, Facial vein (facial artery near mandible), Marginal mandibular nerve, Cervical branch of the facial nerve, , Deep, , Facial artery (inferior to the mandible), Mylohoid muscle, Sub mandibular duct, Hyoglossus muscle, Lingual nerve, Submandibular ganglion
Page 1846 :
Hypoglossal nerve, , Submandibular duct (Wharton's duct), , , , , Opens lateral to the lingual frenulum on the anterior floor of mouth., 5 cm length, Lingual nerve wraps around Wharton's duct. As the duct passes forwards it crosses medial, to the nerve to lie above it and then crosses back, lateral to it, to reach a position below the, nerve., , Innervation, , , , Sympathetic innervation- Derived from superior cervical ganglion, Parasympathetic innervation- Submandibular ganglion via lingual nerve, , Arterial supply, Branch of the facial artery. The facial artery passes through the gland to groove its deep surface. It, then emerges onto the face by passing between the gland and the mandible., Venous drainage, Anterior facial vein (lies deep to the Marginal Mandibular nerve), Lymphatic drainage, Deep cervical and jugular chains of nodes, Next question
Page 1847 :
Question 333 of 560, Which of the following is true in connection with the phrenic nerves?, , They both lie anterior to the hilum of the lungs, , They are derived from spinal roots C 2,3,4, , They pierce the diaphragm at the level of T7, , They consist of motor fibres only, , None of the above, C3,4,5, Keeps the diaphragm alive!, They both lie anterior to the hilum of the lung. The phrenic nerves have both motor and sensory, functions. For this reason sub diaphragmatic pathology may cause referred pain to the shoulder., Please rate this question:, , Discuss and give feedback, , Next question, , Phrenic nerve, Origin, , , C3,4,5, , Supplies, , , Path, , Diaphragm, sensation central diaphragm and pericardium
Page 1848 :
, , , , , The phrenic nerve passes with the internal jugular vein across scalenus anterior. It passes, deep to prevertebral fascia of deep cervical fascia., Left: crosses anterior to the 1st part of the subclavian artery., Right: Anterior to scalenus anterior and crosses anterior to the 2nd part of the subclavian, artery., On both sides, the phrenic nerve runs posterior to the subclavian vein and posterior to the, internal thoracic artery as it enters the thorax., , Right phrenic nerve, , , , , In the superior mediastinum: anterior to right vagus and laterally to superior vena cava, Middle mediastinum: right of pericardium, It passes over the right atrium to exit the diaphragm at T8, , Left phrenic nerve, , , , , Passes lateral to the left subclavian artery, aortic arch and left ventricle, Passes anterior to the root of the lung, Pierces the diaphragm alone, , Image showing the passage of the phrenic nerve in the neck, , Image sourced from Wikipedia, , Next question
Page 1849 :
Question 334 of 560, A 32 year old man presents with an inguinal hernia and undergoes an open surgical repair. The, surgeons decide to place a mesh on the posterior wall of the inguinal canal to complete the repair,, which of the following structures will lie posterior to the mesh?, , Transversalis fascia, , External oblique, , Rectus abdominis, , Obturator nerve, , None of the above, Inguinal canal walls: 'MALT: 2M, 2A, 2L, 2T':, Starting from superior, moving around in order to posterior:, Superior wall (roof): 2 Muscles:Internal oblique, transversus abdominis, Anterior wall: 2 Aponeuroses: Aponeurosis of external oblique, Aponeurosis of internal oblique, Lower wall (floor): 2 Ligaments: Inguinal Ligament, Lacunar Ligament Posterior wall: 2Ts:, Transversalis fascia, Conjoint Tendon, This is actually quite a straightforward question. It is simply asking for the structure that forms the, posterior wall of the inguinal canal. This is composed of the transversalis fascia, the conjoint tendon, and more laterally the deep inguinal ring., Please rate this question:, , Discuss and give feedback, , Next question, , Inguinal canal, Location, , , , , Above the inguinal ligament, The inguinal canal is 4cm long, The superficial ring is located anterior to the pubic tubercle
Page 1850 :
, , The deep ring is located approximately 1.5-2cm above the half way point between the, anterior superior iliac spine and the pubic tubercle, , Boundaries of the inguinal canal, , Floor, , , , , , External oblique aponeurosis, Inguinal ligament, Lacunar ligament, , Roof, , , , , Internal oblique, Transversus abdominis, , Anterior wall, , External oblique aponeurosis, , Posterior wall, , , , , Transversalis fascia, Conjoint tendon, , Laterally, , , , , Internal ring, Fibres of internal oblique, , Medially, , , , , External ring, Conjoint tendon, , Contents, , Males, , Spermatic cord and ilioinguinal, nerve, , As it passes through the canal the spermatic cord, has 3 coverings:, , , , , Females, , External spermatic fascia from external, oblique aponeurosis, Cremasteric fascia, Internal spermatic fascia, , Round ligament of uterus and, ilioinguinal nerve, , Related anatomy of the inguinal region, The boundaries of Hesselbachs triangle are commonly tested and illustrated below:
Page 1851 :
Image sourced from Wikipedia, , The image below demonstrates the close relationship of the vessels to the lower limb with the, inguinal canal. A fact to be borne in mind when repairing hernial defects in this region., , Image sourced from Wikipedia, , Next question
Page 1853 :
Terminates by dividing into the medial and lateral plantar nerves., Next question
Page 1854 :
Question 336 of 560, Which of the following overlies the outer muscular layer of the intrathoracic oesophagus?, , Serosa, , Meissners plexus, , Auerbach's plexus, , Loose connective tissue, , None of the above, , The oesophagus has no serosal covering and hence holds sutures poorly. The Auerbach's and, Meissner's nerve plexuses lie in between the longitudinal and circular muscle layers and, submucosally. The sub mucosal location of the Meissner's nerve plexus facilitates its sensory role., Please rate this question:, , Discuss and give feedback, , Next question, , Oesophagus, , , , , 25cm long, Starts at C6 vertebra, pierces diaphragm at T10 and ends at T11, Squamous epithelium, , Constrictions of the oesophagus, , Structure, , Distance from incisors, , Cricoid cartilage, , 15cm, , Arch of the Aorta, , 22.5cm
Page 1855 :
Left principal bronchus, , 27cm, , Diaphragmatic hiatus, , 40cm, , Relations, , Anteriorly, , , , , , , Trachea to T4, Recurrent laryngeal nerve, Left bronchus, Left atrium, Diaphragm, , Posteriorly, , , , , , , Thoracic duct to left at T5, Hemiazygos to the left T8, Descending aorta, First 2 intercostal branches of aorta, , Left, , , , , Thoracic duct, Left subclavian artery, , Right, , , , Azygos vein, , Arterial, venous and lymphatic drainage of the oesophagus, , Artery, , Vein, , Lymphatics, , Muscularis externa, , Upper, third, , Inferior, thyroid, , Inferior thyroid, , Deep, cervical, , Striated muscle, , Mid third, , Aortic, branches, , Azygos branches, , Mediastinal, , Smooth & striated, muscle, , Lower, third, , Left gastric, , Posterior mediastinal and, coeliac, , Gastric, , Smooth muscle, , Nerve supply
Page 1857 :
Question 337 of 560, Which nerve lies medially on the thyroid gland, in the groove between the oesophagus and trachea?, , Vagus nerve, , External laryngeal nerve, , Recurrent laryngeal nerve, , Ansa cervicalis, , Phrenic nerve, , The recurrent laryngeal nerve may be injured at this site during ligation of the inferior thyroid artery., Please rate this question:, , Discuss and give feedback, , Next question, , Thyroid gland, , , , , , , , Right and left lobes connected by isthmus, Surrounded by sheath from pretracheal layer of deep fascia, Apex: Lamina of thyroid cartilage, Base: 4th-5th tracheal ring, Pyramidal lobe: from isthmus, May be attached to foramen caecum at the base of the tongue, , Relations, , Anteromedially, , Posterolaterally, , , , , , , Sternothyroid, Superior belly of omohyoid, Sternohyoid, Anterior aspect of sternocleidomastoid, , Carotid sheath
Page 1858 :
Medially, , , , , , , , , , Larynx, Trachea, Pharynx, Oesophagus, Cricothyroid muscle, External laryngeal nerve (near superior thyroid artery), Recurrent laryngeal nerve (near inferior thyroid artery), , Posterior, , , , , Parathyroid glands, Anastomosis of superior and inferior thyroid arteries, , Isthmus, , , , , Anteriorly: Sternothyroids, sternohyoids, anterior jugular veins, Posteriorly: 2nd, 3rd, 4th tracheal rings (attached via Ligament of, Berry), , Blood Supply, , Arterial, , , , , , Superior thyroid artery (1st branch of external carotid), Inferior thyroid artery (from thyrocervical trunk), Thyroidea ima (in 10% of population -from brachiocephalic artery or aorta), , Venous, , , , , Superior and middle thyroid veins - into the IJV, Inferior thyroid vein - into the brachiocephalic veins, Next question
Page 1860 :
Left principal bronchus, , 27cm, , Diaphragmatic hiatus, , 40cm, , Relations, , Anteriorly, , , , , , , Trachea to T4, Recurrent laryngeal nerve, Left bronchus, Left atrium, Diaphragm, , Posteriorly, , , , , , , Thoracic duct to left at T5, Hemiazygos to the left T8, Descending aorta, First 2 intercostal branches of aorta, , Left, , , , , Thoracic duct, Left subclavian artery, , Right, , , , Azygos vein, , Arterial, venous and lymphatic drainage of the oesophagus, , Artery, , Vein, , Lymphatics, , Muscularis externa, , Upper, third, , Inferior, thyroid, , Inferior thyroid, , Deep, cervical, , Striated muscle, , Mid third, , Aortic, branches, , Azygos branches, , Mediastinal, , Smooth & striated, muscle, , Lower, third, , Left gastric, , Posterior mediastinal and, coeliac, , Gastric, , Smooth muscle, , Nerve supply
Page 1863 :
Next question, , Ansa cervicalis, Superior, root, , Branch of C1 anterolateral to carotid sheath, , Inferior root, , Derived from C2 and C3 roots, passes posterolateral to the internal jugular vein (may lie, either deep or superficial to it), , Innervation, , Sternohyoid, Sternothyroid, Omohyoid, , The ansa cervicalis lies anterior to the carotid sheath. The nerve supply to the inferior strap muscles, enters at their inferior aspect. Therefore when dividing these muscles to expose a large goitre, the, muscles should be divided in their upper half.
Page 1864 :
Image sourced from Wikipedia, , Next question
Page 1865 :
Question 340 of 560, The anterior interosseous nerve is a branch of which of the following?, , Ulnar nerve, , Superficial branch of the radial nerve, , Axillary nerve, , Deep branch of the radial nerve, , Median nerve, , Please rate this question:, , Discuss and give feedback, , Next question, , Anterior interosseous nerve, The anterior interosseous nerve (volar interosseous nerve) is a branch of the median nerve that, supplies the deep muscles on the front of the forearm, except the ulnar half of the flexor digitorum, profundus., It accompanies the anterior interosseous artery along the anterior of the interosseous membrane of, the forearm, in the interval between the flexor pollicis longus and flexor digitorum profundus,, supplying the whole of the former and (most commonly) the radial half of the latter, and ending, below in the pronator quadratus and wrist joint., Innervation, The anterior interosseous nerve classically innervates 2.5 muscles:, , , , , , Flexor pollicis longus, Pronator quadratus, The radial half of flexor digitorum profundus (the lateral two out of the four tendons)., , These muscles are in the deep level of the anterior compartment of the forearm.
Page 1866 :
Question 341 of 560, , At which of the following anatomical locations does the common peroneal nerve bifurcate into the, superficial and deep peroneal nerves?, , Immediately anterior to the linea aspera, , At the lateral aspect of the neck of the fibula, , Within the substance of tibialis anterior muscle, , At the inferomedial aspect of the popliteal fossa, , Under the medial head of gastrocnemius, , The common peroneal nerve bifurcates at the neck of the fibula (where it is most likely to be injured)., Please rate this question:, , Discuss and give feedback, , Next question, , Common peroneal nerve, Derived from the dorsal divisions of the sacral plexus (L4, L5, S1 and S2)., This nerve supplies the skin and fascia of the anterolateral surface of the leg and the dorsum of the, foot. It also innervates the muscles of the anterior and peroneal compartments of the leg, extensor, digitorum brevis as well as the knee, ankle and foot joints., It is laterally placed within the sciatic nerve. From the bifurcation of the sciatic nerve it passes, inferolaterally in the lateral and proximal part of the popliteal fossa, under the cover of biceps femoris, and its tendon. To reach the posterior aspect of the fibular head. It ends by dividing into the deep
Page 1867 :
and superficial peroneal nerves at the point where it winds around the lateral surface of the neck of, the fibula in the body of peroneus longus, approximately 2cm distal to the apex of the head of the, fibula. It is palpable posterior to the head of the fibula., Branches, , In the thigh, , Nerve to the short head of biceps, Articular branch (knee), , In the popliteal fossa, , Lateral cutaneous nerve of the calf, , Neck of fibula, , Superficial and deep peroneal nerves, Next question
Page 1868 :
Question 342 of 560, A 48 year old motor cyclist sustains a complex lower limb fracture in a motor accident. For a time the, popliteal artery is occluded and eventually repaired. Subsequently he develops a compartment, syndrome and the anterior and superficial posterior compartments of the lower leg are, decompressed. Unfortunately, the operating surgeon neglects to decompress the deep posterior, compartment. Which of the following muscles is least likely to be affected as a result?, , Flexor digitorum longus, , Plantaris, , Tibialis posterior, , Flexor hallucis longus, , None of the above, Muscles of the deep posterior compartment:, , , , , , Tibialis posterior, Flexor hallucis longus, Flexor digitorum longus, Popliteus, , The plantaris muscle lies within the superficial posterior compartment of the lower leg., Please rate this question:, , Discuss and give feedback, , Next question, , Lower limb- Muscular compartments, Anterior compartment, , Muscle, , Nerve, , Action
Page 1871 :
Question 343 of 560, A 23 year old lady is undergoing a trendelenberg procedure for varicose veins. During the dissection, of the saphenofemoral junction, which of the structures listed below is most liable to injury?, , Superficial circumflex iliac artery, , Superficial circumflex iliac vein, , Femoral artery, , Femoral nerve, , Deep external pudendal artery, , Theme from September 2011 exam, The deep external pudendal artery runs under the long saphenous vein close to its origin and may, be injured. It is at greatest risk of injury during the flush ligation of the saphenofemoral junction., Provided an injury is identified and vessel ligated, injury is seldom associated with any serious, adverse sequelae., Please rate this question:, , Discuss and give feedback, , Next question, , Saphenous vein, Long saphenous vein, This vein may be harvested for bypass surgery, or removed as treatment for varicose veins with, saphenofemoral junction incompetence., , , , , , , Originates at the 1st digit where the dorsal vein merges with the dorsal venous arch of the, foot, Passes anterior to the medial malleolus and runs up the medial side of the leg, At the knee, it runs over the posterior border of the medial epicondyle of the femur bone, Then passes laterally to lie on the anterior surface of the thigh before entering an opening in, the fascia lata called the saphenous opening
Page 1872 :
, , It joins with the femoral vein in the region of the femoral triangle at the saphenofemoral, junction, , Tributaries, , , , , , Medial marginal, Superficial epigastric, Superficial iliac circumflex, Superficial external pudendal veins, , Short saphenous vein, , , , , Originates at the 5th digit where the dorsal vein merges with the dorsal venous arch of the, foot, which attaches to the great saphenous vein., It passes around the lateral aspect of the foot (inferior and posterior to the lateral malleolus), and runs along the posterior aspect of the leg (with the sural nerve), Passes between the heads of the gastrocnemius muscle, and drains into the popliteal vein,, approximately at or above the level of the knee joint., Next question
Page 1873 :
Question 344 of 560, Considering the pituitary gland, which of the following is false?, , The anterior pituitary secretes thyroid stimulating hormone, , The anterior pituitary develops from Rathkes pouch, , Patients with craniopharyngioma may develop bi temporal hemianopia, , The pituitary is in direct contact with the optic chiasm, , The posterior pituitary secretes oxytocin via a positive feedback loop, , Although the optic chiasm is closely related to the pituitary, and craniopharyngiomas may compress, this structure leading to bitemporal hemianopia, it is separated from the chiasm itself by a dural fold., Please rate this question:, , Discuss and give feedback, , Next question, , Pituitary Gland, The pituitary gland is located within the sella turcica within the sphenoid bone in the middle cranial, fossa. It is covered by a dural fold and weighs around 0.5g. It is attached to the hypothalamus by the, infundibulum. The anterior pituitary receives hormonal stimuli from the hypothalamus by way of the, hypothalamo-pituitary portal system. It develops from a depression in the wall of the pharynx, (Rathkes pouch)., Anterior pituitary hormones, , , , , , , , Growth hormone, Thyroid stimulating hormone, ACTH, Prolactin, LH and FSH, Melanocyte releasing hormone
Page 1874 :
Posterior pituitary hormones, , , , Oxytocin, Anti diuretic hormone, Next question
Page 1875 :
Question 345 of 560, A 24 year old man is involved in a fight and his face is cut with a knife. The wound lies immediately, anterior to the tragus of the ear and extends anteriorly. The wound is surgically explored and the, laceration is found to be mainly superficial. It extends slightly more deeply immediately inferior to the, main trunk of the facial nerve. Bleeding is observed, from which of the following is it most likely to, originate?, , External carotid artery, , Retromandibular vein, , Occipital artery, , Maxillary artery, , Ascending pharyngeal artery, , The retromandibular vein lies slightly more deeply than the facial nerve in the parotid gland. It is, formed from the maxillary and superficial temporal vein., Please rate this question:, , Discuss and give feedback, , Next question, , Retromandibular vein, , , , , Formed by a union of the maxillary vein and superficial temporal vein, It descends through the parotid gland and bifurcates within it, The anterior division passes forwards to join the facial vein, the posterior division is one of, the tributaries of the external jugular vein, Next question
Page 1876 :
Question 346 of 560, A 52 year female post hysterectomy attends clinic. She reports pain and reduced sensation over the, medial aspect of her thigh. Clinically thigh adduction is weak. What is the most likely nerve injury?, , Obturator nerve, , Sciatic nerve, , Femoral nerve, , L3 cord compression, , Deep peroneal nerve, , The obturator nerve supplies sensation to the medial aspect of the thigh and causes adduction and, internal rotation of the thigh., Injury occurs during pelvic or abdominal surgery., L3 cord compression is unlikely., Please rate this question:, , Discuss and give feedback, , Next question, , Obturator nerve, The obturator nerve arises from L2, L3 and L4 by branches from the ventral divisions of each of, these nerve roots. L3 forms the main contribution and the second lumbar branch is occasionally, absent. These branches unite in the substance of psoas major, descending vertically in its posterior, part to emerge from its medial border at the lateral margin of the sacrum. It then crosses the, sacroiliac joint to enter the lesser pelvis, it descends on obturator internus to enter the obturator, groove. In the lesser pelvis the nerve lies lateral to the internal iliac vessels and ureter, and is joined, by the obturator vessels lateral to the ovary or ductus deferens., Supplies, , , , Medial compartment of thigh, Muscles supplied: external obturator, adductor longus, adductor brevis, adductor magnus, (not the lower part-sciatic nerve), gracilis
Page 1877 :
, , The cutaneous branch is often absent. When present, it passes between gracilis and, adductor longus near the middle part of the thigh, and supplies the skin and fascia of the, distal two thirds of the medial aspect., , Obturator canal, , , Connects the pelvis and thigh: contains the obturator artery, vein, nerve which divides into, anterior and posterior branches., , Cadaveric cross section demonstrating relationships of the obturator nerve, , Image sourced from Wikipedia, , Next question
Page 1878 :
Question 347 of 560, , An ENT surgeon is performing a radical neck dissection. She wishes to fully expose the external, carotid artery. To do so she inserts a self retaining retractor close to its origin. Which of the following, structures lies posterolaterally to the external carotid at this point?, , Superior thyroid artery, , Internal carotid artery, , Lingual artery, , Facial artery, , None of the above, , The internal carotid artery lies posterolaterally to the external carotid artery at it's origin from the, common carotid. The superior thyroid, lingual and facial arteries all arise from its anterior surface., Please rate this question:, , Discuss and give feedback, , Next question, , External carotid artery, The external carotid commences immediately lateral to the pharyngeal side wall. It ascends and lies, anterior to the internal carotid and posterior to the posterior belly of digastric and stylohyoid. More, inferiorly it is covered by sternocleidomastoid, passed by hypoglossal nerves, lingual and facial, veins., It then pierces the fascia of the parotid gland finally dividing into its terminal branches within the, gland itself.
Page 1879 :
Surface marking of the carotid, This is an imaginary line drawn from the bifurcation of the common carotid passing behind the angle, of the jaw to a point immediately anterior to the tragus of the ear., Branches of the external carotid artery, It has six branches, three in front, two behind and one deep., , Three in front, , Superior thyroid, Lingual, Facial, , Two behind, , Occipital, Posterior auricular, , Deep, , Ascending pharyngeal, , It terminates by dividing into the superficial temporal and maxillary arteries in the parotid gland., , Image sourced from Wikipedia
Page 1880 :
Question 348 of 560, In Froment's test which muscle function is tested?, , Flexor pollicis longus, , Abductor pollicis longus, , Abductor pollicis brevis, , Adductor pollicis, , Opponens pollicis, , Please rate this question:, , Discuss and give feedback, , Next question, , Nerve signs, Froment's sign, , , , , , Assess for ulnar nerve palsy, Adductor pollicis muscle function tested, Hold a piece of paper between their thumb and index finger. The object is then pulled away., If ulnar nerve palsy, unable to hold the paper and will flex the flexor pollicis longus to, compensate (flexion of thumb at interphalangeal joint)., , Phalen's test, , , , , , Assess carpal tunnel syndrome, More sensitive than Tinel's sign, Hold wrist in maximum flexion and the test is positive if there is numbness in the median, nerve distribution.
Page 1881 :
Tinel's sign, , , , , Assess for carpal tunnel syndrome, Tap the median nerve at the wrist and the test is positive if there is tingling/electric-like, sensations over the distribution of the median nerve., Next question
Page 1882 :
Question 349 of 560, A 22 year old man is involved in a fight outside a nightclub. He is stabbed in the back, on the left, side, approximately 3cm below the 12th rib in the mid scapular line. The structure most likely to be, injured first as a result is the:, , Spleen, , Left kidney, , Left adrenal gland, , Left ureter, , None of the above, , The left kidney lies in this location and is the most likely structure to be injured. The Spleen lies more, superiorly, and the left adrenal and ureter are unlikely to be injured in isolation., Please rate this question:, , Discuss and give feedback, , Next question, , Levels, Transpyloric plane, Level of the body of L1, , , , , , , , , , , , , , Pylorus stomach, Left kidney hilum (L1- left one!), Fundus of the gallbladder, Neck of pancreas, Duodenojejunal flexure, Superior mesenteric artery, Portal vein, Left and right colic flexure, Root of the transverse mesocolon, 2nd part of the duodenum, Upper part of conus medullaris
Page 1885 :
Question 350-352 of 560, Theme: Cutaneous innervation, , A., B., C., D., E., F., , Ulnar nerve, Fifth cervical spinal segment, Radial nerve, Musculocutaneous nerve, Median nerve, None of these, , Please select the source of innervation for the region described. Each option may be used once,, more than once or not at all., , 350., , The skin on the palmar aspect of the thumb, You answered Ulnar nerve, The correct answer is Median nerve, The median nerve supplies cutaneous sensation to this region., See diagram below, , 351., , The nail bed of the index finger, You answered Ulnar nerve, The correct answer is Median nerve, , 352., , The skin overlying the medial aspect of the palm, Ulnar nerve, This area is innervated by the ulnar nerve., , Please rate this question:, , Discuss and give feedback, , Next question, , Brachial plexus
Page 1886 :
Origin, , Anterior rami of C5 to T1, , Sections of the, plexus, , , , , Roots, trunks, divisions, cords, branches, Mnemonic:Real Teenagers Drink Cold Beer, , Roots, , , , , Located in the posterior triangle, Pass between scalenus anterior and medius, , Trunks, , , , , , Located posterior to middle third of clavicle, Upper and middle trunks related superiorly to the subclavian artery, Lower trunk passes over 1st rib posterior to the subclavian artery, , Divisions, , Apex of axilla, , Cords, , Related to axillary artery, , Diagram illustrating the branches of the brachial plexus, , Image sourced from Wikipedia, , Cutaneous sensation of the upper limb
Page 1887 :
Image sourced from Wikipedia, , Next question
Page 1888 :
Question 353 of 560, At what level does the sciatic nerve usually bifurcate into the tibial and common peroneal nerves?, , At the superior aspect of the popliteal fossa, , At the inferior aspect of the popliteal fossa, , At the inferior border of gluteus maximus, , At the inferior border of the piriformis muscle, , In the pelvis, , The sciatic nerve passes vertically downwards over the posterior surface of the obturator internus, and quadratus femoris to the hamstring compartment of the thigh, here it is crossed posteriorly by, the long head of biceps femoris. In the buttock it lies under the cover of gluteus maximus. It, separates into its tibial and common peroneal components at the upper aspect of the popliteal fossa., Please rate this question:, , Discuss and give feedback, , Next question, , Sciatic nerve, The sciatic nerve is formed from the sacral plexus and is the largest nerve in the body. It is the, continuation of the main part of the plexus arising from ventral rami of L4 to S3. These rami, converge at the inferior border of piriformis to form the nerve itself. It passes through the inferior part, of the greater sciatic foramen and emerges beneath piriformis. Medially, lie the inferior gluteal nerve, and vessels and the pudendal nerve and vessels. It runs inferolaterally under the cover of gluteus, maximus midway between the greater trochanter and ischial tuberosity. It receives its blood supply, from the inferior gluteal artery. The nerve provides cutaneous sensation to the skin of the foot and, the leg. It also innervates the posterior thigh muscles and the lower leg and foot muscles. The nerve, splits into the tibial and common peroneal nerves approximately half way down the posterior thigh., The tibial nerve supplies the flexor muscles and the common peroneal nerve supplies the extensor, muscles and the abductor muscles., Summary points, , Origin, , Spinal nerves L4 - S3
Page 1889 :
Articular Branches, , Hip joint, , Muscular branches in, upper leg, , , , , , , Semitendinosus, Semimembranosus, Biceps femoris, Part of adductor magnus, , Cutaneous sensation, , , , , , Posterior aspect of thigh (via cutaneous nerves), Gluteal region, Entire lower leg (except the medial aspect), , Terminates, , , , , At the upper part of the popliteal fossa by dividing into the tibial and, peroneal nerves, , The nerve to the short head of the biceps femoris comes from the common peroneal part of, the sciatic and the other muscular branches arise from the tibial portion., The tibial nerve goes on to innervate all muscles of the foot except the extensor digitorum, brevis (which is innervated by the common peroneal nerve)., Next question
Page 1890 :
Question 354 of 560, A 28 year old man has a pleomorphic adenoma and the decision is made to resect this surgically., Which of the following structures is least likely to be encountered during surgical resection of the, parotid gland?, , External carotid artery, , Retromandibular vein, , Auriculotemporal nerve, , Mandibular nerve, , Zygomatic branch of the facial nerve, Structures passing through the parotid gland, , , , , , Facial nerve and branches, External carotid artery (and its branches; the maxillary and superficial temporal), Retromandibular vein, Auriculotemporal nerve, , The mandibular nerve is well separated from the parotid gland., The maxillary vein joins to the superficial temporal vein and they form the retromandibular vein which, then runs through the parotid gland., The auriculotemporal nerve runs through the gland. Following a parotidectomy this nerve may be, damaged and during neuronal regrowth may then attach to sweat glands in this region. This can, then cause gustatory sweating (Freys Syndrome)., The facial nerve branch is the marginal mandibular branch and this is related to the gland., Please rate this question:, , Discuss and give feedback, , Next question, , Parotid gland, Anatomy of the parotid gland
Page 1891 :
Location, , Overlying the mandibular ramus; anterior and inferior to the ear., , Salivary duct, , Crosses the masseter, pierces the buccinator and drains adjacent to the, 2nd upper molar tooth (Stensen's duct)., , Structures passing, through the gland, , , , , , , Relations, , , , , Facial nerve (Mnemonic: The Zebra Buggered My Cat; Temporal, Zygomatic, Buccal, Mandibular, Cervical), External carotid artery, Retromandibular vein, Auriculotemporal nerve, Anterior: masseter, medial pterygoid, superficial temporal and, maxillary artery, facial nerve, stylomandibular ligament, Posterior: posterior belly digastric muscle, sternocleidomastoid,, stylohyoid, internal carotid artery, mastoid process, styloid, process, , Arterial supply, , Branches of external carotid artery, , Venous drainage, , Retromandibular vein, , Lymphatic drainage, , Deep cervical nodes, , Nerve innervation, , , , , , Parasympathetic-Secretomotor, Sympathetic-Superior cervical ganglion, Sensory- Greater auricular nerve, , Parasympathetic stimulation produces a water rich, serous saliva. Sympathetic stimulation leads to, the production of a low volume, enzyme-rich saliva., Next question
Page 1892 :
Question 355 of 560, A 23 year old man is undergoing a hernia repair and the mesh is to be sutured to the inguinal, ligament. From which of the following does the inguinal ligament arise?, , Transversus abdominis fascia, , Internal oblique, , Rectus sheath, , Rectus abdominis muscle, , External oblique aponeurosis, , The inguinal ligament is formed by the external oblique aponeurosis. It runs from the pubic tubercle, to the anterior superior iliac spine., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal wall, The 2 main muscles of the abdominal wall are the rectus abdominis (anterior) and the quadratus, lumborum (posterior)., The remaining abdominal wall consists of 3 muscular layers. Each muscle passes from the lateral, aspect of the quadratus lumborum posteriorly to the lateral margin of the rectus sheath anteriorly., Each layer is muscular posterolaterally and aponeurotic anteriorly., , Image sourced from Wikipedia
Page 1893 :
Muscles of abdominal wall, , External, oblique, , , , , , , , , Internal, oblique, , , , , , , Transversus, abdominis, , , , , , , , , , , Lies most superficially, Originates from 5th to 12th ribs, Inserts into the anterior half of the outer aspect of the iliac crest, linea, alba and pubic tubercle, More medially and superiorly to the arcuate line, the aponeurotic layer, overlaps the rectus abdominis muscle, The lower border forms the inguinal ligament, The triangular expansion of the medial end of the inguinal ligament is, the lacunar ligament., Arises from the thoracolumbar fascia, the anterior 2/3 of the iliac crest, and the lateral 2/3 of the inguinal ligament, The muscle sweeps upwards to insert into the cartilages of the lower 3, ribs, The lower fibres form an aponeurosis that runs from the tenth costal, cartilage to the body of the pubis, At its lowermost aspect it joins the fibres of the aponeurosis of, transversus abdominis to form the conjoint tendon., Innermost muscle, Arises from the inner aspect of the costal cartilages of the lower 6 ribs ,, from the anterior 2/3 of the iliac crest and lateral 1/3 of the inguinal, ligament, Its fibres run horizontally around the abdominal wall ending in an, aponeurosis. The upper part runs posterior to the rectus abdominis., Lower down the fibres run anteriorly only., The rectus abdominis lies medially; running from the pubic crest and, symphysis to insert into the xiphoid process and 5th, 6th and 7th costal, cartilages. The muscles lies in a aponeurosis as described above., Nerve supply: anterior primary rami of T7-12, , Surgical notes, During abdominal surgery it is usually necessary to divide either the muscles or their aponeuroses., During a midline laparotomy it is desirable to divide the aponeurosis. This will leave the rectus, sheath intact above the arcuate line and the muscles intact below it. Straying off the midline will, often lead to damage to the rectus muscles, particularly below the arcuate line where they may often, be in close proximity to each other., Next question
Page 1894 :
Question 356 of 560, A 56 year old man is undergoing a carotid endarterectomy. The internal carotid artery is mobilised., How many branches does this vessel give off in the neck?, , 0, , 1, , 2, , 3, , 6, , The internal carotid does not have any branches in the neck., Please rate this question:, , Discuss and give feedback, , Next question, , Internal carotid artery, The internal carotid artery is formed from the common carotid opposite the upper border of the, thyroid cartilage. It extends superiorly to enter the skull via the carotid canal. From the carotid canal, it then passes through the cavernous sinus, above which it divides into the anterior and middle, cerebral arteries., Relations in the neck, , Posterior, , , , , , , Longus capitis, Pre-vertebral fascia, Sympathetic chain, Superior laryngeal nerve, , Medially, , , , , , External carotid (near origin), Wall of pharynx, Ascending pharyngeal artery
Page 1895 :
Laterally, , , , , Internal jugular vein (moves posteriorly at entrance to skull), Vagus nerve (most posterolaterally), , Anteriorly, , , , , , Sternocleidomastoid, Lingual and facial veins, Hypoglossal nerve, , Relations in the carotid canal, , , , , , Internal carotid plexus, Cochlea and middle ear cavity, Trigeminal ganglion (superiorly), Leaves canal lies above the foramen lacerum, , Path and relations in the cranial cavity, The artery bends sharply forwards in the cavernous sinus, the aducens nerve lies close to its, inferolateral aspect. The oculomotor, trochlear, opthalmic and, usually, the maxillary nerves lie in the, lateral wall of the sinus. Near the superior orbital fissure it turns posteriorly and passes posteromedially to pierce the roof of the cavernous sinus inferior to the optic nerve. It then passes between, the optic and oculomotor nerves to terminate below the anterior perforated substance by dividing, into the anterior and middle cerebral arteries., Branches, , , , , , , , Anterior and middle cerebral artery, Ophthalmic artery, Posterior communicating artery, Anterior choroid artery, Meningeal arteries, Hypophyseal arteries, , Image demonstrating the internal carotid artery and its relationship to the external carotid artery
Page 1896 :
Image sourced from Wikipedia, , Next question
Page 1897 :
Question 357 of 560, Which of the following is a content of the adductor canal?, , Saphenous nerve, , Sural nerve, , Femoral nerve, , Profunda branch of the femoral artery, , Saphenous vein, , It contains the saphenous nerve and the superficial branch of the femoral artery., Please rate this question:, , Discuss and give feedback, , Next question, , Adductor canal, , , , Also called Hunter's or subsartorial canal, Immediately distal to the apex of the femoral triangle, lying in the middle third of the thigh., Canal terminates at the adductor hiatus., , Borders, , Contents, , Laterally Vastus medialis muscle, , Saphenous nerve, , Posteriorly Adductor longus, adductor magnus, , Superficial femoral artery, , Roof Sartorius, , Superficial femoral vein
Page 1898 :
In the image below the sartorius muscle is removed to expose the canal contents, , Image sourced from Wikipedia, , Next question
Page 1899 :
Question 358 of 560, , A 56 year old man is undergoing a high anterior resection. Which of the following structures is at, greatest risk of injury in this procedure?, , Superior mesenteric artery, , Left ureter, , External iliac vein, , External iliac artery, , Inferior vena cava, , A careless surgeon may damage all of these structures. However, the structure at greatest risk and, most frequently encountered is the left ureter., Please rate this question:, , Discuss and give feedback, , Next question, , Colon anatomy, The colon commences with the caecum. This represents the most dilated segment of the human, colon and its base (which is intraperitoneal) is marked by the convergence of teniae coli. At this point, is located the vermiform appendix. The colon continues as the ascending colon, the posterior aspect, of which is retroperitoneal. The line of demarcation between the intra and retro peritoneal right colon, is visible as a white line, in the living, and forms the line of incision for colonic resections., The ascending colon becomes the transverse colon after passing the hepatic flexure. At this located, the colon becomes wholly intra peritoneal once again. The superior aspect of the transverse colon is
Page 1900 :
the point of attachment of the transverse colon to the greater omentum. This is an important, anatomical site since division of these attachments permits entry into the lesser sac. Separation of, the greater omentum from the transverse colon is a routine operative step in both gastric and colonic, resections., At the left side of the abdomen the transverse colon passes to the left upper quadrant and makes an, oblique inferior turn at the splenic flexure. Following this, the posterior aspect becomes, retroperitoneal once again., At the level of approximately L4 the descending colon becomes wholly intraperitoneal and becomes, the sigmoid colon. Whilst the sigmoid is wholly intraperitoneal there are usually attachments laterally, between the sigmoid and the lateral pelvic sidewall. These small congenital adhesions are not formal, anatomical attachments but frequently require division during surgical resections., At its distal end the sigmoid passes to the midline and at the region around the sacral promontary it, becomes the upper rectum. This transition is visible macroscopically as the point where the teniae, fuse. More distally the rectum passes through the peritoneum at the region of the peritoneal, reflection and becomes extraperitoneal., Arterial supply, Superior mesenteric artery and inferior mesenteric artery: linked by the marginal artery., Ascending colon: ileocolic and right colic arteries, Transverse colon: middle colic artery, Descending and sigmoid colon: inferior mesenteric artery, Venous drainage, From regional veins (that accompany arteries) to superior and inferior mesenteric vein, Lymphatic drainage, Initially along nodal chains that accompany supplying arteries, then para-aortic nodes., Embryology, Midgut- Second part of duodenum to 2/3 transverse colon, Hindgut- Distal 1/3 transverse colon to anus, Peritoneal location, The right and left colon are part intraperitoneal and part extraperitoneal. The sigmoid and transverse, colon are generally wholly intraperitoneal. This has implications for the sequelae of perforations,, which will tend to result in generalised peritonitis in the wholly intra peritoneal segments., Colonic relations, , Region of colon, , Relation
Page 1901 :
Region of colon, , Relation, , Caecum/ right colon, , Right ureter, gonadal vessels, , Hepatic flexure, , Gallbladder (medially), , Splenic flexure, , Spleen and tail of pancreas, , Distal sigmoid/ upper rectum, , Left ureter, , Rectum, , Ureters, autonomic nerves, seminal vesicles, prostate, urethra (distally), Next question
Page 1902 :
Question 359 of 560, From which of these foraminae does the opthalmic branch of the trigeminal nerve exit the skull?, , Foramen ovale, , Foramen rotundum, , Foramen spinosum, , Superior orbital fissure, , Foramen magnum, Mnemonic:, Standing Room Only -Exit of branches of trigeminal nerve from the skull, V1 -Superior orbital fissure, V2 -foramen Rotundum, V3 -foramen Ovale, The opthalmic branch of the trigeminal nerve exits the skull through the superior orbital fissure., Please rate this question:, , Discuss and give feedback, , Next question, , Trigeminal nerve, The trigeminal nerve is the main sensory nerve of the head. In addition to its major sensory role, it, also innervates the muscles of mastication., Distribution of the trigeminal nerve, , Sensory, , , , , , , , Scalp, Face, Oral cavity (and teeth), Nose and sinuses, Dura mater
Page 1903 :
Motor, , , , , , , , Muscles of mastication, Mylohyoid, Anterior belly of digastric, Tensor tympani, Tensor palati, , Autonomic connections (ganglia), , , , , , , Ciliary, Sphenopalatine, Otic, Submandibular, , Path, , , , , Originates at the pons, Sensory root forms the large, crescentic trigeminal ganglion within Meckel's cave, and, contains the cell bodies of incoming sensory nerve fibres. Here the 3 branches exit., The motor root cell bodies are in the pons and the motor fibres are distributed via the, mandibular nerve. The motor root is not part of the trigeminal ganglion., , Branches of the trigeminal nerve, , Ophthalmic nerve, , Sensory only, , Maxillary nerve, , Sensory only, , Mandibular nerve, , Sensory and motor, , Sensory, , Ophthalmic, , Exits skull via the superior orbital fissure, Sensation of: scalp and forehead, the upper eyelid, the conjunctiva and cornea of, the eye, the nose (including the tip of the nose, except alae nasi), the nasal, mucosa, the frontal sinuses, and parts of the meninges (the dura and blood, vessels)., , Maxillary, nerve, , Exit skull via the foramen rotundum, Sensation: lower eyelid and cheek, the nares and upper lip, the upper teeth and, gums, the nasal mucosa, the palate and roof of the pharynx, the maxillary,
Page 1904 :
ethmoid and sphenoid sinuses, and parts of the meninges., , Mandibular, nerve, , Exit skull via the foramen ovale, Sensation: lower lip, the lower teeth and gums, the chin and jaw (except the angle, of the jaw), parts of the external ear, and parts of the meninges., , Motor, Distributed via the mandibular nerve., The following muscles of mastication are innervated:, , , , , , Masseter, Temporalis, Medial pterygoid, Lateral pterygoid, , Other muscles innervated include:, , , , , , Tensor veli palatini, Mylohyoid, Anterior belly of digastric, Tensor tympani, Next question
Page 1905 :
Question 360 of 560, , A 56 year old lady with metastatic breast cancer develops an oestolytic deposit in the proximal, femur. One morning whilst getting out of bed she notices severe groin pain. X-rays show that the, lesser trochanter has been avulsed. Which muscle is the most likely culprit?, , Vastus lateralis, , Psoas major, , Piriformis, , Gluteus maximus, , Gluteus medius, , The psoas major inserts into the lesser trochanter and contracts when raising the trunk from the, supine position. When oestolytic lesions are present in the femur the lesser trochanter may be, avulsed., Please rate this question:, , Discuss and give feedback, , Next question, , Psoas Muscle, Origin, The deep part originates from the transverse processes of the five lumbar vertebrae, the superficial, part originates from T12 and the first 4 lumbar vertebrae., Insertion, Lesser trochanter of the femur.
Page 1906 :
Innervation, Anterior rami of L1 to L3., Action, Flexion and external rotation of the hip. Bilateral contraction can raise the trunk from the supine, position., Next question
Page 1907 :
Question 361 of 560, Which of the following nerves is responsible for the motor innervation of the sternocleidomastoid, muscle?, , Ansa cervicalis, , Accessory nerve, , Hypoglossal nerve, , Facial nerve, , Vagus nerve, , Theme from January 2013 Exam, The motor supply to the sternocleidomastoid is from the accessory nerve. The ansa cervicalis, supplies sensory information from the muscle., Please rate this question:, , Discuss and give feedback, , Next question, , Sternocleidomastoid, Anatomy, , Origin, , Rounded tendon attached to upper manubrium sterni and muscular head attached to, medial third of the clavicle, , Insertion, , Mastoid process of the temporal bone and lateral area of the superior nuchal line of, the occipital bone, , Innervation, , Spinal part of accessory nerve and anterior rami of C2 and C3 (proprioception)
Page 1908 :
Action, , , , , Both: extend the head at atlanto-occipital joint and flex the cervical, vertebral column. Accessory muscles of inspiration., Single: lateral flexion of neck, rotates head so face looks upward to the, opposite side, , Sternocleidomastoid divides the anterior and posterior triangles of the neck., Next question
Page 1909 :
Question 362 of 560, A 42 year old lady undergoes a difficult cholecystectomy and significant bleeding is occurring. The, surgeons place a vascular clamp transversely across the anterior border of the epiploic foramen., Which of the following structures will be occluded in this manoeuvre?, , Cystic artery, , Cystic duct, , Left gastric artery, , Portal vein, , None of the above, , The portal vein, hepatic artery and common bile duct are occluded., Please rate this question:, , Discuss and give feedback, , Next question, , Epiploic Foramen, The epiploic foramen has the following boundaries:, , Anteriorly (in the free edge of the lesser, omentum), , Bile duct to the right, portal vein behind and hepatic, artery to the left., , Posteriorly, , Inferior vena cava, , Inferiorly, , 1st part of the duodenum, , Superiorly, , Caudate process of the liver
Page 1910 :
During liver surgery bleeding may be controlled using a Pringles manoeuvre, this involves placing a, vascular clamp across the anterior aspect of the epiploic foramen. Thereby occluding:, , , , , Common bile duct, Hepatic artery, Portal vein, Next question
Page 1911 :
Question 363 of 560, , A 34 year old man is injured by farm machinery and sustains a laceration at the superolateral aspect, of the popliteal fossa. The medial aspect of biceps femoris is lacerated. Which of the following, underlying structures is at greatest risk of injury?, , Gracilis, , Sural nerve, , Nerve to semimembranosus, , Popliteal artery, , Common peroneal nerve, , The common peroneal nerve lies under the medial aspect of biceps femoris and is therefore at, greatest risk of injury. The tibial nerve may also be damaged in such an injury (but is not listed here)., The sural nerve branches off more inferiorly., Please rate this question:, , Discuss and give feedback, , Next question, , Common peroneal nerve, Derived from the dorsal divisions of the sacral plexus (L4, L5, S1 and S2)., This nerve supplies the skin and fascia of the anterolateral surface of the leg and the dorsum of the, foot. It also innervates the muscles of the anterior and peroneal compartments of the leg, extensor, digitorum brevis as well as the knee, ankle and foot joints.
Page 1912 :
It is laterally placed within the sciatic nerve. From the bifurcation of the sciatic nerve it passes, inferolaterally in the lateral and proximal part of the popliteal fossa, under the cover of biceps femoris, and its tendon. To reach the posterior aspect of the fibular head. It ends by dividing into the deep, and superficial peroneal nerves at the point where it winds around the lateral surface of the neck of, the fibula in the body of peroneus longus, approximately 2cm distal to the apex of the head of the, fibula. It is palpable posterior to the head of the fibula., Branches, , In the thigh, , Nerve to the short head of biceps, Articular branch (knee), , In the popliteal fossa, , Lateral cutaneous nerve of the calf, , Neck of fibula, , Superficial and deep peroneal nerves, Next question
Page 1913 :
Question 364 of 560, A 56 year old lady undergoes a Hartmans style resection of the sigmoid colon, with ligation of the, vessels close to the colon. Which of the following vessels will be responsible to supplying the rectal, stump directly?, , Superior mesenteric artery, , Middle colic artery, , Superior rectal artery, , Inferior mesenteric artery, , External iliac artery, , This question is addressing the blood supply to the rectum. Which is supplied by the superior rectal, artery. High ligation of the IMA may compromise this structure. However, the question states that, during the Hartmans procedure the vessels were ligated close to the bowel. Implying that the, superior rectal was preserved., Please rate this question:, , Discuss and give feedback, , Next question, , Rectum, The rectum is approximately 12 cm long. It is a capacitance organ. It has both intra and, extraperitoneal components. The transition between the sigmoid colon is marked by the, disappearance of the tenia coli.The extra peritoneal rectum is surrounded by mesorectal fat that also, contains lymph nodes. This mesorectal fatty layer is removed surgically during rectal cancer surgery, (Total Mesorectal Excision). The fascial layers that surround the rectum are important clinical, landmarks, anteriorly lies the fascia of Denonvilliers. Posteriorly lies Waldeyers fascia., Extra peritoneal rectum, , , , , Posterior upper third, Posterior and lateral middle third, Whole lower third
Page 1914 :
Relations, , Anteriorly (Males), , Rectovesical pouch, Bladder, Prostate, Seminal vesicles, , Anteriorly (Females), , Recto-uterine pouch (Douglas), Cervix, Vaginal wall, , Posteriorly, , Sacrum, Coccyx, Middle sacral artery, , Laterally, , Levator ani, Coccygeus, , Arterial supply, Superior rectal artery, Venous drainage, Superior rectal vein, Lymphatic drainage, , , , , Mesorectal lymph nodes (superior to dentate line), Internal iliac and then para-aortic nodes, Inguinal nodes (inferior to dentate line), Next question
Page 1915 :
Question 365 of 560, Which of the nerves listed below is at greatest risk of injury with a laceration to the upper lateral, margin of the popliteal fossa?, , Common peroneal nerve, , Sural nerve, , Sciatic nerve, , Saphenous nerve, , Tibial nerve, , The sural nerve exits at the lower infero-lateral aspect of the fossa and is more at risk in short, saphenous vein surgery. The tibial nerve lies more medially and is even less likely to be injured in, this location., Please rate this question:, , Discuss and give feedback, , Next question, , Popliteal fossa, Boundaries of the popliteal fossa, , Laterally, , Biceps femoris above, lateral head of gastrocnemius and plantaris below, , Medially, , Semimembranosus and semitendinosus above, medial head of gastrocnemius below, , Floor, , Popliteal surface of the femur, posterior ligament of knee joint and popliteus muscle, , Roof, , Superficial and deep fascia
Page 1916 :
Image showing the popliteal fossa, , © Image provided by the University of Sheffield, , Contents, , , , , , , , , Popliteal artery and vein, Small saphenous vein, Common peroneal nerve, Tibial nerve, Posterior cutaneous nerve of the thigh, Genicular branch of the obturator nerve, Lymph nodes, Next question
Page 1917 :
Question 366 of 560, Which option is false in relation to the trigeminal nerve?, , The nerve originates at the pons, , The posterior scalp is supplied by the trigeminal nerve, , The maxillary nerve exits via the foramen rotundum, , The maxillary nerve is purely sensory, , The motor root is not in the trigeminal ganglion, , The posterior scalp is supplied by C2-C3., Please rate this question:, , Discuss and give feedback, , Next question, , Trigeminal nerve, The trigeminal nerve is the main sensory nerve of the head. In addition to its major sensory role, it, also innervates the muscles of mastication., Distribution of the trigeminal nerve, , Sensory, , , , , , , , Scalp, Face, Oral cavity (and teeth), Nose and sinuses, Dura mater, , Motor, , , , , , , Muscles of mastication, Mylohyoid, Anterior belly of digastric, Tensor tympani
Page 1918 :
Autonomic connections (ganglia), , , , Tensor palati, , , , , , , Ciliary, Sphenopalatine, Otic, Submandibular, , Path, , , , , Originates at the pons, Sensory root forms the large, crescentic trigeminal ganglion within Meckel's cave, and, contains the cell bodies of incoming sensory nerve fibres. Here the 3 branches exit., The motor root cell bodies are in the pons and the motor fibres are distributed via the, mandibular nerve. The motor root is not part of the trigeminal ganglion., , Branches of the trigeminal nerve, , Ophthalmic nerve, , Sensory only, , Maxillary nerve, , Sensory only, , Mandibular nerve, , Sensory and motor, , Sensory, , Ophthalmic, , Exits skull via the superior orbital fissure, Sensation of: scalp and forehead, the upper eyelid, the conjunctiva and cornea of, the eye, the nose (including the tip of the nose, except alae nasi), the nasal, mucosa, the frontal sinuses, and parts of the meninges (the dura and blood, vessels)., , Maxillary, nerve, , Exit skull via the foramen rotundum, Sensation: lower eyelid and cheek, the nares and upper lip, the upper teeth and, gums, the nasal mucosa, the palate and roof of the pharynx, the maxillary,, ethmoid and sphenoid sinuses, and parts of the meninges., , Mandibular, , Exit skull via the foramen ovale
Page 1919 :
nerve, , Sensation: lower lip, the lower teeth and gums, the chin and jaw (except the angle, of the jaw), parts of the external ear, and parts of the meninges., , Motor, Distributed via the mandibular nerve., The following muscles of mastication are innervated:, , , , , , Masseter, Temporalis, Medial pterygoid, Lateral pterygoid, , Other muscles innervated include:, , , , , , Tensor veli palatini, Mylohyoid, Anterior belly of digastric, Tensor tympani, Next question
Page 1920 :
Question 367 of 560, A 45 year old man is undergoing a lymph node biopsy from the posterior triangle of his neck. Which, structure forms the posterior border of this region?, , Trapezius muscle, , Diagastric muscle, , External jugular vein, , Omohyoid muscle, , Sternocleidomastoid muscle, , The borders are described below., Please rate this question:, , Discuss and give feedback, , Next question, , Posterior triangle of the neck, Boundaries, , Apex, , Sternocleidomastoid and the Trapezius muscles at the Occipital bone, , Anterior, , Posterior border of the Sternocleidomastoid, , Posterior, , Anterior border of the Trapezius, , Base, , Middle third of the clavicle
Page 1921 :
Image sourced from Wikipedia, , Contents, , Nerves, , , , , , , Accessory nerve, Phrenic nerve, Three trunks of the brachial plexus, Branches of the cervical plexus: Supraclavicular nerve, transverse cervical, nerve, great auricular nerve, lesser occipital nerve, , Vessels, , , , , External jugular vein, Subclavian artery, , Muscles, , , , , Inferior belly of omohyoid, Scalene, , Lymph, nodes, , , , , Supraclavicular, Occipital, Next question
Page 1922 :
Question 368 of 560, On inspecting the caecum, which of the following structures is most likely to be identified at the point, at which all the tenia coli converge?, , Gonadal vessels, , Appendix base, , Appendix tip, , Ileocaecal valve, , Ileocolic artery, , The tenia coli converge at the base of the appendix., Please rate this question:, , Discuss and give feedback, , Next question, , Caecum, Location, , , , , Proximal right colon below the ileocaecal valve, Intraperitoneal, , Posterior relations, , , , , , , , Psoas, Iliacus, Femoral nerve, Genitofemoral nerve, Gonadal vessels, , Anterior relations, , Greater omentum, , Arterial supply, , Ileocolic artery
Page 1923 :
Lymphatic drainage, , , , Mesenteric nodes accompany the venous drainage, , The caecum is the most distensible part of the colon and in complete large bowel obstruction, with a competent ileocaecal valve the most likely site of eventual perforation., Next question
Page 1924 :
Question 369 of 560, A 42 year old lady has had an axillary node clearance for breast malignancy. Post operatively she, reports weakness of the shoulder. She is unable to push herself forwards from a wall with the right, arm and the scapula is pushed out medially from the chest wall. What is the most likely nerve injury?, , C5, C6, , C8, T1, , Axillary nerve, , Long thoracic nerve, , Spinal accessory nerve, , Theme from January 2012 and 2009 Exam, The patient has a winged scapula caused by damage to the long thoracic nerve (C5,6,7) during, surgery. The long thoracic nerve innervates serratus anterior. Serratus anterior causes pushing out, of the scapula during a punch., NB winging of the scapular laterally may indicate trapezius muscle weakness. Innervated by the, spinal accessory nerve., Please rate this question:, , Discuss and give feedback, , Next question, , Long thoracic nerve, , , , , , Derived from ventral rami of C5, C6, and C7 (close to their emergence from intervertebral, foramina), It runs downward and passes either anterior or posterior to the middle scalene muscle, It reaches upper tip of serratus anterior muscle and descends on outer surface of this, muscle, giving branches into it, Winging of Scapula occurs in long thoracic nerve injury (most common) or from spinal, accessory nerve injury (which denervates the trapezius) or a dorsal scapular nerve injury, Next question
Page 1925 :
Question 370 of 560, A 36 year old male is admitted for elective surgery for a lymph node biopsy in the supraclavicular, region. Post operatively the patient has difficulty shrugging his left shoulder. What is the most likely, reason?, , Phrenic nerve lesion, , Axillary nerve lesion, , C5, C6 root lesion, , C8, T1 root lesion, , Accessory nerve lesion, , Theme from September 2011 Exam, Theme from September 2013 Exam, The accessory nerve lies in the posterior triangle and may be injured in this region. Apart from, problems with shrugging the shoulder, he may also have difficulty lifting his arm above his head., Please rate this question:, , Discuss and give feedback, , Next question, , Posterior triangle of the neck, Boundaries, , Apex, , Sternocleidomastoid and the Trapezius muscles at the Occipital bone, , Anterior, , Posterior border of the Sternocleidomastoid, , Posterior, , Anterior border of the Trapezius, , Base, , Middle third of the clavicle
Page 1926 :
Image sourced from Wikipedia, , Contents, , Nerves, , , , , , , Accessory nerve, Phrenic nerve, Three trunks of the brachial plexus, Branches of the cervical plexus: Supraclavicular nerve, transverse cervical, nerve, great auricular nerve, lesser occipital nerve, , Vessels, , , , , External jugular vein, Subclavian artery, , Muscles, , , , , Inferior belly of omohyoid, Scalene, , Lymph, nodes, , , , , Supraclavicular, Occipital, Next question
Page 1927 :
Question 371 of 560, How many fissures are present within the right lung?, , One, , Three, , Two, , Four, , Five, , The right lung has an oblique and horizontal fissure. The upper oblique fissure separates the inferior, from the middle and upper lobes. The short horizontal fissure separates the superior and middle, lobes., Please rate this question:, , Discuss and give feedback, , Next question, , Lung anatomy, The right lung is composed of 3 lobes divided by the oblique and transverse fissures. The left lung, has two lobes divided by the oblique fissure.The apex of both lungs is approximately 4cm superior to, the sterno-costal joint of the first rib. Immediately below this is a sulcus created by the subclavian, artery., Peripheral contact points of the lung, , , , , Base: diaphragm, Costal surface: corresponds to the cavity of the chest, Mediastinal surface: Contacts the mediastinal pleura. Has the cardiac impression. Above and, behind this concavity is a triangular depression named the hilum, where the structures which, form the root of the lung enter and leave the viscus. These structures are invested by pleura,, which, below the hilum and behind the pericardial impression, forms the pulmonary ligament, , Right lung
Page 1928 :
Above the hilum is the azygos vein; Superior to this is the groove for the superior vena cava and, right innominate vein; behind this, and nearer the apex, is a furrow for the innominate artery. Behind, the hilum and the attachment of the pulmonary ligament is a vertical groove for the oesophagus; In, front and to the right of the lower part of the oesophageal groove is a deep concavity for the, extrapericardiac portion of the inferior vena cava., The root of the right lung lies behind the superior vena cava and the right atrium, and below the, azygos vein., The right main bronchus is shorter, wider and more vertical than the left main bronchus and, therefore the route taken by most foreign bodies., , Image sourced from Wikipedia, , Left lung, Above the hilum is the furrow produced by the aortic arch, and then superiorly the groove, accommodating the left subclavian artery; Behind the hilum and pulmonary ligament is a vertical, groove produced by the descending aorta, and in front of this, near the base of the lung, is the lower, part of the oesophagus., The root of the left lung passes under the aortic arch and in front of the descending aorta., , Image sourced from Wikipedia
Page 1929 :
Inferior borders of both lungs, , , , , 6th rib in mid clavicular line, 8th rib in mid axillary line, 10th rib posteriorly, , The pleura runs two ribs lower than the corresponding lung level., Bronchopulmonary segments, , Segment number, , Right lung, , Left lung, , 1, , Apical, , Apical, , 2, , Posterior, , Posterior, , 3, , Anterior, , Anterior, , 4, , Lateral, , Superior lingular, , 5, , Medial, , Inferior lingular, , 6, , Superior (apical), , Superior (apical), , 7, , Medial basal, , Medial basal, , 8, , Anterior basal, , Anterior basal, , 9, , Lateral basal, , Lateral basal, , 10, , Posterior basal, , Posterior basal, Next question
Page 1930 :
Question 372 of 560, Which of the following muscles is supplied by the musculocutaneous nerve?, , Brachialis, , Latissimus dorsi, , Flexor carpi ulnaris, , Teres minor, , Triceps, Mnemonic, Muscles innervated by the musculocutaneous nerve BBC:, Biceps brachii, Brachialis, Coracobrachialis, Please rate this question:, , Discuss and give feedback, , Next question, , Musculocutaneous nerve, , , Branch of lateral cord of brachial plexus, , Path, , , , , , It penetrates the coracobrachialis muscle, Passes obliquely between the biceps brachii and the brachialis to the lateral side of the arm, Above the elbow it pierces the deep fascia lateral to the tendon of the biceps brachii, Continues into the forearm as the lateral cutaneous nerve of the forearm
Page 1932 :
Question 373 of 560, Which of the following statements relating to the posterior cerebral artery is false?, , It supplies the visual cortex, , It is closely related to the 3rd cranial nerve, , It is a branch of the basilar artery, , It is connected to the circle of Willis via the superior cerebellar artery, , When occluded may result in contralateral loss of field of vision, , The posterior cerebral arteries are formed by the bifurcation of the basilar artery and is connected to, the circle of Willis via the posterior communicating artery., The posterior cerebral arteries supply the occipital lobe and part of the temporal lobe., Please rate this question:, , Discuss and give feedback, , Next question, , Circle of Willis, The two internal carotid arteries and two vertebral arteries form an anastomosis known as the Circle, of Willis on the inferior surface of the brain. Each half of the circle is formed by:, 1. Anterior communicating artery, 2. Anterior cerebral artery, 3. Internal carotid artery, 4. Posterior communicating artery, 5. Posterior cerebral arteries and the termination of the basilar artery, The circle and its branches supply; the corpus striatum, internal capsule, diencephalon and, midbrain.
Page 1933 :
Image sourced from Wikipedia, , Vertebral arteries, , , , , , Enter the cranial cavity via foramen magnum, Lie in the subarachnoid space, Ascend on anterior surface of medulla oblongata, Unite to form the basilar artery at the base of the pons, , Branches:, , , , , Posterior spinal artery, Anterior spinal artery, Posterior inferior cerebellar artery, , Basilar artery, Branches:
Page 1934 :
, , , , , , Anterior inferior cerebellar artery, Labyrinthine artery, Pontine arteries, Superior cerebellar artery, Posterior cerebral artery, , Internal carotid arteries, Branches:, , , , , , Posterior communicating artery, Anterior cerebral artery, Middle cerebral artery, Anterior choroid artery, Next question
Page 1935 :
Question 374 of 560, An elderly lady falls and lands on her hip. On examination, her hip is tender to palpation and x-rays, are taken. There are concerns that she may have an intertrochanteric fracture. What is the normal, angle between the femoral neck and the femoral shaft?, , 90o, , 105o, , 80o, , 130o, , 180o, , The normal angle between the femoral head and shaft is 130o. Changes to this angle may occur as a, result of disease or pathology and should be investigated., Please rate this question:, , Discuss and give feedback, , Next question, , Hip joint, , , , , , , , Head of femur articulates with acetabulum of the pelvis, Both covered by articular hyaline cartilage, The acetabulum forms at the union of the ilium, pubis, and ischium, The triradiate cartilage (Y-shaped growth plate) separates the pelvic bones, The acetabulum holds the femoral head by the acetabular labrum, Normal angle between femoral head and femoral shaft is 130o, , Ligaments, , , , Transverse ligament: joints anterior and posterior ends of the articular cartilage, Head of femur ligament (ligamentum teres): acetabular notch to the fovea. Contains arterial, supply to head of femur in children.
Page 1937 :
, , Ischiofemoral ligament: posterior support. Ischium to greater trochanter., , Blood supply, Medial circumflex femoral and lateral circumflex femoral arteries (Branches of profunda femoris)., Also from the inferior gluteal artery. These form an anastomosis and travel to up the femoral neck to, supply the head., Next question
Page 1939 :
Image sourced from Wikipedia, , Please rate this question:, , Discuss and give feedback, , Next question, , Deep peroneal nerve
Page 1941 :
Question 376 of 560, A 17 year old male presents to the clinic. He complains of difficulty using his left hand. It has been a, persistent problem since he sustained a distal humerus fracture as a child. On examination there is, diminished sensation overlying the hypothenar eminence and medial one and half fingers. What is, the most likely nerve lesion?, , Anterior interosseous nerve, , Posterior interosseous nerve, , Ulnar nerve, , Median nerve, , Radial nerve, , Theme from April 2012 Exam, This sensory deficit pattern is most consistent with ulnar nerve injury.
Page 1944 :
Branch, , Supplies, , Muscular branch, , Flexor carpi ulnaris, Medial half of the flexor digitorum profundus, , Palmar cutaneous branch (Arises near the, middle of the forearm), , Skin on the medial part of the palm, , Dorsal cutaneous branch, , Dorsal surface of the medial part of the hand, , Superficial branch, , Cutaneous fibres to the anterior surfaces of the, medial one and one-half digits, , Deep branch, , Hypothenar muscles, All the interosseous muscles, Third and fourth lumbricals, Adductor pollicis, Medial head of the flexor pollicis brevis, , Effects of injury, , Damage at the wrist, , , , , , Wasting and paralysis of intrinsic hand muscles (claw hand), Wasting and paralysis of hypothenar muscles, Loss of sensation medial 1 and half fingers, , Damage at the elbow, , , , , Radial deviation of the wrist, Clawing less in 4th and 5th digits, Next question
Page 1945 :
Question 377 of 560, An 18 year old athlete attends orthopaedic clinic reporting pain and swelling over the medial aspect, of the knee joint. The pain occurs when climbing the stairs, but is not present when walking on flat, ground. Clinically there is pain over the medial, proximal tibia and the McMurray test is negative., What is the most likely cause of this patient's symptoms?, , Anterior cruciate ligament tear, , Prepatellar bursitis, , Medial meniscus injury, , Pes Anserinus Bursitis, , Fracture of tibia, Pes anserinus: GOOSE'S FOOT, Combination of sartorius, gracilis and semitendinous tendons inserting into the anteromedial, proximal tibia., Pes Anserinus Bursitis is common in sportsmen due to overuse injuries. The main sign is of pain in, the medial proximal tibia. As the McMurray test is negative, medial meniscal injury is excluded., Please rate this question:, , Discuss and give feedback, , Next question, , Sartorius, , , , Origin, , Longest strap muscle in the body, Most superficial muscle in the anterior compartment of the thigh, , Anterior superior iliac spine
Page 1946 :
Insertion, , Medial surface of the of the body of the tibia (upper part). It inserts anterior to, gracilis and semitendinosus, , Nerve Supply, , Femoral nerve (L2,3), , Action, , Important, relations, , , , , Flexor of the hip and knee, slight abducts the thigh and rotates it laterally, It assists with medial rotation of the tibia on the femur. For example it, would play a pivotal role in placing the right heel onto the left knee ( and, vice versa), , The middle third of this muscle, and its strong underlying fascia forms the roof of, the adductor canal , in which lie the femoral vessels, the saphenous nerve and the, nerve to vastus medialis., Next question
Page 1947 :
Question 378 of 560, Which of the following structures lies most posteriorly at the porta hepatis?, , Cystic artery, , Common hepatic artery, , Left hepatic artery, , Portal vein, , Common bile duct, , The portal vein is the most posterior structure at the porta hepatis.The common bile duct is a, continuation of the common hepatic duct and is formed by the union of the common hepatic duct and, the cystic duct., Please rate this question:, , Discuss and give feedback, , Next question, , Liver, Structure of the liver, , Right lobe, , , , , Supplied by right hepatic artery, Contains Couinaud segments V to VIII (-/+Sg I), , Left lobe, , , , , Supplied by the left hepatic artery, Contains Couinaud segments II to IV (+/- Sg1), , Quadrate lobe, , , , , , , Part of the right lobe anatomically, functionally is part of the left, Couinaud segment IV, Porta hepatis lies behind, On the right lies the gallbladder fossa
Page 1948 :
Caudate lobe, , , , On the left lies the fossa for the umbilical vein, , , , , , , , Supplied by both right and left hepatic arteries, Couinaud segment I, Lies behind the plane of the porta hepatis, Anterior and lateral to the inferior vena cava, Bile from the caudate lobe drains into both right and left hepatic ducts, , Detailed knowledge of Couinaud segments is not required for MRCS, , , Between the liver lobules are portal canals which contain the portal triad: Hepatic Artery,, Portal Vein, tributary of Bile Duct., , Relations of the liver, , Anterior, , Postero inferiorly, , Diaphragm, , Oesophagus, , Xiphoid process, , Stomach, , Duodenum, , Hepatic flexure of colon, , Right kidney, , Gallbladder, , Inferior vena cava, , Porta hepatis
Page 1949 :
Location, , Postero inferior surface, it joins nearly at right angles with the left sagittal fossa, and, separates the caudate lobe behind from the quadrate lobe in front, , Transmits, , , , , , , , Common hepatic duct, Hepatic artery, Portal vein, Sympathetic and parasympathetic nerve fibres, Lymphatic drainage of the liver (and nodes), , Ligaments, , Falciform ligament, , , , , , 2 layer fold peritoneum from the umbilicus to anterior liver surface, Contains ligamentum teres (remnant umbilical vein), On superior liver surface it splits into the coronary and left, triangular ligaments, , Ligamentum teres, , Joins the left branch of the portal vein in the porta hepatis, , Ligamentum, venosum, , Remnant of ductus venosus, , Arterial supply, , , Hepatic artery, , Venous, , , , Hepatic veins, Portal vein, , Nervous supply, , , Sympathetic and parasympathetic trunks of coeliac plexus, Next question
Page 1950 :
Question 379 of 560, , A 76 year old man is undergoing an abdominal aortic aneurysm repair. The surgeons occlude the, aorta with two clamps, the inferior clamp being placed at the point of aortic bifurcation. Which of the, following vertebral bodies will lie posterior to the clamp at this level?, , L1, , T10, , L4, , L5, , L2, , Theme from September 2013 Exam, The aorta bifurcates at L4. An important landmark that is tested frequently., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal aorta, Abdominal aortic topography, , Origin, , T12
Page 1952 :
Image sourced from Wikipedia, , Next question
Page 1953 :
Question 380 of 560, Which of the following statements relating to the greater omentum is false?, , It is less well developed in children under 5., , It has no relationship to the lesser sac., , It contains the gastroepiploic arteries., , Has an attachment to the transverse colon., , It may be a site of metastatic disease in ovarian cancer., , It is connected with the lesser sac and the transverse colon. This plane is entered when performing, a colonic resection. It is a common site of metastasis in many visceral malignancies., Please rate this question:, , Discuss and give feedback, , Next question, , Omentum, , , , , , The omentum is divided into two parts which invest the stomach. Giving rise to the greater, and lesser omentum. The greater omentum is attached to the inferolateral border of the, stomach and houses the gastro-epiploic arteries., It is of variable size but is less well developed in children. This is important as the omentum, confers protection against visceral perforation (e.g. Appendicitis)., Inferiorly between the omentum and transverse colon is one potential entry point into the, lesser sac., Several malignant processes may involve the omentum of which ovarian cancer is the most, notable., Next question
Page 1954 :
Question 381 of 560, , A 48 year old man with newly diagnosed hypertension is found to have a phaeochromocytoma of the, left adrenal gland and is due to undergo a laparoscopic left adrenalectomy. Which of the following, structures is not directly related to the left adrenal gland?, , Crus of the diaphragm, , Lesser curvature of the stomach, , Kidney, , Pancreas, , Splenic artery, , The left adrenal gland is slightly larger than the right. It is crescent in shape and its concavity is, adapted to the medial border of the upper part of the left kidney. The upper area is covered by, peritoneum of the omental bursa which separates it from the cardia of the stomach. The lower area, is in contact with the pancreas and splenic artery and is not covered by peritoneum. On the anterior, surface is a hilum from which the suprarenal vein emerges. The lateral aspect rests on the kidney., The medial is small and is on the left crus of the diaphragm., Please rate this question:, , Discuss and give feedback, , Next question, , Adrenal gland anatomy, Anatomy
Page 1955 :
Location, , Superomedially to the upper pole of each kidney, , Relationships of the right, adrenal, , Diaphragm-Posteriorly, Kidney-Inferiorly, Vena Cava-Medially, Hepato-renal, pouch and bare area of the liver-Anteriorly, , Relationships of the left, adrenal, , Crus of the diaphragm-Postero- medially, Pancreas and splenic vesselsInferiorly, Lesser sac and stomach-Anteriorly, , Arterial supply, , Superior adrenal arteries- from inferior phrenic artery, Middle adrenal, arteries - from aorta, Inferior adrenal arteries -from renal arteries, , Venous drainage of the, right adrenal, , Via one central vein directly into the IVC, , Venous drainage of the, left adrenal, , Via one central vein into the left renal vein, , Next question
Page 1956 :
Question 382 of 560, , Which of the following nerves innervates the long head of the biceps femoris muscle?, , Inferior gluteal nerve, , Tibial division of sciatic nerve, , Superior gluteal nerve, , Common peroneal division of sciatic nerve, , Obturator nerve, , The short head of biceps femoris, which may occasionally be absent, is innervated by the common, peroneal component of the sciatic nerve. The long head is innervated by the tibial division of the, sciatic nerve., Please rate this question:, , Discuss and give feedback, , Next question, , Biceps femoris, The biceps femoris is one of the hamstring group of muscles located in the posterior upper thigh. It, has two heads., Long head, , Origin, , Ischial tuberosity
Page 1957 :
Insertion, , Fibular head, , Action, , Knee flexion, lateral rotation tibia, extension hip, , Innervation, , Tibial division of sciatic nerve (L5, S1, S2), , Arterial, supply, , Profunda femoris artery, inferior gluteal artery, and the superior muscular branches of, popliteal artery, , Image demonstrating the biceps femoris muscle, with the long head outlined, , Image sourced from Wikipedia, , Short head, , Origin, , Lateral lip of linea aspera, lateral supracondylar ridge of femur, , Insertion, , Fibular head
Page 1959 :
Question 383 of 560, , A 72 year old male with end stage critical ischaemia is undergoing an axillo-femoral bypass. What, structure is not closely related to the axillary artery?, , Posterior cord of the brachial plexus, , Scalenus anterior muscle, , Pectoralis minor muscle, , Axillary vein, , Lateral cord of the brachial plexus, , The axillary artery is the continuation of the subclavian artery. It is surrounded by the cords of the, brachial plexus (from which they are named). The axillary vein runs alongside the axillary artery, throughout its length., Please rate this question:, , Discuss and give feedback, , Next question, , Axilla, Boundaries of the axilla, , Medially, , Chest wall and Serratus anterior
Page 1960 :
Laterally, , Humeral head, , Floor, , Subscapularis, , Anterior aspect, , Lateral border of Pectoralis major, , Fascia, , Clavipectoral fascia, , Content:, , Long thoracic nerve (of, Bell), , Derived from C5-C7 and passes behind the brachial plexus to enter the axilla., It lies on the medial chest wall and supplies serratus anterior. Its location, puts it at risk during axillary surgery and damage will lead to winging of the, scapula., , Thoracodorsal nerve and, thoracodorsal trunk, , Innervate and vascularise latissimus dorsi., , Axillary vein, , Lies at the apex of the axilla, it is the continuation of the basilic vein., Becomes the subclavian vein at the outer border of the first rib., , Intercostobrachial nerves, , Traverse the axillary lymph nodes and are often divided during axillary, surgery. They provide cutaneous sensation to the axillary skin., , Lymph nodes, , The axilla is the main site of lymphatic drainage for the breast., Next question
Page 1961 :
Question 384 of 560, A 28 year old man is shot in the right chest and develops a right haemothorax necessitating a, thoracotomy. The surgeons decide to place a vascular clamp across the hilum of the right lung., Which of the following structures will lie most anteriorly at this point?, , Thoracic duct, , Phrenic nerve, , Vagus nerve, , Pulmonary artery, , Pulmonary vein, , The phrenic nerve lies anteriorly at the root of the right lung., Please rate this question:, , Discuss and give feedback, , Next question, , Lung anatomy, The right lung is composed of 3 lobes divided by the oblique and transverse fissures. The left lung, has two lobes divided by the oblique fissure.The apex of both lungs is approximately 4cm superior to, the sterno-costal joint of the first rib. Immediately below this is a sulcus created by the subclavian, artery., Peripheral contact points of the lung, , , , , Base: diaphragm, Costal surface: corresponds to the cavity of the chest, Mediastinal surface: Contacts the mediastinal pleura. Has the cardiac impression. Above and, behind this concavity is a triangular depression named the hilum, where the structures which, form the root of the lung enter and leave the viscus. These structures are invested by pleura,, which, below the hilum and behind the pericardial impression, forms the pulmonary ligament, , Right lung
Page 1962 :
Above the hilum is the azygos vein; Superior to this is the groove for the superior vena cava and, right innominate vein; behind this, and nearer the apex, is a furrow for the innominate artery. Behind, the hilum and the attachment of the pulmonary ligament is a vertical groove for the oesophagus; In, front and to the right of the lower part of the oesophageal groove is a deep concavity for the, extrapericardiac portion of the inferior vena cava., The root of the right lung lies behind the superior vena cava and the right atrium, and below the, azygos vein., The right main bronchus is shorter, wider and more vertical than the left main bronchus and, therefore the route taken by most foreign bodies., , Image sourced from Wikipedia, , Left lung, Above the hilum is the furrow produced by the aortic arch, and then superiorly the groove, accommodating the left subclavian artery; Behind the hilum and pulmonary ligament is a vertical, groove produced by the descending aorta, and in front of this, near the base of the lung, is the lower, part of the oesophagus., The root of the left lung passes under the aortic arch and in front of the descending aorta., , Image sourced from Wikipedia
Page 1963 :
Inferior borders of both lungs, , , , , 6th rib in mid clavicular line, 8th rib in mid axillary line, 10th rib posteriorly, , The pleura runs two ribs lower than the corresponding lung level., Bronchopulmonary segments, , Segment number, , Right lung, , Left lung, , 1, , Apical, , Apical, , 2, , Posterior, , Posterior, , 3, , Anterior, , Anterior, , 4, , Lateral, , Superior lingular, , 5, , Medial, , Inferior lingular, , 6, , Superior (apical), , Superior (apical), , 7, , Medial basal, , Medial basal, , 8, , Anterior basal, , Anterior basal, , 9, , Lateral basal, , Lateral basal, , 10, , Posterior basal, , Posterior basal, Next question
Page 1964 :
Question 385 of 560, An 18 year old boy is undergoing an appendicectomy for appendicitis. At which of the following, locations is the appendix most likely to be found?, , Pre ileal, , Pelvic, , Retrocaecal, , Post ileal, , None of the above, , Most appendixes lie in the retrocaecal position. If a retrocaecal appendix is difficult to remove then, mobilisation of the right colon significantly improves access., Please rate this question:, , Discuss and give feedback, , Next question, , Appendix, , , , , , , , Location: Base of caecum., Up to 10cm long., Mainly lymphoid tissue (Hence mesenteric adenitis may mimic appendicitis)., Caecal taenia coli converge at base of appendix and form a longitudinal muscle cover over, the appendix. This convergence should facilitate its identification at surgery if it is retrocaecal, and difficult to find (which it can be when people start doing appendicectomies!), Arterial supply: Appendicular artery (branch of the ileocolic)., It is intra peritoneal., , McBurney's point, , , 1/3 of the way along a line drawn from the Anterior Superior Iliac Spine to the Umbilicus
Page 1966 :
Question 386 of 560, A 56 year old man is undergoing a pancreatectomy for carcinoma. During resection of the gland, which of the following structures will the surgeon not encounter posterior to the pancreas itself?, , Left crus of the diaphragm, , Superior mesenteric vein, , Common bile duct, , Portal vein, , Gastroduodenal artery, , Theme from 2010 Exam, The gastroduodenal artery divides into the gastro-epiploic and pancreaticoduodenal arteries at the, superior aspect of the pancreas., Please rate this question:, , Discuss and give feedback, , Next question, , Pancreas, The pancreas is a retroperitoneal organ and lies posterior to the stomach. It may be accessed, surgically by dividing the peritoneal reflection that connects the greater omentum to the transverse, colon. The pancreatic head sits in the curvature of the duodenum. Its tail lies close to the hilum of, the spleen, a site of potential injury during splenectomy., Relations, Posterior to the pancreas, , Pancreatic head, , Inferior vena cava, Common bile duct, Right and left renal veins, Superior mesenteric vein and artery
Page 1967 :
Pancreatic neck, , Superior mesenteric vein, portal vein, , Pancreatic body-, , Left renal vein, Crus of diaphragm, Psoas muscle, Adrenal gland, Kidney, Aorta, , Pancreatic tail, , Left kidney, , Anterior to the pancreas, , Pancreatic head, , 1st part of the duodenum, Pylorus, Gastroduodenal artery, SMA and SMV(uncinate process), , Pancreatic body, , Stomach, Duodenojejunal flexure, , Pancreatic tail, , Splenic hilum, , Superior to the pancreas, Coeliac trunk and its branches common hepatic artery and splenic artery, Grooves of the head of the pancreas, 2nd and 3rd part of the duodenum, Arterial supply, , , , Head: pancreaticoduodenal artery, Rest: splenic artery, , Venous drainage, , , , Head: superior mesenteric vein, Body and tail: splenic vein
Page 1968 :
Ampulla of Vater, , , , Merge of pancreatic duct and common bile duct, Is an important landmark, halfway along the second part of the duodenum, that marks the, anatomical transition from foregut to midgut (also the site of transition between regions, supplied by coeliac trunk and SMA)., , Image sourced from Wikipedia, , Next question
Page 1969 :
Question 387 of 560, Which of the following bones is related to the cuboid's distal articular surface?, , All metatarsals, , 5th metatarsal, , Calcaneum, , Medial cuneiform, , 3rd metatarsal, , Theme from April 2012 Exam, The cuboid is located at the lateral aspect of the foot between the calcaneus posteriorly and the 4th, and 5th metatarsals distally., Please rate this question:, , Discuss and give feedback, , Next question, , Foot- anatomy, Arches of the foot, The foot is conventionally considered to have two arches., , , , , The longitudinal arch is higher on the medial than on the lateral side. The posterior part of, the calcaneum forms a posterior pillar to support the arch. The lateral part of this structure, passes via the cuboid bone and the lateral two metatarsal bones. The medial part of this, structure is more important. The head of the talus marks the summit of this arch, located, between the sustentaculum tali and the navicular bone. The anterior pillar of the medial arch, is composed of the navicular bone, the three cuneiforms and the medial three metatarsal, bones., The transverse arch is situated on the anterior part of the tarsus and the posterior part of the, metatarsus. The cuneiforms and metatarsal bases narrow inferiorly, which contributes to the, shape of the arch., , Intertarsal joints
Page 1970 :
Sub talar joint, , Formed by the cylindrical facet on the lower surface of the body of the, talus and the posterior facet on the upper surface of the calcaneus. The, facet on the talus is concave anteroposteriorly, the other is convex. The, synovial cavity of this joint does not communicate with any other joint., , Talocalcaneonavicular, joint, , The anterior part of the socket is formed by the concave articular, surface of the navicular bone, posteriorly by the upper surface of the, sustentaculum tali. The talus sits within this socket, , Calcaneocuboid joint, , Highest point in the lateral part of the longitudinal arch. The lower, aspect of this joint is reinforced by the long plantar and plantar, calcaneocuboid ligaments., , Transverse tarsal joint, , The talocalcaneonavicular joint and the calcaneocuboid joint extend, across the tarsus in an irregular transverse plane, between the talus and, calcaneus behind and the navicular and cuboid bones in front. This, plane is termed the transverse tarsal joint., , Cuneonavicular joint, , Formed between the convex anterior surface of the navicular bone and, the concave surface of the the posterior ends of the three cuneiforms., , Intercuneiform joints, , Between the three cuneiform bones., , Cuneocuboid joint, , Between the circular facets on the lateral cuneiform bone and the, cuboid. This joint contributes to the tarsal part of the transverse arch., , A detailed knowledge of the joints is not required for MRCS Part A. However, the contribution they, play to the overall structure of the foot should be appreciated, Ligaments of the ankle joint and foot
Page 1971 :
Image sourced from Wikipedia, , Muscles of the foot, , Muscle, , Origin, , Insertion, , Nerve, supply, , Action, , Abductor, hallucis, , Medial side of the calcaneus,, flexor retinaculum, plantar, aponeurosis, , Medial side of, the base of the, proximal, phalanx, , Medial, plantar, nerve, , Abducts the great toe, , Flexor, digitorum, brevis, , Medial process of the, calcaneus, plantar, eponeurosis., , Via 4 tendons, into the, middle, phalanges of, the lateral 4, toes., , Medial, plantar, nerve, , Flexes all the joints of, the lateral 4 toes except, for the interphalangeal, joint., , Abductor, digit, minimi, , From the tubercle of the, calcaneus and from the, plantar aponeurosis, , Together with, flexor digit, minimi brevis, into the lateral, side of the, , Lateral, plantar, nerve, , Abducts the little toe at, the metatarsophalangeal, joint
Page 1972 :
base of the, proximal, phalanx of the, little toe, , Flexor, hallucis, brevis, , From the medial side of the, plantar surface of the cuboid, bone, from the adjacent part, of the lateral cuneiform bone, and from the tendon of, tibialis posterior., , Into the, proximal, phalanx of the, great toe, the, tendon, contains a, sesamoid bone, , Medial, plantar, nerve, , Flexes the, metatarsophalangeal, joint of the great toe., , Adductor, hallucis, , Arises from two heads. The, oblique head arises from the, sheath of the peroneus longus, tendon, and from the plantar, surfaces of the bases of the, 2nd, 3rd and 4th metatarsal, bones. The transverse head, arises from the plantar, surface of the lateral 4, metatarsophalangeal joints, and from the deep transverse, metatarsal ligament., , Lateral side of, the base of the, proximal, phalanx of the, great toe., , Lateral, plantar, nerve, , Adducts the great toe, towards the second toe., Helps maintain the, transverse arch of the, foot., , Extensor, digitorum, brevis, , On the dorsal surface of the, foot from the upper surface of, the calcaneus and its, associated fascia, , Via four thin, tendons which, run forward, and medially, to be inserted, into the, medial four, toes. The, lateral three, tendons join, with hoods of, extensor, digitorum, longus., , Deep, peroneal, , Extend the, metatarsophalangeal, joint of the medial four, toes. It is unable to, extend the, interphalangeal joint, without the assistance of, the lumbrical muscles., , Nerves in the foot
Page 1973 :
Lateral plantar nerve, Passes anterolaterally towards the base of the 5th metatarsal between flexor digitorum brevis and, flexor accessorius. On the medial aspect of the lateral plantar artery. At the base of the 5th, metatarsal it splits into superficial and deep branches., Medial plantar nerve, Passes forwards with the medial plantar artery under the cover of the flexor retinaculum to the, interval between abductor hallucis and flexor digitorum brevis on the sole of the foot., Plantar arteries, Arise under the cover of the flexor retinaculum, midway between the tip of the medial malleolus and, the most prominent part of the medial side of the heel., , , , , Medial plantar artery. Passes forwards medial to medial plantar nerve in the space between, abductor hallucis and flexor digitorum brevis.Ends by uniting with a branch of the 1st plantar, metatarsal artery., Lateral plantar artery. Runs obliquely across the sole of the foot. It lies lateral to the lateral, plantar nerve. At the base of the 5th metatarsal bone it arches medially across the foot on, the metatarsals, , Dorsalis pedis artery, This vessel is a direct continuation of the anterior tibial artery. It commences on the front of the ankle, joint and runs to the proximal end of the first metatarsal space. Here is gives off the arcuate artery, and continues forwards as the first dorsal metatarsal artery. It is accompanied by two veins, throughout its length. It is crossed by the extensor hallucis brevis, Next question
Page 1974 :
Question 388 of 560, From which structure is the central tendon of the diaphragm derived?, , Septum transversum, , Pleuroperitoneal folds, , Diaphragmatic crura, , Dorsal mesocardium, , Oropharyngeal membrane, , The septum transversum is a thick ridge of mesodermal tissue in the developing embryo that, separates the thoracic and abdominal cavities and forms the central tendon of the diaphragm., Please rate this question:, , Discuss and give feedback, , Next question, , Embryology of the diaphragm and diaphragmatic hernia, Embryology, The diaphragm is formed between the 5th and 7th weeks of gestation through the progressive fusion, of the septum transversum, pleuroperitoneal folds and via lateral muscular ingrowth. The muscular, origins of the diaphragm are somites located in cervical segments 3 to 5, which accounts for the long, path taken by the phrenic nerve. The components contribute to the following diaphragmatic, segments:, , , , , Septum transversum - Central tendon, Pleuroperitoneal membranes - Parietal membranes surrounding viscera, Cervical somites C5 to C7 - Muscular component of the diaphragm, , Diaphragmatic hernia, , Type of hernia, , Features
Page 1975 :
Type of hernia, , Features, , Morgagni, , Anteriorly located, Minimal compromise on lung development, Minimal signs on antenatal ultrasound, Usually present later, Usually good prognosis, , Bochdalek hernia, , Posteriorly located, Larger defect, Often diagnosed antenatally, Associated with pulmonary hypoplasia, Poor prognosis, , The posterior hernias of Bochdalek are the most common type and if not diagnosed antenatally will, typically present soon after birth with respiratory distress. The classical finding is that of a scaphoid, abdomen on clinical examination because of herniation of the abdominal contents into the chest., Bochdalek hernias are associated with a number of chromosomal abnormalities such as Trisomy 21, and 18. Infants have considerable respiratory distress due to hypoplasia of the developing lung., Historically this was considered to be due to direct compression of the lung by herniated viscera., This view over simplifies the situation and the pulmonary hypoplasia occurs concomitantly with the, hernial development, rather than as a direct result of it. The pulmonary hypoplasia is associated with, pulmonary hypertension and abnormalities of pulmonary vasculature. The pulmonary hypertension, renders infants at risk of right to left shunting (resulting in progressive and worsening hypoxia)., Diagnostic work up of these infants includes chest x-rays/ abdominal ultrasound scans and cardiac, echo., Surgery forms the mainstay of treatment and both thoracic and abdominal approaches may be, utilised. Following reduction of the hernial contents a careful search needs to be made for a hernial, sac as failure to recognise and correct this will result in a high recurrence rate. Smaller defects may, be primarily closed, larger defects may require a patch to close the defect. Malrotation of the viscera, is a recognised association and may require surgical correct at the same procedure (favoring an, abdominal approach)., The mortality rate is 50-75% and is related to the degree of lung compromise and age at, presentation (considerably better in infants >24 hours old)., Next question
Page 1976 :
Question 389 of 560, Where does Stensens duct primarily open?, , Immediately lateral to the foramen caecum, , Floor of mouth, , Opposite the second molar tooth, , Opposite the fifth molar tooth, , Into the post nasal space, , Stensens duct conveys secretions from the parotid gland and these enter the oral cavity at the level, of the second molar tooth., Please rate this question:, , Discuss and give feedback, , Next question, , Parotid gland, Anatomy of the parotid gland, , Location, , Overlying the mandibular ramus; anterior and inferior to the ear., , Salivary duct, , Crosses the masseter, pierces the buccinator and drains adjacent to the, 2nd upper molar tooth (Stensen's duct)., , Structures passing, through the gland, , , , , , , Facial nerve (Mnemonic: The Zebra Buggered My Cat; Temporal, Zygomatic, Buccal, Mandibular, Cervical), External carotid artery, Retromandibular vein, Auriculotemporal nerve
Page 1977 :
Relations, , , , , Anterior: masseter, medial pterygoid, superficial temporal and, maxillary artery, facial nerve, stylomandibular ligament, Posterior: posterior belly digastric muscle, sternocleidomastoid,, stylohyoid, internal carotid artery, mastoid process, styloid, process, , Arterial supply, , Branches of external carotid artery, , Venous drainage, , Retromandibular vein, , Lymphatic drainage, , Deep cervical nodes, , Nerve innervation, , , , , , Parasympathetic-Secretomotor, Sympathetic-Superior cervical ganglion, Sensory- Greater auricular nerve, , Parasympathetic stimulation produces a water rich, serous saliva. Sympathetic stimulation leads to, the production of a low volume, enzyme-rich saliva., Next question
Page 1978 :
Question 390 of 560, Which of the following nerves is responsible for the innervation of the posterior belly of the digastric, muscle?, , Facial nerve, , Hypoglossal nerve, , Trigeminal nerve, , Ansa cervicalis, , Mylohoid nerve, , The posterior belly of digastric is innervated by the facial nerve and the anterior belly by the, mylohoid nerve., Please rate this question:, , Discuss and give feedback, , Next question, , Anterior triangle of the neck, Boundaries, , Anterior border of the Sternocleidomastoid, Lower border of mandible, Anterior midline, , Sub triangles (divided by Digastric above and Omohyoid), , , , , Muscular triangle: Neck strap muscles, Carotid triangle: Carotid sheath, Submandibular Triangle (digastric)
Page 1979 :
Contents of the anterior triangle, , Digastric triangle, , Submandibular gland, Submandibular nodes, Facial vessels, Hypoglossal nerve, , Muscular triangle, , Strap muscles, External jugular vein, , Carotid triangle, , Carotid sheath (Common carotid, vagus and internal jugular vein), Ansa cervicalis, , Nerve supply to digastric muscle, , , , Anterior: Mylohyoid nerve, Posterior: Facial nerve, , Image sourced from Wikipedia, , Next question
Page 1980 :
Question 391 of 560, Which of the following carpal bones is a sesamoid bone in the tendon of flexor carpi ulnaris?, , Triquetrum, , Lunate, , Pisiform, , Scaphoid, , Capitate, , This small bone has a single articular facet. It projects from the triquetral bone at the ulnar aspect of, the wrist where most regard it as a sesamoid bone lying within the tendon of flexor carpi ulnaris., Please rate this question:, , Discuss and give feedback, , Next question, , Carpal bones, The wrist is comprised of 8 carpal bones, these are arranged in two rows of 4. It is convex from side, to side posteriorly and concave anteriorly., Diagrammatic image of carpal bones
Page 1983 :
Question 392 of 560, , A 70 year old man falls and fractures his scaphoid bone. The fracture is displaced and the decision, is made to insert a screw to fix the fracture. Which of the following structures lies directly medial to, the scaphoid?, , Lunate, , Pisiform, , Trapezoid, , Trapezium, , None of the above, , The lunate lies medially in the anatomical plane. Fractures of the scaphoid that are associated with, high velocity injuries may cause associated lunate dislocation., Please rate this question:, , Discuss and give feedback, , Next question, , Scaphoid bone, The scaphoid has a concave articular surface for the head of the capitate and at the edge of this is a, crescentic surface for the corresponding area on the lunate., Proximally, it has a wide convex articular surface with the radius. It has a distally sited tubercle that, can be palpated. The remaining articular surface is to the lateral side of the tubercle. It faces laterally, and is associated with the trapezium and trapezoid bones., The narrow strip between the radial and trapezial surfaces and the tubercle gives rise to the radial
Page 1984 :
collateral carpal ligament. The tubercle receives part of the flexor retinaculum. This area is the only, part of the scaphoid that is available for the entry of blood vessels. It is commonly fractured and, avascular necrosis may result., Scaphoid bone, , Image sourced from Wikipedia, , Next question
Page 1985 :
Question 393 of 560, , A 55 year old man is admitted with a brisk haematemesis. He is taken to the endoscopy department, and an upper GI endoscopy is performed by the gastroenterologist. He identifies an ulcer on the, posterior duodenal wall and spends an eternity trying to control the bleeding with all the latest, haemostatic techniques. He eventually asks the surgeons for help. A laparotomy and anterior, duodenotomy are performed, as the surgeon opens the duodenum a vessel is spurting blood into the, duodenal lumen. From which of the following does this vessel arise?, , Left gastric artery, , Common hepatic artery, , Right hepatic artery, , Superior mesenteric artery, , Splenic artery, , The vessel will be the gastroduodenal artery, this arises from the common hepatic artery., Please rate this question:, , Discuss and give feedback, , Next question, , Gastroduodenal artery, Supplies, Pylorus, proximal part of the duodenum, and indirectly to the pancreatic head (via the anterior and, posterior superior pancreaticoduodenal arteries), Path
Page 1986 :
Most commonly arises from the common hepatic artery of the coeliac trunk, Terminates by bifurcating into the right gastroepiploic artery and the superior pancreaticoduodenal, artery, Image showing stomach reflected superiorly to illustrate the relationship of the gastroduodenal artery, to the first part of the duodenum, , Image sourced from Wikipedia, , Next question
Page 1987 :
Question 394 of 560, A 73 year old lady is hit by a car. She suffers a complex fracture of the distal aspect of her humerus, with associated injury to the radial nerve. Which of the following movements will be most impaired as, a result?, , Elbow extension, , Elbow flexion, , Shoulder abduction, , Wrist extension, , None of the above, , The triceps will not be affected so elbow extension will be preserved. Loss of wrist extension will be, the most obvious effect., Please rate this question:, , Discuss and give feedback, , Next question, , Radial nerve, Continuation of posterior cord of the brachial plexus (root values C5 to T1), Path, , , , , , , , In the axilla: lies posterior to the axillary artery on subscapularis, latissimus dorsi and teres, major., Enters the arm between the brachial artery and the long head of triceps (medial to humerus)., Spirals around the posterior surface of the humerus in the groove for the radial nerve., At the distal third of the lateral border of the humerus it then pierces the intermuscular, septum and descends in front of the lateral epicondyle., At the lateral epicondyle it lies deeply between brachialis and brachioradialis where it then, divides into a superficial and deep terminal branch., Deep branch crosses the supinator to become the posterior interosseous nerve.
Page 1989 :
Anatomical, location, , Muscle affected, , Effect of paralysis, , Shoulder, , Long head of triceps, , Minor effects on shoulder stability in abduction, , Arm, , Triceps, , Loss of elbow extension, , Forearm, , Supinator, Brachioradialis, Extensor carpi radialis, longus and brevis, , Weakening of supination of prone hand and, elbow flexion in mid prone position, , The cutaneous sensation of the upper limb- illustrating the contribution of the radial nerve, , Image sourced from Wikipedia, , Next question
Page 1990 :
Question 395 of 560, Which of the following is not a content of the rectus sheath?, , Pyramidalis, , Superior epigastric artery, , Inferior epigastric vein, , Internal iliac artery, , Rectus abdominis, , The rectus sheath also contains:, superior epigastric vein, inferior epigastric artery, Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal wall, The 2 main muscles of the abdominal wall are the rectus abdominis (anterior) and the quadratus, lumborum (posterior)., The remaining abdominal wall consists of 3 muscular layers. Each muscle passes from the lateral, aspect of the quadratus lumborum posteriorly to the lateral margin of the rectus sheath anteriorly., Each layer is muscular posterolaterally and aponeurotic anteriorly., , Image sourced from Wikipedia
Page 1991 :
Muscles of abdominal wall, , External, oblique, , , , , , , , , Internal, oblique, , , , , , , Transversus, abdominis, , , , , , , , , , , Lies most superficially, Originates from 5th to 12th ribs, Inserts into the anterior half of the outer aspect of the iliac crest, linea, alba and pubic tubercle, More medially and superiorly to the arcuate line, the aponeurotic layer, overlaps the rectus abdominis muscle, The lower border forms the inguinal ligament, The triangular expansion of the medial end of the inguinal ligament is, the lacunar ligament., Arises from the thoracolumbar fascia, the anterior 2/3 of the iliac crest, and the lateral 2/3 of the inguinal ligament, The muscle sweeps upwards to insert into the cartilages of the lower 3, ribs, The lower fibres form an aponeurosis that runs from the tenth costal, cartilage to the body of the pubis, At its lowermost aspect it joins the fibres of the aponeurosis of, transversus abdominis to form the conjoint tendon., Innermost muscle, Arises from the inner aspect of the costal cartilages of the lower 6 ribs ,, from the anterior 2/3 of the iliac crest and lateral 1/3 of the inguinal, ligament, Its fibres run horizontally around the abdominal wall ending in an, aponeurosis. The upper part runs posterior to the rectus abdominis., Lower down the fibres run anteriorly only., The rectus abdominis lies medially; running from the pubic crest and, symphysis to insert into the xiphoid process and 5th, 6th and 7th costal, cartilages. The muscles lies in a aponeurosis as described above., Nerve supply: anterior primary rami of T7-12, , Surgical notes, During abdominal surgery it is usually necessary to divide either the muscles or their aponeuroses., During a midline laparotomy it is desirable to divide the aponeurosis. This will leave the rectus, sheath intact above the arcuate line and the muscles intact below it. Straying off the midline will, often lead to damage to the rectus muscles, particularly below the arcuate line where they may often, be in close proximity to each other., Next question
Page 1992 :
Question 396 of 560, Which of the following vessels does not drain directly into the inferior vena cava?, , Superior mesenteric vein, , Right common iliac, , Right hepatic vein, , Left hepatic vein, , Right testicular vein, , The superior mesenteric vein drains into the portal vein. The right and left hepatic veins drain into it, directly, this can account for major bleeding in more extensive liver shearing type injuries., Please rate this question:, , Discuss and give feedback, , Next question, , Inferior vena cava, Origin, , , L5, , Path, , , , , , , , , Left and right common iliac veins merge to form the IVC., Passes right of midline, Paired segmental lumbar veins drain into the IVC throughout its length, The right gonadal vein empties directly into the cava and the left gonadal vein generally, empties into the left renal vein., The next major veins are the renal veins and the hepatic veins, Pierces the central tendon of diaphragm at T8, Right atrium
Page 1993 :
Image sourced from Wikipedia, , Relations, , Anteriorly, , Small bowel, first and third part of duodenum, head of pancreas, liver and bile duct,, right common iliac artery, right gonadal artery, , Posteriorly, , Right renal artery, right psoas, right sympathetic chain, coeliac ganglion, , Levels, , Level, , Vein, , T8, , Hepatic vein, inferior phrenic vein, pierces diaphragm, , L1, , Suprarenal veins, renal vein, , L2, , Gonadal vein, , L1-5, , Lumbar veins
Page 1995 :
Question 397 of 560, A 17 year old male has a suspected testicular torsion and the scrotum is to be explored surgically., The surgeon incises the skin and then the dartos muscle. What is the next tissue layer that will be, encountered during the dissection?, , Visceral layer of the tunica vaginalis, , Cremasteric fascia, , Parietal layer of the tunica vaginalis, , External spermatic fascia, , Internal spermatic fascia, , The layers that will be encountered are (in order):, 1. Skin, 2. Dartos fascia and muscle, 3. External spermatic fascia, 4. Cremasteric muscle and fascia, 5. Internal spermatic fascia, 6. Parietal layer of the tunica vaginalis, The layers of the spermatic cord and scrotum are a popular topic in the MRCS exam., Please rate this question:, , Discuss and give feedback, , Next question, , Scrotal and testicular anatomy, Spermatic cord, Formed by the vas deferens and is covered by the following structures:, , Layer, , Origin, , Internal spermatic fascia, , Transversalis fascia
Page 1996 :
Layer, , Origin, , Cremasteric fascia, , From the fascial coverings of internal oblique, , External spermatic fascia, , External oblique aponeurosis, , Contents of the cord, , Vas deferens, , Transmits sperm and accessory gland secretions, , Testicular artery, , Branch of abdominal aorta supplies testis and, epididymis, , Artery of vas deferens, , Arises from inferior vesical artery, , Cremasteric artery, , Arises from inferior epigastric artery, , Pampiniform plexus, , Venous plexus, drains into right or left testicular vein, , Sympathetic nerve fibres, , Lie on arteries, the parasympathetic fibres lie on the, vas, , Genital branch of the genitofemoral, nerve, , Supplies cremaster, , Lymphatic vessels, , Drain to lumbar and para-aortic nodes, , Scrotum, , , , , , Composed of skin and closely attached dartos fascia., Arterial supply from the anterior and posterior scrotal arteries, Lymphatic drainage to the inguinal lymph nodes, Parietal layer of the tunica vaginalis is the innermost layer
Page 1997 :
Testes, , , , , , The testes are surrounded by the tunica vaginalis (closed peritoneal sac). The parietal layer, of the tunica vaginalis adjacent to the internal spermatic fascia., The testicular arteries arise from the aorta immediately inferiorly to the renal arteries., The pampiniform plexus drains into the testicular veins, the left drains into the left renal vein, and the right into the inferior vena cava., Lymphatic drainage is to the para-aortic nodes., Next question
Page 1998 :
Question 398 of 560, A 25 year old man is stabbed in the groin and the area, which lies within the femoral triangle is, explored. Which structure forms the lateral wall of the femoral triangle?, , Adductor longus, , Pectineus, , Adductor magnus, , Sartorius, , Conjoint tendon, , The sartorius forms the lateral wall of the femoral triangle (see below)., Please rate this question:, , Discuss and give feedback, , Next question, , Femoral triangle anatomy, Boundaries, , Superiorly, , Inguinal ligament, , Laterally, , Sartorius, , Medially, , Adductor longus, , Floor, , Iliopsoas, adductor longus and pectineus, , Roof, , , , , Fascia lata and Superficial fascia, Superficial inguinal lymph nodes (palpable below the inguinal ligament)
Page 1999 :
, , Long saphenous vein, , Image sourced from Wikipedia, , Contents, , , , , , , , , Femoral vein (medial to lateral), Femoral artery-pulse palpated at the mid inguinal point, Femoral nerve, Deep and superficial inguinal lymph nodes, Lateral cutaneous nerve, Great saphenous vein, Femoral branch of the genitofemoral nerve, Next question
Page 2000 :
Question 399 of 560, An 18 year old man develops a severe spreading sepsis of the hand. The palm is explored surgically, and the flexor digiti minimi brevis muscle is mobilised to facilitate drainage of the infection. Which of, the following structures is not closely related to this muscle?, , The hook of hamate, , Median nerve, , Superficial palmar arterial arch, , Digital nerves arising from the ulnar nerve, , None of the above, , The flexor digiti minimi brevis originates from the Hamate, on its under- surface lie the ulnar, contribution to the superficial palmar arterial arch and digital nerves derived from the ulnar nerve., The median nerve overlies the flexor tendons., Please rate this question:, , Discuss and give feedback, , Next question, , Hand, Anatomy of the hand, , Bones, , Intrinsic Muscles, , , , , , 8 Carpal bones, 5 Metacarpals, 14 phalanges, , 7 Interossei - Supplied by ulnar nerve, , , , 3 palmar-adduct fingers, 4 dorsal- abduct fingers
Page 2002 :
The fascia of the palm is continuous with the antebrachial fascia and the fascia of the dorsum of the, hand. The palmar fascia is thin over the thenar and hypothenar eminences. In contrast the palmar, fascia is relatively thick. The palmar aponeurosis covers the soft tissues and overlies the flexor, tendons. The apex of the palmar aponeurosis is continuous with the flexor retinaculum and the, palmaris longus tendon. Distally, it forms four longitudinal digital bands that attach to the bases of, the proximal phalanges, blending with the fibrous digital sheaths., A medial fibrous septum extends deeply from the medial border of the palmar aponeurosis to the 5th, metacarpal. Lying medial to this are the hypothenar muscles. In a similar fashion, a lateral fibrous, septum extends deeply from the lateral border of the palmar aponeurosis to the 3rd metacarpal. The, thenar compartment lies lateral to this area., Lying between the thenar and hypothenar compartments is the central compartment. It contains the, flexor tendons and their sheaths, the lumbricals, the superficial palmar arterial arch and the digital, vessels and nerves., The deepest muscular plane is the adductor compartment, which contains adductor pollicis., Short muscles of the hand, These comprise the lumbricals and interossei. The four slender lumbrical muscles flex the fingers at, the metacarpophalangeal joints and extend the interphalangeal joint. The four dorsal interossei are, located between the metacarpals and the four palmar interossei lie on the palmar surface of the, metacarpals in the interosseous compartment of the hand., Long flexor tendons and sheaths in the hand, The tendons of FDS and FDP enter the common flexor sheath deep to the flexor retinaculum. The, tendons enter the central compartment of the hand and fan out to their respective digital synovial, sheaths. Near the base of the proximal phalanx, the tendon of FDS splits to permit the passage of, FDP. The FDP tendons are attached to the margins of the anterior aspect of the base of the distal, phalanx., The fibrous digital sheaths contain the flexor tendons and their synovial sheaths. These extend from, the heads of the metacarpals to the base of the distal phalanges., Next question
Page 2003 :
Question 400 of 560, A 19 year old man undergoes an open inguinal hernia repair. The cord is mobilised and the deep, inguinal ring identified. Which of the following structures forms its lateral wall?, , External oblique aponeurosis, , Transversalis fascia, , Conjoint tendon, , Inferior epigastric artery, , Inferior epigastric vein, , The transversalis fascia forms the superolateral edge of the deep inguinal ring. The epigastric, vessels form its inferomedial wall., Please rate this question:, , Discuss and give feedback, , Next question, , Inguinal canal, Location, , , , , , Above the inguinal ligament, The inguinal canal is 4cm long, The superficial ring is located anterior to the pubic tubercle, The deep ring is located approximately 1.5-2cm above the half way point between the, anterior superior iliac spine and the pubic tubercle, , Boundaries of the inguinal canal, , Floor, , , , , , External oblique aponeurosis, Inguinal ligament, Lacunar ligament
Page 2004 :
, , , Roof, , Anterior wall, , Internal oblique, Transversus abdominis, , External oblique aponeurosis, , Posterior wall, , , , , Transversalis fascia, Conjoint tendon, , Laterally, , , , , Internal ring, Fibres of internal oblique, , Medially, , , , , External ring, Conjoint tendon, , Contents, , Males, , Spermatic cord and ilioinguinal, nerve, , As it passes through the canal the spermatic cord, has 3 coverings:, , , , , Females, , External spermatic fascia from external, oblique aponeurosis, Cremasteric fascia, Internal spermatic fascia, , Round ligament of uterus and, ilioinguinal nerve, , Related anatomy of the inguinal region, The boundaries of Hesselbachs triangle are commonly tested and illustrated below:
Page 2005 :
Image sourced from Wikipedia, , The image below demonstrates the close relationship of the vessels to the lower limb with the, inguinal canal. A fact to be borne in mind when repairing hernial defects in this region., , Image sourced from Wikipedia, , Next question
Page 2007 :
Question 401 of 560, A 22 year old man develops an infection in the pulp of his little finger. What is the most proximal site, to which this infection may migrate?, , The metacarpophalangeal joint, , The distal interphalangeal joint, , The proximal interphalangeal joint, , Proximal to the flexor retinaculum, , Immediately distal to the carpal tunnel, , The 5th tendon sheath extends from the little finger to the proximal aspect of the carpal tunnel. This, carries a significant risk of allowing infections to migrate proximally., Please rate this question:, , Discuss and give feedback, , Next question, , Hand, Anatomy of the hand, , Bones, , Intrinsic Muscles, , , , , , 7 Interossei - Supplied by ulnar nerve, , , , Intrinsic muscles, , 8 Carpal bones, 5 Metacarpals, 14 phalanges, , 3 palmar-adduct fingers, 4 dorsal- abduct fingers, , Lumbricals
Page 2009 :
hand. The palmar fascia is thin over the thenar and hypothenar eminences. In contrast the palmar, fascia is relatively thick. The palmar aponeurosis covers the soft tissues and overlies the flexor, tendons. The apex of the palmar aponeurosis is continuous with the flexor retinaculum and the, palmaris longus tendon. Distally, it forms four longitudinal digital bands that attach to the bases of, the proximal phalanges, blending with the fibrous digital sheaths., A medial fibrous septum extends deeply from the medial border of the palmar aponeurosis to the 5th, metacarpal. Lying medial to this are the hypothenar muscles. In a similar fashion, a lateral fibrous, septum extends deeply from the lateral border of the palmar aponeurosis to the 3rd metacarpal. The, thenar compartment lies lateral to this area., Lying between the thenar and hypothenar compartments is the central compartment. It contains the, flexor tendons and their sheaths, the lumbricals, the superficial palmar arterial arch and the digital, vessels and nerves., The deepest muscular plane is the adductor compartment, which contains adductor pollicis., Short muscles of the hand, These comprise the lumbricals and interossei. The four slender lumbrical muscles flex the fingers at, the metacarpophalangeal joints and extend the interphalangeal joint. The four dorsal interossei are, located between the metacarpals and the four palmar interossei lie on the palmar surface of the, metacarpals in the interosseous compartment of the hand., Long flexor tendons and sheaths in the hand, The tendons of FDS and FDP enter the common flexor sheath deep to the flexor retinaculum. The, tendons enter the central compartment of the hand and fan out to their respective digital synovial, sheaths. Near the base of the proximal phalanx, the tendon of FDS splits to permit the passage of, FDP. The FDP tendons are attached to the margins of the anterior aspect of the base of the distal, phalanx., The fibrous digital sheaths contain the flexor tendons and their synovial sheaths. These extend from, the heads of the metacarpals to the base of the distal phalanges., Next question
Page 2012 :
Branch, , Supplies, , Palmar cutaneous branch (Arises near the, middle of the forearm), , Skin on the medial part of the palm, , Dorsal cutaneous branch, , Dorsal surface of the medial part of the hand, , Superficial branch, , Cutaneous fibres to the anterior surfaces of the, medial one and one-half digits, , Deep branch, , Hypothenar muscles, All the interosseous muscles, Third and fourth lumbricals, Adductor pollicis, Medial head of the flexor pollicis brevis, , Effects of injury, , Damage at the wrist, , , , , , Wasting and paralysis of intrinsic hand muscles (claw hand), Wasting and paralysis of hypothenar muscles, Loss of sensation medial 1 and half fingers, , Damage at the elbow, , , , , Radial deviation of the wrist, Clawing less in 4th and 5th digits, Next question
Page 2013 :
Question 403 of 560, During an inguinal hernia repair the surgeon identifies a small nerve whilst mobilising the cord, structures at the level of the superficial inguinal ring. Which nerve is this most likely to be?, , Subcostal, , Iliohypogastric, , Ilioinguinal, , Obturator, , Pudendal, Ilioinguinal nerve entrapment may be a cause of neuropathic pain following inguinal hernia surgery., The ilioinguinal nerve passes through the superfical inguinal ring and is routinely encountered when, exploring the inguinal canal during hernia surgery. The iliohypogastric nerve pierces the aponeurosis, of the external oblique muscle superior to the superficial inguinal ring., Please rate this question:, , Discuss and give feedback, , Next question, , Ilioinguinal nerve, Arises from the first lumbar ventral ramus with the iliohypogastric nerve. It passes inferolaterally, through the substance of psoas major and over the anterior surface of quadratus lumborum. It, pierces the internal oblique muscle and passes deep to the aponeurosis of the external oblique, muscle. It enters the inguinal canal and then passes through the superficial inguinal ring to reach the, skin., Branches, , , , To supply those muscles of the abdominal wall through which it passes., Skin and fascia over the pubic symphysis, superomedial part of the femoral triangle, surface, of the scrotum, root and dorsum of penis or labum majus in females., Next question
Page 2014 :
Question 404 of 560, From which of the following structures does the anterior cruciate ligament originate?, , Posterolateral aspect of the lateral femoral condyle, , Anterior intercondylar area of tibia, , Posterolateral aspect of the medial femoral condyle, , Posteromedial aspect of the medial femoral condyle, , Posterior intercondylar area of tibia, , The anterior cruciate ligament is attached to the anterior intercondylar area of the tibia. Is then, passes posterolaterally to insert into the posteromedial aspect of the lateral femoral condyle., Please rate this question:, , Discuss and give feedback, , Next question, , Knee joint, The knee joint is a synovial joint, the largest and most complicated. It consists of two condylar joints, between the femur and tibia and a sellar joint between the patella and the femur. The tibiofemoral, articular surfaces are incongruent, however, this is improved by the presence of the menisci. The, degree of congruence is related to the anatomical position of the knee joint and is greatest in full, extension., Knee joint compartments, , Tibiofemoral, , , , Patellofemoral, , , , , Comprised of the patella/femur joint, lateral and medial compartments, (between femur condyles and tibia), Synovial membrane and cruciate ligaments partially separate the medial, and lateral compartments, , Ligamentum patellae, Actions: provides joint stability in full extension
Page 2015 :
Fibrous capsule, The capsule of the knee joint is a complex, composite structure with contributions from adjacent, tendons., Anterior, fibres, , The capsule does not pass proximal to the patella. It blends with the tendinous, expansions of vastus medialis and lateralis, , Posterior, fibres, , These fibres are vertical and run from the posterior surface of the femoral condyles, to the posterior aspect of the tibial condyle, , Medial fibres, , Attach to the femoral and tibial condyles beyond their articular margins, blending, with the tibial collateral ligament, , Lateral, fibres, , Attach to the femur superior to popliteus, pass over its tendon to head of fibula and, tibial condyle, , Bursae, , Anterior, , Laterally, , Medially, , Posterior, , , , , , Subcutaneous prepatellar bursa; between patella and skin, Deep infrapatellar bursa; between tibia and patellar ligament, Subcutaneous infrapatellar bursa; between distal tibial tuberosity and skin, , , , , , Bursa between lateral head of gastrocnemius and joint capsule, Bursa between fibular collateral ligament and tendon of biceps femoris, Bursa between fibular collateral ligament and tendon of popliteus, , , , , Bursa between medial head of gastrocnemius and the fibrous capsule, Bursa between tibial collateral ligament and tendons of sartorius, gracilis and, semitendinosus, Bursa between the tendon of semimembranosus and medial tibial condyle and, medial head of gastrocnemius, , , , Highly variable and inconsistent, , Ligaments, , Medial collateral, ligament, , Medial epicondyle femur to medial tibial condyle: valgus stability, , Lateral collateral, ligament, , Lateral epicondyle femur to fibula head: varus stability, , Anterior cruciate, , Anterior tibia to lateral intercondylar notch femur: prevents tibia sliding
Page 2016 :
ligament, , anteriorly, , Posterior cruciate, ligament, , Posterior tibia to medial intercondylar notch femur: prevents tibia, sliding posteriorly, , Patellar ligament, , Central band of the tendon of quadriceps femoris, extends from patella, to tibial tuberosity, , Image sourced from Wikipedia
Page 2017 :
Image sourced from Wikipedia, , © Image provided by the University of Sheffield, , Menisci, Medial and lateral menisci compensate for the incongruence of the femoral and tibial condyles., Composed of fibrous tissue., Medial meniscus is attached to the tibial collateral ligament., Lateral meniscus is attached to the loose fibres at the lateral edge of the joint and is separate from, the fibular collateral ligament. The lateral meniscus is crossed by the popliteus tendon.
Page 2018 :
Nerve supply, The knee joint is supplied by the femoral, tibial and common peroneal divisions of the sciatic and by, a branch from the obturator nerve. Hip pathology pain may be referred to the knee., Blood supply, Genicular branches of the femoral artery, popliteal and anterior tibial arteries all supply the knee, joint., Next question
Page 2019 :
Question 405 of 560, During an arch aortogram the brachiocephalic artery is entered with an angiography catheter. The, radiologist continues to advance the catheter. Into which of the following vessels is it likely to enter?, , Left subclavian artery, , Left axillary artery, , Right subclavian artery, , Right axillary artery, , None of the above, , The axillary artery is a branch of the subclavian artery and although developmental anomalies may, occur they are rare. The catheter may also enter the right carotid. There is no brachiocephalic artery, on the left side., Please rate this question:, , Discuss and give feedback, , Next question, , Brachiocephalic artery, The brachiocephalic artery is the largest branch of the aortic arch. From its aortic origin it ascends, superiorly, it initially lies anterior to the trachea and then on its right hand side. It branches into the, common carotid and right subclavian arteries at the level of the sternoclavicular joint., Path, Origin- apex of the midline of the aortic arch, Passes superiorly and posteriorly to the right, Divides into the right subclavian and right common carotid artery, Relations, , Anterior, , , , , , , Sternohyoid, Sternothyroid, Thymic remnants, Left brachiocephalic vein
Page 2020 :
, , Right inferior thyroid veins, , Posterior, , , , , Trachea, Right pleura, , Right lateral, , , , , Right brachiocephalic vein, Superior part of SVC, , Left lateral, , , , , , , Thymic remnants, Origin of left common carotid, Inferior thyroid veins, Trachea (higher level), , Branches, Normally none but may have the thyroidea ima artery, , Image sourced from Wikipedia, , Next question
Page 2021 :
Question 406 of 560, Which of the following structures lie between the lateral and medial heads of the triceps muscle?, , Radial nerve, , Median nerve, , Ulnar nerve, , Axillary nerve, , Medial cutaneous nerve of the forearm, , The radial nerve runs in its groove on between the two heads. The ulnar nerve lies anterior to the, medial head. The axillary nerve passes through the quadrangular space. This lies superior to lateral, head of the triceps muscle and thus the lateral border of the quadrangular space is the humerus., Therefore the correct answer is the radial nerve., Please rate this question:, , Discuss and give feedback, , Next question, , Triceps, Origin, , , , , , Insertion, , , , , Long head- infraglenoid tubercle of the scapula., Lateral head- dorsal surface of the humerus, lateral and proximal to the, groove of the radial nerve, Medial head- posterior surface of the humerus on the inferomedial side of, the radial groove and both of the intermuscular septae, Olecranon process of the ulna. Here the olecranon bursa is between the, triceps tendon and olecranon., Some fibres insert to the deep fascia of the forearm, posterior capsule of the, elbow (preventing the capsule from being trapped between olecranon and, olecranon fossa during extension)
Page 2022 :
Innervation, , Radial nerve, , Blood, supply, , Profunda brachii artery, , Action, , Elbow extension. The long head can adduct the humerus and and extend it from a, flexed position, , Relations, , The radial nerve and profunda brachii vessels lie between the lateral and medial, heads, Next question
Page 2023 :
Question 407 of 560, Into which of the following structures does the superior part of the fibrous capsule of the shoulder, joint insert?, , The surgical neck of the humerus, , The body of the humerus, , The bicipital groove, , Immediately distal to the greater tuberosity, , The anatomical neck of the humerus, , The shoulder joint is a shallow joint, hence its great mobility. However, this comes at the expense of, stability. The fibrous capsule attaches to the anatomical neck superiorly and the surgical neck, inferiorly, Please rate this question:, , Discuss and give feedback, , Next question, , Shoulder joint, , , , , Shallow synovial ball and socket type of joint., It is an inherently unstable joint, but is capable to a wide range of movement., Stability is provided by muscles of the rotator cuff that pass from the scapula to insert in the, greater tuberosity (all except sub scapularis-lesser tuberosity)., , Glenoid labrum, , , , , Fibrocartilaginous rim attached to the free edge of the glenoid cavity, Tendon of the long head of biceps arises from within the joint from the supraglenoid tubercle,, and is fused at this point to the labrum., The long head of triceps attaches to the infraglenoid tubercle
Page 2026 :
Question 408 of 560, , A 34 year old lady presents with symptoms of faecal incontinence. Ten years previously she gave, birth to a child by normal vaginal delivery. Injury to which of the following nerves is most likely to, account for this process?, , Genitofemoral, , Ilioinguinal, , Pudendal, , Hypogastric autonomic nerve, , Obturator, S2,3,4 keeps the poo up off the floor - POOdendal nerve, , Theme from April 2013 Exam, Damage to the pudendal nerve is classically associated with faecal incontinence and it is for this, reason that sacral neuromodulation is a popular treatment for the condition. Injury to the hypogastric, autonomic nerves is an aetiological factor in the development of constipation., Please rate this question:, , Discuss and give feedback, , Next question, , Pudendal nerve, The pudendal nerve arises from nerve roots S2, S3 and S4 and exits the pelvis through the greater, sciatic foramen. It re-enters the perineum through the lesser sciatic foramen. It travels inferior to give, innervation to the anal sphincters and external urethral sphincter. It also provides cutaneous
Page 2027 :
innervation to the region of perineum surrounding the anus and posterior vulva., Traction and compression of the pudendal nerve by the foetus in late pregnancy may result in late, onset pudendal neuropathy which may be part of the process involved in the development of faecal, incontinence., Next question
Page 2028 :
Question 409 of 560, During a difficult thyroidectomy haemorrhage is noted from the thyroidea ima vessel. From which, structure does this vessel usually arise?, , External carotid artery, , Internal carotid artery, , Brachiocephalic artery, , Axillary artery, , Superior thyroid artery, Rhyme isthmus location:, Rings 2,3,4 make the isthmus floor, This accessory vessel which usually lies at the inferior aspect of the gland is derived either from the, brachiocephalic artery or the arch of the aorta., Please rate this question:, , Discuss and give feedback, , Next question, , Thyroid gland, , , , , , , , Right and left lobes connected by isthmus, Surrounded by sheath from pretracheal layer of deep fascia, Apex: Lamina of thyroid cartilage, Base: 4th-5th tracheal ring, Pyramidal lobe: from isthmus, May be attached to foramen caecum at the base of the tongue, , Relations, , Anteromedially, , , , , , Sternothyroid, Superior belly of omohyoid, Sternohyoid
Page 2029 :
, , Posterolaterally, , Anterior aspect of sternocleidomastoid, , Carotid sheath, , Medially, , , , , , , , , , Larynx, Trachea, Pharynx, Oesophagus, Cricothyroid muscle, External laryngeal nerve (near superior thyroid artery), Recurrent laryngeal nerve (near inferior thyroid artery), , Posterior, , , , , Parathyroid glands, Anastomosis of superior and inferior thyroid arteries, , Isthmus, , , , , Anteriorly: Sternothyroids, sternohyoids, anterior jugular veins, Posteriorly: 2nd, 3rd, 4th tracheal rings (attached via Ligament of, Berry), , Blood Supply, , Arterial, , , , , , Superior thyroid artery (1st branch of external carotid), Inferior thyroid artery (from thyrocervical trunk), Thyroidea ima (in 10% of population -from brachiocephalic artery or aorta), , Venous, , , , , Superior and middle thyroid veins - into the IJV, Inferior thyroid vein - into the brachiocephalic veins, Next question
Page 2030 :
Question 410 of 560, A 49 year old man undergoes a low anterior resection for cancer. He is assessed in the outpatient, clinic post operatively. His wounds are well healed. However, he complains of impotence. Which of, the following best explains this problem?, , Sciatic nerve injury, , Damage to the internal iliac artery, , Damage to the nervi erigentes, , Damage to the vas, , Damage to the genitofemoral nerve, , Theme from 2012 Exam, The penis takes autonomic nerves from the nervi erigentes that lie near the seminal vesicles. These, may be compromised by direct surgical trauma (such as use of diathermy in this area) and also by, radiotherapy that is used in these patients pre operatively. The result is that up to 50% of patients, may develop impotence following rectal cancer surgery., Please rate this question:, , Discuss and give feedback, , Next question, , Penile erection, Physiology of erection, , Autonomic, , , , , Somatic, nerves, , Sympathetic nerves originate from T11-L2 and parasympathetic nerves, from S2-4 join to form pelvic plexus., Parasympathetic discharge causes erection, sympathetic discharge causes, ejaculation and detumescence., , Supplied by dorsal penile and pudendal nerves. Efferent signals are relayed from, Onufs nucleus (S2-4) to innervate ischiocavernosus and bulbocavernosus muscles., , Autonomic discharge to the penis will trigger the veno-occlusive mechanism which triggers the flow
Page 2031 :
of arterial blood into the penile sinusoidal spaces. As the inflow increases the increased volume in, this space will secondarily lead to compression of the subtunical venous plexus with reduced venous, return. During the detumesence phase the arteriolar constriction will reduce arterial inflow and, thereby allow venous return to normalise., Priapism, Prolonged unwanted erection, in the absence of sexual desire, lasting more than 4 hours., Classification of priaprism, , Low flow priaprism, , Due to veno-occlusion (high intracavernosal pressures)., , , , , , High flow priaprism, , Due to unregulated arterial blood flow., , , Recurrent priaprism, , Most common type, Often painful, Often low cavernosal flow, If present for >4 hours requires emergency treatment, , Usually presents as semi rigid painless erection, , Typically seen in sickle cell disease, most commonly of high flow type., , Causes, , , , , , Intracavernosal drug therapies (e.g. for erectile dysfunction>, Blood disorders such as leukaemia and sickle cell disease, Neurogenic disorders such as spinal cord transection, Trauma to penis resulting in arterio-venous malformations, , Tests, , , , Exclude sickle cell/ leukaemia, Consider blood sampling from cavernosa to determine whether high or low flow (low flow is, often hypoxic), , Management, , , , Ice packs/ cold showers, If due to low flow then blood may be aspirated from copora or try intracavernosal alpha, adrenergic agonists.
Page 2032 :
, , Delayed therapy of low flow priaprism may result in erectile dysfunction., Next question
Page 2033 :
Question 411 of 560, The cephalic vein pierces the clavipectoral fascia to terminate in which of the veins listed below?, , External jugular, , Axillary, , Internal jugular, , Azygos, , Brachial, , Please rate this question:, , Discuss and give feedback, , Next question, , Cephalic vein, Path, , , , , , Dorsal venous arch drains laterally into the cephalic vein, Crosses the anatomical snuffbox and travels laterally up the arm, At the antecubital fossa connected to the basilic vein by the median cubital vein, Pierces deep fascia of deltopectoral groove to join axillary vein, Next question
Page 2034 :
Question 412 of 560, , A 43 year old lady develops a cerebello-pontine angle lesion. Which of the nerves listed below is, likely to be affected first?, , CN X, , CN III, , CN V, , CN IX, , CN XII, , Theme from September 2013 Exam, The most likely lesion to occur in the cerebello-pontine angle is an acoustic neuroma., The trigeminal nerve has a broad base and involvement of at least part of this nerve is the most, likely initial finding. The defect may be subtle such as loss of the ipsilateral corneal reflex. Ipsilateral, hearing loss will also occur. Untreated, progressive lesions, may ultimately affect may cranial nerve, roots in this region., Please rate this question:, , Discuss and give feedback, , Next question, , Cranial nerves, Cranial nerve lesions
Page 2035 :
Olfactory nerve, , May be injured in basal skull fractures or involved in frontal lobe tumour extension., Loss of olfactory nerve function in relation to major CNS pathology is seldom an, isolated event and thus it is poor localiser of CNS pathology., , Optic nerve, , Problems with visual acuity may result from intra ocular disorders. Problems with, the blood supply such as amaurosis fugax may produce temporary visual distortion., More important surgically is the pupillary response to light. The pupillary size may, be altered in a number of disorders. Nerves involved in the resizing of the pupil, connect to the pretectal nucleus of the high midbrain, bypassing the lateral, geniculate nucleus and the primary visual cortex. From the pretectal nucleus, neurones pass to the Edinger - Westphal nucleus, motor axons from here pass along, with the oculomotor nerve. They synapse with ciliary ganglion neurones; the, parasympathetic axons from this then innervate the iris and produce miosis. The, miotic pupil is seen in disorders such as Horner's syndrome or opiate overdose., Mydriasis is the dilatation of the pupil in response to disease, trauma, drugs (or the, dark!). It is pathological when light fails to induce miosis. The radial muscle is, innervated by the sympathetic nervous system. Because the parasympathetic fibres, travel with the oculomotor nerve they will be damaged by lesions affecting this, nerve (e.g. cranial trauma)., The response to light shone in one eye is usually a constriction of both pupils. This, indicates intact direct and consensual light reflexes. When the optic nerve has an, afferent defect the light shining on the affected eye will produce a diminished, pupillary response in both eyes. Whereas light shone on the unaffected eye will, produce a normal pupillary response in both eyes. This is referred to as the Marcus, Gunn pupil and is seen in conditions such as optic neuritis. In a total CN II lesion, shining the light in the affected eye will produce no response., , Oculomotor nerve, , The pupillary effects are described above. In addition it supplies all ocular muscles, apart from lateral rectus and superior oblique. Thus the affected eye will be, deviated inferolaterally. Levator palpebrae superioris may also be impaired resulting, in impaired ability to open the eye., , Trochlear nerve, , The eye will not be able to look down., , Trigeminal nerve, , Largest cranial nerve. Exits the brainstem at the pons. Branches are ophthalmic,, maxillary and mandibular. Only the mandibular branch has both sensory and motor, fibres. Branches converge to form the trigeminal ganglion (located in Meckels cave).
Page 2036 :
It supplies the muscles of mastication and also tensor veli palatine, mylohyoid,, anterior belly of digastric and tensor tympani. The detailed descriptions of the, various sensory functions are described in other areas of the website. The corneal, reflex is important and is elicited by applying a small tip of cotton wool to the, cornea, a reflex blink should occur if it is intact. It is mediated by: the naso ciliary, branch of the ophthalmic branch of the trigeminal (sensory component) and the, facial nerve producing the motor response. Lesions of the afferent arc will produce, bilateral absent blink and lesions of the efferent arc will result in a unilateral absent, blink., , Abducens nerve, , The affected eye will have a deficit of abduction. This cranial nerve exits the, brainstem between the pons and medulla. It thus has a relatively long intra cranial, course which renders it susceptible to damage in raised intra cranial pressure., , Facial nerve, , Emerges from brainstem between pons and medulla. It controls muscles of facial, expression and taste from the anterior 2/3 of the tongue. The nerve passes into the, petrous temporal bone and into the internal auditory meatus. It then passes, through the facial canal and exits at the stylomastoid foramen. It passes through the, parotid gland and divides at this point. It does not innervate the parotid gland. Its, divisions are considered in other parts of the website. Its motor fibres innervate, orbicularis oculi to produce the efferent arm of the corneal reflex. In surgical, practice it may be injured during parotid gland surgery or invaded by malignancies, of the gland and a lower motor neurone on the ipsilateral side will result., , Vestibulo-cochlear, nerve, , Exits from the pons and then passes through the internal auditory meatus. It is, implicated in sensorineural hearing loss. Individuals with sensorineural hearing loss, will localise the sound in webers test to the normal ear. Rinnes test will be reduced, on the affected side but should still work. These two tests will distinguish, sensorineural hearing loss from conductive deafness. In the latter condition webers, test will localise to the affected ear and Rinnes test will be impaired on the affected, side. Surgical lesions affecting this nerve include CNS tumours and basal skull, fractures. It may also be damaged by the administration of ototoxic drugs (of which, gentamicin is the most commonly used in surgical practice)., , Glossopharyngeal, nerve, , Exits the pons just above the vagus. Receives sensory fibres from posterior 1/3, tongue, tonsils, pharynx and middle ear (otalgia may occur following tonsillectomy)., It receives visceral afferents from the carotid bodies. It supplies parasympathetic
Page 2037 :
fibres to the parotid gland via the otic ganglion and motor function to, stylopharyngeaus muscle. The sensory function of the nerve is tested using the gag, reflex., , Vagus nerve, , Leaves the medulla between the olivary nucleus and the inferior cerebellar, peduncle. Passes through the jugular foramen and into the carotid sheath. Details of, the functions of the vagus nerve are covered in the website under relevant organ, sub headings., , Accessory nerve, , Exists from the caudal aspect of the brainstem (multiple branches) supplies, trapezius and sternocleidomastoid muscles. The distal portion of this nerve is most, prone to injury during surgical procedures., , Hypoglossal nerve, , Emerges from the medulla at the preolivary sulcus, passes through the hypoglossal, canal. It lies on the carotid sheath and passes deep to the posterior belly of digastric, to supply muscles of the tongue (except palatoglossus). Its location near the carotid, sheath makes it vulnerable during carotid endarterectomy surgery and damage will, produce ipsilateral defect in muscle function., Next question
Page 2038 :
Question 413 of 560, , Which of the following is not a branch of the abdominal aorta?, , Inferior mesenteric artery, , Inferior phrenic artery, , Superior mesenteric artery, , Superior phrenic artery, , Renal artery, Mnemonic for the Descending abdominal aorta branches from diaphragm to iliacs:, 'Prostitutes Cause Sagging Swollen Red Testicles [in men] Living In Sin':, Phrenic [inferior], Celiac, Superior mesenteric, Suprarenal [middle], Renal, Testicular ['in men' only], Lumbars, Inferior mesenteric, Sacral, , The superior phrenic artery branches from the aorta in the thorax., Please rate this question:, , Discuss and give feedback
Page 2040 :
Question 414 of 560, A 40 year old lady presents with varicose veins, these are found to originate from the short, saphenous vein. As the vein is mobilised close to its origin which structure is at greatest risk of, injury?, , Sciatic nerve, , Sural nerve, , Common peroneal nerve, , Tibial nerve, , Popliteal artery, , The sural nerve is closely related and damage to this structure is a major cause of litigation. The, other structures may all be injured but the risks are lower., Please rate this question:, , Discuss and give feedback, , Next question, , Popliteal fossa, Boundaries of the popliteal fossa, , Laterally, , Biceps femoris above, lateral head of gastrocnemius and plantaris below, , Medially, , Semimembranosus and semitendinosus above, medial head of gastrocnemius below, , Floor, , Popliteal surface of the femur, posterior ligament of knee joint and popliteus muscle, , Roof, , Superficial and deep fascia
Page 2041 :
Image showing the popliteal fossa, , © Image provided by the University of Sheffield, , Contents, , , , , , , , , Popliteal artery and vein, Small saphenous vein, Common peroneal nerve, Tibial nerve, Posterior cutaneous nerve of the thigh, Genicular branch of the obturator nerve, Lymph nodes, Next question
Page 2042 :
Question 415 of 560, A 23 year old man is admitted with a suspected ureteric colic. A KUB style x-ray is obtained. In, which of the following locations is the stone most likely to be visualised?, , The tips of the transverse processes between L2 and L5, , The tips of transverse processes between T10-L1, , At the crest of the ilium, , Over the S3 foramina, , Over the sacrococcygeal joint, , The ureter lies anterior to L2 to L5 and stones may be visualised at these points, they may also be, identified over the sacro-iliac joints., Please rate this question:, , Discuss and give feedback, , Next question, , Ureter, , , , , , , , , 25-35 cm long, Muscular tube lined by transitional epithelium, Surrounded by thick muscular coat. Becomes 3 muscular layers as it crosses the bony pelvis, Retroperitoneal structure overlying transverse processes L2-L5, Lies anterior to bifurcation of iliac vessels, Blood supply is segmental; renal artery, aortic branches, gonadal branches, common iliac, and internal iliac, Lies beneath the uterine artery, Next question
Page 2043 :
Question 416 of 560, A 72 year old man with non reconstructible arterial disease is undergoing an above knee, amputation. The posterior compartment muscles are divided. Which of the following muscles does, not lie in the posterior compartment of the thigh?, , Biceps femoris, , Quadriceps femoris, , Semitendinosus, , Semimembranosus, , None of the above, , The quadriceps femoris lies in the anterior compartment., Please rate this question:, , Discuss and give feedback, , Next question, , Fascial compartments of the leg, Compartments of the thigh, Formed by septae passing from the femur to the fascia lata., , Compartment, , Nerve, , Muscles, , Blood supply, , Anterior compartment, , Femoral, , , , , , , Iliacus, Tensor fasciae latae, Sartorius, Quadriceps femoris, , Femoral artery, , Medial compartment, , Obturator, , , , Adductor, longus/magnus/brevis, Gracilis, , Profunda femoris artery, and obturator artery, ,
Page 2045 :
Question 417 of 560, A woman develops winging of the scapula following a Patey mastectomy. What is the most likely, cause?, , Division of pectoralis minor to access level 3 axillary nodes, , Damage to the brachial plexus during axillary dissection, , Damage to the long thoracic nerve during axillary dissection, , Division of the thoracodorsal trunk during axillary dissection, , Damage to the thoracodorsal trunk during axillary dissection, , Theme from January 2012 exam, The serratus anterior muscle is supplied by the long thoracic nerve which runs along the surface of, serratus anterior and is liable to injury during nodal dissection. Although pectoralis minor is divided, during a Patey mastectomy (now seldom performed) it is rare for this alone to produce winging of the, scapula., Please rate this question:, , Discuss and give feedback, , Next question, , Long thoracic nerve, , , , , , Derived from ventral rami of C5, C6, and C7 (close to their emergence from intervertebral, foramina), It runs downward and passes either anterior or posterior to the middle scalene muscle, It reaches upper tip of serratus anterior muscle and descends on outer surface of this, muscle, giving branches into it, Winging of Scapula occurs in long thoracic nerve injury (most common) or from spinal, accessory nerve injury (which denervates the trapezius) or a dorsal scapular nerve injury, Next question
Page 2046 :
Question 418 of 560, , In a patient with an ectopic kidney where is the adrenal gland most likely to be located?, , In the pelvis, , On the contralateral side, , In its usual position, , Superior to the spleen, , It will be absent, , Because the kidney is present, rather than absent, the adrenal will usual develop and in the normal, location., Please rate this question:, , Discuss and give feedback, , Next question, , Adrenal gland embryology, First detected at 6 weeks' gestation, the adrenal cortex is derived from the mesoderm of the, posterior abdominal wall. Steroid secretion from the fetal cortex begins shortly thereafter. Adult-type, zona glomerulosa and fasciculata are detected in fetal life but make up only a small proportion of the, gland, and the zona reticularis is not present at all. The fetal cortex predominates throughout fetal, life. The adrenal medulla is of ectodermal origin, arising from neural crest cells that migrate to the, medial aspect of the developing cortex., The fetal adrenal gland is relatively large. At 4 months' gestation, it is 4 times the size of the kidney;, however, at birth, it is a third of the size of the kidney. This occurs because of the rapid regression of
Page 2047 :
the fetal cortex at birth. It disappears almost completely by age 1 year; by age 4-5 years, the, permanent adult-type adrenal cortex has fully developed., Anatomic anomalies of the adrenal gland may occur. Because the development of the adrenals is, closely associated with that of the kidneys, agenesis of an adrenal gland is usually associated with, ipsilateral agenesis of the kidney, and fused adrenal glands (whereby the 2 glands join across the, midline posterior to the aorta) are also associated with a fused kidney., Adrenal hypoplasia occurs in the following 2 forms: (1) hypoplasia or absence of the fetal cortex with, a poorly formed medulla and (2) disorganized fetal cortex and medulla with no permanent cortex, present. Adrenal heterotopia describes a normal adrenal gland in an abnormal location, such as, within the renal or hepatic capsules. Accessory adrenal tissue (adrenal rests), which is usually, comprised only of cortex but seen combined with medulla in some cases, is most commonly located, in the broad ligament or spermatic cord but can be found anywhere within the abdomen. Even, intracranial adrenal rests have been reported, Next question
Page 2048 :
Question 419 of 560, Which of the following structures is not closely related to the posterior tibial artery?, , Soleus posteriorly, , Tibial nerve medially, , Deep peroneal nerve laterally, , Flexor hallucis longus postero-inferiorly, , Popliteus, , The deep peroneal nerve lies in the anterior compartment. The tibial nerve lies medially. At its, termination it lies deep to the flexor retinaculum., Please rate this question:, , Discuss and give feedback, , Next question, , Posterior tibial artery, , , , , , Larger terminal branch of the popliteal artery, Terminates by dividing into the medial and lateral plantar arteries, Accompanied by two veins throughout its length, Position of the artery corresponds to a line drawn from the lower angle of the popliteal fossa,, at the level of the neck of the fibula, to a point midway between the medial malleolus and the, most prominent part of the heel, , Relations of the posterior tibial artery, Proximal to distal, , Anteriorly, , Tibialis posterior, Flexor digitorum longus, Posterior surface of tibia and ankle joint
Page 2049 :
Posterior, , Tibial nerve 2.5 cm distal to its origin, Fascia overlying the deep muscular layer, Proximal part covered by gastrocnemius and soleus, Distal part covered by skin and fascia, Next question
Page 2050 :
Question 420 of 560, , Which of the following is not closely related to the capitate bone?, , Lunate bone, , Scaphoid bone, , Ulnar nerve, , Hamate bone, , Trapezoid bone, , The ulnar nerve and artery lie adjacent to the pisiform bone. The capitate bone articulates with the, lunate, scaphoid, hamate and trapezoid bones, which are therefore closely related to it., Please rate this question:, , Discuss and give feedback, , Next question, , Capitate bone, This is the largest of the carpal bones. It is centrally placed with a rounded head set into the cavities, of the lunate and scaphoid bones. Flatter articular surfaces are present for the hamate medially and, the trapezoid laterally. Distally the bone articulates predominantly with the middle metacarpal., Next question
Page 2051 :
Question 421 of 560, Which of the following statements relating to the tympanic membrane is false?, , The umbo marks the point of attachment of the handle of the malleus to the tympanic, membrane, The lateral aspect of the tympanic membrane is lined by stratified squamous epithelium, , The chorda tympani nerve runs medial to the pars tensa, , The medial aspect of the tympanic membrane is lined by mucous membrane, , The tympanic membrane is approximately 1cm in diameter, , The chorda tympani runs medially to the pars flaccida. The relationship is shown from the medial, aspect in the dissection below., , Image sourced from Wikipedia, , Please rate this question:
Page 2052 :
Discuss and give feedback, , Next question, , Ear- anatomy, The ear is composed of three anatomically distinct regions., External ear, Auricle is composed of elastic cartilage covered by skin. The lobule has no cartilage and contains fat, and fibrous tissue., External auditory meatus is approximately 2.5cm long., Lateral third of the external auditory meatus is cartilaginous and the medial two thirds is bony., The region is innervated by the greater auricular nerve. The auriculotemporal branch of the, trigeminal nerve supplies most the of external auditory meatus and the lateral surface of the auricle., Middle ear, Space between the tympanic membrane and cochlea. The aditus leads to the mastoid air cells is the, route through which middle ear infections may cause mastoiditis. Anteriorly the eustacian tube, connects the middle ear to the naso pharynx., The tympanic membrane consists of:, , , , , Outer layer of stratified squamous epithelium., Middle layer of fibrous tissue., Inner layer of mucous membrane continuous with the middle ear., , The tympanic membrane is approximately 1cm in diameter., The chorda tympani nerve passes on the medial side of the pars flaccida., The middle ear is innervated by the glossopharyngeal nerve and pain may radiate to the middle ear, following tonsillectomy., Ossicles, Malleus attaches to the tympanic membrane (the Umbo)., Malleus articulates with the incus (synovial joint)., Incus attaches to stapes (another synovial joint)., Internal ear, Cochlea, semi circular canals and vestibule, Organ of corti is the sense organ of hearing and is located on the inside of the cochlear duct on the, basilar membrane., Vestibule accommodates the utricule and the saccule. These structures contain endolymph and are, surrounded by perilymph within the vestibule., The semicircular canals lie at various angles to the petrous temporal bone. All share a common, opening into the vestibule.
Page 2053 :
Question 422 of 560, An injury to the spinal accessory nerve will affect which of the following movements?, , Lateral rotation of the arm, , Adduction of the arm at the glenohumeral joint, , Protraction of the scapula, , Upward rotation of the scapula, , Depression of the scapula, , The spinal accessory nerve innervates trapezius. The entire muscle will retract the scapula., However, its upper and lower fibres act together to upwardly rotate it., Please rate this question:, , Discuss and give feedback, , Next question, , Shoulder joint, , , , , Shallow synovial ball and socket type of joint., It is an inherently unstable joint, but is capable to a wide range of movement., Stability is provided by muscles of the rotator cuff that pass from the scapula to insert in the, greater tuberosity (all except sub scapularis-lesser tuberosity)., , Glenoid labrum, , , , , Fibrocartilaginous rim attached to the free edge of the glenoid cavity, Tendon of the long head of biceps arises from within the joint from the supraglenoid tubercle,, and is fused at this point to the labrum., The long head of triceps attaches to the infraglenoid tubercle, , Fibrous capsule
Page 2056 :
Question 423 of 560, Which of the following is not contained within the middle mediastinum?, , Main bronchi, , Arch of the azygos vein, , Thoracic duct, , Pericardium, , Aortic root, , The thoracic duct lies within the posterior and superior mediastinum., Please rate this question:, , Discuss and give feedback, , Next question, , Mediastinum, Region between the pulmonary cavities., It is covered by the mediastinal pleura. It does not contain the lungs., It extends from the thoracic inlet superiorly to the diaphragm inferiorly., Mediastinal regions, , , , , , Region, , Superior mediastinum (between manubriosternal angle and T4/5), Middle mediastinum, Posterior mediastinum, Anterior mediastinum, , Contents
Page 2058 :
Question 424 of 560, A 55 year old man is due to undergo a radical prostatectomy for carcinoma of the prostate gland., Which of the following vessels directly supplies the prostate?, , External iliac artery, , Common iliac artery, , Internal iliac artery, , Inferior vesical artery, , None of the above, , The arterial supply to the prostate gland is from the inferior vesical artery, it is a branch of the, prostatovesical artery. The prostatovesical artery usually arises from the internal pudendal and, inferior gluteal arterial branches of the internal iliac artery., Please rate this question:, , Discuss and give feedback, , Next question, , Prostate gland, The prostate gland is approximately the shape and size of a walnut and is located inferior to the, bladder. It is separated from the rectum by Denonvilliers fascia and its blood supply is derived from, the internal iliac vessels (via inferior vesical artery). The internal sphincter lies at the apex of the, gland and may be damaged during prostatic surgery, affected individuals may complain of, retrograde ejaculation., Summary of prostate gland, , Arterial supply, , Inferior vesical artery (from internal iliac), , Venous drainage, , Prostatic venous plexus (to paravertebral veins)
Page 2059 :
Lymphatic, drainage, , Internal iliac nodes, , Innervation, , Inferior hypogastric plexus, , Dimensions, , , , , , Transverse diameter (4cm), AP diameter (2cm), Height (3cm), , Lobes, , , , , , , Posterior lobe: posterior to urethra, Median lobe: posterior to urethra, in between ejaculatory ducts, Lateral lobes x 2, Isthmus, , Zones, , , , Peripheral zone: subcapsular portion of posterior prostate. Most, prostate cancers are here, Central zone, Transition zone, Stroma, , , , , , Relations, , Anterior, , Pubic symphysis, Prostatic venous plexus, , Posterior, , Denonvilliers fascia, Rectum, Ejaculatory ducts, , Lateral, , Venous plexus (lies on prostate), Levator ani (immediately below the puboprostatic ligaments)
Page 2060 :
Image sourced from Wikipedia, , Next question
Page 2061 :
Question 425 of 560, Which nerve directly innervates the sinoatrial node?, , Superior cardiac nerve, , Right vagus nerve, , Left vagus nerve, , Inferior cardiac nerve, , None of the above, , Theme from September 2012 Exam, Theme from April 2016 Exam, No single one of the above nerves is responsible for direct cardiac innervation (which those who, have handled the heart surgically will appreciate)., The heart receives its nerves from the superficial and deep cardiac plexuses. The cardiac plexuses, send small branches to the heart along the major vessels, continuing with the right and left coronary, arteries. The vagal efferent fibres emerge from the brainstem in the roots of the vagus and, accessory nerves, and run to ganglia in the cardiac plexuses and within the heart itself., The background vagal discharge serves to limit heart rate, and loss of this background vagal tone, accounts for the higher resting heart rate seen following cardiac transplant., Please rate this question:, , Discuss and give feedback, , Next question, , Sinoatrial node, , , , , Located in the wall of the right atrium in the upper part of the sulcus terminalis from which it, extends anteriorly over the opening of the superior vena cava., In most cases it is supplied by the right coronary artery., It has a complicated nerve supply from the cardiac nerve plexus that takes both sympathetic, and parasympathetic fibres that run alongside the main vessels., Next question
Page 2062 :
Question 426 of 560, , A 30 year old man presents with back pain and the surgeon tests the ankle reflex. Which of the, following nerve roots are tested in this manoeuvre?, , S3 and S4, , L4 and L5, , L3 and L4, , S1 and S2, , S4 only, , Theme from April 2012 Exam, Please rate this question:, , Discuss and give feedback, , Next question, , Ankle reflex, The ankle reflex is elicited by tapping the Achilles tendon with a tendon hammer. It tests the S1 and, S2 nerve roots. It is typically delayed in L5 and S1 disk prolapses., Next question
Page 2065 :
Question 428 of 560, An 18 year old male presents to casualty with a depressed skull fracture. This is managed surgically., Over the next few days he complains of double vision on walking down stairs and reading. On, testing ocular convergence, the left eye faces downwards and medially, but the right side does not, do so. Which of the nerves listed below is most likely to be responsible?, , Facial, , Oculomotor, , Abducens, , Trochlear, , Trigeminal nerve, , Theme from September 2012 Exam, The trochlear nerve has a relatively long intracranial course and this makes it vulnerable to injury in, head trauma. Head trauma is the commonest cause of an acute fourth nerve palsy. A 4th nerve, palsy is the commonest cause of a vertical diplopia. The diplopia is at its worst when the eye looks, medially which it usually does as part of the accommodation reflex when walking down stairs., Please rate this question:, , Discuss and give feedback, , Next question, , Disorders of the oculomotor system, Nerve, , Oculomotor, nerve, , Path, , , , Nerve palsy features, , Large nucleus at the midbrain, Fibres pass through the red nucleus and the, pyramidal tract; through the cavernous sinus, into the orbit, , Ptosis, Eye down and out, Unable to move the eye, superiorly, inferiorly,, medially, Pupil fixed and dilated
Page 2066 :
Nerve, , Trochlear, nerve, , Path, , , , , Abducens, nerve, , Nerve palsy features, , Longest intracranial course, Only nerve to exit the dorsal aspect of, brainstem, Nucleus at midbrain, passes between the, posterior cerebral and superior cerebellar, arteries, through the cavernous sinus into the, orbit, , Nucleus lies in the mid pons, , Vertical diplopia, (diplopia on descending, the stairs), Unable to look down, and in, , Convergence of eyes in, primary position, Lateral diplopia towards, side of lesion, Eye deviates medially, Next question
Page 2067 :
Question 429 of 560, A 77 year old man with symptoms of intermittent claudication is due to have his ankle brachial, pressure indices measured. The dorsalis pedis artery is impalpable. Which of the following tendinous, structures lies medial to it, that may facilitate its identification?, , Extensor digitorum longus tendon, , Peroneus tertius tendon, , Extensor hallucis longus tendon, , Extensor digitorum brevis tendon, , Flexor digitorum longus tendon, , The extensor hallucis longus tendon lies medial to the dorsalis pedis artery., Please rate this question:, , Discuss and give feedback, , Next question, , Foot- anatomy, Arches of the foot, The foot is conventionally considered to have two arches., , , , , The longitudinal arch is higher on the medial than on the lateral side. The posterior part of, the calcaneum forms a posterior pillar to support the arch. The lateral part of this structure, passes via the cuboid bone and the lateral two metatarsal bones. The medial part of this, structure is more important. The head of the talus marks the summit of this arch, located, between the sustentaculum tali and the navicular bone. The anterior pillar of the medial arch, is composed of the navicular bone, the three cuneiforms and the medial three metatarsal, bones., The transverse arch is situated on the anterior part of the tarsus and the posterior part of the, metatarsus. The cuneiforms and metatarsal bases narrow inferiorly, which contributes to the, shape of the arch., , Intertarsal joints
Page 2068 :
Sub talar joint, , Formed by the cylindrical facet on the lower surface of the body of the, talus and the posterior facet on the upper surface of the calcaneus. The, facet on the talus is concave anteroposteriorly, the other is convex. The, synovial cavity of this joint does not communicate with any other joint., , Talocalcaneonavicular, joint, , The anterior part of the socket is formed by the concave articular, surface of the navicular bone, posteriorly by the upper surface of the, sustentaculum tali. The talus sits within this socket, , Calcaneocuboid joint, , Highest point in the lateral part of the longitudinal arch. The lower, aspect of this joint is reinforced by the long plantar and plantar, calcaneocuboid ligaments., , Transverse tarsal joint, , The talocalcaneonavicular joint and the calcaneocuboid joint extend, across the tarsus in an irregular transverse plane, between the talus and, calcaneus behind and the navicular and cuboid bones in front. This, plane is termed the transverse tarsal joint., , Cuneonavicular joint, , Formed between the convex anterior surface of the navicular bone and, the concave surface of the the posterior ends of the three cuneiforms., , Intercuneiform joints, , Between the three cuneiform bones., , Cuneocuboid joint, , Between the circular facets on the lateral cuneiform bone and the, cuboid. This joint contributes to the tarsal part of the transverse arch., , A detailed knowledge of the joints is not required for MRCS Part A. However, the contribution they, play to the overall structure of the foot should be appreciated, Ligaments of the ankle joint and foot
Page 2069 :
Image sourced from Wikipedia, , Muscles of the foot, , Muscle, , Origin, , Insertion, , Nerve, supply, , Action, , Abductor, hallucis, , Medial side of the calcaneus,, flexor retinaculum, plantar, aponeurosis, , Medial side of, the base of the, proximal, phalanx, , Medial, plantar, nerve, , Abducts the great toe, , Flexor, digitorum, brevis, , Medial process of the, calcaneus, plantar, eponeurosis., , Via 4 tendons, into the, middle, phalanges of, the lateral 4, toes., , Medial, plantar, nerve, , Flexes all the joints of, the lateral 4 toes except, for the interphalangeal, joint., , Abductor, digit, minimi, , From the tubercle of the, calcaneus and from the, plantar aponeurosis, , Together with, flexor digit, minimi brevis, into the lateral, side of the, , Lateral, plantar, nerve, , Abducts the little toe at, the metatarsophalangeal, joint
Page 2070 :
base of the, proximal, phalanx of the, little toe, , Flexor, hallucis, brevis, , From the medial side of the, plantar surface of the cuboid, bone, from the adjacent part, of the lateral cuneiform bone, and from the tendon of, tibialis posterior., , Into the, proximal, phalanx of the, great toe, the, tendon, contains a, sesamoid bone, , Medial, plantar, nerve, , Flexes the, metatarsophalangeal, joint of the great toe., , Adductor, hallucis, , Arises from two heads. The, oblique head arises from the, sheath of the peroneus longus, tendon, and from the plantar, surfaces of the bases of the, 2nd, 3rd and 4th metatarsal, bones. The transverse head, arises from the plantar, surface of the lateral 4, metatarsophalangeal joints, and from the deep transverse, metatarsal ligament., , Lateral side of, the base of the, proximal, phalanx of the, great toe., , Lateral, plantar, nerve, , Adducts the great toe, towards the second toe., Helps maintain the, transverse arch of the, foot., , Extensor, digitorum, brevis, , On the dorsal surface of the, foot from the upper surface of, the calcaneus and its, associated fascia, , Via four thin, tendons which, run forward, and medially, to be inserted, into the, medial four, toes. The, lateral three, tendons join, with hoods of, extensor, digitorum, longus., , Deep, peroneal, , Extend the, metatarsophalangeal, joint of the medial four, toes. It is unable to, extend the, interphalangeal joint, without the assistance of, the lumbrical muscles., , Nerves in the foot
Page 2071 :
Lateral plantar nerve, Passes anterolaterally towards the base of the 5th metatarsal between flexor digitorum brevis and, flexor accessorius. On the medial aspect of the lateral plantar artery. At the base of the 5th, metatarsal it splits into superficial and deep branches., Medial plantar nerve, Passes forwards with the medial plantar artery under the cover of the flexor retinaculum to the, interval between abductor hallucis and flexor digitorum brevis on the sole of the foot., Plantar arteries, Arise under the cover of the flexor retinaculum, midway between the tip of the medial malleolus and, the most prominent part of the medial side of the heel., , , , , Medial plantar artery. Passes forwards medial to medial plantar nerve in the space between, abductor hallucis and flexor digitorum brevis.Ends by uniting with a branch of the 1st plantar, metatarsal artery., Lateral plantar artery. Runs obliquely across the sole of the foot. It lies lateral to the lateral, plantar nerve. At the base of the 5th metatarsal bone it arches medially across the foot on, the metatarsals, , Dorsalis pedis artery, This vessel is a direct continuation of the anterior tibial artery. It commences on the front of the ankle, joint and runs to the proximal end of the first metatarsal space. Here is gives off the arcuate artery, and continues forwards as the first dorsal metatarsal artery. It is accompanied by two veins, throughout its length. It is crossed by the extensor hallucis brevis, Next question
Page 2072 :
Question 430 of 560, A 23 year old man falls over whilst intoxicated and a shard of glass transects his median nerve at the, proximal border of the flexor retinaculum. His tendons escape injury. Which of the following features, is least likely to be present?, , Weakness of thumb abduction, , Loss of sensation on the dorsal aspect of the thenar eminence, , Loss of power of opponens pollicis, , Adduction and lateral rotation of the thumb at rest, , Loss of power of abductor pollicis brevis, , The median nerve may be injured proximal to the flexor retinaculum. This will result in loss of, abductor pollicis brevis, flexor pollicis brevis, opponens pollicis and the first and second lumbricals., When the patient is asked to close the hand slowly there is a lag of the index and middle fingers, reflecting the impaired lumbrical muscle function. The sensory changes are minor and do not extend, to the dorsal aspect of the thenar eminence., Abductor pollicis longus will contribute to thumb abduction (and is innervated by the posterior, interosseous nerve) and therefore abduction will be weaker than prior to the injury., Please rate this question:, , Discuss and give feedback, , Next question, , Median nerve, The median nerve is formed by the union of a lateral and medial root respectively from the lateral, (C5,6,7) and medial (C8 and T1) cords of the brachial plexus; the medial root passes anterior to the, third part of the axillary artery. The nerve descends lateral to the brachial artery, crosses to its, medial side (usually passing anterior to the artery). It passes deep to the bicipital aponeurosis and, the median cubital vein at the elbow., It passes between the two heads of the pronator teres muscle, and runs on the deep surface of, flexor digitorum superficialis (within its fascial sheath)., Near the wrist it becomes superficial between the tendons of flexor digitorum superficialis and flexor, carpi radialis, deep to palmaris longus tendon. It passes deep to the flexor retinaculum to enter the, palm, but lies anterior to the long flexor tendons within the carpal tunnel.
Page 2074 :
Damage at elbow, as above plus:, , , , , unable to pronate forearm, weak wrist flexion, ulnar deviation of wrist, , Anterior interosseous nerve (branch of median nerve), , , , leaves just below the elbow, results in loss of pronation of forearm and weakness of long flexors of thumb and index, finger, , Topography of the median nerve, , Image sourced from Wikipedia, , Next question
Page 2075 :
Question 431 of 560, The following muscles are supplied by the recurrent laryngeal nerve except:, , Transverse arytenoid, , Posterior crico-arytenoid, , Cricothyroid, , Oblique arytenoid, , Thyroarytenoid, Innervates: all intrinsic larynx muscles (excluding cricothyroid), The external branch of the superior laryngeal nerve innervates the cricothyroid muscle., Please rate this question:, , Discuss and give feedback, , Next question, , Recurrent laryngeal nerve, , , Branch of the vagus nerve, , Path, Right, , , , Arises anterior to the subclavian artery and ascends obliquely next to the trachea, behind the, common carotid artery, It is either anterior or posterior to the inferior thyroid artery, , Left, , , Arises left to the arch of the aorta
Page 2076 :
, , , Winds below the aorta, Ascends along the side of the trachea, , Then both, , , , , , Pass in a groove between the trachea and oesophagus, Enters the larynx behind the articulation between the thyroid cartilage and cricoid, Distributed to larynx muscles, , Branches to, , , , , Cardiac plexus, Mucous membrane and muscular coat of the oesophagus and trachea, , Innervates, , , , Intrinsic larynx muscles (excluding cricothyroid), , Image sourced from Wikipedia, , Next question
Page 2077 :
Question 432 of 560, From which embryological structure is the ureter derived?, , Uranchus, , Cloaca, , Vitello-intestinal duct, , Mesonephric duct, , None of the above, , The ureter develops from the mesonephric duct. The mesonephric duct is associated with the, metanephric duct that develops within the metenephrogenic blastema. This forms the site of the, ureteric bud which branches off the mesonephric duct., Please rate this question:, , Discuss and give feedback, , Next question, , Ureter, , , , , , , , , 25-35 cm long, Muscular tube lined by transitional epithelium, Surrounded by thick muscular coat. Becomes 3 muscular layers as it crosses the bony pelvis, Retroperitoneal structure overlying transverse processes L2-L5, Lies anterior to bifurcation of iliac vessels, Blood supply is segmental; renal artery, aortic branches, gonadal branches, common iliac, and internal iliac, Lies beneath the uterine artery, Next question
Page 2078 :
Question 433 of 560, A 16 year old boy is hit by a car and sustains a blow to the right side of his head. He is initially, conscious but on arrival in the emergency department is comatose. On examination his right pupil is, fixed and dilated. The neurosurgeons plan immediate surgery. What type of initial approach should, be made?, , Left parieto-temporal craniotomy, , Right parieto-temporal craniotomy, , Posterior fossa craniotomy, , Left parieto-temporal burr holes, , None of the above, , Theme from April 2012 Exam, A unilateral dilated pupil is a classic sign of transtentorial herniation. The medial aspect of the, temporal lobe (uncus) herniates across the tentorium and causes pressure on the ipsilateral, oculomotor nerve, interrupting parasympathetic input to the eye and resulting in a dilated pupil. In, addition the brainstem is compressed. As the ipsilateral oculomotor nerve is being compressed,, craniotomy (rather than Burr Holes) should be made on the ipsilateral side., Please rate this question:, , Discuss and give feedback, , Next question, , Head injury, Patients who suffer head injuries should be managed according to ATLS principles and extra cranial, injuries should be managed alongside cranial trauma. Inadequate cardiac output will compromise, CNS perfusion irrespective of the nature of the cranial injury., Types of traumatic brain injury, , Extradural, haematoma, , Bleeding into the space between the dura mater and the skull. Often results from, acceleration-deceleration trauma or a blow to the side of the head. The majority, of extradural haematomas occur in the temporal region where skull fractures, cause a rupture of the middle meningeal artery.
Page 2079 :
Features, , , , , Raised intracranial pressure, Some patients may exhibit a lucid interval, , Bleeding into the outermost meningeal layer. Most commonly occur around the, frontal and parietal lobes. May be either acute or chronic., Subdural, haematoma, , Risk factors include old age and alcoholism., Slower onset of symptoms than a extradural haematoma., , Subarachnoid, haemorrhage, , Usually occurs spontaneously in the context of a ruptured cerebral aneurysm, but, may be seen in association with other injuries when a patient has sustained a, traumatic brain injury., , Pathophysiology, , , , , , , , Primary brain injury may be focal (contusion/ haematoma) or diffuse (diffuse axonal injury), Diffuse axonal injury occurs as a result of mechanical shearing following deceleration,, causing disruption and tearing of axons, Intra-cranial haematomas can be extradural, subdural or intracerebral, while contusions may, occur adjacent to (coup) or contralateral (contre-coup) to the side of impact, Secondary brain injury occurs when cerebral oedema, ischaemia, infection, tonsillar or, tentorial herniation exacerbates the original injury. The normal cerebral auto regulatory, processes are disrupted following trauma rendering the brain more susceptible to blood flow, changes and hypoxia, The Cushings reflex (hypertension and bradycardia) often occurs late and is usually a pre, terminal event, , Management, , , , , , , , , , , Where there is life threatening rising ICP such as in extra dural haematoma and whilst, theatre is prepared or transfer arranged use of IV mannitol/ frusemide may be required., Diffuse cerebral oedema may require decompressive craniotomy, Exploratory Burr Holes have little management in modern practice except where scanning, may be unavailable and to thus facilitate creation of formal craniotomy flap, Depressed skull fractures that are open require formal surgical reduction and debridement,, closed injuries may be managed non operatively if there is minimal displacement., ICP monitoring is appropriate in those who have GCS 3-8 and normal CT scan., ICP monitoring is mandatory in those who have GCS 3-8 and abnormal CT scan., Hyponatraemia is most likely to be due to syndrome of inappropriate ADH secretion., Minimum of cerebral perfusion pressure of 70mmHg in adults., Minimum cerebral perfusion pressure of between 40 and 70 mmHg in children.
Page 2080 :
Interpretation of pupillary findings in head injuries, , Pupil size, , Light response, , Interpretation, , Unilaterally dilated, , Sluggish or fixed, , 3rd nerve compression secondary to tentorial, herniation, , Bilaterally dilated, , Sluggish or fixed, , Unilaterally dilated or, equal, , Cross reactive (Marcus Gunn), , Bilaterally constricted, , May be difficult to, assess, , Unilaterally, constricted, , Preserved, , , , , Poor CNS perfusion, Bilateral 3rd nerve palsy, , Optic nerve injury, , , , , Opiates, Pontine lesions, Metabolic encephalopathy, , Sympathetic pathway disruption, Next question
Page 2081 :
Question 434 of 560, Which of the following relationship descriptions regarding the scalene muscles is incorrect?, , The brachial plexus passes anterior to the middle scalene muscle, , The phrenic nerve lies anterior to the anterior scalene muscle, , The subclavian artery passes posterior to the middle scalene, , The subclavian vein lies anterior to the anterior scalene muscle at the level of the first rib, , The anterior scalene inserts into the first rib, , The subclavian artery passes anterior to the middle scalene., Please rate this question:, , Discuss and give feedback, , Next question, , Scalene muscles, The 3 paired muscles are:, , , , , Scalenus anterior: Elevate 1st rib and laterally flex the neck to same side, Scalenus medius: Same action as scalenus anterior, Scalenus posterior: Elevate 2nd rib and tilt neck to opposite side, , Innervation, , Spinal nerves C4-6, , Origin, , Transverse processes C2 to C7, , Insertion, , First and second ribs, , Important, relations, , , , , The brachial plexus and subclavian artery pass between the anterior and, middle scalenes through a space called the scalene hiatus/fissure., The subclavian vein and phrenic nerve pass anteriorly to the anterior
Page 2082 :
scalene as it crosses over the first rib., , Image sourced from Wikipedia, , Thoracic outlet syndrome, The scalenes are at risk of adhering to the fascia surrounding the brachial plexus or shortening, causing compression of the brachial plexus when it passes between the clavicle and 1st rib causing, thoracic outlet syndrome., Next question
Page 2083 :
Question 435 of 560, A 56 year old man is having a long venous line inserted via the femoral vein into the right atrium for, CVP measurements. The catheter is advanced through the IVC. At which of the following levels, does this vessel enter the thorax?, , L2, , T10, , L1, , T8, , T6, , Theme from 2010 Exam, Theme from September 2012 Exam, The IVC passes through the diaphragm at T8., Please rate this question:, , Discuss and give feedback, , Next question, , Inferior vena cava, Origin, , , L5, , Path, , , , , , , Left and right common iliac veins merge to form the IVC., Passes right of midline, Paired segmental lumbar veins drain into the IVC throughout its length, The right gonadal vein empties directly into the cava and the left gonadal vein generally, empties into the left renal vein., The next major veins are the renal veins and the hepatic veins
Page 2084 :
, , , Pierces the central tendon of diaphragm at T8, Right atrium, , Image sourced from Wikipedia, , Relations, , Anteriorly, , Small bowel, first and third part of duodenum, head of pancreas, liver and bile duct,, right common iliac artery, right gonadal artery, , Posteriorly, , Right renal artery, right psoas, right sympathetic chain, coeliac ganglion, , Levels, , Level, , Vein, , T8, , Hepatic vein, inferior phrenic vein, pierces diaphragm, , L1, , Suprarenal veins, renal vein, , L2, , Gonadal vein
Page 2086 :
Question 436 of 560, , A 23 year old man falls and injures his hand. There are concerns that he may have a scaphoid, fracture as there is tenderness in his anatomical snuffbox on clinical examination. Which of the, following forms the posterior border of this structure?, , Basilic vein, , Radial artery, , Extensor pollicis brevis, , Abductor pollicis longus, , Extensor pollicis longus, , Theme from 2009 Exam, Theme from September 2012 Exam, Its boundaries are extensor pollicis longus, medially (posterior border) and laterally (anterior border), by the tendons of abductor pollicis longus and extensor pollicis brevis., Please rate this question:, , Discuss and give feedback, , Next question, , Anatomical snuffbox, Posterior border, , Tendon of extensor pollicis longus
Page 2087 :
Anterior border, , Tendons of extensor pollicis brevis and abductor pollicis longus, , Proximal border, , Styloid process of the radius, , Distal border, , Apex of snuffbox triangle, , Floor, , Trapezium and scaphoid, , Content, , Radial artery, , Image showing the anatomical snuffbox, , Image sourced from Wikipedia, , Next question
Page 2088 :
Question 437 of 560, , Which of the following structures attaches periosteum to bone?, , Sharpeys fibres, , Peripheral lamellae, , Elastic fibres, , Fibrolamellar bundles, , Purkinje fibres, , Periosteum is attached to bone by strong collagenous fibers called Sharpey's fibres, which extend to, the outer circumferential and interstitial lamellae. It also provides an attachment for muscles and, tendons., Please rate this question:, , Discuss and give feedback, , Next question, , Periosteum, Periosteum is a membrane that covers the outer surface of all bones, except at the joints of long, bones. Endosteum lines the inner surface of all bones., Periosteum consists of dense irregular connective tissue. Periosteum is divided into an outer "fibrous, layer" and inner "cambium layer" (or "osteogenic layer"). The fibrous layer contains fibroblasts, while, the cambium layer contains progenitor cells that develop into osteoblasts. These osteoblasts are, responsible for increasing the width of a long bone and the overall size of the other bone types. After, a bone fracture the progenitor cells develop into osteoblasts and chondroblasts, which are essential
Page 2089 :
to the healing process., As opposed to osseous tissue, periosteum has nociceptive nerve endings, making it very sensitive to, manipulation. It also provides nourishment by providing the blood supply. Periosteum is attached to, bone by strong collagenous fibers called Sharpey's fibres, which extend to the outer circumferential, and interstitial lamellae. It also provides an attachment for muscles and tendons., Periosteum that covers the outer surface of the bones of the skull is known as "pericranium" except, when in reference to the layers of the scalp., Next question
Page 2090 :
Question 438 of 560, A 62 year old man is undergoing a left hemicolectomy for carcinoma of the descending colon. The, registrar commences mobilisation of the left colon by pulling downwards and medially. Blood soon, appears in the left paracolic gutter. The most likely source of bleeding is the:, , Marginal artery, , Left testicular artery, , Spleen, , Left renal vein, , None of the above, , The spleen is commonly torn by traction injuries in colonic surgery. The other structures are, associated with bleeding during colonic surgery but would not manifest themselves as blood in the, paracolic gutter prior to incision of the paracolonic peritoneal edge., Please rate this question:, , Discuss and give feedback, , Next question, , Left colon, Position, , , , , , As the left colon passes inferiorly its posterior aspect becomes extraperitoneal, and the, ureter and gonadal vessels are close posterior relations that may become involved in, disease processes, At a level of L3-4 (variable) the left colon becomes the sigmoid colon and wholly, intraperitoneal once again, The sigmoid colon is a highly mobile structure and may even lie on the right side of the, abdomen, It passes towards the midline, the taenia blend and this marks the transition between sigmoid, colon and upper rectum
Page 2091 :
Blood supply, , , , Inferior mesenteric artery, However, the marginal artery (from the right colon) contributes, this contribution becomes, clinically significant when the IMA is divided surgically (e.g. During AAA repair), Next question
Page 2092 :
Question 439 of 560, A man is undergoing excision of a sub mandibular gland. As the gland is mobilised, a vessel is, injured lying between the gland and the mandible. Which of the following is this vessel most likely to, be?, , Lingual artery, , Occipital artery, , Superior thyroid artery, , Facial artery, , External jugular vein, The high salivary viscosity of submandibular gland secretions favors stone formation., Most stones are radio-opaque., The facial artery lies between the gland and mandible and is often ligated during excision of the, gland. The lingual artery may be encountered but this is usually later in the operative process as, Whartons duct is mobilised., Please rate this question:, , Discuss and give feedback, , Next question, , Submandibular gland, Relations of the submandibular gland, , Superficial, , Platysma, deep fascia and mandible, Submandibular lymph nodes, Facial vein (facial artery near mandible), Marginal mandibular nerve, Cervical branch of the facial nerve, , Deep, , Facial artery (inferior to the mandible), Mylohoid muscle
Page 2093 :
Sub mandibular duct, Hyoglossus muscle, Lingual nerve, Submandibular ganglion, Hypoglossal nerve, , Submandibular duct (Wharton's duct), , , , , Opens lateral to the lingual frenulum on the anterior floor of mouth., 5 cm length, Lingual nerve wraps around Wharton's duct. As the duct passes forwards it crosses medial, to the nerve to lie above it and then crosses back, lateral to it, to reach a position below the, nerve., , Innervation, , , , Sympathetic innervation- Derived from superior cervical ganglion, Parasympathetic innervation- Submandibular ganglion via lingual nerve, , Arterial supply, Branch of the facial artery. The facial artery passes through the gland to groove its deep surface. It, then emerges onto the face by passing between the gland and the mandible., Venous drainage, Anterior facial vein (lies deep to the Marginal Mandibular nerve), Lymphatic drainage, Deep cervical and jugular chains of nodes, Next question
Page 2094 :
Question 440-442 of 560, , Theme: Cranial nerves, , A. Facial, B. Trigeminal, C. Vagus, D. Hypoglossal, E. Glossopharyngeal, , For each of the following functions please select the most likely responsible cranial nerve. Each, option may be used once, more than once or not at all., , 440., , Supplies the motor fibres of styloglossus., You answered Facial, The correct answer is Hypoglossal, The hypoglossal nerve supplies motor innervation to all extrinsic and intrinsic muscles of the, tongue. The only possible exception to this is palatoglossus (which is jointly innervated by the, vagus and accessory nerves., , 441., , Provides general sensation to the anterior two thirds of the tongue., You answered Facial, The correct answer is Trigeminal, Taste to the anterior two thirds of the tongue is supplied by the facial nerve, the trigeminal, supplies general sensation, this is mediated by the mandibular branch of the trigeminal nerve, (via the lingual nerve).
Page 2095 :
442., , Supplies general sensation to the posterior third of the tongue., You answered Facial, The correct answer is Glossopharyngeal, The glossopharyngeal nerve supplies general sensation to the posterior third of the tongue and, contributes to the gag reflex., , Please rate this question:, , Discuss and give feedback, , Next question, , Cranial nerves, Cranial nerve lesions, , Olfactory nerve, , May be injured in basal skull fractures or involved in frontal lobe tumour extension., Loss of olfactory nerve function in relation to major CNS pathology is seldom an, isolated event and thus it is poor localiser of CNS pathology., , Optic nerve, , Problems with visual acuity may result from intra ocular disorders. Problems with, the blood supply such as amaurosis fugax may produce temporary visual distortion., More important surgically is the pupillary response to light. The pupillary size may, be altered in a number of disorders. Nerves involved in the resizing of the pupil, connect to the pretectal nucleus of the high midbrain, bypassing the lateral, geniculate nucleus and the primary visual cortex. From the pretectal nucleus, neurones pass to the Edinger - Westphal nucleus, motor axons from here pass along, with the oculomotor nerve. They synapse with ciliary ganglion neurones; the, parasympathetic axons from this then innervate the iris and produce miosis. The, miotic pupil is seen in disorders such as Horner's syndrome or opiate overdose., Mydriasis is the dilatation of the pupil in response to disease, trauma, drugs (or the, dark!). It is pathological when light fails to induce miosis. The radial muscle is
Page 2096 :
innervated by the sympathetic nervous system. Because the parasympathetic fibres, travel with the oculomotor nerve they will be damaged by lesions affecting this, nerve (e.g. cranial trauma)., The response to light shone in one eye is usually a constriction of both pupils. This, indicates intact direct and consensual light reflexes. When the optic nerve has an, afferent defect the light shining on the affected eye will produce a diminished, pupillary response in both eyes. Whereas light shone on the unaffected eye will, produce a normal pupillary response in both eyes. This is referred to as the Marcus, Gunn pupil and is seen in conditions such as optic neuritis. In a total CN II lesion, shining the light in the affected eye will produce no response., , Oculomotor nerve, , The pupillary effects are described above. In addition it supplies all ocular muscles, apart from lateral rectus and superior oblique. Thus the affected eye will be, deviated inferolaterally. Levator palpebrae superioris may also be impaired resulting, in impaired ability to open the eye., , Trochlear nerve, , The eye will not be able to look down., , Trigeminal nerve, , Largest cranial nerve. Exits the brainstem at the pons. Branches are ophthalmic,, maxillary and mandibular. Only the mandibular branch has both sensory and motor, fibres. Branches converge to form the trigeminal ganglion (located in Meckels cave)., It supplies the muscles of mastication and also tensor veli palatine, mylohyoid,, anterior belly of digastric and tensor tympani. The detailed descriptions of the, various sensory functions are described in other areas of the website. The corneal, reflex is important and is elicited by applying a small tip of cotton wool to the, cornea, a reflex blink should occur if it is intact. It is mediated by: the naso ciliary, branch of the ophthalmic branch of the trigeminal (sensory component) and the, facial nerve producing the motor response. Lesions of the afferent arc will produce, bilateral absent blink and lesions of the efferent arc will result in a unilateral absent, blink., , Abducens nerve, , The affected eye will have a deficit of abduction. This cranial nerve exits the, brainstem between the pons and medulla. It thus has a relatively long intra cranial, course which renders it susceptible to damage in raised intra cranial pressure., , Facial nerve, , Emerges from brainstem between pons and medulla. It controls muscles of facial, expression and taste from the anterior 2/3 of the tongue. The nerve passes into the
Page 2097 :
petrous temporal bone and into the internal auditory meatus. It then passes, through the facial canal and exits at the stylomastoid foramen. It passes through the, parotid gland and divides at this point. It does not innervate the parotid gland. Its, divisions are considered in other parts of the website. Its motor fibres innervate, orbicularis oculi to produce the efferent arm of the corneal reflex. In surgical, practice it may be injured during parotid gland surgery or invaded by malignancies, of the gland and a lower motor neurone on the ipsilateral side will result., , Vestibulo-cochlear, nerve, , Exits from the pons and then passes through the internal auditory meatus. It is, implicated in sensorineural hearing loss. Individuals with sensorineural hearing loss, will localise the sound in webers test to the normal ear. Rinnes test will be reduced, on the affected side but should still work. These two tests will distinguish, sensorineural hearing loss from conductive deafness. In the latter condition webers, test will localise to the affected ear and Rinnes test will be impaired on the affected, side. Surgical lesions affecting this nerve include CNS tumours and basal skull, fractures. It may also be damaged by the administration of ototoxic drugs (of which, gentamicin is the most commonly used in surgical practice)., , Glossopharyngeal, nerve, , Exits the pons just above the vagus. Receives sensory fibres from posterior 1/3, tongue, tonsils, pharynx and middle ear (otalgia may occur following tonsillectomy)., It receives visceral afferents from the carotid bodies. It supplies parasympathetic, fibres to the parotid gland via the otic ganglion and motor function to, stylopharyngeaus muscle. The sensory function of the nerve is tested using the gag, reflex., , Vagus nerve, , Leaves the medulla between the olivary nucleus and the inferior cerebellar, peduncle. Passes through the jugular foramen and into the carotid sheath. Details of, the functions of the vagus nerve are covered in the website under relevant organ, sub headings., , Accessory nerve, , Exists from the caudal aspect of the brainstem (multiple branches) supplies, trapezius and sternocleidomastoid muscles. The distal portion of this nerve is most, prone to injury during surgical procedures., , Hypoglossal nerve, , Emerges from the medulla at the preolivary sulcus, passes through the hypoglossal, canal. It lies on the carotid sheath and passes deep to the posterior belly of digastric, to supply muscles of the tongue (except palatoglossus). Its location near the carotid
Page 2098 :
sheath makes it vulnerable during carotid endarterectomy surgery and damage will, produce ipsilateral defect in muscle function., Next question
Page 2099 :
Question 443 of 560, , The integrity of which muscle is assessed by the Trendelenburg test?, , Sartorius, , Quadratus femoris, , Semimembranosus, , Gluteus medius, , Piriformis, , Theme from 2011 Exam, Please rate this question:, , Discuss and give feedback, , Next question, , Trendelenburg test, Injury or division of the superior gluteal nerve results in a motor deficit that consists of weakened, abduction of the thigh by gluteus medius, a disabling gluteus medius limp and a compensatory list of, the body to the weakened gluteal side. The compensation results in a gravitational shift so that the, body is supported on the unaffected limb., When a person is asked to stand on one leg, the gluteus medius usually contracts as soon as the, contralateral leg leaves the floor, preventing the pelvis from dipping towards the unsupported side., When a person with paralysis of the superior gluteal nerve is asked to stand on one leg, the pelvis, on the unsupported side descends, indicating that the gluteus medius on the affected side is weak or, non functional ( a positive Trendelenburg test).
Page 2100 :
This eponymous test also refers to a vascular investigation in which tourniquets are placed around, the upper thigh, these can help determine whether saphenofemoral incompetence is present., Next question
Page 2101 :
Question 444 of 560, A 52 year old female renal patient needs a femoral catheter to allow for haemodialysis. Which of the, structures listed below is least likely to be encountered during its insertion?, , Great saphenous vein, , Deep circumflex iliac artery, , Superficial circumflex iliac artery, , Femoral vein, , Femoral branch of the genitofemoral nerve, , Femoral access catheters are typically inserted in the region of the femoral triangle. Therefore the, physician may encounter the femoral, vein, nerve, branches of the femoral artery and tributaries of, the femoral vein. The deep circumflex iliac artery arises above the inguinal ligament and is therefore, less likely to be encountered than the superficial circumflex iliac artery which arises below the, inguinal ligament., Please rate this question:, , Discuss and give feedback, , Next question, , Femoral triangle anatomy, Boundaries, , Superiorly, , Inguinal ligament, , Laterally, , Sartorius, , Medially, , Adductor longus, , Floor, , Iliopsoas, adductor longus and pectineus
Page 2102 :
, , , , Roof, , Fascia lata and Superficial fascia, Superficial inguinal lymph nodes (palpable below the inguinal ligament), Long saphenous vein, , Image sourced from Wikipedia, , Contents, , , , , , , , , Femoral vein (medial to lateral), Femoral artery-pulse palpated at the mid inguinal point, Femoral nerve, Deep and superficial inguinal lymph nodes, Lateral cutaneous nerve, Great saphenous vein, Femoral branch of the genitofemoral nerve, Next question
Page 2103 :
Question 445 of 560, A 53 year old man with a chronically infected right kidney is due to undergo a nephrectomy. Which of, the following structures would be encountered first during a posterior approach to the hilum of the, right kidney?, , Right renal artery, , Ureter, , Right renal vein, , Inferior vena cava, , Right testicular vein, , The ureter is the most posterior structure at the hilum of the right kidney and would therefore be, encountered first during a posterior approach., Please rate this question:, , Discuss and give feedback, , Next question, , Renal arteries, , , , The right renal artery is longer than the left renal artery, The renal vein/artery/pelvis enter the kidney at the hilum, , Relations, , Right, , Anterior- IVC, right renal vein, the head of the pancreas, and the descending part of the, duodenum, , Left, , Anterior- left renal vein, the tail of the pancreas, , Branches
Page 2104 :
, , , , , The renal arteries are direct branches off the aorta (upper border of L2- right side and L1 left side), In 30% there may be accessory arteries (mainly left side). Instead of entering the kidney at, the hilum, they usually pierce the upper or lower part of the organ., Before reaching the hilum of the kidney, each artery divides into four or five segmental, branches (renal vein anterior and ureter posterior); which then divide within the sinus into, lobar arteries supplying each pyramid and cortex., Each vessel gives off some small inferior suprarenal branches to the suprarenal gland, the, ureter, and the surrounding cellular tissue and muscles., Next question
Page 2105 :
Question 446 of 560, A 28 year old man is stabbed outside a nightclub in the upper arm. The median nerve is transected., Which of the following muscles will demonstrate impaired function as a result?, , Palmaris brevis, , Second and third interossei, , Adductor pollicis, , Abductor pollicis longus, , Abductor pollicis brevis, Palmaris brevis - Ulnar nerve, Palmar interossei- Ulnar nerve, Adductor pollicis - Ulnar nerve, Abductor pollicis longus - Posterior interosseous nerve, Abductor pollicis brevis - Median nerve, The median nerve innervates all the short muscles of the thumb except the adductor and the deep, head of the short flexor. Palmaris and the interossei are innervated by the ulnar nerve., Please rate this question:, , Discuss and give feedback, , Next question, , Median nerve, The median nerve is formed by the union of a lateral and medial root respectively from the lateral, (C5,6,7) and medial (C8 and T1) cords of the brachial plexus; the medial root passes anterior to the, third part of the axillary artery. The nerve descends lateral to the brachial artery, crosses to its, medial side (usually passing anterior to the artery). It passes deep to the bicipital aponeurosis and, the median cubital vein at the elbow., It passes between the two heads of the pronator teres muscle, and runs on the deep surface of, flexor digitorum superficialis (within its fascial sheath)., Near the wrist it becomes superficial between the tendons of flexor digitorum superficialis and flexor, carpi radialis, deep to palmaris longus tendon. It passes deep to the flexor retinaculum to enter the, palm, but lies anterior to the long flexor tendons within the carpal tunnel., Branches
Page 2107 :
, , , , unable to pronate forearm, weak wrist flexion, ulnar deviation of wrist, , Anterior interosseous nerve (branch of median nerve), , , , leaves just below the elbow, results in loss of pronation of forearm and weakness of long flexors of thumb and index, finger, , Topography of the median nerve, , Image sourced from Wikipedia, , Next question
Page 2108 :
Question 447 of 560, A 22 year old man sustains a blow to the side of his head with a baseball bat during a fight. He is, initially conscious. However, he subsequently loses consciousness and then dies. Post mortem, examination shows an extradural haematoma. The most likely culprit vessel is a branch of which of, the following?, , Middle cerebral artery, , Internal carotid artery, , Anterior cerebral artery, , Maxillary artery, , Mandibular artery, , The middle meningeal artery is the most likely source of the extradural haematoma in this setting. It, is a branch of the maxillary artery. The middle cerebral artery does not give rise to the middle, meningeal artery. Note that the question is asking for the vessel which gives rise to the middle, meningeal artery ("the likely culprit vessel is a branch of which of the following"), Please rate this question:, , Discuss and give feedback, , Next question, , Middle meningeal artery, , , , , , , , Middle meningeal artery is typically the third branch of the first part of the maxillary artery,, one of the two terminal branches of the external carotid artery. After branching off the, maxillary artery in the infratemporal fossa, it runs through the foramen spinosum to supply, the dura mater (the outermost meninges) ., The middle meningeal artery is the largest of the three (paired) arteries which supply the, meninges, the others being the anterior meningeal artery and the posterior meningeal artery., The middle meningeal artery runs beneath the pterion. It is vulnerable to injury at this point,, where the skull is thin. Rupture of the artery may give rise to an extra dural hematoma., In the dry cranium, the middle meningeal, which runs within the dura mater surrounding the, brain, makes a deep indention in the calvarium., The middle meningeal artery is intimately associated with the auriculotemporal nerve which, wraps around the artery making the two easily identifiable in the dissection of human, cadavers and also easily damaged in surgery.
Page 2109 :
Question 448 of 560, A 72 year old man with carcinoma of the lung is undergoing a left pneumonectomy. The left main, bronchus is divided. Which of the following thoracic vertebrae lies posterior to this structure?, , T3, , T7, , T6, , T10, , T1, , The left main bronchus lies at T6. Topographical anatomy of the thorax is important as it helps, surgeons to predict the likely structures to be injured in trauma scenarios (so popular with, examiners), Please rate this question:, , Discuss and give feedback, , Next question, , Lung anatomy, The right lung is composed of 3 lobes divided by the oblique and transverse fissures. The left lung, has two lobes divided by the oblique fissure.The apex of both lungs is approximately 4cm superior to, the sterno-costal joint of the first rib. Immediately below this is a sulcus created by the subclavian, artery., Peripheral contact points of the lung, , , , , Base: diaphragm, Costal surface: corresponds to the cavity of the chest, Mediastinal surface: Contacts the mediastinal pleura. Has the cardiac impression. Above and, behind this concavity is a triangular depression named the hilum, where the structures which, form the root of the lung enter and leave the viscus. These structures are invested by pleura,, which, below the hilum and behind the pericardial impression, forms the pulmonary ligament
Page 2110 :
Right lung, Above the hilum is the azygos vein; Superior to this is the groove for the superior vena cava and, right innominate vein; behind this, and nearer the apex, is a furrow for the innominate artery. Behind, the hilum and the attachment of the pulmonary ligament is a vertical groove for the oesophagus; In, front and to the right of the lower part of the oesophageal groove is a deep concavity for the, extrapericardiac portion of the inferior vena cava., The root of the right lung lies behind the superior vena cava and the right atrium, and below the, azygos vein., The right main bronchus is shorter, wider and more vertical than the left main bronchus and, therefore the route taken by most foreign bodies., , Image sourced from Wikipedia, , Left lung, Above the hilum is the furrow produced by the aortic arch, and then superiorly the groove, accommodating the left subclavian artery; Behind the hilum and pulmonary ligament is a vertical, groove produced by the descending aorta, and in front of this, near the base of the lung, is the lower, part of the oesophagus., The root of the left lung passes under the aortic arch and in front of the descending aorta.
Page 2111 :
Image sourced from Wikipedia, , Inferior borders of both lungs, , , , , 6th rib in mid clavicular line, 8th rib in mid axillary line, 10th rib posteriorly, , The pleura runs two ribs lower than the corresponding lung level., Bronchopulmonary segments, , Segment number, , Right lung, , Left lung, , 1, , Apical, , Apical, , 2, , Posterior, , Posterior, , 3, , Anterior, , Anterior, , 4, , Lateral, , Superior lingular, , 5, , Medial, , Inferior lingular, , 6, , Superior (apical), , Superior (apical)
Page 2112 :
Segment number, , Right lung, , Left lung, , 7, , Medial basal, , Medial basal, , 8, , Anterior basal, , Anterior basal, , 9, , Lateral basal, , Lateral basal, , 10, , Posterior basal, , Posterior basal, Next question
Page 2113 :
Question 449 of 560, , Which of the following regions of the male urethra is entirely surrounded by Bucks fascia?, , Preprostatic part, , Prostatic part, , Membranous part, , Spongiose part, , None of the above, , Theme from 2010 Exam, Bucks fascia is a layer of deep fascia that covers the penis it is continuous with the external, spermatic fascia and the penile suspensory ligament. The membranous part of the urethra may, partially pass through Bucks fascia as it passes into the penis. However, the spongiose part of the, urethra is contained wholly within Bucks fascia., Image of penile cross section, Bucks fascia corresponds to the layer of deep fascia, , Image sourced from Wikipedia, , Please rate this question:
Page 2114 :
Discuss and give feedback, , Next question, , Urethral anatomy, Female urethra, The female urethra is shorter and more acutely angulated than the male urethra. It is an extraperitoneal structure and embedded in the endopelvic fascia. The neck of the bladder is subjected to, transmitted intra-abdominal pressure and therefore deficiency in this area may result in stress, urinary incontinence. Between the layers of the urogenital diaphragm the female urethra is, surrounded by the external urethral sphincter, this is innervated by the pudendal nerve. It ultimately, lies anterior to the vaginal orifice., Male urethra, In males the urethra is much longer and is divided into four parts., , Pre-prostatic, urethra, , Extremely short and lies between the bladder and prostate gland.It has a stellate lumen, and is between 1 and 1.5cm long.Innervated by sympathetic noradrenergic fibres, as, this region is composed of striated muscles bundles they may contract and prevent, retrograde ejaculation., , Prostatic, urethra, , This segment is wider than the membranous urethra and contains several openings for, the transmission of semen (at the midpoint of the urethral crest)., , Membranous, urethra, , Narrowest part of the urethra and surrounded by external sphincter. It traverses the, perineal membrane 2.5cm postero-inferior to the symphysis pubis., , Penile urethra, , Travels through the corpus spongiosum on the underside of the penis. It is the longest, urethral segment.It is dilated at its origin as the infrabulbar fossa and again in the gland, penis as the navicular fossa. The bulbo-urethral glands open into the spongiose section, of the urethra 2.5cm below the perineal membrane., , The urothelium is transitional in nature near to the bladder and becomes squamous more distally., Next question
Page 2115 :
Question 450 of 560, Which of the following statements relating to the knee joint is false?, , It is the largest synovial joint in the body, , When the knee is fully extended all ligaments of the knee joint are taut, , Rupture of the anterior cruciate ligament may result in haemarthrosis, , The posterior aspect of the patella is extrasynovial, , The joint is innervated by the femoral, sciatic and obturator nerves, , The posterior aspect is intrasynovial and the knee itself comprises the largest synovial joint in the, body. It may swell considerably following trauma such as ACL injury. Which may be extremely, painful owing to rich innervation from femoral, sciatic and ( a smaller) contribution from the obturator, nerve. During full extension all ligaments are taut and the knee is locked., Please rate this question:, , Discuss and give feedback, , Next question, , Knee joint, The knee joint is a synovial joint, the largest and most complicated. It consists of two condylar joints, between the femur and tibia and a sellar joint between the patella and the femur. The tibiofemoral, articular surfaces are incongruent, however, this is improved by the presence of the menisci. The, degree of congruence is related to the anatomical position of the knee joint and is greatest in full, extension., Knee joint compartments, , Tibiofemoral, , , , Patellofemoral, , , , Comprised of the patella/femur joint, lateral and medial compartments, (between femur condyles and tibia), Synovial membrane and cruciate ligaments partially separate the medial, and lateral compartments, , Ligamentum patellae
Page 2116 :
, , Actions: provides joint stability in full extension, , Fibrous capsule, The capsule of the knee joint is a complex, composite structure with contributions from adjacent, tendons., Anterior, fibres, , The capsule does not pass proximal to the patella. It blends with the tendinous, expansions of vastus medialis and lateralis, , Posterior, fibres, , These fibres are vertical and run from the posterior surface of the femoral condyles, to the posterior aspect of the tibial condyle, , Medial fibres, , Attach to the femoral and tibial condyles beyond their articular margins, blending, with the tibial collateral ligament, , Lateral, fibres, , Attach to the femur superior to popliteus, pass over its tendon to head of fibula and, tibial condyle, , Bursae, , Anterior, , Laterally, , Medially, , Posterior, , , , , , Subcutaneous prepatellar bursa; between patella and skin, Deep infrapatellar bursa; between tibia and patellar ligament, Subcutaneous infrapatellar bursa; between distal tibial tuberosity and skin, , , , , , Bursa between lateral head of gastrocnemius and joint capsule, Bursa between fibular collateral ligament and tendon of biceps femoris, Bursa between fibular collateral ligament and tendon of popliteus, , , , , Bursa between medial head of gastrocnemius and the fibrous capsule, Bursa between tibial collateral ligament and tendons of sartorius, gracilis and, semitendinosus, Bursa between the tendon of semimembranosus and medial tibial condyle and, medial head of gastrocnemius, , , , Highly variable and inconsistent, , Ligaments, , Medial collateral, ligament, , Medial epicondyle femur to medial tibial condyle: valgus stability, , Lateral collateral, ligament, , Lateral epicondyle femur to fibula head: varus stability
Page 2117 :
Anterior cruciate, ligament, , Anterior tibia to lateral intercondylar notch femur: prevents tibia sliding, anteriorly, , Posterior cruciate, ligament, , Posterior tibia to medial intercondylar notch femur: prevents tibia, sliding posteriorly, , Patellar ligament, , Central band of the tendon of quadriceps femoris, extends from patella, to tibial tuberosity, , Image sourced from Wikipedia
Page 2118 :
Image sourced from Wikipedia, , © Image provided by the University of Sheffield, , Menisci, Medial and lateral menisci compensate for the incongruence of the femoral and tibial condyles., Composed of fibrous tissue., Medial meniscus is attached to the tibial collateral ligament., Lateral meniscus is attached to the loose fibres at the lateral edge of the joint and is separate from, the fibular collateral ligament. The lateral meniscus is crossed by the popliteus tendon.
Page 2119 :
Nerve supply, The knee joint is supplied by the femoral, tibial and common peroneal divisions of the sciatic and by, a branch from the obturator nerve. Hip pathology pain may be referred to the knee., Blood supply, Genicular branches of the femoral artery, popliteal and anterior tibial arteries all supply the knee, joint., Next question
Page 2120 :
Question 451 of 560, In the distal third of the upper arm, where is the musculocutaneous nerve located?, , Between the biceps brachii and brachialis muscles, , Between the brachialis and brachioradialis muscles, , Between the brachioradialis and triceps muscles, , Between the brachialis and triceps muscles, , Between the humerus and brachialis muscles, , The musculocutaneous nerve lies between the biceps and brachialis muscles., Please rate this question:, , Discuss and give feedback, , Next question, , Musculocutaneous nerve, , , Branch of lateral cord of brachial plexus, , Path, , , , , , It penetrates the coracobrachialis muscle, Passes obliquely between the biceps brachii and the brachialis to the lateral side of the arm, Above the elbow it pierces the deep fascia lateral to the tendon of the biceps brachii, Continues into the forearm as the lateral cutaneous nerve of the forearm, , Innervates, , , , , , Coracobrachialis, Biceps brachii, Brachialis, Question 452 of 560
Page 2121 :
, , , A 48 year old lady is undergoing a left sided adrenalectomy for an adrenal adenoma. The, superior adrenal artery is injured and starts to bleed, from which of the following does this, vessel arise?, , Left renal artery, , Inferior phrenic artery, , Aorta, , Splenic, , None of the above, , , , The superior adrenal artery is a branch of the inferior phrenic artery., Please rate this question:, , , , , , Discuss and give feedback, , , , , , Adrenal gland anatomy, , , , Anatomy, , Next question, , Location, , Superomedially to the upper pole of each kidney, , Relationships of the right, adrenal, , Diaphragm-Posteriorly, Kidney-Inferiorly, Vena Cava-Medially, Hepato-renal, pouch and bare area of the liver-Anteriorly, , Relationships of the left, , Crus of the diaphragm-Postero- medially, Pancreas and splenic vessels-
Page 2122 :
adrenal, , Inferiorly, Lesser sac and stomach-Anteriorly, , Arterial supply, , Superior adrenal arteries- from inferior phrenic artery, Middle adrenal, arteries - from aorta, Inferior adrenal arteries -from renal arteries, , Venous drainage of the, right adrenal, , Via one central vein directly into the IVC, , Venous drainage of the, left adrenal, , Via one central vein into the left renal vein, , , , , Next question
Page 2123 :
Question 453 of 560, Which of the following does not exit the pelvis through the greater sciatic foramen?, , Superior gluteal artery, , Internal pudendal vessels, , Sciatic nerve, , Obturator nerve, , Inferior gluteal nerve, , The obturator nerve exits through the obturator foramen., Please rate this question:, , Discuss and give feedback, , Next question, , Greater sciatic foramen, Contents, , Nerves, , , , , , , , , Sciatic Nerve, Superior and Inferior Gluteal Nerves, Pudendal Nerve, Posterior Femoral Cutaneous Nerve, Nerve to Quadratus Femoris, Nerve to Obturator internus, , Vessels, , , , , , Superior Gluteal Artery and vein, Inferior Gluteal Artery and vein, Internal Pudendal Artery and vein, , Piriformis, The piriformis is a landmark for identifying structures passing out of the sciatic notch
Page 2128 :
*= In life the foramen lacerum is occluded by a cartilagenous plug. The ICA initially passes into the, carotid canal which ascends superomedially to enter the cranial cavity through the foramen lacerum., Base of skull anatomical overview, , Image sourced from Wikipedia, , Next question
Page 2129 :
Question 455 of 560, , An 80 year old lady with a caecal carcinoma is undergoing a right hemicolectomy performed through, a transverse incision. The procedure is difficult and the incision is extended medially by dividing the, rectus sheath. Brisk arterial haemorrhage ensues. From which of the following does the damaged, vessel originate?, , Internal iliac artery, , External iliac artery, , Superior vesical artery, , Inferior vesical artery, , None of the above, , The vessel damaged is the epigastric artery. This originates from the external iliac artery (see, below)., Please rate this question:, , Discuss and give feedback, , Next question, , Epigastric artery, The inferior epigastric artery arises from the external iliac artery immediately above the inguinal, ligament. It then passes along the medial margin of the deep inguinal ring. From here it continues, superiorly to lie behind the rectus abdominis muscle., This is illustrated below:
Page 2130 :
Image sourced from Wikipedia, , Next question
Page 2131 :
Question 456 of 560, , A 73 year old man has a large abdominal aortic aneurysm. During a laparotomy for planned surgical, repair the surgeons find the aneurysm is far more proximally located and lies near the origin of the, SMA. During the dissection a vessel lying transversely across the aorta is injured. What is this, vessel most likely to be?, , Left renal vein, , Right renal vein, , Inferior mesenteric artery, , Ileocolic artery, , Middle colic artery, , Theme from April 2012 Exam, The left renal vein runs across the surface of the aorta and may require deliberate ligation during, juxtarenal aneurysm repair., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal aorta, Abdominal aortic topography, , Origin, , T12
Page 2133 :
Image sourced from Wikipedia, , Next question
Page 2134 :
Question 457 of 560, Which of the following is not a branch of the posterior cord of the brachial plexus?, , Thoracodorsal nerve, , Axillary nerve, , Radial nerve, , Lower subscapular nerve, , Musculocutaneous nerve, Mnemonic branches off the posterior cord, S ubscapular (upper and lower), T horacodorsal, A xillary, R adial, The musculocutaneous nerve is a branch off the lateral cord., Please rate this question:, , Discuss and give feedback, , Next question, , Brachial plexus, Origin, , Anterior rami of C5 to T1, , Sections of the, plexus, , , , , Roots, trunks, divisions, cords, branches, Mnemonic:Real Teenagers Drink Cold Beer, , Roots, , , , , Located in the posterior triangle, Pass between scalenus anterior and medius
Page 2135 :
Trunks, , , , , , Located posterior to middle third of clavicle, Upper and middle trunks related superiorly to the subclavian artery, Lower trunk passes over 1st rib posterior to the subclavian artery, , Divisions, , Apex of axilla, , Cords, , Related to axillary artery, , Diagram illustrating the branches of the brachial plexus, , Image sourced from Wikipedia, , Cutaneous sensation of the upper limb
Page 2136 :
Image sourced from Wikipedia, , Next question
Page 2137 :
Question 458 of 560, A 18 year old man presents with an indirect inguinal hernia and undergoes surgery. The deep, inguinal ring is exposed and held with a retractor at its medial aspect. Which structure is most likely, to lie under the retractor?, , Ureter, , Inferior epigastric artery, , Internal iliac vein, , Femoral artery, , Lateral border of rectus abdominis, Boundaries of the deep inguinal ring:, , , , Superolaterally - transversalis fascia, Inferomedially - inferior epigastric artery, , The deep inguinal ring is closely related to the inferior epigastric artery. The inferior epigastric artery, forms part of the structure referred to as Hesselbach's triangle.
Page 2138 :
Image sourced from Wikipedia, , Please rate this question:, , Discuss and give feedback, , Next question, , Inguinal canal, Location, , , , , , Above the inguinal ligament, The inguinal canal is 4cm long, The superficial ring is located anterior to the pubic tubercle, The deep ring is located approximately 1.5-2cm above the half way point between the, anterior superior iliac spine and the pubic tubercle, , Boundaries of the inguinal canal, , Floor, , , , , , External oblique aponeurosis, Inguinal ligament, Lacunar ligament
Page 2139 :
, , , Roof, , Anterior wall, , Internal oblique, Transversus abdominis, , External oblique aponeurosis, , Posterior wall, , , , , Transversalis fascia, Conjoint tendon, , Laterally, , , , , Internal ring, Fibres of internal oblique, , Medially, , , , , External ring, Conjoint tendon, , Contents, , Males, , Spermatic cord and ilioinguinal, nerve, , As it passes through the canal the spermatic cord, has 3 coverings:, , , , , Females, , External spermatic fascia from external, oblique aponeurosis, Cremasteric fascia, Internal spermatic fascia, , Round ligament of uterus and, ilioinguinal nerve, , Related anatomy of the inguinal region, The boundaries of Hesselbachs triangle are commonly tested and illustrated below:
Page 2140 :
Image sourced from Wikipedia, , The image below demonstrates the close relationship of the vessels to the lower limb with the, inguinal canal. A fact to be borne in mind when repairing hernial defects in this region., , Image sourced from Wikipedia, , Next question
Page 2141 :
Question 459 of 560, A 73 year old man presents with a tumour at the tip of his tongue. To which of the following regions, will the tumour initially metastasise?, , Sub mental nodes, , Ipsilateral deep cervical nodes, , Tonsil, , Ipsilateral superficial cervical nodes, , Contralateral deep cervical nodes, , Please rate this question:, , Discuss and give feedback, , Next question, , Lymphatic drainage of the tongue, , , , , , The lymphatic drainage of the anterior two thirds of the tongue shows only minimal, communication of lymphatics across the midline, so metastasis to the ipsilateral nodes is, usual., The lymphatic drainage of the posterior third of the tongue have communicating networks, as, a result early bilateral nodal metastases are more common in this area., Lymphatics from the tip of the tongue usually pass to the sub mental nodes and from there to, the deep cervical nodes., Lymphatics from the mid portion of the tongue usually drain to the submandibular nodes and, then to the deep cervical nodes. Mid tongue tumours that are laterally located will usually, drain to the ipsilateral deep cervical nodes, those from more central regions may have, bilateral deep cervical nodal involvement., Next question
Page 2142 :
Question 460 of 560, A 78 year old man is undergoing a femoro-popliteal bypass graft. The operation is not progressing, well and the surgeon is complaining of poor access. Retraction of which of the following structures, will improve access to the femoral artery in the groin?, , Quadriceps, , Adductor longus, , Adductor magnus, , Pectineus, , Sartorius, , At the lower border of the femoral triangle the femoral artery passes under the sartorius muscle. This, can be retracted to improve access., Please rate this question:, , Discuss and give feedback, , Next question, , Femoral triangle anatomy, Boundaries, , Superiorly, , Inguinal ligament, , Laterally, , Sartorius, , Medially, , Adductor longus, , Floor, , Iliopsoas, adductor longus and pectineus
Page 2143 :
, , , , Roof, , Fascia lata and Superficial fascia, Superficial inguinal lymph nodes (palpable below the inguinal ligament), Long saphenous vein, , Image sourced from Wikipedia, , Contents, , , , , , , , , Femoral vein (medial to lateral), Femoral artery-pulse palpated at the mid inguinal point, Femoral nerve, Deep and superficial inguinal lymph nodes, Lateral cutaneous nerve, Great saphenous vein, Femoral branch of the genitofemoral nerve, Next question
Page 2144 :
Question 461 of 560, A builder falls off a ladder whilst laying roof tiles. He sustains a burst fracture of L3. The MRI scan, shows complete nerve transection at this level, as a result of the injury. Which clinical sign will not be, present initially?, , Flaccid paralysis of the legs, , Extensor plantar response, , Sensory loss in the legs, , Incontinence, , Areflexia, In lower motor neuron lesions everything is reduced, , The main purpose of this question is to differentiate the features of an UMN lesion and a LMN lesion., The features of a LMN lesion include:, , , , , , Flaccid paralysis of muscles supplied, Atrophy of muscles supplied., Loss of reflexes of muscles supplied., Muscles fasciculation, , For lesions below L1 LMN signs will occur. Hence in an L3 lesion, there will be loss of the patella, reflex but there will be no extensor plantar reflex., Please rate this question:, , Discuss and give feedback, , Next question, , Spinal cord, , , , Located in a canal within the vertebral column that affords it structural support., Rostrally it continues to the medulla oblongata of the brain and caudally it tapers at a level, corresponding to the L1-2 interspace (in the adult), a central structure, the filum terminale, anchors the cord to the first coccygeal vertebra.
Page 2145 :
, , The spinal cord is characterised by cervico-lumbar enlargements and these, broadly, speaking, are the sites which correspond to the brachial and lumbar plexuses respectively., , There are some key points to note when considering the surgical anatomy of the spinal cord:, * During foetal growth the spinal cord becomes shorter than the spinal canal, hence the adult site of, cord termination at the L1-2 level., * Due to growth of the vertebral column the spine segmental levels may not always correspond to, bony landmarks as they do in the cervical spine., * The spinal cord is incompletely divided into two symmetrical halves by a dorsal median, sulcus andventral median fissure. Grey matter surrounds a central canal that is continuous, rostrally with the ventricular system of the CNS., * The grey matter is sub divided cytoarchitecturally into Rexeds laminae., * Afferent fibres entering through the dorsal roots usually terminate near their point of entry but may, travel for varying distances in Lissauers tract. In this way they may establish synaptic connections, over several levels, * At the tip of the dorsal horn are afferents associated with nociceptive stimuli. The ventral horn, contains neurones that innervate skeletal muscle., The key point to remember when revising CNS anatomy is to keep a clinical perspective in mind. So, it is worth classifying the ways in which the spinal cord may become injured. These include:, , , , , , , , Trauma either direct or as a result of disc protrusion, Neoplasia either by direct invasion (rare) or as a result of pathological vertebral fracture, Inflammatory diseases such as Rheumatoid disease, or OA (formation of osteophytes, compressing nerve roots etc., Vascular either as a result of stroke (rare in cord) or as complication of aortic dissection, Infection historically diseases such as TB, epidural abscesses., , The anatomy of the cord will, to an extent dictate the clinical presentation. Some points/ conditions to, remember:, , , , , Brown- Sequard syndrome-Hemisection of the cord producing ipsilateral loss of, proprioception and upper motor neurone signs, plus contralateral loss of pain and, temperature sensation. The explanation of this is that the fibres decussate at different levels., Lesions below L1 will tend to present with lower motor neurone signs, Next question
Page 2146 :
Question 462 of 560, A 56 year old machinist has his arm entrapped in a steel grinder and is brought to the emergency, department. On examination, he is unable to extend his metacarpophalangeal joints and abduct his, shoulder. He has weakness of his elbow and wrist. What has been injured?, , Ulnar nerve, , Axillary nerve, , Medial cord of brachial plexus, , Lateral cord of brachial plexus, , Posterior cord of brachial plexus, The posterior cord gives rise to:, , , , , , , Radial nerve ((innervates the triceps, brachioradialis, wrist extensors, and finger extensors), Axillary nerve (innervates deltoid and teres minor), Upper subscapular nerve (innervates subscapularis), Lower subscapular nerve (innervates teres major and subscapularis), Thoracodorsal nerve (innervates latissimus dorsi), , Theme from September 2012 exam, This is a description of a posterior cord lesion. Remember that the posterior cord gives rise to the, axillary and radial nerve., Please rate this question:, , Discuss and give feedback, , Next question, , Cords of the brachial plexus, The brachial plexus cords are described according to their relationship with the axillary artery. The, cords pass over the 1st rib near to the dome of the lung and pass beneath the clavicle immediately, posterior to the subclavian artery., Lateral cord
Page 2148 :
Question 463 of 560, A 66 year old man with peripheral vascular disease is undergoing a below knee amputation. In which, of the lower leg compartments does peroneus brevis lie?, , Lateral compartment, , Anterior compartment, , Superficial posterior compartment, , Deep posterior compartment, , None of the above, , The interosseous membrane separates the anterior and posterior compartments. The deep and, superficial compartments are separated by the deep transverse fascia. The peroneus brevis is part, of the lateral compartment., Please rate this question:, , Discuss and give feedback, , Next question, , Fascial compartments of the leg, Compartments of the thigh, Formed by septae passing from the femur to the fascia lata., , Compartment, , Nerve, , Muscles, , Blood supply, , Anterior compartment, , Femoral, , , , , , , Iliacus, Tensor fasciae latae, Sartorius, Quadriceps femoris, , Femoral artery, , Medial compartment, , Obturator, , , , Adductor, longus/magnus/brevis, , Profunda femoris artery, and obturator artery
Page 2150 :
Question 464 of 560, A 70 year old man is due to undergo an arterial bypass procedure for claudication and foot, ulceration. The anterior tibial artery will form the site of the distal arterial anastomosis. Which of the, following structures is not closely related to it?, , Interosseous membrane, , Deep peroneal nerve, , Tibialis posterior, , Extensor hallucis longus, , Dorsalis pedis artery, , As an artery of the anterior compartment, the anterior tibial artery is closely related to tibialis anterior., Please rate this question:, , Discuss and give feedback, , Next question, , Anterior tibial artery, , , , , , , Begins opposite the distal border of popliteus, Terminates in front of the ankle, continuing as the dorsalis pedis artery, As it descends it lies on the interosseous membrane, distal part of the tibia and front of the, ankle joint, Passes between the tendons of extensor digitorum and extensor hallucis longus distally, It is related to the deep peroneal nerve, it lies anterior to the middle third of the vessel and, lateral to it in the lower third, Next question
Page 2152 :
, , , Transverse ligament: joints anterior and posterior ends of the articular cartilage, Head of femur ligament (ligamentum teres): acetabular notch to the fovea. Contains arterial, supply to head of femur in children., , Image sourced from Wikipedia, , Image sourced from Wikipedia
Page 2154 :
Question 466 of 560, Which of the following is not a content of the posterior triangle of the neck?, , Spinal accessory nerve, , Phrenic nerve, , External jugular vein, , Occipital lymph nodes, , Internal jugular vein, , The IJV does not lie in the posterior triangle. However, the terminal branches of the external jugular, vein do., Please rate this question:, , Discuss and give feedback, , Next question, , Posterior triangle of the neck, Boundaries, , Apex, , Sternocleidomastoid and the Trapezius muscles at the Occipital bone, , Anterior, , Posterior border of the Sternocleidomastoid, , Posterior, , Anterior border of the Trapezius, , Base, , Middle third of the clavicle
Page 2155 :
Image sourced from Wikipedia, , Contents, , Nerves, , , , , , , Accessory nerve, Phrenic nerve, Three trunks of the brachial plexus, Branches of the cervical plexus: Supraclavicular nerve, transverse cervical, nerve, great auricular nerve, lesser occipital nerve, , Vessels, , , , , External jugular vein, Subclavian artery, , Muscles, , , , , Inferior belly of omohyoid, Scalene, , Lymph, nodes, , , , , Supraclavicular, Occipital, Next question
Page 2156 :
Question 467 of 560, Which nerve is at risk during submandibular gland excision?, , Maxillary nerve, , Buccal nerve, , Zygomatic nerve, , Marginal mandibular nerve, , Cervical nerve, , The marginal mandibular nerve lies deep to platysma. It supplies the depressor anguli oris and the, depressor labii inferioris. If injured it may lead to facial asymmetry and dribbling., Please rate this question:, , Discuss and give feedback, , Next question, , Submandibular gland, Relations of the submandibular gland, , Superficial, , Platysma, deep fascia and mandible, Submandibular lymph nodes, Facial vein (facial artery near mandible), Marginal mandibular nerve, Cervical branch of the facial nerve, , Deep, , Facial artery (inferior to the mandible), Mylohoid muscle, Sub mandibular duct, Hyoglossus muscle, Lingual nerve, Submandibular ganglion
Page 2157 :
Hypoglossal nerve, , Submandibular duct (Wharton's duct), , , , , Opens lateral to the lingual frenulum on the anterior floor of mouth., 5 cm length, Lingual nerve wraps around Wharton's duct. As the duct passes forwards it crosses medial, to the nerve to lie above it and then crosses back, lateral to it, to reach a position below the, nerve., , Innervation, , , , Sympathetic innervation- Derived from superior cervical ganglion, Parasympathetic innervation- Submandibular ganglion via lingual nerve, , Arterial supply, Branch of the facial artery. The facial artery passes through the gland to groove its deep surface. It, then emerges onto the face by passing between the gland and the mandible., Venous drainage, Anterior facial vein (lies deep to the Marginal Mandibular nerve), Lymphatic drainage, Deep cervical and jugular chains of nodes, Next question
Page 2158 :
Question 468 of 560, In a patient with a carcinoma of the distal sigmoid colon, what is the most likely source of its blood, supply?, , Ileocolic artery, , External iliac artery, , Internal iliac artery, , Superior mesenteric artery, , Inferior mesenteric artery, , Theme from September 2013 Exam, During a high anterior resection of such tumours, the inferior mesenteric artery is ligated. Note that, the branches (mainly middle rectal branch) of the internal iliac artery are important in maintaining, vascularity of the rectal stump and hence the integrity of the anastomoses., Please rate this question:, , Discuss and give feedback, , Next question, , Rectum, The rectum is approximately 12 cm long. It is a capacitance organ. It has both intra and, extraperitoneal components. The transition between the sigmoid colon is marked by the, disappearance of the tenia coli.The extra peritoneal rectum is surrounded by mesorectal fat that also, contains lymph nodes. This mesorectal fatty layer is removed surgically during rectal cancer surgery, (Total Mesorectal Excision). The fascial layers that surround the rectum are important clinical, landmarks, anteriorly lies the fascia of Denonvilliers. Posteriorly lies Waldeyers fascia., Extra peritoneal rectum, , , , , Posterior upper third, Posterior and lateral middle third, Whole lower third
Page 2159 :
Relations, , Anteriorly (Males), , Rectovesical pouch, Bladder, Prostate, Seminal vesicles, , Anteriorly (Females), , Recto-uterine pouch (Douglas), Cervix, Vaginal wall, , Posteriorly, , Sacrum, Coccyx, Middle sacral artery, , Laterally, , Levator ani, Coccygeus, , Arterial supply, Superior rectal artery, Venous drainage, Superior rectal vein, Lymphatic drainage, , , , , Mesorectal lymph nodes (superior to dentate line), Internal iliac and then para-aortic nodes, Inguinal nodes (inferior to dentate line), Next question
Page 2160 :
Question 469 of 560, Which of these openings transmits the facial nerve into the temporal bone?, , Internal acoustic meatus, , Foramen lacerum, , Foramen spinosum, , Stylomastoid foramen, , Jugular foramen, , It enters the temporal bone through the internal acoustic meatus and exits through the stylomastoid, foramen., Please rate this question:, , Discuss and give feedback, , Next question, , Facial nerve, The facial nerve is the main nerve supplying the structures of the second embryonic branchial arch., It is predominantly an efferent nerve to the muscles of facial expression, digastric muscle and also to, many glandular structures. It contains a few afferent fibres which originate in the cells of its genicular, ganglion and are concerned with taste., Supply - 'face, ear, taste, tear', , , , , , Face: muscles of facial expression, Ear: nerve to stapedius, Taste: supplies anterior two-thirds of tongue, Tear: parasympathetic fibres to lacrimal glands, also salivary glands, , Path, Subarachnoid path
Page 2161 :
, , , Origin: motor- pons, sensory- nervus intermedius, Pass through the petrous temporal bone into the internal auditory meatus with the, vestibulocochlear nerve. Here they combine to become the facial nerve., , Facial canal path, , , , The canal passes superior to the vestibule of the inner ear, At the medial aspect of the middle ear, it becomes wider and contains the geniculate, ganglion., , - 3 branches:, 1. greater petrosal nerve, 2. nerve to stapedius, 3. chorda tympani, Stylomastoid foramen, , , , Passes through the stylomastoid foramen (tympanic cavity anterior and mastoid antrum, posteriorly), Posterior auricular nerve and branch to posterior belly of digastric and stylohyoid muscle, , Face, Enters parotid gland and divides into 5 branches:, , , , , , , Temporal branch, Zygomatic branch, Buccal branch, Marginal mandibular branch, Cervical branch, Next question
Page 2162 :
Question 470 of 560, A motor cyclist is involved in a road traffic accident causing severe right shoulder injuries. He is, found to have an adducted, medially rotated shoulder. The elbow is fully extended and the forearm, pronated. Which is the most likely diagnosis?, , C8, T1 root lesion, , C5, C6 root lesion, , Radial nerve lesion, , Ulnar nerve lesion, , Axillary nerve lesion, Erbs Palsy C5, C6 lesion, The features include:, , , , , , , Waiter's tip position, Loss of shoulder abduction (deltoid and supraspinatus paralysis), Loss of external rotation of the shoulder (paralysis of infraspinatus), Loss of elbow flexion (paralysis of biceps, brachialis and brachioradialis), Loss of forearm supination (paralysis of Biceps), , The motorcyclist has had an Erb's palsy (C5, C6 root lesion). This is commonly known to be, associated with birth injury when a baby has a shoulder dystocia., Please rate this question:, , Discuss and give feedback, , Next question, , Brachial plexus, Origin, , Sections of the, , Anterior rami of C5 to T1, , , Roots, trunks, divisions, cords, branches
Page 2163 :
plexus, , , , Mnemonic:Real Teenagers Drink Cold Beer, , Roots, , , , , Located in the posterior triangle, Pass between scalenus anterior and medius, , Trunks, , , , , , Located posterior to middle third of clavicle, Upper and middle trunks related superiorly to the subclavian artery, Lower trunk passes over 1st rib posterior to the subclavian artery, , Divisions, , Apex of axilla, , Cords, , Related to axillary artery, , Diagram illustrating the branches of the brachial plexus, , Image sourced from Wikipedia, , Cutaneous sensation of the upper limb
Page 2164 :
Image sourced from Wikipedia, , Next question
Page 2165 :
Question 471 of 560, A patient is due to undergo a right hemicolectomy for a carcinoma of the caecum. Which of the, following vessels will require high ligation to provide optimal oncological control?, , Middle colic artery, , Inferior mesenteric artery, , Superior mesenteric artery, , Ileo-colic artery, , None of the above, , The ileo - colic artery supplies the caecum and would require high ligation during a right, hemicolectomy. The middle colic artery should generally be preserved when resecting a caecal, lesion., This question is essentially asking you to name the vessel supplying the caecum. The SMA does not, directly supply the caecum, it is the ileocolic artery which does this., Please rate this question:, , Discuss and give feedback, , Next question, , Caecum, Location, , , , , Proximal right colon below the ileocaecal valve, Intraperitoneal, , Posterior relations, , , , , , , , Psoas, Iliacus, Femoral nerve, Genitofemoral nerve, Gonadal vessels, , Anterior relations, , Greater omentum
Page 2166 :
Arterial supply, , Ileocolic artery, , Lymphatic drainage, , Mesenteric nodes accompany the venous drainage, , , , The caecum is the most distensible part of the colon and in complete large bowel obstruction, with a competent ileocaecal valve the most likely site of eventual perforation., Next question
Page 2167 :
Question 472 of 560, A 40-year-old man presents with pain in his lower back and 'sciatica' for the past three days. He, describes bending down to pick up a washing machine when he felt 'something go'. He now has, severe pain radiating from his back down the right leg. On examination he describes paraesthesia, over the anterior aspect of the right knee and the medial aspect of his calf. Power is intact and the, right knee reflex is diminished. The femoral stretch test is positive on the right side. Which nerve or, nerve root is most likely to be affected?, , Common peroneal nerve, , Lateral cutaneous nerve of the thigh, , L5, , L3, , L1, , Please rate this question:, , Discuss and give feedback, , Next question, , Prolapsed disc, A prolapsed lumbar disc usually produces clear dermatomal leg pain associated with neurological, deficits., Features, , , , Leg pain usually worse than back, Pain often worse when sitting, , The table below demonstrates the expected features according to the level of compression:, , L3 nerve root compression, , Sensory loss over anterior thigh/knee, Weak quadriceps
Page 2168 :
Reduced knee reflex, Positive femoral stretch test, , L5 nerve root compression, , Sensory loss dorsum of foot, Weakness in foot and big toe dorsiflexion, Reflexes intact, Positive sciatic nerve stretch test, , S1 nerve root compression, , Sensory loss posterolateral aspect of leg and lateral aspect of foot, Weakness in plantar flexion of foot, Reduced ankle reflex, Positive sciatic nerve stretch test, , Management, , , , , Similar to that of other musculoskeletal lower back pain: analgesia, physiotherapy, exercises, Persistent symptoms, muscular weakness, bladder or bowel dysfunction are indications for, urgent MRI scanning to delineate the disease extent to allow surgical planning, Plain spinal x-rays have no useful role in establishing the extent of disk disease, Next question
Page 2169 :
Question 473 of 560, , A 72 year old man is undergoing a repair of an abdominal aortic aneurysm. The aorta is cross, clamped both proximally and distally. The proximal clamp is applied immediately inferior to the renal, arteries. Both common iliac arteries are clamped distally. A longitudinal aortotomy is performed., After evacuating the contents of the aneurysm sac a significant amount of ongoing bleeding is, encountered. This is most likely to originate from:, , The coeliac axis, , Testicular artery, , Splenic artery, , Superior mesenteric artery, , Lumbar arteries, , The lumbar arteries are posteriorly sited and are a common cause of back bleeding during aortic, surgery. The other vessels cited all exit the aorta in the regions that have been cross clamped., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal aortic branches, Branches, , Level, , Paired, , Type
Page 2171 :
Question 474 of 560, Which of the following statements relating to sartorius is untrue?, , It is supplied by the femoral nerve, , It forms the lateral boundary of the femoral triangle, , The middle third forms the roof of the adductor canal, , It is a flexor of the hip and knee, , It inserts into the medial femoral condyle, , It inserts into the medial aspect of the upper part of the tibia., Please rate this question:, , Discuss and give feedback, , Next question, , Sartorius, , , , Longest strap muscle in the body, Most superficial muscle in the anterior compartment of the thigh, , Origin, , Anterior superior iliac spine, , Insertion, , Medial surface of the of the body of the tibia (upper part). It inserts anterior to, gracilis and semitendinosus, , Nerve Supply, , Femoral nerve (L2,3), , Action, , , , , Flexor of the hip and knee, slight abducts the thigh and rotates it laterally, It assists with medial rotation of the tibia on the femur. For example it
Page 2172 :
would play a pivotal role in placing the right heel onto the left knee ( and, vice versa), , Important, relations, , The middle third of this muscle, and its strong underlying fascia forms the roof of, the adductor canal , in which lie the femoral vessels, the saphenous nerve and the, nerve to vastus medialis., Next question
Page 2173 :
Question 475 of 560, , A 63 year old man undergoes a radical cystectomy for carcinoma of the bladder. During the, procedure there is considerable venous bleeding. What is the primary site of venous drainage of the, urinary bladder?, , Vesicoprostatic venous plexus, , Internal iliac vein, , External iliac vein, , Gonadal vein, , Common iliac vein, , The urinary bladder has a rich venous plexus surrounding it, this drains subsequently into the, internal iliac vein. The vesicoprostatic plexus may be a site of considerable venous bleeding during, cystectomy., Please rate this question:, , Discuss and give feedback, , Next question, , Bladder, The empty bladder is contained within the pelvic cavity. It is usually a three sided pyramid. The apex, of the bladder points forwards towards the symphysis pubis and the base lies immediately anterior to, the rectum or vagina. Continuous with the apex is the median umbilical ligament, during, development this was the site of the uranchus., The inferior aspect of the bladder is retroperitoneal and the superior aspect covered by peritoneum., As the bladder distends it will tend to separate the peritoneum from the fascia of transversalis. For
Page 2174 :
this reason a bladder that is distended due to acute urinary retention may be approached with a, suprapubic catheter that avoids entry into the peritoneal cavity., The trigone is the least mobile part of the bladder and forms the site of the ureteric orifices and, internal urethral orifice. In the empty bladder the ureteric orifices are approximately 2-3cm apart, this, distance may increase to 5cm in the distended bladder., Arterial supply, The superior and inferior vesical arteries provide the main blood supply to the bladder. These are, branches of the internal iliac artery., Venous drainage, In males the bladder is drained by the vesicoprostatic venous plexus. In females the bladder is, drained by the vesicouterine venous plexus. In both sexes this venous plexus will ultimately drain to, the internal iliac veins., Lymphatic drainage, Lymphatic drainage is predominantly to the external iliac nodes, internal iliac and obturator nodes, also form sites of bladder lymphatic drainage., Innervation, Parasympathetic nerve fibres innervate the bladder from the pelvic splanchnic nerves. Sympathetic, nerve fibres are derived from L1 and L2 via the hypogastric nerve plexuses. The parasympathetic, nerve fibres will typically cause detrusor muscle contraction and result in voiding. The muscle of the, trigone is innervated by the sympathetic nervous system. The external urethral sphincter is under, conscious control. During bladder filling the rate of firing of nerve impulses to the detrusor muscle is, low and receptive relaxation occurs. At higher volumes and increased intra vesical pressures the, rate of neuronal firing will increase and eventually voiding will occur., Next question
Page 2175 :
Question 476 of 560, , A man sustains a laceration between the base of the little finger and wrist. Several weeks after the, injury there is loss of thumb adduction power. Which nerve is most likely to have been injured?, , Superficial ulnar nerve, , Deep ulnar nerve, , Median nerve, , Radial nerve, , Recurrent branch of median nerve, , Theme from 2009 Exam, Theme from April 2014 Exam, Please rate this question:, , Discuss and give feedback, , Next question, , Ulnar nerve injury at wrist, Branches of the ulnar nerve in the wrist and hand, At the wrist the ulnar nerve divides into superficial and deep branches. The superficial branch lies, deep to the palmaris brevis. It divides into two; to produce digital nerves, which innervate the skin of, the medial third of the palm and the palmar surface of one and a half fingers., The deep branch arises from the nerve on the flexor retinaculum lateral to the pisiform bone. It, passes posteriorly between the abductor and short flexor of the little finger supplying them, and, supplying and piercing the opponens digiti minimi near its origin from the flexor retinaculum, turns, laterally over the distal surface of the Hook of the Hamate bone. It eventually passes between the
Page 2176 :
two heads of adductor pollicis with the deep palmar arch and ends in the first dorsal interosseous, muscle. In the palm the deep branch also innervates the lumbricals and interosseous muscles., Next question
Page 2177 :
Question 477 of 560, A 60 year old female is undergoing a Whipples procedure for adenocarcinoma of the pancreas. As, the surgeons begin to mobilise the pancreatic head they identify a large vessel passing inferiorly, over the anterior aspect of the uncinate process. What is it likely to be?, , Superior mesenteric artery, , Coeliac axis, , Inferior mesenteric artery, , Aorta, , Left gastric artery, , Theme from January 2012 Exam, The superior mesenteric artery arises from the aorta and passes anterior to the lower part of the, pancreas. Invasion of this structure is a relative contra indication to resectional surgery., Please rate this question:, , Discuss and give feedback, , Next question, , Pancreas, The pancreas is a retroperitoneal organ and lies posterior to the stomach. It may be accessed, surgically by dividing the peritoneal reflection that connects the greater omentum to the transverse, colon. The pancreatic head sits in the curvature of the duodenum. Its tail lies close to the hilum of, the spleen, a site of potential injury during splenectomy., Relations, Posterior to the pancreas, , Pancreatic head, , Inferior vena cava, Common bile duct, Right and left renal veins, Superior mesenteric vein and artery
Page 2178 :
Pancreatic neck, , Superior mesenteric vein, portal vein, , Pancreatic body-, , Left renal vein, Crus of diaphragm, Psoas muscle, Adrenal gland, Kidney, Aorta, , Pancreatic tail, , Left kidney, , Anterior to the pancreas, , Pancreatic head, , 1st part of the duodenum, Pylorus, Gastroduodenal artery, SMA and SMV(uncinate process), , Pancreatic body, , Stomach, Duodenojejunal flexure, , Pancreatic tail, , Splenic hilum, , Superior to the pancreas, Coeliac trunk and its branches common hepatic artery and splenic artery, Grooves of the head of the pancreas, 2nd and 3rd part of the duodenum, Arterial supply, , , , Head: pancreaticoduodenal artery, Rest: splenic artery, , Venous drainage, , , , Head: superior mesenteric vein, Body and tail: splenic vein
Page 2179 :
Ampulla of Vater, , , , Merge of pancreatic duct and common bile duct, Is an important landmark, halfway along the second part of the duodenum, that marks the, anatomical transition from foregut to midgut (also the site of transition between regions, supplied by coeliac trunk and SMA)., , Image sourced from Wikipedia, , Next question
Page 2180 :
Question 478 of 560, A 23 year old man has a cannula inserted into his cephalic vein. Through which structure does the, cephalic vein pass?, , Interosseous membrane, , Triceps, , Pectoralis major, , Clavipectoral fascia, , Tendon of biceps, The cephalic vein is a favored vessel for arteriovenous fistula formation and should be preserved in, patients with end stage renal failure, The cephalic vein penetrates the calvipectoral fascia (but not the pectoralis major) prior to, terminating in the axillary vein., Please rate this question:, , Discuss and give feedback, , Next question, , Cephalic vein, Path, , , , , , Dorsal venous arch drains laterally into the cephalic vein, Crosses the anatomical snuffbox and travels laterally up the arm, At the antecubital fossa connected to the basilic vein by the median cubital vein, Pierces deep fascia of deltopectoral groove to join axillary vein, Next question
Page 2181 :
Question 479 of 560, An 18 year old man is undergoing an orchidectomy via a scrotal approach. The surgeons mobilise, the spermatic cord. From which of the following is the outermost layer of this structure derived?, , Internal oblique aponeurosis, , External oblique aponeurosis, , Transversalis fascia, , Rectus sheath, , Campers fascia, , The outermost covering of the spermatic cord is derived from the external oblique aponeurosis.This, layer is added as the cord passes through the superficial inguinal ring., Please rate this question:, , Discuss and give feedback, , Next question, , Scrotal and testicular anatomy, Spermatic cord, Formed by the vas deferens and is covered by the following structures:, , Layer, , Origin, , Internal spermatic fascia, , Transversalis fascia, , Cremasteric fascia, , From the fascial coverings of internal oblique, , External spermatic fascia, , External oblique aponeurosis, , Contents of the cord
Page 2182 :
Vas deferens, , Transmits sperm and accessory gland secretions, , Testicular artery, , Branch of abdominal aorta supplies testis and, epididymis, , Artery of vas deferens, , Arises from inferior vesical artery, , Cremasteric artery, , Arises from inferior epigastric artery, , Pampiniform plexus, , Venous plexus, drains into right or left testicular vein, , Sympathetic nerve fibres, , Lie on arteries, the parasympathetic fibres lie on the, vas, , Genital branch of the genitofemoral, nerve, , Supplies cremaster, , Lymphatic vessels, , Drain to lumbar and para-aortic nodes, , Scrotum, , , , , , Composed of skin and closely attached dartos fascia., Arterial supply from the anterior and posterior scrotal arteries, Lymphatic drainage to the inguinal lymph nodes, Parietal layer of the tunica vaginalis is the innermost layer, , Testes, , , , , , The testes are surrounded by the tunica vaginalis (closed peritoneal sac). The parietal layer, of the tunica vaginalis adjacent to the internal spermatic fascia., The testicular arteries arise from the aorta immediately inferiorly to the renal arteries., The pampiniform plexus drains into the testicular veins, the left drains into the left renal vein, and the right into the inferior vena cava., Lymphatic drainage is to the para-aortic nodes., Next question
Page 2183 :
Question 480 of 560, Which of the following is not a carpal bone?, , Trapezium, , Triquetrum, , Trapezoid, , Trapezius, , Lunate, Mnemonic for the Carpal Bones, Sally Likes To Play The Tiny Chrome Harmonica, She Looks Too Pretty Try To Catch Her, Scared Lovers Try Positions That They Can't Handle, Trapezius is a muscle of the back., , Please rate this question:, , Discuss and give feedback, , Next question, , Carpal bones, The wrist is comprised of 8 carpal bones, these are arranged in two rows of 4. It is convex from side, to side posteriorly and concave anteriorly., Diagrammatic image of carpal bones
Page 2186 :
Question 481 of 560, A 53 year old male presents with a carcinoma of the transverse colon. Which of the following, structures should be ligated close to their origin to maximise clearance of the tumour?, , Superior mesenteric artery, , Inferior mesenteric artery, , Middle colic artery, , Ileo-colic artery, , Superior rectal artery, , The middle colic artery supplies the transverse colon and requires high ligation during cancer, resections. It is a branch of the superior mesenteric artery., Please rate this question:, , Discuss and give feedback, , Next question, , Transverse colon, , , , , , The right colon undergoes a sharp turn at the level of the hepatic flexure to become the, transverse colon., At this point it also becomes intraperitoneal., It is connected to the inferior border of the pancreas by the transverse mesocolon., The greater omentum is attached to the superior aspect of the transverse colon from which it, can easily be separated. The mesentery contains the middle colic artery and vein. The, greater omentum remains attached to the transverse colon up to the splenic flexure. At this, point the colon undergoes another sharp turn., , Relations, Superior, , Liver and gall-bladder, the greater curvature of the stomach, and the lower end of the, spleen, , Inferior, , Small intestine
Page 2187 :
Anterior, , Greater omentum, , Posterior, , From right to left with the descending portion of the duodenum, the head of the pancreas,, convolutions of the jejunum and ileum, spleen, , Next question
Page 2188 :
Question 482 of 560, , Which of the following structures are not closely related to the adductor longus muscle?, , Long saphenous vein, , Tendon of iliacus, , The profunda branch of the femoral artery, , Pectineus muscle, , Femoral nerve, Femoral triangle:, Adductor longus medially, Inguinal ligament superiorly, Sartorius muscle laterally, , Adductor longus forms the medial border of the femoral triangle. It is closely related to the long, saphenous vein which overlies it and the profunda branch of the femoral artery. The femoral nerve is, related to it inferiorly. However, the tendon of iliacus inserts proximally and is not in contact with, adductor longus., Please rate this question:, , Discuss and give feedback, , Next question, , Adductor longus
Page 2189 :
Origin, , Anterior body of pubis, , Insertion, , Middle third of linea aspera, , Action, , Adducts and flexes the thigh, medially rotate the hip, , Innervation, , Anterior division of obturator nerve (L2, L3, L4), , The schematic image below demonstrates the relationship of the adductor muscles, , Image sourced from Wikipedia, , Next question
Page 2190 :
Question 483 of 560, , Which of the following structures does not lie posterior to the right kidney?, , Psoas major, , 12th rib, , Quadratus lumborum, , Medial arcuate ligament, , 10th rib, , Theme from April 2012 Exam, The 8th and10th ribs lie more superiorly. The 12th rib is a closer relation posteriorly., Quadratus lumborum runs between the posterior part of the iliac crest, iliolumbar ligament and the, transverse processes of the lower lumbar vertebrae to the medial part of the lower border of the last, rib and transverse process of the upper lumbar vertebrae. In these last two locations it is posterior to, the kidney., Please rate this question:, , Discuss and give feedback, , Next question, , Renal anatomy, Each kidney is about 11cm long, 5cm wide and 3cm thick. They are located in a deep gutter, alongside the projecting vertebral bodies, on the anterior surface of psoas major. In most cases the, left kidney lies approximately 1.5cm higher than the right. The upper pole of both kidneys, approximates with the 11th rib (beware pneumothorax during nephrectomy). On the left hand side, the hilum is located at the L1 vertebral level and the right kidney at level L1-2. The lower border of
Page 2191 :
the kidneys is usually alongside L3., The table below shows the anatomical relations of the kidneys:, Relations, , Relations, , Right Kidney, , Left Kidney, , Posterior, , Quadratus lumborum, diaphragm, psoas, major, transversus abdominis, , Quadratus lumborum, diaphragm, psoas, major, transversus abdominis, , Anterior, , Hepatic flexure of colon, , Stomach, Pancreatic tail, , Superior, , Liver, adrenal gland, , Spleen, adrenal gland, , Fascial covering, Each kidney and suprarenal gland is enclosed within a common layer of investing fascia, derived, from the transversalis fascia. It is divided into anterior and posterior layers (Gerotas fascia)., Renal structure, Kidneys are surrounded by an outer cortex and an inner medulla which usually contains between 6, and 10 pyramidal structures. The papilla marks the innermost apex of these. They terminate at the, renal pelvis, into the ureter., Lying in a hollow within the kidney is the renal sinus. This contains:, 1. Branches of the renal artery, 2. Tributaries of the renal vein, 3. Major and minor calyces's, 4. Fat, Structures at the renal hilum, The renal vein lies most anteriorly, then renal artery (it is an end artery) and the ureter lies most, posterior., Next question
Page 2192 :
Question 484 of 560, , A 56 year old man is undergoing a radical nephrectomy via a posterior approach. Which of the, following structures is most likely to be encountered during the operative approach?, , 8th rib, , 10th rib, , 6th rib, , 12th rib, , 9th rib, , The 11th and 12th ribs lie posterior to the kidneys and may be encountered during a posterior, approach. A pneumothorax is a recognised complication of this type of surgery., Please rate this question:, , Discuss and give feedback, , Next question, , Renal anatomy, Each kidney is about 11cm long, 5cm wide and 3cm thick. They are located in a deep gutter, alongside the projecting vertebral bodies, on the anterior surface of psoas major. In most cases the, left kidney lies approximately 1.5cm higher than the right. The upper pole of both kidneys, approximates with the 11th rib (beware pneumothorax during nephrectomy). On the left hand side, the hilum is located at the L1 vertebral level and the right kidney at level L1-2. The lower border of, the kidneys is usually alongside L3., The table below shows the anatomical relations of the kidneys:
Page 2193 :
Relations, , Relations, , Right Kidney, , Left Kidney, , Posterior, , Quadratus lumborum, diaphragm, psoas, major, transversus abdominis, , Quadratus lumborum, diaphragm, psoas, major, transversus abdominis, , Anterior, , Hepatic flexure of colon, , Stomach, Pancreatic tail, , Superior, , Liver, adrenal gland, , Spleen, adrenal gland, , Fascial covering, Each kidney and suprarenal gland is enclosed within a common layer of investing fascia, derived, from the transversalis fascia. It is divided into anterior and posterior layers (Gerotas fascia)., Renal structure, Kidneys are surrounded by an outer cortex and an inner medulla which usually contains between 6, and 10 pyramidal structures. The papilla marks the innermost apex of these. They terminate at the, renal pelvis, into the ureter., Lying in a hollow within the kidney is the renal sinus. This contains:, 1. Branches of the renal artery, 2. Tributaries of the renal vein, 3. Major and minor calyces's, 4. Fat, Structures at the renal hilum, The renal vein lies most anteriorly, then renal artery (it is an end artery) and the ureter lies most, posterior., Next question
Page 2194 :
Question 485 of 560, A 73 year old lady presents with a femoral hernia. Which of the following structures forms the lateral, wall of the femoral canal?, , Pubic tubercle, , Femoral vein, , Femoral artery, , Conjoint tendon, , Femoral nerve, , The canal exists to allow for the physiological expansion of the femoral vein, which lies lateral to it., Please rate this question:, , Discuss and give feedback, , Next question, , Femoral canal, The femoral canal lies at the medial aspect of the femoral sheath. The femoral sheath is a fascial, tunnel containing both the femoral artery laterally and femoral vein medially. The canal lies medial to, the vein., Borders of the femoral canal, , Laterally, , Femoral vein, , Medially, , Lacunar ligament, , Anteriorly, , Inguinal ligament, , Posteriorly, , Pectineal ligament
Page 2195 :
Image showing dissection of femoral canal, , Image sourced from Wikipedia, , Contents, , , , Lymphatic vessels, Cloquet's lymph node, , Physiological significance, Allows the femoral vein to expand to allow for increased venous return to the lower limbs., Pathological significance, As a potential space, it is the site of femoral hernias. The relatively tight neck places these at high, risk of strangulation., Next question
Page 2200 :
Question 488 of 560, , How many unpaired branches leave the abdominal aorta to supply the abdominal viscera?, , One, , Two, , Three, , Four, , Five, , There are three unpaired branches to the abdominal viscera. These include the coeliac axis, the, SMA and IMA. Branches to the adrenals, renal arteries and gonadal vessels are paired. The fourth, unpaired branch of the abdominal aorta, the median sacral artery, does not directly supply the, abdominal viscera., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal aortic branches, Branches, , Level, , Paired, , Type, , Inferior phrenic, , T12 (Upper border), , Yes, , Parietal
Page 2202 :
Question 489 of 560, A 34 year old man with a submandibular gland stone is undergoing excision of the submandibular, gland. The incision is sited transversely approximately 4cm below the mandible. After incising the, skin, platysma and deep fascia which of the following structures is most likely to be encountered., , Facial artery, , Facial vein, , Lingual nerve, , Hypoglossal nerve, , Glossopharyngeal nerve, , When approaching the submandibular gland the facial vein and submandibular lymph nodes are the, most superficially encountered structures. Each sub mandibular gland has a superficial and deep, part, separated by the mylohyoid muscle. The facial artery passes in a groove on the superficial, aspect of the gland. It then emerges onto the surface of the face by passing between the gland and, the mandible. The facial vein is encountered first in this surgical approach because the incision is, made 4cm below the mandible (to avoid injury to the marginal mandibular nerve)., Please rate this question:, , Discuss and give feedback, , Next question, , Submandibular gland, Relations of the submandibular gland, , Superficial, , Platysma, deep fascia and mandible, Submandibular lymph nodes, Facial vein (facial artery near mandible), Marginal mandibular nerve, Cervical branch of the facial nerve, , Deep, , Facial artery (inferior to the mandible), Mylohoid muscle
Page 2203 :
Sub mandibular duct, Hyoglossus muscle, Lingual nerve, Submandibular ganglion, Hypoglossal nerve, , Submandibular duct (Wharton's duct), , , , , Opens lateral to the lingual frenulum on the anterior floor of mouth., 5 cm length, Lingual nerve wraps around Wharton's duct. As the duct passes forwards it crosses medial, to the nerve to lie above it and then crosses back, lateral to it, to reach a position below the, nerve., , Innervation, , , , Sympathetic innervation- Derived from superior cervical ganglion, Parasympathetic innervation- Submandibular ganglion via lingual nerve, , Arterial supply, Branch of the facial artery. The facial artery passes through the gland to groove its deep surface. It, then emerges onto the face by passing between the gland and the mandible., Venous drainage, Anterior facial vein (lies deep to the Marginal Mandibular nerve), Lymphatic drainage, Deep cervical and jugular chains of nodes, Next question
Page 2204 :
Question 490 of 560, You are working as an anatomy demonstrator and the medical students decide to test your, knowledge on the Circle of Willis. Which of the following comments is false?, , Does not include the middle cerebral artery, , Asymmetry of the circle of willis is a risk factor for the development of intracranial, aneurysms, Majority of blood passing through the vessels mix together, , Includes the anterior communicating arteries, , The circle surrounds the stalk of the pituitary gland, , There is minimum mixing of blood passing through the vessels., Please rate this question:, , Discuss and give feedback, , Next question, , Circle of Willis, The two internal carotid arteries and two vertebral arteries form an anastomosis known as the Circle, of Willis on the inferior surface of the brain. Each half of the circle is formed by:, 1. Anterior communicating artery, 2. Anterior cerebral artery, 3. Internal carotid artery, 4. Posterior communicating artery, 5. Posterior cerebral arteries and the termination of the basilar artery, The circle and its branches supply; the corpus striatum, internal capsule, diencephalon and, midbrain.
Page 2205 :
Image sourced from Wikipedia, , Vertebral arteries, , , , , , Enter the cranial cavity via foramen magnum, Lie in the subarachnoid space, Ascend on anterior surface of medulla oblongata, Unite to form the basilar artery at the base of the pons, , Branches:, , , , , Posterior spinal artery, Anterior spinal artery, Posterior inferior cerebellar artery, , Basilar artery, Branches:
Page 2206 :
, , , , , , Anterior inferior cerebellar artery, Labyrinthine artery, Pontine arteries, Superior cerebellar artery, Posterior cerebral artery, , Internal carotid arteries, Branches:, , , , , , Posterior communicating artery, Anterior cerebral artery, Middle cerebral artery, Anterior choroid artery, Next question, , Question 491-493 of 560, Theme: Surgical nerve lesions, , A., B., C., D., E., F., G., H., I., , Recurrent laryngeal nerve, Accessory nerve, Hypoglossal nerve, Vagus nerve, Common peroneal nerve, Tibial nerve, Long saphenous nerve, Phrenic nerve, Thoracodorsal nerve, , Please choose which of the listed nerves is at greatest risk for the procedures given. Each option, may be used once, more than once or not at all., , 491., , A 64 year old man has a suspected lymphoma and lymph node biopsy from the, posterolateral aspect of the right neck is planned., You answered Recurrent laryngeal nerve, The correct answer is Accessory nerve, The accessory nerve has a superficial course and is easily injured. It lies under platysma, and may be divided during the early part of the procedure.
Page 2207 :
492., , A 43 year old woman is due to undergo an axillary node clearance following a positive, sentinel node biopsy., You answered Recurrent laryngeal nerve, The correct answer is Thoracodorsal nerve, The long thoracic nerve is also at risk. The thoracodorsal nerve traverses the level 2, axillary nodes to supply latissimus dorsi and may be divided or damaged with diathermy., , 493., , A 53 year old man is to undergo a thyroidectomy., Recurrent laryngeal nerve, Recurrent laryngeal nerve injury may complicate thyroid surgery in up to 2% of cases., , Please rate this question:, , Discuss and give feedback, , Next question, , Nerve lesions during surgery, A variety of different procedures carry the risk of iatrogenic nerve injury. These are important not, only from the patients perspective but also from a medicolegal standpoint., The following operations and their associated nerve lesions are listed here:, , , , , , , , , , , Posterior triangle lymph node biopsy and accessory nerve lesion., Lloyd Davies stirrups and common peroneal nerve., Thyroidectomy and laryngeal nerve., Anterior resection of rectum and hypogastric autonomic nerves., Axillary node clearance; long thoracic nerve, thoracodorsal nerve and intercostobrachial, nerve., Inguinal hernia surgery and ilioinguinal nerve., Varicose vein surgery- sural and saphenous nerves., Posterior approach to the hip and sciatic nerve., Carotid endarterectomy and hypoglossal nerve., , There are many more, with sound anatomical understanding of the commonly performed procedures, the incidence of nerve lesions can be minimised. They commonly occur when surgeons operate in, an unfamiliar tissue plane or by blind placement of haemostats (not recommended)., Next question
Page 2208 :
Question 494 of 560, , A 45 year old man presents with bilateral inguinal hernias. The surgical team decide to repair these, laparoscopically through an extraperitoneal approach. Through an infraumbilical incision the, surgeons displace the inferior aspect of the rectus abdominis muscle anteriorly and place a, prosthetic mesh into the area to repair the hernias. Which structure will lie posterior to the mesh?, , Peritoneum, , Internal oblique aponeurosis, , External oblique aponeurosis, , Posterior aspect of the rectus sheath, , Bucks fascia, , During a TEP repair of inguinal hernia the only structure to lie posterior to the mesh is peritoneum., The question is really only asking which structure lies posterior to the rectus abdominis muscle., Since this region is below the arcuate line the transversalis fascia and peritoneum lie posterior to it., Bucks fascia lies in the penis., Please rate this question:, , Discuss and give feedback, , Next question, , Rectus abdominis muscle, The rectus sheath is formed by the aponeuroses of the lateral abdominal wall muscles. The rectus, sheath has a composition that varies according to anatomical level., 1. Above the costal margin the anterior sheath is composed of external oblique aponeurosis, the
Page 2209 :
costal cartilages are posterior to it., 2. From the costal margin to the arcuate line, the anterior rectus sheath is composed of external, oblique aponeurosis and the anterior part of the internal oblique aponeurosis. The posterior part of, the internal oblique aponeurosis and transversus abdominis form the posterior rectus sheath., 3. Below the arcuate line the aponeuroses of all the abdominal muscles lie in anterior aspect of the, rectus sheath. Posteriorly lies the transversalis fascia and peritoneum., The arcuate line is the point at which the inferior epigastric vessels enter the rectus sheath., Next question
Page 2210 :
Question 495 of 560, A 20 year old man undergoes an open appendicectomy performed via a lanz incision. This surgeon, places the incision on a level of the anterior superior iliac spine in an attempt to improve cosmesis., During the procedure the appendix is found to be retrocaecal and the incision is extended laterally., Which of the following nerves is at greatest risk of injury?, , Genitofemoral, , Ilioinguinal, , Obturator, , Lateral femoral cutaneous, , Femoral, , Theme from April 2012 Exam, Please rate this question:, , Discuss and give feedback, , Next question, , Ilioinguinal nerve, Arises from the first lumbar ventral ramus with the iliohypogastric nerve. It passes inferolaterally, through the substance of psoas major and over the anterior surface of quadratus lumborum. It, pierces the internal oblique muscle and passes deep to the aponeurosis of the external oblique, muscle. It enters the inguinal canal and then passes through the superficial inguinal ring to reach the, skin., Branches, , , , To supply those muscles of the abdominal wall through which it passes., Skin and fascia over the pubic symphysis, superomedial part of the femoral triangle, surface, of the scrotum, root and dorsum of penis or labum majus in females., Next question
Page 2211 :
Question 496 of 560, The femoral nerve is transected by a rather careless surgeon during a botched femoro-popliteal, bypass operation. Which of the following actions will be impaired?, , Extension of the great toe, , Adduction of the thigh, , Flexion of the knee joint, , Extension of the knee joint, , Eversion of the foot, , The femoral nerve supplies the quadriceps muscle which is responsible for extension at the knee, joint., Please rate this question:, , Discuss and give feedback, , Next question, , Femoral nerve, Root values, , L2, 3, 4, , Innervates, , , , , , , Pectineus, Sartorius, Quadriceps femoris, Vastus lateralis/medialis/intermedius, , Branches, , , , , , Medial cutaneous nerve of thigh, Saphenous nerve, Intermediate cutaneous nerve of thigh
Page 2212 :
Path, Penetrates psoas major and exits the pelvis by passing under the inguinal ligament to enter the, femoral triangle, lateral to the femoral artery and vein., , Image sourced from Wikipedia, , Mnemonic for femoral nerve supply, (don't) M I S V Q Scan for PE, M edial cutaneous nerve of the thigh, I ntermediate cutaneous nerve of the thigh, S aphenous nerve, V astus, Q uadriceps femoris, S artorius, PE ectineus
Page 2213 :
Question 497 of 560, Which of the following is not a direct branch of the facial nerve?, , Greater petrosal nerve, , Nerve to stapedius, , Auriculotemporal, , Chorda tympani, , Buccal, , The auriculotemporal nerve is a direct branch of the mandibular nerve., Other branches of the mandibular nerve include:, Lingual, Inferior alveolar, Nerve to the mylohyoid, Mental, Please rate this question:, , Discuss and give feedback, , Next question, , Facial nerve, The facial nerve is the main nerve supplying the structures of the second embryonic branchial arch., It is predominantly an efferent nerve to the muscles of facial expression, digastric muscle and also to, many glandular structures. It contains a few afferent fibres which originate in the cells of its genicular, ganglion and are concerned with taste., Supply - 'face, ear, taste, tear', , , , , , Face: muscles of facial expression, Ear: nerve to stapedius, Taste: supplies anterior two-thirds of tongue, Tear: parasympathetic fibres to lacrimal glands, also salivary glands
Page 2214 :
Path, Subarachnoid path, , , , Origin: motor- pons, sensory- nervus intermedius, Pass through the petrous temporal bone into the internal auditory meatus with the, vestibulocochlear nerve. Here they combine to become the facial nerve., , Facial canal path, , , , The canal passes superior to the vestibule of the inner ear, At the medial aspect of the middle ear, it becomes wider and contains the geniculate, ganglion., , - 3 branches:, 1. greater petrosal nerve, 2. nerve to stapedius, 3. chorda tympani, Stylomastoid foramen, , , , Passes through the stylomastoid foramen (tympanic cavity anterior and mastoid antrum, posteriorly), Posterior auricular nerve and branch to posterior belly of digastric and stylohyoid muscle, , Face, Enters parotid gland and divides into 5 branches:, , , , , , , Temporal branch, Zygomatic branch, Buccal branch, Marginal mandibular branch, Cervical branch, Next question
Page 2215 :
Question 498 of 560, A 32 year old man is stabbed in the neck and the inferior trunk of his brachial plexus is injured., Which of the modalities listed below is least likely to be affected?, , Initiating abduction of the shoulder, , Abduction of the fingers, , Flexion of the little finger, , Sensation on the palmar aspect of the little finger, , Gripping a screwdriver, Inferior trunk of brachial plexus., , , , C8 and T1 roots, Contributes to ulnar nerve and part of median nerve, , Theme from September 2012 Exam, The inferior trunk of the brachial plexus is rarely injured. Nerve roots C8 and T1 are the main, contributors to this trunk. Therefore an injury to this site will most consistently affect the ulnar nerve., The inferior trunk also contributes to the median nerve by way of the medial cord and therefore some, impairment of grip is almost inevitable., Please rate this question:, , Discuss and give feedback, , Next question, , Brachial plexus, Origin, , Sections of the, plexus, , Anterior rami of C5 to T1, , , , Roots, trunks, divisions, cords, branches, Mnemonic:Real Teenagers Drink Cold Beer
Page 2216 :
Roots, , , , , Located in the posterior triangle, Pass between scalenus anterior and medius, , Trunks, , , , , , Located posterior to middle third of clavicle, Upper and middle trunks related superiorly to the subclavian artery, Lower trunk passes over 1st rib posterior to the subclavian artery, , Divisions, , Apex of axilla, , Cords, , Related to axillary artery, , Diagram illustrating the branches of the brachial plexus, , Image sourced from Wikipedia, , Cutaneous sensation of the upper limb
Page 2217 :
Image sourced from Wikipedia, , Next question
Page 2218 :
Question 499 of 560, During embryological development, which of the following represent the correct origin of the, pancreas?, , Ventral and dorsal endodermal outgrowths of the duodenum, , Ventral and dorsal outgrowths of mesenchymal tissue from the posterior abdominal wall, , Ventral and dorsal outgrowths of the vitellointestinal duct, , Ventral and dorsal biliary tract diverticulae, , Buds from the inferior aspect of the caudate lobe, , The pancreas develops from a ventral and dorsal endodermal outgrowth of the duodenum. The, ventral arises close to, or in common with the hepatic diverticulum, and the larger, dorsal outgrowth, arises slightly cranial to the ventral extending into the mesoduodenum and mesogastrium. When the, buds eventually fuse the duct of the ventral rudiment becomes the main pancreatic duct., Please rate this question:, , Discuss and give feedback, , Next question, , Pancreas, The pancreas is a retroperitoneal organ and lies posterior to the stomach. It may be accessed, surgically by dividing the peritoneal reflection that connects the greater omentum to the transverse, colon. The pancreatic head sits in the curvature of the duodenum. Its tail lies close to the hilum of, the spleen, a site of potential injury during splenectomy., Relations, Posterior to the pancreas, , Pancreatic head, , Inferior vena cava, Common bile duct, Right and left renal veins, Superior mesenteric vein and artery
Page 2219 :
Pancreatic neck, , Superior mesenteric vein, portal vein, , Pancreatic body-, , Left renal vein, Crus of diaphragm, Psoas muscle, Adrenal gland, Kidney, Aorta, , Pancreatic tail, , Left kidney, , Anterior to the pancreas, , Pancreatic head, , 1st part of the duodenum, Pylorus, Gastroduodenal artery, SMA and SMV(uncinate process), , Pancreatic body, , Stomach, Duodenojejunal flexure, , Pancreatic tail, , Splenic hilum, , Superior to the pancreas, Coeliac trunk and its branches common hepatic artery and splenic artery, Grooves of the head of the pancreas, 2nd and 3rd part of the duodenum, Arterial supply, , , , Head: pancreaticoduodenal artery, Rest: splenic artery, , Venous drainage, , , , Head: superior mesenteric vein, Body and tail: splenic vein
Page 2220 :
Ampulla of Vater, , , , Merge of pancreatic duct and common bile duct, Is an important landmark, halfway along the second part of the duodenum, that marks the, anatomical transition from foregut to midgut (also the site of transition between regions, supplied by coeliac trunk and SMA)., , Image sourced from Wikipedia, , Next question
Page 2221 :
Question 500 of 560, Which of the following is not a content of the anterior triangle of the neck?, , Ansa cervicalis, , Vagus nerve, , Anterior jugular vein, , Transverse cervical nerve, , Hypoglossal nerve, , The transverse cervical nerve lies within the posterior triangle. The anterior jugular vein is formed in, the submental region and descends in the superficial fascia near the median plane. It passes inferior, to enter the suprasternal space, it is linked to the contralateral anterior jugular vein by the jugular, venous arch., Please rate this question:, , Discuss and give feedback, , Next question, , Anterior triangle of the neck, Boundaries, , Anterior border of the Sternocleidomastoid, Lower border of mandible, Anterior midline, , Sub triangles (divided by Digastric above and Omohyoid), , , , , Muscular triangle: Neck strap muscles, Carotid triangle: Carotid sheath, Submandibular Triangle (digastric)
Page 2222 :
Contents of the anterior triangle, , Digastric triangle, , Submandibular gland, Submandibular nodes, Facial vessels, Hypoglossal nerve, , Muscular triangle, , Strap muscles, External jugular vein, , Carotid triangle, , Carotid sheath (Common carotid, vagus and internal jugular vein), Ansa cervicalis, , Nerve supply to digastric muscle, , , , Anterior: Mylohyoid nerve, Posterior: Facial nerve, , Image sourced from Wikipedia, , Next question
Page 2223 :
Question 501 of 560, A 23 year old man presents with delayed diagnosis of appendicitis. The appendix is retrocaecal and, has perforated causing a psoas abscess. Into which structure does the psoas major muscle insert?, , Greater trochanter of the femur, , Linea aspera of the femur, , Lesser trochanter of the femur, , Iliac crest, , None of the above, , Theme based on 2011 exam, The psoas major inserts into the lesser trochanter., Please rate this question:, , Discuss and give feedback, , Next question, , Psoas Muscle, Origin, The deep part originates from the transverse processes of the five lumbar vertebrae, the superficial, part originates from T12 and the first 4 lumbar vertebrae., Insertion, Lesser trochanter of the femur., Innervation, Anterior rami of L1 to L3., Action, Flexion and external rotation of the hip. Bilateral contraction can raise the trunk from the supine, position., Next question
Page 2224 :
Question 502 of 560, , A 63 year old man is due to undergo a splenectomy. Which splenic structure lies most posteriorly?, , Gastrosplenic ligament, , Splenic vein, , Splenic artery, , Splenic notch, , Lienorenal ligament, , Theme from 2011 Exam, The lienorenal ligament lies most posteriorly. The antero-lateral connection is via the phrenicocolic, ligament. Anteriorly the gastro splenic ligament. These structures condense around the vessels at, the splenic hilum., Please rate this question:, , Discuss and give feedback, , Next question, , Splenic anatomy, The spleen is the largest lymphoid organ in the body. It is an intraperitoneal organ, the peritoneal, attachments condense at the hilum where the vessels enter the spleen. Its blood supply is from the, splenic artery (derived from the coeliac axis) and the splenic vein (which is joined by the IMV and, unites with the SMV).
Page 2225 :
, , , , , Embryology: derived from mesenchymal tissue, Shape: clenched fist, Position: below 9th-12th ribs, Weight: 75-150g, , Relations, , , , , , , , , Superiorly- diaphragm, Anteriorly- gastric impression, Posteriorly- kidney, Inferiorly- colon, Hilum: tail of pancreas and splenic vessels, Forms apex of lesser sac (containing short gastric vessels), Next question
Page 2226 :
Question 503 of 560, , Which of these statements relating to the external carotid is false?, , It ends by bifurcating into the superficial temporal and ascending pharyngeal artery, , Its first branch is the superior thyroid artery, , The superior thyroid, lingual and facial arteries all arise from its anterior surface, , The ascending pharyngeal artery is a medial branch, , Initially it lies anteromedial to the internal carotid, , It terminates by dividing into the superficial temporal and maxillary branches. The external carotid, has eight branches, 3 from its anterior surface ; thyroid, lingual and facial. The pharyngeal artery is a, medial branch. The posterior auricular and occipital are posterior branches., Please rate this question:, , Discuss and give feedback, , Next question, , External carotid artery, The external carotid commences immediately lateral to the pharyngeal side wall. It ascends and lies, anterior to the internal carotid and posterior to the posterior belly of digastric and stylohyoid. More, inferiorly it is covered by sternocleidomastoid, passed by hypoglossal nerves, lingual and facial, veins., It then pierces the fascia of the parotid gland finally dividing into its terminal branches within the, gland itself., Surface marking of the carotid
Page 2227 :
This is an imaginary line drawn from the bifurcation of the common carotid passing behind the angle, of the jaw to a point immediately anterior to the tragus of the ear., Branches of the external carotid artery, It has six branches, three in front, two behind and one deep., , Three in front, , Superior thyroid, Lingual, Facial, , Two behind, , Occipital, Posterior auricular, , Deep, , Ascending pharyngeal, , It terminates by dividing into the superficial temporal and maxillary arteries in the parotid gland., , Image sourced from Wikipedia, , Next question
Page 2228 :
Question 504 of 560, Which of the following statements about the spleen is false?, , The hilum contains the splenic vessels., , The spleen is derived from endodermal tissue., , The white pulp has immune function., , The colon lies inferiorly., , Weighs 150g., 1,3,5,7,9,11 (odd numbers up to 11), The spleen is: 1 inch thick, 3 inches wide, 5 inches long, weighs 7oz (150-200g), lies between the, 9th and 11th ribs, Most of the gut is derived endodermally except for the spleen which is from mesenchymal tissue., Please rate this question:, , Discuss and give feedback, , Next question, , Spleen, The spleen is located in the left upper quadrant of the abdomen and its size can vary depending, upon the amount of blood it contains. The typical adult spleen is 12.5cm long and 7.5cm wide. The, usual weight of the adult spleen is 150g., The exact position of the spleen can vary with respiratory activity, posture and the state of, surrounding viscera. It usually lies obliquely with its long axis aligned to the 9th, 10th and 11th ribs. It, is separated from these ribs by both diaphragm and pleural cavity. The normal spleen is not, palpable., The shape of the spleen is influenced by the state of the colon and stomach. Gastric distension will, cause the spleen to resemble the shape of an orange segment. Colonic distension will cause it to, become more tetrahedral., The spleen is almost entirely covered by peritoneum, which adheres firmly to its capsule. Recesses, of the greater sac separate it from the stomach and kidney. It develops from the upper dorsal, mesogastrium, remaining connected to the posterior abdominal wall and stomach by two folds of
Page 2229 :
peritoneum; the lienorenal ligament and gastrosplenic ligament. The lienorenal ligament is derived, from peritoneum where the wall of the general peritoneum meets the omental bursa between the left, kidney and spleen; the splenic vessels lie in its layers. The gastrosplenic ligament also has two, layers, formed by the meeting of the walls of the greater sac and omental bursa between spleen and, stomach, the short gastric and left gastroepiploic branches of the splenic artery pass in its layers., Laterally, the spleen is in contact with the phrenicocolic ligament., Relations, Superiorly, , Diaphragm, , Anteriorly, , Gastric impression, , Posteriorly, , Kidney, , Inferiorly, , Colon, , Hilum, , Tail of pancreas and splenic vessels (splenic artery divides here, branches pass to the, white pulp transporting plasma), , Contents, White, pulp, , Immune function. Contains central trabecular artery. The germinal centres are supplied, by arterioles called penicilliary radicles., , Red pulp, , Filters abnormal red blood cells., , Function, , , , , , , , Filtration of abnormal blood cells and foreign bodies such as bacteria., Immunity: IgM. Production of properdin, and tuftsin which help target fungi and bacteria for, phagocytosis., Haematopoiesis: up to 5th month gestation or in haematological disorders., Pooling: storage of 40% platelets., Iron reutilisation, Storage monocytes, , Disorders of the spleen, Massive splenomegaly, , , , , , , Myelofibrosis, Chronic myeloid leukaemia, Visceral leishmaniasis (kala-azar), Malaria, Gaucher's syndrome
Page 2230 :
Other causes (as above plus), , , , , , , , , Portal hypertension e.g. secondary to cirrhosis, Lymphoproliferative disease e.g. CLL, Hodgkin's, Haemolytic anaemia, Infection: hepatitis, glandular fever, Infective endocarditis, Sickle-cell*, thalassaemia, Rheumatoid arthritis (Felty's syndrome), , *the majority of adult patients with sickle-cell will have an atrophied spleen due to repeated infarction, Next question
Page 2231 :
Question 505 of 560, As it exits the axilla the radial nerve lies on which of the following muscles?, , Supraspinatus, , Infraspinatus, , Teres major, , Deltoid, , Pectoralis major, , The radial nerve passes through the triangular space to leave the axilla. The superior border of this, is bounded by the teres major muscle to which the radial nerve is closely related., Please rate this question:, , Discuss and give feedback, , Next question, , Radial nerve, Continuation of posterior cord of the brachial plexus (root values C5 to T1), Path, , , , , , , , In the axilla: lies posterior to the axillary artery on subscapularis, latissimus dorsi and teres, major., Enters the arm between the brachial artery and the long head of triceps (medial to humerus)., Spirals around the posterior surface of the humerus in the groove for the radial nerve., At the distal third of the lateral border of the humerus it then pierces the intermuscular, septum and descends in front of the lateral epicondyle., At the lateral epicondyle it lies deeply between brachialis and brachioradialis where it then, divides into a superficial and deep terminal branch., Deep branch crosses the supinator to become the posterior interosseous nerve., , In the image below the relationships of the radial nerve can be appreciated
Page 2233 :
Anatomical, location, , Muscle affected, , Effect of paralysis, , Shoulder, , Long head of triceps, , Minor effects on shoulder stability in abduction, , Arm, , Triceps, , Loss of elbow extension, , Forearm, , Supinator, Brachioradialis, Extensor carpi radialis, longus and brevis, , Weakening of supination of prone hand and, elbow flexion in mid prone position, , The cutaneous sensation of the upper limb- illustrating the contribution of the radial nerve, , Image sourced from Wikipedia, , Next question
Page 2234 :
Question 506 of 560, Into which of the following veins does the middle thyroid vein drain?, , Vertebral, , External jugular, , Internal jugular, , Subclavian, , Anterior jugular, , It drains to the internal jugular vein. Which is one of the reasons why it bleeds so copiously if a, ligature slips., Please rate this question:, , Discuss and give feedback, , Next question, , Thyroid gland, , , , , , , , Right and left lobes connected by isthmus, Surrounded by sheath from pretracheal layer of deep fascia, Apex: Lamina of thyroid cartilage, Base: 4th-5th tracheal ring, Pyramidal lobe: from isthmus, May be attached to foramen caecum at the base of the tongue, , Relations, , Anteromedially, , Posterolaterally, , , , , , , Sternothyroid, Superior belly of omohyoid, Sternohyoid, Anterior aspect of sternocleidomastoid, , Carotid sheath
Page 2235 :
Medially, , , , , , , , , , Larynx, Trachea, Pharynx, Oesophagus, Cricothyroid muscle, External laryngeal nerve (near superior thyroid artery), Recurrent laryngeal nerve (near inferior thyroid artery), , Posterior, , , , , Parathyroid glands, Anastomosis of superior and inferior thyroid arteries, , Isthmus, , , , , Anteriorly: Sternothyroids, sternohyoids, anterior jugular veins, Posteriorly: 2nd, 3rd, 4th tracheal rings (attached via Ligament of, Berry), , Blood Supply, , Arterial, , , , , , Superior thyroid artery (1st branch of external carotid), Inferior thyroid artery (from thyrocervical trunk), Thyroidea ima (in 10% of population -from brachiocephalic artery or aorta), , Venous, , , , , Superior and middle thyroid veins - into the IJV, Inferior thyroid vein - into the brachiocephalic veins, Next question
Page 2238 :
Question 508 of 560, A 62 year old man presents with arm weakness. On examination he has a weakness of elbow, extension and loss of sensation on the dorsal aspect of the first digit. What is the site of the most, likely underlying defect?, , Axillary nerve, , Median nerve, , Ulnar nerve, , Radial nerve, , Musculocutaneous nerve, , Theme from April 2012 Exam, The long head of the triceps muscle may be innervated by the axillary nerve and therefore complete, loss of triceps muscles function may not be present even with proximally sited nerve lesions., Please rate this question:, , Discuss and give feedback, , Next question, , Radial nerve, Continuation of posterior cord of the brachial plexus (root values C5 to T1), Path, , , , , , , , In the axilla: lies posterior to the axillary artery on subscapularis, latissimus dorsi and teres, major., Enters the arm between the brachial artery and the long head of triceps (medial to humerus)., Spirals around the posterior surface of the humerus in the groove for the radial nerve., At the distal third of the lateral border of the humerus it then pierces the intermuscular, septum and descends in front of the lateral epicondyle., At the lateral epicondyle it lies deeply between brachialis and brachioradialis where it then, divides into a superficial and deep terminal branch., Deep branch crosses the supinator to become the posterior interosseous nerve.
Page 2240 :
Anatomical, location, , Muscle affected, , Effect of paralysis, , Shoulder, , Long head of triceps, , Minor effects on shoulder stability in abduction, , Arm, , Triceps, , Loss of elbow extension, , Forearm, , Supinator, Brachioradialis, Extensor carpi radialis, longus and brevis, , Weakening of supination of prone hand and, elbow flexion in mid prone position, , The cutaneous sensation of the upper limb- illustrating the contribution of the radial nerve, , Image sourced from Wikipedia, , Next question
Page 2241 :
Question 509 of 560, From which of the following structures does the long head of the triceps muscle arise?, , Coracoid process, , Acromion, , Infraglenoid tubercle, , Coraco-acromial ligament, , Coraco-humeral ligament, , The long head arises from the infraglenoid tubercle. The fleshy lateral and medial heads are, attached to the posterior aspect of the humerus between the insertion of the teres minor and the, olecranon fossa., Please rate this question:, , Discuss and give feedback, , Next question, , Triceps, Origin, , , , , , Insertion, , , , , Long head- infraglenoid tubercle of the scapula., Lateral head- dorsal surface of the humerus, lateral and proximal to the, groove of the radial nerve, Medial head- posterior surface of the humerus on the inferomedial side of, the radial groove and both of the intermuscular septae, Olecranon process of the ulna. Here the olecranon bursa is between the, triceps tendon and olecranon., Some fibres insert to the deep fascia of the forearm, posterior capsule of the, elbow (preventing the capsule from being trapped between olecranon and, olecranon fossa during extension)
Page 2242 :
Innervation, , Radial nerve, , Blood, supply, , Profunda brachii artery, , Action, , Elbow extension. The long head can adduct the humerus and and extend it from a, flexed position, , Relations, , The radial nerve and profunda brachii vessels lie between the lateral and medial, heads, Next question
Page 2243 :
Question 510 of 560, A 45 year old man is undergoing a left hemicolectomy. As the surgeons mobilise the left colon they, identify a tubular structure lying at the inferior aspect of psoas major. What is it most likely to be?, , Left ureter, , Left common iliac vein, , Left common iliac artery, , Left external iliac artery, , Left external iliac vein, , The left ureter lies posterior to the left colon. The sigmoid colon and upper rectum may be more, closely related to the iliac vessels. These are not typically found above L4., Please rate this question:, , Discuss and give feedback, , Next question, , Ureter, , , , , , , , , 25-35 cm long, Muscular tube lined by transitional epithelium, Surrounded by thick muscular coat. Becomes 3 muscular layers as it crosses the bony pelvis, Retroperitoneal structure overlying transverse processes L2-L5, Lies anterior to bifurcation of iliac vessels, Blood supply is segmental; renal artery, aortic branches, gonadal branches, common iliac, and internal iliac, Lies beneath the uterine artery, Next question
Page 2244 :
Question 511 of 560, Which muscle is not innervated by the trigeminal nerve?, , Medial pterygoid, , Mylohyoid, , Stylohyoid, , Masseter, , Temporalis, , Stylohyoid is innervated by the facial nerve., Please rate this question:, , Discuss and give feedback, , Next question, , Trigeminal nerve, The trigeminal nerve is the main sensory nerve of the head. In addition to its major sensory role, it, also innervates the muscles of mastication., Distribution of the trigeminal nerve, , Sensory, , , , , , , , Scalp, Face, Oral cavity (and teeth), Nose and sinuses, Dura mater, , Motor, , , , , , , Muscles of mastication, Mylohyoid, Anterior belly of digastric, Tensor tympani
Page 2245 :
Autonomic connections (ganglia), , , , Tensor palati, , , , , , , Ciliary, Sphenopalatine, Otic, Submandibular, , Path, , , , , Originates at the pons, Sensory root forms the large, crescentic trigeminal ganglion within Meckel's cave, and, contains the cell bodies of incoming sensory nerve fibres. Here the 3 branches exit., The motor root cell bodies are in the pons and the motor fibres are distributed via the, mandibular nerve. The motor root is not part of the trigeminal ganglion., , Branches of the trigeminal nerve, , Ophthalmic nerve, , Sensory only, , Maxillary nerve, , Sensory only, , Mandibular nerve, , Sensory and motor, , Sensory, , Ophthalmic, , Exits skull via the superior orbital fissure, Sensation of: scalp and forehead, the upper eyelid, the conjunctiva and cornea of, the eye, the nose (including the tip of the nose, except alae nasi), the nasal, mucosa, the frontal sinuses, and parts of the meninges (the dura and blood, vessels)., , Maxillary, nerve, , Exit skull via the foramen rotundum, Sensation: lower eyelid and cheek, the nares and upper lip, the upper teeth and, gums, the nasal mucosa, the palate and roof of the pharynx, the maxillary,, ethmoid and sphenoid sinuses, and parts of the meninges., , Mandibular, , Exit skull via the foramen ovale
Page 2246 :
nerve, , Sensation: lower lip, the lower teeth and gums, the chin and jaw (except the angle, of the jaw), parts of the external ear, and parts of the meninges., , Motor, Distributed via the mandibular nerve., The following muscles of mastication are innervated:, , , , , , Masseter, Temporalis, Medial pterygoid, Lateral pterygoid, , Other muscles innervated include:, , , , , , Tensor veli palatini, Mylohyoid, Anterior belly of digastric, Tensor tympani, Next question
Page 2247 :
Question 512 of 560, A 42 year old woman is due to undergo a left nephroureterectomy for a transitional cell carcinoma, involving the ureter. Which of the following structures is not related to the left ureter?, , Round ligament of the uterus, , Internal iliac artery, , Ovarian artery, , Peritoneum, , Sigmoid mesocolon, , The ureter is not related to the round ligament of the uterus, it is related to the broad ligament and is, within 1.5cm of the supravaginal part of the cervix., Please rate this question:, , Discuss and give feedback, , Next question, , Ureter, , , , , , , , , 25-35 cm long, Muscular tube lined by transitional epithelium, Surrounded by thick muscular coat. Becomes 3 muscular layers as it crosses the bony pelvis, Retroperitoneal structure overlying transverse processes L2-L5, Lies anterior to bifurcation of iliac vessels, Blood supply is segmental; renal artery, aortic branches, gonadal branches, common iliac, and internal iliac, Lies beneath the uterine artery, Next question
Page 2248 :
Question 513 of 560, Which of the following most commonly arises from the brachiocephalic artery?, , Vertebral artery, , Subscapular artery, , Thyroidea ima artery, , Left Subclavian artery, , None of the above, , Other occasional branches include the thymic and bronchial branch., Please rate this question:, , Discuss and give feedback, , Next question, , Brachiocephalic artery, The brachiocephalic artery is the largest branch of the aortic arch. From its aortic origin it ascends, superiorly, it initially lies anterior to the trachea and then on its right hand side. It branches into the, common carotid and right subclavian arteries at the level of the sternoclavicular joint., Path, Origin- apex of the midline of the aortic arch, Passes superiorly and posteriorly to the right, Divides into the right subclavian and right common carotid artery, Relations, , Anterior, , , , , , , , Sternohyoid, Sternothyroid, Thymic remnants, Left brachiocephalic vein, Right inferior thyroid veins
Page 2249 :
Posterior, , , , , Trachea, Right pleura, , Right lateral, , , , , Right brachiocephalic vein, Superior part of SVC, , Left lateral, , , , , , , Thymic remnants, Origin of left common carotid, Inferior thyroid veins, Trachea (higher level), , Branches, Normally none but may have the thyroidea ima artery, , Image sourced from Wikipedia, , Next question
Page 2250 :
Question 514 of 560, A 28 year old man is undergoing an appendicectomy. The external oblique aponeurosis is incised, and the underlying muscle split in the line of its fibres. At the medial edge of the wound is a tough, fibrous structure. Entry to this structure will most likely encounter which of the following?, , Internal oblique, , Rectus abdominis, , Transversus abdominis, , Linea alba, , Peritoneum, , This structure will be the rectus sheath and when entered the rectus abdominis muscle will be, encountered., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal incisions, Midline incision, , , , , , Paramedian, incision, , , , , , , Commonest approach to the abdomen, Structures divided: linea alba, transversalis fascia, extraperitoneal fat,, peritoneum (avoid falciform ligament above the umbilicus), Bladder can be accessed via an extraperitoneal approach through the, space of Retzius, Parallel to the midline (about 3-4cm), Structures divided/retracted: anterior rectus sheath, rectus (retracted),, posterior rectus sheath, transversalis fascia, extraperitoneal fat,, peritoneum, Incision is closed in layers
Page 2251 :
Battle, , , , , Similar location to paramedian but rectus displaced medially (and thus, denervated), Now seldom used, , Kocher's, , Incision under right subcostal margin e.g. Cholecystectomy (open), , Lanz, , Incision in right iliac fossa e.g. Appendicectomy, , Gridiron, , Oblique incision centered over McBurneys point- usually appendicectomy, (less cosmetically acceptable than Lanz, , Gable, , Rooftop incision, , Pfannenstiel's, , Transverse supra pubic, primarily used to access pelvic organs, , McEvedy's, , Groin incision e.g. Emergency repair strangulated femoral hernia, , Rutherford, Morrison, , Extraperitoneal approach to left or right lower quadrants. Gives excellent, access to iliac vessels and is the approach of choice for first time renal, transplantation., , Image sourced from Wikipedia, , Next question
Page 2252 :
Question 515 of 560, , A 35 year old man presents to the surgical clinic with a suspected direct inguinal hernia. These will, pass through Hesselbach's triangle. Which of the following forms the medial edge of this structure?, , External oblique aponeurosis, , Inferior epigastric artery, , Rectus abdominis muscle, , Inferior epigastric vein, , Obturator nerve, , Direct inguinal hernias pass through Hesselbachs triangle (although this is of minimal clinical, significance!). Its medial boundary is the rectus muscle., Please rate this question:, , Discuss and give feedback, , Next question, , Hesselbach's triangle, Direct hernias pass through Hesselbachs triangle., , Superolaterally, , Epigastric vessels
Page 2253 :
Medially, , Lateral edge of rectus muscle, , Inferiorly, , Inguinal ligament, , The boundaries of Hesselbachs triangle are commonly tested and illustrated below, , Image sourced from Wikipedia, , Next question
Page 2255 :
Superior, root, , Branch of C1 anterolateral to carotid sheath, , Inferior root, , Derived from C2 and C3 roots, passes posterolateral to the internal jugular vein (may lie, either deep or superficial to it), , Innervation, , Sternohyoid, Sternothyroid, Omohyoid, , The ansa cervicalis lies anterior to the carotid sheath. The nerve supply to the inferior strap muscles, enters at their inferior aspect. Therefore when dividing these muscles to expose a large goitre, the, muscles should be divided in their upper half.
Page 2256 :
Image sourced from Wikipedia
Page 2257 :
Question 517 of 560, A 58 year old lady presents with a mass in the upper outer quadrant of the right breast. Which of the, following statements relating to the breast is untrue?, , The internal mammary artery provides the majority of its arterial supply, , Nipple retraction may occur as a result of tumour infiltration of the clavipectoral fascia, , The internal mammary artery is a branch of the subclavian artery, , Up to 70% of lymphatic drainage is to the ipsilateral axillary nodes, , None of the above, , Both skin dimpling and nipple retraction are features of breast malignancy. However, they usually, occur as a result of tumour infiltration of the breast ligaments and ducts respectively. The, clavipectoral fascia encases the axillary contents. The lymphatic drainage of the breast is to the, axilla and also to the internal mammary chain. The breast is well vascularised and the internal, mammary artery is a branch of the subclavian artery., Please rate this question:, , Discuss and give feedback, , Next question, , Breast, The breast itself lies on a layer of pectoral fascia and the following muscles:, 1. Pectoralis major, 2. Serratus anterior, 3. External oblique, Image showing the topography of the female breast
Page 2258 :
Image sourced from Wikipedia, , Breast anatomy, , Nerve supply, , Arterial supply, , Venous drainage, Lymphatic, drainage, , Branches of intercostal nerves from T4-T6., , , , , , Internal mammary (thoracic) artery, External mammary artery (laterally), Anterior intercostal arteries, Thoraco-acromial artery, , Superficial venous plexus to subclavian, axillary and intercostal veins., , , , , 70% Axillary nodes, Internal mammary chain, Other lymphatic sites such as deep cervical and supraclavicular fossa, (later in disease), Next question
Page 2259 :
Question 518 of 560, Where are accessory spleens not found?, , Gonads, , Tail of pancreas, , Greater omentum, , Splenorenal ligament, , Ureter, , Accessory spleens, - 10% population, - 1 cm size, - locations: hilum of the spleen, tail of the pancreas, along the splenic vessels, in the gastrosplenic, ligament, the splenorenal ligament, the walls of the stomach or intestines, the greater omentum, the, mesentery, the gonads, Please rate this question:, , Discuss and give feedback, , Next question, , Spleen, The spleen is located in the left upper quadrant of the abdomen and its size can vary depending, upon the amount of blood it contains. The typical adult spleen is 12.5cm long and 7.5cm wide. The, usual weight of the adult spleen is 150g., The exact position of the spleen can vary with respiratory activity, posture and the state of, surrounding viscera. It usually lies obliquely with its long axis aligned to the 9th, 10th and 11th ribs. It, is separated from these ribs by both diaphragm and pleural cavity. The normal spleen is not, palpable., The shape of the spleen is influenced by the state of the colon and stomach. Gastric distension will, cause the spleen to resemble the shape of an orange segment. Colonic distension will cause it to, become more tetrahedral., The spleen is almost entirely covered by peritoneum, which adheres firmly to its capsule. Recesses
Page 2260 :
of the greater sac separate it from the stomach and kidney. It develops from the upper dorsal, mesogastrium, remaining connected to the posterior abdominal wall and stomach by two folds of, peritoneum; the lienorenal ligament and gastrosplenic ligament. The lienorenal ligament is derived, from peritoneum where the wall of the general peritoneum meets the omental bursa between the left, kidney and spleen; the splenic vessels lie in its layers. The gastrosplenic ligament also has two, layers, formed by the meeting of the walls of the greater sac and omental bursa between spleen and, stomach, the short gastric and left gastroepiploic branches of the splenic artery pass in its layers., Laterally, the spleen is in contact with the phrenicocolic ligament., Relations, Superiorly, , Diaphragm, , Anteriorly, , Gastric impression, , Posteriorly, , Kidney, , Inferiorly, , Colon, , Hilum, , Tail of pancreas and splenic vessels (splenic artery divides here, branches pass to the, white pulp transporting plasma), , Contents, White, pulp, , Immune function. Contains central trabecular artery. The germinal centres are supplied, by arterioles called penicilliary radicles., , Red pulp, , Filters abnormal red blood cells., , Function, , , , , , , , Filtration of abnormal blood cells and foreign bodies such as bacteria., Immunity: IgM. Production of properdin, and tuftsin which help target fungi and bacteria for, phagocytosis., Haematopoiesis: up to 5th month gestation or in haematological disorders., Pooling: storage of 40% platelets., Iron reutilisation, Storage monocytes, , Disorders of the spleen, Massive splenomegaly, , , , , , , Myelofibrosis, Chronic myeloid leukaemia, Visceral leishmaniasis (kala-azar), Malaria, Gaucher's syndrome
Page 2261 :
Other causes (as above plus), , , , , , , , , Portal hypertension e.g. secondary to cirrhosis, Lymphoproliferative disease e.g. CLL, Hodgkin's, Haemolytic anaemia, Infection: hepatitis, glandular fever, Infective endocarditis, Sickle-cell*, thalassaemia, Rheumatoid arthritis (Felty's syndrome), , *the majority of adult patients with sickle-cell will have an atrophied spleen due to repeated infarction, Next question
Page 2262 :
Question 519-521 of 560, Theme: Nerve injury, , A., B., C., D., E., F., G., , Median nerve, Ulnar nerve, Radial nerve, Anterior interosseous nerve, Posterior interosseous nerve, Axillary nerve, Musculocutaneous nerve, , Please select the nerve at risk of injury in each scenario. Each option may be used once, more than, once or not at all., , 519., , A 43 year old typist presents with pain at the dorsal aspect of the upper part of her, forearm. She also complains of weakness when extending her fingers. On examination, triceps and supinator are both functioning normally. There is weakness of most of the, extensor muscles. However, there is no sensory deficit., You answered Median nerve, The correct answer is Posterior interosseous nerve, The radial nerve may become entrapped in the "arcade of Frohse" which is a superficial, part of the supinator muscle which overlies the posterior interosseous nerve. This nerve is, entirely muscular and articular in its distribution. It passes postero-inferiorly and gives, branches to extensor carpi radialis brevis and supinator. It enters supinator and curves, around the lateral and posterior surfaces of the radius. On emerging from the supinator, the posterior interosseous nerve lies between the superficial extensor muscles and the, lowermost fibres of supinator. It then gives branches to the extensors., , 520., , A 28 year teacher reports difficulty with writing. There is no sensory loss. She is known, to have an aberrant Gantzer muscle., You answered Median nerve, The correct answer is Anterior interosseous nerve, Anterior interosseous lesions occur due to fracture, or rarely due to compression. The, Gantzer muscle is an aberrant accessory of the flexor pollicis longus and is a risk factor, for anterior interosseous nerve compression. Remember loss of pincer grip and normal, sensation indicates an interosseous nerve lesion.
Page 2263 :
521., , A 35 year tennis player attends reporting tingling down his arm. He says that his 'funny, bone' was hit very hard by a tennis ball. There is weakness of abduction and adduction of, his extended fingers., You answered Median nerve, The correct answer is Ulnar nerve, Theme from September 2012 exam, The ulnar nerve arises from the medial cord of the brachial plexus (C8, T1 and, contribution from C7). The nerve descends between the axillary artery and vein, posterior, to the cutaneous nerve of the forearm and then lies anterior to triceps on the medial side, of the brachial artery. In the distal half of the arm it passes through the medial, intermuscular septum, and continues between this structure and the medial head of triceps, to enter the forearm between the medial epicondyle of the humerus and the olecranon. It, may be injured at this site in this scenario., , Please rate this question:, , Discuss and give feedback, , Next question, , Brachial plexus, Origin, , Anterior rami of C5 to T1, , Sections of the, plexus, , , , , Roots, trunks, divisions, cords, branches, Mnemonic:Real Teenagers Drink Cold Beer, , Roots, , , , , Located in the posterior triangle, Pass between scalenus anterior and medius, , Trunks, , , , , , Located posterior to middle third of clavicle, Upper and middle trunks related superiorly to the subclavian artery, Lower trunk passes over 1st rib posterior to the subclavian artery, , Divisions, , Apex of axilla, , Cords, , Related to axillary artery
Page 2264 :
Diagram illustrating the branches of the brachial plexus, , Image sourced from Wikipedia, , Cutaneous sensation of the upper limb
Page 2265 :
Image sourced from Wikipedia, , Next question
Page 2266 :
Question 522 of 560, A 72 year old man is undergoing a left pneumonectomy for carcinoma of the bronchus. As the, surgeons approach the root of the lung, which structure will lie most anteriorly (in the anatomical, plane)?, , Vagus nerve, , Phrenic nerve, , Bronchus, , Pulmonary vein, , Pulmonary artery, , The phrenic nerve is the most anteriorly located structure in the lung root. The vagus nerve lies most, posteriorly., Please rate this question:, , Discuss and give feedback, , Next question, , Lung anatomy, The right lung is composed of 3 lobes divided by the oblique and transverse fissures. The left lung, has two lobes divided by the oblique fissure.The apex of both lungs is approximately 4cm superior to, the sterno-costal joint of the first rib. Immediately below this is a sulcus created by the subclavian, artery., Peripheral contact points of the lung, , , , , Base: diaphragm, Costal surface: corresponds to the cavity of the chest, Mediastinal surface: Contacts the mediastinal pleura. Has the cardiac impression. Above and, behind this concavity is a triangular depression named the hilum, where the structures which, form the root of the lung enter and leave the viscus. These structures are invested by pleura,, which, below the hilum and behind the pericardial impression, forms the pulmonary ligament
Page 2267 :
Right lung, Above the hilum is the azygos vein; Superior to this is the groove for the superior vena cava and, right innominate vein; behind this, and nearer the apex, is a furrow for the innominate artery. Behind, the hilum and the attachment of the pulmonary ligament is a vertical groove for the oesophagus; In, front and to the right of the lower part of the oesophageal groove is a deep concavity for the, extrapericardiac portion of the inferior vena cava., The root of the right lung lies behind the superior vena cava and the right atrium, and below the, azygos vein., The right main bronchus is shorter, wider and more vertical than the left main bronchus and, therefore the route taken by most foreign bodies., , Image sourced from Wikipedia, , Left lung, Above the hilum is the furrow produced by the aortic arch, and then superiorly the groove, accommodating the left subclavian artery; Behind the hilum and pulmonary ligament is a vertical, groove produced by the descending aorta, and in front of this, near the base of the lung, is the lower, part of the oesophagus., The root of the left lung passes under the aortic arch and in front of the descending aorta.
Page 2268 :
Image sourced from Wikipedia, , Inferior borders of both lungs, , , , , 6th rib in mid clavicular line, 8th rib in mid axillary line, 10th rib posteriorly, , The pleura runs two ribs lower than the corresponding lung level., Bronchopulmonary segments, , Segment number, , Right lung, , Left lung, , 1, , Apical, , Apical, , 2, , Posterior, , Posterior, , 3, , Anterior, , Anterior, , 4, , Lateral, , Superior lingular, , 5, , Medial, , Inferior lingular, , 6, , Superior (apical), , Superior (apical)
Page 2269 :
Segment number, , Right lung, , Left lung, , 7, , Medial basal, , Medial basal, , 8, , Anterior basal, , Anterior basal, , 9, , Lateral basal, , Lateral basal, , 10, , Posterior basal, , Posterior basal, Next question
Page 2270 :
Question 523 of 560, A 56 year old man is undergoing an anterior resection for a carcinoma of the rectum. Which of the, structures below is least likely to be encountered during the mobilisation of the anterior rectum?, , Denonvilliers' fascia, , Middle sacral artery, , Bladder, , Rectovesical pouch, , Seminal vesicles, , With the exception of the middle sacral artery all of the other structures lie anterior to the rectum., They may all be palpated during digital rectal examination., Please rate this question:, , Discuss and give feedback, , Next question, , Rectum, The rectum is approximately 12 cm long. It is a capacitance organ. It has both intra and, extraperitoneal components. The transition between the sigmoid colon is marked by the, disappearance of the tenia coli.The extra peritoneal rectum is surrounded by mesorectal fat that also, contains lymph nodes. This mesorectal fatty layer is removed surgically during rectal cancer surgery, (Total Mesorectal Excision). The fascial layers that surround the rectum are important clinical, landmarks, anteriorly lies the fascia of Denonvilliers. Posteriorly lies Waldeyers fascia., Extra peritoneal rectum, , , , , Posterior upper third, Posterior and lateral middle third, Whole lower third, , Relations
Page 2271 :
Anteriorly (Males), , Rectovesical pouch, Bladder, Prostate, Seminal vesicles, , Anteriorly (Females), , Recto-uterine pouch (Douglas), Cervix, Vaginal wall, , Posteriorly, , Sacrum, Coccyx, Middle sacral artery, , Laterally, , Levator ani, Coccygeus, , Arterial supply, Superior rectal artery, Venous drainage, Superior rectal vein, Lymphatic drainage, , , , , Mesorectal lymph nodes (superior to dentate line), Internal iliac and then para-aortic nodes, Inguinal nodes (inferior to dentate line), Next question
Page 2274 :
Foramen, , Location, , Contents, , Abducent nerve (VI), Superior ophthalmic vein, , *= In life the foramen lacerum is occluded by a cartilagenous plug. The ICA initially passes into the, carotid canal which ascends superomedially to enter the cranial cavity through the foramen lacerum., Base of skull anatomical overview, , Image sourced from Wikipedia, , Next question
Page 2275 :
Question 525 of 560, During an operation for varicose veins the surgeons are mobilising the long saphenous vein. Near its, point of entry to the femoral vein an artery is injured and bleeding is encountered. From where is the, bleeding most likely to originate?, , Femoral artery, , Profunda femoris artery, , Superficial circumflex iliac artery, , Superficial epigastric artery, , Deep external pudendal artery, , Theme from 2011 Exam, The deep external pudendal artery is a branch of the SFA and it runs medially under the long, saphenous vein near its point of union with the femoral vein. The superficial external pudendal artery, lies superior to the SFJ. Neither vessel is functionally important and if injured they are best ligated., Please rate this question:, , Discuss and give feedback, , Next question, , Femoral triangle anatomy, Boundaries, , Superiorly, , Inguinal ligament, , Laterally, , Sartorius, , Medially, , Adductor longus, , Floor, , Iliopsoas, adductor longus and pectineus
Page 2276 :
, , , , Roof, , Fascia lata and Superficial fascia, Superficial inguinal lymph nodes (palpable below the inguinal ligament), Long saphenous vein, , Image sourced from Wikipedia, , Contents, , , , , , , , , Femoral vein (medial to lateral), Femoral artery-pulse palpated at the mid inguinal point, Femoral nerve, Deep and superficial inguinal lymph nodes, Lateral cutaneous nerve, Great saphenous vein, Femoral branch of the genitofemoral nerve, Next question
Page 2277 :
Question 526 of 560, A 78 year old man is lifting a heavy object when a feels a pain in his forearm and is unable to, continue. He has a swelling over his upper forearm. An MRI scan shows a small cuff of tendon still, attached to the radial tuberosity consistent with a recent tear. Which of the following muscles has, been injured?, , Pronator teres, , Supinator, , Aconeus, , Brachioradialis, , Biceps brachii, , Biceps inserts into the radial tuberosity. Distal injuries of this muscle are rare but are reported and, are clinically more important than more proximal ruptures., Please rate this question:, , Discuss and give feedback, , Next question, , Radius, The radius is one of the two long forearm bones that extends from the lateral side of the elbow to the, thumb side of the wrist. It has two expanded ends, of which the distal end is the larger. Key points, relating to its topography and relations are outlined below;, Upper end, , , , , Articular cartilage- covers medial > lateral side, Articulates with radial notch of the ulna by the annular ligament, Muscle attachment- biceps brachii at the tuberosity, , Shaft, Muscle attachment
Page 2279 :
Question 527 of 560, , What is embryological origin of the pulmonary artery?, , First pharyngeal arch, , Second pharyngeal arch, , Fourth pharyngeal arch, , Fifth pharyngeal arch, , Sixth pharyngeal arch, , Theme from September 2011 Exam, Theme from September 2012 Exam, The proximal part of the sixth right pharyngeal arch gives origin to the right pulmonary artery. The, distal part gives origin to the left pulmonary artery and the ductus arteriosus., Please rate this question:, , Discuss and give feedback, , Next question, , Pharyngeal arches, These develop during the fourth week of embryonic growth from a series of mesodermal, outpouchings of the developing pharynx., They develop and fuse in the ventral midline. Pharyngeal pouches form on the endodermal side, between the arches., There are 6 pharyngeal arches, the fifth does not contribute any useful structures and often fuses, with the sixth arch.
Page 2281 :
Pharyngeal, arch, , Muscular, contributions, , Skeletal, contributions, , Endocrine, , Artery, , Nerve, , ductus, arteriosus, Next question
Page 2282 :
Question 528 of 560, A 53 year old lady presents with pain and discomfort in her hand. She works as a typist and notices, that the pain is worst when she is working. She also suffers symptoms at night. Her little finger is, less affected by the pain. Which of the nerves listed below is most likely to be affected?, , Radial, , Median, , Ulnar, , Anterior interosseous nerve, , Posterior interosseous nerve, Motor supply: LOAF, L ateral 2 lumbricals, O pponens pollicis, A bductor pollicisbrevis, F lexor pollicis brevis, Theme from September 2015 Exam, The most likely diagnosis here is carpal tunnel syndrome, the median nerve is compressed in the, wrist and symptoms usually affect the fingers and wrist either at night or when the hand is being, used (e.g. as a typist)., Please rate this question:, , Discuss and give feedback, , Next question, , Median nerve, The median nerve is formed by the union of a lateral and medial root respectively from the lateral, (C5,6,7) and medial (C8 and T1) cords of the brachial plexus; the medial root passes anterior to the, third part of the axillary artery. The nerve descends lateral to the brachial artery, crosses to its, medial side (usually passing anterior to the artery). It passes deep to the bicipital aponeurosis and, the median cubital vein at the elbow., It passes between the two heads of the pronator teres muscle, and runs on the deep surface of, flexor digitorum superficialis (within its fascial sheath)., Near the wrist it becomes superficial between the tendons of flexor digitorum superficialis and flexor
Page 2284 :
Damage at elbow, as above plus:, , , , , unable to pronate forearm, weak wrist flexion, ulnar deviation of wrist, , Anterior interosseous nerve (branch of median nerve), , , , leaves just below the elbow, results in loss of pronation of forearm and weakness of long flexors of thumb and index, finger, , Topography of the median nerve, , Image sourced from Wikipedia, , Next question
Page 2285 :
Question 529 of 560, Which of the following muscles lies medial to the long thoracic nerve?, , Serratus anterior, , Latissimus dorsi, , Pectoralis major, , Pectoralis minor, , None of the above, , Theme from 2009 Exam, Please rate this question:, , Discuss and give feedback, , Next question, , Long thoracic nerve, , , , , , Derived from ventral rami of C5, C6, and C7 (close to their emergence from intervertebral, foramina), It runs downward and passes either anterior or posterior to the middle scalene muscle, It reaches upper tip of serratus anterior muscle and descends on outer surface of this, muscle, giving branches into it, Winging of Scapula occurs in long thoracic nerve injury (most common) or from spinal, accessory nerve injury (which denervates the trapezius) or a dorsal scapular nerve injury, Next question
Page 2286 :
Question 530 of 560, The thebesian veins contribute to the venous drainage of the heart. Into which of the following, structures do they primarily drain?, , Great cardiac vein, , Atrium, , Superior vena cava, , Oblique vein, , Small cardiac vein, , The thebesian veins are numerous small veins running over the surface of the heart they drain into, the heart itself. Usually this is to the atrium directly., Please rate this question:, , Discuss and give feedback, , Next question, , Heart anatomy, The walls of each cardiac chamber comprise:, , , , , Epicardium, Myocardium, Endocardium, , Cardiac muscle is attached to the cardiac fibrous skeleton., Relations, The heart and roots of the great vessels within the pericardial sac are related anteriorly to the, sternum, medial ends of the 3rd to 5th ribs on the left and their associated costal cartilages. The, heart and pericardial sac are situated obliquely two thirds to the left and one third to the right of the, median plane., The pulmonary valve lies at the level of the left third costal cartilage.
Page 2287 :
The mitral valve lies at the level of the fourth costal cartilage., Coronary sinus, This lies in the posterior part of the coronary groove and receives blood from the cardiac veins. The, great cardiac vein lies at its left and the middle and small cardiac veins lie on its right. The smallest, cardiac vein (anterior cardiac vein) drains into the right atrium directly., Aortic sinus, Right coronary artery arises from the right aortic sinus, the left is derived from the left aortic sinus,, which lies posteriorly., Right and left ventricles, , Structure, , Left Ventricle, , A-V Valve, , Mitral (double leaflet), , Walls, , Twice as thick as right, , Trabeculae carnae, , Much thicker and more numerous, , Right coronary artery, The RCA supplies:, , , , , , , Right atrium, Diaphragmatic part of the left ventricle, Usually the posterior third of the interventricular septum, The sino atrial node (60% cases), The atrio ventricular node (80% cases), , Left coronary artery, The LCA supplies:, , , , , , , Left atrium, Most of left ventricle, Part of the right ventricle, Anterior two thirds of the inter ventricular septum, The sino atrial node (remaining 40% cases), , Innervation of the heart, Autonomic nerve fibres from the superficial and deep cardiac plexus. These lie anterior to the, bifurcation of the trachea, posterior to the ascending aorta and superior to the bifurcation of the
Page 2288 :
pulmonary trunk. The parasympathetic supply to the heart is from presynaptic fibres of the vagus, nerves., Valves of the heart, , Mitral valve, , Aortic valve, , Pulmonary valve, , Tricuspid valve, , 2 cusps, , 3 cusps, , 3 cusps, , 3 cusps, , First heart sound, , Second heart, sound, , Second heart, sound, , First heart sound, , 1 anterior cusp, , 2 anterior cusps, , 2 anterior cusps, , 2 anterior cusps, , Attached to chordae, tendinae, , No chordae, , No chordae, , Attached to chordae, tendinae, Next question
Page 2289 :
Question 531 of 560, , Which of the following is not contained within the deep posterior compartment of the lower leg?, , Tibialis posterior muscle, , Posterior tibial artery, , Tibial nerve, , Sural nerve, , Flexor hallucis longus, , The deep posterior compartment lies anterior to soleus. The sural nerve is superficially sited and, therefore not contained within it., Please rate this question:, , Discuss and give feedback, , Next question, , Lower limb- Muscular compartments, Anterior compartment, , Muscle, , Nerve, , Action, , Tibialis anterior, , Deep peroneal nerve, , Dorsiflexes ankle joint, inverts foot
Page 2292 :
Question 532 of 560, When performing minor surgery in the scalp, which of the following regions is considered a danger, area as regards spread of infection into the CNS?, , Aponeurosis epicranialis, , Skin, , Pericranium, , Connective tissue, , Loose areolar tissue, , This area is most dangerous as infections can spread easily. The emissary veins that drain this area, may allow sepsis to spread to the cranial cavity., Please rate this question:, , Discuss and give feedback, , Next question, , Head injury, Patients who suffer head injuries should be managed according to ATLS principles and extra cranial, injuries should be managed alongside cranial trauma. Inadequate cardiac output will compromise, CNS perfusion irrespective of the nature of the cranial injury., Types of traumatic brain injury, Bleeding into the space between the dura mater and the skull. Often results from, acceleration-deceleration trauma or a blow to the side of the head. The majority, of extradural haematomas occur in the temporal region where skull fractures, cause a rupture of the middle meningeal artery., Extradural, haematoma, , Features, , , , , Raised intracranial pressure, Some patients may exhibit a lucid interval
Page 2293 :
Bleeding into the outermost meningeal layer. Most commonly occur around the, frontal and parietal lobes. May be either acute or chronic., Subdural, haematoma, , Risk factors include old age and alcoholism., Slower onset of symptoms than a extradural haematoma., , Subarachnoid, haemorrhage, , Usually occurs spontaneously in the context of a ruptured cerebral aneurysm, but, may be seen in association with other injuries when a patient has sustained a, traumatic brain injury., , Pathophysiology, , , , , , , , Primary brain injury may be focal (contusion/ haematoma) or diffuse (diffuse axonal injury), Diffuse axonal injury occurs as a result of mechanical shearing following deceleration,, causing disruption and tearing of axons, Intra-cranial haematomas can be extradural, subdural or intracerebral, while contusions may, occur adjacent to (coup) or contralateral (contre-coup) to the side of impact, Secondary brain injury occurs when cerebral oedema, ischaemia, infection, tonsillar or, tentorial herniation exacerbates the original injury. The normal cerebral auto regulatory, processes are disrupted following trauma rendering the brain more susceptible to blood flow, changes and hypoxia, The Cushings reflex (hypertension and bradycardia) often occurs late and is usually a pre, terminal event, , Management, , , , , , , , , , , Where there is life threatening rising ICP such as in extra dural haematoma and whilst, theatre is prepared or transfer arranged use of IV mannitol/ frusemide may be required., Diffuse cerebral oedema may require decompressive craniotomy, Exploratory Burr Holes have little management in modern practice except where scanning, may be unavailable and to thus facilitate creation of formal craniotomy flap, Depressed skull fractures that are open require formal surgical reduction and debridement,, closed injuries may be managed non operatively if there is minimal displacement., ICP monitoring is appropriate in those who have GCS 3-8 and normal CT scan., ICP monitoring is mandatory in those who have GCS 3-8 and abnormal CT scan., Hyponatraemia is most likely to be due to syndrome of inappropriate ADH secretion., Minimum of cerebral perfusion pressure of 70mmHg in adults., Minimum cerebral perfusion pressure of between 40 and 70 mmHg in children., , Interpretation of pupillary findings in head injuries, , Pupil size, , Light response, , Interpretation
Page 2294 :
Pupil size, , Light response, , Interpretation, , Unilaterally dilated, , Sluggish or fixed, , 3rd nerve compression secondary to tentorial, herniation, , Bilaterally dilated, , Sluggish or fixed, , Unilaterally dilated or, equal, , Cross reactive (Marcus Gunn), , Bilaterally constricted, , May be difficult to, assess, , Unilaterally, constricted, , Preserved, , , , , Poor CNS perfusion, Bilateral 3rd nerve palsy, , Optic nerve injury, , , , , Opiates, Pontine lesions, Metabolic encephalopathy, , Sympathetic pathway disruption, Next question
Page 2295 :
Question 533 of 560, Which of the following structures are at risk of direct injury following a fracture dislocation of the, femoral condyles?, , Popliteal artery, , Sciatic nerve, , Plantaris muscle, , Tibial artery, , Tibial nerve, , The heads of gastrocnemius will contract to pull the fracture segment posteriorly. The popliteal artery, lies against the bone and may be damaged or compressed., Please rate this question:, , Discuss and give feedback, , Next question, , Popliteal fossa, Boundaries of the popliteal fossa, , Laterally, , Biceps femoris above, lateral head of gastrocnemius and plantaris below, , Medially, , Semimembranosus and semitendinosus above, medial head of gastrocnemius below, , Floor, , Popliteal surface of the femur, posterior ligament of knee joint and popliteus muscle, , Roof, , Superficial and deep fascia, , Image showing the popliteal fossa
Page 2296 :
© Image provided by the University of Sheffield, , Contents, , , , , , , , , Popliteal artery and vein, Small saphenous vein, Common peroneal nerve, Tibial nerve, Posterior cutaneous nerve of the thigh, Genicular branch of the obturator nerve, Lymph nodes, Next question
Page 2297 :
Question 534 of 560, A 25 year old man is being catheterised, prior to a surgical procedure. As the catheter enters the, prostatic urethra which of the following changes will occur?, , Resistance will increase significantly, , Resistance will increase slightly, , It will lie horizontally, , Resistance will decrease, , It will deviate laterally, , Theme from September 2011 Exam, The prostatic urethra is much wider than the membranous urethra and therefore resistance will, decrease. The prostatic urethra is inclined vertically., Please rate this question:, , Discuss and give feedback, , Next question, , Prostate gland, The prostate gland is approximately the shape and size of a walnut and is located inferior to the, bladder. It is separated from the rectum by Denonvilliers fascia and its blood supply is derived from, the internal iliac vessels (via inferior vesical artery). The internal sphincter lies at the apex of the, gland and may be damaged during prostatic surgery, affected individuals may complain of, retrograde ejaculation., Summary of prostate gland, , Arterial supply, , Inferior vesical artery (from internal iliac), , Venous drainage, , Prostatic venous plexus (to paravertebral veins)
Page 2298 :
Lymphatic, drainage, , Internal iliac nodes, , Innervation, , Inferior hypogastric plexus, , Dimensions, , , , , , Transverse diameter (4cm), AP diameter (2cm), Height (3cm), , Lobes, , , , , , , Posterior lobe: posterior to urethra, Median lobe: posterior to urethra, in between ejaculatory ducts, Lateral lobes x 2, Isthmus, , Zones, , , , Peripheral zone: subcapsular portion of posterior prostate. Most, prostate cancers are here, Central zone, Transition zone, Stroma, , , , , , Relations, , Anterior, , Pubic symphysis, Prostatic venous plexus, , Posterior, , Denonvilliers fascia, Rectum, Ejaculatory ducts, , Lateral, , Venous plexus (lies on prostate), Levator ani (immediately below the puboprostatic ligaments)
Page 2299 :
Image sourced from Wikipedia, , Next question
Page 2302 :
Branch, , Supplies, , Palmar cutaneous branch (Arises near the, middle of the forearm), , Skin on the medial part of the palm, , Dorsal cutaneous branch, , Dorsal surface of the medial part of the hand, , Superficial branch, , Cutaneous fibres to the anterior surfaces of the, medial one and one-half digits, , Deep branch, , Hypothenar muscles, All the interosseous muscles, Third and fourth lumbricals, Adductor pollicis, Medial head of the flexor pollicis brevis, , Effects of injury, , Damage at the wrist, , , , , , Wasting and paralysis of intrinsic hand muscles (claw hand), Wasting and paralysis of hypothenar muscles, Loss of sensation medial 1 and half fingers, , Damage at the elbow, , , , , Radial deviation of the wrist, Clawing less in 4th and 5th digits, Next question
Page 2303 :
Question 536 of 560, During a gangland gunfight a man is shot in the chest. The bullet passes through the posterior, mediastinum (from left to right). Which of the following structures is least likely to be injured, , Thoracic duct, , Oesophagus, , Vagus nerve, , Descending thoracic aorta, , Arch of the azygos vein, , The arch of the azygos vein lies in the middle mediastinum., Please rate this question:, , Discuss and give feedback, , Next question, , Mediastinum, Region between the pulmonary cavities., It is covered by the mediastinal pleura. It does not contain the lungs., It extends from the thoracic inlet superiorly to the diaphragm inferiorly., Mediastinal regions, , , , , , Region, , Superior mediastinum (between manubriosternal angle and T4/5), Middle mediastinum, Posterior mediastinum, Anterior mediastinum, , Contents
Page 2305 :
Question 537 of 560, The space between the vocal cords is referred to as which of the following?, , Piriform recess, , Rima vestibuli, , Vestibule, , Glottis, , Rima glottidis, , The rima glottidis is the narrowest part of the laryngeal cavity., Please rate this question:, , Discuss and give feedback, , Next question, , Larynx, The larynx lies in the anterior part of the neck at the levels of C3 to C6 vertebral bodies. The, laryngeal skeleton consists of a number of cartilagenous segments. Three of these are paired;, arytenoid, corniculate and cuneiform. Three are single; thyroid, cricoid and epiglottic. The cricoid, cartilage forms a complete ring (the only one to do so)., The laryngeal cavity extends from the laryngeal inlet to the level of the inferior border of the cricoid, cartilage., Divisions of the laryngeal cavity, , Laryngeal vestibule, , Superior to the vestibular folds, , Laryngeal ventricle, , Lies between vestibular folds and superior to the vocal cords, , Infraglottic cavity, , Extends from vocal cords to inferior border of the cricoid cartilage
Page 2306 :
The vocal folds (true vocal cords) control sound production. The apex of each fold projects medially, into the laryngeal cavity. Each vocal fold includes:, , , , Vocal ligament, Vocalis muscle (most medial part of thyroarytenoid muscle), , The glottis is composed of the vocal folds, processes and rima glottidis. The rima glottidis is the, narrowest potential site within the larynx, as the vocal cords may be completely opposed, forming a, complete barrier., Muscles of the larynx, , Muscle, , Origin, , Insertion, , Innervation, , Action, , Posterior, cricoarytenoid, , Posterior aspect, of lamina of, cricoid, , Muscular process, of arytenoid, , Recurrent, Laryngeal, , Abducts vocal fold, , Lateral, cricoarytenoid, , Arch of cricoid, , Muscular process, of arytenoid, , Recurrent, laryngeal, , Adducts vocal fold, , Thyroarytenoid, , Posterior aspect, of thyroid, cartilage, , Muscular process, of arytenoid, , Recurrent, laryngeal, , Relaxes vocal fold, , Transverse and, oblique, arytenoids, , Arytenoid, cartilage, , Contralateral, arytenoid, , Recurrent, laryngeal, , Closure of, intercartilagenous, part of the rima, glottidis, , Vocalis, , Depression, between lamina, of thyroid, cartilage, , Vocal ligament, and vocal process, of arytenoid, cartilage, , Recurrent, laryngeal, , Relaxes posterior, vocal ligament, tenses, anterior part, , Cricothyroid, , Anterolateral, part of cricoid, , Inferior margin, and horn of, thyroid cartilage, , External, laryngeal, , Tenses vocal fold
Page 2307 :
Blood supply, Arterial supply is via the laryngeal arteries, branches of the superior and inferior thyroid arteries. The, superior laryngeal artery is closely related to the internal laryngeal nerve. The inferior laryngeal, artery is related to the inferior laryngeal nerve. Venous drainage is via superior and inferior laryngeal, veins, the former draining into the superior thyroid vein and the latter draining into the middle thyroid, vein, or thyroid venous plexus., Lymphatic drainage, The vocal cords have no lymphatic drainage and this site acts as a lymphatic watershed., , Supraglottic part, , Upper deep cervical nodes, , Subglottic part, , Prelaryngeal and pretracheal nodes and inferior deep cervical nodes, , The aryepiglottic fold and vestibular folds have a dense plexus of lymphatics associated with them, and malignancies at these sites have a greater propensity for nodal metastasis., , Topography of the larynx, , Image sourced from Wikipedia, , Next question
Page 2308 :
Question 538 of 560, A 78 year old man develops a carcinoma of the scrotum. To which of the following lymph node, groups may the tumour initially metastasise?, , Para aortic, , Obturator, , Inguinal, , Meso rectal, , None of the above, , The scrotum is drained by the inguinal nodes., Please rate this question:, , Discuss and give feedback, , Next question, , Scrotal and testicular anatomy, Spermatic cord, Formed by the vas deferens and is covered by the following structures:, , Layer, , Origin, , Internal spermatic fascia, , Transversalis fascia, , Cremasteric fascia, , From the fascial coverings of internal oblique, , External spermatic fascia, , External oblique aponeurosis, , Contents of the cord
Page 2309 :
Vas deferens, , Transmits sperm and accessory gland secretions, , Testicular artery, , Branch of abdominal aorta supplies testis and, epididymis, , Artery of vas deferens, , Arises from inferior vesical artery, , Cremasteric artery, , Arises from inferior epigastric artery, , Pampiniform plexus, , Venous plexus, drains into right or left testicular vein, , Sympathetic nerve fibres, , Lie on arteries, the parasympathetic fibres lie on the, vas, , Genital branch of the genitofemoral, nerve, , Supplies cremaster, , Lymphatic vessels, , Drain to lumbar and para-aortic nodes, , Scrotum, , , , , , Composed of skin and closely attached dartos fascia., Arterial supply from the anterior and posterior scrotal arteries, Lymphatic drainage to the inguinal lymph nodes, Parietal layer of the tunica vaginalis is the innermost layer, , Testes, , , , , , The testes are surrounded by the tunica vaginalis (closed peritoneal sac). The parietal layer, of the tunica vaginalis adjacent to the internal spermatic fascia., The testicular arteries arise from the aorta immediately inferiorly to the renal arteries., The pampiniform plexus drains into the testicular veins, the left drains into the left renal vein, and the right into the inferior vena cava., Lymphatic drainage is to the para-aortic nodes., Next question
Page 2310 :
Question 539 of 560, A 63 year old man is undergoing an upper GI endoscopy for dysphagia. At 33 cm (from the incisors), a malignant looking stricture is encountered. The endoscopist attempts a balloon, dilatation.Unfortunately the tumour splits through the oesophageal wall. Into which region will the, oesophageal contents now drain?, , Superior mediastinum, , Posterior mediastinum, , Middle mediastinum, , Anterior mediastinum, , Peritoneal cavity, , At this position the oesophagus is still likely to be intrathoracic and located in the posterior, mediastinum., Please rate this question:, , Discuss and give feedback, , Next question, , Mediastinum, Region between the pulmonary cavities., It is covered by the mediastinal pleura. It does not contain the lungs., It extends from the thoracic inlet superiorly to the diaphragm inferiorly., Mediastinal regions, , , , , , Superior mediastinum (between manubriosternal angle and T4/5), Middle mediastinum, Posterior mediastinum, Anterior mediastinum
Page 2312 :
Question 540 of 560, During a tricuspid valve repair the right atrium is opened, following establishment of cardiopulmonary, bypass. Which of the following structures do not lie within the right atrium?, , Crista terminalis, , Tricuspid valve, , Fossa ovalis, , Trabeculae carnae, , Musculi pectinati, Structures within the right atrium:, , , , , , Musculi pectinati, Crista terminalis, Opening of the coronary sinus, Fossa ovalis, , The trabeculae carnae are located in the right ventricle., Please rate this question:, , Discuss and give feedback, , Next question, , Heart anatomy, The walls of each cardiac chamber comprise:, , , , , Epicardium, Myocardium, Endocardium, , Cardiac muscle is attached to the cardiac fibrous skeleton.
Page 2313 :
Relations, The heart and roots of the great vessels within the pericardial sac are related anteriorly to the, sternum, medial ends of the 3rd to 5th ribs on the left and their associated costal cartilages. The, heart and pericardial sac are situated obliquely two thirds to the left and one third to the right of the, median plane., The pulmonary valve lies at the level of the left third costal cartilage., The mitral valve lies at the level of the fourth costal cartilage., Coronary sinus, This lies in the posterior part of the coronary groove and receives blood from the cardiac veins. The, great cardiac vein lies at its left and the middle and small cardiac veins lie on its right. The smallest, cardiac vein (anterior cardiac vein) drains into the right atrium directly., Aortic sinus, Right coronary artery arises from the right aortic sinus, the left is derived from the left aortic sinus,, which lies posteriorly., Right and left ventricles, , Structure, , Left Ventricle, , A-V Valve, , Mitral (double leaflet), , Walls, , Twice as thick as right, , Trabeculae carnae, , Much thicker and more numerous, , Right coronary artery, The RCA supplies:, , , , , , , Right atrium, Diaphragmatic part of the left ventricle, Usually the posterior third of the interventricular septum, The sino atrial node (60% cases), The atrio ventricular node (80% cases), , Left coronary artery, The LCA supplies:, , , , , Left atrium, Most of left ventricle, Part of the right ventricle
Page 2314 :
, , , Anterior two thirds of the inter ventricular septum, The sino atrial node (remaining 40% cases), , Innervation of the heart, Autonomic nerve fibres from the superficial and deep cardiac plexus. These lie anterior to the, bifurcation of the trachea, posterior to the ascending aorta and superior to the bifurcation of the, pulmonary trunk. The parasympathetic supply to the heart is from presynaptic fibres of the vagus, nerves., Valves of the heart, , Mitral valve, , Aortic valve, , Pulmonary valve, , Tricuspid valve, , 2 cusps, , 3 cusps, , 3 cusps, , 3 cusps, , First heart sound, , Second heart, sound, , Second heart, sound, , First heart sound, , 1 anterior cusp, , 2 anterior cusps, , 2 anterior cusps, , 2 anterior cusps, , Attached to chordae, tendinae, , No chordae, , No chordae, , Attached to chordae, tendinae, Next question
Page 2315 :
Question 541 of 560, Which of the following is a recognised tributary of the retromandibular vein?, , Internal jugular vein, , External jugular vein, , Anterior temporal diploic vein, , Maxillary vein, , Inferior opthalmic vein, , The retromandibular vein is formed from the union of the maxillary and superficial temporal veins., Please rate this question:, , Discuss and give feedback, , Next question, , Retromandibular vein, , , , , Formed by a union of the maxillary vein and superficial temporal vein, It descends through the parotid gland and bifurcates within it, The anterior division passes forwards to join the facial vein, the posterior division is one of, the tributaries of the external jugular vein, Next question
Page 2316 :
Question 542 of 560, , An 22 year old soldier is shot in the abdomen and amongst his various injuries is a major disruption, to the abdominal aorta. There is torrential haemorrhage and the surgeons decide to control the aorta, by placement of a vascular clamp immediately inferior to the diaphragm. Which of the following, vessels may be injured in this maneouvre?, , Inferior phrenic arteries, , Superior phrenic arteries, , Splenic artery, , Renal arteries, , Superior mesenteric artery, , As the first branches of the abdominal aorta the inferior phrenic arteries are at greatest risk. The, superior phrenic arteries lie in the thorax. The potential space at the level of the diaphragmatic hiatus, is a potentially useful site for aortic occlusion. However, leaving the clamp applied for more than, about 10 -15 minutes usually leads to poor outcomes., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal aorta, Abdominal aortic topography
Page 2318 :
Image sourced from Wikipedia, , Next question
Page 2319 :
Question 543 of 560, Which of the following statements relating to the gallbladder is untrue?, , The fundus is usually intra peritoneal, , Arterial supply is from the cystic artery, , The cystic artery is usually located in Calots triangle, , Calots triangle may rarely contain an aberrant hepatic artery, , Cholecystokinin causes relaxation of the gallbladder, , CCK causes gallbladder contraction., Please rate this question:, , Discuss and give feedback, , Next question, , Gallbladder, , , , Fibromuscular sac with capacity of 50ml, Columnar epithelium, , Relations of the gallbladder, , Anterior, , Posterior, , Liver, , , , , Covered by peritoneum, Transverse colon, 1st part of the duodenum, , Laterally, , Right lobe of liver, , Medially, , Quadrate lobe of liver
Page 2320 :
Arterial supply, Cystic artery (branch of Right hepatic artery), Venous drainage, Directly to the liver, Nerve supply, Sympathetic- mid thoracic spinal cord, Parasympathetic- anterior vagal trunk, Common bile duct, , Origin, , Confluence of cystic and common hepatic ducts, , Relations at, origin, , , , , Medially - Hepatic artery, Posteriorly- Portal vein, , Relations distally, , , , , , Duodenum - anteriorly, Pancreas - medially and laterally, Right renal vein - posteriorly, , Arterial supply, , Branches of hepatic artery and retroduodenal branches of gastroduodenal, artery, , Hepatobiliary triangle, , Medially, , Common hepatic duct, , Inferiorly, , Cystic duct, , Superiorly, , Inferior edge of liver, , Contents, , Cystic artery, , Relations of the gallbladder
Page 2321 :
© Image provided by the University of Sheffield, , Next question
Page 2322 :
Question 544 of 560, , Which of the following nerves is the primary source of innervation to the anterior scrotal skin?, , Iliohypogastric nerve, , Pudendal nerve, , Ilioinguinal nerve, , Femoral branch of the genitofemoral nerve, , Obturator nerve, , Theme from April 2012 Exam, The pudendal nerve may innervate the posterior skin of the scrotum. The anterior innervation of the, scrotum is primarily provided by the ilioinguinal nerve. The genital branch of the genitofemoral nerve, provides a smaller contribution., Please rate this question:, , Discuss and give feedback, , Next question, , Scrotal sensation, The scrotum is innervated by the ilioinguinal nerve and the pudendal nerve. The ilioinguinal nerve, arises from L1 and pierces the internal oblique muscle. It eventually passes through the superficial, inguinal ring to innervate the anterior skin of the scrotum., The pudendal nerve is the principal nerve of the perineum. It arises in the pelvis from 3 nerve roots., It passes through both greater and lesser sciatic foramina to enter the perineal region. The perineal, branches pass anteromedially and divide into posterior scrotal branches. The posterior scrotal
Page 2323 :
branches pass superficially to supply the skin and fascia of the perineum. It cross communicates, with the inferior rectal nerve., Next question
Page 2324 :
Question 545 of 560, The transversalis fascia contributes to which of the following?, , Pectineal ligament, , Deep inguinal ring, , Cremaster muscle and fascia, , Inguinal ligament, , External spermatic fascia, The internal spermatic fascia (derived from transversalis fascia) invests:, Ducuts deferens, Testicular vessels, The principal outpouching of the transversalis fascia is the internal spermatic fascia. The mouth of, the outpouching is the deep inguinal ring., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal wall, The 2 main muscles of the abdominal wall are the rectus abdominis (anterior) and the quadratus, lumborum (posterior)., The remaining abdominal wall consists of 3 muscular layers. Each muscle passes from the lateral, aspect of the quadratus lumborum posteriorly to the lateral margin of the rectus sheath anteriorly., Each layer is muscular posterolaterally and aponeurotic anteriorly.
Page 2325 :
Image sourced from Wikipedia, , Muscles of abdominal wall, , External, oblique, , , , , , , , , Internal, oblique, , , , , , , Transversus, abdominis, , , , , , , , , , , Lies most superficially, Originates from 5th to 12th ribs, Inserts into the anterior half of the outer aspect of the iliac crest, linea, alba and pubic tubercle, More medially and superiorly to the arcuate line, the aponeurotic layer, overlaps the rectus abdominis muscle, The lower border forms the inguinal ligament, The triangular expansion of the medial end of the inguinal ligament is, the lacunar ligament., Arises from the thoracolumbar fascia, the anterior 2/3 of the iliac crest, and the lateral 2/3 of the inguinal ligament, The muscle sweeps upwards to insert into the cartilages of the lower 3, ribs, The lower fibres form an aponeurosis that runs from the tenth costal, cartilage to the body of the pubis, At its lowermost aspect it joins the fibres of the aponeurosis of, transversus abdominis to form the conjoint tendon., Innermost muscle, Arises from the inner aspect of the costal cartilages of the lower 6 ribs ,, from the anterior 2/3 of the iliac crest and lateral 1/3 of the inguinal, ligament, Its fibres run horizontally around the abdominal wall ending in an, aponeurosis. The upper part runs posterior to the rectus abdominis., Lower down the fibres run anteriorly only., The rectus abdominis lies medially; running from the pubic crest and, symphysis to insert into the xiphoid process and 5th, 6th and 7th costal, cartilages. The muscles lies in a aponeurosis as described above., Nerve supply: anterior primary rami of T7-12, , Surgical notes, During abdominal surgery it is usually necessary to divide either the muscles or their aponeuroses.
Page 2326 :
During a midline laparotomy it is desirable to divide the aponeurosis. This will leave the rectus, sheath intact above the arcuate line and the muscles intact below it. Straying off the midline will, often lead to damage to the rectus muscles, particularly below the arcuate line where they may often, be in close proximity to each other., Next question
Page 2327 :
Question 546 of 560, A 63 year old man is undergoing a right pneumonectomy for carcinoma of the bronchus. As the, surgeons approach the root of the lung, which structure will lie most posteriorly (in the anatomical, plane)?, , Phrenic nerve, , Main bronchus, , Vagus nerve, , Pulmonary vein, , Pulmonary artery, , The vagus nerve is the most posteriorly located structure at the lung root. The phrenic nerve lies, most anteriorly., Please rate this question:, , Discuss and give feedback, , Next question, , Lung anatomy, The right lung is composed of 3 lobes divided by the oblique and transverse fissures. The left lung, has two lobes divided by the oblique fissure.The apex of both lungs is approximately 4cm superior to, the sterno-costal joint of the first rib. Immediately below this is a sulcus created by the subclavian, artery., Peripheral contact points of the lung, , , , , Base: diaphragm, Costal surface: corresponds to the cavity of the chest, Mediastinal surface: Contacts the mediastinal pleura. Has the cardiac impression. Above and, behind this concavity is a triangular depression named the hilum, where the structures which, form the root of the lung enter and leave the viscus. These structures are invested by pleura,, which, below the hilum and behind the pericardial impression, forms the pulmonary ligament
Page 2328 :
Right lung, Above the hilum is the azygos vein; Superior to this is the groove for the superior vena cava and, right innominate vein; behind this, and nearer the apex, is a furrow for the innominate artery. Behind, the hilum and the attachment of the pulmonary ligament is a vertical groove for the oesophagus; In, front and to the right of the lower part of the oesophageal groove is a deep concavity for the, extrapericardiac portion of the inferior vena cava., The root of the right lung lies behind the superior vena cava and the right atrium, and below the, azygos vein., The right main bronchus is shorter, wider and more vertical than the left main bronchus and, therefore the route taken by most foreign bodies., , Image sourced from Wikipedia, , Left lung, Above the hilum is the furrow produced by the aortic arch, and then superiorly the groove, accommodating the left subclavian artery; Behind the hilum and pulmonary ligament is a vertical, groove produced by the descending aorta, and in front of this, near the base of the lung, is the lower, part of the oesophagus., The root of the left lung passes under the aortic arch and in front of the descending aorta.
Page 2329 :
Image sourced from Wikipedia, , Inferior borders of both lungs, , , , , 6th rib in mid clavicular line, 8th rib in mid axillary line, 10th rib posteriorly, , The pleura runs two ribs lower than the corresponding lung level., Bronchopulmonary segments, , Segment number, , Right lung, , Left lung, , 1, , Apical, , Apical, , 2, , Posterior, , Posterior, , 3, , Anterior, , Anterior, , 4, , Lateral, , Superior lingular, , 5, , Medial, , Inferior lingular, , 6, , Superior (apical), , Superior (apical)
Page 2330 :
Segment number, , Right lung, , Left lung, , 7, , Medial basal, , Medial basal, , 8, , Anterior basal, , Anterior basal, , 9, , Lateral basal, , Lateral basal, , 10, , Posterior basal, , Posterior basal, Next question
Page 2331 :
Question 547 of 560, , A 43 year old lady is undergoing an axillary node clearance for breast cancer. The nodal disease is, bulky. During clearance of the level 3 nodes there is suddenly brisk haemorrhage. The most likely, vessel responsible is:, , Thoracoacromial artery, , Cephalic vein, , Thoracodorsal trunk, , Internal mammary artery, , Posterior circumflex humeral artery, , The thoracoacromial artery pierces the pectoralis major and gives off branches within this space., The level 3 axillary nodes lie between pectoralis major and minor.Although the thoracodorsal trunk, may be injured during an axillary dissection it does not lie within the level 3 nodes., Please rate this question:, , Discuss and give feedback, , Next question, , Thoracoacromial artery, The thoracoacromial artery (acromiothoracic artery; thoracic axis) is a short trunk, which arises from, the forepart of the axillary artery, its origin being generally overlapped by the upper edge of the, Pectoralis minor., Projecting forward to the upper border of the Pectoralis minor, it pierces the coracoclavicular fascia
Page 2332 :
and divides into four branches: pectoral, acromial, clavicular, and deltoid., , Branch, , Description, , Pectoral, branch, , Descends between the two Pectoral muscles, and is distributed to them and to the breast,, anastomosing with the intercostal branches of the internal thoracic artery and with the, lateral thoracic., , Acromial, branch, , Runs laterally over the coracoid process and under the Deltoid, to which it gives branches; it, then pierces that muscle and ends on the acromion in an arterial network formed by, branches from the suprascapular, thoracoacromial, and posterior humeral circumflex, arteries., , Clavicular, branch, , Runs upwards and medially to the sternoclavicular joint, supplying this articulation, and the, Subclavius., , Deltoid, branch, , Arising with the acromial, it crosses over the Pectoralis minor and passes in the same, groove as the cephalic vein, between the Pectoralis major and Deltoid, and gives branches, to both muscles., Next question
Page 2333 :
Question 548 of 560, , A 73 year old lady with long standing atrial fibrillation develops a cold and pulseless white arm. A, brachial embolus is suspected and a brachial embolectomy is performed. Which of the following, structures is at greatest risk of injury during this procedure?, , Radial nerve, , Cephalic vein, , Ulnar nerve, , Median nerve, , None of the above, , The median nerve lies close to the brachial artery in the antecubital fossa. This is the usual site of, surgical access to the brachial artery for an embolectomy procedure. The median nerve may be, damaged during clumsy application of vascular clamps to the artery., Please rate this question:, , Discuss and give feedback, , Next question, , Brachial artery, The brachial artery begins at the lower border of teres major as a continuation of the axillary artery. It, terminates in the cubital fossa at the level of the neck of the radius by dividing into the radial and, ulnar arteries., Relations, Posterior relations include the long head of triceps with the radial nerve and profunda vessels
Page 2334 :
intervening. Anteriorly it is overlapped by the medial border of biceps., It is crossed by the median nerve in the middle of the arm., In the cubital fossa it is separated from the median cubital vein by the bicipital aponeurosis., The basilic vein is in contact at the most proximal aspect of the cubital fossa and lies medially., Next question
Page 2335 :
Question 549 of 560, A 73 year old lady is admitted with right iliac fossa pain. A plain abdominal x-ray is taken and the, caecal diameter measured. Which of the following caecal diameters is pathological?, , 4cm, , 5cm, , 6cm, , 7cm, , 10cm, , 8 cm is still within normal limits. However, caecal diameters of 9 and 10 are pathological and should, prompt further investigation., Please rate this question:, , Discuss and give feedback, , Next question, , Right colon, Ileocaecal valve, , , , , Entry point of the terminal ileum to the caecum, An important colonoscopic landmark, The ileocaecal valve is not always competent and this may allow partial decompression of an, obstructed colon, , Appendix, , , , , At the base of the caecum the taenia coalesce to mark the base of the appendix, This is a reliable way of locating the appendix surgically and is a constant landmark, The appendix has a small mesentery (the mesoappendix) and in this runs the appendiceal, artery, a branch of the ileocolic artery.
Page 2336 :
The posterior aspect of the right colon is extra peritoneal and the anterior aspect intraperitoneal., Relations, , , , Posterior, , Iliacus, Iliolumbar ligament, Quadratus lumborum, Transverse abdominis, Diaphragm at the tip of the, last rib; Lateral cutaneous, ilioinguinal, and iliohypogastric nerves; the iliac branches of the iliolumbar, vessels, the fourth lumbar artery, gonadal vessels, ureter and the right kidney., , , , Superior, , Right kidney which is embedded in the perinephric fat, , , , Medial, , Mesentery which contains the ileocolic artery that supplies the right colon and terminal ileum. A, further branch , the right colic artery, also contributes to supply the hepatic flexure and proximal, transverse colon. Medially these pass through the mesentery to join the SMA. This occurs near to, the head of the pancreas and care has to be taken when ligating the ileocolic artery near to its origin, in cancer cases for fear of impinging on the SMA., - Anterior, Coils of small intestine, the right edge of the greater omentum, and the anterior abdominal wall., Nerve supply, , , Parasympathetic fibres of the vagus nerve (CN X), , Arterial supply, , , Ileocolic artery and right colic artery, both branches of the SMA. While the ileocolic artery is, almost always present, the right colic can be absent in 5-15% of individuals., Next question
Page 2337 :
Question 550 of 560, Which of the following fingers is not a point of attachment for the palmar interossei?, , Middle finger, , Little finger, , Ring finger, , Index finger, , None of the above, , The middle finger has no attachment of the palmar interosseous., , Image sourced from Wikipedia, , Please rate this question:
Page 2339 :
Image sourced from Wikipedia, , Fascia and compartments of the palm, The fascia of the palm is continuous with the antebrachial fascia and the fascia of the dorsum of the, hand. The palmar fascia is thin over the thenar and hypothenar eminences. In contrast the palmar, fascia is relatively thick. The palmar aponeurosis covers the soft tissues and overlies the flexor, tendons. The apex of the palmar aponeurosis is continuous with the flexor retinaculum and the, palmaris longus tendon. Distally, it forms four longitudinal digital bands that attach to the bases of, the proximal phalanges, blending with the fibrous digital sheaths., A medial fibrous septum extends deeply from the medial border of the palmar aponeurosis to the 5th, metacarpal. Lying medial to this are the hypothenar muscles. In a similar fashion, a lateral fibrous, septum extends deeply from the lateral border of the palmar aponeurosis to the 3rd metacarpal. The, thenar compartment lies lateral to this area., Lying between the thenar and hypothenar compartments is the central compartment. It contains the, flexor tendons and their sheaths, the lumbricals, the superficial palmar arterial arch and the digital, vessels and nerves., The deepest muscular plane is the adductor compartment, which contains adductor pollicis., Short muscles of the hand, These comprise the lumbricals and interossei. The four slender lumbrical muscles flex the fingers at, the metacarpophalangeal joints and extend the interphalangeal joint. The four dorsal interossei are, located between the metacarpals and the four palmar interossei lie on the palmar surface of the, metacarpals in the interosseous compartment of the hand., Long flexor tendons and sheaths in the hand, The tendons of FDS and FDP enter the common flexor sheath deep to the flexor retinaculum. The, tendons enter the central compartment of the hand and fan out to their respective digital synovial, sheaths. Near the base of the proximal phalanx, the tendon of FDS splits to permit the passage of
Page 2340 :
FDP. The FDP tendons are attached to the margins of the anterior aspect of the base of the distal, phalanx., The fibrous digital sheaths contain the flexor tendons and their synovial sheaths. These extend from, the heads of the metacarpals to the base of the distal phalanges., Next question
Page 2341 :
Question 551 of 560, , A 33 year old man sustains an injury to his forearm and wrist. When examined in clinic he is unable, to adduct his thumb. What is the most likely underlying nerve lesion?, , Radial nerve, , Superficial branch of the ulnar nerve, , Median nerve, , Posterior interosseous nerve, , Deep branch of the ulnar nerve, , Theme from April 2013 Exam, Theme from April 2014 Exam, Damage to the deep branch of the ulnar nerve may result in an inability to adduct the thumb. This is, tested clinically by trying to withdraw a piece of paper from a patients hand grasped between thumb, and index finger., Please rate this question:, , Discuss and give feedback, , Next question, , Adductor pollicis, , Origin, , Insertion, , Nerve, supply, , Actions
Page 2342 :
Origin, , Insertion, , Tendon sheath of flexor, carpi radialis, Bases of second, third and, fourth metacarpals, Anterior aspect of the, trapezoid and capitate, bones, Transverse head comes, from the longitudinal ride, of the third metacarpal, , Fibres of the two heads converge, on insertion into the ulnar aspect, of the base of the proximal, phalanx of the thumb, , Nerve, supply, , Deep branch, of the ulnar, (C8, T1), , Actions, , Adducts the thumb, into the plane of the, palm and draws it to, the midline, , Next question
Page 2343 :
Question 552 of 560, A 6 year old sustains a supracondylar fracture of the distal humerus. There are concerns that the, radial nerve may have been injured. What is the relationship of the radial nerve to the humerus at, this point?, , Anterolateral, , Anteromedial, , Posterolateral, , Posteromedial, , Immediately anterior, , The radial nerve lies anterolateral to the humerus in the supracondylar area., Please rate this question:, , Discuss and give feedback, , Next question, , Radial nerve, Continuation of posterior cord of the brachial plexus (root values C5 to T1), Path, , , , , , , , In the axilla: lies posterior to the axillary artery on subscapularis, latissimus dorsi and teres, major., Enters the arm between the brachial artery and the long head of triceps (medial to humerus)., Spirals around the posterior surface of the humerus in the groove for the radial nerve., At the distal third of the lateral border of the humerus it then pierces the intermuscular, septum and descends in front of the lateral epicondyle., At the lateral epicondyle it lies deeply between brachialis and brachioradialis where it then, divides into a superficial and deep terminal branch., Deep branch crosses the supinator to become the posterior interosseous nerve., , In the image below the relationships of the radial nerve can be appreciated
Page 2345 :
Anatomical, location, , Muscle affected, , Effect of paralysis, , Shoulder, , Long head of triceps, , Minor effects on shoulder stability in abduction, , Arm, , Triceps, , Loss of elbow extension, , Forearm, , Supinator, Brachioradialis, Extensor carpi radialis, longus and brevis, , Weakening of supination of prone hand and, elbow flexion in mid prone position, , The cutaneous sensation of the upper limb- illustrating the contribution of the radial nerve, , Image sourced from Wikipedia, , Next question
Page 2346 :
Question 553 of 560, Which of the following muscles is penetrated by the parotid duct?, , Medial pterygoid, , Buccinator, , Levator anguli oris, , Temporalis, , Masseter, , The duct crosses the masseter muscle and buccal fat pad and then penetrates the buccinator, muscle to enter the oral cavity opposite the second upper molar tooth., Please rate this question:, , Discuss and give feedback, , Next question, , Parotid gland, Anatomy of the parotid gland, , Location, , Overlying the mandibular ramus; anterior and inferior to the ear., , Salivary duct, , Crosses the masseter, pierces the buccinator and drains adjacent to the, 2nd upper molar tooth (Stensen's duct)., , Structures passing, through the gland, , , , , , , Facial nerve (Mnemonic: The Zebra Buggered My Cat; Temporal, Zygomatic, Buccal, Mandibular, Cervical), External carotid artery, Retromandibular vein, Auriculotemporal nerve
Page 2347 :
Relations, , , , , Anterior: masseter, medial pterygoid, superficial temporal and, maxillary artery, facial nerve, stylomandibular ligament, Posterior: posterior belly digastric muscle, sternocleidomastoid,, stylohyoid, internal carotid artery, mastoid process, styloid, process, , Arterial supply, , Branches of external carotid artery, , Venous drainage, , Retromandibular vein, , Lymphatic drainage, , Deep cervical nodes, , Nerve innervation, , , , , , Parasympathetic-Secretomotor, Sympathetic-Superior cervical ganglion, Sensory- Greater auricular nerve, , Parasympathetic stimulation produces a water rich, serous saliva. Sympathetic stimulation leads to, the production of a low volume, enzyme-rich saliva., Next question
Page 2350 :
Branch, , Supplies, , Palmar cutaneous branch (Arises near the, middle of the forearm), , Skin on the medial part of the palm, , Dorsal cutaneous branch, , Dorsal surface of the medial part of the hand, , Superficial branch, , Cutaneous fibres to the anterior surfaces of the, medial one and one-half digits, , Deep branch, , Hypothenar muscles, All the interosseous muscles, Third and fourth lumbricals, Adductor pollicis, Medial head of the flexor pollicis brevis, , Effects of injury, , Damage at the wrist, , , , , , Wasting and paralysis of intrinsic hand muscles (claw hand), Wasting and paralysis of hypothenar muscles, Loss of sensation medial 1 and half fingers, , Damage at the elbow, , , , , Radial deviation of the wrist, Clawing less in 4th and 5th digits, Next question
Page 2351 :
Question 555 of 560, How many valves lie between the superior vena cava and the right atrium?, , None, , One, , Two, , Three, , Four, , There are no valves which is why it is relatively easy to insert a CVP line from the internal jugular, vein into the right atrium., Please rate this question:, , Discuss and give feedback, , Next question, , Superior vena cava, Drainage, , , , , , Head and neck, Upper limbs, Thorax, Part of abdominal walls, , Formation, , , , , Subclavian and internal jugular veins unite to form the right and left brachiocephalic veins, These unite to form the SVC, Azygos vein joins the SVC before it enters the right atrium, , Relations
Page 2352 :
Anterior, , Anterior margins of the right lung and pleura, , Posteromedial, , Trachea and right vagus nerve, , Posterolateral, , Posterior aspects of right lung and pleura, Pulmonary hilum is posterior, , Right lateral, , Right phrenic nerve and pleura, , Left lateral, , Brachiocephalic artery and ascending aorta, , Developmental variations, Anomalies of the connection of the SVC are recognised. In some individuals a persistent left sided, SVC drains into the right atrium via an enlarged orifice of the coronary sinus. More rarely the left, sided vena cava may connect directly with the superior aspect of the left atrium, usually associated, with an un-roofing of the coronary sinus. The commonest lesion of the IVC is for its abdominal, course to be interrupted, with drainage achieved via the azygos venous system. This may occur in, patients with left sided atrial isomerism., Next question
Page 2353 :
Question 556 of 560, Which of the following options in relation to the liver is true?, , Ligamentum venosum is an anterior relation of the liver, , The portal triad comprises the hepatic artery, hepatic vein and tributary of the bile duct, , The liver is completely covered by peritoneum, , There are no nerves within the porta hepatis, , The caudate lobe is superior to the porta hepatis, 'VC goes with VC', The ligamentun Venosum and Caudate is on same side as Vena Cava [posterior]., Ligamentum venosum is posterior to the liver. The portal triad contains the portal vein rather than the, hepatic vein. There is the 'bare area of the liver' created by a void due to the coronary ligament, layers being widely separated. There are sympathetic and parasympathetic nerves in the porta, hepatis., Please rate this question:, , Discuss and give feedback, , Next question, , Liver, Structure of the liver, , Right lobe, , , , , Supplied by right hepatic artery, Contains Couinaud segments V to VIII (-/+Sg I), , Left lobe, , , , , Supplied by the left hepatic artery, Contains Couinaud segments II to IV (+/- Sg1), , Quadrate lobe, , , , Part of the right lobe anatomically, functionally is part of the left
Page 2354 :
Caudate lobe, , , , , , , Couinaud segment IV, Porta hepatis lies behind, On the right lies the gallbladder fossa, On the left lies the fossa for the umbilical vein, , , , , , , , Supplied by both right and left hepatic arteries, Couinaud segment I, Lies behind the plane of the porta hepatis, Anterior and lateral to the inferior vena cava, Bile from the caudate lobe drains into both right and left hepatic ducts, , Detailed knowledge of Couinaud segments is not required for MRCS, , , Between the liver lobules are portal canals which contain the portal triad: Hepatic Artery,, Portal Vein, tributary of Bile Duct., , Relations of the liver, , Anterior, , Postero inferiorly, , Diaphragm, , Oesophagus, , Xiphoid process, , Stomach, , Duodenum, , Hepatic flexure of colon, , Right kidney, , Gallbladder, , Inferior vena cava
Page 2355 :
Porta hepatis, , Location, , Postero inferior surface, it joins nearly at right angles with the left sagittal fossa, and, separates the caudate lobe behind from the quadrate lobe in front, , Transmits, , , , , , , , Common hepatic duct, Hepatic artery, Portal vein, Sympathetic and parasympathetic nerve fibres, Lymphatic drainage of the liver (and nodes), , Ligaments, , Falciform ligament, , , , , , 2 layer fold peritoneum from the umbilicus to anterior liver surface, Contains ligamentum teres (remnant umbilical vein), On superior liver surface it splits into the coronary and left, triangular ligaments, , Ligamentum teres, , Joins the left branch of the portal vein in the porta hepatis, , Ligamentum, venosum, , Remnant of ductus venosus, , Arterial supply, , , Hepatic artery, , Venous, , , , Hepatic veins, Portal vein, , Nervous supply, , , Sympathetic and parasympathetic trunks of coeliac plexus, Next question
Page 2357 :
Question 558 of 560, The following statements regarding the rectus abdominis muscle are true except:, , It runs from the symphysis pubis to the xiphoid process, , Its nerve supply is from the ventral rami of the lower 6 thoracic nerves, , It has collateral supply from both superior and inferior epigastric vessels, , It lies in a muscular aponeurosis throughout its length, , It has a number of tendinous intersections that penetrate through the anterior layer of the, muscle, Rectus abdominis, , , , , , , Arises from the pubis., Inserts into 5th, 6th, 7th costal cartilages., The muscle lies in the rectal sheath, which also contains the superior and inferior epigastric, artery and vein., Action: flexion of thoracic and lumbar spine., Nerve supply: anterior primary rami of T7-12., , The aponeurosis is deficient below the arcuate line., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal wall, The 2 main muscles of the abdominal wall are the rectus abdominis (anterior) and the quadratus, lumborum (posterior)., The remaining abdominal wall consists of 3 muscular layers. Each muscle passes from the lateral, aspect of the quadratus lumborum posteriorly to the lateral margin of the rectus sheath anteriorly., Each layer is muscular posterolaterally and aponeurotic anteriorly.
Page 2358 :
Image sourced from Wikipedia, , Muscles of abdominal wall, , External, oblique, , , , , , , , , Internal, oblique, , , , , , , Transversus, abdominis, , , , , , , , , , , Lies most superficially, Originates from 5th to 12th ribs, Inserts into the anterior half of the outer aspect of the iliac crest, linea, alba and pubic tubercle, More medially and superiorly to the arcuate line, the aponeurotic layer, overlaps the rectus abdominis muscle, The lower border forms the inguinal ligament, The triangular expansion of the medial end of the inguinal ligament is, the lacunar ligament., Arises from the thoracolumbar fascia, the anterior 2/3 of the iliac crest, and the lateral 2/3 of the inguinal ligament, The muscle sweeps upwards to insert into the cartilages of the lower 3, ribs, The lower fibres form an aponeurosis that runs from the tenth costal, cartilage to the body of the pubis, At its lowermost aspect it joins the fibres of the aponeurosis of, transversus abdominis to form the conjoint tendon., Innermost muscle, Arises from the inner aspect of the costal cartilages of the lower 6 ribs ,, from the anterior 2/3 of the iliac crest and lateral 1/3 of the inguinal, ligament, Its fibres run horizontally around the abdominal wall ending in an, aponeurosis. The upper part runs posterior to the rectus abdominis., Lower down the fibres run anteriorly only., The rectus abdominis lies medially; running from the pubic crest and, symphysis to insert into the xiphoid process and 5th, 6th and 7th costal, cartilages. The muscles lies in a aponeurosis as described above., Nerve supply: anterior primary rami of T7-12, , Surgical notes, During abdominal surgery it is usually necessary to divide either the muscles or their aponeuroses.
Page 2359 :
During a midline laparotomy it is desirable to divide the aponeurosis. This will leave the rectus, sheath intact above the arcuate line and the muscles intact below it. Straying off the midline will, often lead to damage to the rectus muscles, particularly below the arcuate line where they may often, be in close proximity to each other., Next question
Page 2360 :
Question 559 of 560, Which of the following statements relating to sternocleidomastoid is untrue?, , The external jugular vein lies posteromedially., , It is supplied by the accessory nerve., , It has two heads of origin, , It inserts into the lateral aspect of the mastoid process., , It marks the anterior border of the posterior triangle., , The external jugular vein lies lateral (i.e. superficial) to the sternocleidomastoid., Please rate this question:, , Discuss and give feedback, , Next question, , Sternocleidomastoid, Anatomy, , Origin, , Rounded tendon attached to upper manubrium sterni and muscular head attached to, medial third of the clavicle, , Insertion, , Mastoid process of the temporal bone and lateral area of the superior nuchal line of, the occipital bone, , Innervation, , Spinal part of accessory nerve and anterior rami of C2 and C3 (proprioception), , Action, , , , , Both: extend the head at atlanto-occipital joint and flex the cervical, vertebral column. Accessory muscles of inspiration., Single: lateral flexion of neck, rotates head so face looks upward to the
Page 2361 :
opposite side, , Sternocleidomastoid divides the anterior and posterior triangles of the neck., Next question
Page 2362 :
Question 560 of 560, During liver mobilisation for a cadaveric liver transplant the hepatic ligaments will require, mobilisation. Which of the following statements relating to these structures is untrue?, , Lesser omentum arises from the porta hepatis and passes the lesser curvature of the, stomach, The falciform ligament divides into the left triangular ligament and coronary ligament, , The liver has an area devoid of peritoneum, , The coronary ligament is attached to the liver, , The right triangular ligament is an early branch of the left triangular ligament, , The right triangular ligament is a continuation of the coronary ligament., Please rate this question:, , Discuss and give feedback, , Liver, Structure of the liver, , Right lobe, , , , , Supplied by right hepatic artery, Contains Couinaud segments V to VIII (-/+Sg I), , Left lobe, , , , , Supplied by the left hepatic artery, Contains Couinaud segments II to IV (+/- Sg1), , Quadrate lobe, , , , , , , , Part of the right lobe anatomically, functionally is part of the left, Couinaud segment IV, Porta hepatis lies behind, On the right lies the gallbladder fossa, On the left lies the fossa for the umbilical vein
Page 2363 :
Caudate lobe, , , , , , , , Supplied by both right and left hepatic arteries, Couinaud segment I, Lies behind the plane of the porta hepatis, Anterior and lateral to the inferior vena cava, Bile from the caudate lobe drains into both right and left hepatic ducts, , Detailed knowledge of Couinaud segments is not required for MRCS, , , Between the liver lobules are portal canals which contain the portal triad: Hepatic Artery,, Portal Vein, tributary of Bile Duct., , Relations of the liver, , Anterior, , Postero inferiorly, , Diaphragm, , Oesophagus, , Xiphoid process, , Stomach, , Duodenum, , Hepatic flexure of colon, , Right kidney, , Gallbladder, , Inferior vena cava, , Porta hepatis, , Location, , Postero inferior surface, it joins nearly at right angles with the left sagittal fossa, and, separates the caudate lobe behind from the quadrate lobe in front
Page 2364 :
Transmits, , , , , , , , Common hepatic duct, Hepatic artery, Portal vein, Sympathetic and parasympathetic nerve fibres, Lymphatic drainage of the liver (and nodes), , Ligaments, , Falciform ligament, , , , , , 2 layer fold peritoneum from the umbilicus to anterior liver surface, Contains ligamentum teres (remnant umbilical vein), On superior liver surface it splits into the coronary and left, triangular ligaments, , Ligamentum teres, , Joins the left branch of the portal vein in the porta hepatis, , Ligamentum, venosum, , Remnant of ductus venosus, , Arterial supply, , , Hepatic artery, , Venous, , , , Hepatic veins, Portal vein, , Nervous supply, , , Sympathetic and parasympathetic trunks of coeliac plexus
Page 2365 :
Theme: Skin disease, , A., B., C., D., E., F., G., H., , Squamous cell carcinoma, Bowens disease, Actinic keratosis, Basal cell carcinoma, Malignant melanoma, Keratoacanthoma, Apthous ulcer, Pyogenic granuloma, , Please select the most likely underlying diagnosis for each of the following skin lesions. Each option, may be used once, more than once or not at all., , 1., , A 53 year old man presents with a nodule on his chin. He is concerned because it has grown, extremely rapidly over the course of the preceding week. On examination he has a swollen,, red, dome shaped lesion with a central defect that contains a keratinous type material., You answered Squamous cell carcinoma, The correct answer is Keratoacanthoma, Theme from April 2013 Exam, Keratoacanthomas are characterised by a rapid growth phase. This may mimic amelanotic, melanoma (although such rapid growth is rare even in these lesions). The keratin core is the, clue as to the true nature of the lesion., , 2., , A 68 year old farmer presents with a skin lesion on his forehead. It has been present for the, past 6 months and has grown slightly in size during that time. On examination he has an, ulcerated lesion with pearly white raised edges that measures 2cm in diameter., You answered Squamous cell carcinoma, The correct answer is Basal cell carcinoma, The raised pearly edges in an ulcerated lesion at a sun exposed site makes BCC most likely., , 3., , A 34 year old gardener presents with a lesion affecting the dorsum of his right hand. It has, been present for the past 10 days and occurred after he had been pruning rose bushes. On, examination he has a raised ulcerated lesion which bleeds easily on contact., You answered Squamous cell carcinoma
Page 2366 :
The correct answer is Pyogenic granuloma, Trauma is a common precipitant of pyogenic granuloma and contact bleeding and ulceration, are common., Please rate this question:, , Discuss and give feedback, , Next question, , Skin disorders in surgery- malignancy and related lesions, Non melanoma skin cancer (BCC and SCC) are some of the commonest types of human, malignancy. Up to 80% of these are BCC's with approximately 20% comprising SCC's. The, incidence of NMSC's increases with age and whilst there is a female preponderance in those under, 40 years of age, in latter life the sex incidence is roughly equal., The vast majority of NMSC's are related to UV light exposure. For SCC's the major pattern is is, chronic long term exposure. For BCC's, the pattern of sporadic exposure with episodes of burning is, more important. Organ transplant recipients have a markedly increased incidence of SCC, risk, factors include length of immunosuppression, ethnic origin and associated sunlight exposure., Human papilloma virus DNA is found in the majority of transplant recipient SCC's. In addition to this, increased risk, transplant recipients are also more likely to develop locoregional recurrences, following treatment., Actinic keratosis and SCC, Actinic keratosis is viewed as a premalignant lesion because there are atypical keratinocytes present, in the epidermis. In a person with 7 actinic keratosis the risks of subsequent SCC is of the order of, 10% at 10 years. The primary lesion is a rough erythematous papule with a white to yellow scale., Lesions are typically clustered at sites of chronic sun exposure., Squamous cell carcinoma in situ, Also known as Bowens disease the commonest presentation of in situ SCC is with an erythematous, scaling patch or elevated plaque arising on sun exposed skin in an elderly patient. Lesions may, arisede novo or from pre-existing actinic keratosis., Pathologically there is full thickness atypia of dermal keratinocytes over a broad zone. Nuclear, pleomorphism, apoptosis and abnormal mitoses are all seen., Invasive SCC, The commonest clinical presentation of SCC is with an erythematous keratotic papule or nodule on a, background of sun exposure. Ulceration may occur and both exophytic and endophytic areas may, be seen. Regional lymphadenopathy may be present., Pathologically there is downward proliferation of malignant cells and invasion of the basement, membrane. Poorly differentiated lesions may show perineural invasion and require, immunohistochemistry with S100 to distinguish them from melanomas (which stain strongly positive, with this marker)., Basal cell carcinoma
Page 2367 :
Nodular BCC, , Commonest variant (60%), Raised translucent papule, Usually affect the face, Large nodular BCC's are locally destructive, , Superficial BCC, , Usually appears as superficial erythematous macule affecting the trunk, Younger age at presentation (mean 57), May show areas of spontaneous regression, Horizontal growth pattern predominates, High recurrence rate (due to sub clinical lateral spread), , Morpheaform BCC, , Macroscopically resembles flat, slightly atrophic lesion or plaque, without well defined borders, Tumour has sub clinical lateral spread which increases recurrence rates, , Cystic BCC, , Often have clear or blue - grey appearance, Cystic degeneration may not be clinically obvious and tumour may, resemble nodular BCC, , Basosquamous, carcinoma, , Atypical BCC, Basaloid histological BCC features with eosinophillic squamoid, features of SCC, Biologically more aggressive and are more locally destructive, Rare lesion accounts for 1% of all non melanoma skin cancers, Metastatic disease may occur in 9-10% of cases and resemble an SCC, , Keratoacanthoma, Dome shaped erythematous lesions that develop over a period of days and grow rapidly. They often, contain a central pit of keratin. They then begin to necrose and slough off. They are generally benign, lesions although some do view them as precursors of malignancy. They may be treated by curettage, and cautery. If there is diagnostic doubt (they can mimic malignancy) then formal excision biopsy is, warranted., Pyogenic granuloma, These present as friable overgrowths of granulation at sites of minor trauma. They may be ulcerated, and bleeding on contact is common. They may be treated with curretage and cautery, formal, excision may be used if there is diagnostic doubt., Next question
Page 2368 :
Theme: Skin disorders, , A. Basal cell carcinoma, B. Dermatofibroma, C. Pilar cyst, D. Epidermoid cyst, E. Spitz naevus, F. Seborrhoeic keratosis, G. Atypical naevus, H. Capillary cavernous haemangioma, , Please select the most likely underlying nature of the skin lesion described. Each option may be, used once, more than once or not at all., , 4., , A 70 year old lady presents with a number of skin lesions that she describes as unsightly. On, examination she has a number of raised lesions with a greasy surface located over her trunk. Apart, from having a greasy surface the lesions also seem to have scattered keratin plugs located within, them., You answered Basal cell carcinoma, The correct answer is Seborrhoeic keratosis, Theme from September 2012 Exam, Seborrhoeic keratosis may have a number of appearances. However, the scaly, thick, greasy, surface with scattered keratin plugs makes this the most likely diagnosis., , 5., , A 28 year old female presents with a small nodule located on the back of her neck. It is excised for, cosmetic reasons and the histology report states that the lesion consists of a sebum filled lesion, surrounded by the outer root sheath of a hair follicle., You answered Basal cell carcinoma
Page 2369 :
The correct answer is Pilar cyst, Pilar cysts may contain foul smelling cheesy material and are surrounded by the outer part of a hair, follicle. Because of their histological appearances they are more correctly termed pilar cysts than, sebaceous cysts., , 6., , A 21 year old lady presents with a nodule on the posterior aspect of her right calf. It has been, present at the site for the past 6 months and occurred at the site of a previous insect bite., Although the nodule appears small, on palpation it appears to be nearly twice the size it appears, on examination. The overlying skin is faintly pigmented., You answered Basal cell carcinoma, The correct answer is Dermatofibroma, Dermatofibromas may be pigmented and are often larger than they appear. They frequently occur, at sites of previous trauma., , Please rate this question:, , Discuss and give feedback, , Next question, , Benign skin diseases, Seborrhoeic keratosis, , , , , , , , , Most commonly arise in patients over the age of 50 years, often idiopathic, Equal sex incidence and prevalence, Usually multiple lesions over face and trunk, Flat, raised, filiform and pedunculated subtypes are recognised, Variable colours and surface may have greasy scale overlying it, Treatment options consist of leaving alone or simple shave excision
Page 2370 :
Melanocytic naevi, , Congenital, melanocytic naevi, , , , , , Typically appear at, or soon after, birth, Usually greater than 1cm diameter, Increased risk of malignant transformation (increased risk greatest for, large lesions), , Junctional, melanocytic naevi, , , , , , Circular macules, May have heterogeneous colour even within same lesion, Most naevi of the palms, soles and mucous membranes are of this type, , Compound naevi, , , , , Domed pigmented nodules up to 1cm in diameter, Arise from junctional naevi, usually have uniform colour and are smooth, , Spitz naevus, , , , , , Usually develop over a few months in children, May be pink or red in colour, most common on face and legs, May grow up to 1cm and growth can be rapid, this usually results in, excision, , Atypical naevus, syndrome, , , , Atypical melanocytic naevi that may be autosomally dominantly, inherited, Some individuals are at increased risk of melanoma (usually have, mutations of CDKN2A gene), Many people with atypical naevus syndrome AND a parent sibling with, melanoma will develop melanoma, , , , , Epidermoid cysts, , , , , , Common and affect face and trunk, They have a central punctum, they may contain small quantities of sebum, The cyst lining is either normal epidermis (epidermoid cyst) or outer root sheath of hair, follicle (pilar cyst), , Dermatofibroma, , , , , , Solitary dermal nodules, Usually affect extremities of young adults, Lesions feel larger than they appear visually
Page 2372 :
Theme: Skin lesion diagnosis, , A., B., C., D., E., F., G., , Pyogenic granuloma, Amelanotic melanoma, Dermatitis herpetiformis, Scabies, Basal cell carcinoma, Squamous cell carcinoma, Keratoacanthoma, , Please select the most likely underlying diagnosis for the scenario given. Each option may be used, once, more than once or not at all., , 7., , A 72 year old man presents with a large nodule on his face. It is friable. There is no regional, lymphadenopathy. He is lost to follow up and re-attends several months later. On this, occasion the lesion has been noted to resolve with scarring., You answered Pyogenic granuloma, The correct answer is Keratoacanthoma, Keratoacanthomas may reach a considerable size prior to sloughing off and scarring., , 8., , A 22 year old girl is troubled by intensely itchy crops of blisters on her arms and legs. On, examination she is malnourished and she has papulovesicular eruptions over her elbows and, knees., You answered Pyogenic granuloma, The correct answer is Dermatitis herpetiformis, Dermatitis herpetiformis is seen in association with coeliac disease., , 9., , A 30 year old man cuts the corner of his lip whilst shaving. Over the next few days a large, purplish lesion appears at the site which bleeds on contact., Pyogenic granuloma, Pyogenic granulomas often appear at sites of trauma., , Please rate this question:
Page 2373 :
Discuss and give feedback, , Next question, , Skin Diseases, Skin lesions may be referred for surgical assessment, but more commonly will come via a, dermatologist for definitive surgical management., Skin malignancies include basal cell carcinoma, squamous cell carcinoma and malignant melanoma., Basal Cell Carcinoma, , , , , , , , Most common form of skin cancer., Commonly occur on sun exposed sites apart from the ear., Sub types include nodular, morphoeic, superficial and pigmented., Typically slow growing with low metastatic potential., Standard surgical excision, topical chemotherapy and radiotherapy are all successful., As a minimum a diagnostic punch biopsy should be taken if treatment other than standard, surgical excision is planned., , Squamous Cell Carcinoma, , , , , , , Again related to sun exposure., May arise in pre - existing solar keratoses., May metastasize if left., Immunosupression (e.g. following transplant), increases risk., Wide local excision is the treatment of choice and where a diagnostic excision biopsy has, demonstrated SCC, repeat surgery to gain adequate margins may be required., , Malignant Melanoma, , The main diagnostic features (major criteria):, , , , , Change in size, Change in shape, Change in colour, , Secondary features (minor criteria), , , , , , Diameter >6mm, Inflammation, Oozing or bleeding, Altered sensation, , Treatment, , , Suspicious lesions should undergo excision biopsy. The lesion should be removed in, completely as incision biopsy can make subsequent histopathological assessment difficult.
Page 2374 :
, , Once the diagnosis is confirmed the pathology report should be reviewed to determine, whether further re-excision of margins is required (see below):, , Margins of excision-Related to Breslow thickness, , Lesions 0-1mm thick, , 1cm, , Lesions 1-2mm thick, , 1- 2cm (Depending upon site and pathological features), , Lesions 2-4mm thick, , 2-3 cm (Depending upon site and pathological features), , Lesions >4 mm thick, , 3cm, , Marsden J et al. Revised UK guidelines for management of Melanoma. Br J Dermatol 2010 163:238256., Further treatments such as sentinel lymph node mapping, isolated limb perfusion and block, dissection of regional lymph node groups should be selectively applied., Kaposi Sarcoma, , , , , , , Tumour of vascular and lymphatic endothelium., Purple cutaneous nodules., Associated with immuno supression., Classical form affects elderly males and is slow growing., Immunosupression form is much more aggressive and tends to affect those with HIV related, disease., , Non malignant skin disease, Dermatitis Herpetiformis, , , , Chronic itchy clusters of blisters., Linked to underlying gluten enteropathy (coeliac disease)., , Dermatofibroma, , , , , , Benign lesion., Firm elevated nodules., Usually history of trauma., Lesion consists of histiocytes, blood vessels and fibrotic changes.
Page 2375 :
Pyogenic granuloma, , , , , , Overgrowth of blood vessels., Red nodules., Usually follow trauma., May mimic amelanotic melanoma., , Acanthosis nigricans, , , , , , Brown to black, poorly defined, velvety hyperpigmentation of the skin., Usually found in body folds such as the posterior and lateral folds of the neck, the axilla,, groin, umbilicus, forehead, and other areas., The most common cause of acanthosis nigricans is insulin resistance, which leads to, increased circulating insulin levels. Insulin spillover into the skin results in its abnormal, increase in growth (hyperplasia of the skin)., In the context of a malignant disease, acanthosis nigricans is a paraneoplastic syndrome and, is then commonly referred to as acanthosis nigricans maligna. Involvement of mucous, membranes is rare and suggests a coexisting malignant condition
Page 2376 :
A 22 year old man presents with an infected sebaceous cyst. The cyst itself is swollen, discharging, pus and has some surrounding erythema. What is the most appropriate treatment?, , Excision of the cyst of closure of the defect with interrupted 3/0 silk, , Excision of the cyst and closure of the defect with subcuticular 4/0 undyed nylon, , Incision and drainage with excision of the cyst wall and packing of the defect, , Incision and drainage with conservation of the cyst wall and packing of the defect, , Administration of oral co-amoxyclav and definitive surgery once the infection has cleared, , Similar theme in January 2013 Exam, The correct treatment for an infected sebaceous cyst is incision and drainage with removal of the, cyst wall. Conservation of the cyst wall will invariably lead to recurrence. Under no circumstances, should an infected wound like this be primarily closed. The administration of antibiotics without, drainage of sepsis is futile., Please rate this question:, , Discuss and give feedback, , Next question, , Sebaceous cysts, , , , , , , Originate from sebaceous glands and contain sebum., Location: anywhere but most common scalp, ears, back, face, and upper arm (not palms of, the hands and soles of the feet)., They will typically contain a punctum., Excision of the cyst wall needs to be complete to prevent recurrence., A Cock's 'Peculiar' Tumour is a suppurating and ulcerated sebaceous cyst. It may resemble, a squamous cell carcinoma- hence its name.
Page 2377 :
Theme: Management of skin lesions, , A., B., C., D., E., F., G., , Excision biopsy, Excision with 0.5 cm margin, Excision with 2 cm margin, Shave biopsy and cautery, Punch biopsy, Excision and full thickness skin graft, Discharge, , For each skin lesion please select the most appropriate management option. Each option may be, used once, more than once, or not at all., , 11., , A 22 year old women presents with a newly pigmented lesion on her right shin, it has, regular borders and normal appearing dermal appendages. However, she reports a recent, increase in size., Excision biopsy, Lesion bearing normal dermal appendages and regular borders are likely to be a benign, pigmented naevi. Therefore diagnostic and not radical excision is indicated., , 12., , A 58 year old lady presents with changes that are suspicious of lichen sclerosis of the, perineum., You answered Excision biopsy, The correct answer is Punch biopsy, Punch biopsies are a useful option for obtaining a full thickness tissues sample with, minimal tissue disruption. In this situation the other differential would be AIN or VIN and, punch biopsies would be useful in distinguishing these., , 13., , A 73 year old man presents with a 1.5cm ulcerated basal cell carcinoma on his back., You answered Excision biopsy, The correct answer is Excision with 0.5 cm margin, A small lesion such as this is adequately treated by local excision. The British Association, of Dermatology guidelines suggest that excision of conventional BCC (<2cm) with, margins of 3-5mm have locoregional control rates of 85%. Morpoeic lesions have higher, local recurrence rates.
Page 2378 :
Please rate this question:, , Discuss and give feedback, , Next question, , Skin Diseases, Skin lesions may be referred for surgical assessment, but more commonly will come via a, dermatologist for definitive surgical management., Skin malignancies include basal cell carcinoma, squamous cell carcinoma and malignant melanoma., Basal Cell Carcinoma, , , , , , , , Most common form of skin cancer., Commonly occur on sun exposed sites apart from the ear., Sub types include nodular, morphoeic, superficial and pigmented., Typically slow growing with low metastatic potential., Standard surgical excision, topical chemotherapy and radiotherapy are all successful., As a minimum a diagnostic punch biopsy should be taken if treatment other than standard, surgical excision is planned., , Squamous Cell Carcinoma, , , , , , , Again related to sun exposure., May arise in pre - existing solar keratoses., May metastasize if left., Immunosupression (e.g. following transplant), increases risk., Wide local excision is the treatment of choice and where a diagnostic excision biopsy has, demonstrated SCC, repeat surgery to gain adequate margins may be required., , Malignant Melanoma, , The main diagnostic features (major criteria):, , , , , Change in size, Change in shape, Change in colour, , Treatment, , Secondary features (minor criteria), , , , , , Diameter >6mm, Inflammation, Oozing or bleeding, Altered sensation
Page 2379 :
, , , Suspicious lesions should undergo excision biopsy. The lesion should be removed in, completely as incision biopsy can make subsequent histopathological assessment difficult., Once the diagnosis is confirmed the pathology report should be reviewed to determine, whether further re-excision of margins is required (see below):, , Margins of excision-Related to Breslow thickness, , Lesions 0-1mm thick, , 1cm, , Lesions 1-2mm thick, , 1- 2cm (Depending upon site and pathological features), , Lesions 2-4mm thick, , 2-3 cm (Depending upon site and pathological features), , Lesions >4 mm thick, , 3cm, , Marsden J et al. Revised UK guidelines for management of Melanoma. Br J Dermatol 2010 163:238256., Further treatments such as sentinel lymph node mapping, isolated limb perfusion and block, dissection of regional lymph node groups should be selectively applied., Kaposi Sarcoma, , , , , , , Tumour of vascular and lymphatic endothelium., Purple cutaneous nodules., Associated with immuno supression., Classical form affects elderly males and is slow growing., Immunosupression form is much more aggressive and tends to affect those with HIV related, disease., , Non malignant skin disease, Dermatitis Herpetiformis, , , , Chronic itchy clusters of blisters., Linked to underlying gluten enteropathy (coeliac disease)., , Dermatofibroma, , , , Benign lesion., Firm elevated nodules.
Page 2380 :
, , , Usually history of trauma., Lesion consists of histiocytes, blood vessels and fibrotic changes., , Pyogenic granuloma, , , , , , Overgrowth of blood vessels., Red nodules., Usually follow trauma., May mimic amelanotic melanoma., , Acanthosis nigricans, , , , , , Brown to black, poorly defined, velvety hyperpigmentation of the skin., Usually found in body folds such as the posterior and lateral folds of the neck, the axilla,, groin, umbilicus, forehead, and other areas., The most common cause of acanthosis nigricans is insulin resistance, which leads to, increased circulating insulin levels. Insulin spillover into the skin results in its abnormal, increase in growth (hyperplasia of the skin)., In the context of a malignant disease, acanthosis nigricans is a paraneoplastic syndrome and, is then commonly referred to as acanthosis nigricans maligna. Involvement of mucous, membranes is rare and suggests a coexisting malignant condition.
Page 2381 :
Theme: Dermatological manifestations of disease, , A., B., C., D., E., F., G., H., , Pyoderma gangrenosum, Erythroderma, Dermatitis herpetiformis, Acanthosis nigricans, Multiple lipomata, Multiple neurofibromata, Multiple telangectasia, None of the above, , Please select the skin disease associated with the condition described. Each option may be used, once, more than once or not at all., , 14., , A 22 year old man is investigated for weight loss. A duodenal biopsy taken as part of his, investigations shows total villous atrophy and lymphocytic infiltrate. He has a skin lesion, that has small itchy papules., You answered Pyoderma gangrenosum, The correct answer is Dermatitis herpetiformis, Theme from September 2012 Exam, The patient has coeliac disease and this is associated with dermatitis herpetiformis., , 15., , A 72 year old man is investigated for weight loss. On examination he is deeply jaundiced, and cachectic. He also has a dark velvety lesion coating his tongue., You answered Pyoderma gangrenosum, The correct answer is Acanthosis nigricans, Acanthosis nigricans may be associated with GI malignancies such as gastric and, pancreatic cancer., , 16., , A lesion that may occur in a 32 year old man with long standing Crohns disease., Pyoderma gangrenosum, Pyoderma gangrenosum may occur in Crohns disease., , Please rate this question:
Page 2382 :
Discuss and give feedback, , Next question, , Skin Diseases, Skin lesions may be referred for surgical assessment, but more commonly will come via a, dermatologist for definitive surgical management., Skin malignancies include basal cell carcinoma, squamous cell carcinoma and malignant melanoma., Basal Cell Carcinoma, , , , , , , , Most common form of skin cancer., Commonly occur on sun exposed sites apart from the ear., Sub types include nodular, morphoeic, superficial and pigmented., Typically slow growing with low metastatic potential., Standard surgical excision, topical chemotherapy and radiotherapy are all successful., As a minimum a diagnostic punch biopsy should be taken if treatment other than standard, surgical excision is planned., , Squamous Cell Carcinoma, , , , , , , Again related to sun exposure., May arise in pre - existing solar keratoses., May metastasize if left., Immunosupression (e.g. following transplant), increases risk., Wide local excision is the treatment of choice and where a diagnostic excision biopsy has, demonstrated SCC, repeat surgery to gain adequate margins may be required., , Malignant Melanoma, , The main diagnostic features (major criteria):, , , , , Change in size, Change in shape, Change in colour, , Secondary features (minor criteria), , , , , , Diameter >6mm, Inflammation, Oozing or bleeding, Altered sensation, , Treatment, , , Suspicious lesions should undergo excision biopsy. The lesion should be removed in, completely as incision biopsy can make subsequent histopathological assessment difficult.
Page 2383 :
, , Once the diagnosis is confirmed the pathology report should be reviewed to determine, whether further re-excision of margins is required (see below):, , Margins of excision-Related to Breslow thickness, , Lesions 0-1mm thick, , 1cm, , Lesions 1-2mm thick, , 1- 2cm (Depending upon site and pathological features), , Lesions 2-4mm thick, , 2-3 cm (Depending upon site and pathological features), , Lesions >4 mm thick, , 3cm, , Marsden J et al. Revised UK guidelines for management of Melanoma. Br J Dermatol 2010 163:238256., Further treatments such as sentinel lymph node mapping, isolated limb perfusion and block, dissection of regional lymph node groups should be selectively applied., Kaposi Sarcoma, , , , , , , Tumour of vascular and lymphatic endothelium., Purple cutaneous nodules., Associated with immuno supression., Classical form affects elderly males and is slow growing., Immunosupression form is much more aggressive and tends to affect those with HIV related, disease., , Non malignant skin disease, Dermatitis Herpetiformis, , , , Chronic itchy clusters of blisters., Linked to underlying gluten enteropathy (coeliac disease)., , Dermatofibroma, , , , , , Benign lesion., Firm elevated nodules., Usually history of trauma., Lesion consists of histiocytes, blood vessels and fibrotic changes.
Page 2384 :
Pyogenic granuloma, , , , , , Overgrowth of blood vessels., Red nodules., Usually follow trauma., May mimic amelanotic melanoma., , Acanthosis nigricans, , , , , , Brown to black, poorly defined, velvety hyperpigmentation of the skin., Usually found in body folds such as the posterior and lateral folds of the neck, the axilla,, groin, umbilicus, forehead, and other areas., The most common cause of acanthosis nigricans is insulin resistance, which leads to, increased circulating insulin levels. Insulin spillover into the skin results in its abnormal, increase in growth (hyperplasia of the skin)., In the context of a malignant disease, acanthosis nigricans is a paraneoplastic syndrome and, is then commonly referred to as acanthosis nigricans maligna. Involvement of mucous, membranes is rare and suggests a coexisting malignant condition
Page 2385 :
Which of the following statements relating to sebaceous cysts is false?, , When infected are also known as Cocks peculiar tumour, , Typically contain pus, , Are usually associated with a central punctum, , Most commonly occur on the scalp, , They will typically have a cyst wall, , Sebaceous cysts usually contain sebum, pus is only present in infected sebaceous cysts which, should then be treated by surgical incision and drainage., Please rate this question:, , Discuss and give feedback, , Next question, , Sebaceous cysts, , , , , , , Originate from sebaceous glands and contain sebum., Location: anywhere but most common scalp, ears, back, face, and upper arm (not palms of, the hands and soles of the feet)., They will typically contain a punctum., Excision of the cyst wall needs to be complete to prevent recurrence., A Cock's 'Peculiar' Tumour is a suppurating and ulcerated sebaceous cyst. It may resemble, a squamous cell carcinoma- hence its name., Next question
Page 2386 :
Which of the following statements relating to Keloid scars is untrue?, , They have a predilection for sternal , mandibular and deltiod area wounds, , They are confined to the margins of the original injury, , They often recur following excision, , May occur even after superficial injury, , They may be treated by injection of triamcinolone, Hypertrophic scars remain confined to the wound edges., Keloids (by definition) will tend to extend beyond the margins of the wound and in wounds of any, depth., Please rate this question:, , Discuss and give feedback, , Next question, , Wound healing, Surgical wounds are either incisional or excisional and either clean, clean contaminated or dirty., Although the stages of wound healing are broadly similar their contributions will vary according to the, wound type., The main stages of wound healing include:, Haemostasis, , , , Minutes to hours following injury, Vasospasm in adjacent vessels, platelet plug formation and generation of fibrin rich clot., , Inflammation, , , , Typically days 1-5, Neutrophils migrate into wound (function impaired in diabetes).
Page 2387 :
, , , , Growth factors released, including basic fibroblast growth factor and vascular endothelial, growth factor., Fibroblasts replicate within the adjacent matrix and migrate into wound., Macrophages and fibroblasts couple matrix regeneration and clot substitution., , Regeneration, , , , , , Typically days 7 to 56, Platelet derived growth factor and transformation growth factors stimulate fibroblasts and, epithelial cells., Fibroblasts produce a collagen network., Angiogenesis occurs and wound resembles granulation tissue., , Remodeling, , , , , , , From 6 weeks to 1 year, Longest phase of the healing process and may last up to one year (or longer)., During this phase fibroblasts become differentiated (myofibroblasts) and these facilitate, wound contraction., Collagen fibres are remodeled., Microvessels regress leaving a pale scar., , The above description represents an idealised scenario. A number of diseases may distort this, process. Neovascularisation is an important early process. Endothelial cells may proliferate in the, wound bed and recanalise to form a vessel. Vascular disease, shock and sepsis can all compromise, microvascular flow and impair healing., Conditions such as jaundice will impair fibroblast synthetic function and immunity with a detrimental, effect in most parts of the healing process., Problems with scars:, Hypertrophic scars, Excessive amounts of collagen within a scar. Nodules may be present histologically containing, randomly arranged fibrils within and parallel fibres on the surface. The tissue itself is confined to the, extent of the wound itself and is usually the result of a full thickness dermal injury. They may go on, to develop contractures., Image of hypertrophic scarring. Note that it remains confined to the boundaries of the original, wound:
Page 2388 :
Image sourced from Wikipedia, , Keloid scars, Excessive amounts of collagen within a scar. Typically a keloid scar will pass beyond the boundaries, of the original injury. They do not contain nodules and may occur following even trivial injury. They, do not regress over time and may recur following removal., Image of a keloid scar. Note the extension beyond the boundaries of the original incision:, , Image sourced from Wikipedia, , Drugs which impair wound healing:
Page 2389 :
, , , , , Non steroidal anti inflammatory drugs, Steroids, Immunosupressive agents, Anti neoplastic drugs, , Closure, Delayed primary closure is the anatomically precise closure that is delayed for a few days but before, granulation tissue becomes macroscopically evident., Secondary closure refers to either spontaneous closure or to surgical closure after granulation tissue, has formed.
Page 2390 :
A 72 year old man presents with a lesion on his back. Its appearances are as shown below:, , Image sourced from Wikipedia, , What is the most likely diagnosis?, , Amelanotic malignant melanoma, , Squamous cell carcinoma, , Merkel Cell tumour, , Basal cell carcinoma, , None of the above, , The lesion has all the characteristic features of a basal cell carcinoma. Including raised surface and, overlying telangectasia. Amelanotic melanomas are rare lesions and usually have a more ulcerated, appearance. Since the question is directed towards the most likely diagnosis the correct answer is, basal cell carcinoma., Clinical images are not currently part of the MRCS Part A, Please rate this question:, , Discuss and give feedback, , Next question
Page 2391 :
Skin Diseases, Skin lesions may be referred for surgical assessment, but more commonly will come via a, dermatologist for definitive surgical management., Skin malignancies include basal cell carcinoma, squamous cell carcinoma and malignant melanoma., Basal Cell Carcinoma, , , , , , , , Most common form of skin cancer., Commonly occur on sun exposed sites apart from the ear., Sub types include nodular, morphoeic, superficial and pigmented., Typically slow growing with low metastatic potential., Standard surgical excision, topical chemotherapy and radiotherapy are all successful., As a minimum a diagnostic punch biopsy should be taken if treatment other than standard, surgical excision is planned., , Squamous Cell Carcinoma, , , , , , , Again related to sun exposure., May arise in pre - existing solar keratoses., May metastasize if left., Immunosupression (e.g. following transplant), increases risk., Wide local excision is the treatment of choice and where a diagnostic excision biopsy has, demonstrated SCC, repeat surgery to gain adequate margins may be required., , Malignant Melanoma, , The main diagnostic features (major criteria):, , , , , Change in size, Change in shape, Change in colour, , Secondary features (minor criteria), , , , , , Diameter >6mm, Inflammation, Oozing or bleeding, Altered sensation, , Treatment, , , , Suspicious lesions should undergo excision biopsy. The lesion should be removed in, completely as incision biopsy can make subsequent histopathological assessment difficult., Once the diagnosis is confirmed the pathology report should be reviewed to determine, whether further re-excision of margins is required (see below):
Page 2392 :
Margins of excision-Related to Breslow thickness, , Lesions 0-1mm thick, , 1cm, , Lesions 1-2mm thick, , 1- 2cm (Depending upon site and pathological features), , Lesions 2-4mm thick, , 2-3 cm (Depending upon site and pathological features), , Lesions >4 mm thick, , 3cm, , Marsden J et al. Revised UK guidelines for management of Melanoma. Br J Dermatol 2010 163:238256., Further treatments such as sentinel lymph node mapping, isolated limb perfusion and block, dissection of regional lymph node groups should be selectively applied., Kaposi Sarcoma, , , , , , , Tumour of vascular and lymphatic endothelium., Purple cutaneous nodules., Associated with immuno supression., Classical form affects elderly males and is slow growing., Immunosupression form is much more aggressive and tends to affect those with HIV related, disease., , Non malignant skin disease, Dermatitis Herpetiformis, , , , Chronic itchy clusters of blisters., Linked to underlying gluten enteropathy (coeliac disease)., , Dermatofibroma, , , , , , Benign lesion., Firm elevated nodules., Usually history of trauma., Lesion consists of histiocytes, blood vessels and fibrotic changes.
Page 2393 :
Pyogenic granuloma, , , , , , Overgrowth of blood vessels., Red nodules., Usually follow trauma., May mimic amelanotic melanoma., , Acanthosis nigricans, , , , , , Brown to black, poorly defined, velvety hyperpigmentation of the skin., Usually found in body folds such as the posterior and lateral folds of the neck, the axilla,, groin, umbilicus, forehead, and other areas., The most common cause of acanthosis nigricans is insulin resistance, which leads to, increased circulating insulin levels. Insulin spillover into the skin results in its abnormal, increase in growth (hyperplasia of the skin)., In the context of a malignant disease, acanthosis nigricans is a paraneoplastic syndrome and, is then commonly referred to as acanthosis nigricans maligna. Involvement of mucous, membranes is rare and suggests a coexisting malignant condition., Next question
Page 2394 :
A 29 year old man presents with a lump in his scalp. It is located approximately 4cm superior to the, external occipital protuberance. It feels smooth and slightly fluctuant and has a centrally located, small epithelial defect. What is the most likely underlying diagnosis?, , Cocks peculiar tumour, , Dermoid cyst, , Sebaceous cyst, , Merkel cell tumour, , Seborrhoeic wart, , Sebaceous cysts are most frequently located in the scalp and have an associated central punctum., They may become infected and develop superficial ulceration in which case they are known as, "Cocks Peculiar Tumour". The presence of a punctum is highly suggestive of a sebaceous cyst and, are not typically found in the other lesions described., Please rate this question:, , Discuss and give feedback, , Next question, , Sebaceous cysts, , , , , , , Originate from sebaceous glands and contain sebum., Location: anywhere but most common scalp, ears, back, face, and upper arm (not palms of, the hands and soles of the feet)., They will typically contain a punctum., Excision of the cyst wall needs to be complete to prevent recurrence., A Cock's 'Peculiar' Tumour is a suppurating and ulcerated sebaceous cyst. It may resemble, a squamous cell carcinoma- hence its name.
Page 2395 :
Theme: Management of skin diseases, , A., B., C., D., E., F., G., , Excision biopsy, Excision with 1 cm margin, Excision with 5 cm margin, Shave biopsy and cautery, Punch biopsy, Excision and full thickness skin graft, Discharge, , For each scenario please select the most appropriate management option. Each option may be used, once, more than once or not at all., , 21., , A 89 year old women presents with long standing seborrhoeic warts of her abdominal wall, , they have caused troublesome itching., You answered Excision biopsy, The correct answer is Shave biopsy and cautery, These lesions are often extensive and superficial. Shave excision will suffice, material, must be sent for histology., , 22., , A 22 year old man has an excision biopsy of a pigmented lesion from his back, histology, shows a 1mm depth nodular melanoma, all resection margins are clear of tumour and the, nearest is 0.5cm., You answered Excision biopsy, The correct answer is Excision with 1 cm margin, This man will require re-excision of margins so that a 1cm margin around the lesion is, achieved. This can usually be achieved without skin grafting., , 23., , A 73 year old lady presents to the breast clinic with a weeping crusty skin lesion of the left, nipple. There are no masses to feel in the breast itself and imaging is normal., You answered Excision biopsy, The correct answer is Punch biopsy, This is likely to represent Pagets disease of the nipple and is best diagnosed on punch, biopsy.
Page 2396 :
Please rate this question:, , Discuss and give feedback, , Skin Diseases, Skin lesions may be referred for surgical assessment, but more commonly will come via a, dermatologist for definitive surgical management., Skin malignancies include basal cell carcinoma, squamous cell carcinoma and malignant melanoma., Basal Cell Carcinoma, , , , , , , , Most common form of skin cancer., Commonly occur on sun exposed sites apart from the ear., Sub types include nodular, morphoeic, superficial and pigmented., Typically slow growing with low metastatic potential., Standard surgical excision, topical chemotherapy and radiotherapy are all successful., As a minimum a diagnostic punch biopsy should be taken if treatment other than standard, surgical excision is planned., , Squamous Cell Carcinoma, , , , , , , Again related to sun exposure., May arise in pre - existing solar keratoses., May metastasize if left., Immunosupression (e.g. following transplant), increases risk., Wide local excision is the treatment of choice and where a diagnostic excision biopsy has, demonstrated SCC, repeat surgery to gain adequate margins may be required., , Malignant Melanoma, , The main diagnostic features (major criteria):, , , , , Change in size, Change in shape, Change in colour, , Treatment, , Secondary features (minor criteria), , , , , , Diameter >6mm, Inflammation, Oozing or bleeding, Altered sensation
Page 2397 :
, , , Suspicious lesions should undergo excision biopsy. The lesion should be removed in, completely as incision biopsy can make subsequent histopathological assessment difficult., Once the diagnosis is confirmed the pathology report should be reviewed to determine, whether further re-excision of margins is required (see below):, , Margins of excision-Related to Breslow thickness, , Lesions 0-1mm thick, , 1cm, , Lesions 1-2mm thick, , 1- 2cm (Depending upon site and pathological features), , Lesions 2-4mm thick, , 2-3 cm (Depending upon site and pathological features), , Lesions >4 mm thick, , 3cm, , Marsden J et al. Revised UK guidelines for management of Melanoma. Br J Dermatol 2010 163:238256., Further treatments such as sentinel lymph node mapping, isolated limb perfusion and block, dissection of regional lymph node groups should be selectively applied., Kaposi Sarcoma, , , , , , , Tumour of vascular and lymphatic endothelium., Purple cutaneous nodules., Associated with immuno supression., Classical form affects elderly males and is slow growing., Immunosupression form is much more aggressive and tends to affect those with HIV related, disease., , Non malignant skin disease, Dermatitis Herpetiformis, , , , Chronic itchy clusters of blisters., Linked to underlying gluten enteropathy (coeliac disease)., , Dermatofibroma, , , , Benign lesion., Firm elevated nodules.
Page 2398 :
, , , Usually history of trauma., Lesion consists of histiocytes, blood vessels and fibrotic changes., , Pyogenic granuloma, , , , , , Overgrowth of blood vessels., Red nodules., Usually follow trauma., May mimic amelanotic melanoma., , Acanthosis nigricans, , , , , , Brown to black, poorly defined, velvety hyperpigmentation of the skin., Usually found in body folds such as the posterior and lateral folds of the neck, the axilla,, groin, umbilicus, forehead, and other areas., The most common cause of acanthosis nigricans is insulin resistance, which leads to, increased circulating insulin levels. Insulin spillover into the skin results in its abnormal, increase in growth (hyperplasia of the skin)., In the context of a malignant disease, acanthosis nigricans is a paraneoplastic syndrome and, is then commonly referred to as acanthosis nigricans maligna. Involvement of mucous, membranes is rare and suggests a coexisting malignant condition.
Page 2399 :
A 48 year old lady undergoes a laparotomy and a retroperitoneal tumour is identified. The surgeons, suspect that the lesion is a liposarcoma. Which of the following is not typical of liposarcomas?, , They are the most common variant of sarcoma in adults, , Core biopsies in low grade liposarcomas may be normal, , May have a pseudocapsule, , It is unlikely in a lesion measuring less than 5cm, , Pulmonary metastasis are more likely than regional nodal involvement, , Malignant fibrous histiocytoma is the commonest variant of sarcoma and liposarcoma the second, most common. The presence of a pseudocapsule should be borne in mind when performing surgery,, as incomplete removal will result in local recurrence., Please rate this question:, , Discuss and give feedback, , Next question, , Sarcomas, , , Malignant tumours of mesenchymal origin, , Types, May be either bone or soft tissue in origin., Bone sarcoma include:, , , , , Osteosarcoma, Ewings sarcoma (although non bony sites recognised), Chondrosarcoma - originate from Chondrocytes, , Soft tissue sarcoma are a far more heterogeneous group and include:, , , , Liposarcoma-adipocytes, Rhabdomyosarcoma-striated muscle
Page 2400 :
, , , Leiomyosarcoma-smooth muscle, Synovial sarcomas- close to joints (cell of origin not known but not synovium), , Malignant fibrous histiocytoma is a sarcoma that may arise in both soft tissue and bone., Features, Certain features of a mass or swelling should raise suspicion for a sarcoma these include:, , , , , , Large >5cm soft tissue mass, Deep tissue location or intra muscular location, Rapid growth, Painful lump, , Assessment, Imaging of suspicious masses should utilise a combination of MRI, CT and USS. Blind biopsy should, not be performed prior to imaging and where required should be done in such a way that the biopsy, tract can be subsequently included in any resection., Ewings sarcoma, , , , , , , , Commoner in males, Incidence of 0.3 / 1, 000, 000, Onset typically between 10 and 20 years of age, Location by femoral diaphysis is commonest site, Histologically it is a small round tumour, Blood borne metastasis is common and chemotherapy is often combined with surgery, , Osteosarcoma, , , , , , , Mesenchymal cells with osteoblastic differentiation, 20% of all primary bone tumours, Incidence of 5 per 1,000,000, Peak age 15-30, commoner in males, Limb preserving surgery may be possible and many patients will receive chemotherapy, , Liposarcoma, , , , , , , Malignancy of adipocytes, Rare, approximately 2.5 per 1,000,000. They are the second most common soft tissue, sarcoma, Typically located in deep locations such as retroperitoneum, Affect older age group usually >40 years of age, May be well differentiated and thus slow growing although may undergo de-differentiation, and disease progression
Page 2401 :
, , , Many tumours will have a pseudocapsule that can misleadingly allow surgeons to feel that, they can 'shell out' these lesions. In reality, tumour may invade at the edge of the, pseudocapsule and result in local recurrence if this strategy is adopted, Usually resistant to radiotherapy, although this is often used in a palliative setting, , Malignant Fibrous Histiocytoma, , , , , , , Tumour with large number of histiocytes, Most common sarcoma in adults, Also described as undifferentiated pleomorphic sarcoma NOS (i.e. Cell of origin is not, known), Four major subtypes are recognised: storiform-pleomorphic (70% cases), myxoid (less, aggressive), giant cell and inflammatory, Treatment is usually with surgical resection and adjuvant radiotherapy as this reduces the, likelihood of local recurrence, Next question
Page 2402 :
A 63 year old lady with metastatic breast cancer presents with bone pain. Radiological tests show a, metastatic lytic deposit to her femoral shaft. The lesion occupies 75% of the bone diameter. What is, the most appropriate management?, , Surgical fixation with a dynamic compression plate, , Hemi-arthroplasty, , Fixation with intramedullary nail, , Radical radiotherapy, , Chemotherapy, Even with surgical fixation only 30% of pathological fractures unite. The type of fixation should be, chosen accordingly., A lesion of this nature is at high risk of spontaneous fracture. Whilst radiotherapy may palliate her, symptoms of pain it will not reduce the risk of fracture. In fit patients, an intramedullary nail should be, inserted. Very proximal lesions may be best managed by a total hip replacement, Please rate this question:, , Discuss and give feedback, , Next question, , Secondary malignant tumours of bone, Metastatic lesions affecting bone are more common than primary bone tumours., The typical tumours that spread to bone include:, , , , , , , Breast, Bronchus, Renal, Thyroid, Prostate, , 75% cases will affect those over the age of 50
Page 2403 :
The commonest bone sites affected are:, , , , , , , , Vertebrae (usually thoracic), Proximal femur, Ribs, Sternum, Pelvis, Skull, , Pathological fracture, Osteolytic lesions are the greatest risk for pathological fracture, The risk and load required to produce fracture varies according to bone site. Bones with lesions that, occupy 50% or less will be prone to fracture under loading (Harrington). When 75% of the bone is, affected the process of torsion about a bony fulcrum may produce a fracture., The Mirel scoring[1] system may be used to help determine the risk of fracture and is more, systematic than the Harrington system described above., Mirel Scoring system, , Score, points, , Site, , Radiographic, appearance, , Width of bone, involved, , Pain, , 1, , Upper extremity, , Blastic, , Less than 1/3, , Mild, , 2, , Lower, extremity, , Mixed, , 1/3 to 2/3, , Moderate, , 3, , Peritrochanteric, , Lytic, , More than 2/3, , Aggravated by, function, , Depending upon the score the treatment should be as follows:, , Score, , Risk of fracture, , Treatment, , 9 or greater, , Impending (33%), , Prophylactic fixation, , 8, , Borderline, , Consider fixation
Page 2404 :
Score, , Risk of fracture, , Treatment, , 7 or less, , Not impending (4%), , Non operative management, , Where the lesion is an isolated metastatic deposit consideration should be given to excision and, reconstruction as the outcome is better [2]., Non operative treatments, Hypercalcaemia- Treat with re hydration and bisphosphonates., Pain- Opiate analgesics and radiotherapy., Some tumours such as breast and prostate will benefit from chemotherapy and or hormonal agents., References, 1. Mirels, H. Metastatic disease in long bones. A proposed scoring system for diagnosing impending, pathologic fractures. Clin Orthop Relat Res, 1989(249): p. 256-64., 2. Mavrogenis, A.F. et al. Survival analysis of patients with femoral metastases. J Surg Oncol, 2011., Next question
Page 2405 :
Theme: Familial polyposis syndromes, , A. Peutz-Jeghers syndrome, B. Cowden disease, C. Familial adenomatous polyposis coli, D. Lynch syndrome, E. MYH associated polyposis, , Please select the familial cancer syndrome that most closely matches the description provided. Each, option may be used once, more than once or not at all., , 3., , A syndrome consisting of a PTEN mutation and intestinal hamartomas., You answered Peutz-Jeghers syndrome, The correct answer is Cowden disease, PTEN is a tumour supressor gene and loss of function mutations result in up regulation of the, mTOR pathway., , 4., , A syndrome which may be present in a patient with multiple intestinal hamartomas and, pigmentation spots around the mouth., Peutz-Jeghers syndrome, , 5., , A syndrome likely to be present in a 28 year old man who presents with a locally advanced, mucinous carcinoma of the caecum. There are scanty polyps in the remaining colon. His father died, from colorectal cancer aged 34., You answered Peutz-Jeghers syndrome, The correct answer is Lynch syndrome
Page 2406 :
Lynch syndrome is likely when right sided colonic cancers occur at a young age. These tumours are, often poorly differentiated and mucinous. The Amsterdam criteria can be used to identify families, at risk who may benefit from genetic testing., , Please rate this question:, , Discuss and give feedback, , Next question, , Polyposis syndromes, Screening and, management, , Associated, disorders, , Typically over 100, colonic adenomas, Cancer risk of 100%, 20% are new, mutations, , If known to be at risk, then predictive, genetic testing as, teenager, Annual flexible, sigmoidoscopy from, 15 years, If no polyps found, then 5 yearly, colonoscopy started, at age 20, Polyps found =, resectional surgery, (resection and pouch, Vs sub total, colectomy and IRA), , Gastric fundal, polyps (50%)., Duodenal polyps, 90%., If severe, duodenal, polyposis cancer, risk of 30% at 10, years., Abdominal, desmoid, tumours., , Multiple colonic, , Once identified, , Duodenal, , Syndrome, , Genetic defect, , Features, , Familial, adenomatous, polyposis, , Mutation of APC, gene (80%) cases,, dominant, , MYH, , Biallelic mutation
Page 2407 :
Screening and, management, , Associated, disorders, , polyps, Later onset right, sided cancers more, common than in FAP, 100% cancer risk by, age 60, , resection and, ileoanal pouch, reconstruction is, recommended, Attenuated, phenotype - regular, colonoscopy, , polyposis in 30%, Associated with, increased risk of, breast cancer, (self examination), , STK11 (LKB1), mutation on, chromosome 19 in, some (but not all), cases, dominant, , Multiple benign, intestinal, hamartomas, Episodic obstruction, and intussceception, Increased risk of GI, cancers (colorectal, cancer 20%, gastric, 5%), Increased risk of, breast, ovarian,, cervical pancreatic, and testicular, cancers, , Annual examination, Pan intestinal, endoscopy every 2-3, years, , Malignancies at, other sites, Classical, pigmentation, pattern, , Cowden, disease, , Mutation of PTEN, gene on, chromosome, 10q22, dominant, , Macrocephaly, Multiple intestinal, hamartomas, Multiple, trichilemmomas, 89% risk of cancer at, any site, 16% risk of colorectal, cancer, , Targeted, individualised, screening, , Breast cancer, (81% risk), Thyroid cancer, and non toxic, goitre, Uterine cancer, , HNPCC (Lynch, , Germline, , Colo rectal cancer, , Colonoscopy every 1-, , Extra colonic, , Syndrome, , Genetic defect, , Features, , associated, polyposis, , of mut Y human, homologue (MYH), on chromosome, 1p, recessive, , Peutz -Jeghers, syndrome
Page 2408 :
Syndrome, , Genetic defect, , Features, , syndrome), , mutations of DNA, mismatch repair, genes, , 30-70%, Endometrial cancer, 30-70%, Gastric cancer 5-10%, Scanty colonic polyps, may be present, Colonic tumours, likely to be right, sided and mucinous, , Screening and, management, , Associated, disorders, , 2 years from age 25, Consideration of, prophylactic surgery, Extra colonic, surveillance, recommended, , cancers, , Next question
Page 2409 :
A 45 year old women with breast cancer is started on a chemotherapy regime containing epirubicin., What is the primary mode of action of this drug?, , Intercalation of DNA, , Antimetabolite, , Monoclonal antibody to epidermal growth factor, , Inhibition of DNA gyrase, , Inhibition of topoisomerase 1, , Class, , Example, , Mode of action, , Antimetabolites, , 5 FU, , S Phase specific drug, mimics uracil and is, incorporated into RNA, , Anthracyclines*, , Doxorubicin, , Inhibits DNA and RNA synthesis by intercalating, base pairs, , Topoisomerase, inhibitors**, , Etoposide, , Inhibits topoisomerase II, prevents efficient DNA, coiling, , Platinum, , Cisplatin, , Crosslinks DNA, this then distorts molecule and, induces apoptosis (similar to alkylating agents), , Alkylating agent, , Cyclophosphamide, , Phosphoramide mustard forms DNA crosslinks and, then cell death, , Taxanes, , Docetaxal, , Disrupts microtubule formation
Page 2410 :
*=Main adverse effect cardiotoxicity, **=Irinotecan is a similar drug which works by inhibition of topoisomerase I, Please rate this question:, , Discuss and give feedback, , Next question, , Breast cancer treatment, Treatment, , Indication, , Endocrine, therapy, , , , , , Oestrogen receptor positive tumours, Downstaging primary lesions, Definitive treatment in old, infirm patients, , Irradiation, , , , , Wide local excision, Large lesion, high grade or marked vascular invasion following, mastectomy, , Chemotherapy, , , , , Downstaging advanced lesions to facilitate breast conserving surgery, Patients with grade 3 lesions or axillary nodal disease, , Endocrine agents, Tamoxifen is used and works as a partial oestrogen receptor agonist. It will typically block activity at, the breast. It does, however, stimulate the receptors at other sites and it is this that accounts for its, association with endometrial cancer. In post menopausal women the process of aromatisation, accounts for most oestrogen production. Therefore in this group aromatase inhibitors are the, preferred agents. Women who are perimenopausal start on tamoxifen and switch at 3 years., Chemotherapy, The FEC regime is most commonly used (Fluorouracil, epirubicin and cyclophosphamide). This was, found to be superior to the older CMF regime. The Taxanes are commonly used in high risk patients, and in this setting a regime of docetaxal, doxorubicin and cyclophosphamide may be used. The, anthracycline class drugs have marked cardiotoxicity (a property that they share with trastuzumab), and this can limit their use., Next question
Page 2411 :
A 50 year old lady presents with pain in her proximal femur. Imaging demonstrates a bone, metastasis from an unknown primary site. CT scanning with arterial phase contrast shows that the, lesion is hypervascular. From which of the following primary sites is the lesion most likely to have, originated?, , Breast, , Renal, , Bronchus, , Thyroid, , Colon, , Renal metastases have a tendency to be hypervascular. This is of considerable importance if, surgical fixation is planned., Please rate this question:, , Discuss and give feedback, , Next question, , Secondary malignant tumours of bone, Metastatic lesions affecting bone are more common than primary bone tumours., The typical tumours that spread to bone include:, , , , , , , Breast, Bronchus, Renal, Thyroid, Prostate, , 75% cases will affect those over the age of 50, The commonest bone sites affected are:, , , Vertebrae (usually thoracic)
Page 2412 :
, , , , , , Proximal femur, Ribs, Sternum, Pelvis, Skull, , Pathological fracture, Osteolytic lesions are the greatest risk for pathological fracture, The risk and load required to produce fracture varies according to bone site. Bones with lesions that, occupy 50% or less will be prone to fracture under loading (Harrington). When 75% of the bone is, affected the process of torsion about a bony fulcrum may produce a fracture., The Mirel scoring[1] system may be used to help determine the risk of fracture and is more, systematic than the Harrington system described above., Mirel Scoring system, , Score, points, , Site, , Radiographic, appearance, , Width of bone, involved, , Pain, , 1, , Upper extremity, , Blastic, , Less than 1/3, , Mild, , 2, , Lower, extremity, , Mixed, , 1/3 to 2/3, , Moderate, , 3, , Peritrochanteric, , Lytic, , More than 2/3, , Aggravated by, function, , Depending upon the score the treatment should be as follows:, , Score, , Risk of fracture, , Treatment, , 9 or greater, , Impending (33%), , Prophylactic fixation, , 8, , Borderline, , Consider fixation, , 7 or less, , Not impending (4%), , Non operative management
Page 2413 :
Where the lesion is an isolated metastatic deposit consideration should be given to excision and, reconstruction as the outcome is better [2]., Non operative treatments, Hypercalcaemia- Treat with re hydration and bisphosphonates., Pain- Opiate analgesics and radiotherapy., Some tumours such as breast and prostate will benefit from chemotherapy and or hormonal agents., References, 1. Mirels, H. Metastatic disease in long bones. A proposed scoring system for diagnosing impending, pathologic fractures. Clin Orthop Relat Res, 1989(249): p. 256-64., 2. Mavrogenis, A.F. et al. Survival analysis of patients with femoral metastases. J Surg Oncol, 2011., Next question
Page 2414 :
Which of the following group of patients are not screened for colorectal cancer?, , Peutz Jeghers syndrome, , Asymptomatic patients aged 45 years, , Acromegaly, , Ureterosigmoidostomy, , Inflammatory bowel disease, , Other disorders which are screened for colorectal malignancy include:, Familial adenomatous polyposis, Hereditary non polyposis colorectal cancer. The NHS screening, programme starts at 60., Please rate this question:, , Discuss and give feedback, , Next question, , Colorectal cancer screening and diagnosis, Overview, , , , , , Most cancers develop from adenomatous polyps. Screening for colorectal cancer has been, shown to reduce mortality by 16%, The NHS now has a national screening programme offering screening every 2 years to all, men and women aged 60 to 69 years. Patients aged over 70 years may request screening, Eligible patients are sent faecal occult blood (FOB) tests through the post, Patients with abnormal results are offered a colonoscopy, , At colonoscopy, approximately:, , , , , 5 out of 10 patients will have a normal exam, 4 out of 10 patients will be found to have polyps which may be removed due to their, premalignant potential, 1 out of 10 patients will be found to have cancer
Page 2415 :
Diagnosis, Essentially the following patients need referral:, - Altered bowel habit for more than six weeks, - New onset of rectal bleeding, - Symptoms of tenesmus, Colonoscopy is the gold standard, provided it is complete and good mucosal visualisation is, achieved. Other options include double contrast barium enema and CT colonography., Staging, Once a malignant diagnosis is made patients with colonic cancer will be staged using chest /, abdomen and pelvic CT. Patients with rectal cancer will also undergo evaluation of the mesorectum, with pelvic MRI scanning., For examination purposes the Dukes and TNM systems are preferred., Tumour markers, Carcinoembryonic antigen (CEA) is the main tumour marker in colorectal cancer. Not all tumours, secrete this, and it may be raised in conditions such as IBD. However, absolute levels do correlate, (roughly) with disease burden and it is once again being used routinely in follow up., Next question
Page 2416 :
A 56-year-old man with metastatic prostate cancer comes for review. He is known to have spinal, metastases but until now has not had any significant problems with pain control. Unfortunately he is, now getting regular back pain despite taking paracetamol 1g qds. Neurological examination is, unremarkable. What is the most appropriate next step?, , Switch to co-codamol 30/500, , Refer for radiotherapy, , Add oral bisphosphonate, , Add non steroidal anti inflammatory drug, , Add dexamethasone, Metastatic bone pain may respond to NSAIDs, bisphosphonates or radiotherapy, Bone pain often responds well to NSAIDs. Both radiotherapy and bisphosphonates have a role in, managing bony pain but these are not first-line treatments., Please rate this question:, , Discuss and give feedback, , Next question, , Palliative care prescribing: pain, SIGN issued guidance on the control of pain in adults with cancer in 2008. Selected points, , , , , , the breakthrough dose of morphine is one-sixth the daily dose of morphine, all patients who receive opioids should be prescribed a laxative, opioids should be used with caution in patients with chronic kidney disease. Alfentanil,, buprenorphine and fentanyl are preferred, metastatic bone pain may respond to NSAIDs, bisphosphonates or radiotherapy, , When increasing the dose of opioids the next dose should be increased by 30-50%., Conversion between opioids, , From, , To
Page 2417 :
From, , To, , Oral codeine, , Oral morphine, , Divide by 10, , Oral tramadol, , Oral morphine, , Divide by 5, , From, , To, , Oral morphine, , Oral oxycodone, , Divide by 2, , The BNF states that oral morphine sulphate 80-90mg over 24 hours is approximately equivalent to, one '25 mcg/hour' fentanyl patch, therefore product literature should be consulted., , From, , To, , Oral morphine, , Subcutaneous diamorphine, , Divide by 3, , Oral oxycodone, , Subcutaneous diamorphine, , Divide by 1.5, Next question
Page 2418 :
A 62 year old male is found to have colorectal cancer. He has Dukes C disease. What is his 5 year, prognosis?, , 100%, , 90%, , 80%, , 70%, , 60%, , Theme from September 2011 Exam, Please rate this question:, , Discuss and give feedback, , Next question, , Dukes classification, Gives the extent of spread of colorectal cancer, , Dukes A, , Tumour confined to the mucosa (95%), , Dukes B, , Tumour invading bowel wall (80%), , Dukes C, , Lymph node metastases (60%)
Page 2419 :
Dukes D, , Distant metastases (6%)(25% if resectable), , 5 year survival in brackets, Next question
Page 2420 :
Chordoma may typically occur at the following sites, except?, , Ribs, , Clivus, , Sacrum, , Lumbar vertebra, , Cervical vertebra, , Chordoma is a neoplasm originating from ectopic cellular remnants of the notochord and therefore, arises from the midline of the axial skeleton. It accounts for 24% of all primary malignant bone, tumours. Chordoma is the second commonest primary malignancy of the spine and accounts for, over 50% of primary sacral tumours. The neoplasm has a predilection for the sacrococcygeal (50%), and clival (40%) regions, with other areas of the spine rarely involved. More than one vertebral body, can be affected in half the cases. Chordomas most commonly present between 50 and 70 years of, age. Sex incidence is equal below 40 years, but men are affected twice as often at older ages,, particularly in the sacral region., The most frequent radiographic appearance of chordoma is that of a destructive lesion of a vertebral, body centered in the midline, with a large, associated soft-tissue mass., Please rate this question:, , Discuss and give feedback, , Next question, , Chordoma, Chordoma is a rare slow-growing bone tumour. Their favored origin is remnants of the notochord., Chordomas can arise anywhere from the skull base to the sacrum. The two most common locations, are the skull base and sacrum., There are three histological variants of chordoma: classical (or "conventional"), chondroid and dedifferentiated., , , The histological appearance of classical chordoma is of a lobulated tumor composed of, groups of cells separated by fibrous septa. The cells have small round nuclei and abundant, vacuolated cytoplasm.
Page 2421 :
, , Chondroid chordomas histologically show features of both chordoma and chondrosarcoma., , The 10-year tumor free survival rate for sacral chordoma was 46%. Chondroid chordomas appear to, have a more indolent clinical course., In most cases, complete surgical resection followed by radiation therapy offers the best chance of, long-term control. Unfortunately, the lesion has a close proximity to the spine itself and this can, compromise resection margins., Chordomas are relatively radioresistant, requiring high doses of radiation to be controlled. The, proximity of chordomas to vital neurological structures such as the brain stem and nerves limits the, dose of radiation that can safely be delivered. Therefore, highly focused radiation such as proton, therapy and carbon ion therapy are more effective than conventional x-ray radiation., Next question
Page 2422 :
In examining a biopsy of a primary tumour, the clearest evidence of malignancy is provided by:, , Absence of a capsule, , Basophilia of the cytoplasm, , Invasion of surrounding structures, , Excess of mitoses, , Nuclear aberrations, , Invasion is the hallmark of malignancy. The others may occur in insitu disease or dysplastic lesions., Please rate this question:, , Discuss and give feedback, , Next question, , Tissue sampling, Tissue sampling is an important surgical process. Biopsy modalities vary according to the site,, experience and subsequent planned therapeutic outcome, The modalities comprise:, -Fine needle aspiration cytology, -Core biopsy, -Excision biopsy, -Tru cut biopsy, -Punch biopsy, -Cytological smears, -Endoscopic or laparoscopic biopsy, When the lesion is superficial the decision needs to be taken as to whether complete excision is
Page 2423 :
desirable or whether excision biopsy is acceptable. In malignant melanoma for example the need for, safe margins will mean that a more radical surgical approach needs to be adopted after diagnostic, confirmation from excision biopsy than would be the case in basal cell carcinoma. Punch biopsies, are useful in gaining histological diagnosis of unclear skin lesions where excision biopsy is, undesirable such as in establishing whether a skin lesion is vasculitic or not., Fine needle aspiration cytology (FNAC) is an operator dependent procedure that may or may not be, image guided and essentially involves passing a needle through a lesion whilst suction is applied to, a syringe. The material thus obtained is expressed onto a slide and sent for cytological assessment., This test can be limited by operator inexperience and also by the lack of histological architectural, information (e.g. Follicular carcinoma of the thyroid). Where a discharge is present a sample may be, sent for cytology although in some sites (e.g. Nipple discharge ) the information gleaned may be, meaningless., Tissue samples may be obtained by both core and tru cut biopsy. A core biopsy is obtained by use, of a spring loaded gun with a needle passing quickly through the lesion of interest. A tru cut biopsy, achieves the same objective but the needle moved by hand. When performing these techniques, image guidance may be desirable (e.g. In breast lesions). Consideration needs to be given to any, planned surgical resection as it may be necessary to resect the biopsy tract along with the specimen, (e.g. In sarcoma surgery)., Visceral lesions may be accessed percutaneously under image guidance such as ultrasound guided, biopsy of liver metastases. Or under direct vision such as a colonoscopic biopsy., Next question
Page 2424 :
A 45 year old male is referred to clinic for consideration of resection of a lung malignancy. He reports, shortness of breath and haemoptysis. Investigations reveal a corrected calcium of 2.84 mmol/l, an, FEV 1 of 1.9L and histology of a squamous cell carcinoma. The patient is noted to have a hoarse, voice. Which one of the following is a contraindication to surgical resection in lung cancer?, , Haemoptysis, , FEV 1 of 1.9 litres, , Histology shows squamous cell cancer, , Vocal cord paralysis, , Calcium = 2.84 mmol/L, Contraindications to lung cancer surgery include SVC obstruction, FEV < 1.5, MALIGNANT pleural, effusion, and vocal cord paralysis, Paralysis of a vocal cord implies extracapsular spread to mediastinal nodes and is an indication of, inoperability., Please rate this question:, , Discuss and give feedback, , Next question, , Lung cancer: non-small cell management, Management, , , , , , Only 20% suitable for surgery, Mediastinoscopy performed prior to surgery as CT does not always show mediastinal lymph, node involvement, Curative or palliative radiotherapy, Poor response to chemotherapy, , Surgery contraindications, , , , Assess general health, Stage IIIb or IV (i.e. metastases present)
Page 2425 :
, , , , , , FEV1 < 1.5 litres is considered a general cut-off point*, Malignant pleural effusion, Tumour near hilum, Vocal cord paralysis, SVC obstruction, , * However if FEV1 < 1.5 for lobectomy or < 2.0 for pneumonectomy then some authorities advocate, further lung function tests as operations may still go ahead based on the results, Next question
Page 2426 :
A 43 year old lady is receiving chemotherapy for the treatment of metastatic breast cancer. You are, called because it has become apparent that her doxorubicin infusion has extravasated. What is the, most appropriate course of action?, , Stop the infusion and administer dexamethasone through the infusion device, , Stop the infusion and administer hyaluronidase through the infusion device, , Stop the infusion and apply a cold compress to the site, , Stop the infusion and apply a warm compress to the site, , Stop the infusion and administer sodium bicarbonate through the infusion device, , The application of cold compresses is indicated in doxorubicin extravasation. Warm compresses, increase the risk of doxorubicin ulceration. Hyaluronidase is indicated in the extravasation of contrast, media, TPN and vinca alkaloids. However, if administered following doxorubicin extravasation it will, dramatically worsen the situation and is contra indicated., Up to 50% of those sustaining severe injuries will require delayed surgical reconstruction., Please rate this question:, , Discuss and give feedback, , Next question, , Extravasation injury, Chemotherapy may be complicated by extravasation reactions in up to 6% of cases. The following, chemotherapy agents are recognised causes of extravasation reactions; doxorubicin, vincristine,, vinblastine, adriamycin, cisplatin, mitomycin and mithramycin., Up to 30% of extravasation reactions may be complicated by the development of ulceration., When an extravasation reaction is suspected, the infusion should be stopped and the infusing device, aspirated. The extremity should be elevated. As a general rule cold compresses have been shown to, reduce the incidence of subsequent ulceration with doxorubicin. Warm compresses have been found
Page 2427 :
to be beneficial in extravasation of vinca alkaloids. Dimethylsulfoxide may be infused in some cases,, ideally within 5 hours of the event occurring. No conclusive evidence exists to support the use of, corticosteroids or sodium bicarbonate for extravasation injuries., Extravasation of total parenteral nutrition solutions is usually managed by the local administration of, hyaluronidase to the infusion site., Next question
Page 2428 :
A 56 year old lady presents with a pathological fracture of the proximal femur. Which of the following, primary sites is the most likely source of her disease?, , Thyroid, , Breast, , Kidney, , Endometrium, , None of the above, Primary site= BBRTP, , , , , , , Breast, Bronchus, Renal, Thyroid, Prostate, , Theme from September 2011 exam, The correct answer is breast, because the question asks for the most likely primary site. Breast, cancer is the commonest cause of lytic bone metastasis in women of this age, especially from, amongst those options given., Please rate this question:, , Discuss and give feedback, , Next question, , Secondary malignant tumours of bone, Metastatic lesions affecting bone are more common than primary bone tumours., The typical tumours that spread to bone include:, , , , , Breast, Bronchus, Renal
Page 2429 :
, , , Thyroid, Prostate, , 75% cases will affect those over the age of 50, The commonest bone sites affected are:, , , , , , , , Vertebrae (usually thoracic), Proximal femur, Ribs, Sternum, Pelvis, Skull, , Pathological fracture, Osteolytic lesions are the greatest risk for pathological fracture, The risk and load required to produce fracture varies according to bone site. Bones with lesions that, occupy 50% or less will be prone to fracture under loading (Harrington). When 75% of the bone is, affected the process of torsion about a bony fulcrum may produce a fracture., The Mirel scoring[1] system may be used to help determine the risk of fracture and is more, systematic than the Harrington system described above., Mirel Scoring system, , Score, points, , Site, , Radiographic, appearance, , Width of bone, involved, , Pain, , 1, , Upper extremity, , Blastic, , Less than 1/3, , Mild, , 2, , Lower, extremity, , Mixed, , 1/3 to 2/3, , Moderate, , 3, , Peritrochanteric, , Lytic, , More than 2/3, , Aggravated by, function, , Depending upon the score the treatment should be as follows:, , Score, , Risk of fracture, , Treatment
Page 2430 :
Score, , Risk of fracture, , Treatment, , 9 or greater, , Impending (33%), , Prophylactic fixation, , 8, , Borderline, , Consider fixation, , 7 or less, , Not impending (4%), , Non operative management, , Where the lesion is an isolated metastatic deposit consideration should be given to excision and, reconstruction as the outcome is better [2]., Non operative treatments, Hypercalcaemia- Treat with re hydration and bisphosphonates., Pain- Opiate analgesics and radiotherapy., Some tumours such as breast and prostate will benefit from chemotherapy and or hormonal agents., References, 1. Mirels, H. Metastatic disease in long bones. A proposed scoring system for diagnosing impending, pathologic fractures. Clin Orthop Relat Res, 1989(249): p. 256-64., 2. Mavrogenis, A.F. et al. Survival analysis of patients with femoral metastases. J Surg Oncol, 2011., Next question
Page 2431 :
A 67-year-old man with colorectal cancer is currently taking MST 30mg bd for pain relief. What dose, of oral morphine solution should he be prescribed for breakthrough pain?, , 5 mg, , 10 mg, , 15 mg, , 20 mg, , 30 mg, Breakthrough dose = 1/6th of daily morphine dose, The total daily morphine dose is 30 * 2 = 60 mg, therefore the breakthrough dose should be onesixth of this, 10 mg., Please rate this question:, , Discuss and give feedback, , Palliative care prescribing: pain, SIGN issued guidance on the control of pain in adults with cancer in 2008. Selected points, , , , , , the breakthrough dose of morphine is one-sixth the daily dose of morphine, all patients who receive opioids should be prescribed a laxative, opioids should be used with caution in patients with chronic kidney disease. Alfentanil,, buprenorphine and fentanyl are preferred, metastatic bone pain may respond to NSAIDs, bisphosphonates or radiotherapy, , When increasing the dose of opioids the next dose should be increased by 30-50%., Conversion between opioids, , From, , To
Page 2432 :
From, , To, , Oral codeine, , Oral morphine, , Divide by 10, , Oral tramadol, , Oral morphine, , Divide by 5, , From, , To, , Oral morphine, , Oral oxycodone, , Divide by 2, , The BNF states that oral morphine sulphate 80-90mg over 24 hours is approximately equivalent to, one '25 mcg/hour' fentanyl patch, therefore product literature should be consulted., , From, , To, , Oral morphine, , Subcutaneous diamorphine, , Divide by 3, , Oral oxycodone, , Subcutaneous diamorphine, , Divide by 1.5
Page 2434 :
An orthopaedic surgeon makes a modification to an operative approach for total knee arthroplasty., After he has completed 25 cases, he stops and reviews his patient outcomes. He publishes the data., What level of evidence is supplied by this type of data?, , II, , IV, , III, , V, , I, , Case series that are non randomised and lack concurrent controls at best supply level IV evidence, only. To qualify for level I and II evidence a prospective randomised controlled trial with appropriate, blinding, control matching and power calculations is needed., Please rate this question:, , Discuss and give feedback, , Next question, , Levels of evidence, The level of evidence refers to the study design used by investigators to minimise bias., , Level of, evidence, , Source, , I, , Evidence obtained from systematic review of all relevant randomised controlled, trials, , II, , Evidence derived from at least one properly designed randomised controlled trial, , III, , Evidence derived from well designed pseudo-randomised controlled trials (e.g.
Page 2435 :
alternate allocation) or historical controls, , IV, , Evidence derived from case series or case reports, , V, , Panel or expert opinion, , Many of the categories contain sub groups, detailed knowledge of these are not required for MRCS, Part A., References, Interested users will find further information at www.cebm.net, Next question
Page 2436 :
Which of the following is not utilised as a descriptive statistic?, , Mean, , Median, , Mode, , Z score, , Standard deviation, , The z score is determined using the normal distribution and is not a descriptive statistic., Please rate this question:, , Discuss and give feedback, , Next question, , Descriptive statistics, Descriptive statistics include a point estimate of the measured variable as well as a measure of the, variability of the data around that point estimate. Typical examples of point estimates include; mean,, median and mode. The two most commonly employed measurements of variability include standard, deviation and the inter quartile range. The standard deviation is usually considered in association, with the mean, while the inter quartile range is used alongside the median. Other measures of data, variability include the standard error of the mean and confidence interval. The standard error of the, mean represents the measure of variation around the point estimate of the mean of a group of, sample means, as such it should only be used when describing the characteristics of more than one, sample., Next question
Page 2437 :
Theme: Use of suture materials and closure devices, , A. Silk 3/0, B. Polyglactin 3/0, C. Polydioxanone 1/0, D. Stainless steel skin clips, E. Stainless steel wire 1/0, F. 6/0 Polypropylene, G. 3/0 Undyed polyglactin, H. Polypropylene 3/0, , Please select the most appropriate suture material for the situation described. Each option may be, used once, more than once or not at all., , 3., , Mass closure of abdominal wall following elective right hemicolectomy through a midline incision., You answered Silk 3/0, The correct answer is Polydioxanone 1/0, PDS or polydioxanone is the ideal suture material. Non absorbable sutures have higher incidence of, incisional herniae., , 4., , Closure of the sternum following coronary artery bypass grafting., You answered Silk 3/0, The correct answer is Stainless steel wire 1/0, Stainless steel wire is typically used.
Page 2438 :
5., , Application of vein patch to femoral artery following endarterectomy., You answered Silk 3/0, The correct answer is 6/0 Polypropylene, Polypropylene is the suture of choice. Fine sutures are preferred., , Please rate this question:, , Discuss and give feedback, , Next question, , Suture material, Suture materials, , Agent, , Classification, , Durability, , Uses, , Special points, , Silk, , Braided, Biological, , Theoretically, permanent, although, strength not, preserved, , Anchoring devices, skin, closure, , Knots easily, poor, cosmesis, , Catgut, , Braided, Biological, , 5-7 days, , Short term wound, approximation, , Poor cosmesis, Degrades rapidly, Not available in UK, , Chromic catgut, , Braided, Biological, , Up to 12 weeks, , Apposition of deeply, sited tissues, , Unpredictable, degradation pattern
Page 2439 :
Agent, , Classification, , Durability, , Uses, , Special points, , Not in use in UK, , Polydiaxonone, (PDS), , Synthetic, Monofilament, , Up to 3 months, (longer with, thicker sutures), , Widespread surgical, applications including, visceral anastomoses,, dermal closure, mass, closure of abdominal, wall, , Used in most surgical, specialties (avoid dyed, form in dermal, closure), , Polyglycolic acid, (Vicryl, Dexon), , Braided, Synthetic, , Up to 6 weeks, , Most tissues can be, apposed using, polyglycolic acid, , It has good handling, properties, the dyed, form of this suture, should not be used for, skin closure, , Polypropylene, (Prolene), , Synthetic, Monofilament, , Permanent, , Widely used, agent of, choice for vascular, anastomoses, , Poor handling, properties, , Polyester, (Ethibond), , Synthetic, Braided, , Permanent, , Its combination of, permanency and, braiding makes it useful, for laparoscopic surgery, , It is more expensive, and has considerable, tissue drag, , Absorbable vs Non absorbable, , , , , , Time taken to degrade absorbable materials varies, Usually by macrophages hydrolysing material, Consider absorbable sutures in situations where long term tissue apposition is not required., In cardiac and vascular surgery non absorbable sutures are usually used., , Suture size
Page 2440 :
, , , The higher the index number the smaller the suture i.e. : 6/0 prolene is finer than 1/0 prolene., Finer sutures have less tensile strength. For example 6/0 prolene would not be a suture, suitable for abdominal mass closure but would be ideal for small calibre distal arterial, anastomoses., , Braided vs monofilament, Generally speaking braided sutures have better handling characteristics than non braided. However,, they are associated with higher bacterial counts. Braided materials are unsuitable for use in vascular, surgery as they are potentially thrombogenic., Next question
Page 2441 :
Which of the following visceral anastomoses has the lowest risk of anastomotic leak? You may, assume that all are constructed in ideal circumstances., , Stapled ileocolic anastomosis, , Hand sewn anastomosis of the proximal ileum, , Stapled colorectal anastomosis defunctioned with loop ileostomy, , Stapled colorectal anastomosis defunctioned with loop colostomy, , Hand sewn oesophagojejunal anastomosis, , Rectal and oesophageal surgery have some of the highest rates of anastomotic leakage. Following, anterior resection leaks are quoted to occur in up to 10% of cases. Small bowel anastomoses are, the most technically forgiving. Factors increasing the risk of anastamotic leakage include previous, irradiation, sepsis, malnutrition, poor blood supply and poor technique., The defunctioning of rectal anastomoses may reduce the clinical impact of anastomotic leak and, make it amenable to percutaneous drainage, but does not necessarily reduce the incidence of leaks, themselves., Please rate this question:, , Discuss and give feedback, , Next question, , Anastomoses, , , A wide variety of anastomoses are constructed in surgical practice. Essentially the term, refers to the restoration of luminal continuity. As such they are a feature of both abdominal, and vascular surgery., , Visceral anastomoses, For an anastomosis to heal three criteria need to be fulfilled:, , , , , , Adequate blood supply, Mucosal apposition, Minimal tension
Page 2442 :
When these are compromised the anastomosis may break down. Even in the best surgical hands, some anastomoses are more prone to dehiscence than others. Oesophageal and rectal, anastomoses are more prone to leakage and reported leak rates following oesophageal and rectal, surgery can be as high as 20%. This figure includes radiological leaks and those with a clinically, significant leak will be of a lower order of magnitude. As a rule small bowel anastomoses heal most, reliably., The decision as to how best to achieve mucosal apposition is one for each surgeon. Some will prefer, the use of stapling devices as they are quicker to use, others will prefer to perform a sutured, anastomosis. The attention to surgical technique is more important than the method chosen and a, poorly constructed stapled anastomosis in thickened tissue is far more prone to leakage than a hand, sewn anastomosis in the same circumstances., If an anastomosis looks unsafe then it may be best not to construct one at all. In colonic surgery this, is relatively clear cut and most surgeons would bring out an end colostomy. In situations such as, oesophageal surgery this is far more problematic and colonic interposition may be required in this, situation., Vascular anastomoses, Most arterial surgery involving bypasses or aneurysm repairs will require construction of an arterial, anastomosis. Technique is important and for small diameter distal arterial surgery the intimal, hyperplasia resulting from a badly constructed anastomosis may render the whole operation futile, before the patient leaves hospital., Some key points about vascular anastomoses:, , , , , , , Always use non absorbable monofilament suture (e.g. Polypropylene)., Round bodied needle., Correct size for anastamosis ( i.e. 6/0 prolene for bottom end of a femoro-distal bypass)., Suture should be continuous and from inside to outside of artery to avoid raising an intimal, flap., Next question
Page 2443 :
Theme: Management of skin wounds, , A., B., C., D., E., F., G., , Immediate split thickness skin graft, Delayed split thickness skin graft, Primary closure, Delayed primary closure, Compression bandages, Myocutaneous flap, Random free flap, , For each of the following injury scenarios please select the most appropriate management. Each, option may be used once, more than once or not at all., , 7., , A 63 year old male is gardening when he trips and lands on a scythe. He sustains a deep, laceration of his lateral thigh, it measures 3cm depth by 7cm length, it penetrates down to, the bone, but no fracture is evident on imaging or examination. His co- morbidities include, type II diabetes mellitus (diet controlled) and polymyalgia rheumatica (takes regular low, dose prednisolone)., You answered Immediate split thickness skin graft, The correct answer is Delayed primary closure, Theme from September 2012 Exam, Wounds which are contaminated or have the potential to become so are unsafe for, immediate primary closure. The combination of diabetes and steroids makes wound, complications more likely. Despite his high risk a primary skin graft or flap is unlikely to be, a safer option. Either may be used at a later date in the event that delayed primary closure is, unsuccessful., , 8., , A 71 year old lady trips over and falls landing on her left shin. She sustains a large pretibial, laceration of her leg., You answered Immediate split thickness skin graft, The correct answer is Delayed split thickness skin graft, Pretibial lacerations do not heal well. Simple apposition of skin edges almost always fails, due to poor quality dermal tissues and underlying haematoma. Debridement of devitalised, tissues prior to grafting usually gives the best results., , 9., , A 73 year old lady presents with an ulcer overlying her medial malleolus. It is painless and, has been present for 4 months. She has oedema of the lower limbs and her ABPI measures, 0.9.
Page 2444 :
You answered Immediate split thickness skin graft, The correct answer is Compression bandages, This is likely to be a venous leg ulcer. These are typically managed using compression, bandages. Contra indications to this technique include peripheral vascular disease (not, present here)., Please rate this question:, , Discuss and give feedback, , Next question, , Methods of wound closure, Method of, closure, , Indication, , Primary closure, , , , , , Clean wound, usually surgically created or following minor trauma, Standard suturing methods will usually suffice, Wound heals by primary intention, , Delayed primary, closure, , , , , Similar methods of actual closure to primary closure, May be used in situations where primary closure is either not, achievable or not advisable e.g. infection, , Vacuum assisted, closure, , , , , Uses negative pressure therapy to facilitate wound closure, Sponge is inserted into wound cavity and then negative pressure, applied, Advantages include removal of exudate and versatility, Disadvantages include cost and risk of fistulation if used incorrectly, on sites such as bowel, , , , , Split thickness, skin grafts, , , , , , Superficial dermis removed with Watson knife or dermatome, (commonly from thigh), Remaining epithelium regenerates from dermal appendages, Coverage may be increased by meshing
Page 2445 :
Full thickness skin, grafts, , , , , , , Whole dermal thickness is removed, Sub dermal fat is then removed and graft placed over donor site, Better cosmesis and flexibility at recipient site, Donor site "cost", , Flaps, , , , , , , Viable tissue with a blood supply, May be pedicled or free, Pedicled flaps are more reliable, but limited in range, Free flaps have greater range but carry greater risk of breakdown as, they require vascular anastomosis, Next question
Page 2446 :
Theme: Surgical energy devices, , A., B., C., D., E., F., G., H., , Monopolar diathermy, Bipolar diathermy, CUSA device, Argon plasma coagulation device, Ligasure device, Monopolar device in cutting mode, Monopolar device in coagulation mode, Monopolar device in blend mode, , Please select the most appropriate surgical energy device for the procedure described. Each option, may be used once, more than once or not at all., , 10., , Posterior dissection of the thyroid gland during total thyroid lobectomy, You answered Monopolar diathermy, The correct answer is Bipolar diathermy, This will minimise thermal trauma to the recurrent laryngeal nerve, , 11., , Undertaking a snare polypectomy for a villous adenoma of the descending colon, You answered Monopolar diathermy, The correct answer is Monopolar device in blend mode, Blend applies a mixture of coagulation and cutting modes to achieve smooth polypectomy, , 12., , Dissection of temporal lobe for tumour, You answered Monopolar diathermy, The correct answer is CUSA device, The ultrasonic dissector is the preferred tool for this. It is also extensively used in liver, resections, , Please rate this question:, , Discuss and give feedback
Page 2447 :
Next question, , Diathermy, , , , , , Diathermy devices are used by surgeons in all branches of surgery., Use electric currents to produce local heat and thereby facilitate haemostasis or surgical, dissection., Consist of a generator unit that is located outside the patient and can be set to the level of, power required by the surgeon., There are two major types of diathermy machine;, , Monopolar, The current flows through the diathermy unit into a handheld device that is controlled by the, surgeon. Electricity can flow from the tip of the device into the patient. The earth electrode is located, some distance away. The relatively narrow tip of the diathermy device produces local heat and this, can be used to vaporise and fulgurate tissues. The current can be adjusted in terms of frequency so, that different actions can be effected. In cutting mode sufficient power is applied to the tissues to, vaporise their water content. In coagulation mode the power level is reduced so that a coagulum is, formed instead. Some diathermy machines can utilise a setting known as blend that alternates, cutting and coagulation functions, these tend to be used during procedures such as colonoscopic, polypectomy., Bipolar, The electric current flows from one electrode to another however, both electrodes are usually, contained within the same device e.g. a pair of forceps. The result is that heating is localised to the, area between the two electrodes and surrounding tissue damage is minimised., Ultrasound based devices, These include CUSA and Harmonic scalpel. They generate high frequency oscillations that seal and, coagulate tissues. They have different energy settings that allow them to dissect and simultaneously, seal vessels if required. The CUSA device leaves vessels intact that may then be divided., Ligasure device, Delivers tailored energy levels to allow simultaneous haemostasis and dissection. The device, senses the impedance of the tissues and tailors energy levels accordingly., Hazards of diathermy, , , , Inadvertent patient burn. This may result of careless handling of the device or in the case of, monopolar devices forgetting to apply a return electrode plate, In this situation patients may, develop a contact burn when electricity flows to earth, Explosion or fire. This may occur when volatile anaesthetic gases or skin preparation fluid, have been used, Next question
Page 2448 :
Theme: Surgical drains, , A., B., C., D., E., F., G., , Redivac suction drain, Corrugated drain, Wallace Robinson drain (non suction), Penrose tubing, Latex T Tube drain, Silastic T Tube drain, No drain, , Please select the most appropriate surgical drainage system for the indication given. Each option, may be used once, more than once or not at all., , 13., , A 56 year old lady undergoes an open cholecystectomy and exploration of common bile, duct. The bile duct is closed over a drain., You answered Redivac suction drain, The correct answer is Latex T Tube drain, This will elicit a fibrotic response and encourage a track to form., , 14., , A 48 year old lady undergoes a mastectomy and axillary node clearance for an invasive, ductal cancer of the breast with lymph node metastasis., Redivac suction drain, The raw tissue exposed from the mastectomy site will often ooze serous fluid and may, result in seroma formation when the drain is removed., , 15., , A 75 year old man undergoes a Hartman's procedure for sigmoid diverticular disease with, pericolic abscess and colovesical fistula., You answered Redivac suction drain, The correct answer is Wallace Robinson drain (non suction), A non suction drain is the preferred option here., , Please rate this question:, , Discuss and give feedback
Page 2449 :
Next question, , Surgical drains, , , , , , , , Drains are inserted in many surgical procedures and are of many types., As a broad rule they can be divided into those using suction and those which do not., The diameter of the drain will depend upon the substance being drained, for example smaller, lumen drain for pneumothoraces vs haemothorax., Drains can be associated with complications and these begin with insertion when there may, be iatrogenic damage. When in situ they serve as a route for infections. In some specific, situations they may cause other complications, for example suction drains left in contact with, bowel for long periods may carry a risk of inducing fistulation., Drains should be inserted for a defined purpose and removed once the need has passed., , A brief overview of types of drain and sites is given below, CNS, , , Low suction drain or free drainage systems may be used for situations such as drainage of, sub dural haematomas., , CVS, , , Following cardiothoracic procedures of thoracic trauma underwater seal drains are often, placed. These should be carefully secured. When an air leak is present they may be placed, on suction whilst the air leak settles, , Orthopaedics and trauma, , , In this setting drains are usually used to prevent haematoma formation (with associated risk, of infection). Some orthopaedic drains may also be specially adapted to allow the drained, blood to be auto transfused., , Gastro-intestinal surgery, , , Surgeons often place abdominal drains either to prevent or drain abscesses, or to turn an, anticipated complication into one that can be easily controlled such as a bile leak following, cholecystectomy. The type of drain used will depend upon the indication., , Drain types
Page 2450 :
Type of drain, , Features, , Redivac, , , , , , Suction type of drain, Closed drainage system, High pressure vacuum system, , Low pressure, drainage systems, , , , Consist of small systems such as the lantern style drain that may be, used for short term drainage of small wounds and cavities, Larger systems are sometimes used following abdominal surgery,, they have a lower pressure than the redivac system, which decreases, the risks of fistulation, May be emptied and re-pressurised, , , , , , Latex tube drains, , , , , , May be shaped (e.g. T Tube) or straight, Usually used in non pressurised systems and act as sump drains, Most often used when it is desirable to generate fibrosis along the, drain track (e.g. following exploration of the CBD), , Chest drains, , , , , May be large or small diameter (depending on the indication), Connected to underwater seal system to ensure one way flow of air, , Corrugated drain, , , , , Thin, wide sheet of plastic, usually soft, Contains corrugations, along which fluids can track, Next question
Page 2451 :
Which of the following local anaesthetics is not an amino amide type?, , Lignocaine, , Xylocaine, , Procaine, , Bupivicaine, , Prilocaine, , All local anaesthetics have a chemical bond linking an amine to either an amide or an ester. Most, local anaesthetics are of the amino- amide types, these have a more favorable side effect profile and, are more stable in solution. Procaine and benzocaine have amino - ester groups, these are, metabolised by pseudocholinesterases., Please rate this question:, , Discuss and give feedback, , Next question, , Local anaesthetic agents, Lidocaine, , , , , , , , , An amide, Local anaesthetic and a less commonly used antiarrhythmic (affects Na channels in the, axon), Hepatic metabolism, protein bound, renally excreted, Toxicity: due to IV or excess administration. Increased risk if liver dysfunction or low protein, states. Note acidosis causes lidocaine to detach from protein binding., Drug interactions: Beta blockers, ciprofloxacin, phenytoin, Features of toxicity: Initial CNS over activity then depression as lidocaine initially blocks, inhibitory pathways then blocks both inhibitory and activating pathways. Cardiac arrhythmias., Increased doses may be used when combined with adrenaline to limit systemic absorption., , Cocaine
Page 2452 :
, , , , , Pure cocaine is a salt, usually cocaine hydrochloride. It is supplied for local anaesthetic, purposes as a paste., It is supplied for clinical use in concentrations of 4 and 10%. It may be applied topically to the, nasal mucosa. It has a rapid onset of action and has the additional advantage of causing, marked vasoconstriction., It is lipophillic and will readily cross the blood brain barrier. Its systemic effects also include, cardiac arrhythmias and tachycardia., Apart from its limited use in ENT surgery it is otherwise used rarely in mainstream surgical, practice., , Bupivacaine, , , , , , Bupivacaine binds to the intracellular portion of sodium channels and blocks sodium influx, into nerve cells, which prevents depolarization., It has a much longer duration of action than lignocaine and this is of use in that it may be, used for topical wound infiltration at the conclusion of surgical procedures with long duration, analgesic effect., It is cardiotoxic and is therefore contra indicated in regional blockage in case the tourniquet, fails., Levobupivicaine (Chirocaine) is less cardiotoxic and causes less vasodilation., , Prilocaine, , , Similar mechanism of action to other local anaesthetic agents. However, it is far less, cardiotoxic and is therefore the agent of choice for intravenous regional anaesthesia e.g., Biers Block., , All local anaesthetic agents dissociate in tissues and this contributes to their therapeutic effect. The, dissociation constant shifts in tissues that are acidic e.g. where an abscess is present, and this, reduces the efficacy., Doses of local anaesthetics, , Agent, , Dose plain, , Dose with adrenaline, , Lignocaine, , 3mg/Kg, , 7mg/Kg, , Bupivacaine, , 2mg/Kg, , 2mg/Kg, , Prilocaine, , 6mg/Kg, , 9mg/Kg
Page 2453 :
These are a guide only as actual doses depend on site of administration, tissue vascularity and comorbidities., Maximum total local anaesthetic doses, , , , , Lignocaine 1% plain - 3mg/ Kg - 200mg (20ml), Lignocaine 1% with 1 in 200,000 adrenaline - 7mg/Kg - 500mg (50ml), Bupivicaine 0.5% - 2mg/kg- 150mg (30ml), , Maximum doses are based on ideal body weight, Effects of adrenaline, Adrenaline may be added to local anaesthetic drugs. It prolongs the duration of action at the site of, injection and permits usage of higher doses (see above). It is contra indicated in patients taking, MAOI's or tricyclic antidepressants. The toxicity of bupivacaine is related to protein binding and, addition of adrenaline to this drug does not permit increases in the total dose of bupivacaine, in, contrast to the situation with lignocaine., References, An excellent review is provided by:, French J and Sharp L. Local Anaesthetics. Ann R Coll Surg Engl 2012; 94: 76-80., Next question
Page 2454 :
Theme: Biological therapies, , A. Bevacizumab, B. Infliximab, C. Trastuzumab, D. Basiliximab, E. Imatinib, F. Cetuximab, , Please select the most appropriate biological agent for the situation described. Each option may be, used once, more than once or not at all., , 17., , A 32 year old lady has previously undergone a wide local excision and axillary node clearance (5, nodes positive) for an invasive ductal carcinoma. It is oestrogen receptor negative, HER 2 positive,, vascular invasion is present. She has a lesion suspicious for metastatic disease in the left lobe of, her liver., You answered Bevacizumab, The correct answer is Trastuzumab, This ladies young age, coupled with ER negativity and extensive nodal disease with suspicion of, metastatic disease makes her a candidate for treatment with trastuzumab (herceptin)., , 18., , A 22 year old lady has severe peri anal crohns disease with multiple anal fistulae, the acute sepsis, has been drained and setons are in place. She is already receiving standard non biological, therapy., You answered Bevacizumab, The correct answer is Infliximab, Infliximab is a popular choice in managing complex peri anal crohns. It is absolutely vital that all
Page 2455 :
sepsis is drained prior to starting therapy., , 19., , A 63 year old man presents with a locally unresectable gastrointestinal stromal tumour. Biopsies, confirm that it is KIT positive., You answered Bevacizumab, The correct answer is Imatinib, Imatinib is licensed for treatment of GIST in the United Kingdom for this situation. The guidance, from the National Institute of Clinical evidence is that patients be reviewed at 12 weeks after, initiating therapy., , Please rate this question:, , Discuss and give feedback, , Next question, , Biological agents, Agents, , Target, , Uses, , Adalimumab, Infliximab, Etanercept, , TNF alpha inhibitor, , Crohns disease, Rheumatoid disease, , Bevacizumab, , Anti VEGF (anti angiogenic), , Colorectal cancer, Renal, Glioblastoma
Page 2457 :
Which of the following sutures has the largest diameter?, , 6/0 Polypropylene, , 5/0 Silk, , 3/0 Nylon, , 1 Polypropylene, , 0 Polydiaxone, , The sizes of suture material are not related to the composition of the suture material., Please rate this question:, , Discuss and give feedback, , Next question, , Suture sizes, USP Suture size and corresponding suture diameter, , USP Size, , Diameter in mm, , 11-0, , 0.01, , 10-0, , 0.02
Page 2458 :
6-0, , 0.07, , 3-0, , 0.2, , 0, , 0.35, , 1, , 0.4, Next question
Page 2459 :
Theme: Management of bleeding, , A. Ligate vessel, B. Underrun vessel, C. Use of diathermy, D. Application of surgicell, E. Digital pressure, , In each of the following scenarios the surgeon has encountered bleeding. Please select the most, appropriate immediate management of the situation from the list below. Each option may be used, once, more than once or not at all., , 21., , A 23 year old man is undergoing an open appendicectomy. The surgeons extend the incision, medially and suddenly encounter troublesome bleeding., Ligate vessel, Theme from April 2012 Exam, Medial extension of an appendicectomy incision carries the risk of injury to the inferior epigastric, artery. This can bleed briskly and is best managed by ligation., , 22., , A 45 year old man is undergoing a laparotomy and following incision of the skin multiple bleeding, points are identified in the dermis and sub dermal tissues., You answered Ligate vessel, The correct answer is Use of diathermy, Multiple bleeding points are best managed through the use of diathermy., , 23., , A 38 year old lady is undergoing a laparotomy when the surgeons damage the common iliac vein, whilst commencing a pelvic dissection.
Page 2460 :
You answered Ligate vessel, The correct answer is Digital pressure, Major venous bleeding such as this should be controlled with digital pressure in the first instance., The definitive management will usually consist of suturing the defect closed with prolene sutures., Transection of the common iliac vein will necessitate a major venous reconstruction., , Please rate this question:, , Discuss and give feedback, , Next question, , Management of bleeding, Bleeding is a process that is encountered in all branches of surgery. The decision as to how best to, manage bleeding depends upon the site, vessel and circumstances., Management of superficial dermal bleeding, This will usually cease spontaneously. If it is troublesome then direct use of monopolar or bipolar, cautery devices will usually control the situation. Scalp wounds are a notable exception and the, bleeding from these may be brisk. In this situation the use of mattress sutures as a wound closure, method will usually address the problem., Superficial arterial bleeding, If the vessel can be safely identified then the easiest method is to apply a haemostatic clip and ligate, the vessel., Major arterial bleeding, If the vessel can be clearly identified and is accessible then it may be possible to apply a clip and, ligate the vessel. If the vessel is located in a pool of blood then blind application of haemostatic clips, is highly dangerous and may result in collateral injury. In this situation evacuating the clot and, packing the area is often safer. The pack can then be carefully removed when the required, instruments are available. Some vessels may retract and bleeding may then be controlled by, dissection of surrounding structures or under-running the bleeding point., Major venous bleeding, The safest initial course of action is to apply digital pressure to the bleeding point. To control the
Page 2461 :
bleeding the surgeon will need a working suction device. Divided veins may require ligation., Incomplete lacerations of major veins (e.g. IVC) are best repaired. In order to do this it is safest to, apply a Satinsky type vascular clamp and repair the defect with 5/0 prolene., Bleeding from raw surfaces, This may be mixed bleeding and can be troublesome. Spray diathermy and argon plasma, coagulation are both useful agents. Certain topical haemostatic agents such as surgicell are useful, in encouraging clot formation and may be used in conjunction with, or instead of, the above agents., Next question
Page 2462 :
A 7 year old boy is due to undergo a circumcision for phimosis. Which of the following devices would, be the most appropriate agent to use for achieving haemostasis?, , Monopolar unit in cutting mode, , Bipolar unit, , Monopolar unit in coagulation mode, , Monopolar unit in blend mode, , Monopolar unit configured to spray mode, , The danger with the use of any source other than bipolar diathermy in this setting is the risk of, causing trauma to end vessels. All the monopolar units, regardless of the setting will carry this risk., Please rate this question:, , Discuss and give feedback, , Next question, , Diathermy, , , , , , Diathermy devices are used by surgeons in all branches of surgery., Use electric currents to produce local heat and thereby facilitate haemostasis or surgical, dissection., Consist of a generator unit that is located outside the patient and can be set to the level of, power required by the surgeon., There are two major types of diathermy machine;, , Monopolar, The current flows through the diathermy unit into a handheld device that is controlled by the, surgeon. Electricity can flow from the tip of the device into the patient. The earth electrode is located, some distance away. The relatively narrow tip of the diathermy device produces local heat and this, can be used to vaporise and fulgurate tissues. The current can be adjusted in terms of frequency so, that different actions can be effected. In cutting mode sufficient power is applied to the tissues to, vaporise their water content. In coagulation mode the power level is reduced so that a coagulum is, formed instead. Some diathermy machines can utilise a setting known as blend that alternates, cutting and coagulation functions, these tend to be used during procedures such as colonoscopic, polypectomy., Bipolar
Page 2463 :
The electric current flows from one electrode to another however, both electrodes are usually, contained within the same device e.g. a pair of forceps. The result is that heating is localised to the, area between the two electrodes and surrounding tissue damage is minimised., Ultrasound based devices, These include CUSA and Harmonic scalpel. They generate high frequency oscillations that seal and, coagulate tissues. They have different energy settings that allow them to dissect and simultaneously, seal vessels if required. The CUSA device leaves vessels intact that may then be divided., Ligasure device, Delivers tailored energy levels to allow simultaneous haemostasis and dissection. The device, senses the impedance of the tissues and tailors energy levels accordingly., Hazards of diathermy, , , , Inadvertent patient burn. This may result of careless handling of the device or in the case of, monopolar devices forgetting to apply a return electrode plate, In this situation patients may, develop a contact burn when electricity flows to earth, Explosion or fire. This may occur when volatile anaesthetic gases or skin preparation fluid, have been used, Next question
Page 2464 :
If a 2 x 2 cm autologus skin graft is placed on an area of healthy granulation tissue. After about a, week, a thin bluish - white margin appears around the graft and spreads at a rate of 1mm per day., What is it?, , Epidermis alone, , Epidermis and dermis, , Dermis alone, , Inflammatory exudate, , Fibrin, , This is the process of re-epithelialisation., Please rate this question:, , Discuss and give feedback, , Next question, , Wound healing, Surgical wounds are either incisional or excisional and either clean, clean contaminated or dirty., Although the stages of wound healing are broadly similar their contributions will vary according to the, wound type., The main stages of wound healing include:, Haemostasis, , , , , Minutes to hours following injury, Vasospasm in adjacent vessels, platelet plug formation and generation of fibrin rich clot.
Page 2465 :
Inflammation, , , , , , , , Typically days 1-5, Neutrophils migrate into wound (function impaired in diabetes)., Growth factors released, including basic fibroblast growth factor and vascular endothelial, growth factor., Fibroblasts replicate within the adjacent matrix and migrate into wound., Macrophages and fibroblasts couple matrix regeneration and clot substitution., , Regeneration, , , , , , , Typically days 7 to 56, Platelet derived growth factor and transformation growth factors stimulate fibroblasts and, epithelial cells., Fibroblasts produce a collagen network., Angiogenesis occurs and wound resembles granulation tissue., , Remodeling, , , , , , , , From 6 weeks to 1 year, Longest phase of the healing process and may last up to one year (or longer)., During this phase fibroblasts become differentiated (myofibroblasts) and these facilitate, wound contraction., Collagen fibres are remodeled., Microvessels regress leaving a pale scar., , The above description represents an idealised scenario. A number of diseases may distort this, process. Neovascularisation is an important early process. Endothelial cells may proliferate in the, wound bed and recanalise to form a vessel. Vascular disease, shock and sepsis can all compromise, microvascular flow and impair healing., Conditions such as jaundice will impair fibroblast synthetic function and immunity with a detrimental, effect in most parts of the healing process., Problems with scars:, Hypertrophic scars, Excessive amounts of collagen within a scar. Nodules may be present histologically containing, randomly arranged fibrils within and parallel fibres on the surface. The tissue itself is confined to the, extent of the wound itself and is usually the result of a full thickness dermal injury. They may go on, to develop contractures.
Page 2466 :
Image of hypertrophic scarring. Note that it remains confined to the boundaries of the original, wound:, , Image sourced from Wikipedia, , Keloid scars, Excessive amounts of collagen within a scar. Typically a keloid scar will pass beyond the boundaries, of the original injury. They do not contain nodules and may occur following even trivial injury. They, do not regress over time and may recur following removal., Image of a keloid scar. Note the extension beyond the boundaries of the original incision:
Page 2467 :
Image sourced from Wikipedia, , Drugs which impair wound healing:, , , , , , , Non steroidal anti inflammatory drugs, Steroids, Immunosupressive agents, Anti neoplastic drugs, , Closure, Delayed primary closure is the anatomically precise closure that is delayed for a few days but before, granulation tissue becomes macroscopically evident., Secondary closure refers to either spontaneous closure or to surgical closure after granulation tissue, has formed., Next question
Page 2468 :
Which of the following methods is most effective at destroying spores of the tubercle bacilli?, , Immersion in 0.5% chlorhexidine in alcohol, , Immersion in aqueous iodine, , Heating in a hot air oven, , Immersion in 0.1% sodium hypochlorite, , Autoclaving, , The tubercle bacilli has a waxy outer membrane that renders it more resistant to sterilisation and, cleaning methods. Whilst 0.1% sodium hypochlorite will destroy many microbes it is less reliable in, destroying tubercle bacilli. Hot air ovens provide less reliable pathogen destruction than autoclaving,, but may be indicated in situations where the equipment is sensitive to the autoclaving process. From, the list of options above, autoclaving will most reliably destroy tubercle bacilli., Please rate this question:, , Discuss and give feedback, , Next question, , Sterilisation, Surgical equipment has to be cleaned and sterilised prior to use. The extent to which these, processes will be required varies according to the type of equipment and the purpose for which it will, be used. In general, the three processes are relevant; cleaning, disinfection and sterilisation., , , , , , Cleaning refers to removal of physical debris., Disinfection refers to reduction in numbers of viable organisms., Sterilisation is removal of all organisms and spores.
Page 2469 :
Methods, , Method, , Details, , Indication, , Autoclaving, , Air removed and high pressure, steam used (usually 134 oC for, 3 minutes), , Most reusable surgical equipment, must be, physically cleaned prior to autoclaving, unsuitable, for fragile items, , Glutaraldehyde, solution (2%), , Colourless oily liquid, directly, cytocidal and virucidal even at, low temperatures, , Specifically used for endoscopes and some, laparoscopic items, staff can rapidly develop, allergy to this substance which has limited its more, widespread use, , Ethylene oxide, , 3% mixture of gas with carbon, dioxide used, , Used for packaged materials that cannot be, heated, the gas is explosive and environmentally, toxic, it is used mainly in the industrial setting, , Gamma irradiation, , Gamma rays emitted from, radioactive substance such as, cobalt 60 or caesium 137, , Suitable for batch treatment of relatively, thermostable items, typically an industrial process, , Next question
Page 2470 :
Which of the following is a permanent suture material best suited for interrupted mattress dermal, closure?, , 2/0 Polydiaxone, , 3/0 Polydiaxone, , 4/0 Polyglycolic acid, , 1/0 Dexon, , 3/0 Polypropylene, , Of the sutures listed only prolene is a permanent suture material. It is a good agent for skin closure, as it does not incite an inflammatory response and thus provides good cosmesis., Please rate this question:, , Discuss and give feedback, , Next question, , Suture material, Suture materials, , Agent, , Classification, , Durability, , Uses, , Special points, , Silk, , Braided, Biological, , Theoretically, permanent, although, strength not, , Anchoring devices, skin, closure, , Knots easily, poor, cosmesis
Page 2471 :
Agent, , Classification, , Durability, , Uses, , Special points, , preserved, , Catgut, , Braided, Biological, , 5-7 days, , Short term wound, approximation, , Poor cosmesis, Degrades rapidly, Not available in UK, , Chromic catgut, , Braided, Biological, , Up to 12 weeks, , Apposition of deeply, sited tissues, , Unpredictable, degradation pattern, Not in use in UK, , Polydiaxonone, (PDS), , Synthetic, Monofilament, , Up to 3 months, (longer with, thicker sutures), , Widespread surgical, applications including, visceral anastomoses,, dermal closure, mass, closure of abdominal, wall, , Used in most surgical, specialties (avoid dyed, form in dermal, closure), , Polyglycolic acid, (Vicryl, Dexon), , Braided, Synthetic, , Up to 6 weeks, , Most tissues can be, apposed using, polyglycolic acid, , It has good handling, properties, the dyed, form of this suture, should not be used for, skin closure, , Polypropylene, (Prolene), , Synthetic, Monofilament, , Permanent, , Widely used, agent of, choice for vascular, anastomoses, , Poor handling, properties, , Polyester, (Ethibond), , Synthetic, Braided, , Permanent, , Its combination of, permanency and, braiding makes it useful, for laparoscopic surgery, , It is more expensive, and has considerable, tissue drag
Page 2472 :
Absorbable vs Non absorbable, , , , , , Time taken to degrade absorbable materials varies, Usually by macrophages hydrolysing material, Consider absorbable sutures in situations where long term tissue apposition is not required., In cardiac and vascular surgery non absorbable sutures are usually used., , Suture size, , , , , The higher the index number the smaller the suture i.e. : 6/0 prolene is finer than 1/0 prolene., Finer sutures have less tensile strength. For example 6/0 prolene would not be a suture, suitable for abdominal mass closure but would be ideal for small calibre distal arterial, anastomoses., , Braided vs monofilament, Generally speaking braided sutures have better handling characteristics than non braided. However,, they are associated with higher bacterial counts. Braided materials are unsuitable for use in vascular, surgery as they are potentially thrombogenic., Next question
Page 2473 :
Theme: Suture materials, , A. Silk 3/0, B. Polyglactin 3/0, C. Polydiaxone 1/0, D. Stainless steel skin clips, E. Stainless steel wire 1/0, F. 6/0 Polypropylene, G. 1/0 Undyed polyglactin, H. Polypropylene 3/0, , Please select the most appropriate suture for the scenario given. Each option may be used once,, more than once or not at all., , 28., , Anastomosis of ileum to transverse colon following right hemicolectomy., You answered Silk 3/0, The correct answer is Polyglactin 3/0, 3/0 PDS would be an alternative, as would linear stapler but those are not in the list., , 29., , Distal anastomosis in a femorodistal bypass using vein., You answered Silk 3/0, The correct answer is 6/0 Polypropylene, Arterial anastomoses should be constructed using polypropylene. In this case a fine suture, material such as 6/0 is indicated.
Page 2474 :
30., , Closure of skin following thyroidectomy for Graves disease., You answered Silk 3/0, The correct answer is Stainless steel skin clips, Although some use sub cuticular stitches skin clips remain the standard of many. In the event of, post operative haematoma causing respiratory obstruction, they are easier to remove., , Please rate this question:, , Discuss and give feedback, , Next question, , Suture material, Suture materials, , Agent, , Classification, , Durability, , Uses, , Special points, , Silk, , Braided, Biological, , Theoretically, permanent, although, strength not, preserved, , Anchoring devices, skin, closure, , Knots easily, poor, cosmesis, , Catgut, , Braided, Biological, , 5-7 days, , Short term wound, approximation, , Poor cosmesis, Degrades rapidly, Not available in UK, , Chromic catgut, , Braided, , Up to 12 weeks, , Apposition of deeply, , Unpredictable, degradation pattern
Page 2475 :
Agent, , Classification, , Durability, , Biological, , Uses, , Special points, , sited tissues, , Not in use in UK, , Polydiaxonone, (PDS), , Synthetic, Monofilament, , Up to 3 months, (longer with, thicker sutures), , Widespread surgical, applications including, visceral anastomoses,, dermal closure, mass, closure of abdominal, wall, , Used in most surgical, specialties (avoid dyed, form in dermal, closure), , Polyglycolic acid, (Vicryl, Dexon), , Braided, Synthetic, , Up to 6 weeks, , Most tissues can be, apposed using, polyglycolic acid, , It has good handling, properties, the dyed, form of this suture, should not be used for, skin closure, , Polypropylene, (Prolene), , Synthetic, Monofilament, , Permanent, , Widely used, agent of, choice for vascular, anastomoses, , Poor handling, properties, , Polyester, (Ethibond), , Synthetic, Braided, , Permanent, , Its combination of, permanency and, braiding makes it useful, for laparoscopic surgery, , It is more expensive, and has considerable, tissue drag, , Absorbable vs Non absorbable, , , , , , Time taken to degrade absorbable materials varies, Usually by macrophages hydrolysing material, Consider absorbable sutures in situations where long term tissue apposition is not required., In cardiac and vascular surgery non absorbable sutures are usually used., , Suture size
Page 2476 :
, , , The higher the index number the smaller the suture i.e. : 6/0 prolene is finer than 1/0 prolene., Finer sutures have less tensile strength. For example 6/0 prolene would not be a suture, suitable for abdominal mass closure but would be ideal for small calibre distal arterial, anastomoses., , Braided vs monofilament, Generally speaking braided sutures have better handling characteristics than non braided. However,, they are associated with higher bacterial counts. Braided materials are unsuitable for use in vascular, surgery as they are potentially thrombogenic., Next question
Page 2477 :
Theme: Management of skin lesions, , A., B., C., D., E., F., , 5mm punch biopsy, Shave biopsy, Excisional biopsy, Wide excision of 5cm, Tru cut biopsy, Incisional biopsy, , For the skin lesions described please select the most appropriate management option. Each option, may be used once, more than once or not at all., , 31., , An 83 year old lady presents with multiple patches of pigmented irregular, superficial, lesions over the torso. They do not bleed but have become increasingly itchy., You answered 5mm punch biopsy, The correct answer is Shave biopsy, Theme from April 2012 Exam, This is most likely to be seborrhoeic warts. These are usually superficially sited and are, best managed with shave biopsy and cautery., , 32., , A 65 year old man presents with a 5cm ulcerated area over his medial malleolus., 5mm punch biopsy, This is likely to be a venous ulcer and should usually be managed with compression, bandaging if there is no arterial compromise. Long standing lesions may be complicated, by the development of malignancy and for this reason a punch biopsy of long standing or, non healing lesions is advisable., , 33., , A 23 year old lady presents with an itchy, bleeding pigmented lesion on her right thigh., You answered 5mm punch biopsy, The correct answer is Excisional biopsy, This may represent a malignant melanoma. Complete excision is required to allow, accurate histological assessment. If the diagnosis is confirmed then re-excision of margins, may be required. Clearly if the lesion is benign then no further action is required., , Please rate this question:
Page 2478 :
Discuss and give feedback, , Next question, , Treatment of suspicious skin lesions, Skin lesions may be referred to surgeons for treatment or discovered incidentally. The table below, outlines the various therapeutic options:, , Method, , Indication, , Tru-cut, biopsy, , Most often used for percutaneous sampling of deep seated lesions or used intra, operatively for visceral lesions, , 5mm punch, biopsy, , Used for diagnostic confirmation of lesions that are suspected to be benign or, where the definitive management is unlikely to be surgical. Of limited usefulness in, pigmented lesions where they do not include sufficient tissue for accurate, diagnosis. May be used in non melanoma type skin disease to establish diagnosis, prior to more extensive resection., , Wide, excision, , Where the complete excision of the lesion (with healthy margins) is the main, objective. In cosmetically sensitive sites, or where the defect is large, this may need, to be complemented with plastic surgical techniques, , Incisional, biopsy, , Used mainly for deep seated or extensive lesions where there is diagnostic doubt, (usually following core or tru-cut biopsy). Used rarely for skin lesions., , Diagnostic, excision, , Primarily used for lesions that are suspicious for melanoma, the lesion is excised, with a rim of normal tissue. Excision of margins may be required subsequently., Next question
Page 2479 :
Theme: Tissue sampling, , A., B., C., D., E., F., G., , Fine needle aspiration cytology, Surgical excision biopsy, Smear cytology, Core cut biopsy, Conventional surgical excision, Tru cut biopsy, Punch biopsy, , Please select the most appropriate sampling method for the situation given. Each option may be, used once, more than once or not at all., , 34., , A 45 year old patient undergoes a CT scan of the abdomen and is noted to have a 6cm, mass in the right adrenal gland. Urinary catecholamines and other endocrine investigations, are negative. CT of the chest and remainder of the abdomen is otherwise normal., You answered Fine needle aspiration cytology, The correct answer is Conventional surgical excision, Most surgeons would excise a mass of this size rather than attempt biopsy. Further, information relating to adrenal masses is covered under this topic., , 35., , A 67 year old lady is suspected of having Pagets disease of the nipple., You answered Fine needle aspiration cytology, The correct answer is Punch biopsy, This is a relatively clear indication for a punch biopsy. If cellular atypia is present on, punch biopsy then any in situ malignancy should be considered. FNAC would be, unsuitable., , 36., , A 23 year old lady presents with a nodule in the right lobe of the thyroid. Examination of, the neck is otherwise unremarkable and clinically she is euthyroid. Imaging shows a solid, nodule at the site., Fine needle aspiration cytology, FNAC is the first line investigation in this setting.Where as FNAC has declined in, popularity recently, it remain a very popular option in the investigation of thyroid masses., It cannot reliably diagnose a follicular tumour.
Page 2480 :
Please rate this question:, , Discuss and give feedback, , Next question, , Tissue sampling, Tissue sampling is an important surgical process. Biopsy modalities vary according to the site,, experience and subsequent planned therapeutic outcome, The modalities comprise:, -Fine needle aspiration cytology, -Core biopsy, -Excision biopsy, -Tru cut biopsy, -Punch biopsy, -Cytological smears, -Endoscopic or laparoscopic biopsy, When the lesion is superficial the decision needs to be taken as to whether complete excision is, desirable or whether excision biopsy is acceptable. In malignant melanoma for example the need for, safe margins will mean that a more radical surgical approach needs to be adopted after diagnostic, confirmation from excision biopsy than would be the case in basal cell carcinoma. Punch biopsies, are useful in gaining histological diagnosis of unclear skin lesions where excision biopsy is, undesirable such as in establishing whether a skin lesion is vasculitic or not., Fine needle aspiration cytology (FNAC) is an operator dependent procedure that may or may not be, image guided and essentially involves passing a needle through a lesion whilst suction is applied to, a syringe. The material thus obtained is expressed onto a slide and sent for cytological assessment., This test can be limited by operator inexperience and also by the lack of histological architectural, information (e.g. Follicular carcinoma of the thyroid). Where a discharge is present a sample may be, sent for cytology although in some sites (e.g. Nipple discharge ) the information gleaned may be, meaningless., Tissue samples may be obtained by both core and tru cut biopsy. A core biopsy is obtained by use, of a spring loaded gun with a needle passing quickly through the lesion of interest. A tru cut biopsy, achieves the same objective but the needle moved by hand. When performing these techniques, image guidance may be desirable (e.g. In breast lesions). Consideration needs to be given to any, planned surgical resection as it may be necessary to resect the biopsy tract along with the specimen, (e.g. In sarcoma surgery)., Visceral lesions may be accessed percutaneously under image guidance such as ultrasound guided, biopsy of liver metastases. Or under direct vision such as a colonoscopic biopsy., Next question
Page 2481 :
Theme: Management of wounds, , A. Split thickness skin graft, B. Full thickness skin graft, C. Insertion of tissue expander at donor site and delayed split thickness skin, graft, D. Myocutaneous flap reconstruction (pedicled), E. Direct primary closure, F. Delayed primary closure, , Please select the most appropriate management for the wound described. Each option may be used, once, more than once or not at all., , 37., , A 34 year old man has a tissue defect measuring 3 cm by 1 cm following an excision of a lipoma, from the scapula., You answered Split thickness skin graft, The correct answer is Direct primary closure, This wound should be amenable to primary closure. There is minimal associated tissue loss and, the surgery is minor and uncontaminated., , 38., , A 72 year old lady has a 4cm basal cell carcinoma excised from her right cheek. There is a, rhomboid defect measuring 4cm by 4cm., You answered Split thickness skin graft, The correct answer is Full thickness skin graft, Facial wounds that are large and irregularly shaped are best managed with full thickness skin, grafts.
Page 2482 :
39., , A 5 year old suffers 20% burns to the torso. On examination there is fixed pigmentation and the, affected area has a white and dry appearance., Split thickness skin graft, This is a full thickness burn and will require split thickness skin grafting. Meshing the graft may, increase the donor site yield. However, this is at the expense of cosmesis.The burn itself must be, debrided first to ensure an adequate wound bed., , Please rate this question:, , Discuss and give feedback, , Next question, , Tissue reconstruction, Skin Grafts and Flaps, Skin flaps or grafts may be required where primary wound closure cannot be achieved or would, entail either significant cosmetic defect or considerable functional disturbance as a result of wound, contraction., Reconstructive ladder, , Method, , Types, , Direct closure, , The simplest option where possible, , Grafting techniques, , Flap technique, , , , , , , Local:, , Split thickness, Full thickness, Skin Substitute, Composite
Page 2483 :
Method, , Types, , , , , , Transposition, Pivot, Alphabetplasty (e.g. Z-Y), , Regional:, , , , , , Myocutaneous, Fasciocutaneous, Neurocutaneous, , Distant:, , , , Free tissue transfer, , Prelamination, techniques, , Allows creation of specialised flaps e.g. buccal mucosa, , Tissue expansion, , Involves placement of tissue expanders to increase amount of tissue at donor, sites, , Skin Grafts Vs. Flaps, , Skin Grafts, , Flaps, , No size limit (Split)/ Relative size limit (full thickness), , Size limited by territory of blood supply, , Rely on wound bed for blood supply, , Tissue has its own blood supply, , Take better on clean well vascularised wound beds, , Will survive independent of the wound bed
Page 2484 :
Skin Grafts, , Flaps, , Split skin graft donor site typically heals in 12 days, , Direct closure of donor site or secondary skin graft, , Donor site may be reused, , Donor site cannot be reused, , Split thickness skin grafts, , , , , , , Available in range of thicknesses., Thigh is the commonest donor site, Size may be increased by meshing the graft. However this comes with compromise on, cosmesis., Donor sites, especially if thin grafts are taken can be reused following re-epithelialisation, , Full thickness grafts, , , , , , Most commonly used for facial reconstruction, Include dermal appendages, Provide superior cosmetic result, , Composite grafts, These are grafts containing more than one tissue type, such as skin and fat. They are usually used, to cover small defects in cosmetically important areas., Flaps, , , , , , , Flaps have their own blood supply and may be pedicled or free., May have multiple components e.g. skin, skin + fat, skin + fat + muscle., They will have the ability to take regardless of the underlying tissue bed., The type of intrinsic blood supply is important. For example in breast surgery pedicled, latissimus dorsi flaps will be less prone to failure than microsvascular anastomosed free Diep, flaps., Next question
Page 2485 :
You have just completed a laparotomy for peritonitis due to a perforated peptic ulcer. What is the, best surgical strategy for avoidance of a complete abdominal wound dehisence?, , Use of skin clips to close the skin rather than sub cuticular sutures, , Careful approximation of the peritonum with non absorbable sutures, , Mass closure of the midline wound using a 1/0 polydiaxone suture, , Direct apposition of the rectus muscle rather than linea alba aponeurosis, , Mass closure of the midline wound using a 3/0 polypropylene suture, , The incidence of post operative wound dehisence is minimise by following Jenkins rule which, advocates mass closure of the midline wound. However, the suture strength is an important, consideration and 3/0 sutures do not have sufficient tensile strength. Both polydiaxone (PDS) and, polypropylene (Prolene) or nylon (Ethilon) are all equally suitable. Although separate closure of the, peritoneum was practised it has no bearing on the incidence of abdominal wound dehisence., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal wound dehiscence, , , , This is a significant problem facing all surgeons who undertake abdominal surgery on a, regular basis. Traditionally, it is said to occur when all layers of an abdominal mass closure, fail and the viscera protrude externally (associated with 30% mortality)., It can be subdivided into superficial, in which the skin wound alone fails and complete,, implying failure of all layers., , Factors which increase the risk are:, * Malnutrition
Page 2486 :
* Vitamin deficiencies, * Jaundice, * Steroid use, * Major wound contamination (e.g. faecal peritonitis), * Poor surgical technique (Mass closure technique is the preferred method-Jenkins Rule), When sudden full dehiscence occurs the management is as follows:, * Analgesia, * Intravenous fluids, * Intravenous broad spectrum antibiotics, * Coverage of the wound with saline impregnated gauze (on the ward), * Arrangements made for a return to theatre, Surgical strategy, , , , , Correct the underlying cause (e.g. TPN or NG feed if malnourished), Determine the most appropriate strategy for managing the wound, , Options, , Resuturing of the, wound, , This may be an option if the wound edges are healthy and there is enough tissue for, sufficient coverage. Deep tension sutures are traditionally used for this purpose., , Application of a, wound manager, , This is a clear dressing with removable front. Particularly suitable when some, granulation tissue is present over the viscera or where there is a high output bowel, fistula present in the dehisced wound., , Application of a, 'Bogota bag', , This is a clear plastic bag that is cut and sutured to the wound edges and is only a, temporary measure to be adopted when the wound cannot be closed and will, necessitate a return to theatre for definitive management., , Application of a, VAC dressing, system, , These can be safely used BUT ONLY if the correct layer is interposed between the, suction device and the bowel. Failure to adhere to this absolute rule will almost, invariably result in the development of multiple bowel fistulae and create an, extremely difficult management problem., Next question
Page 2487 :
Theme: Instrument cleaning, , A. Immersion in glutaraldehyde, B. Gamma irradiation, C. Autoclaving, D. Ethylene chloride, E. Phenolic lavage, F. Disposal of instrument, , Please select the most appropriate cleaning method of instrument for the situation described. Each, option may be used once, more than once or not at all., , 41., , A company manufacturing scalpel blades wishes to sterilise them in bulk before use., You answered Immersion in glutaraldehyde, The correct answer is Gamma irradiation, Theme from September 2013 Exam, Industry often uses gamma irradiation. It is not routinely used in hospitals, , 42., , For sterilisation and cleaning of a colonoscope., Immersion in glutaraldehyde, Washing systems using glutaraldehyde are often used although development of sensitivity in staff, is well known and it is used in closed systems, , 43., , For cleaning instruments following a tonsillectomy in a patient who recieved human growth, hormone extract in 1981, You answered Immersion in glutaraldehyde
Page 2488 :
The correct answer is Disposal of instrument, High risk of prion disease mandates disposal on instruments which is often undertaken following, all tonsillectomy procedures regardless of level of percieved risk, , Please rate this question:, , Discuss and give feedback, , Next question, , Sterilisation, Surgical equipment has to be cleaned and sterilised prior to use. The extent to which these, processes will be required varies according to the type of equipment and the purpose for which it will, be used. In general, the three processes are relevant; cleaning, disinfection and sterilisation., , , , , , Cleaning refers to removal of physical debris., Disinfection refers to reduction in numbers of viable organisms., Sterilisation is removal of all organisms and spores., , Methods, , Method, , Details, , Indication, , Autoclaving, , Air removed and high pressure, steam used (usually 134 oC for, 3 minutes), , Most reusable surgical equipment, must be, physically cleaned prior to autoclaving, unsuitable, for fragile items, , Glutaraldehyde, solution (2%), , Colourless oily liquid, directly, cytocidal and virucidal even at, low temperatures, , Specifically used for endoscopes and some, laparoscopic items, staff can rapidly develop, allergy to this substance which has limited its more, widespread use
Page 2489 :
Method, , Details, , Indication, , Ethylene oxide, , 3% mixture of gas with carbon, dioxide used, , Used for packaged materials that cannot be, heated, the gas is explosive and environmentally, toxic, it is used mainly in the industrial setting, , Gamma irradiation, , Gamma rays emitted from, radioactive substance such as, cobalt 60 or caesium 137, , Suitable for batch treatment of relatively, thermostable items, typically an industrial process, , Next question
Page 2490 :
Which of the following is not an absorbable suture material?, , Chromic catgut, , Nylon, , Vicryl, , Dexon, , Poly diaxone (PDS)., , Please rate this question:, , Discuss and give feedback, , Next question, , Suture material, Suture materials, , Agent, , Classification, , Durability, , Uses, , Special points, , Silk, , Braided, Biological, , Theoretically, permanent, although, strength not, preserved, , Anchoring devices, skin, closure, , Knots easily, poor, cosmesis
Page 2491 :
Agent, , Classification, , Durability, , Uses, , Special points, , Catgut, , Braided, Biological, , 5-7 days, , Short term wound, approximation, , Poor cosmesis, Degrades rapidly, Not available in UK, , Chromic catgut, , Braided, Biological, , Up to 12 weeks, , Apposition of deeply, sited tissues, , Unpredictable, degradation pattern, Not in use in UK, , Polydiaxonone, (PDS), , Synthetic, Monofilament, , Up to 3 months, (longer with, thicker sutures), , Widespread surgical, applications including, visceral anastomoses,, dermal closure, mass, closure of abdominal, wall, , Used in most surgical, specialties (avoid dyed, form in dermal, closure), , Polyglycolic acid, (Vicryl, Dexon), , Braided, Synthetic, , Up to 6 weeks, , Most tissues can be, apposed using, polyglycolic acid, , It has good handling, properties, the dyed, form of this suture, should not be used for, skin closure, , Polypropylene, (Prolene), , Synthetic, Monofilament, , Permanent, , Widely used, agent of, choice for vascular, anastomoses, , Poor handling, properties, , Polyester, (Ethibond), , Synthetic, Braided, , Permanent, , Its combination of, permanency and, braiding makes it useful, for laparoscopic surgery, , It is more expensive, and has considerable, tissue drag, , Absorbable vs Non absorbable
Page 2492 :
, , , , Time taken to degrade absorbable materials varies, Usually by macrophages hydrolysing material, Consider absorbable sutures in situations where long term tissue apposition is not required., In cardiac and vascular surgery non absorbable sutures are usually used., , Suture size, , , , , The higher the index number the smaller the suture i.e. : 6/0 prolene is finer than 1/0 prolene., Finer sutures have less tensile strength. For example 6/0 prolene would not be a suture, suitable for abdominal mass closure but would be ideal for small calibre distal arterial, anastomoses., , Braided vs monofilament, Generally speaking braided sutures have better handling characteristics than non braided. However,, they are associated with higher bacterial counts. Braided materials are unsuitable for use in vascular, surgery as they are potentially thrombogenic., Next question
Page 2493 :
A 73 year old lady sustains a distal radius fracture and this is manipulated using a Biers block with, prilocaine as the local anaesthetic agent. During the procedure the occlusion cuff deflates and the, patient becomes progressively cyanosed. What is the treatment of choice?, , Intravenous calcium gluconate, , Exchange transfusion, , Intravenous methylene blue, , Intravenous sodium thiosulphate, , Intravenous gelofusine, , Prilocaine is a recognised cause of methaemoglobinaemia, this is characterised by the development, of cyanosis and dyspnoea. This disorder occurs because of the change haemoglobin to a ferric, subtype rather than ferrous (Fe2+). This type of change shifts the oxygen dissociation curve to the left, and tissue hypoxia occurs. Methylene blue will revert the haemoglobin to the ferrous type and, reverse this effect., Please rate this question:, , Discuss and give feedback, , Next question, , Local anaesthetic toxicity, Toxicity results from either accidental intravascular injection (rapid onset of symptoms-usually, correct dose), or from excessive dosage (slower onset). Local anaesthetic agents not only exert a, membrane stabilising effect on peripheral nerves but will also act on excitable membranes within the, CNS and Heart. The sensory neurones in the CNS are suppressed before the motor ones. As a, result the early symptoms will typically be those of circumoral paraesthesia and tinnitus, followed by, falling GCS and eventually coma.
Page 2494 :
Management of toxicity, , , , , , , , , Stop injecting the anaesthetic agent, High flow 100% oxygen via face mask, Cardiovascular monitoring, Administer lipid emulsion (Intralipid 20%) at 1.5ml/Kg over 1 minute as a bolus, Consider lipid emulsion infusion, at 0.25ml/ Kg/ minute, If toxicity due to prilocaine then administer methylene blue, , Safe doses, 10ml of lignocaine 1% contains 100mg of drug, this would constitute 70% of the maximum safe dose, in a 50 kg patient. Up to 7mg / kg can be administered if adrenaline is added to the solution., Doses of local anaesthetics, , Agent, , Dose plain, , Dose with adrenaline, , Lignocaine, , 3mg/Kg, , 7mg/Kg, , Bupivicane, , 2mg/Kg, , 2mg/Kg, , Prilocaine, , 6mg/Kg, , 9mg/Kg, , These are a guide only as actual doses depend on site of administration, tissue vascularity and comorbidities., Next question
Page 2495 :
A 43 year old man has symptoms of carcinoid syndrome. Which of the following is the most effective, therapeutic agent in controlling the symptoms?, , Atenolol, , Octreotide, , Glucagon, , Somatostatin, , Spironolactone, , Theme from April 2012 Exam, Octreotide is the usual treatment for carcinoid syndrome. Somatostatin inhibits the release of a, number of gut hormones. Octreotide is the synthetic alternative to somatostatin and thus the most, appropriate therapeutic agent., Please rate this question:, , Discuss and give feedback, , Next question, , Carcinoid syndrome, , , , , , Carcinoid tumours secrete serotonin, Originate in neuroendocrine cells mainly in the intestine (midgut-distal ileum/appendix), Can occur in the rectum, bronchi, Hormonal symptoms mainly occur when disease spreads outside the bowel, , Clinical features
Page 2496 :
, , , , , , , Onset: insidious over many years, Flushing face, Palpitations, Pulmonary valve stenosis and tricuspid regurgitation causing dyspnoea, Asthma, Severe diarrhoea (secretory, persists despite fasting), , Investigation, , , , , , , 5-HIAA in a 24-hour urine collection, Somatostatin receptor scintigraphy, CT scan, Blood testing for chromogranin A, , Treatment, , , , , Octreotide, Surgical removal, Next question
Page 2497 :
A 43 year old lady is due to undergo a diagnostic laparoscopy. Which of the agents listed below, should be used for inducing pneumoperitoneum?, , Argon, , Helium, , Air, , Carbon dioxide, , Nitrogen, , Carbon dioxide is the agent of choice. It is rapidly re-absorbed, does not support combustion and is, cheap. It is rapidly cleared from the lungs and so effects on pH are unusual., Please rate this question:, , Discuss and give feedback, , Next question, , Gases for laparoscopic surgery, Laparoscopic surgery may be performed in a number of body cavities. In some areas irrigation, solutions are preferred. In the abdomen insufflation with carbon dioxide gas is commonly used. The, amount of gas delivered is adjusted to maintain a constant intra-abdominal pressure of between 12, and 15 mmHg. Excessive intra-abdominal pressure may reduce venous return and lead to, hypotension. Too little insufflation will risk obscuring the surgical view., Next question
Page 2498 :
Theme: Levels of evidence, , A., B., C., D., E., , I, II, III, IV, V, , Please select the level of evidence which is supplied by the following. Each option may be used, once, more than once or not at all., , 48., , One of the senior surgeons in the hospital advises as to the best management of Merkel, cell tumours of the skin in which she has a special interest., You answered I, The correct answer is V, Personal expert opinion qualifies for level V evidence., , 49., , A group of surgeons review a meta-analysis of a series of randomised controlled trials on, the Cochrane database and decide that one type of hip replacement is superior to another., I, A meta- analysis of more than one well designed trials will typically represent level I, evidence. It does, of course, depend on how well the trials were conducted and reported., , 50., , A group of surgeons are trying to decide which type of mesh to use for incisional hernia, repair. Their assimilated evidence includes two case series and one randomised controlled, trial., You answered I, The correct answer is II, Data which includes at least one RCT will usually qualify for level II evidence., , Please rate this question:, , Discuss and give feedback, , Next question
Page 2499 :
Levels of evidence, The level of evidence refers to the study design used by investigators to minimise bias., , Level of, evidence, , Source, , I, , Evidence obtained from systematic review of all relevant randomised controlled, trials, , II, , Evidence derived from at least one properly designed randomised controlled trial, , III, , Evidence derived from well designed pseudo-randomised controlled trials (e.g., alternate allocation) or historical controls, , IV, , Evidence derived from case series or case reports, , V, , Panel or expert opinion, , Many of the categories contain sub groups, detailed knowledge of these are not required for MRCS, Part A., References, Interested users will find further information at www.cebm.net, Next question
Page 2500 :
A surgeon wishes to determine whether different methods of perioperative shaving have an effect on, post operative wound infection rates. Which of the following is the best method for assessing, whether one method is better than the other?, , Cohort study, , Retrospective study, , Case controlled study, , Cross over study, , Randomised controlled study, , A randomised controlled study is the best method for assessing this relationship. It is important to, analyse data from RCT's on an intention to treat basis., Please rate this question:, , Discuss and give feedback, , Next question, , Randomised controlled trials, Randomised controlled trials are an established method of comparing two variables. These may, consist of comparison of treatments or treatment versus placebo. Ideally the trials should be blinded,, usually to the patient and those treating them., In most cases a power calculation should be performed to determine the sample size required to, detect a difference., Next question
Page 2501 :
Theme: Electrosurgery, , A. Cutting current, B. Coagulation current, C. Blended current, D. Fulguration, E. Desiccation, , For each of the following electrosurgical applications please select the most likely modality used., Each option may be used once, more than once or not at all., , 52., , In this modality the active electrode is placed in direct contact with the tissue and is characterised, by low current and high voltage over a broad area., You answered Cutting current, The correct answer is Desiccation, In desiccation the device is placed in direct contact with the tissues (unlike fulguration). Because it, is applied over a broad area it tends not to cause protein damage (unlike coagulation)., , 53., , An electrosurgical mode whereby the electrode is held away from the tissue. The current utilises, a low amplitude and high voltage., You answered Cutting current, The correct answer is Fulguration, Fulguration typically avoids contact between the electrode and the tissue with the current, configured to favor arc formation., , 54., , A modality in which a sinusoidal, non modulated waveform is produced and vaporises the tissues.
Page 2502 :
Cutting current, The high energy levels result in tissue vaporisation and cleavage of tissues., , Please rate this question:, , Discuss and give feedback, , Next question, , Electrosurgery, Electrosurgery utilises the heat generated by the passage of high frequency alternating electrical, current through living tissues. The application of a voltage across human tissue results in the, formation of an electrical circuit between the voltage source and the tissue. The tissue acts as a, resistor and the level of resistance is determined by the water content of the tissue. It is this, resistance that results in the formation of heat., An alternating current constantly changes the direction in which the current flows, the speed with, which this occurs is measured in Hertz. Most diathermy units operate at a frequency of between, 200,000 kHZ to 5MHz. This means that tissue such as nerves and muscles will not depolarise (since, this seldom occurs at frequencies above 10,000Hz). The current waveform can be adjusted to, deliver three main therapeutic modalities; cutting, coagulation and blend., Types of current, , Cutting, , , , , , Sinusoidal and non modulated waveform, High average power and current density, Precise cutting without thermal damage, , Coagulation, , , , , , Modulated current with intermittent dampened sine waves of high peak voltage, Evaporation, rather than vaporisation of intracellular fluid occurs, Results in formation of coagulum, , Desication, , , , , Active electrode in direct contact with tissue, Low current and high voltage system
Page 2503 :
, , Results in loss of cellular water but no protein damage, , Fulguration, , , , , , Electrode probe is held away from tissue, Produces spray effect with local, superficial tissue destruction, Low amplitude and high voltage system, , Blend, , , , , Alternating cutting and coagulation modes, Total average power is less than with cutting, Next question
Page 2504 :
Theme: Surgical site infections, , A. Glutaraldehyde 2% applied to the skin, B. Sodium hypochlorite solution applied to the skin, C. Aqueous iodine applied to the skin, D. Perform surgery in a lamninar flow theatre, E. Surgeon to wear exhaust suit, F. Administration of clindamycin, G. Administration of gentamicin, H. Pre operative shaving, , Please select the most appropriate modality to reduce the risk of developing a surgical site infection, for the scenario given. Each option may be used once, more than once or not at all., , 55., , A 42 year old man is due to undergo a Mayo repair of a paraumbilical hernia. He is otherwise, well., You answered Glutaraldehyde 2% applied to the skin, The correct answer is Aqueous iodine applied to the skin, The patient will require skin preparation. However, use of glutaraldehyde or sodium hypochlorite, would be an inappropriate choice. As the Mayo repair does not involve implantation of prosthetic, mesh the use of antibiotics is not appropriate., , 56., , A 63 year old man with end stage oestoarthritis of the hip is due to undergo a total hip, replacement. The skin has been prepared and antibiotics given., You answered Glutaraldehyde 2% applied to the skin, The correct answer is Perform surgery in a lamninar flow theatre
Page 2505 :
Laminar flow is more important than an exhaust suit although use of both is ideal., , 57., , A 22 year old man is undergoing an appendicectomy. At operation there is copious pus around, the appendix., You answered Glutaraldehyde 2% applied to the skin, The correct answer is Administration of gentamicin, Gentamicin is the preferred agent. Clindamycin is associated with high rate of clostridium dificile, infection., , Please rate this question:, , Discuss and give feedback, , Next question, , Surgical site infection, , , , , , , , , Surgical site infections may occur following a breach in tissue surfaces and allow normal, commensals and other pathogens to initiate infection. They are a major cause of morbidity, and mortality., Surgical site infections (SSI) comprise up to 20% of all healthcare associated infections and, at least 5% of patients undergoing surgery will develop an SSI as a result., In many cases the organisms are derived from the patient's own body. Measures that may, increase the risk of SSI include:, Shaving the wound using a razor (disposable clipper preferred), Using a non iodine impregnated incise drape if one is deemed to be necessary, Tissue hypoxia, Delayed administration of prophylactic antibiotics in tourniquet surgery, , Preoperatively, , , , , Don't remove body hair routinely, If hair needs removal, use electrical clippers with single use head (razors increase infection, risk)
Page 2506 :
, , Antibiotic prophylaxis if:, , - placement of prosthesis or valve, - clean-contaminated surgery, - contaminated surgery, , , , , , Use local formulary, Aim to give single dose IV antibiotic on anaesthesia, If a tourniquet is to be used, give prophylactic antibiotics earlier, , Intraoperatively, , , , , , , Prepare the skin with alcoholic chlorhexidine (Lowest incidence of SSI), Cover surgical site with dressing, A recent meta analysis has confirmed that administration of supplementary oxygen does not, reduce the risk of wound infection. In contrast to previous individual RCT's(1), Wound edge protectors do not appear to confer benefit (2), , Post operatively, Tissue viability advice for management of surgical wounds healing by secondary intention, Use of diathermy for skin incisions, In the NICE guidelines the use of diathermy for skin incisions is not advocated(3). Several, randomised controlled trials have been undertaken and demonstrated no increase in risk of SSI, when diathermy is used(4)., References, 1. Brar M et al.. Perioperative supplemental oxygen in colorectal patients: a meta analysis. J Surg, Res2011 (166): 227 -235., 2. Pinkney T et al. Impact of wound edge protection devices on surgical site infection after, laparotomy: impact of a multicentre randomised controlled trial (ROSSINI Trial). BMJ 2013 (347):10., 3. http://www.nice.org.uk/CG74, 4. Ahmad N and Ahmed A. Meta-analysis of the effectiveness of surgical scalpel or diathermy in, making abdominal skin incisions. Ann Surg 2011, 253(1):8-13., Next question
Page 2507 :
Theme: Suture materials, , A. Silk 3/0, B. Polyglactin 3/0, C. Polydioxanone 1/0, D. Stainless steel skin clips, E. Stainless steel wire 1/0, F. 6/0 Polypropylene, G. 3/0 Undyed polyglactin, H. 3/0 Polypropylene, , Please select the most appropriate suture for the situation described. Each option may be used, once, more than once or not at all., , 58., , Anchoring a RediVac drain to the skin following a mastectomy., Silk 3/0, Silk is traditionally used for this purpose because of its reliable knotting., , 59., , A surgeon wishes to closure the linea alba of the abdominal wall following a laparotomy, You answered Silk 3/0, The correct answer is Polydioxanone 1/0, A large suture such as 1/0 PDS or 1/0 polypropylene is the standard material for this indication., From the list 1/0 PDS is the most appropriate., , 60., , Anastomosis of Dacron graft to proximal abdominal aorta during abdominal aortic aneurysm, repair.
Page 2508 :
You answered Silk 3/0, The correct answer is 3/0 Polypropylene, 3/0 polypropylene is the suture of choice in this setting. 6/0 is too fine and will not withstand the, tensile forces., , Please rate this question:, , Discuss and give feedback, , Next question, , Suture material, Suture materials, , Agent, , Classification, , Durability, , Uses, , Special points, , Silk, , Braided, Biological, , Theoretically, permanent, although, strength not, preserved, , Anchoring devices, skin, closure, , Knots easily, poor, cosmesis, , Catgut, , Braided, Biological, , 5-7 days, , Short term wound, approximation, , Poor cosmesis, Degrades rapidly, Not available in UK, , Chromic catgut, , Braided, Biological, , Up to 12 weeks, , Apposition of deeply, sited tissues, , Unpredictable, degradation pattern, Not in use in UK
Page 2509 :
Agent, , Classification, , Durability, , Uses, , Special points, , Polydiaxonone, (PDS), , Synthetic, Monofilament, , Up to 3 months, (longer with, thicker sutures), , Widespread surgical, applications including, visceral anastomoses,, dermal closure, mass, closure of abdominal, wall, , Used in most surgical, specialties (avoid dyed, form in dermal, closure), , Polyglycolic acid, (Vicryl, Dexon), , Braided, Synthetic, , Up to 6 weeks, , Most tissues can be, apposed using, polyglycolic acid, , It has good handling, properties, the dyed, form of this suture, should not be used for, skin closure, , Polypropylene, (Prolene), , Synthetic, Monofilament, , Permanent, , Widely used, agent of, choice for vascular, anastomoses, , Poor handling, properties, , Polyester, (Ethibond), , Synthetic, Braided, , Permanent, , Its combination of, permanency and, braiding makes it useful, for laparoscopic surgery, , It is more expensive, and has considerable, tissue drag, , Absorbable vs Non absorbable, , , , , , Time taken to degrade absorbable materials varies, Usually by macrophages hydrolysing material, Consider absorbable sutures in situations where long term tissue apposition is not required., In cardiac and vascular surgery non absorbable sutures are usually used., , Suture size, , , , The higher the index number the smaller the suture i.e. : 6/0 prolene is finer than 1/0 prolene.
Page 2510 :
, , Finer sutures have less tensile strength. For example 6/0 prolene would not be a suture, suitable for abdominal mass closure but would be ideal for small calibre distal arterial, anastomoses., , Braided vs monofilament, Generally speaking braided sutures have better handling characteristics than non braided. However,, they are associated with higher bacterial counts. Braided materials are unsuitable for use in vascular, surgery as they are potentially thrombogenic., Next question
Page 2511 :
A 19 year old male presents with axillary lymphadenopathy and symptoms suggestive of Hodgkins, lymphoma. What is the most appropriate investigation?, , Fine needle aspiration of the lymph nodes, , Freehand needle core biopsy of the lymph nodes, , Image guided core biopsy of the lymph nodes, , Excision biopsy of a lymph node, , Axillary node clearance, When a diagnosis of lymphoma is suspected, the correct investigation is excision biopsy of a, complete lymph node to confirm the diagnosis., , Excision of a single node is appropriate. Lymphoma is usually treated with chemotherapy and, axillary node clearance is therefore inappropriate. FNA and core biopsy will not allow accurate, diagnosis and are therefore not appropriate., Please rate this question:, , Discuss and give feedback, , Next question, , Hodgkins lymphoma, Presenting features, , , , , , Asymptomatic lympadenopathy, Cough, Pel Ebstein fever, haemoptysis, dyspnoea, B Symptoms - 10% weight loss, fever, night sweats
Page 2512 :
Staging, All patients are staged with CT scanning of the chest, abdomen and pelvis, The Ann Arbor staging system is commonly used, , Stage, , Features, , I, , Single lymph node region, , II, , Two or more regions on the same side of the diaphragm, , III, , Involvement of lymph node regions on both sides of the diaphragm, , IV, , Involvement of extra nodal sites, , Sub types, Classical Hodgkin lymphoma is classified into the following 4 types:, Nodular sclerosing Hodgkin lymphoma (NSHL), Mixed-cellularity Hodgkin lymphoma (MCHL), Lymphocyte-depleted Hodgkin lymphoma (LDHL), Lymphocyte-rich classical Hodgkin lymphoma (LRHL), A Reed Sternberg cell may be identified histologically., A fifth sub type, Nodular lymphocyte-predominant Hodgkin lymphoma, is characterised by a different, cell type Reed- Sternberg cells are rarely seen., Treatment, This may be multimodal and both chemo and radiotherapy are used., Diagnosis, This is made by excision of a complete lymph node that is then submitted for detailed histological, evaluation., Pathogenesis, Infection with Ebstein Barr virus is linked to the condition (particularly mixed cellularity lymphoma)., Prognosis, Stage I disease is associated with survival figures of up to 85% at 5 years. The lymphocyte rich
Page 2513 :
classical lymphoma has the best prognosis. Lymphocyte depleted Hodgkins lymphoma, advancing, age, male sex and stage IV disease are all associated with a worsening of prognosis., Next question
Page 2514 :
What is the mechanism of action of ciprofloxacin?, , Inhibition of DNA gyrase, , Direct injury to the bacterial cell wall, , Osmotic damage to the cell, , Inhibition of reverse transcriptase, , Destruction of bacterial aquaporin proteins, , Please rate this question:, , Discuss and give feedback, , Next question, , Antibiotics: mechanism of action, The lists below summarise the site of action of the commonly used antibiotics, Inhibit cell wall formation, , , , , penicillins, cephalosporins, , Inhibit protein synthesis, , , , , aminoglycosides (cause misreading of mRNA), chloramphenicol
Page 2516 :
A 73 year old lady with gallstones is about the undergo a laparoscopic cholecystectomy. The, surgeon inserts a Verress needle and performs a successful drop test prior to establishing a, pneumoperitoneum. A 5 minute delay ensues before a 10mm infraumbilical trocar is inserted. The, surgeon performs a diagnostic laparoscopy which shows a thickened gallbladder but is otherwise, normal. The anaesthetist complains that the patient has become hypotensive with a blood pressure, of 80/40 mmHg. Of the options below, which is the most appropriate course of action?, , Release of pneumoperitoneum, , Perform a laparotomy, , Administration of intravenous adrenaline, , Administration of intravenous amiodarone, , End the operation, , Excessive intra-abdominal pressure may cause decreased venous return and hypotension. Since, the preliminary laparoscopy did not show any major vascular catastrophe an emergency laparotomy, would not be indicated. In most cases the release of pressure is often sufficient. In cases of a vasovagal episode (which may be induced by peritoneal stretching) a dose of atropine may be required., Please rate this question:, , Discuss and give feedback, , Next question, , Pneumoperitoneum- therapeutic, During a laparoscopic procedure a surgeon will need to create a pneumoperitoneum. This can be, achieved by use of a Verress needle (risk of visceral injury). An alternative is the open "Hassan", style technique. Once access to the abdominal cavity is secured carbon dioxide gas is insufflated to, induce a working space. Higher intra-abdominal pressures may compromise venous return and, reduce cardiac output. If the blood pressure is seen to drop in this way then release of air, will often, improve matters. Should this not be the case then a laparotomy may be necessary to exclude a, more significant internal injury., Next question
Page 2517 :
Which of the following is least likely to reduce the risk of post operative wound infection?, , Electrical clippers to remove body hair, , Use of poviodone impregnated drapes, , Antibiotic prophylaxis for prosthesis placement, , Routine use of mechanical bowel preparation, , Chlorhexidine to prepare the skin, , The routine use of mechanical bowel preparation is not recommended. There is some recent, evidence to support the use of selective gut decontamination. However, this is not in mainstream, practice at present., Please rate this question:, , Discuss and give feedback, , Next question, , Surgical site infection, , , , , , , , , Surgical site infections may occur following a breach in tissue surfaces and allow normal, commensals and other pathogens to initiate infection. They are a major cause of morbidity, and mortality., Surgical site infections (SSI) comprise up to 20% of all healthcare associated infections and, at least 5% of patients undergoing surgery will develop an SSI as a result., In many cases the organisms are derived from the patient's own body. Measures that may, increase the risk of SSI include:, Shaving the wound using a razor (disposable clipper preferred), Using a non iodine impregnated incise drape if one is deemed to be necessary, Tissue hypoxia, Delayed administration of prophylactic antibiotics in tourniquet surgery
Page 2518 :
Preoperatively, , , , , , Don't remove body hair routinely, If hair needs removal, use electrical clippers with single use head (razors increase infection, risk), Antibiotic prophylaxis if:, , - placement of prosthesis or valve, - clean-contaminated surgery, - contaminated surgery, , , , , , Use local formulary, Aim to give single dose IV antibiotic on anaesthesia, If a tourniquet is to be used, give prophylactic antibiotics earlier, , Intraoperatively, , , , , , , Prepare the skin with alcoholic chlorhexidine (Lowest incidence of SSI), Cover surgical site with dressing, A recent meta analysis has confirmed that administration of supplementary oxygen does not, reduce the risk of wound infection. In contrast to previous individual RCT's(1), Wound edge protectors do not appear to confer benefit (2), , Post operatively, Tissue viability advice for management of surgical wounds healing by secondary intention, Use of diathermy for skin incisions, In the NICE guidelines the use of diathermy for skin incisions is not advocated(3). Several, randomised controlled trials have been undertaken and demonstrated no increase in risk of SSI, when diathermy is used(4)., References, 1. Brar M et al.. Perioperative supplemental oxygen in colorectal patients: a meta analysis. J Surg, Res2011 (166): 227 -235., 2. Pinkney T et al. Impact of wound edge protection devices on surgical site infection after, laparotomy: impact of a multicentre randomised controlled trial (ROSSINI Trial). BMJ 2013 (347):10., 3. http://www.nice.org.uk/CG74, 4. Ahmad N and Ahmed A. Meta-analysis of the effectiveness of surgical scalpel or diathermy in, making abdominal skin incisions. Ann Surg 2011, 253(1):8-13., Next question
Page 2519 :
A 67 year old women is undergoing a femoral hernia repair and the surgeon is using a bipolar, diathermy unit for haemostasis. Which of the following is a recognised risk with the use of bipolar, diathermy?, , Patient burns at the site of the contact plate, , Fires when used near alcoholic skin preparations that have pooled, , Coupling injuries, , Risk of thermal injury to regional vessels as a result of tissue heating, , Capacitance injuries, , In bipolar units the flow of electricity is from one electrode to the other over a small area. As a result, a contact plate is not used and coupling and capacitance injuries are uncommon. They have a low, risk of thermal injury to adjacent structures and are preferred for this reason. However, they may, cause sparks and ignite inflammable solutions., Please rate this question:, , Discuss and give feedback, , Next question, , Diathermy, , , , , , Diathermy devices are used by surgeons in all branches of surgery., Use electric currents to produce local heat and thereby facilitate haemostasis or surgical, dissection., Consist of a generator unit that is located outside the patient and can be set to the level of, power required by the surgeon., There are two major types of diathermy machine;, , Monopolar
Page 2520 :
The current flows through the diathermy unit into a handheld device that is controlled by the, surgeon. Electricity can flow from the tip of the device into the patient. The earth electrode is located, some distance away. The relatively narrow tip of the diathermy device produces local heat and this, can be used to vaporise and fulgurate tissues. The current can be adjusted in terms of frequency so, that different actions can be effected. In cutting mode sufficient power is applied to the tissues to, vaporise their water content. In coagulation mode the power level is reduced so that a coagulum is, formed instead. Some diathermy machines can utilise a setting known as blend that alternates, cutting and coagulation functions, these tend to be used during procedures such as colonoscopic, polypectomy., Bipolar, The electric current flows from one electrode to another however, both electrodes are usually, contained within the same device e.g. a pair of forceps. The result is that heating is localised to the, area between the two electrodes and surrounding tissue damage is minimised., Ultrasound based devices, These include CUSA and Harmonic scalpel. They generate high frequency oscillations that seal and, coagulate tissues. They have different energy settings that allow them to dissect and simultaneously, seal vessels if required. The CUSA device leaves vessels intact that may then be divided., Ligasure device, Delivers tailored energy levels to allow simultaneous haemostasis and dissection. The device, senses the impedance of the tissues and tailors energy levels accordingly., Hazards of diathermy, , , , , Inadvertent patient burn. This may result of careless handling of the device or in the case of, monopolar devices forgetting to apply a return electrode plate, In this situation patients may, develop a contact burn when electricity flows to earth, Explosion or fire. This may occur when volatile anaesthetic gases or skin preparation fluid, have been used, Next question
Page 2521 :
A 34 year old lady is due to undergo a laparoscopic cholecystectomy. Which of the following, intrabdominal pressures should typically be set on the gas insufflation system?, , 4mm Hg, , 10mm Hg, , 20mm Hg, , 40mm Hg, , 60mm Hg, , Pressures lower than 7mm Hg are not usually compatible with satisfactory views. Pressures >15mm, Hg are usually associated with decreased venous return and hypotension., Please rate this question:, , Discuss and give feedback, , Next question, , Gases for laparoscopic surgery, Laparoscopic surgery may be performed in a number of body cavities. In some areas irrigation, solutions are preferred. In the abdomen insufflation with carbon dioxide gas is commonly used. The, amount of gas delivered is adjusted to maintain a constant intra-abdominal pressure of between 12, and 15 mmHg. Excessive intra-abdominal pressure may reduce venous return and lead to, hypotension. Too little insufflation will risk obscuring the surgical view., Next question
Page 2522 :
A 53 year old man undergoes an elective right hemicolectomy. A stapled ileo-colic anastomosis is, constructed. Eight hours later he becomes tachycardic and passes approximately 600ml of dark red, blood per rectum. Which of the following processes is the most likely explanation for this, occurrence?, , Anastomotic leak, , Discharging mesenteric haematoma, , Bleeding peptic ulcer, , Anastomotic staple line bleeding, , Mesenteric infarct, Safe visceral anastamosis requires:, , , , , , Mucosal to mucosal apposition, Adequate vascularity, Minimal tension, , Stapled anastomoses are associated with staple line bleeding and this may typically occur in the, early post operative phase. They should be managed conservatively as most will settle., Stapled anastomoses are quicker to perform. Ironically, although they may appear easy they can, carry considerably more potential pitfalls than their hand sewn equivalent and should be used with, caution by the inexperienced, this is especially true if the bowel is very thick walled., Please rate this question:, , Discuss and give feedback, , Anastomoses
Page 2523 :
, , A wide variety of anastomoses are constructed in surgical practice. Essentially the term, refers to the restoration of luminal continuity. As such they are a feature of both abdominal, and vascular surgery., , Visceral anastomoses, For an anastomosis to heal three criteria need to be fulfilled:, , , , , , Adequate blood supply, Mucosal apposition, Minimal tension, , When these are compromised the anastomosis may break down. Even in the best surgical hands, some anastomoses are more prone to dehiscence than others. Oesophageal and rectal, anastomoses are more prone to leakage and reported leak rates following oesophageal and rectal, surgery can be as high as 20%. This figure includes radiological leaks and those with a clinically, significant leak will be of a lower order of magnitude. As a rule small bowel anastomoses heal most, reliably., The decision as to how best to achieve mucosal apposition is one for each surgeon. Some will prefer, the use of stapling devices as they are quicker to use, others will prefer to perform a sutured, anastomosis. The attention to surgical technique is more important than the method chosen and a, poorly constructed stapled anastomosis in thickened tissue is far more prone to leakage than a hand, sewn anastomosis in the same circumstances., If an anastomosis looks unsafe then it may be best not to construct one at all. In colonic surgery this, is relatively clear cut and most surgeons would bring out an end colostomy. In situations such as, oesophageal surgery this is far more problematic and colonic interposition may be required in this, situation., Vascular anastomoses, Most arterial surgery involving bypasses or aneurysm repairs will require construction of an arterial, anastomosis. Technique is important and for small diameter distal arterial surgery the intimal, hyperplasia resulting from a badly constructed anastomosis may render the whole operation futile, before the patient leaves hospital., Some key points about vascular anastomoses:, , , , , Always use non absorbable monofilament suture (e.g. Polypropylene)., Round bodied needle.
Page 2524 :
, , , Correct size for anastamosis ( i.e. 6/0 prolene for bottom end of a femoro-distal bypass)., Suture should be continuous and from inside to outside of artery to avoid raising an intimal, flap.
Page 2526 :
A 53 year old man undergoes a reversal of a loop colostomy. He recovers well and is discharged, home. He is readmitted 10 days later with symptoms of vomiting and colicky abdominal pain. On, examination he has a swelling of the loop colostomy site and it is tender. What is the most likely, underlying diagnosis?, , Haematoma, , Intra abdominal adhesions, , Anastomotic leak, , Anastomotic stricture, , Obstructed incisional hernia, , Theme from January 2016 Exam, In this scenario the most likely diagnosis would be obstructed incisional hernia. The tender swelling, coupled with symptoms of obstruction point to this diagnosis. Prompt surgical exploration is, warranted. Loop colostomy reversals are at high risk of this complication as the operative site is at, increased risk of the development of post operative wound infections., Please rate this question:, , Discuss and give feedback, , Next question, , Acute incisional hernia, , , , , , , , , Any surgical procedure involving entry into a cavity containing viscera may be complicated, by post operative hernia, The abdomen is the commonest site, The deep layer of the wound has usually broken down, allowing internal viscera to protrude, through, Management is dictated by the patients clinical status and the timing of the hernia in relation, to recent surgery, Bowel obstruction or tenderness at the hernia site both mandate early surgical intervention to, reduce the risk of bowel necrosis, Mature incisional hernias with a wide neck, and no symptoms, may be either left or listed for, elective repair, Risk factors for the development of post operative incisional hernias include; post operative, wound infections, long term steroid use, obesity and chronic cough
Page 2527 :
Theme: Abdominal stomas, , A., B., C., D., E., F., G., , End ileostomy, End colostomy, Loop ileostomy, Loop colostomy, End jejunostomy, Loop jejunostomy, Caecostomy, , For each of the following scenarios, please select the most appropriate type of stoma to be, constructed. Each option may be selected once, more than once or not at all., , 2., , A 56 year old man is undergoing a low anterior resection for carcinoma of the rectum. A, primary anastomosis is planned., You answered End ileostomy, The correct answer is Loop ileostomy, Theme from April 2014 Exam, Colonic resections with an anastomosis below the peritoneal reflection may have an, anastomotic leak rate (both clinical and radiological) of up to 15%. Therefore most surgeons, will defunction such an anastomosis to reduce the clinical severity of an anastomotic leak., A loop ileostomy will achieve this end point and is relatively easy to reverse., , 3., , A 23 year old man with uncontrolled ulcerative colitis is undergoing an emergency sub total, colectomy., End ileostomy, Following a sub total colectomy the immediate surgical options include an end ileostomy or, ileorectal anastomosis. In the emergency setting an ileorectal anastomosis would be unsafe., , 4., , A 63 year old women presents with large bowel obstruction. On examination she has a, carcinoma 10cm from the anal verge., You answered End ileostomy, The correct answer is Loop colostomy, Large bowel obstruction resulting from carcinoma should be resected, stented or, defunctioned. The first two options typically apply to tumours above the peritoneal
Page 2528 :
reflection. Lower tumours should be defunctioned with a loop colostomy and then formal, staging undertaken prior to definitive surgery. An emergency attempted rectal resection, carries a high risk of involvement of the circumferential resection margin and is not, recommended., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal stomas, Stomas may be sited during a range of abdominal procedures and involve bringing the lumen or, visceral contents onto the skin. In most cases this applies to the bowel. However, other organs or, their contents may be diverted in case of need., With bowel stomas the type method of construction and to a lesser extent the site will be determined, by the contents of the bowel. In practice, small bowel stomas should be spouted so that their irritant, contents are not in contact with the skin. Colonic stomas do not need to be spouted as their contents, are less irritant., In the ideal situation the site of the stoma should be marked with the patient prior to surgery. Stoma, siting is important as it will ultimately influence the ability of the patient to manage their stoma and, also reduce the risk of leakage. Leakage of stoma contents and subsequent maceration of the, surrounding skin can rapidly progress into a spiraling loss of control of stoma contents., Types of stomas, , Name of stoma, , Use, , Common sites, , Gastrostomy, , , , , Gastric decompression or fixation, Feeding, , Epigastrium, , Loop, jejunostomy, , , , , Seldom used as very high output, May be used following emergency, laparotomy with planned early closure, , Any location according to, need, , Percutaneous, jejunostomy, , , , Usually performed for feeding, purposes and site in the proximal, bowel, , Usually left upper quadrant, , Loop ileostomy, , , , Defunctioning of colon e.g. following, rectal cancer surgery, , Usually right iliac fossa
Page 2529 :
Name of stoma, , End ilestomy, , Use, , , Does not decompress colon (if, ileocaecal valve competent), , , , Usually following complete excision, of colon or where ileo-colic, anastomosis is not planned, May be used to defunction colon, but, reversal is more difficult, , , , End colostomy, , Loop colostomy, , Where a colon is diverted or resected and, anastomosis is not primarily achievable or, desirable, , , , Caecostomy, Mucous fistula, , Common sites, , To defunction a distal segment of, colon, Since both lumens are present the, distal lumen acts as a vent, , Stoma of last resort where loop colostomy is, not possible, , , , , To decompress a distal segment of, bowel following colonic division or, resection, Where closure of a distal resection, margin is not safe or achievable, , Usually right iliac fossa, , Either left or right iliac fossa, , May be located in any region, of the abdomen, depending, upon colonic segment used, , Right iliac fossa, May be located in any region, of the abdomen according to, clinical need, , Next question
Page 2530 :
A 34 year old man undergoes a sub total colectomy to treat fulminant ulcerative colitis. What type of, stoma is most likely to be fashioned?, , End colostomy, , Loop colostomy, , End ileostomy, , Loop ileostomy, , End jejunostomy, , Theme from January 2016 Exam, A sub total colectomy involves the removal of the entire right, transverse, left and part of the sigmoid, colon. The rectal stump is closed and an end ileostomy fashioned in the right iliac fossa., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal stomas, Stomas may be sited during a range of abdominal procedures and involve bringing the lumen or, visceral contents onto the skin. In most cases this applies to the bowel. However, other organs or, their contents may be diverted in case of need., With bowel stomas the type method of construction and to a lesser extent the site will be determined, by the contents of the bowel. In practice, small bowel stomas should be spouted so that their irritant, contents are not in contact with the skin. Colonic stomas do not need to be spouted as their contents, are less irritant., In the ideal situation the site of the stoma should be marked with the patient prior to surgery. Stoma, siting is important as it will ultimately influence the ability of the patient to manage their stoma and, also reduce the risk of leakage. Leakage of stoma contents and subsequent maceration of the, surrounding skin can rapidly progress into a spiraling loss of control of stoma contents., Types of stomas, , Name of stoma, , Use, , Common sites
Page 2531 :
Name of stoma, , Use, , Common sites, , Gastrostomy, , , , , Gastric decompression or fixation, Feeding, , Epigastrium, , Loop, jejunostomy, , , , , Seldom used as very high output, May be used following emergency, laparotomy with planned early closure, , Any location according to, need, , Percutaneous, jejunostomy, , , , Usually performed for feeding, purposes and site in the proximal, bowel, , Usually left upper quadrant, , Loop ileostomy, , , , Defunctioning of colon e.g. following, rectal cancer surgery, Does not decompress colon (if, ileocaecal valve competent), , Usually right iliac fossa, , Usually following complete excision, of colon or where ileo-colic, anastomosis is not planned, May be used to defunction colon, but, reversal is more difficult, , Usually right iliac fossa, , , , End ilestomy, , , , , , End colostomy, , Loop colostomy, , Where a colon is diverted or resected and, anastomosis is not primarily achievable or, desirable, , , , Caecostomy, Mucous fistula, , To defunction a distal segment of, colon, Since both lumens are present the, distal lumen acts as a vent, , Stoma of last resort where loop colostomy is, not possible, , , To decompress a distal segment of, bowel following colonic division or, resection, , Either left or right iliac fossa, , May be located in any region, of the abdomen, depending, upon colonic segment used, , Right iliac fossa, May be located in any region, of the abdomen according to, clinical need
Page 2532 :
Name of stoma, , Use, , , Common sites, , Where closure of a distal resection, margin is not safe or achievable, Next question
Page 2533 :
Theme: Appendicitis, , A., B., C., D., E., F., G., H., I., , Colonoscopy, MRI Abdomen, Appendicectomy, Abdominal CT scan, Barium enema, Exploratory laparotomy, Conservative management with intravenous antibiotics, Re-assure and discharge, Abdominal ultrasound scan, , Please select the most appropriate management option for the following patients. Each option may, be used once, more than once or not at all., , 6., , A 24 year old man presents with a 10 day history of right sided abdominal pain. Prior to this, he was well. On examination he has a low grade fever and a mass palpable in the right iliac, fossa. The rest of his abdomen is soft. An abdominal USS demonstrates matted bowel loops, surrounding a thickened appendix., You answered Colonoscopy, The correct answer is Conservative management with intravenous antibiotics, This man is likely to have an appendix mass. There is no history suggestive of inflammatory, bowel disease. These are usually managed without surgery, especially in the absence of, peritoneal signs. Broad spectrum antibiotics are required. In the past an interval, appendicectomy was performed. This is rare now and in most cases the process resolves, with fibrosis of the appendix., , 7., , A 22 year old man presents with a 48 hour history of right iliac fossa pain. On examination, he has a low grade pyrexia and is tender with voluntary guarding in the right iliac fossa. His, blood tests reveal a WCC of 13 and a CRP of 6. A urine dipstick is positive for leucocytes., You answered Colonoscopy, The correct answer is Appendicectomy, This is a typical history for acute appendicitis and in a young male, few differentials would, be compatible with this history and signs. Whilst inflammatory markers may be raised this, is by no means universal. Further imaging will delay treatment and is unlikely to alter the, eventual surgical outcome., , 8., , A 63 year old man presents with a 48 hour history of right iliac fossa pain. On examination
Page 2534 :
he has a low grade pyrexia and is tender with some voluntary guarding in the right iliac, fossa. Some of his blood tests are reproduced below:, Hb, , 8.1, , WCC, , 13.8, , Platelets, , 438, , Albumin, , 22, , CRP, , 24, , You answered Colonoscopy, The correct answer is Abdominal CT scan, This man's investigations point to a more longstanding disease process (Hb and albumin),, right sided colonic cancer being the most likely. For this reason a CT scan is a sensible, option as it will adjust the surgical planning., Please rate this question:, , Discuss and give feedback, , Next question, , Appendicitis, History, , , , , , , Peri umbilical abdominal pain (visceral stretching of appendix lumen and appendix is mid gut, structure) radiating to the right iliac fossa due to localised parietal peritoneal inflammation., Vomit once or twice but marked and persistent vomiting is unusual., Diarrhoea is rare. However, pelvic appendicitis may cause localised rectal irritation and some, loose stools. A pelvic abscess may also cause diarrhoea., Mild pyrexia is common - temperature is usually 37.5 -38oC. Higher temperatures are more, typical of conditions like mesenteric adenitis., Anorexia is very common. It is very unusual for patients with appendicitis to be hungry., , Examination, , , , Generalised peritonitis if perforation has occurred or localised peritonism., Retrocaecal appendicitis may have relatively few signs.
Page 2535 :
, , Digital rectal examination may reveal boggy sensation if pelvic abscess is present, or even, tenderness with a pelvic appendix., , Diagnosis, , , , , Typically raised inflammatory markers coupled with compatible history and examination, findings should be enough to justify appendicectomy., Urine analysis may show mild leucocytosis but no nitrites., Ultrasound is useful in females where pelvic organ pathology is suspected. Although it is not, always possible to visualise the appendix on ultrasound, the presence of free fluid (always, pathological in males) should raise suspicion., , Ultrasound examination may show evidence of luminal obstruction and thickening of the appendiceal, wall as shown below, , Image sourced from Wikipedia, , Treatment, , , , , , , Appendicectomy which can be performed via either an open or laparoscopic approach., Administration of metronidazole reduces wound infection rates., Patients with perforated appendicitis require copious abdominal lavage., Patients without peritonitis who have an appendix mass should receive broad spectrum, antibiotics and consideration given to performing an interval appendicectomy., Be wary in the older patients who may have either an underlying caecal malignancy or, perforated sigmoid diverticular disease.
Page 2536 :
Laparoscopic appendicectomy is becoming increasing popular as demonstrated below, , Image sourced from Wikipedia
Page 2537 :
Theme: Acute abdominal pain, , A. Ruptured abdominal aortic aneurysm, B. Perforated peptic ulcer, C. Perforated appendicitis, D. Mesenteric infarction, E. Small bowel obstruction, F. Large bowel obstruction, G. Pelvic inflammatory disease, H. Mesenteric adenitis, I. Pancreatitis, J. None of the above, , Please select the most likely cause of abdominal pain for the scenario given. Each option may be, used once, more than once or not at all., , 9., , A 75 year old man is admitted with sudden onset severe generalised abdominal pain, vomiting, and a single episode of bloody diarrhoea. On examination he looks unwell and is in uncontrolled, atrial fibrillation. Although diffusely tender his abdomen is soft., You answered Ruptured abdominal aortic aneurysm, The correct answer is Mesenteric infarction, In mesenteric infarction there is sudden onset of pain together with vomiting and occasionally, passage of bloody diarrhoea. The pain present is usually out of proportion to the physical signs., , 10., , A 19 year old lady is admitted with lower abdominal pain. On examination she is diffusely tender., A laparoscopy is performed and at operation multiple fine adhesions are noted between the liver, and abdominal wall. Her appendix is normal.
Page 2538 :
You answered Ruptured abdominal aortic aneurysm, The correct answer is Pelvic inflammatory disease, This is Fitz Hugh Curtis syndrome in which pelvic inflammatory disease (usually Chlamydia) causes, the formation of fine peri hepatic adhesions., , 11., , A 78 year old man is walking to the bus stop when he suddenly develops severe back pain and, collapses. On examination he has a blood pressure of 90/40 and pulse rate of 110. His abdomen is, distended and he is obese. Though tender his abdomen itself is soft., Ruptured abdominal aortic aneurysm, This will be a retroperitoneal rupture (anterior ones generally don't survive to hospital). The, debate regarding CT varies, it is the authors opinion that a systolic BP of <100mmHg at, presentation mandates immediate laparotomy., , Acute mesenteric ischaemia- Pain out of proportion to the physical signs., Atrial fibrillation is often present., Fitz Hugh Curtis = Fine Hepatic Connections, , Please rate this question:, , Discuss and give feedback, , Next question, , Acute abdominal pain-diagnoses, Conditions presenting with acute abdominal pain, , Condition, , Features, , Investigations, , Management
Page 2539 :
Condition, , Features, , Investigations, , Management, , Appendicitis, , History of migratory, pain., Fever., Anorexia., Evidence of right iliac, fossa tenderness., Mild pyrexia., , Differential white cell count, Pregnancy test, C-Reactive protein, Amylase, Urine dipstick testing, , Appendicectomy, , Mesenteric, adenitis, , Usually recent upper, respiratory tract, infection., High fever., Generalised abdominal, discomfort- true, localised pain and signs, are rare., , Full blood count- may show, slightly raised white cell, count, Urine dipstick often normal, Abdominal ultrasound scan, - usually no free fluid, , Conservative managementappendicectomy if, diagnostic doubt, , Mittelschmerz, , Only seen in females, Mid cycle pain, Usually occurs two, weeks after last, menstrual period, Pain usually has a suprapubic location, Usually subsides over a, 24-48 hour period., , Full blood count- normal, Urine dipstick- normal, Abdominal and pelvic, ultrasound- may show a, trace of pelvic free fluid, , Manage conservatively if, doubt or symptoms fail to, settle then laparoscopy, , Fitz-Hugh Curtis, syndrome, , Disseminated infection, with Chlamydia., Usually seen in females., Consists of evidence of, pelvic inflammatory, disease together with, peri-hepatic, inflammation and, , Abdominal ultrasound scanmay show free fluid, High vaginal swabs - may, show evidence of sexually, transmitted infections, , Usually medically manageddoxycycline or azithromycin
Page 2540 :
Condition, , Features, , Investigations, , Management, , subsequent adhesion, formation., , Abdominal, aortic aneurysm, (ruptured), , Sudden onset of, abdominal pain, radiating to the back in, older adults (look for, risk factors)., Collapse., May be moribund on, arrival in casualty, more, stable if contained, haematoma., Careful clinical, assessment may reveal, pulsatile mass., , Patients who are, haemodynamically stable, should have a CT scan, , Unstable patients should, undergo immediate surgery, (unless it is not in their best, interests)., Those with evidence of, contained leak on CT should, undergo immediate surgery, Increasing unruptured, aneurysmal size is an, indication for urgent, surgical intervention (that, can wait until the next, working day), , Perforated, peptic ulcer, , Sudden onset of pain, (usually epigastric)., Often preceding history, of upper abdominal, pain., Soon develop, generalised abdominal, pain., On examination may, have clinical evidence of, peritonitis., , Erect CXR may show free, air. A CT scan may be, indicated where there is, diagnostic doubt, , Laparotomy (laparoscopic, surgery for perforated, peptic ulcers is both safe, and feasible in experienced, hands), , Intestinal, obstruction, , Colicky abdominal pain, and vomiting (the, nature of which, depends on the level of, the obstruction)., Abdominal distension, , A plain abdominal film may, help with making the, diagnosis. A CT scan may be, useful where diagnostic, uncertainty exists, , In those with a virgin, abdomen a lower and, earlier threshold for, laparotomy should exist, than in those who may have
Page 2541 :
Condition, , Features, , Investigations, , adhesional obstruction, , and constipation (again, depending upon site of, obstruction)., Features of peritonism, may occur where local, necrosis of bowel loops, is occurring., , Mesenteric, infarction, , Embolic events present, with sudden pain and, forceful evacuation., Acute on chronic events, usually have a longer, history and previous, weight loss., On examination the, pain is typically greater, than the physical signs, would suggest., , Management, , Arterial pH and lactate, Arterial phase CT scanning, is the most sensitive test, , Immediate laparotomy and, resection of affected, segments, in acute embolic, events SMA embolectomy, may be needed., , Next question
Page 2542 :
Theme: Management of splenic trauma, , A., B., C., D., E., F., G., , Splenectomy, Angiography, CT Scan, Admit for bed rest and observation, Ultrasound scan, Splenic conservation, MRI of the abdomen, , Please select the most appropriate intervention for the scenario given. Each option may be used, once, more than once or not at all., , 12., , A 7 year old boy falls off a wall the distance is 7 feet. He lands on his left side and there is, left flank bruising. There is no haematuria. He is otherwise stable and haemoglobin is, within normal limits., You answered Splenectomy, The correct answer is Ultrasound scan, This will demonstrate any overt splenic injury. A CT scan carries a significant dose of, radiation. In the absence of haemodynamic instability or other major associated injuries, the use of USS to exclude intraabdominal free fluid (blood) would seem safe when, coupled with active observation. An USS will also show splenic haematomas., , 13., , A 42 year old motorcyclist is involved in a road traffic accident. A FAST scan in the, emergency department shows free intrabdominal fluid and a laparotomy is performed. At, operation there is evidence of small liver laceration that has stopped bleeding and a tear to, the inferior pole of the spleen., You answered Splenectomy, The correct answer is Splenic conservation, As minimum damage, attempt conservation., , 14., , An 18 year old man is involved in a road traffic accident. A CT scan shows disruption of, the splenic hilum and a moderate sized perisplenic haematoma., Splenectomy, Hilar injuries usually mandate splenectomy. The main risk with conservative management
Page 2543 :
here is that he will rebleed and with hilar injuries this can be dramatic., Please rate this question:, , Discuss and give feedback, , Next question, , Splenic trauma, , , , The spleen is one of the more commonly injured intra abdominal organs, In most cases the spleen can be conserved. The management is dictated by the associated, injuries, haemodynamic status and extent of direct splenic injury., , Management of splenic trauma, , Conservative, , Small subcapsular haematoma, Minimal intra abdominal blood, No hilar disruption, , Laparotomy with conservation, , Increased amounts of intraabdominal blood, Moderate haemodynamic compromise, Tears or lacerations affecting <50%, , Resection, , Hilar injuries, Major haemorrhage, Major associated injuries, , Splenectomy, Technique, Trauma, , , , , , , , , GA, Long midline incision, If time permits insert a self retaining retractor (e.g. Balfour/ omnitract), Large amount of free blood is usually present. Pack all 4 quadrants of the abdomen. Allow, the anaesthetist to 'catch up', Remove the packs and assess the viability of the spleen. Hilar injuries and extensive, parenchymal lacerations will usually require splenectomy., Divide the short gastric vessels and ligate them., Clamp the splenic artery and vein. Two clamps on the patient side are better and allow for, double ligation and serve as a safety net if your assistant does not release the clamp, smoothly.
Page 2544 :
, , , , , Be careful not to damage the tail of the pancreas, if you do then this will need to be formally, removed and the pancreatic duct closed., Wash out the abdomen and place a tube drain to the splenic bed., Some surgeons implant a portion of spleen into the omentum, whether you decide to do this, is a matter of personal choice., Post operatively the patient will require prophylactic penicillin V and pneumococcal vaccine., , Elective, Elective splenectomy is a very different operation from that performed in the emergency setting. The, spleen is often large (sometimes massive). Most cases can be performed laparoscopically. The, spleen will often be macerated inside a specimen bag to facilitate extraction., Complications, , , , , , Haemorrhage (may be early and either from short gastrics or splenic hilar vessels, Pancreatic fistula (from iatrogenic damage to pancreatic tail), Thrombocytosis: prophylactic aspirin, Encapsulated bacteria infection e.g. Strep. pneumoniae, Haemophilus, influenzae and Neisseriameningitidis, Next question
Page 2545 :
Theme: Gastrointestinal bleeding, , A., B., C., D., E., F., G., , Haemorrhoids, Meckels diverticulum, Angiodysplasia, Colonic cancer, Diverticular bleed, Ulcerative colitis, Ischaemic colitis, , Please select the most likely cause of colonic bleeding for the scenario given. Each option may be, used once, more than once or not at all, , 15., , A 73 year old lady is admitted with a brisk rectal bleed. She is otherwise well and the, bleed settles. On examination her abdomen is soft and non tender. Elective colonoscopy, shows a small erythematous lesion in the right colon, but no other abnormality., You answered Haemorrhoids, The correct answer is Angiodysplasia, Angiodysplasia can be difficult to identify and treat. The colonoscopic stigmata are easily, missed by poor bowel preparation., , 16., , A 23 year old man complains of passing bright red blood rectally. It has been occurring, over the past week and tends to occur post defecation. He also suffers from pruritus ani., Haemorrhoids, Classical haemorrhoidal symptoms include bright red rectal bleeding, it typically occurs, post defecation and is noticed on the toilet paper and in the toilet pan. It is usually painless,, however, thrombosed external haemorrhoids may be very painful., , 17., , A 63 year old man presents with episodic rectal bleeding the blood tends to be dark in, colour and may be mixed with stool. His bowel habit has been erratic since an abdominal, aortic aneurysm repair 6 weeks previously., You answered Haemorrhoids, The correct answer is Ischaemic colitis, The inferior mesenteric artery may have been ligated and being an arteriopath collateral, flow through the marginal may be imperfect.
Page 2546 :
Please rate this question:, , Discuss and give feedback, , Next question, , Lower Gastrointestinal bleeding, Colonic bleeding, This typically presents as bright red or dark red blood per rectum. Colonic bleeding rarely presents, as malaena type stool, this is because blood in the colon has a powerful laxative effect and is rarely, retained long enough for transformation to occur and because the digestive enzymes present in the, small bowel are not present in the colon. Up to 15% of patients presenting with haemochezia will, have an upper gastrointestinal source of haemorrhage., As a general rule right sided bleeds tend to present with darker coloured blood than left sided, bleeds. Haemorrhoidal bleeding typically presents as bright red rectal bleeding that occurs post, defecation either onto toilet paper or into the toilet pan. It is very unusual for haemorrhoids alone to, cause any degree of haemodynamic compromise., Causes, , Cause, , Presenting features, , Colitis, , Bleeding may be brisk in advanced cases, diarrhoea is commonly present., Abdominal x-ray may show featureless colon., , Diverticular, disease, , Acute diverticulitis often is not complicated by major bleeding and, diverticular bleeds often occur sporadically. 75% all will cease spontaneously, within 24-48 hours. Bleeding is often dark and of large volume., , Cancer, , Colonic cancers often bleed and for many patients this may be the first sign of, the disease. Major bleeding from early lesions is uncommon, , Haemorrhoidal, bleeding, , Typically bright red bleeding occurring post defecation. Although patients, may give graphic descriptions bleeding of sufficient volume to cause, haemodynamic compromise is rare., , Angiodysplasia, , Apart from bleeding, which may be massive, these arteriovenous lesions, cause little in the way of symptoms. The right side of the colon is more, commonly affected.
Page 2547 :
Management, , , , , , , Prompt correction of any haemodynamic compromise is required. Unlike upper, gastrointestinal bleeding the first line management is usually supportive. This is because in, the acute setting endoscopy is rarely helpful., When haemorrhoidal bleeding is suspected a proctosigmoidoscopy is reasonable as, attempts at full colonoscopy are usually time consuming and often futile., In the unstable patient the usual procedure would be an angiogram (either CT or, percutaneous), when these are performed during a period of haemodynamic instability they, may show a bleeding point and may be the only way of identifying a patch of angiodysplasia., In others who are more stable the standard procedure would be a colonoscopy in the, elective setting. In patients undergoing angiography attempts can be made to address the, lesion in question such as coiling. Otherwise surgery will be necessary., In patients with ulcerative colitis who have significant haemorrhage the standard approach, would be a sub total colectomy, particularly if medical management has already been tried, and is not effective., , Indications for surgery, Patients > 60 years, Continued bleeding despite endoscopic intervention, Recurrent bleeding, Known cardiovascular disease with poor response to hypotension, Surgery, Selective mesenteric embolisation if life threatening bleeding. This is most helpful if conducted, during a period of relative haemodynamic instability. If all haemodynamic parameters are normal, then the bleeding is most likely to have stopped and any angiography normal in appearance. In, many units a CT angiogram will replace selective angiography but the same caveats will apply., If the source of colonic bleeding is unclear; perform a laparotomy, on table colonic lavage and, following this attempt a resection. A blind sub total colectomy is most unwise, for example bleeding, from an small bowel arterio-venous malformation will not be treated by this manoeuvre., Summary of Acute Lower GI bleeding recommendations, Consider admission if:, * Over 60 years, * Haemodynamically unstable/profuse PR bleeding, * On aspirin or NSAID, * Significant co morbidity, Management, , , , All patients should have a history and examination, PR and proctoscopy, Colonoscopic haemostasis aimed for in post polypectomy or diverticular bleeding
Page 2548 :
Theme: Surgical signs, , A., B., C., D., E., F., G., , Rovsing's sign, Boas' sign, Psoas stretch sign, Cullen's sign, Grey-Turner's sign, Murphy's sign, None of the above, , Please select the most appropriate eponymous abdominal sign for the scenario given. Each option, may be used once, more than once or not at all., , 18., , Severe acute peri-umbilical bruising in the setting of acute pancreatitis., You answered Rovsing's sign, The correct answer is Cullen's sign, Cullens sign occurs when there has been intraabdominal haemorrage. It is seen in cases of, severe haemorrhagic pancreatitis and is associated with a poor prognosis. It is also seen in, other cases of intraabdominal haemorrhage (such as ruptured ectopic pregnancy)., , 19., , In acute cholecystitis there is hyperaesthesia beneath the right scapula., You answered Rovsing's sign, The correct answer is Boas' sign, Boas sign refers to this hyperaesthesia. It occurs because the abdominal wall innervation of, this region is from the spinal roots that lie at this level., , 20., , In appendicitis palpation of the left iliac fossa causes pain in the right iliac fossa., Rovsing's sign, Rovsings sign elicits tenderness because the deep palpation induces shift of the appendix, (which is inflamed) against the peritoneal surface. This has somatic innervation and will, therefore localise the pain. It is less reliable in pelvic appendicitis and when the appendix, is truly retrocaecal, , Please rate this question:
Page 2549 :
Discuss and give feedback, , Next question, , Abdominal signs, A number of eponymous abdominal signs are noted. These include:, , , , , , , Rovsings sign- appendicitis, Boas sign -cholecystitis, Murphys sign- cholecystitis, Cullens sign- pancreatitis (other intraabdominal haemorrhage), Grey-Turners sign- pancreatitis (or other retroperitoneal haemorrhage), , In clinical practice haemorrhagic pancreatitis is thankfully rare. The signs are important and thus, shown below:, Cullen's sign, , Image sourced from Wikipedia, , Grey Turner's sign
Page 2551 :
Theme: Surgical access, , A., B., C., D., E., F., G., , Gridiron, Lanz, McEvedy, Midline abdominal, Rutherford Morrison, Battle (abdominal), Lower midline, , Please select the most appropriate incision for the procedure required. Each option may be used, once, more than once or not at all., , 21., , A 78 year old lady is admitted with a tender lump in her right groin. It is within the, femoral triangle and there is concern that there may be small bowel obstruction, developing., You answered Gridiron, The correct answer is McEvedy, This is one approach to an obstructed femoral hernia. It is possible to undertake a small, bowel resection through this approach. Recourse to laparotomy may be needed if access is, difficult., , 22., , A 45 year old woman with end stage renal failure is due to undergo a cadaveric renal, transplant. This will be her first transplant., You answered Gridiron, The correct answer is Rutherford Morrison, This is the incision of choice for the extraperitoneal approach to the iliac vessels which, will be required for a renal transplant., , 23., , A slim 20 year old lady is suffering from appendicitis and requires an appendicectomy., You answered Gridiron, The correct answer is Lanz, Either a Lanz or Gridiron incision will give access for appendicectomy. However, in the, case described a Lanz incision will give better cosmesis and can be extended should pelvic
Page 2552 :
surgery be required eg for gynaecological disease., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal incisions, Midline incision, , , , , , Paramedian, incision, , , , , , , Battle, , , , , Commonest approach to the abdomen, Structures divided: linea alba, transversalis fascia, extraperitoneal fat,, peritoneum (avoid falciform ligament above the umbilicus), Bladder can be accessed via an extraperitoneal approach through the, space of Retzius, Parallel to the midline (about 3-4cm), Structures divided/retracted: anterior rectus sheath, rectus (retracted),, posterior rectus sheath, transversalis fascia, extraperitoneal fat,, peritoneum, Incision is closed in layers, Similar location to paramedian but rectus displaced medially (and thus, denervated), Now seldom used, , Kocher's, , Incision under right subcostal margin e.g. Cholecystectomy (open), , Lanz, , Incision in right iliac fossa e.g. Appendicectomy, , Gridiron, , Oblique incision centered over McBurneys point- usually appendicectomy, (less cosmetically acceptable than Lanz, , Gable, , Rooftop incision, , Pfannenstiel's, , Transverse supra pubic, primarily used to access pelvic organs, , McEvedy's, , Groin incision e.g. Emergency repair strangulated femoral hernia, , Rutherford, Morrison, , Extraperitoneal approach to left or right lower quadrants. Gives excellent, access to iliac vessels and is the approach of choice for first time renal, transplantation.
Page 2553 :
Image sourced from Wikipedia, , Next question
Page 2554 :
Theme: Hernias, , A., B., C., D., E., F., G., , Littres hernia, Richters hernia, Bochdalek hernia, Morgagni hernia, Spigelian hernia, Lumbar hernia, Obturator hernia, , Please select the type of hernia that most closely matches the description given. Each option may, be used once, more than once or not at all., , 24., , A 73 year old lady presents with peritonitis and tenderness of the left groin. At operation, she has a left femoral hernia with perforation of the anti mesenteric border of ileum, associated with the hernia., You answered Littres hernia, The correct answer is Richters hernia, When part of the bowel wall is trapped in a hernia such as this it is termed a Richters, hernia and may complicate any hernia although femoral and obturator hernias are most, typically implicated., , 25., , A 22 year old man is operated on for a left inguinal hernia, at operation the sac is opened, to reveal a large Meckels diverticulum., Littres hernia, Hernia containing Meckels diverticulum is termed a Littres hernia., , 26., , A 45 year old man has recurrent colicky abdominal pain. As part of a series of, investigations he undergoes a CT scan and this demonstrates a hernia lateral to the rectus, muscle at the level of the arcuate line., You answered Littres hernia, The correct answer is Spigelian hernia, This is the site for a spigelian hernia., , Please rate this question:
Page 2555 :
Discuss and give feedback, , Next question, , Hernia, Hernias occur when a viscus or part of it protrudes from within its normal anatomical cavity. Specific, hernias are covered under their designated titles the remainder are addressed here., Spigelian hernia, , , , , , , , Interparietal hernia occurring at the level of the arcuate line, Rare, May lie beneath internal oblique muscle. Usually between internal and external oblique, Equal sex distribution, Position is lateral to rectus abdominis, Both open and laparoscopic repair are possible, the former in cases of strangulation, , Lumbar hernia, The lumbar triangle (through which these may occur) is bounded by:, Crest of ilium (inferiorly), External oblique (laterally), Latissimus dorsi (medially), , , Primary lumbar herniae are rare, most are incisional hernias following renal surgery, , - Direct anatomical repair with or without mesh re-enforcement is the procedure of choice, Obturator hernia, , , , , , , Herniation through the obturator canal, Commoner in females, Usually lies behind pectineus muscle, Elective diagnosis is unusual most will present acutely with obstruction, When presenting acutely most cases with require laparotomy or laparoscopy (and small, bowel resection if indicated), , Richters hernia, , , , Condition in which part of the wall of the small bowel (usually the anti mesenteric border) is, strangulated within a hernia (of any type), They do not present with typical features of intestinal obstruction as lumenal patency is, preserved
Page 2556 :
, , Where vomiting is prominent it usually occurs as a result of paralytic ileus from peritonitis (as, these hernias may perforate), , Incisional hernia, , , , , , Occur through sites of surgical access into the abdominal cavity, Most common following surgical wound infection, To minimise following midline laparotomy Jenkins Rule should be followed and this, necessitates a suture length 4x length of incision with bites taken at 1cm intervals, 1 cm from, the wound edge, Repair may be performed either at open surgery or laparoscopically and a wide variety of, techniques are described, , Bochdalek hernia, , , , , , , , , Typically congenital diaphragmatic hernia, 85% cases are located in the left hemi diaphragm, Associated with lung hypoplasia on the affected side, More common in males, Associated with other birth defects, May contain stomach, May be treated by direct anatomical apposition or placement of mesh. In infants that have, severe respiratory compromise mechanical ventilation may be needed and mortality rate is, high, , Morgagni Hernia, , , , , , , , Rare type of diaphragmatic hernia (approx 2% cases), Herniation through foramen of Morgagni, Usually located on the right and tend to be less symptomatic, More advanced cases may contain transverse colon, As defects are small pulmonary hypoplasia is less common, Direct anatomical repair is performed, , Umbilical hernia, , , , , , , , Hernia through weak umbilicus, Usually presents in childhood, Often symptomatic, Equal sex incidence, 95% will resolve by the age of 2 years, Surgery performed after the third birthday
Page 2557 :
Paraumbilical hernia, , , , , , , Usually a condition of adulthood, Defect is in the linea alba, More common in females, Multiparity and obesity are risk factors, Traditionally repaired using Mayos technique - overlapping repair, mesh may be used though, not if small bowel resection is required owing to acute strangulation, , Littres hernia, , , , Hernia containing Meckels diverticulum, Resection of the diverticulum is usually required and this will preclude a mesh repair
Page 2558 :
Theme: Groin masses, , A., B., C., D., E., F., G., H., I., , Femoral hernia, Lymphadenitis, Inguinal hernia, Psoas abscess, Saphenous varix, Femoral artery aneurysm, Metastatic lymphadenopathy, Lymphoma, False femoral artery aneurysm, , What is the likely diagnosis for groin mass described? Each option may be used once, more than, once, or not at all., , 27., , A 52 year old obese lady reports a painless grape sized mass in her groin area. She has no, medical conditions apart from some varicose veins. There is a cough impulse and the mass, disappears on lying down., You answered Femoral hernia, The correct answer is Saphenous varix, The history of varicose veins should indicate a more likely diagnosis of a varix. The varix, can enlarge during coughing/sneezing. A blue discolouration may be noted., , 28., , A 32 year old male is noted to have a tender mass in the right groin area. There are also, red streaks on the thigh, extending from a small abrasion., You answered Femoral hernia, The correct answer is Lymphadenitis, The red streaks are along the line of the lymphatics, indicating infection of the lymphatic, vessels. Lymphadenitis is infection of the local lymph nodes., , 29., , A 23 year old male suffering from hepatitis C presents with right groin pain and swelling., On examination there is a large abscess in the groin. Adjacent to this is a pulsatile, swelling. There is no cough impulse., You answered Femoral hernia, The correct answer is False femoral artery aneurysm
Page 2559 :
False aneurysms may occur following arterial trauma in IVDU. They may have associated, blood borne virus infections and should undergo duplex scanning prior to surgery. False, aneurysms do not contain all layers of the arterial wall., Please rate this question:, , Discuss and give feedback, , Next question, , Groin masses clinical, Groin masses are common and include:, , , , , , , , Herniae, Lipomas, Lymph nodes, Undescended testis, Femoral aneurysm, Saphena varix (more a swelling than a mass!), , In the history, features relating to systemic illness and tempo of onset will often give a clue as to the, most likely underlying diagnosis., Groin lumps- some key questions, , , , , , , , Is there a cough impulse, Is it pulsatile AND is it expansile (to distinguish between false and true aneurysm), Are both testes intra scrotal, Any lesions in the legs such as malignancy or infections (?lymph nodes), Examine the ano rectum as anal cancer may metastasise to the groin, Is the lump soft, small and very superficial (?lipoma), , Scrotal lumps - some key questions, , , , , Is the lump entirely intra scrotal, Does it transilluminate (?hydrocele), Is there a cough impulse (?hernia), , In most cases a diagnosis can be made clinically. Where it is not clear an ultrasound scan is often, the most convenient next investigation.
Page 2560 :
Theme: Right iliac fossa pain, , A., B., C., D., E., F., G., , Urinary tract infection, Appendicitis, Mittelschmerz, Mesenteric adenitis, Crohns disease, Ulcerative colitis, Meckels diverticulum, , Please select the most likely cause for right iliac fossa pain for the scenario given. Each option may, be used once, more than once or not at all., , 30., , A 17 year old male is admitted with lower abdominal discomfort. He has been suffering, from intermittent right iliac fossa pain for the past few months. His past medical history, includes a negative colonoscopy and gastroscopy for iron deficiency anaemia. The pain is, worse after meals. Inflammatory markers are normal., You answered Urinary tract infection, The correct answer is Meckels diverticulum, This scenario should raise suspicion for Meckels as these may contain ectopic gastric, mucosa which may secrete acid with subsequent bleeding and ulceration., , 31., , A 14 year old female is admitted with sudden onset right iliac fossa pain. She is otherwise, well and on examination has some right iliac fossa tenderness but no guarding. She is, afebrile. Urinary dipstick is normal. Her previous menstrual period two weeks ago was, normal and pregnancy test is negative., You answered Urinary tract infection, The correct answer is Mittelschmerz, Typical story and timing for mid cycle pain. Mid cycle pain typically occurs because a, small amount of fluid is released at the time of ovulation. It will usually resolve over 24-48, hours., , 32., , A 21 year old male is admitted with a 3 month history of intermittent right iliac fossa pain., He suffers from episodic diarrhoea and has lost 2 kilos in weight. On examination he has, some right iliac fossa tenderness and is febrile., You answered Urinary tract infection
Page 2561 :
The correct answer is Crohns disease, Weight loss and chronic symptoms coupled with change in bowel habit should raise, suspicion for Crohns. The presence of intermittent right iliac fossa pain is far more typical, of terminal ileal Crohns disease. Both UC and Crohns may be associated with a low grade, pyrexia. The main concern here would be locally perforated Crohns disease with a small, associated abscess., Please rate this question:, , Discuss and give feedback, , Next question, , Right iliac fossa pain, Differential diagnosis, , Appendicitis, , , , , , , Pain radiating to right iliac fossa, Anorexia (very common), Short history, Diarrhoea and profuse vomiting rare, , Crohn's disease, , , , , , Often long history, Signs of malnutrition, Change in bowel habit, especially diarrhoea, , Mesenteric adenitis, , , , , Mainly affects children, Causes include Adenoviruses, Epstein Barr Virus, betahaemolytic Streptococcus, Staphylococcus spp., Escherichia, coli,Streptococcus viridans and Yersinia spp., Patients have a higher temperature than those with appendicitis, If laparotomy is performed, enlarged mesenteric lymph nodes will, be present, , , , , Diverticulitis, , , , , , Both left and right sided disease may present with right iliac fossa, pain, Clinical history may be similar, although some change in bowel, habit is usual, When suspected, a CT scan may help in refining the diagnosis
Page 2562 :
Meckel's, diverticulitis, , , , , , A Meckel's diverticulum is a congenital abnormality that is present, in about 2% of the population, Typically 2 feet proximal to the ileocaecal valve, May be lined by ectopic gastric mucosal tissue and produce, bleeding, , Perforated peptic, ulcer, , , , , This usually produces upper quadrant pain but pain may be lower, Perforations typically have a sharp sudden onset of pain in the, history, , Incarcerated right, inguinal or femoral, hernia, , , , Usually only right iliac fossa pain if right sided or bowel, obstruction., , Bowel perforation, secondary to caecal, or colon carcinoma, , , , Seldom localised to right iliac fossa, although complete large bowel, obstruction with caecal distension may cause pain prior to, perforation., , Gynaecological, causes, , , , Pelvic inflammatory disease/salpingitis/pelvic abscess/Ectopic, pregnancy/Ovarian torsion/Threatened or complete, abortion/Mittelschmerz, , Urological causes, , , , Ureteric colic/UTI/Testicular torsion, , Other causes, , , , TB/Typhoid/Herpes Zoster/AAA/Situs inversus, Next question
Page 2563 :
A 78 year old lady presents with colicky abdominal pain and a tender mass in her groin. On, examination; there is a small firm mass below and lateral to the pubic tubercle. Which of the, following is the most likely underlying diagnosis?, , Incarcerated inguinal hernia, , Thrombophlebitis of a saphena varix, , Incarcerated femoral hernia, , Incarcerated obturator hernia, , Deep vein thrombosis, Femoral hernia = High risk of strangulation (repair urgently), Femoral herniae account for <10% of all groin hernias. In the scenario the combination of symptoms, of intestinal compromise with a mass in the region of the femoral canal points to femoral hernia as, the most likely cause., Please rate this question:, , Discuss and give feedback, , Next question, , Femoral canal, The femoral canal lies at the medial aspect of the femoral sheath. The femoral sheath is a fascial, tunnel containing both the femoral artery laterally and femoral vein medially. The canal lies medial to, the vein., Borders of the femoral canal, , Laterally, , Femoral vein, , Medially, , Lacunar ligament, , Anteriorly, , Inguinal ligament
Page 2564 :
Pectineal ligament, , Posteriorly, , Image showing dissection of femoral canal, , Image sourced from Wikipedia, , Contents, , , , Lymphatic vessels, Cloquet's lymph node, , Physiological significance, Allows the femoral vein to expand to allow for increased venous return to the lower limbs., Pathological significance, As a potential space, it is the site of femoral hernias. The relatively tight neck places these at high, risk of strangulation.
Page 2565 :
Which of the following is not a typical feature of acute appendicitis?, , Neutrophilia, , Profuse vomiting, , Anorexia, , Low grade pyrexia, , Small amounts of protein on urine analysis, Profuse vomiting and diarrhoea are rare in early appendicitis, Whilst patients may vomit once or twice, profuse vomiting is unusual, and would fit more with, gastroenteritis or an ileus. A trace of protein is not an uncommon occurrence in acute appendicitis. A, free lying pelvic appendix may result in localised bladder irritation, with inflammation occurring as a, secondary phenomena. This latter feature may result in patients being incorrectly diagnosed as, having a urinary tract infection. A urine dipstick test is useful in differentiating between the two, conditions., Please rate this question:, , Discuss and give feedback, , Next question, , Appendicitis, History, , , , , , , Peri umbilical abdominal pain (visceral stretching of appendix lumen and appendix is mid gut, structure) radiating to the right iliac fossa due to localised parietal peritoneal inflammation., Vomit once or twice but marked and persistent vomiting is unusual., Diarrhoea is rare. However, pelvic appendicitis may cause localised rectal irritation and some, loose stools. A pelvic abscess may also cause diarrhoea., Mild pyrexia is common - temperature is usually 37.5 -38oC. Higher temperatures are more, typical of conditions like mesenteric adenitis., Anorexia is very common. It is very unusual for patients with appendicitis to be hungry., , Examination
Page 2566 :
, , , , Generalised peritonitis if perforation has occurred or localised peritonism., Retrocaecal appendicitis may have relatively few signs., Digital rectal examination may reveal boggy sensation if pelvic abscess is present, or even, tenderness with a pelvic appendix., , Diagnosis, , , , , Typically raised inflammatory markers coupled with compatible history and examination, findings should be enough to justify appendicectomy., Urine analysis may show mild leucocytosis but no nitrites., Ultrasound is useful in females where pelvic organ pathology is suspected. Although it is not, always possible to visualise the appendix on ultrasound, the presence of free fluid (always, pathological in males) should raise suspicion., , Ultrasound examination may show evidence of luminal obstruction and thickening of the appendiceal, wall as shown below, , Image sourced from Wikipedia, , Treatment, , , , , , Appendicectomy which can be performed via either an open or laparoscopic approach., Administration of metronidazole reduces wound infection rates., Patients with perforated appendicitis require copious abdominal lavage., Patients without peritonitis who have an appendix mass should receive broad spectrum, antibiotics and consideration given to performing an interval appendicectomy.
Page 2567 :
, , Be wary in the older patients who may have either an underlying caecal malignancy or, perforated sigmoid diverticular disease., , Laparoscopic appendicectomy is becoming increasing popular as demonstrated below, , Image sourced from Wikipedia
Page 2568 :
An 28 year old man presents with a direct inguinal hernia. A decision is made to perform an open, inguinal hernia repair. Which of the following is the best option for abdominal wall reconstruction in, this case?, , Suture plication of the transversalis fascia using PDS only, , Suture plication of the hernial defect with nylon and placement of prolene mesh anterior, to external oblique, Suture plication of the hernia defect using nylon and re-enforcing with a sutured repair of, the abdominal wall, Sutured repair of the hernial defect with prolene and placement of prolene mesh over the, cord structures in the inguinal canal, Sutured repair of the hernial defect using nylon and placement of a prolene mesh posterior, to the cord structures, Laparoscopic repair- bilateral and recurrent cases, During an inguinal hernia repair in males the cord structures will always lie anterior to the mesh. In, the conventional open repairs the cord structures are mobilised and the mesh placed behind them,, with a slit made to allow passage of the cord structures through the deep inguinal ring. Placement of, the mesh over the cord structures results in chronic pain and usually a higher risk of recurrence., Laparoscopic inguinal hernia repair is the procedure of choice for bilateral inguinal hernias., Types of surgery include:, , , , , , , Onlay mesh repair (Lichtenstein style), Inguinal herniorrhaphy, Shouldice repair, Darn repair, Laparoscopic mesh repair, , Open mesh repair and laparoscopic repair are the two main procedures in mainstream use. The, Shouldice repair is a useful procedure in cases where a mesh repair would be associated with, increased risk of infection, e.g. repair of case with strangulated bowel, as it avoids the use of mesh., It is, however, far more technically challenging to perform., Please rate this question:
Page 2569 :
Discuss and give feedback, , Next question, , Inguinal hernia surgery, Inguinal hernias occur when the abdominal viscera protrude through the anterior abdominal wall into, the inguinal canal. They may be classified as being either direct or indirect. The distinction between, these two rests on their relation to Hesselbach's triangle., Boundaries of Hesselbach's Triangle, , , , , Medial: Rectus abdominis, Lateral: Inferior epigastric vessels, Inferior: Inguinal ligament, , Image sourced from Wikipedia, , Hernias occurring within the triangle tend to be direct and those outside - indirect., Diagnosis, Most cases are diagnosed clinically, a reducible swelling may be located at the level of the inguinal, canal. Large hernia's may extend down into the male scrotum, these will not trans-illuminate and it is, not possible to "get above" the swelling., Cases that are unclear on examination, but suspected from the history, may be further investigated
Page 2570 :
using ultrasound or by performing a herniogram., Treatment, Hernias associated with few symptoms may be managed conservatively. Symptomatic hernias or, those which are at risk of developing complications are usually treated surgically., First time hernias may be treated by performing an open inguinal hernia repair; the inguinal canal is, opened, the hernia reduced and the defect repaired. A prosthetic mesh may be placed posterior to, the cord structures to re-enforce the repair and reduce the risk of recurrence., Recurrent hernias and those which are bilateral are generally managed with a laparoscopic, approach. This may be via an intra or extra peritoneal route. As in open surgery a mesh is deployed., However, it will typically lie posterior to the deep ring., Inguinal hernia in children, Inguinal hernias in children are almost always of an indirect type and therefore are usually dealt with, by herniotomy, rather than herniorraphy. Neonatal hernias especially in those children born, prematurely are at highest risk of strangulation and should be repaired urgently. Other hernias may, be repaired on an elective basis., References, The UK Based National Institute of Clinical Excellence has published guidelines relating to the, choice between open and laparoscopic inguinal hernia repair. Which users may find interesting:, http://guidance.nice.org.uk/TA83/Guidance/pdf/English
Page 2571 :
Theme: Abdominal closure methods, , A., B., C., D., E., F., G., H., I., J., , Looped 1 PDS (polydiaxone), Looped 1/0 silk, 1/0 Vicryl (polyglactin), 1/0 Vicryl rapide, 2/0 Prolene (Polypropylene), Re-inforced 1 Nylon, Re-inforced 1/0 Silk, Application of VAC system without separation film, Application of VAC System with separation film, Application of a 'Bogota Bag', , Please select the most appropriate wound closure method (for the deep layer) for the abdominal, surgery described., , 36., , A 59 year old man with morbid obesity undergoes a laparotomy and Hartmans procedure, for perforated sigmoid diverticular disease. At the conclusion of the procedure the, abdomen cannot be primarily closed. The Vac system is not available for use., You answered Looped 1 PDS (polydiaxone), The correct answer is Application of a 'Bogota Bag', Application of a Bogota bag is safest as attempted closure will almost certainly fail., Repeat look at 48 hours to determine the best definitive option is needed., , 37., , A 73 year old lady undergoes a low anterior resection for carcinoma of the rectum., Looped 1 PDS (polydiaxone), Mass closure obeying Jenkins rule is required and this states that the suture must be 4, times the length of the wound with tissue bites 1cm deep and 1 cm apart., , 38., , A 67 year old is returned to theatre after developing a burst abdomen on the ward. She has, originally undergone a right hemicolectomy and the SHO who closed the wound had failed, to tie the midline suture correctly. The wound edges appear healthy., You answered Looped 1 PDS (polydiaxone), The correct answer is Re-inforced 1 Nylon, Attempt at re-closing the wound is reasonable, in which case 1 nylon is often used in
Page 2572 :
preference to a dissolvable suture., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal wound dehiscence, , , , This is a significant problem facing all surgeons who undertake abdominal surgery on a, regular basis. Traditionally, it is said to occur when all layers of an abdominal mass closure, fail and the viscera protrude externally (associated with 30% mortality)., It can be subdivided into superficial, in which the skin wound alone fails and complete,, implying failure of all layers., , Factors which increase the risk are:, * Malnutrition, * Vitamin deficiencies, * Jaundice, * Steroid use, * Major wound contamination (e.g. faecal peritonitis), * Poor surgical technique (Mass closure technique is the preferred method-Jenkins Rule), When sudden full dehiscence occurs the management is as follows:, * Analgesia, * Intravenous fluids, * Intravenous broad spectrum antibiotics, * Coverage of the wound with saline impregnated gauze (on the ward), * Arrangements made for a return to theatre, Surgical strategy, , , , Correct the underlying cause (e.g. TPN or NG feed if malnourished), Determine the most appropriate strategy for managing the wound, , Options, , Resuturing of the, wound, , This may be an option if the wound edges are healthy and there is enough, tissue for sufficient coverage. Deep tension sutures are traditionally used for, this purpose., , Application of a, wound manager, , This is a clear dressing with removable front. Particularly suitable when some, granulation tissue is present over the viscera or where there is a high output
Page 2573 :
bowel fistula present in the dehisced wound., , Application of a, 'Bogota bag', , This is a clear plastic bag that is cut and sutured to the wound edges and is, only a temporary measure to be adopted when the wound cannot be closed, and will necessitate a return to theatre for definitive management., , Application of a, VAC dressing, system, , These can be safely used BUT ONLY if the correct layer is interposed, between the suction device and the bowel. Failure to adhere to this absolute, rule will almost invariably result in the development of multiple bowel, fistulae and create an extremely difficult management problem.
Page 2574 :
Theme: Hernias, , A., B., C., D., E., F., G., , Umbilical hernia, Para umbilical hernia, Morgagni hernia, Littres hernia, Bochdalek hernia, Richters hernia, Obturator hernia, , Please select the hernia that most closely matches the description given. Each option may be used, once, more than once or not at all., , 39., , A 1 day old infant is born with severe respiratory compromise. On examination he has a, scaphoid abdomen and an absent apex beat., You answered Umbilical hernia, The correct answer is Bochdalek hernia, Theme from 2011 exam, The large hernia may displace the heart although true dextrocardia is not present. The, associated pulmonary hypoplasia will compromise lung development., , 40., , A 2 month old infant is troubled by recurrent colicky abdominal pain and intermittent, intestinal obstruction. On imaging the transverse colon is herniated into the thoracic cavity,, through a mid line defect., You answered Umbilical hernia, The correct answer is Morgagni hernia, Morgagni hernia may contain the transverse colon. Unless there is substantial herniation,, pulmonary hypoplasia is uncommon. As a result, major respiratory compromise is often, absent., , 41., , A 78 year old lady is admitted with small bowel obstruction, on examination she has a, distended abdomen and the leg is held semi flexed. She has some groin pain radiating to, the ipsilateral knee., You answered Umbilical hernia, The correct answer is Obturator hernia
Page 2575 :
The groin swelling in obturator hernia is subtle and hard to elicit clinically. There may be, pain in the region of sensory distribution of the obturator nerve. The defect is usually, repaired from within the abdomen., Please rate this question:, , Discuss and give feedback, , Next question, , Hernia, Hernias occur when a viscus or part of it protrudes from within its normal anatomical cavity. Specific, hernias are covered under their designated titles the remainder are addressed here., Spigelian hernia, , , , , , , , Interparietal hernia occurring at the level of the arcuate line, Rare, May lie beneath internal oblique muscle. Usually between internal and external oblique, Equal sex distribution, Position is lateral to rectus abdominis, Both open and laparoscopic repair are possible, the former in cases of strangulation, , Lumbar hernia, The lumbar triangle (through which these may occur) is bounded by:, Crest of ilium (inferiorly), External oblique (laterally), Latissimus dorsi (medially), , , Primary lumbar herniae are rare, most are incisional hernias following renal surgery, , - Direct anatomical repair with or without mesh re-enforcement is the procedure of choice, Obturator hernia, , , , , , , Herniation through the obturator canal, Commoner in females, Usually lies behind pectineus muscle, Elective diagnosis is unusual most will present acutely with obstruction, When presenting acutely most cases with require laparotomy or laparoscopy (and small, bowel resection if indicated)
Page 2576 :
Richters hernia, , , , , Condition in which part of the wall of the small bowel (usually the anti mesenteric border) is, strangulated within a hernia (of any type), They do not present with typical features of intestinal obstruction as lumenal patency is, preserved, Where vomiting is prominent it usually occurs as a result of paralytic ileus from peritonitis (as, these hernias may perforate), , Incisional hernia, , , , , , Occur through sites of surgical access into the abdominal cavity, Most common following surgical wound infection, To minimise following midline laparotomy Jenkins Rule should be followed and this, necessitates a suture length 4x length of incision with bites taken at 1cm intervals, 1 cm from, the wound edge, Repair may be performed either at open surgery or laparoscopically and a wide variety of, techniques are described, , Bochdalek hernia, , , , , , , , , Typically congenital diaphragmatic hernia, 85% cases are located in the left hemi diaphragm, Associated with lung hypoplasia on the affected side, More common in males, Associated with other birth defects, May contain stomach, May be treated by direct anatomical apposition or placement of mesh. In infants that have, severe respiratory compromise mechanical ventilation may be needed and mortality rate is, high, , Morgagni Hernia, , , , , , , , Rare type of diaphragmatic hernia (approx 2% cases), Herniation through foramen of Morgagni, Usually located on the right and tend to be less symptomatic, More advanced cases may contain transverse colon, As defects are small pulmonary hypoplasia is less common, Direct anatomical repair is performed, , Umbilical hernia
Page 2577 :
, , , , , , , Hernia through weak umbilicus, Usually presents in childhood, Often symptomatic, Equal sex incidence, 95% will resolve by the age of 2 years, Surgery performed after the third birthday, , Paraumbilical hernia, , , , , , , Usually a condition of adulthood, Defect is in the linea alba, More common in females, Multiparity and obesity are risk factors, Traditionally repaired using Mayos technique - overlapping repair, mesh may be used though, not if small bowel resection is required owing to acute strangulation, , Littres hernia, , , , Hernia containing Meckels diverticulum, Resection of the diverticulum is usually required and this will preclude a mesh repair, Next question
Page 2578 :
Theme: Right iliac fossa pain, , A., B., C., D., E., F., G., , Open Appendicectomy, Laparoscopic appendicectomy, Laparotomy, CT Scan, Colonoscopy, Ultrasound scan abdomen/pelvis, Active observation, , For each scenario please select the most appropriate management option from the list. Each option, may be used once, more than once or not at all., , 42., , A 21 year old women is admitted with a 48 hour history of worsening right iliac fossa, pain. She has been nauseated and vomited twice. On examination, she is markedly tender, in the right iliac fossa with localised guarding. Vaginal examination is unremarkable., Urine dipstick (including beta HCG) is negative. Blood tests show a WCC of 13.5 and, CRP 70., You answered Open Appendicectomy, The correct answer is Laparoscopic appendicectomy, She is likely to have appendicitis. In women of this age there is always diagnostic, uncertainty. With a normal vaginal exam laparoscopy would be preferred over USS., , 43., , An 8 year old boy presents with a 4 hour history of right iliac fossa pain with nausea and, vomiting. He has been back at school for two days after being kept home with a flu like, illness. On examination he is tender in the right iliac fossa, although his abdomen is soft., Temperature is 38.3oc. Blood tests show a CRP of 40 and a WCC of 8.1., You answered Open Appendicectomy, The correct answer is Active observation, This is mesenteric adenitis. Note history of flu like illness and temp > 38 o c., The decision as to how to manage this situation is based on the abdominal findings., Patients with localising signs such as guarding or peritonism should undergo surgery., , 44., , A 21 year old women presents with right iliac fossa pain. She reports some bloodstained, vaginal discharge. She has a HR of 65 bpm., You answered Open Appendicectomy
Page 2579 :
The correct answer is Ultrasound scan abdomen/pelvis, This patient is suspected of having an ectopic pregnancy. She needs an urgent β HCG and, USS of the pelvis. If she were haemodynamically unstable then laparotomy would be, indicated., Please rate this question:, , Discuss and give feedback, , Next question, , Right iliac fossa pain, Differential diagnosis, , Appendicitis, , , , , , , Pain radiating to right iliac fossa, Anorexia (very common), Short history, Diarrhoea and profuse vomiting rare, , Crohn's disease, , , , , , Often long history, Signs of malnutrition, Change in bowel habit, especially diarrhoea, , Mesenteric adenitis, , , , , Mainly affects children, Causes include Adenoviruses, Epstein Barr Virus, betahaemolytic Streptococcus, Staphylococcus spp., Escherichia, coli,Streptococcus viridans and Yersinia spp., Patients have a higher temperature than those with appendicitis, If laparotomy is performed, enlarged mesenteric lymph nodes will, be present, , , , , Diverticulitis, , , , , , Both left and right sided disease may present with right iliac fossa, pain, Clinical history may be similar, although some change in bowel, habit is usual, When suspected, a CT scan may help in refining the diagnosis, , , , A Meckel's diverticulum is a congenital abnormality that is present, , , , Meckel's
Page 2580 :
diverticulitis, , , , in about 2% of the population, Typically 2 feet proximal to the ileocaecal valve, May be lined by ectopic gastric mucosal tissue and produce, bleeding, , Perforated peptic, ulcer, , , , , This usually produces upper quadrant pain but pain may be lower, Perforations typically have a sharp sudden onset of pain in the, history, , Incarcerated right, inguinal or femoral, hernia, , , , Usually only right iliac fossa pain if right sided or bowel, obstruction., , Bowel perforation, secondary to caecal, or colon carcinoma, , , , Seldom localised to right iliac fossa, although complete large bowel, obstruction with caecal distension may cause pain prior to, perforation., , Gynaecological, causes, , , , Pelvic inflammatory disease/salpingitis/pelvic abscess/Ectopic, pregnancy/Ovarian torsion/Threatened or complete, abortion/Mittelschmerz, , Urological causes, , , , Ureteric colic/UTI/Testicular torsion, , Other causes, , , , TB/Typhoid/Herpes Zoster/AAA/Situs inversus
Page 2581 :
Which of the following is not a typical feature of irritable bowel syndrome?, , A change in the consistency of stools, , Abdominal pain relieved with defecation, , A change in frequency of defecation, , Abdominal bloating, , Pain at a single fixed site, , The pain or discomfort of IBS is typically migratory and variable in intensity. Pain at a fixed site is, suggestive of malignancy., Abdominal bloating is an extremely common feature., Please rate this question:, , Discuss and give feedback, , Next question, , Irritable bowel syndrome, The diagnosis of irritable bowel syndrome is made according to the ROME III diagnostic criteria, which state:, Recurrent abdominal pain or discomfort at 3 days per month for the past 3 months, associated with two or more of the following:, , , , , Improvement with defecation., Onset associated with a change in the frequency of stool., Onset associated with a change in the form of the stool., , Features such as lethargy, nausea, backache and bladder symptoms may also support the, diagnosis, Red flag features should be inquired about:, , , , Rectal bleeding
Page 2582 :
, , , , Unexplained/unintentional weight loss, Family history of bowel or ovarian cancer, Onset after 60 years of age, , Suggested investigations are:, , , , , , , , , Full blood count, ESR/CRP, Coeliac disease screen (tissue transglutaminase antibodies), Colonoscopy (if worrying symptoms, positive family history), Thyroid function tests, Glucose (ensure not diabetic), , The NICE criteria state that blood tests alone will suffice in people fulfilling the diagnostic criteria. We, would point out that luminal colonic studies should be considered early in patients with altered bowel, habit referred to hospital and a diagnosis of IBS should still be largely one of exclusion., Treatment, , , , , , , Usually reduce fibre intake., Tailored prescriptions of laxatives or loperamide according to clinical picture., Dietary modification (caffeine avoidance, less carbonated drinks)., Consider low dose tricyclic antidepressants if pain is a dominant symptom., Biofeedback may help.
Page 2583 :
Theme: Causes of abdominal pain, , A., B., C., D., E., F., G., , Acute on chronic mesenteric ischaemia, Ruptured aortic aneurysm, Acute Pancreatitis, Acute mesenteric embolus, Acute appendicitis, Chronic pancreatitis, Mesenteric vein thrombosis, , Please select the most likely underlying diagnosis from the list above. Each option may be used, once, more than once or not at all., , 46., , A 41 year old man is admitted with peritonitis secondary to a perforated appendix. He is, treated with a laparoscopic appendicectomy but has a stormy post operative course. He is, now developing increasing abdominal pain and has been vomiting. A laparotomy is, performed and at operation a large amount of small bowel shows evidence of patchy areas, of infarction., You answered Acute on chronic mesenteric ischaemia, The correct answer is Mesenteric vein thrombosis, Mesenteric vein thrombosis may complicate severe intra abdominal sepsis and when it, progresses may impair bowel perfusion. The serosa is quite resistant to ischaemia so in this, case the appearances are usually patchy., , 47., , A 68 year old man is admitted with abdominal pain and vomiting of 48 hours duration, the, pain radiates to his back and he has required a considerable amount of volume, replacement. Amylase is 741., You answered Acute on chronic mesenteric ischaemia, The correct answer is Acute Pancreatitis, Although back pain and abdominal pain coupled with haemodynamic compromise may, suggest ruptured AAA the 48 hour history and amylase >3 times normal go against this, diagnosis., , 48., , A 79 year old lady develops sudden onset of abdominal pain and collapses, she has passed, a large amount of diarrhoea. In casualty her pH is 7.35 and WCC is 18., You answered Acute on chronic mesenteric ischaemia
Page 2584 :
The correct answer is Acute mesenteric embolus, Although mesenteric infarct may raise the lactate the pH may be raised often secondary to, vomiting., Please rate this question:, , Discuss and give feedback, , Next question, , Mesenteric vessel disease, Mesenteric ischaemia accounts for 1 in 1000 acute surgical admissions. It is primarily caused by, arterial embolism resulting in infarction of the colon. It is more likely to occur in areas such as the, splenic flexure that are located at the borders of the territory supplied by the superior and inferior, mesenteric arteries., Types, , Acute mesenteric, embolus, (commonest 50%), , , , , , , Sudden onset abdominal pain followed by profuse diarrhoea., May be associated with vomiting., Rapid clinical deterioration., Serological tests: WCC, lactate, amylase may all be abnormal, particularly in established disease. These can be normal in the early, phases., , Acute on chronic, mesenteric, ischaemia, , , , , Usually longer prodromal history., Post prandial abdominal discomfort and weight loss are dominant, features. Patients will usually present with an acute on chronic, event, but otherwise will tend not to present until mesenteric flow is, reduced by greater than 80%., When acute thrombosis occurs presentation may be as above. In the, chronic setting the symptoms will often be those of ischaemic, colitis (mucosa is the most sensitive area to this insult)., , , , Mesenteric vein, thrombosis, , Low flow, , , , , , Usually a history over weeks., Overt abdominal signs and symptoms will not occur until venous, thrombosis has reached a stage to compromise arterial inflow., Thrombophilia accounts for 60% of cases., , , , This occurs in patients with multiple co morbidities in whom
Page 2585 :
mesenteric, infarction, , , mesenteric perfusion is significantly compromised by overuse of, inotropes or background cardiovascular compromise., The end result is that the bowel is not adequately perfused and, infarcts occur from the mucosa outwards., , Diagnosis, , , , , , Serological tests: WCC, lactate, CRP, amylase (can be normal in early disease)., Cornerstone for diagnosis of arterial AND venous mesenteric disease is CT angiography, scanning in the arterial phase with thin slices (<5mm). Venous phase contrast is not helpful., SMA duplex USS is useful in the evaluation of proximal SMA disease in patients with chronic, mesenteric ischaemia., MRI is of limited use due to gut peristalsis and movement artefact., , Management, , , , , Overt signs of peritonism: Laparotomy, Mesenteric vein thrombosis: If no peritonism: Medical management with IV heparin, At operation limited resection of frankly necrotic bowel with view to relook laparotomy at 2448h. In the interim urgent bowel revascularisation via endovascular (preferred) or surgery., , Prognosis, Overall poor. Best outlook is from an acute ischaemia from an embolic event where surgery occurs, within 12h. Survival may be 50%. This falls to 30% with treatment delay. The other conditions carry, worse survival figures.
Page 2586 :
Theme: Groin masses, , A., B., C., D., E., F., G., , Femoral aneurysm, Lymphadenitis, Saphena varix, Femoral hernia, Indirect inguinal hernia, Direct inguinal hernia, Psoas abscess, , What is the likely diagnosis for the groin mass described? Each option may be used once, more than, once or not at all., , 49., , A 3 year old boy is referred to the clinic with a scrotal swelling. On examination the mass, does not transilluminate and it is impossible to palpate normal cord above it., You answered Femoral aneurysm, The correct answer is Indirect inguinal hernia, This is likely to be an indirect hernia. In children these arise from persistent processus, vaginalis and require herniotomy., , 50., , A 52 year old obese lady reports a painless mass in the groin area. A mass is noted on, coughing. It is below and lateral to the pubic tubercle., You answered Femoral aneurysm, The correct answer is Femoral hernia, A mass below and lateral to the pubic tubercle is indicative of a femoral hernia., , 51., , A 21 year old man is admitted with a tender mass in the right groin, fevers and sweats. He, is on multiple medical therapy for HIV infection. On examination he has a swelling in his, right groin, hip extension exacerbates the pain., You answered Femoral aneurysm, The correct answer is Psoas abscess, Psoas abscesses may be either primary or secondary. Primary cases often occur in the, immunosuppressed and may occur as a result of haematogenous spread. Secondary cases, may complicated intra abdominal diseases such as Crohns. Patients usually present with
Page 2587 :
low back pain and if the abscess is extensive a mass that may be localised to the inguinal, region or femoral triangle . Smaller collections may be percutaneously drained. If the, collection is larger, or the percutaneous route fails, then surgery (via a retroperitoneal, approach) should be performed., Please rate this question:, , Discuss and give feedback, , Next question, , Groin masses clinical, Groin masses are common and include:, , , , , , , , Herniae, Lipomas, Lymph nodes, Undescended testis, Femoral aneurysm, Saphena varix (more a swelling than a mass!), , In the history, features relating to systemic illness and tempo of onset will often give a clue as to the, most likely underlying diagnosis., Groin lumps- some key questions, , , , , , , , Is there a cough impulse, Is it pulsatile AND is it expansile (to distinguish between false and true aneurysm), Are both testes intra scrotal, Any lesions in the legs such as malignancy or infections (?lymph nodes), Examine the ano rectum as anal cancer may metastasise to the groin, Is the lump soft, small and very superficial (?lipoma), , Scrotal lumps - some key questions, , , , , Is the lump entirely intra scrotal, Does it transilluminate (?hydrocele), Is there a cough impulse (?hernia), , In most cases a diagnosis can be made clinically. Where it is not clear an ultrasound scan is often, the most convenient next investigation.
Page 2588 :
A 56 year old lady is admitted with colicky abdominal pain. A plain x-ray is performed. Which of the, following should not show fluid levels on a plain abdominal film?, , Stomach, , Jejunum, , Ileum, , Caecum, , Descending colon, , Fluid levels in the distal colon are nearly always pathological. In general contents of the left colon, transit quickly and are seldom held in situ for long periods, the content is also more solid., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal radiology, Plain abdominal x-rays are often used as a first line investigation in patients with acute abdominal, pain. A plain abdominal film may demonstrate free air, evidence of bowel obstruction and possibly, other causes of pain (e.g. renal or gallbladder stones)., Investigation of potential visceral perforation is usually best performed by obtaining an erect chest xray, as this is a more sensitive investigation for suspected visceral perforation., Features which are usually abnormal, , , , , , , , Large amounts of free air (colonic perforation), smaller volumes seen with more proximal, perforations., A positive Riglers sign (gas on both sides of the bowel wall)., Caecal diameter of >8cm, Fluid levels in the colon, Ground glass appearance to film (usually due to large amounts of free fluid)., Sentinel loop in patients with inflammation of other organs (e.g. pancreatitis)., , Features which should be expected/ or occur without pathology
Page 2589 :
, , , , In Chiladitis sign, a loop of bowel may be interposed between the liver and diaphragm, giving, the mistaken impression that free air is present., Following ERCP (and sphincterotomy) air may be identified in the biliary tree., Free intra abdominal air following laparoscopy / laparotomy, although usually dissipates after, 48-72 hours.
Page 2590 :
A 56 year old lady presents with a large bowel obstruction and abdominal distension. Which of the, following confirmatory tests should be performed prior to surgery?, , Abdominal ultrasound scan, , Barium enema, , Rectal MRI Scan, , Endoanal ultrasound scan, , Gastrograffin enema, Patients with suspected large bowel obstruction due to tumour should have this confirmed with, gastrograffin enema, sigmoidoscopy or CT scanning prior to surgery., Patients with clinical evidence of large bowel obstruction, should have the presence or absence of, an obstructing lesion confirmed prior to surgery. This is because colonic pseudo-obstruction may, produce a similar radiological picture. A gastrograffin enema is the traditional test, as barium is too, toxic if it spills into the abdominal cavity. An MRI scan will not provide the relevant information,, unless the lesion is rectal and below the peritoneal reflection.A CT scan would be an acceptable, alternative., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal radiology, Plain abdominal x-rays are often used as a first line investigation in patients with acute abdominal, pain. A plain abdominal film may demonstrate free air, evidence of bowel obstruction and possibly, other causes of pain (e.g. renal or gallbladder stones)., Investigation of potential visceral perforation is usually best performed by obtaining an erect chest xray, as this is a more sensitive investigation for suspected visceral perforation., Features which are usually abnormal, , , , , Large amounts of free air (colonic perforation), smaller volumes seen with more proximal, perforations., A positive Riglers sign (gas on both sides of the bowel wall)., Caecal diameter of >8cm
Page 2591 :
, , , , Fluid levels in the colon, Ground glass appearance to film (usually due to large amounts of free fluid)., Sentinel loop in patients with inflammation of other organs (e.g. pancreatitis)., , Features which should be expected/ or occur without pathology, , , , , In Chiladitis sign, a loop of bowel may be interposed between the liver and diaphragm, giving, the mistaken impression that free air is present., Following ERCP (and sphincterotomy) air may be identified in the biliary tree., Free intra abdominal air following laparoscopy / laparotomy, although usually dissipates after, 48-72 hours.
Page 2592 :
Which of these factors does not increase the risk of abdominal wound dehiscence following, laparotomy?, , Jaundice, , Abdominal compartment syndrome, , Poorly controlled diabetes mellitus, , Administration of intravenous steroids, , Use of Ketamine as an anaesthetic agent, , Ketamine does not affect healing. All the other situations in the list carry a strong association with, poor healing and risk of dehisence., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal wound dehiscence, , , , This is a significant problem facing all surgeons who undertake abdominal surgery on a, regular basis. Traditionally, it is said to occur when all layers of an abdominal mass closure, fail and the viscera protrude externally (associated with 30% mortality)., It can be subdivided into superficial, in which the skin wound alone fails and complete,, implying failure of all layers., , Factors which increase the risk are:, * Malnutrition, * Vitamin deficiencies, * Jaundice, * Steroid use, * Major wound contamination (e.g. faecal peritonitis), * Poor surgical technique (Mass closure technique is the preferred method-Jenkins Rule), When sudden full dehiscence occurs the management is as follows:, * Analgesia, * Intravenous fluids, * Intravenous broad spectrum antibiotics, * Coverage of the wound with saline impregnated gauze (on the ward)
Page 2593 :
* Arrangements made for a return to theatre, Surgical strategy, , , , Correct the underlying cause (e.g. TPN or NG feed if malnourished), Determine the most appropriate strategy for managing the wound, , Options, , Resuturing of the, wound, , This may be an option if the wound edges are healthy and there is enough, tissue for sufficient coverage. Deep tension sutures are traditionally used for, this purpose., , Application of a, wound manager, , This is a clear dressing with removable front. Particularly suitable when some, granulation tissue is present over the viscera or where there is a high output, bowel fistula present in the dehisced wound., , Application of a, 'Bogota bag', , This is a clear plastic bag that is cut and sutured to the wound edges and is, only a temporary measure to be adopted when the wound cannot be closed, and will necessitate a return to theatre for definitive management., , Application of a, VAC dressing, system, , These can be safely used BUT ONLY if the correct layer is interposed, between the suction device and the bowel. Failure to adhere to this absolute, rule will almost invariably result in the development of multiple bowel, fistulae and create an extremely difficult management problem., Next question
Page 2594 :
Theme: Causes of diarrhoea, , A., B., C., D., E., F., G., H., , Campylobacter jejuni infection, Salmonella gastroenteritis infection, Crohns disease, Ulcerative colitis, Irritable bowel syndrome, Ischaemic colitis, Laxative abuse, Clostridium difficile infection, , Please select the most likely cause of diarrhoea for each scenario given. Each option may be used, once, more than once or not at all., , 55., , A 23 year old lady has suffered from diarrhoea for 8 months, she has also lost 2 Kg in, weight. At colonoscopy appearances of melanosis coli are identified and confirmed on, biopsy, You answered Campylobacter jejuni infection, The correct answer is Laxative abuse, This may occur as a result of laxative abuse and consists of lipofuschin laden marcophages, that appear brown., , 56., , A 68 year old lady has recently undergone an abdominal aortic aneurysm repair. The, operation was performed electively and was uncomplicated. Since surgery she has had, repeated episodes of diarrhoea., You answered Campylobacter jejuni infection, The correct answer is Ischaemic colitis, The IMA is commonly ligated during an AAA repair and this may then render the left, colon relatively ischaemic, thereby causing mesenteric colitis. Treatment is supportive and, most cases will settle with conservative management., , 57., , A 23 year old man is admitted to hospital with diarrhoea and severe abdominal pain. He, was previously well and his illness has lasted 18 hours., Campylobacter jejuni infection, Severe abdominal pain tends to favour Campylobacter infection.
Page 2595 :
Please rate this question:, , Discuss and give feedback, , Next question, , Diarrhoea, World Health Organisation definitions, Diarrhoea: > 3 loose or watery stool per day, Acute diarrhoea < 14 days, Chronic diarrhoea > 14 days, , Acute Diarrhoea, , Gastroenteritis, , May be accompanied by abdominal pain or nausea/vomiting, , Diverticulitis, , Classically causes left lower quadrant pain, diarrhoea and fever, , Antibiotic therapy, , More common with broad spectrum antibiotics, Clostridium difficile is also seen with antibiotic use, , Constipation causing, overflow, , A history of alternating diarrhoea and constipation may be, given, May lead to faecal incontinence in the elderly, , Chronic, Diarrhoea, , Irritable bowel, syndrome, , Extremely common. The most consistent features are abdominal pain, bloating, and change in bowel habit. Patients may be divided into those with diarrhoea, predominant IBS and those with constipation predominant IBS., Features such as lethargy, nausea, backache and bladder symptoms may also be, present, , Ulcerative, , Bloody diarrhoea may be seen. Crampy abdominal pain and weight loss are also
Page 2596 :
Chronic, Diarrhoea, , colitis, , common. Faecal urgency and tenesmus may occur, , Crohn's, disease, , Crampy abdominal pains and diarrhoea. Bloody diarrhoea less common than in, ulcerative colitis. Other features include malabsorption, mouth ulcers perianal, disease and intestinal obstruction, , Colorectal, cancer, , Symptoms depend on the site of the lesion but include diarrhoea, rectal, bleeding, anaemia and constitutional symptoms e.g. Weight loss and anorexia, , Coeliac disease, , , , , In children may present with failure to thrive, diarrhoea and abdominal, distension, In adults lethargy, anaemia, diarrhoea and weight loss are seen. Other, autoimmune conditions may coexist, , Other conditions associated with diarrhoea include:, , , , , , Thyrotoxicosis, Laxative abuse, Appendicitis with pelvic abscess or pelvic appendix, Radiation enteritis, , Diagnosis, Stool culture, Abdominal and digital rectal examination, Consider colonoscopy (radiological studies unhelpful), Thyroid function tests, serum calcium, anti endomysial antibodies, glucose, Next question
Page 2597 :
A 6 year old child presents with colicky abdominal pain, vomiting and the passage of red current jelly, stool per rectum. On examination the child has a tender abdomen and a palpable mass in the right, upper quadrant. Imaging shows an intussusception. Which of the conditions below is least, recognised as a precipitant?, , Inflammation of Payers patches, , Cystic fibrosis, , Meckels diverticulum, , Mesenteric cyst, , Mucosal polyps, , Mesenteric cysts may be associated with intra abdominal catastrophes where these occur they are, typically either intestinal volvulus or intestinal infarction. They seldom cause intussusception. Cystic, fibrosis may lead to the formation of meconium ileus equivalent and plugs may occasionally serve as, the lead points for an intussusception., Please rate this question:, , Discuss and give feedback, , Next question, , Intussusception- Paediatric, Intussusception typically presents with colicky abdominal pain and vomiting. The telescoping of the, bowel produces mucosal ischaemia and bleeding may occur resulting in the passage of "red current, jelly" stools. Recognised causes include lumenal pathologies such as polyps, lymphadenopathy and, diseases such as cystic fibrosis. Idiopathic intussceception of the ileocaecal valve and terminal ileum, is the most common variant and typically affects young children and toddlers., The diagnosis is usually made by abdominal ultrasound investigation. The decision as to the optimal, treatment is dictated by the patients physiological status and abdominal signs. In general, children
Page 2598 :
who are unstable with localising peritoneal signs should undergo laparotomy, as should those in, whom attempted radiological reduction has failed., In relatively well children without localising signs attempted pneumatic reduction under fluroscopic, guidance is the usual treatment.
Page 2599 :
Which one of the following is least likely to cause malabsorption?, , Primary biliary cirrhosis, , Ileo-colic bypass, , Chronic pancreatitis, , Whipples disease, , Hartmans procedure, , In a Hartmans procedure the sigmoid colon is removed and an end colostomy is fashioned. The, bowel remains in continuity and no absorptive ability is lost., An ileo-colic bypass leaves a redundant loop of small bowel in continuity, where the contents will, stagnate and bacterial overgrowth will occur. Therefore this is recognised cause of malabsorption., Please rate this question:, , Discuss and give feedback, , Next question, , Malabsorption, Malabsorption is characterised by diarrhoea, steatorrhoea and weight loss. Causes may be broadly, divided into intestinal (e.g. villous atrophy), pancreatic (deficiency of pancreatic enzyme production, or secretion) and biliary (deficiency of bile-salts needed for emulsification of fats), Intestinal causes of malabsorption, , , , , , , , coeliac disease, Crohn's disease, tropical sprue, Whipple's disease, Giardiasis, brush border enzyme deficiencies (e.g. lactase insufficiency), , Pancreatic causes of malabsorption, , , chronic pancreatitis
Page 2600 :
, , , cystic fibrosis, pancreatic cancer, , Biliary causes of malabsorption, , , , biliary obstruction, primary biliary cirrhosis, , Other causes, , , , , bacterial overgrowth (e.g. systemic sclerosis, diverticulae, blind loop), short bowel syndrome, lymphoma
Page 2601 :
Theme: Intra abdominal malignancies, , A., B., C., D., E., F., G., , Metastatic adenocarcinoma of the pancreas, Metastatic appendiceal carcinoid, Metastatic colonic cancer, Pseudomyxoma peritonei, MALT lymphoma, Retroperitoneal liposarcoma, Retroperitoneal fibrosis, , For the disease given please give the most likely primary disease process. Each option may be used, once, more than once or not at all., , 60., , A 32 year old man is admitted with a distended tense abdomen. He previously underwent a, difficult appendicectomy 1 year previously and was discharged. At laparotomy the, abdomen is filled with a gelatinous substance., You answered Metastatic adenocarcinoma of the pancreas, The correct answer is Pseudomyxoma peritonei, Pseudomyxoma is classically associated with mucin production and the appendix is the, commonest source., , 61., , A 62 year old man is admitted with dull lower back pain and abdominal discomfort. On, examination he is hypertensive and a lower abdominal fullness is elicited on examination., An abdominal ultrasound demonstrates hydronephrosis and intravenous urography, demonstrated medially displaced ureters. A CT scan shows a periaortic mass., You answered Metastatic adenocarcinoma of the pancreas, The correct answer is Retroperitoneal fibrosis, Retroperitoneal fibrosis is an uncommon condition and its aetiology is poorly understood., In a significant proportion the ureters are displaced medially. In most retroperitoneal, malignancies they are displaced laterally. Hypertension is another common finding. A CT, scan will often show a para-aortic mass, , 62., , A 48 year old lady is admitted with abdominal distension. On examination she is cachectic, and has ascites. Her CA19-9 returns highly elevated., Metastatic adenocarcinoma of the pancreas
Page 2602 :
Although not specific CA 19-9 in the context of this history is highly suggestive of, pancreatic cancer over the other scenarios., Pseudomyxoma peritoneii- Curative treatment is peritonectomy (Sugarbaker procedure) and heated, intra peritoneal chemotherapy., Please rate this question:, , Discuss and give feedback, , Next question, , Pseudomyxoma Peritonei, , , , , , Rare mucinous tumour, Most commonly arising from the appendix (other abdominal viscera are also recognised as, primary sites), Incidence of 1-2/1,000,000 per year, The disease is characterised by the accumulation of large amounts of mucinous material in, the abdominal cavity, , Treatment, Is usually surgical and consists of cytoreductive surgery (and often peritonectomy c.f Sugarbaker, procedure) combined with intra peritoneal chemotherapy with mitomycin C., Survival is related to the quality of primary treatment and in Sugarbakers own centre 5 year survival, rates of 75% have been quoted. Patients with disseminated intraperitoneal malignancy from another, source fare far worse., In selected patients a second look laparotomy is advocated and some practice this routinely.
Page 2603 :
Theme: Abdominal pain, , A., B., C., D., E., F., G., , Acute mesenteric embolus, Acute on chronic mesenteric ischaemia, Mesenteric vein thrombosis, Ruptured abdominal aortic aneurysm, Pancreatitis, Appendicitis, Acute cholecystitis, , Please select the most likely underlying diagnosis from the list above. Each option may be used, once, more than once or not at all., , 63., , A 72 year old man collapses with sudden onset abdominal pain. He has been suffering, from back pain recently and has been taking ibuprofen., You answered Acute mesenteric embolus, The correct answer is Ruptured abdominal aortic aneurysm, Back pain is a common feature with expanding aneurysms and may be miss classified as, being of musculoskeletal origin., , 64., , A 73 year old women collapses with sudden onset of abdominal pain and the passes a large, amount of diarrhoea. On admission she is vomiting repeatedly. She has recently been, discharged from hospital following a myocardial infarct but recovered well., Acute mesenteric embolus, Sudden onset of abdominal pain and forceful bowel evacuation are features of acute, mesenteric infarct., , 65., , A 66 year old man has been suffering from weight loss and develops severe abdominal, pain. He is admitted to hospital and undergoes a laparotomy. At operation the entire small, bowel is infarcted and only the left colon is viable., You answered Acute mesenteric embolus, The correct answer is Acute on chronic mesenteric ischaemia, This man is likely to have underlying chronic mesenteric vascular disease. Only 15% of, emboli will occlude SMA orifice leading to entire small bowel infarct. The background, history of weight loss also favours an acute on chronic event.
Page 2604 :
Please rate this question:, , Discuss and give feedback, , Next question, , Mesenteric vessel disease, Mesenteric ischaemia accounts for 1 in 1000 acute surgical admissions. It is primarily caused by, arterial embolism resulting in infarction of the colon. It is more likely to occur in areas such as the, splenic flexure that are located at the borders of the territory supplied by the superior and inferior, mesenteric arteries., Types, , Acute mesenteric, embolus, (commonest 50%), , , , , , , Sudden onset abdominal pain followed by profuse diarrhoea., May be associated with vomiting., Rapid clinical deterioration., Serological tests: WCC, lactate, amylase may all be abnormal, particularly in established disease. These can be normal in the early, phases., , Acute on chronic, mesenteric, ischaemia, , , , , Usually longer prodromal history., Post prandial abdominal discomfort and weight loss are dominant, features. Patients will usually present with an acute on chronic, event, but otherwise will tend not to present until mesenteric flow is, reduced by greater than 80%., When acute thrombosis occurs presentation may be as above. In the, chronic setting the symptoms will often be those of ischaemic, colitis (mucosa is the most sensitive area to this insult)., , , , Mesenteric vein, thrombosis, , , , , , Low flow, mesenteric, infarction, , , , , , Usually a history over weeks., Overt abdominal signs and symptoms will not occur until venous, thrombosis has reached a stage to compromise arterial inflow., Thrombophilia accounts for 60% of cases., This occurs in patients with multiple co morbidities in whom, mesenteric perfusion is significantly compromised by overuse of, inotropes or background cardiovascular compromise., The end result is that the bowel is not adequately perfused and, infarcts occur from the mucosa outwards.
Page 2605 :
Diagnosis, , , , , , Serological tests: WCC, lactate, CRP, amylase (can be normal in early disease)., Cornerstone for diagnosis of arterial AND venous mesenteric disease is CT angiography, scanning in the arterial phase with thin slices (<5mm). Venous phase contrast is not helpful., SMA duplex USS is useful in the evaluation of proximal SMA disease in patients with chronic, mesenteric ischaemia., MRI is of limited use due to gut peristalsis and movement artefact., , Management, , , , , Overt signs of peritonism: Laparotomy, Mesenteric vein thrombosis: If no peritonism: Medical management with IV heparin, At operation limited resection of frankly necrotic bowel with view to relook laparotomy at 2448h. In the interim urgent bowel revascularisation via endovascular (preferred) or surgery., , Prognosis, Overall poor. Best outlook is from an acute ischaemia from an embolic event where surgery occurs, within 12h. Survival may be 50%. This falls to 30% with treatment delay. The other conditions carry, worse survival figures.
Page 2606 :
Theme: Surgical incisions, , A., B., C., D., E., F., G., , Lanz incision, Gridiron incision, Kochers incision, Rutherford Morrison, Rooftop incision, McEvedy Incision, Lotheissen Incision, , Please select the most appropriate incision for the procedure described. Each option may be used, once, more than once or not at all., , 66., , A 78 year old lady is admitted with an incarcerated femoral hernia. Abdominal signs are, absent and there are no symptoms of obstruction. AXR is normal., You answered Lanz incision, The correct answer is McEvedy Incision, From the list, the McEvedy approach is the most appropriate. The Lotheissen incision may, compromise the posterior wall of the inguinal canal and is best avoided. The author prefers, a limited pfannenstial type incision for this procedure, as it gives better control of the, hernia, but this is not on the list., , 67., , A 15 year old girl presents with right iliac fossa pain and guarding, pregnancy test is, negative and WCC is 16., Lanz incision, She requires an appendicectomy. Although there is an increasing vogue for performing, this procedure laparoscopically, an open procedure is entirely suitable. However, although, both a Gridiron and Lanz incision are suitable for appendicectomy a Lanz will give a, superior cosmetic result and would be the preferred option for most young females., , 68., , A 45 year old man is due to undergo a live donor renal transplant. This will be his first, procedure., You answered Lanz incision, The correct answer is Rutherford Morrison, The Rutherford Morrison incision will typically give access to the iliac vessels and bladder
Page 2607 :
for the procedure., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal incisions, Midline incision, , , , , , Paramedian, incision, , , , , , , Battle, , , , , Commonest approach to the abdomen, Structures divided: linea alba, transversalis fascia, extraperitoneal fat,, peritoneum (avoid falciform ligament above the umbilicus), Bladder can be accessed via an extraperitoneal approach through the, space of Retzius, Parallel to the midline (about 3-4cm), Structures divided/retracted: anterior rectus sheath, rectus (retracted),, posterior rectus sheath, transversalis fascia, extraperitoneal fat,, peritoneum, Incision is closed in layers, Similar location to paramedian but rectus displaced medially (and thus, denervated), Now seldom used, , Kocher's, , Incision under right subcostal margin e.g. Cholecystectomy (open), , Lanz, , Incision in right iliac fossa e.g. Appendicectomy, , Gridiron, , Oblique incision centered over McBurneys point- usually appendicectomy, (less cosmetically acceptable than Lanz, , Gable, , Rooftop incision, , Pfannenstiel's, , Transverse supra pubic, primarily used to access pelvic organs, , McEvedy's, , Groin incision e.g. Emergency repair strangulated femoral hernia, , Rutherford, Morrison, , Extraperitoneal approach to left or right lower quadrants. Gives excellent, access to iliac vessels and is the approach of choice for first time renal, transplantation.
Page 2608 :
Image sourced from Wikipedia, , Next question
Page 2609 :
Theme: Acute abdominal pain, , A. Appendicitis, B. Henoch Schonlein purpura, C. Diabetes mellitus, D. Intussusception, E. Mittelschmerz, F. Pneumonia, G. Sickle cell crisis, H. Spontaneous bacterial peritonitis, I. Rupure of follicular cyst, , Please select the most likely cause of abdominal pain for the scenario given. Each option may be, used once, more than once or not at all., , 69., , An 11 month-old girl develops sudden onset abdominal pain. She has a high pitched scream and, draws up her legs. Her BP is 90/40 mm/Hg, her pulse 118/min and abdominal examination is, normal., You answered Appendicitis, The correct answer is Intussusception, Intussusception should be considered in toddlers and infants presenting with screaming attacks., The child often has a history of being unwell for one to three days prior to presentation. The child, may pass bloody mucus stool, which is a late sign. Examination of the abdomen is often normal as, the sausage mass in the right upper quadrant is difficult to feel., , 70., , An 8 year-old West Indian boy presents with periumbilical abdominal pain. He has vomited twice, and is refusing fluids. His temperature is 38.1oC and blood tests are as follows: Haemoglobin 8, g/dl, WCC 13 x 109/l, with a neutrophilia.
Page 2610 :
You answered Appendicitis, The correct answer is Sickle cell crisis, Sickle cell anaemia is characterised by severe chronic haemolytic anaemia resulting from poorly, formed erythrocytes. Painful crises result from vaso-occlusive episodes, which may occur, spontaneously or may be precipitated by infection. Consider this diagnosis in all children of, appropriate ethnic background., , 71., , A 15-month-old girl presents with a three day history of periorbital oedema. She is brought to, hospital. On examination she has facial oedema and a tender distended abdomen. Her, temperature is 39oC and her blood pressure is 90/45 mmHg. There is clinical evidence of poor, peripheral perfusion., You answered Appendicitis, The correct answer is Spontaneous bacterial peritonitis, The 15-month-old girl is a patient with nephrotic syndrome. Patients with this condition are at risk, of septicaemia and peritonitis from Streptococcus pneumoniae, due to the loss of, immunoglobulins and opsonins in the urine., , Please rate this question:, , Discuss and give feedback, , Next question, , Acute abdominal pain-diagnoses, Conditions presenting with acute abdominal pain, , Condition, , Features, , Investigations, , Management
Page 2611 :
Condition, , Features, , Investigations, , Management, , Appendicitis, , History of migratory, pain., Fever., Anorexia., Evidence of right iliac, fossa tenderness., Mild pyrexia., , Differential white cell count, Pregnancy test, C-Reactive protein, Amylase, Urine dipstick testing, , Appendicectomy, , Mesenteric, adenitis, , Usually recent upper, respiratory tract, infection., High fever., Generalised abdominal, discomfort- true, localised pain and signs, are rare., , Full blood count- may show, slightly raised white cell, count, Urine dipstick often normal, Abdominal ultrasound scan, - usually no free fluid, , Conservative managementappendicectomy if, diagnostic doubt, , Mittelschmerz, , Only seen in females, Mid cycle pain, Usually occurs two, weeks after last, menstrual period, Pain usually has a suprapubic location, Usually subsides over a, 24-48 hour period., , Full blood count- normal, Urine dipstick- normal, Abdominal and pelvic, ultrasound- may show a, trace of pelvic free fluid, , Manage conservatively if, doubt or symptoms fail to, settle then laparoscopy, , Fitz-Hugh Curtis, syndrome, , Disseminated infection, with Chlamydia., Usually seen in females., Consists of evidence of, pelvic inflammatory, disease together with, peri-hepatic, inflammation and, , Abdominal ultrasound scanmay show free fluid, High vaginal swabs - may, show evidence of sexually, transmitted infections, , Usually medically manageddoxycycline or azithromycin
Page 2612 :
Condition, , Features, , Investigations, , Management, , subsequent adhesion, formation., , Abdominal, aortic aneurysm, (ruptured), , Sudden onset of, abdominal pain, radiating to the back in, older adults (look for, risk factors)., Collapse., May be moribund on, arrival in casualty, more, stable if contained, haematoma., Careful clinical, assessment may reveal, pulsatile mass., , Patients who are, haemodynamically stable, should have a CT scan, , Unstable patients should, undergo immediate surgery, (unless it is not in their best, interests)., Those with evidence of, contained leak on CT should, undergo immediate surgery, Increasing unruptured, aneurysmal size is an, indication for urgent, surgical intervention (that, can wait until the next, working day), , Perforated, peptic ulcer, , Sudden onset of pain, (usually epigastric)., Often preceding history, of upper abdominal, pain., Soon develop, generalised abdominal, pain., On examination may, have clinical evidence of, peritonitis., , Erect CXR may show free, air. A CT scan may be, indicated where there is, diagnostic doubt, , Laparotomy (laparoscopic, surgery for perforated, peptic ulcers is both safe, and feasible in experienced, hands), , Intestinal, obstruction, , Colicky abdominal pain, and vomiting (the, nature of which, depends on the level of, the obstruction)., Abdominal distension, , A plain abdominal film may, help with making the, diagnosis. A CT scan may be, useful where diagnostic, uncertainty exists, , In those with a virgin, abdomen a lower and, earlier threshold for, laparotomy should exist, than in those who may have
Page 2613 :
Condition, , Features, , Investigations, , adhesional obstruction, , and constipation (again, depending upon site of, obstruction)., Features of peritonism, may occur where local, necrosis of bowel loops, is occurring., , Mesenteric, infarction, , Embolic events present, with sudden pain and, forceful evacuation., Acute on chronic events, usually have a longer, history and previous, weight loss., On examination the, pain is typically greater, than the physical signs, would suggest., , Management, , Arterial pH and lactate, Arterial phase CT scanning, is the most sensitive test, , Immediate laparotomy and, resection of affected, segments, in acute embolic, events SMA embolectomy, may be needed., , Next question
Page 2614 :
Which of the following interventions is most likely to reduce the incidence of intra abdominal, adhesions?, , Peritoneal lavage with cetrimide following elective right hemicolectomy, , Use of a laparoscopic approach over open surgery, , Use of talc to coat surgical gloves, , Performing a Nobles plication of the small bowel, , Using stapled rather than a hand sewn anastamosis, , Laparoscopy results in fewer adhesions. When talc was used to coat surgical gloves it was a major, cause of adhesion formation and withdrawn for that reason. A Nobles plication is an old fashioned, operation which has no place in the prevention of adhesion formation. Use of an anastamotic, stapling device will not influence the development of adhesions per se although clearly an, anastamotic leak will result in more adhesion formation, Please rate this question:, , Discuss and give feedback, , Next question, , Surgical complications, Complications occur in all branches of surgery and require vigilance in their detection. In many, cases anticipating the likely complications and appropriate avoidance will minimise their occurrence., For the purposes of the MRCS the important principles to appreciate are:, , , , , , , The anatomical principles that underpin complications, The physiological and biochemical derangements that occur, The most appropriate diagnostic modalities to utilise, The principles which underpin their management, , This is clearly a very broad area and impossible to cover comprehensively. There is considerable, overlap with other topic areas within the website., Avoiding complications
Page 2615 :
Some points to hopefully avert complications:, , , , , , , , , , , , World Health Organisation checklist- now mandatory prior to all operations, Prophylactic antibiotics - right dose, right drug, right time., Assess DVT/ PE risk and ensure adequate prophylaxis, MARK site of surgery, Use tourniquets with caution and with respect for underlying structures, Remember the danger of end arteries and in situations where they occur avoid using, adrenaline containing solutions and monopolar diathermy., Handle tissues with care- devitalised tissue serves as a nidus for infection, Be very wary of the potential for coupling injuries when using diathermy during laparoscopic, surgery, The inferior epigastric artery is a favorite target for laparoscopic ports and surgical drains!, , Anatomical principles, Understanding the anatomy of a surgical field will allow appreciation of local and systemic, complications that may occur. For example, nerve injuries may occur following surgery in specific, regions. The table below lists some of the more important nerves to consider and mechanisms of, injury, , Nerve, , Mechanism, , Accessory, , Posterior triangle lymph node biopsy, , Sciatic, , Posterior approach to hip, , Common peroneal, , Legs in Lloyd Davies position, , Long thoracic, , Axillary node clearance, , Pelvic autonomic nerves, , Pelvic cancer surgery, , Recurrent laryngeal nerves, , During thyroid surgery, , Hypoglossal nerve, , During carotid endarterectomy
Page 2616 :
Nerve, , Mechanism, , Ulnar and median nerves, , During upper limb fracture repairs, , These are just a few. The detailed functional sequelae are particularly important and will often be, tested. In addition to nerve injuries certain procedures carry risks of visceral or structural injury., Again some particular favorites are given below:, , Structure, , Mechanism, , Thoracic duct, , During thoracic surgery e.g. Pneumonectomy, oesphagectomy, , Parathyroid glands, , During difficult thyroid surgery, , Ureters, , During colonic resections/ gynaecological surgery, , Bowel perforation, , Use of Verres Needle to establish pneumoperitoneum, , Bile duct injury, , Failure to delineate Calots triangle carefully and careless use of diathermy, , Facial nerve, , Always at risk during Parotidectomy, , Tail of pancreas, , When ligating splenic hilum, , Testicular vessels, , During re-do open hernia surgery, , Hepatic veins, , During liver mobilisation, , Again many could be predicted from the anatomy of the procedure., Physiological derangements, A very common complication is bleeding and this is covered under the section of haemorrhagic, shock. Another variant is infection either superficial or deep seated. The organisms are covered
Page 2617 :
under microbiology and the features of sepsis covered under shock. Do not forget that, immunocompromised and elderly patients may present will atypical physiological parameters., Selected physiological and biochemical issues are given below:, , Complication, , Physiological/ Biochemical Problem, , Arrhythmias following, cardiac surgery, , Susceptibility to hypokalaemia (K+ <4.0 in cardiac patients), , Neurosurgical electrolyte, disturbance, , SIADH following cranial surgery causing hyponatraemia, , Ileus following, gastrointestinal surgery, , Fluid sequestration and loss of electrolytes, , Pulmonary oedema following, pneumonectomy, , Loss of lung volume makes these patients very sensitive to fluid, overload, , Anastamotic leak, , Generalised sepsis causing mediastinitis or peritonitis depending, on site of leak, , Myocardial infarct, , May follow any type of surgery and in addition to direct cardiac, effects the decreased cardiac output may well compromise grafts, etc., , Try making a short list of problems and causes specific to your own clinical area., Diagnostic modalities, Depends largely on the suspected complication. In the acutely unwell surgical patient the following, baseline investigations are often helpful:, , , , , , , Full blood count, urea and electrolytes, C- reactive protein (trend rather than absolute value),, serum calcium, liver function tests, clotting (don't forget to repeat if on-going bleeding), Arterial blood gases, ECG (+cardiac enzymes if MI suspected), Chest x-ray to identify collapse/ consolidation, Urine analysis for UTI
Page 2618 :
These will often identify the most common complications., Special tests, , , , , , , CT scanning for identification of intra-abdominal abscesses, air and if luminal contrast is, used an anastomotic leak, Doppler USS of leg veins- for identification of DVT, CTPA for PE, Sending peritoneal fluid for U+E (if ureteric injury suspected) or amylase (if pancreatic injury, suspected), Echocardiogram if pericardial effusion suspected post cardiac surgery and no pleural window, made., , Management of complications, The guiding principal should be safe and timely intervention. Patients should be stabilised and if an, operation needs to occur in tandem with resuscitation then generally this should be of a damage, limitation type procedure rather than definitive surgery (which can be more safely undertaken in a, stable patient the following day)., Remember that recent surgery is a contra indication to thrombolysis and that in some patients IV, heparin may be preferable to a low molecular weight heparin (easier to reverse)., As a general rule laparotomies for bleeding should follow the core principle of quadrant packing and, then subsequent pack removal rather than plunging large clamps into pools of blood. The latter, approach invariable worsens the situation is often accompanied by significant visceral injury, particularly when done by the inexperienced. If packing controls a situation it is entirely acceptable, practice to leave packs in situ and return the patient to ITU for pack removal the subsequent day., Next question
Page 2619 :
Theme: Abdominal pain, , A. Appendicitis, B. Threatened miscarriage, C. Ectopic pregnancy, D. Irritable bowel syndrome, E. Mittelschmerz, F. Pelvic inflammatory disease, G. Adnexial torsion, H. Endometriosis, I. Degenerating fibroid, , Please select the most likely cause of abdominal pain for the clinical scenario given. Each option, may be used once, more than once or not at all., , 73., , An 18 year-old girl presents to the Emergency Department with sudden onset sharp, tearing, pelvic pain associated with a small amount of vaginal bleeding. She also complains of shoulder tip, pain. On examination she is hypotensive, tachycardic and has marked cervical excitation., You answered Appendicitis, The correct answer is Ectopic pregnancy, The history of tearing pain and haemodynamic compromise in a women of child bearing years, should prompt a diagnosis of ectopic pregnancy., , 74., , A 25 year-old lady presents to her GP complaining of a two day history of right upper quadrant, pain, fever and a white vaginal discharge. She has seen the GP twice in 12 weeks complaining of, pelvic pain and dyspareunia., You answered Appendicitis
Page 2620 :
The correct answer is Pelvic inflammatory disease, The most likely diagnosis is pelvic inflammatory disease. Right upper quadrant pain occurs as part, of the Fitz Hugh Curtis syndrome in which peri hepatic inflammation occurs., , 75., , A 16 year old female presents to the emergency department with a 12 hour history of pelvic, discomfort. She is otherwise well and her last normal menstrual period was 2 weeks ago. On, examination she has a soft abdomen with some mild supra pubic discomfort., You answered Appendicitis, The correct answer is Mittelschmerz, Mid cycle pain is very common and is due to the small amount of fluid released during ovulation., Inflammatory markers are usually normal and the pain typically subsides over the next 24-48, hours., , Please rate this question:, , Discuss and give feedback, , Next question, , Gynaecological causes of abdominal pain, A number of women will present with abdominal pain and subsequently be diagnosed with a, gynaecological disorder. In addition to routine diagnostic work up of abdominal pain, all female, patients should also undergo a bimanual vaginal examination, urine pregnancy test and, consideration given to abdominal and pelvic ultrasound scanning., When diagnostic doubt persists a laparoscopy provides a reliable method of assessing suspected, tubulo-ovarian pathology., Differential diagnoses of abdominal pain in females, , Diagnosis, , Features, , Investigation, , Treatment
Page 2621 :
Mittelschmerz, , Usually mid cycle pain., Often sharp onset., Little systemic disturbance., May have recurrent, episodes., Usually settles over 24-48, hours., , Full blood countusually normal, Ultrasound- may, show small, quantity of free, fluid, , Conservative, , Endometriosis, , 25% asymptomatic, in a, further 25% associated with, other pelvic organ, pathology., Remaining 50% may have, menstrual irregularity,, infertility, pain and deep, dyspareurina., Complex disease may result, in pelvic adhesional, formation with episodes of, intermittent small bowel, obstruction., Intra-abdominal bleeding, may produce localised, peritoneal inflammation., Recurrent episodes are, common., , Ultrasound- may, show free fluid, Laparoscopy will, usually show, lesions, , Usually managed medically,, complex disease will often, require surgery and some, patients will even require formal, colonic and rectal resections if, these areas are involved, , Ovarian torsion, , Usually sudden onset of, deep seated colicky, abdominal pain., Associated with vomiting, and distress., Vaginal examination may, reveal adnexial tenderness., , Ultrasound may, show free fluid, Laparoscopy is, usually both, diagnostic and, therapeutic, , Laparoscopy, , Ectopic, gestation, , Symptoms of pregnancy, without evidence of intra, uterine gestation., , Ultrasound, showing no intra, uterine pregnancy, , Laparoscopy or laparotomy is, haemodynamically unstable. A, salphingectomy is usually
Page 2622 :
Pelvic, inflammatory, disease, , Present as an emergency, with evidence of rupture or, impending rupture., Open tubular ruptures may, have sudden onset of, abdominal pain and, circulatory collapse, in other, the symptoms may be more, prolonged and less marked., Small amount of vaginal, discharge is common., There is usually adnexial, tenderness., , and beta HCG that, is elevated, May show intra, abdominal free, fluid, , performed., , Bilateral lower abdominal, pain associated with vaginal, discharge., Dysuria may also be present., Peri-hepatic inflammation, secondary to Chlamydia (Fitz, Hugh Curtis Syndrome) may, produce right upper, quadrant discomfort., Fever >38o, , Full blood countLeucocytosis, Pregnancy test, negative (Although, infection and, pregnancy may coexist), Amylase - usually, normal or slightly, raised, High vaginal and, urethral swabs, , Usually medical management
Page 2623 :
Which of the following statements relating to a burst abdomen is false?, , Is seen in 1-2% of modern laparotomies, , Is more common in faecal peritonitis, , Is less common when a 'mass closure' technique is used, , When it does occur is most common at 15 days, , Is similar in incidence regardless of whether 1/0 polydiaxone or 1/0 polypropylene are, used, , When it does occur a burst abdomen is most common at 6 days and is usually the result of technical, error when Jenkins rule is not followed and sutures are placed in the zone of collagenolysis. The, choice of materials given above does not influence dehisence rates., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal wound dehiscence, , , , This is a significant problem facing all surgeons who undertake abdominal surgery on a, regular basis. Traditionally, it is said to occur when all layers of an abdominal mass closure, fail and the viscera protrude externally (associated with 30% mortality)., It can be subdivided into superficial, in which the skin wound alone fails and complete,, implying failure of all layers., , Factors which increase the risk are:, * Malnutrition, * Vitamin deficiencies, * Jaundice, * Steroid use, * Major wound contamination (e.g. faecal peritonitis), * Poor surgical technique (Mass closure technique is the preferred method-Jenkins Rule), When sudden full dehiscence occurs the management is as follows:, * Analgesia, * Intravenous fluids, * Intravenous broad spectrum antibiotics
Page 2624 :
* Coverage of the wound with saline impregnated gauze (on the ward), * Arrangements made for a return to theatre, Surgical strategy, , , , Correct the underlying cause (e.g. TPN or NG feed if malnourished), Determine the most appropriate strategy for managing the wound, , Options, , Resuturing of the, wound, , This may be an option if the wound edges are healthy and there is enough, tissue for sufficient coverage. Deep tension sutures are traditionally used for, this purpose., , Application of a, wound manager, , This is a clear dressing with removable front. Particularly suitable when some, granulation tissue is present over the viscera or where there is a high output, bowel fistula present in the dehisced wound., , Application of a, 'Bogota bag', , This is a clear plastic bag that is cut and sutured to the wound edges and is, only a temporary measure to be adopted when the wound cannot be closed, and will necessitate a return to theatre for definitive management., , Application of a, VAC dressing, system, , These can be safely used BUT ONLY if the correct layer is interposed, between the suction device and the bowel. Failure to adhere to this absolute, rule will almost invariably result in the development of multiple bowel, fistulae and create an extremely difficult management problem.
Page 2625 :
A 35 year old women who is a heavy smoker has long standing stool frequency and crampy, abdominal pain. A colonoscopy is performed (which is macroscopically normal) and pan colonic, biopsies are taken. Histological analysis of the biopsies demonstrates a thickened sub apical, collagen layer together with an increase in lymphocytes in the lamina propria. What is the most likely, diagnosis?, , Microscopic colitis, , Crohns disease, , Ulcerative colitis, , Pseudomembranous colitis, , Irritable bowel syndrome, , Microscopic colitis is a common condition characterised by normal endoscopic appearances,, microscopic features of colonic inflammation and thickening of the sub epithelial collagen layer., Features such as granulomas are absent. It is the normal endoscopic appearance that makes the, other options less likely. IBS is a diagnosis of exclusion and the features of inflammation activity, would favor a different diagnosis. Severe cases can be treated with steroids. Other agents such as, cholestyramine may be beneficial. It is important to exclude infection with a stool culture if this has, not been done, not least because the precipitant of many cases of microscopic colitis is an episode, of infective diarrhoea., Please rate this question:, , Discuss and give feedback, , Next question, , Diarrhoea, World Health Organisation definitions, Diarrhoea: > 3 loose or watery stool per day, Acute diarrhoea < 14 days, Chronic diarrhoea > 14 days, , Acute Diarrhoea
Page 2626 :
Acute Diarrhoea, , Gastroenteritis, , May be accompanied by abdominal pain or nausea/vomiting, , Diverticulitis, , Classically causes left lower quadrant pain, diarrhoea and fever, , Antibiotic therapy, , More common with broad spectrum antibiotics, Clostridium difficile is also seen with antibiotic use, , Constipation causing, overflow, , A history of alternating diarrhoea and constipation may be, given, May lead to faecal incontinence in the elderly, , Chronic, Diarrhoea, , Irritable bowel, syndrome, , Extremely common. The most consistent features are abdominal pain, bloating, and change in bowel habit. Patients may be divided into those with diarrhoea, predominant IBS and those with constipation predominant IBS., Features such as lethargy, nausea, backache and bladder symptoms may also be, present, , Ulcerative, colitis, , Bloody diarrhoea may be seen. Crampy abdominal pain and weight loss are also, common. Faecal urgency and tenesmus may occur, , Crohn's, disease, , Crampy abdominal pains and diarrhoea. Bloody diarrhoea less common than in, ulcerative colitis. Other features include malabsorption, mouth ulcers perianal, disease and intestinal obstruction, , Colorectal, cancer, , Symptoms depend on the site of the lesion but include diarrhoea, rectal, bleeding, anaemia and constitutional symptoms e.g. Weight loss and anorexia, , Coeliac disease, , , , , In children may present with failure to thrive, diarrhoea and abdominal, distension, In adults lethargy, anaemia, diarrhoea and weight loss are seen. Other
Page 2627 :
Chronic, Diarrhoea, , autoimmune conditions may coexist, , Other conditions associated with diarrhoea include:, , , , , , Thyrotoxicosis, Laxative abuse, Appendicitis with pelvic abscess or pelvic appendix, Radiation enteritis, , Diagnosis, Stool culture, Abdominal and digital rectal examination, Consider colonoscopy (radiological studies unhelpful), Thyroid function tests, serum calcium, anti endomysial antibodies, glucose, Next question
Page 2628 :
A 40 year old man presents with a long standing inguinal hernia. On examination he has a small,, direct inguinal hernia. He inquires as to the risk of strangulation over the next twelve months should, he decide not to undergo surgery. Which of the following most closely matches the likely risk of, strangulation over the next 12 months?, , 50%, , 40%, , 25%, , 15%, , <5%, , The annual probability of strangulation is up to 3% and is more common in indirect hernias. Elective, repair poses few risks. However, emergency repair is associated with increased mortality,, particularly in the elderly., Please rate this question:, , Discuss and give feedback, , Next question, , Inguinal hernia surgery, Inguinal hernias occur when the abdominal viscera protrude through the anterior abdominal wall into, the inguinal canal. They may be classified as being either direct or indirect. The distinction between, these two rests on their relation to Hesselbach's triangle., Boundaries of Hesselbach's Triangle, , , , , Medial: Rectus abdominis, Lateral: Inferior epigastric vessels, Inferior: Inguinal ligament
Page 2629 :
Image sourced from Wikipedia, , Hernias occurring within the triangle tend to be direct and those outside - indirect., Diagnosis, Most cases are diagnosed clinically, a reducible swelling may be located at the level of the inguinal, canal. Large hernia's may extend down into the male scrotum, these will not trans-illuminate and it is, not possible to "get above" the swelling., Cases that are unclear on examination, but suspected from the history, may be further investigated, using ultrasound or by performing a herniogram., Treatment, Hernias associated with few symptoms may be managed conservatively. Symptomatic hernias or, those which are at risk of developing complications are usually treated surgically., First time hernias may be treated by performing an open inguinal hernia repair; the inguinal canal is, opened, the hernia reduced and the defect repaired. A prosthetic mesh may be placed posterior to, the cord structures to re-enforce the repair and reduce the risk of recurrence., Recurrent hernias and those which are bilateral are generally managed with a laparoscopic, approach. This may be via an intra or extra peritoneal route. As in open surgery a mesh is deployed., However, it will typically lie posterior to the deep ring., Inguinal hernia in children, Inguinal hernias in children are almost always of an indirect type and therefore are usually dealt with, by herniotomy, rather than herniorraphy. Neonatal hernias especially in those children born, prematurely are at highest risk of strangulation and should be repaired urgently. Other hernias may, be repaired on an elective basis.
Page 2630 :
A 60 year old women has fully recovered from an attack of pancreatitis. Over the following 12, months she develops episodic epigastric discomfort. Un upper GI endoscopy shows gastric varices, only. An abdominal CT scan demonstrates a splenic vein thrombosis. What is the treatment of, choice?, , Splenectomy, , Insertion of transjugular porto-systemic shunt, , Surgical bypass of the splenic vein, , Gastrectomy, , Stapling of the gastro-oesophgeal junction, , Please rate this question:, , Discuss and give feedback, , Next question, , Splenic vein thrombosis, Thrombosis of the splenic vein may complicate pancreatitis, pancreatic carcinoma, iatrogenic trauma, and hypercoagulable diseases. The condition may predispose to the development of gastric varices,, oesophageal varices are uncommon in splenic vein thrombosis alone., Diagnosis is made by CT angiography., Treatment is with splenectomy.
Page 2631 :
Theme: Surgical signs, , A., B., C., D., E., F., G., , Rovsing's sign, Boas' sign, Psoas stretch sign, Cullen's sign, Grey-Turner's sign, Murphy's sign, None of the above, , Please match the clinical sign to the clinical scenario described. Each option may be used once,, more than once or not at all., , 80., , Acute retrocaecal appendicitis is indicated when the right thigh is passively extended with, the patient lying on their side with their knees extended., You answered Rovsing's sign, The correct answer is Psoas stretch sign, , 81., , In acute pancreatitis there is bruising in the flanks., You answered Rovsing's sign, The correct answer is Grey-Turner's sign, Grey-Turners sign occurs in patients with severe haemorrhagic pancreatitis. In this, situation the major vessels surrounding the pancreas bleed. The pancreatitis process also, results in local fat destruction, this results in blood tracking in the tissue planes of the, retroperitoneum and appearing as flank bruising., , 82., , In cholecystitis there is pain/catch of breath elicited on palpation of the right, hypochondrium during inspiration., You answered Rovsing's sign, The correct answer is Murphy's sign, Invariably present when patients are assessed in the emergency department! This sign, occurs because the inflamed gallbladder irritates the parietal peritoneum in this, manoeuvre.
Page 2632 :
Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal signs, A number of eponymous abdominal signs are noted. These include:, , , , , , , Rovsings sign- appendicitis, Boas sign -cholecystitis, Murphys sign- cholecystitis, Cullens sign- pancreatitis (other intraabdominal haemorrhage), Grey-Turners sign- pancreatitis (or other retroperitoneal haemorrhage), , In clinical practice haemorrhagic pancreatitis is thankfully rare. The signs are important and thus, shown below:, Cullen's sign, , Image sourced from Wikipedia, , Grey Turner's sign
Page 2633 :
Image sourced from Wikipedia
Page 2634 :
Which of the following is commonest cause of acute abdominal pain in acute unselected surgical, 'take'?, , Non specific abdominal pain, , Biliary colic, , Acute appendicitis, , Ureteric colic, , Pancreatitis, , Non specific abdominal pain is a commonly recorded diagnosis for patients presenting with acute, abdominal pain. Following careful diagnostic work up, a proportion of patients may be identified with, disorders such as coeliac disease and the diagnosis of non specific abdominal pain should not be, used lightly., Please rate this question:, , Discuss and give feedback, , Next question, , Acute abdominal pain, Acute abdominal pain is a common cause of admission to hospital. The relative proportions of, conditions presenting with abdominal pain is given below:, , , , , , , , , , , Non specific abdominal pain (35%), Appendicitis (17%), Intestinal obstruction (15%), Urological disease (6%), Gallstone disease (5%), Colonic diverticular disease (4%), Abdominal trauma (3%), Perforated peptic ulcer (3%), Pancreatitis (2%), , (Data derived from Irvin T. Br. J. Surg 1989 76:1121-1125), Non specific abdominal pain should really be a diagnosis of exclusion and if care is taken in, excluding organic disease the proportion of cases labeled such should decline. It should also be
Page 2635 :
appreciated that a proportion of patients may have an underlying medical cause for their symptoms, such as pneumonia or diabetic ketoacidosis., Key points in management, , , , , , , , , Early administration of adequate analgesia (including opiates)., Abdominal ultrasound is safe, non invasive and cheap and yields significantly more, information than plain radiology. However, plain radiology is still the main test for suspected, perforated viscus, especially out of hours., In up to 50% cases with perforated peptic ulcer, the plain x-rays may show no evidence of, free air. If clinical signs suggest otherwise, then a CT scan may be a more accurate, investigation, if plain films are normal., Plain film radiology usually cannot detect <1mm free air, and is 33% sensitive for detection of, 1-13mm pockets of free air (Stoker et al. Radiology 2009 253: 31-46)., Think of strangulated intestine when there is fever, raised white cell count, tachycardia and, peritonism., In suspected large bowel obstruction a key investigation is either a water soluble contrast, enema or CT scan., Where need for surgery is difficult to define and imaging is inconclusive the use of, laparoscopy as a definitive diagnostic test is both safe and sensible., Next question
Page 2636 :
A 72 year old obese man undergoes an emergency repair of a ruptured abdominal aortic aneurysm., The wound is closed with an onlay prolene mesh to augment the closure. Post operatively he is, taken to the intensive care unit. Over the following twenty four hours his nasogastric aspirates, increase, his urine output falls and he has a metabolic acidosis. What is the most likely underlying, cause?, , Colonic ischaemia, , Abdominal compartment syndrome, , Peritonitis, , Reactionary haemorrhage, , Aorto-duodenal fistula, , Obese patients with ileus following major abdominal surgery are at increased risk of intra abdominal, compartment syndrome.The risk is increased by the use of prosthetic meshes, which some, surgeons favor following a major vascular case as they may reduce the incidence of incisional, hernia. They prevent abdominal distension and may increase the risk of intra abdominal, hypertension in the short term. Although colonic ischaemia may occur following major aortic surgery, it would not typically present in this way., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal compartment syndrome, Background, Intra-abdominal pressure is the steady state pressure concealed within the abdominal cavity., , , , , , , , In critically ill adults the normal intra abdominal pressure = 5-7mmHg, Intra abdominal hypertension has pressures of 12-25mmHg, Changes >15mmHg are associated with microvascular hypoperfusion, Abdominal compartment syndrome is defined as sustained intra abdominal pressure, >20mmHg coupled with new organ dysfunction / failure, It may occur either primarily without previous surgical intervention e.g. Following intestinal, ischaemia or secondarily following a surgical procedure, Diagnosis is typically made by transvesical pressure measurements coupled with an index of, clinical suspicion.
Page 2637 :
Management, Once the diagnosis is made non operative measures should be instituted including:, , , , , , Gastric decompression, Improve abdominal wall compliance e.g. muscle relaxants/ sedation, Drain abdominal fluid collections., Consider fluid restriction/ diuretics if clinically indicated., , In those whom non operative treatment is failing; the correct treatment is laparotomy and, laparostomy. Options for laparostomy are many although the Bogota bag or VAC techniques are the, most widely practised. Re-look laparotomy and attempts at delayed closure will follow in due course., Next question
Page 2638 :
Theme: Surgical drains, , A., B., C., D., E., F., , Redivac suction drain, Corrugated drain, Wallace Robinson drain, Penrose tubing, Latex T Tube drain, Silastic T Tube drain, , Please select the most appropriate surgical drainage system for the indication given. Each option, may be used once, more than once or not at all., , 85., , A 56 year old lady undergoes and open cholecystectomy and exploration of common bile, duct. The bile duct is closed over a drain., You answered Redivac suction drain, The correct answer is Latex T Tube drain, Latex is used for this indication as it will encourage track formation., , 86., , A 48 year old lady undergoes a mastectomy and axillary node clearance for an invasive, ductal cancer of the breast with lymph node metastasis., Redivac suction drain, Suction drains are commonly used following mastectomy and axillary surgery to prevent, haematoma formation. Not all surgeons routinely drain the axilla., , 87., , A 75 year old man undergoes a hartmans procedure for sigmoid diverticular disease with, pericolic abscess and colovesical fistula., You answered Redivac suction drain, The correct answer is Wallace Robinson drain, These tube drains are often used in abdominal surgery to drain abscess cavities. Debate, might occur around the use of low pressure vs no suction in this setting so this option is, deliberately omitted., , Please rate this question:
Page 2639 :
Discuss and give feedback, , Next question, , Surgical drains, , , , , , , , Drains are inserted in many surgical procedures and are of many types., As a broad rule they can be divided into those using suction and those which do not., The diameter of the drain will depend upon the substance being drained, for example smaller, lumen drain for pneumothoraces vs haemothorax., Drains can be associated with complications and these begin with insertion when there may, be iatrogenic damage. When in situ they serve as a route for infections. In some specific, situations they may cause other complications, for example suction drains left in contact with, bowel for long periods may carry a risk of inducing fistulation., Drains should be inserted for a defined purpose and removed once the need has passed., , A brief overview of types of drain and sites is given below, CNS, , , Low suction drain or free drainage systems may be used for situations such as drainage of, sub dural haematomas., , CVS, , , Following cardiothoracic procedures of thoracic trauma underwater seal drains are often, placed. These should be carefully secured. When an air leak is present they may be placed, on suction whilst the air leak settles, , Orthopaedics and trauma, , , In this setting drains are usually used to prevent haematoma formation (with associated risk, of infection). Some orthopaedic drains may also be specially adapted to allow the drained, blood to be auto transfused., , Gastro-intestinal surgery, , , Surgeons often place abdominal drains either to prevent or drain abscesses, or to turn an, anticipated complication into one that can be easily controlled such as a bile leak following, cholecystectomy. The type of drain used will depend upon the indication., , Drain types
Page 2640 :
Type of drain, , Features, , Redivac, , , , , , Suction type of drain, Closed drainage system, High pressure vacuum system, , Low pressure, drainage systems, , , , Consist of small systems such as the lantern style drain that may be, used for short term drainage of small wounds and cavities, Larger systems are sometimes used following abdominal surgery,, they have a lower pressure than the redivac system, which decreases, the risks of fistulation, May be emptied and re-pressurised, , , , , , Latex tube drains, , , , , , May be shaped (e.g. T Tube) or straight, Usually used in non pressurised systems and act as sump drains, Most often used when it is desirable to generate fibrosis along the, drain track (e.g. following exploration of the CBD), , Chest drains, , , , , May be large or small diameter (depending on the indication), Connected to underwater seal system to ensure one way flow of air, , Corrugated drain, , , , , Thin, wide sheet of plastic, usually soft, Contains corrugations, along which fluids can track, Next question
Page 2641 :
What is the commonest site in the abdomen for fluid to collect following a perforated appendix?, , Pelvis, , Hepatorenal pouch, , Between small bowel loops, , Right iliac fossa, , Lesser sac, , Following perforated appendicitis fluid is most likely to accumulate in the pelvis. Fluid may, accumulate in the hepatorenal pouch although this is less common. Gravity favors the pelvis as the, site of most collections. The incidence of these is higher with laparoscopic rather than open surgery., Please rate this question:, , Discuss and give feedback, , Next question, , Appendicitis, History, , , , , , , Peri umbilical abdominal pain (visceral stretching of appendix lumen and appendix is mid gut, structure) radiating to the right iliac fossa due to localised parietal peritoneal inflammation., Vomit once or twice but marked and persistent vomiting is unusual., Diarrhoea is rare. However, pelvic appendicitis may cause localised rectal irritation and some, loose stools. A pelvic abscess may also cause diarrhoea., Mild pyrexia is common - temperature is usually 37.5 -38oC. Higher temperatures are more, typical of conditions like mesenteric adenitis., Anorexia is very common. It is very unusual for patients with appendicitis to be hungry., , Examination, , , , , Generalised peritonitis if perforation has occurred or localised peritonism., Retrocaecal appendicitis may have relatively few signs., Digital rectal examination may reveal boggy sensation if pelvic abscess is present, or even, tenderness with a pelvic appendix.
Page 2642 :
Diagnosis, , , , , Typically raised inflammatory markers coupled with compatible history and examination, findings should be enough to justify appendicectomy., Urine analysis may show mild leucocytosis but no nitrites., Ultrasound is useful in females where pelvic organ pathology is suspected. Although it is not, always possible to visualise the appendix on ultrasound, the presence of free fluid (always, pathological in males) should raise suspicion., , Ultrasound examination may show evidence of luminal obstruction and thickening of the appendiceal, wall as shown below, , Image sourced from Wikipedia, , Treatment, , , , , , , Appendicectomy which can be performed via either an open or laparoscopic approach., Administration of metronidazole reduces wound infection rates., Patients with perforated appendicitis require copious abdominal lavage., Patients without peritonitis who have an appendix mass should receive broad spectrum, antibiotics and consideration given to performing an interval appendicectomy., Be wary in the older patients who may have either an underlying caecal malignancy or, perforated sigmoid diverticular disease., , Laparoscopic appendicectomy is becoming increasing popular as demonstrated below
Page 2643 :
Image sourced from Wikipedia
Page 2644 :
Theme: Right iliac fossa pathology, , A., B., C., D., E., F., G., , Appendicitis, Mesenteric adenitis, Inflammatory bowel disease, Irritable bowel syndrome, Mesenteric cyst, Campylobacter infection, Appendix abscess, , Please select the most likely diagnosis for the scenario given. Each option may be used once, more, than once or not at all., , 89., , An 8 year old boy is examined by his doctor as part of a routine clinical examination. The, doctor notices a smooth swelling in the right iliac fossa. It is mobile and the patient is, otherwise well., You answered Appendicitis, The correct answer is Mesenteric cyst, Theme from April 2012 Exam, Mesenteric cysts are often smooth. Imaging with ultrasound and CT is usually sufficient., Although rare, they most often occur in young children (up to 30% present before the age, of 15). Many are asymptomatic and discovered incidentally. Acute presentations are, recognised and may occur following cyst torsion, infarction or rupture. Most cysts will be, surgically resected., , 90., , An 8 year old boy presents with abdominal pain,a twelve hour history of vomiting, a fever, of 38.3 oC and four day history of diarrhoea. His abdominal pain has been present for the, past week., You answered Appendicitis, The correct answer is Appendix abscess, The high fever and diarrhoea together with vomiting all point to a pelvic abscess. The, presence of pelvic pus is highly irritant to the rectum, and many patients in this situation, will complain of diarrhoea., , 91., , A 7 year old boy presents with a three day history of right iliac fossa pain and fever. On, examination he has a temperature of 39.9o C. His abdomen is soft and mildly tender in the, right iliac fossa.
Page 2645 :
You answered Appendicitis, The correct answer is Mesenteric adenitis, High fever and mild abdominal signs in a younger child should raise suspicion for, mesenteric adenitis. The condition may mimic appendicitis and many may require surgery., Please rate this question:, , Discuss and give feedback, , Next question, , Right iliac fossa pain, Differential diagnosis, , Appendicitis, , , , , , , Pain radiating to right iliac fossa, Anorexia (very common), Short history, Diarrhoea and profuse vomiting rare, , Crohn's disease, , , , , , Often long history, Signs of malnutrition, Change in bowel habit, especially diarrhoea, , Mesenteric adenitis, , , , , Mainly affects children, Causes include Adenoviruses, Epstein Barr Virus, betahaemolytic Streptococcus, Staphylococcus spp., Escherichia, coli,Streptococcus viridans and Yersinia spp., Patients have a higher temperature than those with appendicitis, If laparotomy is performed, enlarged mesenteric lymph nodes will, be present, , , , , Diverticulitis, , , , , , Both left and right sided disease may present with right iliac fossa, pain, Clinical history may be similar, although some change in bowel, habit is usual, When suspected, a CT scan may help in refining the diagnosis, , , , A Meckel's diverticulum is a congenital abnormality that is present, , , , Meckel's
Page 2646 :
diverticulitis, , , , in about 2% of the population, Typically 2 feet proximal to the ileocaecal valve, May be lined by ectopic gastric mucosal tissue and produce, bleeding, , Perforated peptic, ulcer, , , , , This usually produces upper quadrant pain but pain may be lower, Perforations typically have a sharp sudden onset of pain in the, history, , Incarcerated right, inguinal or femoral, hernia, , , , Usually only right iliac fossa pain if right sided or bowel, obstruction., , Bowel perforation, secondary to caecal, or colon carcinoma, , , , Seldom localised to right iliac fossa, although complete large bowel, obstruction with caecal distension may cause pain prior to, perforation., , Gynaecological, causes, , , , Pelvic inflammatory disease/salpingitis/pelvic abscess/Ectopic, pregnancy/Ovarian torsion/Threatened or complete, abortion/Mittelschmerz, , Urological causes, , , , Ureteric colic/UTI/Testicular torsion, , Other causes, , , , TB/Typhoid/Herpes Zoster/AAA/Situs inversus
Page 2647 :
A 56 year old man undergoes a difficult splenectomy and is left with a pancreatic fistula. There are, ongoing problems with very high fistula output. Which of the following agents may be administered to, reduce the fistula output?, , Metoclopramide, , Erthyromycin, , Octreotide, , Loperamide, , Omeprazole, , Octreotide is a useful agent in reducing the output from pancreatic fistulae. Prokinetic agents will, increase fistula output and should be avoided., Please rate this question:, , Discuss and give feedback, , Next question, , Fistulas, , , , , , A fistula is defined as an abnormal connection between two epithelial surfaces., There are many types ranging from Branchial fistulae in the neck to entero-cutaneous, fistulae abdominally., In general surgical practice the abdominal cavity generates the majority and most of these, arise from diverticular disease and Crohn's., As a general rule all fistulae will resolve spontaneously as long as there is no distal, obstruction. This is particularly true of intestinal fistulae., , The four types of fistulae are:, Enterocutaneous, These link the intestine to the skin. They may be high (>500ml) or low output (<250ml) depending, upon source. Duodenal /jejunal fistulae will tend to produce high volume, electrolyte rich secretions, which can lead to severe excoriation of the skin. Colo-cutaneous fistulae will tend to leak faeculent, material. Both fistulae may result from the spontaneous rupture of an abscess cavity onto the skin, (such as following perianal abscess drainage) or may occur as a result of iatrogenic input. In some, cases it may even be surgically desirable e.g. mucous fistula following sub total colectomy for colitis.
Page 2648 :
Suspect if there is excess fluid in the drain., Enteroenteric or Enterocolic, This is a fistula that involves the large or small intestine. They may originate in a similar manner to, enterocutaneous fistulae. A particular problem with this fistula type is that bacterial overgrowth may, precipitate malabsorption syndromes. This may be particularly serious in inflammatory bowel, disease., Enterovaginal, Aetiology as above., Enterovesicular, This type of fistula goes to the bladder. These fistulas may result in frequent urinary tract infections,, or the passage of gas from the urethra during urination., Management, Some rules relating to fistula management:, , , , , , , , , They will heal provided there is no underlying inflammatory bowel disease and no distal, obstruction, so conservative measures may be the best option, Where there is skin involvement, protect the overlying skin, often using a well fitted stoma, bag- skin damage is difficult to treat, A high output fistula may be rendered more easily managed by the use of octreotide, this will, tend to reduce the volume of pancreatic secretions., Nutritional complications are common especially with high fistula (e.g. high jejunal or, duodenal) these may necessitate the use of TPN to provide nutritional support together with, the concomitant use of octreotide to reduce volume and protect skin., When managing perianal fistulae surgeons should avoid probing the fistula where acute, inflammation is present, this almost always worsens outcomes., When perianal fistulae occur secondary to Crohn's disease the best management option is, often to drain acute sepsis and maintain that drainage through the judicious use of setons, whilst medical management is implemented., Always attempt to delineate the fistula anatomy, for abscesses and fistulae that have an intra, abdominal source the use of barium and CT studies should show a track. For perianal, fistulae surgeons should recall Goodsall's rule in relation to internal and external openings.
Page 2649 :
Theme: Inguinal hernia management, , A., B., C., D., E., F., , Bassini repair, Inguinal herniotomy, Lichtenstein repair, Laparoscopic hernia repair, Shouldice repair, McVey repair, , For the herniae described please select the most appropriate procedure from the list. Each option, may be used once, more than once or not at all., , 93., , A 11 month old child presents with intermittent groin swelling, it has a cough impulse and, is easily reducible., You answered Bassini repair, The correct answer is Inguinal herniotomy, Infants usually suffer from a patent processus vaginalis (a congential problem). As a result, a simple herniotomy is all that is required. A mesh is not required as there is not specific, muscle weakness., , 94., , A 25 year old builder presents with a reducible swelling in the right groin, it is becoming, larger and has not been operated on previously., You answered Bassini repair, The correct answer is Lichtenstein repair, An open Lichtenstein repair using mesh is appropriate. There is a 0.77% recurrence rate, with this technique. A Shouldice repair is an acceptable alternative if the surgeon is, experienced, , 95., , A 28 year old man presents with a recurrent inguinal hernia on the left side of his abdomen, and a newly diagnosed inguinal hernia on the right side., You answered Bassini repair, The correct answer is Laparoscopic hernia repair, Laparoscopic hernia repairs are specifically indicated where there are bilateral hernias or, recurrence of a previous open repair.
Page 2650 :
Please rate this question:, , Discuss and give feedback, , Next question, , Inguinal hernia surgery, Inguinal hernias occur when the abdominal viscera protrude through the anterior abdominal wall into, the inguinal canal. They may be classified as being either direct or indirect. The distinction between, these two rests on their relation to Hesselbach's triangle., Boundaries of Hesselbach's Triangle, , , , , Medial: Rectus abdominis, Lateral: Inferior epigastric vessels, Inferior: Inguinal ligament, , Image sourced from Wikipedia, , Hernias occurring within the triangle tend to be direct and those outside - indirect., Diagnosis
Page 2651 :
Most cases are diagnosed clinically, a reducible swelling may be located at the level of the inguinal, canal. Large hernia's may extend down into the male scrotum, these will not trans-illuminate and it is, not possible to "get above" the swelling., Cases that are unclear on examination, but suspected from the history, may be further investigated, using ultrasound or by performing a herniogram., Treatment, Hernias associated with few symptoms may be managed conservatively. Symptomatic hernias or, those which are at risk of developing complications are usually treated surgically., First time hernias may be treated by performing an open inguinal hernia repair; the inguinal canal is, opened, the hernia reduced and the defect repaired. A prosthetic mesh may be placed posterior to, the cord structures to re-enforce the repair and reduce the risk of recurrence., Recurrent hernias and those which are bilateral are generally managed with a laparoscopic, approach. This may be via an intra or extra peritoneal route. As in open surgery a mesh is deployed., However, it will typically lie posterior to the deep ring., Inguinal hernia in children, Inguinal hernias in children are almost always of an indirect type and therefore are usually dealt with, by herniotomy, rather than herniorraphy. Neonatal hernias especially in those children born, prematurely are at highest risk of strangulation and should be repaired urgently. Other hernias may, be repaired on an elective basis., References, The UK Based National Institute of Clinical Excellence has published guidelines relating to the, choice between open and laparoscopic inguinal hernia repair. Which users may find interesting:, http://guidance.nice.org.uk/TA83/Guidance/pdf/English
Page 2652 :
Theme: Surgical access, , A., B., C., D., E., F., G., , Kocher's, Lanz, Rooftop, Pfannenstiel's, Midline, Paramedian incision, Mcevedy, , Please select the most appropriate incision for the procedure described. Each option may be used, once, more than once or not at all., , 96., , A 19 year old girl who is 39 weeks pregnant goes into labour. The labour is prolonged and, she is found to have an undiagnosed breech baby., You answered Kocher's, The correct answer is Pfannenstiel's, This patient needs an emergency cesarean section., , 97., , A 49 year old woman presents with jaundice and abdominal pain. She is, haemodynamically unstable. An USS shows a dilated common bile duct and gallstones in, the gallbladder., Kocher's, This lady needs a cholecystectomy and bile duct exploration., , 98., , A 42 year old man with history of alcohol abuse is diagnosed with pancreatic cancer and, requires a Whipples resection., You answered Kocher's, The correct answer is Rooftop, A pancreatectomy is usually performed through a roof top incision. This provides, excellent access to the upper abdomen., , Please rate this question:
Page 2653 :
Discuss and give feedback, , Abdominal incisions, Midline incision, , , , , , Paramedian, incision, , , , , , , Battle, , , , , Commonest approach to the abdomen, Structures divided: linea alba, transversalis fascia, extraperitoneal fat,, peritoneum (avoid falciform ligament above the umbilicus), Bladder can be accessed via an extraperitoneal approach through the, space of Retzius, Parallel to the midline (about 3-4cm), Structures divided/retracted: anterior rectus sheath, rectus (retracted),, posterior rectus sheath, transversalis fascia, extraperitoneal fat,, peritoneum, Incision is closed in layers, Similar location to paramedian but rectus displaced medially (and thus, denervated), Now seldom used, , Kocher's, , Incision under right subcostal margin e.g. Cholecystectomy (open), , Lanz, , Incision in right iliac fossa e.g. Appendicectomy, , Gridiron, , Oblique incision centered over McBurneys point- usually appendicectomy, (less cosmetically acceptable than Lanz, , Gable, , Rooftop incision, , Pfannenstiel's, , Transverse supra pubic, primarily used to access pelvic organs, , McEvedy's, , Groin incision e.g. Emergency repair strangulated femoral hernia, , Rutherford, Morrison, , Extraperitoneal approach to left or right lower quadrants. Gives excellent, access to iliac vessels and is the approach of choice for first time renal, transplantation.
Page 2654 :
Image sourced from Wikipedia
Page 2656 :
Theme: Causes of dysphagia, , A., B., C., D., E., F., G., H., , Benign oesophageal stricture, Globus, Carcinoma of the oesophagus, Achalasia, Hiatus hernia, Pharyngeal pouch, Oesophageal web, Oesophageal atresia, , Please select the the most likely cause of swallowing difficulties for the scenarios described. Each, option may be used once, more than once or not at all., , 1., , A 55 year old man presents with a history of progressive dysphagia over the past 4 weeks., For the preceding 5 years he had regularly attended his general practitioner with symptoms, of dyspepsia and reflux., You answered Benign oesophageal stricture, The correct answer is Carcinoma of the oesophagus, Theme from January 2013 Exam, A short history of progressive dysphagia in a middle aged man who has a background, history of reflux is strongly suggestive of malignancy. Long standing reflux symptoms may, be suggestive of a increased risk of developing Barretts oesophagus. Note that not all, patients with Barretts transformation alone are symptomatic., , 2., , A 40 year old man presents with symptoms of dysphagia that have been present for many, months. His investigations demonstrate lack of relaxation of the lower oesophageal, sphincter during swallowing., You answered Benign oesophageal stricture, The correct answer is Achalasia, Patients with dysphagia will usually undergo an upper GI endoscopy as a first line, investigation. Where this investigation is normal, the next stage is to perform studies, assessing oesophageal motility. These comprise fluroscopic barium swallows and, oesophageal manometry and pH studies. Lack of sphincter relaxation suggests achalasia, (pressures are usually high)., , 3., , A 4 year old presents with sudden onset of dysphagia. He undergoes an upper GI endoscopy, and a large bolus of food is identified in the mid oesophagus. He has no significant history,
Page 2657 :
other than a tracheo-oesophageal fistula repair soon after birth., Benign oesophageal stricture, Children with tracheo-oesophageal fistulas will commonly develop oesophageal strictures, following repair. These may require regular dilations throughout childhood., Please rate this question:, , Discuss and give feedback, , Next question, , Dysphagia, Causes of dysphagia, , Extrinsic, , , , , Mediastinal masses, Cervical spondylosis, , Oesophageal wall, , , , , , Achalasia, Diffuse oesophageal spasm, Hypertensive lower oesophageal sphincter, , Intrinsic, , , , , , , Tumours, Strictures, Oesophageal web, Schatzki rings, , Neurological, , , , , , , , CVA, Parkinson's disease, Multiple Sclerosis, Brainstem pathology, Myasthenia Gravis, , Investigation, All patients require an upper GI endoscopy unless there are compelling reasons for this not to be, performed. Motility disorders may be best appreciated by undertaking fluoroscopic swallowing, studies., A full blood count should be performed.
Page 2658 :
Ambulatory oesophageal pH and manometry studies will be required to evaluate conditions such as, achalasia and patients with GORD being considered for fundoplication surgery., Next question
Page 2659 :
A 45 year old man undergoes an upper gastrointestinal endoscopy for a benign oesophageal, stricture. This is dilated and he suffers an iatrogenic perforation at the site. His imaging shows a, small contained leak and a small amount of surgical emphysema. What is the most appropriate, nutritional option?, , Nil by mouth and intravenous fluids alone, , Intravenous fluids and sips orally, , Total parenteral nutrition, , Nasogastric feeding, , PEG tube feeding, , Theme from April 2013 Exam, Iatrogenic perforations of the oesophagus may be managed non operatively. This usually involves a, nil by mouth regime, tube thoracostomy may be needed. Total parenteral nutrition is the safest, option. Insertion of NG feeding tubes and PEG tubes may complicate the process or allow feed to, enter the perforation site., Please rate this question:, , Discuss and give feedback, , Next question, , Nutrition options in surgical patients, Oral intake, , , , , , Easiest option, May be supplemented by calorie rich dietary supplements, May contra indicated following certain procedures, , Naso gastric feeding, , , , , , , Usually administered via fine bore naso gastric feeding tube, Complications relate to aspiration of feed or misplaced tube, May be safe to use in patients with impaired swallow, Often contra indicated following head injury due to risks, associated with tube insertion
Page 2660 :
Naso jejunal feeding, , , , , , Feeding jejunostomy, , , , , , , Percutaneous, endoscopic, gastrostomy, , , , , , Total parenteral, nutrition, , , , , , , Avoids problems of feed pooling in stomach (and risk of, aspiration), Insertion of feeding tube more technically complicated (easiest, if done intra operatively), Safe to use following oesophagogastric surgery, Surgically sited feeding tube, May be used for long term feeding, Low risk of aspiration and thus safe for long term feeding, following upper GI surgery, Main risks are those of tube displacement and peritubal leakage, immediately following insertion, which carries a risk of, peritonitis, Combined endoscopic and percutaneous tube insertion, May not be technically possible in those patients who cannot, undergo successful endoscopy, Risks include aspiration and leakage at the insertion site, The definitive option in those patients in whom enteral feeding, is contra indicated, Individualised prescribing and monitoring needed, Should be administered via a central vein as it is strongly, phlebitic, Long term use is associated with fatty liver and deranged LFT's, Next question
Page 2661 :
A 38 year old women undergoes a gastric bypass procedure. Post operatively she attends the clinic, and complains that following a meal she develops vertigo and develops crampy abdominal pain., What is the most likely underlying explanation?, , Insulin resistance, , Irritable bowel syndrome, , Biliary colic, , Dumping syndrome, , Enterogastric reflux, , Dumping syndrome, which can be divided into early and late, may occur following gastric surgery. It, occurs as a result of a hyperosmolar load rapidly entering the proximal jejunum. Osmosis drags, water into the lumen, this results in lumen distension (pain) and then diarrhoea. Excessive insulin, release also occurs and results in hypoglycaemic symptoms., Please rate this question:, , Discuss and give feedback, , Next question, , Post gastrectomy syndromes, Post gastrectomy syndromes may vary slightly depending upon whether a total of partial, gastrectomy is performed. A Roux en Y reconstruction generally gives the best functional outcomes., Where a gastrojejunostomy is performed as reconstruction following a distal gastrectomy the gastric, emptying is generally better if the jejunal limbs are tunneled in the retrocolic plane., The following may occur following gastrectomy:, , , , , , , , , Small capacity (early satiety), Dumping syndrome, Bile gastritis, Afferent loop syndrome, Efferent loop syndrome, Anaemia (B12 deficiency), Metabolic bone disease, Next question
Page 2662 :
A 63 year old man undergoes an upper GI endoscopy and adrenaline injection for a large actively, bleeding duodenal ulcer. He remains stable for 6 hours and the nurses then call because he has, passed 400ml malaena and has become tachycardic (pulse rate 120) and hypotensive (Bp 80/40)., What is the best option?, , Reassure that blood trapped in the upper portion of the gastrointestinal system will pass, and that this episode will resolve with phosphate enema, Perform a repeat upper GI endoscopy, , Perform a laparotomy and under-running of the ulcer, , Administer tranexamic acid and intravenous proton pump inhibitors, , Insert a Minnesota tube, , The decision as to how best to manage patients with re-bleeding is difficult. Whilst it is tempting to, offer repeat endoscopy, this intervention is best used on those with small ulcers. Large posteriorly, sited duodenal ulcers are at high risk for re-bleeding and the timeframe of this event suggests that, primary endoscopic haemostasis was inadequate. Surgery thus represents the safest way forward., Please rate this question:, , Discuss and give feedback, , Next question, , Upper gastrointestinal bleeding, Patients may present with the following:, , , , , Haematemesis and/ or malaena, Epigastric discomfort, Sudden collapse, , The extent to which these will occur will depend upon the source. Mortality is higher in patients, presenting with haematemesis than malaena alone., Oesophageal bleeding, , Cause, , Presenting features
Page 2663 :
Oesophagitis, , Small volume of fresh blood, often streaking vomit. Malaena rare. Often ceases, spontaneously. Usually history of antecedent GORD type symptoms., , Cancer, , Usually small volume of blood, except as pre terminal event with erosion of, major vessels. Often associated symptoms of dysphagia and constitutional, symptoms such as weight loss. May be recurrent until malignancy managed., , Mallory Weiss, Tear, , Typically brisk small to moderate volume of bright red blood following bout of, repeated vomiting. Malaena rare. Usually ceases spontaneously., , Varices, , Usually large volume of fresh blood. Swallowed blood may cause malaena., Often associated with haemodynamic compromise. May stop spontaneously but, re-bleeds are common until appropriately managed., , Gastric Bleeding, , Cause, , Presenting features, , Gastric, cancer, , May be frank haematemesis or altered blood mixed with vomit. Usually, prodromal features of dyspepsia and may have constitutional symptoms. Amount, of bleeding variable but erosion of major vessel may produce considerable, haemorrhage., , Dieulafoy, Lesion, , Often no prodromal features prior to haematemesis and malaena, but this, arteriovenous malformation may produce quite considerable haemorrhage and, may be difficult to detect endoscopically., , Diffuse, erosive, gastritis, , Usually haematemesis and epigastric discomfort. Usually there is an underlying, cause such as recent NSAID usage. Large volume haemorrhage may occur with, considerable haemodynamic compromise., , Gastric ulcer, , Small low volume bleeds more common so would tend to present as iron, deficiency anaemia. Erosion into a significant vessel may produce considerable, haemorrhage and haematemesis., , Duodenum, Most common cause of major haemorrhage is a posteriorly sited duodenal ulcer. However, ulcers at
Page 2664 :
any site in the duodenum may present with haematemesis, malaena and epigastric discomfort. The, pain of duodenal ulcer is slightly different to that of gastric ulcers and often occurs several hours, after eating. Peri ampullary tumours may bleed but these are rare. In patients with previous, abdominal aortic aneurysm surgery aorto-enteric fistulation remains a rare but important cause of, major haemorrhage associated with high mortality., Management, , , , , , , , , , , , , , , , Admission to hospital careful monitoring, cross match blood, check FBC, LFTs, U+E and, Clotting (as a minimum), Patients with on-going bleeding and haemodynamic instability are likely to require O negative, blood pending cross matched blood, Early control of airway is vital (e.g. Drowsy patient with liver failure), Patients with suspected varices should receive terlipressin prior to endoscopy, Ideally all patients admitted with upper gastrointestinal haemorrhage should undergo Upper, GI endoscopy within 24 hours of admission. In those who are unstable this should occur, immediately after resuscitation or in tandem with it. The endoscopy department is a, potentially dangerous place for unstable patients and it may be safer to perform the, endoscopy in theatre with an anaesthetist present., Varices should be banded or subjected to sclerotherapy. If this is not possible owing to active, bleeding then a Sengaksten- Blakemore tube (or Minnesota tube) should be inserted. This, should be done with care; gastric balloon should be inflated first and oesophageal balloon, second. Remember the balloon will need deflating after 12 hours (ideally sooner) to prevent, necrosis. Portal pressure should be lowered by combination of medical therapy +/- TIPSS., Patients with erosive oesophagitis / gastritis should receive a proton pump inhibitor., Mallory Weiss tears will typically resolve spontaneously, Identifiable bleeding points should receive combination therapy of injection of adrenaline and, either a thermal or mechanical treatment. All who have received intervention should receive, a continuous infusion of a proton pump inhibitor (IV omeprazole for 72 hours) to reduce the, re-bleeding rate., Patients with diffuse erosive gastritis who cannot be managed endoscopically and continue, to bleed may require gastrectomy, Bleeding ulcers that cannot be controlled endoscopically may require laparotomy and ulcer, underruning, , Indications for surgery, , , , , , Patients > 60 years, Continued bleeding despite endoscopic intervention, Recurrent bleeding, Known cardiovascular disease with poor response to hypotension, , Surgery, Duodenal ulcer, Laparotomy, duodenotomy and under running of the ulcer. If bleeding is brisk then the ulcer is, almost always posteriorly sited and will have invaded the gastroduodenal artery. Large bites using 0, Vicryl are taken above and below the ulcer base to occlude the vessel. The duodenotomy should be, longitudinal but closed transversely to avoid stenosis.
Page 2665 :
For gastric ulcer, Under-running of the bleeding site, Partial gastrectomy-antral ulcer, Partial gastrectomy or under running the ulcer- lesser curve ulcer (involving left gastric artery), Total gastrectomy if bleeding persists, Summary of Acute Upper GI bleeding recommendations:, The need for admission and timing of endoscopic intervention may be predicted by using the, Blatchford score. This considers a patients Hb, serum urea, pulse rate and blood pressure. Those, patients with a score of 0 are low risk, all others are considered high risk and require admission and, endoscopy., The requirement for pre endoscopic proton pump inhibition is contentious. In the UK the National, Institute of Clinical Excellence guidelines suggest the pre endoscopic PPI therapy is unnecessary., Whilst it is accepted that such treatment has no impact on mortality or morbidity a Cochrane review, of this practice in 2007 did suggest that it reduced the stigmata of recent haemorrhage at, endoscopy. As a result many will still administer PPI to patients prior to endoscopic intervention., Following endoscopy it is important to calculate the Rockall score for patients to determine their risk, of rebleeding and mortality. A score of 3 or less is associated with a rebleeding rate of 4% and a, very low risk of mortality and identifies a group of patients suitable for early discharge., References, 1. http://www.sign.ac.uk/guidelines/fulltext/105/index.html, 2. Joint Advisory Group on Endoscopy (JAG) Guidelines - http://www.thejag.org.uk, 3. NICE Guideline: Management of acute upper GI bleeding. July 2012., Next question
Page 2666 :
Theme: Oesophgeal disease, , A. Schatzki ring, B. Plummer Vinson syndrome, C. Squamous cell carcinoma, D. Barretts oesophagus, E. Pharyngeal pouch, F. Adenocarcinoma, G. Leiomyoma, H. Oesophageal rupture, I. Diffuse oesophageal spasm, J. Hiatus hernia, , Please select the most likely underlying diagnosis for the scenario described. Each option may be, used once, more than once or not at all., , 7., , A 56 year old man who drinks heavily is found collapsed by friends at his house. He was out, drinking the previous night and following this was noted to have vomited repeatedly so his friends, brought him home., You answered Schatzki ring, The correct answer is Oesophageal rupture, Spontaneous rupture of the oesophagus may occur following an episode of vomiting. The, subsequent mediastinitis can produce severe sepsis and death if not treated promptly. Adequate, drainage of sepsis and early surgery are the cornerstones of management., , 8., , A 43 year old man has been troubled with dysphagia for many years. He is known to have achalasia, and has had numerous dilatations. Over the past 6 weeks his dysphagia has worsened. At, endoscopy a friable mass is noted in the oesophagus.
Page 2667 :
You answered Schatzki ring, The correct answer is Squamous cell carcinoma, The risk of squamous cell carcinoma of the oesophagus is increased in people with achalasia. The, condition often presents late and has a poor prognosis., , 9., , A 73 year old lady is troubled by episodic swallowing difficulty and halitosis. An upper GI, endoscopy is attempted and abandoned due to difficulty in achieving intubation., You answered Schatzki ring, The correct answer is Pharyngeal pouch, Pharyngeal pouches occur when a defect occurs in killians dehiscence. Difficulty in intubation is a, well recognised consequence and care must be taken to take the correct track during OGD to avoid, perforation. Most cases are now treated with endoscopic stapling., , Please rate this question:, , Discuss and give feedback, , Next question, , Oesophageal disease, Disorder, , Features, , Mallory-Weiss Tear, , Usually history of antecedent vomiting. This is then followed by the vomiting of a, small amount of blood. There is usually little in the way of systemic disturbance, or prior symptoms.
Page 2668 :
Disorder, , Features, , Hiatus hernia of, gastric cardia, , Often longstanding history of dyspepsia, patients are often overweight., Uncomplicated hiatus hernias should not be associated with dysphagia or, haematemesis., , Oesophageal rupture, , Complete disruption of the oesophageal wall in absence of pre-existing, pathology. Left postero-lateral oesophageal is commonest site (2-3cm from OG, junction). Suspect in patients with severe chest pain without cardiac diagnosis, and signs suggestive of pneumonia without convincing history, where there is, history of vomiting. Erect CXR shows infiltrate or effusion in 90% of cases(1)., , Squamous cell, carcinoma of the, oesophagus, , History of progressive dysphagia. Often signs of weight loss. Usually little or no, history of previous GORD type symptoms., , Adenocarcinoma of, the oesophagus, , Progressive dysphagia, may have previous symptoms of GORD or Barretts, oesophagus., , Peptic stricture, , Longer history of dysphagia, often not progressive. Usually symptoms of GORD., Often lack systemic features seen with malignancy, , Dysmotility disorder, , May have dysphagia that is episodic and non progressive. Retrosternal pain may, accompany the episodes., , Diagnosis, Most of the differential diagnoses listed above can be accurately categorised by upper GI endoscopy, (usually most patients). Where this fails to demonstrate a mechanical stricture the use of pH and, manometry studies together with radiological contrast swallows will facilitate the diagnosis., References, Blencowe N et al. Spontaneous oesophageal rupture. BMJ 2013 (346):38-39., Next question
Page 2669 :
A 55 year old man presents with symptoms of dyspepsia and on upper GI endoscopy an area of, patchy erythematous tissue is identified protruding proximally from the gastro oesophageal junction., Biopsies are diagnostic of Barretts oesophagus with low grade dysplasia. Which of the following is, the most appropriate management?, , Distal oesophagectomy, , Upper GI endoscopy with quadrantic biopsies from the region, , Photodynamic therapy, , Endoscopic sub mucosal resection of the area, , Argon plasma coagulation, In Barrett's surveillance the safest option is quadrantic (i.e. 4 biopsies, one from each quarter of the, oesophagus at 2cm intervals), Low grade dysplasia in conjunction with Barretts oesphagus should be monitored with regular (6, monthly) upper GI endoscopy and quadrantic biopsies. If the disease remains static at 2 years then, the screening frequency may be decreased., Please rate this question:, , Discuss and give feedback, , Next question, , Barrett's oesophagus, Barretts oesophagus is a condition characterised by the metaplastic transformation of squamous, oesophageal epithelium to columnar gastric type epithelium. Three types of this metaplastic process, are recognised; intestinal (high risk), cardiac and fundic. The latter two categories may cause, difficulties in diagnosis. The most concrete diagnosis can be made when endoscopic features of, Barretts oesophagus are present together with a deep biopsy that demonstrates not just goblet cell, metaplasia but also oesophageal glands., Barrett's can be sub divided into short (<3cm) and long (>3cm). The length of the affected segment, correlates strongly with the chances of identifying metaplasia. The overall prevalence of Barrett's, oesophagus is difficult to determine but may be in the region of 1 in 20 and is identified in up to 12%, of those undergoing endoscopy for reflux., A proportion of patients with metaplasia will progress to dysplasia and for this reason individuals, identified as having Barrett's should undergo endoscopic surveillance (every 2-5 years). Biopsies
Page 2670 :
should be quadrantic and taken at 1-2cm intervals. Biopsies need to be adequate. Where mass, lesions are present consideration should be given to endoscopic sub mucosal resection. Up to 40%, of patients will be upstaged from high grade dysplasia to invasive malignancy with such techniques., Treatment, , , , , , Long term proton pump inhibitor, Consider pH and manometry studies in younger patients who may prefer to consider an anti, reflux procedure, Regular endoscopic monitoring (more frequently if moderate dysplasia). With quadrantic, biopsies every 2-3 cm, If severe dysplasia be very wary of small foci of cancer, , References, A consensus statement of the British approach is provided by:, Bennett C et al Consensus Statements for Management of Barrett's Dysplasia and Early-Stage, Esophageal Adenocarcinoma, Based on a Delphi Process. Gastroenterology Volume 143, Issue 2 ,, Pages 336-346, August 2012., Next question
Page 2671 :
Theme: Causes of dysphagia, , A., B., C., D., E., F., G., , Adenocarcinoma of the oesophagus, Plummer Vinson syndrome, Squamous cell carcinoma of the oesophagus, Achalasia, Benign oesophageal stricture, Pharyngeal pouch, Tracheo-oesophageal fistula, , Please select the most likely underlying cause for dysphagia from the scenario given. Each option, may be used once, more than once or not at all., , 11., , A 78 year old lady presents with episodic dysphagia and halitosis, occasionally she, complains of regurgitation. A recent attempted upper GI endoscopy was poorly tolerated, and abandoned., You answered Adenocarcinoma of the oesophagus, The correct answer is Pharyngeal pouch, This is a pulsion type diverticulum through Killians dehiscence. Patients often complain of, regurgitation of foul smelling liquid. Upper GI endoscopy is potentially hazardous and, may result in iatrogenic perforation., , 12., , An overweight 56 year old man with longstanding Barrett's oesophagus complains of, worsening dysphagia to solids over the past 6 weeks., Adenocarcinoma of the oesophagus, Barrett's metaplasia places patients at increased risk of adenocarcinoma of the oesophagus., Small localised lesions and in situ disease has been treated by endoscopic mucosal, resection and photodynamic therapy. In many centres oesophagectomy is still offered as, the safest and standard treatment. Where dysphagia is present, a significant lesion, (requiring resection if operable) is invariably found., , 13., , A 24 year old man complains of occasional retrosternal chest pain and dysphagia that, occurs to both liquids and solids. He is otherwise well., You answered Adenocarcinoma of the oesophagus, The correct answer is Achalasia
Page 2672 :
This is an atypical cause of these symptoms. Diagnosis is made by upper GI endoscopy,, barium swallow and manometry/ pH studies. Treatments range from botulinum toxin, injection through to Hellers Cardiomyotomy that may be performed laparoscopically., Please rate this question:, , Discuss and give feedback, , Next question, , Dysphagia, Causes of dysphagia, , Extrinsic, , , , , Mediastinal masses, Cervical spondylosis, , Oesophageal wall, , , , , , Achalasia, Diffuse oesophageal spasm, Hypertensive lower oesophageal sphincter, , Intrinsic, , , , , , , Tumours, Strictures, Oesophageal web, Schatzki rings, , Neurological, , , , , , , , CVA, Parkinson's disease, Multiple Sclerosis, Brainstem pathology, Myasthenia Gravis, , Investigation, All patients require an upper GI endoscopy unless there are compelling reasons for this not to be, performed. Motility disorders may be best appreciated by undertaking fluoroscopic swallowing, studies., A full blood count should be performed., Ambulatory oesophageal pH and manometry studies will be required to evaluate conditions such as, achalasia and patients with GORD being considered for fundoplication surgery., Next question
Page 2673 :
A 58 year old lady has a two year history of worsening dysphagia. In addition to this she has a, nocturnal cough. Over this time she has lost a total of 8kg in weight. Which of the processes below is, the most likely explanation for this?, , Gastro-oesophageal reflux disease, , Barretts oesophagus, , Carcinoma, , Mallory Weiss tear, , Achalasia, , Theme from April 2013 Exam, Such marked weight loss should arouse suspicion of cancer. She is most likely to have a, longstanding stricture associated with oesophagitis and Barretts oesophagus. This may progress to, carcinoma which will tend to occur in association with worsening dysphagia and weight loss., Please rate this question:, , Discuss and give feedback, , Next question, , Oesophageal cancer, , , , , , , Incidence is increasing, In most cases in the Western world this increase is accounted for by a rise in the number of, cases of adenocarcinoma. In the UK adenocarcinomas account for 65% of cases., Barretts oesophagus is a major risk factor for most cases of oesophageal adenocarcinoma., In other regions of the world squamous cancer is more common and is linked to smoking,, alcohol intake, diets rich in nitrosamines and achalasia., Surveillance of Barretts is important, as it imparts a 30 fold increase in cancer risk and if, invasive malignancy is diagnosed early then survival may approach 85% at 5 years., , Diagnosis, , , , Upper GI endoscopy is the first line test, Contrast swallow may be of benefit in classifying benign motility disorders but has no place, in the assessment of tumours
Page 2674 :
, , , , Staging is initially undertaken with CT scanning of the chest, abdomen and pelvis. If overt, metastatic disease is identified using this modality then further complex imaging is, unnecessary, If CT does not show metastatic disease, then local stage may be more accurately assessed, by use of endoscopic ultrasound., Staging laparoscopy is performed to detect occult peritoneal disease. PET CT is performed, in those with negative laparoscopy. Thoracoscopy is not routinely performed., , Treatment, Operable disease is best managed by surgical resection. The most standard procedure is an IvorLewis type oesophagectomy. This procedure involves the mobilisation of the stomach and division of, the oesophageal hiatus. The abdomen is closed and a right sided thoracotomy performed. The, stomach is brought into the chest and the oesophagus mobilised further. An intrathoracic, oesophagogastric anastomosis is constructed. Alternative surgical strategies include a transhiatal, resection (for distal lesions), a left thoraco-abdominal resection (difficult access due to thoracic, aorta) and a total oesophagectomy (McKeown) with a cervical oesophagogastric anastomosis., The biggest surgical challenge is that of anastomotic leak, with an intrathoracic anastomosis this will, result in mediastinitis. With high mortality. The McKeown technique has an intrinsically lower, systemic insult in the event of anastomotic leakage., In addition to surgical resection many patients will be treated with adjuvant chemotherapy., Next question
Page 2675 :
Theme: Management of oesophageal cancer, , A., B., C., D., E., F., G., H., , Endo lumenal brachytherapy, Chemo-radiotherapy, Radiotherapy alone, Insertion of expanding metallic stent, Ivor-Lewis oesophagectomy, Total oesophagectomy, Segmental resection of mid oesophagus, Endoscopic mucosal resection, , Please select the most appropriate intervention for the following patients with oesophageal cancer., Each option may be used once, more than once or not at all., , 15., , A 58 year old man with long standing Barretts oesophagus is found to have a nodule on, endoscopic surveillence. Biopsies and endoscopic USS suggest this is at most a 1cm foci, of T1 disease in the distal oesophagus 4 cm proximal to the oesophagogastric junction., You answered Endo lumenal brachytherapy, The correct answer is Endoscopic mucosal resection, EMR is an reasonable option for small areas of malignancy occurring on a background of, Barretts change. Segmental resections of the oesophagus are not practised and the only, resectional strategy in this scenario would be an Ivor- Lewis type resection. The morbidity, such a strategy in T1 disease is probably not justified., , 16., , An 82 year old man presents with dysphagia and on investigation is found to have a, stenosing tumour of the mid oesophagus with a single mestastasis in the right lobe of the, liver (segment VI)., You answered Endo lumenal brachytherapy, The correct answer is Insertion of expanding metallic stent, Distant disease in patients with oesophageal cancer is a contra indication to a resectional, strategy and downstaging with chemotherapy is not routinely undertaken in this age group, as the results are poor. An expanding stent will provide rapid and durable palliation., , 17., , A 56 year old man presents with odynophagia and on investigation is found to have a, squamous cell carcinoma of the upper third of the oesophagus. Staging investigations are, negative for metastatic disease.
Page 2676 :
You answered Endo lumenal brachytherapy, The correct answer is Chemo-radiotherapy, SCC of the oesophagus is treated with chemo-radiotherapy in the first instance., Please rate this question:, , Discuss and give feedback, , Next question, , Oesophageal cancer - treatment, Treatments for SCC's and adenocarcinomas of the oesophagus differ. This is primarily due to the, positive outcomes that are observed when localised SCC's (particularly of the proximal oesophagus, are treated with radical chemoradiotherapy (obviating the need for surgery)., Only those patients whose staging investigations are negative for metastatic disease should be, considered for surgery., Surgical options, , Endoscopic mucosal, resection, , Treatment for early localised adenocarcinoma of the distal oesophagus., Survival mirrors that of surgical resection for Tis and T1 disease, , Transhiatal, oeosphagectomy, , Most commonly used for junctional (type II) (1) tumours where limited, thoracic oesophageal resection is required. Less morbidity than two field, oesophagectomy, , Ivor Lewis, oesophagectomy, , Two stage approach for middle and distal tumours. Very commonly, performed, intrathoracic anastomosis will result in mediastinitis in event of, anastomotic leak. Lower incidence of recurrent laryngeal nerve injury, , McKeown, oesophagectomy, , Three field approach, may be useful for proximal tumours. Anastomotic, leakage is less serious. Higher incidence of recurrent laryngeal nerve, injury, , Neoadjuvent and adjuvent treatment, , , , Neoadjuvent radiotherapy alone prior to resection confers little benefit and is not routinely, performed (2), Preoperative chemotherapy is associated with a survival advantage (OE02 trial)
Page 2677 :
, , , Peri operative (pre and post operative) chemotherapy confers a survival advantage in, junctional tumours, Post operative chemotherapy is not generally recommended following oesophageal, resections outside clinical trials, , Palliation strategies, , , , , , , , Combination chemotherapy improves quality of life and survival in non operable disease (3), Trastuzumab may improve survival in patients with HER 2 positive tumours, Oesophageal intubation with self expanding metal stents is the treatment of choice in, patients with occluding tumours >2cm from the cricopharyngeus, Covered metal stents are useful in cases of malignant fistulas, Laser therapy and argon plasma coagulation may be useful as therapies for tumour, overgrowth and bleeding, Photodynamic therapy and ethanol injections confer little benefit and should not be routinely, used, , References, 1. Hulscher JB, van Sandick JW, de Boer AG, et al. Extended transthoracic resection compared with, limited transhiatal resection for adenocarcinoma of the esophagus. N Engl J Med 2002;347:1662-9, 2. Arnott SJ, Duncan W, Gignoux M, et al. Preoperative radiotherapy for esophageal carcinoma., Cochrane Database Syst Rev 2005;(4):CD001799., 3.Allum W et al. Guidelines for the management of oesophageal and gastric cancer. Gut 2011;60:, 1449-1472, Next question
Page 2678 :
Theme: Oesophageal disease, , A., B., C., D., E., F., , Oesophagectomy, Endoscopic sub mucosal dissection, Photodynamic therapy, Insertion of oesophageal stent, Chemotherapy, Radiotherapy, , Please select the most appropriate treatment modality for the scenario given. Each option may be, used once, more than once or not at all., , 18., , A 52 year old man with long standing Barretts oesophagus is diagnosed with high grade, dysplasia on recent endoscopy. The lesions are multifocal and mainly distally sited., Oesophagectomy, Similar theme in 2011 exams, Some may argue for local therapy. However, in young patients who are otherwise fit,, multifocal disease such as this should probably be resected., , 19., , A 82 year old man presents with dysphagia. He is investigated and found to have an, adenocarcinoma of the distal oesophagus. His staging investigations have revealed a, solitary metastatic lesion in the right lobe of his liver., You answered Oesophagectomy, The correct answer is Insertion of oesophageal stent, Similar theme in 2011 exam, Although he may be palliated with chemotherapy a stent will produce the quickest clinical, response. Metastatic disease is usually a contra indication to oesophageal resection., , 20., , An 83 year old lady with long standing Barretts oesophagus is diagnosed with a 1cm focus, of high grade dysplasia 3cm from the gastrooesophageal junction., You answered Oesophagectomy, The correct answer is Endoscopic sub mucosal dissection, As she is elderly and the disease localised EMR is an appropriate first line step., The technique involves raising the mucosa containing the lesion and then using an
Page 2679 :
endoscopic snare to remove it. This technique is therefore minimally invasive. However, it, is only suitable for early superficial lesions. Deeper invasion would carry a high risk of, recurrence., Please rate this question:, , Discuss and give feedback, , Next question, , Treatment of oesophageal cancer, , , , , , , , , , , In general resections are not offered to those patients with distant metastasis, and usually, not to those with N2 disease., Local nodal involvement is not in itself a contra indication to resection., Surgical resection is the mainstay of treatment., Neoadjuvent chemotherapy is given in most cases prior to surgery., In situ disease may be managed by endoscopic mucosal resection, although this is still, debated., In patients with lower third lesions an Ivor - Lewis type procedure is most commonly, performed. Very distal tumours may be suitable to a transhiatal procedure. Which is an, attractive option as the penetration of two visceral cavities required for an Ivor- Lewis type, procedure increases the morbidity considerably., More proximal lesions will require a total oesphagectomy (Mckeown type) with anastomosis, to the cervical oesophagus., Patients with unresectable disease may derive benefit from local ablative procedures,, palliative chemotherapy or stent insertion., , Operative details of Ivor- Lewis procedure, , , Combined laparotomy and right thoracotomy, , Indication, , , Lower and middle third oesophageal tumours, , Preparation, , , , Staging with a combination of CT chest abdomen and pelvis- if no metastatic disease, detected then patients will undergo a staging laparoscopy to detect peritoneal disease., If both these modalities are negative then patients will finally undergo a PET CT scan to, detect occult metastatic disease. Only in those whom no evidence of advanced disease is, detected will proceed to resection.
Page 2680 :
, , Patients receive a GA, double lumen endotracheal tube to allow for lung deflation, CVP and, arterial monitoring., , Procedure, , , A rooftop incision is made to access the stomach and duodenum., , Laparotomy To mobilize the stomach, , , , , , , The greater omentum is incised away from its attachment to the right gastroepiploic vessels, along the greater curvature of the stomach., Then the short gastric vessels are ligated and detached from the greater curvature from the, spleen., The lesser omentum is incised, preserving the right gastric artery., The retroperitoneal attachments of the duodenum in its second and third portions are, incised, allowing the pylorus to reach the oesophageal hiatus. Some surgeons perform a, pyloroplasty at this point to facilitate gastric emptying., The left gastric vessels are then ligated, avoiding any injury to the common hepatic or splenic, arteries. Care must be taken to avoid inadvertently devascularising the liver owing to, variations in anatomy., , Right Thoracotomy Oesophageal resection and oesophagogastric anastomosis, , , , , , , Through 5th intercostal space, Dissection performed 10cm above the tumour, This may involve transection of the azygos vein., The oesophagus is then removed with the stomach creating a gastric tube., An anastomosis is created., , The chest is closed with underwater seal drainage and tube drains to the abdominal cavity., Post operatively, , , , , Patients will typically recover in ITU initially., A nasogastric tube will have been inserted intraoperatively and must remain in place during, the early phases of recovery., Post operatively these patients are at relatively high risk of developing complications:, , * Atelectasis- due to the effects of thoracotomy and lung collapse, * Anastomotic leakage. The risk is relatively high owing to the presence of a relatively, devascularised stomach. Often the only blood supply is from the gastroepiploic artery as all others, will have been divided. If a leak does occur then many will attempt to manage conservatively with
Page 2681 :
prolonged nasogastric tube drainage and TPN. The reality is that up to 50% of patients developing, an anastomotic leak will not survive to discharge., * Delayed gastric emptying (may be avoided by performing a pyloroplasty)., Next question
Page 2682 :
Theme: Pancreatic tumours, , A., B., C., D., E., F., G., H., , Lymphoma, Gastrinoma, Insulinoma, Glucagonoma, Phaeochromocytoma, Carcinoid syndrome, Vasoactive Intestinal Peptide secreting tumour, Pancreatic adenocarcinoma, , Please select the most likely diagnosis for the scenario given. Each option may be used once, more, than once or not at all., , 21., , A 65 year old male attends surgical out patients with epigastric discomfort. He has, recently been diagnosed with diabetes by the GP and is a heavy smoker. An OGD is, normal., You answered Lymphoma, The correct answer is Pancreatic adenocarcinoma, The dominant differential diagnosis should be of pancreatic adenocarcinoma in this, setting. Glucagonomas are very rare and may be associated with a bullous rash., , 22., , A 50 year old male presents with recurrent episodes of abdominal pain and diarrhoea., Blood tests reveal mild iron deficiency anaemia and an upper GI endoscopy demonstrates, multiple ulcers in the first part of the duodenum., You answered Lymphoma, The correct answer is Gastrinoma, Diarrhoea, abdominal pain and multiple ulcers should raise the suspicion of Zollinger, Ellison syndrome caused by gastrinoma., , 23., , An obese 40 year old male presents with episodes of anxiety, confusion and one, convulsive episode. CT brain is normal. An abdominal CT scan shows a small 1.5cm, lesion in the head of the pancreas., You answered Lymphoma, The correct answer is Insulinoma
Page 2683 :
These episodes are due to hypoglycaemia. Insulinomas are normally solitary tumours and, may not be seen by radiological imaging. Resection is the treatment of choice., Please rate this question:, , Discuss and give feedback, , Next question, , Pancreatic cancer, , , , , , , Adenocarcinoma, Risk factors: Smoking, diabetes, adenoma, familial adenomatous polyposis, Mainly occur in the head of the pancreas (70%), Spread locally and metastasizes to the liver, Carcinoma of the pancreas should be differentiated from other periampullary tumours with, better prognosis, , Clinical features, , , , , , , Weight loss, Painless jaundice, Epigastric discomfort (pain usually due to invasion of the coeliac plexus is a late feature), Pancreatitis, Trousseau's sign: migratory superficial thrombophlebitis, , Investigations, , , , , , , USS: May miss small lesions, CT Scanning (pancreatic protocol). If unresectable on CT then no further staging needed, PET/CT for those with operable disease on CT alone, ERCP/ MRI for bile duct assessment, Staging laparoscopy to exclude peritoneal disease, , Management, , , , , , , Head of pancreas: Whipple's resection (SE dumping and ulcers). Newer techniques include, pylorus preservation and SMA/ SMV resection, Carcinoma body and tail: poor prognosis, distal pancreatectomy, if operable, Usually adjuvent chemotherapy for resectable disease, ERCP and stent for jaundice and palliation, Surgical bypass may be needed for duodenal obstruction
Page 2684 :
A 45 year old man has a 4 week history of epigastric discomfort which is relieved by eating. He, develops haematemesis and undergoes an upper GI endoscopy. An actively bleeding ulcer is noted, in the first part of the duodenum. What is the best management?, , Whipples procedure, , Truncal vagotomy and drainage, , Distal gastrectomy, , Injection with tranexamic acid, , Injection with adrenaline, Current guidance is that bleeding peptic ulcers should be treated with dual therapeutic modalities., Adrenaline injection should be augmented with an additional therapy such as endoscopic clipping, where this is available., Bleeding duodenal ulcers will usually undergo adrenaline injection. This may be augmented by the, placement of endoscopic clips or heat therapy with endoscopic heater probes. Following these, interventions patients should receive a proton pump inhibitor infusion. Those who re-bleed, may, require surgery. For ulcers in this location, laparotomy, duodenotomy and under-running of the ulcer, is usually performed., Please rate this question:, , Discuss and give feedback, , Next question, , Upper gastrointestinal bleeding, Patients may present with the following:, , , , , Haematemesis and/ or malaena, Epigastric discomfort, Sudden collapse, , The extent to which these will occur will depend upon the source. Mortality is higher in patients, presenting with haematemesis than malaena alone.
Page 2685 :
Oesophageal bleeding, , Cause, , Presenting features, , Oesophagitis, , Small volume of fresh blood, often streaking vomit. Malaena rare. Often ceases, spontaneously. Usually history of antecedent GORD type symptoms., , Cancer, , Usually small volume of blood, except as pre terminal event with erosion of, major vessels. Often associated symptoms of dysphagia and constitutional, symptoms such as weight loss. May be recurrent until malignancy managed., , Mallory Weiss, Tear, , Typically brisk small to moderate volume of bright red blood following bout of, repeated vomiting. Malaena rare. Usually ceases spontaneously., , Varices, , Usually large volume of fresh blood. Swallowed blood may cause malaena., Often associated with haemodynamic compromise. May stop spontaneously but, re-bleeds are common until appropriately managed., , Gastric Bleeding, , Cause, , Presenting features, , Gastric, cancer, , May be frank haematemesis or altered blood mixed with vomit. Usually, prodromal features of dyspepsia and may have constitutional symptoms. Amount, of bleeding variable but erosion of major vessel may produce considerable, haemorrhage., , Dieulafoy, Lesion, , Often no prodromal features prior to haematemesis and malaena, but this, arteriovenous malformation may produce quite considerable haemorrhage and, may be difficult to detect endoscopically., , Diffuse, erosive, gastritis, , Usually haematemesis and epigastric discomfort. Usually there is an underlying, cause such as recent NSAID usage. Large volume haemorrhage may occur with, considerable haemodynamic compromise., , Gastric ulcer, , Small low volume bleeds more common so would tend to present as iron, deficiency anaemia. Erosion into a significant vessel may produce considerable
Page 2686 :
haemorrhage and haematemesis., , Duodenum, Most common cause of major haemorrhage is a posteriorly sited duodenal ulcer. However, ulcers at, any site in the duodenum may present with haematemesis, malaena and epigastric discomfort. The, pain of duodenal ulcer is slightly different to that of gastric ulcers and often occurs several hours, after eating. Peri ampullary tumours may bleed but these are rare. In patients with previous, abdominal aortic aneurysm surgery aorto-enteric fistulation remains a rare but important cause of, major haemorrhage associated with high mortality., Management, , , , , , , , , , , , , , , , Admission to hospital careful monitoring, cross match blood, check FBC, LFTs, U+E and, Clotting (as a minimum), Patients with on-going bleeding and haemodynamic instability are likely to require O negative, blood pending cross matched blood, Early control of airway is vital (e.g. Drowsy patient with liver failure), Patients with suspected varices should receive terlipressin prior to endoscopy, Ideally all patients admitted with upper gastrointestinal haemorrhage should undergo Upper, GI endoscopy within 24 hours of admission. In those who are unstable this should occur, immediately after resuscitation or in tandem with it. The endoscopy department is a, potentially dangerous place for unstable patients and it may be safer to perform the, endoscopy in theatre with an anaesthetist present., Varices should be banded or subjected to sclerotherapy. If this is not possible owing to active, bleeding then a Sengaksten- Blakemore tube (or Minnesota tube) should be inserted. This, should be done with care; gastric balloon should be inflated first and oesophageal balloon, second. Remember the balloon will need deflating after 12 hours (ideally sooner) to prevent, necrosis. Portal pressure should be lowered by combination of medical therapy +/- TIPSS., Patients with erosive oesophagitis / gastritis should receive a proton pump inhibitor., Mallory Weiss tears will typically resolve spontaneously, Identifiable bleeding points should receive combination therapy of injection of adrenaline and, either a thermal or mechanical treatment. All who have received intervention should receive, a continuous infusion of a proton pump inhibitor (IV omeprazole for 72 hours) to reduce the, re-bleeding rate., Patients with diffuse erosive gastritis who cannot be managed endoscopically and continue, to bleed may require gastrectomy, Bleeding ulcers that cannot be controlled endoscopically may require laparotomy and ulcer, underruning, , Indications for surgery, , , , , , Patients > 60 years, Continued bleeding despite endoscopic intervention, Recurrent bleeding, Known cardiovascular disease with poor response to hypotension
Page 2687 :
Surgery, Duodenal ulcer, Laparotomy, duodenotomy and under running of the ulcer. If bleeding is brisk then the ulcer is, almost always posteriorly sited and will have invaded the gastroduodenal artery. Large bites using 0, Vicryl are taken above and below the ulcer base to occlude the vessel. The duodenotomy should be, longitudinal but closed transversely to avoid stenosis., For gastric ulcer, Under-running of the bleeding site, Partial gastrectomy-antral ulcer, Partial gastrectomy or under running the ulcer- lesser curve ulcer (involving left gastric artery), Total gastrectomy if bleeding persists, Summary of Acute Upper GI bleeding recommendations:, The need for admission and timing of endoscopic intervention may be predicted by using the, Blatchford score. This considers a patients Hb, serum urea, pulse rate and blood pressure. Those, patients with a score of 0 are low risk, all others are considered high risk and require admission and, endoscopy., The requirement for pre endoscopic proton pump inhibition is contentious. In the UK the National, Institute of Clinical Excellence guidelines suggest the pre endoscopic PPI therapy is unnecessary., Whilst it is accepted that such treatment has no impact on mortality or morbidity a Cochrane review, of this practice in 2007 did suggest that it reduced the stigmata of recent haemorrhage at, endoscopy. As a result many will still administer PPI to patients prior to endoscopic intervention., Following endoscopy it is important to calculate the Rockall score for patients to determine their risk, of rebleeding and mortality. A score of 3 or less is associated with a rebleeding rate of 4% and a, very low risk of mortality and identifies a group of patients suitable for early discharge., References, 1. http://www.sign.ac.uk/guidelines/fulltext/105/index.html, 2. Joint Advisory Group on Endoscopy (JAG) Guidelines - http://www.thejag.org.uk, 3. NICE Guideline: Management of acute upper GI bleeding. July 2012., Next question
Page 2688 :
Which of the following patients should be referred for 1st line bariatric surgery?, , BMI 35 kg/m2 and hypertension, , BMI 40 kg/m2, , BMI 40 kg/m2 and type 2 diabetes, , BMI 52kg/m2, , BMI 40kg/m2, COPD and type 2 diabetes, , With all the other options the patient should have conservative management for a minimum of 6, months first., Please rate this question:, , Discuss and give feedback, , Next question, , Bariatric surgery, Obesity is a major health problem in the Western world. Surgical solutions to the problem have, evolved dramatically over the past few years. Randomised controlled trials have shown that dramatic, weight loss can be achieved following surgical interventions compared with standard medical, therapy. The weight loss process is also more durable following surgery than with non surgical, interventions., Case selection, BMI >/= 40 kg/m 2 or between 35-40 kg/m 2 and other significant disease (for example, type 2, diabetes, hypertension) that could be improved with weight loss., Pre-requisites to surgery (NICE UK Guidelines), , , , , , , All non-surgical measures have failed to achieve or maintain adequate clinically beneficial, weight loss for at least 6 months., Will receive intensive specialist management, They are generally fit for anaesthesia and surgery, They commit to the need for long-term follow-up, First-line option for adults with a BMI > 50 kg/m 2 in whom surgical intervention is considered, appropriate; consider orlistat if there is a long waiting list.
Page 2689 :
Surgical options, , Adjustable gastric, band, , , , , , , , , Gastric bypass, , Sleeve gastrectomy, , , , Laparoscopic placement of adjustable band around proximal, stomach., Contains an adjustable filling port, Effective method for lifestyle control, Reversible, Takes longer to achieve target weight, Complications such as band erosion (rare), slippage or loss of, efficacy may require re-intervention, , , , , , , Combines changes to reservoir size with malabsorptive procedure, for more enduring weight loss., Technically more challenging, Risks related to anastomoses (2% leak rate), Irreversible, Up to 50% may become B12 deficient, , , , , Resection of stomach using stapling devices, Less popular now as initial promising results not sustained, , References, 1. National Institute for Health and Clinical Excellence. Obesity: the prevention, identification,, assessment and management of overweight and obesity in adults and children., www.nice.org.uk/CG43, 2. Leff DR, Heath D. Surgery for obesity in adulthood. BMJ 2009;339:b3402, Next question
Page 2690 :
Theme: Management of gastric cancer, , A., B., C., D., E., F., G., H., , Radical radiotherapy, Endoscopic submucosal resection, Polya Gastrectomy, Distal gastrectomy and anterior gastrojejunostomy, Distal gastrectomy and posterior gastrojejunostomy, Belsey Mark IV procedure, Sub total gastrectomy and Roux and Y reconstruction, Total gastrectomy and Roux en Y reconstruction, , Please select the most appropriate management for the gastric cancer case described. Each option, may be used once, more than once or not at all., , 26., , An otherwise fit 73 year old man presents with gastric outlet obstruction. An upper GI, endoscopy shows a prepyloric tumour occluding the pylorus. Staging investigations show, nodal disease at D2 and an involved paraaortic lymph node., You answered Radical radiotherapy, The correct answer is Distal gastrectomy and anterior gastrojejunostomy, This man does not have disease amenable to curative surgical resection. However, good, palliation can be achieved with a resection and chemotherapy. He is likely to have, recurrent disease in the gastric bed and an anterior gastrojejunostomy is therefore, preferred., , 27., , A 40 year old lady presents with a gastric carcinoma of the greater curvature of the, stomach. Her staging investigations are negative for metastatic disease., You answered Radical radiotherapy, The correct answer is Sub total gastrectomy and Roux and Y reconstruction, This is amenable to potentially curative resection. The proximal stomach can be, conserved., , 28., , A 62 year old man presents with dyspepsia and a tumour of the gastric cardia is diagnosed., He has no evidence of metastatic disease., You answered Radical radiotherapy, The correct answer is Total gastrectomy and Roux en Y reconstruction
Page 2691 :
This will require a total gastrectomy. Retention of a gastric remnant is unlikely to achieve, acceptable resection margins, Please rate this question:, , Discuss and give feedback, , Next question, , Gastric cancer, Overview, There are 700,000 new cases of gastric cancer worldwide each year. It is most common in Japan, and less common in western countries. It is more common in men and incidence rises with, increasing age. The exact cause of many sporadic cancer is not known, however, familial cases do, occur in HNPCC families. In addition, smoking and smoked or preserved foods increase the risk., Japanese migrants retain their increased risk (decreased in subsequent generations). The, distribution of the disease in western countries is changing towards a more proximal location, (perhaps due to rising obesity)., Pathology, There is some evidence of support a stepwise progression of the disease through intestinal, metaplasia progressing to atrophic gastritis and subsequent dysplasia, through to cancer. The, favoured staging system is TNM. The risk of lymph node involvement is related to size and depth of, invasion; early cancers confined to submucosa have a 20% incidence of lymph node metastasis., Tumours of the gastro-oesophageal junction are classified as below:, , Type, 1, , True oesophageal cancers and may be associated with Barrett's oesophagus., , Type, 2, , Carcinoma of the cardia, arising from cardiac type epithelium, or short segments with intestinal metaplasia at the oesophagogastric junction., , Type, 3, , Sub cardial cancers that spread across the junction. Involve similar nodal stations to, gastric cancer., , Groups for close endoscopic monitoring, , , , , Intestinal metaplasia of columnar type, Atrophic gastritis, Low to medium grade dysplasia
Page 2692 :
, , Patients who have previously undergone resections for benign peptic ulcer disease (except, highly selective vagotomy)., , Referral to endoscopy, , Patients of any age with, dyspepsia and any of the, following, , Patients without, dyspepsia, , Worsening dyspepsia, , Chronic gastrointestinal bleeding, , Dysphagia, , Barretts oesophagus, , Dysphagia, , Unexplained abdominal, pain or weight loss, , Intestinal metaplasia, , Weight loss, , Vomiting, , Dysplasia, , Iron deficiency anaemia, , Upper abdominal mass, , Atrophic gastritis, , Upper abdominal mass, , Jaundice, , Patient aged over 55 years with, unexplained or persistent, dyspepsia, , Upper GI endoscopy performed for dyspepsia. The addition of dye spraying (as shown in the bottom, right) may facilitate identification of smaller tumours
Page 2693 :
Image sourced from Wikipedia, , Staging, , , , , CT scanning of the chest abdomen and pelvis is the routine first line staging investigation in, most centres., Laparoscopy to identify occult peritoneal disease, PET CT (particularly for junctional tumours), , Treatment, , , , , , , , Proximally sited disease greater than 5-10cm from the OG junction may be treated by sub, total gastrectomy, Total gastrectomy if tumour is <5cm from OG junction, For type 2 junctional tumours (extending into oesophagus) oesophagogastrectomy is usual, Endoscopic sub mucosal resection may play a role in early gastric cancer confined to the, mucosa and perhaps the sub mucosa (this is debated), Lymphadenectomy should be performed. A D2 lymphadenectomy is widely advocated by the, Japanese, the survival advantages of extended lymphadenectomy have been debated., However, the overall recommendation is that a D2 nodal dissection be undertaken., Most patients will receive chemotherapy either pre or post operatively., , Prognosis
Page 2694 :
UK Data, , Disease extent, , Percentage 5 year survival, , All RO resections, , 54%, , Early gastric cancer, , 91%, , Stage 1, , 87%, , Stage 2, , 65%, , Stage 3, , 18%, , Operative procedure, Total Gastrectomy , lymphadenectomy and Roux en Y anastomosis, General anaesthesia, Prophylactic intravenous antibiotics, Incision: Rooftop., Perform a thorough laparotomy to identify any occult disease., Mobilise the left lobe of the liver off the diaphragm and place a large pack over it. Insert a large self, retaining retractor e.g. omnitract or Balfour (take time with this, the set up should be perfect). Pack, the small bowel away., Begin by mobilising the omentum off the transverse colon., Proceed to detach the short gastric vessels., Mobilise the pylorus and divide it at least 2cm distally using a linear cutter stapling device., Continue the dissection into the lesser sac taking the lesser omentum and left gastric artery flush at, its origin., The lymph nodes should be removed en bloc with the specimen where possible., Place 2 stay sutures either side of the distal oesophagus. Ask the anaesthetist to pull back on the, nasogastric tube. Divide the distal oesophagus and remove the stomach., The oesphago jejunal anastomosis should be constructed. Identify the DJ flexure and bring a loop of, jejunum up to the oesophagus (to check it will reach). Divide the jejunum at this point. Bring the, divided jejunum either retrocolic or antecolic to the oesophagus. Anastamose the oesophagus to the, jejunum, using either interrupted 3/0 vicryl or a stapling device. Then create the remainder of the, Roux en Y reconstruction distally., Place a jejunostomy feeding tube., Wash out the abdomen and insert drains (usually the anastomosis and duodenal stump). Help the, anaesthetist insert the nasogastric tube (carefully!), Close the abdomen and skin.
Page 2695 :
Enteral feeding may commence on the first post-operative day. However, most surgeons will leave, patients on free NG drainage for several days and keep them nil by mouth., Next question
Page 2696 :
Theme: Causes of upper gastrointestinal haemorrhage, , A., B., C., D., E., F., G., , Antral gastric ulcer, Mallory Weiss tear, Oesphageal varices, Dieulafoy lesion, Gastritis, Duodenal ulcer anterior wall, Duodenal ulcer posterior wall, , Please select the most appropriate likely diagnosis for the scenario given. Each option may be used, once, more than once or not at all., , 29., , A 35 year old man is admitted with an episode of collapse and passage of malaena. He has, been suffering from post prandial abdominal pain for 5 weeks and this is most marked, several hours after eating., You answered Antral gastric ulcer, The correct answer is Duodenal ulcer posterior wall, Patients with duodenal ulcers will usually have a history of epigastric pain that occurs, several hours after eating. The pain is often improved by eating food. They are most, frequently located i nthe first part of the duodenum. Anteriorly sited ulcers may perforate, and result in peritonitis, posteriorly sited ulcers may erode the gastroduodenal artery and, present with haematemesis and/ or malaena., , 30., , A 72 year old man is admitted with an episode of brisk haematemesis. Following, resuscitation an upper GI endoscopy is performed and a prominent blood vessel is, identified in the mucosa approximately 6 cm from the O-G junction on the lesser curve of, the stomach., You answered Antral gastric ulcer, The correct answer is Dieulafoy lesion, These small arterial lesions are a rare cause of bleeding and are characterised by a single, large tortuous arteriole in the sub mucosa. Extra gastric lesions may occur., , 31., , A 56 year old man is admitted with a profuse upper gastro intestinal haemorrhage. He is, relatively malnourished and has evidence of gynaecomastia., You answered Antral gastric ulcer
Page 2697 :
The correct answer is Oesphageal varices, Patients presenting with gastrointestinal bleeding and evidence of established liver disease, may have portal hypertension and develop variceal haemorrhage. The patient may have, evidence of jaundice, gynaecomastia, spider naevia, caput medusae and ascites. The, bleeding is usually profuse and painless., Please rate this question:, , Discuss and give feedback, , Next question, , Upper gastrointestinal bleeding, Patients may present with the following:, , , , , Haematemesis and/ or malaena, Epigastric discomfort, Sudden collapse, , The extent to which these will occur will depend upon the source. Mortality is higher in patients, presenting with haematemesis than malaena alone., Oesophageal bleeding, , Cause, , Presenting features, , Oesophagitis, , Small volume of fresh blood, often streaking vomit. Malaena rare. Often ceases, spontaneously. Usually history of antecedent GORD type symptoms., , Cancer, , Usually small volume of blood, except as pre terminal event with erosion of, major vessels. Often associated symptoms of dysphagia and constitutional, symptoms such as weight loss. May be recurrent until malignancy managed., , Mallory Weiss, Tear, , Typically brisk small to moderate volume of bright red blood following bout of, repeated vomiting. Malaena rare. Usually ceases spontaneously., , Varices, , Usually large volume of fresh blood. Swallowed blood may cause malaena., Often associated with haemodynamic compromise. May stop spontaneously but
Page 2698 :
re-bleeds are common until appropriately managed., , Gastric Bleeding, , Cause, , Presenting features, , Gastric, cancer, , May be frank haematemesis or altered blood mixed with vomit. Usually, prodromal features of dyspepsia and may have constitutional symptoms. Amount, of bleeding variable but erosion of major vessel may produce considerable, haemorrhage., , Dieulafoy, Lesion, , Often no prodromal features prior to haematemesis and malaena, but this, arteriovenous malformation may produce quite considerable haemorrhage and, may be difficult to detect endoscopically., , Diffuse, erosive, gastritis, , Usually haematemesis and epigastric discomfort. Usually there is an underlying, cause such as recent NSAID usage. Large volume haemorrhage may occur with, considerable haemodynamic compromise., , Gastric ulcer, , Small low volume bleeds more common so would tend to present as iron, deficiency anaemia. Erosion into a significant vessel may produce considerable, haemorrhage and haematemesis., , Duodenum, Most common cause of major haemorrhage is a posteriorly sited duodenal ulcer. However, ulcers at, any site in the duodenum may present with haematemesis, malaena and epigastric discomfort. The, pain of duodenal ulcer is slightly different to that of gastric ulcers and often occurs several hours, after eating. Peri ampullary tumours may bleed but these are rare. In patients with previous, abdominal aortic aneurysm surgery aorto-enteric fistulation remains a rare but important cause of, major haemorrhage associated with high mortality., Management, , , , , , , Admission to hospital careful monitoring, cross match blood, check FBC, LFTs, U+E and, Clotting (as a minimum), Patients with on-going bleeding and haemodynamic instability are likely to require O negative, blood pending cross matched blood, Early control of airway is vital (e.g. Drowsy patient with liver failure), Patients with suspected varices should receive terlipressin prior to endoscopy, Ideally all patients admitted with upper gastrointestinal haemorrhage should undergo Upper, GI endoscopy within 24 hours of admission. In those who are unstable this should occur
Page 2699 :
, , , , , , , , , immediately after resuscitation or in tandem with it. The endoscopy department is a, potentially dangerous place for unstable patients and it may be safer to perform the, endoscopy in theatre with an anaesthetist present., Varices should be banded or subjected to sclerotherapy. If this is not possible owing to active, bleeding then a Sengaksten- Blakemore tube (or Minnesota tube) should be inserted. This, should be done with care; gastric balloon should be inflated first and oesophageal balloon, second. Remember the balloon will need deflating after 12 hours (ideally sooner) to prevent, necrosis. Portal pressure should be lowered by combination of medical therapy +/- TIPSS., Patients with erosive oesophagitis / gastritis should receive a proton pump inhibitor., Mallory Weiss tears will typically resolve spontaneously, Identifiable bleeding points should receive combination therapy of injection of adrenaline and, either a thermal or mechanical treatment. All who have received intervention should receive, a continuous infusion of a proton pump inhibitor (IV omeprazole for 72 hours) to reduce the, re-bleeding rate., Patients with diffuse erosive gastritis who cannot be managed endoscopically and continue, to bleed may require gastrectomy, Bleeding ulcers that cannot be controlled endoscopically may require laparotomy and ulcer, underruning, , Indications for surgery, , , , , , Patients > 60 years, Continued bleeding despite endoscopic intervention, Recurrent bleeding, Known cardiovascular disease with poor response to hypotension, , Surgery, Duodenal ulcer, Laparotomy, duodenotomy and under running of the ulcer. If bleeding is brisk then the ulcer is, almost always posteriorly sited and will have invaded the gastroduodenal artery. Large bites using 0, Vicryl are taken above and below the ulcer base to occlude the vessel. The duodenotomy should be, longitudinal but closed transversely to avoid stenosis., For gastric ulcer, Under-running of the bleeding site, Partial gastrectomy-antral ulcer, Partial gastrectomy or under running the ulcer- lesser curve ulcer (involving left gastric artery), Total gastrectomy if bleeding persists, Summary of Acute Upper GI bleeding recommendations:, The need for admission and timing of endoscopic intervention may be predicted by using the, Blatchford score. This considers a patients Hb, serum urea, pulse rate and blood pressure. Those, patients with a score of 0 are low risk, all others are considered high risk and require admission and, endoscopy., The requirement for pre endoscopic proton pump inhibition is contentious. In the UK the National, Institute of Clinical Excellence guidelines suggest the pre endoscopic PPI therapy is unnecessary., Whilst it is accepted that such treatment has no impact on mortality or morbidity a Cochrane review, of this practice in 2007 did suggest that it reduced the stigmata of recent haemorrhage at, endoscopy. As a result many will still administer PPI to patients prior to endoscopic intervention.
Page 2700 :
Following endoscopy it is important to calculate the Rockall score for patients to determine their risk, of rebleeding and mortality. A score of 3 or less is associated with a rebleeding rate of 4% and a, very low risk of mortality and identifies a group of patients suitable for early discharge., References, 1. http://www.sign.ac.uk/guidelines/fulltext/105/index.html, 2. Joint Advisory Group on Endoscopy (JAG) Guidelines - http://www.thejag.org.uk, 3. NICE Guideline: Management of acute upper GI bleeding. July 2012., Next question
Page 2701 :
Theme: Gastro intestinal haemorrhage., , A., B., C., D., E., F., G., , Proctoscopy and injection sclerotherapy, IV terlipressin, Pan Proctocolectomy, Sub total colectomy, Colonscopy and bleeding therapy, Barium enema, Angiography of mesenteric artery, , Please select the most appropriate management option for the scenario given. Each option may be, used once more than once or not at all, , 32., , A 56 year old man is admitted with passage of a large volume of blood per rectum. On, examination he is tachycardic, his abdomen is soft, although he has marked dilated veins, on his abdominal wall. Proctoscopy reveals large dilated veins with stigmata of recent, haemorrhage., You answered Proctoscopy and injection sclerotherapy, The correct answer is IV terlipressin, Rectal varices are a recognised complication of portal hypertension. In the first instance, they can be managed with medical therapy to lower pressure in the portal venous system., TIPSS may be considered. Whilst band ligation is an option, attempting to inject these in, same way as haemorroids would carry a high risk of precipitating further haemorrhage., , 33., , A 73 year old lady is admitted with dark red PR bleeding. She undergoes an OGD which is, normal. Digital rectal examination shows blood but no masses. She becomes tachycardic, and BP is 95/40., You answered Proctoscopy and injection sclerotherapy, The correct answer is Angiography of mesenteric artery, This women is actively bleeding and mesenteric angiography may localise the bleeding., Colonoscopy in this situation is seldom helpful or successful., , 34., , A 68 year old man with ulcerative colitis is admitted with an exacerbation. You are called, to see him because he is having brisk dark PR bleeding. He has been on intravenous, hydrocortisone for 5 days. The gastroenterologists have done an OGD to exclude a, duodenal ulcer, this was normal.
Page 2702 :
You answered Proctoscopy and injection sclerotherapy, The correct answer is Sub total colectomy, This man requires surgery to remove the bleeding segment of bowel. Medical management, has failed here. Note that a pan proctocolectomy is not a suitable option in the emergency, setting because there is increased morbidity from the pelvic dissection. In the unlikely, event that a sub total colectomy did not address the bleeding then consideration may have, to be given to removal of the rectum but this would not usually be the case., Please rate this question:, , Discuss and give feedback, , Next question, , Lower Gastrointestinal bleeding, Colonic bleeding, This typically presents as bright red or dark red blood per rectum. Colonic bleeding rarely presents, as malaena type stool, this is because blood in the colon has a powerful laxative effect and is rarely, retained long enough for transformation to occur and because the digestive enzymes present in the, small bowel are not present in the colon. Up to 15% of patients presenting with haemochezia will, have an upper gastrointestinal source of haemorrhage., As a general rule right sided bleeds tend to present with darker coloured blood than left sided, bleeds. Haemorrhoidal bleeding typically presents as bright red rectal bleeding that occurs post, defecation either onto toilet paper or into the toilet pan. It is very unusual for haemorrhoids alone to, cause any degree of haemodynamic compromise., Causes, , Cause, , Presenting features, , Colitis, , Bleeding may be brisk in advanced cases, diarrhoea is commonly present., Abdominal x-ray may show featureless colon., , Diverticular, disease, , Acute diverticulitis often is not complicated by major bleeding and, diverticular bleeds often occur sporadically. 75% all will cease spontaneously, within 24-48 hours. Bleeding is often dark and of large volume., , Cancer, , Colonic cancers often bleed and for many patients this may be the first sign of, the disease. Major bleeding from early lesions is uncommon
Page 2703 :
Cause, , Presenting features, , Haemorrhoidal, bleeding, , Typically bright red bleeding occurring post defecation. Although patients, may give graphic descriptions bleeding of sufficient volume to cause, haemodynamic compromise is rare., , Angiodysplasia, , Apart from bleeding, which may be massive, these arteriovenous lesions, cause little in the way of symptoms. The right side of the colon is more, commonly affected., , Management, , , , , , , Prompt correction of any haemodynamic compromise is required. Unlike upper, gastrointestinal bleeding the first line management is usually supportive. This is because in, the acute setting endoscopy is rarely helpful., When haemorrhoidal bleeding is suspected a proctosigmoidoscopy is reasonable as, attempts at full colonoscopy are usually time consuming and often futile., In the unstable patient the usual procedure would be an angiogram (either CT or, percutaneous), when these are performed during a period of haemodynamic instability they, may show a bleeding point and may be the only way of identifying a patch of angiodysplasia., In others who are more stable the standard procedure would be a colonoscopy in the, elective setting. In patients undergoing angiography attempts can be made to address the, lesion in question such as coiling. Otherwise surgery will be necessary., In patients with ulcerative colitis who have significant haemorrhage the standard approach, would be a sub total colectomy, particularly if medical management has already been tried, and is not effective., , Indications for surgery, Patients > 60 years, Continued bleeding despite endoscopic intervention, Recurrent bleeding, Known cardiovascular disease with poor response to hypotension, Surgery, Selective mesenteric embolisation if life threatening bleeding. This is most helpful if conducted, during a period of relative haemodynamic instability. If all haemodynamic parameters are normal, then the bleeding is most likely to have stopped and any angiography normal in appearance. In, many units a CT angiogram will replace selective angiography but the same caveats will apply., If the source of colonic bleeding is unclear; perform a laparotomy, on table colonic lavage and, following this attempt a resection. A blind sub total colectomy is most unwise, for example bleeding, from an small bowel arterio-venous malformation will not be treated by this manoeuvre., Summary of Acute Lower GI bleeding recommendations
Page 2705 :
Theme: Dysphagia, , A. Mallory Weiss Tear, B. Hiatus hernia, C. Squamous cell carcinoma of the oesophagus, D. Adenocarcinoma of the oesophagus, E. Peptic stricture, F. Motility disorder, , For each of the following scenarios please select the most likely underlying disorder. Each option, may be used once, more than once or not at all., , 35., , A 56 year old lady presents with a 6 month history of dysphagia to solids. She has a long history of, retrosternal chest pain that is worse on lying flat and bending forwards. She undergoes an upper, GI endoscopy where a smooth stricture is identified., You answered Mallory Weiss Tear, The correct answer is Peptic stricture, Theme from April 2012 Exam, A six month history of dysphagia is a relatively long history and makes malignancy less likely. The, lesion should be biopsied for histological confirmation. Long standing oesophagitis may be, complicated by the development of strictures, Barretts oesophagus or both., , 36., , A 76 year old man presents with a 5 week history of progressive dysphagia. An upper GI, endoscopy is performed and the surgeon notices changes that are compatible with Barretts, oesophagus. The oesophagus is filled with food debris that cannot be cleared and the endoscope, encounters a resistance that cannot be passed., You answered Mallory Weiss Tear, The correct answer is Adenocarcinoma of the oesophagus
Page 2706 :
A short history of dysphagia together with food debris and Barretts changes makes, adenocarcinoma the most likely diagnosis., , 37., , A 22 year old man presents with a 5 month history of episodic retrosternal chest pain together, with episodes of dysphagia to liquids. An upper GI endoscopy is performed and no mucosal, abnormality is seen., You answered Mallory Weiss Tear, The correct answer is Motility disorder, Dysphagia that is episodic and varies between solids and liquids is more likely to represent a, motility disorder., , Please rate this question:, , Discuss and give feedback, , Next question, , Oesophageal disease, Disorder, , Features, , Mallory-Weiss Tear, , Usually history of antecedent vomiting. This is then followed by the vomiting of a, small amount of blood. There is usually little in the way of systemic disturbance, or prior symptoms., , Hiatus hernia of, gastric cardia, , Often longstanding history of dyspepsia, patients are often overweight., Uncomplicated hiatus hernias should not be associated with dysphagia or, haematemesis.
Page 2707 :
Disorder, , Features, , Oesophageal rupture, , Complete disruption of the oesophageal wall in absence of pre-existing, pathology. Left postero-lateral oesophageal is commonest site (2-3cm from OG, junction). Suspect in patients with severe chest pain without cardiac diagnosis, and signs suggestive of pneumonia without convincing history, where there is, history of vomiting. Erect CXR shows infiltrate or effusion in 90% of cases(1)., , Squamous cell, carcinoma of the, oesophagus, , History of progressive dysphagia. Often signs of weight loss. Usually little or no, history of previous GORD type symptoms., , Adenocarcinoma of, the oesophagus, , Progressive dysphagia, may have previous symptoms of GORD or Barretts, oesophagus., , Peptic stricture, , Longer history of dysphagia, often not progressive. Usually symptoms of GORD., Often lack systemic features seen with malignancy, , Dysmotility disorder, , May have dysphagia that is episodic and non progressive. Retrosternal pain may, accompany the episodes., , Diagnosis, Most of the differential diagnoses listed above can be accurately categorised by upper GI endoscopy, (usually most patients). Where this fails to demonstrate a mechanical stricture the use of pH and, manometry studies together with radiological contrast swallows will facilitate the diagnosis., References, Blencowe N et al. Spontaneous oesophageal rupture. BMJ 2013 (346):38-39., Next question
Page 2708 :
A 73 year old lady presents with progressive dysphagia and is diagnosed with oesophageal cancer, and liver metastases, it is located 8cm proximal to the gastro-oesophageal junction. Which of the, following treatment options would be the the most appropriate management?, , Insertion of Celestin tube, , Insertion of Minnesota tube, , Insertion of self expanding metal stent, , Photodynamic therapy, , Trans hiatal oesphagectomy, , Most cases of malignant oesophageal obstruction can be managed by the placement of self, expanding metal stents. The Celestin tube requires a laparotomy and is therefore obsolete. A, resectional procedure would be inappropriate in the presence of liver metastasis. The main contra, indication to metallic stent placement are very proximal tumours as it can be difficult to get proximal, control in this situation and chemotherapy may be more appropriate., Please rate this question:, , Discuss and give feedback, , Next question, , Treatment of oesophageal cancer, , , , , , , , , , , In general resections are not offered to those patients with distant metastasis, and usually, not to those with N2 disease., Local nodal involvement is not in itself a contra indication to resection., Surgical resection is the mainstay of treatment., Neoadjuvent chemotherapy is given in most cases prior to surgery., In situ disease may be managed by endoscopic mucosal resection, although this is still, debated., In patients with lower third lesions an Ivor - Lewis type procedure is most commonly, performed. Very distal tumours may be suitable to a transhiatal procedure. Which is an, attractive option as the penetration of two visceral cavities required for an Ivor- Lewis type, procedure increases the morbidity considerably., More proximal lesions will require a total oesphagectomy (Mckeown type) with anastomosis, to the cervical oesophagus., Patients with unresectable disease may derive benefit from local ablative procedures,, palliative chemotherapy or stent insertion.
Page 2709 :
Operative details of Ivor- Lewis procedure, , , Combined laparotomy and right thoracotomy, , Indication, , , Lower and middle third oesophageal tumours, , Preparation, , , , , Staging with a combination of CT chest abdomen and pelvis- if no metastatic disease, detected then patients will undergo a staging laparoscopy to detect peritoneal disease., If both these modalities are negative then patients will finally undergo a PET CT scan to, detect occult metastatic disease. Only in those whom no evidence of advanced disease is, detected will proceed to resection., Patients receive a GA, double lumen endotracheal tube to allow for lung deflation, CVP and, arterial monitoring., , Procedure, , , A rooftop incision is made to access the stomach and duodenum., , Laparotomy To mobilize the stomach, , , , , , , The greater omentum is incised away from its attachment to the right gastroepiploic vessels, along the greater curvature of the stomach., Then the short gastric vessels are ligated and detached from the greater curvature from the, spleen., The lesser omentum is incised, preserving the right gastric artery., The retroperitoneal attachments of the duodenum in its second and third portions are, incised, allowing the pylorus to reach the oesophageal hiatus. Some surgeons perform a, pyloroplasty at this point to facilitate gastric emptying., The left gastric vessels are then ligated, avoiding any injury to the common hepatic or splenic, arteries. Care must be taken to avoid inadvertently devascularising the liver owing to, variations in anatomy., , Right Thoracotomy Oesophageal resection and oesophagogastric anastomosis, , , Through 5th intercostal space
Page 2710 :
, , , , , Dissection performed 10cm above the tumour, This may involve transection of the azygos vein., The oesophagus is then removed with the stomach creating a gastric tube., An anastomosis is created., , The chest is closed with underwater seal drainage and tube drains to the abdominal cavity., Post operatively, , , , , Patients will typically recover in ITU initially., A nasogastric tube will have been inserted intraoperatively and must remain in place during, the early phases of recovery., Post operatively these patients are at relatively high risk of developing complications:, , * Atelectasis- due to the effects of thoracotomy and lung collapse, * Anastomotic leakage. The risk is relatively high owing to the presence of a relatively, devascularised stomach. Often the only blood supply is from the gastroepiploic artery as all others, will have been divided. If a leak does occur then many will attempt to manage conservatively with, prolonged nasogastric tube drainage and TPN. The reality is that up to 50% of patients developing, an anastomotic leak will not survive to discharge., * Delayed gastric emptying (may be avoided by performing a pyloroplasty)., Next question
Page 2711 :
Which of the following statements relating to gastric banding for obesity is false?, , It is one of the safest anti obesity operations, , If successful up to 55% of excess weight may be lost over 2 years, , Excessively tight gastric bands have increased risk of long term complications, , It is associated with early satiety, , It is contra indicated in patients with polycystic ovaries who are trying to conceive, , Adjustable gastric bands are one of the most widely performed anti obesity procedures in the UK., They are relatively easy to insert. Weight loss is slightly slower than with some of the other weight, loss procedures. Up to 15% patients may require revisional surgery., Please rate this question:, , Discuss and give feedback, , Next question, , Bariatric surgery, Obesity is a major health problem in the Western world. Surgical solutions to the problem have, evolved dramatically over the past few years. Randomised controlled trials have shown that dramatic, weight loss can be achieved following surgical interventions compared with standard medical, therapy. The weight loss process is also more durable following surgery than with non surgical, interventions., Case selection, BMI >/= 40 kg/m 2 or between 35-40 kg/m 2 and other significant disease (for example, type 2, diabetes, hypertension) that could be improved with weight loss., Pre-requisites to surgery (NICE UK Guidelines), , , , , , , All non-surgical measures have failed to achieve or maintain adequate clinically beneficial, weight loss for at least 6 months., Will receive intensive specialist management, They are generally fit for anaesthesia and surgery, They commit to the need for long-term follow-up, First-line option for adults with a BMI > 50 kg/m 2 in whom surgical intervention is considered, appropriate; consider orlistat if there is a long waiting list.
Page 2712 :
Surgical options, , Adjustable gastric, band, , , , , , , , , Gastric bypass, , Sleeve gastrectomy, , , , Laparoscopic placement of adjustable band around proximal, stomach., Contains an adjustable filling port, Effective method for lifestyle control, Reversible, Takes longer to achieve target weight, Complications such as band erosion (rare), slippage or loss of, efficacy may require re-intervention, , , , , , , Combines changes to reservoir size with malabsorptive procedure, for more enduring weight loss., Technically more challenging, Risks related to anastomoses (2% leak rate), Irreversible, Up to 50% may become B12 deficient, , , , , Resection of stomach using stapling devices, Less popular now as initial promising results not sustained, , References, 1. National Institute for Health and Clinical Excellence. Obesity: the prevention, identification,, assessment and management of overweight and obesity in adults and children., www.nice.org.uk/CG43, 2. Leff DR, Heath D. Surgery for obesity in adulthood. BMJ 2009;339:b3402, Next question
Page 2713 :
Which of the following procedures is not performed for obesity?, , Sleeve gastrectomy, , Gastric band, , Intra gastric balloon, , Mckeown procedure, , Small bowel bypass, , A McKeown procedure is a total oesophagectomy., Please rate this question:, , Discuss and give feedback, , Next question, , Bariatric surgery, Obesity is a major health problem in the Western world. Surgical solutions to the problem have, evolved dramatically over the past few years. Randomised controlled trials have shown that dramatic, weight loss can be achieved following surgical interventions compared with standard medical, therapy. The weight loss process is also more durable following surgery than with non surgical, interventions., Case selection, BMI >/= 40 kg/m 2 or between 35-40 kg/m 2 and other significant disease (for example, type 2, diabetes, hypertension) that could be improved with weight loss., Pre-requisites to surgery (NICE UK Guidelines), , , , , , , All non-surgical measures have failed to achieve or maintain adequate clinically beneficial, weight loss for at least 6 months., Will receive intensive specialist management, They are generally fit for anaesthesia and surgery, They commit to the need for long-term follow-up, First-line option for adults with a BMI > 50 kg/m 2 in whom surgical intervention is considered, appropriate; consider orlistat if there is a long waiting list.
Page 2714 :
Surgical options, , Adjustable gastric, band, , , , , , , , , Gastric bypass, , Sleeve gastrectomy, , , , Laparoscopic placement of adjustable band around proximal, stomach., Contains an adjustable filling port, Effective method for lifestyle control, Reversible, Takes longer to achieve target weight, Complications such as band erosion (rare), slippage or loss of, efficacy may require re-intervention, , , , , , , Combines changes to reservoir size with malabsorptive procedure, for more enduring weight loss., Technically more challenging, Risks related to anastomoses (2% leak rate), Irreversible, Up to 50% may become B12 deficient, , , , , Resection of stomach using stapling devices, Less popular now as initial promising results not sustained, , References, 1. National Institute for Health and Clinical Excellence. Obesity: the prevention, identification,, assessment and management of overweight and obesity in adults and children., www.nice.org.uk/CG43, 2. Leff DR, Heath D. Surgery for obesity in adulthood. BMJ 2009;339:b3402, Next question
Page 2715 :
Which of the following variables is not included in the Rockall score?, , Congestive cardiac failure, , Liver failure, , Systolic blood pressure < 100mmHg, , Aspirin usage, , Age, A patients should have their Rockall score calculated following endoscopy for upper GI haemorrhage, Mnemonic for Rockall score, ABCDE, A: Age, B: Blood pressure drop (Shock), C: Co-morbidity, D: Diagnosis, E: Evidence of bleeding, Rockall Score, Applies to upper gastrointestinal bleeding, , Variable, , Score 0, , Score 1, , Score 2, , Age, , <60, , 60-79, , >80, , Shock, , None, , Pulse, >100, , Hypotension (systolic, <100mmHg), , Co-Morbidity, , Nil or, minimal, , Major organ disease e.g., IHD, CCF, , Score 3, , Renal or liver failure,, metastatic cancer
Page 2716 :
Variable, , Score 0, , Score 1, , Score 2, , Diagnosis, , MalloryWeiss, , All, , GI Cancer, , Evidence of, Bleeding, , None, , Score 3, , Clot, Blood, spurting, vessel, , Score <3 = Good prognosis (mortality approx. 2%), Score >8= High mortality (Mortality approx. 40%), Please rate this question:, , Discuss and give feedback, , Next question, , Upper gastrointestinal bleeding, Patients may present with the following:, , , , , Haematemesis and/ or malaena, Epigastric discomfort, Sudden collapse, , The extent to which these will occur will depend upon the source. Mortality is higher in patients, presenting with haematemesis than malaena alone., Oesophageal bleeding, , Cause, , Presenting features, , Oesophagitis, , Small volume of fresh blood, often streaking vomit. Malaena rare. Often ceases, spontaneously. Usually history of antecedent GORD type symptoms., , Cancer, , Usually small volume of blood, except as pre terminal event with erosion of, major vessels. Often associated symptoms of dysphagia and constitutional, symptoms such as weight loss. May be recurrent until malignancy managed.
Page 2717 :
Mallory Weiss, Tear, , Typically brisk small to moderate volume of bright red blood following bout of, repeated vomiting. Malaena rare. Usually ceases spontaneously., , Varices, , Usually large volume of fresh blood. Swallowed blood may cause malaena., Often associated with haemodynamic compromise. May stop spontaneously but, re-bleeds are common until appropriately managed., , Gastric Bleeding, , Cause, , Presenting features, , Gastric, cancer, , May be frank haematemesis or altered blood mixed with vomit. Usually, prodromal features of dyspepsia and may have constitutional symptoms. Amount, of bleeding variable but erosion of major vessel may produce considerable, haemorrhage., , Dieulafoy, Lesion, , Often no prodromal features prior to haematemesis and malaena, but this, arteriovenous malformation may produce quite considerable haemorrhage and, may be difficult to detect endoscopically., , Diffuse, erosive, gastritis, , Usually haematemesis and epigastric discomfort. Usually there is an underlying, cause such as recent NSAID usage. Large volume haemorrhage may occur with, considerable haemodynamic compromise., , Gastric ulcer, , Small low volume bleeds more common so would tend to present as iron, deficiency anaemia. Erosion into a significant vessel may produce considerable, haemorrhage and haematemesis., , Duodenum, Most common cause of major haemorrhage is a posteriorly sited duodenal ulcer. However, ulcers at, any site in the duodenum may present with haematemesis, malaena and epigastric discomfort. The, pain of duodenal ulcer is slightly different to that of gastric ulcers and often occurs several hours, after eating. Peri ampullary tumours may bleed but these are rare. In patients with previous, abdominal aortic aneurysm surgery aorto-enteric fistulation remains a rare but important cause of, major haemorrhage associated with high mortality., Management
Page 2718 :
, , , , , , , , , , , , , , , Admission to hospital careful monitoring, cross match blood, check FBC, LFTs, U+E and, Clotting (as a minimum), Patients with on-going bleeding and haemodynamic instability are likely to require O negative, blood pending cross matched blood, Early control of airway is vital (e.g. Drowsy patient with liver failure), Patients with suspected varices should receive terlipressin prior to endoscopy, Ideally all patients admitted with upper gastrointestinal haemorrhage should undergo Upper, GI endoscopy within 24 hours of admission. In those who are unstable this should occur, immediately after resuscitation or in tandem with it. The endoscopy department is a, potentially dangerous place for unstable patients and it may be safer to perform the, endoscopy in theatre with an anaesthetist present., Varices should be banded or subjected to sclerotherapy. If this is not possible owing to active, bleeding then a Sengaksten- Blakemore tube (or Minnesota tube) should be inserted. This, should be done with care; gastric balloon should be inflated first and oesophageal balloon, second. Remember the balloon will need deflating after 12 hours (ideally sooner) to prevent, necrosis. Portal pressure should be lowered by combination of medical therapy +/- TIPSS., Patients with erosive oesophagitis / gastritis should receive a proton pump inhibitor., Mallory Weiss tears will typically resolve spontaneously, Identifiable bleeding points should receive combination therapy of injection of adrenaline and, either a thermal or mechanical treatment. All who have received intervention should receive, a continuous infusion of a proton pump inhibitor (IV omeprazole for 72 hours) to reduce the, re-bleeding rate., Patients with diffuse erosive gastritis who cannot be managed endoscopically and continue, to bleed may require gastrectomy, Bleeding ulcers that cannot be controlled endoscopically may require laparotomy and ulcer, underruning, , Indications for surgery, , , , , , Patients > 60 years, Continued bleeding despite endoscopic intervention, Recurrent bleeding, Known cardiovascular disease with poor response to hypotension, , Surgery, Duodenal ulcer, Laparotomy, duodenotomy and under running of the ulcer. If bleeding is brisk then the ulcer is, almost always posteriorly sited and will have invaded the gastroduodenal artery. Large bites using 0, Vicryl are taken above and below the ulcer base to occlude the vessel. The duodenotomy should be, longitudinal but closed transversely to avoid stenosis., For gastric ulcer, Under-running of the bleeding site, Partial gastrectomy-antral ulcer, Partial gastrectomy or under running the ulcer- lesser curve ulcer (involving left gastric artery), Total gastrectomy if bleeding persists, Summary of Acute Upper GI bleeding recommendations:
Page 2719 :
The need for admission and timing of endoscopic intervention may be predicted by using the, Blatchford score. This considers a patients Hb, serum urea, pulse rate and blood pressure. Those, patients with a score of 0 are low risk, all others are considered high risk and require admission and, endoscopy., The requirement for pre endoscopic proton pump inhibition is contentious. In the UK the National, Institute of Clinical Excellence guidelines suggest the pre endoscopic PPI therapy is unnecessary., Whilst it is accepted that such treatment has no impact on mortality or morbidity a Cochrane review, of this practice in 2007 did suggest that it reduced the stigmata of recent haemorrhage at, endoscopy. As a result many will still administer PPI to patients prior to endoscopic intervention., Following endoscopy it is important to calculate the Rockall score for patients to determine their risk, of rebleeding and mortality. A score of 3 or less is associated with a rebleeding rate of 4% and a, very low risk of mortality and identifies a group of patients suitable for early discharge., References, 1. http://www.sign.ac.uk/guidelines/fulltext/105/index.html, 2. Joint Advisory Group on Endoscopy (JAG) Guidelines - http://www.thejag.org.uk, 3. NICE Guideline: Management of acute upper GI bleeding. July 2012., Next question
Page 2720 :
Which of the following criteria is not an indication for bariatric surgery to be performed in the UK, National Institute of Clinical Excellence Guidelines?, , Patients must be non smoking for at least one year, , Patients must have tried conservative management for at least 6 months, , Commitment to long-term follow up, , Surgery to be performed in a specialist unit, , BMI > 40 kg/m2, , Being a non smoker is not included in the criteria, however poor respiratory function due to smoking, may affect fitness for surgery., Please rate this question:, , Discuss and give feedback, , Next question, , Bariatric surgery, Obesity is a major health problem in the Western world. Surgical solutions to the problem have, evolved dramatically over the past few years. Randomised controlled trials have shown that dramatic, weight loss can be achieved following surgical interventions compared with standard medical, therapy. The weight loss process is also more durable following surgery than with non surgical, interventions., Case selection, BMI >/= 40 kg/m 2 or between 35-40 kg/m 2 and other significant disease (for example, type 2, diabetes, hypertension) that could be improved with weight loss., Pre-requisites to surgery (NICE UK Guidelines), , , , , , , All non-surgical measures have failed to achieve or maintain adequate clinically beneficial, weight loss for at least 6 months., Will receive intensive specialist management, They are generally fit for anaesthesia and surgery, They commit to the need for long-term follow-up, First-line option for adults with a BMI > 50 kg/m 2 in whom surgical intervention is considered, appropriate; consider orlistat if there is a long waiting list.
Page 2721 :
Surgical options, , Adjustable gastric, band, , , , , , , , , Gastric bypass, , Sleeve gastrectomy, , , , Laparoscopic placement of adjustable band around proximal, stomach., Contains an adjustable filling port, Effective method for lifestyle control, Reversible, Takes longer to achieve target weight, Complications such as band erosion (rare), slippage or loss of, efficacy may require re-intervention, , , , , , , Combines changes to reservoir size with malabsorptive procedure, for more enduring weight loss., Technically more challenging, Risks related to anastomoses (2% leak rate), Irreversible, Up to 50% may become B12 deficient, , , , , Resection of stomach using stapling devices, Less popular now as initial promising results not sustained, , References, 1. National Institute for Health and Clinical Excellence. Obesity: the prevention, identification,, assessment and management of overweight and obesity in adults and children., www.nice.org.uk/CG43, 2. Leff DR, Heath D. Surgery for obesity in adulthood. BMJ 2009;339:b3402, Next question
Page 2722 :
A 34-year-old HIV positive man is referred to the surgical out patient department with jaundice and, abnormal liver function tests. Liver function tests are as follows:, , Albumin, , 34 g/l, , ALP, , 540 iu/l, , Bilirubin, , 67 µmol/l, , ALT, , 45 iu/l, , What is the most likely diagnosis?, , Hepatic abscess, , Fungal obstruction of the bile duct, , Duodenal adenoma, , Primary biliary cirrhosis, , Sclerosing cholangitis, , The LFTs clearly show a cholestatic picture. Given the background of HIV the most likely cause is, sclerosing cholangitis., Please rate this question:, , Discuss and give feedback, , Next question
Page 2723 :
HIV: biliary and pancreatic disease, The most common cause of biliary disease in patients with HIV is sclerosing cholangitis due to, infections such as CMV, Cryptosporidium and Microsporidia, Pancreatitis in the context of HIV infection may be secondary to anti-retroviral treatment (especially, didanosine) or by opportunistic infections e.g. CMV, Next question
Page 2724 :
A 42 year old woman with known multiple gastric ulcers attends the surgical out patient unit. She has, not improved despite 2 months of proton pump inhibitor treatment. She is found to have a, gastrinoma. Which of the following is false in relation to her diagnosis?, , Most commonly found in the pancreas, , Associated with multiple endocrine neoplasia I, , Somatostatin sensitive scintigraphy is the most senstive non invasive test for localizing, primary tumours, Primary tumours can occur in the ovary, , Secretory diarrhoea is a feature, , Most commonly found in the duodenum (in up to 50% patients), then the pancreas (approximately, 20%). Other ectopic areas include stomach, spleen, gallbladder and ovary, , , Greater than 4/5 of gastrinomas are found within the triangle bounded by:, , Cystic and common bile duct (Top), 2nd and 3rd part of the duodenum (Bottom), Neck and body of pancreas (Medial), , , , Pancreatic gastrinomas are normally solitary and highly malignant., Zollinger Ellison syndrome is composed of the triad of:, , 1. Non beta islet cell tumours of the pancreas, 2. Hypergastrinaemia, 3. Severe ulcer disease, Clinical features related to peptic ulcer disease. Diagnosis is based on 3 criteria:, 1. Fasting hypergastrinaemia, 2. Increased basal acid output, 3. Secretin stimulation test positive, Management, , , Resection if localised disease, , Please rate this question:
Page 2725 :
Discuss and give feedback, , Next question, , Pancreatic cancer, , , , , , , Adenocarcinoma, Risk factors: Smoking, diabetes, adenoma, familial adenomatous polyposis, Mainly occur in the head of the pancreas (70%), Spread locally and metastasizes to the liver, Carcinoma of the pancreas should be differentiated from other periampullary tumours with, better prognosis, , Clinical features, , , , , , , Weight loss, Painless jaundice, Epigastric discomfort (pain usually due to invasion of the coeliac plexus is a late feature), Pancreatitis, Trousseau's sign: migratory superficial thrombophlebitis, , Investigations, , , , , , , USS: May miss small lesions, CT Scanning (pancreatic protocol). If unresectable on CT then no further staging needed, PET/CT for those with operable disease on CT alone, ERCP/ MRI for bile duct assessment, Staging laparoscopy to exclude peritoneal disease, , Management, , , , , , , Head of pancreas: Whipple's resection (SE dumping and ulcers). Newer techniques include, pylorus preservation and SMA/ SMV resection, Carcinoma body and tail: poor prognosis, distal pancreatectomy, if operable, Usually adjuvent chemotherapy for resectable disease, ERCP and stent for jaundice and palliation, Surgical bypass may be needed for duodenal obstruction, , Next question
Page 2726 :
A 45 year old man is admitted with haematemesis. An upper gastrointestinal endoscopy is, performed. A large ulcer in the first part of the duodenum is noted. Attempts are made to, endoscopically clip and inject the ulcer which is bleeding profusely. These efforts are unsuccessful., What is the most appropriate management option?, , Therapeutic angiogram, , Diagnostic angiography, , Laparotomy and underrunning of the ulcer, , Laparotomy and distal gastrectomy, , Duodenal resection and gastro jejunostomy, , The standard surgical option for bleeding peptic ulcers is to underrun them. Resectional surgery is, very much the option of last resort and is seldom helpful or easy. An isolated duodenal resection, would almost never be performed., Please rate this question:, , Discuss and give feedback, , Next question, , Upper gastrointestinal bleeding, Patients may present with the following:, , , , , Haematemesis and/ or malaena, Epigastric discomfort, Sudden collapse, , The extent to which these will occur will depend upon the source. Mortality is higher in patients, presenting with haematemesis than malaena alone., Oesophageal bleeding, , Cause, , Presenting features
Page 2727 :
Oesophagitis, , Small volume of fresh blood, often streaking vomit. Malaena rare. Often ceases, spontaneously. Usually history of antecedent GORD type symptoms., , Cancer, , Usually small volume of blood, except as pre terminal event with erosion of, major vessels. Often associated symptoms of dysphagia and constitutional, symptoms such as weight loss. May be recurrent until malignancy managed., , Mallory Weiss, Tear, , Typically brisk small to moderate volume of bright red blood following bout of, repeated vomiting. Malaena rare. Usually ceases spontaneously., , Varices, , Usually large volume of fresh blood. Swallowed blood may cause malaena., Often associated with haemodynamic compromise. May stop spontaneously but, re-bleeds are common until appropriately managed., , Gastric Bleeding, , Cause, , Presenting features, , Gastric, cancer, , May be frank haematemesis or altered blood mixed with vomit. Usually, prodromal features of dyspepsia and may have constitutional symptoms. Amount, of bleeding variable but erosion of major vessel may produce considerable, haemorrhage., , Dieulafoy, Lesion, , Often no prodromal features prior to haematemesis and malaena, but this, arteriovenous malformation may produce quite considerable haemorrhage and, may be difficult to detect endoscopically., , Diffuse, erosive, gastritis, , Usually haematemesis and epigastric discomfort. Usually there is an underlying, cause such as recent NSAID usage. Large volume haemorrhage may occur with, considerable haemodynamic compromise., , Gastric ulcer, , Small low volume bleeds more common so would tend to present as iron, deficiency anaemia. Erosion into a significant vessel may produce considerable, haemorrhage and haematemesis., , Duodenum, Most common cause of major haemorrhage is a posteriorly sited duodenal ulcer. However, ulcers at
Page 2728 :
any site in the duodenum may present with haematemesis, malaena and epigastric discomfort. The, pain of duodenal ulcer is slightly different to that of gastric ulcers and often occurs several hours, after eating. Peri ampullary tumours may bleed but these are rare. In patients with previous, abdominal aortic aneurysm surgery aorto-enteric fistulation remains a rare but important cause of, major haemorrhage associated with high mortality., Management, , , , , , , , , , , , , , , , Admission to hospital careful monitoring, cross match blood, check FBC, LFTs, U+E and, Clotting (as a minimum), Patients with on-going bleeding and haemodynamic instability are likely to require O negative, blood pending cross matched blood, Early control of airway is vital (e.g. Drowsy patient with liver failure), Patients with suspected varices should receive terlipressin prior to endoscopy, Ideally all patients admitted with upper gastrointestinal haemorrhage should undergo Upper, GI endoscopy within 24 hours of admission. In those who are unstable this should occur, immediately after resuscitation or in tandem with it. The endoscopy department is a, potentially dangerous place for unstable patients and it may be safer to perform the, endoscopy in theatre with an anaesthetist present., Varices should be banded or subjected to sclerotherapy. If this is not possible owing to active, bleeding then a Sengaksten- Blakemore tube (or Minnesota tube) should be inserted. This, should be done with care; gastric balloon should be inflated first and oesophageal balloon, second. Remember the balloon will need deflating after 12 hours (ideally sooner) to prevent, necrosis. Portal pressure should be lowered by combination of medical therapy +/- TIPSS., Patients with erosive oesophagitis / gastritis should receive a proton pump inhibitor., Mallory Weiss tears will typically resolve spontaneously, Identifiable bleeding points should receive combination therapy of injection of adrenaline and, either a thermal or mechanical treatment. All who have received intervention should receive, a continuous infusion of a proton pump inhibitor (IV omeprazole for 72 hours) to reduce the, re-bleeding rate., Patients with diffuse erosive gastritis who cannot be managed endoscopically and continue, to bleed may require gastrectomy, Bleeding ulcers that cannot be controlled endoscopically may require laparotomy and ulcer, underruning, , Indications for surgery, , , , , , Patients > 60 years, Continued bleeding despite endoscopic intervention, Recurrent bleeding, Known cardiovascular disease with poor response to hypotension, , Surgery, Duodenal ulcer, Laparotomy, duodenotomy and under running of the ulcer. If bleeding is brisk then the ulcer is, almost always posteriorly sited and will have invaded the gastroduodenal artery. Large bites using 0, Vicryl are taken above and below the ulcer base to occlude the vessel. The duodenotomy should be, longitudinal but closed transversely to avoid stenosis.
Page 2729 :
For gastric ulcer, Under-running of the bleeding site, Partial gastrectomy-antral ulcer, Partial gastrectomy or under running the ulcer- lesser curve ulcer (involving left gastric artery), Total gastrectomy if bleeding persists, Summary of Acute Upper GI bleeding recommendations:, The need for admission and timing of endoscopic intervention may be predicted by using the, Blatchford score. This considers a patients Hb, serum urea, pulse rate and blood pressure. Those, patients with a score of 0 are low risk, all others are considered high risk and require admission and, endoscopy., The requirement for pre endoscopic proton pump inhibition is contentious. In the UK the National, Institute of Clinical Excellence guidelines suggest the pre endoscopic PPI therapy is unnecessary., Whilst it is accepted that such treatment has no impact on mortality or morbidity a Cochrane review, of this practice in 2007 did suggest that it reduced the stigmata of recent haemorrhage at, endoscopy. As a result many will still administer PPI to patients prior to endoscopic intervention., Following endoscopy it is important to calculate the Rockall score for patients to determine their risk, of rebleeding and mortality. A score of 3 or less is associated with a rebleeding rate of 4% and a, very low risk of mortality and identifies a group of patients suitable for early discharge., References, 1. http://www.sign.ac.uk/guidelines/fulltext/105/index.html, 2. Joint Advisory Group on Endoscopy (JAG) Guidelines - http://www.thejag.org.uk, 3. NICE Guideline: Management of acute upper GI bleeding. July 2012., Next question
Page 2730 :
Which of the procedures listed below is most strongly associated with delayed gastric emptying?, , Posterior gastrojejunostomy, , Pyloromyotomy, , Pyloroplasty, , Anterior gastrojejunostomy, , Roux en Y gastrojejunostomy, , Anterior gastrojejunostomy is one of the easiest gastric bypass procedures to perform and is still, often used for reconstruction following distal gastrectomy. It is associated with impairment of gastric, emptying and patients may have considerable problems with flatulent dyspepsia. Roux en Y, methods provide the best function. Pyloroplasty enhances gastric emptying (and was historically, performed following vagotomy for this reason). Pyloromyotomy is not associated with an increase in, gastric transit times (though failed procedures may be)., Please rate this question:, , Discuss and give feedback, , Next question, , Gastric emptying, , , , , The stomach serves both a mechanical and immunological function. Solid and liquid are, retained in the stomach during which time repeated peristaltic activity against a closed, pyloric sphincter will cause fragmentation of food bolus material. Contact with gastric acid will, help to neutralise any pathogens present., The amount of time material spends in the stomach is related to its composition and volume., For example a glass of water will empty more quickly than a large meal. The presence of, amino acids and fat will all serve to delay gastric emptying., , Controlling factors, Neuronal stimulation of the stomach is mediated via the vagus and the parasympathetic nervous, system will tend to favor an increase in gastric motility. It is for this reason that individuals who have, undergone truncal vagotomy will tend to routinely require either a pyloroplasty or gastro-enterostomy, as they would otherwise have delayed gastric emptying., The following hormonal factors are all involved:
Page 2731 :
Delay emptying, , Increase emptying, , Gastric inhibitory peptide, , Gastrin, , Cholecystokinin, , Enteroglucagon, , Diseases affecting gastric emptying, All diseases that affect gastric emptying may result in bacterial overgrowth, retained food and, eventually the formation of bezoars that may occlude the pylorus and make gastric emptying even, worse. Fermentation of food may cause dyspepsia, reflux and foul smelling belches of gas., Iatrogenic, Gastric surgery can have profound effects on gastric emptying. As stated above any procedure that, disrupts the vagus can cause delayed emptying. Whilst this is particularly true of vagotomy, this, operation is now rarely performed. Surgeons are divided on the importance of vagal disruption that, occurs during an oesophagectomy, some will routinely perform a pyloroplasty and others will not., When a distal gastrectomy is performed, the type of anastomosis performed will impact on emptying., When a gastro-enterostomy is constructed, a posterior, retrocolic gastroenterostomy will empty, better than an anterior one., Diabetic gastroparesis, This is predominantly due to neuropathy affecting the vagus nerve. The stomach empties poorly and, patients may have episodes of repeated and protracted vomiting. Diagnosis is made by upper GI, endoscopy and contrast studies, in some cases a radio nucleotide scan is needed to demonstrate, the abnormality more clearly. In treating these conditions, drugs such as metoclopramide will be less, effective as they exert their effect via the vagus nerve. One of the few prokinetic drugs that do not, work in this way is the antibiotic erythromycin., Malignancies, Obviously a distal gastric cancer may obstruct the pylorus and delay emptying. In addition,, malignancies of the pancreas may cause extrinsic compression of the duodenum and delay, emptying. Treatment in these cases is by gastric decompression using a wide bore nasogastric tube, and insertion of a stent or, if that is not possible, by a surgical gastroenterostomy. As a general rule, gastroenterostomies constructed for bypass of malignancy are usually placed on the anterior wall of, the stomach (in spite of the fact that they empty less well). A Roux en Y bypass may also be, undertaken, but the increased number of anastomoses for this, in malignant disease that is being, palliated, is probably not justified., Congenital Hypertrophic Pyloric Stenosis, This is typically a disease of infancy. Most babies will present around 6 weeks of age with projectile, non bile stained vomiting. It has an incidence of 2.4 per 1000 live births and is more common in, males. Diagnosis is usually made by careful history and examination and a mass may be palpable in
Page 2732 :
the epigastrium (often cited seldom felt!). The most important diagnostic test is an ultrasound that, usually demonstrates the hypertrophied pylorus. Blood tests may reveal a hypochloraemic metabolic, alkalosis if the vomiting is long standing. Once the diagnosis is made the infant is resuscitated and a, pyloromyotomy is performed (either open or laparoscopically). Once treated there are no long term, sequelae., Next question
Page 2733 :
A 63 year old man undergoes a total gastrectomy for carcinoma of the stomach. Which of the, sequelae below is least likely to occur?, , Metabolic bone disease, , Bile reflux, , Dumping syndrome, , Zinc deficiency, , B12 deficiency, , Zinc is mainly absorbed in the duodenum and jejunum. Bile reflux may occur post gastrectomy. The, risk of bile reflux is lower if a Roux en Y reconstruction is used., Please rate this question:, , Discuss and give feedback, , Next question, , Post gastrectomy syndromes, Post gastrectomy syndromes may vary slightly depending upon whether a total of partial, gastrectomy is performed. A Roux en Y reconstruction generally gives the best functional outcomes., Where a gastrojejunostomy is performed as reconstruction following a distal gastrectomy the gastric, emptying is generally better if the jejunal limbs are tunneled in the retrocolic plane., The following may occur following gastrectomy:, , , , , , , , , Small capacity (early satiety), Dumping syndrome, Bile gastritis, Afferent loop syndrome, Efferent loop syndrome, Anaemia (B12 deficiency), Metabolic bone disease, Next question
Page 2734 :
A 34 year old women with morbid obesity is referred for consideration of bariatric surgery. Which of, the following options is associated with the highest long term failure rates?, , Gastric band, , Intra gastric balloon, , Roux en Y bypass, , Sleeve gastrectomy, , Duodenal switch, , Intragastric balloon is really only suitable as a bridge to a more definitive surgical solution., Bariatric surgery: the main operations, Gastric banding: band applied to upper stomach which can be inflated or deflated with normal, saline. This affects satiety. Over a 5 year period complications requiring further surgery occur in up, to 15% cases., Roux-en-Y gastric bypass: a gastric pouch is formed and connected to the jejunum. Patients, achieve greater and more longterm weight loss than gastric banding., Sleeve gastrectomy: body and fundus resected to leave a small section of stomach, Biliopancreatic diversion +/- duodenal switch: bypass the small bowel. Greatest weight loss but a, very complex procedure associated with malnutrition and diarrhoea., Vertical banded gastroplasty (stomach stapling): rarely performed due to longterm failure rate., Please rate this question:, , Discuss and give feedback, , Next question, , Bariatric surgery, Obesity is a major health problem in the Western world. Surgical solutions to the problem have, evolved dramatically over the past few years. Randomised controlled trials have shown that dramatic, weight loss can be achieved following surgical interventions compared with standard medical, therapy. The weight loss process is also more durable following surgery than with non surgical, interventions.
Page 2735 :
Case selection, BMI >/= 40 kg/m 2 or between 35-40 kg/m 2 and other significant disease (for example, type 2, diabetes, hypertension) that could be improved with weight loss., Pre-requisites to surgery (NICE UK Guidelines), , , , , , , All non-surgical measures have failed to achieve or maintain adequate clinically beneficial, weight loss for at least 6 months., Will receive intensive specialist management, They are generally fit for anaesthesia and surgery, They commit to the need for long-term follow-up, First-line option for adults with a BMI > 50 kg/m 2 in whom surgical intervention is considered, appropriate; consider orlistat if there is a long waiting list., , Surgical options, , Adjustable gastric, band, , , , , , , , , Gastric bypass, , Sleeve gastrectomy, , , , Laparoscopic placement of adjustable band around proximal, stomach., Contains an adjustable filling port, Effective method for lifestyle control, Reversible, Takes longer to achieve target weight, Complications such as band erosion (rare), slippage or loss of, efficacy may require re-intervention, , , , , , , Combines changes to reservoir size with malabsorptive procedure, for more enduring weight loss., Technically more challenging, Risks related to anastomoses (2% leak rate), Irreversible, Up to 50% may become B12 deficient, , , , , Resection of stomach using stapling devices, Less popular now as initial promising results not sustained, , References, 1. National Institute for Health and Clinical Excellence. Obesity: the prevention, identification,, assessment and management of overweight and obesity in adults and children., www.nice.org.uk/CG43, 2. Leff DR, Heath D. Surgery for obesity in adulthood. BMJ 2009;339:b3402, Next question
Page 2736 :
Theme: Gastric ulceration, , A., B., C., D., E., F., G., , Acute peptic ulcer, Adenocarcinoma, Carcinoid Tumour, Gastrointestinal stromal tumour, Chronic peptic ulcer, Lymphosarcoma, Leiomyoma, , Please select the most likely cause of gastric ulceration for the scenario given. Each option may be, used once, more than once or not at all., , 49., , A 53 year old man presents with dyspepsia. At upper GI endoscopy he has a punched out, ulcer on the lesser curve of the stomach. It measures approximately 2cm in diameter and is, seen to penetrate muscle with fibrosis present at the base., You answered Acute peptic ulcer, The correct answer is Chronic peptic ulcer, Fibrosis is usually a sign of chronic ulcer. It should be biopsied carefully, a proton pump, inhibitor started and re endoscopy should occur at 6 weeks., , 50., , A 42 year old man presents with epigastric pain. At endoscopy, he is found to have a, punched out ulcer on the anterior wall of the stomach. It is shallow and measures 1cm in, diameter., Acute peptic ulcer, The absence of fibrosis coupled with small size suggests a more acute ulcer. Management, should include biopsy, PPI and repeat endoscopy at 6 weeks., , 51., , A 65 year old man presents with epigastric discomfort. At endoscopy he is found to have, an ulcer at the antrum, is has thick rolled edges and measures 3cm in diameter., You answered Acute peptic ulcer, The correct answer is Adenocarcinoma, Rolled edges and location favor tumour. Careful biopsies should be taken and staging CT, performed.
Page 2737 :
Please rate this question:, , Discuss and give feedback, , Next question, , Upper gastrointestinal bleeding, Patients may present with the following:, , , , , Haematemesis and/ or malaena, Epigastric discomfort, Sudden collapse, , The extent to which these will occur will depend upon the source. Mortality is higher in patients, presenting with haematemesis than malaena alone., Oesophageal bleeding, , Cause, , Presenting features, , Oesophagitis, , Small volume of fresh blood, often streaking vomit. Malaena rare. Often ceases, spontaneously. Usually history of antecedent GORD type symptoms., , Cancer, , Usually small volume of blood, except as pre terminal event with erosion of, major vessels. Often associated symptoms of dysphagia and constitutional, symptoms such as weight loss. May be recurrent until malignancy managed., , Mallory Weiss, Tear, , Typically brisk small to moderate volume of bright red blood following bout of, repeated vomiting. Malaena rare. Usually ceases spontaneously., , Varices, , Usually large volume of fresh blood. Swallowed blood may cause malaena., Often associated with haemodynamic compromise. May stop spontaneously but, re-bleeds are common until appropriately managed., , Gastric Bleeding, , Cause, , Presenting features, , Gastric, , May be frank haematemesis or altered blood mixed with vomit. Usually
Page 2738 :
cancer, , prodromal features of dyspepsia and may have constitutional symptoms. Amount, of bleeding variable but erosion of major vessel may produce considerable, haemorrhage., , Dieulafoy, Lesion, , Often no prodromal features prior to haematemesis and malaena, but this, arteriovenous malformation may produce quite considerable haemorrhage and, may be difficult to detect endoscopically., , Diffuse, erosive, gastritis, , Usually haematemesis and epigastric discomfort. Usually there is an underlying, cause such as recent NSAID usage. Large volume haemorrhage may occur with, considerable haemodynamic compromise., , Gastric ulcer, , Small low volume bleeds more common so would tend to present as iron, deficiency anaemia. Erosion into a significant vessel may produce considerable, haemorrhage and haematemesis., , Duodenum, Most common cause of major haemorrhage is a posteriorly sited duodenal ulcer. However, ulcers at, any site in the duodenum may present with haematemesis, malaena and epigastric discomfort. The, pain of duodenal ulcer is slightly different to that of gastric ulcers and often occurs several hours, after eating. Peri ampullary tumours may bleed but these are rare. In patients with previous, abdominal aortic aneurysm surgery aorto-enteric fistulation remains a rare but important cause of, major haemorrhage associated with high mortality., Management, , , , , , , , , , , , Admission to hospital careful monitoring, cross match blood, check FBC, LFTs, U+E and, Clotting (as a minimum), Patients with on-going bleeding and haemodynamic instability are likely to require O negative, blood pending cross matched blood, Early control of airway is vital (e.g. Drowsy patient with liver failure), Patients with suspected varices should receive terlipressin prior to endoscopy, Ideally all patients admitted with upper gastrointestinal haemorrhage should undergo Upper, GI endoscopy within 24 hours of admission. In those who are unstable this should occur, immediately after resuscitation or in tandem with it. The endoscopy department is a, potentially dangerous place for unstable patients and it may be safer to perform the, endoscopy in theatre with an anaesthetist present., Varices should be banded or subjected to sclerotherapy. If this is not possible owing to active, bleeding then a Sengaksten- Blakemore tube (or Minnesota tube) should be inserted. This, should be done with care; gastric balloon should be inflated first and oesophageal balloon, second. Remember the balloon will need deflating after 12 hours (ideally sooner) to prevent, necrosis. Portal pressure should be lowered by combination of medical therapy +/- TIPSS., Patients with erosive oesophagitis / gastritis should receive a proton pump inhibitor., Mallory Weiss tears will typically resolve spontaneously
Page 2739 :
, , , , , Identifiable bleeding points should receive combination therapy of injection of adrenaline and, either a thermal or mechanical treatment. All who have received intervention should receive, a continuous infusion of a proton pump inhibitor (IV omeprazole for 72 hours) to reduce the, re-bleeding rate., Patients with diffuse erosive gastritis who cannot be managed endoscopically and continue, to bleed may require gastrectomy, Bleeding ulcers that cannot be controlled endoscopically may require laparotomy and ulcer, underruning, , Indications for surgery, , , , , , Patients > 60 years, Continued bleeding despite endoscopic intervention, Recurrent bleeding, Known cardiovascular disease with poor response to hypotension, , Surgery, Duodenal ulcer, Laparotomy, duodenotomy and under running of the ulcer. If bleeding is brisk then the ulcer is, almost always posteriorly sited and will have invaded the gastroduodenal artery. Large bites using 0, Vicryl are taken above and below the ulcer base to occlude the vessel. The duodenotomy should be, longitudinal but closed transversely to avoid stenosis., For gastric ulcer, Under-running of the bleeding site, Partial gastrectomy-antral ulcer, Partial gastrectomy or under running the ulcer- lesser curve ulcer (involving left gastric artery), Total gastrectomy if bleeding persists, Summary of Acute Upper GI bleeding recommendations:, The need for admission and timing of endoscopic intervention may be predicted by using the, Blatchford score. This considers a patients Hb, serum urea, pulse rate and blood pressure. Those, patients with a score of 0 are low risk, all others are considered high risk and require admission and, endoscopy., The requirement for pre endoscopic proton pump inhibition is contentious. In the UK the National, Institute of Clinical Excellence guidelines suggest the pre endoscopic PPI therapy is unnecessary., Whilst it is accepted that such treatment has no impact on mortality or morbidity a Cochrane review, of this practice in 2007 did suggest that it reduced the stigmata of recent haemorrhage at, endoscopy. As a result many will still administer PPI to patients prior to endoscopic intervention., Following endoscopy it is important to calculate the Rockall score for patients to determine their risk, of rebleeding and mortality. A score of 3 or less is associated with a rebleeding rate of 4% and a, very low risk of mortality and identifies a group of patients suitable for early discharge., References, 1. http://www.sign.ac.uk/guidelines/fulltext/105/index.html, 2. Joint Advisory Group on Endoscopy (JAG) Guidelines - http://www.thejag.org.uk, 3. NICE Guideline: Management of acute upper GI bleeding. July 2012., Next question
Page 2740 :
Theme: Causes of dysphagia, , A., B., C., D., E., F., G., , Oesophageal cancer, Post radiotherapy fibrosis, Benign stricture, Plummer Vinson syndrome, Oesophageal candidiasis, Neuropathy, Globus, , Please select the most likely cause of dysphagia for the scenarios given. Each option may be used, once, more than once or not at all., , 52., , A cachectic 32 year old man with severe perineal Crohns disease is receiving treatment, with intravenous antibiotics. Over the past 72 hours he has complained of intermittent, dysphagia and odynophagia., You answered Oesophageal cancer, The correct answer is Oesophageal candidiasis, Treatment with systemic antibiotics may result in development of candidiasis. Patients, may present with odynophagia and episodic dysphagia. Endoscopic appearances are, usually diagnostic and treatment is with an oral anti fungal agent., , 53., , A 78 year old lady presents 6 years following a successfully treated squamous cell, carcinoma of the oesophagus. She has a long history of dysphagia but it is not progressive., You answered Oesophageal cancer, The correct answer is Post radiotherapy fibrosis, SCC of the oesophagus is commonly treated with chemoradiotherapy. Fibrosis and, dysphagia may occur in survivors., , 54., , A 32 year old lady presents with dysphagia. She has a 10 year history of anaemia, secondary to menorrhagia and has been strongly resistant to treatment., You answered Oesophageal cancer, The correct answer is Plummer Vinson syndrome, Plummer Vinson syndrome (oesophageal web) may occur in association with iron
Page 2741 :
deficiency anaemia (although rare!)., Please rate this question:, , Discuss and give feedback, , Next question, , Dysphagia, Causes of dysphagia, , Extrinsic, , , , , Mediastinal masses, Cervical spondylosis, , Oesophageal wall, , , , , , Achalasia, Diffuse oesophageal spasm, Hypertensive lower oesophageal sphincter, , Intrinsic, , , , , , , Tumours, Strictures, Oesophageal web, Schatzki rings, , Neurological, , , , , , , , CVA, Parkinson's disease, Multiple Sclerosis, Brainstem pathology, Myasthenia Gravis, , Investigation, All patients require an upper GI endoscopy unless there are compelling reasons for this not to be, performed. Motility disorders may be best appreciated by undertaking fluoroscopic swallowing, studies., A full blood count should be performed., Ambulatory oesophageal pH and manometry studies will be required to evaluate conditions such as, achalasia and patients with GORD being considered for fundoplication surgery., Next question
Page 2742 :
Which of the following is false during the pre operative preparation for surgery in pancreatic cancer?, , IV antibiotics should be given intra operatively, , Endotoxamia can be reduced with lactulose, , Subcutaneous heparin should be avoided, , Endotoxaemia can be reduced with IV mannitol, , There is a higher risk of complications if the bilirubin is greater than 150, , Vitamin K should be given to correct abnormal clotting initially, however there is still a risk of, thrombosis so low molecular weight heparin should be used. Bile salts can also be given to reduce, endotoxaemia. Biliary obstruction should be relieved. In the case of biliary obstruction, if a stent is, used it should be a made of plastic. Metallic stents will become embedded and may compromise, attempts at resection., Please rate this question:, , Discuss and give feedback, , Pancreatic cancer, , , , , , , Adenocarcinoma, Risk factors: Smoking, diabetes, adenoma, familial adenomatous polyposis, Mainly occur in the head of the pancreas (70%), Spread locally and metastasizes to the liver, Carcinoma of the pancreas should be differentiated from other periampullary tumours with, better prognosis, , Clinical features, , , , , , , Weight loss, Painless jaundice, Epigastric discomfort (pain usually due to invasion of the coeliac plexus is a late feature), Pancreatitis, Trousseau's sign: migratory superficial thrombophlebitis
Page 2743 :
Investigations, , , , , , , USS: May miss small lesions, CT Scanning (pancreatic protocol). If unresectable on CT then no further staging needed, PET/CT for those with operable disease on CT alone, ERCP/ MRI for bile duct assessment, Staging laparoscopy to exclude peritoneal disease, , Management, , , , , , , Head of pancreas: Whipple's resection (SE dumping and ulcers). Newer techniques include, pylorus preservation and SMA/ SMV resection, Carcinoma body and tail: poor prognosis, distal pancreatectomy, if operable, Usually adjuvent chemotherapy for resectable disease, ERCP and stent for jaundice and palliation, Surgical bypass may be needed for duodenal obstruction
Page 2745 :
A 39 year old man notices a swelling in his left hemiscrotum. On examination he has a left sided, varicocele. The ipsilateral testis is normal on palpation. What is the most appropriate course of, action?, , Scrotal exploration and ligation of the varicocele, , Abdominal ultrasound, , Scrotal ultrasound, , Left orchidectomy, , Discharge, , A left sided varicocele is a recognised presenting sign of a renal tumour occluding the renal vein, (into which the left testicular vein drains). An abdominal ultrasound should be undertaken to exclude, this. Surgery for uncomplicated varicocele is usually unnecessary., Please rate this question:, , Discuss and give feedback, , Next question, , Renal tumours, Renal cell carcinoma, Renal cell carcinoma is an adenocarcinoma of the renal cortex and is believed to arise from the, proximal convoluted tubule. They are usually solid lesions, up to 20% may be multifocal, 20% may, be calcified and 20% may have either a cystic component or be wholly cystic. They are often, circumscribed by a pseudocapsule of compressed normal renal tissue. Spread may occur either by, direct extension into the adrenal gland, renal vein or surrounding fascia. More distant disease, usually occurs via the haematogenous route to lung, bone or brain., Renal cell carcinoma comprise up to 85% of all renal malignancies. Males are more commonly, affected than females and sporadic tumours typically affect patients in their sixth decade., Patients may present with a variety of symptoms including; haematuria (50%), loin pain (40%), mass, (30%) and up to 25% may have symptoms of metastasis.Less than 10% have the classic triad of, haematuria, pain and mass., Investigation, Many cases will present as haematuria and be discovered during diagnostic work up. Benign renal, tumours are rare, so renal masses should be investigated with multislice CT scanning. Some units, will add and arterial and venous phase to the scan to demonstrate vascularity and evidence of caval, ingrowth.
Page 2746 :
CT scanning of the chest and abdomen to detect distant disease should also be undertaken., Routine bone scanning is not indicated in the absence of symptoms., Biopsy should not be performed when a nephrectomy is planned but is mandatory before any, ablative therapies are undertaken., Assessment of the functioning of the contra lateral kidney., Management, T1 lesions may be managed by partial nephrectomy and this gives equivalent oncological results to, total radical nephrectomy. Partial nephrectomy may also be performed when there is inadequate, reserve in the remaining kidney., For T2 lesions and above a radical nephrectomy is standard practice and this may be performed via, a laparoscopic or open approach. Preoperative embolisation is not indicated nor is resection of, uninvolved adrenal glands. During surgery early venous control is mandatory to avoid shedding of, tumour cells into the circulation., Patients with completely resected disease do not benefit from adjuvant therapy with either, chemotherapy or biological agents. These should not be administered outside the setting of clinical, trials., Patients with transitional cell cancer will require a nephroureterectomy with disconnection of the, ureter at the bladder., References, Lungberg B et al. EAU guidelines on renal cell carcinoma: The 2010 update. European Urology 2010, (58): 398-406., Next question
Page 2747 :
Theme: Management of urinary tract calculi, , A., B., C., D., E., F., G., , Nephrectomy, Open ureteric exploration, Extra corporeal shock wave lithotripsy, Percutaneous nephrostomy, Pyeloplasty, Conservative management, Percutaneous nephrolithotomy, , Please select the most appropriate management for the scenario given. Each option may be used, once, more than once or not at all., , 2., , A 23 year old male is admitted with left sided loin pain and fever. His investigations, demonstrate a left sided ureteric calculi that measures 0.7cm in diameter and associated, hydronephrosis., You answered Nephrectomy, The correct answer is Percutaneous nephrostomy, Theme from January 2013 Exam, An obstructed, infected system is an indication for urgent decompression. This may be, achieved by ureteroscopy or nephrostomy. In addition to this the patient should also receive, broad spectrum, intravenous antibiotics., , 3., , A 23 year old man is admitted with left sided loin pain that radiates to his groin. His, investigations demonstrate a 1cm left sided ureteric calculus with no associated, hydronephrosis., You answered Nephrectomy, The correct answer is Extra corporeal shock wave lithotripsy, Stones with a total volume of less than 2cm can be considered for lithotripsy. If it is, impacted in the upper ureter then some may consider a ureteroscopy., , 4., , A 30 year old male presents with left sided loin pain. His investigations demonstrate a large, left sided staghorn calculus that measures 2.3cm in diameter., You answered Nephrectomy, The correct answer is Percutaneous nephrolithotomy
Page 2748 :
Large, proximal stones are generally best managed with a percutaneous nephrolithotomy., The use of lithotripsy has low clearance rates. Where stones remain after the initial, procedure a repeat percutaneous nephrolithotomy is generally preferred over follow up, lithotripsy., Please rate this question:, , Discuss and give feedback, , Next question, , Management of renal stones, Urolithiasis will affect up to 15% of the worldwide population. The development of sudden onset loin, to groin pain which is colicky in nature is a classic feature in the history. It is nearly always, associated with haematuria that is either micro or macroscopic., Where the diagnosis is suspected the most sensitive and specific diagnostic test is helical, non, contrast, computerised tomographic (CT) scanning., Management, Most renal stones measuring less than 5mm in maximum diameter will typically pass within 4 weeks, of symptom onset. More intensive and urgent treatment is indicated in the presence of ureteric, obstruction, renal developmental abnormality such as horseshoe kidney and previous renal, transplant. Ureteric obstruction due to stones together with infection is a surgical emergency and the, system must be decompressed. Options include nephrostomy tube placement, insertion of ureteric, catheters and ureteric stent placement., In the non emergency setting the preferred options for treatment of stone disease include extra, corporeal shock wave lithotripsy, percutaneous nephrolithotomy, ureteroscopy, open surgery, remains an option for selected cases. However, minimally invasive options are the most popular first, line treatment., Shock wave lithotripsy, A shock wave is generated external to the patient, internally cavitation bubbles and mechanical, stress lead to stone fragmentation. The passage of shock waves can result in the development of, solid organ injury. Fragmentation of larger stones may result in the development of ureteric, obstruction. The procedure is uncomfortable for patients and analgesia is required during the, procedure and afterwards., Ureteroscopy, A ureteroscope is passed retrograde through the ureter and into the renal pelvis. It is indicated in, individuals (e.g. pregnant females) where lithotripsy is contraindicated and in complex stone, disease. In most cases a stent is left in situ for 4 weeks after the procedure., Percutaneous nephrolithotomy, In this procedure access is gained to the renal collecting system. Once access is achieved, intra, corporeal lithotripsy or stone fragmentation is performed and stone fragments removed., Therapeutic selection
Page 2750 :
Theme: Testicular disorders, , A. Antibiotics, B. Aspiration, C. Testicular exploration after 6 hours, D. Testicular exploration within 6 hours, E. Orchidectomy via inguinal approach, F. Orchidectomy via scrotal approach, G. No treatment needed, H. Ligation of patent processus vaginalis via inguinal approach, I. Jaboulay procedure via scrotal approach, , For each scenario please select the most appropriate management. Each option may be used once,, more than once or not at all., , 5., , A parent brings her 4 year old child to the surgical clinic. She has noticed an intermittent swelling in, the right scrotum that is worse in the evening. On examination he has a soft fluctuant swelling in, the right scrotum that cannot be separated from the testis. It transilluminates when a pen torch is, held against it., You answered Antibiotics, The correct answer is Ligation of patent processus vaginalis via inguinal approach, In children, a hydrocele is most commonly due to a persistent processus vaginalis. The swelling is, intermittent and in most cases that are diagnosed in infancy the hydrocele resolves. Cases that, persist beyond two years of age are best managed surgically and the surgical approach is usually, made via the inguinal canal where the patent processus is identified and ligated., , 6., , A 20 year old complains of severe pain in the right scrotal area after jumping onto his moped. He, has noticed discomfort intermittently in this area over the past few months. Clinically the testis is, tender.
Page 2751 :
You answered Antibiotics, The correct answer is Testicular exploration within 6 hours, Testicular torsion: Severe pain which can be spontaneous or precipitated by minor trauma. The, patient may have noticed pain previously. Surgical intervention is needed as soon as possible to, prevent the risk of loss of the testis., , 7., , A 44 year old man is referred to the clinic because of an swelling in the right scrotum. This is, present most of the time and he is otherwise well with no urinary symptoms. On examination he, has a soft, fluctuant swelling in the right scrotum that transilluminates easily. An ultrasound is, performed that confirms that the underlying testicle is structurally normal., You answered Antibiotics, The correct answer is Jaboulay procedure via scrotal approach, Adult hydroceles are less commonly due to the persistence of embryonic remnants and therefore, can be managed via a scrotal approach. Both the Lords and Jaboulay procedures are reasonable, options., , Please rate this question:, , Discuss and give feedback, , Next question, , Scrotal swelling, Differential diagnosis, , Inguinal hernia, , If inguinoscrotal swelling; cannot "get above it" on examination, Cough impulse may be present
Page 2752 :
May be reducible, , Testicular tumours, , Often discrete testicular nodule (may have associated hydrocele), Symptoms of metastatic disease may be present, USS scrotum and serum AFP and β HCG required, , Acute epididymoorchitis, , Often history of dysuria and urethral discharge, Swelling may be tender and eased by elevating testis, Most cases due to Chlamydia, Infections with other gram negative organisms may be associated with underlying, structural abnormality, , Epididymal cysts, , Single or multiple cysts, May contain clear or opalescent fluid (spermatoceles), Usually occur over 40 years of age, Painless, Lie above and behind testis, It is usually possible to "get above the lump" on examination, , Hydrocele, , Non painful, soft fluctuant swelling, Often possible to "get above it" on examination, Usually contain clear fluid, Will often transilluminate, May be presenting feature of testicular cancer in young men, , Testicular torsion, , Severe, sudden onset testicular pain, Risk factors include abnormal testicular lie, Typically affects adolescents and young males, On examination testis is tender and pain not eased by elevation, Urgent surgery is indicated, the contra lateral testis should also be fixed, , Varicocele, , Varicosities of the pampiniform plexus, Typically occur on left (because testicular vein drains into renal vein), May be presenting feature of renal cell carcinoma, Affected testis may be smaller and bilateral varicoceles may affect fertility
Page 2753 :
Management, , , , , , , , , Testicular malignancy is always treated with orchidectomy via an inguinal approach. This, allows high ligation of the testicular vessels and avoids exposure of another lymphatic field to, the tumour., Torsion is commonest in young teenagers and the history in older children can be difficult to, elicit. Intermittent torsion is a recognised problem. The treatment is prompt surgical, exploration and testicular fixation. This can be achieved using sutures or by placement of the, testis in a Dartos pouch., Varicoceles are usually managed conservatively. If there are concerns about testicular, function of infertility then surgery or radiological management can be considered., Epididymal cysts can be excised using a scrotal approach, Hydroceles are managed differently in children where the underlying pathology is a patent, processus vaginalis and therefore an inguinal approach is used in children so that the, processus can be ligated. In adults a scrotal approach is preferred and the hydrocele sac, excised or plicated., Next question
Page 2754 :
Theme: Urinary tract trauma, , A., B., C., D., E., F., , Urinary tract infection, Bladder outlet obstruction, Bulbar urethral rupture, Membranous urethral rupture, Bladder rupture, Bladder contusion, , For the scenario given please select the most likely injury. Each option may be used once, more, than once or not at all., , 8., , A 56 year old man is involved in a road traffic accident. He is found to have a pelvic, fracture. He reports that he has some lower abdominal pain. He has peritonism in the lower, abdomen. The nursing staff report that he has not passed any urine. A CT scan shows, evidence of free fluid., You answered Urinary tract infection, The correct answer is Bladder rupture, A pelvic fracture and lower abdominal peritonism should raise suspicions of bladder, rupture (especially as this man cannot pass urine)., , 9., , A 52 year old man falls off his bike. He is found to have a pelvic fracture. On examination, he is found to have perineal oedema and on PR the prostate is not palpable. A urine, dipstick shows blood., You answered Urinary tract infection, The correct answer is Membranous urethral rupture, A pelvic fracture and highly displaced prostate should indicate a diagnosis of membranous, urethral rupture., , 10., , A 52 year old woman falls out of a tree while rescuing a cat. Imaging shows no bony, injury. She has suprapubic tenderness and complains of dysuria. Her abdomen is soft and, non tender. A urine dipstick shows blood, nitrites and leucocytes., Urinary tract infection, There is no indication of a more sinister diagnosis here. The patient's abdomen is normal, and she is able to pass urine. Her dipstick confirms an infection. Also in women urethral
Page 2755 :
injury is rare., Similar theme questions in September 2009 and April 2010, Please rate this question:, , Discuss and give feedback, , Next question, , Lower genitourinary tract trauma, , , , , , Most bladder injuries occur due to blunt trauma, 85% associated with pelvic fractures, Easily overlooked during assessment in trauma, Up to 10% of male pelvic fractures are associated with urethral or bladder injuries, , Types of injury, , Urethral injury, , , , , , Mainly in males, Blood at the meatus (50% cases), There are 2 types:, , i.Bulbar rupture, - most common, - straddle type injury e.g. bicycles, - triad signs: urinary retention, perineal haematoma, blood at the, meatus, ii. Membranous rupture, - can be extra or intraperitoneal, - commonly due to pelvic fracture, - Penile or perineal oedema/ hematoma, - PR: prostate displaced upwards (beware co-existing, retroperitoneal haematomas as they may make examination, difficult), - Investigation: ascending urethrogram, - Management: suprapubic catheter (surgical placement, not, percutaneously), External genitalia injuries, (i.e., the penis and the, scrotum), , , , Secondary to injuries caused by penetration, blunt trauma,, continence- or sexual pleasure-enhancing devices, and, mutilation
Page 2756 :
Bladder injury, , , , , , , , , rupture is intra or extraperitoneal, presents with haematuria or suprapubic pain, history of pelvic fracture and inability to void: always, suspect bladder or urethral injury, inability to retrieve all fluid used to irrigate the bladder, through a Foley catheter indicates bladder injury, investigation- IVU or cystogram, management: laparotomy if intraperitoneal, conservative if, extraperitoneal, Next question
Page 2757 :
Which of the following renal stone types is most radiodense on a plain x-ray?, , Calcium phosphate, , Calcium oxalate, , Uric acid, , Struvite, , Cystine, , Calcium phosphate stones are the most radiodense stones, calcium oxalate stones slightly less so., Uric acid stones are radiolucent (unless they have calcium contained within them)., Please rate this question:, , Discuss and give feedback, , Next question, , Renal stones, Type of, stones, , Calcium, oxalate, , Features, , Hypercalciuria is a major risk factor (various causes), Hyperoxaluria may also increase risk, Hypocitraturia increases risk because citrate forms complexes with, calcium making it more soluble, Stones are radio-opaque (though less than calcium phosphate stones), Hyperuricosuria may cause uric acid stones to which calcium oxalate, , Percentage of, all calculi, , 85%
Page 2758 :
Type of, stones, , Features, , Percentage of, all calculi, , binds, , Cystine, , Inherited recessive disorder of transmembrane cystine transport, leading to decreased absorption of cystine from intestine and renal, tubule, Multiple stones may form, Relatively radiodense because they contain sulphur, , 1%, , Uric acid, , Uric acid is a product of purine metabolism, May precipitate when urinary pH low, May be caused by diseases with extensive tissue breakdown e.g., malignancy, More common in children with inborn errors of metabolism, Radiolucent, , 5-10%, , Calcium, phosphate, , May occur in renal tubular acidosis, high urinary pH increases, supersaturation of urine with calcium and phosphate, Renal tubular acidosis types 1 and 3 increase risk of stone formation, (types 2 and 4 do not), Radio-opaque stones (composition similar to bone), , 10%, , Struvite, , Stones formed from magnesium, ammonium and phosphate, Occur as a result of urease producing bacteria (and are thus, associated with chronic infections), Under the alkaline conditions produced, the crystals can precipitate, Slightly radio-opaque, , 2-20%, , Effect of urinary pH on stone formation, Urine pH will show individual variation (from pH 5-7). Post prandially the pH falls as purine, metabolism will produce uric acid. Then the urine becomes more alkaline (alkaline tide). When the, stone is not available for analysis the pH of urine may help to determine which stone was present.
Page 2759 :
Stone type, , Urine acidity, , Mean urine pH, , Calcium phosphate, , Normal- alkaline, , >5.5, , Calcium oxalate, , Variable, , 6, , Uric acid, , Acid, , 5.5, , Struvate, , Alkaline, , >7.2, , Cystine, , Normal, , 6.5, Next question
Page 2760 :
Theme: Scrotal swellings, , A., B., C., D., E., F., , Haematocele, Epididymal cyst, Hydrocele, Testicular torsion, Orchitis, Epididymo-orchitis, , For each case please select the most likely underlying diagnosis from the list. Each option may be, used once, more than once or not at all., , 12., , A 32 year old male presents with a swollen right scrotum which has developed over 3, weeks after being kicked in the groin area. There is a non tense swelling of the right, scrotum and the underlying testis cannot be easily palpated. A dipstick is positive for, nitrates only., You answered Haematocele, The correct answer is Hydrocele, This is a secondary hydrocele which occurs in patients aged 20-40 years. It develops, rapidly and there may not be a tense swelling. The underlying testis is NOT palpated, therefore indicating a hydrocele. Causes include trauma, infection and tumour., , 13., , A 40 year old male presents with a non painful, bilateral scrotal swellings over 3 years., The testis is felt separately and the swelling transilluminates., You answered Haematocele, The correct answer is Epididymal cyst, The testis is palpated therefore this differentiates it from a hydrocele., , 14., , A 32 year old male presents with a swollen, painful right scrotum after being kicked in the, groin area 1 hour ago. There is a painful swelling of the right scrotum and the underlying, testis cannot be easily palpated., Haematocele, Acute haematocele: tense, tender and non transilluminating mass post trauma. A chronic, haematoma causes a blood clot to surround the testis. The blood clot hardens and contracts, causing a hard mass which may be indistinguishable from a tumour. Therefore the testis
Page 2761 :
will need surgical exploration., Please rate this question:, , Discuss and give feedback, , Next question, , Scrotal swelling, Differential diagnosis, , Inguinal hernia, , If inguinoscrotal swelling; cannot "get above it" on examination, Cough impulse may be present, May be reducible, , Testicular tumours, , Often discrete testicular nodule (may have associated hydrocele), Symptoms of metastatic disease may be present, USS scrotum and serum AFP and β HCG required, , Acute epididymoorchitis, , Often history of dysuria and urethral discharge, Swelling may be tender and eased by elevating testis, Most cases due to Chlamydia, Infections with other gram negative organisms may be associated with, underlying structural abnormality, , Epididymal cysts, , Single or multiple cysts, May contain clear or opalescent fluid (spermatoceles), Usually occur over 40 years of age, Painless, Lie above and behind testis, It is usually possible to "get above the lump" on examination, , Hydrocele, , Non painful, soft fluctuant swelling, Often possible to "get above it" on examination, Usually contain clear fluid, Will often transilluminate, May be presenting feature of testicular cancer in young men
Page 2762 :
Testicular torsion, , Severe, sudden onset testicular pain, Risk factors include abnormal testicular lie, Typically affects adolescents and young males, On examination testis is tender and pain not eased by elevation, Urgent surgery is indicated, the contra lateral testis should also be fixed, , Varicocele, , Varicosities of the pampiniform plexus, Typically occur on left (because testicular vein drains into renal vein), May be presenting feature of renal cell carcinoma, Affected testis may be smaller and bilateral varicoceles may affect fertility, , Management, , , , , , , , Testicular malignancy is always treated with orchidectomy via an inguinal approach. This, allows high ligation of the testicular vessels and avoids exposure of another lymphatic field to, the tumour., Torsion is commonest in young teenagers and the history in older children can be difficult to, elicit. Intermittent torsion is a recognised problem. The treatment is prompt surgical, exploration and testicular fixation. This can be achieved using sutures or by placement of the, testis in a Dartos pouch., Varicoceles are usually managed conservatively. If there are concerns about testicular, function of infertility then surgery or radiological management can be considered., Epididymal cysts can be excised using a scrotal approach, Hydroceles are managed differently in children where the underlying pathology is a patent, processus vaginalis and therefore an inguinal approach is used in children so that the, processus can be ligated. In adults a scrotal approach is preferred and the hydrocele sac, excised or plicated., Next question
Page 2763 :
Theme: Management of testicular disorders, , A., B., C., D., E., F., G., H., I., J., , Fine needle aspiration cytology, Excision biopsy, Orchidectomy via an inguinal approach, Lords procedure, Orchidectomy via a scrotal approach, Division of patent processus vaginalis via an inguinal approach, Division of patent processus vaginalis via a scrotal approach, Fowler Stephens procedure, Immediate scrotal exploration, Conservative management, , Please select the most appropriate management for the following testicular disorders. Each option, may be used once, more than once or not at all., , 15., , An 85 year old man is diagnosed as having prostate cancer and is considered suitable for, hormonal ablation. However, he does not want the repeated injections of GnRH, analogues., You answered Fine needle aspiration cytology, The correct answer is Orchidectomy via a scrotal approach, At one time bilateral orchidectomy was performed routinely when prostate cancer was, diagnosed (sometimes under the same anaesthetic). A combination of modern agents, (GnRH analogues) and better consent processes have made this almost obsolete. Where, required a scrotal approach should be used., , 16., , A 33 year old man presents with a painless lump in his left testes. USS and blood tests are, suspicious for teratoma., You answered Fine needle aspiration cytology, The correct answer is Orchidectomy via an inguinal approach, Oncological orchidectomy is routinely performed via an inguinal approach to avoid, contamination of another lymphatic field., , 17., , A 4 year old boy is brought to the clinic by his mother. He has a swelling in his right, hemiscrotum. On examination is transilluminates brilliantly., You answered Fine needle aspiration cytology
Page 2764 :
The correct answer is Division of patent processus vaginalis via an inguinal approach, Ligation of the patent processus vaginalis is performed via an inguinal approach. There is, no indication for scrotal surgery for hydrocele in young children., Please rate this question:, , Discuss and give feedback, , Next question, , Testicular disorders, Testicular cancer, Testicular cancer is the most common malignancy in men aged 20-30 years. Around 95% of cases, of testicular cancer are germ-cell tumours. Germ cell tumours may essentially be divided into:, , Tumour type, , Seminoma, , Tumour, markers, , Pathology, , Commonest, subtype (50%), Average age at, diagnosis = 40, Even advanced, disease associated, with 5 year, survival of 73%, , AFP usually, normal, HCG elevated, in 10%, seminomas, Lactate, dehydrogenase;, elevated in 1020% seminomas, (but also in many, other conditions), , Sheet like lobular, patterns of cells, with substantial, fibrous, component., Fibrous septa, contain, lymphocytic, inclusions and, granulomas may, be seen., , Younger age at, presentation =20-30, years, Advanced disease, carries worse prognosis, (48% at 5 years), Retroperitoneal lymph, node dissection may be, needed for residual, disease after, chemotherapy, , AFP elevated, in up to 70% of, cases, HCG elevated, in up to 40% of, cases, Other markers, rarely helpful, , Heterogenous, texture with, occasional ectopic, tissue such as hair, , Key features, , , , , Non seminomatous germ, cell tumours (42%), , , , , , Teratoma, Yolk sac tumour, Choriocarcinoma, Mixed germ cell, tumours (10%)
Page 2765 :
Image demonstrating a classical seminoma, these tumours are typically more uniform than, teratomas, , Image sourced from Wikipedia, , Risk factors for testicular cancer, , , , , , , Cryptorchidism, Infertility, Family history, Klinefelter's syndrome, Mumps orchitis
Page 2766 :
Features, , , , , A painless lump is the most common presenting symptom, Pain may also be present in a minority of men, Other possible features include hydrocele, gynaecomastia, , Diagnosis, , , , , Ultrasound is first-line, CT scanning of the chest/ abdomen and pelvis is used for staging, Tumour markers (see above) should be measured, , Management, , , , , Orchidectomy (Inguinal approach), Chemotherapy and radiotherapy may be given depending on staging, Abdominal lesions >1cm following chemotherapy may require retroperitoneal lymph node, dissection., , Prognosis is generally excellent, , , , 5 year survival for seminomas is around 95% if Stage I, 5 year survival for teratomas is around 85% if Stage I, , Benign disease, Epididymo-orchitis, Acute epididymitis is an acute inflammation of the epididymis, often involving the testis and usually, caused by bacterial infection., , , , , Infection spreads from the urethra or bladder. In men <35 years, gonorrhoea or chlamydia, are the usual infections., Amiodarone is a recognised non infective cause of epididymitis, which resolves on stopping, the drug., Tenderness is usually confined to the epididymis, which may facilitate differentiating it from, torsion where pain usually affects the entire testis., , Testicular torsion
Page 2767 :
, , , , , , Twist of the spermatic cord resulting in testicular ischaemia and necrosis., Most common in males aged between 10 and 30 (peak incidence 13-15 years), Pain is usually severe and of sudden onset., Cremasteric reflex is lost and elevation of the testis does not ease the pain., Treatment is with surgical exploration. If a torted testis is identified then both testis should be, fixed as the condition of bell clapper testis is often bilateral., , Hydrocele, , , , , , , Presents as a mass that transilluminates, usually possible to "get above" it on examination., In younger men it should be investigated with USS to exclude tumour., In children it may occur as a result of a patent processus vaginalis., Treatment in adults is with a Lords or Jabouley procedure., Treatment in children is with trans inguinal ligation of PPV., Next question
Page 2768 :
Theme: Management of testicular disorders, , A., B., C., D., E., F., G., , Antibiotics, Aspiration, Testicular exploration after 6 hours, Testicular exploration within 6 hours, Orchidectomy via inguinal approach, Orchidectomy via scrotal approach, No treatment needed, , Please select the most appropriate management for the scenario given. Each option may be used, once, more than once or not at all., , 18., , A 20 year old male notices a mild painful swelling of his right scrotum. He also complains, of abdominal pain. Clinically the patient is found to have a swollen right testicle. Apart, from a supraclavicular node, there is no obvious lymphadenopathy., You answered Antibiotics, The correct answer is Orchidectomy via inguinal approach, The patient is likely to have a teratoma which has metastasized to the supraclavicular, nodes. There is suspicion of spread to the para-aortic nodes due to the abdominal pain. He, will need orchidectomy and combination chemotherapy. There is no role for orchidectomy, via scrotal approach in malignancy., , 19., , A 40 year old male presents with a non painful, bilateral scrotal swellings over 3 years., The testis is felt separately and the swelling transilluminates., You answered Antibiotics, The correct answer is No treatment needed, This is an epididymal cyst, the testis is palpated therefore this differentiates it from a, hydrocele., , 20., , A 32 year old male presents with a swollen, painful right scrotum after being kicked in the, groin area. There is a painful swelling of the right scrotum and the underlying testis cannot, be easily palpated., You answered Antibiotics, The correct answer is Testicular exploration within 6 hours
Page 2769 :
Acute haematocele: tense, tender and non transilluminating mass. The testis will need, surgical exploration to evacuate the blood and repair any damage., Please rate this question:, , Discuss and give feedback, , Next question, , Scrotal swelling, Differential diagnosis, , Inguinal hernia, , If inguinoscrotal swelling; cannot "get above it" on examination, Cough impulse may be present, May be reducible, , Testicular tumours, , Often discrete testicular nodule (may have associated hydrocele), Symptoms of metastatic disease may be present, USS scrotum and serum AFP and β HCG required, , Acute epididymoorchitis, , Often history of dysuria and urethral discharge, Swelling may be tender and eased by elevating testis, Most cases due to Chlamydia, Infections with other gram negative organisms may be associated with, underlying structural abnormality, , Epididymal cysts, , Single or multiple cysts, May contain clear or opalescent fluid (spermatoceles), Usually occur over 40 years of age, Painless, Lie above and behind testis, It is usually possible to "get above the lump" on examination, , Hydrocele, , Non painful, soft fluctuant swelling, Often possible to "get above it" on examination, Usually contain clear fluid, Will often transilluminate, May be presenting feature of testicular cancer in young men
Page 2770 :
Testicular torsion, , Severe, sudden onset testicular pain, Risk factors include abnormal testicular lie, Typically affects adolescents and young males, On examination testis is tender and pain not eased by elevation, Urgent surgery is indicated, the contra lateral testis should also be fixed, , Varicocele, , Varicosities of the pampiniform plexus, Typically occur on left (because testicular vein drains into renal vein), May be presenting feature of renal cell carcinoma, Affected testis may be smaller and bilateral varicoceles may affect fertility, , Management, , , , , , , , Testicular malignancy is always treated with orchidectomy via an inguinal approach. This, allows high ligation of the testicular vessels and avoids exposure of another lymphatic field to, the tumour., Torsion is commonest in young teenagers and the history in older children can be difficult to, elicit. Intermittent torsion is a recognised problem. The treatment is prompt surgical, exploration and testicular fixation. This can be achieved using sutures or by placement of the, testis in a Dartos pouch., Varicoceles are usually managed conservatively. If there are concerns about testicular, function of infertility then surgery or radiological management can be considered., Epididymal cysts can be excised using a scrotal approach, Hydroceles are managed differently in children where the underlying pathology is a patent, processus vaginalis and therefore an inguinal approach is used in children so that the, processus can be ligated. In adults a scrotal approach is preferred and the hydrocele sac, excised or plicated., Next question
Page 2771 :
A 75 year old man presents with locally advanced carcinoma of the prostate and vertebral body, metastasis with impending spinal cord compression. Which of the following agents (if used in, isolation) carries the greatest risk of worsening his symptoms in the short term?, , Surgical orchidectomy, , Cyproterone acetate, , Luetenising hormone releasing hormone analogues, , Flutamide, , None of the above, , Theme from April 2016 Exam, LHRH analogues may cause flare of metastatic disease and anti androgens should be administered, to counter this. Surgical orchidectomy reduces testosterone levels within 8 hours (but fails to reduce, adrenal androgen release). Cyproterone and flutamide are androgen blockers that may be, considered as add on therapy to reduce the risk of tumour flare when commencing treatment with, LH RH analogues., Please rate this question:, , Discuss and give feedback, , Next question, , Prostate Cancer, Prostate Cancer, This is a common condition and up to 30,000 men are diagnosed with the condition each year. Up to, 9,000 will die in in the UK from the condition per year., Diagnosis, Early prostate cancers have few symptoms., Metastatic disease may present as bone pain., Locally advanced disease may present as pelvic pain or with urinary symptoms., Prostate specific antigen measurement, Digital rectal examination, Trans rectal USS (+/- biopsy), MRI/ CT and bone scan for staging., PSA Test, The normal upper limit for PSA is 4ng/ml. However, in this group will lie patients with benign disease
Page 2772 :
and some with localised prostate cancer. False positives may be due to prostatitis, UTI, BPH,, vigorous DRE., The percentage of free: total PSA may help to distinguish benign disease from cancer. Values of, <20% are suggestive of cancer and biopsy is advised., Pathology, , , , , , , 95% adenocarcinoma, In situ malignancy is sometimes found in areas adjacent to cancer. Multiple biopsies needed, to call true in situ disease., Often multifocal- 70% lie in the peripheral zone., Graded using the Gleason grading system, two grades awarded 1 for most dominant grade, (on scale of 1-5) and 2 for second most dominant grade (scale 1-5). The two added together, give the Gleason score. Where 2 is best prognosis and 10 the worst., Lymphatic spread occurs first to the obturator nodes and local extra prostatic spread to the, seminal vesicles is associated with distant disease., , Treatment, , , , , , , , , Watch and wait- Elderly, multiple co-morbidities, low Gleason score, Radiotherapy (External)- Both potentially curative and palliative therapy possible. However,, radiation proctitis and rectal malignancy are late problems. Brachytherapy is a modification, allowing internal radiotherapy., Surgery- Radical prostatectomy. Surgical removal of the prostate is the standard treatment, for localised disease. The robot is being used increasingly for this procedure. As well as the, prostate the obturator nodes are also removed to complement the staging process. Erectile, dysfunction is a common side effect. Survival may be better than with radiotherapy (see, references)., Hormonal therapy- Testosterone stimulates prostate tissue and prostatic cancers usually, show some degree of testosterone dependence. 95% of testosterone is derived from the, testis and bilateral orchidectomy may be used for this reason. Pharmacological alternatives, include LHRH analogues and anti androgens (which may be given in combination)., In the UK the National Institute for Clinical Excellence (NICE) suggests that active, surveillance is the preferred option for low risk men. It is particularly suitable for men with, clinical stage T1c, Gleason score 3+3 and PSA density < 0.15 ng/ml/ml who have cancer in, less than 50% of their biopsy cores, with < 10 mm of any core involved., , Candidates for active surveillance should:, , , , have had at least 10 biopsy cores taken, have at least one re-biopsy., , If men on active surveillance show evidence of disease progression, offer radical treatment., Treatment decisions should be made with the man, taking into account co-morbidities and life, expectancy., References, 1. Prostate cancer pathway. NICE.(http://guidance.nice.org.uk/IPG424)
Page 2773 :
2. Sooriakumaran P et al. Comparative effectiveness of radical prostatectomy and radiotherapy in, prostate cancer: observational study of mortality outcomes. BMJ 2014 (348):13. This study shows, that in men with localised disease survival was greater in those offered surgery., Next question
Page 2774 :
A 42 year old man undergoes a vasectomy at the surgical clinic. He is reviewed at the request of his, general practitioner. On examination he has a small rounded nodule adjacent to the vas. What is the, most likely underlying diagnosis?, , Haematoma, , Sperm granuloma, , Varicocele, , Hydrocele, , Epididymal cyst, , Sperm granulomas are a common sequelae of vasectomy and are smooth round lumps adherant to, the vas. They may be safely left alone., Please rate this question:, , Discuss and give feedback, , Next question, , Vasectomy, Vasectomy is a commonly performed technique for achieving permanent sterilisation. It has a failure, rate of 1 in 2000 and is conveniently performed under local anaesthesia., Reversal success rates are approximately 55% if performed within 10 years of the procedure. For, the purposes of counseling the procedure should be deemed permanent., Procedure, Small bilateral incisions and formal dissection of the vas is the standard technique. A technique, involving the use of haemostats for skin puncture is used in the "no scalpel", technique. It is not necessary to routinely send the vas for histology.
Page 2775 :
Controversies, Be wary of performing the procedure in childless, single men under age 30., Risks, Following the procedure between 12 and 52% of men reported chronic scrotal pain. Of which 5.2%, sought help. Haematomas and sperm granulomas may also occur., Follow up, Viable sperm may persist following surgery. Clearance should not be granted until a negative sperm, sample is available. This is usually taken after 12-16 weeks post procedure (and preferably after 24, ejaculates). Recanalisation may occur in 0.04% of cases.In a small minority of men, non-motile, sperm persist after vasectomy. In such cases, "special clearance" to stop contraception may be, given when less than 10,000 non-motile sperm/mL are found in a fresh specimen examined at least, 7 months after vasectomy., The risks of STI's are unchanged., Next question
Page 2776 :
Theme: Haematuria, , A., B., C., D., E., F., , Retroperitoneal liposarcoma, Transitional cell carcinoma, Retroperitoneal fibrosis, Renal squamous cell carcinoma, Renal adenocarcinoma, Nephroblastoma, , Please select the most likely cause of haematuria for the scenarios given. Each option may be used, once, more than once or not at all., , 23., , A 28 year old man presents with hypertension and haematuria. Haematological, investigations show polycythaemia but otherwise no abnormality. CT scanning shows a, left renal mass., You answered Retroperitoneal liposarcoma, The correct answer is Renal adenocarcinoma, Renal adenocarcinoma is the most common variant and is associated with polycythaemia., , 24., , A 68 year of man presents with recurrent episodes of left sided ureteric colic and, haematuria. Investigations show some dilatation of the renal pelvis but the outline is, irregular., You answered Retroperitoneal liposarcoma, The correct answer is Transitional cell carcinoma, These arise from urothelium and necessitate a nephroureterectomy., , 25., , A 4 year old boy presents with haematuria and on examination is found to have a right, sided renal mass., You answered Retroperitoneal liposarcoma, The correct answer is Nephroblastoma, Wilms tumours (nephroblastoma) usually present in the first 4 years of life and may cause, lung metastases., , Please rate this question:
Page 2777 :
Discuss and give feedback, , Next question, , Haematuria, Causes of haematuria, , Trauma, , , , , , , Injury to renal tract, Renal trauma commonly due to blunt injury (others penetrating, injuries), Ureter trauma rare: iatrogenic, Bladder trauma: due to RTA or pelvic fractures, , Infection, , , , Remember TB, , Malignancy, , , , , , , Renal cell carcinoma (remember paraneoplastic syndromes):, painful or painless, Urothelial malignancies: 90% are transitional cell carcinoma, can, occur anywhere along the urinary tract. Painless haematuria., Squamous cell carcinoma and adenocarcinoma: rare bladder, tumours, Prostate cancer, Penile cancers: SCC, , Renal disease, , , , Glomerulonephritis, , Stones, , , , Microscopic haematuria common, , Structural, abnormalities, , , , , , , Benign prostatic hyperplasia (BPH) causes haematuria due to, hypervascularity of the prostate gland, Cystic renal lesions e.g. polycystic kidney disease, Vascular malformations, Renal vein thrombosis due to renal cell carcinoma, , Coagulopathy, , , , Causes bleeding of underlying lesions, , Drugs, , , , Cause tubular necrosis or interstitial nephritis: aminoglycosides,, , ,
Page 2779 :
A 22 year old man is involved in a road traffic accident. He is found to have a pelvic fracture. While, on the ward the nursing staff report that he is complaining of lower abdominal pain. On examination, you find a distended tender bladder. What is the most likely diagnosis?, , Bladder rupture, , Ureter injury, , Urethral injury, , Clot retention, , Prostate rupture, , Theme from 2009 Exam, Pelvic fractures may cause laceration of the urethra. Urinary retention, blood at the urethral meatus, and a high riding prostate on digital rectal examination are the typical features., Please rate this question:, , Discuss and give feedback, , Next question, , Lower genitourinary tract trauma, , , , , , Most bladder injuries occur due to blunt trauma, 85% associated with pelvic fractures, Easily overlooked during assessment in trauma, Up to 10% of male pelvic fractures are associated with urethral or bladder injuries, , Types of injury, , Urethral injury, , , , , , Mainly in males, Blood at the meatus (50% cases), There are 2 types:, , i.Bulbar rupture, - most common, - straddle type injury e.g. bicycles
Page 2780 :
- triad signs: urinary retention, perineal haematoma, blood at the, meatus, ii. Membranous rupture, - can be extra or intraperitoneal, - commonly due to pelvic fracture, - Penile or perineal oedema/ hematoma, - PR: prostate displaced upwards (beware co-existing, retroperitoneal haematomas as they may make examination, difficult), - Investigation: ascending urethrogram, - Management: suprapubic catheter (surgical placement, not, percutaneously), External genitalia injuries, (i.e., the penis and the, scrotum), , , , Secondary to injuries caused by penetration, blunt trauma,, continence- or sexual pleasure-enhancing devices, and, mutilation, , Bladder injury, , , , , , rupture is intra or extraperitoneal, presents with haematuria or suprapubic pain, history of pelvic fracture and inability to void: always, suspect bladder or urethral injury, inability to retrieve all fluid used to irrigate the bladder, through a Foley catheter indicates bladder injury, investigation- IVU or cystogram, management: laparotomy if intraperitoneal, conservative if, extraperitoneal, , , , , , Next question
Page 2781 :
Theme: Haematuria, , A., B., C., D., E., F., , Benign prostatic hyperplasia, Ureteric calculus, Pyelonephritis, Prostatitis, Cystitis, Prostate cancer, , Please select the most likely source of haematuria for the scenarios given. Each option may be used, once, more than once or not at all., , 27., , A 67 year old man presents with recurrent episodes of haematuria, typically at the end of, the urinary stream, he has been suffering from occasional fevers and has noticed pus on the, urethral meatus on occasion. On examination the prostate has no discernable masses but is, tender., You answered Benign prostatic hyperplasia, The correct answer is Prostatitis, This is most likely prostatitis and the bleeding at the end of micturition suggests a distal, problem. Treatment is usually with prolonged courses of antibiotics., , 28., , A 23 year old girl is admitted with loin pain and a fever, she has noticed haematuria for the, past week accompanied by dysuria, this was treated empirically with trimethoprim., You answered Benign prostatic hyperplasia, The correct answer is Pyelonephritis, This is most likely pyelonephritis and partially treated cystitis is a common cause., , 29., , A 56 year old man is admitted with severe loin to groin pain associated with haematuria., He was well until 1 week ago when he was unwell with diarrhoea and vomiting., You answered Benign prostatic hyperplasia, The correct answer is Ureteric calculus, Ureteric stones may develop in a background of dehydration., , Please rate this question:
Page 2782 :
Discuss and give feedback, , Next question, , Haematuria, Causes of haematuria, , Trauma, , , , , , , Injury to renal tract, Renal trauma commonly due to blunt injury (others penetrating, injuries), Ureter trauma rare: iatrogenic, Bladder trauma: due to RTA or pelvic fractures, , Infection, , , , Remember TB, , Malignancy, , , , , , , Renal cell carcinoma (remember paraneoplastic syndromes):, painful or painless, Urothelial malignancies: 90% are transitional cell carcinoma, can, occur anywhere along the urinary tract. Painless haematuria., Squamous cell carcinoma and adenocarcinoma: rare bladder, tumours, Prostate cancer, Penile cancers: SCC, , Renal disease, , , , Glomerulonephritis, , Stones, , , , Microscopic haematuria common, , Structural, abnormalities, , , , , , , Benign prostatic hyperplasia (BPH) causes haematuria due to, hypervascularity of the prostate gland, Cystic renal lesions e.g. polycystic kidney disease, Vascular malformations, Renal vein thrombosis due to renal cell carcinoma, , Coagulopathy, , , , Causes bleeding of underlying lesions, , Drugs, , , , Cause tubular necrosis or interstitial nephritis: aminoglycosides,, , ,
Page 2784 :
Which of the following would be most consistent with a histologically aggressive form of prostate, cancer?, , FIGO stage 1 disease, , FIGO stage IV disease, , EuroQOL score of 5, , Gleason score of 2, , Gleason score of 10, , Prostate cancer is histologically graded using the Gleason score (see below). A score of 10 is, consistent with a histologically aggressive form of the disease. The FIGO staging system is used to, stage gynaecological malignancy. The EuroQOL score is a quality of life measurement tool., Please rate this question:, , Discuss and give feedback, , Next question, , Prostate Cancer, Prostate Cancer, This is a common condition and up to 30,000 men are diagnosed with the condition each year. Up to, 9,000 will die in in the UK from the condition per year., Diagnosis, Early prostate cancers have few symptoms., Metastatic disease may present as bone pain., Locally advanced disease may present as pelvic pain or with urinary symptoms., Prostate specific antigen measurement, Digital rectal examination, Trans rectal USS (+/- biopsy), MRI/ CT and bone scan for staging., PSA Test, The normal upper limit for PSA is 4ng/ml. However, in this group will lie patients with benign disease, and some with localised prostate cancer. False positives may be due to prostatitis, UTI, BPH,, vigorous DRE., The percentage of free: total PSA may help to distinguish benign disease from cancer. Values of, <20% are suggestive of cancer and biopsy is advised.
Page 2785 :
Pathology, , , , , , , 95% adenocarcinoma, In situ malignancy is sometimes found in areas adjacent to cancer. Multiple biopsies needed, to call true in situ disease., Often multifocal- 70% lie in the peripheral zone., Graded using the Gleason grading system, two grades awarded 1 for most dominant grade, (on scale of 1-5) and 2 for second most dominant grade (scale 1-5). The two added together, give the Gleason score. Where 2 is best prognosis and 10 the worst., Lymphatic spread occurs first to the obturator nodes and local extra prostatic spread to the, seminal vesicles is associated with distant disease., , Treatment, , , , , , , , , Watch and wait- Elderly, multiple co-morbidities, low Gleason score, Radiotherapy (External)- Both potentially curative and palliative therapy possible. However,, radiation proctitis and rectal malignancy are late problems. Brachytherapy is a modification, allowing internal radiotherapy., Surgery- Radical prostatectomy. Surgical removal of the prostate is the standard treatment, for localised disease. The robot is being used increasingly for this procedure. As well as the, prostate the obturator nodes are also removed to complement the staging process. Erectile, dysfunction is a common side effect. Survival may be better than with radiotherapy (see, references)., Hormonal therapy- Testosterone stimulates prostate tissue and prostatic cancers usually, show some degree of testosterone dependence. 95% of testosterone is derived from the, testis and bilateral orchidectomy may be used for this reason. Pharmacological alternatives, include LHRH analogues and anti androgens (which may be given in combination)., In the UK the National Institute for Clinical Excellence (NICE) suggests that active, surveillance is the preferred option for low risk men. It is particularly suitable for men with, clinical stage T1c, Gleason score 3+3 and PSA density < 0.15 ng/ml/ml who have cancer in, less than 50% of their biopsy cores, with < 10 mm of any core involved., , Candidates for active surveillance should:, , , , have had at least 10 biopsy cores taken, have at least one re-biopsy., , If men on active surveillance show evidence of disease progression, offer radical treatment., Treatment decisions should be made with the man, taking into account co-morbidities and life, expectancy., References, 1. Prostate cancer pathway. NICE.(http://guidance.nice.org.uk/IPG424), 2. Sooriakumaran P et al. Comparative effectiveness of radical prostatectomy and radiotherapy in, prostate cancer: observational study of mortality outcomes. BMJ 2014 (348):13. This study shows, that in men with localised disease survival was greater in those offered surgery., Next question
Page 2786 :
A 13 month old boy is brought to the paediatric clinic by his mother who is concerned that his testis, are not palpable. On examination his testis are not palpable either in the scrotum or inguinal region, and cannot be visualised on ultrasound either. What is the most appropriate next stage in, management?, , Laparoscopy, , Re-assess at 5 years of age, , Re-assess at 13 years of age, , Administration of testosterone, , Administration of cyproterone acetate, , Impalpable testes are an indication for laparoscopy. Ultrasound is a relatively unhelpful tool in, evaluating cryptorchid patients and most experienced paediatric surgeons would not use it preoperatively. They may be associated with an intra-abdominal location. Whilst it is reasonable to defer, orchidopexy for retractile testis completely absent testes should be investigated further., Please rate this question:, , Discuss and give feedback, , Next question, , Cryptorchidism, A congenital undescended testis is one that has failed to reach the bottom of the scrotum by 3, months of age. At birth up to 5% of boys will have an undescended testis, post natal descent occurs, in most and by 3 months the incidence of cryptorchidism falls to 1-2%. In the vast majority of cases, the cause of the maldescent is unknown. A proportion may be associated with other congenital, defects including:, Patent processus vaginalis, Abnormal epididymis, Cerebral palsy, Mental retardation, Wilms tumour, Abdominal wall defects (e.g. gastroschisis, prune belly syndrome), Differential diagnosis, These include retractile testes and, in the case of absent bilateral testes the possibility of intersex, conditions. A retractile testis can be brought into the scrotum by the clinician and when released
Page 2787 :
remains in the scrotum. If the examining clinician notes the testis to return rapidly into the inguinal, canal when released then surgery is probably indicated., Reasons for correction of cryptorchidism, , , , , , Reduce risk of infertility, Allows the testes to be examined for testicular cancer, Avoid testicular torsion, Cosmetic appearance, , Males with undescended testis are 40 times as likely to develop testicular cancer (seminoma) as, males without undescended testis, The location of the undescended testis affects the relative risk of testicular cancer (50% intraabdominal testes), Treatment, , , , , Orchidopexy at 6- 18 months of age. The operation usually consists of inguinal exploration,, mobilisation of the testis and implantation into a dartos pouch., Intra-abdominal testis should be evaluated laparoscopically and mobilised. Whether this is a, single stage or two stage procedure depends upon the exact location., After the age of 2 years in untreated individuals the Sertoli cells will degrade and those, presenting late in teenage years may be better served by orchidectomy than to try and, salvage a non functioning testis with an increased risk of malignancy., Next question
Page 2788 :
A 34-year-old man from Zimbabwe is admitted with abdominal pain to the Emergency Department., An abdominal x-ray reveals urinary bladder calcification. What is the most likely cause?, , Schistosoma mansoni, , Sarcoidosis, , Leishmaniasis, , Tuberculosis, , Schistosoma haematobium, Schistosoma haematobium causes haematuria, Theme from April 2016 exam, Schistosomiasis is the most common cause of bladder calcification worldwide. Schistosoma, mansoni typically resided in the colon from where it is excreted., Please rate this question:, , Discuss and give feedback, , Next question, , Schistosomiasis, Schistosomiasis, or bilharzia, is a parasitic flatworm infection. The following types of schistosomiasis, are recognised:, , , , Schistosoma mansoni and Schistosoma intercalatum: intestinal schistosomiasis, Schistosoma haematobium: urinary schistosomiasis, , Schistosoma haematobium, This typically presents as a 'swimmer's itch' in patients who have recently returned from Africa., Schistosoma haematobium is a risk factor for squamous cell bladder cancer, Features, , , , Frequency, Haematuria
Page 2789 :
, , Bladder calcification, , Management, , , Single oral dose of praziquantel, Next question
Page 2790 :
Theme: Testicular disorders, , A., B., C., D., E., F., G., , Testicular tumour, Torsion of the spermatic cord, Acute infective epididymo-orchitis, Non infective epididymo- orchitis, Torsion of testicular appendage, Hydrocele, Haematocele, , Please select the most likely cause for the testicular disorder described. Each option may be used, once, more than once or not at all., , 33., , An 28 year old man presents with pain in the testis and scrotum. It began 10 hours, previously and has worsened during that time. On examination he is pyrexial, the testis is, swollen and tender and there is an associated hydrocele., You answered Testicular tumour, The correct answer is Acute infective epididymo-orchitis, The onset is relatively slow for torsion and the presence of fever favors epididymoorchitis., , 34., , A 15 year old boy develops sudden onset of pain in the left hemiscrotum. He has no other, urinary symptoms. On examination the superior pole of the testis is tender and the, cremasteric reflex is particularly marked., You answered Testicular tumour, The correct answer is Torsion of testicular appendage, The cremasteric reflex is usually preserved when the torsion affects the appendage only., , 35., , A 14 year old boy develops sudden onset severe pain in the left testicle radiating to the left, groin. He is distressed and vomits. On examination the testis is very tender and the, cremasteric reflex is absent., You answered Testicular tumour, The correct answer is Torsion of the spermatic cord, The cremasteric reflex is usually absent in torsion.
Page 2791 :
Similar theme question in September 2011 exam, Please rate this question:, , Discuss and give feedback, , Next question, , Testicular disorders, Testicular cancer, Testicular cancer is the most common malignancy in men aged 20-30 years. Around 95% of cases, of testicular cancer are germ-cell tumours. Germ cell tumours may essentially be divided into:, , Tumour type, , Seminoma, , Tumour, markers, , Pathology, , Commonest, subtype (50%), Average age at, diagnosis = 40, Even advanced, disease associated, with 5 year, survival of 73%, , AFP usually, normal, HCG elevated, in 10%, seminomas, Lactate, dehydrogenase;, elevated in 1020% seminomas, (but also in many, other conditions), , Sheet like lobular, patterns of cells, with substantial, fibrous, component., Fibrous septa, contain, lymphocytic, inclusions and, granulomas may, be seen., , Younger age at, presentation =20-30, years, Advanced disease, carries worse prognosis, (48% at 5 years), Retroperitoneal lymph, node dissection may be, needed for residual, disease after, chemotherapy, , AFP elevated, in up to 70% of, cases, HCG elevated, in up to 40% of, cases, Other markers, rarely helpful, , Heterogenous, texture with, occasional ectopic, tissue such as hair, , Key features, , , , , Non seminomatous germ, cell tumours (42%), , , , , , Teratoma, Yolk sac tumour, Choriocarcinoma, Mixed germ cell, tumours (10%), , Image demonstrating a classical seminoma, these tumours are typically more uniform than, teratomas
Page 2792 :
Image sourced from Wikipedia, , Risk factors for testicular cancer, , , , , , , Cryptorchidism, Infertility, Family history, Klinefelter's syndrome, Mumps orchitis, , Features
Page 2793 :
, , , , A painless lump is the most common presenting symptom, Pain may also be present in a minority of men, Other possible features include hydrocele, gynaecomastia, , Diagnosis, , , , , Ultrasound is first-line, CT scanning of the chest/ abdomen and pelvis is used for staging, Tumour markers (see above) should be measured, , Management, , , , , Orchidectomy (Inguinal approach), Chemotherapy and radiotherapy may be given depending on staging, Abdominal lesions >1cm following chemotherapy may require retroperitoneal lymph node, dissection., , Prognosis is generally excellent, , , , 5 year survival for seminomas is around 95% if Stage I, 5 year survival for teratomas is around 85% if Stage I, , Benign disease, Epididymo-orchitis, Acute epididymitis is an acute inflammation of the epididymis, often involving the testis and usually, caused by bacterial infection., , , , , Infection spreads from the urethra or bladder. In men <35 years, gonorrhoea or chlamydia, are the usual infections., Amiodarone is a recognised non infective cause of epididymitis, which resolves on stopping, the drug., Tenderness is usually confined to the epididymis, which may facilitate differentiating it from, torsion where pain usually affects the entire testis., , Testicular torsion, , , , , , Twist of the spermatic cord resulting in testicular ischaemia and necrosis., Most common in males aged between 10 and 30 (peak incidence 13-15 years), Pain is usually severe and of sudden onset., Cremasteric reflex is lost and elevation of the testis does not ease the pain.
Page 2794 :
, , Treatment is with surgical exploration. If a torted testis is identified then both testis should be, fixed as the condition of bell clapper testis is often bilateral., , Hydrocele, , , , , , , Presents as a mass that transilluminates, usually possible to "get above" it on examination., In younger men it should be investigated with USS to exclude tumour., In children it may occur as a result of a patent processus vaginalis., Treatment in adults is with a Lords or Jabouley procedure., Treatment in children is with trans inguinal ligation of PPV., Next question
Page 2795 :
Which of the following statements is false in relation to renal adenocarcinoma?, , They account for over 75% cases of renal tumours, , Renal biopsy should be performed in all cases considered for radical nephrectomy, , They typically spread via the haematogenous route, , Patients with completely resected T2 disease should not receive adjuvant chemotherapy, , Partial nephrectomy gives equivalent oncological outcomes in patients with T1 disease, Routine chemotherapy is not effective in patients with renal adenocarcinoma and should not be used, following R0 resections., , Routine renal biopsy should not be performed in cases for nephrectomy. Most cases of malignancy, can be accurately classified on imaging., Please rate this question:, , Discuss and give feedback, , Next question, , Renal tumours, Renal cell carcinoma, Renal cell carcinoma is an adenocarcinoma of the renal cortex and is believed to arise from the, proximal convoluted tubule. They are usually solid lesions, up to 20% may be multifocal, 20% may, be calcified and 20% may have either a cystic component or be wholly cystic. They are often, circumscribed by a pseudocapsule of compressed normal renal tissue. Spread may occur either by, direct extension into the adrenal gland, renal vein or surrounding fascia. More distant disease, usually occurs via the haematogenous route to lung, bone or brain., Renal cell carcinoma comprise up to 85% of all renal malignancies. Males are more commonly, affected than females and sporadic tumours typically affect patients in their sixth decade.
Page 2796 :
Patients may present with a variety of symptoms including; haematuria (50%), loin pain (40%), mass, (30%) and up to 25% may have symptoms of metastasis.Less than 10% have the classic triad of, haematuria, pain and mass., Investigation, Many cases will present as haematuria and be discovered during diagnostic work up. Benign renal, tumours are rare, so renal masses should be investigated with multislice CT scanning. Some units, will add and arterial and venous phase to the scan to demonstrate vascularity and evidence of caval, ingrowth., CT scanning of the chest and abdomen to detect distant disease should also be undertaken., Routine bone scanning is not indicated in the absence of symptoms., Biopsy should not be performed when a nephrectomy is planned but is mandatory before any, ablative therapies are undertaken., Assessment of the functioning of the contra lateral kidney., Management, T1 lesions may be managed by partial nephrectomy and this gives equivalent oncological results to, total radical nephrectomy. Partial nephrectomy may also be performed when there is inadequate, reserve in the remaining kidney., For T2 lesions and above a radical nephrectomy is standard practice and this may be performed via, a laparoscopic or open approach. Preoperative embolisation is not indicated nor is resection of, uninvolved adrenal glands. During surgery early venous control is mandatory to avoid shedding of, tumour cells into the circulation., Patients with completely resected disease do not benefit from adjuvant therapy with either, chemotherapy or biological agents. These should not be administered outside the setting of clinical, trials., Patients with transitional cell cancer will require a nephroureterectomy with disconnection of the, ureter at the bladder., References, Lungberg B et al. EAU guidelines on renal cell carcinoma: The 2010 update. European Urology 2010, (58): 398-406., Next question
Page 2797 :
Theme: Haematuria, , A., B., C., D., E., F., G., , Benign prostatic hyperplasia, Transitional cell carcinoma of the bladder, Renal cell carcinoma, Ureteric calculus, Staghorn calculus, Uncomplicated urinary tract infection, Adenocarcinoma of the bladder, , Please select the most likely cause of haematuria from the scenarios given. Each option may be, used once, more than once or not at all., , 37., , A 58 year old man has an episode of painless frank haematuria whilst undergoing a 24, urine collection for investigation of hypertension., You answered Benign prostatic hyperplasia, The correct answer is Renal cell carcinoma, These tumours may often have paraneoplastic effects such as hypertension., , 38., , A 73 year old lady has an episode of haematuria whilst receiving a course of intravesical, BCG therapy., You answered Benign prostatic hyperplasia, The correct answer is Transitional cell carcinoma of the bladder, Transitional cell carcinoma of the bladder may be treated with intravesical BCG therapy., , 39., , A 32 year old lady suffers from severe left sided abdominal pain, that radiates to her groin., As part of her evaluation the nurses identify microscopic haematuria on dipstick., You answered Benign prostatic hyperplasia, The correct answer is Ureteric calculus, Ureteric calculi will often present with loin pain radiating to the groin. It is usually severe., There may be macroscopic or microscopic haematuria. The absence of haematuria on, dipstick testing should prompt investigations for alternative diagnoses. The best, investigation is a non contrast CT scan. CT changes consistent with stone or recent stone, passage include evidence of stone, perinephric stranding, ureteric oedema or
Page 2798 :
hydronephrosis., Please rate this question:, , Discuss and give feedback, , Next question, , Haematuria, Causes of haematuria, , Trauma, , , , , , , Injury to renal tract, Renal trauma commonly due to blunt injury (others penetrating, injuries), Ureter trauma rare: iatrogenic, Bladder trauma: due to RTA or pelvic fractures, , Infection, , , , Remember TB, , Malignancy, , , , , , , Renal cell carcinoma (remember paraneoplastic syndromes):, painful or painless, Urothelial malignancies: 90% are transitional cell carcinoma, can, occur anywhere along the urinary tract. Painless haematuria., Squamous cell carcinoma and adenocarcinoma: rare bladder, tumours, Prostate cancer, Penile cancers: SCC, , Renal disease, , , , Glomerulonephritis, , Stones, , , , Microscopic haematuria common, , Structural, abnormalities, , , , Benign prostatic hyperplasia (BPH) causes haematuria due to, hypervascularity of the prostate gland, Cystic renal lesions e.g. polycystic kidney disease, Vascular malformations, Renal vein thrombosis due to renal cell carcinoma, , , , , , ,
Page 2800 :
A 73 year old man has previously undergone a prostatectomy to treat prostate cancer. On review,, his PSA has risen to 55 and he has developed pain in his lower back. Imaging shows osteosclerotic, lesions in L4 and L3. What is the best treatment strategy?, , Posterior spinal fusion, , Vertebral body reconstruction, , Bisphosphonates and radiotherapy, , Androgen suppression, bisphosphonates and radiotherapy, , Radiotherapy alone, , Theme from April 2015 Exam, In men with metastatic bone lesions from prostate cancer, the best outcomes are achieved with, androgen suppression. Radiotherapy can also produced marked palliation. A 2010 Cochrane review, has clearly demonstrated added benefit, in terms of symptom control, from the addition of a, bisphosphonate., Please rate this question:, , Discuss and give feedback, , Next question, , Prostate Cancer, Prostate Cancer, This is a common condition and up to 30,000 men are diagnosed with the condition each year. Up to, 9,000 will die in in the UK from the condition per year., Diagnosis, Early prostate cancers have few symptoms., Metastatic disease may present as bone pain., Locally advanced disease may present as pelvic pain or with urinary symptoms., Prostate specific antigen measurement, Digital rectal examination, Trans rectal USS (+/- biopsy), MRI/ CT and bone scan for staging., PSA Test, The normal upper limit for PSA is 4ng/ml. However, in this group will lie patients with benign disease, and some with localised prostate cancer. False positives may be due to prostatitis, UTI, BPH,
Page 2801 :
vigorous DRE., The percentage of free: total PSA may help to distinguish benign disease from cancer. Values of, <20% are suggestive of cancer and biopsy is advised., Pathology, , , , , , , 95% adenocarcinoma, In situ malignancy is sometimes found in areas adjacent to cancer. Multiple biopsies needed, to call true in situ disease., Often multifocal- 70% lie in the peripheral zone., Graded using the Gleason grading system, two grades awarded 1 for most dominant grade, (on scale of 1-5) and 2 for second most dominant grade (scale 1-5). The two added together, give the Gleason score. Where 2 is best prognosis and 10 the worst., Lymphatic spread occurs first to the obturator nodes and local extra prostatic spread to the, seminal vesicles is associated with distant disease., , Treatment, , , , , , , , , Watch and wait- Elderly, multiple co-morbidities, low Gleason score, Radiotherapy (External)- Both potentially curative and palliative therapy possible. However,, radiation proctitis and rectal malignancy are late problems. Brachytherapy is a modification, allowing internal radiotherapy., Surgery- Radical prostatectomy. Surgical removal of the prostate is the standard treatment, for localised disease. The robot is being used increasingly for this procedure. As well as the, prostate the obturator nodes are also removed to complement the staging process. Erectile, dysfunction is a common side effect. Survival may be better than with radiotherapy (see, references)., Hormonal therapy- Testosterone stimulates prostate tissue and prostatic cancers usually, show some degree of testosterone dependence. 95% of testosterone is derived from the, testis and bilateral orchidectomy may be used for this reason. Pharmacological alternatives, include LHRH analogues and anti androgens (which may be given in combination)., In the UK the National Institute for Clinical Excellence (NICE) suggests that active, surveillance is the preferred option for low risk men. It is particularly suitable for men with, clinical stage T1c, Gleason score 3+3 and PSA density < 0.15 ng/ml/ml who have cancer in, less than 50% of their biopsy cores, with < 10 mm of any core involved., , Candidates for active surveillance should:, , , , have had at least 10 biopsy cores taken, have at least one re-biopsy., , If men on active surveillance show evidence of disease progression, offer radical treatment., Treatment decisions should be made with the man, taking into account co-morbidities and life, expectancy., References, 1. Prostate cancer pathway. NICE.(http://guidance.nice.org.uk/IPG424), 2. Sooriakumaran P et al. Comparative effectiveness of radical prostatectomy and radiotherapy in
Page 2802 :
prostate cancer: observational study of mortality outcomes. BMJ 2014 (348):13. This study shows, that in men with localised disease survival was greater in those offered surgery., Next question
Page 2803 :
A 24 year old man presents with a persistent and unwanted erection that has been present for the, previous 6 hours. On examination the penis is rigid and tender. Aspiration of blood from the corpus, cavernosa shows dark blood. Which of the following is the most appropriate initial management?, , Discharge the patient home and review in 12 hours, , Admit the patient to hospital and review in 12 hours, , Aspirate further blood from the corpus cavernosa in an attempt to decompress, , Use a trucut needle to induce an arteriovenous shunt, , Administer intracavernosal adrenaline 1 in 500 concentration, , Low flow priaprism is a urological emergency. Aspiration of bright red blood is more reassuring and, may indicate high flow priaprism that may be actively monitored. Low flow priaprism should be, decompressed with aspiration of blood from the corpus caveronsum., Please rate this question:, , Discuss and give feedback, , Next question, , Penile erection, Physiology of erection, , Autonomic, , , , , Somatic, nerves, , Sympathetic nerves originate from T11-L2 and parasympathetic nerves, from S2-4 join to form pelvic plexus., Parasympathetic discharge causes erection, sympathetic discharge causes, ejaculation and detumescence., , Supplied by dorsal penile and pudendal nerves. Efferent signals are relayed from, Onufs nucleus (S2-4) to innervate ischiocavernosus and bulbocavernosus muscles., , Autonomic discharge to the penis will trigger the veno-occlusive mechanism which triggers the flow, of arterial blood into the penile sinusoidal spaces. As the inflow increases the increased volume in, this space will secondarily lead to compression of the subtunical venous plexus with reduced venous, return. During the detumesence phase the arteriolar constriction will reduce arterial inflow and, thereby allow venous return to normalise.
Page 2804 :
Priapism, Prolonged unwanted erection, in the absence of sexual desire, lasting more than 4 hours., Classification of priaprism, , Low flow priaprism, , Due to veno-occlusion (high intracavernosal pressures)., , , , , , High flow priaprism, , Due to unregulated arterial blood flow., , , Recurrent priaprism, , Most common type, Often painful, Often low cavernosal flow, If present for >4 hours requires emergency treatment, , Usually presents as semi rigid painless erection, , Typically seen in sickle cell disease, most commonly of high flow type., , Causes, , , , , , Intracavernosal drug therapies (e.g. for erectile dysfunction>, Blood disorders such as leukaemia and sickle cell disease, Neurogenic disorders such as spinal cord transection, Trauma to penis resulting in arterio-venous malformations, , Tests, , , , Exclude sickle cell/ leukaemia, Consider blood sampling from cavernosa to determine whether high or low flow (low flow is, often hypoxic), , Management, , , , , Ice packs/ cold showers, If due to low flow then blood may be aspirated from copora or try intracavernosal alpha, adrenergic agonists., Delayed therapy of low flow priaprism may result in erectile dysfunction., Next question
Page 2805 :
Theme: Management of urinary obstruction, , A., B., C., D., E., F., G., , Discharge, Start oxybutynin, Intravenous antibiotics, Urethral catheter, Emergency nephrostomy, Antegrade ureteric stent, Retrograde ureteric stent, , What is the best management for the scenario given? Each option may be used once, more than, once or not at all., , 42., , A 68 year old man has a TCC of the bladder. He has a right hydronephrosis detected on, ultrasound and deteriorating renal function. A DMSA scan shows a non functioning left, kidney., You answered Discharge, The correct answer is Antegrade ureteric stent, A TCC occluding the ureteric orifice will obscure its identification during surgery, so that, passage of a retrograde stent is difficult. Therefore passage of a stent from the renal pelvis, is preferable., , 43., , A 52 year old male with hypercalcaemia secondary to primary hyperparathyroidism, presents with renal colic. USS demonstrates ureteric obstruction due to a stone. Multiple, attempts at stone extraction are performed. However, the stone could not be removed. He, is now septic with a pyrexia of 39.5 oc., You answered Discharge, The correct answer is Emergency nephrostomy, The likely scenario is that this man has developed a calculus causing ureteric obstruction., The stagnant column of urine can become colonised and infected. An infected obstructed, system is one of the few true urological emergencies. A nephrostomy is needed as the, stone could not be removed., , 44., , A 56 year old man is admitted with acute retention of urine. He has had a recent urinary, tract infection. An USS shows bilateral hydronephrosis., You answered Discharge
Page 2806 :
The correct answer is Urethral catheter, Establishing bladder drainage will often correct the situation. These patients often have a, significant diuresis with associated electrolyte disturbance., Antegrade ureteric stents pass from the kidney to the bladder., Retrograde stents pass from the bladder to the kidney, Please rate this question:, , Discuss and give feedback, , Next question, , Hydronephrosis, Causes of hydronephrosis, Unilateral: PACT, , , , , , Pelvic-ureteric obstruction (congenital or acquired), Aberrant renal vessels, Calculi, Tumours of renal pelvis, , Bilateral: SUPER, , , , , , , Stenosis of the urethra, Urethral valve, Prostatic enlargement, Extensive bladder tumour, Retro-peritoneal fibrosis, , Investigation, , , , , , USS- identifies presence of hydronephrosis and can assess the kidneys, IVU- assess the position of the obstruction, Antegrade or retrograde pyelography- allows treatment, If renal colic suspected: non contrast CT scan (majority of stones are detected this way), , Management
Page 2807 :
, , , , Remove the obstruction and drainage of urine, Acute upper urinary tract obstruction: Nephrostomy tube, Chronic upper urinary tract obstruction: Ureteric stent or a pyeloplasty, Next question
Page 2808 :
Theme: Haematuria, , A., B., C., D., E., F., G., , Transitional cell carcinoma of the bladder, Squamous cell carcinoma of the bladder, Renal cell carcinoma, Polycystic kidney disease, Wilms tumour, Neuroblastoma, Benign prostatic hyperplasia, , Please select the most likely cause of haematuria for the scenarios given. Each option may be used, once, more than once or not at all., , 45., , A 40 year old women is being investigated for haematuria. She was living with her sister, who has just died from a sub arachnoid haemorrhage. The haematuria is painless and she, has mild renal impairment., You answered Transitional cell carcinoma of the bladder, The correct answer is Polycystic kidney disease, This is likely to be polycystic kidney disease as she has renal failure and family history of, sub arachnoid haemorrhage., , 46., , A 75 year old lady is investigated for episodes of painless haematuria. Apart from COPD, from long term smoking she is otherwise well. She has no other urinary symptoms., Transitional cell carcinoma of the bladder, TCC commonly presents with painless haematuria that may be detected during testing, carried out for other reasons., , 47., , A 78 year old man has a long history of nocturia, urinary frequency and terminal dribbling., He was admitted with urinary retention and was catheterised. On removal of the catheter, he has noticed some haematuria., You answered Transitional cell carcinoma of the bladder, The correct answer is Benign prostatic hyperplasia, The symptoms are typical for prostatic disease., , Please rate this question:
Page 2809 :
Discuss and give feedback, , Next question, , Haematuria, Causes of haematuria, , Trauma, , , , , , , Injury to renal tract, Renal trauma commonly due to blunt injury (others penetrating, injuries), Ureter trauma rare: iatrogenic, Bladder trauma: due to RTA or pelvic fractures, , Infection, , , , Remember TB, , Malignancy, , , , , , , Renal cell carcinoma (remember paraneoplastic syndromes):, painful or painless, Urothelial malignancies: 90% are transitional cell carcinoma, can, occur anywhere along the urinary tract. Painless haematuria., Squamous cell carcinoma and adenocarcinoma: rare bladder, tumours, Prostate cancer, Penile cancers: SCC, , Renal disease, , , , Glomerulonephritis, , Stones, , , , Microscopic haematuria common, , Structural, abnormalities, , , , , , , Benign prostatic hyperplasia (BPH) causes haematuria due to, hypervascularity of the prostate gland, Cystic renal lesions e.g. polycystic kidney disease, Vascular malformations, Renal vein thrombosis due to renal cell carcinoma, , Coagulopathy, , , , Causes bleeding of underlying lesions, , Drugs, , , , Cause tubular necrosis or interstitial nephritis: aminoglycosides,, , ,
Page 2811 :
A 65 year old man presents with significant lower urinary tract symptoms and is diagnosed as having, benign prostatic hyperplasia. Which of the following drug treatments will produce the slowest clinical, response?, , Tamsulosin, , Alfuzosin, , Doxazosin, , Finasteride, , Terazosin, 5 alpha reductase inhibitors have a more favorable side effect profile than α blockers., Alpha blockers have a faster onset of action (but lower reduction of complications from BPH) than 5, α reductase inhibitors., Please rate this question:, , Discuss and give feedback, , Next question, , Benign Prostatic Hyperplasia, Benign prostatic hyperplasia occurs via an increase in the epithelial and stromal cell numbers in the, peri-urethral zone of the prostate. BPH is very common and 90% of men aged over 80 will have at, least microscopic evidence of benign prostatic hyperplasia. The causes of BPH are still not well, understood, but the importance of androgens remains appreciated even if the exact role by which, they induce BPH is elusive., Presentation, The vast majority of men will present with lower urinary tract symptoms. These will typically be:, , , , , , , , , Poor flow, Nocturia, Hesitancy, Incomplete and double voiding, Terminal dribbling, Urgency
Page 2812 :
, , Incontinence, , Investigation, , , , , , , Digital rectal examination to assess prostatic size and morphology., Urine dipstick for infections and haematuria., Uroflowmetry (a flow rate of >15ml/second helps to exclude BOO), Bladder pressure studies may help identify detrusor failure and whilst may not form part of, first line investigations should be included in those with atypical symptoms and prior to redo, surgery., Bladder scanning to demonstrate residual volumes. USS if high pressure chronic retention., , Management, , , , , , Lifestyle changes such as stopping smoking and altering fluid intake may help those with, mild symptoms., Medical therapy includes alpha blockers and 5 α reductase inhibitors. The former work, quickly on receptor zones located at the bladder neck. Cardiovascular side effects are well, documented. The latter work on testosterone metabolising enzymes. Although they have a, slower onset of action, the 5 α reductase inhibitors may prevent acute urinary retention., Surgical therapy includes transurethral resection of the prostate and is the treatment of, choice in those with severe symptoms and those who fail to respond to medical therapy., More tailored bladder neck incision procedures may be considered in those with small, prostates. Retrograde ejaculation may occur following surgery. The change in the type of, irrigation solutions used has helped to minimise the TURP syndrome of electrolyte, disturbances., Next question
Page 2813 :
Theme: Testicular disorders, , A., B., C., D., E., F., , Haematocele, Epididymal cyst, Hydrocele, Testicular torsion, Orchitis, Epididymo-orchitis, , Please select the most likely diagnosis for the scenario given. Each option may be used once, more, than once or not at all., , 49., , A 20 year old complains of severe pain and swelling of the scrotum after a cystoscopy. He, had mumps as a child. The testis is tender. The urine dipstick is positive for leucocytes., You answered Haematocele, The correct answer is Epididymo-orchitis, Epididymo-orchitis: acute pain and swelling after urological intervention. To differentiate, from testicular torsion there is usually pyrexia and positive urine dipstick., , 50., , A 20 year old complains of severe pain in the right scrotal area after jumping onto his, moped. He has also noticed discomfort in this area over the past few months. On, examination there is a swollen, painful testis that is drawn up into the groin., You answered Haematocele, The correct answer is Testicular torsion, Testicular torsion: Severe pain which can be spontaneous or precipitated by minor trauma., There is usually severe pain and the patient will often not tolerate the testis being touched., Urgent scrotal exploration is indicated. It is associated with a high investment of the the, tunica vaginalis with horizontal testicular lie, or when the epididymis and testis are, separated by a mesorchium, in which case the twist occurs at that point., , 51., , An 8 year old presents with scrotal swelling. He has just recovered from an acute viral, illness with swelling of the parotid glands. On examination both testes are tender and, slightly swollen., You answered Haematocele, The correct answer is Orchitis
Page 2814 :
Orchitis may be associated with mumps viral infections., Please rate this question:, , Discuss and give feedback, , Next question, , Scrotal swelling, Differential diagnosis, , Inguinal hernia, , If inguinoscrotal swelling; cannot "get above it" on examination, Cough impulse may be present, May be reducible, , Testicular tumours, , Often discrete testicular nodule (may have associated hydrocele), Symptoms of metastatic disease may be present, USS scrotum and serum AFP and β HCG required, , Acute epididymoorchitis, , Often history of dysuria and urethral discharge, Swelling may be tender and eased by elevating testis, Most cases due to Chlamydia, Infections with other gram negative organisms may be associated with, underlying structural abnormality, , Epididymal cysts, , Single or multiple cysts, May contain clear or opalescent fluid (spermatoceles), Usually occur over 40 years of age, Painless, Lie above and behind testis, It is usually possible to "get above the lump" on examination, , Hydrocele, , Non painful, soft fluctuant swelling, Often possible to "get above it" on examination, Usually contain clear fluid, Will often transilluminate, May be presenting feature of testicular cancer in young men
Page 2815 :
Testicular torsion, , Severe, sudden onset testicular pain, Risk factors include abnormal testicular lie, Typically affects adolescents and young males, On examination testis is tender and pain not eased by elevation, Urgent surgery is indicated, the contra lateral testis should also be fixed, , Varicocele, , Varicosities of the pampiniform plexus, Typically occur on left (because testicular vein drains into renal vein), May be presenting feature of renal cell carcinoma, Affected testis may be smaller and bilateral varicoceles may affect fertility, , Management, , , , , , , , Testicular malignancy is always treated with orchidectomy via an inguinal approach. This, allows high ligation of the testicular vessels and avoids exposure of another lymphatic field to, the tumour., Torsion is commonest in young teenagers and the history in older children can be difficult to, elicit. Intermittent torsion is a recognised problem. The treatment is prompt surgical, exploration and testicular fixation. This can be achieved using sutures or by placement of the, testis in a Dartos pouch., Varicoceles are usually managed conservatively. If there are concerns about testicular, function of infertility then surgery or radiological management can be considered., Epididymal cysts can be excised using a scrotal approach, Hydroceles are managed differently in children where the underlying pathology is a patent, processus vaginalis and therefore an inguinal approach is used in children so that the, processus can be ligated. In adults a scrotal approach is preferred and the hydrocele sac, excised or plicated., Next question
Page 2816 :
Theme: Renal imaging, , A. Non contrast abdominal CT scan, B. DMSA scan, C. PET/CT scan, D. MAG 3 Renogram, E. Renal ultrasound scan, F. DTPA Scan, G. Micturating cystourethrogram, H. Intra venous urography, , Please select the most appropriate imaging modality for the scenario descrived. Each agent may be, used once, more than once or not at all., , 52., , A 43 year old female has undergone a renal transplant 12 months previously. Over the past few, weeks there have been concerns about deteriorating renal function., You answered Non contrast abdominal CT scan, The correct answer is MAG 3 Renogram, Theme from 2010 Exam, Similar theme September 2012 Exam, Because it is excreted by renal tubular cells a MAG 3 renogram provides excellent imaging of renal, function and is often used in investigating failing transplants., , 53., , A 5 year old boy presents with recurrent urinary tract infections and left sided loin pain. On, investigation he is found to have a left sided PUJ obstruction, there are concerns that he may, have developed renal scarring., You answered Non contrast abdominal CT scan
Page 2817 :
The correct answer is DMSA scan, Although MAG 3 renograms may provide some information relating to the structural integrity of, the kidney, many still consider a DMSA scan to be the gold standard for the detection of renal, scarring (which is the main concern in PUJ obstruction and infections)., , 54., , A 17 year old man is referred to the urology clinic. As a child he was diagnosed as having a right, sided PUJ obstruction. However, he was lost to follow up. Over the past 7 months he has been, complaining of recurrent episodes of right loin pain. A CT scan shows considerable renal scarring., You answered Non contrast abdominal CT scan, The correct answer is MAG 3 Renogram, In patients with long standing PUJ obstruction and renal scarring the main diagnostic question is, whether the individual has sufficient renal function to consider a pyeloplasty or whether a, primary nephrectomy is preferable. Since the CT has demonstrated scarring there is no use in, obtaining a DMSA scan. Of the investigations listed both a DTPA and MAG 3 renogram will allow, assessment of renal function. However, MAG 3 is superior in the assessment of renal function in, damaged kidneys (as it is subjected to tubular secretion)., , Please rate this question:, , Discuss and give feedback, , Next question, , Functional renal imaging, DMSA scan, Dimercaptosuccinic acid (DMSA) scintigraphy, DMSA localises to the renal cortex with little accumulation in the renal papilla and medulla. It is, useful for the identification of cortical defects and ectopic or aberrant kidneys. It does not provide, useful information on the ureter of collecting system., Diethylene-triamine-penta-acetic acid (DTPA)
Page 2818 :
This is primarily a glomerular filtration agent. It is most useful for the assessment of renal function., Because it is filtered at the level of the glomerulus it provides useful information about the GFR., Image quality may be degraded in patients with chronic renal impairment and derangement of GFR., MAG 3 renogram, Mercaptoacetyle triglycine is an is extensively protein bound and is primarily secreted by tubular, cells rather than filtered at the glomerulus. This makes it the agent of choice for imaging the kidneys, of patients with existing renal impairment (where GFR is impaired)., Micturating cystourethrogram (MCUG scan), This scan provides information relating to bladder reflux and is obtained by filling the bladder with, contrast media (via a catheter) and asking the child to void. Images are taken during this phase and, the degree of reflux can be calculated, Intra venous urography, This examination is conducted by the administration of intravenous iodinated contrast media. The, agent is filtered by the kidneys and excreted and may provide evidence of renal stones or other, structural lesions. A rough approximation of renal function may be obtained using the technique. But, it is not primarily a technique to be used for this purpose. With the advent of widespread non, contrast CT scan protocols for the detection of urinary tract calculi it is now rarely used., PET/CT, This may be used to evaluate structurally indeterminate lesions in the staging of malignancy., References, Davis A et al. Investigating urinary tract infections in children. BMJ 2013 (346):35-37., Next question
Page 2819 :
A 35-year-old female is admitted to hospital with hypovolaemic shock. CT abdomen reveals a, haemorrhagic lesion in the right kidney. Following surgery and biopsy this is shown to be an, angiomyolipomata. What is the most likely underlying diagnosis?, , Neurofibromatosis, , Budd-Chiari syndrome, , Hereditary haemorrhagic telangiectasia, , Von Hippel-Lindau syndrome, , Tuberous sclerosis, , Please rate this question:, , Discuss and give feedback, , Next question, , Tuberous sclerosis, Tuberous sclerosis (TS) is a genetic condition of autosomal dominant inheritance. Like, neurofibromatosis, the majority of features seen in TS are neuro-cutaneous, Cutaneous features, , , , , , , depigmented 'ash-leaf' spots which fluoresce under UV light, roughened patches of skin over lumbar spine (Shagreen patches), adenoma sebaceum: butterfly distribution over nose, fibromata beneath nails (subungual fibromata), café-au-lait spots* may be seen, , Neurological features, , , , , developmental delay, epilepsy (infantile spasms or partial), intellectual impairment
Page 2820 :
Also, , , , , , retinal hamartomas: dense white areas on retina (phakomata), rhabdomyomas of the heart, gliomatous changes can occur in the brain lesions, polycystic kidneys, renal angiomyolipomata, , *these of course are more commonly associated with neurofibromatosis. However a 1998 study of, 106 children with TS found café-au-lait spots in 28% of patients, Next question
Page 2821 :
A 22 year old man is participating in vigorous intercourse and suddenly feels a snap and his penis, becomes swollen and painful. The admitting surgeon suspects a penile fracture. Which of the, following is the most appropriate initial management?, , MRI scan of the penis, , Immediate surgical exploration, , CT scan of the penis, , USS of the penis, , Cystogram, , Suspected penile fractures should be surgically explored and the injury repaired., Please rate this question:, , Discuss and give feedback, , Next question, , Penile fracture, Penile fractures are a rare type of urological trauma that may be encountered. The injury is usually in, the proximal part of the penile shaft and may involve the urethra. A classically history of a snapping, sensation followed by immediate pain is usually given by the patient (usually during vigorous, intercourse). On examination there is usually a tense haematoma and blood may be seen at the, meatus if the urethra is injured., When there is a a strong suspicion of the diagnosis the correct management is surgical and a, circumferential incision made immediately inferior to the glans. The skin and superficial tissues are, stripped back and the penile shaft inspected. Injuries are usually sutured and the urethra repaired, over a catheter., Next question
Page 2822 :
Which of the following does not cause red urine?, , Rifampicin, , Phosphaturia, , Beetroot, , Rhubarb, , Blackberries, , Phosphaturia causes cloudy urine., Please rate this question:, , Discuss and give feedback, , Next question, , Haematuria, Causes of haematuria, , Trauma, , , , , , , Injury to renal tract, Renal trauma commonly due to blunt injury (others penetrating, injuries), Ureter trauma rare: iatrogenic, Bladder trauma: due to RTA or pelvic fractures, , Infection, , , , Remember TB, , Malignancy, , , , Renal cell carcinoma (remember paraneoplastic syndromes):, painful or painless, Urothelial malignancies: 90% are transitional cell carcinoma, can, occur anywhere along the urinary tract. Painless haematuria., Squamous cell carcinoma and adenocarcinoma: rare bladder, tumours, Prostate cancer, , , ,
Page 2824 :
From the list below, which drug is known to cause haemorrhagic cystitis?, , Rifampicin, , Methotrexate, , Dexamethasone, , Leflunomide, , Cyclophosphamide, , Cyclophosphamide is metabolised into a toxic metabolite acrolein. The effects may be attenuated by, administration of large volumes of intravenous fluids and mesna (which neutralises the metabolite)., The condition may be managed initially by bladder catheterisation and irrigation., Please rate this question:, , Discuss and give feedback, , Next question, , Haematuria, Causes of haematuria, , Trauma, , , , , , , Injury to renal tract, Renal trauma commonly due to blunt injury (others penetrating, injuries), Ureter trauma rare: iatrogenic, Bladder trauma: due to RTA or pelvic fractures, , Infection, , , , Remember TB, , Malignancy, , , , Renal cell carcinoma (remember paraneoplastic syndromes):, painful or painless, Urothelial malignancies: 90% are transitional cell carcinoma, can, occur anywhere along the urinary tract. Painless haematuria., Squamous cell carcinoma and adenocarcinoma: rare bladder, , ,
Page 2826 :
Theme: Management of prostatic disease, , A., B., C., D., E., F., G., H., I., , Commence alpha blocker, Commence 5 alpha reductase inhibitor, Transurethral resection of the prostate, Commence LnRH analogue, Radical prostatectomy, Transvesical prostatectomy, Unilateral orchidectomy, Watch and wait, Radical radiotherapy, , For the prostatic disorders described please select the most appropriate management option. Each, option may be used once, more than once or not at all., , 59., , A 49 year old man presents with a single episode of haematuria. Investigations, demonstrate adenocarcinoma of the prostate gland. Imaging shows T2 disease and no, evidence of metastasis., You answered Commence alpha blocker, The correct answer is Radical prostatectomy, In a young patient with local disease only a radical prostatectomy is the best chance of, cure. Radiotherapy may be given instead but has long term sequelae (and inferior survival, outcomes). A transvesical prostatectomy is a largely historical operation performed for, BPH before TURP was established., , 60., , A 72 year old man is admitted with acute urinary retention. On examination he has a small, but palpable bladder. Digital rectal examination identifies a benign feeling enlarged, prostate gland. He has been treated with finasteride for the past 9 months., You answered Commence alpha blocker, The correct answer is Transurethral resection of the prostate, Medical therapy has failed and although an alpha blocker may help his symptoms he, would fare better with a TURP., , 61., , A 73 year old man presents with haematuria. Investigations demonstrate a localised, high, risk, prostatic cancer. His co-morbidities include COPD and ischaemic heart disease. His, staging investigations show no evidence of metastatic disease
Page 2827 :
You answered Commence alpha blocker, The correct answer is Radical radiotherapy, The co-morbidities of this patient make a surgical approach a less favorable option., Radical radiotherapy offers a more favorable alternative., Please rate this question:, , Discuss and give feedback, , Next question, , Prostate Cancer, Prostate Cancer, This is a common condition and up to 30,000 men are diagnosed with the condition each year. Up to, 9,000 will die in in the UK from the condition per year., Diagnosis, Early prostate cancers have few symptoms., Metastatic disease may present as bone pain., Locally advanced disease may present as pelvic pain or with urinary symptoms., Prostate specific antigen measurement, Digital rectal examination, Trans rectal USS (+/- biopsy), MRI/ CT and bone scan for staging., PSA Test, The normal upper limit for PSA is 4ng/ml. However, in this group will lie patients with benign disease, and some with localised prostate cancer. False positives may be due to prostatitis, UTI, BPH,, vigorous DRE., The percentage of free: total PSA may help to distinguish benign disease from cancer. Values of, <20% are suggestive of cancer and biopsy is advised., Pathology, , , , , , , 95% adenocarcinoma, In situ malignancy is sometimes found in areas adjacent to cancer. Multiple biopsies needed, to call true in situ disease., Often multifocal- 70% lie in the peripheral zone., Graded using the Gleason grading system, two grades awarded 1 for most dominant grade, (on scale of 1-5) and 2 for second most dominant grade (scale 1-5). The two added together, give the Gleason score. Where 2 is best prognosis and 10 the worst., Lymphatic spread occurs first to the obturator nodes and local extra prostatic spread to the, seminal vesicles is associated with distant disease.
Page 2828 :
Treatment, , , , , , , , , Watch and wait- Elderly, multiple co-morbidities, low Gleason score, Radiotherapy (External)- Both potentially curative and palliative therapy possible. However,, radiation proctitis and rectal malignancy are late problems. Brachytherapy is a modification, allowing internal radiotherapy., Surgery- Radical prostatectomy. Surgical removal of the prostate is the standard treatment, for localised disease. The robot is being used increasingly for this procedure. As well as the, prostate the obturator nodes are also removed to complement the staging process. Erectile, dysfunction is a common side effect. Survival may be better than with radiotherapy (see, references)., Hormonal therapy- Testosterone stimulates prostate tissue and prostatic cancers usually, show some degree of testosterone dependence. 95% of testosterone is derived from the, testis and bilateral orchidectomy may be used for this reason. Pharmacological alternatives, include LHRH analogues and anti androgens (which may be given in combination)., In the UK the National Institute for Clinical Excellence (NICE) suggests that active, surveillance is the preferred option for low risk men. It is particularly suitable for men with, clinical stage T1c, Gleason score 3+3 and PSA density < 0.15 ng/ml/ml who have cancer in, less than 50% of their biopsy cores, with < 10 mm of any core involved., , Candidates for active surveillance should:, , , , have had at least 10 biopsy cores taken, have at least one re-biopsy., , If men on active surveillance show evidence of disease progression, offer radical treatment., Treatment decisions should be made with the man, taking into account co-morbidities and life, expectancy., References, 1. Prostate cancer pathway. NICE.(http://guidance.nice.org.uk/IPG424), 2. Sooriakumaran P et al. Comparative effectiveness of radical prostatectomy and radiotherapy in, prostate cancer: observational study of mortality outcomes. BMJ 2014 (348):13. This study shows, that in men with localised disease survival was greater in those offered surgery., Next question
Page 2829 :
Theme: Haematuria, , A., B., C., D., E., F., , Squamous cell carcinoma of the renal pelvis, Renal adenocarcinoma, Nephroblastoma, Retroperitoneal fibrosis, Transitional cell carcinoma of the renal pelvis, Retroperitoneal sarcoma, , Please select the most likely lesion for the scenario given. Each option may be used once, more, than once or not at all., , 62., , A 72 year old man presents with haematuria which is recurrent. On investigation a, retrograde pyelogram shows multiple ureteric filling defects and the renal pelvis is, irregular., You answered Squamous cell carcinoma of the renal pelvis, The correct answer is Transitional cell carcinoma of the renal pelvis, TCC of the renal pelvis may seed down the ureter., , 63., , An 83 year old man with a long standing staghorn calculus presents with recurrent, haematuria and investigation shows a mass of the left renal pelvis., Squamous cell carcinoma of the renal pelvis, SCC of the kidney usually arises in an area of chronic inflammation such as a staghorn, calculus., , 64., , A 28 year old man presents to his GP with haematuria and on examination is noted to have, a varicocele. He was noted to have renal colic 8 weeks ago which was secondary to, hypercalcaemia., You answered Squamous cell carcinoma of the renal pelvis, The correct answer is Renal adenocarcinoma, Renal adenocarcinoma on the left side may invade the gonadal vein and produce, varicocele. They also have paraneoplastic phenomena such as hypercalcaemia., , Please rate this question:
Page 2830 :
Discuss and give feedback, , Next question, , Haematuria, Causes of haematuria, , Trauma, , , , , , , Injury to renal tract, Renal trauma commonly due to blunt injury (others penetrating, injuries), Ureter trauma rare: iatrogenic, Bladder trauma: due to RTA or pelvic fractures, , Infection, , , , Remember TB, , Malignancy, , , , , , , Renal cell carcinoma (remember paraneoplastic syndromes):, painful or painless, Urothelial malignancies: 90% are transitional cell carcinoma, can, occur anywhere along the urinary tract. Painless haematuria., Squamous cell carcinoma and adenocarcinoma: rare bladder, tumours, Prostate cancer, Penile cancers: SCC, , Renal disease, , , , Glomerulonephritis, , Stones, , , , Microscopic haematuria common, , Structural, abnormalities, , , , , , , Benign prostatic hyperplasia (BPH) causes haematuria due to, hypervascularity of the prostate gland, Cystic renal lesions e.g. polycystic kidney disease, Vascular malformations, Renal vein thrombosis due to renal cell carcinoma, , Coagulopathy, , , , Causes bleeding of underlying lesions, , Drugs, , , , Cause tubular necrosis or interstitial nephritis: aminoglycosides,, chemotherapy, Interstitial nephritis: penicillin, sulphonamides, and NSAIDs, , , , ,
Page 2832 :
Theme: Urinary incontinence, , A., B., C., D., E., F., G., H., , Bladder diary for 3 days, Urodynamic studies, Bladder drill training for 6 weeks, Pelvic floor exercises 3 months, Oxybutynin, IV urography, Urinary dye studies, None of the above, , Choose the best management option for each clinical scenario. Each option may be used once,, more than once or not at all., , 65., , A 34 year old woman from Africa presents with continuous dribbling incontinence after, having her 2nd child. Apart from prolonged labour the woman denies any complications, related to her pregnancies. She is normally fit and well., You answered Bladder diary for 3 days, The correct answer is Urinary dye studies, Vesicovaginal fistulae should be suspected in patients with continuous dribbling, incontinence after prolonged labour and from a country with poor obstetric services. A dye, stains the urine and hence identifies the presence of a fistula., , 66., , A 53 year old lady complains of involuntary passage of urine when she coughs or sneezes., She is multiparous G2, P2 with a forceps delivery of her second child., You answered Bladder diary for 3 days, The correct answer is Pelvic floor exercises 3 months, The first line management of stress urinary incontinence, in this case arising for pelvic, floor trauma is pelvic floor exercises. These will help a proportion of patients. Non, responders should have urodynamics performed to confirm the diagnosis., , 67., , A 56 year old lady reports incontinence mainly when walking the dog. A bladder diary is, inconclusive., You answered Bladder diary for 3 days, The correct answer is Urodynamic studies
Page 2833 :
Urodynamic studies are indicated when there is diagnostic uncertainty or plans for surgery., Please rate this question:, , Discuss and give feedback, , Next question, , Urinary incontinence, Involuntary passage of urine. Most cases are female (80%). It has a prevalence of 11% in those, aged greater than 65 years. The commonest variants include:, , , , , Stress urinary incontinence (50%), Urge incontinence (15%), Mixed (35%), , Males, Males may also suffer from incontinence although it is a much rarer condition in men. A number of, anatomical factors contribute to this. Males have 2 powerful sphincters; one at the bladder neck and, the other in the urethra. Damage to the bladder neck mechanism is a factor in causing retrograde, ejaculation following prostatectomy. The short segment of urethra passing through the urogenital, diaphragm consists of striated muscle fibres (the external urethral sphincter) and smooth muscle, capable of more sustained contraction. It is the latter mechanism that maintains continence following, prostatectomy., Females, The sphincter complex at the level of bladder neck is poorly developed in females. As a result the, external sphincter complex is functionally more important, its composition being similar to that of, males. Innervation is via the pudendal nerve and the neuropathy that may accompany obstetric, events may compromise this and lead to stress urinary incontinence., Innervation, Somatic innervation to the bladder is via the pudendal, hypogastric and pelvic nerves. Autonomic, nerves travel in these nerve fibres too. Bladder filling leads to detrusor relaxation (sympathetic), coupled with sphincter contraction. The parasympathetic system causes detrusor contraction and, sphincter relaxation. Overall control of micturition is centrally mediated via centres in the Pons., Stress urinary incontinence, , , , , 50% of cases, especially in females., Damage (often obstetric) to the supporting structures surrounding the bladder may lead to, urethral hypermobility., Other cases due to sphincter dysfunction, usually from neurological disorders (e.g. Pudendal, neuropathy, multiple sclerosis).
Page 2834 :
Urethral mobility:, Pressure not transmitted appropriately to the urethra resulting in involuntary passage of urine during, episodes of raised intra-abdominal pressure., Sphincter dysfunction:, Sphincter fails to adapt to compress urethra resulting in involuntary passage of urine. When the, sphincter completely fails there is often to continuous passage of urine., Urge incontinence, In these patients there is sense of urgency followed by incontinence. The detrusor muscle in these, patients is unstable and urodynamic investigation will demonstrate overactivity of the detrusor, muscle at inappropriate times (e.g. Bladder filling). Urgency may be seen in patients with overt, neurological disorders and those without. The pathophysiology is not well understood but poor, central and peripheral co-ordination of the events surrounding bladder filling are the main, processes., Assessment, Careful history and examination including vaginal examination for cystocele., Bladder diary for at least 3 days, Consider flow cystometry if unclear symptomatology or surgery considered and diagnosis is unclear., Exclusion of other organic disease (e.g. Stones, UTI, Cancer), Management, Conservative measures should be tried first; Stress urinary incontinence or mixed symptoms should, undergo 3 months of pelvic floor exercise. Over active bladder should have 6 weeks of bladder, retraining., Drug therapy for women with overactive bladder should be offered oxybutynin (or solifenacin if, elderly) if conservative measures fail., In women with detrusor instability who fail non operative therapy a trial of sacral neuromodulation, may be considered, with conversion to permanent implant if good response. Augmentation, cystoplasty is an alternative but will involve long term intermittent self catheterisation., In women with stress urinary incontinence a urethral sling type procedure may be undertaken., Where cystocele is present in association with incontinence it should be repaired particularly if it lies, at the introitus., NICE guidelines, , , , , , , , , Initial assessment urinary incontinence should be classified as stress/urge/mixed., At least 3/7 bladder diary if unable to classify easily., Start conservative treatment before urodynamic studies if a diagnosis is obvious from the, history, Urodynamic studies if plans for surgery., Stress incontinence: Pelvic floor exercises 3/12, if fails consider surgery., Urge incontinence: Bladder training >6/52, if fails for oxybutynin (antimuscarinic drugs) then, sacral nerve stimulation., Pelvic floor exercises offered to all women in their 1st pregnancy., Next question
Page 2835 :
A 72 year old man presents with lower urinary tract symptoms. On digital rectal examination, benign, prostatic hyperplasia is suspected. Which of the following treatments is associated with a reduction, in the risk of urinary retention?, , Alfuzosin, , Finasteride, , Prazosin, , Tamsulosin, , Terazosin, , 5 alpha reductase inhibitors reduce the risk of urinary retention., In the PLESS study, data show a reduction in the risk of urinary retention although the absolute risk, reduction was small., Reference, McConnell J et al. The effect of finasteride on the risk of urinary retention and the need for surgical, intervention amongst men with benign prostatic hyperplasia. N Engl J Med 338:557-563, Please rate this question:, , Discuss and give feedback, , Next question, , Benign Prostatic Hyperplasia, Benign prostatic hyperplasia occurs via an increase in the epithelial and stromal cell numbers in the, peri-urethral zone of the prostate. BPH is very common and 90% of men aged over 80 will have at, least microscopic evidence of benign prostatic hyperplasia. The causes of BPH are still not well, understood, but the importance of androgens remains appreciated even if the exact role by which, they induce BPH is elusive., Presentation, The vast majority of men will present with lower urinary tract symptoms. These will typically be:, , , , , , Poor flow, Nocturia, Hesitancy
Page 2836 :
, , , , , Incomplete and double voiding, Terminal dribbling, Urgency, Incontinence, , Investigation, , , , , , , Digital rectal examination to assess prostatic size and morphology., Urine dipstick for infections and haematuria., Uroflowmetry (a flow rate of >15ml/second helps to exclude BOO), Bladder pressure studies may help identify detrusor failure and whilst may not form part of, first line investigations should be included in those with atypical symptoms and prior to redo, surgery., Bladder scanning to demonstrate residual volumes. USS if high pressure chronic retention., , Management, , , , , , Lifestyle changes such as stopping smoking and altering fluid intake may help those with, mild symptoms., Medical therapy includes alpha blockers and 5 α reductase inhibitors. The former work, quickly on receptor zones located at the bladder neck. Cardiovascular side effects are well, documented. The latter work on testosterone metabolising enzymes. Although they have a, slower onset of action, the 5 α reductase inhibitors may prevent acute urinary retention., Surgical therapy includes transurethral resection of the prostate and is the treatment of, choice in those with severe symptoms and those who fail to respond to medical therapy., More tailored bladder neck incision procedures may be considered in those with small, prostates. Retrograde ejaculation may occur following surgery. The change in the type of, irrigation solutions used has helped to minimise the TURP syndrome of electrolyte, disturbances., Next question
Page 2837 :
A 22 year old man is involved in a road traffic accident. He is found to have a pelvic fracture. While, on the ward the nursing staff report that he is complaining of lower abdominal pain. On examination, you find a distended tender bladder. What is the best management?, , 10 Ch foley urethral catheter, , Suprapubic catheter, , 16 Ch foley urethral catheter, , 18 Ch coude tip urethral catheter, , Pain relief and review in 1 hour, , This patient has possible urethral injury based on the history. Urethral catheterisation is, contraindicated in this situation., Please rate this question:, , Discuss and give feedback, , Next question, , Lower genitourinary tract trauma, , , , , , Most bladder injuries occur due to blunt trauma, 85% associated with pelvic fractures, Easily overlooked during assessment in trauma, Up to 10% of male pelvic fractures are associated with urethral or bladder injuries, , Types of injury, , Urethral injury, , , , , , Mainly in males, Blood at the meatus (50% cases), There are 2 types:, , i.Bulbar rupture, - most common, - straddle type injury e.g. bicycles, - triad signs: urinary retention, perineal haematoma, blood at the, meatus
Page 2838 :
ii. Membranous rupture, - can be extra or intraperitoneal, - commonly due to pelvic fracture, - Penile or perineal oedema/ hematoma, - PR: prostate displaced upwards (beware co-existing, retroperitoneal haematomas as they may make examination, difficult), - Investigation: ascending urethrogram, - Management: suprapubic catheter (surgical placement, not, percutaneously), External genitalia injuries, (i.e., the penis and the, scrotum), , , , Secondary to injuries caused by penetration, blunt trauma,, continence- or sexual pleasure-enhancing devices, and, mutilation, , Bladder injury, , , , , , rupture is intra or extraperitoneal, presents with haematuria or suprapubic pain, history of pelvic fracture and inability to void: always, suspect bladder or urethral injury, inability to retrieve all fluid used to irrigate the bladder, through a Foley catheter indicates bladder injury, investigation- IVU or cystogram, management: laparotomy if intraperitoneal, conservative if, extraperitoneal, , , , , , Next question
Page 2839 :
Which of the following procedures represents the optimal operative procedure for testicular cancer?, , Lords procedure, , Orchidectomy via a scrotal approach, , Orchidectomy via inguinal approach, , Orchidectomy via a combined inguino-scrotal approach, , None of the above, , Testicular tumours metastasise to Para aortic nodes and thus an inguinal rather than scrotal, approach should be used. There are two main operations that are termed Lords procedure; one is, for fissure in ano and the other is a procedure for hydrocele., Please rate this question:, , Discuss and give feedback, , Next question, , Testicular disorders, Testicular cancer, Testicular cancer is the most common malignancy in men aged 20-30 years. Around 95% of cases, of testicular cancer are germ-cell tumours. Germ cell tumours may essentially be divided into:, , Tumour type, , Seminoma, , Key features, , , , , Commonest, subtype (50%), Average age at, diagnosis = 40, Even advanced, disease associated, with 5 year, survival of 73%, , Tumour, markers, , Pathology, , AFP usually, normal, HCG elevated, in 10%, seminomas, Lactate, dehydrogenase;, elevated in 1020% seminomas, , Sheet like lobular, patterns of cells, with substantial, fibrous, component., Fibrous septa, contain, lymphocytic, inclusions and
Page 2840 :
Tumour type, , Non seminomatous germ, cell tumours (42%), , , , , , Teratoma, Yolk sac tumour, Choriocarcinoma, Mixed germ cell, tumours (10%), , Key features, , Younger age at, presentation =20-30, years, Advanced disease, carries worse prognosis, (48% at 5 years), Retroperitoneal lymph, node dissection may be, needed for residual, disease after, chemotherapy, , Tumour, markers, , Pathology, , (but also in many, other conditions), , granulomas may, be seen., , AFP elevated, in up to 70% of, cases, HCG elevated, in up to 40% of, cases, Other markers, rarely helpful, , Heterogenous, texture with, occasional ectopic, tissue such as hair, , Image demonstrating a classical seminoma, these tumours are typically more uniform than, teratomas
Page 2841 :
Image sourced from Wikipedia, , Risk factors for testicular cancer, , , , , , , Cryptorchidism, Infertility, Family history, Klinefelter's syndrome, Mumps orchitis, , Features
Page 2842 :
, , , , A painless lump is the most common presenting symptom, Pain may also be present in a minority of men, Other possible features include hydrocele, gynaecomastia, , Diagnosis, , , , , Ultrasound is first-line, CT scanning of the chest/ abdomen and pelvis is used for staging, Tumour markers (see above) should be measured, , Management, , , , , Orchidectomy (Inguinal approach), Chemotherapy and radiotherapy may be given depending on staging, Abdominal lesions >1cm following chemotherapy may require retroperitoneal lymph node, dissection., , Prognosis is generally excellent, , , , 5 year survival for seminomas is around 95% if Stage I, 5 year survival for teratomas is around 85% if Stage I, , Benign disease, Epididymo-orchitis, Acute epididymitis is an acute inflammation of the epididymis, often involving the testis and usually, caused by bacterial infection., , , , , Infection spreads from the urethra or bladder. In men <35 years, gonorrhoea or chlamydia, are the usual infections., Amiodarone is a recognised non infective cause of epididymitis, which resolves on stopping, the drug., Tenderness is usually confined to the epididymis, which may facilitate differentiating it from, torsion where pain usually affects the entire testis., , Testicular torsion, , , , , , Twist of the spermatic cord resulting in testicular ischaemia and necrosis., Most common in males aged between 10 and 30 (peak incidence 13-15 years), Pain is usually severe and of sudden onset., Cremasteric reflex is lost and elevation of the testis does not ease the pain.
Page 2843 :
, , Treatment is with surgical exploration. If a torted testis is identified then both testis should be, fixed as the condition of bell clapper testis is often bilateral., , Hydrocele, , , , , , , Presents as a mass that transilluminates, usually possible to "get above" it on examination., In younger men it should be investigated with USS to exclude tumour., In children it may occur as a result of a patent processus vaginalis., Treatment in adults is with a Lords or Jabouley procedure., Treatment in children is with trans inguinal ligation of PPV., Next question
Page 2844 :
Theme: Management of testicular disorders, , A., B., C., D., E., F., G., , Fine needle aspiration cytology, Tru Cut biopsy, Orchidectomy via inguinal approach, Orchidectomy via scrotal approach, Administration of antibiotics, Exploration of scrotum via scrotal approach, Reassure and discharge, , Please select the most appropriate management option for the scenario given. Each option may be, used once, more than once or not at all., , 71., , A 22 year old man presents with an aching pain and discomfort in his right testicle. He has, felt systemically unwell for the preceding 48 hours. On examination there is tenderness of, the right testicle. He has an exaggerated cremasteric reflex., You answered Fine needle aspiration cytology, The correct answer is Administration of antibiotics, This is likely to represent epididymo-orchitis, this is usually due to infection with, gonorrhoea or chlamydia in this age group. In addition to treatment with antibiotics contact, tracing and appropriate swabs should also be performed., , 72., , A 25 year old man presents with aching and discomfort of his right testicle. He has felt, generally unwell and lethargic over the past few weeks. On examination there is a small, nodule palpable in the testis, on ultrasound this is hypoechoic. Systematic examination, demonstrates supraclavicular lymphadenopathy., You answered Fine needle aspiration cytology, The correct answer is Orchidectomy via inguinal approach, Hypoechoic masses within the testicle in the context are most likely to represent, malignancy. He should have a staging CT scan, thereafter an orchidectomy should be, performed via an inguinal approach. Percutaneous biopsy has no role in the management, of testicular malignancy., , 73., , A 15 year old boy is woken from sleep by a severe pain in his left testicle. He was, previously fit and well. On examination he has a tender left testicle with an absent, cremasteric reflex.
Page 2845 :
You answered Fine needle aspiration cytology, The correct answer is Exploration of scrotum via scrotal approach, This is likely to represent torsion, surgical exploration is warranted., Please rate this question:, , Discuss and give feedback, , Next question, , Testicular disorders, Testicular cancer, Testicular cancer is the most common malignancy in men aged 20-30 years. Around 95% of cases, of testicular cancer are germ-cell tumours. Germ cell tumours may essentially be divided into:, , Tumour type, , Seminoma, , Tumour, markers, , Pathology, , Commonest, subtype (50%), Average age at, diagnosis = 40, Even advanced, disease associated, with 5 year, survival of 73%, , AFP usually, normal, HCG elevated, in 10%, seminomas, Lactate, dehydrogenase;, elevated in 1020% seminomas, (but also in many, other conditions), , Sheet like lobular, patterns of cells, with substantial, fibrous, component., Fibrous septa, contain, lymphocytic, inclusions and, granulomas may, be seen., , Younger age at, presentation =20-30, years, Advanced disease, carries worse prognosis, (48% at 5 years), Retroperitoneal lymph, node dissection may be, needed for residual, disease after, , AFP elevated, in up to 70% of, cases, HCG elevated, in up to 40% of, cases, Other markers, rarely helpful, , Heterogenous, texture with, occasional ectopic, tissue such as hair, , Key features, , , , , Non seminomatous germ, cell tumours (42%), , , , , , Teratoma, Yolk sac tumour, Choriocarcinoma, Mixed germ cell, tumours (10%)
Page 2846 :
Tumour type, , Key features, , Tumour, markers, , Pathology, , chemotherapy, Image demonstrating a classical seminoma, these tumours are typically more uniform than, teratomas, , Image sourced from Wikipedia, , Risk factors for testicular cancer
Page 2847 :
, , , , , , Cryptorchidism, Infertility, Family history, Klinefelter's syndrome, Mumps orchitis, , Features, , , , , A painless lump is the most common presenting symptom, Pain may also be present in a minority of men, Other possible features include hydrocele, gynaecomastia, , Diagnosis, , , , , Ultrasound is first-line, CT scanning of the chest/ abdomen and pelvis is used for staging, Tumour markers (see above) should be measured, , Management, , , , , Orchidectomy (Inguinal approach), Chemotherapy and radiotherapy may be given depending on staging, Abdominal lesions >1cm following chemotherapy may require retroperitoneal lymph node, dissection., , Prognosis is generally excellent, , , , 5 year survival for seminomas is around 95% if Stage I, 5 year survival for teratomas is around 85% if Stage I, , Benign disease, Epididymo-orchitis, Acute epididymitis is an acute inflammation of the epididymis, often involving the testis and usually, caused by bacterial infection., , , , Infection spreads from the urethra or bladder. In men <35 years, gonorrhoea or chlamydia, are the usual infections., Amiodarone is a recognised non infective cause of epididymitis, which resolves on stopping, the drug.
Page 2848 :
, , Tenderness is usually confined to the epididymis, which may facilitate differentiating it from, torsion where pain usually affects the entire testis., , Testicular torsion, , , , , , , Twist of the spermatic cord resulting in testicular ischaemia and necrosis., Most common in males aged between 10 and 30 (peak incidence 13-15 years), Pain is usually severe and of sudden onset., Cremasteric reflex is lost and elevation of the testis does not ease the pain., Treatment is with surgical exploration. If a torted testis is identified then both testis should be, fixed as the condition of bell clapper testis is often bilateral., , Hydrocele, , , , , , , Presents as a mass that transilluminates, usually possible to "get above" it on examination., In younger men it should be investigated with USS to exclude tumour., In children it may occur as a result of a patent processus vaginalis., Treatment in adults is with a Lords or Jabouley procedure., Treatment in children is with trans inguinal ligation of PPV., Next question
Page 2849 :
Theme: Haematuria, , A., B., C., D., E., F., G., , Interstitial nephritis, Membranous glomerulonephritis, Endometriosis, Placenta percreta, Adult polycystic kidney disease, Renal vein thrombosis, Urinary tract infection, , Please select the most likely cause for haematuria for the scenario described. Each option may be, used once, more than once or not at all., , 74., , A 22 year female who is 24 weeks pregnant presents with frank haematuria. She is, sexually active. She has had a previous pregnancy resulting in caesarean section., You answered Interstitial nephritis, The correct answer is Placenta percreta, Pregnancy and frank haematuria, especially if there is a history of placenta previa or prior, caesarean section, should indicate this diagnosis. There is invasive placental implantation, into the myometrium, which can rarely extend into the bladder causing severe bleeding., , 75., , A 22 year old woman presents with macroscopic haematuria. She is sexually active. She is, known to have renal calculi and had a berry aneurysm clipped., You answered Interstitial nephritis, The correct answer is Adult polycystic kidney disease, APKD is associated with liver cysts (70%), berry aneurysms (25%) and pancreatic cysts, (10%). Patients may have a renal mass, hypertension, renal calculi and macroscopic, haematuria., , 76., , A 45 year woman presents with haematuria. She has a temperature of 38 oC and is found to, have a Hb 17. Her urine dipstick shows nitrites and 3+ blood. Blood and urine cultures are, negative., You answered Interstitial nephritis, The correct answer is Renal vein thrombosis
Page 2850 :
Renal vein thrombosis is a common feature of renal cell carcinoma as it invades the renal, vein. Other features include PUO, left varicocele and paraneoplastic endocrine effects due, to erythropoietin factor, renin, ACTH and PTH like substance., Please rate this question:, , Discuss and give feedback, , Next question, , Haematuria, Causes of haematuria, , Trauma, , , , , , , Injury to renal tract, Renal trauma commonly due to blunt injury (others penetrating, injuries), Ureter trauma rare: iatrogenic, Bladder trauma: due to RTA or pelvic fractures, , Infection, , , , Remember TB, , Malignancy, , , , , , , Renal cell carcinoma (remember paraneoplastic syndromes):, painful or painless, Urothelial malignancies: 90% are transitional cell carcinoma, can, occur anywhere along the urinary tract. Painless haematuria., Squamous cell carcinoma and adenocarcinoma: rare bladder, tumours, Prostate cancer, Penile cancers: SCC, , Renal disease, , , , Glomerulonephritis, , Stones, , , , Microscopic haematuria common, , Structural, abnormalities, , , , Benign prostatic hyperplasia (BPH) causes haematuria due to, hypervascularity of the prostate gland, Cystic renal lesions e.g. polycystic kidney disease, Vascular malformations, , , , , ,
Page 2852 :
A 55 year old man presents with an episode of frank haematuria and on investigation is found to, have a T2 transitional cell carcinoma of the bladder. His staging investigations are negative for, metastatic disease. What is the most appropriate treatment?, , Radical cystectomy, , Palliative radiotherapy, , Intravesical BCG, , Intravesical mitomycin C, , Intravesical cisplatin, , T2 lesions in a young fit patient are best managed surgically. Up to 25 % patients may develop, perioperative complications. However, palliative treatments and intravesical chemotherapy (which, does NOT include cisplatin) are not used curatively in this situation., Please rate this question:, , Discuss and give feedback, , Next question, , Bladder cancer, Bladder cancer is the second most common urological cancer. It most commonly affects males aged, between 50 and 80 years of age. Those who are current, or previous (within 20 years), smokers, have a 2-5 fold increased risk of the disease. Exposure to hydrocarbons such as 2-Naphthylamine, increases the risk. Although rare in the UK, chronic bladder inflammation arising from, Schistosomiasis infection remains a common cause of squamous cell carcinomas, in those countries, where the disease is endemic., Benign tumours, Benign tumours of the bladder including inverted urothelial papilloma and nephrogenic adenoma are, uncommon., Bladder malignancies, , , , , Transitional cell carcinoma (>90% of cases), Squamous cell carcinoma ( 1-7% -except in regions affected by schistosomiasis), Adenocarcinoma (2%)
Page 2853 :
Transitional cell carcinomas may arise as solitary lesions, or may be multifocal, owing to the effect of, "field change" within the urothelium. Up to 70% of TCC's will have a papillary growth pattern. These, tumours are usually superficial in location and accordingly have a better prognosis. The remaining, tumours show either mixed papillary and solid growth or pure solid growths. These tumours are, typically more prone to local invasion and may be of higher grade, the prognosis is therefore worse., Those with T3 disease or worse have a 30% (or higher) risk of regional or distant lymph node, metastasis., TNM Staging, , Stage, , Description, , T0, , No evidence of tumour, , Ta, , Non invasive papillary carcinoma, , T1, , Tumour invades sub epithelial connective tissue, , T2a, , Tumor invades superficial muscularis propria (inner half), , T2b, , Tumor invades deep muscularis propria (outer half), , T3, , Tumour extends to perivesical fat, , T4, , Tumor invades any of the following: prostatic stroma, seminal vesicles, uterus, vagina, , T4a, , Invasion of uterus, prostate or bowel, , T4b, , Invasion of pelvic sidewall or abdominal wall, , N0, , No nodal disease, , N1, , Single regional lymph node metastasis in the true pelvis (hypogastric, obturator, external, iliac, or presacral lymph node)
Page 2854 :
Stage, , Description, , N2, , Multiple regional lymph node metastasis in the true pelvis (hypogastric, obturator, external, iliac, or presacral lymph node metastasis), , N3, , Lymph node metastasis to the common iliac lymph nodes, , M0, , No distant metastasis, , M1, , Distant disease, , Presentation, Most patients (85%) will present with painless, macroscopic haematuria. In those patients with, incidental microscopic haematuria, up to 10% of females aged over 50 will be found to have a, malignancy (once infection excluded)., Staging, Most will undergo a cystoscopy and biopsies or TURBT, this provides histological diagnosis and, information relating to depth of invasion. Locoregional spread is best determined using pelvic MRI, and distant disease CT scanning. Nodes of uncertain significance may be investigated using PET, CT., Treatment, Those with superficial lesions may be managed using TURBT in isolation. Those with recurrences or, higher grade/ risk on histology may be offered intravesical chemotherapy. Those with T2 disease are, usually offered either surgery (radical cystectomy and ileal conduit) or radical radiotherapy., Prognosis, , T1, , 90%, , T2, , 60%, , T3, , 35%, , T4a, , 10-25%, , Any T, N1-N2, , 30%
Page 2855 :
Theme: Urinary incontinence, , A., B., C., D., E., F., G., H., , Bladder diary for 3 days, Urodynamic studies, Bladder drill training for 6 weeks, Pelvic floor exercises for 3 months, Oxybutynin, IV urography, Dyes studies including phenazopyridine, None of the above, , Choose the best management option for each clinical scenario. Each option may be used once,, more than once or not at all., , 78., , A 75 year old lady reports urinary incontinence when coughing and sneezing. She has had, 2 children with no complications. She has no significant past medical history and is on no, medications. What is the most appropriate initial management?, You answered Bladder diary for 3 days, The correct answer is Pelvic floor exercises for 3 months, A diagnosis of stress incontinence is obvious from the history, therefore there is no need, for a bladder diary or urodynamic studies., Pelvic floor exercises would be the first line management., , 79., , A 26 year old pregnant woman is having her 1st child and has never had problems with, incontinence., You answered Bladder diary for 3 days, The correct answer is Pelvic floor exercises for 3 months, Pregnant women should receive instructions as to how to perform pelvic floor exercises, during pregnancy as this may help to decrease subsequent risk of stress urinary, incontinence., , 80., , A 67 year old lady reports urinary incontinence. She describes the sensation of needing to, pass urine immediately. She has had 2 children and is on no medications. What is the most, appropriate initial management?, Bladder diary for 3 days
Page 2856 :
The patient appears to be describing urge incontinence. A bladder diary is needed to, establish the baseline frequency of micturition and amounts of urine passed. Then bladder, training can be initiated to increase the volume of urine passed at reduced frequencies., Please rate this question:, , Discuss and give feedback, , Next question, , Urinary incontinence, Involuntary passage of urine. Most cases are female (80%). It has a prevalence of 11% in those, aged greater than 65 years. The commonest variants include:, , , , , Stress urinary incontinence (50%), Urge incontinence (15%), Mixed (35%), , Males, Males may also suffer from incontinence although it is a much rarer condition in men. A number of, anatomical factors contribute to this. Males have 2 powerful sphincters; one at the bladder neck and, the other in the urethra. Damage to the bladder neck mechanism is a factor in causing retrograde, ejaculation following prostatectomy. The short segment of urethra passing through the urogenital, diaphragm consists of striated muscle fibres (the external urethral sphincter) and smooth muscle, capable of more sustained contraction. It is the latter mechanism that maintains continence following, prostatectomy., Females, The sphincter complex at the level of bladder neck is poorly developed in females. As a result the, external sphincter complex is functionally more important, its composition being similar to that of, males. Innervation is via the pudendal nerve and the neuropathy that may accompany obstetric, events may compromise this and lead to stress urinary incontinence., Innervation, Somatic innervation to the bladder is via the pudendal, hypogastric and pelvic nerves. Autonomic, nerves travel in these nerve fibres too. Bladder filling leads to detrusor relaxation (sympathetic), coupled with sphincter contraction. The parasympathetic system causes detrusor contraction and, sphincter relaxation. Overall control of micturition is centrally mediated via centres in the Pons., Stress urinary incontinence, , , , , 50% of cases, especially in females., Damage (often obstetric) to the supporting structures surrounding the bladder may lead to, urethral hypermobility., Other cases due to sphincter dysfunction, usually from neurological disorders (e.g. Pudendal, neuropathy, multiple sclerosis).
Page 2857 :
Urethral mobility:, Pressure not transmitted appropriately to the urethra resulting in involuntary passage of urine during, episodes of raised intra-abdominal pressure., Sphincter dysfunction:, Sphincter fails to adapt to compress urethra resulting in involuntary passage of urine. When the, sphincter completely fails there is often to continuous passage of urine., Urge incontinence, In these patients there is sense of urgency followed by incontinence. The detrusor muscle in these, patients is unstable and urodynamic investigation will demonstrate overactivity of the detrusor, muscle at inappropriate times (e.g. Bladder filling). Urgency may be seen in patients with overt, neurological disorders and those without. The pathophysiology is not well understood but poor, central and peripheral co-ordination of the events surrounding bladder filling are the main, processes., Assessment, Careful history and examination including vaginal examination for cystocele., Bladder diary for at least 3 days, Consider flow cystometry if unclear symptomatology or surgery considered and diagnosis is unclear., Exclusion of other organic disease (e.g. Stones, UTI, Cancer), Management, Conservative measures should be tried first; Stress urinary incontinence or mixed symptoms should, undergo 3 months of pelvic floor exercise. Over active bladder should have 6 weeks of bladder, retraining., Drug therapy for women with overactive bladder should be offered oxybutynin (or solifenacin if, elderly) if conservative measures fail., In women with detrusor instability who fail non operative therapy a trial of sacral neuromodulation, may be considered, with conversion to permanent implant if good response. Augmentation, cystoplasty is an alternative but will involve long term intermittent self catheterisation., In women with stress urinary incontinence a urethral sling type procedure may be undertaken., Where cystocele is present in association with incontinence it should be repaired particularly if it lies, at the introitus., NICE guidelines, , , , , , , , , Initial assessment urinary incontinence should be classified as stress/urge/mixed., At least 3/7 bladder diary if unable to classify easily., Start conservative treatment before urodynamic studies if a diagnosis is obvious from the, history, Urodynamic studies if plans for surgery., Stress incontinence: Pelvic floor exercises 3/12, if fails consider surgery., Urge incontinence: Bladder training >6/52, if fails for oxybutynin (antimuscarinic drugs) then, sacral nerve stimulation., Pelvic floor exercises offered to all women in their 1st pregnancy., Next question
Page 2858 :
A 47-year-old woman presents with loin pain and haematuria. Urine dipstick demonstrates:, Blood, , ++++, , Nitrites, , POS, , Leucocytes, , +++, , Protein, , ++, , Urine culture shows a Proteus infection. An x-ray demonstrates a stag-horn calculus in the left renal, pelvis. What is the most likely composition of the renal stone?, , Xanthine, , Calcium oxalate, , Struvite, , Cystine, , Urate, Stag-horn calculi are composed of struvite and form in alkaline urine (ammonia producing bacteria, therefore predispose), Renal stones on x-ray, , , , cystine stones: semi-opaque, urate + xanthine stones: radio-lucent, , Please rate this question:, , Discuss and give feedback, , Renal stones: imaging, The table below summarises the appearance of different types of renal stone on x-ray
Page 2859 :
Type, , Frequency, , Radiograph appearance, , Calcium oxalate, , 40%, , Opaque, , Mixed calcium oxalate/phosphate stones, , 25%, , Opaque, , Triple phosphate stones*, , 10%, , Opaque, , Calcium phosphate, , 10%, , Opaque, , Urate stones, , 5-10%, , Radio-lucent, , Cystine stones, , 1%, , Semi-opaque, 'ground-glass' appearance, , Xanthine stones, , <1%, , Radio-lucent, , *stag-horn calculi involve the renal pelvis and extend into at least 2 calyces. They develop in alkaline, urine and are composed of struvite (ammonium magnesium phosphate, triple phosphate)., Ureaplasma urealyticum and Proteus infections predispose to their formation
Page 2861 :
Theme: Amputations, , A., B., C., D., E., F., G., H., , Transfemoral amputation, Gritti - Stokes amputation, Digital amputation, Syme's amputation, Hindquarter amputation, Below knee amputation, Trans metatarsal amputation, Amputation of digit, , Please select the most appropriate procedure for the scenario given. Each option may be used, once, more than once or not at all., , 1., , The operation of choice for a 90 year old lady with infected gangrene of the mid foot, secondary to diabetes. She has fixed flexion deformity of the knee., Transfemoral amputation, An elderly patient with diabetes and peripheral vascular disease is a high risk surgical, candidate. It is important that the chances of a successful outcome are maximised at the first, operation. SInce above knee amputations usually heal more reliably than below knee, amputations this is a preferable option, especially since she has a fixed deformity., , 2., , An operation in which Skew flaps are created., You answered Transfemoral amputation, The correct answer is Below knee amputation, This is one variant of a below knee amputation. The Burgess flap is the other commonly, practised approach., , 3., , An amputation of the lower limb in which the femoral condyles are removed and the patella, retained., You answered Transfemoral amputation, The correct answer is Gritti - Stokes amputation, This is a Gritti - Stokes amputation. During a Gritti - Stokes operation the patella is, conserved and swung posteriorly to cover the distal femoral surface.
Page 2862 :
Beware performing amputations in patients with peripheral vascular disease without optimising, inflow first!, Please rate this question:, , Discuss and give feedback, , Next question, , Amputations, Amputations are indicated when the affected limb is one of the following:, , , , , Dead non viable, Deadly where it is posing a major threat to life, Dead useless where it is viable but a prosthesis would be preferable, , Orthopaedic surgery, , , , Amputation is often undertaken as an option of last resort e.g. Limb salvage has failed and, the limb is so non functional that mobility needs would be best met with prosthesis., Chronic fracture non union or significant limb shortening following trauma would fit into this, category. Occasionally following major trauma a primary amputation is preferable. This, would be the case in an open fracture with major distal neurovascular compromise and other, more life threatening injuries are present., , Vascular surgery, , , , , , The first two categories are the most prevalent., Diabetic foot sepsis is often a major cause of sepsis which can spread rapidly in the, presence of established peripheral vascular disease., As a general rule the main issue in vascular surgery is to optimise vascular inflow prior to, surgery. The more distal the planned amputation is to be, the more important this rule, becomes., In other situations there has been something such as an embolic event that has not been, revascularised in time. In this case the limb shows fixed mottling and an amputation will be, needed., , Types of amputations, As the vast majority of commonly performed amputations affect the lower limbs these will be covered, here., The main categories of amputations are:
Page 2863 :
, , , , , , , Pelvic disarticulation (hindquarter), Above knee amputation, Gritti Stokes (through knee amputation), Below knee amputation (using either Skew or Burgess flaps), Syme's amputation (through ankle), Amputations of mid foot and digits, , Choosing a level of amputation depends on:, , , , , The disease process being treated, Desired functional outcome, Co-morbidities of the patient, , Above knee amputations, , , , , , , Quick to perform, Heal reliably, Patients regain their general health quickly, For this benefit, a functional price has to be paid and many patients over the age of 70 will, never walk on an above knee prosthesis., Above knee amputations use equal anterior-posterior flaps, , Below knee amputations, , , , , , Technically more challenging to perform, Heal less reliably than their above knee counterparts., However, many more patients are able to walk using a below knee prosthesis., In below knee amputations the two main flaps are Skew flaps or the Burgess long posterior, flap. Skew flaps result in a less bulky limb that is easier to attach a prosthesis to., , It is worth remembering that whilst it may be technically feasible to offer a below knee amputation, there may be circumstances where an above knee option is preferable. For example, in fixed flexion, deformities of the lower limb, little functional benefit would be gained from below knee amputation, surgery., Next question
Page 2864 :
Theme: Acute limb ischaemia, , A., B., C., D., E., F., G., H., , Primary amputation, Transfemoral embolectomy with prophylactic fasciotomy, Transpopliteal embolectomy without prophylactic fasciotomy, Transfemoral embolectomy without prophylactic fasciotomy, Transpopliteal embolectomy with prophylactic fasciotomy, Angiogram, Systemic heparin infusion, Peripheral thrombolysis, , Please select the most appropriate management for the following patients presenting with acutely, ischaemic limbs. Each option may be used once, more than once or not at all., , 4., , A 76 year old man presents with a painful left leg. The pain began suddenly and with no, previous history. On examination he has a white left leg with no palpable femoral pulse and, loss of sensation. The pulses in the contra lateral limb are normal. It is now three hours, since the pain first started., You answered Primary amputation, The correct answer is Transfemoral embolectomy without prophylactic fasciotomy, A limb which is acutely ischaemic and with normal contralateral pulses normally indicates, an acute embolus. Whilst intra arterial thrombolysis may be an option there is a reasonable, argument for immediate surgery. A fasciotomy is unlikely to be required., , 5., , A 56 year old man presents with a painful left leg. The pain has been present for the past 8, hours although it has also been present (though less severe) about a week ago. At that stage, he noted that his hallux had turned blue. This resolved spontaneously. On examination he, has a weakly palpable femoral pulse on the affected side but no pulses palpable distal to, this. His sensation is mildly impaired., You answered Primary amputation, The correct answer is Angiogram, The history favors a more chronic process and the great toe cyanotic spell may be indicative, of previous embolism from pathology such as an aneurysm. In the ideal scenario a duplex, scan would be performed. However, an angiogram would probably supply sufficient, information and allow appropriate endovascular therapy., , 6., , A 78 year old lady is found by carers with a severely painful left leg. On examination she, has no palpable pulses and the limb is cold, insensate and mottled. The mottling does not
Page 2865 :
blanch with pressure., Primary amputation, This is an unsalvagable limb and is best amputated primarily., Please rate this question:, , Discuss and give feedback, , Next question, , Acute limb ischaemia, , , , , Thrombosis of a pre-existing site of atherosclerosis if the commonest cause of acute limb, ischaemia, Acute thrombosis of popliteal aneurysms poses the greatest threat to the limb, Sudden occlusion of a large proximal vessel results in the typical appearances of acute limb, ischaemia, , Clinical appearances, , , , , Less than 6 hours = White leg, At 6 -12 hours = Mottled limb with blanching on pressure, More than 12-24 hours = Fixed mottling, , Management of acutely ischaemic leg, , Clinical picture, , Treatment, , White leg with sensorimotor deficit, , Surgery and embolectomy, , Dusky leg, mild anaesthesia, , Angiography, , Fixed mottling, , Primary amputation, , Role of thrombolysis, , , Intra arterial thrombolysis is better than peripheral thrombolysis
Page 2866 :
, , , , Mainly indicated in acute on chronic thrombosis, Avoid if within 2 months of CVA or 2 weeks of surgery, Aspiration of clot may improve success rate if the thrombosis is large, , Surgery, , , , , , , , Both groins should be prepared, Transverse arteriotomy is easier to close, Poor inflow should be managed with iliac trawl- if this fails to improve then consider a, femoro-femoral cross over or axillo-femoral cross over., A check angiogram should be performed on table and prior to closure, Systemic heparinisation should follow surgery, Fasciotomy should be considered if the time between onset and surgery exceeds 6 hours, Next question
Page 2867 :
Theme: Vascular disorders affecting the upper limb, , A., B., C., D., E., F., G., , Proximal brachial artery occlusion secondary to atheroma, Distal brachial artery occlusion secondary to atheroma, Axillary artery embolus, Axillary vein thrombosis, Cervical rib, Raynaud's disease, Rheumatoid disease, , Please select the most likely cause for the presenting scenario described. Each option may be used, once, more than once or not at all., , 7., , A 73 year old male presents with a collapse and is brought to the emergency department., On examination he has a cold, painful left hand and forearm., You answered Proximal brachial artery occlusion secondary to atheroma, The correct answer is Axillary artery embolus, Theme from September 2012 Exam, Sudden arterial embolus will affect the axillary artery in up to 30% cases. Because of the, acute nature of the condition there is no time for the development of a collateral circulation, so the limb is usually pale and painful. Emboli occur usually occur as a result of atrial, fibrillation. Fast atrial fibrillation can cause syncope and an acute embolus., , 8., , A 23 year old man presents with intermittent symptoms of altered sensation in his arm and, discomfort when he uses his hands. He works as an electrician and his symptoms are worst, when he is fitting light fixtures., You answered Proximal brachial artery occlusion secondary to atheroma, The correct answer is Cervical rib, Compression of the thoracic outlet by the fibrous band of the "rib" can result in both, neurological and circulatory compromise. When manual tasks are performed in which the, hand works overhead the signs and symptoms will be maximal and this is the basis of, Adsons test., , 9., , A 19 year old lady presents with recurrent episodes of pain in her hands. She notices that, her symptoms are worst in cold weather. When she gets the pain she notices that her hands, are very pale, they then become dark blue in colour.
Page 2868 :
You answered Proximal brachial artery occlusion secondary to atheroma, The correct answer is Raynaud's disease, Raynauds disease is characterised by a series of colour changes and discomfort is often, present. The young age at presentation coupled with the absence of a smoking history (in, most cases) makes occlusive disease unlikely., Please rate this question:, , Discuss and give feedback, , Next question, , Vascular disorders of the upper limb, Upper limb arterial disease is less common than lesions causing symptoms in the lower limb. The, upper limb circulation may be affected by embolic events, stenotic lesions (both internal and, extrinsic), inflammatory disorders and venous diseases., The anatomy of the collateral circulation of the arterial inflow may impact on the history and nature of, disease presentation. In the region of the subclavian and axillary arteries the collateral vessels, passing around the shoulder joint may provide pathways for flow if the main vessels are stenotic or, occluded. During periods of increased metabolic demand the collateral flow is not sufficient and the, vertebral arteries may have diminished flow. This may result in diminished flow to the brain with, neurological sequelae such as syncope., Vascular disease of the upper limb, , Condition, , Axillary/, brachial, embolus, , Features, , , , , , , Arterial, occlusions, , , , , , 50% of upper limb emboli will lodge in the brachial artery, 30% of upper limb emboli will lodge in the axillary artery, Sudden onset of symptoms; pain, pallor, paresis, pulselessness,, paraesthesia, Sources are left atrium with cardiac arrhythmia (mainly AF), mural, thrombus, Cardiac arrhythmias may result in impaired consciousness in addition to, the embolus, Those resulting from atheroma are the most common, trauma may result, in vascular changes and long term occlusion but this is rare, Features may include claudication, ulceration and gangrene. Proximally, sited lesions may result in subclavian steal syndrome, The progressive nature of the disease allows development of collaterals,
Page 2869 :
acute ischaemia may occur as a result of acute thrombosis, Raynaud's, disease, , , , , , , Idiopathic condition affecting young females, Usually affects hands > feet, Digits become: white →blue →red, Treatment is with calcium antagonists, , Upper limb, venous, thrombosis, , , , , , Gradual onset of upper limb swelling and discomfort., Sensation and motor function are normal, Condition may complicate pre-existing malignancy (especially breast, cancer) or arise as a result of repetitive use of the limb in a task such as, painting a ceiling, The condition is diagnosed with duplex ultrasound and treatment is with, anticoagulation, , , , Cervical rib, , , , , , , , , , 0.2-0.4% incidence, Consist of an anomalous fibrous band that often originates from C7 and, may arc towards, but rarely reaches the sternum, Congenital cases may present around the third decade, some cases are, reported to occur following trauma, Bilateral in up to 70%, Compression of the subclavian artery may produce absent radial pulse on, clinical examination and in particular may result in a positive Adsons test, (lateral flexion of the neck away from symptomatic side and traction of, the symptomatic arm- leads to obliteration of radial pulse), Treatment is most commonly undertaken when there is evidence of, neurovascular compromise. A transaxillary approach is the traditional, operative method for excision, Next question
Page 2870 :
Theme: Management of occlusive vascular disease, , A., B., C., D., E., F., , Aorto-bifemoral bypass graft, Femoro-femoral cross over graft, Femoro-popliteal bypass graft, Femoro-distal bypass graft, Axillo-bifemoral bypass graft, Bilateral above knee amputation, , Please select the most appropriate arterial bypass method for the scenario described. Each option, may be used once, more than once or not at all., , 10., , An 83 year old lady with a significant cardiac history is admitted with rest pain and, bilateral leg ulcers. Imaging demonstrates bilateral occlusion of both common iliac arteries, that are unsuitable for stenting., You answered Aorto-bifemoral bypass graft, The correct answer is Axillo-bifemoral bypass graft, Theme from January 2012 Exam, In patients with major cardiac co-morbidities the safest option is to choose an axillobifemoral bypass graft. The long term patency rates are less good than with aortobifemoral bypass grafts, however, the operation is less major., , 11., , A 54 year old man presents to the vascular clinic with severe rest pain and an ulcer on his, right foot that is not healing. On examination he has bilateral absent femoral pulses., Imaging demonstrates a bilateral occlusion of the common iliac arteries that is not suitable, for stenting., Aorto-bifemoral bypass graft, In a young patient consideration should be given to aorto-bifemoral bypass grafts as these, have the best long term functional outcome compared with an axillo-bifemoral bypass, graft., , 12., , A 78 year old man presents with left sided rest pain in his leg and a non healing arterial leg, ulcer on the same leg. Imaging shows normal right leg vessels, on the left side there is a, long occlusion of the external iliac artery that is unsuitable for stenting. He has a, significant cardiac history., You answered Aorto-bifemoral bypass graft
Page 2871 :
The correct answer is Femoro-femoral cross over graft, Femoro-femoral cross over grafts are an option for treatment of iliac occlusions in patients, with significant co-morbidities and healthy contralateral vessels. In reality the idealised, situation presented here seldom applies and the opposite vessels usually have some disease, and one must be careful not to damage the "healthy" side., Please rate this question:, , Discuss and give feedback, , Next question, , Peripheral vascular disease, Indications for surgery to revascularise the lower limb, , , , , , Intermittent claudication, Critical ischaemia, Ulceration, Gangrene, , Intermittent claudication that is not disabling may provide a relative indication, whilst the other, complaints are often absolute indications depending upon the frailty of the patient., Assessment, , , , , , Clinical examination, Ankle brachial pressure index measurement, Duplex arterial ultrasound, Angiography (standard, CT or MRI): usually performed only if intervention being considered., , Angioplasty, In order for angioplasty to be undertaken successfully the artery has to be accessible. The lesion, relatively short and reasonable distal vessel runoff. Longer lesions may be amenable to sub-intimal, angioplasty., Surgery, Surgery will be undertaken where attempts at angioplasty have either failed or are unsuitable., Bypass essentially involves bypassing the affected arterial segment by utilising a graft to run from, above the disease to below the disease. As with angioplasty good runoff improves the outcome., Some key concepts with bypass surgery, Superficial femoral artery occlusion to the above knee popliteal
Page 2872 :
In the ideal scenario, vein (either in situ or reversed LSV) would the used as a conduit. However,, prosthetic material has reasonable 5 year patency rates and some would advocate using this in, preference to vein so that vein can be used for other procedures in the future. In general terms either, technique is usually associated with an excellent outcome (if run off satisfactory)., Procedure, , , , , , , Artery dissected out, IV heparin 3,000 units given and then the vessels are cross clamped, Longitudinal arteriotomy, Graft cut to size and tunneled to arteriotomy sites, Anastomosis to femoral artery usually with 5/0 'double ended' Prolene suture, Distal anastomosis usually using 6/0 'double ended' Prolene, , Distal disease, , , , , Femoro-distal bypass surgery takes longer to perform, is more technically challenging and, has higher failure rates., In elderly diabetic patients with poor runoff a primary amputation may well be a safer and, more effective option. There is no point in embarking on this type of surgery in patients who, are wheelchair bound., In femorodistal bypasses vein gives superior outcomes to PTFE., , Rules, , , , , , Vein mapping 1st to see whether there is suitable vein (the preferred conduit). Sub intimal, hyperplasia occurs early when PTFE is used for the distal anastomosis and will lead to early, graft occlusion and failure., Essential operative procedure as for above knee fem-pop., If there is insufficient vein for the entire conduit then vein can be attached to the end of the, PTFE graft and then used for the distal anastomosis. This type of 'vein boot' is technically, referred to as a Miller Cuff and is associated with better patency rates than PTFE alone., Remember the more distal the arterial anastomosis the lower the success rate., , References, Peach G et al. Diagnosis and management of peripheral arterial disease. BMJ 2012; 345: 36-41., Next question
Page 2873 :
Theme: Causes of arterial occlusion, , A., B., C., D., E., F., G., , Vasculitis, Steal syndrome, Thrombosis, Foreign body embolus, Clot embolus, Vasospasm, Direct arterial injury, , Please select the most likely underlying cause for the scenario provided. Each option may be used, once, more than once or not at all., , 13., , A 73 year old lady develops a cold, pulseless hand 3 days following a myocardial, infarction., You answered Vasculitis, The correct answer is Clot embolus, The development of mural or atrial appendage thrombi may occur following a myocardial, infarct and co-existing atrial fibrillation may contribute to the formation. They tend to, present with classical features of an embolic event., , 14., , A 6 year old child has suffered a displaced supracondylar humeral fracture. On, examination they have a cold and insensate hand with absent pulses., You answered Vasculitis, The correct answer is Direct arterial injury, Both vasospasm and arterial injury may complicate supracondylar fractures and are seen in, 1% of all cases. Vasospasm is usually transient and more likely when the injury is minor, and reduced early. Severely displaced injuries and those with more advanced signs are, usually associated with direct arterial injury., , 15., , A 26 year old man who smokes heavily develops aching, crampy pains in his legs. On, examination distal limb pulses are diminished., Vasculitis, This is likely to represent Buergers disease. It is commonest in young males who smoke, heavily.
Page 2874 :
Please rate this question:, , Discuss and give feedback, , Next question, , Arterial occlusions/ insufficiency, Arterial occlusions may occur as a result of a number of processes. The typical clinical scenarios are, outlined below., , Cause of, occlusion, , Typical picture, , Embolus, , Sudden onset, Depending upon level of occlusion; limb may show typical features of pain, loss, of pulses and pallor. Sensory perceptive changes may also be present, , Thrombosis, , Usually known disease and prodromal symptoms e.g. claudication, Disruption to flow may be incomplete, If background disease process present then collaterals may be present and, picture less dramatic, , Vasospasm, , May be due to Raynauds and affect extremities, Symptoms are often temperature related, Discolouration of the hands may occur (pale, dark, red), Symptoms improve during pregnancy (hyperdynamic circulation), , Steal, syndromes, , Occur secondary to arteriovenous fistula, or partial arterial occlusions (e.g., cervical rib), Pain and diminished pulses distal to fistula are seen, , Vasculitis, Vessel diameter and vasculitis classification, , Aorta and branches, , , , , , Takayasu's arteritis, Buergers disease, Giant cell arteritis
Page 2875 :
Large and medium sized arteries, , , , , , Buergers disease, Giant cell arteritis, Polyarteritis nodosa, , Medium sized muscular arteries, , , , , Polyarteritis nodosa, Wegeners granulomatosis, , Small muscular arteries, , , , , Wegeners granulomatosis, Rheumatoid vasculitis, , Specific conditions, , Takyasu's arteritis, , , , , , , , Inflammatory, obliterative arteritis affecting aorta and branches, Females> Males, Symptoms may include upper limb claudication, Clinical findings include diminished or absent pulses, ESR often affected during the acute phase, , Buergers disease, , , , Segmental thrombotic occlusions of the small and medium sized, lower limb vessels, Commonest in young male smokers, Proximal pulses usually present, but pedal pulses are lost, An acuter hypercellular occlusive thrombus is often present, Tortuous corkscrew shaped collateral vessels may be seen on, angiography, , , , , , , Giant cell arteritis, , , , , , , Polyarteritis nodosa, , , , , , , Systemic granulomatous arteritis that usually affects large and, medium sized vessels, Females > Males, Temporal arteritis is commonest type, Granulomatous lesions may be seen on biopsy (although up to, 50% are normal), Systemic necrotising vasculitis affecting small and medium sized, muscular arteries, Most common in populations with high prevalence of hepatitis B, Renal disease is seen in 70% cases, Angiography may show saccular or fusiform aneurysms and, arterial stenoses
Page 2877 :
Theme: Ankle brachial pressure index, , A., B., C., D., E., , >1.2, 1.0, 0.8, 0.5, 0.3, , Please select the ankle brachial pressure index that is most likely to be present for the scenario, given. Each value may be used once, more than once or not at all., , 16., , A 73 year old lifelong heavy smoker presents to the vascular clinic with symptoms of foot, ulceration and rest pain. On examination her foot has areas of gangrene and pulses are, impalpable., You answered >1.2, The correct answer is 0.3, This is critical limb ischaemia. Values of 0.3 are typical in this setting and urgent further, imaging is needed. Debridement of necrosis prior to improving arterial inflow carries a, high risk of limb loss., , 17., , A 63 year old man presents with a claudication distance of 15 yards. He is a lifelong heavy, smoker. On examination his foot is hyperaemic and there is a small ulcer at the tip of his, great toe., You answered >1.2, The correct answer is 0.5, Hyperaemia may occur in association with severe vascular disease and is referred to, surgically as a "sunset foot". ABPI is usually higher than 0.3, but seldom greater than 0.5., Especially when associated with hyperaemic changes and ulceration. Urgent further, imaging and risk factor modification is needed., , 18., , A 77 year old morbidly obese man with type 2 diabetes presents with leg pain at rest. His, symptoms are worst at night and sometimes improve during the day. He has no areas of, ulceration., >1.2, Type 2 diabetics may have vessel calcification. This will result in abnormally high ABPI
Page 2878 :
readings. Pain of this nature in diabetics is usually neuropathic and if a duplex scan is, normal then treatment with an agent such as duloxetine is sometimes helpful., Theme from September 2011 and September 2012 exam, Please rate this question:, , Discuss and give feedback, , Next question, , Ankle-Brachial pressure index, , , , Measurement of ankle- brachial pressure index (ABPI) is a commonly performed vascular, investigation., Calculated by dividing lower limb pressure by the highest upper limb pressure., , Results of ABPI, 1.2 or greater, , Usually due to vessel calcification, , 1.0- 1.2, , Normal, , 0.8-1.0, , Minor stenotic lesion, Initiate risk factor management, , 0.50-0.8, , Moderate stenotic lesion, Consider duplex, Risk factor management, If mixed ulcers present then avoid tight compression bandages, , 0.5- 0.3, , Likely significant stenosis, Duplex scanning to delineate lesions needed, Compression bandaging contra indicated, , Less than 0.3, , Indicative of critical ischaemia, Urgent detailed imaging required, , Next question
Page 2879 :
A 67 year old patient is due to undergo a femoro-popliteal bypass graft. Which heparin regime, should the surgeon ask for prior to cross clamping the femoral artery?, , Single therapeutic dose of low molecular weight heparin on the ward prior to coming to, theatre, Single therapeutic dose of low molecular weight heparin the night before surgery, , Dose of 10,000 units of unfractionated heparin prior to induction of anaesthesia, , Dose of 3,000 units of unfractionated heparin, 3 minutes prior to cross clamping, , Dose of 30,000 units of unfractionated heparin, 3 minutes prior to cross clamping, , As a rule most vascular surgeons will administer approximately 3,000 units of systemic heparin 3-5, minutes prior to cross clamping to help prevent further intra arterial thromboses. A dose of 30,000, units is given prior to going on cardiopulmonary bypass. Heparin given at induction will cause, bleeding during routine dissection., Please rate this question:, , Discuss and give feedback, , Next question, , Heparin, , , Causes the formation of complexes between antithrombin and activated thrombin/factors, 7,9,10,11 & 12, , Advantages of low molecular weight heparin, , , , , , , Better bioavailability, Lower risk of bleeding, Longer half life, Little effect on APTT at prophylactic dosages, Less risk of HIT, , Complications
Page 2880 :
, , , , , Bleeding, Osteoporosis, Heparin induced thrombocytopenia (HIT): occurs 5-14 days after 1st exposure, Anaphylaxis, , In surgical patients that may need a rapid return to theatre, administration of unfractionated heparin, is preferred; as low molecular weight heparins have a longer duration of action and are harder to, reverse., Next question
Page 2881 :
An 18 year old lady presents with extensive varicose veins of her left leg. There is associated port, wine staining. What is the most likely diagnosis?, , Type 1 diabetes, , Osler syndrome, , Gardner's syndrome, , Proteus syndrome, , Klippel-Trenaunay-Weber syndrome, , A less common cause of venous insufficiency is Klippel-Trenaunay-Weber (KTW) syndrome, which, involves port-wine stains, varicose veins, and bony or soft-tissue hypertrophy., Please rate this question:, , Discuss and give feedback, , Next question, , Lower leg ulcers, Venous leg ulcers, , , , , , , , , , Most due to venous hypertension, secondary to chronic venous insufficiency (other causes, include calf pump dysfunction or neuromuscular disorders), Ulcers form due to capillary fibrin cuff or leucocyte sequestration, Features of venous insufficiency include oedema, brown pigmentation, lipodermatosclerosis,, eczema, Location above the ankle, painless, Deep venous insufficiency is related to previous DVT and superficial venous insufficiency is, associated with varicose veins, Doppler ultrasound looks for presence of reflux and duplex ultrasound looks at the anatomy/, flow of the vein, Management: 4 layer compression banding after exclusion of arterial disease or surgery, If fail to heal after 12 weeks or >10cm 2 skin grafting may be needed, , Marjolin's ulcer
Page 2882 :
Image sourced from Wikipedia, , , , , , Squamous cell carcinoma, Occurring at sites of chronic inflammation e.g; burns, osteomyelitis after 10-20 years, Mainly occur on the lower limb, , Arterial ulcers, , , , , , , Occur on the toes and heel, Painful, There may be areas of gangrene, Cold with no palpable pulses, Low ABPI measurements, , Neuropathic ulcers, , , , , , Commonly over plantar surface of metatarsal head and plantar surface of hallux, The plantar neuropathic ulcer is the condition that most commonly leads to amputation in, diabetic patients, Due to pressure, Management includes cushioned shoes to reduce callous formation, , Pyoderma gangrenosum
Page 2883 :
Image sourced from Wikipedia, , , , , , Associated with inflammatory bowel disease/RA, Can occur at stoma sites, Erythematous nodules or pustules which ulcerate, Next question
Page 2884 :
Theme: Management of peripheral arterial disease, , A., B., C., D., E., F., G., , Primary amputation, Angioplasty, Arterial bypass surgery using vein, Arterial bypass surgery using PTFE, Conservative management with medical therapy and exercise, Watch and wait, Duplex scanning, , Please select the most appropriate management for the scenario given. Each option may be used, once, more than once or not at all., , 21., , A 63 year old man is admitted with rest pain and foot ulceration. An angiogram shows a 3, cm area of occlusion of the distal superficial femoral artery with 3 vessel run off. His ankle, - brachial pressure index is 0.4., You answered Primary amputation, The correct answer is Angioplasty, Short segment disease and good run off with tissue loss is a compelling indication for, angioplasty. He should receive aspirin and a statin if not already taking them., , 22., , A 72 year old man present in the vascular clinic with calf pain present on walking 100, yards. He is an ex-smoker and lives alone. On examination he has reasonable leg pulses., His right dorsalis pedis pulse gives a monophasic doppler signal with an ankle brachial, pressure index measurement of 0.7. All other pressures are acceptable. There is no, evidence of ulceration or gangrene., You answered Primary amputation, The correct answer is Conservative management with medical therapy and exercise, Structured exercise programmes combined with medical therapy will improve many, patients. Should his symptoms worsen or fail to improve then imaging with duplex, scanning would be required., , 23., , An 83 year old lady is admitted from a nursing home with infected lower leg ulcers. She, underwent an attempted long superficial femoral artery sub initimal angioplasty 2 weeks, previously. This demonstrated poor runoff below the knee., Primary amputation
Page 2885 :
Poor runoff and sepsis would equate to poor outcome with attempted bypass surgery., Please rate this question:, , Discuss and give feedback, , Next question, , Peripheral vascular disease, Indications for surgery to revascularise the lower limb, , , , , , Intermittent claudication, Critical ischaemia, Ulceration, Gangrene, , Intermittent claudication that is not disabling may provide a relative indication, whilst the other, complaints are often absolute indications depending upon the frailty of the patient., Assessment, , , , , , Clinical examination, Ankle brachial pressure index measurement, Duplex arterial ultrasound, Angiography (standard, CT or MRI): usually performed only if intervention being considered., , Angioplasty, In order for angioplasty to be undertaken successfully the artery has to be accessible. The lesion, relatively short and reasonable distal vessel runoff. Longer lesions may be amenable to sub-intimal, angioplasty., Surgery, Surgery will be undertaken where attempts at angioplasty have either failed or are unsuitable., Bypass essentially involves bypassing the affected arterial segment by utilising a graft to run from, above the disease to below the disease. As with angioplasty good runoff improves the outcome., Some key concepts with bypass surgery, Superficial femoral artery occlusion to the above knee popliteal, In the ideal scenario, vein (either in situ or reversed LSV) would the used as a conduit. However,, prosthetic material has reasonable 5 year patency rates and some would advocate using this in, preference to vein so that vein can be used for other procedures in the future. In general terms either, technique is usually associated with an excellent outcome (if run off satisfactory).
Page 2886 :
Procedure, , , , , , , Artery dissected out, IV heparin 3,000 units given and then the vessels are cross clamped, Longitudinal arteriotomy, Graft cut to size and tunneled to arteriotomy sites, Anastomosis to femoral artery usually with 5/0 'double ended' Prolene suture, Distal anastomosis usually using 6/0 'double ended' Prolene, , Distal disease, , , , , Femoro-distal bypass surgery takes longer to perform, is more technically challenging and, has higher failure rates., In elderly diabetic patients with poor runoff a primary amputation may well be a safer and, more effective option. There is no point in embarking on this type of surgery in patients who, are wheelchair bound., In femorodistal bypasses vein gives superior outcomes to PTFE., , Rules, , , , , , Vein mapping 1st to see whether there is suitable vein (the preferred conduit). Sub intimal, hyperplasia occurs early when PTFE is used for the distal anastomosis and will lead to early, graft occlusion and failure., Essential operative procedure as for above knee fem-pop., If there is insufficient vein for the entire conduit then vein can be attached to the end of the, PTFE graft and then used for the distal anastomosis. This type of 'vein boot' is technically, referred to as a Miller Cuff and is associated with better patency rates than PTFE alone., Remember the more distal the arterial anastomosis the lower the success rate., , References, Peach G et al. Diagnosis and management of peripheral arterial disease. BMJ 2012; 345: 36-41., Next question
Page 2887 :
A 32 year old woman attends clinic for assessment of varicose veins. She has suffered for varicose, veins for many years and can trace their development back to when she suffered a complex tibial, fracture. On examination she has marked truncal varicosities with a long tortuous long saphenous, vein. What is the most appropriate next step?, , Arrange a venogram, , Arrange a venous duplex scan, , List her for a trendelenberg procedure, , List her for injection foam sclerotherapy, , List her for multiple avulsion phlebectomies, , This lady is likely to have deep venous incompetence as she will have been immobilised for her tibial, fracture and may well have had a DVT. A duplex scan is mandatory prior to any form of surgical, intervention. A venogram would provide similar information but is more invasive., Please rate this question:, , Discuss and give feedback, , Next question, , Chronic venous insufficiency and varicose veins, Wide spectrum of disease ranging from minor cosmetic problem through to ulceration and disability., It is commoner in women than men and is worse during pregnancy. Varicose veins are best, considered as being a saccular dilation of veins (WHO). Chronic venous insufficiency is a series of, tissue changes which occur in relation to pooling of blood in the extremities with associated venous, hypertension occurring as a result of incompetent deep vein valves., The veins of the lower limb consist of an interconnected network of superficial and deep venous, systems. Varices occur because of localised weakness in the vein wall resulting in dilatation and, reflux of blood due to non union of valve cusps. Histologically the typical changes include fibrous, scar tissue dividing smooth muscle within media in the vessel wall., Tissue damage in chronic venous insufficiency occurs because of perivascular cytokine leakage, resulting in localised tissue damage coupled with impaired lymphatic flow., Diagnosis, Typical symptoms of varicose veins include:
Page 2888 :
, , , , , , , Cosmetic appearance, Aching, Ankle swelling that worsens as the day progresses, Episodic thrombophlebitis, Bleeding, Itching, , Symptoms of chronic venous insufficiency include:, , , , , , Dependant leg pain, Prominent leg swelling, Oedema extending beyond the ankle, Venous stasis ulcers, , The typical venous stasis ulcer is:, , , , , , , Located above the medial malleolus, Indolent appearance with basal granulation tissue, Variable degree of scarring, Non ischaemic edges, Haemosiderin deposition in the gaiter area (and also lipodermatosclerosis)., , Differential diagnosis, , , , , , , Lower limb arterial disease, Marjolins ulcer, Claudication, Spinal stenosis, Swelling due to medical causes e.g. CCF., , Exclusion of these differentials is by means of physical examination and ankle brachial pressure, index measurement., Examination, , , , , Assess for dilated short saphenous vein (popliteal fossa) and palpate for saphena varix, medial to the femoral artery, Brodie-Trendelenburg test: to assess level of incompetence, Perthes' walking test: assess if deep venous system competent, , Investigation
Page 2889 :
, , , Doppler exam: if incompetent a biphasic signal due to retrograde flow is detected, Duplex scanning: to ensure patent deep venous system (do if DVT or trauma), , All patients should have a Doppler assessment to assess for venous reflux and should be classified, as having uncomplicated varicose veins or varicose veins with associated chronic venous, insufficiency. In the history establishing a previous thrombotic event (DVT/ lower limb fracture) is, important and patients with such a history and all who have evidence of chronic venous insufficiency, should have a duplex scan performed., Owing to litigation patients with saphenopopliteal incompetence should have a duplex scan, performed and the site marked by scan on the day of surgery., Treatment, Indications for surgery:, , , , , , Cosmetic: majority, Lipodermatosclerosis causing venous ulceration, Recurrent superficial thrombophlebitis, Bleeding from ruptured varix, , Condition, , Therapy, , Minor varicose veins no complications, , Reassure/ cosmetic therapy, , Symptomatic, uncomplicated varicose, veins, , In those without deep venous insufficiency options include; endothermal, ablation, foam sclerotherapy, saphenofemoral / popliteal disconnection,, stripping and avulsions, compression stockings, , Varicose veins with, skin changes, , Therapy as above (if compression minimum is formal class I stockings), , Chronic venous, insufficiency or ulcers, , Class 2-3 compression stockings (ensure no arterial disease)., , , , Application of formal compression stockings (usually class II/III). In patients who have, suffered ulceration, compression stockings should be worn long term. Where ulceration is
Page 2890 :
, , , present and established saphenofemoral reflux exists this should be addressed surgically for, durable relief of symptoms, either at the outset or following ulcer healing., Injection sclerotherapy (5% Ethanolamine oleate), foam is increasingly popular, though, transient blindness has been reported. Endo venous laser therapy is another minimally, invasive option, Sapheno-femoral or sapheno-popliteal ligation, in the case of the LSV; stripping and multiple, phlebectomies, , Current best practice guidance, In the United Kingdom the National Institute of Clinical Excellence guidance on varicose veins, suggests that for patients with symptomatic varicose veins the first line procedure of choice should, be endothermal ablation (see reference for more information). Where this is unavailable or, unsuitable then foam sclerotherapy should be the second line option. Surgery is currently the third, line treatment option., Trendelenburg procedure (sapheno-femoral junction ligation), , , , , , , Head tilt 15 degrees and legs abducted, Oblique incision 1cm medial from artery, Tributaries ligated (Superficial circumflex iliac vein, Superficial inferior epigastric vein,, Superficial and deep external pudendal vein), SF junction double ligated, Saphenous vein stripped to level of knee/upper calf. NB increased risk of saphenous, neuralgia if stripped more distally, , References, Marsden G et al. Diagnosis of management of varicose veins in the the legs: summary of NICE, guidance. BMJ 2013 (347): 30-31., Next question
Page 2891 :
Theme: Management of abdominal aortic aneurysms, , A., B., C., D., E., F., G., H., I., , Immediate laparotomy, Immediate CT, AAA repair during next 48 hours, USS in 6 months, CT scan during next 4 weeks, Endovascular aortic aneurysm repair, Discharge, Palliate, None of the above, , Please select the most appropriate management for the scenario given. Each option may be used, once, more than once or not at all., , 25., , A 66 year old man is referred via the aneurysm screening programme with an abdominal, aortic aneurysm measuring 4.4 cm. Apart from well controlled type 2 DM he is otherwise, well, You answered Immediate laparotomy, The correct answer is USS in 6 months, At this point continue with ultrasound surveillance, , 26., , A 72 year old man has a CT scan for abdominal discomfort and the surgeon suspects, AAA. This shows a 6.6cm aneurysm with a 3.5cm neck and it continues to involve the, right common iliac. The left iliac is occluded. He is hypertensive and has Type 2 DM, which is well controlled., You answered Immediate laparotomy, The correct answer is AAA repair during next 48 hours, Assuming he is fit enough. This would be a typical 'open ' case as the marked iliac disease, would make EVAR difficult, , 27., , An 89 year old man presents with hypotension and collapse and is found by the staff in the, toilet of his care home. He is moribund and unable to give a clear history. He had suffered, a cardiac arrest in the ambulance but has since been resuscitated and now has a Bp of 95, systolic. He has an obviously palpable AAA., You answered Immediate laparotomy
Page 2892 :
The correct answer is Palliate, He will not survive aortic surgery and whilst some may disagree, I would argue that taking, this case to theatre would be futile, Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal aorta aneurysm, , , , , Abdominal aortic aneurysms are a common problem in vascular surgery., They may occur as either true or false aneurysm. With the former all 3 layers of the arterial, wall are involved, in the latter only a single layer of fibrous tissue forms the aneurysm wall., True abdominal aortic aneurysms have an approximate incidence of 0.06 per 1000 people., They are commonest in elderly men and for this reason the UK is now introducing the, aneurysm screening program with the aim of performing an abdominal aortic ultrasound, measurement in all men aged 65 years., , Causes, , , , , Several different groups of patients suffer from aneurysmal disease., The commonest group is those who suffer from standard arterial disease, i.e. Those who, arehypertensive, have diabetes and have been or are smokers., Other patients such as those suffering from connective tissue diseases such as Marfan's, may also develop aneurysms. In patients with abdominal aortic aneurysms the extracellular, matrix becomes disrupted with a change in the balance of collagen and elastic fibres., , Management, , , , , , , , , Most abdominal aortic aneurysms are an incidental finding., Symptoms most often relate to rupture or impending rupture., 20% rupture anteriorly into the peritoneal cavity. Very poor prognosis., 80% rupture posteriorly into the retroperitoneal space, The risk of rupture is related to aneurysm size, only 2% of aneurysms measuring less than, 4cm in diameter will rupture over a 5 year period. This contrasts with 75% of aneurysms, measuring over 7cm in diameter., This is well explained by Laplaces' law which relates size to transmural pressure., For this reason most vascular surgeons will subject patients with an aneurysm size of 5cm or, greater to CT scanning of the chest, abdomen and pelvis with the aim of delineating anatomy, and planning treatment. Depending upon co-morbidities, surgery is generally offered once, the aneurysm is between 5.5cm and 6cm.
Page 2893 :
A CT reconstruction showing an infrarenal abdominal aortic aneurysm. The walls of the sac are, calcified which may facilitate identification on plain x-rays, , Image sourced from Wikipedia, , Indications for surgery
Page 2894 :
, , , , Symptomatic aneurysms (80% annual mortality if untreated), Increasing size above 5.5cm if asymptomatic, Rupture (100% mortality without surgery), , Surgical procedures, Abdominal aortic aneurysm repair, Procedure:, GA, Invasive monitoring (A-line, CVP, catheter), Incision: Midline or transverse, Bowel and distal duodenum mobilised to access aorta., Aneurysm neck and base dissected out and prepared for cross clamp, Systemic heparinisation, Cross clamp (proximal first), Longitudinal aortotomy, Atherectomy, Deal with back bleeding from lumbar vessels and inferior mesenteric artery, Insert graft either tube or bifurcated depending upon anatomy, Suture using Prolene (3/0 for proximal , distal anastomosis suture varies according to site), Clamps off: End tidal CO2 will rise owing to effects of reperfusion, at this point major risk of, myocardial events., Haemostasis, Closure of aneurysm sac to minimise risk of aorto-enteric fistula, Closure: Loop 1 PDS or Prolene to abdominal wall, Skin- surgeons preference, Post operatively:, ITU (Almost all), Greatest risk of complications following emergency repair, Complications: Embolic- gut and foot infarcts, Cardiac - owing to premorbid states, re-perfusion injury and effects of cross clamp, Wound problems, Later risks related to graft- infection and aorto-enteric fistula, Special groups, Supra renal AAA, These patients will require a supra renal clamp and this carries a far higher risk of complications and, risk of renal failure., Ruptured AAA, Pre-operatively the management depends upon haemodynamic instability. In patients with, symptoms of rupture (typical pain, haemodynamic compromise and risk factors) then ideally prompt, laparotomy. In those with vague symptoms and haemodynamic stability the ideal test is CT scan to, determine whether rupture has occurred or not. Most common rupture site is retroperitoneal 80%., These patients will tend to develop retroperitoneal haematoma. This can be disrupted if Bp is, allowed to rise too high so aim for Bp 100mmHg., Operative details are similar to elective repair although surgery should be swift, blind rushing often, makes the situation worse. Plunging vascular clamps blindly into a pool of blood at the aneurysm
Page 2895 :
neck carries the risk of injury the vena cava that these patients do not withstand. Occasionally a, supracoeliac clamp is needed to effect temporary control, although leaving this applied for more than, 20 minutes tends to carry a dismal outcome., EVAR, Increasingly patients are now being offered endovascular aortic aneurysm repair. This is undertaken, by surgeons and radiologists working jointly. The morphology of the aneurysm is important and not, all are suitable. Here is a typical list of those features favoring a suitable aneurysm:, , , , , Long neck, Straight iliac vessels, Healthy groin vessels, , Clearly few AAA patients possess the above and compromise has to be made. The use of, fenestrated grafts can allow supra renal AAA to be treated., Procedure:, GA, Radiology or theatre, Bilateral groin incisions, Common femoral artery dissected out, Heparinisation, Arteriotomy and insertion of guide wire, Dilation of arteriotomy, Insertion of EVAR Device, Once in satisfactory position it is released, Arteriotomy closed once check angiogram shows good position and no endoleak, Complications:, Endoleaks depending upon site are either Type I or 2. These may necessitate re-intervention and all, EVAR patients require follow up . Details are not needed for MRCS., References, A reasonable review is provided by:, Sakalihasan N, Limet R, Defawe O. Abdominal aortic aneurysm. Lancet 2005 (365):1577- 1589, Next question
Page 2896 :
During short saphenous vein surgery for varicose veins which of the following nerves is particularly, at risk?, , Sural nerve, , Popliteal nerve, , Tibial nerve, , Femoral nerve, , Saphenous nerve, , Please rate this question:, , Discuss and give feedback, , Next question, , Saphenous vein, Long saphenous vein, This vein may be harvested for bypass surgery, or removed as treatment for varicose veins with, saphenofemoral junction incompetence., , , , , , , , Originates at the 1st digit where the dorsal vein merges with the dorsal venous arch of the, foot, Passes anterior to the medial malleolus and runs up the medial side of the leg, At the knee, it runs over the posterior border of the medial epicondyle of the femur bone, Then passes laterally to lie on the anterior surface of the thigh before entering an opening in, the fascia lata called the saphenous opening, It joins with the femoral vein in the region of the femoral triangle at the saphenofemoral, junction, , Tributaries, , , , , Medial marginal, Superficial epigastric, Superficial iliac circumflex
Page 2897 :
, , Superficial external pudendal veins, , Short saphenous vein, , , , , Originates at the 5th digit where the dorsal vein merges with the dorsal venous arch of the, foot, which attaches to the great saphenous vein., It passes around the lateral aspect of the foot (inferior and posterior to the lateral malleolus), and runs along the posterior aspect of the leg (with the sural nerve), Passes between the heads of the gastrocnemius muscle, and drains into the popliteal vein,, approximately at or above the level of the knee joint., Next question
Page 2898 :
A 21 year old badminton player attends A&E with a painful, swollen right arm. He is right handed., Clinically he has dusky fingers and his upper limb pulses are present. An axillary vein thrombosis is, confirmed. What is the best acute treatment to achieve vein patency?, , Intravenous heparin, , Warfarin, , Catheter directed tPA, , Low molecular weight heparin, , Aspirin, , Heparin and warfarin prevent propagation of the clot., Please rate this question:, , Discuss and give feedback, , Next question, , Axillary vein thrombosis, , , , , 1-2% of all deep venous thrombosis, Primary cause is associated with trauma, thoracic outlet obstruction or repeated effort in a, dominant arm (young active individuals), Secondary causes include central line insertion, malignancy, pacemakers, , Clinical features, , , , , , , Pain and swelling (non pitting), Numbness, Discolouration: mottling, dusky, Pulses present, Congested veins, , Investigations
Page 2899 :
, , , , , , , FBC: viscosity, platelet function, Clotting, Liver function tests, D-dimer, Duplex scan: investigation of choice, CT scan: thoracic outlet obstruction, , Treatment, , , , , Local catheter directed TPA, Heparin, Warfarin, Next question
Page 2900 :
A 23 year old man presents with a brachial artery embolus. A cervical rib is suspected as being the, underlying cause. From which of the following vertebral levels do they most often arise?, , C7, , C5, , C4, , C3, , C2, , They usually arise from C7., Please rate this question:, , Discuss and give feedback, , Next question, , Cervical ribs, , , , , , , , , , 0.2-0.4% incidence, Most cases present with neurological symptoms, Consist of an anomalous fibrous band that often originates from C7 and may arc towards,, but rarely reaches the sternum, Congenital cases may present around the third decade, some cases are reported to occur, following trauma, Bilateral in up to 70%, Compression of the subclavian artery may produce absent radial pulse on clinical, examination and in particular may result in a positive Adsons test (lateral flexion of the neck, towards the symptomatic side and traction of the symptomatic arm- leads to obliteration of, radial pulse), Treatment is most commonly undertaken when there is evidence of neurovascular, compromise. A transaxillary approach is the traditional operative method for excision.
Page 2901 :
Image sourced from Wikipedia, , 3D reconstruction of a left-sided cervical rib, Next question
Page 2902 :
A 73 year old man with rest pain and ulceration of the foot undergoes a femoro-distal bypass graft, with a PTFE graft. At the end of the procedure there are good distal foot pulses and a warm pink, foot. Over the ensuing 60 days the foot becomes progressively cooler and the pulses diminish. What, is the most likely underlying explanation for this process?, , Embolus, , Neo-intimal flap, , Neo-intimal hyperplasia, , Polyarteritis, , Steal syndrome, Neo-intimal hyperplasia in distal arterial anastamoses may be reduced by use of a Miller Cuff when, PTFE is the bypass conduit., PTFE may induce neo-intimal hyperplasia with subsequent occlusion of the distal anastomosis. In, more proximal arterial bypass surgery the process of neo-intimal hyperplasia is not sufficient to, cause anastomotic occlusion. However, distal bypasses are at greater risk and if vein cannot be, used as a conduit then the distal end of the PTFE should anastomosed to a vein cuff to minimise the, risk of neo-intimal hyperplasia., Please rate this question:, , Discuss and give feedback, , Next question, , Anastomoses, , , A wide variety of anastomoses are constructed in surgical practice. Essentially the term, refers to the restoration of luminal continuity. As such they are a feature of both abdominal, and vascular surgery., , Visceral anastomoses, For an anastomosis to heal three criteria need to be fulfilled:, , , , Adequate blood supply
Page 2903 :
, , , Mucosal apposition, Minimal tension, , When these are compromised the anastomosis may break down. Even in the best surgical hands, some anastomoses are more prone to dehiscence than others. Oesophageal and rectal, anastomoses are more prone to leakage and reported leak rates following oesophageal and rectal, surgery can be as high as 20%. This figure includes radiological leaks and those with a clinically, significant leak will be of a lower order of magnitude. As a rule small bowel anastomoses heal most, reliably., The decision as to how best to achieve mucosal apposition is one for each surgeon. Some will prefer, the use of stapling devices as they are quicker to use, others will prefer to perform a sutured, anastomosis. The attention to surgical technique is more important than the method chosen and a, poorly constructed stapled anastomosis in thickened tissue is far more prone to leakage than a hand, sewn anastomosis in the same circumstances., If an anastomosis looks unsafe then it may be best not to construct one at all. In colonic surgery this, is relatively clear cut and most surgeons would bring out an end colostomy. In situations such as, oesophageal surgery this is far more problematic and colonic interposition may be required in this, situation., Vascular anastomoses, Most arterial surgery involving bypasses or aneurysm repairs will require construction of an arterial, anastomosis. Technique is important and for small diameter distal arterial surgery the intimal, hyperplasia resulting from a badly constructed anastomosis may render the whole operation futile, before the patient leaves hospital., Some key points about vascular anastomoses:, , , , , , , Always use non absorbable monofilament suture (e.g. Polypropylene)., Round bodied needle., Correct size for anastamosis ( i.e. 6/0 prolene for bottom end of a femoro-distal bypass)., Suture should be continuous and from inside to outside of artery to avoid raising an intimal, flap., Next question
Page 2904 :
Theme: Lymphoedema Management, , A., B., C., D., E., F., , Homans operation, Charles operation, Frusemide at high doses, Frusemide at low doses, Multilayer compression bandaging, Lymphovenous anastomosis, , Please select the most appropriate management for the lymphoedema scenario given. Each option, may be used once, more than once or not at all., , 32., , A 52 year old lady develops lower leg swelling following redo varicose vein surgery., There is evidence of swelling of the left leg up to the knee. The overlying skin appears, healthy., You answered Homans operation, The correct answer is Multilayer compression bandaging, Unfortunately lymphoedema may complicate redo varicose vein surgery (in 0.5% of, cases). As the presentation is mild, she should be managed using compression hosiery., Diuretics do not help in cases of true lymphoedema and a dramatic response suggests an, alternative underlying cause., , 33., , A 57 year old lady has suffered from lymphoedema for many years. The left leg is swollen, to the mid thigh. Severe limb deformity has developed as a result of process and in spite of, compression hosiery. Lymphoscintography shows no patent lymphatics in the proximal, leg. The overlying skin is healthy., Homans operation, Surgery is indicated in less than 10% of cases. However, severe deformity is one of the, indications for surgery. Lymphovenous anastomosis is indicated where the proximal, lymphatics are not patent. When the overlying skin is healthy (and limb deformity a, problem), a Homans procedure is a reasonable first line operative option., , 34., , A 38 year old lady is troubled by lymphoedema that occurred following a block dissection, of the groin for malignant melanoma many years previously. Despite therapy with, compression bandages she has persistent lower leg swelling impairing her activities of, daily living. She has no evidence of recurrent malignancy. Lymphoscintography, demonstrates occlusion of the groin lymphatics. However, the distal lymphatic system, appears healthy.
Page 2905 :
You answered Homans operation, The correct answer is Lymphovenous anastomosis, In young patients with proximal disease and healthy distal lymphatics a lymphovenous, anastomosis may be considered. Such cases are rare., Please rate this question:, , Discuss and give feedback, , Next question, , Lymphoedema, , , , , Due to impaired lymphatic drainage in the presence of normal capillary function., Lymphoedema causes the accumulation of protein rich fluid, subdermal fibrosis and dermal, thickening., Characteristically fluid is confined to the epifascial space (skin and subcutaneous tissues);, muscle compartments are free of oedema. It involves the foot, unlike other forms of oedema., There may be a 'buffalo hump' on the dorsum of the foot and the skin cannot be pinched due, to subcutaneous fibrosis., , Causes of lymphoedema, , Primary, , , , , , Congenital < 1 year: sporadic, Milroy's disease, Onset 1-35 years: sporadic, Meige's disease, > 35 years: Tarda, , Secondary, , , , , , , , , Bacterial/fungal/parasitic infection (filariasis), Lymphatic malignancy, Radiotherapy to lymph nodes, Surgical resection of lymph nodes, DVT, Thrombophlebitis, , Indications for surgery, , , , , Marked disability or deformity from limb swelling, Lymphoedema caused by proximal lymphatic obstruction with patent distal lymphatics, suitable for a lymphatic drainage procedure, Lymphocutaneous fistulae and megalymphatics
Page 2906 :
Procedures, , Homans operation, , Reduction procedure with preservation of overlying skin (which must be in, good condition). Skin flaps are raised and the underlying tissue excised., Limb circumference typically reduced by a third., , Charles operation, , All skin and subcutaneous tissue around the calf are excised down to the, deep fascia. Split skin grafts are placed over the site. May be performed if, overlying skin is not in good condition. Larger reduction in size than with, Homans procedure., , Lymphovenous, anastamosis, , Identifiable lymphatics are anastomosed to sub dermal venules. Usually, indicated in 2% of patients with proximal lymphatic obstruction and normal, distal lymphatics., Next question
Page 2907 :
Which of the following is not a typical feature of a chronic venous leg ulcer?, , Heaped raised borders if the ulcer has been present more than 5 years, , Evidence of surrounding lipodermatosclerosis, , Irregular shape to the ulcer, , 20% of cases will have a previous history of deep vein thrombosis, , Haemosiderin deposits in surrounding skin, , The borders of the ulcer are often well defined even though they may be irregular. Heaped or raised, borders should raise suspicion of a marjolins ulcer., Please rate this question:, , Discuss and give feedback, , Next question, , Lower leg ulcers, Venous leg ulcers, , , , , , , , , , Most due to venous hypertension, secondary to chronic venous insufficiency (other causes, include calf pump dysfunction or neuromuscular disorders), Ulcers form due to capillary fibrin cuff or leucocyte sequestration, Features of venous insufficiency include oedema, brown pigmentation, lipodermatosclerosis,, eczema, Location above the ankle, painless, Deep venous insufficiency is related to previous DVT and superficial venous insufficiency is, associated with varicose veins, Doppler ultrasound looks for presence of reflux and duplex ultrasound looks at the anatomy/, flow of the vein, Management: 4 layer compression banding after exclusion of arterial disease or surgery, If fail to heal after 12 weeks or >10cm 2 skin grafting may be needed, , Marjolin's ulcer
Page 2908 :
Image sourced from Wikipedia, , , , , , Squamous cell carcinoma, Occurring at sites of chronic inflammation e.g; burns, osteomyelitis after 10-20 years, Mainly occur on the lower limb, , Arterial ulcers, , , , , , , Occur on the toes and heel, Painful, There may be areas of gangrene, Cold with no palpable pulses, Low ABPI measurements, , Neuropathic ulcers, , , , , , Commonly over plantar surface of metatarsal head and plantar surface of hallux, The plantar neuropathic ulcer is the condition that most commonly leads to amputation in, diabetic patients, Due to pressure, Management includes cushioned shoes to reduce callous formation, , Pyoderma gangrenosum
Page 2909 :
Image sourced from Wikipedia, , , , , , Associated with inflammatory bowel disease/RA, Can occur at stoma sites, Erythematous nodules or pustules which ulcerate, Next question
Page 2910 :
Which of the following is not a typical feature of an arterial leg ulcer?, , Well demarcated edges, , A grey - white base to the ulcer, , Men are affected more than women, , Painful, , Ankle swelling, , Ankle swelling is often absent. If present it may be due to mixed arteriovenous disease. With mixed, disease the arterial component is treated first., Please rate this question:, , Discuss and give feedback, , Next question, , Peripheral vascular disease, Indications for surgery to revascularise the lower limb, , , , , , Intermittent claudication, Critical ischaemia, Ulceration, Gangrene, , Intermittent claudication that is not disabling may provide a relative indication, whilst the other, complaints are often absolute indications depending upon the frailty of the patient., Assessment, , , , , , Clinical examination, Ankle brachial pressure index measurement, Duplex arterial ultrasound, Angiography (standard, CT or MRI): usually performed only if intervention being considered.
Page 2911 :
Angioplasty, In order for angioplasty to be undertaken successfully the artery has to be accessible. The lesion, relatively short and reasonable distal vessel runoff. Longer lesions may be amenable to sub-intimal, angioplasty., Surgery, Surgery will be undertaken where attempts at angioplasty have either failed or are unsuitable., Bypass essentially involves bypassing the affected arterial segment by utilising a graft to run from, above the disease to below the disease. As with angioplasty good runoff improves the outcome., Some key concepts with bypass surgery, Superficial femoral artery occlusion to the above knee popliteal, In the ideal scenario, vein (either in situ or reversed LSV) would the used as a conduit. However,, prosthetic material has reasonable 5 year patency rates and some would advocate using this in, preference to vein so that vein can be used for other procedures in the future. In general terms either, technique is usually associated with an excellent outcome (if run off satisfactory)., Procedure, , , , , , , Artery dissected out, IV heparin 3,000 units given and then the vessels are cross clamped, Longitudinal arteriotomy, Graft cut to size and tunneled to arteriotomy sites, Anastomosis to femoral artery usually with 5/0 'double ended' Prolene suture, Distal anastomosis usually using 6/0 'double ended' Prolene, , Distal disease, , , , , Femoro-distal bypass surgery takes longer to perform, is more technically challenging and, has higher failure rates., In elderly diabetic patients with poor runoff a primary amputation may well be a safer and, more effective option. There is no point in embarking on this type of surgery in patients who, are wheelchair bound., In femorodistal bypasses vein gives superior outcomes to PTFE., , Rules, , , , , , Vein mapping 1st to see whether there is suitable vein (the preferred conduit). Sub intimal, hyperplasia occurs early when PTFE is used for the distal anastomosis and will lead to early, graft occlusion and failure., Essential operative procedure as for above knee fem-pop., If there is insufficient vein for the entire conduit then vein can be attached to the end of the, PTFE graft and then used for the distal anastomosis. This type of 'vein boot' is technically, referred to as a Miller Cuff and is associated with better patency rates than PTFE alone., Remember the more distal the arterial anastomosis the lower the success rate.
Page 2912 :
Theme: Lower limb ulceration, , A., B., C., D., E., F., G., , Mixed ulcer, Chronic obliterative arterial disease, Superficial venous insufficiency, Deep venous insufficiency, Neuropathic ulcer, Basal cell carcinoma, Squamous cell carcinoma, , Please select the most likely cause of ulceration for the scenario given. Each option may be used, once, more than once or not at all., , 37., , A 65 year old diabetic female presents with a painless ulcer at the medial malleolus, it has, been present for the past 16 years. On examination she has evidence of truncal varicosities, and a brownish discolouration of the skin overlying the affected area., You answered Mixed ulcer, The correct answer is Superficial venous insufficiency, Theme from September 2012 Exam, Venous ulcers are usually associated with features of venous insufficiency. These include, haemosiderin deposition and varicose veins. Neuropathic ulcers will tend to present at sites, of pressure, which is not typically at the medial malleolus., , 38., , A 71 year old man presents with a painful lower calf ulcer, mild pitting oedema and an, ABPI of 0.3., You answered Mixed ulcer, The correct answer is Chronic obliterative arterial disease, Painful ulcers associated with a low ABPI are usually arterial in nature. The question does, not indicate that features of chronic venous insufficiency are present. Patients may have, mild pitting oedema as many vascular patients will also have ischaemic heart disease and, elevated right heart pressures. The absence of more compelling signs of venous, insufficiency makes a mixed ulcer less likely., , 39., , A 79 year old retired teacher has had an ulcer for 15 years. It is at the medial malleolus and, has associated lipodermatosclerosis of the lower limb. The ulcer base is heaped up and, irregular.
Page 2913 :
You answered Mixed ulcer, The correct answer is Squamous cell carcinoma, If after many years an ulcer becomes heaped up and irregular, with rolled edges then, suspect a, squamous cell carcinoma., Please rate this question:, , Discuss and give feedback, , Next question, , Lower leg ulcers, Venous leg ulcers, , , , , , , , , , Most due to venous hypertension, secondary to chronic venous insufficiency (other causes, include calf pump dysfunction or neuromuscular disorders), Ulcers form due to capillary fibrin cuff or leucocyte sequestration, Features of venous insufficiency include oedema, brown pigmentation, lipodermatosclerosis,, eczema, Location above the ankle, painless, Deep venous insufficiency is related to previous DVT and superficial venous insufficiency is, associated with varicose veins, Doppler ultrasound looks for presence of reflux and duplex ultrasound looks at the anatomy/, flow of the vein, Management: 4 layer compression banding after exclusion of arterial disease or surgery, If fail to heal after 12 weeks or >10cm 2 skin grafting may be needed, , Marjolin's ulcer
Page 2914 :
Image sourced from Wikipedia, , , , , , Squamous cell carcinoma, Occurring at sites of chronic inflammation e.g; burns, osteomyelitis after 10-20 years, Mainly occur on the lower limb, , Arterial ulcers, , , , , , , Occur on the toes and heel, Painful, There may be areas of gangrene, Cold with no palpable pulses, Low ABPI measurements, , Neuropathic ulcers, , , , , , Commonly over plantar surface of metatarsal head and plantar surface of hallux, The plantar neuropathic ulcer is the condition that most commonly leads to amputation in, diabetic patients, Due to pressure, Management includes cushioned shoes to reduce callous formation, , Pyoderma gangrenosum
Page 2915 :
Image sourced from Wikipedia, , , , , , Associated with inflammatory bowel disease/RA, Can occur at stoma sites, Erythematous nodules or pustules which ulcerate, Next question
Page 2916 :
A 66 year old man is admitted with severe angina. There is a lesion of the proximal left anterior, descending coronary artery. Which of the following would be the most suitable conduit for bypass?, , Long saphenous vein, , Short saphenous vein, , Cephalic vein, , Internal mammary artery, , Thoraco-acromial artery, , The internal mammary artery is an excellent conduit for coronary artery bypass. It has better long, term patency rates than venous grafts. The thoraco-acromial artery is seldom used., Please rate this question:, , Discuss and give feedback, , Next question, , Cardiopulmonary bypass, Indications for surgery, , , , , Left main stem stenosis or equivalent (proximal LAD and proximal circumflex), Triple vessel disease, Diffuse disease unsuitable for PCI, , The guidelines state that CABG is the preferred treatment in high-risk patients with severe, ventricular dysfunction or diabetes mellitus., Technique, General anaesthesia, Central and arterial lines, Midline sternotomy or left sub mammary incision, Aortic root and pericardium dissected, Heart inspected, Bypass grafting may be performed using a cardiopulmonary bypass circuit with cardiac arrest or, using a number of novel 'off pump' techniques.
Page 2917 :
Procedure cardiopulmonary bypass, , , , , , , , , Aortic root cannulated, Right atrial cannula, Circuit primed and patient fully heparinised (30,000 Units unfractionated heparin) as the, circuit is highly thrombogenic, Flow established through circuit, Aortic cross clamp applied, Cardioplegia solution instilled into the aortic root below cross clamp, Heart now asystolic and ready for surgery, , Off pump techniques are evolving on a constant basis and details are beyond the scope of the, MRCS., Conduits for bypass, > Internal mammary artery is best. Use of both is associated with increased risk of sternal wound, dehiscence. However, many surgeons will use both especially for redo surgery., > Radial artery harvested from forearm. Ensure ulnar collateral working first!, > Reversed long saphenous vein grafts, Typically anastamosed using 7/0-8/0 prolene sutures (distally) and 6/0 prolene for top end., Once flow established, Anticoagulation reversed using protamine, Patient is taken off bypass, Inotropes given if needed, Sternum closed using sternal closure device or stainless steel wire, Complications, , , , , , , , , Post perfusion syndrome: transient cognitive impairment, Non union of the sternum; due to loss of the internal thoracic artery, Myocardial infarction, Late graft stenosis, Acute renal failure, Stroke, Gastrointestinal, , Perioperative risk is quantified using the Parsonnet and Euroscores and unit outcomes are audited, using this data., Reference, Eagle KA, Guyton RA, Davidoff R, et al: ACC/AHA 2004 guideline update for coronary artery bypass, graft surgery: A report of the American College of Cardiology/American Heart Association Task, Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for Coronary Artery Bypass, Graft Surgery). Circulation 2004; 110, Next question
Page 2918 :
Concerning proximal aortic dissection (Debakey types 1 and 2/ Stanford type A) which statement is, false?, , The intimal tear is typically >50% of the aortic circumference., , It is usually treated using an endovascular approach., , They have a 50% mortality in the first 2 days., , Arch reconstructions may require deep hypothermic circulatory arrest., , Target systolic pressure of <110mmHg should be maintained., , Usually open surgery is required for these lesions as customised grafts are not usually available for, this type of repair yet., Please rate this question:, , Discuss and give feedback, , Next question, , Aortic dissection, , , , , , , More common than rupture of the abdominal aorta, 33% of patients die within the first 24 hours, and 50% die within 48 hours if no treatment, received, Associated with hypertension, Features of aortic dissection: tear in the intimal layer, followed by formation and propagation, of a subintimal hematoma. Cystic medial necrosis (Marfan's), Most common site of dissection: 90% occurring within 10 centimetres of the aortic valve, , Stanford Classification, , Type, , Location, , Treatment, , A, , Ascending aorta/ aortic root, , Surgery- aortic root replacement, , B, , Descending aorta, , Medical therapy with antihypertensives
Page 2919 :
DeBakey classification, , Type, , Site affected, , I, , Ascending aorta, aortic arch, descending aorta, , II, , Ascending aorta only, , III, , Descending aorta distal to left subclavian artery, , Clinical features, , , , , , Tearing, sudden onset chest pain (painless 10%), Hypertension or Hypotension, A blood pressure difference (in each arm) greater than 20 mm Hg, Neurologic deficits (20%), , Investigations, , , , , , CXR: widened mediastinum, abnormal aortic knob, ring sign, deviation of the, trachea/oesophagus, CT angiography of the thoracic aorta, MRI angiography, Conventional angiography (now rarely used diagnostically), , Management, , , , Beta-blockers: aim HR 60-80 bpm and systolic BP 100-120 mm Hg, For type A dissections the standard of care is aortic root replacement, Next question
Page 2920 :
A 67 year old male is diagnosed as having a 7cm infra renal abdominal aortic aneurysm. What is the, likely risk of rupture over the next 5 years?, , <10%, , 20%, , 25%, , 75%, , 35%, Risks of abdominal aortic aneurysm rupture (over 5 years):, , , , , 5-5.9cm = 25%, 6-6.9cm= 35%, 7cm and over = 75%, , Aneuryms greater than 5cm in diameter on USS should be formally assessed using CT scanning, with arterial phases to delineate anatomy and facilitate surgical planning., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal aorta aneurysm, , , , , Abdominal aortic aneurysms are a common problem in vascular surgery., They may occur as either true or false aneurysm. With the former all 3 layers of the arterial, wall are involved, in the latter only a single layer of fibrous tissue forms the aneurysm wall., True abdominal aortic aneurysms have an approximate incidence of 0.06 per 1000 people., They are commonest in elderly men and for this reason the UK is now introducing the, aneurysm screening program with the aim of performing an abdominal aortic ultrasound, measurement in all men aged 65 years., , Causes
Page 2921 :
, , , , Several different groups of patients suffer from aneurysmal disease., The commonest group is those who suffer from standard arterial disease, i.e. Those who, arehypertensive, have diabetes and have been or are smokers., Other patients such as those suffering from connective tissue diseases such as Marfan's, may also develop aneurysms. In patients with abdominal aortic aneurysms the extracellular, matrix becomes disrupted with a change in the balance of collagen and elastic fibres., , Management, , , , , , , , , Most abdominal aortic aneurysms are an incidental finding., Symptoms most often relate to rupture or impending rupture., 20% rupture anteriorly into the peritoneal cavity. Very poor prognosis., 80% rupture posteriorly into the retroperitoneal space, The risk of rupture is related to aneurysm size, only 2% of aneurysms measuring less than, 4cm in diameter will rupture over a 5 year period. This contrasts with 75% of aneurysms, measuring over 7cm in diameter., This is well explained by Laplaces' law which relates size to transmural pressure., For this reason most vascular surgeons will subject patients with an aneurysm size of 5cm or, greater to CT scanning of the chest, abdomen and pelvis with the aim of delineating anatomy, and planning treatment. Depending upon co-morbidities, surgery is generally offered once, the aneurysm is between 5.5cm and 6cm., , A CT reconstruction showing an infrarenal abdominal aortic aneurysm. The walls of the sac are, calcified which may facilitate identification on plain x-rays
Page 2922 :
Image sourced from Wikipedia, , Indications for surgery, , , , , Symptomatic aneurysms (80% annual mortality if untreated), Increasing size above 5.5cm if asymptomatic, Rupture (100% mortality without surgery)
Page 2923 :
Surgical procedures, Abdominal aortic aneurysm repair, Procedure:, GA, Invasive monitoring (A-line, CVP, catheter), Incision: Midline or transverse, Bowel and distal duodenum mobilised to access aorta., Aneurysm neck and base dissected out and prepared for cross clamp, Systemic heparinisation, Cross clamp (proximal first), Longitudinal aortotomy, Atherectomy, Deal with back bleeding from lumbar vessels and inferior mesenteric artery, Insert graft either tube or bifurcated depending upon anatomy, Suture using Prolene (3/0 for proximal , distal anastomosis suture varies according to site), Clamps off: End tidal CO2 will rise owing to effects of reperfusion, at this point major risk of, myocardial events., Haemostasis, Closure of aneurysm sac to minimise risk of aorto-enteric fistula, Closure: Loop 1 PDS or Prolene to abdominal wall, Skin- surgeons preference, Post operatively:, ITU (Almost all), Greatest risk of complications following emergency repair, Complications: Embolic- gut and foot infarcts, Cardiac - owing to premorbid states, re-perfusion injury and effects of cross clamp, Wound problems, Later risks related to graft- infection and aorto-enteric fistula, Special groups, Supra renal AAA, These patients will require a supra renal clamp and this carries a far higher risk of complications and, risk of renal failure., Ruptured AAA, Pre-operatively the management depends upon haemodynamic instability. In patients with, symptoms of rupture (typical pain, haemodynamic compromise and risk factors) then ideally prompt, laparotomy. In those with vague symptoms and haemodynamic stability the ideal test is CT scan to, determine whether rupture has occurred or not. Most common rupture site is retroperitoneal 80%., These patients will tend to develop retroperitoneal haematoma. This can be disrupted if Bp is, allowed to rise too high so aim for Bp 100mmHg., Operative details are similar to elective repair although surgery should be swift, blind rushing often, makes the situation worse. Plunging vascular clamps blindly into a pool of blood at the aneurysm, neck carries the risk of injury the vena cava that these patients do not withstand. Occasionally a, supracoeliac clamp is needed to effect temporary control, although leaving this applied for more than, 20 minutes tends to carry a dismal outcome.
Page 2924 :
EVAR, Increasingly patients are now being offered endovascular aortic aneurysm repair. This is undertaken, by surgeons and radiologists working jointly. The morphology of the aneurysm is important and not, all are suitable. Here is a typical list of those features favoring a suitable aneurysm:, , , , , Long neck, Straight iliac vessels, Healthy groin vessels, , Clearly few AAA patients possess the above and compromise has to be made. The use of, fenestrated grafts can allow supra renal AAA to be treated., Procedure:, GA, Radiology or theatre, Bilateral groin incisions, Common femoral artery dissected out, Heparinisation, Arteriotomy and insertion of guide wire, Dilation of arteriotomy, Insertion of EVAR Device, Once in satisfactory position it is released, Arteriotomy closed once check angiogram shows good position and no endoleak, Complications:, Endoleaks depending upon site are either Type I or 2. These may necessitate re-intervention and all, EVAR patients require follow up . Details are not needed for MRCS., References, A reasonable review is provided by:, Sakalihasan N, Limet R, Defawe O. Abdominal aortic aneurysm. Lancet 2005 (365):1577- 1589, Next question
Page 2925 :
Theme: Venous disease, , A., B., C., D., E., F., G., H., I., , No further management needed, Injection sclerotherapy using 0.5% Sodium tetradecyl sulphate, Injection sclerotherapy using 5% phenol, Long saphenous vein ligation, Long saphenous vein stripped to the ankle, Long saphenous vein stripped to the knee, Doppler scan, Duplex scan, Endothermal ablation, , Please select the most appropriate management plan for the scenario given. Each option may be, used once, more than once or not at all., , 43., , A 42 year old teacher presents with an ulcer associated with varicose veins in the long, saphenous vein territory. Apart from a DVT 1 year ago, she has no other past medical, history., You answered No further management needed, The correct answer is Duplex scan, This patient needs a duplex scan to assess the patency of her deep venous system before, surgery can be undertaken. Other indications for duplex scan include recurrent varicose, veins or complications., , 44., , A 42 year old accountant presents with thrombophlebitis of a long standing varicosity of, the inner thigh. His past medical history is unremarkable apart from a conservatively, managed tibial fracture of the ipsilateral limb 10 years ago. Doppler and clinical, assessment demonstrate saphenofemoral junction incompetence., You answered No further management needed, The correct answer is Duplex scan, Tibial fractures are a well recognised risk factor for occult lower limb deep venous, thrombosis and most surgeons would perform a duplex scan to exclude deep venous, insufficiency prior to surgery., , 45., , A 43 year old lady presents with a thigh varicosity in the territory of the long saphenous, vein. She underwent endovenous laser therapy 5 years previously. On duplex assessment, she has a patent deep venous system and sapheno-femoral junction incompetence.
Page 2926 :
You answered No further management needed, The correct answer is Long saphenous vein stripped to the knee, In the UK, NICE, suggest the use non operative measures such as endothermal ablation for, first time varicose veins. Recurrences respond far less favourably and are best managed, with surgery., Please rate this question:, , Discuss and give feedback, , Next question, , Chronic venous insufficiency and varicose veins, Wide spectrum of disease ranging from minor cosmetic problem through to ulceration and disability., It is commoner in women than men and is worse during pregnancy. Varicose veins are best, considered as being a saccular dilation of veins (WHO). Chronic venous insufficiency is a series of, tissue changes which occur in relation to pooling of blood in the extremities with associated venous, hypertension occurring as a result of incompetent deep vein valves., The veins of the lower limb consist of an interconnected network of superficial and deep venous, systems. Varices occur because of localised weakness in the vein wall resulting in dilatation and, reflux of blood due to non union of valve cusps. Histologically the typical changes include fibrous, scar tissue dividing smooth muscle within media in the vessel wall., Tissue damage in chronic venous insufficiency occurs because of perivascular cytokine leakage, resulting in localised tissue damage coupled with impaired lymphatic flow., Diagnosis, Typical symptoms of varicose veins include:, , , , , , , , Cosmetic appearance, Aching, Ankle swelling that worsens as the day progresses, Episodic thrombophlebitis, Bleeding, Itching, , Symptoms of chronic venous insufficiency include:, , , , , , Dependant leg pain, Prominent leg swelling, Oedema extending beyond the ankle, Venous stasis ulcers
Page 2927 :
The typical venous stasis ulcer is:, , , , , , , Located above the medial malleolus, Indolent appearance with basal granulation tissue, Variable degree of scarring, Non ischaemic edges, Haemosiderin deposition in the gaiter area (and also lipodermatosclerosis)., , Differential diagnosis, , , , , , , Lower limb arterial disease, Marjolins ulcer, Claudication, Spinal stenosis, Swelling due to medical causes e.g. CCF., , Exclusion of these differentials is by means of physical examination and ankle brachial pressure, index measurement., Examination, , , , , Assess for dilated short saphenous vein (popliteal fossa) and palpate for saphena varix, medial to the femoral artery, Brodie-Trendelenburg test: to assess level of incompetence, Perthes' walking test: assess if deep venous system competent, , Investigation, , , , Doppler exam: if incompetent a biphasic signal due to retrograde flow is detected, Duplex scanning: to ensure patent deep venous system (do if DVT or trauma), , All patients should have a Doppler assessment to assess for venous reflux and should be classified, as having uncomplicated varicose veins or varicose veins with associated chronic venous, insufficiency. In the history establishing a previous thrombotic event (DVT/ lower limb fracture) is, important and patients with such a history and all who have evidence of chronic venous insufficiency, should have a duplex scan performed., Owing to litigation patients with saphenopopliteal incompetence should have a duplex scan, performed and the site marked by scan on the day of surgery., Treatment, Indications for surgery:
Page 2928 :
, , , , , Cosmetic: majority, Lipodermatosclerosis causing venous ulceration, Recurrent superficial thrombophlebitis, Bleeding from ruptured varix, , Condition, , Therapy, , Minor varicose veins no complications, , Reassure/ cosmetic therapy, , Symptomatic, uncomplicated varicose, veins, , In those without deep venous insufficiency options include; endothermal, ablation, foam sclerotherapy, saphenofemoral / popliteal disconnection,, stripping and avulsions, compression stockings, , Varicose veins with, skin changes, , Therapy as above (if compression minimum is formal class I stockings), , Chronic venous, insufficiency or ulcers, , Class 2-3 compression stockings (ensure no arterial disease)., , , , , , , Application of formal compression stockings (usually class II/III). In patients who have, suffered ulceration, compression stockings should be worn long term. Where ulceration is, present and established saphenofemoral reflux exists this should be addressed surgically for, durable relief of symptoms, either at the outset or following ulcer healing., Injection sclerotherapy (5% Ethanolamine oleate), foam is increasingly popular, though, transient blindness has been reported. Endo venous laser therapy is another minimally, invasive option, Sapheno-femoral or sapheno-popliteal ligation, in the case of the LSV; stripping and multiple, phlebectomies, , Current best practice guidance, In the United Kingdom the National Institute of Clinical Excellence guidance on varicose veins, suggests that for patients with symptomatic varicose veins the first line procedure of choice should, be endothermal ablation (see reference for more information). Where this is unavailable or, unsuitable then foam sclerotherapy should be the second line option. Surgery is currently the third, line treatment option., Trendelenburg procedure (sapheno-femoral junction ligation)
Page 2929 :
, , , , , , Head tilt 15 degrees and legs abducted, Oblique incision 1cm medial from artery, Tributaries ligated (Superficial circumflex iliac vein, Superficial inferior epigastric vein,, Superficial and deep external pudendal vein), SF junction double ligated, Saphenous vein stripped to level of knee/upper calf. NB increased risk of saphenous, neuralgia if stripped more distally, , References, Marsden G et al. Diagnosis of management of varicose veins in the the legs: summary of NICE, guidance. BMJ 2013 (347): 30-31., Next question
Page 2930 :
A 24-year-old female is referred to the acute surgical team as she is noted to have an absent left, radial pulse. Apart from some dizziness and lethargy, the patient does not have any features, suggestive of an acute ischaemic limb. Blood tests are as follows:, Na+, , 136 mmol/l, , K+, , 4.1 mmol/l, , Urea, , 2.3 mmol/l, , Creatinine, , 77 µmol/l, , ESR, , 66 mm/hr, , What is the most likely diagnosis?, , Turner's syndrome, , Takayasu's arteritis, , Kawasaki disease, , Coarctation of the aorta, , Breast carcinoma with local spread, , , , , , , , Inflammatory, obliterative arteritis affecting aorta and branches, Females> Males, Symptoms may include upper limb claudication, Clinical findings include diminished or absent pulses, ESR often affected during the acute phase, , Please rate this question:, , Discuss and give feedback, , Next question, , Takayasu's arteritis
Page 2931 :
Takayasu's arteritis is a large vessel vasculitis. It typically causes occlusion of the aorta and, questions commonly refer to an absent limb pulse. It is more common in females and Asian people, Associations, , , renal artery stenosis, , Management, , , steroids, Next question
Page 2932 :
Theme: Leg swelling, , A., B., C., D., E., F., G., , Milroy's disease, Meige's disease, Lymphoedema tarda, Filariasis, Tuberculosis, Locally advanced bladder carcinoma, Malaria, , Which is the most likely diagnosis for the scenario given? Each option may be used once, more than, once or not at all., , 47., , The medical team refer a 72 year old lady with a bilateral swollen legs. Deep vein, thrombosis has been excluded and there is no response to diuretics. On further questioning,, the patient reveals that she was born with the swelling in both of her legs., Milroy's disease, Milroy's disease is present from birth and is due to failure of the lymphatic vessels to, develop. Note that Meige's disease develops AFTER birth., , 48., , A 52 year old woman presents with rapid swelling of the left leg. The swelling is greater in, the thigh compared to the calf., You answered Milroy's disease, The correct answer is Locally advanced bladder carcinoma, Always consider a malignancy in an older adult with new lymphoedema in a limb,, especially if the swelling is greater proximally than distally. If malignancy is excluded, consider the diagnosis of lymphoedema tarda., , 49., , A 34 year old African teacher attends A&E with a swollen leg. She has been in England, for 2 weeks. She lives in an area prevalent with mosquitoes and where there is poor, sanitation., You answered Milroy's disease, The correct answer is Filariasis, Filariasis is caused by the nematode Wuchereria bancrofti, which is mainly spread by, mosquito. The oedema can be gross leading to elephantitis. Treatment is with
Page 2933 :
diethylcarbamazine., Please rate this question:, , Discuss and give feedback, , Next question, , Lymphoedema, , , , , Due to impaired lymphatic drainage in the presence of normal capillary function., Lymphoedema causes the accumulation of protein rich fluid, subdermal fibrosis and dermal, thickening., Characteristically fluid is confined to the epifascial space (skin and subcutaneous tissues);, muscle compartments are free of oedema. It involves the foot, unlike other forms of oedema., There may be a 'buffalo hump' on the dorsum of the foot and the skin cannot be pinched due, to subcutaneous fibrosis., , Causes of lymphoedema, , Primary, , , , , , Congenital < 1 year: sporadic, Milroy's disease, Onset 1-35 years: sporadic, Meige's disease, > 35 years: Tarda, , Secondary, , , , , , , , , Bacterial/fungal/parasitic infection (filariasis), Lymphatic malignancy, Radiotherapy to lymph nodes, Surgical resection of lymph nodes, DVT, Thrombophlebitis, , Indications for surgery, , , , , Marked disability or deformity from limb swelling, Lymphoedema caused by proximal lymphatic obstruction with patent distal lymphatics, suitable for a lymphatic drainage procedure, Lymphocutaneous fistulae and megalymphatics, , Procedures, , Homans operation, , Reduction procedure with preservation of overlying skin (which must be in, good condition). Skin flaps are raised and the underlying tissue excised.
Page 2934 :
Limb circumference typically reduced by a third., , Charles operation, , All skin and subcutaneous tissue around the calf are excised down to the, deep fascia. Split skin grafts are placed over the site. May be performed if, overlying skin is not in good condition. Larger reduction in size than with, Homans procedure., , Lymphovenous, anastamosis, , Identifiable lymphatics are anastomosed to sub dermal venules. Usually, indicated in 2% of patients with proximal lymphatic obstruction and normal, distal lymphatics., Next question
Page 2935 :
A 21 year old post man notices leg pain after 5 minutes walking during his round. It improves 3, minutes after stopping. Clinically he is noted to have reduced hair of the lower limbs and his calf, muscles appear atrophied. There is a weak popliteal pulse, but it is still present when the knee is, fully extended. What is the most likely diagnosis?, , Occlusive arterial disease caused by atherosclerosis, , Popliteal fossa entrapment, , Cerebral vascular accident, , Diabetes mellitus, , Adductor canal compression syndrome, , Adductor canal compression syndrome most commonly presents in young males and is an important, differential diagnosis in men presenting with symptoms of acute limb ischaemia on exertion. It is, caused by compression of the femoral artery by the musculotendinous band from adductor magnus, muscle., The treatment consists of the division of the abnormal band and restoration of the arterial circulation., Popliteal fossa entrapment is the main differential diagnosis, however the pulse disappears when the, knee is fully extended., Please rate this question:, , Discuss and give feedback, , Next question, , Adductor canal, , , , Also called Hunter's or subsartorial canal, Immediately distal to the apex of the femoral triangle, lying in the middle third of the thigh., Canal terminates at the adductor hiatus., , Borders, , Contents, , Laterally Vastus medialis muscle, , Saphenous nerve
Page 2937 :
Theme: Peripheral arterial disease, , A., B., C., D., E., F., G., H., , Femoro-above knee popliteal bypass graft using PTFE, Femoro-above knee popliteal bypass graft using long saphenous vein, Femoro-distal bypass graft using PTFE, Femoro-distal bypass graft using PTFE with Miller Cuff, Femoro-distal bypass graft using long saphenous vein, Above knee amputation, Below knee amputation, Angioplasty, , Please select the most appropriate management for the vascular scenario given. Each option may, be used once, more than once or not at all., , 51., , A 63 year old man presents with a non healing ulcer on his foot. His ABPI measurements, are 0.35. A duplex scan shows a 4 cm 90% stenotic lesion of the superficial femoral artery, with no distal disease., You answered Femoro-above knee popliteal bypass graft using PTFE, The correct answer is Angioplasty, Short occlusions are generally reasonable candidates for primary attempts at angioplasty., , 52., , A 63 year old man who previously smoked 20 cigarettes a day and has newly diagnosed, type II diabetes. He presents with rest pain. A diagnostic angiogram demonstrates, occlusion of the distal superficial femoral artery continuing below the knee. He has, reasonable posterior tibial artery below this level which branches to give good runoff to, the foot. He has varicose veins., You answered Femoro-above knee popliteal bypass graft using PTFE, The correct answer is Femoro-distal bypass graft using PTFE with Miller Cuff, This man needs a bypass operation. Using PTFE alone will not give a good result as sub, intimal hyperplasia will give poor outcome early. Using a vein cuff (Miller cuff) at the end, of a PTFE graft will improve the situation., , 53., , A wheelchair bound 78 year old women with ischaemic heart disease secondary to long, smoking history and longstanding type II diabetes presents with rest pain and a non, healing ulcer on the dorsum of her foot. Angiogram shows reasonable superficial femoral, artery and iliacs. At the level of the popliteal there is an occlusion. Below this there is a, short area of patent posterior tibial and this reconstitutes lower down the leg to flow to the, foot.
Page 2938 :
You answered Femoro-above knee popliteal bypass graft using PTFE, The correct answer is Above knee amputation, A femoro-distal bypass graft would carry a high risk of failure and risk of peri-operative, myocardial infarct. This lady would be well suited to primary amputation., Please rate this question:, , Discuss and give feedback, , Next question, , Peripheral vascular disease, Indications for surgery to revascularise the lower limb, , , , , , Intermittent claudication, Critical ischaemia, Ulceration, Gangrene, , Intermittent claudication that is not disabling may provide a relative indication, whilst the other, complaints are often absolute indications depending upon the frailty of the patient., Assessment, , , , , , Clinical examination, Ankle brachial pressure index measurement, Duplex arterial ultrasound, Angiography (standard, CT or MRI): usually performed only if intervention being considered., , Angioplasty, In order for angioplasty to be undertaken successfully the artery has to be accessible. The lesion, relatively short and reasonable distal vessel runoff. Longer lesions may be amenable to sub-intimal, angioplasty., Surgery, Surgery will be undertaken where attempts at angioplasty have either failed or are unsuitable., Bypass essentially involves bypassing the affected arterial segment by utilising a graft to run from, above the disease to below the disease. As with angioplasty good runoff improves the outcome., Some key concepts with bypass surgery
Page 2939 :
Superficial femoral artery occlusion to the above knee popliteal, In the ideal scenario, vein (either in situ or reversed LSV) would the used as a conduit. However,, prosthetic material has reasonable 5 year patency rates and some would advocate using this in, preference to vein so that vein can be used for other procedures in the future. In general terms either, technique is usually associated with an excellent outcome (if run off satisfactory)., Procedure, , , , , , , Artery dissected out, IV heparin 3,000 units given and then the vessels are cross clamped, Longitudinal arteriotomy, Graft cut to size and tunneled to arteriotomy sites, Anastomosis to femoral artery usually with 5/0 'double ended' Prolene suture, Distal anastomosis usually using 6/0 'double ended' Prolene, , Distal disease, , , , , Femoro-distal bypass surgery takes longer to perform, is more technically challenging and, has higher failure rates., In elderly diabetic patients with poor runoff a primary amputation may well be a safer and, more effective option. There is no point in embarking on this type of surgery in patients who, are wheelchair bound., In femorodistal bypasses vein gives superior outcomes to PTFE., , Rules, , , , , , Vein mapping 1st to see whether there is suitable vein (the preferred conduit). Sub intimal, hyperplasia occurs early when PTFE is used for the distal anastomosis and will lead to early, graft occlusion and failure., Essential operative procedure as for above knee fem-pop., If there is insufficient vein for the entire conduit then vein can be attached to the end of the, PTFE graft and then used for the distal anastomosis. This type of 'vein boot' is technically, referred to as a Miller Cuff and is associated with better patency rates than PTFE alone., Remember the more distal the arterial anastomosis the lower the success rate., , References, Peach G et al. Diagnosis and management of peripheral arterial disease. BMJ 2012; 345: 36-41., Next question
Page 2940 :
Which of the following is not a feature of a Charcot foot?, , Bounding foot pulses in the early phases, , Often occurs in the complete absence of trauma, , Erythema of the foot in the early phase, , Autonomic neuropathy, , Peripheral neuropathy, Do not confuse the early phase of Charcot foot with cellulitis, Trauma (even if only minor) is a prerequisite. Patients cannot usually recall the traumatic event. The, associated neuropathy means that patients continue to walk on the affected foot with subsequent, deformity developing over time., Please rate this question:, , Discuss and give feedback, , Next question, , Peripheral vascular disease, Indications for surgery to revascularise the lower limb, , , , , , Intermittent claudication, Critical ischaemia, Ulceration, Gangrene, , Intermittent claudication that is not disabling may provide a relative indication, whilst the other, complaints are often absolute indications depending upon the frailty of the patient., Assessment, , , , , Clinical examination, Ankle brachial pressure index measurement, Duplex arterial ultrasound
Page 2941 :
, , Angiography (standard, CT or MRI): usually performed only if intervention being considered., , Angioplasty, In order for angioplasty to be undertaken successfully the artery has to be accessible. The lesion, relatively short and reasonable distal vessel runoff. Longer lesions may be amenable to sub-intimal, angioplasty., Surgery, Surgery will be undertaken where attempts at angioplasty have either failed or are unsuitable., Bypass essentially involves bypassing the affected arterial segment by utilising a graft to run from, above the disease to below the disease. As with angioplasty good runoff improves the outcome., Some key concepts with bypass surgery, Superficial femoral artery occlusion to the above knee popliteal, In the ideal scenario, vein (either in situ or reversed LSV) would the used as a conduit. However,, prosthetic material has reasonable 5 year patency rates and some would advocate using this in, preference to vein so that vein can be used for other procedures in the future. In general terms either, technique is usually associated with an excellent outcome (if run off satisfactory)., Procedure, , , , , , , Artery dissected out, IV heparin 3,000 units given and then the vessels are cross clamped, Longitudinal arteriotomy, Graft cut to size and tunneled to arteriotomy sites, Anastomosis to femoral artery usually with 5/0 'double ended' Prolene suture, Distal anastomosis usually using 6/0 'double ended' Prolene, , Distal disease, , , , , Femoro-distal bypass surgery takes longer to perform, is more technically challenging and, has higher failure rates., In elderly diabetic patients with poor runoff a primary amputation may well be a safer and, more effective option. There is no point in embarking on this type of surgery in patients who, are wheelchair bound., In femorodistal bypasses vein gives superior outcomes to PTFE., , Rules, , , , , Vein mapping 1st to see whether there is suitable vein (the preferred conduit). Sub intimal, hyperplasia occurs early when PTFE is used for the distal anastomosis and will lead to early, graft occlusion and failure., Essential operative procedure as for above knee fem-pop., If there is insufficient vein for the entire conduit then vein can be attached to the end of the, PTFE graft and then used for the distal anastomosis. This type of 'vein boot' is technically, referred to as a Miller Cuff and is associated with better patency rates than PTFE alone.
Page 2942 :
, , Remember the more distal the arterial anastomosis the lower the success rate., , References, Peach G et al. Diagnosis and management of peripheral arterial disease. BMJ 2012; 345: 36-41., Next question
Page 2943 :
A 34 year old man presents with varicose veins and it is suspected that these are part of the KlippelTrenaunay syndrome. Which of the following is not a characteristic of this condition?, , Presence of varicose veins, , Gigantism of a limb, , Long saphenous vein involvement, , Port wine stains with clear borders, , Arteriovenous fistulae, , The Klippel-Trenaunay vein is a large, lateral, superficial vein sometimes seen at birth. This vein, begins in the foot or the lower leg and travels proximally until it enters the thigh or the gluteal area., Otherwise, varicosities may not be clinically evident until the child begins to ambulate., Varicosities may be extensive, though they often spare the saphenous distribution. They are seen, below the knee, laterally above the knee, and occasionally in the pelvic region. Varicosities may, affect the superficial, deep, and perforating venous systems., Surgical exploration has demonstrated atresia and agenesis of deep veins, compression due to, fibrous bands, aberrant arteries, abnormal muscles, or venous sheaths., Rarely, varicosities have been found in the bladder, the colon, and the pulmonary vessels, Please rate this question:, , Discuss and give feedback, , Next question, , Klippel-Trenaunay syndrome, Klippel-Trenaunay-Weber syndrome generally affects a single extremity, although cases of multiple, affected limbs have been reported. The leg is the most common site followed by the arms, the trunk,, and rarely the head and the neck, Signs and symptoms, The birth defect is diagnosed by the presence of a combination of these symptoms:, , , , , , One or more distinctive port-wine stains with sharp borders, Varicose veins, Hypertrophy of bony and soft tissues, that may lead to local gigantism or shrinking., An improperly developed lymphatic system
Page 2944 :
In some cases, port-wine stains (capillary port wine type) may be absent. Such cases are very rare, and may be classified as "atypical Klippel-Trenaunay syndrome"., KTS can either affect blood vessels, lymph vessels, or both. The condition most commonly presents, with a mixture of the two. Those with venous involvement experience increased pain and, complications., Next question
Page 2945 :
Theme: Diabetic foot sepsis, , A., B., C., D., E., F., G., H., , IV broad spectrum antibiotics, Incision and drainage of pus, Ray amputation, Below knee amputation, Above knee amputation, Vacuum Assisted Closure device (VAC), Discharge home, Application of 4 layer bandages, , Please select the most appropriate management for the scenario given. Each option may be used, once, more than once or not at all., , 56., , A 68 year old man with type II diabetes has a non healing ulcer following a ray amputation, 2 weeks ago. An x-ray shows no osteomyelitis and the ABPI is >1., You answered IV broad spectrum antibiotics, The correct answer is Vacuum Assisted Closure device (VAC), A VAC dressing may avoid the need for further surgery., , 57., , A 48 year old woman is admitted with sepsis secondary to an infected diabetic foot ulcer., She has a necrotic and infected forefoot with necrosis of the heel. There is a boggy, indurated swelling anterior to the ankle joint. Pulses are normal., You answered IV broad spectrum antibiotics, The correct answer is Below knee amputation, A below knee amputation is the best option here. The foot is non salvageable. However,, she may ambulate with a prosthesis., , 58., , An 84 year old lady is admitted with an infected diabetic foot. An x-ray shows, osteomyelitis of her calcaneum. She has a fixed flexion deformity of her knee, but normal, pulses., You answered IV broad spectrum antibiotics, The correct answer is Above knee amputation, This patient will not be able to walk with a below knee amputation, therefore an above
Page 2946 :
knee amputation would be preferable, as it guarantees better healing the short term., Consider above knee amputation in patients with fixed flexion deformity., Please rate this question:, , Discuss and give feedback, , Next question, , Amputations, Amputations are indicated when the affected limb is one of the following:, , , , , Dead non viable, Deadly where it is posing a major threat to life, Dead useless where it is viable but a prosthesis would be preferable, , Orthopaedic surgery, , , , Amputation is often undertaken as an option of last resort e.g. Limb salvage has failed and, the limb is so non functional that mobility needs would be best met with prosthesis., Chronic fracture non union or significant limb shortening following trauma would fit into this, category. Occasionally following major trauma a primary amputation is preferable. This, would be the case in an open fracture with major distal neurovascular compromise and other, more life threatening injuries are present., , Vascular surgery, , , , , , The first two categories are the most prevalent., Diabetic foot sepsis is often a major cause of sepsis which can spread rapidly in the, presence of established peripheral vascular disease., As a general rule the main issue in vascular surgery is to optimise vascular inflow prior to, surgery. The more distal the planned amputation is to be, the more important this rule, becomes., In other situations there has been something such as an embolic event that has not been, revascularised in time. In this case the limb shows fixed mottling and an amputation will be, needed., , Types of amputations, As the vast majority of commonly performed amputations affect the lower limbs these will be covered, here.
Page 2947 :
The main categories of amputations are:, , , , , , , , Pelvic disarticulation (hindquarter), Above knee amputation, Gritti Stokes (through knee amputation), Below knee amputation (using either Skew or Burgess flaps), Syme's amputation (through ankle), Amputations of mid foot and digits, , Choosing a level of amputation depends on:, , , , , The disease process being treated, Desired functional outcome, Co-morbidities of the patient, , Above knee amputations, , , , , , , Quick to perform, Heal reliably, Patients regain their general health quickly, For this benefit, a functional price has to be paid and many patients over the age of 70 will, never walk on an above knee prosthesis., Above knee amputations use equal anterior-posterior flaps, , Below knee amputations, , , , , , Technically more challenging to perform, Heal less reliably than their above knee counterparts., However, many more patients are able to walk using a below knee prosthesis., In below knee amputations the two main flaps are Skew flaps or the Burgess long posterior, flap. Skew flaps result in a less bulky limb that is easier to attach a prosthesis to., , It is worth remembering that whilst it may be technically feasible to offer a below knee amputation, there may be circumstances where an above knee option is preferable. For example, in fixed flexion, deformities of the lower limb, little functional benefit would be gained from below knee amputation, surgery., Next question
Page 2948 :
Which of the following statements related to coronary artery bypass surgery is true?, , Late graft stenosis is mainly associated with saphenous vein grafts, , Is indicated if there is stenosis > 70% of the right coronary artery, , The left atrium is cannulated during the procedure, , The CHADS score is used to assess peri operative risk, , Cardioplegia is always undertaken at a 37 degrees, , Indications are:, 1. Left main stem stenosis or equivalent (proximal LAD and proximal circumflex), 2. Triple vessel disease, 3. Diffuse disease unsuitable for PCI, The right atrium is cannulated. The CHADS score assesses whether a patient should be, warfarinised if they have atrial fibrillation. Cardioplegia can be undertaken at cold or warm, temperatures., Please rate this question:, , Discuss and give feedback, , Next question, , Cardiopulmonary bypass, Indications for surgery, , , , , Left main stem stenosis or equivalent (proximal LAD and proximal circumflex), Triple vessel disease, Diffuse disease unsuitable for PCI, , The guidelines state that CABG is the preferred treatment in high-risk patients with severe, ventricular dysfunction or diabetes mellitus., Technique, General anaesthesia, Central and arterial lines, Midline sternotomy or left sub mammary incision
Page 2949 :
Aortic root and pericardium dissected, Heart inspected, Bypass grafting may be performed using a cardiopulmonary bypass circuit with cardiac arrest or, using a number of novel 'off pump' techniques., Procedure cardiopulmonary bypass, , , , , , , , , Aortic root cannulated, Right atrial cannula, Circuit primed and patient fully heparinised (30,000 Units unfractionated heparin) as the, circuit is highly thrombogenic, Flow established through circuit, Aortic cross clamp applied, Cardioplegia solution instilled into the aortic root below cross clamp, Heart now asystolic and ready for surgery, , Off pump techniques are evolving on a constant basis and details are beyond the scope of the, MRCS., Conduits for bypass, > Internal mammary artery is best. Use of both is associated with increased risk of sternal wound, dehiscence. However, many surgeons will use both especially for redo surgery., > Radial artery harvested from forearm. Ensure ulnar collateral working first!, > Reversed long saphenous vein grafts, Typically anastamosed using 7/0-8/0 prolene sutures (distally) and 6/0 prolene for top end., Once flow established, Anticoagulation reversed using protamine, Patient is taken off bypass, Inotropes given if needed, Sternum closed using sternal closure device or stainless steel wire, Complications, , , , , , , , , Post perfusion syndrome: transient cognitive impairment, Non union of the sternum; due to loss of the internal thoracic artery, Myocardial infarction, Late graft stenosis, Acute renal failure, Stroke, Gastrointestinal, , Perioperative risk is quantified using the Parsonnet and Euroscores and unit outcomes are audited, using this data., Reference, Eagle KA, Guyton RA, Davidoff R, et al: ACC/AHA 2004 guideline update for coronary artery bypass
Page 2950 :
graft surgery: A report of the American College of Cardiology/American Heart Association Task, Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for Coronary Artery Bypass, Graft Surgery). Circulation 2004; 110, Next question
Page 2951 :
A 73 year old man develops sudden onset abdominal pain and collapses. On examination he has a, tender pulsatile mass in his upper abdomen. He has a blood pressure of 90/60mmHg and pulse rate, of 105 beats per minute. Which of the following intravenous fluid regimens is most appropriate,, whilst waiting for operative repair?, , 1 Litre of pentastarch over 15 minutes, , 1 litre of Hartmans solution over 4 hours, , 1 litre of gelofusin over 30 minutes, , 1 litre of Hartmans solution over 30 minutes, , 1 litre of blood over 15 minutes, , This man will have a contained haematoma and is awaiting surgery. Rapid, high volume infusions, may cause this to dislodge with disastrous consequences, Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal aorta aneurysm, , , , , Abdominal aortic aneurysms are a common problem in vascular surgery., They may occur as either true or false aneurysm. With the former all 3 layers of the arterial, wall are involved, in the latter only a single layer of fibrous tissue forms the aneurysm wall., True abdominal aortic aneurysms have an approximate incidence of 0.06 per 1000 people., They are commonest in elderly men and for this reason the UK is now introducing the, aneurysm screening program with the aim of performing an abdominal aortic ultrasound, measurement in all men aged 65 years., , Causes, , , , , Several different groups of patients suffer from aneurysmal disease., The commonest group is those who suffer from standard arterial disease, i.e. Those who, arehypertensive, have diabetes and have been or are smokers., Other patients such as those suffering from connective tissue diseases such as Marfan's, may also develop aneurysms. In patients with abdominal aortic aneurysms the extracellular, matrix becomes disrupted with a change in the balance of collagen and elastic fibres.
Page 2952 :
Management, , , , , , , , , Most abdominal aortic aneurysms are an incidental finding., Symptoms most often relate to rupture or impending rupture., 20% rupture anteriorly into the peritoneal cavity. Very poor prognosis., 80% rupture posteriorly into the retroperitoneal space, The risk of rupture is related to aneurysm size, only 2% of aneurysms measuring less than, 4cm in diameter will rupture over a 5 year period. This contrasts with 75% of aneurysms, measuring over 7cm in diameter., This is well explained by Laplaces' law which relates size to transmural pressure., For this reason most vascular surgeons will subject patients with an aneurysm size of 5cm or, greater to CT scanning of the chest, abdomen and pelvis with the aim of delineating anatomy, and planning treatment. Depending upon co-morbidities, surgery is generally offered once, the aneurysm is between 5.5cm and 6cm., , A CT reconstruction showing an infrarenal abdominal aortic aneurysm. The walls of the sac are, calcified which may facilitate identification on plain x-rays
Page 2953 :
Image sourced from Wikipedia, , Indications for surgery, , , , , Symptomatic aneurysms (80% annual mortality if untreated), Increasing size above 5.5cm if asymptomatic, Rupture (100% mortality without surgery)
Page 2954 :
Surgical procedures, Abdominal aortic aneurysm repair, Procedure:, GA, Invasive monitoring (A-line, CVP, catheter), Incision: Midline or transverse, Bowel and distal duodenum mobilised to access aorta., Aneurysm neck and base dissected out and prepared for cross clamp, Systemic heparinisation, Cross clamp (proximal first), Longitudinal aortotomy, Atherectomy, Deal with back bleeding from lumbar vessels and inferior mesenteric artery, Insert graft either tube or bifurcated depending upon anatomy, Suture using Prolene (3/0 for proximal , distal anastomosis suture varies according to site), Clamps off: End tidal CO2 will rise owing to effects of reperfusion, at this point major risk of, myocardial events., Haemostasis, Closure of aneurysm sac to minimise risk of aorto-enteric fistula, Closure: Loop 1 PDS or Prolene to abdominal wall, Skin- surgeons preference, Post operatively:, ITU (Almost all), Greatest risk of complications following emergency repair, Complications: Embolic- gut and foot infarcts, Cardiac - owing to premorbid states, re-perfusion injury and effects of cross clamp, Wound problems, Later risks related to graft- infection and aorto-enteric fistula, Special groups, Supra renal AAA, These patients will require a supra renal clamp and this carries a far higher risk of complications and, risk of renal failure., Ruptured AAA, Pre-operatively the management depends upon haemodynamic instability. In patients with, symptoms of rupture (typical pain, haemodynamic compromise and risk factors) then ideally prompt, laparotomy. In those with vague symptoms and haemodynamic stability the ideal test is CT scan to, determine whether rupture has occurred or not. Most common rupture site is retroperitoneal 80%., These patients will tend to develop retroperitoneal haematoma. This can be disrupted if Bp is, allowed to rise too high so aim for Bp 100mmHg., Operative details are similar to elective repair although surgery should be swift, blind rushing often, makes the situation worse. Plunging vascular clamps blindly into a pool of blood at the aneurysm, neck carries the risk of injury the vena cava that these patients do not withstand. Occasionally a, supracoeliac clamp is needed to effect temporary control, although leaving this applied for more than, 20 minutes tends to carry a dismal outcome.
Page 2955 :
EVAR, Increasingly patients are now being offered endovascular aortic aneurysm repair. This is undertaken, by surgeons and radiologists working jointly. The morphology of the aneurysm is important and not, all are suitable. Here is a typical list of those features favoring a suitable aneurysm:, , , , , Long neck, Straight iliac vessels, Healthy groin vessels, , Clearly few AAA patients possess the above and compromise has to be made. The use of, fenestrated grafts can allow supra renal AAA to be treated., Procedure:, GA, Radiology or theatre, Bilateral groin incisions, Common femoral artery dissected out, Heparinisation, Arteriotomy and insertion of guide wire, Dilation of arteriotomy, Insertion of EVAR Device, Once in satisfactory position it is released, Arteriotomy closed once check angiogram shows good position and no endoleak, Complications:, Endoleaks depending upon site are either Type I or 2. These may necessitate re-intervention and all, EVAR patients require follow up . Details are not needed for MRCS., References, A reasonable review is provided by:, Sakalihasan N, Limet R, Defawe O. Abdominal aortic aneurysm. Lancet 2005 (365):1577- 1589, Next question
Page 2956 :
Theme: Mesenteric vascular disease, , A. Abdominal ultrasound, B. Abdominal CT with venous phase contrast, C. CT angiogram, D. Magnetic resonance angiogram, E. Duplex ultrasound, F. Abdominal x-ray, G. Mesenteric angiography via brachial artery, , Please select the most appropriate investigation for the scenario given. Each option may be used, once, more than once or not at all., , 61., , A thin 72 year old lady has a 3 week history of postprandial abdominal pain that is centrally, located. She has episodic diarrhoea and occasionally has passed blood PR. She has a history of, ischaemic heart disease and marked renal impairment from ACE inhibitor usage., You answered Abdominal ultrasound, The correct answer is Duplex ultrasound, She is likely to have mesenteric vascular disease. Proximal SMA disease would be the most serious, variant. Ideally a CT angiogram would be the best test but with her impaired renal function and, low BMI, make a duplex of the SMA is a reasonable first line investigation. Gut peristalsis may, impair acquisition of magnetic resonance images., , 62., , A 78 year old man develops sudden onset abdominal pain and almost immediately afterwards, passes a large amount of diarrhoea., You answered Abdominal ultrasound, The correct answer is CT angiogram
Page 2957 :
Sudden onset of abdominal pain followed by forceful evacuation are the classical presenting, features of acute mesenteric infarction. This is best investigated by CT angiography, which has a, sensitivity of 95% for the diagnosis., , 63., , A 28 year old female has suffered from abdominal pain for the past 2 weeks since she was started, on the contraceptive pill. The pain has increased significantly over the post 10 hours and has been, associated with vomiting., You answered Abdominal ultrasound, The correct answer is Abdominal CT with venous phase contrast, Mesenteric venous thrombosis is the likely underlying cause and an angiogram is the sensible step, as it will also facilitate the identification of areas of infarcted bowel , similar to that which may, occur in the leg when massive DVT is present., , Please rate this question:, , Discuss and give feedback, , Next question, , Vascular investigations, Venous disease, Venous Doppler, The simplest investigation for assessment of venous junctional incompetence is a Doppler, assessment. This involves the patient standing and manual compression of the limb distal to the, junction of interest. Flow should normally occur in one direction only. Where junctional incompetence, is present reverse flow will occur and is relatively easy to identify., Venograms and duplex scans, Structural venous information is historically obtained using a venogram. This is an invasive test and, rarely required in modern clinical practice. The most helpful test is a venous duplex scan which will, provide information relating to flow and vessel characteristics. Duplex is also useful in providing vein, maps for bypass surgery.
Page 2958 :
Arterial disease, Ankle-brachial pressure, The ankle brachial pressure index measurement is an important investigation as it will allow, classification of the severity of the flow compromise present. False readings may occur in those with, calcified vessels such as diabetics and results in such settings should be interpreted with caution., When auscultating the vessel note should be made of the character of the signal. Monophasic, signals are associated with a proximal stenosis and reduction in flow. Triphasic signals provide, reassurance of a healthy vessel., Arterial Duplex, As with the vein the duplex scan can provide a substantial amount of information about arterial, patency and flow patterns. In skilled hands they can provide insight as to the state of proximal, vessels that are anatomically inaccessible to duplex (e.g. Iliacs). Through assessment of distal flow, patterns. It is an operator dependent test., Conventional angiogram, Vessel puncture and catheter angiography is the gold standard method of assessing arteries. High, quality information can usually be obtained. Limitations of the technique include the risk of contrast, toxicity and risks of vessel damage. Severely calcified vessels may be difficult to puncture and in this, situation a remote access site (e.g. brachial) may be used. This technique is particularly useful in, providing a distal arterial roadmap prior to femoro-distal bypass., CT angiography, These tests provide a considerable amount of structural and flow information. They require contrast, and thus carry the risks associated with this. They are particularly useful in the setting of GI bleeding, as they are rapidly available and can be performed by a non vascular radiologist. However, they lack, the facility for endovascular intervention. In general they do not provide high enough resolution for, distal arterial surgery., Magnetic resonance angiography, This has the advantage of being non-invasive and not using nephrotoxic contrast. Movement artifact, remains a problem in some sites and distal arterial resolution is imperfect., Next question
Page 2959 :
A 52 year old male attends the stroke unit with dizziness and vertigo while playing tennis. He is, known to have hypertension and a previous myocardial infarct. He now complains of right arm pain., What is the most likely diagnosis?, , Posterior circulation infarct, , Vertebrobasilar aneurysm, , Dissection of thoracic aorta, , Subclavian steal syndrome, , Left middle cerebral artery infarct, , Subclavian steal syndrome characteristically presents with posterior circulation symptoms, such as, dizziness and vertigo, during exertion of an arm. There is subclavian artery steno-occlusive disease, proximal to the origin of the vertebral artery and is associated with flow reversal in the vertebral, artery. Management involves percutaneous transluminal angioplasty or a stent., Please rate this question:, , Discuss and give feedback, , Next question, , Subclavian artery, Path, , , , , The left subclavian comes directly off the arch of aorta, The right subclavian arises from the brachiocephalic artery (trunk) when it bifurcates into the, subclavian and the right common carotid artery., From its origin, the subclavian artery travels laterally, passing between anterior and middle, scalene muscles, deep to scalenus anterior and anterior to scalenus medius. As the, subclavian artery crosses the lateral border of the first rib, it becomes the axillary artery. At, this point it is superficial and within the subclavian triangle.
Page 2960 :
Image sourced from Wikipedia, , Branches, , , , , , , Vertebral artery, Internal thoracic artery, Thyrocervical trunk, Costocervical trunk, Dorsal scapular artery, Next question
Page 2961 :
A 74 year old lady has a long standing venous leg ulcer overlying her medial malleolus. Which of the, following statements relating to the management of this condition is false?, , Pentoxifylline may speed ulcer healing, , Treatment with daily low dose flucloxacillin may speed ulcer healing, , Multilayer bandages may provide compression equivalent to 40mmHg, , Large ulcers may be considered for skin grafting, , They should not be treated with compression stockings if the ankle / brachial pressure, index is 0.6, , Routine use of antibiotics is not advised as this may predispose to resistant organisms., Pentoxifylline was subjected to a Cochrane review in 2007 and shown to improve healing rates., Please rate this question:, , Discuss and give feedback, , Next question, , Lower leg ulcers, Venous leg ulcers, , , , , , , , , , Most due to venous hypertension, secondary to chronic venous insufficiency (other causes, include calf pump dysfunction or neuromuscular disorders), Ulcers form due to capillary fibrin cuff or leucocyte sequestration, Features of venous insufficiency include oedema, brown pigmentation, lipodermatosclerosis,, eczema, Location above the ankle, painless, Deep venous insufficiency is related to previous DVT and superficial venous insufficiency is, associated with varicose veins, Doppler ultrasound looks for presence of reflux and duplex ultrasound looks at the anatomy/, flow of the vein, Management: 4 layer compression banding after exclusion of arterial disease or surgery, If fail to heal after 12 weeks or >10cm 2 skin grafting may be needed, , Marjolin's ulcer
Page 2962 :
Image sourced from Wikipedia, , , , , , Squamous cell carcinoma, Occurring at sites of chronic inflammation e.g; burns, osteomyelitis after 10-20 years, Mainly occur on the lower limb, , Arterial ulcers, , , , , , , Occur on the toes and heel, Painful, There may be areas of gangrene, Cold with no palpable pulses, Low ABPI measurements, , Neuropathic ulcers, , , , , , Commonly over plantar surface of metatarsal head and plantar surface of hallux, The plantar neuropathic ulcer is the condition that most commonly leads to amputation in, diabetic patients, Due to pressure, Management includes cushioned shoes to reduce callous formation, , Pyoderma gangrenosum
Page 2963 :
Image sourced from Wikipedia, , , , , , Associated with inflammatory bowel disease/RA, Can occur at stoma sites, Erythematous nodules or pustules which ulcerate, Next question
Page 2964 :
Theme: Investigation of vascular disease, , A. Angiography, B. Arterial duplex scan, C. Arch aortogram, D. CXR, E. CT scan, F. Venous duplex scan, , Please select the most appropriate investigation for the scenario given. Each option may be used, once, more than once or not at all., , 66., , A 22 year old professional tennis player attends A&E with a swollen painful right arm. His fingers, are dusky., You answered Angiography, The correct answer is Venous duplex scan, This patient has an axillary vein thrombosis. It classically presents with pain and swelling of an, effort induced limb. Duplex scan is needed to exclude a thombus., , 67., , A 65 year old man presents with expressive dysphasia and left sided weakness over 4 hours. His, symptoms have now completely resolved. A CT scan of his head is normal., You answered Angiography, The correct answer is Arterial duplex scan, This patient has had a transient ischaemic attack. He urgently needs carotid duplex scanning to, assess if he needs a carotid endarterectomy.
Page 2965 :
68., , A 65 year old man presents, for the first time, with pain at the back of his calves when he, mobilises 10 metres. He is known to have hypertension., You answered Angiography, The correct answer is Arterial duplex scan, An arterial duplex should be performed first, before progression to an angiography., , Please rate this question:, , Discuss and give feedback, , Next question, , Vascular investigations, Venous disease, Venous Doppler, The simplest investigation for assessment of venous junctional incompetence is a Doppler, assessment. This involves the patient standing and manual compression of the limb distal to the, junction of interest. Flow should normally occur in one direction only. Where junctional incompetence, is present reverse flow will occur and is relatively easy to identify., Venograms and duplex scans, Structural venous information is historically obtained using a venogram. This is an invasive test and, rarely required in modern clinical practice. The most helpful test is a venous duplex scan which will, provide information relating to flow and vessel characteristics. Duplex is also useful in providing vein, maps for bypass surgery., Arterial disease, Ankle-brachial pressure, The ankle brachial pressure index measurement is an important investigation as it will allow, classification of the severity of the flow compromise present. False readings may occur in those with, calcified vessels such as diabetics and results in such settings should be interpreted with caution., When auscultating the vessel note should be made of the character of the signal. Monophasic
Page 2966 :
signals are associated with a proximal stenosis and reduction in flow. Triphasic signals provide, reassurance of a healthy vessel., Arterial Duplex, As with the vein the duplex scan can provide a substantial amount of information about arterial, patency and flow patterns. In skilled hands they can provide insight as to the state of proximal, vessels that are anatomically inaccessible to duplex (e.g. Iliacs). Through assessment of distal flow, patterns. It is an operator dependent test., Conventional angiogram, Vessel puncture and catheter angiography is the gold standard method of assessing arteries. High, quality information can usually be obtained. Limitations of the technique include the risk of contrast, toxicity and risks of vessel damage. Severely calcified vessels may be difficult to puncture and in this, situation a remote access site (e.g. brachial) may be used. This technique is particularly useful in, providing a distal arterial roadmap prior to femoro-distal bypass., CT angiography, These tests provide a considerable amount of structural and flow information. They require contrast, and thus carry the risks associated with this. They are particularly useful in the setting of GI bleeding, as they are rapidly available and can be performed by a non vascular radiologist. However, they lack, the facility for endovascular intervention. In general they do not provide high enough resolution for, distal arterial surgery., Magnetic resonance angiography, This has the advantage of being non-invasive and not using nephrotoxic contrast. Movement artifact, remains a problem in some sites and distal arterial resolution is imperfect., Next question
Page 2967 :
Theme: Ankle Brachial pressure index measurements, , A., B., C., D., E., , >1, 0.6- 0.8, 1, 0.4-0.6, <0.4, , For the scenarios described below, please select the most likely ankle brachial pressure index, measurement. Each option may be used once, more than once or not at all., , 69., , An 83 year old male with rest pain., You answered >1, The correct answer is <0.4, Theme from September 2015 Exam, Rest pain is typically associated with low ABPI values., , 70., , A 45 year old man who develops calf pain after walking 600 yards. It resolves during, periods of rest., You answered >1, The correct answer is 0.6- 0.8, Since this is a long claudication distance it may be that only a minor lesion is present., Whilst resting ABPI may be normal, they are usually abnormal following exercise., , 71., , A 43 year old lady with long standing diabetes who complains of calf pain. It is worse at, night and during minor exercise., >1, Diabetes may be complicated by vessel calcification and neuropathic pain. Therefore, individuals may present with pain which is atypical for claudation both in terms of its, tempo of onset and location., , Please rate this question:, , Discuss and give feedback
Page 2968 :
Next question, , Ankle-Brachial pressure index, , , , Measurement of ankle- brachial pressure index (ABPI) is a commonly performed vascular, investigation., Calculated by dividing lower limb pressure by the highest upper limb pressure., , Results of ABPI, 1.2 or greater, , Usually due to vessel calcification, , 1.0- 1.2, , Normal, , 0.8-1.0, , Minor stenotic lesion, Initiate risk factor management, , 0.50-0.8, , Moderate stenotic lesion, Consider duplex, Risk factor management, If mixed ulcers present then avoid tight compression bandages, , 0.5- 0.3, , Likely significant stenosis, Duplex scanning to delineate lesions needed, Compression bandaging contra indicated, , Less than 0.3, , Indicative of critical ischaemia, Urgent detailed imaging required, , Next question
Page 2969 :
Theme: Causes of ulceration, , A., B., C., D., E., F., G., H., , Marjolin's ulcer, Neuropathic ulcer, Arterial ulcer, Deep venous dysfunction, Superficial venous dysfunction, Rheumatoid arthritis, Pyoderma gangrenosum, Pressure ulcer, , Please select the most likely cause of ulceration for the scenario given. Each option may be used, once, more than once or not at all., , 72., , A 62 year old diabetic man presents with long standing plantar ulcer he has clinical, evidence of a charcot foot., You answered Marjolin's ulcer, The correct answer is Neuropathic ulcer, Plantar ulcers in association with peripheral neuropathy are often neuropathic. They, classically occur at pressure points., , 73., , A 66 year old female has long standing mixed arteriovenous ulcers of the lower leg. Over, the past 6 months one of the ulcers has become much worse and despite a number of, different topical therapies is increasing in size., Marjolin's ulcer, Marjolin's ulcer is a squamous cell carcinoma occurring at sites of chronic inflammation or, previous injury., , 74., , A 28 year old man undergoes a ileocaecal resection and end ileostomy for Crohn's disease., One year later he presents with a deep painful ulcer at his stoma site., You answered Marjolin's ulcer, The correct answer is Pyoderma gangrenosum, Pyoderma gangrenosum is associated with inflammatory bowel disease (this patient had a, stoma for crohns!). It is commonly found on lower limbs and described as being painful,, the size of an insect bite and growing. It looks like a margarita pizza (with a red base and
Page 2970 :
yellow topping!) Treatment involves steroids., Please rate this question:, , Discuss and give feedback, , Lower leg ulcers, Venous leg ulcers, , , , , , , , , , Most due to venous hypertension, secondary to chronic venous insufficiency (other causes, include calf pump dysfunction or neuromuscular disorders), Ulcers form due to capillary fibrin cuff or leucocyte sequestration, Features of venous insufficiency include oedema, brown pigmentation, lipodermatosclerosis,, eczema, Location above the ankle, painless, Deep venous insufficiency is related to previous DVT and superficial venous insufficiency is, associated with varicose veins, Doppler ultrasound looks for presence of reflux and duplex ultrasound looks at the anatomy/, flow of the vein, Management: 4 layer compression banding after exclusion of arterial disease or surgery, If fail to heal after 12 weeks or >10cm 2 skin grafting may be needed, , Marjolin's ulcer, , Image sourced from Wikipedia
Page 2971 :
, , , , Squamous cell carcinoma, Occurring at sites of chronic inflammation e.g; burns, osteomyelitis after 10-20 years, Mainly occur on the lower limb, , Arterial ulcers, , , , , , , Occur on the toes and heel, Painful, There may be areas of gangrene, Cold with no palpable pulses, Low ABPI measurements, , Neuropathic ulcers, , , , , , Commonly over plantar surface of metatarsal head and plantar surface of hallux, The plantar neuropathic ulcer is the condition that most commonly leads to amputation in, diabetic patients, Due to pressure, Management includes cushioned shoes to reduce callous formation, , Pyoderma gangrenosum, , Image sourced from Wikipedia, , , , , , Associated with inflammatory bowel disease/RA, Can occur at stoma sites, Erythematous nodules or pustules which ulcerate
Page 2973 :
A 43 year old lady is diagnosed as having a malignant lesion in the inferior aspect of her left breast., There is palpable axillary lymphadenopathy. What is the most appropriate course of action?, , Mastectomy and axillary node clearance, , Wide local excision and axillary node clearance, , Wide local excision and sentinel lymph node biopsy, , Image guided fine needle aspiration of the axillary nodes, , CT scanning of the chest, abdomen and pelvis, , Where axillary nodal involvement is suspected from the outset it is important to establish whether, this is the case prior to surgery. This is because, if axillary metastatic disease is present then the, correct management would be an axillary node clearance and this is irrespective of the surgical, plans for the breast primary. In the case of breast cancer, image guided FNAC is acceptable as it is, accurate and if carcinoma cells are identified at FNA then axillary node clearance can be performed., If FNAC is negative then a sentinel node biopsy should accompany excision of the primary tumour., Where the axilla is clinically clear on palpation and imaging then a sentinel lymph node biopsy, should accompany excision of the primary tumour., Please rate this question:, , Discuss and give feedback, , Next question, , Management of the axilla- breast cancer, Lymph node stage, Accurate staging of the axilla is an essential component of breast cancer management. Involvement, of the axillary nodes has an adverse effect on prognosis with 10 year survival reduced from 75% to, 25%[1]. Involvement of level 3 nodes carries the worst prognosis[2]. Historically, management of the, axilla ranged from limited level 1 axillary node excision through to full level 3 axillary nodal, clearances. Attempts to mimimise the morbidity of axillary node clearance led to targeted operations, including axillary nodal sampling and sentinel lymph node biopsy. The focus on sentinel lymph node, biopsy has led to more detailed pathological analysis of excised lymph nodes (e.g. using, immunohistochemistry). This has led to increasing focus on the develop of axillary nodal, micrometastasis. The presence of micrometastasis and its impact on survival is debated. In some, studies it seems to confer an increased risk of locoregional recurrence [3] and a reduction of disease, free survival [4], whilst in others it shows no overall impact[5]. It is important to distinguish between, micrometastasis and isolated tumour cells, as the latter do not have an adverse impact on, prognosis[6]. The need for definitive treatment of the axilla in women with positive sentinel nodes
Page 2974 :
was addressed by the ASCOG Z0011trial. In this trial women were randomised to either undergo, axillary node clearance or observation, groups were adjusted for other prognostic factors and, treatments. The investigators found no survival benefit in routinely undertaking axillary node, clearance where axillary nodal disease was limited in its extent., Regardless of the options in women with a low risk axilla, those individuals who have overt evidence, of axillary nodal involvement either through positive SLNB or preoperative USS and FNA, should still, receive axillary clearance as a standard of care., References, 1. Carter, C.L., C. Allen, and D.E. Henson, Relation of tumor size, lymph node status, and survival in, 24,740 breast cancer cases. Cancer, 1989. 63(1): p. 181-7., 2. Clark, G.M. Integrating prognostic factors. Breast Cancer Res Treat, 1992. 22(3): p. 187-91., 3. Lupe, K., et al. Ten-year locoregional recurrence risks in women with nodal micrometastatic, breast cancer staged with axillary dissection. Int J Radiat Oncol Biol Phys, 2011. 81(5): 681-8., 4. Park, D. et al. The prognostic impact of occult nodal metastasis in early breast carcinoma. Breast, Cancer Res Treat, 2009. 118(1): 57-66., 5. Galimberti, V., et al. Positive axillary sentinel lymph node: is axillary dissection always necessary?, Breast, 2011. 20 Suppl 3: S96-8., 6. Ahmad, N. and J. Park, Defining Semantic Structure Features for Content-Based Visual Object, Class Recognition. Journal of Imaging Science and Technology, 2011. 55(2)., Next question
Page 2975 :
Theme: Breast conditions, , A., B., C., D., E., F., G., H., I., , Mondors disease, Duct ectasia, Periductal mastitis, Lactational breast abscess, Fibroadenoma, Breast cyst, Intraductal papilloma, Atypical ductal hyperplasia, Radial scar, , Please select the most likely underlying diagnosis for the scenario given. Each option may be used, once, more than once or not at all., , 2., , A 20 year old lady presents with a mobile lump in the upper outer aspect of her right breast., On examination she has a firm mobile mass in the upper outer quadrant of her right breast., You answered Mondors disease, The correct answer is Fibroadenoma, Fibroadenomas account for 60% of discrete breast lesions in the 18-25 year age group. They, are mobile lesions. Core biopsy should be performed in lesions measuring more than 4cm in, diameter., , 3., , A 55 year old women presents with nipple discharge. On examination she has a slit like, retraction of the nipple in the centre of this area is a small amount of cheese like material., No discrete mass lesion is palpable in the underlying breast., You answered Mondors disease, The correct answer is Duct ectasia, Duct ectasia is a common alteration in the breast that occurs with aging. As the ducts, shorten and dilate a degree of symmetrical slit like retraction occurs. A small amount of, cheese like discharge may occur., , 4., , A 48 year old lady presents with discomfort in the right breast. On examination she has a, discrete soft fluctuant area in the upper outer quadrant of her right breast. A mammogram is, performed and a "halo sign" is seen by the radiologist., You answered Mondors disease
Page 2976 :
The correct answer is Breast cyst, Lesions such as breast cysts compress the underlying fat and produce a radiolucent area, (halo sign). If symptomatic, these cysts should be aspirated., Theme January 2014 exam, Please rate this question:, , Discuss and give feedback, , Next question, , Abberations of normal development and involution- breast, Fibroadenoma, Under the age of 25 years the breast is usually classified as undergoing development. Lobular units, are being formed and a dense stroma is formed within the breast tissue. This may result in the, development of fibroadenomas., As a group, fibroadenomas account for 13% of all palpable breast lesions. However, in women aged, 18-25 they constitute up to 60% of all palpable breast lesions. The are classified as juvenile,, common and giant. The former occur in early adolescence and the latter are characterised by a size, greater than 4cm. In young females with small fibroadenomas (less than 3cm on imaging) a policy of, watchful waiting without biopsy may be adopted. A size of greater than 4cm attracts a, recommendation for core biopsy to exclude a phyllodes tumour. The natural history of, fibroadenomas is that 10% will increase in size, 30% regress and the remainder stay the same. This, does not apply during pregnancy and lactation when they may increase in size substantially and, subsequently sequester milk., Some women may wish to have their fibroadenomas excised, they can usually be shelled out, through a circumareolar incision. Smaller lesions may be removed using a mammotome., Breast cysts, Palpable cysts constitute 15% of all breast lumps. They occur most frequently in perimenopausal, females and are caused by distended and involuted lobules., They may be readily apparent on clinical examination as soft, fluctuant swellings. It is important to, exclude the presence of an underlying mass lesion. On imaging they will usually show a "halo, appearance" on mammography. Ultrasound will confirm the fluid filled nature of the cyst., Symptomatic cysts may be aspirated and following aspiration the breast re-examined to ensure that, the lump has gone., Duct ectasia, As women progress through the menopause the breast ducts shorten and dilate. In some women, this may cause a cheese like nipple discharge and slit like retraction of the nipple. No specific, treatment is required., Next question
Page 2977 :
A 43 year old lady has recently undergone a wide local excision and sentinel lymph node biopsy for, carcinoma of the breast. Of the factors listed below, which will provide the most important prognostic, information?, , Mitotic number, , Grade, , Nodal status, , Size, , Oestrogen receptor status, Nodal status is the single most important prognostic factor in breast cancer., , Theme from April 2012 Exam, Theme from January 2013 Exam, Theme from April 2014 Exam, Nodal status is important because it serves as a marker of tumour metastatic potential. This, translates to survival advantages of up to 40% at five years. Both grade and size are of secondary, importance as they both less concerning in the absence of nodal involvement., Please rate this question:, , Discuss and give feedback, , Next question, , Breast cancer, , , , Commoner in the older age group, Invasive ductal carcinomas are the most common type. Some may arise as a result, of ductal carcinoma in situ (DCIS). There are associated carcinomas of special type e.g., Tubular that may carry better prognosis.
Page 2978 :
, , , , , , The pathological assessment involves assessment of the tumour and lymph nodes, sentinel, lymph node biopsy is often used to minimise the morbidity of an axillary dissection., Treatment, typically this is either wide local excision or mastectomy. There are many sub, types of both of these that fall outside of the MRCS. Some key rules to bear in mind., Whatever operation is contemplated the final cosmetic outcome does have a bearing. A, woman with small breasts and a large tumour will tend to fare better with mastectomy, even, if clear pathological and clinical margins can be obtained. Conversely a women with larger, breasts may be able to undergo breast conserving surgery even with a relatively large, primary lesion (NB tumours >4cm used to attract recommendation for mastectomy). For, screen detected and impalpable tumour image guidance will be necessary., Reconstruction is always an option following any resectional procedure. However, its exact, type must be tailored to age and co-morbidities of the patient. The main operations in, common use include latissimus dorsi myocutaneous flap and sub pectoral implants. Women, wishing to avoid a prosthesis may be offered TRAM or DIEP flaps., , Surgical options, Mastectomy vs Wide local excision, , Mastectomy, , Wide Local Excision, , Multifocal tumour, , Solitary lesion, , Central tumour, , Peripheral tumour, , Large lesion in small breast, , Small lesion in large breast, , DCIS >4cm, , DCIS <4cm, , Patient Choice, , Patient choice, , Central lesions may be managed using breast conserving surgery where an acceptable cosmetic, result may be obtained, this is rarely the case in small breasts, A compelling indication for mastectomy, a larger tumour that would be unsuitable for breast, conserving surgery
Page 2979 :
Image sourced from Wikipedia, , Whatever surgical option is chosen the aim should be to have a local recurrence rate of 5% or less, at 5 years [1]., Nottingham Prognostic Index, The Nottingham Prognostic Index can be used to give an indication of survival. In this system the, tumour size is weighted less heavily than other major prognostic parameters., Calculation of NPI, Tumour Size x 0.2 + Lymph node score(From table below)+Grade score(From table below)., , Score, , Lymph nodes involved, , Grade, , 1, , 0, , 1, , 2, , 1-3, , 2, , 3, , >3, , 3
Page 2980 :
Prognosis, , Score, , Percentage 5 year survival, , 2.0 to 2.4, , 93%, , 2.5 to 3.4, , 85%, , 3.5 to 5.4, , 70%, , >5.4, , 50%, , This data was originally published in 1992. It should be emphasised that other factors such as, vascular invasion and receptor status also impact on survival and are not included in this data and, account for varying prognoses often cited in the literature., References, Surgical guidelines for the management of breast cancer, Association of Breast Surgery at BASO, 2009, Eur J Surg Oncol (2009), doi:10.1016/j.ejso.2009.01.008, Next question
Page 2981 :
Theme: Management of nipple discharge, , A., B., C., D., E., F., G., H., , Prescribe danazol, Microdochectomy, Total duct excision, Cytology of duct fluid, Core biopsy, Prescribe co-amoxiclav, Reassure and discharge, Mastectomy, , What is the best management for each nipple discharge presentation? Each option may be used, once, more than once or not at all., , 6., , A 23 year old women with greenish nipple discharge on one occasion. Clinical examination, of the breast is normal. Ultrasound report is U1., You answered Prescribe danazol, The correct answer is Reassure and discharge, Theme from April 2016 Exam, This is likely to be simple duct ectasia and U1 (normal USS) coupled with normal, examination would favor discharge from clinic. Mammography is generally unhelpful in, this age group, , 7., , A 43 year old women has had recurrent episodes of periductal mastitis. She has received, multiple courses of antibiotics and is troubled by persisting green nipple discharge. Clinical, examination reveals green nipple discharge, but no discrete lump. Imaging with, mammography and ultrasound is reassuring (U2, M2), You answered Prescribe danazol, The correct answer is Total duct excision, This woman has troublesome duct ectasia and total duct excision is warranted., , 8., , A 55 year old women complains of nipple discharge. This was blood stained on one, occasion. But not subsequently. Clinical examination shows clear fluid but no discrete, lump. Imaging with ultrasound and mammography is normal., You answered Prescribe danazol
Page 2982 :
The correct answer is Microdochectomy, Although this is likely to be benign disease, her age coupled with an episode of blood, stained discharge would attract a recommendation for microdochectomy. She may have an, intraductal papilloma. But the concern would be DCIS., Please rate this question:, , Discuss and give feedback, , Next question, , Nipple discharge, Causes of nipple discharge, , Physiological, , During breast feeding, , Galactorrhoea, , Commonest cause may be response to emotional events, drugs such as, histamine receptor antagonists are also implicated, , Hyperprolactinaemia, , , , , , , Commonest type of pituitary tumour, Microadenomas <1cm in diameter, Macroadenomas >1cm in diameter, Pressure on optic chiasm may cause bitemporal hemianopia, , Mammary duct, ectasia, , , , , , , Dilatation breast ducts., Most common in menopausal women, Discharge typically thick and green in colour, Most common in smokers, , Carcinoma, , , , , Often blood stained, May be underlying mass or axillary lymphadenopathy, , Intraductal papilloma, , , , , , Commoner in younger patients, May cause blood stained discharge, There is usually no palpable lump, , Assessment of patients
Page 2983 :
, , , Examine breast and determine whether there is mass lesion present, All mass lesions should undergo Triple assessment., , Reporting of investigations, Where a mass lesion is suspected or investigations are requested these are prefixed using a system, that denotes the investigation type e.g. M for mammography, followed by a numerical code as, shown below:, , 1, , No abnormality, , 2, , Abnormality with benign features, , 3, , Indeterminate probably benign, , 4, , Indeterminate probably malignant, , 5, , Malignant, , Management of non malignant nipple discharge, , , , , , Exclude endocrine disease, Nipple cytology unhelpful, Smoking cessation advice for duct ectasia, For duct ectasia with severe symptoms, total duct excision may be warranted., Next question
Page 2984 :
Theme: Breast disease, , A., B., C., D., E., F., G., H., I., , Ductal carcinoma in situ, Lobular carcinoma in situ, Invasive ductal carcinoma, Invasive lobular carcinoma, Inflammatory carcinoma, Phyllodes tumour, Paget's disease of the nipple, Fibroadenoma, Mucinous breast carcinoma, , From the list please select the most likely diagnosis for the scenario given. Each diagnosis may be, used once, more than once or not at all., , 9., , A 32 year old Indian lady presents with breast lump. She has a 4 month old child., Clinically she has jaundice and there is erythema of the left breast., You answered Ductal carcinoma in situ, The correct answer is Inflammatory carcinoma, Inflammatory breast cancers have an aggressive nature. Dissemination occurs early and is, more resistant to adjuvent treatments than other types of breast cancer. Often occurs in, pregnancy or lactation., , 10., , A 72 year old female presents with a painless breast lump. Clinically she has a 4cm, diameter irregular breast mass, with no other palpable masses., You answered Ductal carcinoma in situ, The correct answer is Invasive ductal carcinoma, A post menopausal woman is more likely to have a ductal carcinoma and they tend to, occur at a single focus within the breast., , 11., , A 72 year old woman presents with 2 breast lumps. She has a history of breast cancer in, the opposite breast 5 years ago., You answered Ductal carcinoma in situ, The correct answer is Invasive lobular carcinoma
Page 2985 :
This is likely to be an invasive lobular carcinoma, mainly due to the multifocal lesions and, the history of previous breast cancer in the opposite breast., Please rate this question:, , Discuss and give feedback, , Next question, , Breast cancer, , , , , , , , , Commoner in the older age group, Invasive ductal carcinomas are the most common type. Some may arise as a result, of ductal carcinoma in situ (DCIS). There are associated carcinomas of special type e.g., Tubular that may carry better prognosis., The pathological assessment involves assessment of the tumour and lymph nodes, sentinel, lymph node biopsy is often used to minimise the morbidity of an axillary dissection., Treatment, typically this is either wide local excision or mastectomy. There are many sub, types of both of these that fall outside of the MRCS. Some key rules to bear in mind., Whatever operation is contemplated the final cosmetic outcome does have a bearing. A, woman with small breasts and a large tumour will tend to fare better with mastectomy, even, if clear pathological and clinical margins can be obtained. Conversely a women with larger, breasts may be able to undergo breast conserving surgery even with a relatively large, primary lesion (NB tumours >4cm used to attract recommendation for mastectomy). For, screen detected and impalpable tumour image guidance will be necessary., Reconstruction is always an option following any resectional procedure. However, its exact, type must be tailored to age and co-morbidities of the patient. The main operations in, common use include latissimus dorsi myocutaneous flap and sub pectoral implants. Women, wishing to avoid a prosthesis may be offered TRAM or DIEP flaps., , Surgical options, Mastectomy vs Wide local excision, , Mastectomy, , Wide Local Excision, , Multifocal tumour, , Solitary lesion, , Central tumour, , Peripheral tumour, , Large lesion in small breast, , Small lesion in large breast
Page 2986 :
Mastectomy, , Wide Local Excision, , DCIS >4cm, , DCIS <4cm, , Patient Choice, , Patient choice, , Central lesions may be managed using breast conserving surgery where an acceptable cosmetic, result may be obtained, this is rarely the case in small breasts, A compelling indication for mastectomy, a larger tumour that would be unsuitable for breast, conserving surgery, , Image sourced from Wikipedia, , Whatever surgical option is chosen the aim should be to have a local recurrence rate of 5% or less, at 5 years [1]., Nottingham Prognostic Index, The Nottingham Prognostic Index can be used to give an indication of survival. In this system the, tumour size is weighted less heavily than other major prognostic parameters., Calculation of NPI, Tumour Size x 0.2 + Lymph node score(From table below)+Grade score(From table below).
Page 2987 :
Score, , Lymph nodes involved, , Grade, , 1, , 0, , 1, , 2, , 1-3, , 2, , 3, , >3, , 3, , Prognosis, , Score, , Percentage 5 year survival, , 2.0 to 2.4, , 93%, , 2.5 to 3.4, , 85%, , 3.5 to 5.4, , 70%, , >5.4, , 50%, , This data was originally published in 1992. It should be emphasised that other factors such as, vascular invasion and receptor status also impact on survival and are not included in this data and, account for varying prognoses often cited in the literature., References, Surgical guidelines for the management of breast cancer, Association of Breast Surgery at BASO, 2009, Eur J Surg Oncol (2009), doi:10.1016/j.ejso.2009.01.008, Next question
Page 2990 :
A 72 year old female is found to have a malignant lesion in her left arm. She had a mastectomy of, the left breast 10 years ago and has chronic lymph oedema of the left arm. What is the most likely, cause of the malignancy?, , Lymphangiosarcoma, , Lymphoma, , Myeloma, , Angiomyolipoma, , Giant cell tumour, , Lymphangiosarcoma is a rare condition arising as a result of chronic oedema. It is an aggressive, malignancy., Please rate this question:, , Discuss and give feedback, , Next question, , Lymphoedema, , , , , Due to impaired lymphatic drainage in the presence of normal capillary function., Lymphoedema causes the accumulation of protein rich fluid, subdermal fibrosis and dermal, thickening., Characteristically fluid is confined to the epifascial space (skin and subcutaneous tissues);, muscle compartments are free of oedema. It involves the foot, unlike other forms of oedema., There may be a 'buffalo hump' on the dorsum of the foot and the skin cannot be pinched due, to subcutaneous fibrosis., , Causes of lymphoedema, , Primary, , , , , , Congenital < 1 year: sporadic, Milroy's disease, Onset 1-35 years: sporadic, Meige's disease, > 35 years: Tarda, , Secondary, , , , Bacterial/fungal/parasitic infection (filariasis)
Page 2991 :
, , , , , , Lymphatic malignancy, Radiotherapy to lymph nodes, Surgical resection of lymph nodes, DVT, Thrombophlebitis, , Indications for surgery, , , , , Marked disability or deformity from limb swelling, Lymphoedema caused by proximal lymphatic obstruction with patent distal lymphatics, suitable for a lymphatic drainage procedure, Lymphocutaneous fistulae and megalymphatics, , Procedures, , Homans operation, , Reduction procedure with preservation of overlying skin (which must be in, good condition). Skin flaps are raised and the underlying tissue excised., Limb circumference typically reduced by a third., , Charles operation, , All skin and subcutaneous tissue around the calf are excised down to the, deep fascia. Split skin grafts are placed over the site. May be performed if, overlying skin is not in good condition. Larger reduction in size than with, Homans procedure., , Lymphovenous, anastamosis, , Identifiable lymphatics are anastomosed to sub dermal venules. Usually, indicated in 2% of patients with proximal lymphatic obstruction and normal, distal lymphatics., Next question
Page 2992 :
A 58 year old male is referred to endocrinology clinic for a parathyroidectomy by the F1 in medicine., His corrected calcium is 2.85 (2.2-2.6), PTH 7.5 (3-7) and 24h urinary calcium is 1.5 (2.5-7.5). What, is the diagnosis?, , Primary hyperparathyroidism, , Secondary hyperparathyroidism, , Tertiary hyperparathyroidism, , Familial hypocalciuric hypercalcaemia, , Hypercalacemia associated with malignancy, , This F1 should have spoken to his senior. This patient has familial hypocalciuric hypercalcaemia,, which requires no further action. A calcium to creatinine clearance ratio of <0.01 will confirm this, diagnosis., Please rate this question:, , Discuss and give feedback, , Next question, , Parathyroid glands and disorders of calcium metabolism, Hyperparathyroidism, , Disease type, , Primary, hyperparathyroidism, , Hormone profile, , , , , , PTH (Elevated), Ca2+(Elevated), Phosphate (Low), Urine calcium :, creatinine clearance, ratio > 0.01, , Clinical features, , Cause, , May be, asymptomatic if, mild, Recurrent, abdominal pain, (pancreatitis, renal, colic), Changes to, emotional or, cognitive state, , Most cases due to, solitary adenoma, (80%), multifocal, disease occurs in 1015% and parathyroid, carcinoma in 1% or, less
Page 2993 :
Disease type, , Secondary, hyperparathyroidism, , Hormone profile, , , , , , Tertiary, hyperparathyroidism, , , , , , , , , Clinical features, , Cause, , PTH (Elevated), Ca2+ (Low or, normal), Phosphate, (Elevated), Vitamin D levels, (Low), , May have few, symptoms, Eventually may, develop bone, disease, osteitis, fibrosa cystica and, soft tissue, calcifications, , Parathyroid gland, hyperplasia occurs as, a result of low, calcium, almost, always in a setting of, chronic renal failure, , Ca2+(Normal or, high), PTH (Elevated), Phosphate levels, (Decreased or, Normal), Vitamin D (Normal, or decreased), Alkaline, phosphatase, (Elevated), , Metastatic, calcification, Bone pain and /, or fracture, Nephrolithiasis, Pancreatitis, , Occurs as a result of, ongoing hyperplasia, of the parathyroid, glands after, correction of, underlying renal, disorder, hyperplasia, of all 4 glands is, usually the cause, , Differential diagnoses, It is important to consider the rare but relatively benign condition of benign familial hypocalciuric, hypercalcaemia, caused by an autosomal dominant genetic disorder. Diagnosis is usually made by, genetic testing and concordant biochemistry (urine calcium : creatinine clearance ratio <0.01distinguished from primary hyperparathyroidism)., Treatment, Primary hyperparathyroidism, Indications for surgery, , , , , , , , , , Elevated serum Calcium > 1mg/dL above normal, Hypercalciuria > 400mg/day, Creatinine clearance < 30% compared with normal, Episode of life threatening hypercalcaemia, Nephrolithiasis, Age < 50 years, Neuromuscular symptoms, Reduction in bone mineral density of the femoral neck, lumbar spine, or distal radius of more, than 2.5 standard deviations below peak bone mass (T score lower than -2.5)
Page 2994 :
Secondary hyperparathyroidism, Usually managed with medical therapy., Indications for surgery in secondary (renal) hyperparathyroidism:, , , , , Bone pain, Persistent pruritus, Soft tissue calcifications, , Tertiary hyperparathyroidism, Allow 12 months to elapse following transplant as many cases will resolve, The presence of an autonomously functioning parathyroid gland may require surgery. If the culprit, gland can be identified then it should be excised. Otherwise total parathyroidectomy and reimplantation of part of the gland may be required., References, 1. Pitt S et al. Secondary and Tertiary Hyperparathyroidism, State of the Art Surgical, Management.Surg Clin North Am 2009 Oct;89(5):1227-39., 2. MacKenzie-Feder J et al. Primary Hyperparathyroidism: An Overview. Int J Endocrinol 2011;, 2011: 251410., Next question
Page 2995 :
Theme: Management of breast cancer, , A., B., C., D., E., F., G., H., , Simple mastectomy alone, Radical mastectomy alone, Simple mastectomy and sentinel lymph node biopsy, Wide local excision and sentinel lymph node biopsy, Simple mastectomy and axillary node clearance, Radical mastectomy and axillary node clearance, Wide local excision and axillary node clearance, Wide local excision alone, , Please select the most appropriate treatment for the situation described. Each option may be used, once, more than once or not at all., , 15., , A 44 year old lady presents with a mass in the upper outer quadrant of her right breast., Imaging, histology and clinical examination confirm a 1.5cm malignant mass lesion with, no clinical evidence of axillary nodal disease., You answered Simple mastectomy alone, The correct answer is Wide local excision and sentinel lymph node biopsy, A small peripheral lesion such as this would usually be suitable for breast conserving, surgery. Since imaging and clinical examination is not suspicious for axillary disease, a, sentinel lymph node biopsy should be performed., , 16., , A 44 year old lady presents with a mass lesion in the upper outer quadrant of the left, breast. On clinical examination she has a 2cm mass lesion which on core biopsy is, demonstrated to have invasive ductal carcinoma. An FNA of a bulky axillary lymph node, contains malignant cells., You answered Simple mastectomy alone, The correct answer is Wide local excision and axillary node clearance, Although the primary lesion is small enough for breast conserving surgery, the presence of, overt axillary lymph node metastasis will attract a recommendation for axillary node, clearance., , 17., , A 39 year old lady presents with a mass lesion in her right breast. Clinical examination,, biopsy and imaging confirm a 2.5 cm lesion in the upper inner quadrant of her right breast, and a 1.5 cm lesion at the central aspect of the same breast. Her axilla shows, lymphadenopathy and a fine needle aspirate from the node shows malignant cells.
Page 2996 :
You answered Simple mastectomy alone, The correct answer is Simple mastectomy and axillary node clearance, A combination of established axillary disease and multifocal invasive lesions attracts an, indication for mastectomy and axillary clearance. A radical mastectomy is less frequently, indicated in modern surgical practice, disease that is locally advanced is often best, downstaged using medical therapy, rather than embarking on the operations for breast, cancer that were first popularised over 100 years ago., Please rate this question:, , Discuss and give feedback, , Next question, , Breast cancer management, , , , , , Surgery is performed in most patients suffering from breast cancer., Chemotherapy may be used to downstage tumours and allow breast conserving surgery., Hormonal therapy may also be used for the same purposes., Radiotherapy is given to all patients who have undergone breast conserving surgery., Patients who have undergone mastectomy may be offered a reconstructive procedure either, in conjunction with their primary resection or as a staged procedure at a later date., , Surgical options, Mastectomy vs Wide local excision, , Mastectomy, , Wide Local Excision, , Multifocal tumour, , Solitary lesion, , Central tumour, , Peripheral tumour, , Large lesion in small breast, , Small lesion in large breast, , DCIS >4cm, , DCIS <4cm
Page 2997 :
Patient Choice, , Patient choice, , Central lesions may be managed using breast conserving surgery, where an acceptable cosmetic, result may be obtained, this is rarely the case in small breasts, Axillary disease, , , , , As a minimum, all patients with invasive breast cancer should have their axilla staged. In, those who do not have overt evidence of axillary nodal involvement this can be undertaken, using sentinel lymph node biopsy., Patients with a positive sentinel lymph node biopsy or who have imaging and cytological or, histological evidence of axillary nodal metastasis should undergo axillary node clearance., Axillary node clearance is associated with the development of lymphoedema, increased risk, of cellulitis and frozen shoulder., Next question
Page 2998 :
A 50 year old lady is commenced on tamoxifen for the treatment of an oestrogen receptor positive, breast cancer. Which of the following malignancies are associated with tamoxifen use?, , Adenocarcinoma of the colon, , Hodgkins lymphoma, , Adenocarcinoma of the lung, , Ovarian cancer, , Endometrial cancer, , Tamoxifen is an oestrogen receptor antagonist in breast tissues. However, at other sites, such as, the endometrium it may act as an agonist. Hence the reason for increasing risk of endometrial, cancer., Please rate this question:, , Discuss and give feedback, , Next question, , Tamoxifen, , , , , , , , Synthetic partial oestrogen agonist, acts primarily by binding to the oestrogen receptor., Half life of 7 days, takes 4 weeks for drug to reach plasma steady state., Should usually be considered in patients with oestrogen receptor positive tumours, (alternative agents may be preferred in some groups)., Although antagonistic with respects to breast tissue tamoxifen may serve as an agonist at, other sites. Therefore risk of endometrial cancer is increased, preservation of bone density, and decreased cardiovascular risks., Climateric side effects are common, 3% stop taking the drug because of these., Aromatase inhibitors are an alternative class of drugs, these work by blocking the peripheral, aromatization of androgens (post menopausal women produce oestrogens in this way). They, may treat cancers for which tamoxifen is no longer effective., Next question
Page 2999 :
Theme: Thyroid nodules, , A., B., C., D., E., F., G., H., , Toxic adenoma, Anaplastic carcinoma of thyroid, Follicular carcinoma of thyroid, Papillary carcinoma of thyroid, Medullary carcinoma of thyroid, Thyroid lymphoma, Multinodular goitre, Parathyroid gland tumour, , For each scenario please select the most likely underlying diagnosis. Each option may be used, once, more than once or not at all., , 19., , A 52 year old woman with known Hashimotos thyroiditis presents with a neck swelling., She describes it as rapidly increasing in size over 3 months and she complains of, dysphagia to solids. On examination there is an asymmetrical swelling of the thyroid, gland., You answered Toxic adenoma, The correct answer is Thyroid lymphoma, Thyroid lymphoma (Non Hodgkin's B cell lymphoma) is rare. It should be considered in, patients with a background of Hashimoto's thyroiditis and a rapid growth in size of the, thyroid gland. Diagnosis can be made with core needle biopsy; however an incisional, biopsy may be needed. Radiotherapy is the main treatment option., , 20., , A 52 year old woman presents with a neck swelling. On examination she is noted to have, single nodule on the thyroid gland. A CXR shows two mass lesions., You answered Toxic adenoma, The correct answer is Follicular carcinoma of thyroid, A solitary nodule with signs of haematogenous spread indicates a follicular tumour. Note, that papillary tumours tend to be multinodular and spread via the lymphatic, system.Lymphatic spread from a papillary thyroid cancer is nearly always to neck nodes in, the first instance and mediastinal lymphadenopathy is vanishingly rare. Lung lesions are, typically synonymous with haematogenous metastasis of which a follicular lesion is the, most likely culprit., , 21., , A 52 year old woman presents with a neck swelling. Her GP reports that her TSH value is, low at 0.01. A scintigraphy demonstrates a hot nodule.
Page 3000 :
Toxic adenoma, This lady has thyrotoxicosis (low TSH) and a hot solitary nodule indicating a toxic, adenoma. Thyroid cancer rarely causes thyrotoxicosis or hot nodules., Please rate this question:, , Discuss and give feedback, , Next question, , Thyroid disease, Patients may present with a number of different manifestations of thyroid disease. They can be, broadly sub classified according to whether they are euthyroid or have clinical signs of thyroid, dysfunction. In addition it needs to be established whether they have a mass or not., Assessment, , , , , , History, Examination including USS, If a nodule is identified then it should be sampled ideally via an image guided fine needle, aspiration, Radionucleotide scanning is of limited use, , Thyroid Tumours, , , , , , , Papillary carcinoma, Follicular carcinoma, Anaplastic carcinoma, Medullary carcinoma, Lymphoma's, , Multinodular goitre, , , , , , One of the most common reasons for presentation, Provided the patient is euthyroid and asymptomatic and no discrete nodules are seen, they, can be reassured., In those with compressive symptoms surgery is required and the best operation is a total, thyroidectomy., Sub total resections were practised in the past and simply result in recurrent disease that, requires a difficult revisional resection.
Page 3001 :
Endocrine dysfunction, , , , , In general these patients are managed by physicians initially., Surgery may be offered alongside radio iodine for patients with Graves disease that fails with, medical management or in patients who would prefer not to be irradiated (e.g. pregnant, women)., Patients with hypothyroidism do not generally get offered a thyroidectomy. Sometimes, people inadvertently get offered resections during the early phase of Hashimotos thyroiditis,, however, with time the toxic phase passes and patients can simply be managed with, thyroxine., , Complications following surgery, , , , , Anatomical such as recurrent laryngeal nerve damage., Bleeding. Owing to the confined space haematoma's may rapidly lead to respiratory, compromise owing to laryngeal oedema., Damage to the parathyroid glands resulting in hypocalcaemia., , Further sources of information, 1. http://www.acb.org.uk/docs/TFTguidelinefinal.pdf- Association of Clinical Biochemistry guidelines, for thyroid function tests., 2. British association of endocrine surgeons website- http://www.baets.org.uk, Next question
Page 3002 :
Which investigation is best for initial assessment of recurrence of follicular carcinoma of the thyroid?, , Free T4, , Thyroid stimulating hormone, , Scintigraphy, , Serum thyroglobulin, , USS thyroid gland, , Elevated thyroglobulin levels raises suspicion of recurrence., Please rate this question:, , Discuss and give feedback, , Next question, , Thyroid malignancy, Papillary carcinoma, , , , , , Commonest sub-type, Accurately diagnosed on fine needle aspiration cytology, Histologically, they may demonstrate psammoma bodies (areas of calcification) and so, called 'orphan Annie' nuclei, They typically metastasise via the lymphatics and thus laterally located apparently ectopic, thyroid tissue is usually a metastasis from a well differentiated papillary carcinoma, , Follicular carcinoma, , , , , , Are less common than papillary lesions, Like papillary tumours, they may present as a discrete nodule. Although they appear to be, well encapsulated macroscopically there is invasion on microscopic evaluation, Lymph node metastases are uncommon and these tumours tend to spread, haematogenously. This translates into a higher mortality rate, Follicular lesions cannot be accurately diagnosed on fine needle aspiration cytology and thus, all follicular FNA's (THY 3f) will require at least a hemi thyroidectomy
Page 3003 :
Anaplastic carcinoma, , , , Less common and tend to occur in elderly females, Disease is usually advanced at presentation and often only palliative decompression and, radiotherapy can be offered., , Medullary carcinoma, , , , , , These are tumours of the parafollicular cells ( C Cells) and are of neural crest origin., The serum calcitonin may be elevated which is of use when monitoring for recurrence., They may be familial and occur as part of the MEN -2A disease spectrum., Spread may be either lymphatic or haematogenous and as these tumours are not derived, primarily from thyroid cells they are not responsive to radioiodine., , Lymphoma, , , , These respond well to radiotherapy, Radical surgery is unnecessary once the disease has been diagnosed on biopsy material., Such biopsy material is not generated by an FNA and thus a core biopsy has to be obtained, (with care!)., Next question
Page 3004 :
A 33 year old lady attends the clinic with a 3 month history of palpitations and irritability. Her thyroid, function, PTH and calcium are measured:, Thyroid function, Free T4, , 40 pmol/L, , TSH, , < 0.1 miu/L, , Free T3, , 25 p mol/L (normal 3.5-7.7 p mol/L), , PTH, , 10pg/ml (normal 10-55pg/ml), , (Normal values listed in reference range link), What is the most likely diagnosis?, , Hypothyroidism, , Hyperthyroidism, , Hypoparathyroidism, , Hyperparathyroidism, , Euthyroid, , Theme from April 2012 Exam, Elevated T4 and suppressed TSH makes this the most likely diagnosis. The PTH level is normal., Please rate this question:, , Discuss and give feedback, , Next question, , Hyperthyroidism, Causes of hyperthyroidism include:, , , , , , Diffuse toxic goitre (Graves Disease), Toxic nodular goitre, Toxic nodule, Rare causes
Page 3005 :
Graves disease, Graves disease is characterised by a diffuse vascular goitre that appears at the same time as the, clinical manifestations of hyperthyroidism. It is commonest in younger females and may be, associated with eye signs. Thyrotoxic symptoms will predominate. Up to 50% of patients will have a, familial history of autoimmune disorders. The glandular hypertrophy and hyperplasia occur as a, result of the thyroid stimulating effects of the TSH receptor antibodies., Toxic nodular goitre, In this disorder the goitre is present for a long period of time prior to the development of clinical, symptoms. In most goitres the nodules are inactive and in some cases it is the internodular tissue, that is responsible for the hyperthyroidism., Toxic nodule, Overactive, autonomously functioning nodule. It may occur as part of generalised nodularity or be a, true toxic adenoma. The TSH levels are usually low as the autonomously functioning thyroid tissue, will exert a negative feedback effect., Signs and symptoms, , Symptoms, , Signs, , Lethargy, , Tachycardia, , Emotionally labile, , Agitation, , Heat intolerance, , Hot, moist palms, , Weight loss, , Exopthalmos, , Excessive appetite, , Thyroid goitre and bruit, , Palpitations, , Lid lag/retraction, , Diagnosis, The most sensitive test for diagnosing hyperthyroidism is plasma T3 (which is raised). Note in, hypothyroidism the plasma T4 and TSH are the most sensitive tests. A TSH level of <0.5U/L, suggests hyperthyroidism. TSH receptor antibodies may be tested for in the diagnosis of Graves., Treatment, First line treatment for Graves disease is usually medical and the block and replace regime is the, favored option. Carbimazole is administered at higher doses and thyroxine is administered orally., Patient are maintained on this regime for between 6 and 12 months. Attempts are then made to
Page 3006 :
wean off medication. Where relapse then occurs the options are between ongoing medical therapy,, radioiodine or surgery., Next question
Page 3007 :
A 23 year old lady has Graves disease that has relapsed on stopping anti thyroid drugs, radioiodine, is offered as the next treatment by the endocrinologists. Which statement is false?, , Close contact with children is not permitted for up to 4 weeks following treatment, , 15% of patients with opthalmopathy will see worsening of eye signs, , Symptomatic improvement takes 6-8 weeks, , Up to 80% of patients will become hypothyroid, , It increases the risk of parathyroid carcinoma, Radio-iodine- may worsen opthalmopathy, contraindicated in pregnancy and those wishing to, concieve within 6 months., Radioiodine vs. Surgery, , Surgery, , Radioiodine, , Symptomatic improvement within 10 days, , Symptomatic improvement takes up to 2, months, , No effect on opthalmopathy, , Eye signs may worsen, , Risk of damage to adjacent anatomical, structures, , No risk of anatomical damage, , No restrictions on contact, , No contact with children for 4 weeks, , Please rate this question:, , Discuss and give feedback, , Next question, , Thyroid disease
Page 3008 :
Patients may present with a number of different manifestations of thyroid disease. They can be, broadly sub classified according to whether they are euthyroid or have clinical signs of thyroid, dysfunction. In addition it needs to be established whether they have a mass or not., Assessment, , , , , , History, Examination including USS, If a nodule is identified then it should be sampled ideally via an image guided fine needle, aspiration, Radionucleotide scanning is of limited use, , Thyroid Tumours, , , , , , , Papillary carcinoma, Follicular carcinoma, Anaplastic carcinoma, Medullary carcinoma, Lymphoma's, , Multinodular goitre, , , , , , One of the most common reasons for presentation, Provided the patient is euthyroid and asymptomatic and no discrete nodules are seen, they, can be reassured., In those with compressive symptoms surgery is required and the best operation is a total, thyroidectomy., Sub total resections were practised in the past and simply result in recurrent disease that, requires a difficult revisional resection., , Endocrine dysfunction, , , , , In general these patients are managed by physicians initially., Surgery may be offered alongside radio iodine for patients with Graves disease that fails with, medical management or in patients who would prefer not to be irradiated (e.g. pregnant, women)., Patients with hypothyroidism do not generally get offered a thyroidectomy. Sometimes, people inadvertently get offered resections during the early phase of Hashimotos thyroiditis,, however, with time the toxic phase passes and patients can simply be managed with, thyroxine., , Complications following surgery
Page 3009 :
, , , , Anatomical such as recurrent laryngeal nerve damage., Bleeding. Owing to the confined space haematoma's may rapidly lead to respiratory, compromise owing to laryngeal oedema., Damage to the parathyroid glands resulting in hypocalcaemia., , Further sources of information, 1. http://www.acb.org.uk/docs/TFTguidelinefinal.pdf- Association of Clinical Biochemistry guidelines, for thyroid function tests., 2. British association of endocrine surgeons website- http://www.baets.org.uk, Next question
Page 3010 :
Theme: Thyroid disease, , A., B., C., D., E., F., G., H., , Papillary carcinoma, Follicular carcinoma, Multinodular goitre, Parathyroid adenoma, Anaplastic thyroid carcinoma, Medullary carcinoma, Toxic nodule, Graves disease, , Please select the most likely thyroid lesion for the scenario given. Each option may be used once,, more than once or not at all., , 25., , A 34 year old female presents with a thyroid nodule. She has a family history of thyroid, disease and both her sisters have undergone total thyroidectomies. Her past medical, history includes hypertension which has been difficult to manage., You answered Papillary carcinoma, The correct answer is Medullary carcinoma, This is a typical scenario for medullary carcinoma in which a phaeochromocytoma may, also be present. It may be inherited in an autosomal dominant fashion and affected family, members may be offered prophylactic thyroidectomy., , 26., , A 46 year old man is admitted to hospital with a femoral shaft fracture that occurred, suddenly whilst he was out walking his dog. On examination there is no neurovascular, deficit distal to the fracture site. He has a large firm nodule in the left lobe of the thyroid,, there is no associated lymphadenopathy., You answered Papillary carcinoma, The correct answer is Follicular carcinoma, Follicular carcinomas may metastasise haematogenously (often to bone) where they may, give rise to pathological fractures as in this case., , 27., , An 18 year old female presents with 3 nodules in the right lobe of the thyroid. Clinically, she is euthyroid and there is associated cervical lymphadenopathy. She has no family, history of thyroid disease., Papillary carcinoma
Page 3011 :
Papillary thyroid cancers are the most common type of thyroid cancer and are the more, common in females (M:F=1:3). Papillary tumours are more likely to develop lymphatic, spread than follicular tumours., Please rate this question:, , Discuss and give feedback, , Next question, , Thyroid disease, Patients may present with a number of different manifestations of thyroid disease. They can be, broadly sub classified according to whether they are euthyroid or have clinical signs of thyroid, dysfunction. In addition it needs to be established whether they have a mass or not., Assessment, , , , , , History, Examination including USS, If a nodule is identified then it should be sampled ideally via an image guided fine needle, aspiration, Radionucleotide scanning is of limited use, , Thyroid Tumours, , , , , , , Papillary carcinoma, Follicular carcinoma, Anaplastic carcinoma, Medullary carcinoma, Lymphoma's, , Multinodular goitre, , , , , , One of the most common reasons for presentation, Provided the patient is euthyroid and asymptomatic and no discrete nodules are seen, they, can be reassured., In those with compressive symptoms surgery is required and the best operation is a total, thyroidectomy., Sub total resections were practised in the past and simply result in recurrent disease that, requires a difficult revisional resection.
Page 3012 :
Endocrine dysfunction, , , , , In general these patients are managed by physicians initially., Surgery may be offered alongside radio iodine for patients with Graves disease that fails with, medical management or in patients who would prefer not to be irradiated (e.g. pregnant, women)., Patients with hypothyroidism do not generally get offered a thyroidectomy. Sometimes, people inadvertently get offered resections during the early phase of Hashimotos thyroiditis,, however, with time the toxic phase passes and patients can simply be managed with, thyroxine., , Complications following surgery, , , , , Anatomical such as recurrent laryngeal nerve damage., Bleeding. Owing to the confined space haematoma's may rapidly lead to respiratory, compromise owing to laryngeal oedema., Damage to the parathyroid glands resulting in hypocalcaemia., , Further sources of information, 1. http://www.acb.org.uk/docs/TFTguidelinefinal.pdf- Association of Clinical Biochemistry guidelines, for thyroid function tests., 2. British association of endocrine surgeons website- http://www.baets.org.uk, Next question
Page 3013 :
A 19 year old male presents with bilateral gynaecomastia, poor vision and nipple discharge. Which, of the following blood tests is most likely to be abnormal?, , Oestrogen, , Testosterone, β HCG, , Prolactin, , Calcitonin, , A combination of nipple discharge, gynaecomastia and poor vision may well be associated with a, prolactinoma. The poor vision results from compression of the optic chiasm resulting in bi temporal, hemianopia., Please rate this question:, , Discuss and give feedback, , Next question, , Gynaecomastia, Gynaecomastia describes an abnormal amount of breast tissue in males and is usually caused by, an increased oestrogen:androgen ratio. It is important to differentiate the causes of galactorrhoea, (due to the actions of prolactin on breast tissue) from those of gynaecomastia, Causes of gynaecomastia, , , , , , , , , , , , physiological: normal in puberty, syndromes with androgen deficiency: Kallman's, Klinefelter's, testicular failure: e.g. Mumps, liver disease, testicular cancer e.g. Seminoma secreting HCG, ectopic tumour secretion, hyperthyroidism, haemodialysis, drugs: see below
Page 3015 :
Theme: Management of calcium metabolic disorders, , A., B., C., D., E., F., G., , No action needed, Intravenous fluid (0.9% N.Saline), Risedronate and calcium supplements, Calcium supplements, Exploration and parathyroidectomy, DEXA bone scan, Pamidronate IV, , For each scenario please select the most appropriate management plan. Each option may be used, once, more than once or not at all., , 29., , An 80 year old woman has a hip fracture. Her calcium is normal. She has never been given, a diagnosis of osteoporosis., You answered No action needed, The correct answer is Risedronate and calcium supplements, The osteoporosis guidelines state if a postmenopausal woman has a fracture she should be, put on bisphosphonates (there is no need for a DEXA scan)., , 30., , A 60 year old man presents with recurrent renal stones. He is found to have a calcium of, 2.72 (elevated) and a PTH of 12 (elevated)., You answered No action needed, The correct answer is Exploration and parathyroidectomy, This patient has primary hyperparathyroidism and nephrolithiasis, which is an indication, for parathyroidectomy., , 31., , An 82 year old woman from a nursing home is admitted to the orthopaedic ward with a hip, fracture. She is acutely confused and agitated. Her Calcium is 2.95 (elevated)., You answered No action needed, The correct answer is Intravenous fluid (0.9% N.Saline), This patient needs rehydration due to hypercalcaemia. An intravenous bisphosphonate is, indicated if the Ca is above 3.
Page 3016 :
Please rate this question:, , Discuss and give feedback, , Next question, , Parathyroid glands and disorders of calcium metabolism, Hyperparathyroidism, , Disease type, , Hormone profile, , Clinical features, , Cause, , Primary, hyperparathyroidism, , , , , , , PTH (Elevated), Ca2+(Elevated), Phosphate (Low), Urine calcium :, creatinine clearance, ratio > 0.01, , May be, asymptomatic if, mild, Recurrent, abdominal pain, (pancreatitis, renal, colic), Changes to, emotional or, cognitive state, , Most cases due to, solitary adenoma, (80%), multifocal, disease occurs in 1015% and parathyroid, carcinoma in 1% or, less, , Secondary, hyperparathyroidism, , , , , PTH (Elevated), Ca2+ (Low or, normal), Phosphate, (Elevated), Vitamin D levels, (Low), , May have few, symptoms, Eventually may, develop bone, disease, osteitis, fibrosa cystica and, soft tissue, calcifications, , Parathyroid gland, hyperplasia occurs as, a result of low, calcium, almost, always in a setting of, chronic renal failure, , Ca2+(Normal or, high), PTH (Elevated), Phosphate levels, (Decreased or, Normal), Vitamin D (Normal, or decreased), Alkaline, phosphatase, (Elevated), , Metastatic, calcification, Bone pain and /, or fracture, Nephrolithiasis, Pancreatitis, , Occurs as a result of, ongoing hyperplasia, of the parathyroid, glands after, correction of, underlying renal, disorder, hyperplasia, of all 4 glands is, usually the cause, , , , , Tertiary, hyperparathyroidism, , , , , , , , , Differential diagnoses
Page 3017 :
It is important to consider the rare but relatively benign condition of benign familial hypocalciuric, hypercalcaemia, caused by an autosomal dominant genetic disorder. Diagnosis is usually made by, genetic testing and concordant biochemistry (urine calcium : creatinine clearance ratio <0.01distinguished from primary hyperparathyroidism)., Treatment, Primary hyperparathyroidism, Indications for surgery, , , , , , , , , , Elevated serum Calcium > 1mg/dL above normal, Hypercalciuria > 400mg/day, Creatinine clearance < 30% compared with normal, Episode of life threatening hypercalcaemia, Nephrolithiasis, Age < 50 years, Neuromuscular symptoms, Reduction in bone mineral density of the femoral neck, lumbar spine, or distal radius of more, than 2.5 standard deviations below peak bone mass (T score lower than -2.5), , Secondary hyperparathyroidism, Usually managed with medical therapy., Indications for surgery in secondary (renal) hyperparathyroidism:, , , , , Bone pain, Persistent pruritus, Soft tissue calcifications, , Tertiary hyperparathyroidism, Allow 12 months to elapse following transplant as many cases will resolve, The presence of an autonomously functioning parathyroid gland may require surgery. If the culprit, gland can be identified then it should be excised. Otherwise total parathyroidectomy and reimplantation of part of the gland may be required., References, 1. Pitt S et al. Secondary and Tertiary Hyperparathyroidism, State of the Art Surgical, Management.Surg Clin North Am 2009 Oct;89(5):1227-39., 2. MacKenzie-Feder J et al. Primary Hyperparathyroidism: An Overview. Int J Endocrinol 2011;, 2011: 251410., Next question
Page 3018 :
Theme: Management of thyroid disease, , A., B., C., D., E., F., G., H., , Total Thyroidectomy, Thyroid lobectomy, Sub total thyroidectomy, Radioactive iodine, Carbimazole, Tru cut biopsy, Further fine needle aspiration, Observation, , For each scenario please select the most appropriate management option. Each option may be used, once, more than once or not at all., , 32., , A 59 year old man is referred with symptoms of dysphagia. On examination he has a large, goitre and on imaging there is significant retrosternal extension and features of a, multinodular goitre., Total Thyroidectomy, Sub total thyroidectomy is no longer routinely undertaken in this group., , 33., , A 48 year old lady with thyrotoxicosis is referred to the clinic, she was poorly controlled, on carbimazole and has received orbital radiotherapy for severe proptosis. This has, improved matters but she relapsed on stopping her carbimazole., Total Thyroidectomy, Eye signs worsen with radioiodine., , 34., , A 23 year old lady has re attended the clinic on three occasions with a cyst in her thyroid, that refills. Cytology on each occasion is reassuring., You answered Total Thyroidectomy, The correct answer is Thyroid lobectomy, Persist refilling cysts may be associated with a well differentiated tumour and should be, removed by lobectomy., , Please rate this question:
Page 3019 :
Discuss and give feedback, , Next question, , Thyroid disease, Patients may present with a number of different manifestations of thyroid disease. They can be, broadly sub classified according to whether they are euthyroid or have clinical signs of thyroid, dysfunction. In addition it needs to be established whether they have a mass or not., Assessment, , , , , , History, Examination including USS, If a nodule is identified then it should be sampled ideally via an image guided fine needle, aspiration, Radionucleotide scanning is of limited use, , Thyroid Tumours, , , , , , , Papillary carcinoma, Follicular carcinoma, Anaplastic carcinoma, Medullary carcinoma, Lymphoma's, , Multinodular goitre, , , , , , One of the most common reasons for presentation, Provided the patient is euthyroid and asymptomatic and no discrete nodules are seen, they, can be reassured., In those with compressive symptoms surgery is required and the best operation is a total, thyroidectomy., Sub total resections were practised in the past and simply result in recurrent disease that, requires a difficult revisional resection., , Endocrine dysfunction, , , , , In general these patients are managed by physicians initially., Surgery may be offered alongside radio iodine for patients with Graves disease that fails with, medical management or in patients who would prefer not to be irradiated (e.g. pregnant, women)., Patients with hypothyroidism do not generally get offered a thyroidectomy. Sometimes, people inadvertently get offered resections during the early phase of Hashimotos thyroiditis,
Page 3020 :
however, with time the toxic phase passes and patients can simply be managed with, thyroxine., , Complications following surgery, , , , , Anatomical such as recurrent laryngeal nerve damage., Bleeding. Owing to the confined space haematoma's may rapidly lead to respiratory, compromise owing to laryngeal oedema., Damage to the parathyroid glands resulting in hypocalcaemia., , Further sources of information, 1. http://www.acb.org.uk/docs/TFTguidelinefinal.pdf- Association of Clinical Biochemistry guidelines, for thyroid function tests., 2. British association of endocrine surgeons website- http://www.baets.org.uk, Next question
Page 3021 :
Which of the following are not true of follicular thyroid cancer?, , They often appear to be encapsulated., , Those with a Hurthle cell subtype have an excellent prognosis., , Haematogenous metastasis is more common than in Papillary carcinoma., , The overall mortality rate is 24%., , Vascular invasion is seen in up to 60% of cases., , The Hurthle cell subtype have a worse prognosis., Please rate this question:, , Discuss and give feedback, , Next question, , Thyroid malignancy, Papillary carcinoma, , , , , , Commonest sub-type, Accurately diagnosed on fine needle aspiration cytology, Histologically, they may demonstrate psammoma bodies (areas of calcification) and so, called 'orphan Annie' nuclei, They typically metastasise via the lymphatics and thus laterally located apparently ectopic, thyroid tissue is usually a metastasis from a well differentiated papillary carcinoma, , Follicular carcinoma, , , , , , Are less common than papillary lesions, Like papillary tumours, they may present as a discrete nodule. Although they appear to be, well encapsulated macroscopically there is invasion on microscopic evaluation, Lymph node metastases are uncommon and these tumours tend to spread, haematogenously. This translates into a higher mortality rate, Follicular lesions cannot be accurately diagnosed on fine needle aspiration cytology and thus, all follicular FNA's (THY 3f) will require at least a hemi thyroidectomy
Page 3022 :
Anaplastic carcinoma, , , , Less common and tend to occur in elderly females, Disease is usually advanced at presentation and often only palliative decompression and, radiotherapy can be offered., , Medullary carcinoma, , , , , , These are tumours of the parafollicular cells ( C Cells) and are of neural crest origin., The serum calcitonin may be elevated which is of use when monitoring for recurrence., They may be familial and occur as part of the MEN -2A disease spectrum., Spread may be either lymphatic or haematogenous and as these tumours are not derived, primarily from thyroid cells they are not responsive to radioiodine., , Lymphoma, , , , These respond well to radiotherapy, Radical surgery is unnecessary once the disease has been diagnosed on biopsy material., Such biopsy material is not generated by an FNA and thus a core biopsy has to be obtained, (with care!)., Next question
Page 3023 :
Theme: Thyroid function tests, , A. Thyrotoxicosis, B. Sick euthyroid syndrome, C. Hypothyroidism, D. Poor compliance with thyroid medication, E. Hashimotos thyroiditis, F. Multinodular goitre, , Please select the most likely diagnosis for the scenario given. Each option may be used once, more, than once or not at all., , 36., , A 52 year old woman presents with an acute ischaemic right arm. She is found to have fast atrial, fibrillation. Her blood results reveal a free T4 level of 20 and a TSH of < 0.01., Thyrotoxicosis, Theme from January 2013, The diagnosis is thyrotoxicosis. An elevated T4 and a low TSH should indicate this diagnosis., Remember atrial fibrillation and its complications i.e acute ischaemic limbs can be precipitated by, hyperthyroid disorders., , 37., , A 42 year old woman presents with a goitre. On examination the goitre feels 'lumpy'. The blood, results reveal a TSH of 12 and a free T4 of 2. Antithyroid peroxidase antibodies are high., You answered Thyrotoxicosis, The correct answer is Hashimotos thyroiditis, Hashimotos usually presents in women aged between 30- 50 years. They are normally associated, with a goitre. To differentiate from hypothyroidism, the antithyroid peroxidase antibodies will be, elevated.
Page 3024 :
38., , A 55 year old man is on the intensive care unit for many months after open aortic surgery. He is, maintained on total parenteral nutrition. Clinically he is euthyroid, but his thyroid function tests, reveal a low TSH and low T4., You answered Thyrotoxicosis, The correct answer is Sick euthyroid syndrome, Sick euthyroid syndrome is most commonly seen in chronically ill patients or those with, starvation. The thyroid function tests are often low and the patient clinically euthyroid., , Please rate this question:, , Discuss and give feedback, , Next question, , Thyroid function tests, The interpretation of thyroid function tests is usually straightforward:, , Disorder, , TSH, , Free T4, , Thyrotoxicosis (e.g. Graves' disease), , Low, , High, , Primary hypothyroidism (primary, atrophic hypothyroidism), , High, , Low, , Secondary hypothyroidism, , Low, , Low, , In T3 thyrotoxicosis the free T4 will be, normal, , Replacement steroid therapy is, required prior to thyroxine
Page 3025 :
Disorder, , TSH, , Free T4, , Sick euthyroid syndrome*, , Low**, , Low, , Poor compliance with thyroxine, , High, , Normal /, high, , Steroid therapy, , Low, , Normal, , Common in hospital inpatients, , *now referred to as non-thyroidal illness, **TSH may be normal in some cases, Next question
Page 3026 :
Theme: Nottingham prognostic index, , A. <2.5, B. <3.4, C. 3.4-5.4, D. >5.4, , Please match the prognosis of patients who have undergone breast cancer surgery to the most, appropriate Nottingham Prognostic Index score. Each option may be used once, more than once or, not at all., , 39., , Worst prognostic group, You answered <2.5, The correct answer is >5.4, The Nottingham prognostic index may be used to stratify patients into various prognostic groups, (see below). An excellent prognosis is seen with a score of <2.4. Scores of over 5 equate to a, greatly reduced survival rate., , 40., , Intermediate prognosis, You answered <2.5, The correct answer is 3.4-5.4, , 41., , Excellent prognosis, <2.5
Page 3027 :
Please rate this question:, , Discuss and give feedback, , Next question, , Nottingham prognostic index, The Nottingham Prognostic Index can be used to give an indication of survival following breast, cancer surgery. In this system, the tumour size is weighted less heavily than other major prognostic, parameters., Calculation of NPI, Tumour Size x 0.2 + Lymph node score(From table below)+Grade score(From table below)., , Lymph nodes involved, , Grade, , 1, , 0, , 1, , 2, , 1-3, , 2, , 3, , >3, , 3, , Score, , Prognosis, , Score, , Percentage 5 year survival, , 2.0 to 2.4, , 93%, , 2.5 to 3.4, , 85%
Page 3028 :
3.5 to 5.4, , 70%, , >5.4, , 50%, , This data was originally published in 1992. It should be emphasised that other factors such as, vascular invasion and receptor status also impact on survival and are not included in this data and, account for varying prognoses often cited in the literature., Reference, Galea, M.H., et al., The Nottingham Prognostic Index in primary breast cancer. Breast Cancer Res, Treat, 1992. 22(3): p. 207-19., Next question
Page 3029 :
A 56 year old lady undergoes a mastectomy as treatment for multifocal ductal carcinoma in situ. Two, weeks post operatively she attends the clinic and complains of a diffuse swelling at the surgical site., On examination she has a large, fluctuant area underlying the mastectomy skin flaps. She is, otherwise well. What is the most likely cause?, , Abscess, , Seroma, , Haematoma, , Disease recurrence, , Arteriovenous malformation, , Seromas are very common after breast surgery. The exposed raw surfaces created during the, elevation of the skin flaps are a common cause. Treatment usually involves percutaneous drainage, under aseptic conditions., Please rate this question:, , Discuss and give feedback, , Next question, , Complications of breast surgery, Breast surgery may be associated with the following complications:, , , , , , , , Long thoracic nerve injury. This may occur during the axillary dissection and result in winging, of the scapula., Intercostobrachial nerve injury. These nerves traverse the axilla. When they are divided, (which they often are) the patient will notice an area of parasthesia in the armpit., Injury to the thoracodorsal trunk. This nerve and vessels supply latissimus dorsi. If they are, damaged the functional effects are not too serious, the greatest setback is that a latissimus, dorsi flap cannot be used for reconstruction purposes., Infections. Cellulitis of the chest wall and arm may be a major problem if axillary nodal, clearance is undertaken. Infections may run a protracted course and require polytherapy for, treatment., Lymphoedema. Usually complicates axillary node clearance or irradiation. Treatment is with, manual lymphatic drainage and compression sleeves., Seroma. This is an accumulation of fluid at the site of surgery. The fluid is usually straw, coloured and may re-accumulate despite drainage. Most will resolve with time.
Page 3030 :
You are the specialist trainee in endocrinology clinic. The medical team have referred a man for a, parathyroidectomy who has a corrected calcium of 2.82 (elevated) and a PTH of 11 (elevated)., Which of the following is not an indication for parathyroidectomy?, , Nephrolithiasis, , Reduction in bone mineral density of the femoral neck, lumbar spine, or distal radius of, more than 2.5 standard deviations below peak bone mass, Age < 50 years, , Episode of life threatening hypercalcaemia, , None of the above, , All of the situations listed are indications for parathyroidectomy. See below for more information., Please rate this question:, , Discuss and give feedback, , Next question, , Parathyroid glands and disorders of calcium metabolism, Hyperparathyroidism, , Disease type, , Hormone profile, , Clinical features, , Cause, , Primary, hyperparathyroidism, , , , , , , PTH (Elevated), Ca2+(Elevated), Phosphate (Low), Urine calcium :, creatinine clearance, ratio > 0.01, , May be, asymptomatic if, mild, Recurrent, abdominal pain, (pancreatitis, renal, colic), Changes to, emotional or, cognitive state, , Most cases due to, solitary adenoma, (80%), multifocal, disease occurs in 1015% and parathyroid, carcinoma in 1% or, less, , Secondary, , , , PTH (Elevated), , May have few, , Parathyroid gland
Page 3031 :
Disease type, , hyperparathyroidism, , Hormone profile, , , , , Tertiary, hyperparathyroidism, , , , , , , , , Clinical features, , Cause, , Ca2+ (Low or, normal), Phosphate, (Elevated), Vitamin D levels, (Low), , symptoms, Eventually may, develop bone, disease, osteitis, fibrosa cystica and, soft tissue, calcifications, , hyperplasia occurs as, a result of low, calcium, almost, always in a setting of, chronic renal failure, , Ca2+(Normal or, high), PTH (Elevated), Phosphate levels, (Decreased or, Normal), Vitamin D (Normal, or decreased), Alkaline, phosphatase, (Elevated), , Metastatic, calcification, Bone pain and /, or fracture, Nephrolithiasis, Pancreatitis, , Occurs as a result of, ongoing hyperplasia, of the parathyroid, glands after, correction of, underlying renal, disorder, hyperplasia, of all 4 glands is, usually the cause, , Differential diagnoses, It is important to consider the rare but relatively benign condition of benign familial hypocalciuric, hypercalcaemia, caused by an autosomal dominant genetic disorder. Diagnosis is usually made by, genetic testing and concordant biochemistry (urine calcium : creatinine clearance ratio <0.01distinguished from primary hyperparathyroidism)., Treatment, Primary hyperparathyroidism, Indications for surgery, , , , , , , , , , Elevated serum Calcium > 1mg/dL above normal, Hypercalciuria > 400mg/day, Creatinine clearance < 30% compared with normal, Episode of life threatening hypercalcaemia, Nephrolithiasis, Age < 50 years, Neuromuscular symptoms, Reduction in bone mineral density of the femoral neck, lumbar spine, or distal radius of more, than 2.5 standard deviations below peak bone mass (T score lower than -2.5), , Secondary hyperparathyroidism
Page 3032 :
Usually managed with medical therapy., Indications for surgery in secondary (renal) hyperparathyroidism:, , , , , Bone pain, Persistent pruritus, Soft tissue calcifications, , Tertiary hyperparathyroidism, Allow 12 months to elapse following transplant as many cases will resolve, The presence of an autonomously functioning parathyroid gland may require surgery. If the culprit, gland can be identified then it should be excised. Otherwise total parathyroidectomy and reimplantation of part of the gland may be required., References, 1. Pitt S et al. Secondary and Tertiary Hyperparathyroidism, State of the Art Surgical, Management.Surg Clin North Am 2009 Oct;89(5):1227-39., 2. MacKenzie-Feder J et al. Primary Hyperparathyroidism: An Overview. Int J Endocrinol 2011;, 2011: 251410., Next question
Page 3033 :
Theme: Breast disease treatment, , A., B., C., D., E., F., G., H., I., J., , Mastectomy, Sentinel lymph node biopsy, Axillary node clearance, Wide local excision, Breast lump excision biopsy, Image guided wide local excision, Radiotherapy, Chemotherapy, Excision of margins, Discharge to routine follow-up, , Please select the most appropriate management option from the list for the scenario given. Each, option may be used once, more than once or not at all., , 44., , A 35 year old woman has undergone a wide local excision. The histology shows an, invasive lobular carcinoma present at 3 of the resection margins. Cavity shavings taken at, the original operation are also involved. Sentinel node biopsy was negative., Mastectomy, This patient has an extensive disease process and lobular cancers are notorious for being, multifocal. In this case a mastectomy is the safest next step., , 45., , A 56 year old woman has undergone a wide local excision and axillary node sample. The, histology shows a 2.5cm invasive ductal carcinoma grade 1 which is completely excised., None of the axillary lymph nodes show evidence of metastatic disease., You answered Mastectomy, The correct answer is Radiotherapy, This woman has a good prognosis. However, irradiation of the breast is mandatory after, breast cancer has been treated using breast conserving surgery., , 46., , A 28 year old female presents with a painless lump in the upper outer quadrant of her left, breast. Imaging using ultrasound is indeterminate (U3). Two core biopsies have now been, performed and both show normal breast tissue (B1)., You answered Mastectomy, The correct answer is Breast lump excision biopsy
Page 3034 :
The imaging and biopsy results are not concordant. At this stage an excision biopsy is the, safest option., Please rate this question:, , Discuss and give feedback, , Next question, , Breast cancer management, , , , , , Surgery is performed in most patients suffering from breast cancer., Chemotherapy may be used to downstage tumours and allow breast conserving surgery., Hormonal therapy may also be used for the same purposes., Radiotherapy is given to all patients who have undergone breast conserving surgery., Patients who have undergone mastectomy may be offered a reconstructive procedure either, in conjunction with their primary resection or as a staged procedure at a later date., , Surgical options, Mastectomy vs Wide local excision, , Mastectomy, , Wide Local Excision, , Multifocal tumour, , Solitary lesion, , Central tumour, , Peripheral tumour, , Large lesion in small breast, , Small lesion in large breast, , DCIS >4cm, , DCIS <4cm, , Patient Choice, , Patient choice, , Central lesions may be managed using breast conserving surgery, where an acceptable cosmetic, result may be obtained, this is rarely the case in small breasts, Axillary disease
Page 3035 :
, , , , As a minimum, all patients with invasive breast cancer should have their axilla staged. In, those who do not have overt evidence of axillary nodal involvement this can be undertaken, using sentinel lymph node biopsy., Patients with a positive sentinel lymph node biopsy or who have imaging and cytological or, histological evidence of axillary nodal metastasis should undergo axillary node clearance., Axillary node clearance is associated with the development of lymphoedema, increased risk, of cellulitis and frozen shoulder., Next question
Page 3036 :
Theme: Non operative treatment of breast cancer, , A., B., C., D., E., F., , Radiotherapy, Cytotoxic chemotherapy, Surveillence alone, Endocrine therapy using tamoxifen, Endocrine therapy using letrozole, Endocrine therapy using medroxyprogesterone acetate, , Please select the most appropriate agent for the situation described. Each option may be used once,, more than once or not at all., , 47., , A 55 year old lady has undergone a wide local excision and sentinel lymph node biopsy, for breast cancer. The histology report shows a completely excised 1.3cm grade 1 invasive, ductal carcinoma. The sentinel node contained no evidence of metastatic disease. The, tumour is oestrogen receptor negative., Radiotherapy, Radiotherapy is routine following breast conserving surgery. Without irradiation the local, recurrence rates are approximately 40%., , 48., , An 88 year old lady presents with a large mass in the upper inner quadrant of her right, breast. Investigations confirm an oestrogen receptor positive, invasive ductal carcinoma., She has declined operative treatment., You answered Radiotherapy, The correct answer is Endocrine therapy using letrozole, Elderly patients may be managed using endocrine therapy alone. Eventually most will, escape hormonal control. In post menopausal women oestrogens are produced by the, peripheral aromatization of androgens and aromatase inhibitors are therefore the most, popular agent in this age group., , 49., , A 38 year old lady has undergone a mastectomy and axillary node clearance for invasive, ductal carcinoma. The histology report shows a completely excised 3.5cm lesion which is, grade 3. Two of the axillary lymph nodes contain metastatic disease. The tumour is, oestrogen receptor negative., You answered Radiotherapy, The correct answer is Cytotoxic chemotherapy
Page 3037 :
The combination of a grade 3 tumour and axillary nodal metastasis in a young female, would attract a recommendation for chemotherapy. Some may also add herceptin (if they, are HER 2 positive)., Please rate this question:, , Discuss and give feedback, , Next question, , Breast cancer treatment, Treatment, , Indication, , Endocrine, therapy, , , , , , Oestrogen receptor positive tumours, Downstaging primary lesions, Definitive treatment in old, infirm patients, , Irradiation, , , , , Wide local excision, Large lesion, high grade or marked vascular invasion following, mastectomy, , Chemotherapy, , , , , Downstaging advanced lesions to facilitate breast conserving surgery, Patients with grade 3 lesions or axillary nodal disease, , Endocrine agents, Tamoxifen is used and works as a partial oestrogen receptor agonist. It will typically block activity at, the breast. It does, however, stimulate the receptors at other sites and it is this that accounts for its, association with endometrial cancer. In post menopausal women the process of aromatisation, accounts for most oestrogen production. Therefore in this group aromatase inhibitors are the, preferred agents. Women who are perimenopausal start on tamoxifen and switch at 3 years., Chemotherapy, The FEC regime is most commonly used (Fluorouracil, epirubicin and cyclophosphamide). This was, found to be superior to the older CMF regime. The Taxanes are commonly used in high risk patients, and in this setting a regime of docetaxal, doxorubicin and cyclophosphamide may be used. The, anthracycline class drugs have marked cardiotoxicity (a property that they share with trastuzumab), and this can limit their use., Next question
Page 3038 :
Which of the following statements regarding papillary carcinoma of the thyroid is false?, , They account for the majority of thyroid carcinomas, , Spread predominantly via the lymphatics, , May be diagnosed using fine needle aspiration cytology, , When viewed microscopically may demonstrate 'orphan Annie 'nuclei, , Have a five year survival of 65% if confined to the thyroid alone, , The prognosis for localised papillary carcinomas is excellent. Survival rates at 5 years approach, 90%., Please rate this question:, , Discuss and give feedback, , Next question, , Thyroid malignancy, Papillary carcinoma, , , , , , Commonest sub-type, Accurately diagnosed on fine needle aspiration cytology, Histologically, they may demonstrate psammoma bodies (areas of calcification) and so, called 'orphan Annie' nuclei, They typically metastasise via the lymphatics and thus laterally located apparently ectopic, thyroid tissue is usually a metastasis from a well differentiated papillary carcinoma, , Follicular carcinoma, , , , , , Are less common than papillary lesions, Like papillary tumours, they may present as a discrete nodule. Although they appear to be, well encapsulated macroscopically there is invasion on microscopic evaluation, Lymph node metastases are uncommon and these tumours tend to spread, haematogenously. This translates into a higher mortality rate, Follicular lesions cannot be accurately diagnosed on fine needle aspiration cytology and thus, all follicular FNA's (THY 3f) will require at least a hemi thyroidectomy
Page 3039 :
Anaplastic carcinoma, , , , Less common and tend to occur in elderly females, Disease is usually advanced at presentation and often only palliative decompression and, radiotherapy can be offered., , Medullary carcinoma, , , , , , These are tumours of the parafollicular cells ( C Cells) and are of neural crest origin., The serum calcitonin may be elevated which is of use when monitoring for recurrence., They may be familial and occur as part of the MEN -2A disease spectrum., Spread may be either lymphatic or haematogenous and as these tumours are not derived, primarily from thyroid cells they are not responsive to radioiodine., , Lymphoma, , , , These respond well to radiotherapy, Radical surgery is unnecessary once the disease has been diagnosed on biopsy material., Such biopsy material is not generated by an FNA and thus a core biopsy has to be obtained, (with care!)., Next question
Page 3040 :
Theme: Breast malignancy, , A., B., C., D., E., F., G., , Eczema of the nipple, Ductal carcinoma in situ, Mucinous carcinoma, Invasive ductal carcinoma, Invasive lobular carcinoma, Paget's disease of the nipple, Lobular carcinoma in situ., , What is the likely diagnosis for the scenario given? Each option may be used once, more than once,, or not at all., , 51., , A 74 year old woman presents with a breast lump. On examination is has a soft, consistency. The lump is removed and sliced apart. Macroscopically there is a grey,, gelatinous surface., You answered Eczema of the nipple, The correct answer is Mucinous carcinoma, Mucinous carcinomas comprise 2-3% of all breast cancers. They are one of the special, type of carcinomas. These have a better prognosis that tumours of Non Special Type, (NST) and axillary nodal disease is rare in this group., , 52., , A 74 year old woman presents with an erythematous rash originating in the nipple. It is, spreading to the surrounding areolar area and the associated normal tissue., You answered Eczema of the nipple, The correct answer is Paget's disease of the nipple, Paget's is associated with DCIS or invasive carcinoma.Unlike eczema of the nipple which, predominantly affects the areolar region, Pagets will usually affect the nipple first and then, spread to the areolar area. Diagnosis is made by punch biopsy., , 53., , A 53 year old woman presents with a bloody nipple discharge. On mammography there is, calcification behind the nipple areolar complex. A core biopsy shows background benign, change, but cells that show comedo necrosis which have not breached the basement, membrane., You answered Eczema of the nipple
Page 3041 :
The correct answer is Ductal carcinoma in situ, Comedo necrosis is a feature of high nuclear grade ductal carcinoma in situ. It is has a high, risk of being associated with foci of invasion., Please rate this question:, , Discuss and give feedback, , Breast cancer, , , , , , , , , Commoner in the older age group, Invasive ductal carcinomas are the most common type. Some may arise as a result, of ductal carcinoma in situ (DCIS). There are associated carcinomas of special type e.g., Tubular that may carry better prognosis., The pathological assessment involves assessment of the tumour and lymph nodes, sentinel, lymph node biopsy is often used to minimise the morbidity of an axillary dissection., Treatment, typically this is either wide local excision or mastectomy. There are many sub, types of both of these that fall outside of the MRCS. Some key rules to bear in mind., Whatever operation is contemplated the final cosmetic outcome does have a bearing. A, woman with small breasts and a large tumour will tend to fare better with mastectomy, even, if clear pathological and clinical margins can be obtained. Conversely a women with larger, breasts may be able to undergo breast conserving surgery even with a relatively large, primary lesion (NB tumours >4cm used to attract recommendation for mastectomy). For, screen detected and impalpable tumour image guidance will be necessary., Reconstruction is always an option following any resectional procedure. However, its exact, type must be tailored to age and co-morbidities of the patient. The main operations in, common use include latissimus dorsi myocutaneous flap and sub pectoral implants. Women, wishing to avoid a prosthesis may be offered TRAM or DIEP flaps., , Surgical options, Mastectomy vs Wide local excision, , Mastectomy, , Wide Local Excision, , Multifocal tumour, , Solitary lesion, , Central tumour, , Peripheral tumour, , Large lesion in small breast, , Small lesion in large breast
Page 3042 :
Mastectomy, , Wide Local Excision, , DCIS >4cm, , DCIS <4cm, , Patient Choice, , Patient choice, , Central lesions may be managed using breast conserving surgery where an acceptable cosmetic, result may be obtained, this is rarely the case in small breasts, A compelling indication for mastectomy, a larger tumour that would be unsuitable for breast, conserving surgery, , Image sourced from Wikipedia, , Whatever surgical option is chosen the aim should be to have a local recurrence rate of 5% or less, at 5 years [1]., Nottingham Prognostic Index, The Nottingham Prognostic Index can be used to give an indication of survival. In this system the, tumour size is weighted less heavily than other major prognostic parameters., Calculation of NPI, Tumour Size x 0.2 + Lymph node score(From table below)+Grade score(From table below).
Page 3043 :
Score, , Lymph nodes involved, , Grade, , 1, , 0, , 1, , 2, , 1-3, , 2, , 3, , >3, , 3, , Prognosis, , Score, , Percentage 5 year survival, , 2.0 to 2.4, , 93%, , 2.5 to 3.4, , 85%, , 3.5 to 5.4, , 70%, , >5.4, , 50%, , This data was originally published in 1992. It should be emphasised that other factors such as, vascular invasion and receptor status also impact on survival and are not included in this data and, account for varying prognoses often cited in the literature., References, Surgical guidelines for the management of breast cancer, Association of Breast Surgery at BASO, 2009, Eur J Surg Oncol (2009), doi:10.1016/j.ejso.2009.01.008
Page 3044 :
A 68 year old man with poorly controlled diabetes presents with severe otalgia and headaches. On, examination, there is granulation tissue within the external auditory meatus. What is the most likely, underlying infective agent?, , Pseudomonas aeruginosa, , Streptococcus pyogenes, , Staphylococcus aureus, , Actinomyces, , Bacteroides fragilis, Malignant otitis externa is caused by Pseudomonas aeruginosa, Severe pain, headaches and granulation tissue within the external auditory meatus are key features, of malignant otitis externa. Diabetes mellitus is one of the commonest risk factors., Please rate this question:, , Discuss and give feedback, , Next question, , Malignant otitis externa, , , , , , Uncommon type of otitis externa that is found in immunocompromised individuals (90%, cases found in diabetics), Infective organism is usually Pseudomonas aeruginosa, Infection commences in the soft tissues of the external auditory meatus, then progresses to, involve the soft tissues and into the bony ear canal, Progresses to temporal bone osteomyelitis, , Key features in history, Diabetes (90%) or immunosuppression (illness or treatment related), Severe, unrelenting, deep-seated otalgia, Temporal headaches, Purulent otorrhea, Possibly dysphagia, hoarseness, and/or facial nerve dysfunction, Treatment
Page 3045 :
Anti pseudomonal antimicrobial agents, Topical agents, Hyperbaric oxygen is sometimes used in refractory cases, Next question
Page 3046 :
A 53 year old man presents with an ulcerated mass at the anal verge. A biopsy is taken and the, histology demonstrates as squamous cell carcinoma. Infection with which of the viruses below is, most likely to have contributed to the development of the condition?, , Human papillomavirus 7, , Human immunodeficiency virus 1, , Human immunodeficiency virus 2, , Human papillomavirus 16, , Human T-lymphotropic virus 1, , Theme from January 2013 exam, Infection with human papilloma virus 16 is a risk factor for the development of intra epithelial, dysplasia of the anal skin with subsequent increased risk of invasive malignancy., Please rate this question:, , Discuss and give feedback, , Next question, , Oncoviruses, , , , Viruses which cause cancer, These may be detected on blood test and prevented by vaccine, , These are the main types of oncoviruses and their diseases:, , Oncovirus, , Cancer, , Epstein-Barr virus, , Burkitt's lymphoma, Hodgkin's lymphoma, Post transplant lymphoma, Nasopharyngeal carcinoma
Page 3047 :
Human papillomavirus 16/18, , Cervical cancer, Anal cancer, Penile cancer, Vulval cancer, Oropharyneal cancer, , Human herpes virus 8, , Kaposi's sarcoma, , Hepatitis B virus, , Hepatocellular carcinoma, , Hepatitis C virus, , Hepatocellular carcinoma, , Human T-lymphotropic virus 1, , Tropical spastic paraparesis, Adult T cell leukaemia, Next question
Page 3048 :
Theme: Parasitic infections, , A., B., C., D., E., F., G., , Giardia Infection, Cryptosporidium infection, Clonorchis sinensis infection, Ancylostoma duodenale infection, Ascaris lumbricoides infection, Echinococcus granulosus infection, Enterobius vermicularis infection, , Please select the most likely infective organism for the scenario given. Each option may be used, once, more than once or not at all., , 3., , A 6 year old boy presents with symptoms of recurrent pruritus ani. On examination there is, evidence of a small worm like structure protruding from the anus., You answered Giardia Infection, The correct answer is Enterobius vermicularis infection, Similar theme to September 2011 Exam, Infection with enterobius is extremely common. Pruritus is the main symptom, as there is a, lack of tissue invasion it is rare for individuals to have any signs of systemic sepsis., , 4., , A 58 year old man is reviewed in the clinic following a successful cadaveric renal transplant, the previous year. He has been able to return to work as a swimming instructor. Over the, past week he reports that he has been suffering from recurrent episodes of diarrhoea. It has, made him feel lethargic and exhausted. Stool microscopy shows evidence of cysts., You answered Giardia Infection, The correct answer is Cryptosporidium infection, Cryptosporidium is associated with infection, particularly in those who are, immunocompromised. Diarrhoea is the main disease. The cysts are typically identified on, stool microscopy., , 5., , A 25 year old man returns from a backpacking holiday in India. He presents with symptoms, of coughing and also of episodic abdominal discomfort. Peri anal examination is normal., Stool microscopy demonstrates both worms and eggs within the faeces., You answered Giardia Infection
Page 3049 :
The correct answer is Ascaris lumbricoides infection, Infection with Ascaris lumbricoides usually occurs after individuals have visited places like, sub Saharan Africa or the far east. Unlike ancylostoma duodenale infection there is usually, evidence of both worms and eggs in the stool. The absence of pruritus makes enterobius less, likely. The presence of coughing may be due to the migration of the larva through the lungs., Please rate this question:, , Discuss and give feedback, , Next question, , Gastro intestinal parasitic infections, Common infections, , Enterobiasis, , , , , , , Ancylostoma, duodenale, , , , , , , , Ascariasis, , Strongyloidiasis, , , , , Due to organism Enterobius vermicularis, Common cause of pruritus ani, Diagnosis usually made by placing scotch tape at the anus, this will, trap eggs that can then be viewed microscopically, Treatment is with mebendazole, Hookworms that anchor in proximal small bowel, Most infections are asymptomatic although may cause iron, deficiency anaemia, Larvae may be found in stools left at ambient temperature,, otherwise infection is difficult to diagnose, Infection occurs as a result of cutaneous penetration, migrates to, lungs, coughed up and then swallowed, Treatment is with mebendazole, , , , , Due to infection with roundworm Ascaris lumbricoides, Infections begin in gut following ingestion, then penetrate duodenal, wall to migrate to lungs, coughed up and swallowed, cycle begins, again, Diagnosis is made by identification of worm or eggs within faeces, Treatment is with mebendazole, , , , , , Due to infection with Strongyloides stercoralis, Rare in west, Organism is a nematode living in duodenum of host
Page 3050 :
, , , , , , , Cryptosporidium, , , , , , , , Giardiasis, , , , , , , , Initial infection is via skin penetration. They then migrate to lungs, and are coughed up and swallowed. Then mature in small bowel are, excreted and cycle begins again, An auto infective cycle is also recognised where larvae will, penetrate colonic wall, Individuals may be asymptomatic, although they may also have, respiratory disease and skin lesions, Diagnosis is usually made by stool microscopy, In the UK mebendazole is used for treatment, Protozoal infection, Organisms produce cysts which are excreted and thereby cause new, infections, Symptoms consist of diarrhoea and cramping abdominal pains., Symptoms are worse in immunosuppressed people, Cysts may be identified in stools, Treatment is with metronidazole, Diarrhoeal infection caused by Giardia lamblia (protozoan), Infections occur as a result of ingestion of cysts, Symptoms are usually gastrointestinal with abdominal pain,, bloating and passage of soft or loose stools, Diagnosis is by serology or stool microscopy, First line treatment is with metronidazole, Next question
Page 3051 :
A 29 year old female undergoes a sub total thyroidectomy. Five days post operatively the wound, becomes erythematous and discharges pus. What is the most likely causative organism?, , Streptococcus pyogenes, , Haemophilus influenzae, , Pseudomonas aeruginosa, , Staphylococcus aureus, , Proteus mirabilis, , Theme from 2011 Exam, In this setting Staphylococcus aureus Infection is the most likely cause. In the UK between 2010 and, 2011 the commonest cause of wound infection was enterobacter infections (usually following cardiac, or colonic surgery). 23% of infections were due to Staph aureus, which fits the scenario above., Infection with the other organisms including strep pyogenes was much rarer., Please rate this question:, , Discuss and give feedback, , Next question, , Surgical site infection, , , , , , , , , Surgical site infections may occur following a breach in tissue surfaces and allow normal, commensals and other pathogens to initiate infection. They are a major cause of morbidity, and mortality., Surgical site infections (SSI) comprise up to 20% of all healthcare associated infections and, at least 5% of patients undergoing surgery will develop an SSI as a result., In many cases the organisms are derived from the patient's own body. Measures that may, increase the risk of SSI include:, Shaving the wound using a razor (disposable clipper preferred), Using a non iodine impregnated incise drape if one is deemed to be necessary, Tissue hypoxia, Delayed administration of prophylactic antibiotics in tourniquet surgery, , Preoperatively, , , Don't remove body hair routinely
Page 3052 :
, , , If hair needs removal, use electrical clippers with single use head (razors increase infection, risk), Antibiotic prophylaxis if:, , - placement of prosthesis or valve, - clean-contaminated surgery, - contaminated surgery, , , , , Use local formulary, Aim to give single dose IV antibiotic on anaesthesia, If a tourniquet is to be used, give prophylactic antibiotics earlier, , Intraoperatively, , , , , , Prepare the skin with alcoholic chlorhexidine (Lowest incidence of SSI), Cover surgical site with dressing, A recent meta analysis has confirmed that administration of supplementary oxygen does not, reduce the risk of wound infection. In contrast to previous individual RCT's(1), Wound edge protectors do not appear to confer benefit (2), , Post operatively, Tissue viability advice for management of surgical wounds healing by secondary intention, Use of diathermy for skin incisions, In the NICE guidelines the use of diathermy for skin incisions is not advocated(3). Several, randomised controlled trials have been undertaken and demonstrated no increase in risk of SSI, when diathermy is used(4)., References, 1. Brar M et al.. Perioperative supplemental oxygen in colorectal patients: a meta analysis. J Surg, Res2011 (166): 227 -235., 2. Pinkney T et al. Impact of wound edge protection devices on surgical site infection after, laparotomy: impact of a multicentre randomised controlled trial (ROSSINI Trial). BMJ 2013 (347):10., 3. http://www.nice.org.uk/CG74, 4. Ahmad N and Ahmed A. Meta-analysis of the effectiveness of surgical scalpel or diathermy in, making abdominal skin incisions. Ann Surg 2011, 253(1):8-13., Next question
Page 3053 :
Which of the following cancers is not associated with the human papillomavirus?, , Anal cancer, , Oropharyngeal cancer, , Tracheal cancer, , Vulval cancer, , Penile cancer, , HPV is associated with:, 1. Cervical cancer (HPV 16/18 most common), 2. Anal cancer, 3. Penile cancer, 4. Vulval cancer, 5. Oropharyngeal cancer, Please rate this question:, , Discuss and give feedback, , Next question, , Oncoviruses, , , , Viruses which cause cancer, These may be detected on blood test and prevented by vaccine, , These are the main types of oncoviruses and their diseases:, , Oncovirus, , Cancer, , Epstein-Barr virus, , Burkitt's lymphoma, Hodgkin's lymphoma, Post transplant lymphoma, Nasopharyngeal carcinoma
Page 3054 :
Human papillomavirus 16/18, , Cervical cancer, Anal cancer, Penile cancer, Vulval cancer, Oropharyneal cancer, , Human herpes virus 8, , Kaposi's sarcoma, , Hepatitis B virus, , Hepatocellular carcinoma, , Hepatitis C virus, , Hepatocellular carcinoma, , Human T-lymphotropic virus 1, , Tropical spastic paraparesis, Adult T cell leukaemia, Next question
Page 3055 :
Which of the following is not associated with Epstein-Barr virus?, , Burkitt's lymphoma, , Post-transplantation lymphoma, , Hodgkin's lymphoma, , Nasopharyngeal carcinoma, , Mycosis fungoides, , Please rate this question:, , Discuss and give feedback, , Next question, , Oncoviruses, , , , Viruses which cause cancer, These may be detected on blood test and prevented by vaccine, , These are the main types of oncoviruses and their diseases:, , Oncovirus, , Cancer, , Epstein-Barr virus, , Burkitt's lymphoma, Hodgkin's lymphoma, Post transplant lymphoma, Nasopharyngeal carcinoma, , Human papillomavirus 16/18, , Cervical cancer, Anal cancer, Penile cancer, Vulval cancer
Page 3056 :
Oropharyneal cancer, , Human herpes virus 8, , Kaposi's sarcoma, , Hepatitis B virus, , Hepatocellular carcinoma, , Hepatitis C virus, , Hepatocellular carcinoma, , Human T-lymphotropic virus 1, , Tropical spastic paraparesis, Adult T cell leukaemia, Next question
Page 3057 :
Which organism is most likely to cause osteomyelitis in children with sickle cell disease?, , Group A Streptococcus species, , Staphylococcus aureus, , Enterobacter, , Salmonella species, , Group B Streptococcus species, , Theme from January 2013 Exam, Worldwide the Salmonella species remains the most common infecting organism in children with, osteomyelitis. Reference: "Etiology of Osteomyelitis Complicating Sickle Cell Disease (Burnett, et, al.Pediatrics 1998; 101:2 296-297)", Please rate this question:, , Discuss and give feedback, , Next question, , Osteomyelitis, Infection of the bone, Causes, , , , S aureus and occasionally Enterobacter or Streptococcus species, In sickle cell: Salmonella species, , Clinical features, , , , , Erythema, Pain, Fever, , Investigation
Page 3058 :
, , , X-ray: lytic centre with a ring of sclerosis, Bone biopsy and culture, , Treatment, , , , Prolonged antibiotics, Sequestra may need surgical removal, Next question
Page 3059 :
A 22 year old man has undergone an inguinal hernia repair. Seven days later he presents with an, erythematous and tender wound that is discharging a purulent material. What is the most likely, cause?, , Infection with Staphylococcus aureus, , Discharging haematoma, , Infection with Pseudomonas, , Infection with Streptococcus pyogenes, , Infection with Bacteroides, , In this setting Staphylococcus aureus Infection is the most likely cause. In the UK between 2010 and, 2011 the commonest cause of wound infection was enterobacter infections (usually following cardiac, or colonic surgery). 23% of infections were due to Staph aureus, which fits the scenario above., Infection with the other organisms including strep pyogenes was much rarer., Please rate this question:, , Discuss and give feedback, , Next question, , Surgical site infection, , , , , , , , , Surgical site infections may occur following a breach in tissue surfaces and allow normal, commensals and other pathogens to initiate infection. They are a major cause of morbidity, and mortality., Surgical site infections (SSI) comprise up to 20% of all healthcare associated infections and, at least 5% of patients undergoing surgery will develop an SSI as a result., In many cases the organisms are derived from the patient's own body. Measures that may, increase the risk of SSI include:, Shaving the wound using a razor (disposable clipper preferred), Using a non iodine impregnated incise drape if one is deemed to be necessary, Tissue hypoxia, Delayed administration of prophylactic antibiotics in tourniquet surgery, , Preoperatively, , , Don't remove body hair routinely
Page 3060 :
, , , If hair needs removal, use electrical clippers with single use head (razors increase infection, risk), Antibiotic prophylaxis if:, , - placement of prosthesis or valve, - clean-contaminated surgery, - contaminated surgery, , , , , Use local formulary, Aim to give single dose IV antibiotic on anaesthesia, If a tourniquet is to be used, give prophylactic antibiotics earlier, , Intraoperatively, , , , , , Prepare the skin with alcoholic chlorhexidine (Lowest incidence of SSI), Cover surgical site with dressing, A recent meta analysis has confirmed that administration of supplementary oxygen does not, reduce the risk of wound infection. In contrast to previous individual RCT's(1), Wound edge protectors do not appear to confer benefit (2), , Post operatively, Tissue viability advice for management of surgical wounds healing by secondary intention, Use of diathermy for skin incisions, In the NICE guidelines the use of diathermy for skin incisions is not advocated(3). Several, randomised controlled trials have been undertaken and demonstrated no increase in risk of SSI, when diathermy is used(4)., References, 1. Brar M et al.. Perioperative supplemental oxygen in colorectal patients: a meta analysis. J Surg, Res2011 (166): 227 -235., 2. Pinkney T et al. Impact of wound edge protection devices on surgical site infection after, laparotomy: impact of a multicentre randomised controlled trial (ROSSINI Trial). BMJ 2013 (347):10., 3. http://www.nice.org.uk/CG74, 4. Ahmad N and Ahmed A. Meta-analysis of the effectiveness of surgical scalpel or diathermy in, making abdominal skin incisions. Ann Surg 2011, 253(1):8-13., Next question
Page 3061 :
A 22 year old female is admitted to A&E with a splenic rupture. She has not been involved in any, trauma. What infection can cause spontaneous splenic rupture?, , Measles, , Mumps, , Influenza, , Epstein-Barr virus, , Rubella, , Theme from 2009 and 2011 Exams, Epstein - Barr Virus may cause generalised lymphadenopathy. This may be associated with, splenomegaly. This enlargement has been associated with spontaneous rupture., Please rate this question:, , Discuss and give feedback, , Next question, , Spleen, The spleen is located in the left upper quadrant of the abdomen and its size can vary depending, upon the amount of blood it contains. The typical adult spleen is 12.5cm long and 7.5cm wide. The, usual weight of the adult spleen is 150g., The exact position of the spleen can vary with respiratory activity, posture and the state of, surrounding viscera. It usually lies obliquely with its long axis aligned to the 9th, 10th and 11th ribs. It, is separated from these ribs by both diaphragm and pleural cavity. The normal spleen is not, palpable., The shape of the spleen is influenced by the state of the colon and stomach. Gastric distension will, cause the spleen to resemble the shape of an orange segment. Colonic distension will cause it to, become more tetrahedral., The spleen is almost entirely covered by peritoneum, which adheres firmly to its capsule. Recesses, of the greater sac separate it from the stomach and kidney. It develops from the upper dorsal, mesogastrium, remaining connected to the posterior abdominal wall and stomach by two folds of, peritoneum; the lienorenal ligament and gastrosplenic ligament. The lienorenal ligament is derived, from peritoneum where the wall of the general peritoneum meets the omental bursa between the left, kidney and spleen; the splenic vessels lie in its layers. The gastrosplenic ligament also has two
Page 3062 :
layers, formed by the meeting of the walls of the greater sac and omental bursa between spleen and, stomach, the short gastric and left gastroepiploic branches of the splenic artery pass in its layers., Laterally, the spleen is in contact with the phrenicocolic ligament., Relations, Superiorly, , Diaphragm, , Anteriorly, , Gastric impression, , Posteriorly, , Kidney, , Inferiorly, , Colon, , Hilum, , Tail of pancreas and splenic vessels (splenic artery divides here, branches pass to the, white pulp transporting plasma), , Contents, White, pulp, , Immune function. Contains central trabecular artery. The germinal centres are supplied, by arterioles called penicilliary radicles., , Red pulp, , Filters abnormal red blood cells., , Function, , , , , , , , Filtration of abnormal blood cells and foreign bodies such as bacteria., Immunity: IgM. Production of properdin, and tuftsin which help target fungi and bacteria for, phagocytosis., Haematopoiesis: up to 5th month gestation or in haematological disorders., Pooling: storage of 40% platelets., Iron reutilisation, Storage monocytes, , Disorders of the spleen, Massive splenomegaly, , , , , , , Myelofibrosis, Chronic myeloid leukaemia, Visceral leishmaniasis (kala-azar), Malaria, Gaucher's syndrome, , Other causes (as above plus), , , Portal hypertension e.g. secondary to cirrhosis
Page 3063 :
, , , , , , , Lymphoproliferative disease e.g. CLL, Hodgkin's, Haemolytic anaemia, Infection: hepatitis, glandular fever, Infective endocarditis, Sickle-cell*, thalassaemia, Rheumatoid arthritis (Felty's syndrome), , *the majority of adult patients with sickle-cell will have an atrophied spleen due to repeated infarction, Next question
Page 3064 :
A group of consultant surgeons are meeting at a symposium. The chef preparing the canapes has, an infection on his finger. Approximately 40 minutes after eating the canapes the group are struck, down with severe vomiting. What is the most likely underlying explanation for this process?, , Presence of enterotoxin from Staphylococcus aureus in the food, , Presence of enterotoxin from Streptococcus pyogenes in the food, , Infection with Campylobacter jejuni, , Presence of enterotoxin from Clostridium perfringens in the food, , Infection with Shigella soneii, , Staphylococcus aureus may release an enterotoxin, this is preformed and thus will typically result in, rapid onset of symptoms in affected individuals., Please rate this question:, , Discuss and give feedback, , Next question, , Surgical Microbiology, An extensive topic so an overview is given here. Organisms causing common surgical infections are, reasonable topics in the examination. However, microbiology is less rigorously tested than anatomy,, for example., Common organisms, Staphylococcus aureus, , , , , , , , , , Facultative anaerobe, Gram positive coccus, Haemolysis on blood agar plates, Catalase positive, 20% population are long term carriers, Exo and entero toxin may result in toxic shock syndrome and gastroenteritis respectively, Ideally treated with penicillin although many strains now resistant through beta Lactamase, production. In the UK less than 5% of isolates are sensitive to penicillin., Resistance to methicillin (and other antibiotics) is mediated by the mec operon , essentially, penicillin binding protein is altered and resistance to this class of antibiotics ensues
Page 3065 :
, , Common cause of cutaneous infections and abscesses, , Streptococcus pyogenes, , , , , , , , , Gram positive, forms chain like colonies, Lancefield Group A Streptococcus, Produces beta haemolysis on blood agar plates, Rarely part of normal skin microflora, Catalase negative, Releases a number of proteins/ virulence factors into host including hyaluronidase,, streptokinase which allow rapid tissue destruction, Releases superantigens such as pyogenic exotoxin A which results in scarlet fever, Remains sensitive to penicillin, macrolides may be used as an alternative., , Escherichia coli, , , , , , , , , Gram negative rod, Facultative anaerobe, non sporing, Wide range of subtypes and some are normal gut commensals, Some subtypes such as 0157 may produce lethal toxins resulting in haemolytic-uraemic, syndrome, Enterotoxigenic E-Coli produces an enterotoxin (ST enterotoxin) that results in large, volume fluid secretion into the gut lumen (Via cAMP activation), Enteropathogenic E-Coli binds to intestinal cells and cause structural damage, this coupled, with a moderate (or in case of enteroinvasive E-Coli significant) invasive component, produces enteritis and large volume diarrhoea together with fever., They are resistant to many antibiotics used to treat gram positive infections and acquire, resistance rapidly and are recognised as producing beta lactamases, , Campylobacter jejuni, , , , , , , Curved, gram negative, non sporulating bacteria, One of the commonest causes of diarrhoea worldwide, Produces enteritis which is often diffuse and blood may be passed, Remains a differential for right iliac fossa pain with diarrhoea, Self limiting infection so antibiotics are not usually advised. However, the quinolones are, often rapidly effective., , Helicobacter pylori, , , , , , Gram negative, helix shaped rod, microaerophillic, Produces hydrogenase that can derive energy from hydrogen released by intestinal bacteria, Flagellated and mobile, Those carrying the cag A gene may cause ulcers
Page 3066 :
, , , , , , It secretes urease that breaks down gastric urea> Carbon dioxide and ammonia>, ammonium>bicarbonate (simplified!) The bicarbonate can neutralise the gastric acid., Usually colonises the gastric antrum and irritates resulting in increased gastrin release and, higher levels of gastric acid. These patients will develop duodenal ulcers. In those with more, diffuse H-Pylori infection gastric acid levels are lower and ulcers develop by local tissue, damage from H-Pylori- these patients get gastric ulcers., Diagnosis may be made by serology (approx. 75% sensitive). Biopsy urease test during, endoscopy probably the most sensitive., In patients who are colonised 10-20% risk of peptic ulcer, 1-2% risk gastric cancer, <1% risk, MALT lymphoma., Next question
Page 3067 :
Theme: Infective organisms, , A., B., C., D., E., F., G., H., , Clostridium difficle, Cryptosporidium, Escherichia coli, Streptococcus bovis, Staphylococcus epidermidis, Clostridium botulinum, Staphylococcus aureus, Streptococcus pyogenes, , Please select the most likely microorganism for the infection scenarios given. Each option may be, used once, more than once or not at all., , 13., , A 56 year old man undergoes a difficult colonoscopy for assessment of a caecal cancer. 48, hours after the procedure he is admitted with septicaemia. His abdomen is soft and non, tender. Blood cultures grow gram positive cocci., You answered Clostridium difficle, The correct answer is Streptococcus bovis, Streptococcus bovis septicaemia is associated with carcinoma of the colon. It also can also, cause endocarditis., , 14., , A 23 year old woman is admitted with sepsis and right loin pain. She has a history of a, UTI that was treated by the GP with a course of trimethoprim that was commenced 24, hours previously., You answered Clostridium difficle, The correct answer is Escherichia coli, Ascending infection is most likely to be caused by E-Coli (from the list)., , 15., , A 34 year old homosexual is admitted with diarrhoea of 3 months duration. He is found to, by HIV positive with a CD4 count <50., You answered Clostridium difficle, The correct answer is Cryptosporidium, Although a self limiting diarrhoea is the norm, this is not the case in immunocompromised
Page 3068 :
individuals who can develop severe illness. Other organisms may, include Salmonella,Shigella, and Campylobacter., Please rate this question:, , Discuss and give feedback, , Next question, , Surgical Microbiology, An extensive topic so an overview is given here. Organisms causing common surgical infections are, reasonable topics in the examination. However, microbiology is less rigorously tested than anatomy,, for example., Common organisms, Staphylococcus aureus, , , , , , , , , , , Facultative anaerobe, Gram positive coccus, Haemolysis on blood agar plates, Catalase positive, 20% population are long term carriers, Exo and entero toxin may result in toxic shock syndrome and gastroenteritis respectively, Ideally treated with penicillin although many strains now resistant through beta Lactamase, production. In the UK less than 5% of isolates are sensitive to penicillin., Resistance to methicillin (and other antibiotics) is mediated by the mec operon , essentially, penicillin binding protein is altered and resistance to this class of antibiotics ensues, Common cause of cutaneous infections and abscesses, , Streptococcus pyogenes, , , , , , , , , Gram positive, forms chain like colonies, Lancefield Group A Streptococcus, Produces beta haemolysis on blood agar plates, Rarely part of normal skin microflora, Catalase negative, Releases a number of proteins/ virulence factors into host including hyaluronidase,, streptokinase which allow rapid tissue destruction, Releases superantigens such as pyogenic exotoxin A which results in scarlet fever, Remains sensitive to penicillin, macrolides may be used as an alternative., , Escherichia coli
Page 3069 :
, , , , , , , , Gram negative rod, Facultative anaerobe, non sporing, Wide range of subtypes and some are normal gut commensals, Some subtypes such as 0157 may produce lethal toxins resulting in haemolytic-uraemic, syndrome, Enterotoxigenic E-Coli produces an enterotoxin (ST enterotoxin) that results in large, volume fluid secretion into the gut lumen (Via cAMP activation), Enteropathogenic E-Coli binds to intestinal cells and cause structural damage, this coupled, with a moderate (or in case of enteroinvasive E-Coli significant) invasive component, produces enteritis and large volume diarrhoea together with fever., They are resistant to many antibiotics used to treat gram positive infections and acquire, resistance rapidly and are recognised as producing beta lactamases, , Campylobacter jejuni, , , , , , , Curved, gram negative, non sporulating bacteria, One of the commonest causes of diarrhoea worldwide, Produces enteritis which is often diffuse and blood may be passed, Remains a differential for right iliac fossa pain with diarrhoea, Self limiting infection so antibiotics are not usually advised. However, the quinolones are, often rapidly effective., , Helicobacter pylori, , , , , , , , , , , Gram negative, helix shaped rod, microaerophillic, Produces hydrogenase that can derive energy from hydrogen released by intestinal bacteria, Flagellated and mobile, Those carrying the cag A gene may cause ulcers, It secretes urease that breaks down gastric urea> Carbon dioxide and ammonia>, ammonium>bicarbonate (simplified!) The bicarbonate can neutralise the gastric acid., Usually colonises the gastric antrum and irritates resulting in increased gastrin release and, higher levels of gastric acid. These patients will develop duodenal ulcers. In those with more, diffuse H-Pylori infection gastric acid levels are lower and ulcers develop by local tissue, damage from H-Pylori- these patients get gastric ulcers., Diagnosis may be made by serology (approx. 75% sensitive). Biopsy urease test during, endoscopy probably the most sensitive., In patients who are colonised 10-20% risk of peptic ulcer, 1-2% risk gastric cancer, <1% risk, MALT lymphoma., Next question
Page 3070 :
What is the mechanism of action of macrolides?, , Causes misreading of mRNA, , Interferes with cell wall formation, , Inhibits DNA synthesis, , Inhibits RNA synthesis, , Inhibits protein synthesis, , Macrolides act by inhibiting bacterial protein synthesis. If pushed to give an answer they are, bacteriostatic in nature, but in reality this depends on the dose and type of organism being treated., Erythromycin was the first macrolide used clinically. Newer examples include clarithromycin and, azithromycin., Adverse effects of erythromycin, , , , , gastrointestinal side-effects are common, cholestatic jaundice: risk may be reduced if erythromycin stearate is used, P450 inhibitor, , Please rate this question:, , Discuss and give feedback, , Next question, , Antibiotics: mechanism of action, The lists below summarise the site of action of the commonly used antibiotics, Inhibit cell wall formation, , , , penicillins, cephalosporins, , Inhibit protein synthesis
Page 3072 :
Theme: Diarrhoea, , A., B., C., D., E., F., G., , Vibrio cholera, Yersinia enterocolitica, Clostridium difficile, Campylobacter jejuni, Salmonella spp., E. coli (Enterohaemorrhagic), E.Coli (Enteroinvasive), , What is the most likely infective organism for the scenario given? Each option may be used once,, more than once or not at all., , 17., , A 22 year old chef presents to the medical team with profuse bloody diarrhoea. On further, questioning he describes tenesmus. They arrange a sigmoidoscopy which reveals necrosis, and ulceration of the descending colon mucosa., You answered Vibrio cholera, The correct answer is E.Coli (Enteroinvasive), Necrosis and ulcers of the large bowel are a feature of enteroinvasive E.coli. It presents, with a dysentery type illness similar to shigellosis., , 18., , A 22 year old Chef presents with abdominal pain in the right iliac fossa. There is an, associated temperature and diarrhoea. The SHO takes the patient to theatre for an, appendicectomy, but the appendix appears normal. The terminal ileum appears thickened, and engorged., You answered Vibrio cholera, The correct answer is Yersinia enterocolitica, Yersinia can be mistaken for acute appendicitis due to mesenteric lymphadenitis and, ileitis. Yersinia infection of the terminal ileum typically produces more marked clinical, changes of this segment of bowel than infection with campylobacter., , 19., , A 30 year old aid worker becomes unwell whilst helping at the scene of a recent, earthquake. He develops vomiting and soon afterwards a diarrhoea that is loose and, extremely watery., Vibrio cholera
Page 3074 :
Causative organisms, , enterocolitica, , Features, , , , , , Vibrio cholera, , , , , , , , Typically produces a protracted terminal ileitis that may mimic, Crohns disease, Differential diagnosis acute appendicitis, May progress to septicaemia in susceptible individuals, Usually sensitive to quinolone or tetracyclines, Short, gram negative rods, Transmitted by contaminated water, seafood, Symptoms include sudden onset of effortless vomiting and profuse, watery diarrhoea, Correction of fluid and electrolyte losses are the mainstay of, treatment, Most cases will resolve, antibiotics are not generally indicated, Next question
Page 3075 :
Which of the following is true regarding the Salmonella species?, , Rose spots appear in all patients with typhoid, , They are normally present in the gut as commensals, , Subsequent chronic biliary infection occurs in 75% of cases, , A relative bradycardia is often seen in typhoid fever, , Salmonella typhi can be categorised into type A, B and C, , Please rate this question:, , Discuss and give feedback, , Next question, , Salmonella, The Salmonella group contains many members, most of which cause diarrhoeal diseases. They are, facultative anaerobes, Gram negative rods which are not normally present as commensals in the, gut., Typhoid and paratyphoid are caused by Salmonella typhi and Salmonella paratyphi (types A, B & C), respectively. They are often termed enteric fevers, producing systemic symptoms such as, headache, fever, arthralgia, Features, , , , , , , initially systemic upset as above, relative bradycardia, abdominal pain, distension, constipation: although Salmonella is a recognised cause of diarrhoea, constipation is more, common in typhoid, rose spots: present on the trunk in 40% of patients, and are more common in paratyphoid, , Possible complications include
Page 3076 :
, , , , , , osteomyelitis (especially in sickle cell disease where Salmonella is one of the most common, pathogens), GI bleed/perforation, meningitis, cholecystitis, chronic carriage (1%, more likely if adult females), Next question
Page 3077 :
A 77-year-old female presents with a non-healing ulcer on her right foot. Blood cultures grow MRSA., Which antibiotic would you consider in addition to vancomycin to cover this?, , Flucloxacillin, , Ceftazidime, , Ciprofloxacin, , Metronidazole, , Rifampicin, , The MRSA would or may be resistant to Other antibiotics. Rifampicin is normally given in, combination with another antibiotic., Please rate this question:, , Discuss and give feedback, , Next question, , MRSA, Methicillin-resistant Staphylococcus aureus (MRSA) was one of the first organisms which highlighted, the dangers of hospital-acquired infections., Who should be screened for MRSA?, , , , all patients awaiting elective admissions (exceptions include day patients having terminations, of pregnancy and ophthalmic surgery. Patients admitted to mental health trusts are also, excluded), in the UK all emergency admissions are currently screened, , How should a patient be screened for MRSA?, , , , , nasal swab and skin lesions or wounds, the swab should be wiped around the inside rim of a patient's nose for 5 seconds, the microbiology form must be labelled 'MRSA screen'
Page 3078 :
Suppression of MRSA from a carrier once identified, , , , nose: mupirocin 2% in white soft paraffin, tds for 5 days, skin: chlorhexidine gluconate, od for 5 days. Apply all over but particularly to the axilla, groin, and perineum, , The following antibiotics are commonly used in the treatment of MRSA infections:, , , , vancomycin, teicoplanin, , Some strains may be sensitive to the antibiotics listed below but they should not generally be used, alone because resistance may develop:, , , , , , , rifampicin, macrolides, tetracyclines, aminoglycosides, clindamycin, , Relatively new antibiotics such as linezolid, quinupristin/dalfopristin combinations and tigecycline, have activity against MRSA but should be reserved for resistant cases, Next question
Page 3079 :
Theme: Infective organisms, , A., B., C., D., E., F., G., H., , E-coli and bacteroides, Staphylococcus aureus, Streptococcus viridians, Staphylococcus epidermidis, Klebsiella, Clostridium tetani, Clostridium difficile, None of the above, , Which is the most likely infective organism for the scenario given? Each option may be used once,, more than once or not at all., , 22., , A 32 year old women undergoes mastectomy and latissimus dorsi flap reconstruction for, breast cancer, to provide optimal cosmesis a McGhan implant is placed under the, myocutaneous flap. Three weeks post operatively the patient continues to suffer from, recurrent wound infections that have proved resistant to multiple courses of antibiotics., You answered E-coli and bacteroides, The correct answer is Staphylococcus epidermidis, This tends to colonise plastic devices and forms a biofilm which allows colonisation with, other bacterial agents. It is notoriously difficult to eradicate once established and the usual, treatment is removal of the device., , 23., , A 68 year old man with diabetes presents with an area of necrosis of the perineum at the, base of the scrotum, there is some surrounding erythema. He is systemically unwell and, hypotensive., E-coli and bacteroides, This is likely to be Fournier's Gangrene. A number of agents are implicated. E-coli and, bacteroides are the most commonly isolated organisms. The key point is that both aerobic, and anaerobic organisms must be present and only A has this option., , 24., , A 68 year old women with previous rheumatic fever is admitted with pyrexia of unknown, origin. Her blood cultures are unhelpful but transoesophageal echocardiography reveals, vegetations on the mitral valve., You answered E-coli and bacteroides
Page 3080 :
The correct answer is Streptococcus viridians, This is the most common organism affecting previously abnormal heart valves., Please rate this question:, , Discuss and give feedback, , Next question, , Surgical Microbiology, An extensive topic so an overview is given here. Organisms causing common surgical infections are, reasonable topics in the examination. However, microbiology is less rigorously tested than anatomy,, for example., Common organisms, Staphylococcus aureus, , , , , , , , , , , Facultative anaerobe, Gram positive coccus, Haemolysis on blood agar plates, Catalase positive, 20% population are long term carriers, Exo and entero toxin may result in toxic shock syndrome and gastroenteritis respectively, Ideally treated with penicillin although many strains now resistant through beta Lactamase, production. In the UK less than 5% of isolates are sensitive to penicillin., Resistance to methicillin (and other antibiotics) is mediated by the mec operon , essentially, penicillin binding protein is altered and resistance to this class of antibiotics ensues, Common cause of cutaneous infections and abscesses, , Streptococcus pyogenes, , , , , , , , , Gram positive, forms chain like colonies, Lancefield Group A Streptococcus, Produces beta haemolysis on blood agar plates, Rarely part of normal skin microflora, Catalase negative, Releases a number of proteins/ virulence factors into host including hyaluronidase,, streptokinase which allow rapid tissue destruction, Releases superantigens such as pyogenic exotoxin A which results in scarlet fever, Remains sensitive to penicillin, macrolides may be used as an alternative., , Escherichia coli
Page 3081 :
, , , , , , , , Gram negative rod, Facultative anaerobe, non sporing, Wide range of subtypes and some are normal gut commensals, Some subtypes such as 0157 may produce lethal toxins resulting in haemolytic-uraemic, syndrome, Enterotoxigenic E-Coli produces an enterotoxin (ST enterotoxin) that results in large, volume fluid secretion into the gut lumen (Via cAMP activation), Enteropathogenic E-Coli binds to intestinal cells and cause structural damage, this coupled, with a moderate (or in case of enteroinvasive E-Coli significant) invasive component, produces enteritis and large volume diarrhoea together with fever., They are resistant to many antibiotics used to treat gram positive infections and acquire, resistance rapidly and are recognised as producing beta lactamases, , Campylobacter jejuni, , , , , , , Curved, gram negative, non sporulating bacteria, One of the commonest causes of diarrhoea worldwide, Produces enteritis which is often diffuse and blood may be passed, Remains a differential for right iliac fossa pain with diarrhoea, Self limiting infection so antibiotics are not usually advised. However, the quinolones are, often rapidly effective., , Helicobacter pylori, , , , , , , , , , , Gram negative, helix shaped rod, microaerophillic, Produces hydrogenase that can derive energy from hydrogen released by intestinal bacteria, Flagellated and mobile, Those carrying the cag A gene may cause ulcers, It secretes urease that breaks down gastric urea> Carbon dioxide and ammonia>, ammonium>bicarbonate (simplified!) The bicarbonate can neutralise the gastric acid., Usually colonises the gastric antrum and irritates resulting in increased gastrin release and, higher levels of gastric acid. These patients will develop duodenal ulcers. In those with more, diffuse H-Pylori infection gastric acid levels are lower and ulcers develop by local tissue, damage from H-Pylori- these patients get gastric ulcers., Diagnosis may be made by serology (approx. 75% sensitive). Biopsy urease test during, endoscopy probably the most sensitive., In patients who are colonised 10-20% risk of peptic ulcer, 1-2% risk gastric cancer, <1% risk, MALT lymphoma., Next question
Page 3082 :
A 48 year old lady undergoes an ERCP for jaundice. 36 hours following the procedure she develops, a fever and rigors. A blood culture is taken, which of the following organisms is most likely to be, cultured?, , Pseudomonas aeruginosa, , Streptococcus, , Enterobacter, , Staphylococcus, , Escherichia coli, Charcots triad = Surgical emergency., Patients need: Biliary decompression and broad spectrum antibiotics., E Coli is the most common organism implicated in cholangitis infections. Whilst enterobacter is, occasionally cultured it is not the most common organism., Please rate this question:, , Discuss and give feedback, , Next question, , Cholangitis, , , , Combination of bacterial infection and biliary obstruction, Most common organisms are: (most frequent at top of list), , Escherichia coli, Klebsiella species, Enterococcus species, Streptococcus species, Clinical features, Charcot's triad:, Fever (90% cases), Right upper quadrant pain, Jaundice, Reynolds pentad: Above plus confusion and hypotension
Page 3083 :
Investigations, USS 1st line, CT scan, ERCP: may be 1st line if high clinical suspicion and suitable for treatment, Treatment, ERCP -usually after 72 hours of antibiotics, Percutaneous transhepatic cholangiogram and biliary drain, Next question
Page 3084 :
In a 72 year old man undergoing a sigmoid colectomy for diverticular disease, which of the following, interventions is most likely to reduce his risk of developing a post operative wound infection?, , Using a plain clear incise type drape to cover the operative field, , Administering mechanical bowel preparation pre operatively, , Shaving his abdominal wall one day prior to surgery, , Administration of single dose of broad spectrum antibiotics prior to the procedure, , None of the above, , Administration of prophylactic antibiotics will reduce the risk of wound infection. Plain incise drapes, increase the risk of wound infections and should not be used. Iodophor impregnated drapes have, been demonstrated to reduce the risk of wound infection. Shaving one day prior to surgery will, increase the risk., Please rate this question:, , Discuss and give feedback, , Next question, , Surgical site infection, , , , , , , , , Surgical site infections may occur following a breach in tissue surfaces and allow normal, commensals and other pathogens to initiate infection. They are a major cause of morbidity, and mortality., Surgical site infections (SSI) comprise up to 20% of all healthcare associated infections and, at least 5% of patients undergoing surgery will develop an SSI as a result., In many cases the organisms are derived from the patient's own body. Measures that may, increase the risk of SSI include:, Shaving the wound using a razor (disposable clipper preferred), Using a non iodine impregnated incise drape if one is deemed to be necessary, Tissue hypoxia, Delayed administration of prophylactic antibiotics in tourniquet surgery, , Preoperatively, , , Don't remove body hair routinely
Page 3085 :
, , , If hair needs removal, use electrical clippers with single use head (razors increase infection, risk), Antibiotic prophylaxis if:, , - placement of prosthesis or valve, - clean-contaminated surgery, - contaminated surgery, , , , , Use local formulary, Aim to give single dose IV antibiotic on anaesthesia, If a tourniquet is to be used, give prophylactic antibiotics earlier, , Intraoperatively, , , , , , Prepare the skin with alcoholic chlorhexidine (Lowest incidence of SSI), Cover surgical site with dressing, A recent meta analysis has confirmed that administration of supplementary oxygen does not, reduce the risk of wound infection. In contrast to previous individual RCT's(1), Wound edge protectors do not appear to confer benefit (2), , Post operatively, Tissue viability advice for management of surgical wounds healing by secondary intention, Use of diathermy for skin incisions, In the NICE guidelines the use of diathermy for skin incisions is not advocated(3). Several, randomised controlled trials have been undertaken and demonstrated no increase in risk of SSI, when diathermy is used(4)., References, 1. Brar M et al.. Perioperative supplemental oxygen in colorectal patients: a meta analysis. J Surg, Res2011 (166): 227 -235., 2. Pinkney T et al. Impact of wound edge protection devices on surgical site infection after, laparotomy: impact of a multicentre randomised controlled trial (ROSSINI Trial). BMJ 2013 (347):10., 3. http://www.nice.org.uk/CG74, 4. Ahmad N and Ahmed A. Meta-analysis of the effectiveness of surgical scalpel or diathermy in, making abdominal skin incisions. Ann Surg 2011, 253(1):8-13., Next question
Page 3086 :
Which one of the following statements regarding hepatitis C is correct?, , Cannot be transmitted vertically from mother to child, , Interferon-alpha and ribavirin are the treatments of choice, , It is more infectious than hepatitis B following a needle stick injury, , Breast feeding is contraindicated in mothers with hepatitis C, , HCV RNA is the initial investigation of choice for at-risk groups, , Please rate this question:, , Discuss and give feedback, , Next question, , Hepatitis C, Hepatitis C is likely to become a significant public health problem in the UK in the next decade. It is, thought around 200,000 people are chronically infected with the virus. At risk groups include, intravenous drug users and patients who received a blood transfusion prior to 1991 (e.g., haemophiliacs)., Transmission, , , , , , the risk of transmission during a needle stick injury is about 2%, the vertical transmission rate from mother to child is about 6%, breast feeding is not contraindicated in mothers with hepatitis C, the risk of transmitting the virus during sexual intercourse is probably less than 5%, , Features, , , after exposure to the hepatitis C virus less than 20% of patients develop an acute hepatitis, , Complications
Page 3087 :
, , , , , chronic infection (80-85%) - only 15-20% of patients will clear the virus after an acute, infection and hence the majority will develop chronic hepatitis C, cirrhosis (20-30% of those with chronic disease), hepatocellular cancer, cryoglobulinaemia, , Management of chronic infection, , , , currently a combination of pegylated interferon-alpha and ribavirin are used, up to 55% of patients successfully clear the virus, with success rates of around 80% for, some strains, , Complications of treatment, , , , ribavirin - side-effects: haemolytic anaemia, cough. Women should not become pregnant, within 6 months of stopping ribavirin as it is teratogenic, interferon alpha - side-effects: flu-like symptoms, depression, fatigue, leukopenia,, thrombocytopenia, Next question
Page 3088 :
A 22 year old man presents with a 5 day history of sore throat, malaise and fatigue. On examination, he has a large peritonsillar abscess. What is the most likely underlying infective organism?, , Epstein Barr Virus, , Streptococcus pyogenes, , Cytomegalovirus, , Moraxella catarrhalis, , Streptococcus viridans, , Similar theme in September 2011 Exam, Quinsy usually occurs as a result of bacterial tonsillitis and the most common cause of bacterial, tonsillitis is streptococcal organisms., Please rate this question:, , Discuss and give feedback, , Next question, , Acute tonsillitis, , , , , , , , Characterised by pharyngitis, fever, malaise and lymphadenopathy., Over half of all cases are bacterial with Streptococcus pyogenes the most common organism, The tonsils are typically oedematous and yellow or white pustules may be present, Infectious mononucleosis may mimic the condition., Treatment with penicillin type antibiotics is indicated for bacterial tonsillitis., Bacterial tonsillitis may result in local abscess formation (quinsy), , Acute streptococcal tonsillitis
Page 3089 :
Image sourced from Wikipedia, , Next question
Page 3090 :
Which of the following statements relating to osteomyelitis is false?, , Is the result of haematogenous spread in most cases, , Is due to Staphylococcus aureus in 50% cases, , Should be treated by aggressive surgical debridement initially, , Plain radiographs may be normal in the early stages, , The presence of associated septic joint involvement will significantly alter management, , It is managed medically in the first instance (with an antistaphylococcal antibiotic). This differs from, the situation in septic joints where early joint washout is mandatory., Please rate this question:, , Discuss and give feedback, , Next question, , Osteomyelitis, Infection of the bone, Causes, , , , S aureus and occasionally Enterobacter or Streptococcus species, In sickle cell: Salmonella species, , Clinical features, , , , , Erythema, Pain, Fever, , Investigation
Page 3091 :
, , , X-ray: lytic centre with a ring of sclerosis, Bone biopsy and culture, , Treatment, , , , Prolonged antibiotics, Sequestra may need surgical removal, Next question
Page 3092 :
A 48 year old lady is admitted with crampy abdominal pain and diarrhoea. She has been unwell for, the past 12 hours. In the history she complains that her milk bottles have been pecked repeatedly by, birds, she otherwise has had no dietary changes. Which of the following is the most likely causative, organism?, , Staphylococcus aureus, , Campylobacter jejuni, , Clostridium difficile, , Norovirus, , Clostridium botulinum, , Birds are a recognised reservoir of campylobacter., Please rate this question:, , Discuss and give feedback, , Next question, , Bacterial Gastroenteritis, Causative organisms, , Features, , Campylobacterjejuni, , , , , , Shigella spp., , , , , Most common cause of acute infective diarrhoea, Spiral, gram negative rods, Usually infects caecum and terminal ileum. Local, lymphadenopathy is common, May mimic appendicitis as it has marked right iliac fossa pain, Reactive arthritis is seen in 1-2% of cases, , , , , , , , Members of the enterobacteriaceae, Gram negative bacilli, Clinically causes dysentery, Shigella soneii is the commonest infective organism (mild illness), Usually self limiting, ciprofloxacin may be required if individual
Page 3093 :
Causative organisms, , Features, , is in a high risk group, , Salmonellaspp, , , , , , Facultatively anaerobic, gram negative, enterobacteriaceae, Infective dose varies according to subtype, Salmonellosis: usually transmitted by infected meat (especially, poultry) and eggs, , E. coli, , , , , , , Enteropathogenic, Enteroinvasive: dysentery, large bowel necrosis/ulcers, Enterotoxigenic: small intestine, travelers diarrhoea, Enterohaemorrhagic: 0157, cause a haemorrhagic colitis,, haemolytic uraemic syndrome and thrombotic thrombocytopaenic, purpura, , Yersinia, enterocolitica, , , , , Gram negative, coccobacilli, Typically produces a protracted terminal ileitis that may mimic, Crohns disease, Differential diagnosis acute appendicitis, May progress to septicaemia in susceptible individuals, Usually sensitive to quinolone or tetracyclines, , , , , , Vibrio cholera, , , , , , , , Short, gram negative rods, Transmitted by contaminated water, seafood, Symptoms include sudden onset of effortless vomiting and profuse, watery diarrhoea, Correction of fluid and electrolyte losses are the mainstay of, treatment, Most cases will resolve, antibiotics are not generally indicated, Next question
Page 3094 :
A 50-year-old female with a history of rheumatoid presents with a suspected septic knee joint. A, diagnostic aspiration is performed and sent to microbiology. Which of the organisms below is most, likely to be responsible?, , Staphylococcus aureus, , Staphylococcus epidermidis, , Escherichia coli, , Neisseria gonorrhoeae, , Streptococcus pneumoniae, Septic arthritis - most common organism: Staphylococcus aureus, Please rate this question:, , Discuss and give feedback, , Next question, , Septic arthritis, Overview, , , , Most common organism overall is Staphylococcus aureus, In young adults who are sexually active Neisseria gonorrhoeae should also be considered, , Management, , , , , , , Synovial fluid should be obtained before starting treatment, Intravenous antibiotics which cover Gram-positive cocci are indicated. The BNF currently, recommends flucloxacillin or clindamycin if penicillin allergic, Antibiotic treatment is normally be given for several weeks (BNF states 6-12 weeks), Needle aspiration should be used to decompress the joint, Arthroscopic lavage may be required, Next question
Page 3095 :
A 22 year old man presents with crampy abdominal pain diarrhoea and bloating. He has just, returned from a holiday in Egypt. He had been swimming in the local pool a few days ago. He, reports that he is opening his bowels 5 times a day. The stool floats in the toilet water, but there is no, blood. What is the most likely cause?, , Cryptosporidium, , Salmonella sp, , E.coli sp, , Chronic pancreatitis, , Giardia lamblia, , Giardia causes fat malabsorption, therefore greasy stool can occur. It is resistant to chlorination,, hence risk of transfer in swimming pools., Please rate this question:, , Discuss and give feedback, , Next question, , Diarrhoea, World Health Organisation definitions, Diarrhoea: > 3 loose or watery stool per day, Acute diarrhoea < 14 days, Chronic diarrhoea > 14 days, , Acute Diarrhoea, , Gastroenteritis, , May be accompanied by abdominal pain or nausea/vomiting, , Diverticulitis, , Classically causes left lower quadrant pain, diarrhoea and fever
Page 3096 :
Acute Diarrhoea, , Antibiotic therapy, , More common with broad spectrum antibiotics, Clostridium difficile is also seen with antibiotic use, , Constipation causing, overflow, , A history of alternating diarrhoea and constipation may be, given, May lead to faecal incontinence in the elderly, , Chronic, Diarrhoea, , Irritable bowel, syndrome, , Extremely common. The most consistent features are abdominal pain, bloating, and change in bowel habit. Patients may be divided into those with diarrhoea, predominant IBS and those with constipation predominant IBS., Features such as lethargy, nausea, backache and bladder symptoms may also be, present, , Ulcerative, colitis, , Bloody diarrhoea may be seen. Crampy abdominal pain and weight loss are also, common. Faecal urgency and tenesmus may occur, , Crohn's, disease, , Crampy abdominal pains and diarrhoea. Bloody diarrhoea less common than in, ulcerative colitis. Other features include malabsorption, mouth ulcers perianal, disease and intestinal obstruction, , Colorectal, cancer, , Symptoms depend on the site of the lesion but include diarrhoea, rectal, bleeding, anaemia and constitutional symptoms e.g. Weight loss and anorexia, , Coeliac disease, , , , , In children may present with failure to thrive, diarrhoea and abdominal, distension, In adults lethargy, anaemia, diarrhoea and weight loss are seen. Other, autoimmune conditions may coexist, , Other conditions associated with diarrhoea include:
Page 3097 :
, , , , , Thyrotoxicosis, Laxative abuse, Appendicitis with pelvic abscess or pelvic appendix, Radiation enteritis, , Diagnosis, Stool culture, Abdominal and digital rectal examination, Consider colonoscopy (radiological studies unhelpful), Thyroid function tests, serum calcium, anti endomysial antibodies, glucose, Next question
Page 3098 :
A 54-year-old female is admitted one week following a cholecystectomy with profuse diarrhoea., Apart from a minor intra-operative bile spillage incurred during removal of the gallbladder, the, procedure was uncomplicated. What is the most likely diagnosis?, , Campylobacter infection, , E. coli infection, , Clostridium difficile infection, , Salmonella infection, , Pelvic abscess, , Antibiotics are not routinely administered during an uncomplicated cholecystectomy. Indications for, administration of broad spectrum antibiotics include intraoperative bile spillage. Delayed pelvic, abscesses following bile spills are extremely rare since most surgeons will manage these intraoperatively., Please rate this question:, , Discuss and give feedback, , Next question, , Clostridium difficile, Clostridium difficile is a Gram positive rod often encountered in hospital practice. In the UK it can be, found in 3% of normal adults and up to 66% of babies. It produces an exotoxin which causes, intestinal damage leading to a syndrome called pseudomembranous colitis., Risk factors, , , , , Broad spectrum antibiotics, Use of PPI and H2 receptor antagonists, Contacted with persons infected with c.difficile, , Features, , , , Diarrhoea, Abdominal pain
Page 3099 :
, , , A raised white blood cell count is characteristic, If severe, toxic megacolon may develop, , Diagnosis is made by detecting Clostridium difficile toxin (CDT) in the stool, Management, , , , , , First-line therapy is oral metronidazole for 10-14 days, If severe, or not responding to metronidazole, then oral vancomycin may be used, Patients who do not respond to vancomycin may respond to oral fidaxomicin, Patients with severe and unremitting colitis should be considered for colectomy, Next question
Page 3100 :
Which of the following is not a feature of Campylobacter jejuni infection?, , Infection may present in a similar manner to acute appendicitis, , Pyrexia is unusual, , They are gram negative organisms, , Infection accounts for 26% case of Guillain-Barre syndrome, , It is the commonest cause of infective diarrhoea arising from non viral causes, , A prodromal period of fever and generalised malaise precedes abdominal pain (which may mimic, appendicitis) and diarrhoea., Please rate this question:, , Discuss and give feedback, , Next question, , Bacterial Gastroenteritis, Causative organisms, , Features, , Campylobacterjejuni, , , , , , , , Shigella spp., , , , , , , , Most common cause of acute infective diarrhoea, Spiral, gram negative rods, Usually infects caecum and terminal ileum. Local, lymphadenopathy is common, May mimic appendicitis as it has marked right iliac fossa pain, Reactive arthritis is seen in 1-2% of cases, Members of the enterobacteriaceae, Gram negative bacilli, Clinically causes dysentery, Shigella soneii is the commonest infective organism (mild illness), Usually self limiting, ciprofloxacin may be required if individual, is in a high risk group
Page 3102 :
A 53-year-old woman is diagnosed with cellulitis surrounding her leg ulcer. A swab is taken and oral, flucloxacillin is started. The following result is obtained:, Skin swab:, , Group A streptococcus, , How should the antibiotic therapy be changed?, , No change, , Add topical fusidic acid, , Add clindamycin, , Add penicillin, , Add erythromycin, , Penicillin is the antibiotic of choice for group A streptococcal infections. The BNF suggests stopping, flucloxacillin if streptococcal infection is confirmed in patients with cellulitis, due to the high, sensitivity. This should be balanced however with the variable absorption of phenoxymethylpenicillin., Please rate this question:, , Discuss and give feedback, , Next question, , Streptococci, Streptococci may be divided into alpha and beta haemolytic types, Alpha haemolytic streptococci, The most important alpha haemolytic streptococcus is Streptococcus pneumoniae (pneumococcus)., Pneumococcus is a common cause of pneumonia, meningitis and otitis media. Another clinical, example is Streptococcus viridans, Beta haemolytic streptococci, These can be subdivided into group A and B, Group A
Page 3103 :
, , , , , most important organism is Streptococcus pyogenes, responsible for erysipelas, impetigo, cellulitis, type 2 necrotizing fasciitis and, pharyngitis/tonsillitis, immunological reactions can cause rheumatic fever or post-streptococcal glomerulonephritis, erythrogenic toxins cause scarlet fever, , Group B, , , Streptococcus agalactiae may lead to neonatal meningitis and septicaemia, Next question
Page 3104 :
Theme: Infectious disease, , A., B., C., D., E., F., G., H., I., , Clostridium difficile, Clostridium perfringens, Clostridium tetani, Streptococcus pyogenes, Steptococcus Bovis, Staphylococcus aureus, Staphylococcus epidermidis, Bacteroides fragilis, None of the above, , Please select the most likely infective organism for the scenario given. Each option may be used, once, more than once or not at all., , 36., , A 23 year old man is readmitted following a difficult appendicectomy. His wound is, erythematous and, on incision, foul smelling pus is drained., You answered Clostridium difficile, The correct answer is Bacteroides fragilis, Bacteroides is commonly present in severe peritoneal infections and as it is facultatively, anaerobic may be present in pus. It smells foul!, , 37., , A 62 year old lady is unwell following a difficult acute cholecystectomy for acute, cholecystitis. Her gallbladder spilled stones intraoperatively and she has been on, ciprofloxacin intravenously for this for the past 4 days. She now has colicky abdominal, pain and profuse, foul smelling diarrhoea., Clostridium difficile, C. difficile may complicate administration of broad spectrum antibiotics., , 38., , A 21 year old man is admitted with crampy abdominal pain and diarrhoea. He attended a, large wedding earlier in the day. Several other guests are also affected with the same, illness., You answered Clostridium difficile, The correct answer is Clostridium perfringens, C. Perfringens is a common cause of food borne illness and its ability to form spores may
Page 3105 :
make it relatively resistant to cooking. The timing of onset would favor C. Perfringens, which typically evolves over several hours, rather than staphylococcus aureus poisening, which may occur sooner., Please rate this question:, , Discuss and give feedback, , Next question, , Surgical Microbiology, An extensive topic so an overview is given here. Organisms causing common surgical infections are, reasonable topics in the examination. However, microbiology is less rigorously tested than anatomy,, for example., Common organisms, Staphylococcus aureus, , , , , , , , , , , Facultative anaerobe, Gram positive coccus, Haemolysis on blood agar plates, Catalase positive, 20% population are long term carriers, Exo and entero toxin may result in toxic shock syndrome and gastroenteritis respectively, Ideally treated with penicillin although many strains now resistant through beta Lactamase, production. In the UK less than 5% of isolates are sensitive to penicillin., Resistance to methicillin (and other antibiotics) is mediated by the mec operon , essentially, penicillin binding protein is altered and resistance to this class of antibiotics ensues, Common cause of cutaneous infections and abscesses, , Streptococcus pyogenes, , , , , , , , , Gram positive, forms chain like colonies, Lancefield Group A Streptococcus, Produces beta haemolysis on blood agar plates, Rarely part of normal skin microflora, Catalase negative, Releases a number of proteins/ virulence factors into host including hyaluronidase,, streptokinase which allow rapid tissue destruction, Releases superantigens such as pyogenic exotoxin A which results in scarlet fever, Remains sensitive to penicillin, macrolides may be used as an alternative., , Escherichia coli
Page 3106 :
, , , , , , , , Gram negative rod, Facultative anaerobe, non sporing, Wide range of subtypes and some are normal gut commensals, Some subtypes such as 0157 may produce lethal toxins resulting in haemolytic-uraemic, syndrome, Enterotoxigenic E-Coli produces an enterotoxin (ST enterotoxin) that results in large, volume fluid secretion into the gut lumen (Via cAMP activation), Enteropathogenic E-Coli binds to intestinal cells and cause structural damage, this coupled, with a moderate (or in case of enteroinvasive E-Coli significant) invasive component, produces enteritis and large volume diarrhoea together with fever., They are resistant to many antibiotics used to treat gram positive infections and acquire, resistance rapidly and are recognised as producing beta lactamases, , Campylobacter jejuni, , , , , , , Curved, gram negative, non sporulating bacteria, One of the commonest causes of diarrhoea worldwide, Produces enteritis which is often diffuse and blood may be passed, Remains a differential for right iliac fossa pain with diarrhoea, Self limiting infection so antibiotics are not usually advised. However, the quinolones are, often rapidly effective., , Helicobacter pylori, , , , , , , , , , , Gram negative, helix shaped rod, microaerophillic, Produces hydrogenase that can derive energy from hydrogen released by intestinal bacteria, Flagellated and mobile, Those carrying the cag A gene may cause ulcers, It secretes urease that breaks down gastric urea> Carbon dioxide and ammonia>, ammonium>bicarbonate (simplified!) The bicarbonate can neutralise the gastric acid., Usually colonises the gastric antrum and irritates resulting in increased gastrin release and, higher levels of gastric acid. These patients will develop duodenal ulcers. In those with more, diffuse H-Pylori infection gastric acid levels are lower and ulcers develop by local tissue, damage from H-Pylori- these patients get gastric ulcers., Diagnosis may be made by serology (approx. 75% sensitive). Biopsy urease test during, endoscopy probably the most sensitive., In patients who are colonised 10-20% risk of peptic ulcer, 1-2% risk gastric cancer, <1% risk, MALT lymphoma., Next question
Page 3107 :
Which of the following statements related to necrotising fasciitis is false?, , Mainly polymicrobial, , A feature may include 'dirty dishwater fluid' in the wound, , The presence of crepitus is needed to make the diagnosis, , Further surgery is mandatory 24-48h after initial surgery to review extension of infection, , The muscles are relatively spared, Never attempt primary closure after the initial debridement of necrotising fasciitis., Crepitus may be present in only 35% of cases, therefore its absence should not exclude a diagnosis, of necrotising fasciitis., Please rate this question:, , Discuss and give feedback, , Next question, , Meleney's Gangrene and Necrotising Fasciitis, Necrotising fasciitis, , , , , , , Advancing soft tissue infection associated with fascial necrosis, Uncommon, but can be fatal, In many cases there is underlying background immunosuppression e.g. Diabetes, Caused by polymicrobial flora (aerobic and anaerobic) and MRSA is seen increasingly in, cases of necrotising fasciitis, Streptococcus is the commonest organism in isolated pathogen infection (15%), , Meleneys gangrene, , , Meleneys is a similar principle but the infection is more superficially sited than necrotising, fasciitis and often confined to the trunk
Page 3108 :
Fournier gangrene, , , , Necrotising fasciitis affecting the perineum, Polymicrobial with E-coli and Bacteroides acting in synergy, , Clinical features, Fever, Pain, Cellulitis, Oedema, Induration, Numbness, Late findings, Purple/black skin discolouration, Blistering, Haemorrhagic bullae, Crepitus, Dirty Dishwater fluid discharge, Septic shock, A typical case of gas gangrene presenting late demonstrating some of the features described above, , Image sourced from Wikipedia, , Diagnosis is mainly clinical, Management
Page 3109 :
, , , , Radical surgical debridement forms the cornerstone of management, Sterile dressing is used to dress the wound, Reconstructive surgery is considered once the infection is completely treated, , Reference, Hasham S, Matteucci P, Stanley PR, Hart NB. Necrotising fasciitis. BMJ 2005;330:830-833., Next question
Page 3110 :
A surgical trainee is incising a groin "abscess" in an intravenous drug abuser. Unfortunately the, "abscess" is a false aneurysm and torrential bleeding ensues. In the panic of the situation the doctor, then stabs himself in the finger. It transpires that the patient is a Hepatitis B carrier and the doctor is, not immunised! What type of virus is Hepatitis B?, , Double stranded DNA virus, , Single stranded DNA virus, , Double stranded RNA virus, , Single stranded RNA virus, , Retrovirus, , Please rate this question:, , Discuss and give feedback, , Next question, , Hepatitis B, Hepatitis B is a double-stranded DNA virus and is spread through exposure to infected blood or body, fluids, including vertical transmission from mother to child. The incubation period is 6-20 weeks., Immunisation against hepatitis B, , , , , , , , , Contains HBsAg absorbed onto aluminium hydroxide adjuvant and is prepared from yeast, cells using recombinant DNA technology, Most schedules give 3 doses of the vaccine with a recommendation for a one-off booster 5, years following the initial primary vaccination, At risk groups who should be vaccinated include: healthcare workers, intravenous drug, users, sex workers, close family contacts of an individual with hepatitis B, individuals, receiving blood transfusions regularly, chronic kidney disease patients who may soon require, renal replacement therapy, prisoners, chronic liver disease patients, Around 10-15% of adults fail to respond or respond poorly to 3 doses of the vaccine. Risk, factors include age over 40 years, obesity, smoking, alcohol excess and immunosuppression, Testing for anti-HBs is only recommended for those at risk of occupational exposure (i.e., Healthcare workers) and patients with chronic kidney disease. In these patients anti-HBs, levels should be checked 1-4 months after primary immunisation, The table below shows how to interpret anti-HBs levels:
Page 3111 :
Anti-HBs, level, (mIU/ml), , Response, , > 100, , Indicates adequate response, no further testing required. Should still receive, booster at 5 years, , 10 - 100, , Suboptimal response - one additional vaccine dose should be given. If, immunocompetent no further testing is required, , < 10, , Non-responder. Test for current or past infection. Give further vaccine course, (i.e. 3 doses again) with testing following. If still fails to respond then HBIG, would be required for protection if exposed to the virus, , Complications of hepatitis B infection, , , , , , , , Chronic hepatitis (5-10%), Fulminant liver failure (1%), Hepatocellular carcinoma, Glomerulonephritis, Polyarteritis nodosa, Cryoglobulinaemia, , Management of hepatitis B, , , , , , Pegylated interferon-alpha used to be the only treatment available. It reduces viral replication, in up to 30% of chronic carriers. A better response is predicted by being female, < 50 years, old, low HBV DNA levels, non-Asian, HIV negative, high degree of inflammation on liver, biopsy, However, due to the side-effects of pegylated interferon it is now used less commonly in, clinical practice. Oral antiviral medication is increasingly used with an aim to suppress viral, replication (not in dissimilar way to treating HIV patients), Examples include lamivudine, tenofovir and entecavir, Next question
Page 3112 :
Which virus is implicated in cervical carcinoma?, , Human papilloma virus 16, , Human papilloma virus 2, , Human herpes virus 8, , Human herpes virus 2, , Epstein-Barr virus, , Theme from September 2013, Please rate this question:, , Discuss and give feedback, , Next question, , Oncoviruses, , , , Viruses which cause cancer, These may be detected on blood test and prevented by vaccine, , These are the main types of oncoviruses and their diseases:, , Oncovirus, , Cancer, , Epstein-Barr virus, , Burkitt's lymphoma, Hodgkin's lymphoma, Post transplant lymphoma, Nasopharyngeal carcinoma, , Human papillomavirus 16/18, , Cervical cancer, Anal cancer, Penile cancer, Vulval cancer
Page 3113 :
Oropharyneal cancer, , Human herpes virus 8, , Kaposi's sarcoma, , Hepatitis B virus, , Hepatocellular carcinoma, , Hepatitis C virus, , Hepatocellular carcinoma, , Human T-lymphotropic virus 1, , Tropical spastic paraparesis, Adult T cell leukaemia, Next question
Page 3114 :
A young woman is admitted to hospital with E-coli 0157 after visiting Germany during an outbreak., Which of the following is not true of the condition?, , It may be complicated by micro-angiopathic haemolytic anaemia., , Adults typically develop haemolytic uraemic syndome., , It is most commonly transmitted by consumption of contaminated food., , Plasmids typically confer antibiotic resistance., , E-Coli is a gram negative organism., , Children typically develop this complication., Please rate this question:, , Discuss and give feedback, , Next question, , Bacterial Gastroenteritis, Causative organisms, , Features, , Campylobacterjejuni, , , , , , , , Shigella spp., , , , , , , , Most common cause of acute infective diarrhoea, Spiral, gram negative rods, Usually infects caecum and terminal ileum. Local, lymphadenopathy is common, May mimic appendicitis as it has marked right iliac fossa pain, Reactive arthritis is seen in 1-2% of cases, Members of the enterobacteriaceae, Gram negative bacilli, Clinically causes dysentery, Shigella soneii is the commonest infective organism (mild illness), Usually self limiting, ciprofloxacin may be required if individual, is in a high risk group
Page 3116 :
Theme: Infections, , A., B., C., D., E., F., G., H., I., , Staphylococcus aureus, Streptococcus bovis, Clostridium perfringens, Clostridium difficile, Clostridium tetani, Klebsiella, Streptococcus pyogenes, Yersinia enterocolitica, None of the above, , Please select the most likely pathogen to account for the scenario given. Each option may be used, once, more than once or not at all., , 43., , A 72 year old man with peripheral vascular disease develops a gangrenous toe. This, becomes infected and there is evidence of infection in the surrounding tissues. On clinical, palpation there is crepitus present within the tissues., You answered Staphylococcus aureus, The correct answer is Clostridium perfringens, Theme from January 2013 Exam, Clostridium perfringens is the most likely pathogen to be associated with gangrene., , 44., , A 22 year old lady is breastfeeding her first child. One week post partum she presents with, a tender indurated mass in the right breast., Staphylococcus aureus, Staphylococcus aureus is the commonest cause of lactational mastitis., , 45., , A 45 year old man is recovering in hospital following a total hip replacement. He develops, a profuse and watery diarrhoea. Several other patients have been suffering from similar, symptoms., You answered Staphylococcus aureus, The correct answer is Clostridium difficile, Clostridium difficile can spread rapidly on surgical wards. The use of broad spectrum, prophylactic antibiotics during arthroplasty surgery can increase the risk.
Page 3117 :
Please rate this question:, , Discuss and give feedback, , Next question, , Surgical Microbiology, An extensive topic so an overview is given here. Organisms causing common surgical infections are, reasonable topics in the examination. However, microbiology is less rigorously tested than anatomy,, for example., Common organisms, Staphylococcus aureus, , , , , , , , , , , Facultative anaerobe, Gram positive coccus, Haemolysis on blood agar plates, Catalase positive, 20% population are long term carriers, Exo and entero toxin may result in toxic shock syndrome and gastroenteritis respectively, Ideally treated with penicillin although many strains now resistant through beta Lactamase, production. In the UK less than 5% of isolates are sensitive to penicillin., Resistance to methicillin (and other antibiotics) is mediated by the mec operon , essentially, penicillin binding protein is altered and resistance to this class of antibiotics ensues, Common cause of cutaneous infections and abscesses, , Streptococcus pyogenes, , , , , , , , , Gram positive, forms chain like colonies, Lancefield Group A Streptococcus, Produces beta haemolysis on blood agar plates, Rarely part of normal skin microflora, Catalase negative, Releases a number of proteins/ virulence factors into host including hyaluronidase,, streptokinase which allow rapid tissue destruction, Releases superantigens such as pyogenic exotoxin A which results in scarlet fever, Remains sensitive to penicillin, macrolides may be used as an alternative., , Escherichia coli, , , , , Gram negative rod, Facultative anaerobe, non sporing, Wide range of subtypes and some are normal gut commensals
Page 3118 :
, , , , , Some subtypes such as 0157 may produce lethal toxins resulting in haemolytic-uraemic, syndrome, Enterotoxigenic E-Coli produces an enterotoxin (ST enterotoxin) that results in large, volume fluid secretion into the gut lumen (Via cAMP activation), Enteropathogenic E-Coli binds to intestinal cells and cause structural damage, this coupled, with a moderate (or in case of enteroinvasive E-Coli significant) invasive component, produces enteritis and large volume diarrhoea together with fever., They are resistant to many antibiotics used to treat gram positive infections and acquire, resistance rapidly and are recognised as producing beta lactamases, , Campylobacter jejuni, , , , , , , Curved, gram negative, non sporulating bacteria, One of the commonest causes of diarrhoea worldwide, Produces enteritis which is often diffuse and blood may be passed, Remains a differential for right iliac fossa pain with diarrhoea, Self limiting infection so antibiotics are not usually advised. However, the quinolones are, often rapidly effective., , Helicobacter pylori, , , , , , , , , , , Gram negative, helix shaped rod, microaerophillic, Produces hydrogenase that can derive energy from hydrogen released by intestinal bacteria, Flagellated and mobile, Those carrying the cag A gene may cause ulcers, It secretes urease that breaks down gastric urea> Carbon dioxide and ammonia>, ammonium>bicarbonate (simplified!) The bicarbonate can neutralise the gastric acid., Usually colonises the gastric antrum and irritates resulting in increased gastrin release and, higher levels of gastric acid. These patients will develop duodenal ulcers. In those with more, diffuse H-Pylori infection gastric acid levels are lower and ulcers develop by local tissue, damage from H-Pylori- these patients get gastric ulcers., Diagnosis may be made by serology (approx. 75% sensitive). Biopsy urease test during, endoscopy probably the most sensitive., In patients who are colonised 10-20% risk of peptic ulcer, 1-2% risk gastric cancer, <1% risk, MALT lymphoma., Next question
Page 3119 :
A 27-year-old male presents to urology for investigation of pyelonephritis. He reports malaise,, pyrexia, lymphadenopathy and a maculopapular rash. The Monospot test is negative. Given a, history of high-risk sexual behaviour you are asked to exclude a HIV seroconversion illness. What is, the most appropriate investigation?, , Antibodies to HIV-2, , gp120 polymerase chain reaction, , p24 antigen test, , CCR5 polymerase chain reaction, , Antibodies to HIV-1, , Please rate this question:, , Discuss and give feedback, , Next question, , HIV testing, HIV seroconversion is symptomatic in 60-80% of patients and typically presents as a glandular fever, type illness. Increased symptomatic severity is associated with poorer long term prognosis. It, typically occurs 3-12 weeks after infection, Features, , , , , , , , , sore throat, lymphadenopathy, malaise, myalgia, arthralgia, diarrhoea, maculopapular rash, mouth ulcers, rarely meningoencephalitis, , Diagnosis, , , antibodies to HIV may not be present
Page 3120 :
, , HIV PCR and p24 antigen tests can confirm diagnosis, , HIV antibody test, , , , , most common and accurate test, usually consists of both a screening ELISA (Enzyme Linked Immuno-Sorbent Assay) test, and a confirmatory Western Blot Assay, most people develop antibodies to HIV at 4-6 weeks but 99% do by 3 months, , p24 antigen test, , , , usually positive from about 1 week to 3 - 4 weeks after infection with HIV, sometimes used as an additional screening test in blood banks, Next question
Page 3121 :
Which statement relating to actinomycosis is false?, , They are gram positive bacilli, , They are strict aerobes, , It may be a cause of chronic multiple abscesses, , Abdominal cases may develop in the appendix, , Open biopsy of the lesions is the best diagnostic test, , They are facultative anaerobes and may be difficult to culture. Direct visualisation of organisms and, sulphur granules from lesions themselves is the easiest way to make a diagnosis. It remains a, differential of conditions such as hydradenitis supprativa, particularly if it is occurring in odd locations, and with deeper abscesses than usual., Please rate this question:, , Discuss and give feedback, , Surgical Microbiology, An extensive topic so an overview is given here. Organisms causing common surgical infections are, reasonable topics in the examination. However, microbiology is less rigorously tested than anatomy,, for example., Common organisms, Staphylococcus aureus, , , , , , , , , , , Facultative anaerobe, Gram positive coccus, Haemolysis on blood agar plates, Catalase positive, 20% population are long term carriers, Exo and entero toxin may result in toxic shock syndrome and gastroenteritis respectively, Ideally treated with penicillin although many strains now resistant through beta Lactamase, production. In the UK less than 5% of isolates are sensitive to penicillin., Resistance to methicillin (and other antibiotics) is mediated by the mec operon , essentially, penicillin binding protein is altered and resistance to this class of antibiotics ensues, Common cause of cutaneous infections and abscesses
Page 3122 :
Streptococcus pyogenes, , , , , , , , , Gram positive, forms chain like colonies, Lancefield Group A Streptococcus, Produces beta haemolysis on blood agar plates, Rarely part of normal skin microflora, Catalase negative, Releases a number of proteins/ virulence factors into host including hyaluronidase,, streptokinase which allow rapid tissue destruction, Releases superantigens such as pyogenic exotoxin A which results in scarlet fever, Remains sensitive to penicillin, macrolides may be used as an alternative., , Escherichia coli, , , , , , , , , Gram negative rod, Facultative anaerobe, non sporing, Wide range of subtypes and some are normal gut commensals, Some subtypes such as 0157 may produce lethal toxins resulting in haemolytic-uraemic, syndrome, Enterotoxigenic E-Coli produces an enterotoxin (ST enterotoxin) that results in large, volume fluid secretion into the gut lumen (Via cAMP activation), Enteropathogenic E-Coli binds to intestinal cells and cause structural damage, this coupled, with a moderate (or in case of enteroinvasive E-Coli significant) invasive component, produces enteritis and large volume diarrhoea together with fever., They are resistant to many antibiotics used to treat gram positive infections and acquire, resistance rapidly and are recognised as producing beta lactamases, , Campylobacter jejuni, , , , , , , Curved, gram negative, non sporulating bacteria, One of the commonest causes of diarrhoea worldwide, Produces enteritis which is often diffuse and blood may be passed, Remains a differential for right iliac fossa pain with diarrhoea, Self limiting infection so antibiotics are not usually advised. However, the quinolones are, often rapidly effective., , Helicobacter pylori, , , , , , , Gram negative, helix shaped rod, microaerophillic, Produces hydrogenase that can derive energy from hydrogen released by intestinal bacteria, Flagellated and mobile, Those carrying the cag A gene may cause ulcers, It secretes urease that breaks down gastric urea> Carbon dioxide and ammonia>, ammonium>bicarbonate (simplified!) The bicarbonate can neutralise the gastric acid.
Page 3123 :
, , , , , Usually colonises the gastric antrum and irritates resulting in increased gastrin release and, higher levels of gastric acid. These patients will develop duodenal ulcers. In those with more, diffuse H-Pylori infection gastric acid levels are lower and ulcers develop by local tissue, damage from H-Pylori- these patients get gastric ulcers., Diagnosis may be made by serology (approx. 75% sensitive). Biopsy urease test during, endoscopy probably the most sensitive., In patients who are colonised 10-20% risk of peptic ulcer, 1-2% risk gastric cancer, <1% risk, MALT lymphoma.
Page 3124 :
What is the earliest complication that can occur following construction of an ileostomy?, , Prolapse, , Retraction, , Necrosis, , Parastomal hernia, , Dermatitis, , Construction of a stoma may be complicated by several factors. Necrosis may occur because of, technical errors in mesenteric division, excessive tension or failure to construct a fascial defect of, adequate size to permit safe passage of the mesentery and the bowel., Please rate this question:, , Discuss and give feedback, , Next question, , Ileostomy, Ileostomies are generally fashioned in the right iliac fossa in a triangle between the anterior superior, iliac spine, symphysis pubis and umbilicus. They should lie one-third of the distance between the, umbilicus and anterior superior iliac spine. A 2cm skin incision is made and dissection continued, through the rectus muscle. A cruciate incision should be made, and generally dilated to admit two, fingers. The ileum is brought through the incisions and should generally be spouted to a final length, of 2.5cm. Ileostomies that are too short may cause problems with appliance fixation and those which, are too long may cause problems with tension and subsequent ulceration or prolapse., Complications following ileostomy construction include dermatitis (most common), bowel obstruction, (usually adhesional) and prolapse., Ileostomy output is roughly in the range of 5-10ml/Kg/ 24 hours. Output in excess of 20ml/Kg/24, hours usually requires supplementary intravenous fluids. Excessive fluid losses are generally, managed by administration of oral loperamide (up to 4mg QDS) to try and slow the output. Foods, containing gelatine may also thicken output. Early high output is not uncommon and most patients, (50%) will respond to conservative management., Next question
Page 3125 :
Theme: Proctology, , A. Fissure in ano, B. Fistula in ano, C. Rectal prolapse, D. Juvenile polyps, E. Rectal adenoma, F. Intersphincteric abscess, G. Haemorrhoids, , Please select the most likely underlying cause for the presentations described. Each option may be, used once, more than once or not at all., , 2., , A 21 year old female presents with a 24 hour history of increasingly severe ano-rectal pain. On, examination she is febrile and the skin surrounding the anus looks normal. She did not tolerate an, attempted digital rectal examination., You answered Fissure in ano, The correct answer is Intersphincteric abscess, Theme from September 2012 Exam, The presence of fever and severe pain makes an abscess more likely than a fissure. Although, fissures may be painful they do not, in themselves, cause fever. The usual management for this, condition is examination of the ano-rectum under general anaesthesia and drainage of the sepsis., , 3., , A 21 year old male presents with a 4 week history of frank, bright red, rectal bleeding. This typically, occurs post defecation into the toilet pan. He has a long standing history of constipation and a, previous fissure in ano. On examination the skin surrounding the anus is normal and digital rectal, examination is normal., You answered Fissure in ano
Page 3126 :
The correct answer is Haemorrhoids, Haemorrhoids are a common cause of bright red rectal bleeding. The bleeding is typically painless., A history of constipation is usual and may have been previously associated with a fissure (though, this is less common). Haemorrhoids are not always associated with external features and digital, rectal examination is usually unremarkable., , 4., , A 21 year old lady presents with a 6 month history of an offensive discharge from the anus. She is, otherwise well, but is increasingly annoyed at the need to wear pads. On examination she has a, small epithelial defect in the 5 o'clock position, approximately 3cm from the anal verge., You answered Fissure in ano, The correct answer is Fistula in ano, Fistulas usually occur following previous ano-rectal sepsis. The discharge may be foul smelling and, troublesome. Patients should be listed for examination under anaesthesia. Fistulas which are low, and have little or no sphincter involvement are usually laid open., , Please rate this question:, , Discuss and give feedback, , Next question, , Ano rectal disease, , Haemorrhoids, , Fissure in ano, , Location: 3, 7, 11 o'clock position, Internal or external, Treatment: Conservative, Rubber band ligation, Haemorrhoidectomy, , Location: midline 6 (posterior midline 90%) and 12 o'clock position. Distal to the, dentate line
Page 3127 :
Chronic fissure > 6/52: triad: Ulcer, sentinel pile, enlarged anal papillae, , Proctitis, , Causes: Crohn's, ulcerative colitis, Clostridium difficile, , Ano rectal, abscess, , E.coli, staph aureus, Positions: Perianal, Ischiorectal, Pelvirectal, Intersphincteric, , Anal fistula, , Usually due to previous ano-rectal abscess, Intersphincteric, transsphincteric, suprasphincteric, and extrasphincteric. Goodsalls, rule determines location, , Rectal prolapse, , Associated with childbirth and rectal intussceception. May be internal or external, , Pruritus ani, , Systemic and local causes, , Anal neoplasm, , Squamous cell carcinoma commonest unlike adenocarcinoma in rectum, , Solitary rectal, ulcer, , Associated with chronic straining and constipation. Histology shows mucosal, thickening, lamina propria replaced with collagen and smooth muscle (fibromuscular, obliteration), , Rectal prolapse, , , , , , , , Common especially in multiparous women., May be internal or external., Internal rectal prolapse can present insidiously., External prolapse can ulcerate and in long term impair continence., Diagnostic work up includes colonoscopy, defecating proctogram, ano rectal manometry, studies and if doubt exists an examination under anaesthesia., , Treatments for prolapse, , , , In the acute setting reduce it (covering it with sugar may reduce swelling.
Page 3128 :
, , , , Delormes procedure which excises mucosa and plicates the rectum (high recurrence rates), may be used for external prolapse., Altmeirs procedure which resects the colon via the perineal route has lower recurrence rates, but carries the risk of anastamotic leak., Rectopexy is an abdominal procedure in which the rectum is elevated and usually supported, at the level of the sacral promontory. Post operative constipation may be reduced by limiting, the dissection to the anterior plane (laparoscopic ventral mesh rectopexy)., , Pruritus ani, , , , , , , , , Extremely common., Check not secondary to altered bowel habits (e.g. Diarrhoea), Associated with underlying diseases such as haemorrhoids., Examine to look for causes such as worms., Proctosigmoidoscopy to identify associated haemorrhoids and exclude cancer., Treatment is largely supportive and patients should avoid using perfumed products around, the area., , Fissure in ano, , , , , , Typically painful PR bleeding (bright red)., Nearly always in the posterior midline., Usually solitary., , Treatment, , , , , , , , Stool softeners., Topical diltiazem (or GTN)., If topical treatments fail then botulinum toxin should be injected., If botulinum toxin fails then males should probably undergo lateral internal sphincterotomy., Females who do not respond to botulinum toxin should undergo ano rectal manometry, studies and endo anal USS prior to being offered surgery such as sphincterotomy., Next question
Page 3129 :
Theme: Management of ano-rectal disease, , A. Excision and primary closure, B. Incision and drainage, C. Topical steroids, D. Topical diltiazem, E. Steroid injections, F. Haemorroidectomy, G. Manual anal dilation, H. Injection with 88% aqueous phenol, I. Sphincterotomy, , Please select the most appropriate management for the situation described. Each option may be, used once, more than once or not at all., , 5., , A 19 year old female presents with severe anal pain and bleeding which typically occurs post, defecation. On examination she has a large posteriorly sited fissure in ano., You answered Excision and primary closure, The correct answer is Topical diltiazem, Theme from January 2013 Exam, Theme from April 2014 Exam, Initial therapy should be with pharmacological agents to relax the sphincter and facilitate healing., This is particularly true in females presenting for the first time., , 6., , A 43 year old male has been troubled with symptoms of post defecation bleeding for many years., On examination he has large prolapsed haemorroids, colonoscopy shows no other disease., You answered Excision and primary closure
Page 3130 :
The correct answer is Haemorroidectomy, Prolapsed haemorroids are best managed surgically if symptomatic. Note that phenol injections, are usually only used for minor internal haemorroids. Where used low concentration phenol in oil, is used, the phenolic solution above is used to ablate the nail bed in toe nail surgery!, , 7., , A 20 year old man presents with a 24 hour history of anal pain. On examination he has a peri anal, abscess., You answered Excision and primary closure, The correct answer is Incision and drainage, Abscesses require incision and drainage as a first line treatment., , Please rate this question:, , Discuss and give feedback, , Next question, , Benign proctology, Condition, , Features, , Treatment, , Fissure in ano, , Painful, bright red rectal bleeding, , Stool softeners, topical diltiazem or GTN,, botulinum toxin, Sphincterotomy, , Haemorroids, , Painless, bright red rectal bleeding, occurs following defecation and bleeds, onto the toilet paper and into the toilet, pan, , Stool softeners, avoid straining, surgery (see, below)
Page 3131 :
Fistula in ano, , May initially present with an abscess and, then persisting discharge onto the, perineum, separate from the anus, , Lay open if low, no sphincter involvement or, IBD, if complex, high or IBD insert seton and, consider other options (see below), , Peri anal, abscess, , Peri anal swelling and surrounding, erythema, , Incision and drainage, leave the cavity open, to heal by secondary intention, , Pruritus ani, , Peri anal itching, occasional mild, bleeding (if severe skin damage), , Avoid scented products, use wet wipes rather, than tissue, avoidance of scratching, ensure, no underlying faecal incontinence, , Overview of surgical therapies, Haemorroidal disease, The treatment of haemorroids is usually conservative. Acutely thrombosed haemorroids may be, extremely painful. Treatment of this acute condition is usually conservative and consists of stool, softeners, ice compressions and topical GTN or diltiazem to reduce sphincter spasm. Most cases, managed with this approach will settle over the next 5-7 days. After this period there may be residual, skin tags that merit surgical excision or indeed residual haemorroidal disease that may necessitate, haemorroidectomy., Patients with more chronic symptoms are managed according to the stage of their disease, small, mild internal haemorroids causing little symptoms are best managed conservatively. More marked, symptoms of bleeding and occasional prolapse, where the haemorroidal complex is largely internal, may benefit from stapled haemorroidopexy. This procedure excises rectal tissue above the dentate, line and disrupts the haemorroidal blood supply. At the same time the excisional component of the, procedure means that the haemorroids are less prone to prolapse. Adverse effects of this procedure, include urgency, which can affect up to 40% of patients (but settles over 6-12 months) and, recurrence. The procedure does not address skin tags and therefore this procedure is unsuitable if, this is the dominant symptom., Large haemorroids with a substantial external component may be best managed with a Milligan, Morgan style conventional haemorroidectomy. In this procedure three haemorroidal cushions are, excised, together with their vascular pedicle. Excision of excessive volumes of tissue may result in, anal stenosis. The procedure is quite painful and most surgeons prescribe metronidazole post, operatively as it decreases post operative pain., Fissure in ano, Probably the most efficient and definitive treatment for fissure in ano is lateral internal, sphincterotomy. The treatment is permanent and nearly all patients will recover. Up to 30% will, develop incontinence to flatus. There are justifiable concerns about using this procedure in females, as pregnancy and pelvic floor damage together with a sphincterotomy may result in faecal, incontinence. The usual first line therapy is relaxation of the internal sphincter with either GTN or, diltiazem (the latter being better tolerated) applied topically for 6 weeks. Treatment failures with
Page 3132 :
topical therapy will usually go on to have treatment with botulinum toxin. This leads to more, permanent changes in the sphincter and this may facilitate healing., Typical fissures usually present in the posterior midline, multiple or unusually located fissures should, prompt a search for an underlying cause such as inflammatory bowel disease or internal prolapse., Refractory cases where the above treatments have failed may be considered for advancement, flaps., Fistula in ano, The most effective treatment for fistula is laying it open (fistulotomy). When the fistula is below the, sphincter and uncomplicated, this is a reasonable option. Sphincter involvement and complex, underlying disease should be assessed both surgically and ideally with imaging (either MRI or, endoanal USS). Surgery is then usually staged, in the first instance a draining seton suture may be, inserted. This avoids the development of recurrent sepsis and may allow resolution. In patients with, Crohns disease the seton should be left in situ long term and the patient managed medically, as in, these cases attempts at complex surgical repair nearly always fail. Fistulas not associated with IBD, may be managed by advancement flaps, instillation of plugs and glue is generally unsuccessful. A, newer technique of ligation of intersphincteric tract (LIFT procedure) is reported to have good results, in selected centres., Next question
Page 3133 :
Theme: Management of colonic polypoidal lesions, , A. Reassure and discharge, B. Pan proctocolectomy, C. Hot biopsy, D. Snare polypectomy, E. Segmental colonic resection, F. Repeat endoscopy at 3 years, G. Repeat endoscopy at 1 year, H. Repeat endoscopy at 5 years, , Please select the most appropriate management for the scenario given. Each option may be used, once, more than once or not at all., , 8., , A 43 year old man is investigated for altered bowel habit. At colonoscopy he is found to have a, 2cm polyp on a long stalk in the proximal sigmoid colon. The rest of the colonoscopy is normal. It, bears no macroscopic features of malignancy., You answered Reassure and discharge, The correct answer is Snare polypectomy, Polyps on long stalks are best managed by snare excision. It is important to retrieve the polyp for, histology., , 9., , A 60 year old lady is investigated for abdominal pain. A polyp is identified at the proximal, descending colon, three small polyps are also noted in the sigmoid colon. The largest lesion is, removed by snare polypectomy and the pathology report states that this polyp is a low grade, dysplastic adenoma measuring 3cm in diameter. The remaining lesions are ablated using, diathermy., You answered Reassure and discharge
Page 3134 :
The correct answer is Repeat endoscopy at 1 year, She is at high risk of malignancy and should be closely followed up. Fulguration of polyps without, histology is unhelpful., , 10., , A 73 year old lady is investigated for anaemia. At colonoscopy she is found to have a flat broad, based lesion in the caecum. This is biopsied and the histology report states that these have, diagnostic features of an adenoma with high grade dysplasia., You answered Reassure and discharge, The correct answer is Segmental colonic resection, Management of right sided colonic polyps such as this is controversial. There is a high liklihood, that this lesion will harbor an focus on invasive malignancy (which should generally be managed, with resection). This is further suggested by the background history of anaemia. It is for this, reason that resection over right sided colonic endoscopic mucosal resection is chosen., , Polypectomy of flat broad lesions in the right colon is difficult and where concern arises a right, hemicolectomy is probably the safest option., , Please rate this question:, , Discuss and give feedback, , Next question, , Colonic polyps, Colonic Polyps, May occur in isolation, or greater numbers as part of the polyposis syndromes. In FAP greater than, 100 polyps are typically present. The risk of malignancy in association with adenomas is related to, size, and is the order of 10% in a 1cm adenoma. Isolated adenomas seldom give risk of symptoms, (unless large and distal). Distally sited villous lesions may produce mucous and if very large,, electrolyte disturbances may occur.
Page 3135 :
Follow up of colonic polyps, , Group, , Features, , Action, , Low risk, , 1 or 2 adenomas less than 1cm, , No follow up or re-colonoscopy, at 5 years, , Moderate, risk, , 3 or 4 small adenomas or 1 adenoma greater than 1cm, , Re-scope at 3 years, , High risk, , More than 5 small adenomas or more than 3 with 1 of, them greater than 1cm, , Re scope at 1 year, , From Atkins and Saunders Gut 2002 51 (suppl V:V6-V9). It is important to stratify patients, appropriately and ensure that a complete colonoscopy with good views was performed., Segmental resection or complete colectomy should be considered when:, 1. Incomplete excision of malignant polyp, 2. Malignant sessile polyp, 3. Malignant pedunculated polyp with submucosal invasion, 4. Polyps with poorly differentiated carcinoma, 5. Familial polyposis coli, -Screening from teenager up to 40 years by 2 yearly sigmoidoscopy/colonoscopy, -Panproctocolectomy and Ileostomy or Restorative Panproctocolectomy., Rectal polypoidal lesions may be amenable to trans anal endoscopic microsurgery., References, Cairns S et al. Guidelines for colorectal cancer screening and surveillance in moderate and high risk, groups (update from 2002). Gut 2010;59:666-690., Next question
Page 3136 :
Theme: Colonic resections, , A. End ileostomy, B. Loop ileostomy, C. Ileo anal pouch, D. Loop colostomy, E. Pan proctocelectomy, F. Extended right hemicolectomy, G. Right hemicolectomy, H. Anterior resection, I. Anterior resection with covering loop ileostomy, , Please select the most appropriate procedure from the list, each option may be used once, more, than once or not at all., , 11., , A 75 year old man requires resection of an obstructing carcinoma of the splenic flexure., You answered End ileostomy, The correct answer is Extended right hemicolectomy, Carcinoma of the splenic flexure requires extended right hemicolectomy. Or a left, hemicolectomy. The ileocolic anastomosis has a lower leak rate, particularly when the bowel is, obstructed., , 12., , A patient presenting with a large bowel obstruction from a low rectal cancer., You answered End ileostomy, The correct answer is Loop colostomy, This patient should be defunctioned, definitive surgery should wait until staging is completed. A
Page 3137 :
loop ileostomy will not satisfactorily decompress an acutely obstructed colon. Low rectal cancers, that are obstructed should not usually be primarily resected. The obstructed colon that would be, used for anastomosis would carry a high risk of anastomotic dehisence. In addition, as this is an, emergency presentation, staging may not be completed, an attempted resection may therefore, compromise the circumferential resection margin, with an associated risk of local recurrence., , 13., , A 45 year old man presents with a carcinoma 10cm from the anal verge, he has completed a long, course of chemoradiotherapy and has achieved downstaging with no evidence of threatened, circumferential margin on MRI scanning., You answered End ileostomy, The correct answer is Anterior resection with covering loop ileostomy, Low rectal cancer is usually treated with a low anterior resection. Contraindications to this include, involvement of the sphincters (unlikely here) and poor sphincter function that would lead to, unsatisfactory function post resection. Most colorectal surgeons defunction resections below the, peritoneal reflection as they have an intrinsically high risk of anastomotic leak. A loop ileostomy, provides a safe an satisfactory method of defunctioning these patients. A contrast enema should, be performed prior to stoma reversal., , Please rate this question:, , Discuss and give feedback, , Next question, , Colorectal cancer treatment, Patients diagnosed as having colorectal cancer should be completely staged using CT of the chest/, abdomen and pelvis. Their entire colon should have been evaluated with colonoscopy or CT, colonography. Patients whose tumours lie below the peritoneal reflection should have their, mesorectum evaluated with MRI., Once their staging is complete patients should be discussed within a dedicated colorectal MDT, meeting and a treatment plan formulated.
Page 3138 :
Treatment of colonic cancer, Cancer of the colon is nearly always treated with surgery. Stents, surgical bypass and diversion, stomas may all be used as palliative adjuncts. Resectional surgery is the only option for cure in, patients with colon cancer. The procedure is tailored to the patient and the tumour location. The, lymphatic drainage of the colon follows the arterial supply and therefore most resections are tailored, around the resection of particular lymphatic chains (e.g. ileo-colic pedicle for right sided tumours)., Some patients may have confounding factors that will govern the choice of procedure, for example a, tumour in a patient from a HNPCC family may be better served with a panproctocolectomy rather, than segmental resection. Following resection the decision has to be made regarding restoration of, continuity. For an anastomosis to heal the key technical factors include; adequate blood supply,, mucosal apposition and no tissue tension. Surrounding sepsis, unstable patients and inexperienced, surgeons may compromise these key principles and in such circumstances it may be safer to, construct an end stoma rather than attempting an anastomosis., When a colonic cancer presents with an obstructing lesion; the options are to either stent it or resect., In modern practice it is unusual to simply defunction a colonic tumour with a proximal loop stoma., This differs from the situation in the rectum (see below)., Following resection patients with risk factors for disease recurrence are usually offered, chemotherapy, a combination of 5FU and oxaliplatin is common., Rectal cancer, The management of rectal cancer is slightly different to that of colonic cancer. This reflects the, rectum's anatomical location and the challenges posed as a result. Tumours located in the rectum, can be surgically resected with either an anterior resection or an abdomino - perineal resection. The, technical aspects governing the choice between these two procedures can be complex to appreciate, and the main point to appreciate for the MRCS is that involvement of the sphincter complex or very, low tumours require APER. In the rectum a 2cm distal clearance margin is required and this may, also impact on the procedure chosen. In addition to excision of the rectal tube an integral part of the, procedure is a meticulous dissection of the mesorectal fat and lymph nodes (total mesorectal, excision/ TME). In rectal cancer surgery invovlement of the cirumferential resection margin carries a, high risk of disease recurrence. Because the rectum is an extraperitoneal structure (until you remove, it that is!) it is possible to irradiate it, something which cannot be offered for colonic tumours. This, has a major impact in rectal cancer treatment and many patients will be offered neoadjuvent, radiotherapy (both long and short course) prior to resectional surgery. Patients with T1 and 2 /N0, disease on imaging do not require irradiation and should proceed straight to surgery. Patients with, T4 disease will typically have long course chemo radiotherapy. Those with T3 , N0 tumours may be, offered short course radiotherapy prior to surgery. Patients presenting with large bowel obstruction, from rectal cancer should not undergo resectional surgery without staging as primary treatment (very, different from colonic cancer). This is because rectal surgery is more technically demanding, the, anastomotic leak rate is higher and the danger of a positive resection margin in an unstaged patient, is high. Therefore patients with obstructing rectal cancer should have a defunctioning loop, colostomy., Summary of procedures, The operations for cancer are segmental resections based on blood supply and lymphatic drainage., These commonly performed procedures are core knowledge for the MRCS and should be
Page 3139 :
understood., , Site of cancer, , Type of resection, , Anastomosis, , Risk of, leak, , Right colon, , Right hemicolectomy, , Ileo-colic, , Low <5%, , Transverse, , Extended right hemicolectomy, , Ileo-colic, , Low <5%, , Splenic, flexure, , Extended right hemicolectomy, , Ileo-colic, , Low <5%, , Splenic, flexure, , Left hemicolectomy, , Colo-colon, , 2-5%, , Left colon, , Left hemicolectomy, , Colo-colon, , 2-5%, , Sigmoid colon, , High anterior resection, , Colo-rectal, , 5%, , Upper rectum, , Anterior resection (TME), , Colo-rectal, , 5%, , Low rectum, , Anterior resection (Low TME), , Colo-rectal, (+/- Defunctioning, stoma), , 10%, , Anal verge, , Abdomino-perineal excision of colon and, rectum, , None, , n/a, , In the emergency setting, where the bowel has perforated, the risk of an anastomosis is much, greater, particularly when the anastomosis is colon-colon. In this situation, an end colostomy is often, safer and can be reversed later. When resection of the sigmoid colon is performed and an end, colostomy is fashioned the operation is referred to as a Hartmans procedure. Whilst left sided, resections are more risky, ileo-colic anastomoses are relatively safe even in the emergency setting
Page 3140 :
and do not need to be defunctioned., References, A review of the diagnosis and management of colorectal cancer and a summary of the UK National, Institute of Clinical Excellence guidelines is provided in:, Poston G, et al . Diagnosis and management of colorectal cancer:summary of NICE, guidance. BMJ2011: 343: d 6751., Next question
Page 3141 :
A 62 year old man has previously undergone a left hemicolectomy for carcinoma of the descending, colon. On follow up imaging he is found to have two deposits of metastatic disease located in the, right lobe of his liver. What is the best treatment strategy?, , Chemotherapy alone, , Chemotherapy followed by surgical resection, , Radiofrequency ablation, , Chemoradiotherapy, , Palliation, , Theme from April 2016 Exam, Liver metastasis from colorectal cancer is still potentially curable. Without resection, survival at 5, years is around 5%. With resection, this figure rises to around 20%. The best outcomes are seen, where chemotherapy is given, followed by resection. Radiofrequency ablation is an option for those, patients who lack the physiological reserve for surgery. However, there is longer term recurrence, rates will all the non resectional strategies. There is no role for radiotherapy., Please rate this question:, , Discuss and give feedback, , Next question, , Colorectal cancer, , , , , , , , , , Annually about 150,000 new cases are diagnosed and 50,000 deaths from the disease, About 75% will have sporadic disease and 25% will have a family history, Colorectal tumours comprise a spectrum of disease ranging from adenomas through to polyp, cancers and frank malignancy., Polyps may be categorised into: neoplastic polyps, adenomatous polyps and non neoplastic, polyps., The majority of adenomas are polypoidal lesions, although flat lesions do occur and may, prove to be dysplastic., Non-neoplastic polyps include hyperplastic, juvenile, hamartomatous, inflammatory, and, lymphoid polyps, which have not generally been thought of as precursors of cancer., Three characteristics of adenomas that correlate with malignant potential have been, characterised. These include increased size, villous architecture and dysplasia. For this, reason most polyps identified at colonoscopy should be removed., The transformation from polyp to cancer is described by the adenoma - carcinoma sequence, and its principles should be appreciated. Essentially genetic changes accompany the
Page 3143 :
A 70 year old female is admitted with a history of passing brown coloured urine and abdominal, distension. Clinically she has features of large bowel obstruction with central abdominal tenderness., She is maximally tender in the left iliac fossa. There is no evidence of haemodynamic instability., What is the most appropriate investigation?, , Cystogram, , Abdominal X-ray of the kidney, ureters and bladder, , Computerised tomogram of the abdomen and pelvis, , Flexible sigmoidoscopy, , Barium enema, , Theme from April 2013 Exam, Theme from April 2014 exam, This lady is most likely to have a colovesical fistula complicating diverticular disease of the sigmoid, colon. In addition she may also have developed a diverticular stricture resulting in large bowel, obstruction. A locally advanced tumour of the sigmoid colon may produce a similar clinical picture., The best investigation of this acute surgical patient is an abdominal CT scan, this will demonstrate, the site of the disease and also supply regional information such as organ involvement and other, local complications such as a pericolic abscess. A barium enema would require formal bowel, preparation and this is contra indicated where large bowel obstruction is suspected. A flexible, sigmoidoscopy is unlikely to be helpful and the air insufflated at the time of endoscopy may make the, colonic distension worse. A cystogram would provide only very limited information., Please rate this question:, , Discuss and give feedback, , Next question, , Diverticular disease, Diverticular disease is a common surgical problem. It consists of herniation of colonic mucosa, through the muscular wall of the colon. The usual site is between the taenia coli where vessels, pierce the muscle to supply the mucosa. For this reason, the rectum, which lacks taenia, is often, spared., Symptoms, , , Altered bowel habit
Page 3144 :
, , , Bleeding, Abdominal pain, , Complications, , , , , , , , Diverticulitis, Haemorrhage, Development of fistula, Perforation and faecal peritonitis, Perforation and development of abscess, Development of diverticular phlegmon, , Diagnosis, Patients presenting in clinic will typically undergo either a colonoscopy, CT cologram or barium, enema as part of their diagnostic work up. All tests can identify diverticular disease. It can be far, more difficult to confidently exclude cancer, particularly in diverticular strictures., Acutely unwell surgical patients should be investigated in a systematic way. Plain abdominal films, and an erect chest x-ray will identify perforation. An abdominal CT scan (not a CT cologram) with, oral and intravenous contrast will help to identify whether acute inflammation is present but also the, presence of local complications such as abscess formation., , Severity Classification- Hinchey, , I, , Para-colonic abscess, , II, , Pelvic abscess, , III, , Purulent peritonitis, , IV, , Faecal peritonitis, , Treatment, , , , , , Increase dietary fibre intake., Mild attacks of diverticulitis may be managed conservatively with antibiotics., Peri colonic abscesses should be drained either surgically or radiologically., Recurrent episodes of acute diverticulitis requiring hospitalisation are a relative indication for, a segmental resection.
Page 3145 :
, , Hinchey IV perforations (generalised faecal peritonitis) will require a resection and usually a, stoma. This group have a very high risk of post operative complications and usually require, HDU admission. Less severe perforations may be managed by laparoscopic washout and, drain insertion., Next question
Page 3146 :
Which of the following statements in relation to fistula in ano is untrue?, , High fistulae are safest treated with a seton insertion, , Low fistulae may be laid open, , They are typically probed with Lockhart Mummary probes, , When discovered during incision and drainage of peri anal abscess; should always be, probed to locate the internal opening, When complicating Crohns disease, may respond to infliximab, , Probing fistulae during acute sepsis is associated with a high complication rate and should not be, undertaken routinely., Please rate this question:, , Discuss and give feedback, , Next question, , Fistulas, , , , , , A fistula is defined as an abnormal connection between two epithelial surfaces., There are many types ranging from Branchial fistulae in the neck to entero-cutaneous, fistulae abdominally., In general surgical practice the abdominal cavity generates the majority and most of these, arise from diverticular disease and Crohn's., As a general rule all fistulae will resolve spontaneously as long as there is no distal, obstruction. This is particularly true of intestinal fistulae., , The four types of fistulae are:, Enterocutaneous, These link the intestine to the skin. They may be high (>500ml) or low output (<250ml) depending, upon source. Duodenal /jejunal fistulae will tend to produce high volume, electrolyte rich secretions, which can lead to severe excoriation of the skin. Colo-cutaneous fistulae will tend to leak faeculent, material. Both fistulae may result from the spontaneous rupture of an abscess cavity onto the skin, (such as following perianal abscess drainage) or may occur as a result of iatrogenic input. In some, cases it may even be surgically desirable e.g. mucous fistula following sub total colectomy for colitis., Suspect if there is excess fluid in the drain.
Page 3147 :
Enteroenteric or Enterocolic, This is a fistula that involves the large or small intestine. They may originate in a similar manner to, enterocutaneous fistulae. A particular problem with this fistula type is that bacterial overgrowth may, precipitate malabsorption syndromes. This may be particularly serious in inflammatory bowel, disease., Enterovaginal, Aetiology as above., Enterovesicular, This type of fistula goes to the bladder. These fistulas may result in frequent urinary tract infections,, or the passage of gas from the urethra during urination., Management, Some rules relating to fistula management:, , , , , , , , , They will heal provided there is no underlying inflammatory bowel disease and no distal, obstruction, so conservative measures may be the best option, Where there is skin involvement, protect the overlying skin, often using a well fitted stoma, bag- skin damage is difficult to treat, A high output fistula may be rendered more easily managed by the use of octreotide, this will, tend to reduce the volume of pancreatic secretions., Nutritional complications are common especially with high fistula (e.g. high jejunal or, duodenal) these may necessitate the use of TPN to provide nutritional support together with, the concomitant use of octreotide to reduce volume and protect skin., When managing perianal fistulae surgeons should avoid probing the fistula where acute, inflammation is present, this almost always worsens outcomes., When perianal fistulae occur secondary to Crohn's disease the best management option is, often to drain acute sepsis and maintain that drainage through the judicious use of setons, whilst medical management is implemented., Always attempt to delineate the fistula anatomy, for abscesses and fistulae that have an intra, abdominal source the use of barium and CT studies should show a track. For perianal, fistulae surgeons should recall Goodsall's rule in relation to internal and external openings., Next question
Page 3148 :
Theme: Large bowel obstruction, , A. Ileocolic bypass, B. Loop ileostomy, C. High anterior resection, D. Insertion of self expanding metallic stent, E. Left hemicolectomy and on table colonic lavage and primary anastomosis, F. Extended right hemicolectomy and ileocolic anastomosis, G. Low anterior resection, H. Loop colostomy of the transverse colon, I. Loop colostomy of the sigmoid colon, J. Right hemicolectomy, , Please select the most appropriate initial procedure for the following patients with large bowel, obstruction. Each option may be used once, more than once or not at all., , 17., , A 49 year old lady presents with an 18 hour history of absolute constipation. A CT scan is, performed and demonstrates an obstructing T3 tumour of the distal descending colon. There is, no evidence of distant visceral metastatic disease., You answered Ileocolic bypass, The correct answer is Left hemicolectomy and on table colonic lavage and primary anastomosis, Resection of the distal descending colon will provide the best method of oncological control., Careful bowel washout will hopefully create the optimal circumstances for anastomosis. A self, expanding metallic stent is not likely to be beneficial (see below)., , 18., , A 65 year old man presents with absolute constipation and abdominal pain. On examination he, has marked abdominal distension. A digital rectal examination reveals an empty rectum. A rectal, contrast study shows an obstructing lesion of the proximal rectum.
Page 3149 :
You answered Ileocolic bypass, The correct answer is Loop colostomy of the sigmoid colon, Rectal cancers should not be primarily resected prior to definitive staging and a tumour of this, nature is likely to have circumferential margin involvement. Whilst a sigmoid and transverse loop, colostomy would both provide an equal relief of obstruction the former procedure has the added, benefit of making a subsequent resection safer, since a transverse colostomy would have to be, taken down and closed during the course of subsequent surgery., , 19., , A 70 year old lady presents with a two day history of constipation and vomiting. On examination, she has right iliac fossa tenderness and little abdominal distension. A CT scan is performed and is, suggestive of an obstructing carcinoma of the colonic hepatic flexure (stage T3)., You answered Ileocolic bypass, The correct answer is Right hemicolectomy, This lesion should be amenable to standard right hemicolectomy. Extending the resection to take, the middle colic vessels and distal transverse colon is unlikely to provide additional oncological, benefit., , Please rate this question:, , Discuss and give feedback, , Next question, , Large bowel obstruction, Colonic obstruction remains a common surgical problem. It is most commonly due to malignancy, (60%) and diverticular disease (20%). Volvulus affecting the colon accounts for 5% of cases. Acute, colonic pseudo-obstruction remains a potential differential diagnosis in all cases. Intussusception, affecting the colon (most often due to tumours in the adult population) remains a rare but recognised, cause.
Page 3150 :
The typical patient will present with gradual onset of progressive abdominal distension, colicky, abdominal pain and either obstipation or absolute constipation., On examination abdominal distension is present, the presence of caecal tenderness (assuming no, overt evidence of peritonitis) is a useful sign to elicit. A digital rectal examination and rigid, sigmoidoscopy should be performed., A plain abdominal x-ray is the usual first line test and; the caecal diameter and ileocaecal valve, competency should be assessed on this film., Imaging modalities, Debate long surrounds the use of CT versus gastrograffin enemas. The latter investigation has, always been the traditional method of determining whether a structural lesion is indeed present., However, in the UK the use of this technique has declined and in most units a CT scan will be, offered as the first line investigation by the majority of radiologists (and is advocated by the, ACPGBI). In most cases this will provide sufficient detail to allow operative planning, and since, malignancy accounts for most presentations may also stage the disease. In the event that the, radiologist cannot provide a clear statement of lesion site, the surgeon should have no hesitation in, requesting a contrast enema., Surgical options, The decision as to when to operate or not is determined firstly by the patients physiological status., Unstable patients require resuscitation prior to surgery and admission to a critical care unit for, invasive monitoring and potential inotropic support may be needed. In patients who are otherwise, stable the decision then rests on the radiological and clinical findings. As a general rule the old, adage that the sun should not rise and set on unrelieved large bowel obstruction still holds true. A, caecal diameter of 12cm or more in the presence of complete obstruction with a competent, ileocaecal valve and caecal tenderness is a sign of impending perforation and a relative indication, for prompt surgery., Right sided and transverse lesions, Right sided lesions producing large bowel obstruction should generally be treated by right, hemicolectomy or its extended variant if the lesion lies in the distal transverse colon or splenic, flexure. In these cases an ileocolic anastomosis may be easily constructed and even in the, emergency setting has a low risk of anastomotic leak., Left sided lesions, The options here lie between sub total colectomy and anastomosis, left hemicolectomy with on table, lavage and primary anastomosis, left hemicolectomy and end colostomy formation and finally colonic, stent insertion., The usefulness of colonic stents was the subject of a Cochrane review in 2011. The authors, concluded that on the basis of the data that they reviewed, there was no benefit from the use of, colonic stents over conventional surgical resection with a tendency to better outcomes seen in the, surgical group (1). A more recently conducted meta analysis met with the same conclusion (2)., There remains some enthusiasm for use of stents as a bridge to surgery but this may too pass with, the passage of time. They do remain an option in selected cases such as patients who are unfit for, anaesthesia. However, in this group the development of complications at the time of stent insertion, would have dire consequences.
Page 3151 :
Rectosigmoid lesions, Lesions below the peritoneal reflection that are causing obstruction should generally be treated with, a loop colostomy. Primary resection of unstaged rectal cancer would most likely carry a high CRM, positivity rate and cannot be condoned. Where the lesion occupies the distal sigmoid colon the usual, practice would be to perform a high anterior resection. The decision surrounding restoration of, intestinal continuity would lie with the operating surgeon., References, 1. Sagar J. Colorectal stents for the management of malignant colonic obstructions. Cochrane, Database of Systematic Reviews 2011, Issue 11. Art. No.: CD007378. DOI:, 10.1002/14651858.CD007378.pub2., 2. Cirrochi et al Safety and efficacy of endoscopic colonic stenting as a bridge to surgery in the, management of intestinal obstruction due to left colon and rectal cancer: A systematic review and, meta-analysis. Surg Oncol. 2013 Mar;22(1):14-21., Next question
Page 3152 :
A 48 year old lady has previously undergone a sigmoid colectomy for carcinoma. On follow up, imaging she is found to have a 3cm foci of metastatic disease in segment IV of the liver. What is the, most appropriate course of action?, , Palliative chemotherapy, , External beam radiotherapy, , Brachytherapy, , Surgical resection alone, , Chemotherapy followed by surgical resection, , Theme from January 2015 Exam, The treatment of colorectal liver metastasis is usually with chemotherapy followed by surgical, resection. Where surgery is performed for liver metastasis with curative intent, the 5 year survival is, 20%. Palliation would generally only be considered if the patient were frail or widespread disease, found on imaging. Radiotherapy is not part of the treatment of liver metastasis., Please rate this question:, , Discuss and give feedback, , Next question, , Colorectal cancer treatment, Patients diagnosed as having colorectal cancer should be completely staged using CT of the chest/, abdomen and pelvis. Their entire colon should have been evaluated with colonoscopy or CT, colonography. Patients whose tumours lie below the peritoneal reflection should have their, mesorectum evaluated with MRI., Once their staging is complete patients should be discussed within a dedicated colorectal MDT, meeting and a treatment plan formulated.
Page 3153 :
Treatment of colonic cancer, Cancer of the colon is nearly always treated with surgery. Stents, surgical bypass and diversion, stomas may all be used as palliative adjuncts. Resectional surgery is the only option for cure in, patients with colon cancer. The procedure is tailored to the patient and the tumour location. The, lymphatic drainage of the colon follows the arterial supply and therefore most resections are tailored, around the resection of particular lymphatic chains (e.g. ileo-colic pedicle for right sided tumours)., Some patients may have confounding factors that will govern the choice of procedure, for example a, tumour in a patient from a HNPCC family may be better served with a panproctocolectomy rather, than segmental resection. Following resection the decision has to be made regarding restoration of, continuity. For an anastomosis to heal the key technical factors include; adequate blood supply,, mucosal apposition and no tissue tension. Surrounding sepsis, unstable patients and inexperienced, surgeons may compromise these key principles and in such circumstances it may be safer to, construct an end stoma rather than attempting an anastomosis., When a colonic cancer presents with an obstructing lesion; the options are to either stent it or resect., In modern practice it is unusual to simply defunction a colonic tumour with a proximal loop stoma., This differs from the situation in the rectum (see below)., Following resection patients with risk factors for disease recurrence are usually offered, chemotherapy, a combination of 5FU and oxaliplatin is common., Rectal cancer, The management of rectal cancer is slightly different to that of colonic cancer. This reflects the, rectum's anatomical location and the challenges posed as a result. Tumours located in the rectum, can be surgically resected with either an anterior resection or an abdomino - perineal resection. The, technical aspects governing the choice between these two procedures can be complex to appreciate, and the main point to appreciate for the MRCS is that involvement of the sphincter complex or very, low tumours require APER. In the rectum a 2cm distal clearance margin is required and this may, also impact on the procedure chosen. In addition to excision of the rectal tube an integral part of the, procedure is a meticulous dissection of the mesorectal fat and lymph nodes (total mesorectal, excision/ TME). In rectal cancer surgery invovlement of the cirumferential resection margin carries a, high risk of disease recurrence. Because the rectum is an extraperitoneal structure (until you remove, it that is!) it is possible to irradiate it, something which cannot be offered for colonic tumours. This, has a major impact in rectal cancer treatment and many patients will be offered neoadjuvent, radiotherapy (both long and short course) prior to resectional surgery. Patients with T1 and 2 /N0, disease on imaging do not require irradiation and should proceed straight to surgery. Patients with, T4 disease will typically have long course chemo radiotherapy. Those with T3 , N0 tumours may be, offered short course radiotherapy prior to surgery. Patients presenting with large bowel obstruction, from rectal cancer should not undergo resectional surgery without staging as primary treatment (very, different from colonic cancer). This is because rectal surgery is more technically demanding, the, anastomotic leak rate is higher and the danger of a positive resection margin in an unstaged patient, is high. Therefore patients with obstructing rectal cancer should have a defunctioning loop, colostomy., Summary of procedures, The operations for cancer are segmental resections based on blood supply and lymphatic drainage., These commonly performed procedures are core knowledge for the MRCS and should be
Page 3154 :
understood., , Site of cancer, , Type of resection, , Anastomosis, , Risk of, leak, , Right colon, , Right hemicolectomy, , Ileo-colic, , Low <5%, , Transverse, , Extended right hemicolectomy, , Ileo-colic, , Low <5%, , Splenic, flexure, , Extended right hemicolectomy, , Ileo-colic, , Low <5%, , Splenic, flexure, , Left hemicolectomy, , Colo-colon, , 2-5%, , Left colon, , Left hemicolectomy, , Colo-colon, , 2-5%, , Sigmoid colon, , High anterior resection, , Colo-rectal, , 5%, , Upper rectum, , Anterior resection (TME), , Colo-rectal, , 5%, , Low rectum, , Anterior resection (Low TME), , Colo-rectal, (+/- Defunctioning, stoma), , 10%, , Anal verge, , Abdomino-perineal excision of colon and, rectum, , None, , n/a, , In the emergency setting, where the bowel has perforated, the risk of an anastomosis is much, greater, particularly when the anastomosis is colon-colon. In this situation, an end colostomy is often, safer and can be reversed later. When resection of the sigmoid colon is performed and an end, colostomy is fashioned the operation is referred to as a Hartmans procedure. Whilst left sided, resections are more risky, ileo-colic anastomoses are relatively safe even in the emergency setting
Page 3155 :
and do not need to be defunctioned., References, A review of the diagnosis and management of colorectal cancer and a summary of the UK National, Institute of Clinical Excellence guidelines is provided in:, Poston G, et al . Diagnosis and management of colorectal cancer:summary of NICE, guidance. BMJ2011: 343: d 6751., Next question
Page 3156 :
What is the commonest type of fistula in ano?, , Trans-sphincteric, , Supra levator, , Complex supra levator, , Intersphincteric, , Suprasphincteric, , Intersphincteric fistulas are the commonest type and the external opening may be internal or, external. These are the classical type of fistula and will have an internal opening near the anal verge, and obey Goodsalls rule. Primary fistulotomy in this situation usually poses little risk to continence., Please rate this question:, , Discuss and give feedback, , Next question, , Anal fistula, Fistula in ano is the most common form of ano rectal sepsis. Fistulae will have both an internal, opening and external opening, these will be connected by tract(s). Complexity arises because of the, potential for multiple entry and exit sites, together with multiple tracts. Fistulae are classified into four, main groups according to anatomical location and the degree of sphincter involvement. Simple, uncomplicated fistulae are low and do not involve more than 30% of the external sphincter. Complex, fistulae involve the sphincter, have multiple branches or are non cryptoglandular in origin[1], Assessment, Examination of the perineum for signs of trauma, external openings or the stigmata of IBD is, important. Digital rectal examination may reveal the cord linking the internal and external openings., At the same time the integrity of the sphincter mechanism can be assessed. Low, uncomplicated
Page 3157 :
fistulas may not require any further assessment, other groups will usually require more detailed, investigation. For the fistula, the use of endo-anal USS with instillation of hydrogen peroxide into the, fistula tract may be helpful. Ano-rectal MRI scanning is also a useful tool, it is sensitive and specific, for the identification of fistula anatomy, branching tracts and identifying occult sphincter, involvement[2]., Identification of the internal opening, Fistulas with an external opening less than 3cm from the anal verge will typically obey Goodsalls rule, (see below)., , Image sourced from Wikipedia, , Therapies, Seton suture, A seton is a piece of material that is passed through the fistula between the internal and external, openings that allows the drainage of sepsis. This is important as undrained septic foci may drain, along the path of least resistance, which may result in the development of accessory tracts and, openings. Their main use is in treating complex fistula. Two types of seton are recognised, simple, and cutting. Simple setons lie within the fistula tract and encourage both drainage and fibrosis. A, cutting seton is inserted and the skin incised. The suture is tightened and re-tightened at regular, intervals. This may convert a high fistula to a low fistula. Since the tissue will scar surrounding the, fistula it is hoped that this technique will minimise incontinence[3]. Unfortunately, a large, retrospective review of the literature related to the use of cutting setons has found that they are, associated with a 12% long term incontinence rate [4], Fistulotomy, Low fistulas, that are simple should be treated by fistulotomy once the acute sepsis has been, controlled. Fistulotomy (where safe) provides the highest healing rates [5]. Because fistulotomy is, regarded as having a high cure rate, there are some who prefer to use this technique with more
Page 3158 :
extensive sphincter involvement. In these patients the fistulotomy is performed as for a low fistula., However, the muscle that is encountered is then divided and reconstructed with an overlapping, sphincter repair. A price is paid in terms of incontinence with this technique and up to 12.5% of, patients who were continent pre-operatively will have issues relating to continence post, procedure[6]. The same group also randomised between fistulotomy and sphincter reconstruction, and ano-rectal advancement flaps for the treatment of complex cryptoglandular fistulas and reported, similar outcomes in terms of recurrence (>90%) and disturbances to continence (20%)[7]., Other authors have found adverse outcomes following fistulotomy in patients who have undergone, previous surgery, are of female gender or who have high internal openings [8], in these patients, careful assessment of pre-operative sphincter function should be considered mandatory prior to, fistulotomy., Anal fistula plugs and fibrin glue, The desire to avoid injury to the sphincter complex has led to surgeons using both fibrin glue and, plugs to try and improve fistula healing. Meticulous preparation of the tract and prior use of a, draining seton is likely to improve chances of success., The use of anal fistula plugs in high transphincteric fistula of cryptoglandular origin is to be, discouraged because of the high incidence of non response in patients treated with such devices, [9]In most patients septic complications are the reasons for failure [10]. Fibrin glue is a popular, option for the treatment of fistula. There is variability of reported healing rates In some cases initial, success rates of up to 50% healing at six months are reported (in patients with complex cryptogenic, fistula). Of these successes 25% suffer a long term recurrence of fistula [11]. There are, however, no, obvious cases of damage to the sphincter complex and the use of the devices does not appear to, adversely impact on subsequent surgical options., Ano-rectal advancement flaps, This procedure is primarily directed at high fistulae, and is considered attractive as a sphincter, saving operation. The procedure is performed either with the patient in the prone jack knife position, or in lithotomy (depending upon the site of the fistula). The dissection is commenced in the sub, mucosal plane (which may be infiltrated with dilute adrenaline solution to ease dissection). The, dissection is continued into healthy proximal tissue. This is brought down and sutured over the, defect., Follow up of patients with cryptoglandular fistulas treated with advancement flaps shows a success, in up to 80% patients[12-14]. With most recurrences occurring in the first 6 months following, surgery[12]. Continence was affected in some patients, with up to 10% describing major continence, issues post operatively., Ligation of the intersphincteric tract procedure, In this procedure an incision is made in the intersphincteric groove and the fistula tract dissected out, in this plane and divided. A greater than 90% cure rate within 4 weeks was initially reported[15]., Others have subsequently performed similar studies on larger numbers of patients with similar, success rates., Fistulotomy at the time of abscess drainage?, A Cochrane review conducted in 2010 suggests that primary fistulotomy for low, uncomplicated, fistula in ano may be safe and associated with better outcomes in relation to long term chronic
Page 3159 :
sepsis[16]. However, there is a danger that such surgery performed by non specialists may result in, a higher complication rate and therefore the traditional teaching is that primary treatment of acute, sepsis is incision and drainage only. All agree that high/ complex fistulae should never be subject to, primary fistulotomy in the acute setting., References, 1. Parks, A.G., P.H. Gordon, and J.D. Hardcastle, A classification of fistula-in-ano. Br J Surg, 1976., 63(1): p. 1-12., 2. Lunniss, P.J., et al., Magnetic resonance imaging of fistula-in-ano. Dis Colon Rectum, 1994., 37(7): p. 708-18., 3. Misra, M.C. and B.M. Kapur, A new non-operative approach to fistula in ano. Br J Surg, 1988., 75(11): p. 1093-4., 4. Ritchie, R.D., J.M. Sackier, and J.P. Hodde, Incontinence rates after cutting seton treatment for, anal fistula. Colorectal Dis, 2009. 11(6): p. 564-71., 5. Tyler, K.M., C.B. Aarons, and S.M. Sentovich, Successful sphincter-sparing surgery for all anal, fistulas. Dis Colon Rectum, 2007. 50(10): p. 1535-9., 6. Perez, F., et al., Prospective clinical and manometric study of fistulotomy with primary sphincter, reconstruction in the management of recurrent complex fistula-in-ano. Int J Colorectal Dis, 2006., 21(6): p. 522-6., 7. Perez, F., et al., Randomized clinical and manometric study of advancement flap versus, fistulotomy with sphincter reconstruction in the management of complex fistula-in-ano. Am J Surg,, 2006. 192(1): p. 34-40., 8. Garcia-Aguilar, J., et al., Anal fistula surgery. Factors associated with recurrence and, incontinence. Dis Colon Rectum, 1996. 39(7): p. 723-9., 9. Ortiz, H., et al., Randomized clinical trial of anal fistula plug versus endorectal advancement flap, for the treatment of high cryptoglandular fistula in ano. Br J Surg, 2009. 96(6): p. 608-12., 10. El-Gazzaz, G., M. Zutshi, and T. Hull, A retrospective review of chronic anal fistulae treated by, anal fistulae plug. Colorectal Dis, 2010. 12(5): p. 442-7., 11. Haim, N., et al., Long-term results of fibrin glue treatment for cryptogenic perianal fistulas: a, multicenter study. Dis Colon Rectum, 2011. 54(10): p. 1279-83., 12. Ortiz, H., et al., Length of follow-up after fistulotomy and fistulectomy associated with endorectal, advancement flap repair for fistula in ano. Br J Surg, 2008. 95(4): p. 484-7., 13. Kodner, I.J., et al., Endorectal advancement flap repair of rectovaginal and other complicated, anorectal fistulas. Surgery, 1993. 114(4): p. 682-9; discussion 689-90., 14. Abbas, M.A., R. Lemus-Rangel, and A. Hamadani, Long-term outcome of endorectal, advancement flap for complex anorectal fistulae. Am Surg, 2008. 74(10): p. 921-4., 15. Rojanasakul, A., et al., Total anal sphincter saving technique for fistula-in-ano; the ligation of, intersphincteric fistula tract. J Med Assoc Thai, 2007. 90(3): p. 581-6., 16. Malik, A.I., R.L. Nelson, and S. Tou, Incision and drainage of perianal abscess with or without, treatment of anal fistula. Cochrane Database Syst Rev, 2010(7): p. CD006827., , Next question
Page 3160 :
You embark on a laparoscopic appendicectomy and find an appendix mass. There is no free fluid, and the patient has no evidence of peritonitis. Which is the best option?, , Convert to a midline laparotomy and perform a limited right hemicolectomy and end, ileostomy, Convert to midline laparotomy and perform and appendicectomy after taking down the, adhesions, Place a drain laparoscopically and administer parenteral antibiotics, , Send the patient for CT guided drainage, , Wrap omentum around the area and avoid drainage, Attempt conservative management for appendix mass without peritonitis., Dissection of appendix masses can be associated with a considerable degree of morbidity, the gains, of formally dissecting them over simple drainage and antibiotics are minimal., This was initially described as the Ochsner-Sherren regime and was based on the teachings of, Albert Ochsner of Chicago and James Sherren of the London hospital. The key facts of both, methods (which essentially consisted of non surgical management and careful observation) were, combined and published by Hamilton Bailey in 1930 (Bailey H. The Oschner- Sherren treatment of, acute appendicitis.BMJ 1930 Jan 25; 1(3603): 140143.), Please rate this question:, , Discuss and give feedback, , Next question, , Appendicitis, History, , , , , , , Peri umbilical abdominal pain (visceral stretching of appendix lumen and appendix is mid gut, structure) radiating to the right iliac fossa due to localised parietal peritoneal inflammation., Vomit once or twice but marked and persistent vomiting is unusual., Diarrhoea is rare. However, pelvic appendicitis may cause localised rectal irritation and some, loose stools. A pelvic abscess may also cause diarrhoea., Mild pyrexia is common - temperature is usually 37.5 -38oC. Higher temperatures are more, typical of conditions like mesenteric adenitis., Anorexia is very common. It is very unusual for patients with appendicitis to be hungry.
Page 3161 :
Examination, , , , , Generalised peritonitis if perforation has occurred or localised peritonism., Retrocaecal appendicitis may have relatively few signs., Digital rectal examination may reveal boggy sensation if pelvic abscess is present, or even, tenderness with a pelvic appendix., , Diagnosis, , , , , Typically raised inflammatory markers coupled with compatible history and examination, findings should be enough to justify appendicectomy., Urine analysis may show mild leucocytosis but no nitrites., Ultrasound is useful in females where pelvic organ pathology is suspected. Although it is not, always possible to visualise the appendix on ultrasound, the presence of free fluid (always, pathological in males) should raise suspicion., , Ultrasound examination may show evidence of luminal obstruction and thickening of the appendiceal, wall as shown below, , Image sourced from Wikipedia, , Treatment, , , , Appendicectomy which can be performed via either an open or laparoscopic approach., Administration of metronidazole reduces wound infection rates.
Page 3162 :
, , , , Patients with perforated appendicitis require copious abdominal lavage., Patients without peritonitis who have an appendix mass should receive broad spectrum, antibiotics and consideration given to performing an interval appendicectomy., Be wary in the older patients who may have either an underlying caecal malignancy or, perforated sigmoid diverticular disease., , Laparoscopic appendicectomy is becoming increasing popular as demonstrated below, , Image sourced from Wikipedia, , Next question
Page 3163 :
A 28 year old male presents with painful, bright red, rectal bleeding. On examination he is found to, have a posteriorly sited, midline, fissure in ano. What is the most appropriate treatment?, , Topical GTN paste, , Sub lingual GTN paste, , Anal stretch, , Advancement flap, , Tailored division of the external anal sphincter, , Theme from January 2015 Exam, Topical vasodilator therapy is the most commonly utilised treatment for fissure in ano. Surgical, division of the internal anal sphincter is a reasonable treatment option in a young male. Division of, the external sphincter will almost certainly result in incontinence and is not performed. Anal stretches, were associated with a high rate of external sphincter injuries and have been discontinued for this, reason., Please rate this question:, , Discuss and give feedback, , Next question, , Anal fissure, Anal fissures are a common cause of painful, bright red, rectal bleeding., Most fissures are idiopathic and present as a painful mucocutaneous defect in the posterior midline, (90% cases). Fissures are more likely to be anteriorly located in females, particularly if they are, multiparous. Multiple fissures and those which are located at other sites are more likely to be due to, an underlying cause., Diseases associated with fissure in ano include:, , , , , Crohns disease, Tuberculosis, Internal rectal prolapse, , Diagnosis, In most cases the defect can be visualised as a posterior midline epithelial defect. Where symptoms, are highly suggestive of the condition and examination findings are unclear an examination under
Page 3164 :
anaesthesia may be helpful. Atypical disease presentation should be investigated with colonoscopy, and EUA with biopsies of the area., Treatment, Stool softeners are important as the hard stools may tear the epithelium and result in recurrent, symptoms. The most effective first line agents are topically applied GTN (0.2%) or Diltiazem (2%), paste. Side effects of diltiazem are better tolerated., Resistant cases may benefit from injection of botulinum toxin or lateral internal sphincterotomy, (beware in females). Advancement flaps may be used to treat resistant cases., Sphincterotomy produces the best healing rates. It is associated with incontinence to flatus in up to, 10% of patients in the long term., Next question
Page 3165 :
A 73 year old lady presents with constipation and no organic disease is identified on investigation., Which of the following types of laxatives works by direct bowel stimulation?, , Magnesium sulphate, , Lactulose, , Potassium sodium tatrate, , Methylcellulose, , Senna, , Senna contains glycosides. It passes unchanged into the colon where bacteria hydrolyse the, glycosidic bond, releasing the anthracene derivatives. These stimulate the myenteric plexus., Please rate this question:, , Discuss and give feedback, , Next question, , Laxatives, Bulk forming laxatives, , Bran, Psyllium, Methylcellulose
Page 3167 :
A 32 year old man is diagnosed as having a carcinoma of the caecum. On questioning, his mother, developed uterine cancer at the age of 39 and his maternal uncle died from colonic cancer aged 38., His older brother developed a colonic cancer with micro satellite instability aged 37. What is the most, appropriate operative treatment?, , Limited ileocaecal resection, , Right hemicolectomy, , Extended right hemicolectomy, , Panproctocolectomy, , Sub total colectomy, , The likely diagnosis is one of a familial cancer syndrome and now that he has developed a colonic, cancer the safest operative strategy is a total colectomy and end ileostomy., Please rate this question:, , Discuss and give feedback, , Next question, , Polyposis syndromes, , Syndrome, , Genetic defect, , Features, , Screening and, management, , Familial, adenomatous, , Mutation of APC, gene (80%) cases,, , Typically over 100, colonic adenomas, Cancer risk of 100%, , If known to be at risk, then predictive, genetic testing as, , Associated, disorders, , Gastric fundal, polyps (50%)., Duodenal polyps
Page 3168 :
Screening and, management, , Associated, disorders, , 20% are new, mutations, , teenager, Annual flexible, sigmoidoscopy from, 15 years, If no polyps found, then 5 yearly, colonoscopy started, at age 20, Polyps found =, resectional surgery, (resection and pouch, Vs sub total, colectomy and IRA), , 90%., If severe, duodenal, polyposis cancer, risk of 30% at 10, years., Abdominal, desmoid, tumours., , Biallelic mutation, of mut Y human, homologue (MYH), on chromosome, 1p, recessive, , Multiple colonic, polyps, Later onset right, sided cancers more, common than in FAP, 100% cancer risk by, age 60, , Once identified, resection and, ileoanal pouch, reconstruction is, recommended, Attenuated, phenotype - regular, colonoscopy, , Duodenal, polyposis in 30%, Associated with, increased risk of, breast cancer, (self examination), , STK11 (LKB1), mutation on, chromosome 19 in, some (but not all), cases, dominant, , Multiple benign, intestinal, hamartomas, Episodic obstruction, and intussceception, Increased risk of GI, cancers (colorectal, cancer 20%, gastric, 5%), Increased risk of, breast, ovarian,, cervical pancreatic, , Annual examination, Pan intestinal, endoscopy every 2-3, years, , Malignancies at, other sites, Classical, pigmentation, pattern, , Syndrome, , Genetic defect, , Features, , polyposis, , dominant, , MYH, associated, polyposis, , Peutz -Jeghers, syndrome
Page 3169 :
Syndrome, , Genetic defect, , Features, , Screening and, management, , Associated, disorders, , and testicular, cancers, , Cowden, disease, , Mutation of PTEN, gene on, chromosome, 10q22, dominant, , Macrocephaly, Multiple intestinal, hamartomas, Multiple, trichilemmomas, 89% risk of cancer at, any site, 16% risk of colorectal, cancer, , Targeted, individualised, screening, , Breast cancer, (81% risk), Thyroid cancer, and non toxic, goitre, Uterine cancer, , HNPCC (Lynch, syndrome), , Germline, mutations of DNA, mismatch repair, genes, , Colo rectal cancer, 30-70%, Endometrial cancer, 30-70%, Gastric cancer 5-10%, Scanty colonic polyps, may be present, Colonic tumours, likely to be right, sided and mucinous, , Colonoscopy every 12 years from age 25, Consideration of, prophylactic surgery, Extra colonic, surveillance, recommended, , Extra colonic, cancers, , Next question
Page 3170 :
A 53 year old man has a 1.5cm polyp identified and completely removed during a colonoscopy., Histology confirms a low grade adenoma. What is the correct follow up?, , Discharge., , Repeat endoscopy in 5 years., , Repeat endoscopy in 3 years., , Segmental resection of the affected area., , Barium enema at 5 years., , It would be unsafe to discharge. Follow up with barium enemas for polyps is counter intuitive. In the, UK NICE guidance (2011) this patient would only be classified as high risk if other adenomas were, present, or the removal incomplete, in which case a repeat endoscopy at 1 year would be required., Otherwise the patient is at intermediate risk and repeat endoscopy at 3 years is warranted., Please rate this question:, , Discuss and give feedback, , Next question, , Colonic polyps, Colonic Polyps, May occur in isolation, or greater numbers as part of the polyposis syndromes. In FAP greater than, 100 polyps are typically present. The risk of malignancy in association with adenomas is related to, size, and is the order of 10% in a 1cm adenoma. Isolated adenomas seldom give risk of symptoms, (unless large and distal). Distally sited villous lesions may produce mucous and if very large,, electrolyte disturbances may occur., Follow up of colonic polyps
Page 3171 :
Group, , Features, , Action, , Low risk, , 1 or 2 adenomas less than 1cm, , No follow up or re-colonoscopy, at 5 years, , Moderate, risk, , 3 or 4 small adenomas or 1 adenoma greater than 1cm, , Re-scope at 3 years, , High risk, , More than 5 small adenomas or more than 3 with 1 of, them greater than 1cm, , Re scope at 1 year, , From Atkins and Saunders Gut 2002 51 (suppl V:V6-V9). It is important to stratify patients, appropriately and ensure that a complete colonoscopy with good views was performed., Segmental resection or complete colectomy should be considered when:, 1. Incomplete excision of malignant polyp, 2. Malignant sessile polyp, 3. Malignant pedunculated polyp with submucosal invasion, 4. Polyps with poorly differentiated carcinoma, 5. Familial polyposis coli, -Screening from teenager up to 40 years by 2 yearly sigmoidoscopy/colonoscopy, -Panproctocolectomy and Ileostomy or Restorative Panproctocolectomy., Rectal polypoidal lesions may be amenable to trans anal endoscopic microsurgery., References, Cairns S et al. Guidelines for colorectal cancer screening and surveillance in moderate and high risk, groups (update from 2002). Gut 2010;59:666-690., Next question
Page 3172 :
Theme: Bowel cancer management, , A. Loop colostomy, B. Loop ileostomy, C. Ileo-colic bypass, D. Hartman's procedure, E. Sub total colectomy, F. Right hemicolectomy, G. Left hemicolectomy, H. Abdomino-perineal excision of the colon and rectum, I. Anterior resection, , Please select the most appropriate management option for the scenario given. Each option may be, used once, more than once or not at all., , 27., , A 67 year old man is admitted with acute abdominal pain. He has features of large bowel, obstruction. At laparotomy he has a carcinoma of the sigmoid colon and perforation of the, caecum., You answered Loop colostomy, The correct answer is Sub total colectomy, Large bowel obstruction will typically result in caecal perforation once the caecal diameter, exceeds 10cm. Once this has occurred the only realistic option is a sub total colectomy and end, ileostomy., , 28., , A 89 year old lady is admitted with large bowel obstruction. She has tenderness of the right side, of her abdomen and CT scanning shows a sigmoid lesion with liver metastasis. Her caecum, measures 11cm., Loop colostomy
Page 3173 :
A loop colostomy is the safest option. A stent would be ideal (but is not on the list)., , 29., , A patient has a tumour 10cm from the anal verge. Staging investigations show localised disease, only., You answered Loop colostomy, The correct answer is Anterior resection, This should be manageable with a low anterior resection. A covering loop ileostomy should be, constructed to mitigate the effects of any anastomotic leakage. The functional effects of low, anterior resection can be variable and some patients with poor pre-operative anal function (e.g., faecal incontinence) may be better served with a non restorative procedure (such as a low, Hartmans type resection/ low anterior resection and end colostomy)., , Loop colostomy remains the traditional method for relieving inoperable large bowel obstruction., Colonic stents are becoming increasing popular alternatives, especially as a bridge to surgery., , Please rate this question:, , Discuss and give feedback, , Next question, , Colorectal cancer treatment, Patients diagnosed as having colorectal cancer should be completely staged using CT of the chest/, abdomen and pelvis. Their entire colon should have been evaluated with colonoscopy or CT, colonography. Patients whose tumours lie below the peritoneal reflection should have their, mesorectum evaluated with MRI., Once their staging is complete patients should be discussed within a dedicated colorectal MDT, meeting and a treatment plan formulated., Treatment of colonic cancer, Cancer of the colon is nearly always treated with surgery. Stents, surgical bypass and diversion
Page 3174 :
stomas may all be used as palliative adjuncts. Resectional surgery is the only option for cure in, patients with colon cancer. The procedure is tailored to the patient and the tumour location. The, lymphatic drainage of the colon follows the arterial supply and therefore most resections are tailored, around the resection of particular lymphatic chains (e.g. ileo-colic pedicle for right sided tumours)., Some patients may have confounding factors that will govern the choice of procedure, for example a, tumour in a patient from a HNPCC family may be better served with a panproctocolectomy rather, than segmental resection. Following resection the decision has to be made regarding restoration of, continuity. For an anastomosis to heal the key technical factors include; adequate blood supply,, mucosal apposition and no tissue tension. Surrounding sepsis, unstable patients and inexperienced, surgeons may compromise these key principles and in such circumstances it may be safer to, construct an end stoma rather than attempting an anastomosis., When a colonic cancer presents with an obstructing lesion; the options are to either stent it or resect., In modern practice it is unusual to simply defunction a colonic tumour with a proximal loop stoma., This differs from the situation in the rectum (see below)., Following resection patients with risk factors for disease recurrence are usually offered, chemotherapy, a combination of 5FU and oxaliplatin is common., Rectal cancer, The management of rectal cancer is slightly different to that of colonic cancer. This reflects the, rectum's anatomical location and the challenges posed as a result. Tumours located in the rectum, can be surgically resected with either an anterior resection or an abdomino - perineal resection. The, technical aspects governing the choice between these two procedures can be complex to appreciate, and the main point to appreciate for the MRCS is that involvement of the sphincter complex or very, low tumours require APER. In the rectum a 2cm distal clearance margin is required and this may, also impact on the procedure chosen. In addition to excision of the rectal tube an integral part of the, procedure is a meticulous dissection of the mesorectal fat and lymph nodes (total mesorectal, excision/ TME). In rectal cancer surgery invovlement of the cirumferential resection margin carries a, high risk of disease recurrence. Because the rectum is an extraperitoneal structure (until you remove, it that is!) it is possible to irradiate it, something which cannot be offered for colonic tumours. This, has a major impact in rectal cancer treatment and many patients will be offered neoadjuvent, radiotherapy (both long and short course) prior to resectional surgery. Patients with T1 and 2 /N0, disease on imaging do not require irradiation and should proceed straight to surgery. Patients with, T4 disease will typically have long course chemo radiotherapy. Those with T3 , N0 tumours may be, offered short course radiotherapy prior to surgery. Patients presenting with large bowel obstruction, from rectal cancer should not undergo resectional surgery without staging as primary treatment (very, different from colonic cancer). This is because rectal surgery is more technically demanding, the, anastomotic leak rate is higher and the danger of a positive resection margin in an unstaged patient, is high. Therefore patients with obstructing rectal cancer should have a defunctioning loop, colostomy., Summary of procedures, The operations for cancer are segmental resections based on blood supply and lymphatic drainage., These commonly performed procedures are core knowledge for the MRCS and should be, understood.
Page 3175 :
Site of cancer, , Type of resection, , Anastomosis, , Risk of, leak, , Right colon, , Right hemicolectomy, , Ileo-colic, , Low <5%, , Transverse, , Extended right hemicolectomy, , Ileo-colic, , Low <5%, , Splenic, flexure, , Extended right hemicolectomy, , Ileo-colic, , Low <5%, , Splenic, flexure, , Left hemicolectomy, , Colo-colon, , 2-5%, , Left colon, , Left hemicolectomy, , Colo-colon, , 2-5%, , Sigmoid colon, , High anterior resection, , Colo-rectal, , 5%, , Upper rectum, , Anterior resection (TME), , Colo-rectal, , 5%, , Low rectum, , Anterior resection (Low TME), , Colo-rectal, (+/- Defunctioning, stoma), , 10%, , Anal verge, , Abdomino-perineal excision of colon and, rectum, , None, , n/a, , In the emergency setting, where the bowel has perforated, the risk of an anastomosis is much, greater, particularly when the anastomosis is colon-colon. In this situation, an end colostomy is often, safer and can be reversed later. When resection of the sigmoid colon is performed and an end, colostomy is fashioned the operation is referred to as a Hartmans procedure. Whilst left sided, resections are more risky, ileo-colic anastomoses are relatively safe even in the emergency setting, and do not need to be defunctioned., References
Page 3176 :
A review of the diagnosis and management of colorectal cancer and a summary of the UK National, Institute of Clinical Excellence guidelines is provided in:, Poston G, et al . Diagnosis and management of colorectal cancer:summary of NICE, guidance. BMJ2011: 343: d 6751., Next question
Page 3177 :
Theme: Causes of rectal bleeding, , A., B., C., D., E., F., G., H., , Ulcerative colitis proctitis, Diversion proctitis, Haemorrhoidal disease, Fissure in ano, Crohns Proctitis, Diverticular bleed, Ischaemic colitis, Rectal intussceception, , Please select the most likely cause of bleeding for the scenario given. Each option may be used, once, more than once or not at all., , 30., , A previously well 21 year old man is admitted with 2 week history of diarrhoea and, passage of blood and mucous rectally. He has previously undergone an ileocaecal, resection in the past for an inflammatory bowel disorder and takes mesalazine., You answered Ulcerative colitis proctitis, The correct answer is Crohns Proctitis, His previous right sided resection makes crohns disease the most likely scenario., , 31., , A 56 year old lady has undergone a Hartman's procedure for diverticulitis. 6 months post, operatively she complains of painless passage of blood stained mucous per rectum., You answered Ulcerative colitis proctitis, The correct answer is Diversion proctitis, Rectal diversion may result in proctitis., , 32., , A 74 year old lady has been admitted with sudden onset profuse dark red rectal bleeding., She was previously well. At the time of assessment her bleeding had stopped but, haemoglobin was 10.5., You answered Ulcerative colitis proctitis, The correct answer is Diverticular bleed, This pattern of sudden onset profuse bleeding is typical of diverticular bleeding. This often, ceases spontaneously.
Page 3178 :
Please rate this question:, , Discuss and give feedback, , Next question, , Rectal bleeding, Rectal bleeding is a common cause for patients to be referred to the surgical clinic. In the clinical, history it is useful to try and localise the anatomical source of the blood. Bright red blood is usually of, rectal anal canal origin, whilst dark red blood is more suggestive of a proximally sited bleeding, source. Blood which has entered the GI tract from a gastro-duodenal source will typically resemble, malaena due to the effects of the digestive enzymes on the blood itself., In the table below we give some typical bleeding scenarios together with physical examination, findings and causation., , Cause, , Type of, bleeding, , Features in history, , Examination findings, , Fissure in, ano, , Bright red, rectal, bleeding, , Painful bleeding that occurs, post defecation in small, volumes. Usually antecedent, features of constipation, , Muco-epithelial defect usually, in the midline posteriorly, (anterior fissures more likely to, be due to underlying disease), , Haemorroids, , Bright red, rectal, bleeding, , Post defecation bleeding noted, both on toilet paper and drips, into pan. May be alteration of, bowel habit and history of, straining. No blood mixed with, stool. No local pain., , Normal colon and rectum., Proctoscopy may show internal, haemorrhoids. Internal, haemorrhoids are usually, impalpable., , Crohns, disease, , Bright red or, mixed blood, , Bleeding that is accompanied, by other symptoms such as, altered bowel habit, malaise,, history of fissures (especially, anterior) and abscesses., , Perineal inspection may show, fissures or fistulae. Proctoscopy, may demonstrate indurated, mucosa and possibly strictures., Skip lesions may be noted at, colonoscopy., , Ulcerative, colitis, , Bright red, bleeding, often mixed, , Diarrhoea, weight loss,, nocturnal incontinence, passage, , Proctitis is the most marked, finding. Peri anal disease is, usually absent. Colonoscopy
Page 3179 :
Rectal cancer, , with stool, , of mucous PR., , will show continuous mucosal, lesion., , Bright red, blood mixed, volumes, , Alteration of bowel habit., Tenesmus may be present., Symptoms of metastatic, disease., , Usually obvious mucosal, abnormality. Lesion may be, fixed or mobile depending upon, disease extent. Surrounding, mucosa often normal, although, polyps may be present., , Image showing a fissure in ano. Typically these are located posteriorly and in the midline. Fissures, at other sites may be associated with underlying disease., , Image sourced from Wikipedia, , Colonoscopic image of internal haemorroids. Note these may often be impalpable.
Page 3180 :
Image sourced from Wikipedia, , Investigation, , , , , , , , , All patients presenting with rectal bleeding require digital rectal examination and proctosigmoidoscopy as a minimal baseline., Remember that haemorrhoids are typically impalpable and to attribute bleeding to these in, the absence of accurate internal inspection is unsatisfactory., In young patients with no other concerning features in the history a carefully performed, sigmoidoscopy that demonstrates clear haemorrhoidal disease may be sufficient. If clear, views cannot be obtained then patients require bowel preparation with an enema and a, flexible sigmoidscopy performed., In those presenting with features of altered bowel habit or suspicion of inflammatory bowel, disease a colonoscopy is the best test., Patients with excessive pain who are suspected of having a fissure may require an, examination under general or local anaesthesia., In young patients with external stigmata of fissure and a compatible history it is acceptable to, treat medically and defer internal examination until the fissure is healed. If the fissure fails to, heal then internal examination becomes necessary along the lines suggested above to, exclude internal disease., , Special tests, , , In patients with a malignancy of the rectum the staging investigations comprise an MRI of the, rectum to identify circumferential resection margin compromise and to identify mesorectal, nodal disease. In addition to this CT scanning of the chest abdomen and pelvis is necessary
Page 3181 :
to stage for more distant disease. Some centres will still stage the mesorectum with endo, rectal ultrasound but this is becoming far less common., , , , Patients with fissure in ano who are being considered for surgical sphincterotomy and are, females who have an obstetric history should probably have ano rectal manometry testing, performed together with endo anal ultrasound. As this service is not universally available it is, not mandatory but in the absence of such information there are continence issues that may, arise following sphincterotomy., , Management, , Disease, , Management, , Fissure in ano, , GTN ointment 0.2% or diltiazem cream applied topically is the usual first line, treatment. Botulinum toxin for those who fail to respond. Internal, sphincterotomy for those who fail with botox, can be considered earlier in, males., , Haemorroids, , Lifestyle advice, for small internal haemorrhoids can consider injection, sclerotherapy or rubber band ligation. For external haemorrhoids consider, haemorrhoidectomy. Modern options include HALO procedure and stapled, haemorrhoidectomy., , Inflammatory, bowel disease, , Medical management- although surgery may be needed for fistulating Crohns, (setons)., , Rectal cancer, , Anterior resection or abdomino-perineal excision of the colon and rectum., Total mesorectal excision is now standard of care. Most resections below the, peritoneal reflection will require defunctioning ileostomy. Most patients will, require preoperative radiotherapy., Next question
Page 3182 :
Theme: Diverticular disease management, , A., B., C., D., E., F., G., H., , Active observation, Colonoscopy acutely, Intravenous antibiotics, Abdominal CT Scan, Ultrasound scan, Defecating proctogram, Flexible sigmoidoscopy, Laparotomy, , Please select the most appropriate immediate management for the diverticular presentations given., Each option may be used once, more than once or not at all., , 33., , A 40 year old man with known diverticular disease diagnosed on colonoscopy 1 year, previously is admitted with acute abdominal pain. His abdomen is maximally tender in the, left iliac fossa and he describes pneumaturia. His GP has been giving him metronidazole, for 2 days., You answered Active observation, The correct answer is Abdominal CT Scan, A colovesical fistula has formed and CT will help to delineate the other complications, which may have occurred., , 34., , An 83 year old lady with known diverticular disease is admitted with a brisk PR bleed. On, assessment the bleeding is settling and her abdomen is soft. Hb 10.2, other blood tests are, normal, Active observation, Diverticular bleeds often settle spontaneously. Acute colonoscopy is rarely helpful. She, may require an elective endoscopy. Isolated diverticular bleeds without evidence of, infection do not necessarily require antibiotics., , 35., , A 72 year old man is admitted with large bowel obstruction and CT scan suggests, diverticular stricture in the sigmoid colon., You answered Active observation, The correct answer is Laparotomy
Page 3183 :
The stricture could be benign or malignant and although a luminal study would establish, aetiology the opportunity for that intervention has passed., 70% of diverticular bleeds will settle with conservative management., Please rate this question:, , Discuss and give feedback, , Next question, , Diverticular disease, Diverticular disease is a common surgical problem. It consists of herniation of colonic mucosa, through the muscular wall of the colon. The usual site is between the taenia coli where vessels, pierce the muscle to supply the mucosa. For this reason, the rectum, which lacks taenia, is often, spared., Symptoms, , , , , Altered bowel habit, Bleeding, Abdominal pain, , Complications, , , , , , , , Diverticulitis, Haemorrhage, Development of fistula, Perforation and faecal peritonitis, Perforation and development of abscess, Development of diverticular phlegmon, , Diagnosis, Patients presenting in clinic will typically undergo either a colonoscopy, CT cologram or barium, enema as part of their diagnostic work up. All tests can identify diverticular disease. It can be far, more difficult to confidently exclude cancer, particularly in diverticular strictures., Acutely unwell surgical patients should be investigated in a systematic way. Plain abdominal films, and an erect chest x-ray will identify perforation. An abdominal CT scan (not a CT cologram) with, oral and intravenous contrast will help to identify whether acute inflammation is present but also the, presence of local complications such as abscess formation.
Page 3184 :
Severity Classification- Hinchey, , I, , Para-colonic abscess, , II, , Pelvic abscess, , III, , Purulent peritonitis, , IV, , Faecal peritonitis, , Treatment, , , , , , , Increase dietary fibre intake., Mild attacks of diverticulitis may be managed conservatively with antibiotics., Peri colonic abscesses should be drained either surgically or radiologically., Recurrent episodes of acute diverticulitis requiring hospitalisation are a relative indication for, a segmental resection., Hinchey IV perforations (generalised faecal peritonitis) will require a resection and usually a, stoma. This group have a very high risk of post operative complications and usually require, HDU admission. Less severe perforations may be managed by laparoscopic washout and, drain insertion., Next question
Page 3185 :
A 34 year old man presents with symptoms attributable to a fistula in ano. He is examined in the, lithotomy position and the external opening of the fistula is identified in the 7 o'clock position. At, which of the following locations is the internal opening most likely to be identified?, , 7 o'clock, , 12 o'clock, , 9 o'clock, , 3 o'clock, , 6 o'clock, Goodsals rule:, Anterior fistulae will tend to have an internal opening opposite the external opening., Posterior fistulae will tend to have a curved track that passes towards the midline., According to Goodsalls rule the track of a posteriorly sited fistula will track to the posterior midline, (i.e. 6 o'clock), Please rate this question:, , Discuss and give feedback, , Next question, , Fistulas, , , , , , A fistula is defined as an abnormal connection between two epithelial surfaces., There are many types ranging from Branchial fistulae in the neck to entero-cutaneous, fistulae abdominally., In general surgical practice the abdominal cavity generates the majority and most of these, arise from diverticular disease and Crohn's., As a general rule all fistulae will resolve spontaneously as long as there is no distal, obstruction. This is particularly true of intestinal fistulae., , The four types of fistulae are:, Enterocutaneous, These link the intestine to the skin. They may be high (>500ml) or low output (<250ml) depending, upon source. Duodenal /jejunal fistulae will tend to produce high volume, electrolyte rich secretions, which can lead to severe excoriation of the skin. Colo-cutaneous fistulae will tend to leak faeculent
Page 3186 :
material. Both fistulae may result from the spontaneous rupture of an abscess cavity onto the skin, (such as following perianal abscess drainage) or may occur as a result of iatrogenic input. In some, cases it may even be surgically desirable e.g. mucous fistula following sub total colectomy for colitis., Suspect if there is excess fluid in the drain., Enteroenteric or Enterocolic, This is a fistula that involves the large or small intestine. They may originate in a similar manner to, enterocutaneous fistulae. A particular problem with this fistula type is that bacterial overgrowth may, precipitate malabsorption syndromes. This may be particularly serious in inflammatory bowel, disease., Enterovaginal, Aetiology as above., Enterovesicular, This type of fistula goes to the bladder. These fistulas may result in frequent urinary tract infections,, or the passage of gas from the urethra during urination., Management, Some rules relating to fistula management:, , , , , , , , , They will heal provided there is no underlying inflammatory bowel disease and no distal, obstruction, so conservative measures may be the best option, Where there is skin involvement, protect the overlying skin, often using a well fitted stoma, bag- skin damage is difficult to treat, A high output fistula may be rendered more easily managed by the use of octreotide, this will, tend to reduce the volume of pancreatic secretions., Nutritional complications are common especially with high fistula (e.g. high jejunal or, duodenal) these may necessitate the use of TPN to provide nutritional support together with, the concomitant use of octreotide to reduce volume and protect skin., When managing perianal fistulae surgeons should avoid probing the fistula where acute, inflammation is present, this almost always worsens outcomes., When perianal fistulae occur secondary to Crohn's disease the best management option is, often to drain acute sepsis and maintain that drainage through the judicious use of setons, whilst medical management is implemented., Always attempt to delineate the fistula anatomy, for abscesses and fistulae that have an intra, abdominal source the use of barium and CT studies should show a track. For perianal, fistulae surgeons should recall Goodsall's rule in relation to internal and external openings., Next question
Page 3187 :
Theme: Proctology, , A., B., C., D., E., F., G., , Haemorrhoids, Rectal intussceception, Fistula in ano, Fissure in ano, Peri-anal abscess, Solitary rectal ulcer, Marjolins ulcer, , Please select the most likely disorder for the scenario given. Each option may be used once, more, than once or not at all., , 37., , A 38 year old lady presents with symptoms of obstructed defecation that date back to the, birth of her second child by use of ventouse. She passes mucous and suffers from pelvic, pain. Digital rectal examination and barium enema are normal., You answered Haemorrhoids, The correct answer is Rectal intussceception, Rectal intussceception (internal rectal prolapse) typically presents with symptoms of, obstructed defecation. The pathology is best demonstrated by a defecating procotogram, rather than barium enema., , 38., , A 23 year old male presents with bright red rectal bleeding that occurs post defecation, onto the toilet paper. He has been suffering from severe pain associated with this. On, external anal examination there is a skin tag located at the 6 O'clock position., You answered Haemorrhoids, The correct answer is Fissure in ano, This is a typical story for fissure and should be treated with laxatives and topical, vasodilator (eg GTN) in the first instance., , 39., , A 19 year old male presents with bright red rectal bleeding that occurs post defecation, onto the paper and into the pan. Apart from constipation his bowel habit is normal. Digital, rectal examination is normal., Haemorrhoids, This is likely to be haemorrhoidal disease. A sigmoidoscopy should always be performed
Page 3188 :
to exclude more sinister pathology., Please rate this question:, , Discuss and give feedback, , Next question, , Ano rectal disease, , Haemorrhoids, , Location: 3, 7, 11 o'clock position, Internal or external, Treatment: Conservative, Rubber band ligation, Haemorrhoidectomy, , Fissure in ano, , Location: midline 6 (posterior midline 90%) and 12 o'clock position. Distal to, the dentate line, Chronic fissure > 6/52: triad: Ulcer, sentinel pile, enlarged anal papillae, , Proctitis, , Causes: Crohn's, ulcerative colitis, Clostridium difficile, , Ano rectal, abscess, , E.coli, staph aureus, Positions: Perianal, Ischiorectal, Pelvirectal, Intersphincteric, , Anal fistula, , Usually due to previous ano-rectal abscess, Intersphincteric, transsphincteric, suprasphincteric, and extrasphincteric., Goodsalls rule determines location, , Rectal prolapse, , Associated with childbirth and rectal intussceception. May be internal or, external, , Pruritus ani, , Systemic and local causes, , Anal neoplasm, , Squamous cell carcinoma commonest unlike adenocarcinoma in rectum, , Solitary rectal, , Associated with chronic straining and constipation. Histology shows mucosal, thickening, lamina propria replaced with collagen and smooth muscle
Page 3189 :
(fibromuscular obliteration), , ulcer, , Rectal prolapse, , , , , , , Common especially in multiparous women., May be internal or external., Internal rectal prolapse can present insidiously., External prolapse can ulcerate and in long term impair continence., Diagnostic work up includes colonoscopy, defecating proctogram, ano rectal manometry, studies and if doubt exists an examination under anaesthesia., , Treatments for prolapse, , , , , , In the acute setting reduce it (covering it with sugar may reduce swelling., Delormes procedure which excises mucosa and plicates the rectum (high recurrence rates), may be used for external prolapse., Altmeirs procedure which resects the colon via the perineal route has lower recurrence rates, but carries the risk of anastamotic leak., Rectopexy is an abdominal procedure in which the rectum is elevated and usually supported, at the level of the sacral promontory. Post operative constipation may be reduced by limiting, the dissection to the anterior plane (laparoscopic ventral mesh rectopexy)., , Pruritus ani, , , , , , , , Extremely common., Check not secondary to altered bowel habits (e.g. Diarrhoea), Associated with underlying diseases such as haemorrhoids., Examine to look for causes such as worms., Proctosigmoidoscopy to identify associated haemorrhoids and exclude cancer., Treatment is largely supportive and patients should avoid using perfumed products around, the area., , Fissure in ano, , , , , Typically painful PR bleeding (bright red)., Nearly always in the posterior midline., Usually solitary., , Treatment
Page 3190 :
, , , , , , Stool softeners., Topical diltiazem (or GTN)., If topical treatments fail then botulinum toxin should be injected., If botulinum toxin fails then males should probably undergo lateral internal sphincterotomy., Females who do not respond to botulinum toxin should undergo ano rectal manometry, studies and endo anal USS prior to being offered surgery such as sphincterotomy., Next question
Page 3191 :
Theme: Management of inflammatory bowel disease, , A. Ileo-anal pouch, B. Panproctocolectomy, C. Sub total colectomy, D. Hartmans procedure, E. Right hemicolectomy, F. Intravenous steroids, G. Infliximab, H. Proctectomy, , Please select the most appropriate management option from the list. Each option may be used once,, more than once or not at all., , 40., , A 20 year old man is admitted with bloody diarrhoea. He has been passing 10 stools per day, Hb8.0, albumin-20. Stool culture negative. Evidence of colitis on endoscopy. He has been on, intravenous steroids for 5 days and has now developed megacolon. His haemoglobin is falling and, inflammatory markers are static., You answered Ileo-anal pouch, The correct answer is Sub total colectomy, This man requires a sub total colectomy. Conservative management has failed. Patients with, ulcerative colitis should undergo colectomy if there is no significant improvement in 5-7 days after, initiating medical therapy if they have a severe attack of the disease., , 41., , A 19 year old lady has a long standing history of diarrhoea and weight loss. She is investigated, with an upper gastro intestinal endoscopy which is normal. A small bowel contrast study shows a, terminal ileal stricture. A colonoscopy was performed which was normal but the endoscopist was, unable to intubate the terminal ileum. One week after the colonoscopy she is admitted with small, bowel obstruction. Steroids are administered but despite this she fails to improve.
Page 3192 :
You answered Ileo-anal pouch, The correct answer is Right hemicolectomy, It is likely that this lady has terminal ileal disease. Although , first presentation of Crohns disease is, usually managed with IV steroids, these have been trialled here and failed. A resection will, remove the stricturing disease. If proximal small bowel disease has not been excluded preoperatively then this must be evaluated "on table" during surgery to exclude other small bowel, strictures., , 42., , A 28 year old man is reviewed in the clinic. He has suffered from Crohns disease for many years,, he has recently undergone a sub total colectomy. However, he has residual Crohns in his rectum, and this is the cause of ongoing symptoms. Medical therapy is proving ineffective., You answered Ileo-anal pouch, The correct answer is Proctectomy, In Crohns patients who have rectal disease and a previous sub total colectomy, a proctectomy is, the best option. An ileo-anal pouch is contra indicated in Crohns as they may fistulate and have, major post operative complications., , Please rate this question:, , Discuss and give feedback, , Next question, , IBD, Ulcerative colitis Vs Crohns, , Crohn's disease, , Ulcerative colitis
Page 3193 :
Crohn's disease, , Ulcerative colitis, , Distribution, , Mouth to anus, , Rectum and colon, , Macroscopic, changes, , Cobblestone appearance, apthoid ulceration, , Contact bleeding, , Depth of disease, , Transmural inflammation, , Superficial inflammation, , Distribution, pattern, , Patchy, , Continuous, , Histological, features, , Granulomas (non caseating epithelioid cell, aggregates with Langerhans' giant cells), , Crypt abscesses, Inflammatory cells, in the lamina propria, , Surgical treatment, Ulcerative colitis, In UC the main place for surgery is when medical treatment has failed, in the emergency setting this, will be a sub total colectomy, end ileostomy and a mucous fistula. Electively it will be a pan, proctocolectomy, an ileoanal pouch may be a selected option for some. Remember that, longstanding UC increases colorectal cancer risk.
Page 3194 :
Image sourced from Wikipedia, , Crohn's disease, Unlike UC Crohn's patients need to avoid surgeons, minimal resections are the rule. They should not, have ileoanal pouches as they will do poorly with them. Management of Crohn's ano rectal sepsis is, with a minimal approach, simply drain sepsis and use setons to facilitate drainage. Definitive fistula, surgery should be avoided.
Page 3195 :
Image sourced from Wikipedia, , Next question
Page 3196 :
A 19 year old man presents with painful rectal bleeding and is found to have an anal fissure. Which, of the following is least associated with this condition?, , Leukaemia, , Syphilis, , Tuberculosis, , Sickle cell disease, , Crohn's disease, , Anal fissures are associated with:, , , , , , , , Sexually transmitted diseases (syphilis, HIV), Inflammatory bowel disease (Crohn's up to 50%), Leukaemia (25% of patients), Tuberculosis, Previous anal surgery, , Please rate this question:, , Discuss and give feedback, , Next question, , Ano rectal disease, , Haemorrhoids, , Fissure in ano, , Location: 3, 7, 11 o'clock position, Internal or external, Treatment: Conservative, Rubber band ligation, Haemorrhoidectomy, , Location: midline 6 (posterior midline 90%) and 12 o'clock position. Distal to, the dentate line, Chronic fissure > 6/52: triad: Ulcer, sentinel pile, enlarged anal papillae
Page 3197 :
Proctitis, , Causes: Crohn's, ulcerative colitis, Clostridium difficile, , Ano rectal, abscess, , E.coli, staph aureus, Positions: Perianal, Ischiorectal, Pelvirectal, Intersphincteric, , Anal fistula, , Usually due to previous ano-rectal abscess, Intersphincteric, transsphincteric, suprasphincteric, and extrasphincteric., Goodsalls rule determines location, , Rectal prolapse, , Associated with childbirth and rectal intussceception. May be internal or, external, , Pruritus ani, , Systemic and local causes, , Anal neoplasm, , Squamous cell carcinoma commonest unlike adenocarcinoma in rectum, , Solitary rectal, ulcer, , Associated with chronic straining and constipation. Histology shows mucosal, thickening, lamina propria replaced with collagen and smooth muscle, (fibromuscular obliteration), , Rectal prolapse, , , , , , , Common especially in multiparous women., May be internal or external., Internal rectal prolapse can present insidiously., External prolapse can ulcerate and in long term impair continence., Diagnostic work up includes colonoscopy, defecating proctogram, ano rectal manometry, studies and if doubt exists an examination under anaesthesia., , Treatments for prolapse, , , , , In the acute setting reduce it (covering it with sugar may reduce swelling., Delormes procedure which excises mucosa and plicates the rectum (high recurrence rates), may be used for external prolapse., Altmeirs procedure which resects the colon via the perineal route has lower recurrence rates, but carries the risk of anastamotic leak.
Page 3198 :
, , Rectopexy is an abdominal procedure in which the rectum is elevated and usually supported, at the level of the sacral promontory. Post operative constipation may be reduced by limiting, the dissection to the anterior plane (laparoscopic ventral mesh rectopexy)., , Pruritus ani, , , , , , , , Extremely common., Check not secondary to altered bowel habits (e.g. Diarrhoea), Associated with underlying diseases such as haemorrhoids., Examine to look for causes such as worms., Proctosigmoidoscopy to identify associated haemorrhoids and exclude cancer., Treatment is largely supportive and patients should avoid using perfumed products around, the area., , Fissure in ano, , , , , Typically painful PR bleeding (bright red)., Nearly always in the posterior midline., Usually solitary., , Treatment, , , , , , , Stool softeners., Topical diltiazem (or GTN)., If topical treatments fail then botulinum toxin should be injected., If botulinum toxin fails then males should probably undergo lateral internal sphincterotomy., Females who do not respond to botulinum toxin should undergo ano rectal manometry, studies and endo anal USS prior to being offered surgery such as sphincterotomy., Next question
Page 3199 :
Theme: Treatment of bowel cancer, , A. Active observation, B. Long course chemoirradiation, C. Chemotherapy with oxaliplatin, D. Short course chemotherapy (5 days), E. Proceed straight to surgery, F. Post operative radiotherapy, G. Chemotherapy with methotrexate, H. Brachytherapy, I. Anterior pelvic exenteration, , Please select the most appropriate management option from the list below. Each option may be, used once, more than once or not at all., , 44., , A 45 year old female is diagnosed as having a carcinoma of the caecum. She undergoes a CT scan, which shows a tumour invading the muscularis propria with some regional lymphadenopathy., You answered Active observation, The correct answer is Proceed straight to surgery, Right sided colonic cancers should proceed straight to surgery. Radiotherapy to this area is poorly, tolerated and almost never offered as first line treatment. The decision as to whether or not, chemotherapy is given is dependent upon the final histology., , 45., , A 55 year old man presents with tenesmus and rectal bleeding. On examination he has a large, bulky rectal cancer at 5cm with tethering to the prostate gland. Imaging shows no distant disease., You answered Active observation, The correct answer is Long course chemoirradiation
Page 3200 :
T4 rectal cancers are managed with long course chemoradiotherapy. A dramatic response is not, uncommon. To embark on attempted resection at this stage is to court failure., , 46., , A 43 year old women undergoes a sigmoid colectomy for carcinoma. The histology report shows, Dukes C disease. She is otherwise well., You answered Active observation, The correct answer is Chemotherapy with oxaliplatin, Chemotherapy for colonic cancer is usually with oxaliplatin. Neuropathy is a recognised side effect, of this treatment., , Patients with suspected large bowel obstruction should have pseudobstruction excluded with CT, scan, gastrograffin enema or endoscopy prior to intervention., , Please rate this question:, , Discuss and give feedback, , Next question, , Colorectal cancer treatment, Patients diagnosed as having colorectal cancer should be completely staged using CT of the chest/, abdomen and pelvis. Their entire colon should have been evaluated with colonoscopy or CT, colonography. Patients whose tumours lie below the peritoneal reflection should have their, mesorectum evaluated with MRI., Once their staging is complete patients should be discussed within a dedicated colorectal MDT, meeting and a treatment plan formulated., Treatment of colonic cancer, Cancer of the colon is nearly always treated with surgery. Stents, surgical bypass and diversion, stomas may all be used as palliative adjuncts. Resectional surgery is the only option for cure in, patients with colon cancer. The procedure is tailored to the patient and the tumour location. The
Page 3201 :
lymphatic drainage of the colon follows the arterial supply and therefore most resections are tailored, around the resection of particular lymphatic chains (e.g. ileo-colic pedicle for right sided tumours)., Some patients may have confounding factors that will govern the choice of procedure, for example a, tumour in a patient from a HNPCC family may be better served with a panproctocolectomy rather, than segmental resection. Following resection the decision has to be made regarding restoration of, continuity. For an anastomosis to heal the key technical factors include; adequate blood supply,, mucosal apposition and no tissue tension. Surrounding sepsis, unstable patients and inexperienced, surgeons may compromise these key principles and in such circumstances it may be safer to, construct an end stoma rather than attempting an anastomosis., When a colonic cancer presents with an obstructing lesion; the options are to either stent it or resect., In modern practice it is unusual to simply defunction a colonic tumour with a proximal loop stoma., This differs from the situation in the rectum (see below)., Following resection patients with risk factors for disease recurrence are usually offered, chemotherapy, a combination of 5FU and oxaliplatin is common., Rectal cancer, The management of rectal cancer is slightly different to that of colonic cancer. This reflects the, rectum's anatomical location and the challenges posed as a result. Tumours located in the rectum, can be surgically resected with either an anterior resection or an abdomino - perineal resection. The, technical aspects governing the choice between these two procedures can be complex to appreciate, and the main point to appreciate for the MRCS is that involvement of the sphincter complex or very, low tumours require APER. In the rectum a 2cm distal clearance margin is required and this may, also impact on the procedure chosen. In addition to excision of the rectal tube an integral part of the, procedure is a meticulous dissection of the mesorectal fat and lymph nodes (total mesorectal, excision/ TME). In rectal cancer surgery invovlement of the cirumferential resection margin carries a, high risk of disease recurrence. Because the rectum is an extraperitoneal structure (until you remove, it that is!) it is possible to irradiate it, something which cannot be offered for colonic tumours. This, has a major impact in rectal cancer treatment and many patients will be offered neoadjuvent, radiotherapy (both long and short course) prior to resectional surgery. Patients with T1 and 2 /N0, disease on imaging do not require irradiation and should proceed straight to surgery. Patients with, T4 disease will typically have long course chemo radiotherapy. Those with T3 , N0 tumours may be, offered short course radiotherapy prior to surgery. Patients presenting with large bowel obstruction, from rectal cancer should not undergo resectional surgery without staging as primary treatment (very, different from colonic cancer). This is because rectal surgery is more technically demanding, the, anastomotic leak rate is higher and the danger of a positive resection margin in an unstaged patient, is high. Therefore patients with obstructing rectal cancer should have a defunctioning loop, colostomy., Summary of procedures, The operations for cancer are segmental resections based on blood supply and lymphatic drainage., These commonly performed procedures are core knowledge for the MRCS and should be, understood.
Page 3202 :
Site of cancer, , Type of resection, , Anastomosis, , Risk of, leak, , Right colon, , Right hemicolectomy, , Ileo-colic, , Low <5%, , Transverse, , Extended right hemicolectomy, , Ileo-colic, , Low <5%, , Splenic, flexure, , Extended right hemicolectomy, , Ileo-colic, , Low <5%, , Splenic, flexure, , Left hemicolectomy, , Colo-colon, , 2-5%, , Left colon, , Left hemicolectomy, , Colo-colon, , 2-5%, , Sigmoid colon, , High anterior resection, , Colo-rectal, , 5%, , Upper rectum, , Anterior resection (TME), , Colo-rectal, , 5%, , Low rectum, , Anterior resection (Low TME), , Colo-rectal, (+/- Defunctioning, stoma), , 10%, , Anal verge, , Abdomino-perineal excision of colon and, rectum, , None, , n/a, , In the emergency setting, where the bowel has perforated, the risk of an anastomosis is much, greater, particularly when the anastomosis is colon-colon. In this situation, an end colostomy is often, safer and can be reversed later. When resection of the sigmoid colon is performed and an end, colostomy is fashioned the operation is referred to as a Hartmans procedure. Whilst left sided, resections are more risky, ileo-colic anastomoses are relatively safe even in the emergency setting, and do not need to be defunctioned., References
Page 3203 :
A review of the diagnosis and management of colorectal cancer and a summary of the UK National, Institute of Clinical Excellence guidelines is provided in:, Poston G, et al . Diagnosis and management of colorectal cancer:summary of NICE, guidance. BMJ2011: 343: d 6751., Next question
Page 3204 :
A 53 year old man presents with a full thickness external rectal prolapse. Which of the following, procedures would be the most suitable surgical option?, , Rectopexy, , Delormes, , Altmeirs, , Thirsch tape, , Abdomino-perineal excision of the rectum, , Theme from 2012 Exam, As this man is young and has full thickness prolapse a rectopexy is the most appropriate procedure., It will give the lowest recurrence rates., Please rate this question:, , Discuss and give feedback, , Next question, , Rectal prolapse, Rectal prolapse may be divided into internal and external prolapse. Patients with the former, condition may have internal intussceception of the rectum and present with constipation, obstructed, defecation and occasionally faecal incontinence. Patients with external rectal prolapse have a full, thickness external protrusion of the rectum. Risk factors for the condition include multiparity, pelvic, floor trauma and connective tissue disorders., Diagnosis, External prolapse is usually evident. Internal prolapse may be identified by defecating proctography, and examination under anaesthesia., Sinister pathology should be excluded with endoscopy, Treatment, , , Perineal approaches include the Delormes operation, this avoids resection and is relatively, safe but is associated with high recurrence rates. An Altmeirs operation involves a perineal, excision of the sigmoid colon and rectum, it may be a more effective procedure than a, Delormes but carries the risk of anastomotic leak.
Page 3205 :
, , , Rectopexy - this is an abdominal procedure. The rectum is mobilised and fixed onto the, sacral promontary. A prosthetic mesh may be inserted. The recurrence rates are low and the, procedure is well tolerated (particularly if performed laparoscopically)., Thirsch tape- this is a largely historical procedure and involves encircling the rectum with, tape or wire. It may be of use in a palliative setting., Next question
Page 3206 :
A patient has an appendicectomy and a 1.2cm carcinoid tumour is identified in the tip of the, appendix. What is the most appropriate management?, , Watchful waiting, , Discharge, , Right hemicolectomy, , Limited ileocaecal resection, , Radioisotope scan, , Individuals with small carcinoids can be discharged (<2cm and limited to the appendix). Larger, tumours should have a radioisotope scan. Where the resection margin is positive or where the, isotope scan suggests lymphatic metastasis a right hemicolectomy should be performed., Please rate this question:, , Discuss and give feedback, , Next question, , Carcinoid syndrome, , , , , , Carcinoid tumours secrete serotonin, Originate in neuroendocrine cells mainly in the intestine (midgut-distal ileum/appendix), Can occur in the rectum, bronchi, Hormonal symptoms mainly occur when disease spreads outside the bowel, , Clinical features, , , , , , , , Onset: insidious over many years, Flushing face, Palpitations, Pulmonary valve stenosis and tricuspid regurgitation causing dyspnoea, Asthma, Severe diarrhoea (secretory, persists despite fasting), , Investigation
Page 3208 :
Theme: Management of colonic disease, , A. Reassure and discharge, B. Right hemicolectomy, C. Left hemicolectomy, D. Hot biopsy, E. Snare polypectomy, F. Single colonoscopy, G. Annual colonoscopy, H. Colonoscopy every 3-5 years, I. Panproctocolectomy, , For each scenario given please select the most appropriate management option. Each option may, be used once, more than once or not at all., , 49., , A 25 year old male presents with altered bowel habit. He is known to have familial polyposis coli., A colonoscopy shows widespread polyps, with high grade dysplasia in a polyp removed from the, rectum., You answered Reassure and discharge, The correct answer is Panproctocolectomy, There is a high risk of conversion to malignancy, therefore panproctocolectomy is the safest, option., , 50., , A 19 year old female presents with colicky abdominal pain, bloating and alternating, constipation/diarrhoea. Her grandmother died from colon cancer at the age of 77 years. A digital, rectal examination and general physical examination are normal., Reassure and discharge
Page 3209 :
This girl fulfills the Rome criteria for irritable bowel syndrome. Examination is normal, therefore, there is no indication for further investigation., , 51., , A 62 year old man is being investigated for iron deficiency anaemia. During a colonoscopy a flat, polypoidal lesion is identified in the caecum. Biopsies of this lesion demonstrate high grade, dysplasia., You answered Reassure and discharge, The correct answer is Right hemicolectomy, High grade dysplasia in a flat villous lesion of the right colon is highly likely to be associated with, an invasive lesion at this site. Hot biopsy of right sided colonic lesions is unwise an snare, polypectomy would be unlikely to remove the entire lesion., , Please rate this question:, , Discuss and give feedback, , Next question, , Colonic polyps, Colonic Polyps, May occur in isolation, or greater numbers as part of the polyposis syndromes. In FAP greater than, 100 polyps are typically present. The risk of malignancy in association with adenomas is related to, size, and is the order of 10% in a 1cm adenoma. Isolated adenomas seldom give risk of symptoms, (unless large and distal). Distally sited villous lesions may produce mucous and if very large,, electrolyte disturbances may occur., Follow up of colonic polyps, , Group, , Features, , Action
Page 3210 :
Group, , Features, , Action, , Low risk, , 1 or 2 adenomas less than 1cm, , No follow up or re-colonoscopy, at 5 years, , Moderate, risk, , 3 or 4 small adenomas or 1 adenoma greater than 1cm, , Re-scope at 3 years, , High risk, , More than 5 small adenomas or more than 3 with 1 of, them greater than 1cm, , Re scope at 1 year, , From Atkins and Saunders Gut 2002 51 (suppl V:V6-V9). It is important to stratify patients, appropriately and ensure that a complete colonoscopy with good views was performed., Segmental resection or complete colectomy should be considered when:, 1. Incomplete excision of malignant polyp, 2. Malignant sessile polyp, 3. Malignant pedunculated polyp with submucosal invasion, 4. Polyps with poorly differentiated carcinoma, 5. Familial polyposis coli, -Screening from teenager up to 40 years by 2 yearly sigmoidoscopy/colonoscopy, -Panproctocolectomy and Ileostomy or Restorative Panproctocolectomy., Rectal polypoidal lesions may be amenable to trans anal endoscopic microsurgery., References, Cairns S et al. Guidelines for colorectal cancer screening and surveillance in moderate and high risk, groups (update from 2002). Gut 2010;59:666-690., Next question
Page 3211 :
Theme: Fistula management, , A., B., C., D., E., F., G., H., , No further action needed, Intravenous fluids, Intravenous fluids and nasogastric tube, Total parenteral nutrition and octreotide, Defunctioning stoma, Insertion of seton, Intravenous octreotide, Lay open fistula, , What is the best management for the following types of fistula? Each option may be used once,, more than once or not at all., , 52., , A 45 year old man develops a colocutaneous fistulae following reversal of a loop, colostomy fashioned for the defunctioning of an anterior resection. Pre-operative, gastrograffin enema showed no distal obstruction or anastamotic stricture., No further action needed, Colocutaneous fistulae may occur as a result of anastomotic leakage following loop, colostomy reversal. In the absence of abdominal signs a laparotomy is not necessarily, required. Signs of wound sepsis may require antibiotics. Because there is not any distal, obstruction (note normal pre-operative gastrograffin enema) these fistulae will usually, close spontaneously., , 53., , A 43 year old man has suffered from small bowel Crohns disease for 15 years. Following a, recent stricturoplasty he develops an enterocutaneous fistula which is high output. Small, bowel follow through shows it to be 15 cm from the DJ flexure. His overlying skin is, becoming excoriated., You answered No further action needed, The correct answer is Total parenteral nutrition and octreotide, This man has a high output and anatomically high fistula. Drying up the fistula with, octreotide will not suffice, his nutrition is compromised and TPN will help., , 54., , A 33 year old lady presented with jaundice secondary to common bile duct stones. A, cholecystectomy and common bile duct exploration is performed and the bile duct closed, over a T tube. Six weeks post operatively a T tube cholangiogram is performed and shows, no residual stones. The T tube is removed and five hours after removal a small amount of, bile is noted to be draining from the T tube site.
Page 3212 :
No further action needed, When the bile duct is closed over a T Tube the latex in the T tube encourages tract fibrosis., This actually encourages a fistula to develop. The result is that when the tube is removed, any bile which leaks will usually drain through the tract. Provided that there are no, residual stones in the duct the fistula will slowly close. Persistent high volume drainage, may be managed with ERCP and sphincterotomy., Fistulas are more likely to heal in the absence of distal lumenal obstruction, Please rate this question:, , Discuss and give feedback, , Next question, , Fistulas, , , , , , A fistula is defined as an abnormal connection between two epithelial surfaces., There are many types ranging from Branchial fistulae in the neck to entero-cutaneous, fistulae abdominally., In general surgical practice the abdominal cavity generates the majority and most of these, arise from diverticular disease and Crohn's., As a general rule all fistulae will resolve spontaneously as long as there is no distal, obstruction. This is particularly true of intestinal fistulae., , The four types of fistulae are:, Enterocutaneous, These link the intestine to the skin. They may be high (>500ml) or low output (<250ml) depending, upon source. Duodenal /jejunal fistulae will tend to produce high volume, electrolyte rich secretions, which can lead to severe excoriation of the skin. Colo-cutaneous fistulae will tend to leak faeculent, material. Both fistulae may result from the spontaneous rupture of an abscess cavity onto the skin, (such as following perianal abscess drainage) or may occur as a result of iatrogenic input. In some, cases it may even be surgically desirable e.g. mucous fistula following sub total colectomy for colitis., Suspect if there is excess fluid in the drain., Enteroenteric or Enterocolic, This is a fistula that involves the large or small intestine. They may originate in a similar manner to, enterocutaneous fistulae. A particular problem with this fistula type is that bacterial overgrowth may, precipitate malabsorption syndromes. This may be particularly serious in inflammatory bowel, disease., Enterovaginal, Aetiology as above., Enterovesicular
Page 3213 :
This type of fistula goes to the bladder. These fistulas may result in frequent urinary tract infections,, or the passage of gas from the urethra during urination., Management, Some rules relating to fistula management:, , , , , , , , , They will heal provided there is no underlying inflammatory bowel disease and no distal, obstruction, so conservative measures may be the best option, Where there is skin involvement, protect the overlying skin, often using a well fitted stoma, bag- skin damage is difficult to treat, A high output fistula may be rendered more easily managed by the use of octreotide, this will, tend to reduce the volume of pancreatic secretions., Nutritional complications are common especially with high fistula (e.g. high jejunal or, duodenal) these may necessitate the use of TPN to provide nutritional support together with, the concomitant use of octreotide to reduce volume and protect skin., When managing perianal fistulae surgeons should avoid probing the fistula where acute, inflammation is present, this almost always worsens outcomes., When perianal fistulae occur secondary to Crohn's disease the best management option is, often to drain acute sepsis and maintain that drainage through the judicious use of setons, whilst medical management is implemented., Always attempt to delineate the fistula anatomy, for abscesses and fistulae that have an intra, abdominal source the use of barium and CT studies should show a track. For perianal, fistulae surgeons should recall Goodsall's rule in relation to internal and external openings., Next question
Page 3214 :
Theme: Surgery for inflammatory bowel disease, , A., B., C., D., E., F., , Proctectomy, Anterior resection, Panproctocolectomy, Panproctocolectomy and ileoanal pouch, Sub total colectomy, Right hemicolectomy, , Please select the most appropriate surgical modality for treating the inflammatory bowel disease, scenarios described. Each option may be used once, more than once or not at all., , 55., , A 22 year old man presents with his first presentation of ulcerative colitis. Despite, aggressive medical management with steroids, azathioprine and infliximab his symptoms, remain unchanged and he has developed a megacolon., You answered Proctectomy, The correct answer is Sub total colectomy, In patients with fulminant UC a sub total colectomy is the safest treatment option. The, rectum will be left in situ as resection of the rectum in these acutely unwell patients carries, an extremely high risk of complications., , 56., , A 22 year old lady has a long history of severe perianal Crohns disease with multiple, fistulae. She is keen to avoid a stoma. However, she has progressive disease and multiple, episodes of rectal bleeding. A colonoscopy shows rectal disease only and a small bowel, study shows no involvement with Crohns., Proctectomy, Severe rectal Crohns that has developed complications such as haemorrhage and multiple, fistulae is usually best managed with proctectomy. Although a diverting stoma may reduce, the risk of local sepsis it is unlikely to reduce the bleeding. She is keen to conserve a, rectum, however, an ileoanal pouch in this setting is unwise., , 57., , A 22 year old man has a long history of ulcerative colitis. His symptoms are well, controlled with steroids. However, attempts at steroid weaning and use of steroid sparing, drugs have repeatedly failed. He wishes to avoid a permanent stoma., You answered Proctectomy, The correct answer is Panproctocolectomy and ileoanal pouch
Page 3215 :
In patients with UC where medical management is not successful, surgical resection may, offer a chance of cure. Those patients wishing to avoid a permanent stoma may be, considered for an ileoanal pouch. However, this procedure is only offered in the elective, setting., Please rate this question:, , Discuss and give feedback, , Next question, , Surgery for inflammatory bowel disease, Patients with inflammatory bowel disease (UC and Crohns) frequently present in surgical practice., Ulcerative colitis may be cured by surgical resection (Proctocolectomy), this is not the case in, Crohns disease which may recur and affect other areas of the gastrointestinal tract., Ulcerative colitis, , , , , , , , , Elective indications for surgery include disease that is requiring maximal therapy, or, prolonged courses of steroids., Longstanding UC is associated with a risk of malignant transformation. Dysplastic, transformation of the colonic epithelium with associated mass lesions is an absolute, indication for a proctocolectomy., Emergency presentations of poorly controlled colitis that fails to respond to medical therapy, should usually be managed with a sub total colectomy. Excision of the rectum is a procedure, with a higher morbidity and is not generally performed in the emergency setting. An end, ileostomy is usually created and the rectum either stapled off and left in situ, or, if the bowel, is very oedematous, may be brought to the surface as a mucous fistula., Patients with IBD have a high incidence of DVT and appropriate thromboprophylaxis is, mandatory., Restorative options in UC include an ileoanal pouch. This procedure can only be performed, whilst the rectum is in situ and cannot usually be undertaken as a delayed procedure, following proctectomy., Ileoanal pouch complications include, anastomotic dehiscence, pouchitis and poor, physiological function with seepage and soiling., , Crohns disease, , , , , Surgical resection of Crohns disease does not equate with cure, but may produce substantial, symptomatic improvement., Indications for surgery include complications such as fistulae, abscess formation and, strictures., Extensive small bowel resections may result in short bowel syndrome and localised, stricturoplasty may allow preservation of intestinal length.
Page 3216 :
, , , , , , Staging of Crohns will usually involve colonoscopy and a small bowel study (e.g. MRI, enteroclysis)., Complex perianal fistulae are best managed with long term draining seton sutures, complex, attempts at fistula closure e.g. advancement flaps, may be complicated by non healing and, fistula recurrence., Severe perianal and / or rectal Crohns may require proctectomy. Ileoanal pouch, reconstruction in Crohns carries a high risk of fistula formation and pouch failure and is not, recommended., Terminal ileal Crohns remains the commonest disease site and these patients may be, treated with limited ileocaecal resections., Terminal ileal Crohns may affect enterohepatic bile salt recycling and increase the risk of, gallstones., Next question
Page 3217 :
A 55 year old man develops an acute colonic pseudo-obstruction following a laminectomy. Despite, correction of his electrolytes and ongoing supportive care he fails to settle. Which of the drugs listed, below may improve the situation?, , Buscopan, , Neostigmine, , Metoclopramide, , Mebevrine, , Sodium picosulphate, , Neostigmine affects the degradation of acetylcholine and will therefore stimulate both nicotinic and, muscarinic receptors. It may produce symptomatic bradycardia and should therefore only be, administered in a monitored environment. In colonic pseudo-obstruction it produces generalised, colonic contractions and its onset is usually rapid., Please rate this question:, , Discuss and give feedback, , Next question, , Colonic pseudo-obstruction, Colonic pseudo-obstruction is characterised by the progressive and painless dilation of the colon., The abdomen may become grossly distended and tympanic. Unless a complication such as, impending bowel necrosis or perforation occurs, there is usually little pain., Diagnosis involves excluding a mechanical bowel obstruction with a plain film and contrast enema., The underlying cause is usually electrolyte imbalance and the condition will resolve with correction of, this and supportive care., Patients who do not respond to supportive measures should be treated with attempted colonoscopic, decompression and/ or the drug neostigmine. In rare cases surgery may be required.
Page 3218 :
A 55 year old man is found to have a carcinoma of the sigmoid colon on screening colonoscopy., How should this be staged?, , MRI of the abdomen and CT of the chest, , Liver MRI and Chest CT, , CT scanning of the chest, abdomen and pelvis alone, , MRI of the rectum and CT of the abdomen and chest, , Endoluminal USS and CT scanning of the abdomen, Colonic cancers are staged with CT scanning of the chest, abdomen and pelvis., Theme from January 2015 Exam, Rectal cancer is staged with MRI rectum (and sometimes endolumenal USS for low T1 lesions), together with CT scanning of the chest, abdomen and pelvis. Historically, colonic cancer was staged, with liver USS and CXR. However, modern imaging has made this practice obsolete., Please rate this question:, , Discuss and give feedback, , Next question, , Colorectal cancer screening and diagnosis, Overview, , , , , , Most cancers develop from adenomatous polyps. Screening for colorectal cancer has been, shown to reduce mortality by 16%, The NHS now has a national screening programme offering screening every 2 years to all, men and women aged 60 to 69 years. Patients aged over 70 years may request screening, Eligible patients are sent faecal occult blood (FOB) tests through the post, Patients with abnormal results are offered a colonoscopy, , At colonoscopy, approximately:, , , 5 out of 10 patients will have a normal exam
Page 3219 :
, , , 4 out of 10 patients will be found to have polyps which may be removed due to their, premalignant potential, 1 out of 10 patients will be found to have cancer, , Diagnosis, Essentially the following patients need referral:, - Altered bowel habit for more than six weeks, - New onset of rectal bleeding, - Symptoms of tenesmus, Colonoscopy is the gold standard, provided it is complete and good mucosal visualisation is, achieved. Other options include double contrast barium enema and CT colonography., Staging, Once a malignant diagnosis is made patients with colonic cancer will be staged using chest /, abdomen and pelvic CT. Patients with rectal cancer will also undergo evaluation of the mesorectum, with pelvic MRI scanning., For examination purposes the Dukes and TNM systems are preferred., Tumour markers, Carcinoembryonic antigen (CEA) is the main tumour marker in colorectal cancer. Not all tumours, secrete this, and it may be raised in conditions such as IBD. However, absolute levels do correlate, (roughly) with disease burden and it is once again being used routinely in follow up., Next question
Page 3220 :
Theme: Causes of rectal bleeding, , A., B., C., D., E., F., G., , Fissure in ano, Intersphincteric abscess, Haemorroidal disease, Proctitis, Solitary rectal ulcer syndrome, Rectal cancer, Anal cancer, , Please select the most likely cause of rectal bleeding from the list above. Each option may be used, once, more than once or not at all., , 60., , An 18 year old man with a previous history of constipation presents with bright red rectal, bleeding and diarrhoea. He has suffered episodes of faecal incontinence, which have, occurred randomly throughout the day and night., You answered Fissure in ano, The correct answer is Proctitis, Nocturnal diarrhoea and incontinence are typical of inflammatory bowel disease., , 61., , A 56 year old man presents with episodes of pruritus ani and bright red rectal bleeding. On, examination there is a mass in the ano rectal region and biopsies confirm squamous cell, cancer., You answered Fissure in ano, The correct answer is Anal cancer, These are features of anal cancer. Anal cancers arise from the cutaneous epithelium and, are therefore typically squamous cell. They are usually sensitive to chemoradiotherapy., , 62., , A 19 year old man presents with bright red rectal bleeding. He has a longstanding history, of irritable bowel syndrome. At flexible sigmoidoscopy a lesion is biopsied and reported as, showing 'fibromuscular obliteration'., You answered Fissure in ano, The correct answer is Solitary rectal ulcer syndrome, This is the typical presentation of SRUS. These patients require careful diagnostic work up
Page 3221 :
to elicit the underlying cause of their altered bowel habit. The histological appearances of, solitary rectal ulcers are characteristic and extensive collagenous deposits are often seen., This is usually termed fibromuscular obliteration., Please rate this question:, , Discuss and give feedback, , Next question, , Rectal bleeding, Rectal bleeding is a common cause for patients to be referred to the surgical clinic. In the clinical, history it is useful to try and localise the anatomical source of the blood. Bright red blood is usually of, rectal anal canal origin, whilst dark red blood is more suggestive of a proximally sited bleeding, source. Blood which has entered the GI tract from a gastro-duodenal source will typically resemble, malaena due to the effects of the digestive enzymes on the blood itself., In the table below we give some typical bleeding scenarios together with physical examination, findings and causation., , Cause, , Type of, bleeding, , Features in history, , Examination findings, , Fissure in, ano, , Bright red, rectal, bleeding, , Painful bleeding that occurs, post defecation in small, volumes. Usually antecedent, features of constipation, , Muco-epithelial defect usually, in the midline posteriorly, (anterior fissures more likely to, be due to underlying disease), , Haemorroids, , Bright red, rectal, bleeding, , Post defecation bleeding noted, both on toilet paper and drips, into pan. May be alteration of, bowel habit and history of, straining. No blood mixed with, stool. No local pain., , Normal colon and rectum., Proctoscopy may show internal, haemorrhoids. Internal, haemorrhoids are usually, impalpable., , Crohns, disease, , Bright red or, mixed blood, , Bleeding that is accompanied, by other symptoms such as, altered bowel habit, malaise,, history of fissures (especially, anterior) and abscesses., , Perineal inspection may show, fissures or fistulae. Proctoscopy, may demonstrate indurated, mucosa and possibly strictures., Skip lesions may be noted at
Page 3222 :
colonoscopy., , Ulcerative, colitis, , Bright red, bleeding, often mixed, with stool, , Diarrhoea, weight loss,, nocturnal incontinence, passage, of mucous PR., , Proctitis is the most marked, finding. Peri anal disease is, usually absent. Colonoscopy, will show continuous mucosal, lesion., , Rectal cancer, , Bright red, blood mixed, volumes, , Alteration of bowel habit., Tenesmus may be present., Symptoms of metastatic, disease., , Usually obvious mucosal, abnormality. Lesion may be, fixed or mobile depending upon, disease extent. Surrounding, mucosa often normal, although, polyps may be present., , Image showing a fissure in ano. Typically these are located posteriorly and in the midline. Fissures, at other sites may be associated with underlying disease., , Image sourced from Wikipedia, , Colonoscopic image of internal haemorroids. Note these may often be impalpable.
Page 3223 :
Image sourced from Wikipedia, , Investigation, , , , , , , , , All patients presenting with rectal bleeding require digital rectal examination and proctosigmoidoscopy as a minimal baseline., Remember that haemorrhoids are typically impalpable and to attribute bleeding to these in, the absence of accurate internal inspection is unsatisfactory., In young patients with no other concerning features in the history a carefully performed, sigmoidoscopy that demonstrates clear haemorrhoidal disease may be sufficient. If clear, views cannot be obtained then patients require bowel preparation with an enema and a, flexible sigmoidscopy performed., In those presenting with features of altered bowel habit or suspicion of inflammatory bowel, disease a colonoscopy is the best test., Patients with excessive pain who are suspected of having a fissure may require an, examination under general or local anaesthesia., In young patients with external stigmata of fissure and a compatible history it is acceptable to, treat medically and defer internal examination until the fissure is healed. If the fissure fails to, heal then internal examination becomes necessary along the lines suggested above to, exclude internal disease., , Special tests, , , In patients with a malignancy of the rectum the staging investigations comprise an MRI of the, rectum to identify circumferential resection margin compromise and to identify mesorectal, nodal disease. In addition to this CT scanning of the chest abdomen and pelvis is necessary
Page 3224 :
to stage for more distant disease. Some centres will still stage the mesorectum with endo, rectal ultrasound but this is becoming far less common., , , , Patients with fissure in ano who are being considered for surgical sphincterotomy and are, females who have an obstetric history should probably have ano rectal manometry testing, performed together with endo anal ultrasound. As this service is not universally available it is, not mandatory but in the absence of such information there are continence issues that may, arise following sphincterotomy., , Management, , Disease, , Management, , Fissure in ano, , GTN ointment 0.2% or diltiazem cream applied topically is the usual first line, treatment. Botulinum toxin for those who fail to respond. Internal, sphincterotomy for those who fail with botox, can be considered earlier in, males., , Haemorroids, , Lifestyle advice, for small internal haemorrhoids can consider injection, sclerotherapy or rubber band ligation. For external haemorrhoids consider, haemorrhoidectomy. Modern options include HALO procedure and stapled, haemorrhoidectomy., , Inflammatory, bowel disease, , Medical management- although surgery may be needed for fistulating Crohns, (setons)., , Rectal cancer, , Anterior resection or abdomino-perineal excision of the colon and rectum., Total mesorectal excision is now standard of care. Most resections below the, peritoneal reflection will require defunctioning ileostomy. Most patients will, require preoperative radiotherapy., Next question
Page 3225 :
A 56 year old man presents with his first attack of diverticulitis. Which of these complications is least, likely to ensue?, , Formation of colonic strictures, , Malignant transformation, , Development of colovesical fistula, , Formation of a pericolic abscess, , Formation of a phlegmon, , Diverticulitis may result in a number of complications. However, whilst malignant disease may, coincide with diverticulitis it is not, in itself, a risk factor for colonic cancer., Please rate this question:, , Discuss and give feedback, , Next question, , Diverticular disease, Diverticular disease is a common surgical problem. It consists of herniation of colonic mucosa, through the muscular wall of the colon. The usual site is between the taenia coli where vessels, pierce the muscle to supply the mucosa. For this reason, the rectum, which lacks taenia, is often, spared., Symptoms, , , , , Altered bowel habit, Bleeding, Abdominal pain, , Complications, , , , , , Diverticulitis, Haemorrhage, Development of fistula, Perforation and faecal peritonitis
Page 3226 :
, , , Perforation and development of abscess, Development of diverticular phlegmon, , Diagnosis, Patients presenting in clinic will typically undergo either a colonoscopy, CT cologram or barium, enema as part of their diagnostic work up. All tests can identify diverticular disease. It can be far, more difficult to confidently exclude cancer, particularly in diverticular strictures., Acutely unwell surgical patients should be investigated in a systematic way. Plain abdominal films, and an erect chest x-ray will identify perforation. An abdominal CT scan (not a CT cologram) with, oral and intravenous contrast will help to identify whether acute inflammation is present but also the, presence of local complications such as abscess formation., , Severity Classification- Hinchey, , I, , Para-colonic abscess, , II, , Pelvic abscess, , III, , Purulent peritonitis, , IV, , Faecal peritonitis, , Treatment, , , , , , , Increase dietary fibre intake., Mild attacks of diverticulitis may be managed conservatively with antibiotics., Peri colonic abscesses should be drained either surgically or radiologically., Recurrent episodes of acute diverticulitis requiring hospitalisation are a relative indication for, a segmental resection., Hinchey IV perforations (generalised faecal peritonitis) will require a resection and usually a, stoma. This group have a very high risk of post operative complications and usually require, HDU admission. Less severe perforations may be managed by laparoscopic washout and, drain insertion., Next question
Page 3228 :
The correct answer is Hartman's procedure, , Please rate this question:, , Discuss and give feedback, , Next question, , Colorectal cancer treatment, Patients diagnosed as having colorectal cancer should be completely staged using CT of the chest/, abdomen and pelvis. Their entire colon should have been evaluated with colonoscopy or CT, colonography. Patients whose tumours lie below the peritoneal reflection should have their, mesorectum evaluated with MRI., Once their staging is complete patients should be discussed within a dedicated colorectal MDT, meeting and a treatment plan formulated., Treatment of colonic cancer, Cancer of the colon is nearly always treated with surgery. Stents, surgical bypass and diversion, stomas may all be used as palliative adjuncts. Resectional surgery is the only option for cure in, patients with colon cancer. The procedure is tailored to the patient and the tumour location. The, lymphatic drainage of the colon follows the arterial supply and therefore most resections are tailored, around the resection of particular lymphatic chains (e.g. ileo-colic pedicle for right sided tumours)., Some patients may have confounding factors that will govern the choice of procedure, for example a, tumour in a patient from a HNPCC family may be better served with a panproctocolectomy rather, than segmental resection. Following resection the decision has to be made regarding restoration of, continuity. For an anastomosis to heal the key technical factors include; adequate blood supply,, mucosal apposition and no tissue tension. Surrounding sepsis, unstable patients and inexperienced, surgeons may compromise these key principles and in such circumstances it may be safer to, construct an end stoma rather than attempting an anastomosis., When a colonic cancer presents with an obstructing lesion; the options are to either stent it or resect., In modern practice it is unusual to simply defunction a colonic tumour with a proximal loop stoma., This differs from the situation in the rectum (see below)., Following resection patients with risk factors for disease recurrence are usually offered, chemotherapy, a combination of 5FU and oxaliplatin is common., Rectal cancer
Page 3229 :
The management of rectal cancer is slightly different to that of colonic cancer. This reflects the, rectum's anatomical location and the challenges posed as a result. Tumours located in the rectum, can be surgically resected with either an anterior resection or an abdomino - perineal resection. The, technical aspects governing the choice between these two procedures can be complex to appreciate, and the main point to appreciate for the MRCS is that involvement of the sphincter complex or very, low tumours require APER. In the rectum a 2cm distal clearance margin is required and this may, also impact on the procedure chosen. In addition to excision of the rectal tube an integral part of the, procedure is a meticulous dissection of the mesorectal fat and lymph nodes (total mesorectal, excision/ TME). In rectal cancer surgery invovlement of the cirumferential resection margin carries a, high risk of disease recurrence. Because the rectum is an extraperitoneal structure (until you remove, it that is!) it is possible to irradiate it, something which cannot be offered for colonic tumours. This, has a major impact in rectal cancer treatment and many patients will be offered neoadjuvent, radiotherapy (both long and short course) prior to resectional surgery. Patients with T1 and 2 /N0, disease on imaging do not require irradiation and should proceed straight to surgery. Patients with, T4 disease will typically have long course chemo radiotherapy. Those with T3 , N0 tumours may be, offered short course radiotherapy prior to surgery. Patients presenting with large bowel obstruction, from rectal cancer should not undergo resectional surgery without staging as primary treatment (very, different from colonic cancer). This is because rectal surgery is more technically demanding, the, anastomotic leak rate is higher and the danger of a positive resection margin in an unstaged patient, is high. Therefore patients with obstructing rectal cancer should have a defunctioning loop, colostomy., Summary of procedures, The operations for cancer are segmental resections based on blood supply and lymphatic drainage., These commonly performed procedures are core knowledge for the MRCS and should be, understood., , Site of cancer, , Type of resection, , Anastomosis, , Risk of, leak, , Right colon, , Right hemicolectomy, , Ileo-colic, , Low <5%, , Transverse, , Extended right hemicolectomy, , Ileo-colic, , Low <5%, , Splenic, flexure, , Extended right hemicolectomy, , Ileo-colic, , Low <5%, , Splenic, flexure, , Left hemicolectomy, , Colo-colon, , 2-5%
Page 3230 :
Site of cancer, , Type of resection, , Anastomosis, , Risk of, leak, , Left colon, , Left hemicolectomy, , Colo-colon, , 2-5%, , Sigmoid colon, , High anterior resection, , Colo-rectal, , 5%, , Upper rectum, , Anterior resection (TME), , Colo-rectal, , 5%, , Low rectum, , Anterior resection (Low TME), , Colo-rectal, (+/- Defunctioning, stoma), , 10%, , Anal verge, , Abdomino-perineal excision of colon and, rectum, , None, , n/a, , In the emergency setting, where the bowel has perforated, the risk of an anastomosis is much, greater, particularly when the anastomosis is colon-colon. In this situation, an end colostomy is often, safer and can be reversed later. When resection of the sigmoid colon is performed and an end, colostomy is fashioned the operation is referred to as a Hartmans procedure. Whilst left sided, resections are more risky, ileo-colic anastomoses are relatively safe even in the emergency setting, and do not need to be defunctioned., References, A review of the diagnosis and management of colorectal cancer and a summary of the UK National, Institute of Clinical Excellence guidelines is provided in:, Poston G, et al . Diagnosis and management of colorectal cancer:summary of NICE, guidance. BMJ2011: 343: d 6751., Next question
Page 3231 :
A 34 year old lady presents to her general practitioner with peri anal discomfort. The general, practitioner diagnoses pruritus ani, which of the following is least associated with the condition?, , Hyperbilirubinaemia, , Anal fissure, , Leukaemia, , Syphilis, , Tuberculosis, , Causes:, , , , , , , , , Systemic (DM, Hyperbilirubinaemia, aplastic anaemia), Mechanical (diarrhoea, constipation, anal fissure), Infections (STDs), Dermatological, Drugs (quinidine, colchicine), Topical agents, , Please rate this question:, , Discuss and give feedback, , Next question, , Ano rectal disease, , Haemorrhoids, , Fissure in ano, , Location: 3, 7, 11 o'clock position, Internal or external, Treatment: Conservative, Rubber band ligation, Haemorrhoidectomy, , Location: midline 6 (posterior midline 90%) and 12 o'clock position. Distal to, the dentate line
Page 3232 :
Chronic fissure > 6/52: triad: Ulcer, sentinel pile, enlarged anal papillae, , Proctitis, , Causes: Crohn's, ulcerative colitis, Clostridium difficile, , Ano rectal, abscess, , E.coli, staph aureus, Positions: Perianal, Ischiorectal, Pelvirectal, Intersphincteric, , Anal fistula, , Usually due to previous ano-rectal abscess, Intersphincteric, transsphincteric, suprasphincteric, and extrasphincteric., Goodsalls rule determines location, , Rectal prolapse, , Associated with childbirth and rectal intussceception. May be internal or, external, , Pruritus ani, , Systemic and local causes, , Anal neoplasm, , Squamous cell carcinoma commonest unlike adenocarcinoma in rectum, , Solitary rectal, ulcer, , Associated with chronic straining and constipation. Histology shows mucosal, thickening, lamina propria replaced with collagen and smooth muscle, (fibromuscular obliteration), , Rectal prolapse, , , , , , , Common especially in multiparous women., May be internal or external., Internal rectal prolapse can present insidiously., External prolapse can ulcerate and in long term impair continence., Diagnostic work up includes colonoscopy, defecating proctogram, ano rectal manometry, studies and if doubt exists an examination under anaesthesia., , Treatments for prolapse, , , , In the acute setting reduce it (covering it with sugar may reduce swelling., Delormes procedure which excises mucosa and plicates the rectum (high recurrence rates), may be used for external prolapse.
Page 3233 :
, , , Altmeirs procedure which resects the colon via the perineal route has lower recurrence rates, but carries the risk of anastamotic leak., Rectopexy is an abdominal procedure in which the rectum is elevated and usually supported, at the level of the sacral promontory. Post operative constipation may be reduced by limiting, the dissection to the anterior plane (laparoscopic ventral mesh rectopexy)., , Pruritus ani, , , , , , , , Extremely common., Check not secondary to altered bowel habits (e.g. Diarrhoea), Associated with underlying diseases such as haemorrhoids., Examine to look for causes such as worms., Proctosigmoidoscopy to identify associated haemorrhoids and exclude cancer., Treatment is largely supportive and patients should avoid using perfumed products around, the area., , Fissure in ano, , , , , Typically painful PR bleeding (bright red)., Nearly always in the posterior midline., Usually solitary., , Treatment, , , , , , , Stool softeners., Topical diltiazem (or GTN)., If topical treatments fail then botulinum toxin should be injected., If botulinum toxin fails then males should probably undergo lateral internal sphincterotomy., Females who do not respond to botulinum toxin should undergo ano rectal manometry, studies and endo anal USS prior to being offered surgery such as sphincterotomy., Next question
Page 3234 :
Theme: Fistula, , A., B., C., D., E., F., G., H., , Recurrent urinary tract infection secondary to catheter, Nephroenteric fistula, Enterovesical fistula, High Enterocutaneous fistula, Low Enterocutaneous fistula, Enteroenteric fistula, Colocutaneous fistula, Wound infection, , Please select the most likely diagnosis for the scenario given. Each option may be used once, more, than once or not at all., , 68., , You are the specialist trainee asked to review a 39 year old man post gastrectomy for, bleeding duodenal ulcers. He is hypotensive and tachycardic. His drain has increased, output, contains pus and has bubbles. There is excoriated skin around the drain site., You answered Recurrent urinary tract infection secondary to catheter, The correct answer is High Enterocutaneous fistula, Suspect an enterocutaneous fistula if there is excessive drainage and bubbles. Pus may, confuse surgeons, leading them to make a diagnosis of wound infection. If there is any, uncertainty, methylene blue can be given. If methylene blue is found in the drain, this, confirms a fistula., , 69., , A 43 year old female presents with recurrent urinary tract infections. She describes blood, and frothy urine. She is 6 weeks post operative for a left hemicolectomy for crohn's, disease., You answered Recurrent urinary tract infection secondary to catheter, The correct answer is Enterovesical fistula, A nephroenteric fistula causes a chronic urinary tract infection, hence develops over a, longer time frame., , 70., , A 2 week infant has foul smelling material discharging from the umbilicus., You answered Recurrent urinary tract infection secondary to catheter, The correct answer is Low Enterocutaneous fistula
Page 3235 :
This baby has an enterocutaneous fistula at the umbilicus due to complete failure of the, omphalomesenteric duct to obliterate. This is treated with resection., Please rate this question:, , Discuss and give feedback, , Next question, , Fistulas, , , , , , A fistula is defined as an abnormal connection between two epithelial surfaces., There are many types ranging from Branchial fistulae in the neck to entero-cutaneous, fistulae abdominally., In general surgical practice the abdominal cavity generates the majority and most of these, arise from diverticular disease and Crohn's., As a general rule all fistulae will resolve spontaneously as long as there is no distal, obstruction. This is particularly true of intestinal fistulae., , The four types of fistulae are:, Enterocutaneous, These link the intestine to the skin. They may be high (>500ml) or low output (<250ml) depending, upon source. Duodenal /jejunal fistulae will tend to produce high volume, electrolyte rich secretions, which can lead to severe excoriation of the skin. Colo-cutaneous fistulae will tend to leak faeculent, material. Both fistulae may result from the spontaneous rupture of an abscess cavity onto the skin, (such as following perianal abscess drainage) or may occur as a result of iatrogenic input. In some, cases it may even be surgically desirable e.g. mucous fistula following sub total colectomy for colitis., Suspect if there is excess fluid in the drain., Enteroenteric or Enterocolic, This is a fistula that involves the large or small intestine. They may originate in a similar manner to, enterocutaneous fistulae. A particular problem with this fistula type is that bacterial overgrowth may, precipitate malabsorption syndromes. This may be particularly serious in inflammatory bowel, disease., Enterovaginal, Aetiology as above., Enterovesicular, This type of fistula goes to the bladder. These fistulas may result in frequent urinary tract infections,, or the passage of gas from the urethra during urination., Management, Some rules relating to fistula management:
Page 3236 :
, , , , , , , , They will heal provided there is no underlying inflammatory bowel disease and no distal, obstruction, so conservative measures may be the best option, Where there is skin involvement, protect the overlying skin, often using a well fitted stoma, bag- skin damage is difficult to treat, A high output fistula may be rendered more easily managed by the use of octreotide, this will, tend to reduce the volume of pancreatic secretions., Nutritional complications are common especially with high fistula (e.g. high jejunal or, duodenal) these may necessitate the use of TPN to provide nutritional support together with, the concomitant use of octreotide to reduce volume and protect skin., When managing perianal fistulae surgeons should avoid probing the fistula where acute, inflammation is present, this almost always worsens outcomes., When perianal fistulae occur secondary to Crohn's disease the best management option is, often to drain acute sepsis and maintain that drainage through the judicious use of setons, whilst medical management is implemented., Always attempt to delineate the fistula anatomy, for abscesses and fistulae that have an intra, abdominal source the use of barium and CT studies should show a track. For perianal, fistulae surgeons should recall Goodsall's rule in relation to internal and external openings., Next question
Page 3237 :
A 28 year old male presents with a discharging sinus in his natal cleft. He is found to have a pilonidal, sinus. Which statement is false?, , Can occur in webs of fingers and the axilla, , After drainage pilonidal abscesses should not be primarily closed, , A rare complication is squamous cell carcinoma, , In a patient with an acute abscess the Bascoms procedure is the treatment of choice., , Treatment involves excising or laying open the sinus tract., When performing incision and drainage for pilonidal abscess try to avoid making the incision in the, midline of the natal cleft., Acute pilonidal abscesses should receive simple incision and drainage. Definitive treatments such as, a Bascoms procedure should not be undertaken when acute sepsis is present., Please rate this question:, , Discuss and give feedback, , Next question, , Pilonidal sinus, , , , , , , , , , Occur as a result of hair debris creating sinuses in the skin (Bascom theory)., Usually in the natal cleft of male patients after puberty., It is more common in Caucasians related to their hair type and growth patterns., The opening of the sinus is lined by squamous epithelium, but most of its wall consists of, granulation tissue. Up to 50 cases of squamous cell carcinoma have been described in, patients with chronic pilonidal sinus disease., Hairs become trapped within the sinus., Clinically the sinus presents when acute inflammation occurs, leading to an abscess., Patients may describe cycles of being asymptomatic and periods of pain and discharge from, the sinus., Treatment is difficult and opinions differ. Definitive treatment should never be undertaken, when acute infection or abscess is present as this will result in failure., Definitive treatments include the Bascom procedure with excision of the pits and obliteration, of the underlying cavity. The Karydakis procedure involves wide excision of the natal cleft, such that the surface is recontoured once the wound is closed. This avoids the shearing, forces that break off the hairs and has reasonable results.
Page 3238 :
Pilonidal sinuses are most commonly located in the midline of the natal cleft, as illustrated below, , Image sourced from Wikipedia, , Next question
Page 3239 :
Theme: Colonic resections, , A. Right hemicolectomy and ileocolic anastomosis, B. Extended right hemicolectomy and ileocolic anastomosis, C. Hartman's procedure, D. Defunctioning loop ileostomy only, E. Anterior resection and colo-rectal anastomosis, F. Abdomino-perineal excision of colon and rectum, , Please select the most appropriate resection for the scenario given. Each option may be used once,, more than once or not at all., , 72., , A 58 year old man with a tumour of the splenic flexure that requires resection., You answered Right hemicolectomy and ileocolic anastomosis, The correct answer is Extended right hemicolectomy and ileocolic anastomosis, Beware of the anatomy at the base of the middle colic which will require high ligation., , 73., , A 63 year old man presents with a carcinoma of the upper rectum. Staging investigations, demonstrate localised disease and he is not deemed to require and neo adjuvent therapy., You answered Right hemicolectomy and ileocolic anastomosis, The correct answer is Anterior resection and colo-rectal anastomosis, Upper rectal tumours are usually amenable to restoration of intestinal continuity and therefore, an anterior resection is a reasonable treatment option., , 74., , A 66 year old lady presents with a tumour of the low rectum. There is a projection inferior to, within 1cm of the dentate line.
Page 3240 :
You answered Right hemicolectomy and ileocolic anastomosis, The correct answer is Abdomino-perineal excision of colon and rectum, Low rectal tumours such as this will require APER., , Please rate this question:, , Discuss and give feedback, , Next question, , Colorectal cancer treatment, Patients diagnosed as having colorectal cancer should be completely staged using CT of the chest/, abdomen and pelvis. Their entire colon should have been evaluated with colonoscopy or CT, colonography. Patients whose tumours lie below the peritoneal reflection should have their, mesorectum evaluated with MRI., Once their staging is complete patients should be discussed within a dedicated colorectal MDT, meeting and a treatment plan formulated., Treatment of colonic cancer, Cancer of the colon is nearly always treated with surgery. Stents, surgical bypass and diversion, stomas may all be used as palliative adjuncts. Resectional surgery is the only option for cure in, patients with colon cancer. The procedure is tailored to the patient and the tumour location. The, lymphatic drainage of the colon follows the arterial supply and therefore most resections are tailored, around the resection of particular lymphatic chains (e.g. ileo-colic pedicle for right sided tumours)., Some patients may have confounding factors that will govern the choice of procedure, for example a, tumour in a patient from a HNPCC family may be better served with a panproctocolectomy rather, than segmental resection. Following resection the decision has to be made regarding restoration of, continuity. For an anastomosis to heal the key technical factors include; adequate blood supply,, mucosal apposition and no tissue tension. Surrounding sepsis, unstable patients and inexperienced, surgeons may compromise these key principles and in such circumstances it may be safer to, construct an end stoma rather than attempting an anastomosis., When a colonic cancer presents with an obstructing lesion; the options are to either stent it or resect., In modern practice it is unusual to simply defunction a colonic tumour with a proximal loop stoma., This differs from the situation in the rectum (see below).
Page 3241 :
Following resection patients with risk factors for disease recurrence are usually offered, chemotherapy, a combination of 5FU and oxaliplatin is common., Rectal cancer, The management of rectal cancer is slightly different to that of colonic cancer. This reflects the, rectum's anatomical location and the challenges posed as a result. Tumours located in the rectum, can be surgically resected with either an anterior resection or an abdomino - perineal resection. The, technical aspects governing the choice between these two procedures can be complex to appreciate, and the main point to appreciate for the MRCS is that involvement of the sphincter complex or very, low tumours require APER. In the rectum a 2cm distal clearance margin is required and this may, also impact on the procedure chosen. In addition to excision of the rectal tube an integral part of the, procedure is a meticulous dissection of the mesorectal fat and lymph nodes (total mesorectal, excision/ TME). In rectal cancer surgery invovlement of the cirumferential resection margin carries a, high risk of disease recurrence. Because the rectum is an extraperitoneal structure (until you remove, it that is!) it is possible to irradiate it, something which cannot be offered for colonic tumours. This, has a major impact in rectal cancer treatment and many patients will be offered neoadjuvent, radiotherapy (both long and short course) prior to resectional surgery. Patients with T1 and 2 /N0, disease on imaging do not require irradiation and should proceed straight to surgery. Patients with, T4 disease will typically have long course chemo radiotherapy. Those with T3 , N0 tumours may be, offered short course radiotherapy prior to surgery. Patients presenting with large bowel obstruction, from rectal cancer should not undergo resectional surgery without staging as primary treatment (very, different from colonic cancer). This is because rectal surgery is more technically demanding, the, anastomotic leak rate is higher and the danger of a positive resection margin in an unstaged patient, is high. Therefore patients with obstructing rectal cancer should have a defunctioning loop, colostomy., Summary of procedures, The operations for cancer are segmental resections based on blood supply and lymphatic drainage., These commonly performed procedures are core knowledge for the MRCS and should be, understood., , Site of cancer, , Type of resection, , Anastomosis, , Risk of, leak, , Right colon, , Right hemicolectomy, , Ileo-colic, , Low <5%, , Transverse, , Extended right hemicolectomy, , Ileo-colic, , Low <5%, , Splenic, flexure, , Extended right hemicolectomy, , Ileo-colic, , Low <5%
Page 3242 :
Site of cancer, , Type of resection, , Anastomosis, , Risk of, leak, , Splenic, flexure, , Left hemicolectomy, , Colo-colon, , 2-5%, , Left colon, , Left hemicolectomy, , Colo-colon, , 2-5%, , Sigmoid colon, , High anterior resection, , Colo-rectal, , 5%, , Upper rectum, , Anterior resection (TME), , Colo-rectal, , 5%, , Low rectum, , Anterior resection (Low TME), , Colo-rectal, (+/- Defunctioning, stoma), , 10%, , Anal verge, , Abdomino-perineal excision of colon and, rectum, , None, , n/a, , In the emergency setting, where the bowel has perforated, the risk of an anastomosis is much, greater, particularly when the anastomosis is colon-colon. In this situation, an end colostomy is often, safer and can be reversed later. When resection of the sigmoid colon is performed and an end, colostomy is fashioned the operation is referred to as a Hartmans procedure. Whilst left sided, resections are more risky, ileo-colic anastomoses are relatively safe even in the emergency setting, and do not need to be defunctioned., References, A review of the diagnosis and management of colorectal cancer and a summary of the UK National, Institute of Clinical Excellence guidelines is provided in:, Poston G, et al . Diagnosis and management of colorectal cancer:summary of NICE, guidance. BMJ2011: 343: d 6751., Next question
Page 3243 :
A 23 year old lady presents with a posteriorly sited fissure in ano. Treatment with stool softeners and, topical GTN has failed to improve matters. Which of the following would be the most appropriate, next management step?, , Lords procedure, , Fissurectomy and injection of botulinum toxin, , Lateral internal sphincterotomy, , Endoanal advancement flap, , Surgical division of the external anal sphincter, , The next most appropriate management option when GTN or other topical nitrates has failed is to, consider botulinum toxin injection. In males a lateral internal sphincterotomy would be an acceptable, alternative. In a female who has yet to conceive this may predispose to delayed increased risk of, sphincter dysfunction. Division of the external sphincter will result in faecal incontinence and is not a, justified treatment for fissure., Please rate this question:, , Discuss and give feedback, , Rectal bleeding, Rectal bleeding is a common cause for patients to be referred to the surgical clinic. In the clinical, history it is useful to try and localise the anatomical source of the blood. Bright red blood is usually of, rectal anal canal origin, whilst dark red blood is more suggestive of a proximally sited bleeding, source. Blood which has entered the GI tract from a gastro-duodenal source will typically resemble, malaena due to the effects of the digestive enzymes on the blood itself., In the table below we give some typical bleeding scenarios together with physical examination, findings and causation., , Cause, , Type of, bleeding, , Features in history, , Examination findings, , Fissure in, , Bright red, rectal, , Painful bleeding that occurs, post defecation in small, , Muco-epithelial defect usually, in the midline posteriorly
Page 3244 :
ano, , bleeding, , volumes. Usually antecedent, features of constipation, , (anterior fissures more likely to, be due to underlying disease), , Haemorroids, , Bright red, rectal, bleeding, , Post defecation bleeding noted, both on toilet paper and drips, into pan. May be alteration of, bowel habit and history of, straining. No blood mixed with, stool. No local pain., , Normal colon and rectum., Proctoscopy may show internal, haemorrhoids. Internal, haemorrhoids are usually, impalpable., , Crohns, disease, , Bright red or, mixed blood, , Bleeding that is accompanied, by other symptoms such as, altered bowel habit, malaise,, history of fissures (especially, anterior) and abscesses., , Perineal inspection may show, fissures or fistulae. Proctoscopy, may demonstrate indurated, mucosa and possibly strictures., Skip lesions may be noted at, colonoscopy., , Ulcerative, colitis, , Bright red, bleeding, often mixed, with stool, , Diarrhoea, weight loss,, nocturnal incontinence, passage, of mucous PR., , Proctitis is the most marked, finding. Peri anal disease is, usually absent. Colonoscopy, will show continuous mucosal, lesion., , Rectal cancer, , Bright red, blood mixed, volumes, , Alteration of bowel habit., Tenesmus may be present., Symptoms of metastatic, disease., , Usually obvious mucosal, abnormality. Lesion may be, fixed or mobile depending upon, disease extent. Surrounding, mucosa often normal, although, polyps may be present., , Image showing a fissure in ano. Typically these are located posteriorly and in the midline. Fissures, at other sites may be associated with underlying disease.
Page 3245 :
Image sourced from Wikipedia, , Colonoscopic image of internal haemorroids. Note these may often be impalpable., , Image sourced from Wikipedia, , Investigation, , , All patients presenting with rectal bleeding require digital rectal examination and proctosigmoidoscopy as a minimal baseline.
Page 3246 :
, , , , , , , Remember that haemorrhoids are typically impalpable and to attribute bleeding to these in, the absence of accurate internal inspection is unsatisfactory., In young patients with no other concerning features in the history a carefully performed, sigmoidoscopy that demonstrates clear haemorrhoidal disease may be sufficient. If clear, views cannot be obtained then patients require bowel preparation with an enema and a, flexible sigmoidscopy performed., In those presenting with features of altered bowel habit or suspicion of inflammatory bowel, disease a colonoscopy is the best test., Patients with excessive pain who are suspected of having a fissure may require an, examination under general or local anaesthesia., In young patients with external stigmata of fissure and a compatible history it is acceptable to, treat medically and defer internal examination until the fissure is healed. If the fissure fails to, heal then internal examination becomes necessary along the lines suggested above to, exclude internal disease., , Special tests, , , In patients with a malignancy of the rectum the staging investigations comprise an MRI of the, rectum to identify circumferential resection margin compromise and to identify mesorectal, nodal disease. In addition to this CT scanning of the chest abdomen and pelvis is necessary, to stage for more distant disease. Some centres will still stage the mesorectum with endo, rectal ultrasound but this is becoming far less common., , , , Patients with fissure in ano who are being considered for surgical sphincterotomy and are, females who have an obstetric history should probably have ano rectal manometry testing, performed together with endo anal ultrasound. As this service is not universally available it is, not mandatory but in the absence of such information there are continence issues that may, arise following sphincterotomy., , Management, , Disease, , Management, , Fissure in ano, , GTN ointment 0.2% or diltiazem cream applied topically is the usual first line, treatment. Botulinum toxin for those who fail to respond. Internal, sphincterotomy for those who fail with botox, can be considered earlier in, males., , Haemorroids, , Lifestyle advice, for small internal haemorrhoids can consider injection, sclerotherapy or rubber band ligation. For external haemorrhoids consider
Page 3247 :
haemorrhoidectomy. Modern options include HALO procedure and stapled, haemorrhoidectomy., , Inflammatory, bowel disease, , Medical management- although surgery may be needed for fistulating Crohns, (setons)., , Rectal cancer, , Anterior resection or abdomino-perineal excision of the colon and rectum., Total mesorectal excision is now standard of care. Most resections below the, peritoneal reflection will require defunctioning ileostomy. Most patients will, require preoperative radiotherapy.
Page 3249 :
A 21 year old man is involved in a road traffic accident. After a transient period of concussion he is, found to have a GCS of 15 by the paramedics. On arrival at hospital he is monitored in a side room, of the emergency department. When he is next observed he is noted to have a GCS of 3 and a, blown right pupil. Which of the processes below best accounts for this deterioration?, , Hydrocephalus, , Intraventricular bleed, , Sub dural bleed, , Trans tentorial herniation, , Sub arachnoid haemorrhage, , Theme from April 2012 Exam, The presence of a blown right pupil is a sign of a third cranial nerve compression. The most likely, cause is an extradural bleed. However, since this option is not listed the process of trans tentorial, herniation would be the most applicable answer. Intraventricular bleeds are typically more common, in premature neonates, deterioration due to hydrocephalus is more chronic., Please rate this question:, , Discuss and give feedback, , Next question, , Head injuries, Head injury is the commonest cause of death and disability in people aged 1-40 years in the UK. In, the UK 1.4 million people will attend emergency departments each year with a recent head injury., The typical patterns are described below:, , Extradural, haematoma, , Bleeding into the space between the dura mater and the skull. Often results, from acceleration-deceleration trauma or a blow to the side of the head. The, majority of extradural haematomas occur in the temporal region where skull, fractures cause a rupture of the middle meningeal artery., Features, , , Raised intracranial pressure
Page 3250 :
, , Subdural, haematoma, , Some patients may exhibit a lucid interval, , Bleeding into the outermost meningeal layer. Most commonly occur around, the frontal and parietal lobes. May be either acute or chronic., Risk factors include old age and alcoholism., Slower onset of symptoms than a extradural haematoma., , Subarachnoid, haemorrhage, , Usually occurs spontaneously in the context of a ruptured cerebral aneurysm, but may be seen in association with other injuries when a patient has, sustained a traumatic brain injury
Page 3251 :
Theme: Intracranial bleeds, , A., B., C., D., E., , Intraventricular haemorrhage, Chronic sub dural bleed, Acute sub dural bleed, Extra dural haemorrhage, Sub arachnoid haemorrhage, , Please select the most likely underlying diagnosis for the scenario described. Each option may be, used once, more than once or not at all., , 2., , A 50 year old alcoholic man attends the emergency department. His main reason for, presenting is that he has no home to go to. On examination he has no evidence of, involvement in recent trauma, a skull x-ray fails to show any evidence of skull fracture. He, is admitted and twelve hours following admission he develops sudden onset headache,, becomes comatose and then dies., You answered Intraventricular haemorrhage, The correct answer is Sub arachnoid haemorrhage, Theme from April 2013 Exam, The absence of trauma here makes an acute sub dural and extra dural bleed unlikely., Chronic sub dural bleeds would usually cause a more gradual deterioration than is seen, here. The absence of any skull fracture also makes an underlying intra cranial bleed less, likely. Sudden onset headaches, together with sudden deterioration in neurological function, are typical of a sub arachnoid haemorrhage., , 3., , A 50 year old lady is admitted having fallen down some stairs sustaining multiple rib, fractures 36 hours previously. On examination she is confused and agitated and has clinical, evidence of lateralising signs. She deteriorates further and then dies with no response to, resuscitation., You answered Intraventricular haemorrhage, The correct answer is Acute sub dural bleed, The time frame of deterioration of an acute sub dural bleed would fit with this scenario., They are highly lethal and not uncommon injuries. As the bleed enlarges, lateralising signs, may be seen and eventually coning and death will occur., , 4., , A male infant is born at 28 weeks gestation by emergency cesarean section. He is taken to, theatre for a colostomy due to an imperforate anus. He initially seems to be progressing, well. However, he begins to develop decerebrate posturing and is becoming increasingly
Page 3252 :
obtunded., Intraventricular haemorrhage, Acute neurological deterioration in premature neonates is usually due to intraventricular, haemorrhage. Diagnosis is made by cranial ultrasound. Development of hydrocephalus may, necessitate surgery., Please rate this question:, , Discuss and give feedback, , Next question, , Intra cranial haemorrhage, Extradural, haematoma, , Bleeding into the space between the dura mater and the skull. Often results, from acceleration-deceleration trauma or a blow to the side of the head. The, majority of extradural haematomas occur in the temporal region where skull, fractures cause a rupture of the middle meningeal artery., Features, , , , Subdural, haematoma, , Raised intracranial pressure, Some patients may exhibit a lucid interval, , Bleeding into the outermost meningeal layer. Most commonly occur around, the frontal and parietal lobes. May be either acute or chronic., Risk factors include old age and alcoholism., Slower onset of symptoms than a extradural haematoma., , Intracerebral, haematoma, , Usually hyperdense lesions on CT scanning. Arise in areas of traumatic, contusion with fuse to become a haematoma. Areas of clot and fresh blood, may co-exist on the same CT scan (Swirl sign). Large haematomas and, those associated with mass effect should be evacuated., , Subarachnoid, haemorrhage, , Usually occurs spontaneously in the context of a ruptured cerebral, aneurysm but may be seen in association with other injuries when a patient, has sustained a traumatic brain injury
Page 3253 :
Intraventricular, haemorrhage, , Haemorrhage that occurs into the ventricular system of the brain. It is, relatively rare in adult surgical practice and when it does occur, it is, typically associated with severe head injuries. In premature neonates it may, occur spontaneously. The blood may clot and occlude CSF flow,, hydrocephalus may result., In neonatal practice the vast majority of IVH occur in the first 72 hours, after birth, the aetiology is not well understood and it is suggested to occur, as a result of birth trauma combined with cellular hypoxia, together with the, delicate neonatal CNS.
Page 3254 :
Theme: Cranial nerve lesions, , A. Optic nerve, B. Oculomotor nerve, C. Trigeminal nerve, D. Facial nerve, E. Abducens nerve, F. Glossopharyngeal nerve, G. Vestibulocochlear nerve, H. Accessory nerve, I. Hypoglossal nerve, , For each of the scenarios given please give the most likely cranial nerve responsible for the, symptom or lesion described. Each nerve may be used once, more than once or not at all., , 5., , A 63 year old man is admitted with severe headache, nausea and recent epileptic fit. Fundoscopy, shows papilloedema. He is also noted to have diplopia., You answered Optic nerve, The correct answer is Abducens nerve, The long intracranial course of this nerve makes it susceptible to damage early in the course of, raised ICP., , 6., , A 32 year old lady is admitted with weakness, visual disturbance and peri orbital pain. On, examination, she is noted to have mydriasis and diminished direct response to light shone into the, affected eye. The consensual response is preserved when light is shone into the unaffected eye., Optic nerve, This describes a relative afferent pupillary defect (RAPD). RAPD is a defect in the direct response to
Page 3255 :
light. It is due to damage in optic nerve or severe retinal disease. If an optic nerve lesion is present, the affected pupil will not constrict to light when light is shone in the that pupil during the swinging, flashlight test. However, it will constrict if light is shone in the other eye (consensual response)., The most likely cause for this is an optic neuritis (not really surgical!). Other causes include, ischemic optic disease or retinal disease, severe glaucoma causing trauma to optic nerve and direct, optic nerve damage (trauma, radiation, tumor)., , 7., , An 18 year old boy undergoes an uncomplicated tonsillectomy for recurrent attacks of tonsillitis., Post operatively he complains of otalgia., You answered Optic nerve, The correct answer is Glossopharyngeal nerve, The glossopharyngeal nerve supplies this area and the ear and otalgia may be the result of referred, pain., , Please rate this question:, , Discuss and give feedback, , Next question, , Cranial nerves, Cranial nerve lesions, , Olfactory nerve, , May be injured in basal skull fractures or involved in frontal lobe tumour extension., Loss of olfactory nerve function in relation to major CNS pathology is seldom an, isolated event and thus it is poor localiser of CNS pathology., , Optic nerve, , Problems with visual acuity may result from intra ocular disorders. Problems with, the blood supply such as amaurosis fugax may produce temporary visual distortion.
Page 3256 :
More important surgically is the pupillary response to light. The pupillary size may, be altered in a number of disorders. Nerves involved in the resizing of the pupil, connect to the pretectal nucleus of the high midbrain, bypassing the lateral, geniculate nucleus and the primary visual cortex. From the pretectal nucleus, neurones pass to the Edinger - Westphal nucleus, motor axons from here pass along, with the oculomotor nerve. They synapse with ciliary ganglion neurones; the, parasympathetic axons from this then innervate the iris and produce miosis. The, miotic pupil is seen in disorders such as Horner's syndrome or opiate overdose., Mydriasis is the dilatation of the pupil in response to disease, trauma, drugs (or the, dark!). It is pathological when light fails to induce miosis. The radial muscle is, innervated by the sympathetic nervous system. Because the parasympathetic fibres, travel with the oculomotor nerve they will be damaged by lesions affecting this, nerve (e.g. cranial trauma)., The response to light shone in one eye is usually a constriction of both pupils. This, indicates intact direct and consensual light reflexes. When the optic nerve has an, afferent defect the light shining on the affected eye will produce a diminished, pupillary response in both eyes. Whereas light shone on the unaffected eye will, produce a normal pupillary response in both eyes. This is referred to as the Marcus, Gunn pupil and is seen in conditions such as optic neuritis. In a total CN II lesion, shining the light in the affected eye will produce no response., , Oculomotor nerve, , The pupillary effects are described above. In addition it supplies all ocular muscles, apart from lateral rectus and superior oblique. Thus the affected eye will be, deviated inferolaterally. Levator palpebrae superioris may also be impaired resulting, in impaired ability to open the eye., , Trochlear nerve, , The eye will not be able to look down., , Trigeminal nerve, , Largest cranial nerve. Exits the brainstem at the pons. Branches are ophthalmic,, maxillary and mandibular. Only the mandibular branch has both sensory and motor, fibres. Branches converge to form the trigeminal ganglion (located in Meckels cave)., It supplies the muscles of mastication and also tensor veli palatine, mylohyoid,, anterior belly of digastric and tensor tympani. The detailed descriptions of the, various sensory functions are described in other areas of the website. The corneal, reflex is important and is elicited by applying a small tip of cotton wool to the, cornea, a reflex blink should occur if it is intact. It is mediated by: the naso ciliary, branch of the ophthalmic branch of the trigeminal (sensory component) and the, facial nerve producing the motor response. Lesions of the afferent arc will produce
Page 3257 :
bilateral absent blink and lesions of the efferent arc will result in a unilateral absent, blink., , Abducens nerve, , The affected eye will have a deficit of abduction. This cranial nerve exits the, brainstem between the pons and medulla. It thus has a relatively long intra cranial, course which renders it susceptible to damage in raised intra cranial pressure., , Facial nerve, , Emerges from brainstem between pons and medulla. It controls muscles of facial, expression and taste from the anterior 2/3 of the tongue. The nerve passes into the, petrous temporal bone and into the internal auditory meatus. It then passes, through the facial canal and exits at the stylomastoid foramen. It passes through the, parotid gland and divides at this point. It does not innervate the parotid gland. Its, divisions are considered in other parts of the website. Its motor fibres innervate, orbicularis oculi to produce the efferent arm of the corneal reflex. In surgical, practice it may be injured during parotid gland surgery or invaded by malignancies, of the gland and a lower motor neurone on the ipsilateral side will result., , Vestibulo-cochlear, nerve, , Exits from the pons and then passes through the internal auditory meatus. It is, implicated in sensorineural hearing loss. Individuals with sensorineural hearing loss, will localise the sound in webers test to the normal ear. Rinnes test will be reduced, on the affected side but should still work. These two tests will distinguish, sensorineural hearing loss from conductive deafness. In the latter condition webers, test will localise to the affected ear and Rinnes test will be impaired on the affected, side. Surgical lesions affecting this nerve include CNS tumours and basal skull, fractures. It may also be damaged by the administration of ototoxic drugs (of which, gentamicin is the most commonly used in surgical practice)., , Glossopharyngeal, nerve, , Exits the pons just above the vagus. Receives sensory fibres from posterior 1/3, tongue, tonsils, pharynx and middle ear (otalgia may occur following tonsillectomy)., It receives visceral afferents from the carotid bodies. It supplies parasympathetic, fibres to the parotid gland via the otic ganglion and motor function to, stylopharyngeaus muscle. The sensory function of the nerve is tested using the gag, reflex., , Vagus nerve, , Leaves the medulla between the olivary nucleus and the inferior cerebellar, peduncle. Passes through the jugular foramen and into the carotid sheath. Details of, the functions of the vagus nerve are covered in the website under relevant organ
Page 3258 :
sub headings., , Accessory nerve, , Exists from the caudal aspect of the brainstem (multiple branches) supplies, trapezius and sternocleidomastoid muscles. The distal portion of this nerve is most, prone to injury during surgical procedures., , Hypoglossal nerve, , Emerges from the medulla at the preolivary sulcus, passes through the hypoglossal, canal. It lies on the carotid sheath and passes deep to the posterior belly of digastric, to supply muscles of the tongue (except palatoglossus). Its location near the carotid, sheath makes it vulnerable during carotid endarterectomy surgery and damage will, produce ipsilateral defect in muscle function.
Page 3259 :
Theme: Head injury- assessment, , A., B., C., D., E., F., G., H., I., J., , 3, 4, 6, 8, 10, 15, 12, 13, 5, 7, , For each of the scenarios given please determine the most likely Glasgow Coma Score. Each option, may be used once, more than once or not at all., , 8., , A 20 year old man is hit over the head with a mallet. On arrival in the accident and, emergency department he opens his eyes to pain and groans or grunts. On application of a, painful stimulus to his hands, he extends his arm at the elbow., You answered 3, The correct answer is 6, Theme from 2011 Exam, Theme from September 2012 Exam, E=2, V= 2, M=2., , 9., , A 20 year old man falls over and bangs his head whilst intoxicated. On arrival in the, emergency department he opens his eyes in response to speech, and is able to speak,, although he is disorientated. He obeys motor commands., You answered 3, The correct answer is 13, E=3, V=4, M=6., , 10., , A 20 year old man is hit over the head with an iron bar. On arrival in the emergency, department he opens his eyes in response to pain, his only verbal responses are in the form, of groans and grunts. On application of a painful stimulus to his hands, he flexes his, forearms away from the painful stimuli.
Page 3260 :
You answered 3, The correct answer is 8, E=2, V=2, M=4., Appropriate flexion to pain carries a higher score than decorticate posturing or, inappropriate flexion., Please rate this question:, , Discuss and give feedback, , Next question, , Glasgow coma scale, Modality, , Options, , Eye opening, , , , , , , Spontaneous, To speech, To pain, None, , Verbal response, , , , , , , , Orientated, Confused, Words, Sounds, None, , Motor response, , , , , , , , , Obeys commands, Localises to pain, Withdraws from pain, Abnormal flexion to pain (decorticate posture), Extending to pain, None, , Responses are taken from each category (marks in descending order) to produce an overall score., Severe brain injuries are generally associated with GCS <8.
Page 3261 :
A 33 year old lady develops a thunderclap headache and collapses. A CT scan shows that she has, developed a subarachnoid haemorrhage. She currently has no evidence of raised intracranial, pressure. Which of the following drugs should be administered?, , None, , Atenotol, , Labetolol, , Nimodipine, , Mannitol, , Theme from 2007 Exam, Nimodipine is a calcium channel blocker. It reduces cerebral vasospasm and improves outcomes. It, is administered to most cases of sub arachnoid haemorrhage., Please rate this question:, , Discuss and give feedback, , Next question, , Sub arachnoid haemorrhage, Spontaneous intracranial haemorrhage, Most commonly sub arachnoid haemorrhage. It is due to intra cranial aneurysm in 85% cases., Approximately 10% of cases will have normal angiography and the cause will remain unclear., Patients with inherited connective tissue disorders are at higher risk although most cases are, sporadic., >95% cases will have headache (often thunderclap), >15% will have coma, Investigation, CT scan for all (although as CSF blood clears the sensitivity declines)
Page 3262 :
Lumbar puncture if CT normal (very unlikely if normal), CT angiogram to look for aneurysms., Management, Supportive treatment, optimising BP (not too high if untreated aneurysm) and ventilation if needed., Nimodipine reduces cerebral vasospasm and reduces poor outcomes., Untreated patients most likely to rebleed in first 2 weeks., Patients developing hydrocephalus will need a V-P shunt (external ventricular drain acutely)., Electrolytes require careful monitoring and hyponatraemia is common., Treatment of aneurysm, >80% aneuryms arise from the anterior circulation, Craniotomy and clipping of aneurysm is standard treatment, alternatively suitable lesions may be, coiled using an endovascular approach. Where both options are suitable data suggests that, outcomes are better with coiling than surgery.
Page 3263 :
A 65 year old male with known nasopharyngeal carcinoma presents with double vision over a few, weeks. On examination he is found to have left eye proptosis and it is down and out. He reports pain, on attempting to move the eye. There is an absent corneal reflex. What is the most likely diagnosis?, , Posterior communicating artery aneurysm, , Cavernous sinus syndrome, , Optic nerve tumour, , Migraine, , Cerebral metastases, , Cavernous sinus syndrome is most commonly caused by cavernous sinus tumours. In this case, the, nasopharyngeal malignancy has locally invaded the left cavernous sinus. Diagnosis is based on, signs of pain, opthalmoplegia, proptosis, trigeminal nerve lesion (opthalmic branch) and Horner's, syndrome., Please rate this question:, , Discuss and give feedback, , Next question, , Cavernous sinus, The cavernous sinuses are paired and are situated on the body of the sphenoid bone. It runs from, the superior orbital fissure to the petrous temporal bone., Relations, Medial, , Lateral
Page 3264 :
Pituitary fossa, Sphenoid sinus, , Temporal lobe, , Contents, , Lateral wall components, , (from top to bottom:), Oculomotor nerve, Trochlear nerve, Ophthalmic nerve, Maxillary nerve, , Contents of the sinus, , (from medial to lateral:), Internal carotid artery (and sympathetic plexus), Abducens nerve, , Blood supply, Ophthalmic vein, superficial cortical veins, basilar plexus of veins posteriorly., Drains into the internal jugular vein via: the superior and inferior petrosal sinuses, , Image sourced from Wikipedia
Page 3265 :
Theme: Head injury, , A., B., C., D., E., F., G., H., , Subdural haematoma, Extradural haematoma, Subarachnoid haemorrhage, Basal skull fracture, Intracerebral haematoma, Le fort 1 fracture of maxilla, Le fort fracture 3 of maxilla, Mandibular fracture, , What is the most likely diagnosis for the scenario given? Each option may be used once, more than, once or not at all., , 13., , A 32 year old female hits her head on the steering wheel during a collision with another, car. She has periorbital swelling and a flattened appearance of the face., You answered Subdural haematoma, The correct answer is Le fort fracture 3 of maxilla, The flattened appearance of the face is a classical description of the dish/pan face, associated with Le fort fracture 2 or 3 of the maxilla., , 14., , A 29 year bouncer is hit on the side of the head with a bat. He now presents to A&E with, odd behaviour and complaining of a headache. Whilst waiting for a CT scan he becomes, drowsy and unresponsive., You answered Subdural haematoma, The correct answer is Extradural haematoma, The middle meningeal artery is prone to damage when the temporal side of the head is hit., Note that there may NOT be any initial LOC or lucid interval., , 15., , A 40 year old alcoholic presents with worsening confusion over 2 weeks. He has weakness, of the left side of the body., Subdural haematoma, Subdural haematomas can have a history over weeks/months. It is common in alcoholics, due to cerebral atrophy causing increased stretching of veins.
Page 3266 :
Please rate this question:, , Discuss and give feedback, , Next question, , Head injury, Patients who suffer head injuries should be managed according to ATLS principles and extra cranial, injuries should be managed alongside cranial trauma. Inadequate cardiac output will compromise, CNS perfusion irrespective of the nature of the cranial injury., Types of traumatic brain injury, Bleeding into the space between the dura mater and the skull. Often results from, acceleration-deceleration trauma or a blow to the side of the head. The majority, of extradural haematomas occur in the temporal region where skull fractures, cause a rupture of the middle meningeal artery., Extradural, haematoma, , Features, , , , , Raised intracranial pressure, Some patients may exhibit a lucid interval, , Bleeding into the outermost meningeal layer. Most commonly occur around the, frontal and parietal lobes. May be either acute or chronic., Subdural, haematoma, , Risk factors include old age and alcoholism., Slower onset of symptoms than a extradural haematoma., , Subarachnoid, haemorrhage, , Usually occurs spontaneously in the context of a ruptured cerebral aneurysm, but, may be seen in association with other injuries when a patient has sustained a, traumatic brain injury., , Pathophysiology, , , , , , , , Primary brain injury may be focal (contusion/ haematoma) or diffuse (diffuse axonal injury), Diffuse axonal injury occurs as a result of mechanical shearing following deceleration,, causing disruption and tearing of axons, Intra-cranial haematomas can be extradural, subdural or intracerebral, while contusions may, occur adjacent to (coup) or contralateral (contre-coup) to the side of impact, Secondary brain injury occurs when cerebral oedema, ischaemia, infection, tonsillar or, tentorial herniation exacerbates the original injury. The normal cerebral auto regulatory, processes are disrupted following trauma rendering the brain more susceptible to blood flow, changes and hypoxia, The Cushings reflex (hypertension and bradycardia) often occurs late and is usually a pre, terminal event
Page 3267 :
Management, , , , , , , , , , , Where there is life threatening rising ICP such as in extra dural haematoma and whilst, theatre is prepared or transfer arranged use of IV mannitol/ frusemide may be required., Diffuse cerebral oedema may require decompressive craniotomy, Exploratory Burr Holes have little management in modern practice except where scanning, may be unavailable and to thus facilitate creation of formal craniotomy flap, Depressed skull fractures that are open require formal surgical reduction and debridement,, closed injuries may be managed non operatively if there is minimal displacement., ICP monitoring is appropriate in those who have GCS 3-8 and normal CT scan., ICP monitoring is mandatory in those who have GCS 3-8 and abnormal CT scan., Hyponatraemia is most likely to be due to syndrome of inappropriate ADH secretion., Minimum of cerebral perfusion pressure of 70mmHg in adults., Minimum cerebral perfusion pressure of between 40 and 70 mmHg in children., , Interpretation of pupillary findings in head injuries, , Pupil size, , Light response, , Interpretation, , Unilaterally dilated, , Sluggish or fixed, , 3rd nerve compression secondary to tentorial, herniation, , Bilaterally dilated, , Sluggish or fixed, , Unilaterally dilated or, equal, , Cross reactive (Marcus Gunn), , Bilaterally constricted, , May be difficult to, assess, , Unilaterally, constricted, , Preserved, , , , , Poor CNS perfusion, Bilateral 3rd nerve palsy, , Optic nerve injury, , , , , Opiates, Pontine lesions, Metabolic encephalopathy, , Sympathetic pathway disruption, Next question
Page 3268 :
A 28 year old women collapses and is found to be deeply comatose with a GCS of 3. She is, admitted to hospital, intubated and ventilated. A CT scan shows an extensive sub arachnoid, haemorrhage. A urinary catheter is inserted. What type of urine output would be expected?, , 85ml concentrated urine per hour, , 30ml diluted urine per hour, , 60ml diluted urine per hour, , 300ml concentrated urine per hour, , 300ml diluted urine per hour, , Theme from 2011 Exam, An extensive CNS insult is likely to result in cerebral salt wasting (low Na, low plasma osmolality and, high urine output) or centrally mediated diabetes insipidus (high Na, high plasma osmolality and high, urine output). This may either be the result of hypothalamic injury directly or the result of disruption, of the hypothalamic-pituitary connections. The result is a large volume diuresis with diluted urine., Please rate this question:, , Discuss and give feedback, , Next question, , Sub arachnoid haemorrhage, Spontaneous intracranial haemorrhage, Most commonly sub arachnoid haemorrhage. It is due to intra cranial aneurysm in 85% cases., Approximately 10% of cases will have normal angiography and the cause will remain unclear., Patients with inherited connective tissue disorders are at higher risk although most cases are, sporadic., >95% cases will have headache (often thunderclap), >15% will have coma
Page 3269 :
Investigation, CT scan for all (although as CSF blood clears the sensitivity declines), Lumbar puncture if CT normal (very unlikely if normal), CT angiogram to look for aneurysms., Management, Supportive treatment, optimising BP (not too high if untreated aneurysm) and ventilation if needed., Nimodipine reduces cerebral vasospasm and reduces poor outcomes., Untreated patients most likely to rebleed in first 2 weeks., Patients developing hydrocephalus will need a V-P shunt (external ventricular drain acutely)., Electrolytes require careful monitoring and hyponatraemia is common., Treatment of aneurysm, >80% aneuryms arise from the anterior circulation, Craniotomy and clipping of aneurysm is standard treatment, alternatively suitable lesions may be, coiled using an endovascular approach. Where both options are suitable data suggests that, outcomes are better with coiling than surgery., Next question
Page 3270 :
A patient is referred due to the development of a third nerve palsy associated with a headache. On, examination meningism is present. Which one of the following diagnoses needs to be urgently, excluded?, , Weber's syndrome, , Internal carotid artery aneurysm, , Multiple sclerosis, , Posterior communicating artery aneurysm, , Anterior communicating artery aneurysm, Painful third nerve palsy = posterior communicating artery aneurysm, Given the combination of a headache and third nerve palsy it is important to exclude a posterior, communicating artery aneurysm, Please rate this question:, , Discuss and give feedback, , Next question, , Third nerve palsy, Features, , , , , eye is deviated 'down and out', ptosis, pupil may be dilated (sometimes called a 'surgical' third nerve palsy), , Causes, , , , , , , diabetes mellitus, vasculitis e.g. temporal arteritis, SLE, false localizing sign* due to uncal herniation through tentorium if raised ICP, posterior communicating artery aneurysm (pupil dilated), cavernous sinus thrombosis
Page 3271 :
, , , Weber's syndrome: ipsilateral third nerve palsy with contralateral hemiplegia -caused by, midbrain strokes, other possible causes: amyloid, multiple sclerosis, , *this term is usually associated with sixth nerve palsies but it may be used for a variety of, neurological presentations
Page 3272 :
A 23 year old man was driving a car at high speed whilst intoxicated, he was wearing a seat belt., The car collides with a brick wall at around 140km/h. When he arrives in the emergency department, he is comatose. His CT scan appears to be normal. He remains in a persistent vegetative state., What is the most likely underlying cause?, , Extradural haemorrhage, , Sub dural haemorrhage, , Sub arachnoid haemorrhage, , Intracerebral haemorrhage, , Diffuse axonal injury, , Diffuse axonal injury occurs when the head is rapidly accelerated or decelerated. There are 2, components:, 1. Multiple haemorrhages, 2. Diffuse axonal damage in the white matter, Up to 2/3 occur at the junction of grey/white matter due to the different densities of the tissue. The, changes are mainly histological and axonal damage is secondary to biochemical cascades. Often, there are no signs of a fracture or contusion., Please rate this question:, , Discuss and give feedback, , Next question, , Head injury, Patients who suffer head injuries should be managed according to ATLS principles and extra cranial, injuries should be managed alongside cranial trauma. Inadequate cardiac output will compromise, CNS perfusion irrespective of the nature of the cranial injury., Types of traumatic brain injury, , Extradural, haematoma, , Bleeding into the space between the dura mater and the skull. Often results from, acceleration-deceleration trauma or a blow to the side of the head. The majority, of extradural haematomas occur in the temporal region where skull fractures, cause a rupture of the middle meningeal artery.
Page 3273 :
Features, , , , , Raised intracranial pressure, Some patients may exhibit a lucid interval, , Bleeding into the outermost meningeal layer. Most commonly occur around the, frontal and parietal lobes. May be either acute or chronic., Subdural, haematoma, , Risk factors include old age and alcoholism., Slower onset of symptoms than a extradural haematoma., , Subarachnoid, haemorrhage, , Usually occurs spontaneously in the context of a ruptured cerebral aneurysm, but, may be seen in association with other injuries when a patient has sustained a, traumatic brain injury., , Pathophysiology, , , , , , , , Primary brain injury may be focal (contusion/ haematoma) or diffuse (diffuse axonal injury), Diffuse axonal injury occurs as a result of mechanical shearing following deceleration,, causing disruption and tearing of axons, Intra-cranial haematomas can be extradural, subdural or intracerebral, while contusions may, occur adjacent to (coup) or contralateral (contre-coup) to the side of impact, Secondary brain injury occurs when cerebral oedema, ischaemia, infection, tonsillar or, tentorial herniation exacerbates the original injury. The normal cerebral auto regulatory, processes are disrupted following trauma rendering the brain more susceptible to blood flow, changes and hypoxia, The Cushings reflex (hypertension and bradycardia) often occurs late and is usually a pre, terminal event, , Management, , , , , , , , , , , Where there is life threatening rising ICP such as in extra dural haematoma and whilst, theatre is prepared or transfer arranged use of IV mannitol/ frusemide may be required., Diffuse cerebral oedema may require decompressive craniotomy, Exploratory Burr Holes have little management in modern practice except where scanning, may be unavailable and to thus facilitate creation of formal craniotomy flap, Depressed skull fractures that are open require formal surgical reduction and debridement,, closed injuries may be managed non operatively if there is minimal displacement., ICP monitoring is appropriate in those who have GCS 3-8 and normal CT scan., ICP monitoring is mandatory in those who have GCS 3-8 and abnormal CT scan., Hyponatraemia is most likely to be due to syndrome of inappropriate ADH secretion., Minimum of cerebral perfusion pressure of 70mmHg in adults., Minimum cerebral perfusion pressure of between 40 and 70 mmHg in children.
Page 3274 :
Interpretation of pupillary findings in head injuries, , Pupil size, , Light response, , Interpretation, , Unilaterally dilated, , Sluggish or fixed, , 3rd nerve compression secondary to tentorial, herniation, , Bilaterally dilated, , Sluggish or fixed, , Unilaterally dilated or, equal, , Cross reactive (Marcus Gunn), , Bilaterally constricted, , May be difficult to, assess, , Unilaterally, constricted, , Preserved, , , , , Poor CNS perfusion, Bilateral 3rd nerve palsy, , Optic nerve injury, , , , , Opiates, Pontine lesions, Metabolic encephalopathy, , Sympathetic pathway disruption, Next question
Page 3275 :
Theme: Visual defects, , A., B., C., D., E., F., G., H., , Right homonymous hemianopia, Left homonymous hemianopia, Right superior quadranopia, Left superior quadranopia, Right inferior quadranopia, Left inferior quadranopia, Upper bitemporal hemianopia, Lower bitemporal hemianopia, , What is the most likely visual field defect for the scenario given? Each option may be used once,, more than once or not at all., , 19., , A 42 year old woman is admitted to the vascular ward for an endarterectomy. Her CT, report confirms a left temporal lobe infarct., You answered Right homonymous hemianopia, The correct answer is Right superior quadranopia, Temporal lesions cause a contralateral superior quadranopia. Think temporal area is at the, top of the head i.e. superior quadranopia., , 20., , A 22 year old man is referred to urology with possible urinary retention. He is passing, huge amounts of urine. Post void bladder ultrasound is normal., You answered Right homonymous hemianopia, The correct answer is Lower bitemporal hemianopia, Theme from January 2012 exam, This patient has diabetes insipidus due to a craniopharyngioma. Lesions at the optic, chiasm classically produce a bitemporal hemianopia, however note lesions that spread up, from below ie pituitary tumours, the defect is worse in the upper fields and if a lesion, spreads down from above ie craniopharyngiomas, the visual defect is worse in the lower, quadrants. Therefore this patient is likely to have a lower bitemporal hemianopia., , 21., , A 53 year old man is admitted to the vascular ward for a carotid endarterectomy. His CT, head report confirms a left parietal lobe infarct., You answered Right homonymous hemianopia
Page 3276 :
The correct answer is Right inferior quadranopia, Parietal lesions cause a contralateral inferior quadranopia., Superior quadranopia = temporal lobe lesion, Inferior quadranopia = parietal lobe lesion, Please rate this question:, , Discuss and give feedback, , Next question, , Visual field defects, Theme from January 2012 exam, Theme from April 2012 exam, , , , , , left homonymous hemianopia means visual field defect to the left, i.e. Lesion of right optic, tract, homonymous quadrantanopias: PITS (Parietal-Inferior, Temporal-Superior), incongruous defects = optic tract lesion; congruous defects = optic radiation lesion or, occipital cortex, , Homonymous hemianopia, , , , , Incongruous defects: lesion of optic tract, Congruous defects: lesion of optic radiation or occipital cortex, Macula sparing: lesion of occipital cortex, , Homonymous quadrantanopias, , , , , Superior: lesion of temporal lobe, Inferior: lesion of parietal lobe, Mnemonic = PITS (Parietal-Inferior, Temporal-Superior), , Bitemporal hemianopia, , , , Lesion of optic chiasm, Upper quadrant defect > lower quadrant defect = inferior chiasmal compression, commonly a, pituitary tumour
Page 3277 :
, , Lower quadrant defect > upper quadrant defect = superior chiasmal compression, commonly, a craniopharyngioma
Page 3278 :
A middle aged lady is brought to the clinic by her husband who has noted a change in her, appearance. She finds removal of rings difficult, her shoe size has changed and photographs show a, marked change in her appearance. Which of the following is most likely to be identified on, neurological examination?, , Bi nasal hemianopia, , Bi temporal hemianopia, , Inferior quadrantanopia, , Homonymous hemianopia, , Unilateral loss of vision, , Theme from 2011 Exam, The patient is most likely to have developed acromegaly. Since a pituitary lesion is likely to be, present; compression of the optic chiasm may occur., Please rate this question:, , Discuss and give feedback, , Next question, , Visual field defects, Theme from January 2012 exam, Theme from April 2012 exam, , , , , , left homonymous hemianopia means visual field defect to the left, i.e. Lesion of right optic, tract, homonymous quadrantanopias: PITS (Parietal-Inferior, Temporal-Superior), incongruous defects = optic tract lesion; congruous defects = optic radiation lesion or, occipital cortex, , Homonymous hemianopia, , , , Incongruous defects: lesion of optic tract, Congruous defects: lesion of optic radiation or occipital cortex
Page 3280 :
Theme: Intra cranial haemorrhage, , A., B., C., D., E., F., , Acute sub dural haematoma, Chronic sub dural haematoma, Acute extradural haematoma, Chronic extradural haematoma, Intraventricular haemorrhage, Sub arachnoid haemorrhage, , Please select the most likely intra cranial bleeding event to account for the scenario described. Each, option may be used once, more than once or not at all., , 23., , A 28 year old man is playing tennis when he suddenly collapses and has a GCS of 4 when, examined., You answered Acute sub dural haematoma, The correct answer is Sub arachnoid haemorrhage, Theme from April 2012 Exam, A sudden collapse and loss of consciousness is most likely to be due to a sub arachnoid, haemorrhage. The other potential causes in the list usually occur as a sequel to a traumatic, event, which has not occurred here., , 24., , A 2 day old premature neonate is born by emergency cesarean section for maternal illness., The baby is noted to become floppy and unresponsive., You answered Acute sub dural haematoma, The correct answer is Intraventricular haemorrhage, Neonatal deterioration in premature babies is not infrequently due to intra ventricular, haemorrhage. In extreme prematurity the prognosis can be very poor., , 25., , A 78 year old man is brought to the emergency department by the police. He is found, wandering around the town centre and is confused. His family report that he is usually well, apart from a simple mechanical fall 3 weeks previously from which he sustained no, obvious injuries., You answered Acute sub dural haematoma, The correct answer is Chronic sub dural haematoma
Page 3281 :
The injuries that are responsible for chronic sub dural haematomas are usually fairly trivial, and forgotten by the patient and their families. The onset of symptoms can be insidious, with vague symptomatology and confusion predominating., Please rate this question:, , Discuss and give feedback, , Next question, , Intra cranial haemorrhage, Extradural, haematoma, , Bleeding into the space between the dura mater and the skull. Often results, from acceleration-deceleration trauma or a blow to the side of the head. The, majority of extradural haematomas occur in the temporal region where skull, fractures cause a rupture of the middle meningeal artery., Features, , , , Subdural, haematoma, , Raised intracranial pressure, Some patients may exhibit a lucid interval, , Bleeding into the outermost meningeal layer. Most commonly occur around, the frontal and parietal lobes. May be either acute or chronic., Risk factors include old age and alcoholism., Slower onset of symptoms than a extradural haematoma., , Intracerebral, haematoma, , Usually hyperdense lesions on CT scanning. Arise in areas of traumatic, contusion with fuse to become a haematoma. Areas of clot and fresh blood, may co-exist on the same CT scan (Swirl sign). Large haematomas and, those associated with mass effect should be evacuated., , Subarachnoid, haemorrhage, , Usually occurs spontaneously in the context of a ruptured cerebral, aneurysm but may be seen in association with other injuries when a patient, has sustained a traumatic brain injury, , Intraventricular, haemorrhage, , Haemorrhage that occurs into the ventricular system of the brain. It is, relatively rare in adult surgical practice and when it does occur, it is, typically associated with severe head injuries. In premature neonates it may, occur spontaneously. The blood may clot and occlude CSF flow,, hydrocephalus may result.
Page 3282 :
In neonatal practice the vast majority of IVH occur in the first 72 hours, after birth, the aetiology is not well understood and it is suggested to occur, as a result of birth trauma combined with cellular hypoxia, together with the, delicate neonatal CNS.
Page 3283 :
Theme: Management of head injuries, , A., B., C., D., E., F., G., , Intravenous mannitol, Parietotemporal craniotomy, Burr Hole decompression, Posterior fossa craniotomy, Insertion of intracranial bolt monitor, Discharge, Intravenous frusemide, , What is the best immediate management plan for the injury described? Each option may be used, once, more than once or not at all., , 26., , A 25 year old cyclist is hit by a bus traveling at 30mph. He is not wearing a helmet. He, arrives with a GCS of 3/15 and is intubated. A CT scan shows evidence of cerebral, contusion but no localising clinical signs are present, You answered Intravenous mannitol, The correct answer is Insertion of intracranial bolt monitor, This patient may well develop raised ICP over the next few days and Intracranial pressure, monitoring will help with management., , 27., , A 32 year old rugby player is crushed in a scrum. He is briefly concussed but then regains, consciousness. He then collapses and is brought to A+E. His GCS on arrival is 6/15 and, his left pupil is dilated., You answered Intravenous mannitol, The correct answer is Parietotemporal craniotomy, This man needs urgent decompression and extradural haematoma is the most likely event,, from a lacerated middle meningeal artery. The debate as to whether Burr Holes or, craniotomy is the best option continues. Most neurosurgeons would perform a craniotomy., However, rural units and those units without neurosurgical kit facing this emergency may, resort to Burr Holes., , 28., , A 30 year old women is injured in a skiing accident. She suffers a blow to the occiput and, is concussed for 5 minutes. On arrival in A+E she is confused with GCS 10/15. A CT scan, shows no evidence of acute bleed or fracture but some evidence of oedema with the, beginnings of mass effect
Page 3284 :
Intravenous mannitol, This women has raised ICP and mannitol will help reduce this in the acute phase., Please rate this question:, , Discuss and give feedback, , Next question, , Head injury management- NICE Guidelines, Summary of guidelines, , , , , , , All patients should be assessed within 15 minutes on arrival to A&E, Document all 3 components of the GCS, If GCS <8 or = to 8, consider stabilising the airway, Treat pain with low dose IV opiates (if safe), Full spine immobilisation until assessment if:, , - GCS < 15, - neck pain/tenderness, - paraesthesia extremities, - focal neurological deficit, - suspected c-spine injury, If a c-spine injury is suspected a 3 view c-spine x-ray is indicated. CT c-spine is preferred if:, - Intubated, - GCS <13, - Normal x-ray but continued concerns regarding c-spine injury, - Any focal neurology, - A CT head scan is being performed, - Initial plain films are abnormal, Immediate CT head (within 1 hour) if:, , , , , , , , , , GCS < 13 on admission, GCS < 15 2 hours after admission, Suspected open or depressed skull fracture, Suspected skull base fracture (panda eyes, Battle's sign, CSF from nose/ear, bleeding ear), Focal neurology, Vomiting > 1 episode, Post traumatic seizure, Coagulopathy
Page 3285 :
Contact neurosurgeon if:, , , , , , , , , Persistent GCS < 8 or = 8, Unexplained confusion > 4h, Reduced GCS after admission, Progressive neurological signs, Incomplete recovery post seizure, Penetrating injury, Cerebrospinal fluid leak, , Observations, , , 1/2 hourly GCS until 15
Page 3287 :
Theme: Head injury, , A., B., C., D., E., F., G., , Acute sub dural haematoma, Intra cerebral haematoma, Extra dural haematoma, Chronic sub dural haematoma, Basal skull fracture, Subarachnoid haemorrhage, Diffuse axonal injury, , What is the most likely diagnosis for the scenario given? Each option may be used once, more than, once or not at all., , 30., , A 18 year old boy is involved in a fall from a balcony whilst intoxicated. He has bruising, over the mastoid area and is unconscious., You answered Acute sub dural haematoma, The correct answer is Basal skull fracture, Bruising over the mastoid process of the temporal bone is battle's sign caused by a basal, skull fracture., , 31., , A 18 year old boy falls off a balcony and hits the right side of the head. He is admitted to, the emergency department and has a GCS of 8. He is admitted for observation, and over, the following twelve hours develops an increasing headache and confusion. A CT scan, shows a crescent shaped collection of fluid between the brain and the dura with associated, midline shift., Acute sub dural haematoma, Sub dural haematomas are the commonest intracranial mass lesions resulting from trauma., They are classified as acute, sub acute or chronic according to tempo of onset. Acute sub, dural haematomas will present within 72 hours of the original injury and have hyperdense,, crescent shaped appearances on CT scanning., , 32., , A baby is brought to casualty unconscious and in a vegetative state. She has cigarette, burns on her legs., You answered Acute sub dural haematoma, The correct answer is Diffuse axonal injury
Page 3288 :
The baby is likely to be a victim of shaken baby syndrome. This may result in diffuse, axonal injury causing extensive lesions in the white matter., Please rate this question:, , Discuss and give feedback, , Next question, , Head injury, Patients who suffer head injuries should be managed according to ATLS principles and extra cranial, injuries should be managed alongside cranial trauma. Inadequate cardiac output will compromise, CNS perfusion irrespective of the nature of the cranial injury., Types of traumatic brain injury, Bleeding into the space between the dura mater and the skull. Often results from, acceleration-deceleration trauma or a blow to the side of the head. The majority, of extradural haematomas occur in the temporal region where skull fractures, cause a rupture of the middle meningeal artery., Extradural, haematoma, , Features, , , , , Raised intracranial pressure, Some patients may exhibit a lucid interval, , Bleeding into the outermost meningeal layer. Most commonly occur around the, frontal and parietal lobes. May be either acute or chronic., Subdural, haematoma, , Risk factors include old age and alcoholism., Slower onset of symptoms than a extradural haematoma., , Subarachnoid, haemorrhage, , Usually occurs spontaneously in the context of a ruptured cerebral aneurysm, but, may be seen in association with other injuries when a patient has sustained a, traumatic brain injury., , Pathophysiology, , , , , Primary brain injury may be focal (contusion/ haematoma) or diffuse (diffuse axonal injury), Diffuse axonal injury occurs as a result of mechanical shearing following deceleration,, causing disruption and tearing of axons, Intra-cranial haematomas can be extradural, subdural or intracerebral, while contusions may, occur adjacent to (coup) or contralateral (contre-coup) to the side of impact
Page 3289 :
, , , , Secondary brain injury occurs when cerebral oedema, ischaemia, infection, tonsillar or, tentorial herniation exacerbates the original injury. The normal cerebral auto regulatory, processes are disrupted following trauma rendering the brain more susceptible to blood flow, changes and hypoxia, The Cushings reflex (hypertension and bradycardia) often occurs late and is usually a pre, terminal event, , Management, , , , , , , , , , , Where there is life threatening rising ICP such as in extra dural haematoma and whilst, theatre is prepared or transfer arranged use of IV mannitol/ frusemide may be required., Diffuse cerebral oedema may require decompressive craniotomy, Exploratory Burr Holes have little management in modern practice except where scanning, may be unavailable and to thus facilitate creation of formal craniotomy flap, Depressed skull fractures that are open require formal surgical reduction and debridement,, closed injuries may be managed non operatively if there is minimal displacement., ICP monitoring is appropriate in those who have GCS 3-8 and normal CT scan., ICP monitoring is mandatory in those who have GCS 3-8 and abnormal CT scan., Hyponatraemia is most likely to be due to syndrome of inappropriate ADH secretion., Minimum of cerebral perfusion pressure of 70mmHg in adults., Minimum cerebral perfusion pressure of between 40 and 70 mmHg in children., , Interpretation of pupillary findings in head injuries, , Pupil size, , Light response, , Interpretation, , Unilaterally dilated, , Sluggish or fixed, , 3rd nerve compression secondary to tentorial, herniation, , Bilaterally dilated, , Sluggish or fixed, , Unilaterally dilated or, equal, , Cross reactive (Marcus Gunn), , Bilaterally constricted, , May be difficult to, assess, , Unilaterally, constricted, , Preserved, , , , , Poor CNS perfusion, Bilateral 3rd nerve palsy, , Optic nerve injury, , , , , Opiates, Pontine lesions, Metabolic encephalopathy, , Sympathetic pathway disruption, Next question
Page 3290 :
A 28 year old man falls and hits his head against a wall. There is a brief loss of consciousness., When assessed in accident and emergency he is alert and orientated with a GCS of 15, imaging, shows no fracture of the skull. What is his risk of having an intracranial haematoma requiring, removal?, , 1 in 6000, , 1 in 40, , 1 in 4, , 1 in 50,000, , 1 in 120, , Please rate this question:, , Discuss and give feedback, , Next question, , Head injury and haematoma, Risk of haematoma (requiring removal) in adults attending accident and emergency units following, head injury., , Injury, , Conscious level, , Risk of haematoma requiring removal, , Concussion, no skull fracture, , Orientated, , 1 in 6000, , Concussion, no skull fracture, , Not orientated, , 1 in 120
Page 3291 :
Skull fracture, , Orientated, , 1 in 32, , Skull fracture, , Not orientated, , 1 in 4, Next question, , The term signature fracture is synonymous with which of the following injuries?
Page 3292 :
Depressed skull fracture, , Le Fort II fracture, , Orbital blow out, , Oblique fracture of the tibia, , Supracondylar fracture, , Signature fractures are synonymous with depressed skull fractures, they are usually low velocity, injuries where the fracture impression resembles the injurious source., Please rate this question:, , Discuss and give feedback, , Next question, , Depressed skull fracture, , , , , , , , , Depressed skull fractures are also referred to as signature fractures., Results from the focal impact of a moving object on the cranial vault., High velocity objects will not only disrupt bone, but may also drive the fracture fragments into, the brain., Blunt objects moving at low velocity may produce a defect in the skull that is of similar, dimensions to the object (c.f. signature), Injuries may affect the outer table alone or extend to involve the inner table., Open fractures and those associated with intracranial haematomas may require surgery,, uncomplicated fractures without significant cosmetic deformities may be managed, conservatively., CT scanning is the initial imaging modality of choice., , Which of the following is not a form of primary brain injury?
Page 3293 :
Sub dural haemorrhage after being hit in the head with a hammer, , Meningitis resulting from infected CSF rhinorrhoea after a basal skull fracture, , A truck driver is involved in a road traffic accident and suffers an axonal stretch injury, , A man is hit with a baseball bat and suffers a cerebral contusion, , A man suffers an intraparenchymal haemorrhage after being hit in head during a car crash, , Primary brain damage occurs at the point of injury. It includes contusions and diffuse axonal injury., Non reversible., Secondary brain damage occurs after the injury. Complications include:, 1. Haemorrhage, 2. Meningitis, 3. Herniation, 4. Hypoxia, 5. Oedema, 6. Arterial damage: internal carotid, vertebral artery common, Please rate this question:, , Discuss and give feedback, , Head injury, Patients who suffer head injuries should be managed according to ATLS principles and extra cranial, injuries should be managed alongside cranial trauma. Inadequate cardiac output will compromise, CNS perfusion irrespective of the nature of the cranial injury., Types of traumatic brain injury, Bleeding into the space between the dura mater and the skull. Often results from, acceleration-deceleration trauma or a blow to the side of the head. The majority, of extradural haematomas occur in the temporal region where skull fractures, cause a rupture of the middle meningeal artery., Extradural, haematoma, , Features, , , , , Raised intracranial pressure, Some patients may exhibit a lucid interval
Page 3294 :
Bleeding into the outermost meningeal layer. Most commonly occur around the, frontal and parietal lobes. May be either acute or chronic., Subdural, haematoma, , Risk factors include old age and alcoholism., Slower onset of symptoms than a extradural haematoma., , Subarachnoid, haemorrhage, , Usually occurs spontaneously in the context of a ruptured cerebral aneurysm, but, may be seen in association with other injuries when a patient has sustained a, traumatic brain injury., , Pathophysiology, , , , , , , , Primary brain injury may be focal (contusion/ haematoma) or diffuse (diffuse axonal injury), Diffuse axonal injury occurs as a result of mechanical shearing following deceleration,, causing disruption and tearing of axons, Intra-cranial haematomas can be extradural, subdural or intracerebral, while contusions may, occur adjacent to (coup) or contralateral (contre-coup) to the side of impact, Secondary brain injury occurs when cerebral oedema, ischaemia, infection, tonsillar or, tentorial herniation exacerbates the original injury. The normal cerebral auto regulatory, processes are disrupted following trauma rendering the brain more susceptible to blood flow, changes and hypoxia, The Cushings reflex (hypertension and bradycardia) often occurs late and is usually a pre, terminal event, , Management, , , , , , , , , , , Where there is life threatening rising ICP such as in extra dural haematoma and whilst, theatre is prepared or transfer arranged use of IV mannitol/ frusemide may be required., Diffuse cerebral oedema may require decompressive craniotomy, Exploratory Burr Holes have little management in modern practice except where scanning, may be unavailable and to thus facilitate creation of formal craniotomy flap, Depressed skull fractures that are open require formal surgical reduction and debridement,, closed injuries may be managed non operatively if there is minimal displacement., ICP monitoring is appropriate in those who have GCS 3-8 and normal CT scan., ICP monitoring is mandatory in those who have GCS 3-8 and abnormal CT scan., Hyponatraemia is most likely to be due to syndrome of inappropriate ADH secretion., Minimum of cerebral perfusion pressure of 70mmHg in adults., Minimum cerebral perfusion pressure of between 40 and 70 mmHg in children., , Interpretation of pupillary findings in head injuries, , Pupil size, , Light response, , Interpretation
Page 3295 :
Pupil size, , Light response, , Interpretation, , Unilaterally dilated, , Sluggish or fixed, , 3rd nerve compression secondary to tentorial, herniation, , Bilaterally dilated, , Sluggish or fixed, , Unilaterally dilated or, equal, , Cross reactive (Marcus Gunn), , Bilaterally constricted, , May be difficult to, assess, , Unilaterally, constricted, , Preserved, , , , , Poor CNS perfusion, Bilateral 3rd nerve palsy, , Optic nerve injury, , , , , Opiates, Pontine lesions, Metabolic encephalopathy, , Sympathetic pathway disruption
Page 3296 :
A 25 year old man is shot in the abdomen and is transferred to the operating theatre following arrival, in the emergency department, as he is unstable and a FAST scan is positive. At operation there is, an extensive laceration to the right lobe of the liver and involvement of the IVC. There is massive, haemorrhage. What is the most appropriate approach to blood component therapy?, , Use Factor VIII concentrates early, , Avoid use of "o" negative blood, , Transfuse packed cells, FFP and platelets in fixed ratios of 1:1:1, , Transfuse packed cells and FFP in a fixed ratio of 4:1, , Perform goal directed transfusion based on the Hb, PT and TEG studies, , There is strong evidence to support the use of haemostatic transfusion in the setting of major, haemorrhage due to trauma. This advocates the use of 1:1:1 ratios., Please rate this question:, , Discuss and give feedback, , Next question, , Transfusions in major trauma, Uncontrolled haemorrhage accounts for up to 39% of all trauma related death. In the UK, approximately 2% of all trauma patients will need massive transfusion.Massive transfusion is defined, as the replacement of a patient's total blood volume in less than 24 hours, or as the acute, administration of more than half the patient's estimated blood volume per hour. In haemorrhaging, patients following trauma there is evidence to support the initial administration of tranexamic acid, (CRASH study). During acute bleeding the practice of haemostatic resuscitation has been shown to, reduce mortality rates. The principle of haemostatic resuscitation is that blood components are, transfused in fixed ratios. For example; packed red cells, FFP and platelets are administered in a, ratio of 1:1:1., The typical therapeutic end points include:, , , , , , , Hb: 8-10 g/dl, Platelets > 100, PT and APTT (INR)< 1.5, Fibrinogen > 1.0 g/l, Ca2+ > 1 mmol/l
Page 3297 :
, , , , pH: 7.35-7.45, BE: +/- 2, ToC > 36 °C, Next question
Page 3298 :
A 76 year old woman with a body weight of 50 kg is undergoing an excision of a lipoma from her, forehead. It is the first time the senior house officer has performed the procedure. He administers, 30ml of 2% lignocaine to the area. The procedure is complicated by bleeding and the patient, experiences discomfort, a further 10ml of the same anaesthetic formulation is then administered., Over the following 5 minutes the patient complains of tinnitus and becomes drowsy. Which of the, drugs listed below should be administered?, , Temazepam, , Lorazepam, , Naloxone, , Intralipid 20%, , Sodium bicarbonate 20%, Local anaesthetic toxicity treatment = Intralipid, Intralipid is indicated for the treatment of local anaesthetic toxicity. In this case the safe dose of local, anaesthetic has been exceeded and is thus this lady's symptoms are likely to represent toxicity., Please rate this question:, , Discuss and give feedback, , Next question, , Local anaesthetic toxicity, Toxicity results from either accidental intravascular injection (rapid onset of symptoms-usually, correct dose), or from excessive dosage (slower onset). Local anaesthetic agents not only exert a, membrane stabilising effect on peripheral nerves but will also act on excitable membranes within the, CNS and Heart. The sensory neurones in the CNS are suppressed before the motor ones. As a, result the early symptoms will typically be those of circumoral paraesthesia and tinnitus, followed by, falling GCS and eventually coma., Management of toxicity, , , , , , Stop injecting the anaesthetic agent, High flow 100% oxygen via face mask, Cardiovascular monitoring, Administer lipid emulsion (Intralipid 20%) at 1.5ml/Kg over 1 minute as a bolus
Page 3299 :
, , , Consider lipid emulsion infusion, at 0.25ml/ Kg/ minute, If toxicity due to prilocaine then administer methylene blue, , Safe doses, 10ml of lignocaine 1% contains 100mg of drug, this would constitute 70% of the maximum safe dose, in a 50 kg patient. Up to 7mg / kg can be administered if adrenaline is added to the solution., Doses of local anaesthetics, , Agent, , Dose plain, , Dose with adrenaline, , Lignocaine, , 3mg/Kg, , 7mg/Kg, , Bupivicane, , 2mg/Kg, , 2mg/Kg, , Prilocaine, , 6mg/Kg, , 9mg/Kg, , These are a guide only as actual doses depend on site of administration, tissue vascularity and comorbidities., Next question
Page 3300 :
A 27 year old man is involved in a road traffic accident. He is seen in the emergency department, with chest pain. Clinical examination is essentially unremarkable and he is discharged. He, subsequently is found dead at home. What is the most likely underlying injury?, , Tracheobronchial tree injury, , Traumatic aortic disruption, , Cardiac laceration, , Diaphragmatic rupture, , Rupture of the oesophagus, , Theme from January 2013 Exam, Aortic injuries that do not die at the scene may have a contained haematoma. Clinical signs are, subtle and the diagnosis may not be apparent on clinical examination. Without prompt treatment the, haematoma usually bursts and the patient dies., Please rate this question:, , Discuss and give feedback, , Next question, , Thoracic aorta rupture, , , , , Mechanism of injury: Decelerating force i.e. RTA, fall from a great height, Most people die at scene, Survivors may have an incomplete laceration at the ligamentum arteriosum of the aorta., , Clinical features, , , , Contained haematoma: persistent hypotension, Detected mainly by history, CXR changes, , CXR changes, , , Widened mediastinum
Page 3301 :
, , , , , , Trachea/Oesophagus to right, Depression of left main stem bronchus, Widened paratracheal stripe/paraspinal interfaces, Space between aorta and pulmonary artery obliterated, Rib fracture/left haemothorax, , Diagnosis, Angiography, usually CT aortogram., Treatment, Repair or replacement. Ideally they should undergo endovascular repair., Next question
Page 3302 :
A patient is brought to the emergency department following a motor vehicle accident. He is, unconscious and has a deep scalp laceration. His heart rate is 120/min, blood pressure is 80/40, mmHg, and respiratory rate is 35/min. Despite rapid administration of 2 litres of Hartmans solution,, the patient's vital signs do not change significantly. The injury likely to explain this patient's, hypotension is:, , Epidural haematoma, , Sub dural haematoma, , Intra parenchymal brain haemorrhage, , Base of skull fracture, , None of the above, Raised intracranial pressure (Cushing response), , , , , Hypertension, Bradycardia, Respiratory depression, , In the patient described, hypotension and tachycardia should not be uncritically attributed to the, head injury, since these findings in the setting of blunt trauma are suggestive of serious thoracic,, abdominal, or pelvic hemorrhage. When cardiovascular collapse occurs as a result of rising, intracranial pressure, it is generally accompanied by hypertension, bradycardia, and respiratory, depression., Please rate this question:, , Discuss and give feedback, , Next question, , Head injury, Patients who suffer head injuries should be managed according to ATLS principles and extra cranial, injuries should be managed alongside cranial trauma. Inadequate cardiac output will compromise, CNS perfusion irrespective of the nature of the cranial injury., Types of traumatic brain injury, Extradural, , Bleeding into the space between the dura mater and the skull. Often results from
Page 3303 :
haematoma, , acceleration-deceleration trauma or a blow to the side of the head. The majority, of extradural haematomas occur in the temporal region where skull fractures, cause a rupture of the middle meningeal artery., Features, , , , , Raised intracranial pressure, Some patients may exhibit a lucid interval, , Bleeding into the outermost meningeal layer. Most commonly occur around the, frontal and parietal lobes. May be either acute or chronic., Subdural, haematoma, , Risk factors include old age and alcoholism., Slower onset of symptoms than a extradural haematoma., , Subarachnoid, haemorrhage, , Usually occurs spontaneously in the context of a ruptured cerebral aneurysm, but, may be seen in association with other injuries when a patient has sustained a, traumatic brain injury., , Pathophysiology, , , , , , , , Primary brain injury may be focal (contusion/ haematoma) or diffuse (diffuse axonal injury), Diffuse axonal injury occurs as a result of mechanical shearing following deceleration,, causing disruption and tearing of axons, Intra-cranial haematomas can be extradural, subdural or intracerebral, while contusions may, occur adjacent to (coup) or contralateral (contre-coup) to the side of impact, Secondary brain injury occurs when cerebral oedema, ischaemia, infection, tonsillar or, tentorial herniation exacerbates the original injury. The normal cerebral auto regulatory, processes are disrupted following trauma rendering the brain more susceptible to blood flow, changes and hypoxia, The Cushings reflex (hypertension and bradycardia) often occurs late and is usually a pre, terminal event, , Management, , , , , , , , , Where there is life threatening rising ICP such as in extra dural haematoma and whilst, theatre is prepared or transfer arranged use of IV mannitol/ frusemide may be required., Diffuse cerebral oedema may require decompressive craniotomy, Exploratory Burr Holes have little management in modern practice except where scanning, may be unavailable and to thus facilitate creation of formal craniotomy flap, Depressed skull fractures that are open require formal surgical reduction and debridement,, closed injuries may be managed non operatively if there is minimal displacement., ICP monitoring is appropriate in those who have GCS 3-8 and normal CT scan., ICP monitoring is mandatory in those who have GCS 3-8 and abnormal CT scan., Hyponatraemia is most likely to be due to syndrome of inappropriate ADH secretion.
Page 3304 :
, , , Minimum of cerebral perfusion pressure of 70mmHg in adults., Minimum cerebral perfusion pressure of between 40 and 70 mmHg in children., , Interpretation of pupillary findings in head injuries, , Pupil size, , Light response, , Interpretation, , Unilaterally dilated, , Sluggish or fixed, , 3rd nerve compression secondary to tentorial, herniation, , Bilaterally dilated, , Sluggish or fixed, , Unilaterally dilated or, equal, , Cross reactive (Marcus Gunn), , Bilaterally constricted, , May be difficult to, assess, , Unilaterally, constricted, , Preserved, , , , , Poor CNS perfusion, Bilateral 3rd nerve palsy, , Optic nerve injury, , , , , Opiates, Pontine lesions, Metabolic encephalopathy, , Sympathetic pathway disruption, Next question
Page 3306 :
Addisonian crisis, Features of an addisonian crisis:, , , , , Hyponatraemia, Hyperkalaemia, Hypoglycaemia, , This man is on steroids for polymyalgia rheumatica. Surgery can precipitate acute adrenal, deficiency. The diagnosis is further confirmed by the blood results of hyponatraemia, hyperkalaemia, and hypoglycaemia. This patient urgently needs hydrocortisone., Please rate this question:, , Discuss and give feedback, , Next question, , Addisonian crisis, Causes, , , , , Sepsis or surgery causing an acute exacerbation of chronic insufficiency (Addison's,, Hypopituitarism), Adrenal haemorrhage eg Waterhouse-Friderichsen syndrome (fulminant meningococcemia), Steroid withdrawal, , Management, , , , , , Hydrocortisone 100 mg im or iv, 1 litre normal saline infused over 30-60 mins or with dextrose if hypoglycaemic, Continue hydrocortisone 6 hourly until the patient is stable. No fludrocortisone is required, because high cortisol exerts weak mineralocorticoid action, Oral replacement may begin after 24 hours and be reduced to maintenance over 3-4 days, Next question
Page 3307 :
A 32 year old man is involved in a motorcycle accident and sustains a closed unstable spiral tibial, fracture. This is managed with an intramedullary nail. On return to the ward he is noted to have, increasing pain in the limb and on examination the limb is swollen and tender with pain on passive, stretching of the toes. The most likely diagnosis is:, , Tibial nerve neuropraxia, , Displaced tibial nail, , Compartment syndrome, , Deep vein thrombosis, , Sciatic nerve injury, , Theme from September 2014 Exam, Severe pain in a limb should raise suspicions of compartment syndrome especially in tibial fractures, following fixation with intra medullary devices., Please rate this question:, , Discuss and give feedback, , Next question, , Compartment syndrome, , , , This is a particular complication that may occur following fractures (or following ischaemia reperfusion injury in vascular patients). It is characterised by raised pressure within a closed, anatomical space., The raised pressure within the compartment will eventually compromise tissue perfusion, resulting in necrosis. The two main fractures carrying this complication include supracondylar, fractures and tibial shaft injuries., , Symptoms and signs, , , , , , , Pain, especially on movement (even passive), Parasthesiae, Pallor may be present, Arterial pulsation may still be felt as the necrosis occurs as a result of microvascular, compromise, Paralysis of the muscle group may occur
Page 3308 :
Diagnosis, , , Is made by measurement of intracompartmental pressure measurements. Pressures in, excess of 20mmHg are abnormal and >40mmHg is diagnostic., , Treatment, , , , , , , This is essentially prompt and extensive fasciotomies, In the lower limb the deep muscles may be inadequately decompressed by the, inexperienced operator when smaller incisions are performed, Myoglobinuria may occur following fasciotomy and result in renal failure and for this reason, these patients require aggressive IV fluids, Where muscle groups are frankly necrotic at fasciotomy they should be debrided and, amputation may have to be considered, Death of muscle groups may occur within 4-6 hours, Next question
Page 3309 :
A 28 year old man is involved in a road traffic accident and sustains a flail chest injury. On arrival in, the emergency department he is hypotensive. On examination; he has an elevated jugular venous, pulse and auscultation of the heart reveals quiet heard sounds. What is the most likely diagnosis?, , Pneumothorax, , Myocardial contusion, , Cardiac tamponade, , Haemothorax, , Ventricular septal defect, , Theme from 2010 exam, The presence of a cardiac tamponade is suggested by Becks Triad:, , , , , Hypotension, Muffled heart sounds, Raised JVP, , Please rate this question:, , Discuss and give feedback, , Next question, , Thoracic trauma, Types of thoracic trauma, , Tension, pneumothorax, , , , , , , Flail chest, , , , Often laceration to lung parenchyma with flap, Pressure develops in thorax, Most common cause is mechanical ventilation in patient with, pleural injury, Symptoms overlap with cardiac tamponade, hyper-resonant, percussion note is more likely in tension pnemothorax, Chest wall disconnects from thoracic cage
Page 3310 :
, , , , , Multiple rib fractures (at least two fractures per rib in at least two, ribs), Associated with pulmonary contusion, Abnormal chest motion, Avoid over hydration and fluid overload, , Pneumothorax, , , , , , Most common cause is lung laceration with air leakage, Most traumatic pneumothoraces should have a chest drain, Patients with traumatic pneumothorax should never be, mechanically ventilated until a chest drain is inserted, , Haemothorax, , , , Most commonly due to laceration of lung, intercostal vessel or, internal mammary artery, Haemothoraces large enough to appear on CXR are treated with, large bore chest drain, Surgical exploration is warranted if >1500ml blood drained, immediately, , , , , , , , , Beck's triad: elevated venous pressure, reduced arterial pressure,, reduced heart sounds, Pulsus paradoxus, May occur with as little as 100ml blood, , Pulmonary contusion, , , , , , Most common potentially lethal chest injury, Arterial blood gases and pulse oximetry important, Early intubation within an hour if significant hypoxia, , Blunt cardiac injury, , , , , , Usually occurs secondary to chest wall injury, ECG may show features of myocardial infarction, Sequelae: hypotension, arrhythmias, cardiac wall motion, abnormalities, , Aorta disruption, , , , , , Deceleration injuries, Contained haematoma, Widened mediastinum, , Diaphragm, disruption, , , , Most due to motor vehicle accidents and blunt trauma causing, large radial tears (laceration injuries result in small tears), More common on left side, , Cardiac tamponade, ,
Page 3311 :
Mediastinal, traversing wounds, , , , Insert gastric tube, may pass into intrathoracic stomach, , , , Entrance wound in one hemithorax and exit wound/foreign body, in opposite hemithorax, Mediastinal haematoma or pleural cap suggests great vessel, injury, Mortality is 20%, , , , , References, ATLS Manual 8th Edition, Next question
Page 3312 :
A 31 year old lady is struck by a car and is 32 weeks pregnant. On arrival in the emergency, department she has a systolic blood pressure of 105mmHg and a pulse rate of 126 beats per, minute. Abdominal examination demonstrates a diffusely tender abdomen and some left sided flank, bruising. A FAST scan is normal. What is the most appropriate course of action?, , Arrange a departmental abdominal USS scan, , Arrange an urgent abdominal MRI scan, , Perform a laparotomy, , Perform diagnostic peritoneal lavage, , Arrange an urgent abdominal CT scan, , The patient's mechanism of injury makes a solid organ injury likely. FAST scanning is associated, with a false negative rate in pregnancy which makes the negative result less reassuring. CT, scanning remains the gold standard., Please rate this question:, , Discuss and give feedback, , Next question, , Imaging in the pregnant trauma patient, Sonography and FAST scanning are established in pregnancy and have the advantage of avoiding, ionising radiation. However, the sensitivity of the FAST scan is reduced in pregnancy especially with, advanced gestational age. Sensitivity of FAST scanning is 60-80% across all trimesters and 90% in, the first. CT scanning remains the first line investigation in major trauma where significant visceral, injury is suspected. The maximum permitted safe dose of radiation in pregnancy is 5mSv. A pelvic, CT scan would fall below this level. That said, early exposure to radiation will increase the risk of, developmental anomalies and foetal loss. Late exposure increases the risk of childhood cancer
Page 3313 :
twofold. CT scanning remains the most sensitive test for identifying complications such as placental, abruption in this group., Next question
Page 3314 :
Theme: Trauma, , A., B., C., D., E., F., G., H., , Tension pneumothorax, Haemopericardium, Haemothorax, Aortic transection, Ruptured spleen, Duodeno-jejunal flexure disruption, Aorto iliac disruption, Ileo-colic junction disruption, , For each scenario please select the most likely injury. Each option may be used once, more than, once or not at all., , 9., , A 24 year old motorist is involved in a road traffic accident in which he collides with the, wall of a tunnel in a head on car crash, speed 85mph. He is wearing a seatbelt and the, airbags have deployed. When rescuers arrive he is lucid and conscious and then dies, suddenly., You answered Tension pneumothorax, The correct answer is Aortic transection, Aortic transections typically occur distal to the ligamentum arteriosum. A temporary, haematoma may prevent the immediate death that usually occurs. This is a deceleration, injury. A widened mediastinum may be seen on x-ray., , 10., , A 30 year old women is involved in a road traffic accident she is a passenger in a car, involved in a head on collision with another vehicle. Her car is travelling at 60mph. She, has been haemodynamically stable throughout with only minimal tachycardia. On, examination she has marked abdominal tenderness and a large amount of intra abdominal, fluid on CT scan, You answered Tension pneumothorax, The correct answer is Duodeno-jejunal flexure disruption, This is another site of sudden deceleration injury. Given the large amount of free fluid, if it, were blood, then a greater degree of haemodynamic instability would be expected., , 11., , A 17 year old boy is involved in a motorcycle accident in which he is thrown from his, motorcycle. On admission he has distended neck veins and a weak pulse. The trachea is, central.
Page 3315 :
You answered Tension pneumothorax, The correct answer is Haemopericardium, This is most likely a cardiac tamponade produced by haemopericardium. As little as 100ml, of blood may result in tamponade as the pericardial sac is not distensible. Diagnosis is, suggested by muffled heart sounds, paradoxical pulse and jugular vein distension., Please rate this question:, , Discuss and give feedback, , Next question, , Thoracic trauma, Types of thoracic trauma, , Tension, pneumothorax, , , , , , , Flail chest, , , , , , , , Often laceration to lung parenchyma with flap, Pressure develops in thorax, Most common cause is mechanical ventilation in patient with, pleural injury, Symptoms overlap with cardiac tamponade, hyper-resonant, percussion note is more likely in tension pnemothorax, Chest wall disconnects from thoracic cage, Multiple rib fractures (at least two fractures per rib in at least two, ribs), Associated with pulmonary contusion, Abnormal chest motion, Avoid over hydration and fluid overload, , Pneumothorax, , , , , , Most common cause is lung laceration with air leakage, Most traumatic pneumothoraces should have a chest drain, Patients with traumatic pneumothorax should never be, mechanically ventilated until a chest drain is inserted, , Haemothorax, , , , Most commonly due to laceration of lung, intercostal vessel or, internal mammary artery, Haemothoraces large enough to appear on CXR are treated with, large bore chest drain, Surgical exploration is warranted if >1500ml blood drained, , ,
Page 3316 :
immediately, , , , , Beck's triad: elevated venous pressure, reduced arterial pressure,, reduced heart sounds, Pulsus paradoxus, May occur with as little as 100ml blood, , Pulmonary contusion, , , , , , Most common potentially lethal chest injury, Arterial blood gases and pulse oximetry important, Early intubation within an hour if significant hypoxia, , Blunt cardiac injury, , , , , , Usually occurs secondary to chest wall injury, ECG may show features of myocardial infarction, Sequelae: hypotension, arrhythmias, cardiac wall motion, abnormalities, , Aorta disruption, , , , , , Deceleration injuries, Contained haematoma, Widened mediastinum, , Diaphragm, disruption, , , , Most due to motor vehicle accidents and blunt trauma causing, large radial tears (laceration injuries result in small tears), More common on left side, Insert gastric tube, may pass into intrathoracic stomach, , Cardiac tamponade, , , , , Mediastinal, traversing wounds, , , , , , Entrance wound in one hemithorax and exit wound/foreign body, in opposite hemithorax, Mediastinal haematoma or pleural cap suggests great vessel, injury, Mortality is 20%, , References, ATLS Manual 8th Edition, Next question
Page 3317 :
A 14-year-old boy is admitted to the acute surgical unit with appendicitis. He is normally fit and well., Apart from metoclopramide, the patient has had no other medications. The nursing staff contact you, as the patient is acting strange. On examination he is agitated, has a clenched jaw and his eyes are, deviated upwards. What is the most likely diagnosis?, , Functional disorder, , Malignant hyperthermia, , Oculogyric crisis, , Epilepsy, , Serotonin syndrome, , This is a classic description of an oculogyric crisis, a form of extrapyramidal disorder. An oculogyric, crisis is an acute dystonic reaction. This is precipitated by antipsychotics (haloperidol) and, metoclopramide in susceptible individuals with a genetic predisposition to this. Treatment is with, procyclidine IM., Please rate this question:, , Discuss and give feedback, , Next question, , Oculogyric crisis, An oculogyric crisis is a dystonic reaction to certain drugs or medical conditions, Features, , , , Restlessness, agitation, Involuntary upward deviation of the eyes, , Causes, , , , , , Phenothiazines, Haloperidol, Metoclopramide, Postencephalitic Parkinson's disease
Page 3319 :
A 6 year old boy pulls over a kettle and suffers superficial partial thickness burns to his legs. Which, of the following will not occur?, , Preservation of hair follicles, , Formation of vesicles or bullae, , Damage to sweat glands, , Healing by re-epithelialisation, , Pain at the burn site, , Partial thickness burns are divided into superficial and deep burns, however, this is often not, possible on initial assessment and it may be a week or more before the distinction is clear cut., Dermal appendages are, by definition, intact. Superficial partial thickness burns will typically heal by, re-epithelialisation, deeper burns will heal with scarring., Please rate this question:, , Discuss and give feedback, , Next question, , Burns, Burns may be thermal, chemical or electrical. In the former category are burns which occur as a, result of heat. Chemical burns occur when the skin is exposed to an extremely caustic or alkaline, substance. Electrical burns occur following exposure to electrical current. The immediate, management includes removal of the burning source which usually includes irrigation of the burned, area. A detailed assessment then needs to be made of the extent of the burns and a number of, charts are available for recording this information. The degree of injury relates to the temperature, and duration of exposure. Most domestic burns are mainly scalds in young children., Following the burn, there is a local response with progressive tissue loss and release of, inflammatory cytokines. Systemically, there are cardiovascular effects resulting from fluid loss and, sequestration of fluid into the third space. There is a marked catabolic response. Immunosupression, is common with large burns and bacterial translocation from the gut lumen is a recognised event., Sepsis is a common cause of death following major burns., Types of burn
Page 3320 :
Type of burn, , Skin layers, affected, , Skin, appearance, , Blanching, , Epidermal/Superficial, , Epidermis, , Red, moist, , Yes, , Superficial partial, thickness, , Epidermis and part, of papillary dermis, affected, , Pale, dry, , Yes, , Normally heals, with no, intervention, , Deep partial thickness, , Epidermis, whole, papillary dermis, affected, , Mottled red, colour, , No, , Needs surgical, intervention, (depending on site), , Full thickness, , Whole skin layer, and subcutaneous, tissue affected, , Dry, leathery, hard wound, , No, , Burns centre, , Depth of burn assessment, , , , , , Bleeding on needle prick, Sensation, Appearance, Blanching to pressure, , Percentage burn estimation, Lund Browder chart: most accurate even in children, Wallace rule of nines, Palmar surface: surface area palm = 0.8% burn, >15% body surface area burns in adults needs urgent burn fluid resuscitation, Transfer to burn centre if:, , , , , , Need burn shock resuscitation, Face/hands/genitals affected, Deep partial thickness or full thickness burns, Significant electrical/chemical burns, , Management, , Management
Page 3321 :
The initial aim is to stop the burning process and resuscitate the patient. Intravenous fluids will be, required for children with burns greater than 10% of total body surface area. Adults with burns, greater than 15% of total body surface area will also require IV fluids. The fluids are calculated using, the Parkland formula which is; volume of fluid= total body surface area of the burn % x weight (Kg), x4. Half of the fluid is administered in the first 8 hours. A urinary catheter should be inserted., Analgesia should be given. Complex burns, burns involving the hand perineum and face and burns, >10% in adults and >5% in children should be transferred to a burns unit., Circumferential burns affecting a limb or severe torso burns impeding respiration may require, escharotomy to divide the burnt tissue., Conservative management is appropriate for superficial burns and mixed superficial burns that will, heal in 2 weeks. More complex burns may require excision and skin grafting. Excision and primary, closure is not generally practised as there is a high risk of infection., There is no evidence to support the use of anti microbial prophylaxis or topical antibiotics in burn, patients., Escharotomies, , , , Indicated in circumferential full thickness burns to the torso or limbs., Careful division of the encasing band of burn tissue will potentially improve ventilation (if the, burn involves the torso), or relieve compartment syndrome and oedema (where a limb is, involved), , References, www.euroburn.org/e107files/downloads/guidelinesburncare.pdf, Barajas-Nava LA, López-Alcalde J, Roqué i Figuls M, Solà I, Bonfill Cosp X. Antibiotic prophylaxis, for preventing burn wound infection. Cochrane Database of Systematic Reviews 2013, Issue 6. Art., No.: CD008738. DOI: 10.1002/14651858.CD008738.pub2., Hettiaratchy S & Papini R. Initial management of a major burn: assessment and resuscitation. BMJ, 2004;329:101-103, Next question
Page 3322 :
You are called to the acute surgical unit. A patient who has short gut syndrome has developed a, broad complex tachycardia. You suspect a diagnosis of ventricular tachycardia. What is the most, likely precipitant?, , Hypoglycaemia, , Bisoprolol, , Hypomagnesaemia, , Dehydration, , Hyperthyroidism, , Please rate this question:, , Discuss and give feedback, , Next question, , Ventricular tachcardia, Ventricular tachycardia (VT)is broad-complex tachycardia originating from a ventricular ectopic, focus. It has the potential to precipitate ventricular fibrillation and hence requires urgent treatment., There are two main types of VT:, , , , monomorphic VT: most commonly caused by myocardial infarction, polymorphic VT: A subtype of polymorphic VT is torsades de pointes which is precipitated by, prolongation of the QT interval. The causes of a long QT interval are listed below, , Causes of a prolonged QT interval, , Congenital, , , Jervell-Lange-Nielsen, syndrome (includes, deafness and is due to an, , Drugs, , , Other, , amiodarone, sotalol,, class 1a, antiarrhythmic drugs, , , , electrolyte:, hypocalcaemia,, hypokalaemia,
Page 3324 :
Based on the current guidelines, which option regarding management of head injuries is false?, , Opiates should be avoided, , Consider intubation if the GCS is <8 or = 8, , Immediate CT head if there is > 1 episode of vomiting, , Half hourly GCS assessment until GCS is 15, , Contact neurosurgeons if suspected penetrating injury, Once eight, intubate!, Pain should be controlled, with opiates preferably, as this avoids distress and hypertension post, injury., Please rate this question:, , Discuss and give feedback, , Next question, , Head injury management- NICE Guidelines, Summary of guidelines, , , , , , , All patients should be assessed within 15 minutes on arrival to A&E, Document all 3 components of the GCS, If GCS <8 or = to 8, consider stabilising the airway, Treat pain with low dose IV opiates (if safe), Full spine immobilisation until assessment if:, , - GCS < 15, - neck pain/tenderness, - paraesthesia extremities, - focal neurological deficit, - suspected c-spine injury, If a c-spine injury is suspected a 3 view c-spine x-ray is indicated. CT c-spine is preferred if:, - Intubated, - GCS <13
Page 3325 :
- Normal x-ray but continued concerns regarding c-spine injury, - Any focal neurology, - A CT head scan is being performed, - Initial plain films are abnormal, Immediate CT head (within 1 hour) if:, , , , , , , , , , GCS < 13 on admission, GCS < 15 2 hours after admission, Suspected open or depressed skull fracture, Suspected skull base fracture (panda eyes, Battle's sign, CSF from nose/ear, bleeding ear), Focal neurology, Vomiting > 1 episode, Post traumatic seizure, Coagulopathy, , Contact neurosurgeon if:, , , , , , , , , Persistent GCS < 8 or = 8, Unexplained confusion > 4h, Reduced GCS after admission, Progressive neurological signs, Incomplete recovery post seizure, Penetrating injury, Cerebrospinal fluid leak, , Observations, , , 1/2 hourly GCS until 15, , Reference, 1. http://guidance.nice.org.uk/CG56/QuickRefGuide/pdf/English, 2. Hodgkinson S et al. Early management of head injury: summary of NICE guidance. BMJ 2014, (348):34-37., Next question
Page 3326 :
A 22 year old man suffers 20% partial and full thickness burns in a house fire. There is an, associated inhalational injury. It is decided to administer intravenous fluids to replace fluid losses., Which of the intravenous fluids listed below should be used for initial resuscitation?, , Dextran 40, , 5% Dextrose, , Fresh frozen plasma, , Hartmans solution, , Blood, , In most units a crystalloid such as Hartmans (Ringers lactate) is administered initially. Controversy, does remain and some units do prefer colloid. Should this leak in the interstial tissues this may, increase the risk of oedema., Please rate this question:, , Discuss and give feedback, , Next question, , Fluid resuscitation burns, Indication: >15% total body area burns in adults (>10% children), , , , , , , The main aim of resuscitation is to prevent the burn deepening, Most fluid is lost 24 hours after injury, First 8-12 hour fluid shifts are from intravascular to interstitial fluid compartments, Therefore circulatory volume can be compromised. However fluid resuscitation causes more, fluid into the interstitial compartment especially colloid (therefore avoided in first 8-24 hours), Protein loss occurs, , Fluid resuscitation formula, Parkland formula, (Crystalloid only e.g. Hartman's solution/Ringers' lactate), Total fluid requirement in 24 hours =, 4 ml x (total burn surface area (%)) x (body weight (kg))
Page 3327 :
, , , 50% given in first 8 hours, 50% given in next 16 hours, , Resuscitation endpoint:Urine output of 0.5-1.0 ml/kg/hour in adults (increase rate of fluid to, achieve this), Points to note:, , , , , Starting point of resuscitation is time of injury, Deduct fluids already given, , After 24 hours, , , , , , , Maintenance crystalloid (usually dextrose-saline) is continued at a rate of 1.5 ml x(burn, area)x(body weight), Colloids are rarely used (e.g. albumin), Antioxidants, such as vitamin C, can be used to minimize oxidant-mediated contributions to, the inflammatory cascade in burns, High tension electrical injuries and inhalation injuries require more fluid, Monitor: packed cell volume, plasma sodium, base excess, and lactate, Next question
Page 3328 :
A 23 year old man sustains a severe facial fracture and reconstruction is planned. Which of the, following investigations will facilitate pre-operative planning?, , Mandibular tomography, , Magnetic resonance scan of face, , Skull X-ray, , Computerised tomography of the head, , Orthopantomogram, , Theme from 2011 Exam, Significant facial fractures may have intracranial communication. CT scanning will allow delineation, of injury extent and 3D reconstruction images can be created. An Orthopantomogram (OPT) will, provide good images of mandible and surrounding bony structures but will not give intracranial, detail. A skull x-ray lacks the detail for modern practice., Please rate this question:, , Discuss and give feedback, , Next question, , Craniomaxillofacial injuries, Craniomaxillofacial injuries in the UK are due to:, , , , , , Interpersonal violence (52%), Motor vehicle accidents (16%), Sporting injuries (19%), Falls (11%), , Le Fort Fractures, , Grade, , Feature, , Le, , The fracture extends from the nasal septum to the lateral pyriform rims, travels, horizontally above the teeth apices, crosses below the zygomaticomaxillary junction, and
Page 3329 :
Grade, , Feature, , Fort 1, , traverses the pterygomaxillary junction to interrupt the pterygoid plates., , Le, Fort 2, , These fractures have a pyramidal shape and extend from the nasal bridge at or below the, nasofrontal suture through the frontal process of the maxilla, inferolaterally through the, lacrimal bones and inferior orbital floor and rim through or near the inferior orbital, foramen, and inferiorly through the anterior wall of the maxillary sinus; it then travels, under the zygoma, across the pterygomaxillary fissure, and through the pterygoid plates., , Le, Fort 3, , These fractures start at the nasofrontal and frontomaxillary sutures and extend posteriorly, along the medial wall of the orbit through the nasolacrimal groove and ethmoid bones., The thicker sphenoid bone posteriorly usually prevents continuation of the fracture into, the optic canal. Instead, the fracture continues along the floor of the orbit along the, inferior orbital fissure and continues superolaterally through the lateral orbital wall,, through the zygomaticofrontal junction and the zygomatic arch. Intranasally, a branch of, the fracture extends through the base of the perpendicular plate of the ethmoid, through, the vomer, and through the interface of the pterygoid plates to the base of the sphenoid., This type of fracture predisposes the patient to CSF rhinorrhea more commonly than the, other types., , Ocular injuries, Superior orbital fissure syndrome, Severe force to the lateral wall of the orbit resulting in compression of neurovascular structures., Results in :, , , , , , Complete opthalmoplegia and ptosis (Cranial nerves 3, 4, 6 and nerve to levator palpebrae, superioris), Relative afferent pupillary defect, Dilatation of the pupil and loss of accommodation and corneal reflexes, Altered sensation from forehead to vertex (frontal branch of trigeminal nerve), , Orbital blow out fracture, Typically occurs when an object of slightly larger diameter than the orbital rim strikes the, incompressible eyeball. The bone fragment is displaced downwards into the antral cavity, remaining, attached to the orbital periosteum. Periorbital fat may be herniated through the defect, interfering, with the inferior rectus and inferior oblique muscles which are contained within the same fascial, sheath. This prevents upward movement and outward rotation of the eye and the patient, experiences diplopia on upward gaze. The initial bruising and swelling may make assessment, difficult and patients should usually be reviewed 5 days later. Residual defects may require orbital, floor reconstruction.
Page 3330 :
Nasal Fractures, , , , , , , Common injury, Ensure new and not old deformity, Control epistaxis, CSF rhinorrhoea implies that the cribriform plate has been breached and antibiotics will be, required., Usually best to allow bruising and swelling to settle and then review patient clinically. Major, persistent deformity requires fracture manipulation, best performed within 10 days of injury., , Retrobulbar haemorrhage, Rare but important ocular emergency. Presents with:, , , , , , , Pain (usually sharp and within the globe), Proptosis, Pupil reactions are lost, Paralysis (eye movements lost), Visual acuity is lost (colour vision is lost first), , May be the result of Le Fort type facial fractures., Management:, , , , , , Mannitol 1g/Kg as 20% infusion, Osmotic diuretic, Contra-indicated in congestive heart, failure and pulmonary oedema, Acetazolamide 500mg IV, (Monitor FBC/U+E) Reduces aqueous pressure by inhibition of, carbonic anhydrase (used in glaucoma), Dexamethasone 8mg orally or intravenously, In a traumatic setting an urgent cantholysis may be needed prior to definitive surgery., , Consider, Papaverine 40mg smooth muscle relaxant, Dextran 40 500mls IV improves perfusion, Next question
Page 3331 :
A 23 year old man is stabbed in the right upper quadrant and is haemodynamically unstable. A, laparotomy is performed and the liver has some extensive superficial lacerations and is bleeding, profusely. The patient becomes progressively more haemodynamically unstable. What is the best, management option?, , Pack the liver and close the abdomen, , Occlude the hepatic inflow with a pringles manoeuvre and suture the defects, , Occlude vascular inflow and resect the most severely affected area anatomically, , Perform a portosystemic shunt procedure, , Suture the defects without vascular occlusion, , Packing of the liver is the safest option and resection or repair considered later when the physiology, is normalised. Often when the packs are removed all the bleeding has ceased and the abdomen can, be closed without further action. Definitive attempts at suturing or resection at the primary, laparotomy are often complicated by severe bleeding., Please rate this question:, , Discuss and give feedback, , Next question, , Trauma management, The cornerstone of trauma management is embodied in the principles of ATLS., Following trauma there is a trimodal death distribution:, , , , , Immediately following injury. Typically as result of brain or high spinal injuries, cardiac or, great vessel damage. Salvage rate is low., In early hours following injury. In this group deaths are due to phenomena such as splenic, rupture, sub dural haematomas and haemopneumothoraces, In the days following injury. Usually due to sepsis or multi organ failure., , Aspects of trauma management, , , ABCDE approach.
Page 3332 :
, , , , , Tension pneumothoraces will deteriorate with vigorous ventilation attempts., External haemorrhage is managed as part of the primary survey. As a rule tourniquets, should not be used. Blind application of clamps will tend to damage surrounding structures, and packing is the preferred method of haemorrhage control., Urinary catheters and naso gastric tubes may need inserting. Be wary of basal skull fractures, and urethral injuries., Patients with head and neck trauma should be assumed to have a cervical spine injury until, proven otherwise., , Thoracic injuries, , , , , , , , , , Simple pneumothorax, Mediastinal traversing wounds, Tracheobronchial tree injury, Haemothorax, Blunt cardiac injury, Diaphragmatic injury, Aortic disruption, Pulmonary contusion, , Management of thoracic trauma, , , , , , , , , , , , Simple pneumothorax insert chest drain. Aspiration is risky in trauma as pneumothorax, may be from lung laceration and convert to tension pneumothorax., Mediastinal traversing wounds These result from situations like stabbings. Exit and entry, wounds in separate hemithoraces. The presence of a mediastinal haematoma indicates the, likelihood of a great vessel injury. All patients should undergo CT angiogram and, oesophageal contrast swallow. Indications for thoracotomy are largely related to blood loss, and will be addressed below., Tracheobronchial tree injury Unusual injuries. In blunt trauma most injuries occur within, 4cm of the carina. Features suggesting this injury include haemoptysis and surgical, emphysema. These injuries have a very large air leak and may have tension pneumothorax., Haemothorax Usually caused by laceration of lung vessel or internal mammary artery by rib, fracture. Patients should all have a wide bore 36F chest drain. Indications for thoracotomy, include loss of more than 1.5L blood initially or ongoing losses of >200ml per hour for >2, hours., Cardiac contusions Usually cardiac arrhythmias, often overlying sternal fracture. Perform, echocardiography to exclude pericardial effusions and tamponade. Risk of arrhythmias falls, after 24 hours., Diaphragmatic injury Usually left sided. Direct surgical repair is performed., Traumatic aortic disruption Commonest cause of death after RTA or falls. Usually, incomplete laceration near ligamentum arteriosum. All survivors will have contained, haematoma. Only 1-2% of patients with this injury will have a normal chest x-ray., Pulmonary contusion Common and lethal. Insidious onset. Early intubation and ventilation., , Abdominal trauma
Page 3333 :
, , , , , , , , , Deceleration injuries are common., In blunt trauma requiring laparotomy the spleen is most commonly injured (40%), Stab wounds traverse structures most commonly liver (40%), Gunshot wounds have variable effects depending upon bullet type. Small bowel is most, commonly injured (50%), Patients with stab wounds and no peritoneal signs up to 25% will not enter the peritoneal, cavity, Blood at urethral meatus suggests a urethral tear, High riding prostate on PR = urethral disruption, Mechanical testing for pelvic stability should only be performed once, , Investigations in abdominal trauma, , Diagnostic Peritoneal, Lavage, , Abdominal CT scan, , USS, , Indication, , Document bleeding if, hypotensive, , Document organ injury if, normotensive, , Document fluid if, hypotensive, , Advantages, , Early diagnosis and, sensitive; 98% accurate, , Most specific for, localising injury; 92 to, 98% accurate, , Early diagnosis, non, invasive and repeatable;, 86 to 95% accurate, , Disadvantages, , Invasive and may miss, retroperitoneal and, diaphragmatic injury, , Location of scanner away, from facilities, time taken, for reporting, need for, contrast, , Operator dependent and, may miss, retroperitoneal injury, , , , , Amylase may be normal following pancreatic trauma, Urethrography if suspected urethral injury, Next question
Page 3334 :
A 62 year old woman presents with acute bowel obstruction. She has been vomiting up to 15 times a, day and is taking erythromycin. She suddenly complains of dizziness. Her ECG shows torsades de, pointes. What is the management of choice?, , IV Atropine, , IV Potassium, , IV Magnesium sulphate, , IV Bicarbonate, , IV Adrenaline, Torsades de pointes: Treatment IV magnesium sulphate, This woman is likely to have hypokalaemia and hypomagnasaemia as a result of vomiting. In, addition to this, the erythromycin will predispose her to torsades de pointes. The patient needs, Magnesium 2g over 10 minutes. Knowledge of the management of this peri arrest diagnosis is, hence important in surgical practice., Please rate this question:, , Discuss and give feedback, , Next question, , Torsades de pointes, Torsades de pointes ('twisting of the points') is a rare arrhythmia associated with a long QT interval., It may deteriorate into ventricular fibrillation and hence lead to sudden death, Causes of long QT interval, , , , , , , , , , , congenital: Jervell-Lange-Nielsen syndrome, Romano-Ward syndrome, antiarrhythmics: amiodarone, sotalol, class 1a antiarrhythmic drugs, tricyclic antidepressants, antipsychotics, chloroquine, terfenadine, erythromycin, electrolyte: hypocalcaemia, hypokalaemia, hypomagnesaemia, myocarditis
Page 3336 :
A 27 year old man sustains a single gunshot wound to the left thigh. In the emergency department,, he is noted to have a large haematoma of his medial thigh. He complains of parasthesia in his foot., On examination, there are weak pulses palpable distal to the injury and the patient is unable to move, his foot. The appropriate initial management of this patient is:, , Conventional angiography, , Immediate exploration and repair, , Fasciotomy of the anterior compartment, , Observation for resolution of spasm, , Local wound exploration, , The five P's of arterial injury include pain, parasthesias, pallor, pulselessness and paralysis. In the, extremities, the tissues most sensitive to anoxia are the peripheral nerves and striated muscle. The, early developments of paresthesias and paralysis are signals that there is significant ischemia, present, and immediate exploration and repair are warranted. The presence of palpable pulse does, not exclude an arterial injury because this presence may represent a transmitted pulsation through a, blood clot. When severe ischemia is present, the repair must be completed within 6 to 8 h to prevent, irreversible muscle ischemia and loss of limb function. Delay to obtain a conventional angiogram or, to observe for change needlessly prolongs the ischemic time. A CT angiogram may be a reasonable, alternative. Fasciotomy may be required but should be done in conjunction with and after reestablishment of arterial flow. Local wound exploration is not recommended because brisk, hemorrhage may be encountered without the securing of prior vascular control., Please rate this question:, , Discuss and give feedback, , Next question, , Vascular trauma, Peripheral and central vessels may be injured by blunt, penetrating or shearing injuries. Fractures of, bones close to vessels may also be associated with vascular injury or vessel occlusion., Assessment, , , , , Check for signs of distal perfusion, Doppler signal distally (monophasic/ biphasic or triphasic), Anatomical location (which vessel is likely to be involved)
Page 3337 :
, , Duplex scanning and angiography are "gold standard" tests but may not be immediately, available in the trauma setting, , Management, , , , , , , Almost always operative., Obtaining proximal and distal control of affected vessels is crucial., Simple lacerations of arteries may be directly closed, or a vein patch applied if there is a risk, of subsequent stenosis., Transection of the vessel should be treated by either end to end anastomosis (often not, possible) or an interposition vein graft., Use of PTFE in traumatic open injuries will invariably result in infection., Next question
Page 3338 :
Theme: Paediatric emergencies, , A., B., C., D., E., , Manage conservatively, Immediate emergency theatre, Treat in emergency department, Treat in emergency department under sedation, Operate on next emergency list, , Please select the most appropriate intervention for the scenario given. Each option may be used, once, more than once or not at all., , 21., , A 3 year old child inserts a crayon into their external auditory meatus. Attempts to remove, it have not been successful., You answered Manage conservatively, The correct answer is Operate on next emergency list, Theme from September 2011 Exam, They would not tolerate removal in the emergency department. The tympanic membrane, should be carefully inspected and again this will be easier under general anaesthesia., , 22., , A 2 year old accidentally inhales a peanut. They arrive in the emergency department, extremely distressed and cyanotic. Imaging shows it to be lodged in the left main, bronchus., You answered Manage conservatively, The correct answer is Immediate emergency theatre, As they are cyanosed it requires immediate removal and this should be undertaken in a, fully staffed theatre. Ideally a rigid bronchoscopy should be performed., , 23., , A 10 year old boy is shot in the head with an airgun pellet. He is concerned that he will get, into trouble and the injury remains concealed for 10 days. Imaging using CT scanning, shows it to be lodged in the frontal lobe., Manage conservatively, The pellet is small and no serious injury has occurred at this stage. This should therefore, be managed conservatively., , Please rate this question:
Page 3339 :
Discuss and give feedback, , Next question, , Management of acute cases- Paediatric, , , , , , , , , , Children will often insert objects into orifices such as the nose and external auditory meatus, Assessment includes assessment of airway and haemodynamic status, Where the airway is not immediately threatened decisions can be made as to whether to, manage in the emergency department or transfer to theatre, In general children do not tolerate procedures well and it is usually safer to remove objects in, theatre and under general anaesthesia with a secure airway, A chest x-ray is required to ensure that no object is present in the chest, not all objects are, radioopaque. However, signs such as focal consolidation may indicate small airway, obstruction, In the case of small bore missile injuries the decision relating to surgery depends on the size, of the missile and its location. Airgun pellets are a common culprit, if there is a long time, interval between the incident and presentation and the object has not caused any significant, problems then it may be best left alone, Airgun pellets (and glass) lodged in the soft tissues are usually notoriously difficult to localise, and extract, no matter how superficial. Removal in theatre is usually the best option. If the, object is radioopaque then an image intensifier should be used, Next question
Page 3340 :
A 32 year old male is receiving a blood transfusion after being involved in a road traffic accident. A, few minutes after the transfusion he complains of loin pain. His observations show temperature, 39 oC, HR 130bpm and blood pressure is 95/40mmHg. What is the best test to confirm his, diagnosis?, , USS abdomen, , Direct Coomb's test, , Blood cultures, , Blood film, , Sickle cell test, Mnemonic for transfusion reactions:, Got a bad unit, G raft vs. Host disease, O verload, T hrombocytopaenia, A lloimmunization, B lood pressure unstable, A cute haemolytic reaction, D elayed haemolytic reaction, U rticaria, N eutrophilia, I nfection, T ransfusion associated lung injury, , The diagnosis is of an acute haemolytic transfusion reaction, normally due to ABO incompatibility., Haemolysis of the transfused cells occurs causing the combination of shock, haemoglobinaemia and, loin pain. This may subsequently lead to disseminated intravascular coagulation. A Coomb's test, should confirm haemolysis. Other tests for haemolysis include: unconjugated bilirubin, haptoglobin,, serum and urine free haemoglobin.
Page 3341 :
Note that delayed haemolytic reactions are normally associated with antibodies to the Rh system, and occur 5-10 days after transfusion., Please rate this question:, , Discuss and give feedback, , Next question, , Blood transfusion reactions, Acute transfusion reactions present as adverse signs or symptoms during or within 24 hours of a, blood transfusion. The most frequent reactions are fever, chills, pruritus, or urticaria, which typically, resolve promptly without specific treatment or complications. Other signs occurring in temporal, relationship with a blood transfusion, such as severe dyspnoea, pyrexia, or loss of consciousness, may be the first indication of a more severe potentially fatal reaction., The causes of adverse reactions are multi-factorial. Immune mediated reactions, some of the most, feared, occur as a result of component mismatch, the commonest cause of which is clerical error., More common, non immune mediated, complications may occur as a result of product, contamination, this may be bacterial or viral., Transfusion related lung injury is well recognised and there are two proposed mechanisms which, underpin this. One involves the sequestration of primed neutrophils within the recipient pulmonary, capillary bed. The other proposed mechanism suggests that HLA mismatches between donor, neutrophils and recipient lung tissue is to blame., The table below summarises the main types of transfusion reaction., , Immune mediated, , Non immune mediated, , Pyrexia, , Hypocalcaemia, , Alloimmunization, , CCF, , Thrombocytopaenia, , Infections, , Transfusion associated lung injury, , Hyperkalaemia
Page 3342 :
Immune mediated, , Non immune mediated, , Graft vs Host disease, , Urticaria, , Acute or delayed haemolysis, , ABO incompatibility, , Rhesus incompatibility, Next question
Page 3343 :
A 45 year old man complains of sharp chest pain. He is due to have elective surgery to replace his, left hip. He has been bed bound for 3 months. He suddenly collapses; his blood pressue is, 70/40mmHg, heart rate 120 bpm and his saturations are 74% on air. He is deteriorating in front of, you. What is the next best management plan?, , Aspirin, , Thrombolysis with Alteplase, , Unfractionated heparin, , Thrombolysis with streptokinase, , Clopidogrel, , This man is peri arrest with the diagnosis of pulmonary embolism (chest pain,bedbound, collapse,, low saturations). He needs urgent thrombolysis with alteplase (he may not survive if you wait for the, medical Spr/ITU to arrive!)., Please rate this question:, , Discuss and give feedback, , Next question, , Pulmonary embolism: management, A summary of the British Thoracic Society guidelines, , , , , , , , , Heparin should be given if intermediate or high clinical probability before imaging., Unfractionated heparin (UFH) should be considered (a) as a first dose bolus, (b) in massive, PE, or (c) where rapid reversal of effect may be needed., Otherwise, low molecular weight heparin (LMWH) should be considered as preferable to, UFH, having equal efficacy and safety and being easier to use., Oral anticoagulation should only be commenced once VTE has been reliably confirmed., The target INR should be 2.0-3.0; when this is achieved, heparin can be discontinued., The standard duration of oral anticoagulation is: 4 to 6 weeks for temporary risk factors, 3, months for first idiopathic, and at least 6 months for other; the risk of bleeding should be, balanced with that of further VTE., , Massive PE
Page 3344 :
, , , , CTPA or echocardiography will reliably diagnose clinically massive PE., Thrombolysis is 1st line for massive PE (ie circulatory failure) and may be instituted on, clinical grounds alone if cardiac arrest is imminent; a 50 mg bolus of alteplase is, recommended., Invasive approaches (thrombus fragmentation and IVC filter insertion) should be considered, where facilities and expertise are readily available., Next question
Page 3345 :
A 30 year old woman, who is 30 weeks pregnant, attends the varicose vein clinic. The patient is, normally fit and well, with no lung disorders. She suddenly complains of shortness of breath and, chest pain. She has no underlying lung condition. Her saturations are 92 % air, blood pressure, 150/80 mmHg and her chest sounds clear. What would be the main investigation recommended to, establish her diagnosis?, , Lung spirometry, , Half dose scintigraphy, , CTPA, , Echocardiogram, , Full dose scintigraphy, , The main differential diagnosis is pulmonary embolism. A CXR should be performed first in second, and third trimester to exclude other diagnoses such as pneumothorax or pneumonia. Concerns, surrounding radiation exposure by CXR have been discounted at this stage, as the need to establish, a diagnosis is the major priority. If the chest x-ray is normal, then half dose scintigraphy should be, performed. If there is underlying lung pathology, then a CTPA is performed., This is a controversial topic area, however the answer is related to guidance from the Royal College, of Obstetricians and Gynaecologists. The official line is that half dose scintigraphy is undertaken in, those with normal CXR (or no chest signs) and no pre- existing lung disease. The reason for this is, the significant subsequent increase in risk of maternal breast cancer with CTPA (lifetime risk, increased by up to 13.6% with CTPA, background risk of 1/200 for study population) vs scintigraphy., The vast majority of female patients are not found to have a PE which is also an important, component. However, we recognise that in most hospitals a CTPA is still performed first line., Reference, The acute management of thrombosis and embolism during pregnancy and the puerperium RCOG, guidelines February 2007, Scarsbrook A.Fand Gleeson V. Investigating suspected pulmonary embolism in, pregnancy. BMJ 2007 (326) : 1135 doi: 10.1136/bmj.7399.1135., Please rate this question:, , Discuss and give feedback, , Next question, , Chest pain in pregnancy
Page 3346 :
Aortic dissection, , , , , , , Predisposing factors in pregnancy are hypertension, congenital heart disease and Marfan's, syndrome, Mainly Stanford type A dissections, Sudden tearing chest pain, transient syncope, Patient may be cold and clammy, hypertensive and have an aortic regurgitation murmur, Involvement of the right coronary artery may cause inferior myocardial infarction, , Surgical management, , Gestational timeframe, , Management, , < 28/40, , Aortic repair with the fetus kept in utero, , 28-32/40, , Dependent on fetal condition, , > 32/40, , Primary Cesarean section followed by aortic repair at the same operation, , Mitral stenosis, , , , , , , Most cases associated with rheumatic heart disease, Becoming less common in British women; suspect in Immigrant women, Commonest cardiac condition in pregnancy, Commonly associated with mortality, Valve surgery; balloon valvuloplasty preferable, , Pulmonary embolism, , , , , , Leading cause of mortality in pregnancy, Half dose scintigraphy; CT chest if underlying lung disease, should aid diagnosis, Treatment with low molecular weight heparin throughout pregnancy and 4-6 weeks after, childbirth, Warfarin is contra indicated in pregnancy (though may be continued in women with, mechanical heart valves due to the significant risk of thromboembolism), , References, 1. Bates S.M. and Ginsberg J.S. How we manage venous thromboembolism during, pregnancy. Blood2002 (100): 3470-3478.
Page 3347 :
2. Scarsbrook A.Fand Gleeson V. Investigating suspected pulmonary embolism in, pregnancy. BMJ2007 (326) : 1135 doi: 10.1136/bmj.7399.1135., 3. Morley C. A. and Lim B. A. Lesson of the Week: The risks of delay in diagnosis of breathlessness, in pregnancy. BMJ 1995 (311) : 1083., Next question
Page 3348 :
Theme: Bleeding disorders, , A. Vitamin K deficiency, B. von Willebrand's disease, C. Acquired haemophilia, D. Haemophilia B, E. Protein C deficiency, F. Disseminated intravascular coagulation, G. Factor V Leiden, H. Excess heparin, I. Warfarin overdose, J. Antiphospholipid syndrome, , What is the most likely diagnosis for the scenario given? Each option may be used once, more than, once or not at all., , 27., , A 33 year old female is admitted for varicose vein surgery. She is fit and well. After the procedure, she is persistently bleeding. She is known to have menorrhagia. Investigations show a prolonged, bleeding time and increased APTT. She has a normal PT and platelet count., You answered Vitamin K deficiency, The correct answer is von Willebrand's disease, Bleeding post operatively, epistaxis and menorrhagia may indicate a diagnosis of vWD., Haemoarthroses are rare. The bleeding time is usually normal in haemophilia (X-linked) and, vitamin K deficiency., , 28., , A 70 year old heavy smoker presents with 3 weeks of haematuria and bruising. He is normally fit, and well. He is on no medications. His results reveal:, Hb 9.0
Page 3349 :
WCC 11, Pl 255, PT 16 (normal), APTT 58 (increased), Thrombin time 20 (normal)., You answered Vitamin K deficiency, The correct answer is Acquired haemophilia, This patient has Factor 8 acquired disorder. He is likely to have developed a lung malignancy, (smoker) and as a result aquired a haemophilia disorder. The elderly, pregnancy, malignancy and, autoimmune conditions are associated with acquired haemophilia. Prolonged APTT is key to the, diagnosis. Management involves steroids., , 29., , A 28 year old female is attends the gynaecology unit for a D+C following an incomplete, miscarriage. She has previously had recurrent pulmonary embolic events. After the procedure she, is persistently bleeding. Her APTT is 52 (increased)., You answered Vitamin K deficiency, The correct answer is Antiphospholipid syndrome, A combination of thromboembolism and bleeding in a young woman should raise the possibility, of antiphospholipid syndrome. Other features may include foetal loss, venous and arterial, thrombosis and thrombocytopenia. A Lupus anticoagulant may be present and the APTT is, prolonged., , Theme from January 2012 exam, , Please rate this question:, , Discuss and give feedback, , Next question
Page 3350 :
Abnormal coagulation, Cause, , Factors affected, , Heparin, , Prevents activation factors 2,9,10,11, , Warfarin, , Affects synthesis of factors 2,7,9,10, , DIC, , Factors 1,2,5,8,11, , Liver disease, , Factors 1,2,5,7,9,10,11, , Interpretation blood clotting test results, , Disorder, , APTT, , PT, , Bleeding time, , Haemophilia, , Increased, , Normal, , Normal, , von Willebrand's disease, , Increased, , Normal, , Increased, , Vitamin K deficiency, , Increased, , Increased, , Normal, Next question
Page 3351 :
A 54-year-old man is brought to the Emergency Department after being found collapsed in the, street. He is known to have a history of alcoholic liver disease. Blood tests reveal the following:, Calcium, , 1.62 mmol/l, , Albumin, , 33 g/l, , Which one of the following is the most appropriate management of the calcium result?, , 10ml of 10% calcium chloride over 10 minutes, , 20% albumin infusion, , 10ml of 50% calcium gluconate over 10 minutes, , No action, , 10ml of 10% calcium chloride over 4 hours, Current UK ALS guidance is to use calcium chloride, Even after correction for the low albumin level this patient has significant hypocalcaemia which, should be corrected., Please rate this question:, , Discuss and give feedback, , Next question, , Hypocalcaemia: causes and management, The clinical history combined with parathyroid hormone levels will reveal the cause of, hypocalcaemia in the majority of cases, Causes, , , , , , , Vitamin D deficiency (osteomalacia), Acute pancreatitis, Chronic renal failure, Hypoparathyroidism (e.g. post thyroid/parathyroid surgery), Pseudohypoparathyroidism (target cells insensitive to PTH)
Page 3352 :
, , , Rhabdomyolysis (initial stages), Magnesium deficiency (due to end organ PTH resistance), , Management, , , , , , Acute management of severe hypocalcaemia is with intravenous replacement. The preferred, method is with intravenous calcium chloride, 10ml of 10% solution over 10 minutes, ECG monitoring is recommended, Further management depends on the underlying cause, Calcium and bicarbonate should not be administered via the same route, Next question
Page 3353 :
A 25 year old male pedestrian is hit by a van on a busy road. He is brought to the Emergency, Department by ambulance. On examination he is dyspneoic, and hypoxic despite administration of, high flow 100% oxygen. His blood pressure is 110/70 and pulse rate is 115 bpm. The right side of, his chest is hyper-resonant on percussion and has decreased breath sounds. The trachea is, deviated to the left. What is the most likely underlying diagnosis?, , Fat embolism, , Tension pneumothorax, , Rupture of the right main bronchus, , Rupture of the diaphragm, , Pulmonary contusion, , Blunt or penetrating chest trauma that creates a flap type defect on the surface of the lung can result, in a tension pneumothorax. Typical features include dyspnoea, progressive hypoxia,, hyperresonance and tracheal deviation. Treatment is with needle decompression and chest tube, insertion., Please rate this question:, , Discuss and give feedback, , Next question, , Thoracic trauma, Types of thoracic trauma, , Tension, pneumothorax, , , , , , , Flail chest, , , , , Often laceration to lung parenchyma with flap, Pressure develops in thorax, Most common cause is mechanical ventilation in patient with, pleural injury, Symptoms overlap with cardiac tamponade, hyper-resonant, percussion note is more likely in tension pnemothorax, Chest wall disconnects from thoracic cage, Multiple rib fractures (at least two fractures per rib in at least two, ribs)
Page 3354 :
, , , , Associated with pulmonary contusion, Abnormal chest motion, Avoid over hydration and fluid overload, , Pneumothorax, , , , , , Most common cause is lung laceration with air leakage, Most traumatic pneumothoraces should have a chest drain, Patients with traumatic pneumothorax should never be, mechanically ventilated until a chest drain is inserted, , Haemothorax, , , , Most commonly due to laceration of lung, intercostal vessel or, internal mammary artery, Haemothoraces large enough to appear on CXR are treated with, large bore chest drain, Surgical exploration is warranted if >1500ml blood drained, immediately, , , , , , , , , Beck's triad: elevated venous pressure, reduced arterial pressure,, reduced heart sounds, Pulsus paradoxus, May occur with as little as 100ml blood, , Pulmonary contusion, , , , , , Most common potentially lethal chest injury, Arterial blood gases and pulse oximetry important, Early intubation within an hour if significant hypoxia, , Blunt cardiac injury, , , , , , Usually occurs secondary to chest wall injury, ECG may show features of myocardial infarction, Sequelae: hypotension, arrhythmias, cardiac wall motion, abnormalities, , Aorta disruption, , , , , , Deceleration injuries, Contained haematoma, Widened mediastinum, , Diaphragm, disruption, , , , Most due to motor vehicle accidents and blunt trauma causing, large radial tears (laceration injuries result in small tears), More common on left side, Insert gastric tube, may pass into intrathoracic stomach, , Cardiac tamponade, , ,
Page 3356 :
Theme: Management of skin injuries, , A., B., C., D., E., F., G., H., I., , Wound excision and primary closure, Simple primary closure, Delayed primary closure, Debridement and healing by secondary intention, Split thickness skin graft, Full thickness skin graft, Free flap, Pedicled flap, Debridement and rotational flap, , For the injuries described please select the most appropriate management. Each option may be, used once, more than once or not at all., , 32., , A 32 year old man is involved in a road traffic accident and sustains a significant, laceration to the lateral aspect of the nose which is associated with tissue loss., You answered Wound excision and primary closure, The correct answer is Debridement and rotational flap, Theme from April 2011 Exam, Nasal injuries can be challenging to manage and where there is tissue loss, it can be, difficult to primarily close them and still obtain a satisfactory aesthetic result. Debridement, together with a rotational flap would obtain the best results here., , 33., , A 7 year old boy falls over and sustains a 6cm laceration to his head. On inspection his, wound contains some dirt in it., Wound excision and primary closure, By debriding the wound, the area can then be primarily closed. Prophylactic antibiotics, should be administered., , 34., , A 45 year old man is gardening and damages his foot with a fork. On examination there, are cutaneous defects and the surrounding skin looks dusky., You answered Wound excision and primary closure, The correct answer is Debridement and healing by secondary intention, The skin changes described here should be debrided. Closure would not be safe with the
Page 3357 :
skin changes documented and the wound should be left open., Please rate this question:, , Discuss and give feedback, , Next question, , Methods of wound closure, Method of, closure, , Indication, , Primary closure, , , , , , Clean wound, usually surgically created or following minor trauma, Standard suturing methods will usually suffice, Wound heals by primary intention, , Delayed primary, closure, , , , , Similar methods of actual closure to primary closure, May be used in situations where primary closure is either not, achievable or not advisable e.g. infection, , Vacuum assisted, closure, , , , , Uses negative pressure therapy to facilitate wound closure, Sponge is inserted into wound cavity and then negative pressure, applied, Advantages include removal of exudate and versatility, Disadvantages include cost and risk of fistulation if used incorrectly, on sites such as bowel, , , , , Split thickness, skin grafts, , , , , , Superficial dermis removed with Watson knife or dermatome, (commonly from thigh), Remaining epithelium regenerates from dermal appendages, Coverage may be increased by meshing, , Full thickness skin, grafts, , , , , , , Whole dermal thickness is removed, Sub dermal fat is then removed and graft placed over donor site, Better cosmesis and flexibility at recipient site, Donor site "cost", , Flaps, , , , Viable tissue with a blood supply
Page 3358 :
, , , , May be pedicled or free, Pedicled flaps are more reliable, but limited in range, Free flaps have greater range but carry greater risk of breakdown as, they require vascular anastomosis, Next question
Page 3359 :
A 19 year old student is involved in a head on car collision. He complains of severe chest pain. A, Chest x-ray performed as part of a trauma series shows widening of the mediastinum. Which is the, most likely injury in this scenario?, , Rupture of the distal oesophagus, , Rupture of the left main bronchus, , Rupture of the aorta proximal to the left subclavian artery, , Rupture of the aorta distal to the left subclavian artery, , Rupture of the inferior vena cava, , The aorta may be injured in deceleration accidents. In the setting of deceleration injury, chest pain, and mediastinal widening the most likely problem is aortic rupture. This will typically occur distal to, the left subclavian artery. Rupture of the proximal aorta may occur. However, survival is unlikely. It is, important to note that the question uses the term Most likely injury as this is the component that, distinguishes an ascending rupture from a descending rupture., Please rate this question:, , Discuss and give feedback, , Next question, , Thoracic aorta rupture, , , , , Mechanism of injury: Decelerating force i.e. RTA, fall from a great height, Most people die at scene, Survivors may have an incomplete laceration at the ligamentum arteriosum of the aorta., , Clinical features, , , , Contained haematoma: persistent hypotension, Detected mainly by history, CXR changes, , CXR changes
Page 3360 :
, , , , , , , Widened mediastinum, Trachea/Oesophagus to right, Depression of left main stem bronchus, Widened paratracheal stripe/paraspinal interfaces, Space between aorta and pulmonary artery obliterated, Rib fracture/left haemothorax, , Diagnosis, Angiography, usually CT aortogram., Treatment, Repair or replacement. Ideally they should undergo endovascular repair., Next question
Page 3361 :
Theme: Management of head and neck trauma, , A., B., C., D., E., F., G., , Observation, CT head within 1 hour, CT head within 8 hours, Urgent neurosurgical review (even before CT head performed), 3 view c-spine xray, 2 view c-spine xray, CT c-spine, , What is the best initial management plan for the injuries described? Each option may be used once,, more than once or not at all., , 36., , A 22 year old mechanic is involved in a fight. He is hit on the head with a hammer. On, examination he had clinical evidence of an open depressed skull fracture and a GCS of, 6/15., You answered Observation, The correct answer is Urgent neurosurgical review (even before CT head performed), A patient with GCS <8 or = to 8 needs urgent neurosurgical review. Especially when an, open fracture is present., , 37., , A 67 year old retired lawyer falls down the stairs. His GCS is 15/15 and he has some, bruising over the mastoid., You answered Observation, The correct answer is CT head within 1 hour, This patient has a basal skull fracture, which is indicated by a positive Battle's sign. He, should have a CT head within 1h., , 38., , A 52 year old secretary falls down the stairs. She complains of neck pain. She has a GCS, of 15/15 and no neurology. She is unable to rotate her c-spine 45 degrees to the left and, right., You answered Observation, The correct answer is 3 view c-spine xray, In the January 2014 NICE guidance relating to the diagnosis of head and spinal injury the
Page 3362 :
evidence for initial imaging of the C spine was reviewed. The current UK practice is that, "low risk" patients with pain but no neurology undergo a 3 view C spine x-ray. The more, detailed 5 view x-ray was not found to be any better than 3 view films. In patients with, high risk injuries (which the patient in the scenario does not have) there is a likelihood that, 1 in 6 injuries would be missed on plain films alone and therefore CT scanning of the C, spine is recommended in this group., Please rate this question:, , Discuss and give feedback, , Next question, , Head injury management- NICE Guidelines, Summary of guidelines, , , , , , , All patients should be assessed within 15 minutes on arrival to A&E, Document all 3 components of the GCS, If GCS <8 or = to 8, consider stabilising the airway, Treat pain with low dose IV opiates (if safe), Full spine immobilisation until assessment if:, , - GCS < 15, - neck pain/tenderness, - paraesthesia extremities, - focal neurological deficit, - suspected c-spine injury, If a c-spine injury is suspected a 3 view c-spine x-ray is indicated. CT c-spine is preferred if:, - Intubated, - GCS <13, - Normal x-ray but continued concerns regarding c-spine injury, - Any focal neurology, - A CT head scan is being performed, - Initial plain films are abnormal, Immediate CT head (within 1 hour) if:, , , , , , , , , GCS < 13 on admission, GCS < 15 2 hours after admission, Suspected open or depressed skull fracture, Suspected skull base fracture (panda eyes, Battle's sign, CSF from nose/ear, bleeding ear), Focal neurology, Vomiting > 1 episode, Post traumatic seizure
Page 3364 :
A 28 year old African man is admitted with acute severe abdominal pain. He has just flown into the, UK long haul and the pain developed whilst in flight. On examination he is tender in the left upper, quadrant. His blood tests are as shown., Hb 6 g/dl, Reticulocyte count 15%., Ultrasound shows a spleen with a heterogeous texture and a few small gallstones but is otherwise, normal., What is the most likely diagnosis?, , Pancreatitis, , Parvovirus infection, , Sickle cell anaemia, , Pulmonary embolism, , Beta Thalassaemia minor, , A combination of a high reticulocyte count and severe anaemia indicates sickle cell anaemia,, however another differential can be of a transient aplastic crisis due to parvovirus. This is less likely, as this causes a reticulocytopenia rather than a reticulocytosis., Parvovirus B19 infects erythroid progenitor cells in the bone marrow and causes temporary, cessation of red blood cell production, patients who have underlying hematologic abnormalities are, at risk of cessation of red blood cell production if they become infected. This can result in a transient, aplastic crisis. Thus, patients with sickle cell anaemia are at risk. Typically, these patients have a, viral prodrome followed by anaemia, often with haemoglobin concentrations falling below 5.0 g/dL, and reticulocytosis., Please rate this question:, , Discuss and give feedback, , Next question, , Sickle cell anaemia, , , , , , , Autosomal recessive, Single base mutation, Deoxygenated cells become sickle in shape, Causes: short red cell survival, obstruction of microvessels and infarction, Sickling is precipitated by: dehydration, infection, hypoxia
Page 3365 :
, , , , Manifest at 6 months age, Africans, Middle East, Indian, Diagnosis: Hb electrophoresis, , Sickle crises, , , , , , , , , , Bone pain, Pleuritic chest pain: acute sickle chest syndrome commonest cause of death, CVA, seizures, Papillary necrosis, Splenic infarcts, Priapism, Hepatic pain, , Hb does not fall during a crisis, unless there is, , , , , , Aplasia: parvovirus, Acute sequestration, Haemolysis, , Long-term complications, , , , , , , , , Infections: Streptococcus pnemoniae, Chronic leg ulcers, Gallstones: haemolysis, Aseptic necrosis of bone, Chronic renal disease, Retinal detachment, proliferative retinopathy, , Surgical complications, , , , , , Bowel ischaemia, Cholecystitis, Avascular necrosis, , Management
Page 3367 :
Theme: Blood transfusion reactions, , A. Neutrophilic febrile reaction, B. Acute haemolytic transfusion reaction, C. Delayed haemolytic transfusion reaction, D. Pulmonary oedema, E. Sickle cell crisis, F. Transfusion associated lung injury, G. Graft vs. Host disease, , Please select the most likely underlying cause for each scenario. Each option may be used once,, more than once or not at all., , 40., , A 22 year old man is having a blood transfusion after losing blood from a peptic ulcer. He is, normally fit and well. Four hours after the transfusion; he complains of sudden onset shortness of, breath and chest pain. On examination his temperature is 37.2, saturations are 88% on air, blood, pressure 100/55 mmHg and HR 110 bpm. He has crepitations bilaterally up to the midzones. He is, given IV frusemide, but deteriorates and is admitted to ITU. A pulmonary catheter is inserted and, the PCWP is 10 mmHg., You answered Neutrophilic febrile reaction, The correct answer is Transfusion associated lung injury, The pulmonary catheter reading indicates that this is not a case of fluid overload (the PCWP, should be high, normal values PCWP systolic 7mmHg, diastolic 10mmHg). Transfusion associated, lung injury is a rare reaction causing neutrophilic mediated allergic pulmonary oedema. Patient's, have antibodies to donor leukocytes. It is important to consider this as a diagnosis when patients, don't respond to treatment for pulmonary oedema. Patients normally respond to supportive, therapy including fluids and oxygen., , 41., , A 32 year male with leukaemia attends the day unit for a blood transfusion. Five days after the, transfusion he attends A&E with a temperature of 38.5, erythroderma and desquamation.
Page 3368 :
You answered Neutrophilic febrile reaction, The correct answer is Graft vs. Host disease, This is associated with transfusion of unirradiated blood in immunosupressed patients., Transfusion associated GVHD can occur 4-30 days after a transfusion and follows a sub acute, pathway. Patients may also have diarrhoea and abnormal liver function tests. Management, involves steroid therapy., , 42., , A 22 year old man is having a blood transfusion after losing blood from haemorrhoids. He is, normally fit and well. 3h during the transfusion he complains of sudden onset abdominal pain and, nausea. His temperature is 39 degrees, Blood pressure 98/42 mmHg, HR 105 bpm and saturations, 94% air. His urine appears dark., You answered Neutrophilic febrile reaction, The correct answer is Acute haemolytic transfusion reaction, Rapid intravascular haemolysis leading to shock, DIC and death can occur with this reaction., , Please rate this question:, , Discuss and give feedback, , Next question, , Blood transfusion reactions, Acute transfusion reactions present as adverse signs or symptoms during or within 24 hours of a, blood transfusion. The most frequent reactions are fever, chills, pruritus, or urticaria, which typically, resolve promptly without specific treatment or complications. Other signs occurring in temporal, relationship with a blood transfusion, such as severe dyspnoea, pyrexia, or loss of consciousness, may be the first indication of a more severe potentially fatal reaction., The causes of adverse reactions are multi-factorial. Immune mediated reactions, some of the most, feared, occur as a result of component mismatch, the commonest cause of which is clerical error.
Page 3369 :
More common, non immune mediated, complications may occur as a result of product, contamination, this may be bacterial or viral., Transfusion related lung injury is well recognised and there are two proposed mechanisms which, underpin this. One involves the sequestration of primed neutrophils within the recipient pulmonary, capillary bed. The other proposed mechanism suggests that HLA mismatches between donor, neutrophils and recipient lung tissue is to blame., The table below summarises the main types of transfusion reaction., , Immune mediated, , Non immune mediated, , Pyrexia, , Hypocalcaemia, , Alloimmunization, , CCF, , Thrombocytopaenia, , Infections, , Transfusion associated lung injury, , Hyperkalaemia, , Graft vs Host disease, , Urticaria, , Acute or delayed haemolysis, , ABO incompatibility, , Rhesus incompatibility, Next question
Page 3370 :
A 49-year-old male sustained a severe blunt injury just below the bridge of the nose with industrial, machinery. Imaging demonstrates a fracture involving the superior orbital fissure. On examination an, ipsilateral pupillary defect is present and loss of the corneal reflexes. In addition to these, examination findings, which of the following will not be present?, , Altered cutaneous sensation from the forehead to the vertex, , Ptosis, , Complete opthalmoplegia, , Nystagmus, , Enopthalmos, Orbital apex syndrome, This is an extension of superior orbital fissure syndrome and includes compression of the optic nerve, passing through the optic foramen. It is indicated by features of superior orbital fissure syndrome, and ipsilateral afferent pupillary defect., This type of injury will result in the orbital apex syndrome (See above). As such opthalmoplegia will, be present and nystagmus cannot occur., Please rate this question:, , Discuss and give feedback, , Next question, , Craniomaxillofacial injuries, Craniomaxillofacial injuries in the UK are due to:, , , , , , Interpersonal violence (52%), Motor vehicle accidents (16%), Sporting injuries (19%), Falls (11%), , Le Fort Fractures, , Grade, , Feature
Page 3371 :
Grade, , Feature, , Le, Fort 1, , The fracture extends from the nasal septum to the lateral pyriform rims, travels, horizontally above the teeth apices, crosses below the zygomaticomaxillary junction, and, traverses the pterygomaxillary junction to interrupt the pterygoid plates., , Le, Fort 2, , These fractures have a pyramidal shape and extend from the nasal bridge at or below the, nasofrontal suture through the frontal process of the maxilla, inferolaterally through the, lacrimal bones and inferior orbital floor and rim through or near the inferior orbital, foramen, and inferiorly through the anterior wall of the maxillary sinus; it then travels, under the zygoma, across the pterygomaxillary fissure, and through the pterygoid plates., , Le, Fort 3, , These fractures start at the nasofrontal and frontomaxillary sutures and extend posteriorly, along the medial wall of the orbit through the nasolacrimal groove and ethmoid bones., The thicker sphenoid bone posteriorly usually prevents continuation of the fracture into, the optic canal. Instead, the fracture continues along the floor of the orbit along the, inferior orbital fissure and continues superolaterally through the lateral orbital wall,, through the zygomaticofrontal junction and the zygomatic arch. Intranasally, a branch of, the fracture extends through the base of the perpendicular plate of the ethmoid, through, the vomer, and through the interface of the pterygoid plates to the base of the sphenoid., This type of fracture predisposes the patient to CSF rhinorrhea more commonly than the, other types., , Ocular injuries, Superior orbital fissure syndrome, Severe force to the lateral wall of the orbit resulting in compression of neurovascular structures., Results in :, , , , , , Complete opthalmoplegia and ptosis (Cranial nerves 3, 4, 6 and nerve to levator palpebrae, superioris), Relative afferent pupillary defect, Dilatation of the pupil and loss of accommodation and corneal reflexes, Altered sensation from forehead to vertex (frontal branch of trigeminal nerve), , Orbital blow out fracture, Typically occurs when an object of slightly larger diameter than the orbital rim strikes the, incompressible eyeball. The bone fragment is displaced downwards into the antral cavity, remaining, attached to the orbital periosteum. Periorbital fat may be herniated through the defect, interfering, with the inferior rectus and inferior oblique muscles which are contained within the same fascial, sheath. This prevents upward movement and outward rotation of the eye and the patient, experiences diplopia on upward gaze. The initial bruising and swelling may make assessment, difficult and patients should usually be reviewed 5 days later. Residual defects may require orbital
Page 3372 :
floor reconstruction., Nasal Fractures, , , , , , , Common injury, Ensure new and not old deformity, Control epistaxis, CSF rhinorrhoea implies that the cribriform plate has been breached and antibiotics will be, required., Usually best to allow bruising and swelling to settle and then review patient clinically. Major, persistent deformity requires fracture manipulation, best performed within 10 days of injury., , Retrobulbar haemorrhage, Rare but important ocular emergency. Presents with:, , , , , , , Pain (usually sharp and within the globe), Proptosis, Pupil reactions are lost, Paralysis (eye movements lost), Visual acuity is lost (colour vision is lost first), , May be the result of Le Fort type facial fractures., Management:, , , , , , Mannitol 1g/Kg as 20% infusion, Osmotic diuretic, Contra-indicated in congestive heart, failure and pulmonary oedema, Acetazolamide 500mg IV, (Monitor FBC/U+E) Reduces aqueous pressure by inhibition of, carbonic anhydrase (used in glaucoma), Dexamethasone 8mg orally or intravenously, In a traumatic setting an urgent cantholysis may be needed prior to definitive surgery., , Consider, Papaverine 40mg smooth muscle relaxant, Dextran 40 500mls IV improves perfusion, Next question
Page 3373 :
Which option is not recommended during the management of compartment syndrome?, , Anticoagulation, , Keep limb level with the body, , Intravenous fluids, , Pain control, , Fasciotomy, , Anticoagulation will worsen compartment syndrome., Please rate this question:, , Discuss and give feedback, , Next question, , Compartment syndrome, , , , This is a particular complication that may occur following fractures (or following ischaemia reperfusion injury in vascular patients). It is characterised by raised pressure within a closed, anatomical space., The raised pressure within the compartment will eventually compromise tissue perfusion, resulting in necrosis. The two main fractures carrying this complication include supracondylar, fractures and tibial shaft injuries., , Symptoms and signs, , , , , , , Pain, especially on movement (even passive), Parasthesiae, Pallor may be present, Arterial pulsation may still be felt as the necrosis occurs as a result of microvascular, compromise, Paralysis of the muscle group may occur, , Diagnosis
Page 3374 :
, , Is made by measurement of intracompartmental pressure measurements. Pressures in, excess of 20mmHg are abnormal and >40mmHg is diagnostic., , Treatment, , , , , , , This is essentially prompt and extensive fasciotomies, In the lower limb the deep muscles may be inadequately decompressed by the, inexperienced operator when smaller incisions are performed, Myoglobinuria may occur following fasciotomy and result in renal failure and for this reason, these patients require aggressive IV fluids, Where muscle groups are frankly necrotic at fasciotomy they should be debrided and, amputation may have to be considered, Death of muscle groups may occur within 4-6 hours, Next question
Page 3375 :
Theme: Complications of burns, , A., B., C., D., E., F., G., H., I., , Deep vein thrombosis, Curlings Ulcer, Contracture, Type I respiratory failure, Type II respiratory failure, Toxic shock syndrome, Compartment syndrome, Rhabdomyolysis, Disseminated intravascular coagulation, , For each clinical scenario please select the most likely complication to have occurred. Each option, may be used once, more than once or not at all., , 45., , A 10 year old child is admitted with severe 30% burns following a house fire. After wound, cleaning and dressings he is admitted to critical care. 1 day following skin grafts he, becomes tachycardic and hypotensive. He vomits twice and this shows evidence of, haematemesis, You answered Deep vein thrombosis, The correct answer is Curlings Ulcer, Stress ulcers may occur in the duodenum of burns patients and are more common in, children., , 46., , A 26 year old electrician suffers a full thickness high voltage burn to his leg. On routine, urine analysis he has + blood. His U+E's show mild hyperkalaemia and a CK of 3000, You answered Deep vein thrombosis, The correct answer is Rhabdomyolysis, Electrical high voltage burns are associated with rhabdomyolysis. Acute tubular necrosis, may occur. Aggressive IV fluids should be given, , 47., , A 45 year old man is admitted after his clothing caught fire. He suffers a full thickness, circumferential burn to his lower thigh. He complains of increasing pain in lower leg and, on examination there is parasthesia and severe pain in the lower leg. Foot pulses are, normal, You answered Deep vein thrombosis
Page 3376 :
The correct answer is Compartment syndrome, Circumferential burns may constrict the limb and cause a compartment syndrome to, develop. Eshcarotomy is required, and compartmental decompression., Please rate this question:, , Discuss and give feedback, , Next question, , Burns, Burns may be thermal, chemical or electrical. In the former category are burns which occur as a, result of heat. Chemical burns occur when the skin is exposed to an extremely caustic or alkaline, substance. Electrical burns occur following exposure to electrical current. The immediate, management includes removal of the burning source which usually includes irrigation of the burned, area. A detailed assessment then needs to be made of the extent of the burns and a number of, charts are available for recording this information. The degree of injury relates to the temperature, and duration of exposure. Most domestic burns are mainly scalds in young children., Following the burn, there is a local response with progressive tissue loss and release of, inflammatory cytokines. Systemically, there are cardiovascular effects resulting from fluid loss and, sequestration of fluid into the third space. There is a marked catabolic response. Immunosupression, is common with large burns and bacterial translocation from the gut lumen is a recognised event., Sepsis is a common cause of death following major burns., Types of burn, , Type of burn, , Skin layers, affected, , Skin, appearance, , Blanching, , Management, , Epidermal/Superficial, , Epidermis, , Red, moist, , Yes, , Superficial partial, thickness, , Epidermis and part, of papillary dermis, affected, , Pale, dry, , Yes, , Normally heals, with no, intervention, , Deep partial thickness, , Epidermis, whole, papillary dermis, affected, , Mottled red, colour, , No, , Needs surgical, intervention, (depending on site)
Page 3377 :
Full thickness, , Whole skin layer, and subcutaneous, tissue affected, , Dry, leathery, hard wound, , No, , Burns centre, , Depth of burn assessment, , , , , , Bleeding on needle prick, Sensation, Appearance, Blanching to pressure, , Percentage burn estimation, Lund Browder chart: most accurate even in children, Wallace rule of nines, Palmar surface: surface area palm = 0.8% burn, >15% body surface area burns in adults needs urgent burn fluid resuscitation, Transfer to burn centre if:, , , , , , Need burn shock resuscitation, Face/hands/genitals affected, Deep partial thickness or full thickness burns, Significant electrical/chemical burns, , Management, The initial aim is to stop the burning process and resuscitate the patient. Intravenous fluids will be, required for children with burns greater than 10% of total body surface area. Adults with burns, greater than 15% of total body surface area will also require IV fluids. The fluids are calculated using, the Parkland formula which is; volume of fluid= total body surface area of the burn % x weight (Kg), x4. Half of the fluid is administered in the first 8 hours. A urinary catheter should be inserted., Analgesia should be given. Complex burns, burns involving the hand perineum and face and burns, >10% in adults and >5% in children should be transferred to a burns unit., Circumferential burns affecting a limb or severe torso burns impeding respiration may require, escharotomy to divide the burnt tissue., Conservative management is appropriate for superficial burns and mixed superficial burns that will, heal in 2 weeks. More complex burns may require excision and skin grafting. Excision and primary, closure is not generally practised as there is a high risk of infection., There is no evidence to support the use of anti microbial prophylaxis or topical antibiotics in burn, patients., Escharotomies
Page 3379 :
A 23 year old man who plays rugby for a hobby presents with recurrent anterior dislocation of the, shoulder. Which of the following abnormalities is most likely to be present to account for this?, , Rotator cuff tear, , Biceps tendon rupture, , Bankart lesion, , Axillary nerve injury, , Infraspinatus tendinitis, A Bankart lesion is an injury of the anterior (inferior) glenoid labrum of the shoulder due to anterior, shoulder dislocation. When this happens, a pocket at the front of the glenoid forms that allows the, humeral head to dislocate into it., Anterior dislocations are the most common. When recurrent, a Bankart lesion is the most common, underlying abnormality. This is usually visualised by CT and MRI scanning and often repaired, arthroscopically., Please rate this question:, , Discuss and give feedback, , Next question, , Shoulder disorders, Shoulder fractures and dislocations, Fractures, Proximal humerus, Background, , , , , Third most common fragility fracture in the elderly., Results from low energy fall in predominantly elderly females, or from high energy trauma in, young males., Can be associated with nerve injury (commonly axillary), and fracture-dislocation of the, humeral head. Detailed neurological assessment is essential for all upper limb injuries., , Anatomy, Osteology, Consists of articular head, greater tuberosity, lesser tuberosity, metaphysis and diaphysis. Between
Page 3380 :
the articular head and the tuberosities is the anatomical neck (previous physis). Between the, tuberosities and the metaphysis is the surgical neck., The supraspinatus, infraspinatus and teres minor muscles attach to the greater tuberosity. The, subscapularis muscle attaches to the lesser tuberosity., Vascular Supply, Humeral head is supplied by the anterior and posterior humeral circumflex arteries. Anatomical neck, fractures are at greatest risk of osteonecrosis., Imaging, Imaging aims to both delineate the fracture pattern, and confirm/exlude the presence of an, associated dislocation., , , , Radiographs - True anteroposterior (AP), axillary lateral and/or scapula Y view., CT - indicated to better define intra-articular involvement and to aid pre-operative planning., MRI is not useful for fracture imaging., , Classification, Description of the fracture is often more useful than classification. Particular attention should be paid, to humeral alignment, fracture displacement, and greater tuberosity position (rotator cuff will pull the, GT supero-posterioly, which can cause impingement problems with malunion)., - Neer Classification: Most commonly used. Describes fracture as 2,3,or 4 part depending upon the, number main fragments. Also comments on the degree of displacement. Fragments:, -greater tuberosity, -lesser tuberosity, - articular surface, - shaft, Displacement: >1cm or angulation >45 degrees., Treatment, The vast majority of proximal humeral fractures are minimally displaced, and therefore can be, managed conservatively. This involves immobilisation in a polysling, and progressive mobilisation., Pendular exercise can commence at 14 days, and active abduction from 4-6 weeks., Irreducible fracture dislocation is an indication for operative management. Other indications include, large displacement, younger patient, head splitting (intra-articular fractures). However, the recent, PROFHER trial (1) has suggested no benefit to operative intervention on patient outcome (it must be, applied cautiously as majority of patients were elderly with extraarticular fractures). Options available, for surgical management include:, , ORIF, , Most commonly used. Plate and screw fixation. Can reconstruct, complex fractures., , Intramedullary nail, , Suitable for extra-articular configuration, predominantly surgical neck, +/- GT fractures.
Page 3381 :
Hemiarthroplasty, , Used for un-reconstructable fractures in the older patient who has good, glenoid quality., , Total shoulder, arthroplasty, , Unconstructable fractures where high functioning shoulder is required, (hemiarthroplasty will cause glenoid erosion), , Reverse shoulder, arthroplasty, , Total shoulder arthroplasty that provides better functional outcome than, conventional total shoulder replacement., , Scapula, Background, Uncommon fractures usually associated with high energy trauma. Most commonly involve scapula, body or spine (50%), glenoid fossa and glenoid neck. Important to exclude associated life, threatening injury., Imaging, Plain radiographs should include true anteroposterior (AP), axillary lateral and/or scapula Y view. CT, scanning is useful for defining intra-articular involvement, displacement and for three dimensional, reconstruction., Classification, Based on the location of the fracture (coracoid, acromion, glenoid neck, glenoid fossa, scapula, body). Beware of ipsilateral glenoid neck and clavicle fracture -floating shoulder - where limb is, effectively dissociated from axial skeleton., Treatment, The vast majority of scapula fractures are amenable to conservative management, consisting of, sling immobilisation for two weeks followed by early rehabilitation. Floating shoulder will usually, require fixation, and consideration of surgery should also be given to intra-articular and, displaced/angulated glenoid fractures., Dislocations, Types, Dislocations around the shoulder joint include glenohumeral dislocation, acromioclavicular joint, disruption and sternoclavicular dislocation. Only glenohumeral dislocation will be covered here., Glenohumeral dislocation, Diagnosis, classification and management are covered here., Background, Shoulder dislocation is commonly seen in A&E. It has a high recurrence rate that is as high as 80%, in teenagers. Initial management requires emergent reduction to prevent lasting chondral damage., Early assessment and management
Page 3382 :
Usually a traumatic cause (multi-directional instability in frequent dislocations requires discussion, with orthopaedics and is not covered here). Careful history, examination and documentation of, neurovascular status of the limb, in particular the axillary nerve (regimental badge sensation). This, should be re-assessed post manipulation. Early radiographs to confirm direction of dislocation., Initial management consists of emergent closed reduction under under entanox and analgesia, but, often requires conscious sedation. Arm should then be immobilised in a polysling, and XR to confirm, relocation., Imaging - True anteroposterior (AP), axillary lateral and/or scapula Y view. Reduced humeral head, should lie between acromion and coracoid on lateral/scapula view., Types, , Direction, , Features, , Cause, , Examination, , Reduction, techniques, , Anterior, , Most, Common, >90%, , Usually traumatic - anterior, force on arm when shoulder, is abducted, eternally, rotated, , Loss of shoulder, contour - sulcus sign., Humeral head can be, felt anteriorly., , Hippocratic., Milch., Stimson., Kocher not, advised due to, complication of, fracture, , Posterior, , 50%, missed in, A&E, , 50% traumatic, but, classically post seizure or, electrocution, , Shoulder locked in, internal rotation. XR, may show lightbulb, appearance., , Gentle lateral, traction to, adducted arm., , Inferior, , Rare, , Associated with pectorals, and rotator cuff tears, and, glenoid fracture, , As for primary injury, , Management of, primary injury, , Rare, , Associated with, acrominon/clavicle fracture, , As for primary injury, , Management of, primary injury, , Superior, , Associated injuries
Page 3383 :
, , , , , , Bankart lesion - avulsion of the anterior glenoid labrum with an anterior shoulder dislocation, (reverse Bankart if poster labrum in posterior dislocation)., Hill Sachs defect - chondral impaction on posteriosuperior humeral head from contact with, gleonoid rim. Can be large enough to lock shoulder, requiring open reduction. (Reverse Hill, Sachs in posterior dislocation)., Rotator cuff tear - increases with age., Greater or lesser tuberosity fracture - increases with age., Humeral neck fracture - shoulder fracture dislocation. More common in high energy trauma, and elderly. Should be discussed with orthopaedics prior to any attempted reduction., , Rotator Cuff Disease, Rotator cuff disease is a spectrum of conditions that ranges from subacromial impingement to rotator, cuff tears and eventually to rotator cuff arthropathy (arthritis)., Anatomy, The rotator cuff is a group of four muscles that are important in shoulder movements, and, maintenance of glenohumeral stability., , Scapular, attachment, , Humeral, attachment, , Supraspinatus, , Supraspinatus, fossa, , Infraspinatus, , Muscle, , Action, , Innervation, , Superior facet of, greater tuberosity, , Initiation of, abduction of, humerus, , Suprascapular nerve, , Infraspinatus, fossa, , Posterior facet of, greater tuberosity, , External rotation, of humerus, , Suprascapular nerve, , Teres Minor, , Lateral border, , Inferior facet of, greater tuberosity, , External rotation, of humerus, , Axillary Nerve, , Subscapularis, , Subscapular, fossa, , Lesser tuberosity, , Internal rotation, of humerus, , Upper and lower, subscapular nerve, , , , , The inferior rotator cuff muscles (infraspinatus, teres minor, and subscapularis) balance the, superior pull of the deltoid. Injury/tear results in upward migration of the humeral head on the, glenoid (can be seen on AP radiograph)., Likewise, the anterior muscles (subscapularis) are balanced with the posterior muscles, (infraspinatus, teres minor).
Page 3384 :
Subacromial Impingement, , , , , , The most common cause of shoulder pain, which results from impingement of the superior, cuff on the undersurface of the acromion, and an inflammatory bursitis., Associated with certain types of acromial morphology (Bigliani classification)., Presents as insidious pain which is exacerbated by overhead activities., , Rotator Cuff Tear, , , , , , Often presents as an acute event on the background of chronic subacromial impingement in, the older patient, but can present as an avulsion injury in younger patients., Majority of tears are to the superior cuff (supraspinatus, infraspinatus, teres minor), though a, tear to subscapularis is associated with subcoracoid impingement., Tears present as pain and weakness when using the muscles in question., , Rotator Cuff Arthropathy, , , , , Defined as shoulder arthritis in the setting of rotator cuff dysfunction. Results from superior, migration due to the loss of rotator cuff function and integrity. Unopposed deltoid pulls the, humeral head superiorly., Associated with massive chronic cuff tears., , Imaging, Plain radiographs, , , , AP of the shoulder may show superior migration of the humerus with a cuff tear, and features, of arthritis with arthropathy. Other causes of pain may also be identified (e.g. calcific, tendonitis/fracture), Outlet view is useful for defining the acromial morphology, , USS, , , MRI, , Allows dynamic imaging of the cuff, and is inexpensive. However, it is very user dependent.
Page 3385 :
, , , Best imaging modality for cuff pathology., Also allows imaging of the rest of the shoulder. When intra-articular pathology is suspected,, can be combined with an arthrogram for improved sensitivity and specificity., , Treatment, Subacromial impingement, , , , , Physiotherapy, oral anti-inflammatory medication, Subacromial steroid injection can settle inflammation, Arthroscopic subacromial decompression by shaving away the undersurface of the, acromion, more space is created for the rotator cuff. Cuff integrity is assessed also at time of, surgery, and can be repaired if necessary., , Rotator cuff tear, , , , , When considering repair of a cuff tear, the age and activity of the patient, the nature of the, tear (degenerative vs. acute traumatic), and the size and retraction of the tear should be, considered when making a surgical plan., Mild tears or tears in the elderly can be managed conservatively, as outlined above., Moderate tears can be repaired arthroscopically. Massive or retracted tears will often require, an open repair (occasionally with a tendon transfer). Subacromial decompression is, performed at the same time to reduce impingement, symptoms and recurrence., , Calcific tendonitis, Calcific tendonitis involves calcific deposits within tendons anywhere in the body, but most, commonly in the rotator cuff (specifically the supraspinatus tendon). When present in the shoulder, it, is associated with subacromial impingement and pain., Pathology, , , , More common in women aged 30-60 years., Association with diabetes and hypothyroidism, , There are three stages of calcification, , , , , Formative phase characterized by calcific deposits, Resting phase deposit is stable, but presents with impingement problems, Resorptive phase phagocytic resorption. Most painful stage., , Presentation
Page 3386 :
, , Similar in presentation to subacromial impingement, with pain especially with over head, activities. Atraumatic in nature., , Imaging, , , Plain radiographs show calcification of the rotator cuff, usually within 1.5cm of its insertion on, the humerus. Supraspinatus outlet views can show level of impingment. Further imaging is, rarely needed., , Treatment, , , , Non-operative NSAIDS, steroid injection (controversial, but practiced) and physiotherapy., Approximately 75% will resolve by 6 months with conservative management., Ultrasound guided or surgical needle barbotage can break down deposits and resolve, symptoms. Occasionally surgical excision is required., , Adhesive capsulitis (Frozen Shoulder), , , , , Pain and loss of movement of shoulder joint, which involves fibroplastic proliferation of, capsular tissue, causing soft tissue scarring and contracture. Patients present with a painful, and decreased arc of motion., Associated with prolonged immobilization, previous surgery, thyroid disorders (AI) and, diabetes, Classically three stages which can take up to two years to resolve:, , Stage one the freezing and painful stage, Stage two the frozen and stiff stage, Stage three the thawing stage, where shoulder movement slowly improves, Imaging, , , , Plain radiographs to exclude other causes of a painful shoulder, MRI arthrogram may show capsular contracture, and again may be used to exclude cuff, pathology. However, often not performed as diagnosis is largely clinical., , Treatment, , , , Non-operative NSAIDS, steroid injection and physiotherapy. Patience is required as, condition can take up to 2 years to improve., Operative MUA or arthroscopic adhesiolysis (release of adhesions) can expedite recovery,, followed by intensive physiotherapy.
Page 3387 :
Glenohumeral Arthritis, Shoulder arthritis presents with the normal symptoms of arthritis, however primary osteoarthritis is, not as commonly the primary cause as seen in other large joints.. A large proportion of shoulder, arthritis is rheumatoid (RA), post traumatic, or secondary to rotator cuff arthropathy (discussed, above)., Treatment, , , Surgical options include hemiarthroplasty, total shoulder replacement and reverse geometry, total shoulder replacement (used when rotator cuff function is absent)., , References, 1. JAMA. 2015;313(10):1037-1047. doi:10.1001/jama.2015.1629, Next question
Page 3388 :
A 44 year old man is involved in a road traffic accident. He suffers significant injuries to his thorax,, he has bilateral haemopneumothoraces and a suspected haemopericardium. He is to undergo, surgery, what is the best method of accessing these injuries?, , Bilateral thoracoscopy and mediastinoscopy, , Midline sternotomy, , Bilateral posterolateral thoracotomy, , Clam shell thoracotomy, , None of the above, , Patients with significant mediastinal and lung injuries are best operated on using a Clam shell, thoracotomy. All modes of access involve a degree of compromise. A sternotomy would give good, access to the heart. However, it takes longer to perform and does not provide good access to the, lungs. Trauma should not be managed using laparoscopy., Please rate this question:, , Discuss and give feedback, , Next question, , Trauma management, The cornerstone of trauma management is embodied in the principles of ATLS., Following trauma there is a trimodal death distribution:, , , , , Immediately following injury. Typically as result of brain or high spinal injuries, cardiac or, great vessel damage. Salvage rate is low., In early hours following injury. In this group deaths are due to phenomena such as splenic, rupture, sub dural haematomas and haemopneumothoraces, In the days following injury. Usually due to sepsis or multi organ failure., , Aspects of trauma management, , , , ABCDE approach., Tension pneumothoraces will deteriorate with vigorous ventilation attempts.
Page 3389 :
, , , , External haemorrhage is managed as part of the primary survey. As a rule tourniquets, should not be used. Blind application of clamps will tend to damage surrounding structures, and packing is the preferred method of haemorrhage control., Urinary catheters and naso gastric tubes may need inserting. Be wary of basal skull fractures, and urethral injuries., Patients with head and neck trauma should be assumed to have a cervical spine injury until, proven otherwise., , Thoracic injuries, , , , , , , , , , Simple pneumothorax, Mediastinal traversing wounds, Tracheobronchial tree injury, Haemothorax, Blunt cardiac injury, Diaphragmatic injury, Aortic disruption, Pulmonary contusion, , Management of thoracic trauma, , , , , , , , , , , , Simple pneumothorax insert chest drain. Aspiration is risky in trauma as pneumothorax, may be from lung laceration and convert to tension pneumothorax., Mediastinal traversing wounds These result from situations like stabbings. Exit and entry, wounds in separate hemithoraces. The presence of a mediastinal haematoma indicates the, likelihood of a great vessel injury. All patients should undergo CT angiogram and, oesophageal contrast swallow. Indications for thoracotomy are largely related to blood loss, and will be addressed below., Tracheobronchial tree injury Unusual injuries. In blunt trauma most injuries occur within, 4cm of the carina. Features suggesting this injury include haemoptysis and surgical, emphysema. These injuries have a very large air leak and may have tension pneumothorax., Haemothorax Usually caused by laceration of lung vessel or internal mammary artery by rib, fracture. Patients should all have a wide bore 36F chest drain. Indications for thoracotomy, include loss of more than 1.5L blood initially or ongoing losses of >200ml per hour for >2, hours., Cardiac contusions Usually cardiac arrhythmias, often overlying sternal fracture. Perform, echocardiography to exclude pericardial effusions and tamponade. Risk of arrhythmias falls, after 24 hours., Diaphragmatic injury Usually left sided. Direct surgical repair is performed., Traumatic aortic disruption Commonest cause of death after RTA or falls. Usually, incomplete laceration near ligamentum arteriosum. All survivors will have contained, haematoma. Only 1-2% of patients with this injury will have a normal chest x-ray., Pulmonary contusion Common and lethal. Insidious onset. Early intubation and ventilation., , Abdominal trauma
Page 3390 :
, , , , , , , , , Deceleration injuries are common., In blunt trauma requiring laparotomy the spleen is most commonly injured (40%), Stab wounds traverse structures most commonly liver (40%), Gunshot wounds have variable effects depending upon bullet type. Small bowel is most, commonly injured (50%), Patients with stab wounds and no peritoneal signs up to 25% will not enter the peritoneal, cavity, Blood at urethral meatus suggests a urethral tear, High riding prostate on PR = urethral disruption, Mechanical testing for pelvic stability should only be performed once, , Investigations in abdominal trauma, , Diagnostic Peritoneal, Lavage, , Abdominal CT scan, , USS, , Indication, , Document bleeding if, hypotensive, , Document organ injury if, normotensive, , Document fluid if, hypotensive, , Advantages, , Early diagnosis and, sensitive; 98% accurate, , Most specific for, localising injury; 92 to, 98% accurate, , Early diagnosis, non, invasive and repeatable;, 86 to 95% accurate, , Disadvantages, , Invasive and may miss, retroperitoneal and, diaphragmatic injury, , Location of scanner away, from facilities, time taken, for reporting, need for, contrast, , Operator dependent and, may miss, retroperitoneal injury, , , , , Amylase may be normal following pancreatic trauma, Urethrography if suspected urethral injury, Next question
Page 3391 :
A 63 year old male is admitted to the surgical ward for an elective femoral popliteal bypass. He, suddenly starts complaining of central, crushing chest pain which is radiating to the left arm. The, Nursing staff start high flow oxygen and give a spray of glyceryl trinitrate spray. Unfortunately there, is no relief of symptoms. What is the next agent to be administered?, , Aspirin 75mg, , Clopidogrel 75mg, , Aspirin 300mg, , Clopidogrel 300mg, , Direct admission to angiography suite, , Aspirin 300mg should be given as soon as possible. If the patient has a moderate to high risk of, myocardial infarction, then Clopidogrel should be given with a low molecular weight heparin., Thromboloysis or urgent percutaneous intervention should be given if there are significant ECG, changes., Please rate this question:, , Discuss and give feedback, , Next question, , Management of acute coronary syndrome, NICE produced guidelines in 2010 on the management of unstable angina and non-ST elevation, myocardial infarction (NSTEMI). They advocate managing patients based on the early risk, assessment using a recognised scoring system such as GRACE (Global Registry of Acute Cardiac, Events) to calculate a predicted 6 month mortality., All patients should receive, - aspirin 300mg
Page 3392 :
- nitrates or morphine to relieve chest pain if required, Whilst it is common that non-hypoxic patients receive oxygen therapy there is little evidence to, support this approach. The 2008 British Thoracic Society oxygen therapy guidelines advise not, giving oxygen unless the patient is hypoxic., Antithrombin treatment. Low molecular weight heparin should be offered to patients who are not at, a high risk of bleeding and who are not having angiography within the next 24 hours. If angiography, is likely within 24 hours or a patients creatinine is > 265 umol/l unfractionated heparin should be, given., Clopidogrel 300mg should be given to patients with a predicted 6 month mortality of more than, 1.5% or patients who may undergo percutaneous coronary intervention within 24 hours of admission, to hospital. Clopidogrel should be continued for 12 months., Intravenous glycoprotein IIb/IIIa receptor antagonists (eptifibatide or tirofiban) should be given to, patients who have an intermediate or higher risk of adverse cardiovascular events (predicted 6month mortality above 3.0%), and who are scheduled to undergo angiography within 96 hours of, hospital admission., Coronary angiography should be considered within 96 hours of first admission, to hospital to patients who have a predicted 6-month mortality above 3.0%. It should also be, performed as soon as possible in patients who are clinically unstable., Next question
Page 3393 :
Which of the following is not a change found on an ECG in acute pulmonary embolism?, , No changes, , J waves, , P pulmonale, , Right ventricular strain, , T wave inversion in the inferior leads, S1, Q3, T3, J waves are pathognomonic of hypothermia., Please rate this question:, , Discuss and give feedback, , Next question, , Pulmonary Embolism: ECG changes, , , , , , , , , , No changes, S1, Q3, T3, Tall R waves: V1, P pulmonale (peaked P waves): inferior leads, Right axis deviation, Right bundle branch block, Atrial arrhythmias, T wave inversion: V1, V2, V3, Right ventricular strain: if identified is associated with adverse short-term outcome and adds, prognostic value to echocardiographic evidence of right ventricular dysfunction in patients, with acute pulmonary embolism and normal blood pressure., , References, Vanni S et al. Prognostic value of ECG among patients with acute pulmonary embolism and normal, blood pressure. Am J Med. 2009 Mar;122(3):257-64., Next question
Page 3394 :
A 21 year old man falls down a ravine whilst skiing and is trapped for several hours. He is finally, brought to the emergency department profoundly hypothermic with a core temperature of 29 oC., Which method is most effective at raising the core temperature?, , Re-warming with electric blankets, , Increasing the room temperature, , Instillation of warm intravesical fluid, , Instillation of warmed rectal fluid, , Instillation of warmed intra peritoneal fluid, , Theme from 2011 Examination, Visceral cavity re-warming be it lung or abdomen (or both) provides rapid rewarming. Only, extracorporeal circulatory devices provide faster rates of re-warming., Please rate this question:, , Discuss and give feedback, , Next question, , Hypothermia, Core body temperature below 35oC. Severe hypothermia is present when the core temperature is, below 30oC. Hypothermia is associated with a reduction in both respiratory and cardiac activity., Management, An organised cardiac rhythm may be converted to fibrillation if CPR is attempted inappropriately so, ECG should be analysed with care. The rewarming technique used depends upon the degree of, hypothermia and the physiological state of the patient. Mild hypothermia may respond to external, rewarming devices. Severe hypothermia may require active core rewarming techniques such as, peritoneal lavage, haemodialysis or cardiac bypass. Patients who develop cardiac arrhythmias who
Page 3395 :
are severely hypothermic may respond to bretylium toslyte (sadly no longer available in most, centres), but do not generally respond to standard therapies or DC cardioversion., Next question
Page 3397 :
Discuss and give feedback, , Next question, , Addisonian crisis, Causes, , , , , Sepsis or surgery causing an acute exacerbation of chronic insufficiency (Addison's,, Hypopituitarism), Adrenal haemorrhage eg Waterhouse-Friderichsen syndrome (fulminant meningococcemia), Steroid withdrawal, , Management, , , , , , Hydrocortisone 100 mg im or iv, 1 litre normal saline infused over 30-60 mins or with dextrose if hypoglycaemic, Continue hydrocortisone 6 hourly until the patient is stable. No fludrocortisone is required, because high cortisol exerts weak mineralocorticoid action, Oral replacement may begin after 24 hours and be reduced to maintenance over 3-4 days, Next question
Page 3398 :
Theme: Thoracic trauma, , A., B., C., D., E., F., G., , Thoracotomy, Manage conservatively, Intercostal tube drain insertion, CT scanning, Bronchoscopy, Negative pressure intercostal tube drainage, Video assisted thoracoscopy and pleurectomy, , For each of the following scenarios please select the most appropriate management option from the, list. Each option may be used once, more than once or not at all., , 54., , A 28 year old male is involved in a road traffic accident he is thrown from his motorbike, onto the pavement and sustains a haemopneumothorax and flail segment of the right chest., You answered Thoracotomy, The correct answer is Intercostal tube drain insertion, He requires a chest drain and analgesia. In general all haemopneumothoraces should be, managed by intercostal chest drain insertion as they have a risk of becoming a tension, pneumothorax until the lung laceration has sealed., , 55., , A 19 year old man is stabbed in the chest at a nightclub. He develops a cardiac arrest in, casualty following an attempted transfer to the CT scanning room., Thoracotomy, This is one indication for an 'emergency room' thoracotomy, there are not many others!, Typical injuries include ventricular penetration, great vessel disruption and hilar lung, injuries., , 56., , A 32 year old male falls over and sustains a small pneumothorax following a simple rib, fracture. He has no physiological compromise., You answered Thoracotomy, The correct answer is Intercostal tube drain insertion, Unlike spontaneous pneumothoraces most would advocate chest tube drainage in the, context of pneumothorax resulting from trauma. This is because of the risk of the lung, laceration developing a tension. Once there is no further evidence of air leak the chest
Page 3399 :
drain may be removed and a check x-ray performed to check there is no re-accumulation, prior to discharge., Please rate this question:, , Discuss and give feedback, , Next question, , Thoracic trauma, Types of thoracic trauma, , Tension, pneumothorax, , , , , , , Flail chest, , , , , , , , Often laceration to lung parenchyma with flap, Pressure develops in thorax, Most common cause is mechanical ventilation in patient with, pleural injury, Symptoms overlap with cardiac tamponade, hyper-resonant, percussion note is more likely in tension pnemothorax, Chest wall disconnects from thoracic cage, Multiple rib fractures (at least two fractures per rib in at least two, ribs), Associated with pulmonary contusion, Abnormal chest motion, Avoid over hydration and fluid overload, , Pneumothorax, , , , , , Most common cause is lung laceration with air leakage, Most traumatic pneumothoraces should have a chest drain, Patients with traumatic pneumothorax should never be, mechanically ventilated until a chest drain is inserted, , Haemothorax, , , , Most commonly due to laceration of lung, intercostal vessel or, internal mammary artery, Haemothoraces large enough to appear on CXR are treated with, large bore chest drain, Surgical exploration is warranted if >1500ml blood drained, immediately, , , , , Cardiac tamponade, , , , Beck's triad: elevated venous pressure, reduced arterial pressure,, reduced heart sounds
Page 3400 :
, , , Pulsus paradoxus, May occur with as little as 100ml blood, , Pulmonary contusion, , , , , , Most common potentially lethal chest injury, Arterial blood gases and pulse oximetry important, Early intubation within an hour if significant hypoxia, , Blunt cardiac injury, , , , , , Usually occurs secondary to chest wall injury, ECG may show features of myocardial infarction, Sequelae: hypotension, arrhythmias, cardiac wall motion, abnormalities, , Aorta disruption, , , , , , Deceleration injuries, Contained haematoma, Widened mediastinum, , Diaphragm, disruption, , , , Most due to motor vehicle accidents and blunt trauma causing, large radial tears (laceration injuries result in small tears), More common on left side, Insert gastric tube, may pass into intrathoracic stomach, , , , , Mediastinal, traversing wounds, , , , , , Entrance wound in one hemithorax and exit wound/foreign body, in opposite hemithorax, Mediastinal haematoma or pleural cap suggests great vessel, injury, Mortality is 20%, , References, ATLS Manual 8th Edition, Next question
Page 3401 :
A 21 year old man is undergoing an inguinal hernia repair and receives a dose of intravenous coamoxiclav. He is reported to have a penicillin allergy. Over the next few minutes his vital signs are:, Pulse - 130bpm, blood pressure- 60/40mmHg. What is the first line treatment?, , Hydrocortisone 100mg IV, , Adrenaline 1:1000 IV, , Chlorpheniramine 10mg IV, , Adrenaline 1:1000 IM, , Adrenaline 1:10000 IV, , Theme from 2009 Exam, Theme from September 2013 Exam, The first line treatment of anaphylactic shock is intra muscular adrenaline., Please rate this question:, , Discuss and give feedback, , Next question, , Anaphylactic shock, , , Suspect if there has been exposure to an allergen, , Management, - Remove allergen, - ABCD, - Drugs:, Adrenaline 1:1000 0.5ml INTRAMUSCULARLY (not IV). Repeat after 5 mins if no response., Then Chlorpheniramine 10mg IV, Then Hydrocortisone 100-200mg IV, Reference, Emergency treatment of anaphylactic reactions. Guidelines for healthcare providers. Working Group, of the Resuscitation Council (UK).2008, Next question
Page 3403 :
Theme: Types of stroke, , A., B., C., D., E., F., G., H., I., , Anterior cerebral artery infarct, Middle cerebral artery infarct, Posterior cerebral artery infarct, Pituitary mass, Lacunar infarct, Lateral medullary syndrome, Pontine infarct, Horner's syndrome, Cerebellar infarct, , Please select the most likely cause for the symptoms given. Each option may be used once, more, than once or not at all., , 58., , A 53 year old teacher is admitted to the vascular ward for a carotid endarterectomy. Your, house officer does a preoperative assessment and notes that there is a right homonymous, hemianopia. There is no other neurology., You answered Anterior cerebral artery infarct, The correct answer is Posterior cerebral artery infarct, This patient has had a left occipital infarct, as there is only a homonymous hemianopia. If, this patient had a temporal or parietal lobe infarct, there would be associated hemiparesis, and higher cortical dysfunction. This is important to differentiate, as the carotid, endarterectomy is inappropriate in this patient as the lesion is in the posterior cerebral, artery., , 59., , A 52 year man is admitted to the vascular ward for an amputation. The patient complains, of unsteadiness. On further examination you detect right facial numbness and right sided, nystagmus. There is sensory loss of the left side of the body., You answered Anterior cerebral artery infarct, The correct answer is Lateral medullary syndrome, A combination of ipsilateral ataxia, nystagmus, dysphagia, facial numbness, cranial nerve, palsy with contralateral hemisensory loss indicates this diagnosis., , 60., , A 48 year old type 2 diabetic complains of numbness in his left arm and leg. Otherwise, there is no other neurological signs.
Page 3404 :
You answered Anterior cerebral artery infarct, The correct answer is Lacunar infarct, Isolated hemisensory loss is a feature of a lacunar infarct., Please rate this question:, , Discuss and give feedback, , Next question, , Stroke: types, Primary intracerebral, haemorrhage (PICH, c. 10%), , , , Presents with headache, vomiting, loss of, consciousness, , Total anterior circulation, infarcts (TACI, c. 15%), , , , , , , Involves middle and anterior cerebral arteries, Hemiparesis/hemisensory loss, Homonymous hemianopia, Higher cognitive dysfunction e.g. Dysphasia, , Partial anterior circulation, infarcts (PACI, c. 25%), , , , Involves smaller arteries of anterior circulation e.g., upper or lower division of middle cerebral artery, Higher cognitive dysfunction or two of the three TACI, features, , , , Lacunar infarcts (LACI, c., 25%), , , , , Involves perforating arteries around the internal, capsule, thalamus and basal ganglia, Present with either isolated hemiparesis, hemisensory, loss or hemiparesis with limb ataxia, , Posterior circulation infarcts, (POCI, c. 25%), , , , , , Vertebrobasilar arteries, Presents with features of brainstem damage, Ataxia, disorders of gaze and vision, cranial nerve, lesions, , Lateral medullary syndrome, (posterior inferior cerebellar, , , , , Wallenberg's syndrome, Ipsilateral: ataxia, nystagmus, dysphagia, facial
Page 3407 :
A 22 year old man has a full thickness burn on his chest. It is well circumscribed. In A&E his, saturations are reduced to 92% on 15L Oxygen, Blood pressure 102/66 mmHg and HR 105bpm., What is the best management?, , Haemodialysis, , Escharotomy, , Fasciotomy, , Cardiac bypass, , Non invasive ventilation, , The chest burn and its associated oedema is limiting respiration. Therefore an escharotomy of the, chest is indicated, this will remove the constriction on the chest wall and improve ventilation., Please rate this question:, , Discuss and give feedback, , Next question, , Burns, Burns may be thermal, chemical or electrical. In the former category are burns which occur as a, result of heat. Chemical burns occur when the skin is exposed to an extremely caustic or alkaline, substance. Electrical burns occur following exposure to electrical current. The immediate, management includes removal of the burning source which usually includes irrigation of the burned, area. A detailed assessment then needs to be made of the extent of the burns and a number of, charts are available for recording this information. The degree of injury relates to the temperature, and duration of exposure. Most domestic burns are mainly scalds in young children., Following the burn, there is a local response with progressive tissue loss and release of, inflammatory cytokines. Systemically, there are cardiovascular effects resulting from fluid loss and, sequestration of fluid into the third space. There is a marked catabolic response. Immunosupression, is common with large burns and bacterial translocation from the gut lumen is a recognised event., Sepsis is a common cause of death following major burns., Types of burn, , Type of burn, , Skin layers, , Skin, , Blanching, , Management
Page 3408 :
affected, , appearance, , Epidermal/Superficial, , Epidermis, , Red, moist, , Yes, , Superficial partial, thickness, , Epidermis and part, of papillary dermis, affected, , Pale, dry, , Yes, , Normally heals, with no, intervention, , Deep partial thickness, , Epidermis, whole, papillary dermis, affected, , Mottled red, colour, , No, , Needs surgical, intervention, (depending on site), , Full thickness, , Whole skin layer, and subcutaneous, tissue affected, , Dry, leathery, hard wound, , No, , Burns centre, , Depth of burn assessment, , , , , , Bleeding on needle prick, Sensation, Appearance, Blanching to pressure, , Percentage burn estimation, Lund Browder chart: most accurate even in children, Wallace rule of nines, Palmar surface: surface area palm = 0.8% burn, >15% body surface area burns in adults needs urgent burn fluid resuscitation, Transfer to burn centre if:, , , , , , Need burn shock resuscitation, Face/hands/genitals affected, Deep partial thickness or full thickness burns, Significant electrical/chemical burns, , Management, The initial aim is to stop the burning process and resuscitate the patient. Intravenous fluids will be
Page 3409 :
required for children with burns greater than 10% of total body surface area. Adults with burns, greater than 15% of total body surface area will also require IV fluids. The fluids are calculated using, the Parkland formula which is; volume of fluid= total body surface area of the burn % x weight (Kg), x4. Half of the fluid is administered in the first 8 hours. A urinary catheter should be inserted., Analgesia should be given. Complex burns, burns involving the hand perineum and face and burns, >10% in adults and >5% in children should be transferred to a burns unit., Circumferential burns affecting a limb or severe torso burns impeding respiration may require, escharotomy to divide the burnt tissue., Conservative management is appropriate for superficial burns and mixed superficial burns that will, heal in 2 weeks. More complex burns may require excision and skin grafting. Excision and primary, closure is not generally practised as there is a high risk of infection., There is no evidence to support the use of anti microbial prophylaxis or topical antibiotics in burn, patients., Escharotomies, , , , Indicated in circumferential full thickness burns to the torso or limbs., Careful division of the encasing band of burn tissue will potentially improve ventilation (if the, burn involves the torso), or relieve compartment syndrome and oedema (where a limb is, involved), , References, www.euroburn.org/e107files/downloads/guidelinesburncare.pdf, Barajas-Nava LA, López-Alcalde J, Roqué i Figuls M, Solà I, Bonfill Cosp X. Antibiotic prophylaxis, for preventing burn wound infection. Cochrane Database of Systematic Reviews 2013, Issue 6. Art., No.: CD008738. DOI: 10.1002/14651858.CD008738.pub2., Hettiaratchy S & Papini R. Initial management of a major burn: assessment and resuscitation. BMJ, 2004;329:101-103, Next question
Page 3410 :
A 16 year old man sustains a basal skull fracture and is suspected of having CSF rhinorrhoea., Which of the following laboratory tests would most accurately identify whether CSF is present or, not?, , Microscopy to identify red blood cells, , Lab stix testing for glucose, , Lab stix testing for protein, , Beta 2 transferrin assay, , Microscopy, gram stain and culture, , Beta 2 transferrin is a carbohydrate free form of transferrin that is almost exclusively found in the, CSF. Although lab stix testing for glucose is traditional it is associated with false positive results, secondary to contamination with other glucose containing bodily secretions., Please rate this question:, , Discuss and give feedback, , Next question, , Head injury management- NICE Guidelines, Summary of guidelines, , , , , , , All patients should be assessed within 15 minutes on arrival to A&E, Document all 3 components of the GCS, If GCS <8 or = to 8, consider stabilising the airway, Treat pain with low dose IV opiates (if safe), Full spine immobilisation until assessment if:, , - GCS < 15, - neck pain/tenderness, - paraesthesia extremities, - focal neurological deficit, - suspected c-spine injury, If a c-spine injury is suspected a 3 view c-spine x-ray is indicated. CT c-spine is preferred if:, - Intubated
Page 3411 :
- GCS <13, - Normal x-ray but continued concerns regarding c-spine injury, - Any focal neurology, - A CT head scan is being performed, - Initial plain films are abnormal, Immediate CT head (within 1 hour) if:, , , , , , , , , , GCS < 13 on admission, GCS < 15 2 hours after admission, Suspected open or depressed skull fracture, Suspected skull base fracture (panda eyes, Battle's sign, CSF from nose/ear, bleeding ear), Focal neurology, Vomiting > 1 episode, Post traumatic seizure, Coagulopathy, , Contact neurosurgeon if:, , , , , , , , , Persistent GCS < 8 or = 8, Unexplained confusion > 4h, Reduced GCS after admission, Progressive neurological signs, Incomplete recovery post seizure, Penetrating injury, Cerebrospinal fluid leak, , Observations, , , 1/2 hourly GCS until 15, , Reference, 1. http://guidance.nice.org.uk/CG56/QuickRefGuide/pdf/English, 2. Hodgkinson S et al. Early management of head injury: summary of NICE guidance. BMJ 2014, (348):34-37., Next question
Page 3412 :
A 66 year old male is admitted to the vascular ward for an amputation. He reports episodes of, vertigo and dysarthria to the house officer. He suddenly collapses with a Glasgow Coma Score of 3., What is the most likely diagnosis?, , Cerebral haemorrhage in left temporal parietal area, , Opiate overdose, , Cerebral haemorrhage in right temporal parietal area, , Diazepam overdose, , Basilar artery occlusion, , Vertigo and dysarthria suggest a posterior circulation event. In the scenario of a patient complaining, of posterior symptoms and a sudden deterioration in consciousness, the main differential diagnosis, is of a basilar artery occlusion., Please rate this question:, , Discuss and give feedback, , Next question, , Stroke: types, Primary intracerebral, haemorrhage (PICH, c. 10%), , , , Presents with headache, vomiting, loss of, consciousness, , Total anterior circulation, infarcts (TACI, c. 15%), , , , , , , Involves middle and anterior cerebral arteries, Hemiparesis/hemisensory loss, Homonymous hemianopia, Higher cognitive dysfunction e.g. Dysphasia, , Partial anterior circulation, infarcts (PACI, c. 25%), , , , Involves smaller arteries of anterior circulation e.g., upper or lower division of middle cerebral artery, Higher cognitive dysfunction or two of the three TACI, features, ,
Page 3415 :
A 22 year old man is brought to the emergency department. He was found lying unconscious on his, right arm and it is evident that he has taken a temazepam overdose. His right arm is mottled in, colour and swollen, his hand is insensate and stiff. What substance is most likely to be present in the, urine in increased quantities?, , Protein, , Haemoglobin, , Myoglobin, , Erythrocytes, , Lymphocytes, , Theme from 2011 Exam, This man is likely to have muscle death secondary to compartment syndrome. This will result in, muscle breakdown and release of myoglobin. This may accumulate in the kidney and result in renal, failure., Please rate this question:, , Discuss and give feedback, , Next question, , Compartment syndrome, , , , This is a particular complication that may occur following fractures (or following ischaemia reperfusion injury in vascular patients). It is characterised by raised pressure within a closed, anatomical space., The raised pressure within the compartment will eventually compromise tissue perfusion, resulting in necrosis. The two main fractures carrying this complication include supracondylar, fractures and tibial shaft injuries., , Symptoms and signs, , , , , , Pain, especially on movement (even passive), Parasthesiae, Pallor may be present, Arterial pulsation may still be felt as the necrosis occurs as a result of microvascular, compromise
Page 3416 :
, , Paralysis of the muscle group may occur, , Diagnosis, , , Is made by measurement of intracompartmental pressure measurements. Pressures in, excess of 20mmHg are abnormal and >40mmHg is diagnostic., , Treatment, , , , , , , This is essentially prompt and extensive fasciotomies, In the lower limb the deep muscles may be inadequately decompressed by the, inexperienced operator when smaller incisions are performed, Myoglobinuria may occur following fasciotomy and result in renal failure and for this reason, these patients require aggressive IV fluids, Where muscle groups are frankly necrotic at fasciotomy they should be debrided and, amputation may have to be considered, Death of muscle groups may occur within 4-6 hours, Next question
Page 3417 :
A 19 year intravenous drug abuser is recovering following a surgical drainage of a psoas abscess., He is found collapsed in the ward toilet unresponsive and with pinpoint pupils. What is the most, appropriate immediate management?, , Intravenous flumazenil, , Intravenous nalaxone, , Intravenous benxhexol, , No further management, , Intravenous glycopyrolate, , Intravenous nalaxone is needed to treat the patient who has had an overdose of opiate. Naloxone, has the quickest onset of action, however it is important to be aware of its short acting duration and, the need for further administration. There is also the risk of rebound pain once naloxone is given., Please rate this question:, , Discuss and give feedback, , Next question, , Opioid misuse, Opioids are substances which bind to opioid receptors. This includes both naturally occurring opiates, such as morphine and synthetic opioids such as buprenorphine and methadone., Features of opioid misuse, , , , , , Rhinorrhoea, Needle track marks, Pinpoint pupils, Drowsiness, , Complications of intravenous opioid misuse, , , , Viral infection secondary to sharing needles: HIV, hepatitis B & C, Bacterial infection secondary to injection: infective endocarditis, septic arthritis, septicaemia,, necrotising fasciitis, groin abscess
Page 3418 :
, , , , , Pseudoaneurysm, Venous thromboembolism, Osteomyelitis, Overdose may lead to respiratory depression and death, , Emergency management of opioid overdose, , , IV or IM naloxone: has a rapid onset and relatively short duration of action, , Next question
Page 3419 :
A 68 year old male is admitted to the surgical ward for assessment of severe epigastric pain. His, abdomen is soft and non tender. However the Nurse forces you to look at the ECG. It looks, abnormal. Which of the following features is an indication for urgent coronary thrombolysis or, percutaneous intervention?, , Right bundle branch block, , ST elevation of 1mm in leads V1 to V6, , Ventricular tachycardia, , Q waves in leads V1 to V6, , ST elevation of 1mm in leads II, III and aVF, ECG changes for thrombolysis or percutaneous intervention:, ST elevation of > 2mm (2 small squares) in 2 or more consecutive anterior leads (V1-V6) OR, ST elevation of greater than 1mm (1 small square) in greater than 2 consecutive inferior leads (II, III,, avF, avL) OR, New Left bundle branch block, ST elevation of 1mm in leads II, III and aVF reflects significant cardiac ischaemia due to the right, coronary artery occlusion. The medical registrar should be contacted to urgently assess the patient., Note right coronary artery occlusions puts the patient at risk of cardiac arrhythmias (due to blood, supply to the sino atrial node)., Please rate this question:, , Discuss and give feedback, , Next question, , Thrombolysis or percutaneous intervention in myocardial infarction, Thrombolytic drugs activate plasminogen to form plasmin. This in turn degrades fibrin and help, breaks up thrombi. They in primarily used in patients who present with a ST elevation myocardial, infarction. Other indications include acute ischaemic stroke and pulmonary embolism, although strict, inclusion criteria apply., Examples
Page 3420 :
, , , , alteplase, tenecteplase, streptokinase, , Contraindications to thrombolysis, , , , , , , , , , , active internal bleeding, recent haemorrhage, trauma or surgery (including dental extraction), coagulation and bleeding disorders, intracranial neoplasm, stroke < 3 months, aortic dissection, recent head injury, pregnancy, severe hypertension, , Side-effects, , , , , haemorrhage, hypotension - more common with streptokinase, allergic reactions may occur with streptokinase, Next question
Page 3421 :
Which of the following is not typically associated with a degloving injury?, , Overlying pallor of the skin, , Abnormal motility of the overlying skin, , History of friction type injury, , Improved results when the degloved segment is left in situ as a temporary closure, , Poor results when primary compression treatment is used in preference to skin grafting, , Degloving injuries typically involve extremities and are usually friction injuries e.g. arm being run, over. There is abnormal motility of the overlying skin, pallor, loss of sensation. Early treatment is key, and should involve skin grafting which may use the degloved segment. This however, should be, formally prepared for the role and simple compression bandaging gives poor results., Please rate this question:, , Discuss and give feedback, , Next question, , Wound healing, Surgical wounds are either incisional or excisional and either clean, clean contaminated or dirty., Although the stages of wound healing are broadly similar their contributions will vary according to the, wound type., The main stages of wound healing include:, Haemostasis, , , , Minutes to hours following injury, Vasospasm in adjacent vessels, platelet plug formation and generation of fibrin rich clot., , Inflammation, , , , Typically days 1-5, Neutrophils migrate into wound (function impaired in diabetes).
Page 3422 :
, , , , Growth factors released, including basic fibroblast growth factor and vascular endothelial, growth factor., Fibroblasts replicate within the adjacent matrix and migrate into wound., Macrophages and fibroblasts couple matrix regeneration and clot substitution., , Regeneration, , , , , , Typically days 7 to 56, Platelet derived growth factor and transformation growth factors stimulate fibroblasts and, epithelial cells., Fibroblasts produce a collagen network., Angiogenesis occurs and wound resembles granulation tissue., , Remodeling, , , , , , , From 6 weeks to 1 year, Longest phase of the healing process and may last up to one year (or longer)., During this phase fibroblasts become differentiated (myofibroblasts) and these facilitate, wound contraction., Collagen fibres are remodeled., Microvessels regress leaving a pale scar., , The above description represents an idealised scenario. A number of diseases may distort this, process. Neovascularisation is an important early process. Endothelial cells may proliferate in the, wound bed and recanalise to form a vessel. Vascular disease, shock and sepsis can all compromise, microvascular flow and impair healing., Conditions such as jaundice will impair fibroblast synthetic function and immunity with a detrimental, effect in most parts of the healing process., Problems with scars:, Hypertrophic scars, Excessive amounts of collagen within a scar. Nodules may be present histologically containing, randomly arranged fibrils within and parallel fibres on the surface. The tissue itself is confined to the, extent of the wound itself and is usually the result of a full thickness dermal injury. They may go on, to develop contractures., Image of hypertrophic scarring. Note that it remains confined to the boundaries of the original, wound:
Page 3423 :
Image sourced from Wikipedia, , Keloid scars, Excessive amounts of collagen within a scar. Typically a keloid scar will pass beyond the boundaries, of the original injury. They do not contain nodules and may occur following even trivial injury. They, do not regress over time and may recur following removal., Image of a keloid scar. Note the extension beyond the boundaries of the original incision:, , Image sourced from Wikipedia, , Drugs which impair wound healing:
Page 3424 :
, , , , , Non steroidal anti inflammatory drugs, Steroids, Immunosupressive agents, Anti neoplastic drugs, , Closure, Delayed primary closure is the anatomically precise closure that is delayed for a few days but before, granulation tissue becomes macroscopically evident., Secondary closure refers to either spontaneous closure or to surgical closure after granulation tissue, has formed., Next question
Page 3425 :
Which of the following statements relating to large volume blood loss in trauma is incorrect?, , Tranexamic acid reduces the incidence of rebleeding following surgery, , Hypocalcaemia may complicate resuscitation, , Colloids are preferred initially as they reduce the incidence of coagulopathy, , When patients receive over 5 units of whole blood mortality increases when blood, products greater than 3 weeks old are utilised, In the battlefield setting a ratio of 1:1:1 for blood, plasma and platelets is used, , Fresh blood is the fluid of choice when large volume blood loss complicates trauma. Mortality is, doubled when blood >3 weeks old is used., Please rate this question:, , Discuss and give feedback, , Next question, , Trauma management, The cornerstone of trauma management is embodied in the principles of ATLS., Following trauma there is a trimodal death distribution:, , , , , Immediately following injury. Typically as result of brain or high spinal injuries, cardiac or, great vessel damage. Salvage rate is low., In early hours following injury. In this group deaths are due to phenomena such as splenic, rupture, sub dural haematomas and haemopneumothoraces, In the days following injury. Usually due to sepsis or multi organ failure., , Aspects of trauma management, , , , , ABCDE approach., Tension pneumothoraces will deteriorate with vigorous ventilation attempts., External haemorrhage is managed as part of the primary survey. As a rule tourniquets, should not be used. Blind application of clamps will tend to damage surrounding structures, and packing is the preferred method of haemorrhage control.
Page 3426 :
, , , Urinary catheters and naso gastric tubes may need inserting. Be wary of basal skull fractures, and urethral injuries., Patients with head and neck trauma should be assumed to have a cervical spine injury until, proven otherwise., , Thoracic injuries, , , , , , , , , , Simple pneumothorax, Mediastinal traversing wounds, Tracheobronchial tree injury, Haemothorax, Blunt cardiac injury, Diaphragmatic injury, Aortic disruption, Pulmonary contusion, , Management of thoracic trauma, , , , , , , , , , , , Simple pneumothorax insert chest drain. Aspiration is risky in trauma as pneumothorax, may be from lung laceration and convert to tension pneumothorax., Mediastinal traversing wounds These result from situations like stabbings. Exit and entry, wounds in separate hemithoraces. The presence of a mediastinal haematoma indicates the, likelihood of a great vessel injury. All patients should undergo CT angiogram and, oesophageal contrast swallow. Indications for thoracotomy are largely related to blood loss, and will be addressed below., Tracheobronchial tree injury Unusual injuries. In blunt trauma most injuries occur within, 4cm of the carina. Features suggesting this injury include haemoptysis and surgical, emphysema. These injuries have a very large air leak and may have tension pneumothorax., Haemothorax Usually caused by laceration of lung vessel or internal mammary artery by rib, fracture. Patients should all have a wide bore 36F chest drain. Indications for thoracotomy, include loss of more than 1.5L blood initially or ongoing losses of >200ml per hour for >2, hours., Cardiac contusions Usually cardiac arrhythmias, often overlying sternal fracture. Perform, echocardiography to exclude pericardial effusions and tamponade. Risk of arrhythmias falls, after 24 hours., Diaphragmatic injury Usually left sided. Direct surgical repair is performed., Traumatic aortic disruption Commonest cause of death after RTA or falls. Usually, incomplete laceration near ligamentum arteriosum. All survivors will have contained, haematoma. Only 1-2% of patients with this injury will have a normal chest x-ray., Pulmonary contusion Common and lethal. Insidious onset. Early intubation and ventilation., , Abdominal trauma, , , , , Deceleration injuries are common., In blunt trauma requiring laparotomy the spleen is most commonly injured (40%), Stab wounds traverse structures most commonly liver (40%)
Page 3427 :
, , , , , , Gunshot wounds have variable effects depending upon bullet type. Small bowel is most, commonly injured (50%), Patients with stab wounds and no peritoneal signs up to 25% will not enter the peritoneal, cavity, Blood at urethral meatus suggests a urethral tear, High riding prostate on PR = urethral disruption, Mechanical testing for pelvic stability should only be performed once, , Investigations in abdominal trauma, , Diagnostic Peritoneal, Lavage, , Abdominal CT scan, , USS, , Indication, , Document bleeding if, hypotensive, , Document organ injury if, normotensive, , Document fluid if, hypotensive, , Advantages, , Early diagnosis and, sensitive; 98% accurate, , Most specific for, localising injury; 92 to, 98% accurate, , Early diagnosis, non, invasive and repeatable;, 86 to 95% accurate, , Disadvantages, , Invasive and may miss, retroperitoneal and, diaphragmatic injury, , Location of scanner away, from facilities, time taken, for reporting, need for, contrast, , Operator dependent and, may miss, retroperitoneal injury, , , , , Amylase may be normal following pancreatic trauma, Urethrography if suspected urethral injury, Next question
Page 3428 :
The following features are typical of superficial partial dermal burns except:, , Erythema, , Absence of blisters, , Spontaneous healing in most cases, , No extension beyond proximal dermal papillae, , Good capillary refill at the burn site, , Superficial dermal burns are typically erythematous, do not extend beyond the upper part of the, dermal papillae, capillary return and blisters are both usually present., A Typical example of a superficial dermal burn is shown below, , Image sourced from Wikipedia, , Please rate this question:, , Discuss and give feedback, , Next question
Page 3429 :
Burns, Burns may be thermal, chemical or electrical. In the former category are burns which occur as a, result of heat. Chemical burns occur when the skin is exposed to an extremely caustic or alkaline, substance. Electrical burns occur following exposure to electrical current. The immediate, management includes removal of the burning source which usually includes irrigation of the burned, area. A detailed assessment then needs to be made of the extent of the burns and a number of, charts are available for recording this information. The degree of injury relates to the temperature, and duration of exposure. Most domestic burns are mainly scalds in young children., Following the burn, there is a local response with progressive tissue loss and release of, inflammatory cytokines. Systemically, there are cardiovascular effects resulting from fluid loss and, sequestration of fluid into the third space. There is a marked catabolic response. Immunosupression, is common with large burns and bacterial translocation from the gut lumen is a recognised event., Sepsis is a common cause of death following major burns., Types of burn, , Type of burn, , Skin layers, affected, , Skin, appearance, , Blanching, , Epidermal/Superficial, , Epidermis, , Red, moist, , Yes, , Superficial partial, thickness, , Epidermis and part, of papillary dermis, affected, , Pale, dry, , Yes, , Normally heals, with no, intervention, , Deep partial thickness, , Epidermis, whole, papillary dermis, affected, , Mottled red, colour, , No, , Needs surgical, intervention, (depending on site), , Full thickness, , Whole skin layer, and subcutaneous, tissue affected, , Dry, leathery, hard wound, , No, , Burns centre, , Depth of burn assessment, , , , , , Bleeding on needle prick, Sensation, Appearance, Blanching to pressure, , Management
Page 3430 :
Percentage burn estimation, Lund Browder chart: most accurate even in children, Wallace rule of nines, Palmar surface: surface area palm = 0.8% burn, >15% body surface area burns in adults needs urgent burn fluid resuscitation, Transfer to burn centre if:, , , , , , Need burn shock resuscitation, Face/hands/genitals affected, Deep partial thickness or full thickness burns, Significant electrical/chemical burns, , Management, The initial aim is to stop the burning process and resuscitate the patient. Intravenous fluids will be, required for children with burns greater than 10% of total body surface area. Adults with burns, greater than 15% of total body surface area will also require IV fluids. The fluids are calculated using, the Parkland formula which is; volume of fluid= total body surface area of the burn % x weight (Kg), x4. Half of the fluid is administered in the first 8 hours. A urinary catheter should be inserted., Analgesia should be given. Complex burns, burns involving the hand perineum and face and burns, >10% in adults and >5% in children should be transferred to a burns unit., Circumferential burns affecting a limb or severe torso burns impeding respiration may require, escharotomy to divide the burnt tissue., Conservative management is appropriate for superficial burns and mixed superficial burns that will, heal in 2 weeks. More complex burns may require excision and skin grafting. Excision and primary, closure is not generally practised as there is a high risk of infection., There is no evidence to support the use of anti microbial prophylaxis or topical antibiotics in burn, patients., Escharotomies, , , , Indicated in circumferential full thickness burns to the torso or limbs., Careful division of the encasing band of burn tissue will potentially improve ventilation (if the, burn involves the torso), or relieve compartment syndrome and oedema (where a limb is, involved), , References, www.euroburn.org/e107files/downloads/guidelinesburncare.pdf, Barajas-Nava LA, López-Alcalde J, Roqué i Figuls M, Solà I, Bonfill Cosp X. Antibiotic prophylaxis, for preventing burn wound infection. Cochrane Database of Systematic Reviews 2013, Issue 6. Art., No.: CD008738. DOI: 10.1002/14651858.CD008738.pub2.
Page 3431 :
Which of the following is not a feature found on a CXR in traumatic aortic disruption?, , Widened mediastinum, , Trachea deviated to the left, , Depression of the left main stem bronchus, , Obliteration of the aortic knob, , Widened paraspinal interfaces, , The trachea is normally deviated to the right., Please rate this question:, , Discuss and give feedback, , Next question, , Thoracic aorta rupture, , , , , Mechanism of injury: Decelerating force i.e. RTA, fall from a great height, Most people die at scene, Survivors may have an incomplete laceration at the ligamentum arteriosum of the aorta., , Clinical features, , , , Contained haematoma: persistent hypotension, Detected mainly by history, CXR changes, , CXR changes, , , , , , Widened mediastinum, Trachea/Oesophagus to right, Depression of left main stem bronchus, Widened paratracheal stripe/paraspinal interfaces
Page 3432 :
, , , Space between aorta and pulmonary artery obliterated, Rib fracture/left haemothorax, , Diagnosis, Angiography, usually CT aortogram., Treatment, Repair or replacement. Ideally they should undergo endovascular repair., Next question
Page 3433 :
Theme: Head injury management, , A., B., C., D., E., F., G., H., , Observation, CT head within 1 hour, CT head within 8 hours, Urgent neurosurgical review (even before CT head performed), 3 view c-spine xray, 2 view c-spine xray, CT c-spine, MRI c-spine, , What is the best initial management plan for the scenario given? Each option may be used once,, more than once or not at all., , 3., , A 22 year old male falls of a ladder. He complains of neck pain and cannot feel his legs. His, GCS suddenly deteriorates and a CT head confirms an extradural haematoma. What is the, best imaging for his neck?, You answered Observation, The correct answer is CT c-spine, This man needs a CT scan of his c-spine. A CT scan will give the best resolution of any, bony injury., , 4., , A 25 year old teacher falls down the stairs. She complains of a headache and has vomited 3, times. She has a GCS of 15/15., You answered Observation, The correct answer is CT head within 1 hour, This lady has a head injury and vomiting > 1, therefore an urgent CT head is indicated., , 5., , An 18 year old student is shot in the back of the head., You answered Observation, The correct answer is Urgent neurosurgical review (even before CT head performed), A penetrating injury needs urgent neurosurgical review., , Please rate this question:
Page 3434 :
Discuss and give feedback, , Next question, , Head injury management- NICE Guidelines, Summary of guidelines, , , , , , , All patients should be assessed within 15 minutes on arrival to A&E, Document all 3 components of the GCS, If GCS <8 or = to 8, consider stabilising the airway, Treat pain with low dose IV opiates (if safe), Full spine immobilisation until assessment if:, , - GCS < 15, - neck pain/tenderness, - paraesthesia extremities, - focal neurological deficit, - suspected c-spine injury, If a c-spine injury is suspected a 3 view c-spine x-ray is indicated. CT c-spine is preferred if:, - Intubated, - GCS <13, - Normal x-ray but continued concerns regarding c-spine injury, - Any focal neurology, - A CT head scan is being performed, - Initial plain films are abnormal, Immediate CT head (within 1 hour) if:, , , , , , , , , , GCS < 13 on admission, GCS < 15 2 hours after admission, Suspected open or depressed skull fracture, Suspected skull base fracture (panda eyes, Battle's sign, CSF from nose/ear, bleeding ear), Focal neurology, Vomiting > 1 episode, Post traumatic seizure, Coagulopathy, , Contact neurosurgeon if:, , , , , , Persistent GCS < 8 or = 8, Unexplained confusion > 4h, Reduced GCS after admission, Progressive neurological signs
Page 3436 :
A 60-year-old man develops palpitations while on the acute surgical unit. An ECG shows a broad, complex tachycardia at a rate of 150 bpm. His blood pressure is 124/82 mmHg and there is no, evidence of heart failure. The surgical consultant wants to give rate control (the medical team are not, answering their bleeps). Which one of the following is it least appropriate to give?, , Procainamide, , Lidocaine, , Amiodarone, , Adenosine, , Verapamil, Ventricular tachycardia - verapamil is contraindicated, Verapamil should never be given to a patient with a broad complex tachycardia as it may precipitate, ventricular fibrillation in patients with ventricular tachycardia. Adenosine is sometimes given in this, situation as a 'trial' if there is a strong suspicion the underlying rhythm is a supraventricular, tachycardia with aberrant conduction, Please rate this question:, , Discuss and give feedback, , Next question, , Ventricular tachycardia: management, Whilst a broad complex tachycardia may result from a supraventricular rhythm with aberrant, conduction, the European Resuscitation Council advise that in a peri-arrest situation it is assumed to, be ventricular in origin, If the patient has adverse signs (systolic BP < 90 mmHg, chest pain, heart failure or rate > 150, beats/min) then immediate cardioversion is indicated. In the absence of such signs antiarrhythmics, may be used. If these fail, then electrical cardioversion may be needed with synchronised DC, shocks, Drug therapy, , , , amiodarone: ideally administered through a central line, lidocaine: use with caution in severe left ventricular impairment
Page 3438 :
A 62 year old male attends the hernia clinic. He suddenly develops speech problems, left facial, weakness and left sided arm and leg weakness lasting longer than 5 minutes. A CT head shows no, intracerebral bleed. What is the next line of management?, , Aspirin 300mg, , Aspirin 75 mg, , Clopidogrel 300mg, , Urgent referral for thrombolysis, , Carotid endarterectomy, , This patient is within 3h of symptom onset of a stroke. Therefore he should be urgently referred to, the medical team for thrombolysis, before Aspirin is given. There are concerns that high dose aspirin, would increase the risk of intracerebral haemorrhage if thrombolysis is undertaken., This is an example of the type of medical problem you should be aware of as a surgeon, as, ultimately you can make a difference by referring QUICKLY to the correct specialty for management., Please rate this question:, , Discuss and give feedback, , Next question, , Stroke: types, Primary intracerebral, haemorrhage (PICH, c. 10%), , , , Presents with headache, vomiting, loss of, consciousness, , Total anterior circulation, infarcts (TACI, c. 15%), , , , , , , Involves middle and anterior cerebral arteries, Hemiparesis/hemisensory loss, Homonymous hemianopia, Higher cognitive dysfunction e.g. Dysphasia, , Partial anterior circulation, infarcts (PACI, c. 25%), , , , Involves smaller arteries of anterior circulation e.g., upper or lower division of middle cerebral artery, Higher cognitive dysfunction or two of the three TACI, ,
Page 3441 :
A 45-year-old man is seen in the Emergency Department with nausea, pallor and lethargy. He has, no past medical history of note. A cannula is inserted and serum urea and electrolytes show the, following, Na+, , 140 mmol/l, , K+, , 6.7 mmol/l, , Bicarbonate, , 14 mmol/l, , Urea, , 18.2 mmol/l, , Creatinine, , 230 µmol/l, , What is the most appropriate initial management?, , Nebulised salbutamol, , Intravenous bicarbonate, , Haemodialysis, , Insulin/dextrose infusion, , Intravenous calcium gluconate, , The first priority in this patient is to stabilise the myocardium with intravenous calcium gluconate., Please rate this question:, , Discuss and give feedback, , Next question, , Management of hyperkalaemia, Untreated hyperkalaemia may cause life-threatening arrhythmias. Precipitating factors should be, addressed (e.g. acute renal failure) and aggravating drugs stopped (e.g. ACE inhibitors)., Management may be categorised by the aims of treatment, Stabilisation of the cardiac membrane
Page 3442 :
, , Intravenous calcium gluconate, , Short-term shift in potassium from extracellular to intracellular fluid compartment, , , , Combined insulin/dextrose infusion, Nebulised salbutamol, , Removal of potassium from the body, , , , , Calcium resonium (orally or enema), Loop diuretics, Dialysis, Next question
Page 3443 :
Theme: Visceral injury, , A., B., C., D., E., F., G., , Ruptured spleen, Ileum injury, Duodenal injury, Urethral injury, Rectal injury, Oesophageal injury, Liver laceration, , Please select the most likely injury for the scenario given. Each option may be used once, more than, once or not at all., , 9., , A motorcyclist is involved in a head on road traffic accident with a lorry. He is comatose, at scene and trauma series x-rays confirm a pelvic fracture. On rectal examination he has a, high riding prostate., You answered Ruptured spleen, The correct answer is Urethral injury, This is classical for urethral injury. Features of a urethral injury include; pelvic fracture,, high riding prostate on digital rectal examination and blood at the urethral meatus. Where, this is the suspected diagnosis a suprapubic catheter and urethral contrast studies, performed., , 10., , A cyclist loses control and falls off the side of a road landing on the bicycle handlebars., CT scanning shows a large amount of retroperitoneal air., You answered Ruptured spleen, The correct answer is Duodenal injury, Theme from 2012 exam, Retroperitoneal air is more likely with a duodenal injury. As it is largely retroperitoneal. A, handlebar type injury is the commonest cause and the pancreas should be carefully, inspected as it too may be injured. It would be unusual for the ileum to be injured in this, type of scenario as it is mobile., , 11., , A 23 year old man is shot in the abdomen. He is haemodynamically stable but on, ultrasound he has a large amount of intra abdominal free fluid., You answered Ruptured spleen
Page 3444 :
The correct answer is Ileum injury, Small bowel injury is the most common type of injury in this scenario. The enteric, contents will tend to result in a large amount of intra abdominal fluid., Please rate this question:, , Discuss and give feedback, , Next question, , Trauma management, The cornerstone of trauma management is embodied in the principles of ATLS., Following trauma there is a trimodal death distribution:, , , , , Immediately following injury. Typically as result of brain or high spinal injuries, cardiac or, great vessel damage. Salvage rate is low., In early hours following injury. In this group deaths are due to phenomena such as splenic, rupture, sub dural haematomas and haemopneumothoraces, In the days following injury. Usually due to sepsis or multi organ failure., , Aspects of trauma management, , , , , , , ABCDE approach., Tension pneumothoraces will deteriorate with vigorous ventilation attempts., External haemorrhage is managed as part of the primary survey. As a rule tourniquets, should not be used. Blind application of clamps will tend to damage surrounding structures, and packing is the preferred method of haemorrhage control., Urinary catheters and naso gastric tubes may need inserting. Be wary of basal skull fractures, and urethral injuries., Patients with head and neck trauma should be assumed to have a cervical spine injury until, proven otherwise., , Thoracic injuries, , , , , , , , Simple pneumothorax, Mediastinal traversing wounds, Tracheobronchial tree injury, Haemothorax, Blunt cardiac injury, Diaphragmatic injury
Page 3445 :
, , , Aortic disruption, Pulmonary contusion, , Management of thoracic trauma, , , , , , , , , , , , Simple pneumothorax insert chest drain. Aspiration is risky in trauma as pneumothorax, may be from lung laceration and convert to tension pneumothorax., Mediastinal traversing wounds These result from situations like stabbings. Exit and entry, wounds in separate hemithoraces. The presence of a mediastinal haematoma indicates the, likelihood of a great vessel injury. All patients should undergo CT angiogram and, oesophageal contrast swallow. Indications for thoracotomy are largely related to blood loss, and will be addressed below., Tracheobronchial tree injury Unusual injuries. In blunt trauma most injuries occur within, 4cm of the carina. Features suggesting this injury include haemoptysis and surgical, emphysema. These injuries have a very large air leak and may have tension pneumothorax., Haemothorax Usually caused by laceration of lung vessel or internal mammary artery by rib, fracture. Patients should all have a wide bore 36F chest drain. Indications for thoracotomy, include loss of more than 1.5L blood initially or ongoing losses of >200ml per hour for >2, hours., Cardiac contusions Usually cardiac arrhythmias, often overlying sternal fracture. Perform, echocardiography to exclude pericardial effusions and tamponade. Risk of arrhythmias falls, after 24 hours., Diaphragmatic injury Usually left sided. Direct surgical repair is performed., Traumatic aortic disruption Commonest cause of death after RTA or falls. Usually, incomplete laceration near ligamentum arteriosum. All survivors will have contained, haematoma. Only 1-2% of patients with this injury will have a normal chest x-ray., Pulmonary contusion Common and lethal. Insidious onset. Early intubation and ventilation., , Abdominal trauma, , , , , , , , , , Deceleration injuries are common., In blunt trauma requiring laparotomy the spleen is most commonly injured (40%), Stab wounds traverse structures most commonly liver (40%), Gunshot wounds have variable effects depending upon bullet type. Small bowel is most, commonly injured (50%), Patients with stab wounds and no peritoneal signs up to 25% will not enter the peritoneal, cavity, Blood at urethral meatus suggests a urethral tear, High riding prostate on PR = urethral disruption, Mechanical testing for pelvic stability should only be performed once, , Investigations in abdominal trauma, , Diagnostic Peritoneal, , Abdominal CT scan, , USS
Page 3446 :
Lavage, , Indication, , Document bleeding if, hypotensive, , Document organ injury if, normotensive, , Document fluid if, hypotensive, , Advantages, , Early diagnosis and, sensitive; 98% accurate, , Most specific for, localising injury; 92 to, 98% accurate, , Early diagnosis, non, invasive and repeatable;, 86 to 95% accurate, , Disadvantages, , Invasive and may miss, retroperitoneal and, diaphragmatic injury, , Location of scanner away, from facilities, time taken, for reporting, need for, contrast, , Operator dependent and, may miss, retroperitoneal injury, , , , , Amylase may be normal following pancreatic trauma, Urethrography if suspected urethral injury, Next question
Page 3447 :
A 22 year old man has a full thickness burn of his leg after being trapped in a burning car. There are, no fractures of the limb. There burn is well circumscribed. After 2 hours he complains of tingling of, his leg and it appears dusky. What is the best management for this?, , Fasciotomy, , Escharotomy, , Angioplasty, , Pain control, , Anticoagulation, , The full thickness burn has oedema which is affecting the peripheral circulation. Therefore the burn, needs to be divided (not the fascia) to allow normal circulation to return., Please rate this question:, , Discuss and give feedback, , Next question, , Burns, Burns may be thermal, chemical or electrical. In the former category are burns which occur as a, result of heat. Chemical burns occur when the skin is exposed to an extremely caustic or alkaline, substance. Electrical burns occur following exposure to electrical current. The immediate, management includes removal of the burning source which usually includes irrigation of the burned, area. A detailed assessment then needs to be made of the extent of the burns and a number of, charts are available for recording this information. The degree of injury relates to the temperature, and duration of exposure. Most domestic burns are mainly scalds in young children., Following the burn, there is a local response with progressive tissue loss and release of, inflammatory cytokines. Systemically, there are cardiovascular effects resulting from fluid loss and, sequestration of fluid into the third space. There is a marked catabolic response. Immunosupression, is common with large burns and bacterial translocation from the gut lumen is a recognised event., Sepsis is a common cause of death following major burns., Types of burn, , Type of burn, , Skin layers, , Skin, , Blanching, , Management
Page 3448 :
affected, , appearance, , Epidermal/Superficial, , Epidermis, , Red, moist, , Yes, , Superficial partial, thickness, , Epidermis and part, of papillary dermis, affected, , Pale, dry, , Yes, , Normally heals, with no, intervention, , Deep partial thickness, , Epidermis, whole, papillary dermis, affected, , Mottled red, colour, , No, , Needs surgical, intervention, (depending on site), , Full thickness, , Whole skin layer, and subcutaneous, tissue affected, , Dry, leathery, hard wound, , No, , Burns centre, , Depth of burn assessment, , , , , , Bleeding on needle prick, Sensation, Appearance, Blanching to pressure, , Percentage burn estimation, Lund Browder chart: most accurate even in children, Wallace rule of nines, Palmar surface: surface area palm = 0.8% burn, >15% body surface area burns in adults needs urgent burn fluid resuscitation, Transfer to burn centre if:, , , , , , Need burn shock resuscitation, Face/hands/genitals affected, Deep partial thickness or full thickness burns, Significant electrical/chemical burns, , Management, The initial aim is to stop the burning process and resuscitate the patient. Intravenous fluids will be
Page 3449 :
required for children with burns greater than 10% of total body surface area. Adults with burns, greater than 15% of total body surface area will also require IV fluids. The fluids are calculated using, the Parkland formula which is; volume of fluid= total body surface area of the burn % x weight (Kg), x4. Half of the fluid is administered in the first 8 hours. A urinary catheter should be inserted., Analgesia should be given. Complex burns, burns involving the hand perineum and face and burns, >10% in adults and >5% in children should be transferred to a burns unit., Circumferential burns affecting a limb or severe torso burns impeding respiration may require, escharotomy to divide the burnt tissue., Conservative management is appropriate for superficial burns and mixed superficial burns that will, heal in 2 weeks. More complex burns may require excision and skin grafting. Excision and primary, closure is not generally practised as there is a high risk of infection., There is no evidence to support the use of anti microbial prophylaxis or topical antibiotics in burn, patients., Escharotomies, , , , Indicated in circumferential full thickness burns to the torso or limbs., Careful division of the encasing band of burn tissue will potentially improve ventilation (if the, burn involves the torso), or relieve compartment syndrome and oedema (where a limb is, involved), , References, www.euroburn.org/e107files/downloads/guidelinesburncare.pdf, Barajas-Nava LA, López-Alcalde J, Roqué i Figuls M, Solà I, Bonfill Cosp X. Antibiotic prophylaxis, for preventing burn wound infection. Cochrane Database of Systematic Reviews 2013, Issue 6. Art., No.: CD008738. DOI: 10.1002/14651858.CD008738.pub2., Hettiaratchy S & Papini R. Initial management of a major burn: assessment and resuscitation. BMJ, 2004;329:101-103, Next question
Page 3450 :
A 28 year old man is in the surgical intensive care unit. He has suffered a flail chest injury several, hours earlier and he was intubated and ventilated. Over the past few minutes he has become, increasingly hypoxic and is now needing increased ventilation pressures. What is the most common, cause?, , Pulmonary embolism, , Cardiac tamponade, , Fat embolism, , Tension pneumothorax, , Adult respiratory distress syndrome, , Theme from April 2011 Exam, A flail chest segment may lacerate the underlying lung and create a flap valve. A tension, pneumothorax can be created by intubation and ventilation in this situation. Sudden hypoxia and, increased ventilation pressure are clues., Please rate this question:, , Discuss and give feedback, , Next question, , Tension Pneumothorax, Tension pneumothorax is a state of positive pressure within a pneumothorax throughout the, respiratory cycle. A breach in the pleura allows air into the intra pleural space via a one way valve., The initial pressure pneumothorax expands until positive pressure is present throughout the, respiratory cycle. The risk is greatest in the ventilated trauma patient as positive pressure is used., Undiagnosed tension pneumothorax accounts for 3.8% of trauma deaths., Clinically, the classic features include chest pain, dyspnoea, hypoxia, hypotension, tracheal, deviation, ipsilateral hyperpercussion note, decreased air entry. In ventilated patients, cardiovascular, disturbance and sub cutaneous emphysema are relatively common and more so than in a case, where the patient is breathing spontaneously., Chest x-ray features, , , Lung collapse towards the hilum
Page 3451 :
, , , , , Diaphragmatic depression Increased rib separation, Increased thoracic volume, Ipsilateral flattening of the heart border, Contra lateral mediastinal deviation, , Management, Immediate needle decompression followed by definitive wide bore chest drain insertion, Image showing mediastinal shift with a tension pneumothorax, , Image sourced from Wikipedia, , Next question
Page 3452 :
A 10 year old boy is playing with a firework which explodes and he sustains a full thickness burn to, his left arm. Which of the following statements is not characteristic of this situation?, , They have a leathery appearance, , The burn area is extremely painful until skin grafted, , They always heal with scarring, , Blanching does not occur under pressure, , Absence of,or few, blisters, , Full thickness burns involve complete injury to the dermis and sub dermal appendages. They have a, leathery, often white appearance. They are initially insensate although pain often occurs during, healing following skin grafting. They do not blanch under pressure., Please rate this question:, , Discuss and give feedback, , Next question, , Burns, Burns may be thermal, chemical or electrical. In the former category are burns which occur as a, result of heat. Chemical burns occur when the skin is exposed to an extremely caustic or alkaline, substance. Electrical burns occur following exposure to electrical current. The immediate, management includes removal of the burning source which usually includes irrigation of the burned, area. A detailed assessment then needs to be made of the extent of the burns and a number of, charts are available for recording this information. The degree of injury relates to the temperature, and duration of exposure. Most domestic burns are mainly scalds in young children., Following the burn, there is a local response with progressive tissue loss and release of, inflammatory cytokines. Systemically, there are cardiovascular effects resulting from fluid loss and, sequestration of fluid into the third space. There is a marked catabolic response. Immunosupression, is common with large burns and bacterial translocation from the gut lumen is a recognised event., Sepsis is a common cause of death following major burns., Types of burn, , Type of burn, , Skin layers, , Skin, , Blanching, , Management
Page 3453 :
affected, , appearance, , Epidermal/Superficial, , Epidermis, , Red, moist, , Yes, , Superficial partial, thickness, , Epidermis and part, of papillary dermis, affected, , Pale, dry, , Yes, , Normally heals, with no, intervention, , Deep partial thickness, , Epidermis, whole, papillary dermis, affected, , Mottled red, colour, , No, , Needs surgical, intervention, (depending on site), , Full thickness, , Whole skin layer, and subcutaneous, tissue affected, , Dry, leathery, hard wound, , No, , Burns centre, , Depth of burn assessment, , , , , , Bleeding on needle prick, Sensation, Appearance, Blanching to pressure, , Percentage burn estimation, Lund Browder chart: most accurate even in children, Wallace rule of nines, Palmar surface: surface area palm = 0.8% burn, >15% body surface area burns in adults needs urgent burn fluid resuscitation, Transfer to burn centre if:, , , , , , Need burn shock resuscitation, Face/hands/genitals affected, Deep partial thickness or full thickness burns, Significant electrical/chemical burns, , Management, The initial aim is to stop the burning process and resuscitate the patient. Intravenous fluids will be
Page 3454 :
required for children with burns greater than 10% of total body surface area. Adults with burns, greater than 15% of total body surface area will also require IV fluids. The fluids are calculated using, the Parkland formula which is; volume of fluid= total body surface area of the burn % x weight (Kg), x4. Half of the fluid is administered in the first 8 hours. A urinary catheter should be inserted., Analgesia should be given. Complex burns, burns involving the hand perineum and face and burns, >10% in adults and >5% in children should be transferred to a burns unit., Circumferential burns affecting a limb or severe torso burns impeding respiration may require, escharotomy to divide the burnt tissue., Conservative management is appropriate for superficial burns and mixed superficial burns that will, heal in 2 weeks. More complex burns may require excision and skin grafting. Excision and primary, closure is not generally practised as there is a high risk of infection., There is no evidence to support the use of anti microbial prophylaxis or topical antibiotics in burn, patients., Escharotomies, , , , Indicated in circumferential full thickness burns to the torso or limbs., Careful division of the encasing band of burn tissue will potentially improve ventilation (if the, burn involves the torso), or relieve compartment syndrome and oedema (where a limb is, involved), , References, www.euroburn.org/e107files/downloads/guidelinesburncare.pdf, Barajas-Nava LA, López-Alcalde J, Roqué i Figuls M, Solà I, Bonfill Cosp X. Antibiotic prophylaxis, for preventing burn wound infection. Cochrane Database of Systematic Reviews 2013, Issue 6. Art., No.: CD008738. DOI: 10.1002/14651858.CD008738.pub2., Hettiaratchy S & Papini R. Initial management of a major burn: assessment and resuscitation. BMJ, 2004;329:101-103, Next question
Page 3455 :
Theme: Thoracic injuries, , A., B., C., D., E., F., G., H., , Pneumothorax, Tension pneumothorax, Flail chest, Cardiac tamponade, Aorta rupture, Cardiac contusion, Diaphragmatic rupture, Acute phrenic nerve injury, , For each of the scenarios given, please select the most likely underlying injury. Each option may be, used once, more than once or not at all., , 15., , An 18 year old student is involved in a car crash, with another car crashing into the side of, the car., A CXR shows an indistinct left hemidiaphragm., You answered Pneumothorax, The correct answer is Diaphragmatic rupture, A lateral blunt injury during a road traffic accident is a common cause of diaphragmatic, rupture. Diagnosis is usually evident on chest x-ray. CXR changes include non visible, diaphragm, bowel loops in the hemithorax and displacement of the mediastinum. In most, cases direct surgical repair is the best option., , 16., , A 19 year old motorcyclist is involved in a road traffic accident. His chest movements are, irregular. He is found to have multiple rib fractures, with 2 fractures in the 3rd rib and 3, fractures in the 4th rib., You answered Pneumothorax, The correct answer is Flail chest, Multiple rib fractures with > or = 2 rib fractures in more than 2 ribs is diagnosed as a flail, chest. This is associated with pulmonary contusion., , 17., , A 19 year old student falls from a 2nd floor window. He is persistently hypotensive. A, CXR shows depression of the left main bronchus and deviation of the trachea to the right., You answered Pneumothorax
Page 3456 :
The correct answer is Aorta rupture, He has a deceleration injury, with persistent hypotension (contained haematoma). This, should indicate aorta rupture. Widened mediastinum may not always be present on a CXR., A CT angiogram will provide clearer evidence of the extent of injury. The presence of, persistent hypotension, from a early stage is more consistent with haematoma than a, tension pneumothorax in which it occurs as a final periarrest phenomena., CXR findings in diaphragmatic rupture:, Hemidiaphragm is not visible, Bowel loops in the lower half of the hemi-thorax, Mediastinum is displaced, Please rate this question:, , Discuss and give feedback, , Next question, , Thoracic trauma, Types of thoracic trauma, , Tension, pneumothorax, , , , , , , Flail chest, , , , , , , , Often laceration to lung parenchyma with flap, Pressure develops in thorax, Most common cause is mechanical ventilation in patient with, pleural injury, Symptoms overlap with cardiac tamponade, hyper-resonant, percussion note is more likely in tension pnemothorax, Chest wall disconnects from thoracic cage, Multiple rib fractures (at least two fractures per rib in at least two, ribs), Associated with pulmonary contusion, Abnormal chest motion, Avoid over hydration and fluid overload, , Pneumothorax, , , , , , Most common cause is lung laceration with air leakage, Most traumatic pneumothoraces should have a chest drain, Patients with traumatic pneumothorax should never be, mechanically ventilated until a chest drain is inserted, , Haemothorax, , , , Most commonly due to laceration of lung, intercostal vessel or
Page 3457 :
, , , , , internal mammary artery, Haemothoraces large enough to appear on CXR are treated with, large bore chest drain, Surgical exploration is warranted if >1500ml blood drained, immediately, , , , , Beck's triad: elevated venous pressure, reduced arterial pressure,, reduced heart sounds, Pulsus paradoxus, May occur with as little as 100ml blood, , Pulmonary contusion, , , , , , Most common potentially lethal chest injury, Arterial blood gases and pulse oximetry important, Early intubation within an hour if significant hypoxia, , Blunt cardiac injury, , , , , , Usually occurs secondary to chest wall injury, ECG may show features of myocardial infarction, Sequelae: hypotension, arrhythmias, cardiac wall motion, abnormalities, , Aorta disruption, , , , , , Deceleration injuries, Contained haematoma, Widened mediastinum, , Diaphragm, disruption, , , , Most due to motor vehicle accidents and blunt trauma causing, large radial tears (laceration injuries result in small tears), More common on left side, Insert gastric tube, may pass into intrathoracic stomach, , Cardiac tamponade, , , , , Mediastinal, traversing wounds, , , , , , Entrance wound in one hemithorax and exit wound/foreign body, in opposite hemithorax, Mediastinal haematoma or pleural cap suggests great vessel, injury, Mortality is 20%, , References, ATLS Manual 8th Edition, Next question
Page 3458 :
Which of the features below, following a head injury, is not an indication for an immediate CT head, scan in children?, , Drowsiness, , A single, discrete episode of vomiting, , A 9 month old child with a 6cm haematoma on the head, , Numb left arm, , Suspicion of a non accidental head injury, , Whilst not an indication for immediate CT there should be a low threshold for admission and, observation., Please rate this question:, , Discuss and give feedback, , Next question, , Head injury paediatrics, Criteria for immediate request for CT scan of the head (children), * Loss of consciousness lasting more than 5 minutes (witnessed), * Amnesia (antegrade or retrograde) lasting more than 5 minutes, * Abnormal drowsiness, * Three or more discrete episodes of vomiting, * Clinical suspicion of non-accidental injury, * Post-traumatic seizure but no history of epilepsy, * GCS less than 14, or for a baby under 1 year GCS (paediatric) less than 15, on assessment in the, emergency department, * Suspicion of open or depressed skull injury or tense fontanelle, * Any sign of basal skull fracture (haemotympanum, panda' eyes, cerebrospinal fluid leakage from
Page 3459 :
the ear or nose, Battle's sign), * Focal neurological deficit, * If under 1 year, presence of bruise, swelling or laceration of more than 5 cm on the head, * Dangerous mechanism of injury (high-speed road traffic accident either as pedestrian, cyclist or, vehicle occupant, fall from a height of greater than 3 m, high-speed injury from a projectile or an, object), Next question
Page 3460 :
Theme: Management of osteomyelitis, , A., B., C., D., E., F., G., , Lautenbach regime, Below knee amputation, Hindquater amputation, Above knee amputation, Removal of metalwork and implantation of local antibiotics, Removal of metalwork and bone grafting, Intravenous antibiotics, , Which option is the best management plan? Each option may be used once, more than once or not, at all, , 19., , A 65 year old type 2 diabetic with poor glycaemic control is admitted with forefoot, cellulitis. X-ray of the foot shows some evidence of osteomyelitis of the 2nd ray but, overlying skin is healthy., You answered Lautenbach regime, The correct answer is Intravenous antibiotics, It is worth attempting to try and resolve this situation with antibiotics at first presentation., A primary amputation will not heal well and may result in progressive surgery., , 20., , A 28 year old infantryman is shot in the leg during combat. Primary debridement and, lavage of the wound is undertaken. Several months post surgery there is ongoing discharge, from a sinus originating in the proximal femur, X-ray and MRI shows evidence of, osteomyelitis of the proximal femur. There are no obvious sequestra., Lautenbach regime, This involves local administration of antibiotics via intramedullary lines and is an, intensive regime. However, the morbidity of a high above knee or hindquater amputation, makes conservative management an attractive option., , 21., , A 70 year old man undergoes a revision total hip replacement. 10 days post operatively the, hip dislocates and pus is discharging from the wound. He is systemically unwell with a, temperature of 38.5 and WCC 19., You answered Lautenbach regime, The correct answer is Removal of metalwork and implantation of local antibiotics
Page 3461 :
Removal of metal work implantation of gentamicin beads and delayed revision is the, mainstay of managing this complication., Please rate this question:, , Discuss and give feedback, , Next question, , Osteomyelitis, Infection of the bone, Causes, , , , S aureus and occasionally Enterobacter or Streptococcus species, In sickle cell: Salmonella species, , Clinical features, , , , , Erythema, Pain, Fever, , Investigation, , , , X-ray: lytic centre with a ring of sclerosis, Bone biopsy and culture, , Treatment, , , , Prolonged antibiotics, Sequestra may need surgical removal, Next question
Page 3462 :
What is the least likely examination finding in patients with Le Fort II fractures?, , Excessive mobility of the palate, , Paraesthesia in the region supplied by the inferior alveolar nerve, , Malocclusion of the teeth, , Enopthalmos, , Parasthesia in the region supplied by the infraorbital nerve, , Le Fort II fractures have a pyramidal shape. The fracture line involves the orbit and extends to, involve the bridge of the nose and the ethmoids. In continues to involve the infraorbital rim and, usually through the infraorbital foramen. As a result infraorbital parasthesia, palatal mobility and, malocclusion are common findings. Severe fractures may result in endopthalmos. However, the, fracture does not, by definition, involve the inferior alveolar nerve., Please rate this question:, , Discuss and give feedback, , Next question, , Craniomaxillofacial injuries, Craniomaxillofacial injuries in the UK are due to:, , , , , , Interpersonal violence (52%), Motor vehicle accidents (16%), Sporting injuries (19%), Falls (11%), , Le Fort Fractures, , Grade, , Feature, , Le, Fort 1, , The fracture extends from the nasal septum to the lateral pyriform rims, travels, horizontally above the teeth apices, crosses below the zygomaticomaxillary junction, and
Page 3463 :
Grade, , Feature, , traverses the pterygomaxillary junction to interrupt the pterygoid plates., , Le, Fort 2, , These fractures have a pyramidal shape and extend from the nasal bridge at or below the, nasofrontal suture through the frontal process of the maxilla, inferolaterally through the, lacrimal bones and inferior orbital floor and rim through or near the inferior orbital, foramen, and inferiorly through the anterior wall of the maxillary sinus; it then travels, under the zygoma, across the pterygomaxillary fissure, and through the pterygoid plates., , Le, Fort 3, , These fractures start at the nasofrontal and frontomaxillary sutures and extend posteriorly, along the medial wall of the orbit through the nasolacrimal groove and ethmoid bones., The thicker sphenoid bone posteriorly usually prevents continuation of the fracture into, the optic canal. Instead, the fracture continues along the floor of the orbit along the, inferior orbital fissure and continues superolaterally through the lateral orbital wall,, through the zygomaticofrontal junction and the zygomatic arch. Intranasally, a branch of, the fracture extends through the base of the perpendicular plate of the ethmoid, through, the vomer, and through the interface of the pterygoid plates to the base of the sphenoid., This type of fracture predisposes the patient to CSF rhinorrhea more commonly than the, other types., , Ocular injuries, Superior orbital fissure syndrome, Severe force to the lateral wall of the orbit resulting in compression of neurovascular structures., Results in :, , , , , , Complete opthalmoplegia and ptosis (Cranial nerves 3, 4, 6 and nerve to levator palpebrae, superioris), Relative afferent pupillary defect, Dilatation of the pupil and loss of accommodation and corneal reflexes, Altered sensation from forehead to vertex (frontal branch of trigeminal nerve), , Orbital blow out fracture, Typically occurs when an object of slightly larger diameter than the orbital rim strikes the, incompressible eyeball. The bone fragment is displaced downwards into the antral cavity, remaining, attached to the orbital periosteum. Periorbital fat may be herniated through the defect, interfering, with the inferior rectus and inferior oblique muscles which are contained within the same fascial, sheath. This prevents upward movement and outward rotation of the eye and the patient, experiences diplopia on upward gaze. The initial bruising and swelling may make assessment, difficult and patients should usually be reviewed 5 days later. Residual defects may require orbital, floor reconstruction.
Page 3464 :
Nasal Fractures, , , , , , , Common injury, Ensure new and not old deformity, Control epistaxis, CSF rhinorrhoea implies that the cribriform plate has been breached and antibiotics will be, required., Usually best to allow bruising and swelling to settle and then review patient clinically. Major, persistent deformity requires fracture manipulation, best performed within 10 days of injury., , Retrobulbar haemorrhage, Rare but important ocular emergency. Presents with:, , , , , , , Pain (usually sharp and within the globe), Proptosis, Pupil reactions are lost, Paralysis (eye movements lost), Visual acuity is lost (colour vision is lost first), , May be the result of Le Fort type facial fractures., Management:, , , , , , Mannitol 1g/Kg as 20% infusion, Osmotic diuretic, Contra-indicated in congestive heart, failure and pulmonary oedema, Acetazolamide 500mg IV, (Monitor FBC/U+E) Reduces aqueous pressure by inhibition of, carbonic anhydrase (used in glaucoma), Dexamethasone 8mg orally or intravenously, In a traumatic setting an urgent cantholysis may be needed prior to definitive surgery., , Consider, Papaverine 40mg smooth muscle relaxant, Dextran 40 500mls IV improves perfusion, Next question
Page 3465 :
A Medical F1 phones you as he is concerned his patient has had a major internal bleed. The patient, is 42 years old and is known to have sickle cell anaemia. His blood results are:, Hb 3.7 g /dl, Reticulocyte count 0.4%, His Hb is normally 7g/dl. What is the diagnosis?, , Psoas haemorrhage, , Acute sequestration, , Parvovirus, , Splenic haemorrhage, , Acute haemolysis, , A sudden anemia and a LOW reticulocute count indicates parvovirus. Acute sequestration and, haemolysis causes a high reticulocyte count. There is no clinical indication to suspect a bleed,, therefore you can advise the F1 not to panic and to speak to the haematologists!, Please rate this question:, , Discuss and give feedback, , Next question, , Sickle cell anaemia, , , , , , , , , , Autosomal recessive, Single base mutation, Deoxygenated cells become sickle in shape, Causes: short red cell survival, obstruction of microvessels and infarction, Sickling is precipitated by: dehydration, infection, hypoxia, Manifest at 6 months age, Africans, Middle East, Indian, Diagnosis: Hb electrophoresis, , Sickle crises
Page 3468 :
Theme: Management of chest trauma, , A., B., C., D., E., F., G., H., I., , Thoracotomy in operating theatre, 36F intercostal chest drain, 14F intercostal chest drain, Active observation, Thoracotomy in the emergency room, MRI of aortic arch, Bronchoscopy, Pericardiocentesis, Further transfusion, , For each of the following scenarios please select the most appropriate next stage of management., Each option may be used once, more than once or not at all., , 24., , A 30 year old male is stabbed outside a nightclub he has a brisk haemoptysis and in, casualty has a chest drain inserted into the left chest. This drained 750ml frank blood. He, fails to improve with this intervention. He has received 4 units of blood. His CVP is now, 13., You answered Thoracotomy in operating theatre, The correct answer is Pericardiocentesis, This man has cardiac tamponade. The raised CVP in the setting of haemodynamic, compromise is the pointer to this. Whilst he will almost certainly require surgery, he, requires urgent decompression of his heart first., , 25., , A 26 year old male falls from a cliff. He suffers from multiple fractures and has a right, sided pneumothorax that has collapsed a 1/3 of his lung. He has no respiratory, compromise., You answered Thoracotomy in operating theatre, The correct answer is 14F intercostal chest drain, Simple observation is unsafe as he will almost certainly have suffered an oblique, laceration to his lung. These can become tension pneumothoraces. In the absence of blood, a 36 F drain is probably not required, , 26., , An 18 year old male is shot in the left chest he was unstable but his blood pressure has, improved with 1 litre of colloid. His chest x-ray shows a left sided pneumothorax with no, lung visible.
Page 3469 :
You answered Thoracotomy in operating theatre, The correct answer is 36F intercostal chest drain, This man requires wide bore intercostal tube drainage. Smaller intercostal chest drains can, become occluded with blood clot and fail to function adequately., Please rate this question:, , Discuss and give feedback, , Next question, , Thoracic trauma, Types of thoracic trauma, , Tension, pneumothorax, , , , , , , Flail chest, , , , , , , , Often laceration to lung parenchyma with flap, Pressure develops in thorax, Most common cause is mechanical ventilation in patient with, pleural injury, Symptoms overlap with cardiac tamponade, hyper-resonant, percussion note is more likely in tension pnemothorax, Chest wall disconnects from thoracic cage, Multiple rib fractures (at least two fractures per rib in at least two, ribs), Associated with pulmonary contusion, Abnormal chest motion, Avoid over hydration and fluid overload, , Pneumothorax, , , , , , Most common cause is lung laceration with air leakage, Most traumatic pneumothoraces should have a chest drain, Patients with traumatic pneumothorax should never be, mechanically ventilated until a chest drain is inserted, , Haemothorax, , , , Most commonly due to laceration of lung, intercostal vessel or, internal mammary artery, Haemothoraces large enough to appear on CXR are treated with, large bore chest drain, Surgical exploration is warranted if >1500ml blood drained, , ,
Page 3470 :
immediately, , , , , Beck's triad: elevated venous pressure, reduced arterial pressure,, reduced heart sounds, Pulsus paradoxus, May occur with as little as 100ml blood, , Pulmonary contusion, , , , , , Most common potentially lethal chest injury, Arterial blood gases and pulse oximetry important, Early intubation within an hour if significant hypoxia, , Blunt cardiac injury, , , , , , Usually occurs secondary to chest wall injury, ECG may show features of myocardial infarction, Sequelae: hypotension, arrhythmias, cardiac wall motion, abnormalities, , Aorta disruption, , , , , , Deceleration injuries, Contained haematoma, Widened mediastinum, , Diaphragm, disruption, , , , Most due to motor vehicle accidents and blunt trauma causing, large radial tears (laceration injuries result in small tears), More common on left side, Insert gastric tube, may pass into intrathoracic stomach, , Cardiac tamponade, , , , , Mediastinal, traversing wounds, , , , , , Entrance wound in one hemithorax and exit wound/foreign body, in opposite hemithorax, Mediastinal haematoma or pleural cap suggests great vessel, injury, Mortality is 20%, , References, ATLS Manual 8th Edition, Next question
Page 3471 :
Theme: Management of burns, , A., B., C., D., E., F., G., H., , Escharotomy, Endotracheal intubation, Broad spectrum intravenous antibiotics, Intravenous fluids calculated according to extent of burned area, Discharge with review in outpatients, Transfer to regional burn centre once stabilised, Split thickness skin graft, Full thickness skin graft, , What is the best management for the scenario given? Each option may be used once, more than, once or not at all., , 27., , A 34 year old women trips over and falls into a bonfire whilst intoxicated at a party. She, suffers burns to her arms, torso and face. These are calculated to be 25% body surface, area. She is otherwise stable. The burns to the torso are superficial, her left forearm has a, full thickness burn and the burns to her face are superficial. There is no airway, compromise. She has received 1000ml of intravenous Hartman's solution, with a further, 1000ml prescribed to run over 4 hours., You answered Escharotomy, The correct answer is Transfer to regional burn centre once stabilised, This women has been resuscitated and requires transfer for specialist management., , 28., , A 20 year old man is trapped in a warehouse fire. He has sustained 60% burns to his torso, and limbs. The limb burns are partial thickness but the torso burns are full thickness. He, was intubated by paramedics at the scene and is receiving intravenous fluids. His, ventilation pressure requirements are rising., Escharotomy, He requires an escharotomy as this will be contributing to impaired ventilation., , 29., , An 18 year old man accidentally pours boiling water onto his left arm. The area is, erythematous and has a blister measuring 5cm. The wound is extremely painful., You answered Escharotomy, The correct answer is Discharge with review in outpatients
Page 3472 :
This is a superficial burn and should recover with no further input than simple dressings,, an alternative would be deroofing the blister and applying dressings prior to outpatient, review., Please rate this question:, , Discuss and give feedback, , Next question, , Burns, Burns may be thermal, chemical or electrical. In the former category are burns which occur as a, result of heat. Chemical burns occur when the skin is exposed to an extremely caustic or alkaline, substance. Electrical burns occur following exposure to electrical current. The immediate, management includes removal of the burning source which usually includes irrigation of the burned, area. A detailed assessment then needs to be made of the extent of the burns and a number of, charts are available for recording this information. The degree of injury relates to the temperature, and duration of exposure. Most domestic burns are mainly scalds in young children., Following the burn, there is a local response with progressive tissue loss and release of, inflammatory cytokines. Systemically, there are cardiovascular effects resulting from fluid loss and, sequestration of fluid into the third space. There is a marked catabolic response. Immunosupression, is common with large burns and bacterial translocation from the gut lumen is a recognised event., Sepsis is a common cause of death following major burns., Types of burn, , Type of burn, , Skin layers, affected, , Skin, appearance, , Blanching, , Management, , Epidermal/Superficial, , Epidermis, , Red, moist, , Yes, , Superficial partial, thickness, , Epidermis and part, of papillary dermis, affected, , Pale, dry, , Yes, , Normally heals, with no, intervention, , Deep partial thickness, , Epidermis, whole, papillary dermis, affected, , Mottled red, colour, , No, , Needs surgical, intervention, (depending on site)
Page 3473 :
Full thickness, , Whole skin layer, and subcutaneous, tissue affected, , Dry, leathery, hard wound, , No, , Burns centre, , Depth of burn assessment, , , , , , Bleeding on needle prick, Sensation, Appearance, Blanching to pressure, , Percentage burn estimation, Lund Browder chart: most accurate even in children, Wallace rule of nines, Palmar surface: surface area palm = 0.8% burn, >15% body surface area burns in adults needs urgent burn fluid resuscitation, Transfer to burn centre if:, , , , , , Need burn shock resuscitation, Face/hands/genitals affected, Deep partial thickness or full thickness burns, Significant electrical/chemical burns, , Management, The initial aim is to stop the burning process and resuscitate the patient. Intravenous fluids will be, required for children with burns greater than 10% of total body surface area. Adults with burns, greater than 15% of total body surface area will also require IV fluids. The fluids are calculated using, the Parkland formula which is; volume of fluid= total body surface area of the burn % x weight (Kg), x4. Half of the fluid is administered in the first 8 hours. A urinary catheter should be inserted., Analgesia should be given. Complex burns, burns involving the hand perineum and face and burns, >10% in adults and >5% in children should be transferred to a burns unit., Circumferential burns affecting a limb or severe torso burns impeding respiration may require, escharotomy to divide the burnt tissue., Conservative management is appropriate for superficial burns and mixed superficial burns that will, heal in 2 weeks. More complex burns may require excision and skin grafting. Excision and primary, closure is not generally practised as there is a high risk of infection., There is no evidence to support the use of anti microbial prophylaxis or topical antibiotics in burn, patients., Escharotomies
Page 3475 :
A 52 year old male type 2 diabetic is admitted to the vascular ward for a femoral popliteal bypass., He suddenly develops expressive dysphasia and marked right sided weakness. The Senior house, officer arranges a CT head scan which shows a 60% left middle cerebral artery territory infarct., There are no beds on the stroke unit. Overnight the patient becomes unresponsive and a CT head, confirms no bleed. What is the next best management option?, , IV heparin, , Clopidogrel, , Burr hole surgery, , Aspirin, , Hemicranieotomy, , The likely cause for the reduced consciousness is raised intracranial pressure due to increasing, cerebral oedema related to the infarct. In this situation, urgent neurosurgical review is needed for, possible decompressive hemicranieotomy to relieve the pressure. Ideally no further antiplatelet or, anticoagulation therapy should be given until a plan for surgery is confirmed., Indications for hemicranieotomy include:, , , , , , , Age under 60 years, Clinical deficit in middle cerebral artery territory, Decreased consciousness, >50% territory infarct, , Please rate this question:, , Discuss and give feedback, , Next question, , Stroke: types, Primary intracerebral, haemorrhage (PICH, c. 10%), , , , Presents with headache, vomiting, loss of, consciousness
Page 3476 :
Total anterior circulation, infarcts (TACI, c. 15%), , , , , , , Involves middle and anterior cerebral arteries, Hemiparesis/hemisensory loss, Homonymous hemianopia, Higher cognitive dysfunction e.g. Dysphasia, , Partial anterior circulation, infarcts (PACI, c. 25%), , , , Involves smaller arteries of anterior circulation e.g., upper or lower division of middle cerebral artery, Higher cognitive dysfunction or two of the three TACI, features, , , , Lacunar infarcts (LACI, c., 25%), , , , , Involves perforating arteries around the internal, capsule, thalamus and basal ganglia, Present with either isolated hemiparesis, hemisensory, loss or hemiparesis with limb ataxia, , Posterior circulation infarcts, (POCI, c. 25%), , , , , , Vertebrobasilar arteries, Presents with features of brainstem damage, Ataxia, disorders of gaze and vision, cranial nerve, lesions, , Lateral medullary syndrome, (posterior inferior cerebellar, artery), , , , , , Wallenberg's syndrome, Ipsilateral: ataxia, nystagmus, dysphagia, facial, numbness, cranial nerve palsy, Contralateral: limb sensory loss, , , , , Ipsilateral III palsy, Contralateral weakness, , Weber's syndrome, , -------------------------------------Anterior cerebral artery, , , , Contralateral hemiparesis and sensory loss, lower extremity > upper, Disconnection syndrome, , Middle cerebral artery
Page 3478 :
A 56-year-old female is admitted to ITU with a severe pancreatitis. Thyroid function tests show:, TSH = 0.5 Low, Thyroxine = 1.0 Low, T3 = 0.5 Low, What is the most likely cause?, , Sick euthyroid syndrome, , Graves disease, , Hashimotos thyroiditis, , Levothyroxine, , None of the above, , This patient has sick euthyroid syndrome as all thyroid parameters are reduced. Graves disease and, levothyroxine will cause hyperthyroidism (low TSH and elevated thyroxine/T3). Hashimotos, thyroiditis is associated with hypothyroidism (high TSH and low thyroxine/T3)., Please rate this question:, , Discuss and give feedback, , Sick euthyroid syndrome, In sick euthyroid syndrome (now referred to as non-thyroidal illness) it is often said that everything, (TSH, thyroxine and T3) is low. In the majority of cases however the TSH level is within the normal, range (inappropriately normal given the low thyroxine and T3)., Changes are reversible upon recovery from the systemic illness.
Page 3480 :
Theme: Hand disorders, , A., B., C., D., E., F., G., H., I., , de Quervain's tenosynovitis, Dupuytren's contracture, Bouchard's nodes, Ganglion, Carpal tunnel syndrome, Radial nerve injury, Ulnar nerve injury, Heberden's nodes, Tendon sheath infection, , Please select the most likely diagnosis to account for the scenario given. Each option may be used, once, more than once or not at all., , 1., , A 49 -year-old male presents with discomfort in the fingers of his left hand. On examination, the ring and little fingers of his left hand are flexed and unable to extend completely. He is, able to make a fist with the hand. Palpation reveals thickened nodules on the medial half of, the palm., You answered de Quervain's tenosynovitis, The correct answer is Dupuytren's contracture, Discomfort of the hand is not uncommon in Dupuytrens contracture, true pain is unusual., The disease most commonly affects the ring and little fingers., , 2., , A 62 year old man presents after his wife commented on the unusual shape of his fingers., On examination he has a hard swelling adjacent to the distal interphalangeal joint of his, index finger of the right hand with lateral deviation of the finger tip. There is no sensory, disturbance and the swelling is not tender., You answered de Quervain's tenosynovitis, The correct answer is Heberden's nodes, These are bony outgrowths that occur in the distal interphalangeal joint in association with, osteoarthritis. They may skew the finger tip sideways. Bouchards nodes are similar, but, affect the proximal interphalangeal joint., , 3., , A 57 year - old lady presents with a three month history of pins and needles in the fingers of, the right hand, particularly at night. On examination, there is some loss of the sensation over, the palmar aspect of the lateral three fingers and wasting of the thenar eminence.
Page 3481 :
You answered de Quervain's tenosynovitis, The correct answer is Carpal tunnel syndrome, Carpal tunnel syndrome commonly produces pain at night as the wrists are flexed during, sleep. Compromise of the median nerve may produce wasting of the thenar eminence, muscles., Please rate this question:, , Discuss and give feedback, , Next question, , Hand diseases, Dupuytrens contracture, , , , , , , , , Fixed flexion contracture of the hand where the fingers bend towards the palm and cannot be, fully extended., Caused by underlying contractures of the palmar aponeurosis . The ring finger and little, finger are the fingers most commonly affected. The middle finger may be affected in, advanced cases, but the index finger and the thumb are nearly always spared., Progresses slowly and is usually painless. In patients with this condition, the tissues under, the skin on the palm of the hand thicken and shorten so that the tendons connected to the, fingers cannot move freely. The palmar aponeurosis becomes hyperplastic and undergoes, contracture., Commonest in males over 40 years of age., Association with liver cirrhosis and alcoholism. However, many cases are idiopathic., Treatment is surgical and involves fasciectomy. However, the condition may recur and many, surgical therapies are associated with risk of neurovascular damage to the digital nerves and, arteries., , Carpel tunnel syndrome, , , , , , , , Idiopathic median neuropathy at the carpal tunnel., Characterised by altered sensation of the lateral 3 fingers., The condition is commoner in females and is associated with other connective tissue, disorders such as rheumatoid disease. It may also occur following trauma to the distal, radius., Symptoms occur mainly at night in early stages of the condition., Examination may demonstrate wasting of the muscles of the thenar eminence and, symptoms may be reproduced by Tinels test (compression of the contents of the carpal, tunnel)., Formal diagnosis is usually made by electrophysiological studies.
Page 3482 :
, , Treatment is by surgical decompression of the carpal tunnel, a procedure achieved by, division of the flexor retinaculum. Non - surgical options include splinting and bracing., , Miscellaneous hand lumps, , Osler's, nodes, , Osler's nodes are painful, red, raised lesions found on the hands and feet. They are, the result of the deposition of immune complexes., , Bouchards, nodes, , Hard, bony outgrowths or gelatinous cysts on the proximal interphalangeal joints, (the middle joints of fingers or toes.) They are a sign of osteoarthritis, and are, caused by formation of calcific spurs of the articular cartilage., , Heberdens, nodes, , Typically develop in middle age, beginning either with a chronic swelling of the, affected joints or the sudden painful onset of redness, numbness, and loss of, manual dexterity. This initial inflammation and pain eventually subsides, and the, patient is left with a permanent bony outgrowth that often skews the fingertip, sideways. It typically affects the DIP joint., , Ganglion, , Swelling in association with a tendon sheath commonly near a joint. They are, common lesions in the wrist and hand. Usually they are asymptomatic and cause, little in the way of functional compromise. They are fluid filled although the fluid, is similar to synovial fluid it is slightly more viscous. When the cysts are, troublesome they may be excised.
Page 3483 :
Theme: Hand disorders, , A., B., C., D., E., F., G., H., I., , Malignant fibrous histiocytoma, Oslers nodes, Heberdens nodes, Bouchards nodes, Carpal tunnel syndrome, Complex regional pain syndrome, Osteoclastoma, Osteosarcoma, Ganglion, , Please select the most likely diagnosis for the lesion described. Each option may be used once,, more than once or not at all., , 4., , A 42 year old lady who has systemic lupus erythematosus presents to the clinic with a 5 day, history of a painful purple lesion on her index finger. On examination she has a tender red, lesion on the index finger., You answered Malignant fibrous histiocytoma, The correct answer is Oslers nodes, Osler nodes are normally described as tender, purple/red raised lesions with a pale centre., These lesions occur as a result of immune complex deposition. These occur most often in, association with endocarditis. However, other causes include SLE, gonorrhoea, typhoid and, haemolytic anaemia., , 5., , A 62 year old lady presents with an non tender lump overlying the distal interphalangeal, joint of the index finger. On examination she has a hard, non tender lump overlying the joint, and deviation of the tip of the finger., You answered Malignant fibrous histiocytoma, The correct answer is Heberdens nodes, Heberdens nodes may produce swelling of the distal interphalangeal joint with deviation of, the finger tip., , 6., , A 17 year old boy is brought to the clinic by his mother who is concerned about a lesion, that has developed on the dorsal surface of his left hand. On examination he has a soft, fluctuant swelling on the dorsal aspect of the hand, it is most obvious on making a fist.
Page 3484 :
You answered Malignant fibrous histiocytoma, The correct answer is Ganglion, Ganglions commonly occur in the hand and are usually associated with tendons. They are, typically soft and fluctuant. They do not require removal unless they are atypical or causing, symptoms., Please rate this question:, , Discuss and give feedback, , Hand diseases, Dupuytrens contracture, , , , , , , , , Fixed flexion contracture of the hand where the fingers bend towards the palm and cannot be, fully extended., Caused by underlying contractures of the palmar aponeurosis . The ring finger and little, finger are the fingers most commonly affected. The middle finger may be affected in, advanced cases, but the index finger and the thumb are nearly always spared., Progresses slowly and is usually painless. In patients with this condition, the tissues under, the skin on the palm of the hand thicken and shorten so that the tendons connected to the, fingers cannot move freely. The palmar aponeurosis becomes hyperplastic and undergoes, contracture., Commonest in males over 40 years of age., Association with liver cirrhosis and alcoholism. However, many cases are idiopathic., Treatment is surgical and involves fasciectomy. However, the condition may recur and many, surgical therapies are associated with risk of neurovascular damage to the digital nerves and, arteries., , Carpel tunnel syndrome, , , , , , , , , Idiopathic median neuropathy at the carpal tunnel., Characterised by altered sensation of the lateral 3 fingers., The condition is commoner in females and is associated with other connective tissue, disorders such as rheumatoid disease. It may also occur following trauma to the distal, radius., Symptoms occur mainly at night in early stages of the condition., Examination may demonstrate wasting of the muscles of the thenar eminence and, symptoms may be reproduced by Tinels test (compression of the contents of the carpal, tunnel)., Formal diagnosis is usually made by electrophysiological studies., Treatment is by surgical decompression of the carpal tunnel, a procedure achieved by, division of the flexor retinaculum. Non - surgical options include splinting and bracing.
Page 3485 :
Miscellaneous hand lumps, , Osler's, nodes, , Osler's nodes are painful, red, raised lesions found on the hands and feet. They are, the result of the deposition of immune complexes., , Bouchards, nodes, , Hard, bony outgrowths or gelatinous cysts on the proximal interphalangeal joints, (the middle joints of fingers or toes.) They are a sign of osteoarthritis, and are, caused by formation of calcific spurs of the articular cartilage., , Heberdens, nodes, , Typically develop in middle age, beginning either with a chronic swelling of the, affected joints or the sudden painful onset of redness, numbness, and loss of, manual dexterity. This initial inflammation and pain eventually subsides, and the, patient is left with a permanent bony outgrowth that often skews the fingertip, sideways. It typically affects the DIP joint., , Ganglion, , Swelling in association with a tendon sheath commonly near a joint. They are, common lesions in the wrist and hand. Usually they are asymptomatic and cause, little in the way of functional compromise. They are fluid filled although the fluid, is similar to synovial fluid it is slightly more viscous. When the cysts are, troublesome they may be excised.
Page 3486 :
Theme: Parotid gland disease, , A., B., C., D., E., F., , Pleomorphic adenoma, Adenoid cystic carcinoma, Sarcoid, Sjogrens syndrome, Sialolithiasis, Wharthins tumour, , Please select the most likely explanation for the following patients with parotid gland symptoms., Each option may be used once, more than once or not at all., , 1., , A 50 year old female presents with bilateral parotid gland swelling and symptoms of a dry, mouth. On examination she has bilateral facial nerve palsies. This improved following, steroid treatment., You answered Pleomorphic adenoma, The correct answer is Sarcoid, Theme from April 2013 exam, Sarcoid occurs bilaterally in 70% of cases and facial nerve involvement is recognised., Treatment is conservative in most cases although individuals with facial nerve palsy will, usually receive steroids with good effect., , 2., , A 50 year old women presents with a diffuse swelling in the region of her right parotid, together with facial pain. On examination she has a right sided facial nerve palsy., You answered Pleomorphic adenoma, The correct answer is Adenoid cystic carcinoma, Theme from April 2015 exam, Adenoid cystic carcinoma commonly infiltrates the facial nerve and may cause neuropathy, and facial pain., , 3., , A 50 year old lady presents with symptoms of a dry mouth that has been present for the past, few months. She also has a sensation of grittiness in her eyes. On examination she has a, diffuse swelling of her parotid gland. There is no evidence of facial nerve palsy., You answered Pleomorphic adenoma, The correct answer is Sjogrens syndrome
Page 3487 :
Theme from April 2014 exam, Most patients with Sjogrens present in the post menopausal years. Multi system, involvement is common., Please rate this question:, , Discuss and give feedback, , Next question, , Parotid gland clinical, Benign neoplasms, Up to 80% of all salivary gland tumours occur in the parotid gland and up to 80% of these are, benign. There is no consistent correlation between the rate of growth and the malignant potential of, the lesion. However, benign tumours should not invade structures such as the facial nerve., With the exception of Warthins tumours, they are commoner in women than men. The median age of, developing a lesion is in the 5th decade of life., Benign tumour types, , Tumour type, , Features, , Benign pleomorphic adenoma or, benign mixed tumor, , Most common parotid neoplasm (80%), Proliferation of epithelial and myoepithelial cells of the ducts, and an increase in stromal components, Slow growing, lobular, and not well encapsulated, Recurrence rate of 1-5% with appropriate excision, (parotidectomy), Recurrence possibly secondary to capsular disruption during, surgery, Malignant degeneration occurring in 2-10% of adenomas, observed for long periods, with carcinoma ex-pleomorphic, adenoma occurring most frequently as adenocarcinoma, , Warthin tumor (papillary, cystadenoma lymphoma or, adenolymphoma), , Second most common benign parotid tumor (5%), Most common bilateral benign neoplasm of the parotid, Marked male as compared to female predominance, Occurs later in life (sixth and seventh decades), Presents as a lymphocytic infiltrate and cystic epithelial, proliferation, May represent heterotopic salivary gland epithelial tissue, trapped within intraparotid lymph nodes, Incidence of bilaterality and multicentricity of 10%
Page 3488 :
Tumour type, , Features, , Malignant transformation rare (almost unheard of), , Monomorphic adenoma, , Account for less than 5% of tumours, Slow growing, Consist of only one morphological cell type (hence term, mono), Include; basal cell adenoma, canalicular adenoma,, oncocytoma, myoepitheliomas, , Haemangioma, , Should be considered in the differential of a parotid mass in a, child, Accounts for 90% of parotid tumours in children less than 1, year of age, Hypervascular on imaging, Spontaneous regression may occur and malignant, transformation is almost unheard of, , Malignant salivary gland tumours, Types of malignancy, , Mucoepidermoid, carcinoma, , 30% of all parotid malignancies, Usually low potential for local invasiveness and metastasis (depends, mainly on grade), , Adenoid cystic, carcinoma, , Unpredictable growth pattern, Tendency for perineural spread, Nerve growth may display skip lesions resulting in incomplete excision, Distant metastasis more common (visceral rather than nodal spread), 5 year survival 35%, , Mixed tumours, , Often a malignancy occurring in a previously benign parotid lesion, , Acinic cell carcinoma, , Intermediate grade malignancy, May show perineural invasion, Low potential for distant metastasis
Page 3489 :
5 year survival 80%, , Adenocarcinoma, , Develops from secretory portion of gland, Risk of regional nodal and distant metastasis, 5 year survival depends upon stage at presentation, may be up to 75%, with small lesions with no nodal involvement, , Lymphoma, , Large rubbery lesion, may occur in association with Warthins tumours, Diagnosis should be based on regional nodal biopsy rather than parotid, resection, Treatment is with chemotherapy (and radiotherapy), , Diagnostic evaluation, , , , , , , , Plain x-rays may be used to exclude calculi, Sialography may be used to delineate ductal anatomy, FNAC is used in most cases, Superficial parotidectomy may be either diagnostic of therapeutic depending upon the nature, of the lesion, Where malignancy is suspected the primary approach should be definitive resection rather, than excisional biopsy, CT/ MRI may be used in cases of malignancy for staging primary disease, , Treatment, For nearly all lesions this consists of surgical resection, for benign disease this will usually consist of, a superficial parotidectomy. For malignant disease a radical or extended radical parotidectomy is, performed. The facial nerve is included in the resection if involved. The need for neck dissection is, determined by the potential for nodal involvement., Other parotid disorders, HIV infection, , , , , Lymphoepithelial cysts associated with HIV occur almost exclusively in the parotid, Typically presents as bilateral, multicystic, symmetrical swelling, Risk of malignant transformation is low and management usually conservative, , Sjogren syndrome, , , , Autoimmune disorder characterised by parotid enlargement, xerostomia and, keratoconjunctivitis sicca, 90% of cases occur in females
Page 3490 :
, , , , , , Second most common connective tissue disorder, Bilateral, non tender enlargement of the gland is usual, Histologically, the usual findings are of a lymphocytic infiltrate in acinar units and, epimyoepithelial islands surrounded by lymphoid stroma, Treatment is supportive, There is an increased risk of subsequent lymphoma, , Sarcoid, , , , , , , Parotid involvement occurs in 6% of patients with sarcoid, Bilateral in most cases, Gland is not tender, Xerostomia may occur, Management of isolated parotid disease is usually conservative, Next question
Page 3491 :
A 53 year old man presents with a mass lesion slightly inferior to the tragus of his right ear. An FNA, and USS are performed and a 2cm pleomorphic adenoma is diagnosed. What is the most, appropriate course of action?, , USS guided core biopsy, , Radical parotidectomy, , Superficial parotidectomy, , Discharge, , MRI scanning of the region, Pleomorphic adenoma of the parotid= surgical excision, Theme from September 2014 Exam, Pleomorphic adenomas a usually benign tumours. However, they will enlarge over time and a, proportion can undergo malignant transformation. Therefore, all pleomorphic adenomas are excised, and a superficial parotidectomy is generally the procedure of choice. The facial nerve is preserved., More recently, there has been a move towards partial superficial parotidectomy. However, complete, resection of the lesion is still madatory., Please rate this question:, , Discuss and give feedback, , Next question, , Parotid gland clinical, Benign neoplasms, Up to 80% of all salivary gland tumours occur in the parotid gland and up to 80% of these are, benign. There is no consistent correlation between the rate of growth and the malignant potential of, the lesion. However, benign tumours should not invade structures such as the facial nerve., With the exception of Warthins tumours, they are commoner in women than men. The median age of, developing a lesion is in the 5th decade of life., Benign tumour types, , Tumour type, , Features, , Benign pleomorphic adenoma or, , Most common parotid neoplasm (80%)
Page 3492 :
Tumour type, , Features, , benign mixed tumor, , Proliferation of epithelial and myoepithelial cells of the ducts, and an increase in stromal components, Slow growing, lobular, and not well encapsulated, Recurrence rate of 1-5% with appropriate excision, (parotidectomy), Recurrence possibly secondary to capsular disruption during, surgery, Malignant degeneration occurring in 2-10% of adenomas, observed for long periods, with carcinoma ex-pleomorphic, adenoma occurring most frequently as adenocarcinoma, , Warthin tumor (papillary, cystadenoma lymphoma or, adenolymphoma), , Second most common benign parotid tumor (5%), Most common bilateral benign neoplasm of the parotid, Marked male as compared to female predominance, Occurs later in life (sixth and seventh decades), Presents as a lymphocytic infiltrate and cystic epithelial, proliferation, May represent heterotopic salivary gland epithelial tissue, trapped within intraparotid lymph nodes, Incidence of bilaterality and multicentricity of 10%, Malignant transformation rare (almost unheard of), , Monomorphic adenoma, , Account for less than 5% of tumours, Slow growing, Consist of only one morphological cell type (hence term, mono), Include; basal cell adenoma, canalicular adenoma,, oncocytoma, myoepitheliomas, , Haemangioma, , Should be considered in the differential of a parotid mass in a, child, Accounts for 90% of parotid tumours in children less than 1, year of age, Hypervascular on imaging, Spontaneous regression may occur and malignant, transformation is almost unheard of, , Malignant salivary gland tumours
Page 3493 :
Types of malignancy, , Mucoepidermoid, carcinoma, , 30% of all parotid malignancies, Usually low potential for local invasiveness and metastasis (depends, mainly on grade), , Adenoid cystic, carcinoma, , Unpredictable growth pattern, Tendency for perineural spread, Nerve growth may display skip lesions resulting in incomplete excision, Distant metastasis more common (visceral rather than nodal spread), 5 year survival 35%, , Mixed tumours, , Often a malignancy occurring in a previously benign parotid lesion, , Acinic cell carcinoma, , Intermediate grade malignancy, May show perineural invasion, Low potential for distant metastasis, 5 year survival 80%, , Adenocarcinoma, , Develops from secretory portion of gland, Risk of regional nodal and distant metastasis, 5 year survival depends upon stage at presentation, may be up to 75%, with small lesions with no nodal involvement, , Lymphoma, , Large rubbery lesion, may occur in association with Warthins tumours, Diagnosis should be based on regional nodal biopsy rather than parotid, resection, Treatment is with chemotherapy (and radiotherapy), , Diagnostic evaluation, , , , , , , , Plain x-rays may be used to exclude calculi, Sialography may be used to delineate ductal anatomy, FNAC is used in most cases, Superficial parotidectomy may be either diagnostic of therapeutic depending upon the nature, of the lesion, Where malignancy is suspected the primary approach should be definitive resection rather, than excisional biopsy, CT/ MRI may be used in cases of malignancy for staging primary disease
Page 3494 :
Treatment, For nearly all lesions this consists of surgical resection, for benign disease this will usually consist of, a superficial parotidectomy. For malignant disease a radical or extended radical parotidectomy is, performed. The facial nerve is included in the resection if involved. The need for neck dissection is, determined by the potential for nodal involvement., Other parotid disorders, HIV infection, , , , , Lymphoepithelial cysts associated with HIV occur almost exclusively in the parotid, Typically presents as bilateral, multicystic, symmetrical swelling, Risk of malignant transformation is low and management usually conservative, , Sjogren syndrome, , , , , , , , , Autoimmune disorder characterised by parotid enlargement, xerostomia and, keratoconjunctivitis sicca, 90% of cases occur in females, Second most common connective tissue disorder, Bilateral, non tender enlargement of the gland is usual, Histologically, the usual findings are of a lymphocytic infiltrate in acinar units and, epimyoepithelial islands surrounded by lymphoid stroma, Treatment is supportive, There is an increased risk of subsequent lymphoma, , Sarcoid, , , , , , , Parotid involvement occurs in 6% of patients with sarcoid, Bilateral in most cases, Gland is not tender, Xerostomia may occur, Management of isolated parotid disease is usually conservative, Next question
Page 3495 :
Theme: Disorders affecting the ear, , A., B., C., D., E., F., G., , Acoustic neuroma, Otosclerosis, Preauricular sinus, Acute suppurative otitis media, Cholesteatoma, Long standing perforation of the pars tensa, Otitis externa, , Please select the most likely underlying explanation for the disorder described. Each option may be, used once, more than once or not at all., , 5., , A 34 year old lady presents with a long standing offensive discharge from the ear and on, examination is noted to have a reduction in her hearing of 40 decibels compared to the, opposite side., You answered Acoustic neuroma, The correct answer is Cholesteatoma, Theme from January 2013 Exam, The combination of offensive discharge and hearing loss is strongly suggestive of, cholesteatoma., , 6., , A 4 year old is brought to the general practitioner by her mother. She has been distressed, with ear pain for the past 14 hours. She is constantly touching and pulling at her ear. Whilst, she is sat in the waiting room her mother notices a discharge of foul smelling fluid from the, ear, following which the pain resolves., You answered Acoustic neuroma, The correct answer is Acute suppurative otitis media, In young children acute suppurative otitis media is a common condition. Rupture of the, tympanic membrane is a rare, but recognised complication., , 7., , A 4 year old child is brought to the clinic by his father. They are concerned because the, child has been noted to have a small epithelial defect anterior to the left ear and is has been, noted to discharge foul smelling material for the past 2 days., You answered Acoustic neuroma
Page 3496 :
The correct answer is Preauricular sinus, Pre auricular sinuses that a deeper may accumulate secretions and produce foul smelling, discharge., Please rate this question:, , Discuss and give feedback, , Next question, , Disorders affecting the ear, Otitis externa, , Variant, , Cause, , Features, , Treatment, , Acute, otitis, externa, , Boil in external auditory meatus, , Acute pain on, moving the pinna, Conductive hearing, loss if lesion is large, When rupture occurs, pus will flow from, ear, , Ear packs may be used, Topical antibiotics, Operative debridement, may be needed in severe, cases, , Chronic, otitis, externa, , Chronic combined infection in, the external auditory meatus, usually combined, staphylococcal and fungal, infection, , Chronic discharge, from affected ear,, hearing loss and, severe pain rare, , Cleansing of the external, ear and treatment with, antifungal and, antibacterial ear drops, , Otitis media, , Variant, , Cause, , Features, , Treatment, , Acute, suppurative, otitis media, , Viral induced middle, ear effusions, secondary to eustacian, tube dysfunction, , Most common in, children and rare in, adults, May present with, symptoms elsewhere, (e.g. vomiting) in, children, , Antibiotics (usually, amoxycillin)
Page 3497 :
Variant, , Cause, , Features, , Treatment, , Severe pain and, sometimes fever, May present with, discharge is tympanic, rupture occurs, , Chronic, suppurative, otitis media, , May occur with or, without cholesteatoma, Those without, cholesteatoma have a, perforation of the pars, tensa, Those with, cholesteatoma have a, perforation of the pars, flaccida, , Those without, cholesteatoma may, complain of, intermittent discharge, (non offensive), Those with, cholesteatoma have, impaired hearing and, foul smelling discharge, , Simple pars tensa, perforations may be managed, non operatively or a, myringoplasty considered if, symptoms troublesome., Pars flaccida perforations, will usually require a radical, mastoidectomy, , Otosclerosis, , , , , Progressive conductive deafness, Secondary to fixation of the stapes in the oval window, Treatment is with stapedectomy and insertion of a prosthesis, , Acoustic neuroma, , , , , Symptoms of gradually progressive unilateral perceptive deafness and tinnitus, Involvement of the vestibular nerve may cause vertigo, Extension to involve the facial nerve may cause weakness and then paralysis., , Pre auricular sinus, , , , , Common congenital condition in which an epithelial defect forms around the external ear, Small sinuses require no treatment, Deeper sinuses may become blocked and develop episodes of infection, they may be closely, related to the facial nerve and are challenging to excise, Next question
Page 3498 :
A 46-year-old woman is referred to endocrine surgery for a possible thyroidectomy. She has a, tender neck swelling. Blood results are as follows:, TSH, , <0.1 mU/l, , T4, , 188 nmol/l, , Hb, , 14.2 g/dl, , Plt, , 377 * 10^9/l, , WBC, , 6.4 * 10^9/l, , ESR, , 65 mm/hr, , Technetium thyroid scan shows decreased uptake globally, What is the most likely diagnosis?, , Sick thyroid syndrome, , Acute bacterial thyroiditis, , Hashimoto's thyroiditis, , Subacute thyroiditis, , Toxic multinodular goitre, , This patient does not need surgery! Subacute thyroiditis is suggested by the tender goitre,, hyperthyroidism and raised ESR. The globally reduced uptake on technetium thyroid scan is also, typical. This should resolve without any active intervention., Please rate this question:, , Discuss and give feedback, , Next question, , Thyroiditis
Page 3499 :
Sub acute thyroiditis, Subacute thyroiditis (also known as De Quervain's thyroiditis) is thought to occur following viral, infection and typically presents with hyperthyroidism, Features, , , , , , Hyperthyroidism, Painful goitre, Raised ESR, Globally reduced uptake on iodine-131 scan, , Management, , , , , Usually self-limiting - most patients do not require treatment, Thyroid pain may respond to aspirin or other NSAIDs, In more severe cases steroids are used, particularly if hypothyroidism develops, , Hashimotos thyroiditis, Hashimotos thyroiditis is an immunological disorder in which lymphocytes become sensitised to, thyroidal antigens. The three most important antibodies include; thyroglobulin, TPO and TSH-R., During the early phase of Hashimotos the the thyroglobulin antibody is markedly elevated and then, declines., Features, , , , Goitre and either euthyroid or mild hypothyroidism, Progressive hypothyroidism (and associated symptoms), , Management, , , , During the hyperthyroid phase of illness beta blockers may manage symptoms, As hypothyroidism develops patients may require thyroxine, Next question
Page 3500 :
Theme: Voice disorders, , A., B., C., D., E., F., G., H., , Vagus nerve injury, Thyroid nerve injury, Superior laryngeal nerve injury, Unilateral inferior laryngeal nerve injury, Bilateral inferior laryngeal nerves injuries, Stroke, Lacunar infarcts, None of the above, , Please select the most likely reason for the scenarios given. Each option may be used once, more, than once or not at all., , 9., , A 42 year old singer is admitted for a thyroidectomy. Post operatively she is only able to, make a gargling noise. Her voice sounds breathy., You answered Vagus nerve injury, The correct answer is Unilateral inferior laryngeal nerve injury, This patient has diplophonia which causes a gargling sound. This is associated with, dysphagia. This can also be caused by a vagus nerve lesion, but the recurrent laryngeal, nerve is more at risk of damage., , 10., , A 42 year old singer is admitted for a thyroidectomy. Post operatively she is unable to sing, high pitched notes., You answered Vagus nerve injury, The correct answer is Superior laryngeal nerve injury, Theme from September 2011 Exam, SLN lesions cause difficulty in voice pitch., , 11., , A 42 year old singer is admitted for a thyroidectomy. Post operatively the patient develops, dyspnoea and is unable to speak., You answered Vagus nerve injury, The correct answer is Bilateral inferior laryngeal nerves injuries
Page 3501 :
This patient has aphonia due to bilateral damage to the recurrent laryngeal nerve., Please rate this question:, , Discuss and give feedback, , Next question, , Voice production, There are 2 main nerves involved:, Superior laryngeal nerve (SLN), , , Innervates the cricothyroid muscle, , Since the cricothyroid muscle is involved in adjusting the tension of the vocal fold for high notes, during singing, SLN paresis and paralysis result in:, a. Abnormalities in pitch, b. Inability to sing with smooth change to each higher note (glissando or pitch glide), Recurrent laryngeal nerve (RLN)/Inferior laryngeal nerve, , , Innervates intrinsic larynx muscles, , a. Opening vocal folds (as in breathing, coughing), b. Closing vocal folds for vocal fold vibration during voice use, c. Closing vocal folds during swallowing, Next question
Page 3502 :
Theme: Nasal diseases, , A., B., C., D., E., F., G., H., I., , Ethmoid sinus cancer, Maxillary sinus cancer, Ethmoid adenoma, Maxillary adenoma, Ethmoidal fracture, Nasal polyps, Sphenoid osteoma, Ethmoidal sinusitis, Maxillary sinusitis, , Please select the most likely diagnosis for the scenario given. Each option may be used once, more, than once or not at all., , 12., , A 56 year old man presents with symptoms of nasal pain, anosmia and rhinorrhea. He has, been well until recently and has worked as a wood carver for many years., Ethmoid sinus cancer, Theme from September 2012 Exam, Theme from September 2013 Exam, Nasopharyngeal cancer is strongly associated with wood work. Most cases require an, occupational exposure of greater than 10 years and are adenocarcinomas on histology., Most cases are ethmoidal in origin (Hadfield E. Ann R Coll Surg Engl. 1970 June; 46(6):, 301319), , 13., , A 32 year old female presents with recurrent episodes of rhinorrhoea, the discharge is, watery. She has a medical history of asthma and intolerance of aspirin. On examination, she has multiple soft, semi- transparent polyps within her nasal cavity., You answered Ethmoid sinus cancer, The correct answer is Nasal polyps, The combination of nasal polyps and atopy is well described. Some cases will respond, favourably to systemic steroids and avoid surgery., , 14., , A child is brought to casualty complaining of a headache and a sensation of pressure, between the eyes. On examination she is febrile with a smooth swelling overlying the, superomedial aspect of the right eye. The eye is uncomfortable and there is a purulent, discharge from the inner canthus.
Page 3503 :
You answered Ethmoid sinus cancer, The correct answer is Ethmoidal sinusitis, Ethmoidal sinusitis may spread to the periorbital tissues resulting in periorbital cellulitis., The superomedial distribution makes a maxillary sinusitis less likely., Please rate this question:, , Discuss and give feedback, , Next question, , Diseases of nose and sinuses, Benign Tumours, , , , , , , , , Simple papillomas may be an incidental finding or present with obstructive symptoms., Excision under general anaesthesia is sufficient management., Transitional cell papillomas may be more extensive and produce obstructive symptoms., Erosion of local structures is a recognised complication. These lesions may rarely undergo, malignant transformation and therefore careful and complete excision is required, some, cases may require partial or total maxillectomy., Pleomorphic adenomas of the maxillary sinuses are reported but are extremely rare, their, symptoms typically include nasal obstruction and pain if the sinus is obstructed. Treatment is, by complete surgical excision, the diagnosis is not infrequently made post operatively., Benign osteomas may develop in the paranasal sinuses, the frontal sinus is the most, frequent location of such lesions. Symptoms include; pain, rhinorrhoea and anosmia. Most, osteomas may be observed if asymptomatic, sphenoid osteomas should be resected soon, after diagnosis as enlargement may compromise visual fields. Many sinus osteomas can, now be resected endoscopically, complete surgical resection is required., Nasal polyps are benign lesions of the ethmoid sinus mucosa. Many patients may also have, asthma, cystic fibrosis and a sensitivity to aspirin. Symptoms include watery rhinorrhoea,, infection and anosmia. The polyps are usually a semi transparent grey mass. They are rare, in childhood. Treatment is either with systemic steroids or surgical resection. The latter, should be combined with antral washout. Low dose, nasal, steroid drops may reduce the risk, of recurrence., , Malignant disease, , , , , Malignancies encountered in the nose and paranasal sinuses include; adenoid cystic, carcinoma, squamous cell carcinoma and adenocarcinoma., Adenocarcinoma of the paranasal sinuses and nasopharynx is strongly linked to exposure to, hard wood dust (after >10 years exposure)., Adenoid cystic carcinoma usually originate in the smaller salivary glands.
Page 3504 :
, , , , The majority of cancers (50%) arise from the lateral nasal wall, a smaller number (33%) arise, from the maxillary antrum, ethmoid and sphenoid cancers comprise only 7%., Signs of malignancy on clinical examination include loose teeth, cranial nerve palsies and, lymphadenopathy., Nasopharyngeal cancers are most common in individuals presenting from China and Asia, and are linked to viral infection with Epstein Barr Virus. Radiotherapy and chemotherapy are, the most commonly used modalities., , Maxillary sinusitis, , , , , , Common symptoms include post nasal discharge, pain, headache and toothache., Imaging may show a fluid level in the antrum., Common organisms include Haemophilus influenzae or Streptococcus pneumoniae., Treatment with antral lavage may facilitate diagnosis and relieve symptoms. Antimicrobial, therapy has to be continued for long periods. Antrostomy may be needed., , Frontoethmoidal sinusitis, , , , , Usually presents with frontal headache, nasal obstruction and altered sense of smell., Inflammation may progress to involve periorbital tissues. Ocular symptoms may occur and, secondary CNS involvement brought about by infection entering via emissary veins., CT scanning is the imaging modality of choice. Early cases may be managed with antibiotics., More severe cases usually require surgical drainage., Next question
Page 3505 :
Which of the following statements relating to branchial cysts is untrue?, , The greater auricular nerve may be divided during excision, , They typically occur in young adults, , They move upwards on swallowing, , They are rare over the age of 40 years, , They are usually located in the anterior triangle of the neck, Nerves at risk during branchial cyst excision: Mandibular branch of facial nerve, greater auricular, nerve and accessory nerve., , They do not move on swallowing. They should be diagnosed with caution in those aged >40 years,, as lumps in this age group may in fact be metastatic disease from oropharyngeal cancer., Please rate this question:, , Discuss and give feedback, , Next question, , Neck lumps, The table below gives characteristic exam question features for conditions causing neck lumps:, , Reactive, lymphadenopathy, , By far the most common cause of neck swellings. There may be a history of, local infection or a generalised viral illness
Page 3506 :
Lymphoma, , Rubbery, painless lymphadenopathy, The phenomenon of pain whilst drinking alcohol is very uncommon, There may be associated night sweats and splenomegaly, , Thyroid swelling, , May be hypo-, eu- or hyperthyroid symptomatically, Moves upwards on swallowing, , Thyroglossal cyst, , More common in patients < 20 years old, Usually midline, between the isthmus of the thyroid and the hyoid bone, Moves upwards with protrusion of the tongue, May be painful if infected, , Pharyngeal pouch, , More common in older men, Represents a posteromedial herniation between thyropharyngeus and, cricopharyngeus muscles, Usually not seen, but if large then a midline lump in the neck that gurgles on, palpation, Typical symptoms are dysphagia, regurgitation, aspiration and chronic cough, , Cystic hygroma, , A congenital lymphatic lesion (lymphangioma) typically found in the neck,, classically on the left side, Most are evident at birth, around 90% present before 2 years of age, , Branchial cyst, , An oval, mobile cystic mass that develops between the sternocleidomastoid, muscle and the pharynx, Develop due to failure of obliteration of the second branchial cleft in, embryonic development, Usually present in early adulthood, , Cervical rib, , More common in adult females, Around 10% develop thoracic outlet syndrome, , Carotid aneurysm, , Pulsatile lateral neck mass which doesn't move on swallowing, Next question
Page 3507 :
A 22 year old female attends clinic after noticing a painless neck lump. On examination she is noted, to have bilateral thyroid masses and multicentric nodes near the base of the thyroid. Her corrected, Ca is 2.18. What is the most likely diagnosis?, , Sporadic medullary carcinoma of the thyroid, , Medullary carcinoma of the thyroid associated with multiple endocrine neoplasia, , Follicular thyroid carcinoma, , Anaplastic thyroid carcinoma, , Toxic nodular goitre, , Medullary thyroid cancer is a tumour of the parafollicular cells of the thyroid. Less than 10% of, thyroid cancers are of this type. Patients typically present in children or young adults. Diarrhoea, occurs in 30% of cases. Toxic nodular goitre are very rare. In sporadic medullary thyroid cancer,, patients typically present with a unilateral solitary nodule and it tends to spread early to the neck, lymph nodes. In association with multiple endocrine neoplasia (MEN) syndromes, medullary thyroid, cancers are always bilateral and multicentric. It may be the presenting feature in MEN 2a and 2b;, almost all MEN 2a patients develop medullary thyroid carcinoma., Please rate this question:, , Discuss and give feedback, , Next question, , Thyroid malignancy, Papillary carcinoma, , , , , , Commonest sub-type, Accurately diagnosed on fine needle aspiration cytology, Histologically, they may demonstrate psammoma bodies (areas of calcification) and so, called 'orphan Annie' nuclei, They typically metastasise via the lymphatics and thus laterally located apparently ectopic, thyroid tissue is usually a metastasis from a well differentiated papillary carcinoma, , Follicular carcinoma
Page 3508 :
, , , , , Are less common than papillary lesions, Like papillary tumours, they may present as a discrete nodule. Although they appear to be, well encapsulated macroscopically there is invasion on microscopic evaluation, Lymph node metastases are uncommon and these tumours tend to spread, haematogenously. This translates into a higher mortality rate, Follicular lesions cannot be accurately diagnosed on fine needle aspiration cytology and thus, all follicular FNA's (THY 3f) will require at least a hemi thyroidectomy, , Anaplastic carcinoma, , , , Less common and tend to occur in elderly females, Disease is usually advanced at presentation and often only palliative decompression and, radiotherapy can be offered., , Medullary carcinoma, , , , , , These are tumours of the parafollicular cells ( C Cells) and are of neural crest origin., The serum calcitonin may be elevated which is of use when monitoring for recurrence., They may be familial and occur as part of the MEN -2A disease spectrum., Spread may be either lymphatic or haematogenous and as these tumours are not derived, primarily from thyroid cells they are not responsive to radioiodine., , Lymphoma, , , , These respond well to radiotherapy, Radical surgery is unnecessary once the disease has been diagnosed on biopsy material., Such biopsy material is not generated by an FNA and thus a core biopsy has to be obtained, (with care!)., Next question
Page 3509 :
Theme: Parotid gland disorders, , A., B., C., D., E., F., G., H., , Sialectasis, Pleomorphic adenoma, Bacterial parotitis, Viral parotitis, Sjogren's syndrome, Adenoid cystic carcinoma, Mucoepidermoid carcinoma, Warthins tumour, , Please select the most likely diagnosis for the scenario given. Each option may be used once, more, than once or not at all., , 17., , A 40 year old lady with longstanding rheumatoid arthritis presents with a dry mouth and, parotid gland swelling. Her symptoms transiently improved following administration of a, course of steroids for her rheumatoid disease., You answered Sialectasis, The correct answer is Sjogren's syndrome, Theme from April 2012 Exam, Sjogrens syndrome is linked to other autoimmune conditions such as rheumatoid disease., A transient improvement may be seen with steroid administration. Most patients are, treated with artificial saliva., , 18., , A 77 year old lady presents with facial pain and on examination is found to have clinical, evidence of a facial nerve palsy and a parotid mass. Following surgical excision of the, lesion the histological report comments on extensive perineural invasion., You answered Sialectasis, The correct answer is Adenoid cystic carcinoma, Extensive perineural invasion is most commonly seen in patients with adenoid cystic, carcinoma. Both Warthins tumours and mucoepidermoid carcinoma rarely show such, marked perineural infiltration., , 19., , An 18 year old boy presents with pancreatitis. He has bilateral painful parotid, enlargement., You answered Sialectasis
Page 3510 :
The correct answer is Viral parotitis, In a young adult with parotid swelling and pancreatitis/orchitis/reduced, hearing/meningoencephalitis suspect mumps., Please rate this question:, , Discuss and give feedback, , Next question, , Parotid gland clinical, Benign neoplasms, Up to 80% of all salivary gland tumours occur in the parotid gland and up to 80% of these are, benign. There is no consistent correlation between the rate of growth and the malignant potential of, the lesion. However, benign tumours should not invade structures such as the facial nerve., With the exception of Warthins tumours, they are commoner in women than men. The median age of, developing a lesion is in the 5th decade of life., Benign tumour types, , Tumour type, , Features, , Benign pleomorphic adenoma or, benign mixed tumor, , Most common parotid neoplasm (80%), Proliferation of epithelial and myoepithelial cells of the ducts, and an increase in stromal components, Slow growing, lobular, and not well encapsulated, Recurrence rate of 1-5% with appropriate excision, (parotidectomy), Recurrence possibly secondary to capsular disruption during, surgery, Malignant degeneration occurring in 2-10% of adenomas, observed for long periods, with carcinoma ex-pleomorphic, adenoma occurring most frequently as adenocarcinoma, , Warthin tumor (papillary, cystadenoma lymphoma or, adenolymphoma), , Second most common benign parotid tumor (5%), Most common bilateral benign neoplasm of the parotid, Marked male as compared to female predominance, Occurs later in life (sixth and seventh decades), Presents as a lymphocytic infiltrate and cystic epithelial, proliferation, May represent heterotopic salivary gland epithelial tissue, trapped within intraparotid lymph nodes
Page 3511 :
Tumour type, , Features, , Incidence of bilaterality and multicentricity of 10%, Malignant transformation rare (almost unheard of), , Monomorphic adenoma, , Account for less than 5% of tumours, Slow growing, Consist of only one morphological cell type (hence term, mono), Include; basal cell adenoma, canalicular adenoma,, oncocytoma, myoepitheliomas, , Haemangioma, , Should be considered in the differential of a parotid mass in a, child, Accounts for 90% of parotid tumours in children less than 1, year of age, Hypervascular on imaging, Spontaneous regression may occur and malignant, transformation is almost unheard of, , Malignant salivary gland tumours, Types of malignancy, , Mucoepidermoid, carcinoma, , 30% of all parotid malignancies, Usually low potential for local invasiveness and metastasis (depends, mainly on grade), , Adenoid cystic, carcinoma, , Unpredictable growth pattern, Tendency for perineural spread, Nerve growth may display skip lesions resulting in incomplete excision, Distant metastasis more common (visceral rather than nodal spread), 5 year survival 35%, , Mixed tumours, , Often a malignancy occurring in a previously benign parotid lesion, , Acinic cell carcinoma, , Intermediate grade malignancy, May show perineural invasion, Low potential for distant metastasis
Page 3512 :
5 year survival 80%, , Adenocarcinoma, , Develops from secretory portion of gland, Risk of regional nodal and distant metastasis, 5 year survival depends upon stage at presentation, may be up to 75%, with small lesions with no nodal involvement, , Lymphoma, , Large rubbery lesion, may occur in association with Warthins tumours, Diagnosis should be based on regional nodal biopsy rather than parotid, resection, Treatment is with chemotherapy (and radiotherapy), , Diagnostic evaluation, , , , , , , , Plain x-rays may be used to exclude calculi, Sialography may be used to delineate ductal anatomy, FNAC is used in most cases, Superficial parotidectomy may be either diagnostic of therapeutic depending upon the nature, of the lesion, Where malignancy is suspected the primary approach should be definitive resection rather, than excisional biopsy, CT/ MRI may be used in cases of malignancy for staging primary disease, , Treatment, For nearly all lesions this consists of surgical resection, for benign disease this will usually consist of, a superficial parotidectomy. For malignant disease a radical or extended radical parotidectomy is, performed. The facial nerve is included in the resection if involved. The need for neck dissection is, determined by the potential for nodal involvement., Other parotid disorders, HIV infection, , , , , Lymphoepithelial cysts associated with HIV occur almost exclusively in the parotid, Typically presents as bilateral, multicystic, symmetrical swelling, Risk of malignant transformation is low and management usually conservative, , Sjogren syndrome, , , , Autoimmune disorder characterised by parotid enlargement, xerostomia and, keratoconjunctivitis sicca, 90% of cases occur in females
Page 3513 :
, , , , , , Second most common connective tissue disorder, Bilateral, non tender enlargement of the gland is usual, Histologically, the usual findings are of a lymphocytic infiltrate in acinar units and, epimyoepithelial islands surrounded by lymphoid stroma, Treatment is supportive, There is an increased risk of subsequent lymphoma, , Sarcoid, , , , , , , Parotid involvement occurs in 6% of patients with sarcoid, Bilateral in most cases, Gland is not tender, Xerostomia may occur, Management of isolated parotid disease is usually conservative, Next question
Page 3514 :
Theme: Neck lumps, , A. Dermoid cyst, B. Thyroglossal cyst, C. Sjogren's syndrome, D. Mikulicz's syndrome, E. Pleomorphic adenoma of the parotid, F. Carcinoma of the parotid, G. Cystic hygroma, H. Branchial cyst, I. Pharyngeal pouch, , Please select the most likely diagnosis for the scenario given. Each option may be used once, more, than once or not at all., , 20., , A dentist treating a women with rheumatoid arthritis for recurrent episodes of dental sepsis, notices that both parotid and submandibular glands are symmetrically enlarged., You answered Dermoid cyst, The correct answer is Sjogren's syndrome, Sjogren's is associated with autoimmune disorders. Mikulicz's is similar but there is no sicca or, arthritis., , 21., , A patient presents with a facial nerve palsy. This occurred following repeat excision of a facial, lump. The histology report remarks on the biphasic appearance of the lesion and mucinous, connective tissue., You answered Dermoid cyst, The correct answer is Pleomorphic adenoma of the parotid
Page 3515 :
The histological features are as described with a classic biphasic (mixed stromal and epithelial, elements), although benign local recurrence can complicate incomplete excision. As this is a, benign lesion direct extension into the facial nerve is unlikely to occur. Facial nerve injury can, happen during repeat parotid surgery., , 22., , A patient is recovering from a Sistrunk's procedure, what lesion was treated with this operation?, You answered Dermoid cyst, The correct answer is Thyroglossal cyst, This is the procedure for excision of the cyst and its associated track. Excision must be complete, and thus a small segment of the hyoid bone is removed to gain access to the upper part of the, cyst tract., , Please rate this question:, , Discuss and give feedback, , Next question, , Neck lumps, The table below gives characteristic exam question features for conditions causing neck lumps:, , Reactive, lymphadenopathy, , By far the most common cause of neck swellings. There may be a history of, local infection or a generalised viral illness, , Lymphoma, , Rubbery, painless lymphadenopathy, The phenomenon of pain whilst drinking alcohol is very uncommon, There may be associated night sweats and splenomegaly
Page 3516 :
Thyroid swelling, , May be hypo-, eu- or hyperthyroid symptomatically, Moves upwards on swallowing, , Thyroglossal cyst, , More common in patients < 20 years old, Usually midline, between the isthmus of the thyroid and the hyoid bone, Moves upwards with protrusion of the tongue, May be painful if infected, , Pharyngeal pouch, , More common in older men, Represents a posteromedial herniation between thyropharyngeus and, cricopharyngeus muscles, Usually not seen, but if large then a midline lump in the neck that gurgles on, palpation, Typical symptoms are dysphagia, regurgitation, aspiration and chronic cough, , Cystic hygroma, , A congenital lymphatic lesion (lymphangioma) typically found in the neck,, classically on the left side, Most are evident at birth, around 90% present before 2 years of age, , Branchial cyst, , An oval, mobile cystic mass that develops between the sternocleidomastoid, muscle and the pharynx, Develop due to failure of obliteration of the second branchial cleft in, embryonic development, Usually present in early adulthood, , Cervical rib, , More common in adult females, Around 10% develop thoracic outlet syndrome, , Carotid aneurysm, , Pulsatile lateral neck mass which doesn't move on swallowing, Next question
Page 3517 :
A 10 year old girl presents with epistaxis. From which of the following regions is the bleeding most, likely to originate?, , Posterior nasal space, , Alar rim, , Kiesselbach's plexus, , Cribriform plate, , None of the above, , Kiesselbachs plexus has an arterial supply derived from both the internal and external carotid, arteries and is the commonest area for bleeding in idiopathic epistaxis., Please rate this question:, , Discuss and give feedback, , Next question, , Epistaxis, Usually trivial and insignificant but severe haemorrhage may compromise airway and pose a risk to, life., Anatomy:, Arterial supply, , , , , , , From internal and external carotid, An arterial plexus exists at Little's area and is the source of bleeding in 90% cases, Major arterial supply is from the sphenopalatine and greater palatine arteries (branches of, the maxillary artery), The facial artery supplies the more anterior aspect of the nose, Ethmoidal arteries are branches of the ophthalmic artery. They supply the posterosuperior, nasal cavity, , Venous drainage follows the arterial pattern
Page 3518 :
Classification, , , , , Primary idiopathic epistaxis accounts for 75% of all cases, Secondary cases arise as a result of events such as anticoagulants, trauma and, coagulopathy, Classification into anterior and posterior epistaxis may help to locate the source and, becomes more important when invasive treatment is required, , Management, , , , , , , , , Resuscitate if required, Subject should sit upright and pinch nose firmly, Nasal cavity should be examined using a headlight, Simple anterior epistaxis may be managed using silver nitrate cautery. If difficult to manage, then custom manufactured packs may be inserted, Posterior packing or tamponade may be achieved by passing a balloon tamponade device, and inflating it. This is indicated where anterior packing alone has failed to achieve, haemostasis., Post nasal pack patients should receive antibiotics, Failure of these methods will require more invasive therapy. Where a vascular radiology, suite is available, consideration may be given to angiographic techniques. Direct ligation of, the nasal arterial supply may also be undertaken. Of the arterial ligation techniques, available, the endo nasal sphenopalatine arterial ligation procedure is most popular., Next question
Page 3519 :
A 56 year old man presents with a painless swelling in the upper part of the anterior triangle of his, neck. On examination a mass lesion involving the sub mandibular gland is identified. On CT, scanning this is shown to be a solid lesion. There is no regional lymphadenopathy. Two fine needle, aspirates have failed to be diagnostic. Which of the following is the most appropriate management, option?, , Sub mandibular gland excision, , Incisional biopsy of the mass, , Manage conservatively and repeat the CT scan in 6 months, , Sub mandibular gland excision and radical neck dissection, , Diagnostic excision of the superficial lobe of the submandibular gland, , There is a 50% risk that this lesion is malignant (in some series up to 70%). Therefore the gland, should be excised entirely. At this stage a radical neck dissection is not justified., Please rate this question:, , Discuss and give feedback, , Next question, , Submandibular glands- disease, Physiology, The submandibular glands secrete approximately 800- 1000ml saliva per day. They typically, produce mixed seromucinous secretions. When parasympathetic activity is dominant; the secretions, will be more serous. The parasympathetic fibres are derived from the chorda tympani nerves and the, submandibular ganglion. Sensory fibres are conveyed by the lingual branch of the mandibular nerve., Sialolithiasis, , , , , , , , 80% of all salivary gland calculi occur in the submandibular gland, 70% of the these calculi are radio-opaque, Stones are usually composed of calcium phosphate or calcium carbonate, Patients typically develop colicky pain and post prandial swelling of the gland, Investigation involves sialography to demonstrate the site of obstruction and associated, other stones, Stones impacted in the distal aspect of Whartons duct may be removed orally, other stones, and chronic inflammation will usually require gland excision
Page 3520 :
Sialadenitis, , , , , Usually occurs as a result of Staphylococcus aureus infection, Pus may be seen leaking from the duct, erythema may also be noted, Development of a sub mandibular abscess is a serious complication as it may spread, through the other deep fascial spaces and occlude the airway, , Submandibular tumours, , , , , , , Only 8% of salivary gland tumours affect the sub mandibular gland, Of these 50% are malignant (usually adenoid cystic carcinoma), Diagnosis usually involves fine needle aspiration cytology, Imaging is with CT and MRI, In view of the high prevalence of malignancy, all masses of the submandibular glands should, generally be excised., Next question
Page 3521 :
A 36-year-old woman who presented with a goitre is diagnosed with autoimmune thyroiditis. Which, one of the following types of thyroid cancer is she predisposed to developing?, , Anaplastic, , Lymphoma, , Medullary, , Follicular, , None of the above, Hashimoto's thyroiditis is associated with thyroid lymphoma, Rarely, a patient with Hashimotos thyroiditis may develop a lymphoma of the thyroid gland. The, exact aetiology of thyroid gland lymphoma is unknown. Hashimotos thyroiditis is a definite risk factor., It is possible that the lymphoma may represent the expansion of a clone of immortalised, intrathyroidal lymphocytes. Lymphoma of the gland is characterised by rapid thyroid growth despite, T4 therapy. Whilst adenocarcinoma of the thyroid may occur in association with thyroiditis there are, no studies, to date, showing a correlation between these two conditions. The commonest sequelae, of thyroiditis is hypothyroidism., Please rate this question:, , Discuss and give feedback, , Next question, , Thyroiditis, Sub acute thyroiditis, Subacute thyroiditis (also known as De Quervain's thyroiditis) is thought to occur following viral, infection and typically presents with hyperthyroidism, Features, , , , , , Hyperthyroidism, Painful goitre, Raised ESR, Globally reduced uptake on iodine-131 scan
Page 3522 :
Management, , , , , Usually self-limiting - most patients do not require treatment, Thyroid pain may respond to aspirin or other NSAIDs, In more severe cases steroids are used, particularly if hypothyroidism develops, , Hashimotos thyroiditis, Hashimotos thyroiditis is an immunological disorder in which lymphocytes become sensitised to, thyroidal antigens. The three most important antibodies include; thyroglobulin, TPO and TSH-R., During the early phase of Hashimotos the the thyroglobulin antibody is markedly elevated and then, declines., Features, , , , Goitre and either euthyroid or mild hypothyroidism, Progressive hypothyroidism (and associated symptoms), , Management, , , , During the hyperthyroid phase of illness beta blockers may manage symptoms, As hypothyroidism develops patients may require thyroxine, Next question
Page 3523 :
An elderly diabetic male presents with a severe deep seated otalgia and a facial nerve palsy, he has, completed a course of amoxycillin with no benefit. What is the most likely diagnosis?, , Malignant otitis externa, , Otosclerosis, , Acoustic neuroma, , Meniers disease, , Viral illness, , A combination of severe otalgia and facial nerve palsy in a diabetic should raise suspicion of, malignant otitis externa. This is a condition caused by pseudomonas. It commences as otitis externa, and then progresses to involve the temporal bone. Spread of the disease outside the external, auditory canal occurs through the fissures of Santorini and the osseocartilaginous junction., Please rate this question:, , Discuss and give feedback, , Next question, , Disorders affecting the ear, Otitis externa, , Variant, , Cause, , Features, , Treatment, , Acute, otitis, externa, , Boil in external auditory meatus, , Acute pain on, moving the pinna, Conductive hearing, loss if lesion is large, When rupture occurs, pus will flow from, ear, , Ear packs may be used, Topical antibiotics, Operative debridement, may be needed in severe, cases, , Chronic, otitis, , Chronic combined infection in, the external auditory meatus, , Chronic discharge, from affected ear,, , Cleansing of the external, ear and treatment with
Page 3524 :
Variant, , Cause, , Features, , Treatment, , externa, , usually combined, staphylococcal and fungal, infection, , hearing loss and, severe pain rare, , antifungal and, antibacterial ear drops, , Otitis media, , Variant, , Cause, , Features, , Treatment, , Acute, suppurative, otitis media, , Viral induced middle, ear effusions, secondary to eustacian, tube dysfunction, , Most common in, children and rare in, adults, May present with, symptoms elsewhere, (e.g. vomiting) in, children, Severe pain and, sometimes fever, May present with, discharge is tympanic, rupture occurs, , Antibiotics (usually, amoxycillin), , Chronic, suppurative, otitis media, , May occur with or, without cholesteatoma, Those without, cholesteatoma have a, perforation of the pars, tensa, Those with, cholesteatoma have a, perforation of the pars, flaccida, , Those without, cholesteatoma may, complain of, intermittent discharge, (non offensive), Those with, cholesteatoma have, impaired hearing and, foul smelling discharge, , Simple pars tensa, perforations may be managed, non operatively or a, myringoplasty considered if, symptoms troublesome., Pars flaccida perforations, will usually require a radical, mastoidectomy, , Otosclerosis, , , , , Progressive conductive deafness, Secondary to fixation of the stapes in the oval window, Treatment is with stapedectomy and insertion of a prosthesis
Page 3525 :
Acoustic neuroma, , , , , Symptoms of gradually progressive unilateral perceptive deafness and tinnitus, Involvement of the vestibular nerve may cause vertigo, Extension to involve the facial nerve may cause weakness and then paralysis., , Pre auricular sinus, , , , , Common congenital condition in which an epithelial defect forms around the external ear, Small sinuses require no treatment, Deeper sinuses may become blocked and develop episodes of infection, they may be closely, related to the facial nerve and are challenging to excise, Next question
Page 3526 :
Which of the following does not cause parotid enlargement?, , Liver cirrhosis, , Myxoedema, , Amiodarone, , Tuberculosis, , Sjogrens syndrome, , Drugs commonly implicated in parotid gland enlargement include:, Thiouracil, isoprenaline, phenylbutazone, high oestrogen dose contraceptive pills., Please rate this question:, , Discuss and give feedback, , Next question, , Parotid gland clinical, Benign neoplasms, Up to 80% of all salivary gland tumours occur in the parotid gland and up to 80% of these are, benign. There is no consistent correlation between the rate of growth and the malignant potential of, the lesion. However, benign tumours should not invade structures such as the facial nerve., With the exception of Warthins tumours, they are commoner in women than men. The median age of, developing a lesion is in the 5th decade of life., Benign tumour types, , Tumour type, , Features, , Benign pleomorphic adenoma or, benign mixed tumor, , Most common parotid neoplasm (80%), Proliferation of epithelial and myoepithelial cells of the ducts, and an increase in stromal components, Slow growing, lobular, and not well encapsulated, Recurrence rate of 1-5% with appropriate excision, (parotidectomy), Recurrence possibly secondary to capsular disruption during, surgery
Page 3527 :
Tumour type, , Features, , Malignant degeneration occurring in 2-10% of adenomas, observed for long periods, with carcinoma ex-pleomorphic, adenoma occurring most frequently as adenocarcinoma, , Warthin tumor (papillary, cystadenoma lymphoma or, adenolymphoma), , Second most common benign parotid tumor (5%), Most common bilateral benign neoplasm of the parotid, Marked male as compared to female predominance, Occurs later in life (sixth and seventh decades), Presents as a lymphocytic infiltrate and cystic epithelial, proliferation, May represent heterotopic salivary gland epithelial tissue, trapped within intraparotid lymph nodes, Incidence of bilaterality and multicentricity of 10%, Malignant transformation rare (almost unheard of), , Monomorphic adenoma, , Account for less than 5% of tumours, Slow growing, Consist of only one morphological cell type (hence term, mono), Include; basal cell adenoma, canalicular adenoma,, oncocytoma, myoepitheliomas, , Haemangioma, , Should be considered in the differential of a parotid mass in a, child, Accounts for 90% of parotid tumours in children less than 1, year of age, Hypervascular on imaging, Spontaneous regression may occur and malignant, transformation is almost unheard of, , Malignant salivary gland tumours, Types of malignancy, , Mucoepidermoid, carcinoma, , 30% of all parotid malignancies, Usually low potential for local invasiveness and metastasis (depends, mainly on grade)
Page 3528 :
Adenoid cystic, carcinoma, , Unpredictable growth pattern, Tendency for perineural spread, Nerve growth may display skip lesions resulting in incomplete excision, Distant metastasis more common (visceral rather than nodal spread), 5 year survival 35%, , Mixed tumours, , Often a malignancy occurring in a previously benign parotid lesion, , Acinic cell carcinoma, , Intermediate grade malignancy, May show perineural invasion, Low potential for distant metastasis, 5 year survival 80%, , Adenocarcinoma, , Develops from secretory portion of gland, Risk of regional nodal and distant metastasis, 5 year survival depends upon stage at presentation, may be up to 75%, with small lesions with no nodal involvement, , Lymphoma, , Large rubbery lesion, may occur in association with Warthins tumours, Diagnosis should be based on regional nodal biopsy rather than parotid, resection, Treatment is with chemotherapy (and radiotherapy), , Diagnostic evaluation, , , , , , , , Plain x-rays may be used to exclude calculi, Sialography may be used to delineate ductal anatomy, FNAC is used in most cases, Superficial parotidectomy may be either diagnostic of therapeutic depending upon the nature, of the lesion, Where malignancy is suspected the primary approach should be definitive resection rather, than excisional biopsy, CT/ MRI may be used in cases of malignancy for staging primary disease, , Treatment, For nearly all lesions this consists of surgical resection, for benign disease this will usually consist of, a superficial parotidectomy. For malignant disease a radical or extended radical parotidectomy is, performed. The facial nerve is included in the resection if involved. The need for neck dissection is, determined by the potential for nodal involvement., Other parotid disorders
Page 3529 :
HIV infection, , , , , Lymphoepithelial cysts associated with HIV occur almost exclusively in the parotid, Typically presents as bilateral, multicystic, symmetrical swelling, Risk of malignant transformation is low and management usually conservative, , Sjogren syndrome, , , , , , , , , Autoimmune disorder characterised by parotid enlargement, xerostomia and, keratoconjunctivitis sicca, 90% of cases occur in females, Second most common connective tissue disorder, Bilateral, non tender enlargement of the gland is usual, Histologically, the usual findings are of a lymphocytic infiltrate in acinar units and, epimyoepithelial islands surrounded by lymphoid stroma, Treatment is supportive, There is an increased risk of subsequent lymphoma, , Sarcoid, , , , , , , Parotid involvement occurs in 6% of patients with sarcoid, Bilateral in most cases, Gland is not tender, Xerostomia may occur, Management of isolated parotid disease is usually conservative, Next question
Page 3530 :
At which of the following time frames is secondary haemorrhage most likely to occur following, tonsillectomy?, , Between 5 and 10 days after surgery, , During the first 6 hours after surgery, , Between 6 and 12 hours after surgery, , Upon resumption of normal feeding, , Between 2 and 3 days post operatively, , Haemorrhage in the first 6 hours after surgery is termed reactionary haemorrhage. Feeding does not, increase the risk and may actually lower the risks of infection developing., Please rate this question:, , Discuss and give feedback, , Next question, , Secondary haemorrhage after tonsillectomy, Haemorrhage is a feared complication following tonsillectomy. Primary, or reactionary haemorrhage, most commonly occurs in the first 6-8 hours following surgery. It is managed by immediate return to, theatre., Secondary haemorrhage occurs between 5 and 10 days after surgery, it is often associated with a, wound infection. Treatment is usually with admission and antibiotics. Severe bleeding may require, surgery. Secondary haemorrhage occurs in 3% of all tonsillectomies., Next question
Page 3531 :
A 8 year old boy with recurrent attacks of otitis media is suspected of developing a glue ear. If his, sound conduction is tested, which of the following is most consistent with a unilateral middle ear, effusion?, , Negative Rinne's test on the ipsilateral side, , Positive Rinne's test on the ipsilateral side, , Positive Webers and Rinnes tests on the ipsilateral side, , Positive Rinne's test on the contralateral side, , Negative Webers test only on the contralateral side, , Theme from 2008 Exam, Rinne's test will localise to the affected side (i.e. it is negative in conductive deafness). In a positive, Rinne's test sound heard by air conduction is better than that conveyed by bone conduction., Reduction of both air and bone conduction in equal measure is a feature of sensorineural hearing, loss., Please rate this question:, , Discuss and give feedback, , Next question, , Hearing Loss, Hearing loss may be conductive or sensorineural. To determine which is present patients will often, require a formal assessment with pure tone audiometry. In the clinical setting Webers and Rinnes, tests may be helpful in categorising various types of hearing loss., Webers and Rinnes Tests, In a normal patient, the Weber tuning fork sound is heard equally loud in both ears with no one ear, hearing the sound louder than the other. A patient with symmetrical hearing loss will hear the Weber
Page 3532 :
tuning fork sound equally well with diagnostic utility only in asymmetric (one-sided) hearing losses. In, a patient with asymmetrical hearing loss, the Weber tuning fork sound is heard louder in one ear, versus the other. This clinical finding should be confirmed by repeating the procedure and having the, patient occlude one ear with a finger; the sound should be heard best in the occluded ear., , Weber without, lateralisation, , Weber lateralises to left, , Weber lateralises to right, , Normal, , Sensorineural loss on right, , Sensorineural loss on left, , Left Bone >, Air, , Conductive loss on left, , Combined loss on left, , Right Bone>, Air, , Combined loss on right, , Conductive loss on right, , Both Bone >, Air, , Combined loss on right and, conductive on left, , Combined loss on left and, conductive on right, , Rinne Test, , Both ears, Air>Bone, , Next question
Page 3533 :
Theme: Head and neck lesions, , A. Dermoid cyst, B. Thyroglossal cyst, C. Sjogren's syndrome, D. Mikulicz's syndrome, E. Pleomorphic adenoma of the parotid, F. Carcinoma of the parotid, G. Cystic hygroma, H. Branchial cyst, I. Pharyngeal pouch, , Please select the most likely diagnosis for the scenario given. Each option may be used once, more, than once or not at all., , 30., , The parents of a 2 year old child are concerned after he develops a lump in his neck. On, examination there is a swelling in the subcutaneous tissue of the posterior triangle which, transilluminates., You answered Dermoid cyst, The correct answer is Cystic hygroma, This is a classical description. Collection of dilated lymphatic sacs which are fluctuant and, brilliantly transilluminable. Recurrence is common., , 31., , A 40 year old female presents with a painless neck lump. There is a mass noted beneath the, sternocleidomastoid muscle. There is a long history and somewhat unkindly her husband, remarked on her rather noticeable halitosis., You answered Dermoid cyst
Page 3534 :
The correct answer is Pharyngeal pouch, Usual history of regurgitation of undigested food or coughing at night. Associated with halitosis, and throat infections., , 32., , A 32 year old lady is referred to the clinic with recurrent infections and abscesses in the neck. On, examination she has a midline defect with an overlying scab, which moves upwards on tongue, protrusion., You answered Dermoid cyst, The correct answer is Thyroglossal cyst, Thyroglossal cyst is always located in the midline as it is this route that the thyroid takes during its, embryological descent. Its connection with the foramen caecum means it will move on tongue, protrusion., , Similar theme question in September 2011 exam, , Please rate this question:, , Discuss and give feedback, , Neck lumps, The table below gives characteristic exam question features for conditions causing neck lumps:, , Reactive, lymphadenopathy, , By far the most common cause of neck swellings. There may be a history of, local infection or a generalised viral illness, , Lymphoma, , Rubbery, painless lymphadenopathy, The phenomenon of pain whilst drinking alcohol is very uncommon
Page 3535 :
There may be associated night sweats and splenomegaly, , Thyroid swelling, , May be hypo-, eu- or hyperthyroid symptomatically, Moves upwards on swallowing, , Thyroglossal cyst, , More common in patients < 20 years old, Usually midline, between the isthmus of the thyroid and the hyoid bone, Moves upwards with protrusion of the tongue, May be painful if infected, , Pharyngeal pouch, , More common in older men, Represents a posteromedial herniation between thyropharyngeus and, cricopharyngeus muscles, Usually not seen, but if large then a midline lump in the neck that gurgles on, palpation, Typical symptoms are dysphagia, regurgitation, aspiration and chronic cough, , Cystic hygroma, , A congenital lymphatic lesion (lymphangioma) typically found in the neck,, classically on the left side, Most are evident at birth, around 90% present before 2 years of age, , Branchial cyst, , An oval, mobile cystic mass that develops between the sternocleidomastoid, muscle and the pharynx, Develop due to failure of obliteration of the second branchial cleft in, embryonic development, Usually present in early adulthood, , Cervical rib, , More common in adult females, Around 10% develop thoracic outlet syndrome, , Carotid aneurysm, , Pulsatile lateral neck mass which doesn't move on swallowing
Page 3537 :
Theme: Management of biliary disease, , A., B., C., D., E., F., G., H., , Acute laparoscopic cholecystectomy, Delayed laparoscopic cholecystectomy, Percutaneous cholecystostomy, Elective cholecystectomy and intra operative cholangiogram, Endoscopic retrograde cholangiopancreatography, Choledochoduodenostomy, Bile duct excision and hepatico-jejunostomy, Operative cholecystostomy, , For each scenario please select the most appropriate management option. Each option may be used, once, more than once or not at all., , 1., , A 72 year old lady underwent an open cholecystectomy 12 years previously. She has been, admitted since with 2 episodes of cholangitis and stones were retrieved at ERCP. She has, just recovered from a further episode of sepsis and MRCP has shown further biliary stones., You answered Acute laparoscopic cholecystectomy, The correct answer is Choledochoduodenostomy, A patient with long standing common bile duct stones is at risk of developing duct fibrosis, and ductal disproportion. This can result in impaired biliary drainage. Not only may further, stones be formed in the bile that is present, but because of the ductal disproportion the, tendency will be for the stones to accumulate (rather than pass spontaneously, as would, usually be the case post ERCP and sphincterotomy). A biliary bypass procedure is the, standard method dealing with this and a choledochoduodenstomy is one procedure that can, be used., , 2., , A 26 year old women is admitted with acute cholecystitis of 24 hours duration. LFT's are, normal and Ultrasound shows a thick walled gallbladder containing stones., Acute laparoscopic cholecystectomy, This is an ideal case for an acute cholecystectomy, provided that surgery can be undertaken, promptly. After 48 -72 hours the patient should receive parenteral antibiotics and delayed, cholecystectomy performed., , 3., , A 32 year old lady is seen in the outpatients. She has had multiple episodes of biliary colic, and ultrasound shows thin walled gallbladder with multiple calculi. Her ALT is slightly, raised but other parameters are normal.
Page 3538 :
You answered Acute laparoscopic cholecystectomy, The correct answer is Elective cholecystectomy and intra operative cholangiogram, The easiest option is to perform an intraoperative cholangiogram. It is unlikely to reveal any, stones. If is does then either laparoscopic bile duct exploration or urgent ERCP can be, performed. An MRCP pre op is an alternative strategy., Please rate this question:, , Discuss and give feedback, , Next question, , Biliary disease, Diagnosis, , Typical features, , Pathogenesis, , Gallstones, , Typically history of, biliary colic or, episodes of, chlolecystitis., Obstructive type, history and test results., , Usually small calibre gallstones which can, pass through the cystic duct. In Mirizzi, syndrome the stone may compress the bile, duct directly- one of the rare times that, cholecystitis may present with jaundice, , Cholangitis, , Usually obstructive, and will have Charcot's, triad of symptoms, (pain, fever, jaundice), , Ascending infection of the bile ducts usually, by E. coliand by definition occurring in a pool, of stagnant bile., , Pancreatic cancer, , Typically painless, jaundice with palpable, gallbladder, (Courvoisier's Law), , Direct occlusion of distal bile duct or, pancreatic duct by tumour. Sometimes nodal, disease at the portal hepatis may be the culprit, in which case the bile duct may be of normal, calibre., , TPN (total parenteral, nutrition) associated, jaundice, , Usually follows long, term use and is usually, painless with non, , Often due to hepatic dysfunction and fatty, liver which may occur with long term TPN, usage.
Page 3539 :
obstructive features, , Bile duct injury, , Depending upon the, type of injury may be, of sudden or gradual, onset and is usually of, obstructive type, , Often due to a difficult laparoscopic•, cholecystectomy when anatomy in Calots, triangle is not appreciated. In the worst, scenario the bile duct is excised and jaundice, develops rapidly post operatively. More, insidious is that of bile duct stenosis which, may be caused by clips or diathermy injury., , Cholangiocarcinoma, , Gradual onset, obstructive pattern, , Direct occlusion by disease and also extrinsic, compression by nodal disease at the porta, hepatis., , Septic surgical patient, , Usually hepatic, features, , Combination of impaired biliary excretion and, drugs such as ciprofloxacin which may cause, cholestasis., , Metastatic disease, , Mixed hepatic and post, hepatic, , Combination of liver synthetic failure (late), and extrinsic compression by nodal disease, and anatomical compression of intra hepatic, structures (earlier), , A gallbladder may develop a thickened wall in chronic cholecystitis, microscopically RoikitanskyAschoff Sinuses may be seen, , Image sourced from Wikipedia, , Next question
Page 3540 :
Theme: Management of pancreatic malignancy, , A. Gastrojejunostomy, B. Pancreatoduodenectomy, C. MRI guided pancreatic stent, D. Endoscopic pancreatic stent, E. Duodenoduodenostomy, F. Pancreatic radiotherapy, , Please select the most appropriate treatment for these patients with pancreatic cancer. Each option, may be used once, more than once or not at all., , 4., , A 40 year old lady presents with new onset dyspepsia. She is diagnosed as having a localised, cacinoma of the pancreatic head., You answered Gastrojejunostomy, The correct answer is Pancreatoduodenectomy, Theme from January 2013 exam, Localised carcinoma of the pancreas is treated with a pancreatoduodenectomy, the eponymous, name for this is a Whipples procedure. Newer variants of the procedure include pylorus, preservation. Adjuvent chemotherapy is often used., , 5., , A 67 year old lady presents with jaundice and abdominal pain. Her investigations show a dilated, common bile duct, a carcinoma of the pancreatic head compressing the pancreatic duct. Her liver, contains bi-lobar metastasis., You answered Gastrojejunostomy, The correct answer is Endoscopic pancreatic stent, Jaundice associated with pancreatic cancer is best managed with a stent. These are usually, inserted at the time of ERCP. Consideration here should be given to the use of a metallic stent
Page 3541 :
(which is contra indicated where resection is contemplated)., , 6., , A 67 year old lady presents with symptoms of persistent vomiting. Her investigations show gastric, outlet obstruction from a carcinoma of the pancreatic head. Her liver contains bi-lobar metastases., Gastrojejunostomy, Gastric outlet obstruction from pancreatic cancer is best managed with a surgical bypass procedure, or a duodenal stent (if the disease is not resectable or curable)., , Please rate this question:, , Discuss and give feedback, , Next question, , Pancreatic cancer, , , , , , , Adenocarcinoma, Risk factors: Smoking, diabetes, adenoma, familial adenomatous polyposis, Mainly occur in the head of the pancreas (70%), Spread locally and metastasizes to the liver, Carcinoma of the pancreas should be differentiated from other periampullary tumours with, better prognosis, , Clinical features, , , , , , , , Weight loss, Painless jaundice, Epigastric discomfort (pain usually due to invasion of the coeliac plexus is a late feature), Pancreatitis, Trousseau's sign: migratory superficial thrombophlebitis, , Investigations
Page 3542 :
, , , , , , USS: May miss small lesions, CT Scanning (pancreatic protocol). If unresectable on CT then no further staging needed, PET/CT for those with operable disease on CT alone, ERCP/ MRI for bile duct assessment, Staging laparoscopy to exclude peritoneal disease, , Management, , , , , , , , Head of pancreas: Whipple's resection (SE dumping and ulcers). Newer techniques include, pylorus preservation and SMA/ SMV resection, Carcinoma body and tail: poor prognosis, distal pancreatectomy, if operable, Usually adjuvent chemotherapy for resectable disease, ERCP and stent for jaundice and palliation, Surgical bypass may be needed for duodenal obstruction, , Next question
Page 3543 :
Theme: Management of jaundice, , A. ERCP, B. MRCP, C. Percutaneous transhepatic cholangiogram, D. Laparotomy, E. Laparotomy and formation of hepatico-jejunostomy, F. Laparoscopic biliary bypass, G. CT scan, , For each of the following scenarios please select the most appropriate next stage of management., Each option may be used once, more than once or not at all., , 7., , A 65 year old man is admitted with jaundice and investigations demonstrate a carcinoma of the, pancreatic head. An ERCP is attempted but the surgeon is unable to cannulate the ampulla., You answered ERCP, The correct answer is Percutaneous transhepatic cholangiogram, Theme from September 2012 Exam, Cancer of the pancreatic head will cause obstructive jaundice and intrahepatic duct dilatation., When an ERCP has failed the most appropriate option is to attempt a PTC. This procedure is always, preceded by an ultrasound (which presumably this patient has already had or they would not be, undergoing an ERCP). Prior to performing the PTC it is important to stage the disease and establish, resectability or not. This is because the PTC drains frequently dislodge and fall out. It is usually, desirable to pass a stent at the time of doing the PTC to mitigate the effects of this problem., , 8., , A 48 year old lady is admitted with attacks of biliary colic and investigations show gallstones. A, laparoscopic cholecystectomy is performed. The operation is technically challenging due to a large, stone impacted in Hartmans pouch. Following the operation she fails to settle and becomes, jaundiced and has bile draining into a drain placed at the surgical site.
Page 3544 :
ERCP, In this scenario it must be assumed that the bile duct has been damaged. In most cases an ERCP is, the most appropriate investigation. This can also allow the passage of a stent if this is deemed to, be safe and sensible., , 9., , A 34 year old lady is admitted with jaundice and undergoes an ERCP. The procedure is technically, difficult and she is returned to the ward still jaundiced. Unfortunately she now has severe, generalised abdominal pain., You answered ERCP, The correct answer is CT scan, There are two main differential diagnoses here. One is pancreatitis, repeated trauma to the, ampulla and duct (if partially cannulated) is a major risk factor for pancreatitis. The second is the, possibility that the duodenum has been perforated. ERCP is performed using a side viewing, endoscope, the manipulation of which can be technically challenging for the inexperienced, operator in a patient with abnormal anatomy. A CT scan is the best investigation to distinguish, between these two differential diagnoses., , Please rate this question:, , Discuss and give feedback, , Next question, , Surgical jaundice, Jaundice can present in a manner of different surgical situations. As with all types of jaundice a, careful history and examination will often give clues as to the most likely underlying cause. Liver, function tests whilst conveying little in the way of information about liver synthetic function, will often, facilitate classification as to whether the jaundice is pre hepatic, hepatic or post hepatic. The typical, LFT patterns are given below:
Page 3545 :
Location, , Bilirubin, , ALT/ AST, , Alkaline phosphatase, , Pre hepatic, , Normal or high, , Normal, , Normal, , Hepatic, , High, , Elevated (often very high), , Elevated but seldom to very high levels, , Post hepatic, , High-very high, , Moderate elevation, , High- very high, , In post hepatic jaundice the stools are often of pale colour and this feature should be specifically, addressed in the history., Modes of presentation, These are addressed in the table below:, , Diagnosis, , Typical features, , Pathogenesis, , Gallstones, , Typically history of biliary, colic or episodes of, chlolecystitis. Obstructive, type history and test, results., , Usually small calibre gallstones which can pass, through the cystic duct. In Mirizzi syndrome the stone, may compress the bile duct directly- one of the rare, times that cholecystitis may present with jaundice, , Cholangitis, , Usually obstructive and, will have Charcots triad of, symptoms (pain, fever,, jaundice), , Ascending infection of the bile ducts usually by E., coliand by definition occurring in a pool of stagnant, bile., , Pancreatic cancer, , Typically painless jaundice, with palpable gallbladder, (Courvoisier's Law), , Direct occlusion of distal bile duct or pancreatic duct, by tumour. Sometimes nodal disease at the portal, hepatis may be the culprit in which case the bile duct, may be of normal calibre., , TPN associated, , Usually follows long term, , Often due to hepatic dysfunction and fatty liver
Page 3546 :
Diagnosis, , Typical features, , Pathogenesis, , jaundice, , use and is usually painless, with non obstructive, features, , which may occur with long term TPN usage., , Bile duct injury, , Depending upon the type, of injury may be of, sudden or gradual onset, and is usually of, obstructive type, , Often due to a difficult cholecystectomy when, anatomy in Calots triangle is not appreciated. In the, worst scenario the bile duct is excised and jaundice, offers rapidly post operatively. More insidious is that, of bile duct stenosis which may be caused by clips or, diathermy injury., , Cholangiocarcinoma, , Gradual onset obstructive, pattern, , Direct occlusion by disease and also extrinsic, compression by nodal disease at the porta hepatis., , Septic surgical, patient, , Usually hepatic features, , Combination of impaired biliary excretion and drugs, such as ciprofloxacin which may cause cholestasis., , Metastatic disease, , Mixed hepatic and post, hepatic, , Combination of liver synthetic failure (late) and, extrinsic compression by nodal disease and, anatomical compression of intra hepatic structures, (earlier), , Diagnosis, An ultrasound of the liver and biliary tree is the most commonly used first line test. This will establish, bile duct calibre, often ascertain the presence of gallstones, may visualise pancreatic masses and, other lesions. The most important clinical question is essentially the extent of biliary dilatation and its, distribution., Where pancreatic neoplasia is suspected, the next test should be a pancreatic protocol CT scan., With liver tumours and cholangiocarcinoma an MRI/ MRCP is often the preferred option. PET scans, may be used to stage a number of malignancies but do not routinely form part of first line testing., Where MRCP fails to give adequate information an ERCP may be necessary. In many cases this, may form part of patient management. It is however, invasive and certainly not without risk and, highly operator dependent.
Page 3547 :
Management, Clearly this will depend to an extent upon the underlying cause but relief of jaundice is important,, even if surgery forms part of the planned treatment. Patients with unrelieved jaundice have a much, higher incidence of septic complications, bleeding and death., Screen for and address any clotting irregularities, In patients with malignancy a stent will need to be inserted. These come in two main types; metal, and plastic. Plastic stents are cheap and easy to replace and should be used if any surgical, intervention (e.g. Whipples) is planned. However, they are prone to displacement and blockage., Metal stents are much more expensive and may compromise a surgical resection. However, they, are far less prone to displacement and to a lesser extent blockage than their plastic counterparts., If malignancy is in bile duct/ pancreatic head and stenting has been attempted and has failed, then, an alternative strategy is to drain the biliary system percutaneously via a transhepatic route. It may, also be possible to insert a stent in this way. One of the main problems with temporary PTC's is their, propensity to displacement, which may result in a bile leak., In patients who have a bile duct injury surgery will be required to repair the defect. If the bile duct, has been inadvertently excised then a hepatico-jejunostomy will need to be created (difficult!), If gallstones are the culprit, then these may be removed by ERCP and a cholecystectomy, performed. Where there is doubt about the efficacy of the ERCP an operative cholangiogram should, be performed and bile duct exploration undertaken where stones remain. When the bile duct has, been formally opened the options are between closure over a T tube, a choledochoduodenostomy or, choledochojejunostomy., Patients with cholangitis should receive high dose broad spectrum antibiotics via the intravenous, route. Biliary decompression should follow soon afterwards, instrumenting the bile duct of these, patients will often provoke a septic episode (but should be done anyway)., Next question
Page 3548 :
Theme: Gallstone disease, , A., B., C., D., E., F., G., , Uncomplicated biliary colic, Acute cholecystitis, Cholangitis, Gallbladder abscess, Acalculous cholecystitis, Pancreatitis, Gallstone ileus, , Please select the most likely underlying diagnosis for the scenario given. Each option may be used, once, more than once or not at all., , 10., , A 68 year old man with type 2 diabetes is admitted to hospital unwell. On examination he, has features of septic shock and right upper quadrant tenderness. He is not jaundiced., Imaging shows a normal calibre bile duct and no stones in the gallbladder., You answered Uncomplicated biliary colic, The correct answer is Acalculous cholecystitis, Theme from April 2013 Exam, Acalculous cholecystitis is more common in patients with an underlying co-morbidity. The, morbidity and mortality following intervention are higher than in conventional gallstone, disease., , 11., , A 43 year old lady with known gallstones is admitted with a high fever and jaundice. On, examination, she looks extremely unwell. Her abdomen is generally soft although there is, some mild tenderness in the right upper quadrant., You answered Uncomplicated biliary colic, The correct answer is Cholangitis, Features of jaundice, fever and systemic sepsis are typical of cholangitis., , 12., , A 34 year old lady is admitted with a 3 day history of colicky right upper quadrant pain, which radiates to her back. The pain is now more constant. On examination she is not, jaundiced, but has a temperature of 38.5oC. She has localised peritonism in the right upper, quadrant., You answered Uncomplicated biliary colic
Page 3549 :
The correct answer is Acute cholecystitis, The features of pain and fever with right upper quadrant pain are suggestive of acute, cholecystitis. The short nature of the history makes an abscess less likely., Please rate this question:, , Discuss and give feedback, , Next question, , Gallstones, Up to 24% of women and 12% of men may have gallstones. Of these up to 30% may develop local, infection and cholecystitis. In patients subjected to surgery 12% will have stones contained within the, common bile duct. The majority of gallstones are of a mixed composition (50%) with pure cholesterol, stones accounting for 20% of cases., The aetiology of CBD stones differs in the world, in the West most CBD stones are the result of, migration. In the East a far higher proportion arise in the CBD de novo., The classical symptoms are of colicky right upper quadrant pain that occurs post prandially. The, symptoms are usually worst following a fatty meal when cholecystokinin levels are highest and, gallbladder contraction is maximal., Investigation, In almost all suspected cases the standard diagnostic work up consists of abdominal ultrasound and, liver function tests. Of patients who have stones within the bile duct, 60% will have at least one, abnormal result on LFT's. Ultrasound is an important test, but is operator dependent and therefore, may occasionally need to be repeated if a negative result is at odds with the clinical picture. Where, stones are suspected in the bile duct, the options lie between magnetic resonance cholangiography, and intraoperative imaging. The choice between these two options is determined by the skills and, experience of the surgeon. The advantages of intra operative imaging are less useful in making, therapeutic decisions if the operator is unhappy about proceeding the bile duct exploration, and in, such circumstances pre operative MRCP is probably a better option., Specific gallstone and gallbladder related disease, , Disease, , Features, , Management, , Biliary colic, , Colicky abdominal pain, worse, post prandially, worse after fatty, foods, , If imaging shows gallstones and history, compatible then laparoscopic cholecystectomy, , Acute, cholecystitis, , , , , , Right upper quadrant, pain, Fever, Murphys sign on, , Imaging (USS) and cholecystectomy (ideally, within 48 hours of presentation) (2)
Page 3550 :
Disease, , Features, , , , Gallbladder, abscess, , , , , , , , Cholangitis, , , , , , Gallstone, ileus, , , , , , Acalculous, cholecystitis, , , , , , , , , Management, , examination, Occasionally mildly, deranged LFT's, (especially if Mirizzi, syndrome), Usually prodromal, illness and right upper, quadrant pain, Swinging pyrexia, Patient may be, systemically unwell, Generalised peritonism, not present, , Imaging with USS +/- CT Scanning, Ideally surgery, sub total cholecystectomy may, be needed if Calots triangle is hostile, In unfit patients percutaneous drainage may be, considered, , Patient severely septic, and unwell, Jaundice, Right upper quadrant, pain, , , , , , , Patients may have a, history of previous, cholecystitis and known, gallstones, Small bowel obstruction, (may be intermittent), , Laparotomy and removal of gallstone from, small bowel, the enterotomy must be made, proximal to the site of obstruction and not at, the site of obstruction. The fistula between the, gallbladder and duodenum should not be, interfered with., , Patients with inter, current illness (e.g., diabetes, organ failure), Patient of systemically, unwell, Gallbladder, inflammation in absence, of stones, High fever, , If patient fit then cholecystectomy, if unfit then, percutaneous cholecystostomy, , Fluid resuscitation, Broad spectrum intravenous antibiotics, Correct any coagulopathy, Early ERCP
Page 3551 :
Treatment, Patients with asymptomatic gallstones rarely develop symptoms related to them (less than 2% per, year) and may therefore be managed expectantly. In almost all cases of symptomatic gallstones the, treatment of choice is cholecystectomy performed via the laparoscopic route. In the very frail patient, there is sometimes a role for selective use of ultrasound guided cholecystostomy., During the course of the procedure some surgeons will routinely perform either intra operative, cholangiography to either confirm anatomy or to exclude CBD stones. The latter may be more easily, achieved by use of laparoscopic ultrasound. If stones are found then the options lie between early, ERCP in the day or so following surgery or immediate surgical exploration of the bile duct. When, performed via the trans cystic route this adds little in the way of morbidity and certainly results in, faster recovery. Where transcystic exploration fails the alternative strategy is that of formal, choledochotomy. The exploration of a small duct is challenging and ducts of less than 8mm should, not be explored. Small stones that measure less than 5mm may be safely left and most will pass, spontaneously., Risks of ERCP(1), , , , , , Bleeding 0.9% (rises to 1.5% if sphincterotomy performed), Duodenal perforation 0.4%, Cholangitis 1.1%, Pancreatitis 1.5%, , References, 1. Williams E et al. Guidelines on the management of common bile duct stones, (CBDS)Gut2008;57:10041021, 2. Gurusamy KS, Samraj K. Early versus delayed laparoscopic cholecystectomy for acute, cholecystitis. Cochrane Database Syst Rev. 2006 Oct 18;(4):CD005440., 3. Gurusamy K and Davidson B. Gallstones. BMJ 2014 (348):27-30., Next question
Page 3552 :
Which of the following is the most sensitive blood test for diagnosis of acute pancreatitis?, , Amylase, , Lipase, , C-peptide, , Trypsin, , Trysinogen, , The serum amylase may rise and fall quite quickly and lead to a false negative result. Should the, clinical picture not be concordant with the amylase level then serum lipase or a CT Scan should be, performed., Please rate this question:, , Discuss and give feedback, , Next question, , Management of Pancreatitis, Management of Acute Pancreatitis in the UK, Diagnosis, , , , , , Traditionally hyperamylasaemia has been utilised with amylase being elevated three times, the normal range., However, amylase may give both false positive and negative results., Serum lipase is both more sensitive and specific than serum amylase. It also has a longer, half life., Serum amylase levels do not correlate with disease severity., , Differential causes of hyperamylasaemia, , Acute pancreatitis
Page 3553 :
Pancreatic pseudocyst, , Mesenteric infarct, , Perforated viscus, , Acute cholecystitis, , Diabetic ketoacidosis, , Assessment of severity, , , , Glasgow, Ranson scoring systems and APACHE II, Biochemical scoring e.g. using CRP, , Features that may predict a severe attack within 48 hours of admission to hospital, , Initial assessment, , , , , , , Clinical impression of severity, Body mass index >30, Pleural effusion, APACHE score >8, , 24 hours after admission, , , , , , , , Clinical impression of severity, APACHE II >8, Glasgow score of 3 or more, Persisting multiple organ failure, CRP>150, , 48 hours after admission, , , , , , Glasgow Score of >3, CRP >150, Persisting or progressive organ failure, , Table adapted from UK guidelines for management of acute pancreatitis. GUT 2005, 54 suppl III, Management, Nutrition
Page 3554 :
, , , , There is reasonable evidence to suggest that the use of enteral nutrition does not worsen the, outcome in pancreatitis, Most trials to date were underpowered to demonstrate a conclusive benefit., The rationale behind feeding is that it helps to prevent bacterial translocation from the gut,, thereby contributing to the development of infected pancreatic necrosis., , Use of antibiotic therapy, , , , , Many UK surgeons administer antibiotics to patients with acute pancreatitis. However, there, is very little evidence to support this practice., A recent Cochrane review highlights the potential benefits of administering Imipenem to, patients with established pancreatic necrosis in the hope of averting the progression to, infection., There are concerns that the administration of antibiotics in mild attacks of pancreatitis will not, affect outcome and may contribute to antibiotic resistance and increase the risks of antibiotic, associated diarrhoea., , Surgery, , , , , , Patients with acute pancreatitis due to gallstones should undergo early cholecystectomy., Patients with obstructed biliary system due to stones should undergo early ERCP., Patients with extensive necrosis where infection is suspected should usually undergo FNA, for culture., Patients with infected necrosis should undergo either radiological drainage or surgical, necrosectomy. The choice of procedure depends upon local expertise., , References, www.bsg.org.uk/pdfworddocs/pancreatic.pdf, Antibiotic therapy for prophylaxis against infection of pancreatic necrosis in acute, pancreatitis. Villatoro et al. Cochrane Library DOI: 10.1002/14651858.CD002941.pub3. 2010, version., Next question
Page 3555 :
Theme: Jaundice, , A. Gilberts syndrome, B. Crigler Najjar syndrome, C. Hepatocellular carcinoma, D. Mirizzi syndrome, E. Hepatitis A, F. Hepatitis E, G. Bile duct stones, H. Multi cystic liver disease, , Please select the most likely cause of jaundice for the scenario given. Each option may be used, once, more than once or not at all., , 14., , A 22 year old man returns to the UK from holiday in India. He presents with painless jaundice. On, examination he is not deeply jaundiced and there is no organomegaly., You answered Gilberts syndrome, The correct answer is Hepatitis A, Infective hepatitis is the most likely cause. In the UK, foreign travel is a common cause of, developing infectious hepatitis, of which hepatitis A is the most common., , 15., , A 56 year old man presents with jaundice. He has a long history of alcohol misuse. On, examination he is jaundiced and ultrasound shows multiple echo dense lesions in both lobes of, the liver. His alpha feto protein is elevated 6 times the normal range, You answered Gilberts syndrome, The correct answer is Hepatocellular carcinoma
Page 3556 :
HCC may complicate cirrhosis. AFP is often raised in HCC., , 16., , A 32 year old man who has suffered from Crohns disease for many years presents with, intermittent jaundice. When it occurs it is obstructive in nature. It then usually resolves, spontaneously., You answered Gilberts syndrome, The correct answer is Bile duct stones, Bile salts are absorbed in the terminal ileum. When this process is impaired as in Crohns the, patient may develop gallstones, if these pass into the CBD then obstructive jaundice will result., , Please rate this question:, , Discuss and give feedback, , Next question, , Surgical jaundice, Jaundice can present in a manner of different surgical situations. As with all types of jaundice a, careful history and examination will often give clues as to the most likely underlying cause. Liver, function tests whilst conveying little in the way of information about liver synthetic function, will often, facilitate classification as to whether the jaundice is pre hepatic, hepatic or post hepatic. The typical, LFT patterns are given below:, , Location, , Bilirubin, , ALT/ AST, , Alkaline phosphatase, , Pre hepatic, , Normal or high, , Normal, , Normal, , Hepatic, , High, , Elevated (often very high), , Elevated but seldom to very high levels
Page 3557 :
Location, , Bilirubin, , ALT/ AST, , Alkaline phosphatase, , Post hepatic, , High-very high, , Moderate elevation, , High- very high, , In post hepatic jaundice the stools are often of pale colour and this feature should be specifically, addressed in the history., Modes of presentation, These are addressed in the table below:, , Diagnosis, , Typical features, , Pathogenesis, , Gallstones, , Typically history of biliary, colic or episodes of, chlolecystitis. Obstructive, type history and test, results., , Usually small calibre gallstones which can pass, through the cystic duct. In Mirizzi syndrome the stone, may compress the bile duct directly- one of the rare, times that cholecystitis may present with jaundice, , Cholangitis, , Usually obstructive and, will have Charcots triad of, symptoms (pain, fever,, jaundice), , Ascending infection of the bile ducts usually by E., coliand by definition occurring in a pool of stagnant, bile., , Pancreatic cancer, , Typically painless jaundice, with palpable gallbladder, (Courvoisier's Law), , Direct occlusion of distal bile duct or pancreatic duct, by tumour. Sometimes nodal disease at the portal, hepatis may be the culprit in which case the bile duct, may be of normal calibre., , TPN associated, jaundice, , Usually follows long term, use and is usually painless, with non obstructive, features, , Often due to hepatic dysfunction and fatty liver, which may occur with long term TPN usage.
Page 3558 :
Diagnosis, , Typical features, , Pathogenesis, , Bile duct injury, , Depending upon the type, of injury may be of, sudden or gradual onset, and is usually of, obstructive type, , Often due to a difficult cholecystectomy when, anatomy in Calots triangle is not appreciated. In the, worst scenario the bile duct is excised and jaundice, offers rapidly post operatively. More insidious is that, of bile duct stenosis which may be caused by clips or, diathermy injury., , Cholangiocarcinoma, , Gradual onset obstructive, pattern, , Direct occlusion by disease and also extrinsic, compression by nodal disease at the porta hepatis., , Septic surgical, patient, , Usually hepatic features, , Combination of impaired biliary excretion and drugs, such as ciprofloxacin which may cause cholestasis., , Metastatic disease, , Mixed hepatic and post, hepatic, , Combination of liver synthetic failure (late) and, extrinsic compression by nodal disease and, anatomical compression of intra hepatic structures, (earlier), , Diagnosis, An ultrasound of the liver and biliary tree is the most commonly used first line test. This will establish, bile duct calibre, often ascertain the presence of gallstones, may visualise pancreatic masses and, other lesions. The most important clinical question is essentially the extent of biliary dilatation and its, distribution., Where pancreatic neoplasia is suspected, the next test should be a pancreatic protocol CT scan., With liver tumours and cholangiocarcinoma an MRI/ MRCP is often the preferred option. PET scans, may be used to stage a number of malignancies but do not routinely form part of first line testing., Where MRCP fails to give adequate information an ERCP may be necessary. In many cases this, may form part of patient management. It is however, invasive and certainly not without risk and, highly operator dependent., Management, Clearly this will depend to an extent upon the underlying cause but relief of jaundice is important,, even if surgery forms part of the planned treatment. Patients with unrelieved jaundice have a much, higher incidence of septic complications, bleeding and death.
Page 3559 :
Screen for and address any clotting irregularities, In patients with malignancy a stent will need to be inserted. These come in two main types; metal, and plastic. Plastic stents are cheap and easy to replace and should be used if any surgical, intervention (e.g. Whipples) is planned. However, they are prone to displacement and blockage., Metal stents are much more expensive and may compromise a surgical resection. However, they, are far less prone to displacement and to a lesser extent blockage than their plastic counterparts., If malignancy is in bile duct/ pancreatic head and stenting has been attempted and has failed, then, an alternative strategy is to drain the biliary system percutaneously via a transhepatic route. It may, also be possible to insert a stent in this way. One of the main problems with temporary PTC's is their, propensity to displacement, which may result in a bile leak., In patients who have a bile duct injury surgery will be required to repair the defect. If the bile duct, has been inadvertently excised then a hepatico-jejunostomy will need to be created (difficult!), If gallstones are the culprit, then these may be removed by ERCP and a cholecystectomy, performed. Where there is doubt about the efficacy of the ERCP an operative cholangiogram should, be performed and bile duct exploration undertaken where stones remain. When the bile duct has, been formally opened the options are between closure over a T tube, a choledochoduodenostomy or, choledochojejunostomy., Patients with cholangitis should receive high dose broad spectrum antibiotics via the intravenous, route. Biliary decompression should follow soon afterwards, instrumenting the bile duct of these, patients will often provoke a septic episode (but should be done anyway)., Next question
Page 3560 :
Theme: Surgical jaundice, , A. Carcinoma of the head of the pancreas, B. Bile duct stricture, C. Mirizzi syndrome, D. Bile duct stones, E. Chronic cholecystitis, F. Peri hilar lymphadenopathy, G. Fitz - Hugh Curtis syndrome, , Please select the most appropriate cause of the jaundice scenario given. Each option may be used, once, more than once or not at all., , 17., , A 63 year old man is admitted with obstructive jaundice that has developed over the past 3, weeks. He was previously well and on examination has a smooth mass in his right upper quadrant., Carcinoma of the head of the pancreas, Carcinoma of the pancreas (Courvoisiers law!). The development of jaundice in association with a, smooth right upper quadrant mass is typical of distal biliary obstruction secondary to pancreatic, malignancy. A bile duct stricture would not present in this way, all the other choices are related to, gallstones and Fitz Hugh Curtis syndrome is a complication of pelvic inflammatory disease., , 18., , A 41 year old lady is admitted with colicky right upper quadrant pain. On clinical examination she, has a mild pyrexia and is clinically jaundiced. An ultrasound scan is reported as showing gallstones, and the patient is taken to theatre for an open cholecystectomy. At operation, Calots triangle is, almost completely impossible to delineate., You answered Carcinoma of the head of the pancreas, The correct answer is Mirizzi syndrome, In Mirizzi syndrome the gallstone becomes impacted in Hartmans pouch. Episodes of recurrent
Page 3561 :
inflammation occur and this causes compression of the bile duct. In severe cases this then, progresses to fistulation. Surgery is extremely difficult as Calots triangle is often completely, obliterated and the risks of causing injury to the CBD are high., , 19., , A 72 year old man undergoes a distal gastrectomy for carcinoma of the stomach. He presents with, jaundice approximately 8 months post operatively. Ultrasound of the liver and bile ducts shows, no focal liver lesion and normal calibre common bile duct with intra hepatic duct dilatation., You answered Carcinoma of the head of the pancreas, The correct answer is Peri hilar lymphadenopathy, Unfortunately metastatic disease is the most likely event. Peri hilar lymphadenopathy would be a, common culprit., , Courvoisiers Law:, Obstructive jaundice in the presence of a palpable gallbladder is unlikely to be due to stones., This is due to the fibrotic effect that stones have on the gallbladder. Like all these laws there are, numerous exceptions and many cases will not present in the typical manner., Bile duct injury, Inadvertent bile duct injury during laparoscopic surgery should be referred to a specialist, hepatobiliary surgeon. Outcomes are far worse when repair is undertaken by a non specialist, surgeon in a district hospital., , Please rate this question:, , Discuss and give feedback, , Next question, , Surgical jaundice, Jaundice can present in a manner of different surgical situations. As with all types of jaundice a, careful history and examination will often give clues as to the most likely underlying cause. Liver, function tests whilst conveying little in the way of information about liver synthetic function, will often, facilitate classification as to whether the jaundice is pre hepatic, hepatic or post hepatic. The typical
Page 3562 :
LFT patterns are given below:, , Location, , Bilirubin, , ALT/ AST, , Alkaline phosphatase, , Pre hepatic, , Normal or high, , Normal, , Normal, , Hepatic, , High, , Elevated (often very high), , Elevated but seldom to very high levels, , Post hepatic, , High-very high, , Moderate elevation, , High- very high, , In post hepatic jaundice the stools are often of pale colour and this feature should be specifically, addressed in the history., Modes of presentation, These are addressed in the table below:, , Diagnosis, , Typical features, , Pathogenesis, , Gallstones, , Typically history of biliary, colic or episodes of, chlolecystitis. Obstructive, type history and test, results., , Usually small calibre gallstones which can pass, through the cystic duct. In Mirizzi syndrome the stone, may compress the bile duct directly- one of the rare, times that cholecystitis may present with jaundice, , Cholangitis, , Usually obstructive and, will have Charcots triad of, symptoms (pain, fever,, jaundice), , Ascending infection of the bile ducts usually by E., coliand by definition occurring in a pool of stagnant, bile., , Pancreatic cancer, , Typically painless jaundice, with palpable gallbladder, (Courvoisier's Law), , Direct occlusion of distal bile duct or pancreatic duct, by tumour. Sometimes nodal disease at the portal, hepatis may be the culprit in which case the bile duct, may be of normal calibre.
Page 3563 :
Diagnosis, , Typical features, , Pathogenesis, , TPN associated, jaundice, , Usually follows long term, use and is usually painless, with non obstructive, features, , Often due to hepatic dysfunction and fatty liver, which may occur with long term TPN usage., , Bile duct injury, , Depending upon the type, of injury may be of, sudden or gradual onset, and is usually of, obstructive type, , Often due to a difficult cholecystectomy when, anatomy in Calots triangle is not appreciated. In the, worst scenario the bile duct is excised and jaundice, offers rapidly post operatively. More insidious is that, of bile duct stenosis which may be caused by clips or, diathermy injury., , Cholangiocarcinoma, , Gradual onset obstructive, pattern, , Direct occlusion by disease and also extrinsic, compression by nodal disease at the porta hepatis., , Septic surgical, patient, , Usually hepatic features, , Combination of impaired biliary excretion and drugs, such as ciprofloxacin which may cause cholestasis., , Metastatic disease, , Mixed hepatic and post, hepatic, , Combination of liver synthetic failure (late) and, extrinsic compression by nodal disease and, anatomical compression of intra hepatic structures, (earlier), , Diagnosis, An ultrasound of the liver and biliary tree is the most commonly used first line test. This will establish, bile duct calibre, often ascertain the presence of gallstones, may visualise pancreatic masses and, other lesions. The most important clinical question is essentially the extent of biliary dilatation and its, distribution., Where pancreatic neoplasia is suspected, the next test should be a pancreatic protocol CT scan., With liver tumours and cholangiocarcinoma an MRI/ MRCP is often the preferred option. PET scans, may be used to stage a number of malignancies but do not routinely form part of first line testing., Where MRCP fails to give adequate information an ERCP may be necessary. In many cases this, may form part of patient management. It is however, invasive and certainly not without risk and
Page 3564 :
highly operator dependent., Management, Clearly this will depend to an extent upon the underlying cause but relief of jaundice is important,, even if surgery forms part of the planned treatment. Patients with unrelieved jaundice have a much, higher incidence of septic complications, bleeding and death., Screen for and address any clotting irregularities, In patients with malignancy a stent will need to be inserted. These come in two main types; metal, and plastic. Plastic stents are cheap and easy to replace and should be used if any surgical, intervention (e.g. Whipples) is planned. However, they are prone to displacement and blockage., Metal stents are much more expensive and may compromise a surgical resection. However, they, are far less prone to displacement and to a lesser extent blockage than their plastic counterparts., If malignancy is in bile duct/ pancreatic head and stenting has been attempted and has failed, then, an alternative strategy is to drain the biliary system percutaneously via a transhepatic route. It may, also be possible to insert a stent in this way. One of the main problems with temporary PTC's is their, propensity to displacement, which may result in a bile leak., In patients who have a bile duct injury surgery will be required to repair the defect. If the bile duct, has been inadvertently excised then a hepatico-jejunostomy will need to be created (difficult!), If gallstones are the culprit, then these may be removed by ERCP and a cholecystectomy, performed. Where there is doubt about the efficacy of the ERCP an operative cholangiogram should, be performed and bile duct exploration undertaken where stones remain. When the bile duct has, been formally opened the options are between closure over a T tube, a choledochoduodenostomy or, choledochojejunostomy., Patients with cholangitis should receive high dose broad spectrum antibiotics via the intravenous, route. Biliary decompression should follow soon afterwards, instrumenting the bile duct of these, patients will often provoke a septic episode (but should be done anyway)., Next question
Page 3565 :
A 59 year old man is diagnosed as having carcinoma of the pancreas with two malignant deposits in, the right lobe of the liver. What is the most appropriate treatment?, , Palliative chemotherapy, , Liver resection followed by chemotherapy, , Simultaneous resection of liver metastasis and en bloc segmental pancreatic resection, , Pancreatic resection followed by liver resection once recovered, , Radical radiotherapy followed by surgery, , Pancreatic cancer has a poor prognosis and most cases have metastatic disease at presentation., There is no role in pancreatic cancer for liver resection together with pancreatic surgery as there is, no survival benefit. Most centres will offer palliative chemotherapy which has improved both, longevity and quality of life., Please rate this question:, , Discuss and give feedback, , Next question, , Pancreatic cancer, , , , , , , Adenocarcinoma, Risk factors: Smoking, diabetes, adenoma, familial adenomatous polyposis, Mainly occur in the head of the pancreas (70%), Spread locally and metastasizes to the liver, Carcinoma of the pancreas should be differentiated from other periampullary tumours with, better prognosis, , Clinical features, , , , , , , Weight loss, Painless jaundice, Epigastric discomfort (pain usually due to invasion of the coeliac plexus is a late feature), Pancreatitis, Trousseau's sign: migratory superficial thrombophlebitis
Page 3566 :
Investigations, , , , , , , USS: May miss small lesions, CT Scanning (pancreatic protocol). If unresectable on CT then no further staging needed, PET/CT for those with operable disease on CT alone, ERCP/ MRI for bile duct assessment, Staging laparoscopy to exclude peritoneal disease, , Management, , , , , , , Head of pancreas: Whipple's resection (SE dumping and ulcers). Newer techniques include, pylorus preservation and SMA/ SMV resection, Carcinoma body and tail: poor prognosis, distal pancreatectomy, if operable, Usually adjuvent chemotherapy for resectable disease, ERCP and stent for jaundice and palliation, Surgical bypass may be needed for duodenal obstruction, , Next question
Page 3567 :
A 41 year old lady with colicky right upper quadrant pain is identified as having gallstones on an, abdominal ultrasound scan. What is the most appropriate course of action?, , Laparoscopic cholecystectomy, , Open cholecystectomy, , Liver function tests, , MRCP, , ERCP, , Liver function testing is part of the core diagnostic work up of biliary colic and surgical planning, cannot proceed until this (and the diameter of the CBD on USS) are known., Please rate this question:, , Discuss and give feedback, , Next question, , Gallstones, Up to 24% of women and 12% of men may have gallstones. Of these up to 30% may develop local, infection and cholecystitis. In patients subjected to surgery 12% will have stones contained within the, common bile duct. The majority of gallstones are of a mixed composition (50%) with pure cholesterol, stones accounting for 20% of cases., The aetiology of CBD stones differs in the world, in the West most CBD stones are the result of, migration. In the East a far higher proportion arise in the CBD de novo., The classical symptoms are of colicky right upper quadrant pain that occurs post prandially. The, symptoms are usually worst following a fatty meal when cholecystokinin levels are highest and, gallbladder contraction is maximal., Investigation, In almost all suspected cases the standard diagnostic work up consists of abdominal ultrasound and, liver function tests. Of patients who have stones within the bile duct, 60% will have at least one, abnormal result on LFT's. Ultrasound is an important test, but is operator dependent and therefore, may occasionally need to be repeated if a negative result is at odds with the clinical picture. Where, stones are suspected in the bile duct, the options lie between magnetic resonance cholangiography, and intraoperative imaging. The choice between these two options is determined by the skills and, experience of the surgeon. The advantages of intra operative imaging are less useful in making, therapeutic decisions if the operator is unhappy about proceeding the bile duct exploration, and in, such circumstances pre operative MRCP is probably a better option.
Page 3568 :
Specific gallstone and gallbladder related disease, , Disease, , Features, , Management, , Biliary colic, , Colicky abdominal pain, worse, post prandially, worse after fatty, foods, , If imaging shows gallstones and history, compatible then laparoscopic cholecystectomy, , Acute, cholecystitis, , , , , , , Gallbladder, abscess, , , , , , , , Cholangitis, , , , , , Gallstone, ileus, , , , , , Right upper quadrant, pain, Fever, Murphys sign on, examination, Occasionally mildly, deranged LFT's, (especially if Mirizzi, syndrome), , Imaging (USS) and cholecystectomy (ideally, within 48 hours of presentation) (2), , Usually prodromal, illness and right upper, quadrant pain, Swinging pyrexia, Patient may be, systemically unwell, Generalised peritonism, not present, , Imaging with USS +/- CT Scanning, Ideally surgery, sub total cholecystectomy may, be needed if Calots triangle is hostile, In unfit patients percutaneous drainage may be, considered, , Patient severely septic, and unwell, Jaundice, Right upper quadrant, pain, , , , , , , Patients may have a, history of previous, cholecystitis and known, gallstones, Small bowel obstruction, (may be intermittent), , Laparotomy and removal of gallstone from, small bowel, the enterotomy must be made, proximal to the site of obstruction and not at, the site of obstruction. The fistula between the, gallbladder and duodenum should not be, interfered with., , Fluid resuscitation, Broad spectrum intravenous antibiotics, Correct any coagulopathy, Early ERCP
Page 3569 :
Disease, , Features, , Acalculous, cholecystitis, , , , , , , , , Patients with inter, current illness (e.g., diabetes, organ failure), Patient of systemically, unwell, Gallbladder, inflammation in absence, of stones, High fever, , Management, , If patient fit then cholecystectomy, if unfit then, percutaneous cholecystostomy, , Treatment, Patients with asymptomatic gallstones rarely develop symptoms related to them (less than 2% per, year) and may therefore be managed expectantly. In almost all cases of symptomatic gallstones the, treatment of choice is cholecystectomy performed via the laparoscopic route. In the very frail patient, there is sometimes a role for selective use of ultrasound guided cholecystostomy., During the course of the procedure some surgeons will routinely perform either intra operative, cholangiography to either confirm anatomy or to exclude CBD stones. The latter may be more easily, achieved by use of laparoscopic ultrasound. If stones are found then the options lie between early, ERCP in the day or so following surgery or immediate surgical exploration of the bile duct. When, performed via the trans cystic route this adds little in the way of morbidity and certainly results in, faster recovery. Where transcystic exploration fails the alternative strategy is that of formal, choledochotomy. The exploration of a small duct is challenging and ducts of less than 8mm should, not be explored. Small stones that measure less than 5mm may be safely left and most will pass, spontaneously., Risks of ERCP(1), , , , , , Bleeding 0.9% (rises to 1.5% if sphincterotomy performed), Duodenal perforation 0.4%, Cholangitis 1.1%, Pancreatitis 1.5%, , References, 1. Williams E et al. Guidelines on the management of common bile duct stones, (CBDS)Gut2008;57:10041021, 2. Gurusamy KS, Samraj K. Early versus delayed laparoscopic cholecystectomy for acute, cholecystitis. Cochrane Database Syst Rev. 2006 Oct 18;(4):CD005440., 3. Gurusamy K and Davidson B. Gallstones. BMJ 2014 (348):27-30., Next question
Page 3570 :
A 42 year old female presents with symptoms of biliary colic and on investigation is identified as, having gallstones. Of the procedures listed below, which is most likely to increase the risk of, gallstone formation?, , Partial gastrectomy, , Jejunal resection, , Liver lobectomy, , Ileal resection, , Left hemicolectomy, , Bile salt reabsorption occurs at the ileum. Therefore cholesterol gallstones form as a result of ileal, resection., Please rate this question:, , Discuss and give feedback, , Next question, , Biliary disease, Diagnosis, , Typical features, , Pathogenesis, , Gallstones, , Typically history of, biliary colic or episodes, of chlolecystitis., Obstructive type history, , Usually small calibre gallstones which can pass, through the cystic duct. In Mirizzi syndrome the, stone may compress the bile duct directly- one of, the rare times that cholecystitis may present with
Page 3571 :
and test results., , jaundice, , Cholangitis, , Usually obstructive and, will have Charcot's triad, of symptoms (pain,, fever, jaundice), , Ascending infection of the bile ducts usually by E., coliand by definition occurring in a pool of stagnant, bile., , Pancreatic cancer, , Typically painless, jaundice with palpable, gallbladder, (Courvoisier's Law), , Direct occlusion of distal bile duct or pancreatic, duct by tumour. Sometimes nodal disease at the, portal hepatis may be the culprit in which case the, bile duct may be of normal calibre., , TPN (total parenteral, nutrition) associated, jaundice, , Usually follows long, term use and is usually, painless with non, obstructive features, , Often due to hepatic dysfunction and fatty liver, which may occur with long term TPN usage., , Bile duct injury, , Depending upon the, type of injury may be of, sudden or gradual onset, and is usually of, obstructive type, , Often due to a difficult laparoscopic•, cholecystectomy when anatomy in Calots triangle is, not appreciated. In the worst scenario the bile duct, is excised and jaundice develops rapidly post, operatively. More insidious is that of bile duct, stenosis which may be caused by clips or diathermy, injury., , Cholangiocarcinoma, , Gradual onset, obstructive pattern, , Direct occlusion by disease and also extrinsic, compression by nodal disease at the porta hepatis., , Septic surgical patient, , Usually hepatic features, , Combination of impaired biliary excretion and, drugs such as ciprofloxacin which may cause, cholestasis., , Metastatic disease, , Mixed hepatic and post, hepatic, , Combination of liver synthetic failure (late) and, extrinsic compression by nodal disease and, anatomical compression of intra hepatic structures
Page 3572 :
(earlier), , A gallbladder may develop a thickened wall in chronic cholecystitis, microscopically RoikitanskyAschoff Sinuses may be seen, , Image sourced from Wikipedia, , Next question
Page 3573 :
Theme: Management of pancreatitis, , A., B., C., D., E., F., G., , Non Contrast enhanced CT scan, USS abdomen, ERCP alone, ERCP with Sphincterotomy and biliary drainage, Fine needle aspiration of necrosis, Pancreatic necrosectomy, Contrast enhanced CT scan, , What is the next best step in management for the scenario given? Each option may be used once,, more than once or not at all., , 23., , A 58 year old woman is admitted with an attack of severe acute pancreatitis. She is, managed on the intensive care unit and is making progress. She then deteriorates and a CT, scan shows extensive pancreatic necrosis (>40%). There are concerns that this may have, become infected., You answered Non Contrast enhanced CT scan, The correct answer is Fine needle aspiration of necrosis, When there are concerns that pancreatic necrosis may have become infected the usual, approach is to perform an image guided FNA for culture. There is always the risk of, seeding infection with such a strategy so it must be performed with care. Pancreatic, necrosectomy is not usually undertaken until the presence of infection is proven., , 24., , A 22 year old teacher is admitted with severe epigastric pain. Serum amylase is normal., You wish to exclude a perforated viscus, and determine whether pancreatitis is present., You answered Non Contrast enhanced CT scan, The correct answer is Contrast enhanced CT scan, An ultrasound will not accurately answer this question. Therefore a CT scan is required., Oral and IV contrast would usually be given., , 25., , A 55 year old accountant has jaundice and a temperature of 39 oC. He is known to have, gallstones. Blood cultures have grown a gram negative bacilli. Imaging shows a bile duct, measuring 1.2cm in diameter., You answered Non Contrast enhanced CT scan
Page 3574 :
The correct answer is ERCP with Sphincterotomy and biliary drainage, You should suspect cholangitis in a patient with fevers and jaundice. Charcot's triad may, only be present in 20% of patients. This patient needs biliary drainage with an ERCP., Infected pancreatic necrosis is one of the few indications for surgery in pancreatitis, Please rate this question:, , Discuss and give feedback, , Next question, , Management of Pancreatitis, Management of Acute Pancreatitis in the UK, Diagnosis, , , , , , Traditionally hyperamylasaemia has been utilised with amylase being elevated three times, the normal range., However, amylase may give both false positive and negative results., Serum lipase is both more sensitive and specific than serum amylase. It also has a longer, half life., Serum amylase levels do not correlate with disease severity., , Differential causes of hyperamylasaemia, , Acute pancreatitis, , Pancreatic pseudocyst, , Mesenteric infarct, , Perforated viscus, , Acute cholecystitis, , Diabetic ketoacidosis
Page 3575 :
Assessment of severity, , , , Glasgow, Ranson scoring systems and APACHE II, Biochemical scoring e.g. using CRP, , Features that may predict a severe attack within 48 hours of admission to hospital, , Initial assessment, , , , , , , Clinical impression of severity, Body mass index >30, Pleural effusion, APACHE score >8, , 24 hours after admission, , , , , , , , Clinical impression of severity, APACHE II >8, Glasgow score of 3 or more, Persisting multiple organ failure, CRP>150, , 48 hours after admission, , , , , , Glasgow Score of >3, CRP >150, Persisting or progressive organ failure, , Table adapted from UK guidelines for management of acute pancreatitis. GUT 2005, 54 suppl III, Management, Nutrition, , , , , There is reasonable evidence to suggest that the use of enteral nutrition does not worsen the, outcome in pancreatitis, Most trials to date were underpowered to demonstrate a conclusive benefit., The rationale behind feeding is that it helps to prevent bacterial translocation from the gut,, thereby contributing to the development of infected pancreatic necrosis., , Use of antibiotic therapy, , , , Many UK surgeons administer antibiotics to patients with acute pancreatitis. However, there, is very little evidence to support this practice., A recent Cochrane review highlights the potential benefits of administering Imipenem to, patients with established pancreatic necrosis in the hope of averting the progression to, infection.
Page 3576 :
, , There are concerns that the administration of antibiotics in mild attacks of pancreatitis will not, affect outcome and may contribute to antibiotic resistance and increase the risks of antibiotic, associated diarrhoea., , Surgery, , , , , , Patients with acute pancreatitis due to gallstones should undergo early cholecystectomy., Patients with obstructed biliary system due to stones should undergo early ERCP., Patients with extensive necrosis where infection is suspected should usually undergo FNA, for culture., Patients with infected necrosis should undergo either radiological drainage or surgical, necrosectomy. The choice of procedure depends upon local expertise., , References, www.bsg.org.uk/pdfworddocs/pancreatic.pdf, Antibiotic therapy for prophylaxis against infection of pancreatic necrosis in acute, pancreatitis. Villatoro et al. Cochrane Library DOI: 10.1002/14651858.CD002941.pub3. 2010, version., Next question
Page 3577 :
A 43 year old male with long standing chronic hepatitis is being followed up. Recently his AFP is, noted to be increased and an abdominal USS demonstrates a 2cm lesion in segment V of the liver., What is the most appropriate course of action?, , PET CT scan, , Liver MRI, , USS guided liver biopsy, , Laparoscopic biopsy, , Segmental resection of segment V, , Liver lesions that are suspicious of HCC should be scanned prior to resection as there is a risk of, multifocal lesions that would either preclude or otherwise affect the decision to proceed with, segmental resection., Please rate this question:, , Discuss and give feedback, , Next question, , Hepatocellular carcinoma, Hepatocellular carcinoma is the second leading cause of cancer deaths globally. Up to 750,000, cases are reported annually. Unfortunately the incidence approximates to the death rate so there are, few long term survivors[1]. The disease occurs most commonly in those with chronic hepatitis and, established liver cirrhosis. Therefore, these individuals should be closely screened for the, development of HCC with serum AFP and liver USS every 6-12 months. Rising AFP and liver USS, showing a nodule greater than 1cm in diameter makes HCC much more likely and such patients, should then undergo MRI scanning., The presence of adenomas in an otherwise healthy liver is a recognised risk factor for HCC [2, 3], and many surgeons will remove liver adenomas for this reason[4].
Page 3578 :
Diagnosis, The aim is to avoid unnecessary percutaneous biopsy. Radiologically on CT the classical feature is a, suspicious lesion which is highlighted during the arterial phase with washout during the venous, phase, this reflects the hypervascularity of the lesions.The risk of tumour seeding as a result of a, liver biopsy is 2.7% with a median time interval between biopsy and seeding of 17 months[5]., Barcelona Clinic Liver Classification, There are many classification systems for addressing the management and prognosis, the BCLC, system has the convenience of categorising disease extent with treatment and prognostic outcomes., In determining the ideal treatment modality for HCC the key points are not just disease extent, but, also the functional state of the liver and patient., , Stage, , Features, , Treatment, , Prognosis-5 yr, survival, , Stage, 0, , Child-Pugh A, Single lesion (less than 2cm), Normal portal pressures, , Resection, , 40-70%, , Stage, A, , Single nodule greater than 3cm or, multiple nodules (no more than 3), Child Pugh A/ B, , If associated disease then, radiofrequency ablation, If no associated disease then, transplantation, , May be up to 70%, in some, , Stage, B, , Multiple nodules, Child Pugh A/B, , Trans arterial chemo-embolisation, (usually with doxorubicin), , 26% at 3 years, , Stage, C, , Advanced tumours, Invasion of portal vein, Child Pugh A/B, , Sorafenib, , Usually survive, 10.7 months, , Stage, D, , Child Pugh stage C, Advanced tumours, , Best supportive care, , Less than 6, months survival, , [6], In selected patients the best outcomes are achieved with surgical resection, or transplantation where, surgical resection is precluded. Anatomical resections with minimum 2cm margins provide the best
Page 3579 :
outcomes., At the present time there is no evidence to recommend treatment with adjuvant chemotherapy[6]., Sorafenib, This is an oral multi tyrosine kinase inhibitor. It is the only drug that has been currently demonstrated, to extend survival in individuals with advanced hepatocellular cancer[7]. The improvement in survival, is from a median of 7 months to 10 months., References, 1. Jemal, A., et al., Global cancer statistics. CA Cancer J Clin, 2011. 61(2): p. 69-90., 2. Leese, T., O. Farges, and H. Bismuth, Liver cell adenomas. A 12-year surgical experience from a, specialist hepato-biliary unit. Ann Surg, 1988. 208(5): p. 558-64., 3. Farges, O. and S. Dokmak, Malignant transformation of liver adenoma: an analysis of the, literature. Dig Surg, 2010. 27(1): p. 32-8., 4. Ehrl, D., et al., "Incidentaloma" of the liver: management of a diagnostic and therapeutic dilemma., HPB Surg, 2012. 2012: p. 891787., 5. Silva, M.A., et al., Needle track seeding following biopsy of liver lesions in the diagnosis of, hepatocellular cancer: a systematic review and meta-analysis. Gut, 2008. 57(11): p. 1592-6., 6. EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol,, 2012. 56(4): p. 908-43., 7. Abou-Alfa, G.K., et al., Phase II study of sorafenib in patients with advanced hepatocellular, carcinoma. J Clin Oncol, 2006. 24(26): p. 4293-300., Next question
Page 3580 :
Theme: Management of biliary diseases, , A. Acute laparoscopic cholecystectomy, B. Delayed laparoscopic cholecystectomy, C. Percutaneous cholecystostomy, D. Lithotripsy, E. Endoscopic retrograde cholangiopancreatography, F. Choledochoduodenostomy, G. Bile duct excision and hepatico-jejunostomy, H. Operative cholecystostomy, , Please select the most appropriate management option for the scenario given. Each option may be, used once, more than once or not at all., , 27., , A 43 year old women is admitted with acute cholecystitis and fails to settle. A laparoscopic, cholecystectomy is being performed, at operation the gallbladder has evidence of an empyema, and Calots triangle is inflamed and the surgeon suspects that a Mirizzi syndrome has occurred., You answered Acute laparoscopic cholecystectomy, The correct answer is Operative cholecystostomy, This will address the acute sepsis and resolve the situation. Attempts at completing the surgery at, this stage, even in expert hands carries a very high risk of bile duct injury., , 28., , Following a difficult cholecystectomy a surgeon leaves a drain. 24 hours later bile is seen to be, accumulating in the drain and this fails to resolve over the next 48 hours. The patient is otherwise, well., You answered Acute laparoscopic cholecystectomy, The correct answer is Endoscopic retrograde cholangiopancreatography
Page 3581 :
This will delineate the presence of potential bile duct injury. Usually this is result of leakage from, the cystic duct and placement of a stent will allow free biliary drainage and the leak should settle., , 29., , A 40 year old woman is admitted with abdominal pain. She has suffered from repeated episodes, of this colicky right upper quadrant pain. On examination she is pyrexial with right upper quadrant, peritonism. Her blood tests show a white cell count of 23. However, the liver function tests are, normal. An abdominal ultrasound scan shows multiple gallstones in a thick walled gallbladder, the, bile duct measures 4mm., Acute laparoscopic cholecystectomy, This lady has acute cholecystitis and needs an acute cholecystectomy. This operation should, usually be performed within 48 hours of admission. Delay beyond this timeframe will usually, result in increased operative complications and most surgeons would administer antibiotics and, perform and interval cholecystectomy if the early window for an acute procedure is missed. A bile, duct measuring 4mm is usually normal., , Please rate this question:, , Discuss and give feedback, , Next question, , Biliary disease, Diagnosis, , Typical features, , Pathogenesis, , Gallstones, , Typically history of, biliary colic or episodes, of chlolecystitis., Obstructive type history, and test results., , Usually small calibre gallstones which can pass, through the cystic duct. In Mirizzi syndrome the, stone may compress the bile duct directly- one of, the rare times that cholecystitis may present with, jaundice
Page 3582 :
Cholangitis, , Usually obstructive and, will have Charcot's triad, of symptoms (pain,, fever, jaundice), , Ascending infection of the bile ducts usually by E., coliand by definition occurring in a pool of stagnant, bile., , Pancreatic cancer, , Typically painless, jaundice with palpable, gallbladder, (Courvoisier's Law), , Direct occlusion of distal bile duct or pancreatic, duct by tumour. Sometimes nodal disease at the, portal hepatis may be the culprit in which case the, bile duct may be of normal calibre., , TPN (total parenteral, nutrition) associated, jaundice, , Usually follows long, term use and is usually, painless with non, obstructive features, , Often due to hepatic dysfunction and fatty liver, which may occur with long term TPN usage., , Bile duct injury, , Depending upon the, type of injury may be of, sudden or gradual onset, and is usually of, obstructive type, , Often due to a difficult laparoscopic•, cholecystectomy when anatomy in Calots triangle is, not appreciated. In the worst scenario the bile duct, is excised and jaundice develops rapidly post, operatively. More insidious is that of bile duct, stenosis which may be caused by clips or diathermy, injury., , Cholangiocarcinoma, , Gradual onset, obstructive pattern, , Direct occlusion by disease and also extrinsic, compression by nodal disease at the porta hepatis., , Septic surgical patient, , Usually hepatic features, , Combination of impaired biliary excretion and, drugs such as ciprofloxacin which may cause, cholestasis., , Metastatic disease, , Mixed hepatic and post, hepatic, , Combination of liver synthetic failure (late) and, extrinsic compression by nodal disease and, anatomical compression of intra hepatic structures, (earlier)
Page 3583 :
A gallbladder may develop a thickened wall in chronic cholecystitis, microscopically RoikitanskyAschoff Sinuses may be seen, , Image sourced from Wikipedia, , Next question
Page 3584 :
Theme: Liver tumours, , A., B., C., D., E., F., G., H., , Rhabdomyosarcoma, Yolk sac tumour, Hepatocellular carcinoma, Metastatic lesion, Haemangioendothelioma, Cholangiocarcinoma, Hepatoblastoma, Angiosarcoma, , Please select the most likely diagnosis for the scenario given. Each answer may be used once, more, than once or not at all., , 30., , A 56 year old man with long standing ulcerative colitis and a DALM lesion in the rectum, is admitted with jaundice. On CT scanning the liver has 3 nodules in the right lobe and 1, nodule in the left lobe. Carcinoembryonic antigen levels are elevated., You answered Rhabdomyosarcoma, The correct answer is Metastatic lesion, This is likely to be due to metastatic lesions from a colonic primary. DALM lesions should, be excised by oncological colectomy for this reason. This burden of metastatic disease is, unlikely to precipitate jaundice directly and nodal disease at the porta hepatis is the most, likely cause in this case., , 31., , A 48 year old lady with chronic hepatitis B infection is noted to have worsening liver, function tests and progressive jaundice. Her alpha feto protein levels are grossly elevated., You answered Rhabdomyosarcoma, The correct answer is Hepatocellular carcinoma, This is most likely to be hepatocellular carcinoma and markedly elevated AFP levels in, association with a compatible risk factor should make this the diagnosis., , 32., , A 55 year old man with long standing ulcerative colitis is admitted with cholangitis and, weight loss. Blood tests reveal a markedly elevated CA 19-9., You answered Rhabdomyosarcoma, The correct answer is Cholangiocarcinoma
Page 3585 :
This is most likely a cholangiocarcinoma. UC with sclerosing cholangitis increases the risk, of cholangiocarcinoma. CA19-9 is elevated in approximately 80% cases., Please rate this question:, , Discuss and give feedback, , Next question, , Liver tumours, Primary liver tumours, The most common primary tumours are cholangiocarcinoma and hepatocellular carcinoma. Overall, metastatic disease accounts for 95% of all liver malignancies making the primary liver tumours, comparatively rare., Primary liver tumours include:, , , , , , , , Cholangiocarcinoma, Hepatocellular carcinoma, Hepatoblastoma, Sarcomas (Rare), Lymphomas, Carcinoids (most often secondary although primary may occur), , Hepatocellular carcinoma, These account for the bulk of primary liver tumours (75% cases). Its worldwide incidence reflects its, propensity to occur on a background of chronic inflammatory activity. Most cases arise in cirrhotic, livers or those with chronic hepatitis B infection, especially where viral replication is actively, occurring. In the UK it accounts for less than 5% of all cancers, although in parts of Asia its, incidence is 100 per 100,000., The majority of patients (80%) present with existing liver cirrhosis, with a mass discovered on, screening ultrasound., Diagnosis, , , , , , CT/ MRI (usually both) are the imaging modalities of choice, a-fetoprotein is elevated in almost all cases, Biopsy should be avoided as it seeds tumours cells through a resection plane., In cases of diagnostic doubt serial CT and αFP measurements are the preferred strategy., , Treatment
Page 3586 :
, , , , , , Patients should be staged with liver MRI and chest, abdomen and pelvic CT scan., The testis should be examined in males (testicular tumours may cause raised AFP). PET CT, may be used to identify occult nodal disease., Surgical resection is the mainstay of treatment in operable cases. In patients with a small, primary tumour in a cirrhotic liver whose primary disease process is controlled, consideration, may be given to primary whole liver resection and transplantation., Liver resections are an option but since most cases occur in an already diseased liver the, operative risks and post-operative hepatic dysfunction are far greater than is seen following, metastectomy., These tumours are not particularly chemo or radiosensitive however, both may be used in a, palliative setting. Tumour ablation is a more popular strategy., , Survival, Poor, overall survival is 15% at 5 years., Cholangiocarcinoma, This is the second most common type of primary liver malignancy. As its name suggests these, tumours arise in the bile ducts. Up to 80% of tumours arise in the extra hepatic biliary tree. Most, patients present with jaundice and by this stage the majority will have disease that is not resectable., Primary sclerosing cholangitis is the main risk factor. In deprived countries typhoid and liver flukes, are also major risk factors., Diagnosis, , , , , Patients will typically have an obstructive picture on liver function tests., CA 19-9, CEA and CA 125 are often elevated, CT/ MRI and MRCP are the imaging methods of choice., , Treatment, , , , Surgical resection offers the best chance of cure. Local invasion of peri hilar tumours is a, particular problem and this coupled with lobar atrophy will often contra indicate surgical, resection., Palliation of jaundice is important, although metallic stents should be avoided in those, considered for resection., , Survival, Is poor, approximately 5-10% 5 year survival., Next question
Page 3587 :
A 45 year old man presents with an episode of alcoholic pancreatitis. He makes slow but steady, progress. He is reviewed clinically at 6 weeks following admission. He has a diffuse fullness of his, upper abdomen and on imaging a collection of fluid is found to be located behind the stomach. His, serum amylase is mildly elevated. Which of the following is the most likely explanation?, , Early fluid collection, , Pancreatic abscess, , Peripancreatic necrosis, , Pseudocyst, , Sterile necrosis, , Psuedocysts are unlikely to be present less than 4 weeks after an attack of acute pancreatitis., However, they are more common at this stage and are associated with a raised amylase., Please rate this question:, , Discuss and give feedback, , Next question, , Pancreatitis: sequelae, Peripancreatic fluid collections, , , , , , Occur in 25% cases, Located in or near the pancreas and lack a wall of granulation or fibrous tissue, May resolve or develop into pseudocysts or abscesses, Since most resolve aspiration and drainage is best avoided as it may precipitate infection, , Pseudocysts, , , , , , In acute pancreatitis result from organisation of peripancreatic fluid collection. They may or, may not communicate with the ductal system., The collection is walled by fibrous or granulation tissue and typically occurs 4 weeks or more, after an attack of acute pancreatitis, Most are retrogastric, 75% are associated with persistent mild elevation of amylase
Page 3588 :
, , , , Investigation is with CT, ERCP and MRI or Endoscopic USS, Symptomatic cases may be observed for 12 weeks as up to 50% resolve, Treatment is either with endoscopic or surgical cystogastrostomy or aspiration, , Pancreatic necrosis, , , , , , , Pancreatic necrosis may involve both the pancreatic parenchyma and surrounding fat, Complications are directly linked to extent of parenchymal necrosis and extent of necrosis, overall, Early necrosectomy is associated with a high mortality rate (and should be avoided unless, compelling indications for surgery exist), Sterile necrosis should be managed conservatively (at least initially), Some centres will perform fine needle aspiration sampling of necrotic tissue if infection is, suspected. False negatives may occur. The extent of sepsis and organ dysfunction may be a, better guide to surgery, , Pancreatic abscess, , , , , Intra abdominal collection of pus associated with pancreas but in the absence of necrosis, Typically occur as a result of infected pseudocyst, They are usually managed by placement of percutaneous drains, , Haemorrhage, , , , Infected necrosis may involve vascular structures with resultant haemorrhage that may occur, de novo or as a result of surgical necrosectomy., When retroperitoneal haemorrhage occurs Grey Turners sign may be identified, Next question
Page 3589 :
A 34 year old lady is admitted with pancreatitis. The aetiology is unclear and it is classified as an, attack of moderate severity according to the Glasgow criteria. Her imaging shows no gallstones and, fluid around the pancreas. Which of the following is the most appropriate initial management option?, , Laparotomy, , Laparoscopy, , Radiological aspiration of the fluid, , Active observation, , Administration of octreotide, LEARN THIS!, Mnemonic for the assessment of the severity of pancreatitis: PANCREAS, (Ann R Coll Surg Engl 2000; 82: 16-17, P a02 < 60 mmHg, A ge > 55 years, N eutrophils > 15 x 10/l, C alcium < 2 mmol/l, R aised urea > 16 mmol/l, E nzyme (lactate dehydrogenase) > 600 units/l, A lbumin < 32 g/l, S ugar (glucose) > 10 mmol/l, > 3 positive criteria indicates severe pancreatitis., Acute early fluid collections are seen in 25% of patients with pancreatitis and require no specific, treatment. Attempts at drainage may introduce infection and result in pancreatic abscess formation., Please rate this question:, , Discuss and give feedback, , Next question, , Management of Pancreatitis, Management of Acute Pancreatitis in the UK
Page 3590 :
Diagnosis, , , , , , Traditionally hyperamylasaemia has been utilised with amylase being elevated three times, the normal range., However, amylase may give both false positive and negative results., Serum lipase is both more sensitive and specific than serum amylase. It also has a longer, half life., Serum amylase levels do not correlate with disease severity., , Differential causes of hyperamylasaemia, , Acute pancreatitis, , Pancreatic pseudocyst, , Mesenteric infarct, , Perforated viscus, , Acute cholecystitis, , Diabetic ketoacidosis, , Assessment of severity, , , , Glasgow, Ranson scoring systems and APACHE II, Biochemical scoring e.g. using CRP, , Features that may predict a severe attack within 48 hours of admission to hospital, , Initial assessment, , , , , , , Clinical impression of severity, Body mass index >30, Pleural effusion, APACHE score >8, , 24 hours after admission, , , , , Clinical impression of severity, APACHE II >8
Page 3591 :
48 hours after admission, , , , , , Glasgow score of 3 or more, Persisting multiple organ failure, CRP>150, , , , , , Glasgow Score of >3, CRP >150, Persisting or progressive organ failure, , Table adapted from UK guidelines for management of acute pancreatitis. GUT 2005, 54 suppl III, Management, Nutrition, , , , , There is reasonable evidence to suggest that the use of enteral nutrition does not worsen the, outcome in pancreatitis, Most trials to date were underpowered to demonstrate a conclusive benefit., The rationale behind feeding is that it helps to prevent bacterial translocation from the gut,, thereby contributing to the development of infected pancreatic necrosis., , Use of antibiotic therapy, , , , , Many UK surgeons administer antibiotics to patients with acute pancreatitis. However, there, is very little evidence to support this practice., A recent Cochrane review highlights the potential benefits of administering Imipenem to, patients with established pancreatic necrosis in the hope of averting the progression to, infection., There are concerns that the administration of antibiotics in mild attacks of pancreatitis will not, affect outcome and may contribute to antibiotic resistance and increase the risks of antibiotic, associated diarrhoea., , Surgery, , , , , , Patients with acute pancreatitis due to gallstones should undergo early cholecystectomy., Patients with obstructed biliary system due to stones should undergo early ERCP., Patients with extensive necrosis where infection is suspected should usually undergo FNA, for culture., Patients with infected necrosis should undergo either radiological drainage or surgical, necrosectomy. The choice of procedure depends upon local expertise., , References, www.bsg.org.uk/pdfworddocs/pancreatic.pdf
Page 3593 :
A 43 year old lady presents with an attack of acute pancreatitis. It is classified as a mild attack on, severity scoring. Imaging identifies gallstones but a normal calibre bile duct, and a peripancreatic, fluid collection. Which of the following management options is most appropriate?, , Intravenous octreotide, , Cholecystectomy within 4 weeks, , Nasogastric tube drainage of the stomach, , Insertion of a radiological drain, , Avoidance of enteral feeding, , Patients with gallstone pancreatitis should undergo early cholecystectomy., Enteral feeding helps minimise gut bacterial translocation and should be given to most patients with, pancreatitis. Many studies have evaluated the role of octreotide in reducing pancreatic secretions, and shown no benefit (Uhl W et al Gut 1999 45:97-104, McKay C et al. Int J Pancreatol 1997; 21:, 13-19)., The use of antibiotics in pancreatitis is controversial. However, a recent Cochrane review has, presented reasonable evidence in favor of administration of imipenem to prevent infection in, established necrosis., Please rate this question:, , Discuss and give feedback, , Next question, , Management of Pancreatitis, Management of Acute Pancreatitis in the UK, Diagnosis
Page 3594 :
, , , , , Traditionally hyperamylasaemia has been utilised with amylase being elevated three times, the normal range., However, amylase may give both false positive and negative results., Serum lipase is both more sensitive and specific than serum amylase. It also has a longer, half life., Serum amylase levels do not correlate with disease severity., , Differential causes of hyperamylasaemia, , Acute pancreatitis, , Pancreatic pseudocyst, , Mesenteric infarct, , Perforated viscus, , Acute cholecystitis, , Diabetic ketoacidosis, , Assessment of severity, , , , , Glasgow, Ranson scoring systems and APACHE II, Biochemical scoring e.g. using CRP, , Features that may predict a severe attack within 48 hours of admission to hospital, , Initial assessment, , , , , , , Clinical impression of severity, Body mass index >30, Pleural effusion, APACHE score >8, , 24 hours after admission, , , , , , , Clinical impression of severity, APACHE II >8, Glasgow score of 3 or more, Persisting multiple organ failure
Page 3595 :
48 hours after admission, , , , CRP>150, , , , , , Glasgow Score of >3, CRP >150, Persisting or progressive organ failure, , Table adapted from UK guidelines for management of acute pancreatitis. GUT 2005, 54 suppl III, Management, Nutrition, , , , , , There is reasonable evidence to suggest that the use of enteral nutrition does not worsen the, outcome in pancreatitis, Most trials to date were underpowered to demonstrate a conclusive benefit., The rationale behind feeding is that it helps to prevent bacterial translocation from the gut,, thereby contributing to the development of infected pancreatic necrosis., , Use of antibiotic therapy, , , , , , Many UK surgeons administer antibiotics to patients with acute pancreatitis. However, there, is very little evidence to support this practice., A recent Cochrane review highlights the potential benefits of administering Imipenem to, patients with established pancreatic necrosis in the hope of averting the progression to, infection., There are concerns that the administration of antibiotics in mild attacks of pancreatitis will not, affect outcome and may contribute to antibiotic resistance and increase the risks of antibiotic, associated diarrhoea., , Surgery, , , , , , , Patients with acute pancreatitis due to gallstones should undergo early cholecystectomy., Patients with obstructed biliary system due to stones should undergo early ERCP., Patients with extensive necrosis where infection is suspected should usually undergo FNA, for culture., Patients with infected necrosis should undergo either radiological drainage or surgical, necrosectomy. The choice of procedure depends upon local expertise., , References, www.bsg.org.uk/pdfworddocs/pancreatic.pdf
Page 3597 :
A 43 year old lady with repeated episodes of abdominal pain is admitted with small bowel, obstruction. A laparotomy is performed and at surgery a gallstone ileus is identified. What is the, most appropriate course of action?, , Remove the gallstone via a proximally sited terminal ileal enterotomy and decompress the small, bowel. Leave the gallbladder in situ., , Remove the gallstone via a proximally sited terminal ileal enterotomy and decompress the small, bowel. Remove the gallbladder., , Remove the gallstone via a proximally sited terminal ileal enterotomy and decompress the small, bowel. Perform a choledochoduodenostomy., , Remove the gallstone from an enterotomy at the site of the obstruction and leave the, gallbladder in situ., , Remove the gallstone from an enterotomy at the site of the obstruction and remove the, gallbladder., , Gallstone ileus occurs as a result of the fistula developing between the gallbladder and the, duodenum. These tend to become impacted somewhat proximal to the ileocaecal valve and cause, small bowel obstruction. The correct management is to remove the gallstone from an enterotomy, proximal to the site of stone impaction. The bowel at the site of impaction itself may not heal well and, an enterotomy performed at this site may well result in the need for a resection. The standard, surgical teaching is that under almost all circumstances the gallbladder should be left in situ, as the, anatomy in this area is often hostile and unpredictable. Disconnecting it from the duodenum leaves a, large defect that is difficult to close., Please rate this question:, , Discuss and give feedback, , Next question, , Gallstones
Page 3598 :
Up to 24% of women and 12% of men may have gallstones. Of these up to 30% may develop local, infection and cholecystitis. In patients subjected to surgery 12% will have stones contained within the, common bile duct. The majority of gallstones are of a mixed composition (50%) with pure cholesterol, stones accounting for 20% of cases., The aetiology of CBD stones differs in the world, in the West most CBD stones are the result of, migration. In the East a far higher proportion arise in the CBD de novo., The classical symptoms are of colicky right upper quadrant pain that occurs post prandially. The, symptoms are usually worst following a fatty meal when cholecystokinin levels are highest and, gallbladder contraction is maximal., Investigation, In almost all suspected cases the standard diagnostic work up consists of abdominal ultrasound and, liver function tests. Of patients who have stones within the bile duct, 60% will have at least one, abnormal result on LFT's. Ultrasound is an important test, but is operator dependent and therefore, may occasionally need to be repeated if a negative result is at odds with the clinical picture. Where, stones are suspected in the bile duct, the options lie between magnetic resonance cholangiography, and intraoperative imaging. The choice between these two options is determined by the skills and, experience of the surgeon. The advantages of intra operative imaging are less useful in making, therapeutic decisions if the operator is unhappy about proceeding the bile duct exploration, and in, such circumstances pre operative MRCP is probably a better option., Specific gallstone and gallbladder related disease, , Disease, , Features, , Management, , Biliary colic, , Colicky abdominal pain, worse, post prandially, worse after fatty, foods, , If imaging shows gallstones and history compatible, then laparoscopic cholecystectomy, , Acute, cholecystitis, , , , , , , Gallbladder, abscess, , , , , , , Right upper quadrant pain, Fever, Murphys sign on, examination, Occasionally mildly, deranged LFT's (especially, if Mirizzi syndrome), , Imaging (USS) and cholecystectomy (ideally within, 48 hours of presentation) (2), , Usually prodromal illness, and right upper quadrant, pain, Swinging pyrexia, Patient may be, systemically unwell, , Imaging with USS +/- CT Scanning, Ideally surgery, sub total cholecystectomy may be, needed if Calots triangle is hostile, In unfit patients percutaneous drainage may be
Page 3599 :
Disease, , Cholangitis, , Features, , Management, , , , Generalised peritonism, not present, , considered, , , , Patient severely septic, and unwell, Jaundice, Right upper quadrant pain, , Fluid resuscitation, , , , , Broad spectrum intravenous antibiotics, Correct any coagulopathy, Early ERCP, , Gallstone, ileus, , , , , , Acalculous, cholecystitis, , , , , , , , Patients may have a, history of previous, cholecystitis and known, gallstones, Small bowel obstruction, (may be intermittent), , Laparotomy and removal of gallstone from small, bowel, the enterotomy must be made proximal to, the site of obstruction and not at the site of, obstruction. The fistula between the gallbladder and, duodenum should not be interfered with., , Patients with inter, current illness (e.g., diabetes, organ failure), Patient of systemically, unwell, Gallbladder inflammation, in absence of stones, High fever, , If patient fit then cholecystectomy, if unfit then, percutaneous cholecystostomy, , Treatment, Patients with asymptomatic gallstones rarely develop symptoms related to them (less than 2% per, year) and may therefore be managed expectantly. In almost all cases of symptomatic gallstones the, treatment of choice is cholecystectomy performed via the laparoscopic route. In the very frail patient, there is sometimes a role for selective use of ultrasound guided cholecystostomy., During the course of the procedure some surgeons will routinely perform either intra operative, cholangiography to either confirm anatomy or to exclude CBD stones. The latter may be more easily, achieved by use of laparoscopic ultrasound. If stones are found then the options lie between early, ERCP in the day or so following surgery or immediate surgical exploration of the bile duct. When, performed via the trans cystic route this adds little in the way of morbidity and certainly results in, faster recovery. Where transcystic exploration fails the alternative strategy is that of formal, choledochotomy. The exploration of a small duct is challenging and ducts of less than 8mm should, not be explored. Small stones that measure less than 5mm may be safely left and most will pass
Page 3600 :
spontaneously., Risks of ERCP(1), , , , , , , Bleeding 0.9% (rises to 1.5% if sphincterotomy performed), Duodenal perforation 0.4%, Cholangitis 1.1%, Pancreatitis 1.5%, , References, 1. Williams E et al. Guidelines on the management of common bile duct stones, (CBDS)Gut2008;57:10041021, 2. Gurusamy KS, Samraj K. Early versus delayed laparoscopic cholecystectomy for acute, cholecystitis. Cochrane Database Syst Rev. 2006 Oct 18;(4):CD005440., 3. Gurusamy K and Davidson B. Gallstones. BMJ 2014 (348):27-30., Next question
Page 3601 :
A 43 year old lady presents with jaundice and is diagnosed as having a carcinoma of the head of the, pancreas. Although she is deeply jaundiced, her staging investigations are negative for metastatic, disease. What is the best method of biliary decompression in this case?, , ERCP and placement of metallic stent, , ERCP alone, , ERCP and placement of plastic stent, , Cholecystostomy, , Choledochoduodenostomy, Metallic stents are contraindicated in resectable biliary disease, A plastic stent is the best option for biliary decompression in resectable disease. Surgical bypasses, have no place in the management of operable malignancy as a bridge to definitive surgery., Please rate this question:, , Discuss and give feedback, , Next question, , Pancreatic stents, Both benign and malignant biliary obstruction may be treated by placement of stents. These may be, either plastic tubes or self expanding metallic stents. They can be placed either percutaneously, at, ERCP, or, less commonly now, open surgery. Complications include blockage, displacement and, those related to the method of insertion., Metallic Vs Plastic stents, , Metallic stents, , Plastic stents, , Expensive, , Cheap, , Embed in surrounding tissues, , Do not usually embed
Page 3602 :
Displacement rare, , Displacement common, , Blockage rare, , Blockage common, , Contraindicated in resectable malignant disease, , May be used as a bridge to resectional surgery, Next question
Page 3603 :
Theme: Pancreatitis management, , A. Pancreatic necrosectomy, B. Staging laparotomy to assess severity, C. Endoscopic retrograde cholangiopancreatography, D. Emergency cystogastrostomy, E. Cholecystectomy within 4 weeks, F. Elective cystogastrostomy, G. Parenteral nutrition, , Please select the most appropriate next stage in management for the scenario given. Each option, may be used once, more than once or not at all., , 38., , A 34 year old women is admitted with cholangitis. Her bilirubin is 180 and alkaline phosphatase is, 348. She becomes progressively more unwell and develops abdominal pain. The houseman checks, her amylase which is elevated at 1080. Standard treatment is initiated and her Glasgow score is 3., You answered Pancreatic necrosectomy, The correct answer is Endoscopic retrograde cholangiopancreatography, She requires urgent decompression of her biliary system. An ERCP is the conventional method of, performing this. It is important to ensure that her coagulation status is normalised prior to, performing this procedure., , 39., , A 63 year old man is admitted to ITU with an attack of severe gallstone pancreatitis. He requires, ventillatory support for ARDS. Over the past few days he has become more unwell and a CT scan, is organised. This demonstrates an area of necrosis, culture from this area shows a gram negative, bacillus. His CRP is 400 and WCC 25.1., Pancreatic necrosectomy, This man requires necrosectomy as he has infected pancreatic necrosis and is haemodynamically
Page 3604 :
unstable. A radiological drainage procedure is unlikely to be sufficient., , 40., , A 53 year old alcoholic develops acute pancreatitis and is making slow but reasonable progress., He is troubled by persisting ileus and for this reason a CT scan is undertaken. This demonstrates a, large pancreatic pseudocyst. This is monitored by repeat CT scanning which shows no resolution, and he is now complaining of early satiety., You answered Pancreatic necrosectomy, The correct answer is Elective cystogastrostomy, Drainage of this man's pseudocyst is required. This could be accomplished radiologically or, endoscopically or surgically. As the other options are not on the list this is the best option from, those available., , Please rate this question:, , Discuss and give feedback, , Next question, , Management of Pancreatitis, Management of Acute Pancreatitis in the UK, Diagnosis, , , , , , , Traditionally hyperamylasaemia has been utilised with amylase being elevated three times, the normal range., However, amylase may give both false positive and negative results., Serum lipase is both more sensitive and specific than serum amylase. It also has a longer, half life., Serum amylase levels do not correlate with disease severity., , Differential causes of hyperamylasaemia
Page 3605 :
Acute pancreatitis, , Pancreatic pseudocyst, , Mesenteric infarct, , Perforated viscus, , Acute cholecystitis, , Diabetic ketoacidosis, , Assessment of severity, , , , , Glasgow, Ranson scoring systems and APACHE II, Biochemical scoring e.g. using CRP, , Features that may predict a severe attack within 48 hours of admission to hospital, , Initial assessment, , , , , , , Clinical impression of severity, Body mass index >30, Pleural effusion, APACHE score >8, , 24 hours after admission, , , , , , , , Clinical impression of severity, APACHE II >8, Glasgow score of 3 or more, Persisting multiple organ failure, CRP>150, , 48 hours after admission, , , , , , Glasgow Score of >3, CRP >150, Persisting or progressive organ failure
Page 3606 :
Table adapted from UK guidelines for management of acute pancreatitis. GUT 2005, 54 suppl III, Management, Nutrition, , , , , , There is reasonable evidence to suggest that the use of enteral nutrition does not worsen the, outcome in pancreatitis, Most trials to date were underpowered to demonstrate a conclusive benefit., The rationale behind feeding is that it helps to prevent bacterial translocation from the gut,, thereby contributing to the development of infected pancreatic necrosis., , Use of antibiotic therapy, , , , , , Many UK surgeons administer antibiotics to patients with acute pancreatitis. However, there, is very little evidence to support this practice., A recent Cochrane review highlights the potential benefits of administering Imipenem to, patients with established pancreatic necrosis in the hope of averting the progression to, infection., There are concerns that the administration of antibiotics in mild attacks of pancreatitis will not, affect outcome and may contribute to antibiotic resistance and increase the risks of antibiotic, associated diarrhoea., , Surgery, , , , , , , Patients with acute pancreatitis due to gallstones should undergo early cholecystectomy., Patients with obstructed biliary system due to stones should undergo early ERCP., Patients with extensive necrosis where infection is suspected should usually undergo FNA, for culture., Patients with infected necrosis should undergo either radiological drainage or surgical, necrosectomy. The choice of procedure depends upon local expertise., , References, www.bsg.org.uk/pdfworddocs/pancreatic.pdf, Antibiotic therapy for prophylaxis against infection of pancreatic necrosis in acute, pancreatitis. Villatoro et al. Cochrane Library DOI: 10.1002/14651858.CD002941.pub3. 2010, version., Next question
Page 3607 :
What proportion of patients presenting for cholecystectomy for treatment of biliary colic due to, gallstones will have stones in the common bile duct?, , 10%, , 30%, , 2%, , 50%, , 25%, , Up to 10% of all patients may have stones in the CBD. Therefore, all patients should have their liver, function tests checked prior to embarking on a cholecystectomy., Please rate this question:, , Discuss and give feedback, , Biliary disease, Diagnosis, , Typical features, , Pathogenesis, , Gallstones, , Typically history of, biliary colic or, episodes of, chlolecystitis., Obstructive type, history and test results., , Usually small calibre gallstones which can, pass through the cystic duct. In Mirizzi, syndrome the stone may compress the bile, duct directly- one of the rare times that, cholecystitis may present with jaundice, , Cholangitis, , Usually obstructive, and will have Charcot's, triad of symptoms, (pain, fever, jaundice), , Ascending infection of the bile ducts usually, by E. coliand by definition occurring in a pool, of stagnant bile.
Page 3608 :
Pancreatic cancer, , Typically painless, jaundice with palpable, gallbladder, (Courvoisier's Law), , Direct occlusion of distal bile duct or, pancreatic duct by tumour. Sometimes nodal, disease at the portal hepatis may be the culprit, in which case the bile duct may be of normal, calibre., , TPN (total parenteral, nutrition) associated, jaundice, , Usually follows long, term use and is usually, painless with non, obstructive features, , Often due to hepatic dysfunction and fatty, liver which may occur with long term TPN, usage., , Bile duct injury, , Depending upon the, type of injury may be, of sudden or gradual, onset and is usually of, obstructive type, , Often due to a difficult laparoscopic•, cholecystectomy when anatomy in Calots, triangle is not appreciated. In the worst, scenario the bile duct is excised and jaundice, develops rapidly post operatively. More, insidious is that of bile duct stenosis which, may be caused by clips or diathermy injury., , Cholangiocarcinoma, , Gradual onset, obstructive pattern, , Direct occlusion by disease and also extrinsic, compression by nodal disease at the porta, hepatis., , Septic surgical patient, , Usually hepatic, features, , Combination of impaired biliary excretion and, drugs such as ciprofloxacin which may cause, cholestasis., , Metastatic disease, , Mixed hepatic and post, hepatic, , Combination of liver synthetic failure (late), and extrinsic compression by nodal disease, and anatomical compression of intra hepatic, structures (earlier), , A gallbladder may develop a thickened wall in chronic cholecystitis, microscopically RoikitanskyAschoff Sinuses may be seen
Page 3609 :
Image sourced from Wikipedia
Page 3611 :
Theme: Consent, , A., B., C., D., E., F., , Consent the patient, Consent the parents, Proceed without consent, Refer the matter to a court, Do not proceed with treatment, Consent by proxy, , For each of the scenarios given please select the most appropriate course of action. Each option, may be used once, more than once or not at all., , 1., , A 6 year old is hit by a car and is brought to the emergency department. He is, haemodynamically unstable with bilateral femoral shaft fractures and concerns that he may, have a ruptured spleen. The parents have refused blood transfusions on religious grounds., You answered Consent the patient, The correct answer is Proceed without consent, In the UK the GMC and common law advises that emergency life saving treatment can be, given to a child irrespective of the parents views. There is clearly insufficient time here to, apply to a court., , 2., , A 63 year old lady with advanced motor neurone disease is developing progressive feeding, difficulties. Her daughter and the team treating her would like a PEG inserted. However, the, patients partner produces an advanced directive which the patient had signed 15 years, previously and registered with their solicitor at the time the couple wrote their wills. In it, she states she would not wish such treatment., You answered Consent the patient, The correct answer is Do not proceed with treatment, A properly completed and registered advanced medical directive signed by a mentally, competent adult is legally binding and cannot be overridden., , 3., , A 15 year old girl presents with right iliac fossa pain. She becomes progressively, tachycardic and a ruptured ectopic pregnancy is suspected. She is deemed to be mentally, competent and will agree to surgery, but not if her parents are informed., Consent the patient
Page 3612 :
Since she is likely to be Gillick competent she can consent for herself., Please rate this question:, , Discuss and give feedback, , Next question, , Consent, There are 3 types of consent:, 1. Informed, 2. Expressed, 3. Implied, Consent forms used in UK NHS, , Consent, Form 1, , For competent adults who are able to consent for themselves where, consciousness may be impaired (e.g. GA), , Consent, Form 2, , For an adult consenting on behalf of a child where consciousness is impaired, , Consent, Form 3, , For an adult or child where consciousness is not impaired, , Consent, Form 4, , For adults who lack capacity to provide informed consent, , Capacity, Key points include:, 1. Understand and retain information, 2. Patient believes the information to be true, 3. Patient is able to weigh the information to make a decision, All patients must be assumed to have capacity, Consent in minors, Young children and older children who are not Gillick competent cannot consent for themselves. In, British law the patients biological mother can always provide consent. The child's father can consent, if the parents are married (and the father is the biological father), or if the father is named on the, birth certificate (irrespective of marital status). If parents are not married and the father is not named, on the birth certificate then the father cannot consent., Next question
Page 3613 :
What is the reciprocal of absolute risk reduction?, , Odds ratio, , Number needed to treat, , False positive, , False negative, , None of the above, , Similar theme to September 2011 Exam, In epidemiology, the absolute risk reduction, or risk difference is the decrease in risk of a given, activity or treatment in relation to a control activity or treatment. It is the inverse of the number, needed to treat., Please rate this question:, , Discuss and give feedback, , Next question, , Absolute risk reduction, The absolute risk reduction is the decrease in risk of a given activity or treatment in relation to a, control activity or treatment. It is the inverse of the number needed to treat., The absolute risk reduction is usually calculated for two different treatments. For example, consider, surgical resection (X) versus watchful waiting (Y) for prostate cancer. A defined end point, such as 5, year survival is required. If the probabilities pX and pY of this end point are known then the absolute, risk reduction is calculated (pX-pY)., The inverse of absolute risk reduction is the Number Needed to Treat . This is useful in determining, the cost Vs benefit of many treatments., Number needed to treat, Definition: how many patients would need to receive a treatment to prevent one event. It is the, absolute difference between two treatments., Next question
Page 3614 :
You have been asked to investigate the potential benefit of setting up a service to help patients with, stomas in the local area. What is the most important factor when determining how many resources, will be required?, , Incidence, , Bayesian factor, , Prevalence, , Denominator data, , P value, , Please rate this question:, , Discuss and give feedback, , Next question, , Incidence and prevalence, These two terms are used to describe the frequency of a condition in a population., The incidence is the number of new cases per population in a given time period., For example, if condition X has caused 40 new cases over the past 12 months per 1,000 of the, population the annual incidence is 0.04 or 4%., The prevalence is the total number of cases per population at a particular point in time., For example, imagine a questionnaire is sent to 2,500 adults asking them how much they weigh. If, from this sample population, 500 of the adults were obese then the prevalence of obesity would be, 0.2 or 20%.
Page 3615 :
Relationship, , , , , , prevalence = incidence * duration of condition, in chronic diseases the prevalence is much greater than the incidence, in acute diseases the prevalence and incidence are similar. For conditions such as the, common cold the incidence may be greater than the prevalence, Next question
Page 3616 :
In medical statistics, which of the following does a p value of 0.04 represent?, , Risk of type 1 Error, , Risk of type 2 Error, , Size of power of the study, , Sample size, , Number of degrees of freedom, , P values are related to the significance levels of a statistical test and therefore are in effect, measuring the risk of a type 1 error., Please rate this question:, , Discuss and give feedback, , Next question, , Statistical error, Type 1 Error, , , , , , Test rejects true null hypothesis, Rate of type 1 error is the given the value of α, It usually equals the significance level of a test, , Type 2 Error, , , , , , Test fails to reject a false null hypothesis, Rate of type 2 errors is given the value of β, It is related to the power of the test, Next question
Page 3617 :
Which of the following statements relating to quantitative data is false?, , Discrete data cannot be sub divided, , The median is less susceptible to extreme outliers than the mean, , The mean is susceptible to extreme outliers, , Data that fits the standard distribution perfectly will have a mode that is half the value of the, mean, , Values obtained have a numerical scale, , Data that fits the standard distribution perfectly will have a mean, median and mode that are all the, same value., Please rate this question:, , Discuss and give feedback, , Next question, , Qualitative and quantitative data, Qualitative and quantitative data, Qualitative (categorical) data refers to different descriptions of a characteristic, although it may be, possible to allocate a number it has no scale., Quantitative data is associated with numerical values on a numerical scale., Since quantitative data is based on a numerical scale it can be organised to create a distribution, curve. The central tendency may be estimated using the mode, median and mean. The standard, deviation gives an estimation of the spread of data., , Next question
Page 3618 :
A surgical team wish to conduct a meta analysis of randomised controlled trials of the use of low, molecular weight heparins in the prevention of post operative deep vein thrombosis. How would, these results be best displayed graphically?, , Forest plot, , Box Whisker plot, , Violin plot, , Kaplan Meier graph, , None of the above, , Data from multiple RCT's are best displayed using Forest plots. Funnel plots may be used to, determine the effect of small studies and their overall effect on the data. Violin plots and Box, Whisker plots are often used to graphically display non parametric data from single studies and are, not generally used to display data from meta analyses., Please rate this question:, , Discuss and give feedback, , Next question, , Forest plots, A Forest plot is a graphical display designed to illustrate the relative strength of treatment effects in, multiple quantitative scientific studies, addressing the same question. It is often used to graphically, display meta analyses of randomised controlled trials., The graph may be plotted on a natural logarithmic scale when using odds ratios or other ratio-based, effect measures, so that the confidence intervals are symmetrical about the means from each study, and to ensure undue emphasis is not given to odds ratios greater than 1 when compared to those, less than 1. The area of each square is proportional to the study's weight in the meta-analysis. The
Page 3619 :
overall meta-analysed measure of effect is often represented on the plot as a vertical line. This, meta-analysed measure of effect is commonly plotted as a diamond, the lateral points of which, indicate confidence intervals for this estimate., A vertical line representing no effect is also plotted. If the confidence intervals for individual studies, overlap with this line, it demonstrates that at the given level of confidence their effect sizes do not, differ from no effect for the individual study. The same applies for the meta-analysed measure of, effect: if the points of the diamond overlap the line of no effect the overall meta-analysed result, cannot be said to differ from no effect at the given level of confidence., Next question
Page 3620 :
A rapid finger-prick blood test to help diagnosis deep vein thrombosis is developed. Comparing the, test to current standard techniques a study is done on 1,000 patients:, , DVT present, , DVT absent, , New test positive, , 200, , 100, , New test negative, , 20, , 680, , What is the specificity of the new test?, , 680/880, , 200/220, , 680/780, , 680/700, , 200/300, , Specificity = true negatives / (true negatives + false positives), = 680 / (680 + 100), Please rate this question:, , Discuss and give feedback, , Next question
Page 3621 :
Screening test statistics, It would be unusual for a medical exam not to feature a question based around screening test, statistics. The available data should be used to construct a contingency table as below:, TP = true positive; FP = false positive; TN = true negative; FN = false negative, , Disease present, , Disease absent, , Test positive, , TP, , FP, , Test negative, , FN, , TN, , The table below lists the main statistical terms used in relation to screening tests:, , Sensitivity, , TP / (TP + FN ), , Proportion of patients with the condition who have a, positive test result, , Specificity, , TN / (TN + FP), , Proportion of patients without the condition who, have a negative test result, , Positive predictive value, , TP / (TP + FP), , The chance that the patient has the condition if the, diagnostic test is positive, , Negative predictive value, , TN / (TN + FN), , The chance that the patient does not have the, condition if the diagnostic test is negative, , Likelihood ratio for a, positive test result, , sensitivity / (1 specificity), , How much the odds of the disease increase when a, test is positive, , Likelihood ratio for a, negative test result, , (1 - sensitivity) /, specificity, , How much the odds of the disease decrease when a, test is negative
Page 3622 :
Positive and negative predictive values are prevalence dependent. Likelihood ratios are not, prevalence dependent, Next question
Page 3623 :
Theme: Statistics, , A. LSD post hoc test, B. Bonferroni test, C. Mann Whitney U test, D. Paired T test, E. Chi squared test, F. Fishers exact test, G. Unpaired T Test, , Please select the statistical test that is most appropriate for the scenario provided. Each option may, be used once, more than once or not at all., , 10., , A surgeon has conducted a piece of research and is try to make his data appear interesting for, publication. To do this he is conducting multiple analyses of sub group data using multiple tests., You answered LSD post hoc test, The correct answer is Bonferroni test, This is a process referred to as "data dredging" and can lead to erroneous results. Post hoc testing, in general can be a problem in research and to try and minimise the potential for error some, advocate the use of the Bonferroni method. This adjusts the test to take account of the number, of tests that have been performed on the data., , 11., , A surgical unit are conducting a study to determine whether patients who have bowel, preparation have a lower risk of colonic anastomotic leakage than those having none. The, planned sample size is 25., You answered LSD post hoc test, The correct answer is Fishers exact test
Page 3624 :
It is likely to be underpowered with the number provided. However, it would be possible to, classify such data into a 2x2 contingency table. However, when the sample size is small the Chi, squared test is not suitable and in these situations the Fishers exact test is used., , 12., , A surgeon wishes to conduct a national study relating patient weight to the length of inpatient, stay following all major operations., You answered LSD post hoc test, The correct answer is Unpaired T Test, Weight is likely to be normally distributed and when a large size is used it is possible that this will, be suitable for testing using a parametric method. The T Test is a powerful test providing it is used, correctly and would probably be best suited for analysis of this data set., , Please rate this question:, , Discuss and give feedback, , Next question, , Statistics, Statistics is a topic that generally strikes fear and dread into most surgeons hearts. The MRCS is not, an examination designed to test mathematical skill but the examiners do expect you to have working, knowledge of commonly used tests so that you can appraise the literature properly., Data types, Before selecting a method of statistical analysis it is imperative that the type of data to be analysed, is correctly categorised. Commonly used terms include nominal, ordinal, interval and continuous., , Term, , Interpretation, , Nominal, , Data can be allocated a numerical code that is arbitrary. For example allocating people as
Page 3625 :
Term, , Interpretation, , alive or dead using codes of 0 or 1, , Ordinal data, , Data using numbers that can be used on a scale. Severity of pain is often measured in this, way, , Interval, scale, , Data is measured numerically. However, the zero point is arbitrary, , Continuous, , Data is measured numerically where the numerical value is a real number and may be any, value. Examples include height and weight, , Analysing data, Having ascribed the data it is then possible to begin the process of analysis. Nominal data is often, tabulated into categories because of the nature of the underlying data sets. Continuous data may be, displayed graphically often as individual data points. When the sample size is large enough,, continuous data can be analysed to determine the distribution of the data points. Often, but not, always these will be in the form of a gaussian distribution. Determining whether data is normally, distributed or not is key to making sense of the subsequent statistical tests. Parametric tests are, used to test normally distributed data, the T Test is one of the best examples. Data which is not, normally distributed cannot be analysed in this way and a non parametric test must be used., Examples of such tests include Chi Squared and Mann Whitney U tests. Chi squared tests often, appear in the medical literature. There are some assumptions that are made in relation to Chi, squared tests; these include the need to use 2 degrees of freedom (usually) and the minimum, sample size. Where the sample size is small then a different test is appropriate and the Fishers, exact test is often used., In situations where data is normally distributed and paired samples are taken from the same, individuals (such as following an intervention) then the paired T Test may be used., Multiple testing and post hoc analysis, In the ideal world statistical analysis is conducted on data that is collected prospectively according to, pre set power calculations and defined end points. Occasionally, data does not produce an expected, outcome or a certain type of patient appears to have a different result. Subsequent analysis of such, groups is termed a post hoc analysis. This can be perfectly legitimate, alternatively it can represent, the last ditch attempt of a researcher to try and find any aspect of the data that is worthwhile. This, can lead to errors and false rejection of a null hypothesis. A statistically significant result is more, likely to occur if the same dataset is subjected to multiple analyses. To counteract this problem some, researchers will apply a Bonferroni correction, this adjusts the analysis to allow for multiple testing.
Page 3626 :
A new test to screen for pulmonary embolism (PE) is used in 100 patients who present to the, Emergency Department. The test is positive in 30 of the 40 patients who are proven to have a PE., Of the remaining 60 patients, only 5 have a positive test. What is the sensitivity of the new test?, , 8.33%, , 30%, , 40%, , 66.66%, , 75%, , A contingency table can be constructed from the above data, as shown below:, {PE diagnosed}{No PE} {Test positive}305 {Test negative}1055, The sensitivity is therefore 30 / (30 + 10) = 75%, Please rate this question:, , Discuss and give feedback, , Next question, , Screening test statistics, It would be unusual for a medical exam not to feature a question based around screening test, statistics. The available data should be used to construct a contingency table as below:, TP = true positive; FP = false positive; TN = true negative; FN = false negative
Page 3627 :
Disease present, , Disease absent, , Test positive, , TP, , FP, , Test negative, , FN, , TN, , The table below lists the main statistical terms used in relation to screening tests:, , Sensitivity, , TP / (TP + FN ), , Proportion of patients with the condition who have a, positive test result, , Specificity, , TN / (TN + FP), , Proportion of patients without the condition who, have a negative test result, , Positive predictive value, , TP / (TP + FP), , The chance that the patient has the condition if the, diagnostic test is positive, , Negative predictive value, , TN / (TN + FN), , The chance that the patient does not have the, condition if the diagnostic test is negative, , Likelihood ratio for a, positive test result, , sensitivity / (1 specificity), , How much the odds of the disease increase when a, test is positive, , Likelihood ratio for a, negative test result, , (1 - sensitivity) /, specificity, , How much the odds of the disease decrease when a, test is negative, , Positive and negative predictive values are prevalence dependent. Likelihood ratios are not, prevalence dependent, Next question
Page 3628 :
Theme: Consent processes, , A. Consent form 1 (competent adult), B. Consent form 2 (procedure on a child), C. Consent form 3 (procedure on a child or adult where conciousness not, impaired), D. Consent form 4 (Undertaking procedure where patient lacks capacity), E. Verbal consent will suffice, F. Research consent form, , Please select the most appropriate consent modality for the procedure described. Each option may, be used once, more than once or not at all, , 14., , A 65 year old patient has a wound which is discharging following a laparotomy. The wound is, closed with clips and underlying this is a small superficial collection measuring 2 x 3cm., You answered Consent form 1 (competent adult), The correct answer is Verbal consent will suffice, This is done on the ward and is a straightforward procedure. Written consent is not required., , 15., , An 18 year old male has appendicitis and requires an appendicectomy., Consent form 1 (competent adult), The patient is 18 so technically an adult where consent is concerned., , 16., , An 85 year old lady with severe vascular dementia is admitted from a nursing home with a, displaced femoral neck fracture and it is proposed to undertake a hemi arthroplasty., You answered Consent form 1 (competent adult)
Page 3629 :
The correct answer is Consent form 4 (Undertaking procedure where patient lacks capacity), Where an individual lacks capacity it is necessary to act in the patients best interest. In the case of, a femoral neck fracture this can be managed using form 4. Where treatment is more controversial, and less immediately required an IMCA can be considered (under UK law)., , Please rate this question:, , Discuss and give feedback, , Next question, , Consent, There are 3 types of consent:, 1. Informed, 2. Expressed, 3. Implied, Consent forms used in UK NHS, , Consent Form, 1, , For competent adults who are able to consent for themselves where consciousness may, be impaired (e.g. GA), , Consent Form, 2, , For an adult consenting on behalf of a child where consciousness is impaired, , Consent Form, 3, , For an adult or child where consciousness is not impaired, , Consent Form, 4, , For adults who lack capacity to provide informed consent
Page 3630 :
Capacity, Key points include:, 1. Understand and retain information, 2. Patient believes the information to be true, 3. Patient is able to weigh the information to make a decision, All patients must be assumed to have capacity, Consent in minors, Young children and older children who are not Gillick competent cannot consent for themselves. In, British law the patients biological mother can always provide consent. The child's father can consent, if the parents are married (and the father is the biological father), or if the father is named on the, birth certificate (irrespective of marital status). If parents are not married and the father is not named, on the birth certificate then the father cannot consent., Next question
Page 3631 :
Which one of the following statements best describes a type II statistical error?, , The p value fails to reach statistical significance, , The alternative hypothesis is rejected when it is false, , The null hypothesis is rejected when it is true, , The null hypothesis is accepted when it is false, , None of the above, , Please rate this question:, , Discuss and give feedback, , Next question, , Significance tests, A null hypothesis (H0) states that two treatments are equally effective (and is hence negatively, phrased). A significance test uses the sample data to assess how likely the null hypothesis is to be, correct., For example:, , , 'there is no difference in the prevalence of colorectal cancer in patients taking low-dose, aspirin compared to those who are not', , The alternative hypothesis (H1) is the opposite of the null hypothesis, i.e. There is a difference, between the two treatments, The p value is the probability of obtaining a result by chance at least as extreme as the one that was, actually observed, assuming that the null hypothesis is true. It is therefore equal to the chance of, making a type I error (see below)., Two types of errors may occur when testing the null hypothesis, , , type I: the null hypothesis is rejected when it is true - i.e. Showing a difference between two, groups when it doesn't exist, a false positive. This is determined against a preset significance
Page 3632 :
, , level (termed alpha). As the significance level is determined in advance the chance of, making a type I error is not affected by sample size. It is however increased if the number of, end-points are increased. For example if a study has 20 end-points it is likely one of these, will be reached, just by chance., type II: the null hypothesis is accepted when it is false - i.e. Failing to spot a difference when, one really exists, a false negative. The probability of making a type II error is termed beta. It, is determined by both sample size and alpha, , Study accepts H0, , Type 1 error (alpha), , Reality H0, , Reality H1, , Study rejects H0, , Type 2 error (beta), , Power (1 - beta), , The power of a study is the probability of (correctly) rejecting the null hypothesis when it is false, , , , power = 1 - the probability of a type II error, power can be increased by increasing the sample size, Next question
Page 3633 :
As part of a research project you are trying to ascertain whether the use of dummies in infants is, linked to sudden infant death syndrome. What is the most appropriate form of study design?, , Randomised controlled trial, , Cross-over trial, , Cross-sectional survey, , Case-control study, , Cohort study, , As sudden infant death syndrome is relatively rare a case-control design is more appropriate than a, cohort study., Please rate this question:, , Discuss and give feedback, , Next question, , Study design, The following table highlights the main features of the main types of study:, , Randomised, controlled trial, , Participants randomly allocated to intervention or control group (e.g. standard, treatment or placebo), Practical or ethical problems may limit use
Page 3634 :
Cohort study, , Observational and prospective. Two (or more) are selected according to their, exposure to a particular agent (e.g. medicine, toxin) and followed up to see how, many develop a disease or other outcome., The usual outcome measure is the relative risk., Examples include Framingham Heart Study, , Case-control, study, , Observational and retrospective. Patients with a particular condition (cases) are, identified and matched with controls. Data is then collected on past exposure to a, possible causal agent for the condition., The usual outcome measure is the odds ratio., Inexpensive, produce quick results, Useful for studying rare conditions, Prone to confounding, , Cross-sectional, survey, , Provide a 'snapshot', sometimes called prevalence studies, Provide weak evidence of cause and effect, Next question
Page 3635 :
Which of the following has the greatest impact on the positive predictive value of a test?, , Prevalence, , Subjects who are true negatives, , Specificity, , Relative risk, , None of the above, , The positive predictive value (PPV) is the probability that an individual with a positive screening, result has the disease. The sensitivity is the probability that an individual with the disease is, screened positive and the specificity is the probability that an individual without the disease is, screened negative., Its value depends upon the prevalence of the condition being tested for and the sensitivity of the test, used., It may be calculated by dividing the number of true positives by the number of true positives and the, number of false positives., Please rate this question:, , Discuss and give feedback, , Next question, , Positive predictive values, Screening tests, , , , , , Sensitivity: proportion of true positives identified by a test, Specificity: proportion of true negatives correctly identified by a test, Positive predictive value: proportion of those who have a positive test who actually have the, disease, Negative predictive value: proportion of those who test negative who do not have the disease, , Predictive values are dependent on the prevalence, , , , Likelihood ratio for a positive test result = sensitivity/(1-specificity)
Page 3636 :
, , Likelihood ratio for a negative test result = (1-sensitivity)/specificity, , Likelihood ratios are not prevalence dependent, Next question
Page 3637 :
Considering cluster randomised trials, which of the following statements is false?, , They consider interventions targeted at groups, , They require increased recruitment to achieve the same level of statistical power as, individual trials, If results are analysed on an individual basis a lower P value may be obtained, , They are less prone to unit of analyses errors than trials involving individual observations, , The statistical analyses for these trials is more complex than that required for trials based, on individuals, , Cluster randomised trials are more prone to unit of analyses errors than individual based trials., Clustering needs to be considered in trial design and data analysis. One of the commonest errors is, where a study is a cluster study but researchers have failed to recognise this fact. This will then, result in the incorrect analysis being pursued. A lower P value will then result and a false positive, error will occur., Please rate this question:, , Discuss and give feedback, , Next question, , Cluster randomised controlled trials, , , , , , , Groups are randomised rather than individuals, Avoids cross contamination amongst participants, Participants in any one cluster are more likely to respond in a similar fashion, Higher risk of unit of analysis error as these studies should be analysed as clusters rather, than on an individual basis. This leads to a higher false positive rate., It is possible to adjust for clustering in statistical analyses, Next question
Page 3638 :
Theme: Timing of surgery, , A., B., C., D., E., F., G., , Immediate surgery, Surgery within 2 hours, Surgery within 6 hours, Surgery within 24 hours, Surgery within same hospital admission, Urgent elective surgery within 4 weeks, True elective surgery, , For each procedure please select the most appropriate time interval for surgery. Each option may be, selected once, more than once or not at all., , 21., , A 43 year old women is admitted with acute cholecystitis, her USS confirms the diagnosis, and LFT's are normal. It is now 10 hours since admission., You answered Immediate surgery, The correct answer is Surgery within 24 hours, Ideal case for acute cholecystectomy. This will enable prompt discharge and facilitate, recovery. Whilst expedient surgery is desirable an emergency procedure is not justified., , 22., , A 5 year old boy is admitted with a suspected acute appendicitis. He has tenderness but no, guarding as yet. He requires appendicectomy., You answered Surgery within 2 hours, The correct answer is Surgery within 6 hours, The kind of case that can wait till the following day if presenting out of hours., Appendicectomy may be deferred where peritoneal signs are absent. Where tenderness and, guarding are present a more urgent approach is warranted., , 23., , A 72 year old man is admitted with large bowel obstruction. He has been vomiting for 24, hours and his caecum is tender and measures 11cm., You answered Surgery within 2 hours, The correct answer is Surgery within 6 hours, The sun should not rise and set on unrelieved large bowel obstruction! This patient has a, competent ileocaecal valve. As a result lack of surgery would result in caecal perforation
Page 3639 :
leading to faecal peritonitis with and associated high mortality rate., Please rate this question:, , Discuss and give feedback, , Next question, , Preparation for surgery, Elective and emergency patients require different preparation., Elective cases, , , , , , , , Consider pre admission clinic to address medical issues., Blood tests including FBC, U+E, LFT's, Clotting, Group and Save, Urine analysis, Pregnancy test, Sickle cell test, ECG/ Chest x-ray, , Exact tests to be performed will depend upon the proposed procedure and patient fitness., Risk factors for development of deep vein thrombosis should be assessed and a plan for, thromboprophylaxis formulated., Diabetes, Diabetic patients have greater risk of complications., Poorly controlled diabetes carries high risk of wound infections., Patients with diet or tablet controlled diabetes may be managed using a policy of omitting medication, and checking blood glucose levels regularly. Diabetics who are poorly controlled or who take insulin, will require a intravenous sliding scale. Potassium supplementation should also be given., Diabetic cases should be operated on first., Emergency cases, Stabilise and resuscitate where needed., Consider whether antibiotics are needed and when and how they should be administered., Inform blood bank if major procedures planned particularly where coagulopathies are present at the, outset or anticipated (e.g. Ruptured AAA repair), Don't forget to consent and inform relatives., Special preparation, Some procedures require special preparation:, , , , , Thyroid surgery; vocal cord check., Parathyroid surgery; consider methylene blue to identify gland., Sentinel node biopsy; radioactive marker/ patent blue dye.
Page 3640 :
, , , , , , Surgery involving the thoracic duct; consider administration of cream., Pheochromocytoma surgery; will need alpha and beta blockade., Surgery for carcinoid tumours; will need covering with octreotide., Colorectal cases; bowel preparation (especially left sided surgery), Thyrotoxicosis; lugols iodine/ medical therapy., , References, Management of adults with diabetes undergoing surgery and elective procedures. NHS Diabetes., April 2011., Next question
Page 3641 :
In a randomized study of chemotherapy drugs for bowel cancer, a group receiving treatment A had a, recurrence rate of 12.5% and a group receiving treatment B had a recurrence rate of 15%. Both, groups are matched for size and length of follow up. What is the number needed to treat to prevent a, recurrence?, , 2.5, , 25, , 4, , 40, , 5, , There is an absolute risk reduction of 15-12.5%= 2.5% for treatment A, Therefore the NNT = 1/0.025 = 40, Please rate this question:, , Discuss and give feedback, , Next question, , Absolute risk reduction, The absolute risk reduction is the decrease in risk of a given activity or treatment in relation to a, control activity or treatment. It is the inverse of the number needed to treat., The absolute risk reduction is usually calculated for two different treatments. For example, consider, surgical resection (X) versus watchful waiting (Y) for prostate cancer. A defined end point, such as 5, year survival is required. If the probabilities pX and pY of this end point are known then the absolute, risk reduction is calculated (pX-pY)., The inverse of absolute risk reduction is the Number Needed to Treat . This is useful in determining
Page 3642 :
the cost Vs benefit of many treatments., Number needed to treat, Definition: how many patients would need to receive a treatment to prevent one event. It is the, absolute difference between two treatments., Next question
Page 3643 :
A new blood test to screen patients for colorectal cancer is trialled on 500 patients. The test was, positive in 40 of the 50 patients shown to have colorectal cancer by colonscopy. It was also positive, in 20 patients who were shown not to have colorectal cancer. What is the positive predictive value of, the test?, , 0.8, , 0.66, , 0.33, , 0.1, , Cannot be calculated, , A contingency table can be constructed from the above data, as shown below:, , Colorectal cancer, , No colorectal cancer, , Test positive, , 40, , 20, , Test negative, , 10, , 430, , Positive predictive value = TP / (TP + FP) = 40 / (40 + 20) = 0.66, Please rate this question:, , Discuss and give feedback, , Next question
Page 3644 :
Screening test statistics, It would be unusual for a medical exam not to feature a question based around screening test, statistics. The available data should be used to construct a contingency table as below:, TP = true positive; FP = false positive; TN = true negative; FN = false negative, , Disease present, , Disease absent, , Test positive, , TP, , FP, , Test negative, , FN, , TN, , The table below lists the main statistical terms used in relation to screening tests:, , Sensitivity, , TP / (TP + FN ), , Proportion of patients with the condition who have a, positive test result, , Specificity, , TN / (TN + FP), , Proportion of patients without the condition who, have a negative test result, , Positive predictive value, , TP / (TP + FP), , The chance that the patient has the condition if the, diagnostic test is positive, , Negative predictive value, , TN / (TN + FN), , The chance that the patient does not have the, condition if the diagnostic test is negative, , Likelihood ratio for a, positive test result, , sensitivity / (1 specificity), , How much the odds of the disease increase when a, test is positive, , Likelihood ratio for a, negative test result, , (1 - sensitivity) /, specificity, , How much the odds of the disease decrease when a, test is negative
Page 3645 :
Positive and negative predictive values are prevalence dependent. Likelihood ratios are not, prevalence dependent, Next question
Page 3646 :
Which of the following statements relating to randomised controlled trials is false?, , Consist of a control group recruited during the same time interval as the treatment group., , Are not applicable to retrospectively analysed data even if captured on a prospectively created, database., , They require concealment of treatment throughout the duration of the study., , They require concealment of treatment until after randomisation., , They are less susceptible to researcher bias than non-randomised controlled trials., , An RCT does not have to include concealment although many medical trials may do so. Indeed in, the case of surgical research it may not be practicable or possible to include concealment in the, protocol. This does not mean that the trial is not an RCT, simply that it is not blinded., Please rate this question:, , Discuss and give feedback, , Next question, , Audit and Research, Clinical audit, Quality improvement process that seeks to improve patient care and outcomes through systematic, review of care against explicit criteria and the implementation of change. Aspects of the structure,, processes, and outcomes of care are selected and systematically evaluated against explicit criteria., Where indicated, changes are implemented at an individual, team, or service level and further, monitoring is used to confirm improvement in healthcare delivery. (NICE)., Research, Aims to derive new knowledge which is potentially generalisable or transferable., Next question
Page 3647 :
Which of the following most closely describes the risk of a type I statistical error?, , Power calculation, , P value, , Odds ratio, , Relative risk, , None of the above, , Type 1 errors occur when a test rejects a true null hypothesis and is therefore related to the, significance level of the test result. To explain consider the following arbitrary example., We hypothesise that bowel preparation vs no bowel preparation has no effect on anastomotic leak, rates following left hemicolectomy. If we compare the rates of anastomotic leak and perform a Chi, Squared test and obtained a P value of 0.95 we should conclude that we unable to reject the null, hypothesis. Should we choose to do so then we are at risk of committing a type 1 error. In reality the, knowledge that a type 1 error was committed is usually some time after the event. When other, studies have been performed that have shown an effect., Power calculations are related to type 2 errors., Please rate this question:, , Discuss and give feedback, , Next question, , Power calculations and statistical error, Statistical error, , Type 1, , A test rejects a true null hypothesis. Analogus to false positive. It usually equates to the
Page 3648 :
Error, , significance level assigned to a test., , Type 2, Error, , A test fails to reject a false null hypothesis. It is related to the power of a test., , Statistical power, The power of a test is the probability that the test will reject the null hypothesis when it is false, (thereby avoiding a type 2 error). Increasing the power of a test will reduce the probability of a type 2, error. Usually a value of 0.8 is selected., Next question
Page 3649 :
A cohort study is being designed to look at the relationship between smoking and breast cancer., What is the usual outcome measure in a cohort study?, , Odds ratio, , Experimental event rate, , Relative risk, , Absolute risk increase, , Numbers needed to harm, Cohort studies - relative risk, , Please rate this question:, , Discuss and give feedback, , Next question, , Study design, The following table highlights the main features of the main types of study:, , Randomised, controlled trial, , Participants randomly allocated to intervention or control group (e.g. standard, treatment or placebo), Practical or ethical problems may limit use
Page 3650 :
Cohort study, , Observational and prospective. Two (or more) are selected according to their, exposure to a particular agent (e.g. medicine, toxin) and followed up to see how, many develop a disease or other outcome., The usual outcome measure is the relative risk., Examples include Framingham Heart Study, , Case-control, study, , Observational and retrospective. Patients with a particular condition (cases) are, identified and matched with controls. Data is then collected on past exposure to a, possible causal agent for the condition., The usual outcome measure is the odds ratio., Inexpensive, produce quick results, Useful for studying rare conditions, Prone to confounding, , Cross-sectional, survey, , Provide a 'snapshot', sometimes called prevalence studies, Provide weak evidence of cause and effect, Next question
Page 3651 :
Which of the following statements relating to consenting patients for surgery is false?, , Consent should be taken by a person who has sufficient knowledge of the procedure, , All risks with a frequency of 1 in 500 or greater must be disclosed, , Patients who have received sedating pre medication may no longer be able to provide informed, consent, , Written consent is required for operative procedures performed under local anaesthesia, , Where a procedure (or part thereof) consists of research this should be recorded on a separate, research consent form, , Generally risks with an incidence of 1% or greater are disclosed. Exceptions to this are where a rarer, complication is particularly serious., Please rate this question:, , Discuss and give feedback, , Next question, , Consent, There are 3 types of consent:, 1. Informed, 2. Expressed, 3. Implied, Consent forms used in UK NHS, , Consent Form, , For competent adults who are able to consent for themselves where consciousness may
Page 3652 :
1, , be impaired (e.g. GA), , Consent Form, 2, , For an adult consenting on behalf of a child where consciousness is impaired, , Consent Form, 3, , For an adult or child where consciousness is not impaired, , Consent Form, 4, , For adults who lack capacity to provide informed consent, , Capacity, Key points include:, 1. Understand and retain information, 2. Patient believes the information to be true, 3. Patient is able to weigh the information to make a decision, All patients must be assumed to have capacity, Consent in minors, Young children and older children who are not Gillick competent cannot consent for themselves. In, British law the patients biological mother can always provide consent. The child's father can consent, if the parents are married (and the father is the biological father), or if the father is named on the, birth certificate (irrespective of marital status). If parents are not married and the father is not named, on the birth certificate then the father cannot consent., Next question
Page 3653 :
A group of surgeons conduct a meta analysis of randomised controlled trials comparing the use of, analgesic regimes following laparoscopic cholecystectomy. What level of evidence is provided by, such an analysis?, , V, , I, , II, , III, , IV, , Please rate this question:, , Discuss and give feedback, , Next question, , Study design: evidence and recommendations, Levels of evidence, , , , , , , I - evidence from meta-analysis of randomised controlled trials, II - evidence from at least one well designed controlled trial which is not randomised, III - evidence from correlation and comparative studies or use of historical controls, IV - evidence from case series, V - Expert opinion or founded on basic principles, , Knowledge of the sub groups of the levels of evidence are not routinely tested in MRCS Part A., Grading of recommendation, , , , , Grade A - based on evidence from at least one randomised controlled trial (i.e. Ia or Ib), Grade B - based on evidence from non-randomised controlled trials (i.e. IIa, IIb or III), Grade C - based on evidence from a panel of experts (i.e. IV), Next question
Page 3654 :
Theme: Audit, , A. Standards based audit, B. Departmental review, C. Systems based audit, D. Operational audit, E. Financial audit, F. Peer review, , Please select the most appropriate type of audit method for the situation described. Each option may, be used once, more than once or not at all., , 31., , A surgical department wishes to determine whether it is using types of prosthetic mesh material, for incisional hernia surgery in the most effective manner. Recently there have been cases of non, mesh usage and loss of material as a result of the implants being "out of date"., You answered Standards based audit, The correct answer is Systems based audit, Theme from April 2015 Exam, Theme from April 2013 Exam, This is primarily an issue of stock control. However, the system by which the materials are used, within the theatre will need evaluation. Because it is the usage and stock that are a problem,, rather than the sourcing the systems based audit will be more effective than an operational audit., , 32., , A group of surgeons wish to determine whether patients are receiving adequate deep vein, thrombosis prophylaxis following surgery., Standards based audit, This type of audit is widely undertaken in most trusts in the UK.
Page 3655 :
33., , Surgeons are becoming increasing concerned about the adverse results of Mrs X performing a, new an innovative operative procedure not widely practised elsewhere., You answered Standards based audit, The correct answer is Peer review, In the situation where a surgeon performs an unfamiliar procedure a peer review is often the best, way to evaluate the problem. This does not have to be externally based, but often is., , Please rate this question:, , Discuss and give feedback, , Next question, , Audit categories, Audits may be used in a variety of clinical settings. These range from standards based audits, which, will be familiar to most clinicians, through to systems based audits which focus more on the, processes within an organisation., Types of audit, , Financial audit, , A historically oriented, independent evaluation performed for the purpose of attesting, to the fairness, accuracy, and reliability of financial data, , Operational, audit, , A future-oriented, systematic, and independent evaluation of organizational activities., Financial data may be used, but the primary sources of evidence are the operational, policies and achievements related to organizational objectives. Internal controls and, efficiencies may be evaluated during this type of review., , Departmental, , A current period analysis of administrative functions, to evaluate the adequacy of, controls, safeguarding of assets, efficient use of resources, compliance with related
Page 3656 :
review, , laws, regulations and institutional policy and integrity of financial information., , Standards, based audit, , Comparison of care or passage of care against set and widely agreed standards or, outcomes., , Systems based, audit, , Evaluation of processes occurring within an institution., , Systems based audits are an integral part of the process of clinical governance., Next question
Page 3657 :
Theme: Statistics in surgery, , A. Mann Whitney U test, B. Analysis of variance, C. LSR post hoc test, D. Bonferroni test, E. Kruskall Wallis test, F. T Test, , Please select the most appropriate statistical test for the situation described. Each option may be, used once, more than once or not at all., , 34., , We wish to determine whether there are significantly more patients in a surgical unit presenting, with post appendicectomy wound complications than there were one year previously. Review of, the dataset suggests a normal distribution., You answered Mann Whitney U test, The correct answer is T Test, This will involve the comparison of absolute numbers of patients and therefore this can be, assessed using a T -Test. It does make the assumption that the data is normally distributed., However, the other tests would not be suitable., , 35., , We want to make multiple comparisons of different types of side effects of a new drug., You answered Mann Whitney U test, The correct answer is Bonferroni test, As more types of side effects are considered, it becomes more likely that the new drug will appear, to be less safe than existing drugs in terms of at least one side effect. Methods are available to, adjust the p value to reflect the multiple comparisons being made, the aim being to avoid, spurious results. A frequently applied correction is the Bonferroni Method in which the observed
Page 3658 :
p values are multiplied by the number of tests performed, any resulting p value which is greater, than 1 is set to 1 and any which remains at less than 0.05 can be considered significant at the 5%, level., , 36., , 5 surgeons in a colorectal unit wish to determine whether there is a significant difference in their, individual leak rates for anterior resection of the rectum., You answered Mann Whitney U test, The correct answer is Kruskall Wallis test, In this scenario the data is derived from 5 groups of surgeons. If the data were normally, distributed then an ANOVA could be considered. Since these assumptions cannot be met, or, satisfied by transforming the data then the Kruskall-Wallis test provides a non parametric, alternative. This is essentially an extension of the Wilcoxon Rank sum test and detects differences, in median values between each group. To compare more accurately differences between two, individual surgeons a Mann Whitney U test may be a more acceptable alternative., , Please rate this question:, , Discuss and give feedback, , Next question, , Qualitative and quantitative data, Qualitative and quantitative data, Qualitative (categorical) data refers to different descriptions of a characteristic, although it may be, possible to allocate a number it has no scale., Quantitative data is associated with numerical values on a numerical scale., Since quantitative data is based on a numerical scale it can be organised to create a distribution, curve. The central tendency may be estimated using the mode, median and mean. The standard, deviation gives an estimation of the spread of data., , Next question
Page 3659 :
Theme: Governance issues, , A. Clinical audit, B. Service evaluation, C. Refer to research ethics committee, D. Implement procedure with no further monitoring, E. Cease activity and refer individual to GMC, F. Cease activity and undertake full service evaluation, G. Obtain written consent from each participant, , For the following research/ audit scenarios please select the most appropriate governance modality., Each option may be used once, more than once or not at all., , 37., , A general surgical unit has become increasingly concerned about the behaviour of consultant, Slasher. Over the past 48 months he has persisted in performing neonatal tracheoesphageal, fistula repairs. Unfortunately he has resisted efforts to prevent him from undertaking these, unsupervised. 2 more babies die and the Chief Executive would like your guidance., You answered Clinical audit, The correct answer is Cease activity and refer individual to GMC, While most surgical and departmental problems can be handled in house is can be seen that this, approach has been tried and failed. Given the deaths there is no other option than E, , 38., , As the SpR in general surgery you wish to determine whether your breast cancer unit is complying, with the British Association of Surgical Oncology guidelines for management of high grade ductal, carcinoma in situ, Clinical audit, Where there are clear guidelines, an audit is the best measure.
Page 3660 :
39., , A surgeon wishes to undertake some laboratory research into the migratory behaviour patterns, of metastatic colorectal cancer cells. These will be harvested from patients who are undergoing, hepatic resection of metastatic colorectal cancer; apart from diseased tissue no other samples, will be taken., You answered Clinical audit, The correct answer is Refer to research ethics committee, Whenever patient tissue is taken for research it is necessary practice to gain ethics approval., Some units may have blanket policies in place for taking tissue for research to tissue banks but as, a general rule most people should seek ethics approval PRIOR to starting research., , Please rate this question:, , Discuss and give feedback, , Next question, , Audit and Research, Clinical audit, Quality improvement process that seeks to improve patient care and outcomes through systematic, review of care against explicit criteria and the implementation of change. Aspects of the structure,, processes, and outcomes of care are selected and systematically evaluated against explicit criteria., Where indicated, changes are implemented at an individual, team, or service level and further, monitoring is used to confirm improvement in healthcare delivery. (NICE)., Research, Aims to derive new knowledge which is potentially generalisable or transferable., Next question
Page 3661 :
Which one of the following is equivalent to the pre-test probability?, , Post test odds / (1 + post-test odds), , Pre-test odds x likelihood ratio, , The prevalence of a condition, , The incidence of a condition, , Post-test odds / likelihood ratio, , The prevalence is the proportion of a population that have the condition at a point in time whilst the, incidence is the rate at which new cases occur in a population during a specified time period., Please rate this question:, , Discuss and give feedback, , Next question, , Pre- and post- test odds and probability, Pre-test probability, The proportion of people with the target disorder in the population at risk at a specific time (point, prevalence) or time interval (period prevalence), For example, the prevalence of rheumatoid arthritis in the UK is 1%, Post-test probability, The proportion of patients with that particular test result who have the target disorder, Post-test probability = post test odds / (1 + post-test odds), Pre-test odds
Page 3662 :
The odds that the patient has the target disorder before the test is carried out, Pre-test odds = pre-test probability / (1 - pre-test probability), Post-test odds, The odds that the patient has the target disorder after the test is carried out, Post-test odds = pre-test odds x likelihood ratio, where the likelihood ratio for a positive test result = sensitivity / (1 - specificity), Next question
Page 3663 :
You are performing a study of weight in patients attending pre operative assessment clinic for, elective knee replacement. Assuming that the results are normally distributed, what percentage of, values lie within two standard deviations of the mean weight?, , 95.4%, , 5.3%, , 98.3%, , 10%, , 97.5%, In statistics, the 68-95-99.7 rule or three-sigma rule, or empirical rule states that for a normal, distribution, nearly all values lie within 3 standard deviations of the mean., About 68.27% of the values lie within 1 standard deviation of the mean. Similarly, about 95.45% of, the values lie within 2 standard deviations of the mean. Nearly all (99.73%) of the values lie within 3, standard deviations of the mean, 95.4% of values lie within 2 SD of the mean., Please rate this question:, , Discuss and give feedback, , Next question, , Normal distribution, The normal distribution is also known as the Gaussian distribution or 'bell-shaped' distribution. It, describes the spread of many biological and clinical measurements, Properties of the Normal distribution, , , , , , , , symmetrical i.e. Mean = mode = median, 68.3% of values lie within 1 SD of the mean, 95.4% of values lie within 2 SD of the mean, 99.7% of values lie within 3 SD of the mean, this is often reversed, so that within 1.96 SD of the mean lie 95% of the sample values, the range of the mean - (1.96 *SD) to the mean + (1.96 * SD) is called the 95% confidence, interval, i.e. If a repeat sample of 100 observations are taken from the same group 95 of, them would be expected to lie in that range
Page 3664 :
Standard deviation, , , , the standard deviation (SD) represents the average difference each observation in a sample, lies from the sample mean, SD = square root (variance), Next question
Page 3665 :
In Intention to treat analysis, which statement is untrue?, , It is based on the initial treatment intended., , Excludes those who cross over to alternative treatment arms of a trial., , Is different from a per protocol analysis., , Will affect the statistical power calculation to compare outcomes of treatment., , Helps to minimise observer bias., An intention to treat analysis considers data according to the treatment to which the patient was, randomised, rather than the treatment which was recieved., , It includes those who cross over which is how it helps provide additional information relating to those, groups., Please rate this question:, , Discuss and give feedback, , Next question, , Audit and Research, Clinical audit, Quality improvement process that seeks to improve patient care and outcomes through systematic, review of care against explicit criteria and the implementation of change. Aspects of the structure,, processes, and outcomes of care are selected and systematically evaluated against explicit criteria., Where indicated, changes are implemented at an individual, team, or service level and further, monitoring is used to confirm improvement in healthcare delivery. (NICE)., Research, Aims to derive new knowledge which is potentially generalisable or transferable.
Page 3666 :
Which of the following is not usually required to make a power calculation?, , The specificity of the intervention being tested, , The desired significance level, , The size of the effect being measured, , The desired power value, , Sample size used to detect the effect, , The specificity of a test is related to type 1 errors., The components that are nearly always needed for power calculations are :, Size of effect, Significance level, Sample size used to detect the effect, Desired power value, Please rate this question:, , Discuss and give feedback, , Next question, , Power calculations and statistical error, Statistical error, , Type 1, Error, , A test rejects a true null hypothesis. Analogus to false positive. It usually equates to the, significance level assigned to a test.
Page 3667 :
Type 2, Error, , A test fails to reject a false null hypothesis. It is related to the power of a test., , Statistical power, The power of a test is the probability that the test will reject the null hypothesis when it is false, (thereby avoiding a type 2 error). Increasing the power of a test will reduce the probability of a type 2, error. Usually a value of 0.8 is selected., Next question
Page 3668 :
A new hernia mesh designed to prevent the risk of infection undergoes clinical trials. One hundred, patients are given the new mesh. During a three month period 10 of the patients have an episode of, infection. In the control group there are 300 patients who are given a placebo. In this group 50, people have an infection during the same time period. What is the relative risk of having an infection, when the new mesh is used?, , 0.8, , 0.2, , 1.66, , 0.6, , 0.06, , Experimental event rate, EER = 10 / 100 = 0.10, Control event rate, CER = 50 / 300 = 0.166, Therefore the relative risk = EER / CER = 0.1 / 0.166 = 0.6, Please rate this question:, , Discuss and give feedback, , Next question, , Relative risk, Relative risk (RR) is the ratio of risk in the experimental group (experimental event rate, EER) to, risk in the control group (control event rate, CER), To recap, , , , EER = rate at which events occur in the experimental group, CER = rate at which events occur in the control group, , For example, if we look at a trial comparing the use of paracetamol for back pain compared to, placebo we may get the following results
Page 3669 :
Total number of patients, , Experienced significant pain relief, , Paracetamol, , 100, , 60, , Placebo, , 80, , 20, , Experimental event rate, EER = 60 / 100 = 0.6, Control event rate, CER = 20 / 80 = 0.25, Therefore the relative risk = EER / CER = 0.6 / 0.25 = 2.4, If the risk ratio is > 1 then the rate of an event (in this case experiencing significant pain relief) is, increased compared to controls. It is therefore appropriate to calculate the relative risk increase if, necessary (see below)., If the risk ratio is < 1 then the rate of an event is decreased compared to controls. The relative risk, reduction should therefore be calculated (see below)., Relative risk reduction (RRR) or relative risk increase (RRI) is calculated by dividing the absolute, risk change by the control event rate, Using the above data, RRI = (EER - CER) / CER = (0.6 - 0.25) / 0.25 = 1.4 = 140%, Next question
Page 3670 :
Which of the following statements relating to audit and governance is untrue?, , An audit standard is a threshold of compliance with an audit criterion, , Sample size calculations are an important part of audit planning, , Clinical audit is part of clinical governance, , Audits should be performed regularly when a novel surgical technique is introduced and where, there is little knowledge of anticipated complications or outcomes, , An audit criterion is a measurable outcome of care, aspect of practice or capacity, 6 pillars of clinical governance:, Clinical effectiveness, Research and development, Openness, Risk management, Education and training, Clinical audit, , Audits should compare performance against known standards. Where a novel technique is being, introduced standards are unlikely to exist, sample sizes cannot therefore be accurately calculated., This is an example of research, which is not an audit., Please rate this question:, , Discuss and give feedback, , Next question, , Audit and Research, Clinical audit, Quality improvement process that seeks to improve patient care and outcomes through systematic, review of care against explicit criteria and the implementation of change. Aspects of the structure,
Page 3671 :
processes, and outcomes of care are selected and systematically evaluated against explicit criteria., Where indicated, changes are implemented at an individual, team, or service level and further, monitoring is used to confirm improvement in healthcare delivery. (NICE)., Research, Aims to derive new knowledge which is potentially generalisable or transferable., Next question
Page 3672 :
Which of the following statements relating to qualitative data is false?, , The data has no true numerical scale, , It may comprise multiple data groups, , May be reported using odds ratios, , May be reported using frequency histograms, , It is best analysed statistically using a students T test when multiple factors are present, , The students T test should be performed if two sets of data have a normal distribution, the T test, cannot be used to analyse multiple data sets., Please rate this question:, , Discuss and give feedback, , Next question, , Qualitative and quantitative data, Qualitative and quantitative data, Qualitative (categorical) data refers to different descriptions of a characteristic, although it may be, possible to allocate a number it has no scale., Quantitative data is associated with numerical values on a numerical scale., Since quantitative data is based on a numerical scale it can be organised to create a distribution, curve. The central tendency may be estimated using the mode, median and mean. The standard, deviation gives an estimation of the spread of data., , Next question
Page 3673 :
Which of the following statements is false in relation to consent?, , All adults by law are assumed to be competent, , The Bolam test defines if a patient has capacity or not, , Consent 2 is the form signed by parents on behalf of their children, , Implied consent is a form of consent, , Consent 4 is the form signed when a patient is unable to consent for a treatment or investigation, , The Bolam test defines if a decision made by a doctor is in agreement with the professional standard, of medical practise., Please rate this question:, , Discuss and give feedback, , Consent, There are 3 types of consent:, 1. Informed, 2. Expressed, 3. Implied, Consent forms used in UK NHS, , Consent Form, 1, , For competent adults who are able to consent for themselves where consciousness may, be impaired (e.g. GA)
Page 3674 :
Consent Form, 2, , For an adult consenting on behalf of a child where consciousness is impaired, , Consent Form, 3, , For an adult or child where consciousness is not impaired, , Consent Form, 4, , For adults who lack capacity to provide informed consent, , Capacity, Key points include:, 1. Understand and retain information, 2. Patient believes the information to be true, 3. Patient is able to weigh the information to make a decision, All patients must be assumed to have capacity, Consent in minors, Young children and older children who are not Gillick competent cannot consent for themselves. In, British law the patients biological mother can always provide consent. The child's father can consent, if the parents are married (and the father is the biological father), or if the father is named on the, birth certificate (irrespective of marital status). If parents are not married and the father is not named, on the birth certificate then the father cannot consent.
Page 3676 :
Theme: Transplantation, , A., B., C., D., , Xenograft, Allograft, Autograft, Isograft, , Please select the type of transplantation that has occurred in the situation described. Each option, may be used once, more than once or not at all., , 1., , A 38 year old lady donates her kidney to her identical twin sibling., You answered Xenograft, The correct answer is Isograft, Theme from 2015 Exam, Identical twin- twin donations are usually genetically identical and are therefore isografts., , 2., , A 53 year old man with severe angina undergoes a coronary artery bypass procedure and his, long saphenous vein is used as a bypass conduit., You answered Xenograft, The correct answer is Autograft, The long saphenous vein is one of the commonest autografts in surgery., , 3., , A 38 year old lady donates her kidney to her niece., You answered Xenograft, The correct answer is Allograft, Though related this donor will not be genetically identical and thus this will be an allograft., , Please rate this question:, , Discuss and give feedback, , Next question, , Transplant types
Page 3677 :
Graft, , Features, , Uses, , Allograft, , Transplant of tissue from genetically non identical, donor from the same species, , Solid organ transplant from, non related donor, , Isograft, , Graft of tissue between two individuals who are, genetically identical, , Solid organ transplant in, identical twins, , Autograft, , Transplantation of organs or tissues from one part of, the body to another in the same individual, , Skin graft, , Xenograft, , Tissue transplanted from another species, , Porcine heart valve, Next question
Page 3678 :
In matching donated kidneys to the most appropriate recipient, apart from ABO matching, which of, the following is most important?, , HLA DR, , Rhesus, , HLA A, , HLA B, , Duffy antigen, , Theme from January 2013 Exam, The rhesus group is not important in matching donor and recipient kidneys., Please rate this question:, , Discuss and give feedback, , Next question, , Renal transplant:HLA typing and graft failure, The human leucocyte antigen (HLA) system is the name given to the major histocompatibility, complex (MHC) in humans. It is coded for on chromosome 6., Some basic points on the HLA system, , , , , Class 1 antigens include A, B and C. Class 2 antigens include DP,DQ and DR, When HLA matching for a renal transplant the relative importance of the HLA antigens are as, follows DR > B > A
Page 3679 :
Graft survival, , , , , 1 year = 90%, 10 years = 60% for cadaveric transplants, 1 year = 95%, 10 years = 70% for living-donor transplants, , Post-op problems, , , , , , , ATN of graft, Vascular thrombosis, Urine leakage, UTI, , Hyperacute acute rejection, , , , , Due to antibodies against donor HLA type 1 antigens, Rarely seen due to HLA matching, , Acute graft failure (< 6 months), , , , , , Usually due to mismatched HLA, Other causes include cytomegalovirus infection, Management: give steroids, if resistant use monoclonal antibodies, , Causes of chronic graft failure (> 6 months), , , , , , Chronic allograft nephropathy, Ureteric obstruction, Recurrence of original renal disease (MCGN > IgA > FSGS), Next question
Page 3680 :
A 43 year old lady undergoes a live donor related renal transplant. Over the next few years it is, noted that her renal function progressively deteriorates. What is the most likely underlying, explanation?, , Type I hypersensitivity reaction, , Type III hypersensitivity reaction, , Type II hypersensitivity reaction, , Type IV hypersensitivity reaction, , None of the above, , Chronic rejection of renal transplants is mediated via T lymphocytes and is therefore a type IV, hypersensitivity reaction. This process can be mitigated by immunosupression., Please rate this question:, , Discuss and give feedback, , Next question, , Organ Transplant, A number of different organ and tissue transplants are now available. In many cases an allograft is, performed, where an organ is transplanted from one individual to another. Allografts will elicit an, immune response and this is one of the main reasons for organ rejection., Graft rejection occurs because allografts have allelic differences at genes that code, immunohistocompatability complex genes. The main antigens that give rise to rejection are:, , , , , ABO blood group, Human leucocyte antigens (HLA), Minor histocompatability antigens, , ABO Matching, ABO incompatibility will result in early organ rejection (hyperacute) because of pre existing, antibodies to other groups. Group O donors can give organs to any type of ABO recipient whereas, group AB donor can only donate to AB recipient., HLA System
Page 3681 :
The four most important HLA alleles are:, , , , , , , HLA A, HLA B, HLA C, HLA DR, , An ideal organ match would be one in which all 8 alleles are matched (remember 2 from each, parent, four each = 8 alleles). Modern immunosuppressive regimes help to manage the potential, rejection due to HLA mismatching. However, the greater the number of mismatches the worse the, long term outcome will be. T lymphocytes will recognise antigens bound to HLA molecules and will, then become activated. Clonal expansion then occurs with a response directed against that antigen., Types of organ rejection, , , , , Hyperacute. This occurs immediately through presence of pre formed antibodies (such as, ABO incompatibility)., Acute. Occurs during the first 6 months and is usually T cell mediated. Usually tissue, infiltrates and vascular lesions., Chronic. Occurs after the first 6 months. Vascular changes predominate., , Hyperacute, Renal transplants at greatest risk and liver transplants at least risk. Although ABO incompatibility, and HLA Class I incompatible transplants will all fare worse in long term., Acute, All organs may undergo acute rejection. Mononuclear cell infiltrates predominate. All types of, transplanted organ are susceptible and it may occur in up to 50% cases., Chronic, Again all transplants with HLA mismatch may suffer this fate. Previous acute rejections and other, immunosensitising events all increase the risk. Vascular changes are most prominent with, myointimal proliferation leading to organ ischaemia. Organ specific changes are also seen such as, loss of acinar cells in pancreas transplants and rapidly progressive coronary artery disease in, cardiac transplants., Surgical overview-Renal transplantation, A brief overview of the steps involved in renal transplantation is given., Patients with end stage renal failure who are dialysis dependent or likely to become so in the, immediate future are considered for transplant. Exclusion criteria include; active malignancy, old age, (due to limited organ availability). Patients are medically optimised., Donor kidneys, these may be taken from live related donors and close family, members may have, less HLA mismatch than members of the general population. Laparoscopic donor nephrectomy, further minimises the operative morbidity for the donor. Other organs are typically taken from brain, dead or dying patients who have a cardiac arrest and in whom resuscitation is futile. The key event, is to minimise the warm ischaemic time in the donor phase.
Page 3682 :
The kidney once removed is usually prepared on the bench in theatre by the transplant surgeon, immediately prior to implantation and factors such as accessory renal arteries and vessel length are, assessed and managed., For first time recipients the operation is performed under general anaesthesia. A RutherfordMorrison incision is made on the preferred side. This provides excellent extraperitoneal access to, the iliac vessels. The external iliac artery and vein are dissected out and following systemic, heparinisation are cross clamped. The vein and artery are anastamosed to the iliacs and the clamps, removed. The ureter is then implanted into the bladder and a stent is usually placed to maintain, patency. The wounds are then closed and the patient recovered from surgery., In the immediate phase a common problem encountered in cadaveric kidneys is acute tubular, necrosis and this tends to resolve., Graft survival times from cadaveric donors are typically of the order of 9 years and monozygotic twin, transplant (live donor) may survive as long as 25 years., Next question
Page 3683 :
Theme: Renal transplant complications, , A., B., C., D., E., F., G., , Acute tubular necrosis, Renal artery thrombosis, Bladder occlusion, Ureteric occlusion, Acute rejection, Acute on chronic rejection, Hyperacute rejection, , For each of the scenarios given please select the most likely underlying process from the list below., Each option may be used once, more than once or not at all., , 6., , A 45 year old man with end stage renal failure undergoes a cadaveric renal transplant. The, transplanted organ has a cold ischaemic time of 26 hours and a warm ischaemic time of 54, minutes. Post operatively the patient receives immunosuppressive therapy. Ten days later, the patient has gained weight, becomes oliguric and feels systemically unwell. He also, complains of swelling over the transplant site that is painful., You answered Acute tubular necrosis, The correct answer is Acute rejection, Theme from April 2012 Exam, The features described are those of worsening graft function and acute rejection. The fact, that there is a 10 day delay goes against hyperacute rejection. Cold ischaemic times are a, major factor for delayed graft function. However, even 26 hours is not incompatible with, graft survival., , 7., , A 44 year old man with end stage renal failure undergoes a live donor renal transplant., During the immediate post operative period a good urine output is recorded. However, on, return to the ward the nursing staff notice that the urinary catheter is no longer draining., However, the urostomy is continuing to drain urine., You answered Acute tubular necrosis, The correct answer is Bladder occlusion, The most likely explanation for this event is a blocked catheter. This may be the result of, blood clot from the ureteric anastomosis. Bladder irrigation will usually resolve the, problem., , 8., , A 43 year old man undergoes a live donor renal transplant. The donor's right kidney is, anastomosed to the recipient. On removal of the arterial clamps there is good urinary flow
Page 3684 :
noted and the wounds are closed. On return to the ward the nurses notice that the patient, suddenly becomes anuric and irrigation of the bladder does not improve the situation., You answered Acute tubular necrosis, The correct answer is Renal artery thrombosis, Right sided live donor transplants are extremely rare. This is because the vena cava, precludes mobilisation of the right renal artery. The short right renal artery that is produced, therefore presents a major challenge. The sudden cessation of urine output in this context is, highly suggestive of an acute thrombosis. Delay in thrombectomy beyond 1 hour almost, inevitably results in graft loss., Please rate this question:, , Discuss and give feedback, , Next question, , Complications following renal transplant, Renal transplantation is widely practised. The commonest technical related complications are related, to the ureteric anastomosis. The warm ischaemic time is also of considerable importance and graft, survival is directly related to this. Long warm ischaemic times increase the risk of acute tubular, necrosis which may occur in all types of renal transplanation and provided other insults are, minimised, will usually recover. Organ rejection may occur at any phase following the transplantation, process., Immunological complications, Types of organ rejection, , , , , Hyperacute. This occurs immediately through presence of pre formed antibody (such as, ABO incompatibility)., Acute. Occurs during the first 6 months and is usually T cell mediated. Usually tissue, infiltrates and vascular lesions., Chronic. Occurs after the first 6 months. Vascular changes predominate., , Hyperacute, Renal transplants are most susceptible to this process. Risk factors include major HLA mismatch, and ABO incompatibility. The rejection occurs almost immediately and the macroscopic features, may become manifest following completion of the vascular anastomosis and removal of clamps. The, kidney becomes mottled, dusky and the vessels will thrombose. The only treatment is removal of the, graft, if left in situ it will result in abscess formation., Acute, All organs may undergo acute rejection. Mononuclear cell infiltrates predominate. All types of
Page 3685 :
transplanted organ are susceptible and it may occur in up to 50% cases. Most cases can be, managed medically., Chronic, Again all transplants with HLA mismatch may suffer this fate. Previous acute rejections and other, immunosensitising events all increase the risk. Vascular changes are most prominent with, myointimal proliferation leading to organ ischaemia. Organ specific changes are also seen such as, loss of acinar cells in pancreas transplants and rapidly progressive coronary artery disease in, cardiac transplants., Technical complications, , Complication, , Presenting features, , Treatment, , Renal artery, thrombosis, , Sudden complete loss of urine, output, , Immediate surgery may salvage the graft,, delays beyond 30 minutes are associated, with a high rate of graft loss, , Renal artery, stenosis, , Uncontrolled hypertension,, allograft dysfunction and oedema, , Angioplasty is the treatment of choice, , Renal vein, thrombosis, , Pain and swelling over the graft, site, haematuria and oliguria, , The graft is usually lost, , Urine leaks, , Diminished urine output, rising, creatinine, fever and abdominal, pain, , USS shows perigraft collection, necrosis, of ureter tip is the commonest cause and, the anastomosis may need revision, , Lymphocele, , Common complication (occurs in, 15%), may present as a mass, if, large may compress ureter, , May be drained with percutaneous, technique and sclerotherapy, or, intraperitoneal drainage, Next question
Page 3686 :
A 43 year old man undergoes a cadaveric renal transplant. The operation is uncomplicated. On, removal of the vascular clamps the transplanted kidney immediately turns dusky and over the, ensuing hours appears non viable. Which of the following best explains this event?, , Chronic rejection, , Hyper acute rejection, , Acute rejection, , Sub chronic rejection, , Infection of the graft, , Immediate rejection is due to the presence of pre-existing antibodies e.g. ABO mismatch. The, transplanted organ should be removed., Please rate this question:, , Discuss and give feedback, , Next question, , Organ Transplant, A number of different organ and tissue transplants are now available. In many cases an allograft is, performed, where an organ is transplanted from one individual to another. Allografts will elicit an, immune response and this is one of the main reasons for organ rejection., Graft rejection occurs because allografts have allelic differences at genes that code, immunohistocompatability complex genes. The main antigens that give rise to rejection are:, , , , , ABO blood group, Human leucocyte antigens (HLA), Minor histocompatability antigens, , ABO Matching, ABO incompatibility will result in early organ rejection (hyperacute) because of pre existing, antibodies to other groups. Group O donors can give organs to any type of ABO recipient whereas, group AB donor can only donate to AB recipient., HLA System
Page 3687 :
The four most important HLA alleles are:, , , , , , , HLA A, HLA B, HLA C, HLA DR, , An ideal organ match would be one in which all 8 alleles are matched (remember 2 from each, parent, four each = 8 alleles). Modern immunosuppressive regimes help to manage the potential, rejection due to HLA mismatching. However, the greater the number of mismatches the worse the, long term outcome will be. T lymphocytes will recognise antigens bound to HLA molecules and will, then become activated. Clonal expansion then occurs with a response directed against that antigen., Types of organ rejection, , , , , Hyperacute. This occurs immediately through presence of pre formed antibodies (such as, ABO incompatibility)., Acute. Occurs during the first 6 months and is usually T cell mediated. Usually tissue, infiltrates and vascular lesions., Chronic. Occurs after the first 6 months. Vascular changes predominate., , Hyperacute, Renal transplants at greatest risk and liver transplants at least risk. Although ABO incompatibility, and HLA Class I incompatible transplants will all fare worse in long term., Acute, All organs may undergo acute rejection. Mononuclear cell infiltrates predominate. All types of, transplanted organ are susceptible and it may occur in up to 50% cases., Chronic, Again all transplants with HLA mismatch may suffer this fate. Previous acute rejections and other, immunosensitising events all increase the risk. Vascular changes are most prominent with, myointimal proliferation leading to organ ischaemia. Organ specific changes are also seen such as, loss of acinar cells in pancreas transplants and rapidly progressive coronary artery disease in, cardiac transplants., Surgical overview-Renal transplantation, A brief overview of the steps involved in renal transplantation is given., Patients with end stage renal failure who are dialysis dependent or likely to become so in the, immediate future are considered for transplant. Exclusion criteria include; active malignancy, old age, (due to limited organ availability). Patients are medically optimised., Donor kidneys, these may be taken from live related donors and close family, members may have, less HLA mismatch than members of the general population. Laparoscopic donor nephrectomy, further minimises the operative morbidity for the donor. Other organs are typically taken from brain, dead or dying patients who have a cardiac arrest and in whom resuscitation is futile. The key event, is to minimise the warm ischaemic time in the donor phase.
Page 3688 :
The kidney once removed is usually prepared on the bench in theatre by the transplant surgeon, immediately prior to implantation and factors such as accessory renal arteries and vessel length are, assessed and managed., For first time recipients the operation is performed under general anaesthesia. A RutherfordMorrison incision is made on the preferred side. This provides excellent extraperitoneal access to, the iliac vessels. The external iliac artery and vein are dissected out and following systemic, heparinisation are cross clamped. The vein and artery are anastamosed to the iliacs and the clamps, removed. The ureter is then implanted into the bladder and a stent is usually placed to maintain, patency. The wounds are then closed and the patient recovered from surgery., In the immediate phase a common problem encountered in cadaveric kidneys is acute tubular, necrosis and this tends to resolve., Graft survival times from cadaveric donors are typically of the order of 9 years and monozygotic twin, transplant (live donor) may survive as long as 25 years., Next question
Page 3689 :
Theme: Complications following renal transplant, , A., B., C., D., E., F., G., H., , Ureteric anastomotic leak, Renal vein thrombosis, Acute rejection, Chronic allograft nephropathy, Renal artery thrombosis, Renal artery stenosis, Lymphocele, Hyperacute rejection, , For each of the patients described below, please select the most appropriate underlying explanation, for the situation described. Each option may be used once, more than once or not at all., , 10., , A 45 year old lady undergoes a renal transplant from a living related donor. She is well for, several months but on review in the outpatient department is noted to have persistent, hypertension and a slight deterioration in renal function., You answered Ureteric anastomotic leak, The correct answer is Renal artery stenosis, Renal artery stenosis typically occurs over several months and will usually result in the, development of hypertension. Most cases can be assessed using duplex scanning and, managed with angioplasty., , 11., , A 43 year old lady undergoes a live related renal transplant. At the conclusion of the, operation she has a good urine output and the graft appeared well perfused. On the ward, she suddenly becomes anuric., You answered Ureteric anastomotic leak, The correct answer is Renal artery thrombosis, Sudden loss of urine output is most commonly due to a blocked catheter. However, if this, is excluded (and is not included in the options) the most worrisome cause is arterial, thrombosis. This will often be a delayed diagnosis and the rate of graft loss is high., , 12., , A 39 year old lady undergoes a live related renal transplant. She progresses well. Two, weeks following the transplant she is noted to have swelling overlying the transplant site, and swelling of the ipsilateral limb.Urine output is acceptable and creatinine unchanged., You answered Ureteric anastomotic leak
Page 3690 :
The correct answer is Lymphocele, Swelling over the graft site is often due to a lymphocele and this is further suggested by, the normal renal function. They cause symptoms through mass effect and limb swelling, may occur. Treatment is often surgical., Please rate this question:, , Discuss and give feedback, , Next question, , Complications of renal transplantation, A number of complications may occur following renal transplantation. A critical aspect of post, operative care is evaluation of graft function. Post operatively, urine output is the most readily, available, and easily measured, indicator of graft function. If an individual was relatively anuric pretransplant and has a good urine output following surgery then this is more useful than it would be in, someone who had a higher volume diuresis prior to transplantation. Recipients can be divided into, three main groups following renal transplantation, with regard to their graft function:, , , , , Immediate graft function; brisk diuresis and falling serum creatinine, Slow graft function; modest urine output and slowly falling creatinine levels, Delayed graft function; defined as need for dialysis post transplant, , Decreased urine output following surgery can be the result of hypovolvaemia or a blocked catheter, (commonest causes). Other important causes include rejection, or a vascular complication., Vascular complications, These may involve the donor vessels, those of the recipient or both. Renal artery thrombosis usually, occurs early post transplant, but is uncommon with an incidence of less than 1%. It typically results, in graft loss. It usually occurs as a result of a technical problem such a vessel torsion or sub intimal, flaps. The usual presenting feature is a sudden cessation of urine output. When suspected, the, occlusion is usually well demonstrated with duplex scanning. Ideally immediate surgical reexploration should occur. Sadly, the graft has usually been lost by this stage and will require graft, nephrectomy. Renal vein thrombosis is not as common as arterial graft thrombosis and the usual, presenting features include discomfort at the graft site and swelling of the graft associated with loss, of urine output. Again, duplex scanning is indicated. Unfortunately, this complication is also, associated with a high incidence of graft loss., Over a longer time frame (typically months) some individuals will develop renal artery stenosis., These individuals will typically develop hypertension and over time graft function will decline as, hypertensive nephropathy occurs. It is usually demonstrated by duplex scanning and is usually, amenable to endovascular intervention., Urological complications, Urinary tract complications manifesting as leakage or obstruction are common complications, following renal transplantation and occur in up to 10% of patients. The main underlying cause is the
Page 3691 :
relatively poor blood supply to the transplanted ureter. Patients typically present relatively early in, the first 5 weeks following transplantation with pain and swelling at the graft site. Imaging with USS, is often the initial test. Therapeutic options include surgical re-implantation of the ureter for large, leaks and stent insertion and nephrostomy placement for smaller leaks., Lymphocele, These do not generally occur until 2 weeks or longer after surgery. They are, however, relatively, common and may be seen in up to 18% of patients. Symptoms usually occur as a result of mass, effect with compression of adjacent structures. These include the vessels supplying both the graft,, with deterioration in graft function, the ureter, with alteration in urine output and the recipients lower, limb vessels, with development of leg swelling. Creation of a laparoscopic or open peritoneal window, is a favored treatment., Rejection, Four types of graft rejection are recognised; hyperacute, accelerated acute, acute and chronic., , Type of, rejection, , Key features, , Hyperacute, , Occurs within minutes of clamp release, Due to pre formed antibodies, Immediate loss of graft occurs, , Accelerated, acute, , Occurs in first few days following surgery, Involved both cellular and antibody mediated injury, Pre-sensitisation of the donor is a common cause, , Acute, , Traditionally the most common type of rejection, Seen days to weeks after surgery, Predominantly a cell mediated process mediated by lymphocytes, Organ biopsy demonstrates cellular infiltrates and graft cell apoptosis, , Chronic, , Increasingly common problem, Typically; graft atrophy and atherosclerosis are seen. Fibrosis often occurs as a, late event, Next question
Page 3692 :
A 48 year old lady with end stage renal failure receives a cadaveric renal transplant. The organ is, ABO group matched only. On completion of the vascular anastomoses the surgeons remove the, clamps. Over the course of the next twelve minutes the donated kidney becomes dusky and swollen, and appears non viable. Which of the following is the most likely process that has caused this event?, , IgG anti HLA Class I antibodies in the recipient, , IgM anti HLA Class I antibodies in the recipient, , IgG anti HLA Class I antibodies from the donor, , IgM anti HLA Class I antibodies from the donor, , IgM anti HLA Class II antibodies from the recipient, , Episodes of hyperacute rejection are typically due to preformed antibodies. ABO mismatch is the, best example. However, IgG anti HLA Class I antibodies are another potential cause. These events, are now seen less commonly because the cross matching process generally takes this possibility, into account., Please rate this question:, , Discuss and give feedback, , Next question, , Organ Transplant, A number of different organ and tissue transplants are now available. In many cases an allograft is, performed, where an organ is transplanted from one individual to another. Allografts will elicit an, immune response and this is one of the main reasons for organ rejection., Graft rejection occurs because allografts have allelic differences at genes that code, immunohistocompatability complex genes. The main antigens that give rise to rejection are:, , , , , ABO blood group, Human leucocyte antigens (HLA), Minor histocompatability antigens, , ABO Matching, ABO incompatibility will result in early organ rejection (hyperacute) because of pre existing, antibodies to other groups. Group O donors can give organs to any type of ABO recipient whereas
Page 3693 :
group AB donor can only donate to AB recipient., HLA System, The four most important HLA alleles are:, , , , , , , HLA A, HLA B, HLA C, HLA DR, , An ideal organ match would be one in which all 8 alleles are matched (remember 2 from each, parent, four each = 8 alleles). Modern immunosuppressive regimes help to manage the potential, rejection due to HLA mismatching. However, the greater the number of mismatches the worse the, long term outcome will be. T lymphocytes will recognise antigens bound to HLA molecules and will, then become activated. Clonal expansion then occurs with a response directed against that antigen., Types of organ rejection, , , , , Hyperacute. This occurs immediately through presence of pre formed antibodies (such as, ABO incompatibility)., Acute. Occurs during the first 6 months and is usually T cell mediated. Usually tissue, infiltrates and vascular lesions., Chronic. Occurs after the first 6 months. Vascular changes predominate., , Hyperacute, Renal transplants at greatest risk and liver transplants at least risk. Although ABO incompatibility, and HLA Class I incompatible transplants will all fare worse in long term., Acute, All organs may undergo acute rejection. Mononuclear cell infiltrates predominate. All types of, transplanted organ are susceptible and it may occur in up to 50% cases., Chronic, Again all transplants with HLA mismatch may suffer this fate. Previous acute rejections and other, immunosensitising events all increase the risk. Vascular changes are most prominent with, myointimal proliferation leading to organ ischaemia. Organ specific changes are also seen such as, loss of acinar cells in pancreas transplants and rapidly progressive coronary artery disease in, cardiac transplants., Surgical overview-Renal transplantation, A brief overview of the steps involved in renal transplantation is given., Patients with end stage renal failure who are dialysis dependent or likely to become so in the, immediate future are considered for transplant. Exclusion criteria include; active malignancy, old age, (due to limited organ availability). Patients are medically optimised., Donor kidneys, these may be taken from live related donors and close family, members may have, less HLA mismatch than members of the general population. Laparoscopic donor nephrectomy, further minimises the operative morbidity for the donor. Other organs are typically taken from brain
Page 3694 :
dead or dying patients who have a cardiac arrest and in whom resuscitation is futile. The key event, is to minimise the warm ischaemic time in the donor phase., The kidney once removed is usually prepared on the bench in theatre by the transplant surgeon, immediately prior to implantation and factors such as accessory renal arteries and vessel length are, assessed and managed., For first time recipients the operation is performed under general anaesthesia. A RutherfordMorrison incision is made on the preferred side. This provides excellent extraperitoneal access to, the iliac vessels. The external iliac artery and vein are dissected out and following systemic, heparinisation are cross clamped. The vein and artery are anastamosed to the iliacs and the clamps, removed. The ureter is then implanted into the bladder and a stent is usually placed to maintain, patency. The wounds are then closed and the patient recovered from surgery., In the immediate phase a common problem encountered in cadaveric kidneys is acute tubular, necrosis and this tends to resolve., Graft survival times from cadaveric donors are typically of the order of 9 years and monozygotic twin, transplant (live donor) may survive as long as 25 years., Next question
Page 3695 :
A 54-year-old man who has end stage diabetic nephropathy is being assessed for a renal transplant., When assessing the HLA matching between donor and recipient what is the most important HLA, antigen to match?, , DP, , B, , DR, , C, , A, Renal transplant HLA matching - DR is the most important, Please rate this question:, , Discuss and give feedback, , Next question, , Renal transplant:HLA typing and graft failure, The human leucocyte antigen (HLA) system is the name given to the major histocompatibility, complex (MHC) in humans. It is coded for on chromosome 6., Some basic points on the HLA system, , , , Class 1 antigens include A, B and C. Class 2 antigens include DP,DQ and DR, When HLA matching for a renal transplant the relative importance of the HLA antigens are as, follows DR > B > A, , Graft survival, , , , 1 year = 90%, 10 years = 60% for cadaveric transplants, 1 year = 95%, 10 years = 70% for living-donor transplants
Page 3696 :
Post-op problems, , , , , , ATN of graft, Vascular thrombosis, Urine leakage, UTI, , Hyperacute acute rejection, , , , Due to antibodies against donor HLA type 1 antigens, Rarely seen due to HLA matching, , Acute graft failure (< 6 months), , , , , Usually due to mismatched HLA, Other causes include cytomegalovirus infection, Management: give steroids, if resistant use monoclonal antibodies, , Causes of chronic graft failure (> 6 months), , , , , Chronic allograft nephropathy, Ureteric obstruction, Recurrence of original renal disease (MCGN > IgA > FSGS), Next question
Page 3697 :
Which of the following transplants is most susceptible to donor- recipient HLA mismatches?, , Autologous skin graft, , Renal allograft, , Liver allograft, , Corneal allograft, , Cardiac valve allograft, Autologous transplant- same individual (genetically identical), Allograft - Genetically different, The kidney is highly susceptible to HLA mismatches and hyperacute rejection may occur in patients, with IgG anti HLA Class I antibodies. The liver is at far lower risk of rejection of this nature. Although, the heart is sensitive to HLA mismatches this is less than the kidney. Cardiac valves and the cornea, incite little immunological response., Please rate this question:, , Discuss and give feedback, , Next question, , Organ Transplant, A number of different organ and tissue transplants are now available. In many cases an allograft is, performed, where an organ is transplanted from one individual to another. Allografts will elicit an, immune response and this is one of the main reasons for organ rejection., Graft rejection occurs because allografts have allelic differences at genes that code, immunohistocompatability complex genes. The main antigens that give rise to rejection are:, , , , , ABO blood group, Human leucocyte antigens (HLA), Minor histocompatability antigens, , ABO Matching, ABO incompatibility will result in early organ rejection (hyperacute) because of pre existing, antibodies to other groups. Group O donors can give organs to any type of ABO recipient whereas
Page 3698 :
group AB donor can only donate to AB recipient., HLA System, The four most important HLA alleles are:, , , , , , , HLA A, HLA B, HLA C, HLA DR, , An ideal organ match would be one in which all 8 alleles are matched (remember 2 from each, parent, four each = 8 alleles). Modern immunosuppressive regimes help to manage the potential, rejection due to HLA mismatching. However, the greater the number of mismatches the worse the, long term outcome will be. T lymphocytes will recognise antigens bound to HLA molecules and will, then become activated. Clonal expansion then occurs with a response directed against that antigen., Types of organ rejection, , , , , Hyperacute. This occurs immediately through presence of pre formed antibodies (such as, ABO incompatibility)., Acute. Occurs during the first 6 months and is usually T cell mediated. Usually tissue, infiltrates and vascular lesions., Chronic. Occurs after the first 6 months. Vascular changes predominate., , Hyperacute, Renal transplants at greatest risk and liver transplants at least risk. Although ABO incompatibility, and HLA Class I incompatible transplants will all fare worse in long term., Acute, All organs may undergo acute rejection. Mononuclear cell infiltrates predominate. All types of, transplanted organ are susceptible and it may occur in up to 50% cases., Chronic, Again all transplants with HLA mismatch may suffer this fate. Previous acute rejections and other, immunosensitising events all increase the risk. Vascular changes are most prominent with, myointimal proliferation leading to organ ischaemia. Organ specific changes are also seen such as, loss of acinar cells in pancreas transplants and rapidly progressive coronary artery disease in, cardiac transplants., Surgical overview-Renal transplantation, A brief overview of the steps involved in renal transplantation is given., Patients with end stage renal failure who are dialysis dependent or likely to become so in the, immediate future are considered for transplant. Exclusion criteria include; active malignancy, old age, (due to limited organ availability). Patients are medically optimised., Donor kidneys, these may be taken from live related donors and close family, members may have, less HLA mismatch than members of the general population. Laparoscopic donor nephrectomy, further minimises the operative morbidity for the donor. Other organs are typically taken from brain
Page 3699 :
dead or dying patients who have a cardiac arrest and in whom resuscitation is futile. The key event, is to minimise the warm ischaemic time in the donor phase., The kidney once removed is usually prepared on the bench in theatre by the transplant surgeon, immediately prior to implantation and factors such as accessory renal arteries and vessel length are, assessed and managed., For first time recipients the operation is performed under general anaesthesia. A RutherfordMorrison incision is made on the preferred side. This provides excellent extraperitoneal access to, the iliac vessels. The external iliac artery and vein are dissected out and following systemic, heparinisation are cross clamped. The vein and artery are anastamosed to the iliacs and the clamps, removed. The ureter is then implanted into the bladder and a stent is usually placed to maintain, patency. The wounds are then closed and the patient recovered from surgery., In the immediate phase a common problem encountered in cadaveric kidneys is acute tubular, necrosis and this tends to resolve., Graft survival times from cadaveric donors are typically of the order of 9 years and monozygotic twin, transplant (live donor) may survive as long as 25 years., Next question
Page 3700 :
Which of the following is not true of hyper acute solid organ transplant rejection?, , It may occur during the surgical procedure itself., , May occur as a result of blood group A, B or O incompatibility., , May be due to pre existing anti HLA antibodies., , On biopsy will typically show neo intimal hyperplasia of donor arterioles., , Complement system activation is one of the key mediators., , These changes are more often seen in the chronic setting. Thrombosis is more commonly seen in, the hyperacute phase., Please rate this question:, , Discuss and give feedback, , Next question, , Organ Transplant, A number of different organ and tissue transplants are now available. In many cases an allograft is, performed, where an organ is transplanted from one individual to another. Allografts will elicit an, immune response and this is one of the main reasons for organ rejection., Graft rejection occurs because allografts have allelic differences at genes that code, immunohistocompatability complex genes. The main antigens that give rise to rejection are:, , , , , ABO blood group, Human leucocyte antigens (HLA), Minor histocompatability antigens, , ABO Matching, ABO incompatibility will result in early organ rejection (hyperacute) because of pre existing, antibodies to other groups. Group O donors can give organs to any type of ABO recipient whereas, group AB donor can only donate to AB recipient., HLA System, The four most important HLA alleles are:
Page 3701 :
, , , , , HLA A, HLA B, HLA C, HLA DR, , An ideal organ match would be one in which all 8 alleles are matched (remember 2 from each, parent, four each = 8 alleles). Modern immunosuppressive regimes help to manage the potential, rejection due to HLA mismatching. However, the greater the number of mismatches the worse the, long term outcome will be. T lymphocytes will recognise antigens bound to HLA molecules and will, then become activated. Clonal expansion then occurs with a response directed against that antigen., Types of organ rejection, , , , , Hyperacute. This occurs immediately through presence of pre formed antibodies (such as, ABO incompatibility)., Acute. Occurs during the first 6 months and is usually T cell mediated. Usually tissue, infiltrates and vascular lesions., Chronic. Occurs after the first 6 months. Vascular changes predominate., , Hyperacute, Renal transplants at greatest risk and liver transplants at least risk. Although ABO incompatibility, and HLA Class I incompatible transplants will all fare worse in long term., Acute, All organs may undergo acute rejection. Mononuclear cell infiltrates predominate. All types of, transplanted organ are susceptible and it may occur in up to 50% cases., Chronic, Again all transplants with HLA mismatch may suffer this fate. Previous acute rejections and other, immunosensitising events all increase the risk. Vascular changes are most prominent with, myointimal proliferation leading to organ ischaemia. Organ specific changes are also seen such as, loss of acinar cells in pancreas transplants and rapidly progressive coronary artery disease in, cardiac transplants., Surgical overview-Renal transplantation, A brief overview of the steps involved in renal transplantation is given., Patients with end stage renal failure who are dialysis dependent or likely to become so in the, immediate future are considered for transplant. Exclusion criteria include; active malignancy, old age, (due to limited organ availability). Patients are medically optimised., Donor kidneys, these may be taken from live related donors and close family, members may have, less HLA mismatch than members of the general population. Laparoscopic donor nephrectomy, further minimises the operative morbidity for the donor. Other organs are typically taken from brain, dead or dying patients who have a cardiac arrest and in whom resuscitation is futile. The key event, is to minimise the warm ischaemic time in the donor phase.
Page 3702 :
The kidney once removed is usually prepared on the bench in theatre by the transplant surgeon, immediately prior to implantation and factors such as accessory renal arteries and vessel length are, assessed and managed., For first time recipients the operation is performed under general anaesthesia. A RutherfordMorrison incision is made on the preferred side. This provides excellent extraperitoneal access to, the iliac vessels. The external iliac artery and vein are dissected out and following systemic, heparinisation are cross clamped. The vein and artery are anastamosed to the iliacs and the clamps, removed. The ureter is then implanted into the bladder and a stent is usually placed to maintain, patency. The wounds are then closed and the patient recovered from surgery., In the immediate phase a common problem encountered in cadaveric kidneys is acute tubular, necrosis and this tends to resolve., Graft survival times from cadaveric donors are typically of the order of 9 years and monozygotic twin, transplant (live donor) may survive as long as 25 years., Next question
Page 3703 :
You review a 42-year-old woman six weeks following a renal transplant for focal segmental, glomerulosclerosis. Following the procedure she was discharged on a combination of tacrolimus,, mycophenolate, and prednisolone. She has now presented with a five day history of feeling, generally unwell with anorexia, fatigue and arthralgia. On examination she has a temperature of 37.9, and has widespread lymphadenopathy. What is the most likely diagnosis?, , Hepatitis C, , Epstein-Barr virus, , HIV, , Hepatitis B, , Cytomegalovirus, Cytomegalovirus is the most common and important viral infection in solid organ transplant, recipients, Primary infection with CMV typically occurs 6 weeks post transplantation in a seronegative individual, who receives an organ from a seropositive donor. Symptoms may occur as early as 20 days but can, occur up to 6 months post transplant . Symptoms are often vague, retinitis can be pathognomonic,, but is rarely seen in the transplant population. CMV disease is seen in 8% of renal transplant, patients. Intravenous ganciclovir is the treatment of choice in such patients. Unfortunately, relapses, are not uncommon., Please rate this question:, , Discuss and give feedback, , Next question, , Renal transplant:HLA typing and graft failure, The human leucocyte antigen (HLA) system is the name given to the major histocompatibility, complex (MHC) in humans. It is coded for on chromosome 6., Some basic points on the HLA system, , , , Class 1 antigens include A, B and C. Class 2 antigens include DP,DQ and DR, When HLA matching for a renal transplant the relative importance of the HLA antigens are as, follows DR > B > A
Page 3704 :
Graft survival, , , , 1 year = 90%, 10 years = 60% for cadaveric transplants, 1 year = 95%, 10 years = 70% for living-donor transplants, , Post-op problems, , , , , , ATN of graft, Vascular thrombosis, Urine leakage, UTI, , Hyperacute acute rejection, , , , Due to antibodies against donor HLA type 1 antigens, Rarely seen due to HLA matching, , Acute graft failure (< 6 months), , , , , Usually due to mismatched HLA, Other causes include cytomegalovirus infection, Management: give steroids, if resistant use monoclonal antibodies, , Causes of chronic graft failure (> 6 months), , , , , Chronic allograft nephropathy, Ureteric obstruction, Recurrence of original renal disease (MCGN > IgA > FSGS), Next question
Page 3705 :
A 43 year old lady is recovering following a live donor related renal transplant. She has significant, abdominal pain. Which of the following analgesic drugs should be avoided?, , Paracetamol, , Morphine, , Nefopam, , Diclofenac, , Co-codamol, , Non steroidal anti inflammatory drugs may be nephrotoxic and therefore are usually avoided in, patients who have undergone renal transplants. Paracetamol and morphine are metabolised, predominantly in the liver. There is some renal contribution to morphine metabolism and excretion, and the drug should be administered in reduced doses or avoided if the transplanted kidney stops, functioning., Please rate this question:, , Discuss and give feedback, , Next question, , Organ Transplant, A number of different organ and tissue transplants are now available. In many cases an allograft is, performed, where an organ is transplanted from one individual to another. Allografts will elicit an, immune response and this is one of the main reasons for organ rejection., Graft rejection occurs because allografts have allelic differences at genes that code, immunohistocompatability complex genes. The main antigens that give rise to rejection are:, , , , , ABO blood group, Human leucocyte antigens (HLA), Minor histocompatability antigens, , ABO Matching, ABO incompatibility will result in early organ rejection (hyperacute) because of pre existing, antibodies to other groups. Group O donors can give organs to any type of ABO recipient whereas, group AB donor can only donate to AB recipient.
Page 3706 :
HLA System, The four most important HLA alleles are:, , , , , , , HLA A, HLA B, HLA C, HLA DR, , An ideal organ match would be one in which all 8 alleles are matched (remember 2 from each, parent, four each = 8 alleles). Modern immunosuppressive regimes help to manage the potential, rejection due to HLA mismatching. However, the greater the number of mismatches the worse the, long term outcome will be. T lymphocytes will recognise antigens bound to HLA molecules and will, then become activated. Clonal expansion then occurs with a response directed against that antigen., Types of organ rejection, , , , , Hyperacute. This occurs immediately through presence of pre formed antibodies (such as, ABO incompatibility)., Acute. Occurs during the first 6 months and is usually T cell mediated. Usually tissue, infiltrates and vascular lesions., Chronic. Occurs after the first 6 months. Vascular changes predominate., , Hyperacute, Renal transplants at greatest risk and liver transplants at least risk. Although ABO incompatibility, and HLA Class I incompatible transplants will all fare worse in long term., Acute, All organs may undergo acute rejection. Mononuclear cell infiltrates predominate. All types of, transplanted organ are susceptible and it may occur in up to 50% cases., Chronic, Again all transplants with HLA mismatch may suffer this fate. Previous acute rejections and other, immunosensitising events all increase the risk. Vascular changes are most prominent with, myointimal proliferation leading to organ ischaemia. Organ specific changes are also seen such as, loss of acinar cells in pancreas transplants and rapidly progressive coronary artery disease in, cardiac transplants., Surgical overview-Renal transplantation, A brief overview of the steps involved in renal transplantation is given., Patients with end stage renal failure who are dialysis dependent or likely to become so in the, immediate future are considered for transplant. Exclusion criteria include; active malignancy, old age, (due to limited organ availability). Patients are medically optimised., Donor kidneys, these may be taken from live related donors and close family, members may have, less HLA mismatch than members of the general population. Laparoscopic donor nephrectomy, further minimises the operative morbidity for the donor. Other organs are typically taken from brain, dead or dying patients who have a cardiac arrest and in whom resuscitation is futile. The key event
Page 3707 :
is to minimise the warm ischaemic time in the donor phase., The kidney once removed is usually prepared on the bench in theatre by the transplant surgeon, immediately prior to implantation and factors such as accessory renal arteries and vessel length are, assessed and managed., For first time recipients the operation is performed under general anaesthesia. A RutherfordMorrison incision is made on the preferred side. This provides excellent extraperitoneal access to, the iliac vessels. The external iliac artery and vein are dissected out and following systemic, heparinisation are cross clamped. The vein and artery are anastamosed to the iliacs and the clamps, removed. The ureter is then implanted into the bladder and a stent is usually placed to maintain, patency. The wounds are then closed and the patient recovered from surgery., In the immediate phase a common problem encountered in cadaveric kidneys is acute tubular, necrosis and this tends to resolve., Graft survival times from cadaveric donors are typically of the order of 9 years and monozygotic twin, transplant (live donor) may survive as long as 25 years., Next question
Page 3708 :
A 52 year old male attends renal transplant clinic for a post operative assessment. You note that he, is on ciclosporin and that a recent blood test shows that the ciclosporin level is elevated. Which of, the following is a recognised side effect of ciclosporin?, , Hyperthyroidism, , Diabetes, , Alopecia, , Hypothermia, , Nephrotoxicity, Ciclosporin- nephrotoxicity, This patient is at risk of nephrotoxicity and should be referred to the renal team as soon as possible., Alopecia is associated with azathioprine and diabetes is associated with tacrolimus., Please rate this question:, , Discuss and give feedback, , Next question, , Organ transplantation: immunosupressants, A number of drugs are available which help to mitigate the processes resulting in acute rejection., Cyclosporin and tacrolimus are commonly used drugs., Example regime, , , , , Initial: ciclosporin/tacrolimus with a monoclonal antibody, Maintenance: ciclosporin/tacrolimus with MMF or sirolimus, Add steroids if more than one steroid responsive acute rejection episode, , Ciclosporin, , , , , Inhibits calcineurin, a phosphatase involved in T cell activation, Nephrotoxic, Monitor levels
Page 3709 :
Azathioprine, , , , Metabolised to form 6 mercaptopurine which inhibits DNA synthesis and cell division, Side effects include myelosupression, alopecia and nausea, , Tacrolimus, , , , , Lower incidence of acute rejection compared to ciclosporin, Also less hypertension and hyperlipidaemia, However, high incidence of impaired glucose tolerance and diabetes, , Mycophenolate mofetil (MMF), , , , , Blocks purine synthesis by inhibition of IMPDH, Therefore inhibits proliferation of B and T cells, Side-effects: GI and marrow suppression, , Sirolimus (rapamycin), , , , Blocks T cell proliferation by blocking the IL-2 receptor, Can cause hyperlipidaemia, , Monoclonal antibodies, , , , , Selective inhibitors of IL-2 receptor, Daclizumab, Basilximab, Next question
Page 3710 :
A 48 year old woman with end stage renal failure is undergoing a live donor renal transplant. The, surgeon decides to implant the kidney in the left iliac fossa via a Rutherford Morrison incision. To, which of the following vessels should the transplanted kidney be anastomosed?, , Aorta and inferior vena cava, , Internal iliac artery and vein, , Common iliac artery and vein, , External iliac artery and vein, , Inferior epigastric artery and vein, , First time renal tranplants and typically implanted in the left or right iliac fossae. The vessels are, usually joined to the external iliac artery and vein as these are the most easily accessible. The, Rutherford Morrison incision provides access to the external iliac vessels., Please rate this question:, , Discuss and give feedback, , Next question, , Organ Transplant, A number of different organ and tissue transplants are now available. In many cases an allograft is, performed, where an organ is transplanted from one individual to another. Allografts will elicit an, immune response and this is one of the main reasons for organ rejection., Graft rejection occurs because allografts have allelic differences at genes that code, immunohistocompatability complex genes. The main antigens that give rise to rejection are:, , , , , ABO blood group, Human leucocyte antigens (HLA), Minor histocompatability antigens, , ABO Matching, ABO incompatibility will result in early organ rejection (hyperacute) because of pre existing, antibodies to other groups. Group O donors can give organs to any type of ABO recipient whereas, group AB donor can only donate to AB recipient.
Page 3711 :
HLA System, The four most important HLA alleles are:, , , , , , , HLA A, HLA B, HLA C, HLA DR, , An ideal organ match would be one in which all 8 alleles are matched (remember 2 from each, parent, four each = 8 alleles). Modern immunosuppressive regimes help to manage the potential, rejection due to HLA mismatching. However, the greater the number of mismatches the worse the, long term outcome will be. T lymphocytes will recognise antigens bound to HLA molecules and will, then become activated. Clonal expansion then occurs with a response directed against that antigen., Types of organ rejection, , , , , Hyperacute. This occurs immediately through presence of pre formed antibodies (such as, ABO incompatibility)., Acute. Occurs during the first 6 months and is usually T cell mediated. Usually tissue, infiltrates and vascular lesions., Chronic. Occurs after the first 6 months. Vascular changes predominate., , Hyperacute, Renal transplants at greatest risk and liver transplants at least risk. Although ABO incompatibility, and HLA Class I incompatible transplants will all fare worse in long term., Acute, All organs may undergo acute rejection. Mononuclear cell infiltrates predominate. All types of, transplanted organ are susceptible and it may occur in up to 50% cases., Chronic, Again all transplants with HLA mismatch may suffer this fate. Previous acute rejections and other, immunosensitising events all increase the risk. Vascular changes are most prominent with, myointimal proliferation leading to organ ischaemia. Organ specific changes are also seen such as, loss of acinar cells in pancreas transplants and rapidly progressive coronary artery disease in, cardiac transplants., Surgical overview-Renal transplantation, A brief overview of the steps involved in renal transplantation is given., Patients with end stage renal failure who are dialysis dependent or likely to become so in the, immediate future are considered for transplant. Exclusion criteria include; active malignancy, old age, (due to limited organ availability). Patients are medically optimised., Donor kidneys, these may be taken from live related donors and close family, members may have, less HLA mismatch than members of the general population. Laparoscopic donor nephrectomy, further minimises the operative morbidity for the donor. Other organs are typically taken from brain, dead or dying patients who have a cardiac arrest and in whom resuscitation is futile. The key event, is to minimise the warm ischaemic time in the donor phase.
Page 3712 :
The kidney once removed is usually prepared on the bench in theatre by the transplant surgeon, immediately prior to implantation and factors such as accessory renal arteries and vessel length are, assessed and managed., For first time recipients the operation is performed under general anaesthesia. A RutherfordMorrison incision is made on the preferred side. This provides excellent extraperitoneal access to, the iliac vessels. The external iliac artery and vein are dissected out and following systemic, heparinisation are cross clamped. The vein and artery are anastamosed to the iliacs and the clamps, removed. The ureter is then implanted into the bladder and a stent is usually placed to maintain, patency. The wounds are then closed and the patient recovered from surgery., In the immediate phase a common problem encountered in cadaveric kidneys is acute tubular, necrosis and this tends to resolve., Graft survival times from cadaveric donors are typically of the order of 9 years and monozygotic twin, transplant (live donor) may survive as long as 25 years., Next question
Page 3713 :
A 28-year-old female undergoes a renal transplant for focal segmental glomerulosclerosis. Within, hours of the operation the patient becomes unwell with features consistent with severe systemic, inflammatory response syndrome. The patient is immediately taken back to theatre and the, transplanted kidney is removed. What type of immunoglobulins are responsible for the graft, rejection?, , IgE, , IgM, , IgG, , IgD, , IgA, , Hyperacute graft rejection is due to pre-existent antibodies to HLA antigens and is therefore IgG, mediated, Please rate this question:, , Discuss and give feedback, , Next question, , Renal transplant:HLA typing and graft failure, The human leucocyte antigen (HLA) system is the name given to the major histocompatibility, complex (MHC) in humans. It is coded for on chromosome 6., Some basic points on the HLA system, , , , Class 1 antigens include A, B and C. Class 2 antigens include DP,DQ and DR, When HLA matching for a renal transplant the relative importance of the HLA antigens are as, follows DR > B > A, , Graft survival, , , , 1 year = 90%, 10 years = 60% for cadaveric transplants, 1 year = 95%, 10 years = 70% for living-donor transplants
Page 3714 :
Post-op problems, , , , , , ATN of graft, Vascular thrombosis, Urine leakage, UTI, , Hyperacute acute rejection, , , , Due to antibodies against donor HLA type 1 antigens, Rarely seen due to HLA matching, , Acute graft failure (< 6 months), , , , , Usually due to mismatched HLA, Other causes include cytomegalovirus infection, Management: give steroids, if resistant use monoclonal antibodies, , Causes of chronic graft failure (> 6 months), , , , , Chronic allograft nephropathy, Ureteric obstruction, Recurrence of original renal disease (MCGN > IgA > FSGS)
Page 3715 :
A 38 year old man is recovering following a live donor related renal transplant. The surgeon, prescribes corticosteroids to reduce the risk of graft rejection. Which of the following will not occur as, a result of their administration?, , Suppression of macrophage activation, , Reduction of expression of major histocompatability complex antigens on the graft, , Reduction in the proliferation of lymphocytes, , Necrosis of activated lymphocytes, , Reduction of expression of endothelial cell adhesion molecules, , Corticosteroids at higher doses are able to induce apoptosis of activated lymphocytes. Necrosis is a, different process and not induced by steroids., Please rate this question:, , Discuss and give feedback, , Next question, , Organ Transplant, A number of different organ and tissue transplants are now available. In many cases an allograft is, performed, where an organ is transplanted from one individual to another. Allografts will elicit an, immune response and this is one of the main reasons for organ rejection., Graft rejection occurs because allografts have allelic differences at genes that code, immunohistocompatability complex genes. The main antigens that give rise to rejection are:, , , , , ABO blood group, Human leucocyte antigens (HLA), Minor histocompatability antigens, , ABO Matching, ABO incompatibility will result in early organ rejection (hyperacute) because of pre existing, antibodies to other groups. Group O donors can give organs to any type of ABO recipient whereas, group AB donor can only donate to AB recipient.
Page 3716 :
HLA System, The four most important HLA alleles are:, , , , , , , HLA A, HLA B, HLA C, HLA DR, , An ideal organ match would be one in which all 8 alleles are matched (remember 2 from each, parent, four each = 8 alleles). Modern immunosuppressive regimes help to manage the potential, rejection due to HLA mismatching. However, the greater the number of mismatches the worse the, long term outcome will be. T lymphocytes will recognise antigens bound to HLA molecules and will, then become activated. Clonal expansion then occurs with a response directed against that antigen., Types of organ rejection, , , , , Hyperacute. This occurs immediately through presence of pre formed antibodies (such as, ABO incompatibility)., Acute. Occurs during the first 6 months and is usually T cell mediated. Usually tissue, infiltrates and vascular lesions., Chronic. Occurs after the first 6 months. Vascular changes predominate., , Hyperacute, Renal transplants at greatest risk and liver transplants at least risk. Although ABO incompatibility, and HLA Class I incompatible transplants will all fare worse in long term., Acute, All organs may undergo acute rejection. Mononuclear cell infiltrates predominate. All types of, transplanted organ are susceptible and it may occur in up to 50% cases., Chronic, Again all transplants with HLA mismatch may suffer this fate. Previous acute rejections and other, immunosensitising events all increase the risk. Vascular changes are most prominent with, myointimal proliferation leading to organ ischaemia. Organ specific changes are also seen such as, loss of acinar cells in pancreas transplants and rapidly progressive coronary artery disease in, cardiac transplants., Surgical overview-Renal transplantation, A brief overview of the steps involved in renal transplantation is given., Patients with end stage renal failure who are dialysis dependent or likely to become so in the, immediate future are considered for transplant. Exclusion criteria include; active malignancy, old age, (due to limited organ availability). Patients are medically optimised., Donor kidneys, these may be taken from live related donors and close family, members may have, less HLA mismatch than members of the general population. Laparoscopic donor nephrectomy, further minimises the operative morbidity for the donor. Other organs are typically taken from brain, dead or dying patients who have a cardiac arrest and in whom resuscitation is futile. The key event
Page 3717 :
is to minimise the warm ischaemic time in the donor phase., The kidney once removed is usually prepared on the bench in theatre by the transplant surgeon, immediately prior to implantation and factors such as accessory renal arteries and vessel length are, assessed and managed., For first time recipients the operation is performed under general anaesthesia. A RutherfordMorrison incision is made on the preferred side. This provides excellent extraperitoneal access to, the iliac vessels. The external iliac artery and vein are dissected out and following systemic, heparinisation are cross clamped. The vein and artery are anastamosed to the iliacs and the clamps, removed. The ureter is then implanted into the bladder and a stent is usually placed to maintain, patency. The wounds are then closed and the patient recovered from surgery., In the immediate phase a common problem encountered in cadaveric kidneys is acute tubular, necrosis and this tends to resolve., Graft survival times from cadaveric donors are typically of the order of 9 years and monozygotic twin, transplant (live donor) may survive as long as 25 years., Next question
Page 3718 :
A 52 year old female underwent a cadaveric renal transplant and recovers well post operatively. Her, immunosupression regime consists of tacrolimus. Which of the substances listed below should be, avoided?, , Paracetamol, , Apple juice, , Penicillin, , Prune juice, , Grapefruit juice, , Tacrolimus is metabolised by the P450 enzyme system. This is inhibited by a number of naturally, occurring substances, these include grapefruit, watercress and St.Johns Wort. These should all be, avoided in immunosupressed patients taking tacrolimus., Please rate this question:, , Discuss and give feedback, , Organ transplantation: immunosupressants, A number of drugs are available which help to mitigate the processes resulting in acute rejection., Cyclosporin and tacrolimus are commonly used drugs., Example regime, , , , , Initial: ciclosporin/tacrolimus with a monoclonal antibody, Maintenance: ciclosporin/tacrolimus with MMF or sirolimus, Add steroids if more than one steroid responsive acute rejection episode, , Ciclosporin, , , , , Inhibits calcineurin, a phosphatase involved in T cell activation, Nephrotoxic, Monitor levels
Page 3719 :
Azathioprine, , , , Metabolised to form 6 mercaptopurine which inhibits DNA synthesis and cell division, Side effects include myelosupression, alopecia and nausea, , Tacrolimus, , , , , Lower incidence of acute rejection compared to ciclosporin, Also less hypertension and hyperlipidaemia, However, high incidence of impaired glucose tolerance and diabetes, , Mycophenolate mofetil (MMF), , , , , Blocks purine synthesis by inhibition of IMPDH, Therefore inhibits proliferation of B and T cells, Side-effects: GI and marrow suppression, , Sirolimus (rapamycin), , , , Blocks T cell proliferation by blocking the IL-2 receptor, Can cause hyperlipidaemia, , Monoclonal antibodies, , , , , Selective inhibitors of IL-2 receptor, Daclizumab, Basilximab
Page 3720 :
Theme: Spinal disorders, , A., B., C., D., E., F., G., H., I., , Osteomyelitis, Potts disease of the spine, Scheuermanns disease, Transverse myelitis, Tabes dorsalis, Subacute degeneration of the cord, Brown-Sequard syndrome, Syringomyelia, Epidural haematoma, , Which is the most likely diagnosis for the scenario given. Each option may be used once, more than, once or not at all., , 1., , A 68 year old man presents to the plastics team with severe burns to his hands. He is not, distressed by the burns. He has bilateral charcot joints. On examination; there is loss of pain, and temperature sensation of the upper limbs., You answered Osteomyelitis, The correct answer is Syringomyelia, This patient has syringomyelia which selectively affects the spinotholamic tracts., Syringomyelia is a disorder in which a cystic cavity forms within the spinal cord. The, commonest variant is the Arnold- Chiari malformation in which the cavity connects with a, congenital malformation affecting the cerebellum. Acquired forms of the condition may, occur as a result of previous meningitis, surgery or tumours. Many neurological, manifestations have been reported, although the classical variety spares the dorsal columns, and medial lemniscus and affecting only the spinothalamic tract with loss of pain and, temperature sensation. The bilateral distribution of this patients symptoms would therefore, favor syringomyelia over SCID or Brown Sequard syndrome. Osteomyelitis would tend to, present with back pain and fever in addition to any neurological signs. Epidural haematoma, large enough to produce neurological impairment will usually have motor symptoms in, addition to any selective sensory loss, and the history is usually shorter., , 2., , A 24 year old man presents with localised spinal pain over 2 months which is worsened on, movement. He is known to be an IVDU. He has no history suggestive of tuberculosis. The, pain is now excruciating at rest and not improving with analgesia. He has a temperature of, 39 oC., Osteomyelitis, In an IVDU with back pain and pyrexia have a high suspicion for osteomylelitis. The most
Page 3721 :
likely organism is staph aureus and the cervical spine is the most common region affected., TB tends to affect the thoracic spine and in other causes of osteomyelitis the lumbar spine is, affected., 3., , A 22 year man is shot in the back, in the lumbar region. He has increased tone and hyperreflexia of his right leg. He cannot feel his left leg., You answered Osteomyelitis, The correct answer is Brown-Sequard syndrome, Theme from January 2012 exam, Brown -Sequard syndrome is caused by hemisection of the spinal cord. It may result from, stab injuries or lateral vertebral fractures. It results in ipsilateral paralysis (pyramidal tract) ,, and also loss of proprioception and fine discrimination (dorsal columns). Pain and, temperature sensation are lost on the contra-lateral side. This is because the fibres of the, spinothalamic tract have decussated below the level of the cord transection., , Please rate this question:, , Discuss and give feedback, , Next question, , Spinal disorders, Dorsal column lesion, , , , , Loss vibration and proprioception, Tabes dorsalis, SACD, , Spinothalamic tract, lesion, , , , Loss of pain, sensation and temperature, , Central cord lesion, , , , Flaccid paralysis of the upper limbs, , Osteomyelitis, , , , , , , Normally progressive, Staph aureus in IVDU, normally cervical region affected, Fungal infections in immunocompromised, Thoracic region affected in TB, , Infarction spinal cord, , , , Dorsal column signs (loss of proprioception and fine
Page 3723 :
Image sourced from Wikipedia
Page 3727 :
A 24 year old man is brought to the emergency department have suffered a crush injury to his, forearm. Assessment demonstrates that the arm is tender, red and swollen. There is clinical, evidence of an ulnar fracture and the patient cannot move their fingers. Which is the most, appropriate course of action?, , Application of an external fixation device, , Closed reduction, , Debridement, , Discharge and review in fracture clinic, , Fasciotomy, , Theme from April 2012, The combination of a crush injury, limb swelling and inability to move digits should raise suspicion of, a compartment syndrome that will require a fasciotomy. Paralysis is a very late sign., Please rate this question:, , Discuss and give feedback, , Next question, , Compartment syndrome, , , , This is a particular complication that may occur following fractures (or following ischaemia reperfusion injury in vascular patients). It is characterised by raised pressure within a closed, anatomical space., The raised pressure within the compartment will eventually compromise tissue perfusion, resulting in necrosis. The two main fractures carrying this complication include supracondylar, fractures and tibial shaft injuries., , Symptoms and signs, , , , , , , Pain, especially on movement (even passive), Parasthesiae, Pallor may be present, Arterial pulsation may still be felt as the necrosis occurs as a result of microvascular, compromise, Paralysis of the muscle group may occur
Page 3728 :
Diagnosis, , , Is made by measurement of intracompartmental pressure measurements. Pressures in, excess of 20mmHg are abnormal and >40mmHg is diagnostic., , Treatment, , , , , , , This is essentially prompt and extensive fasciotomies, In the lower limb the deep muscles may be inadequately decompressed by the, inexperienced operator when smaller incisions are performed, Myoglobinuria may occur following fasciotomy and result in renal failure and for this reason, these patients require aggressive IV fluids, Where muscle groups are frankly necrotic at fasciotomy they should be debrided and, amputation may have to be considered, Death of muscle groups may occur within 4-6 hours, Next question
Page 3729 :
Theme: Disorders of the knee, , A., B., C., D., E., F., G., , Chondromalacia patellae, Dislocated patella, Undisplaced fracture patella, Displaced patella fracture, Avulsion fracture of the tibial tubercle, Quadriceps tendon rupture, Osgood Schlatters disease, , Please select the most likely explanation for the scenario given. Each option may be used once,, more than once or not at all., , 5., , A 19 year old sportswoman presents with knee pain which is worse on walking down the, stairs and when sitting still. On examination there is wasting of the quadriceps and, pseudolocking of the knee., Chondromalacia patellae, A teenage girl with knee pain on walking down the stairs is characteristic for, chondromalacia patellae (anterior knee pain). Most cases are managed with physiotherapy., , 6., , A tall 18 year old male athlete is admitted to the emergency room after being hit in the knee, by a hockey stick. On examination his knee is tense and swollen. X-ray shows no fractures., You answered Chondromalacia patellae, The correct answer is Dislocated patella, A patella dislocation is a common cause of haemarthrosis and many will spontaneously, reduce when the leg is straightened. In the chronic setting physiotherapy is used to, strengthen the quadriceps muscles., , 7., , An athletic 15 year old boy presents with knee pain of 3 weeks duration. It is worst during, activity and settles with rest. On examination there is tenderness overlying the tibial, tuberosity and an associated swelling at this site., You answered Chondromalacia patellae, The correct answer is Osgood Schlatters disease, Athletic boys and girls may develop this condition in their teenage years. It is caused by, multiple micro fractures at the point of insertion of the tendon into the tibial tuberosity.
Page 3730 :
Most cases settle with physiotherapy and rest., Please rate this question:, , Discuss and give feedback, , Next question, , Knee injury, Types of injury, , , , , , , Sport injury, Mechanism: high twisting force applied to a bent knee, Typically presents with: loud crack, pain and RAPID joint, swelling (haemoarthrosis), Poor healing, Management: intense physiotherapy or surgery, , Ruptured posterior, cruciate ligament, , , , , , Mechanism: hyperextension injuries, Tibia lies back on the femur, Paradoxical anterior draw test, , Rupture of medial, collateral ligament, , , , , Mechanism: leg forced into valgus via force outside the leg, Knee unstable when put into valgus position, , Menisceal tear, , , , , , , Rotational sporting injuries, Delayed knee swelling, Joint locking (Patient may develop skills to "unlock" the knee, Recurrent episodes of pain and effusions are common, often, following minor trauma, , Chondromalacia, patellae, , , , Teenage girls, following an injury to knee e.g. Dislocation, patella, Typical history of pain on going downstairs or at rest, Tenderness, quadriceps wasting, , Ruptured anterior, cruciate ligament, , , , , Dislocation of the, patella, , , , Most commonly occurs as a traumatic primary event, either, through direct trauma or through severe contraction of, quadriceps with knee stretched in valgus and external rotation
Page 3731 :
, , , , , Genu valgum, tibial torsion and high riding patella are risk, factors, Skyline x-ray views of patella are required, although displaced, patella may be clinically obvious, An osteochondral fracture is present in 5%, The condition has a 20% recurrence rate, , , , 2 types:, , , , Fractured patella, , i. Direct blow to patella causing undisplaced fragments, ii. Avulsion fracture, Tibial plateau fracture, , , , , , , Occur in the elderly (or following significant trauma in young), Mechanism: knee forced into valgus or varus, but the knee, fractures before the ligaments rupture, Varus injury affects medial plateau and if valgus injury, lateral, plateau depressed fracture occurs, Classified using the Schatzker system (see below), , Schatzker Classification system for tibial plateau fractures, , Type, , Anatomical description, , Features, , 1, , Vertical split of lateral, condyle, , Fracture through dense bone, usually in the young. It may be, virtually undisplaced, or the condylar fragment may be, pushed inferiorly and tilted, , 2, , Vertical split of the lateral, condyle combined with an, adjacent load bearing part, of the condyle, , The wedge fragment (which may be of variable size), is, displaced laterally; the joint is widened. Untreated, a valgus, deformity may develop, , 3, , Depression of the articular, surface with intact condylar, rim, , The split does not extend to the edge of the plateau., Depressed fragments may be firmly embedded in, subchondral bone, the joint is stable, , 4, , Fragment of the medial, tibial condyle, , Two injuries are seen in this category; (1) a depressed, fracture of osteoporotic bone in the elderly. (2) a high, energy fracture resulting in a condylar split that runs from, the intercondylar eminence to the medial cortex. Associated
Page 3732 :
Type, , Anatomical description, , Features, , ligamentous injury may be severe, , 5, , Fracture of both condyles, , Both condyles fractured but the column of the metaphysis, remains in continuity with the tibial shaft, , 6, , Combined condylar and, subcondylar fractures, , High energy fracture with marked comminution, , Next question
Page 3733 :
An 8 year old boy presents with symptoms of right knee pain. The pain has been present on most, occasions for the past three months and the pain typically lasts for several hours at a time. On, examination; he walks with an antalgic gait and has apparent right leg shortening. What is the most, likely diagnosis?, , Perthes Disease, , Osteosarcoma of the femur, , Osteoarthritis of the hip, , Transient synovitis of the hip, , Torn medial meniscus, , Theme from September 2012 Exam, There are many causes of the irritable hip in the 10-14 year age group. Many of these may cause, both hip pain or knee pain. Transient synovitis of the hip the commonest disorder but does not, typically last for 3 months. An osteosarcoma would not usually present with apparent limb shortening, unless pathological fracture had occurred. A slipped upper femoral epiphysis can cause a similar, presentation although it typically presents later and with different patient characteristics., Please rate this question:, , Discuss and give feedback, , Next question, , Perthes disease, Perthes disease, , , , Idiopathic avascular necrosis of the femoral epiphysis of the femoral head, Impaired blood supply to femoral head, causing bone infarction. New vessels develop and, ossification occurs. The bone either heals or a subchondral fracture occurs., , Clinical features, , , , , Males 4x's greater than females, Age between 2-12 years (the younger the age of onset, the better the prognosis), Limp
Page 3734 :
, , , Hip pain, Bilateral in 20%, , Diagnosis, Plain x-ray, Technetium bone scan or magnetic resonance imaging if normal x-ray and symptoms, persist., Catterall staging, , Stage, , Features, , Stage 1, , Clinical and histological features only, , Stage 2, , Sclerosis with or without cystic changes and preservation of the articular surface, , Stage 3, , Loss of structural integrity of the femoral head, , Stage 4, , Loss of acetabular integrity, , Management, , , , , , To keep the femoral head within the acetabulum: cast, braces, If less than 6 years: observation, Older: surgical management with moderate results, Operate on severe deformities, , Prognosis, Most cases will resolve with conservative management. Early diagnosis improves outcomes., Next question
Page 3735 :
Which of the following types of growth plate fractures may have similar radiological appearances?, , Salter Harris types 1 and 5, , Salter Harris types 4 and 5, , Salter Harris types 3 and 5, , Salter Harris types 1 and 2, , Salter Harris types 1 and 3, Mnemonic: SALTER, S (Type 1): Straight through the growth plate, A (Type 2): Above - through growth plate and Above involving the metaphysis, L (Type 3): Lower -through growth plate and beLow involving the epiphysis, T (Type 4):Through - Through both metaphysis, epiphysis and growth plate, E (Type 5): Everything - Crush / compression injury, R (Type 5): Ruined, As recommended by one of our users, , Salter Harris injury types 1 and 5 (transverse fracture through growth plate Vs. Compression, fracture) may mimic each other radiologically. Type 5 injuries have the worst outcomes. Radiological, signs of type 5 injuries are subtle and may include narrowing of the growth plate., Please rate this question:, , Discuss and give feedback, , Next question, , Epiphyseal fractures
Page 3736 :
Fractures involving the growth plate in children are classified using the Salter - Harris system., There are 5 main types., Salter Harris Classification, , Type, , Description, , Type 1, , Transverse fracture through the growth plate, , Type 2, , Fracture through the growth plate to the metaphysis (commonest type), , Type 3, , Fracture through the growth plate and the epiphysis with metaphysis spared, , Type 4, , Fracture involving the growth plate, metaphysis and epiphysis, , Type 5, , Compression fracture of the growth plate (worst outcome), , Management, Non displaced type 1 injuries can generally be managed conservatively. Unstable or more extensive, injuries will usually require surgical reduction and/ or fixation, as proper alignment is crucial., Next question
Page 3737 :
Theme: Pathological fractures, , A., B., C., D., E., F., G., , Osteosarcoma, Osteomalacia, Osteoporosis, Metastatic carcinoma, Osteoblastoma, Giant cell tumour, Ewing's sarcoma, , For each pathological fracture please select the most likely aetiology for the scenario given. Each, option may be used once, more than once or not at all., , 10., , A 30 year old woman presents with pain and swelling of the left shoulder. There is a large, radiolucent lesion in the head of the humerus extending to the subchondral plate., You answered Osteosarcoma, The correct answer is Giant cell tumour, Giant cell tumours on x-ray have a 'soap bubble' appearance. They present as pain or, pathological fractures. They commonly metastasize to the lungs., , 11., , A 72 year old woman has a lumbar vertebral crush fracture. She has hypocalcaemia and a, low urinary calcium., You answered Osteosarcoma, The correct answer is Osteomalacia, Hypocalcemia and low urinary calcium are biochemical features of osteomalacia., Unfortunately surgeons do need to look at some blood results!, , 12., , A 16 year old boy presents with severe groin pain after kicking a football. Imaging, confirms a pelvic fracture. A previous pelvic x-ray performed 2 weeks ago shows a lytic, lesion with 'onion type' periosteal reaction., You answered Osteosarcoma, The correct answer is Ewing's sarcoma, A Ewings sarcoma is most common in males between 10-20 years. It can occur in girls. A, lytic lesion with a lamellated or onion type periosteal reaction is a classical finding on x-
Page 3738 :
rays. Most patients present with metastatic disease with a 5 year prognosis between 510%., Please rate this question:, , Discuss and give feedback, , Next question, , Pathological fractures, , , A pathological fracture occurs in abnormal bone due to insignificant injury, , Causes, , Metastatic tumours, , , , , , , , Breast, Lung, Thyroid, Renal, Prostate, , Bone disease, , , , , , , Osteogenesis imperfecta, Osteoporosis, Metabolic bone disease, Paget's disease, , Local benign conditions, , , , , Chronic osteomyelitis, Solitary bone cyst, , Primary malignant tumours, , , , , , Chondrosarcoma, Osteosarcoma, Ewing's tumour, Next question
Page 3739 :
An 8 year old boy falls onto an outstretched hand and is brought to the emergency department. He is, examined by a doctor and a bony injury is cleared clinically. He re-presents a week later with pain in, his hand. What is the most likely underlying injury?, , Fracture of the distal radius, , Fracture of the scaphoid, , Dislocation of the lunate, , Rupture of flexor pollicis longus tendon, , Bennett's fracture, , Theme from January 2013 Exam, Scaphoid fractures in children are rare, will usually involve the distal pole and are easily missed. The, initial clinical examination (and sometimes x-rays) may be normal and repeated clinical examination, and imaging is advised for this reason. Whilst the other injuries may be sustained from a fall onto an, outstretched hand they are less likely to be overlooked on clinical examination. In the case of a, Bennetts fracture, the injury mechanism is less compatible with this type of injury., Please rate this question:, , Discuss and give feedback, , Next question, , Scaphoid fractures, , , , , , , , Scaphoid fractures are the commonest carpal fractures., Surface of scaphoid is covered by articular cartilage with small area available for blood, vessels (fracture risks blood supply), Forms floor of anatomical snuffbox, Risk of fracture associated with fall onto outstretched hand (tubercle, waist, or proximal third), Ulnar deviation AP needed for visualization of scaphoid, Immobilization of scaphoid fractures difficult, , Management, , Non-displaced fractures, , - Casts or splints, - Percutaneous scaphoid fixation
Page 3740 :
Displaced fracture, , Surgical fixation, usually with a screw, , Complications, , , , , , Non union of scaphoid, Avascular necrosis of the scaphoid, Scapholunate disruption and wrist collapse, Degenerative changes of the adjacent joint, Next question
Page 3741 :
Theme: Shoulder injuries, , A., B., C., D., E., F., G., , Glenohumeral dislocation, Acromioclavicular dislocation, Sternoclavicular dislocation, Biceps tendon tear, Supraspinatus tear, Fracture of the surgical neck of the humerus, Infra spinatus tear, , For each scenario please select the most likely underlying diagnosis. Each option may be used, once, more than once or not at all., , 14., , A 23 year old rugby player falls directly onto his shoulder. There is pain and swelling of, the shoulder joint. The clavicle is prominent and there appears to be a step deformity., You answered Glenohumeral dislocation, The correct answer is Acromioclavicular dislocation, Acromioclavicular joint (ACJ) dislocation normally occurs secondary to direct injury to, the superior aspect of the acromion. Loss of shoulder contour and prominent clavicle are, key features. Note; rotator cuff tears rarely occur in the second decade., , 15., , A 22 year old man falls over and presents to casualty. A shoulder x-ray is performed, the, radiologist comments that a Hill-Sachs lesion is present., Glenohumeral dislocation, A Hill-Sachs lesion occurs when the cartilage surface of the humerus is in contact with the, rim of the glenoid. About 50% of anterior glenohumeral dislocations are associated with, this lesion., , 16., , An 82 year old female presents to A&E after tripping on a step. She complains of shoulder, pain. On examination there is pain to 90o on abduction., You answered Glenohumeral dislocation, The correct answer is Supraspinatus tear, A supraspinatus tear is the most common of rotator cuff tears. It occurs as a result of, degeneration and is rare in younger adults.
Page 3742 :
Please rate this question:, , Discuss and give feedback, , Next question, , Shoulder disorders, Shoulder fractures and dislocations, Fractures, Proximal humerus, Background, , , , , Third most common fragility fracture in the elderly., Results from low energy fall in predominantly elderly females, or from high energy trauma in, young males., Can be associated with nerve injury (commonly axillary), and fracture-dislocation of the, humeral head. Detailed neurological assessment is essential for all upper limb injuries., , Anatomy, Osteology, Consists of articular head, greater tuberosity, lesser tuberosity, metaphysis and diaphysis. Between, the articular head and the tuberosities is the anatomical neck (previous physis). Between the, tuberosities and the metaphysis is the surgical neck., The supraspinatus, infraspinatus and teres minor muscles attach to the greater tuberosity. The, subscapularis muscle attaches to the lesser tuberosity., Vascular Supply, Humeral head is supplied by the anterior and posterior humeral circumflex arteries. Anatomical neck, fractures are at greatest risk of osteonecrosis., Imaging, Imaging aims to both delineate the fracture pattern, and confirm/exlude the presence of an, associated dislocation., , , , Radiographs - True anteroposterior (AP), axillary lateral and/or scapula Y view., CT - indicated to better define intra-articular involvement and to aid pre-operative planning., MRI is not useful for fracture imaging., , Classification, Description of the fracture is often more useful than classification. Particular attention should be paid, to humeral alignment, fracture displacement, and greater tuberosity position (rotator cuff will pull the, GT supero-posterioly, which can cause impingement problems with malunion)., - Neer Classification: Most commonly used. Describes fracture as 2,3,or 4 part depending upon the, number main fragments. Also comments on the degree of displacement. Fragments:, -greater tuberosity, -lesser tuberosity, - articular surface
Page 3743 :
- shaft, Displacement: >1cm or angulation >45 degrees., Treatment, The vast majority of proximal humeral fractures are minimally displaced, and therefore can be, managed conservatively. This involves immobilisation in a polysling, and progressive mobilisation., Pendular exercise can commence at 14 days, and active abduction from 4-6 weeks., Irreducible fracture dislocation is an indication for operative management. Other indications include, large displacement, younger patient, head splitting (intra-articular fractures). However, the recent, PROFHER trial (1) has suggested no benefit to operative intervention on patient outcome (it must be, applied cautiously as majority of patients were elderly with extraarticular fractures). Options available, for surgical management include:, , ORIF, , Most commonly used. Plate and screw fixation. Can reconstruct, complex fractures., , Intramedullary nail, , Suitable for extra-articular configuration, predominantly surgical neck, +/- GT fractures., , Hemiarthroplasty, , Used for un-reconstructable fractures in the older patient who has good, glenoid quality., , Total shoulder, arthroplasty, , Unconstructable fractures where high functioning shoulder is required, (hemiarthroplasty will cause glenoid erosion), , Reverse shoulder, arthroplasty, , Total shoulder arthroplasty that provides better functional outcome than, conventional total shoulder replacement., , Scapula, Background, Uncommon fractures usually associated with high energy trauma. Most commonly involve scapula, body or spine (50%), glenoid fossa and glenoid neck. Important to exclude associated life, threatening injury., Imaging, Plain radiographs should include true anteroposterior (AP), axillary lateral and/or scapula Y view. CT, scanning is useful for defining intra-articular involvement, displacement and for three dimensional, reconstruction., Classification, Based on the location of the fracture (coracoid, acromion, glenoid neck, glenoid fossa, scapula
Page 3744 :
body). Beware of ipsilateral glenoid neck and clavicle fracture -floating shoulder - where limb is, effectively dissociated from axial skeleton., Treatment, The vast majority of scapula fractures are amenable to conservative management, consisting of, sling immobilisation for two weeks followed by early rehabilitation. Floating shoulder will usually, require fixation, and consideration of surgery should also be given to intra-articular and, displaced/angulated glenoid fractures., Dislocations, Types, Dislocations around the shoulder joint include glenohumeral dislocation, acromioclavicular joint, disruption and sternoclavicular dislocation. Only glenohumeral dislocation will be covered here., Glenohumeral dislocation, Diagnosis, classification and management are covered here., Background, Shoulder dislocation is commonly seen in A&E. It has a high recurrence rate that is as high as 80%, in teenagers. Initial management requires emergent reduction to prevent lasting chondral damage., Early assessment and management, Usually a traumatic cause (multi-directional instability in frequent dislocations requires discussion, with orthopaedics and is not covered here). Careful history, examination and documentation of, neurovascular status of the limb, in particular the axillary nerve (regimental badge sensation). This, should be re-assessed post manipulation. Early radiographs to confirm direction of dislocation., Initial management consists of emergent closed reduction under under entanox and analgesia, but, often requires conscious sedation. Arm should then be immobilised in a polysling, and XR to confirm, relocation., Imaging - True anteroposterior (AP), axillary lateral and/or scapula Y view. Reduced humeral head, should lie between acromion and coracoid on lateral/scapula view., Types, , Direction, , Features, , Cause, , Examination, , Reduction, techniques, , Anterior, , Most, Common, >90%, , Usually traumatic - anterior, force on arm when shoulder, is abducted, eternally, rotated, , Loss of shoulder, contour - sulcus sign., Humeral head can be, felt anteriorly., , Hippocratic., Milch., Stimson., Kocher not, advised due to, complication of, fracture
Page 3745 :
Reduction, techniques, , Direction, , Features, , Cause, , Examination, , Posterior, , 50%, missed in, A&E, , 50% traumatic, but, classically post seizure or, electrocution, , Shoulder locked in, internal rotation. XR, may show lightbulb, appearance., , Gentle lateral, traction to, adducted arm., , Inferior, , Rare, , Associated with pectorals, and rotator cuff tears, and, glenoid fracture, , As for primary injury, , Management of, primary injury, , Rare, , Associated with, acrominon/clavicle fracture, , As for primary injury, , Management of, primary injury, , Superior, , Associated injuries, , , , , , , Bankart lesion - avulsion of the anterior glenoid labrum with an anterior shoulder dislocation, (reverse Bankart if poster labrum in posterior dislocation)., Hill Sachs defect - chondral impaction on posteriosuperior humeral head from contact with, gleonoid rim. Can be large enough to lock shoulder, requiring open reduction. (Reverse Hill, Sachs in posterior dislocation)., Rotator cuff tear - increases with age., Greater or lesser tuberosity fracture - increases with age., Humeral neck fracture - shoulder fracture dislocation. More common in high energy trauma, and elderly. Should be discussed with orthopaedics prior to any attempted reduction., , Rotator Cuff Disease, Rotator cuff disease is a spectrum of conditions that ranges from subacromial impingement to rotator, cuff tears and eventually to rotator cuff arthropathy (arthritis)., Anatomy, The rotator cuff is a group of four muscles that are important in shoulder movements, and, maintenance of glenohumeral stability., , Muscle, , Scapular, attachment, , Humeral, attachment, , Action, , Innervation
Page 3746 :
Scapular, attachment, , Humeral, attachment, , Supraspinatus, , Supraspinatus, fossa, , Infraspinatus, , Muscle, , Action, , Innervation, , Superior facet of, greater tuberosity, , Initiation of, abduction of, humerus, , Suprascapular nerve, , Infraspinatus, fossa, , Posterior facet of, greater tuberosity, , External rotation, of humerus, , Suprascapular nerve, , Teres Minor, , Lateral border, , Inferior facet of, greater tuberosity, , External rotation, of humerus, , Axillary Nerve, , Subscapularis, , Subscapular, fossa, , Lesser tuberosity, , Internal rotation, of humerus, , Upper and lower, subscapular nerve, , , , , The inferior rotator cuff muscles (infraspinatus, teres minor, and subscapularis) balance the, superior pull of the deltoid. Injury/tear results in upward migration of the humeral head on the, glenoid (can be seen on AP radiograph)., Likewise, the anterior muscles (subscapularis) are balanced with the posterior muscles, (infraspinatus, teres minor)., , Subacromial Impingement, , , , , , The most common cause of shoulder pain, which results from impingement of the superior, cuff on the undersurface of the acromion, and an inflammatory bursitis., Associated with certain types of acromial morphology (Bigliani classification)., Presents as insidious pain which is exacerbated by overhead activities., , Rotator Cuff Tear, , , , , Often presents as an acute event on the background of chronic subacromial impingement in, the older patient, but can present as an avulsion injury in younger patients., Majority of tears are to the superior cuff (supraspinatus, infraspinatus, teres minor), though a, tear to subscapularis is associated with subcoracoid impingement.
Page 3747 :
, , Tears present as pain and weakness when using the muscles in question., , Rotator Cuff Arthropathy, , , , , Defined as shoulder arthritis in the setting of rotator cuff dysfunction. Results from superior, migration due to the loss of rotator cuff function and integrity. Unopposed deltoid pulls the, humeral head superiorly., Associated with massive chronic cuff tears., , Imaging, Plain radiographs, , , , AP of the shoulder may show superior migration of the humerus with a cuff tear, and features, of arthritis with arthropathy. Other causes of pain may also be identified (e.g. calcific, tendonitis/fracture), Outlet view is useful for defining the acromial morphology, , USS, , , Allows dynamic imaging of the cuff, and is inexpensive. However, it is very user dependent., , MRI, , , , Best imaging modality for cuff pathology., Also allows imaging of the rest of the shoulder. When intra-articular pathology is suspected,, can be combined with an arthrogram for improved sensitivity and specificity., , Treatment, Subacromial impingement, , , , , Physiotherapy, oral anti-inflammatory medication, Subacromial steroid injection can settle inflammation, Arthroscopic subacromial decompression by shaving away the undersurface of the, acromion, more space is created for the rotator cuff. Cuff integrity is assessed also at time of, surgery, and can be repaired if necessary., , Rotator cuff tear
Page 3748 :
, , , , When considering repair of a cuff tear, the age and activity of the patient, the nature of the, tear (degenerative vs. acute traumatic), and the size and retraction of the tear should be, considered when making a surgical plan., Mild tears or tears in the elderly can be managed conservatively, as outlined above., Moderate tears can be repaired arthroscopically. Massive or retracted tears will often require, an open repair (occasionally with a tendon transfer). Subacromial decompression is, performed at the same time to reduce impingement, symptoms and recurrence., , Calcific tendonitis, Calcific tendonitis involves calcific deposits within tendons anywhere in the body, but most, commonly in the rotator cuff (specifically the supraspinatus tendon). When present in the shoulder, it, is associated with subacromial impingement and pain., Pathology, , , , More common in women aged 30-60 years., Association with diabetes and hypothyroidism, , There are three stages of calcification, , , , , Formative phase characterized by calcific deposits, Resting phase deposit is stable, but presents with impingement problems, Resorptive phase phagocytic resorption. Most painful stage., , Presentation, , , Similar in presentation to subacromial impingement, with pain especially with over head, activities. Atraumatic in nature., , Imaging, , , Plain radiographs show calcification of the rotator cuff, usually within 1.5cm of its insertion on, the humerus. Supraspinatus outlet views can show level of impingment. Further imaging is, rarely needed., , Treatment, , , , Non-operative NSAIDS, steroid injection (controversial, but practiced) and physiotherapy., Approximately 75% will resolve by 6 months with conservative management., Ultrasound guided or surgical needle barbotage can break down deposits and resolve, symptoms. Occasionally surgical excision is required.
Page 3749 :
Adhesive capsulitis (Frozen Shoulder), , , , , Pain and loss of movement of shoulder joint, which involves fibroplastic proliferation of, capsular tissue, causing soft tissue scarring and contracture. Patients present with a painful, and decreased arc of motion., Associated with prolonged immobilization, previous surgery, thyroid disorders (AI) and, diabetes, Classically three stages which can take up to two years to resolve:, , Stage one the freezing and painful stage, Stage two the frozen and stiff stage, Stage three the thawing stage, where shoulder movement slowly improves, Imaging, , , , Plain radiographs to exclude other causes of a painful shoulder, MRI arthrogram may show capsular contracture, and again may be used to exclude cuff, pathology. However, often not performed as diagnosis is largely clinical., , Treatment, , , , Non-operative NSAIDS, steroid injection and physiotherapy. Patience is required as, condition can take up to 2 years to improve., Operative MUA or arthroscopic adhesiolysis (release of adhesions) can expedite recovery,, followed by intensive physiotherapy., , Glenohumeral Arthritis, Shoulder arthritis presents with the normal symptoms of arthritis, however primary osteoarthritis is, not as commonly the primary cause as seen in other large joints.. A large proportion of shoulder, arthritis is rheumatoid (RA), post traumatic, or secondary to rotator cuff arthropathy (discussed, above)., Treatment, , , Surgical options include hemiarthroplasty, total shoulder replacement and reverse geometry, total shoulder replacement (used when rotator cuff function is absent)., , References, 1. JAMA. 2015;313(10):1037-1047. doi:10.1001/jama.2015.1629, Next question
Page 3750 :
Which of the following statements relating to menisceal tears is false?, , The medial meniscus is most often affected, , True locking of the knee joint may occur, , Most established tears will heal with conservative management, , In the chronic setting there is typically little to find on examination if the knee is not, locked, An arthroscopic approach may be used to treat most lesions, , Menisci have no nerve or blood supply and thus heal poorly. Established tears with associated, symptoms are best managed by arthroscopic menisectomy., Please rate this question:, , Discuss and give feedback, , Next question, , Knee injury, Types of injury, , , , , , , Sport injury, Mechanism: high twisting force applied to a bent knee, Typically presents with: loud crack, pain and RAPID joint, swelling (haemoarthrosis), Poor healing, Management: intense physiotherapy or surgery, , Ruptured posterior, cruciate ligament, , , , , , Mechanism: hyperextension injuries, Tibia lies back on the femur, Paradoxical anterior draw test, , Rupture of medial, collateral ligament, , , , Mechanism: leg forced into valgus via force outside the leg, , Ruptured anterior, cruciate ligament
Page 3751 :
, , Knee unstable when put into valgus position, , Menisceal tear, , , , , , , Rotational sporting injuries, Delayed knee swelling, Joint locking (Patient may develop skills to "unlock" the knee, Recurrent episodes of pain and effusions are common, often, following minor trauma, , Chondromalacia, patellae, , , , Teenage girls, following an injury to knee e.g. Dislocation, patella, Typical history of pain on going downstairs or at rest, Tenderness, quadriceps wasting, , , , , Dislocation of the, patella, , , , , , , Most commonly occurs as a traumatic primary event, either, through direct trauma or through severe contraction of, quadriceps with knee stretched in valgus and external rotation, Genu valgum, tibial torsion and high riding patella are risk, factors, Skyline x-ray views of patella are required, although displaced, patella may be clinically obvious, An osteochondral fracture is present in 5%, The condition has a 20% recurrence rate, , , , 2 types:, , , , , Fractured patella, , i. Direct blow to patella causing undisplaced fragments, ii. Avulsion fracture, Tibial plateau fracture, , , , , , , Occur in the elderly (or following significant trauma in young), Mechanism: knee forced into valgus or varus, but the knee, fractures before the ligaments rupture, Varus injury affects medial plateau and if valgus injury, lateral, plateau depressed fracture occurs, Classified using the Schatzker system (see below), , Schatzker Classification system for tibial plateau fractures, , Type, , Anatomical description, , Features
Page 3752 :
Type, , Anatomical description, , Features, , 1, , Vertical split of lateral, condyle, , Fracture through dense bone, usually in the young. It may be, virtually undisplaced, or the condylar fragment may be, pushed inferiorly and tilted, , 2, , Vertical split of the lateral, condyle combined with an, adjacent load bearing part, of the condyle, , The wedge fragment (which may be of variable size), is, displaced laterally; the joint is widened. Untreated, a valgus, deformity may develop, , 3, , Depression of the articular, surface with intact condylar, rim, , The split does not extend to the edge of the plateau., Depressed fragments may be firmly embedded in, subchondral bone, the joint is stable, , 4, , Fragment of the medial, tibial condyle, , Two injuries are seen in this category; (1) a depressed, fracture of osteoporotic bone in the elderly. (2) a high, energy fracture resulting in a condylar split that runs from, the intercondylar eminence to the medial cortex. Associated, ligamentous injury may be severe, , 5, , Fracture of both condyles, , Both condyles fractured but the column of the metaphysis, remains in continuity with the tibial shaft, , 6, , Combined condylar and, subcondylar fractures, , High energy fracture with marked comminution, , Next question
Page 3753 :
Theme: Developmental bone disorders, , A., B., C., D., E., F., G., H., I., J., , Rickets, Craniocleidodysostosis, Achondroplasia, Scurvy, Pagets disease, Multiple myeloma, Osteogenesis imperfecta, Osteomalacia, Osteopetrosis, None of the above, , Please select the most likely disease process to account for the clinical scenario. Each option may, be used once, more than once or not at all., , 18., , A 15 year-old boy presents to the out-patient clinic with tiredness, recurrent throat and, chest infections, and gradual loss of vision. Multiple x-rays show brittle bones with no, differentiation between the cortex and the medulla., You answered Rickets, The correct answer is Osteopetrosis, Osteopetrosis is an autosomal recessive condition. It is commonest in young adults. They, may present with symptoms of anaemia or thrombocytopaenia due to decreased marrow, space. Radiology reveals a lack of differentiation between the cortex and the medulla, described as marble bone. These bones are very dense and brittle., , 19., , A 12 year-old boy who is small for his age presents to the clinic with poor muscular, development and hyper-mobile fingers. His x-rays show multiple fractures of the long, bones and irregular patches of ossification., You answered Rickets, The correct answer is Osteogenesis imperfecta, Osteogenesis imperfecta is caused by defective osteoid formation due to congenital, inability to produce adequate intercellular substances like osteoid, collagen and dentine., There is a failure of maturation of collagen in all the connective tissues.Radiology may, show translucent bones, multiple fractures, particularly of the long bones, wormian bones, (irregular patches of ossification) and a trefoil pelvis., , 20., , A 1 year-old is brought to the Emergency Department with a history of failure to thrive.
Page 3754 :
On examination, the child is small for age and has a large head. X-ray shows a cupped, appearance of the epiphysis of the wrist., Rickets, Rickets is the childhood form of osteomalacia. It is due to the failure of the osteoid to, ossify due to vitamin D deficiency. Symptoms start about the age of one. The child is, small for age and there is a history of failure to thrive. Bony deformities include bowing of, the femur and tibia, a large head, deformity of the chest wall with thickening of the, costochondral junction (rickettary rosary), and a transverse sulcus in the chest caused by, the pull of the diaphragm (Harrison's sulcus). X- Rays show widening and cupping of the, epiphysis of the long bones, most readily apparent in the wrist., Please rate this question:, , Discuss and give feedback, , Next question, , Paediatric fractures, Paediatric fracture types, , Type, , Injury pattern, , Complete fracture, , Both sides of cortex are breached, , Toddlers fracture, , Oblique tibial fracture in infants, , Plastic deformity, , Stress on bone resulting in deformity without cortical disruption, , Greenstick fracture, , Unilateral cortical breach only, , Buckle fracture, , Incomplete cortical disruption resulting in periosteal haematoma only, , Growth plate fractures, In paediatric practice fractures may also involve the growth plate and these injuries are classified, according to the Salter- Harris system (given below):
Page 3755 :
Type, , Injury pattern, , I, , Fracture through the physis only (x-ray often normal), , II, , Fracture through the physis and metaphysis, , III, , Fracture through the physis and epiphyisis to include the joint, , IV, , Fracture involving the physis, metaphysis and epiphysis, , V, , Crush injury involving the physis (x-ray may resemble type I, and appear normal), , As a general rule it is safer to assume that growth plate tenderness is indicative of an underlying, fracture even if the x-ray appears normal. Injuries of Types III, IV and V will usually require surgery., Type V injuries are often associated with disruption to growth., Non accidental injury, , , , , , , , Delayed presentation, Delay in attaining milestones, Lack of concordance between proposed and actual mechanism of injury, Multiple injuries, Injuries at sites not commonly exposed to trauma, Children on the at risk register, , Pathological fractures, Genetic conditions, such as osteogenesis imperfecta, may cause pathological fractures., Osteogenesis imperfecta, , , , , Defective osteoid formation due to congenital inability to produce adequate intercellular, substances like osteoid, collagen and dentine., Failure of maturation of collagen in all the connective tissues., Radiology may show translucent bones, multiple fractures, particularly of the long bones,, wormian bones (irregular patches of ossification) and a trefoil pelvis., , Subtypes
Page 3756 :
, , , , , Type I The collagen is normal quality but insufficient quantity., Type II- Poor collagen quantity and quality., Type III- Collagen poorly formed. Normal quantity., Type IV- Sufficient collagen quantity but poor quality., , Osteopetrosis, , , , , , Bones become harder and more dense., Autosomal recessive condition., It is commonest in young adults., Radiology reveals a lack of differentiation between the cortex and the medulla described as, marble bone., Next question
Page 3757 :
Theme: Hip fractures, , A. Conservative management, B. Percutaneous pinning, C. Fracture reduction and internal fixation, D. Hemiarthroplasty, E. Total hip replacement, F. Dynamic hip screw, G. Intramedullary femoral nail, , For each scenario please select the most appropriate management option. Each option may be used, once, more than once or not at all., , 21., , A 60 year old male is admitted to A&E with a fall. He lives with his wife and still works as a, restaurant manager. He has a past history of benign prostatic hypertrophy and is currently taking, tamsulosin. He is otherwise fit and healthy. On examination there is right hip tenderness on, movement in all directions. A hip x-ray confirms an intertrochanteric fracture., You answered Conservative management, The correct answer is Dynamic hip screw, The blood supply to the femoral head may be intact and the fracture should heal with, compression type devices such as gamma nails or dynamic hip screws. The latter device being the, most commonly performed therapeutic intervention., , 22., , An 86 year old retired pharmacist is admitted to A&E following a fall. She complains of right hip, pain. She is known to have hypertension and is currently on bendrofluazide. She lives alone and, mobilises with a Zimmer frame. Her right leg is shortened and externally rotated. A hip x-ray, confirms a displaced intracapsular fracture., You answered Conservative management
Page 3758 :
The correct answer is Hemiarthroplasty, Hemiarthroplasty is offered to older, less mobile individuals compared to fracture reduction and, fixation in younger patients., , 23., , A 74 year old male is admitted to A&E with a fall. He is known to have rheumatoid arthritis and is, on methotrexate and paracetamol. He lives alone in a bungalow and enjoys playing golf. He is, independent with his ADLs. He complains of left groin pain, therefore has a hip x-ray which, confirms a displaced intracapsular fracture., You answered Conservative management, The correct answer is Total hip replacement, This patient has pre-existing joint disease, good level of activity and a relatively high life, expectancy, therefore THR is preferable to hemiarthroplasty., , Please rate this question:, , Discuss and give feedback, , Next question, , Hip fractures, Background, Neck of femur (NOF) fracture is a common orthopaedic presentation, with over 65000 fractures in, the UK per year. Like many orthopaedic injuries, there is a bimodal age distribution. It is imperative, to distinguish between the high energy injury in a young patient, and the low energy osteoporotic, fracture in the elderly, as their management aims are very different:, Young patient - Usually high energy trauma (e.g road traffic accident, horse riding) and needs, treating in accordance with Advanced Trauma Life Support (ATLS) principles. Will often have, associated injuries. Aim is to retain the patients own anatomy, and optimise their function., Elderly patient - Predominantly female, fall from standing height (fragility fracture). Often patients, have multiple comorbidities that will ultimately dictate their prognosis. Aim of orthopaedic treatment
Page 3759 :
is to immediately regain patient mobility so that morbidity (infection, thromboembolic events,, pressure sores etc) and mortality associated with prolonged bed rest is avoided. Left untreated, a, neck of femur fracture can be considered a terminal event. Historically, mortality associated with, elderly hip fracture is 10% at one month, and 30% at one year. However, this has been improved in, the UK with the introduction of multidisciplinary, orthogeriatric lead care and the National Hip, Fracture Database and Best Practice Tariff., Pertinent anatomy, Osteology - normal neck-shaft angle is 130 +/- 7 degrees, and 10 +/- 7 degrees of neck anteversion., Vascular supply - The predominant blood supply to the femoral head and neck is from the medial, and lateral femoral circumflex arteries (branches of profunda femoris). These anastomose and, pierce the joint capsule at the base of the neck, mainly posteriorly. There is a small vascular, contribution from the artery of the ligament teres. Understanding the blood supply is fundamental to, the decision making process in treating NOF fractures., Presentation and initial management, Typically, patients present with pain in the hip/groin, a shortened, abducted, externally rotated leg, (due to the unopposed pull of the muscles that act across the hip joint) and the inability to straightleg-raise. With undisplaced fractures, signs are more subtle., High energy injuries should be treated in line with ATLS principles. All patients should be fluid, resuscitated, have adequate pain relief (often with a fascio-iliiaca nerve block), and be optimised for, surgery. In addition, elderly patients should be assessed by an orthogeriatrician., Imaging, Anteroposterior and cross-table lateral plain radiographs are sufficient to diagnose the majority of, NOF fractures. If the fracture extends below the level of the lesser trochanter, or there is any, possibility of pathological fracture, full length femur views are essential to plan surgery., Where there is a high index of suspicion of fracture, but plain radiographs are inconclusive, gold, standard investigation is MRI. However, if unavailable within 24 hours, or if the patient will not, tolerate MRI, CT is appropriate. The majority of fractures can be seen with modern CT techniques,, and so this is becoming first line in many hospitals., Classification, There has been a move away from named classification systems towards descriptive classification, systems., Two main types of NOF exist: Intra-capsular, and extra-capsular. Extra-capsular fractures are further, divided into pertrochanteric or subtrochanteric (within 5cm distal to the lesser trochanter). All, fractures are then described as undisplaced, minimally displaced, or displaced., Femoral neck and head blood supply disruption is common with intracapsular NOF fractures, and, rare with extracapsular fractures. This fundamental principle underpins the practise of arthroplasty, for intracapsular fractures, and fixation for extracapsular fractures., If you wish to use a named classification system, the most commonly used are below:, Elderly intracapsular - Garden Classification, Young intrasapsular - Pauvels Classification
Page 3760 :
Intertrochanteric - Evans, Subtrochanteric - Russell Taylor, Treatment, In general, NOF fractures are treated operatively except if the patient is deemed unlikely to survive, an anaesthetic. Best Practice Tarif (BPT) dictates that surgery should happen within 36 hours, as, delay of greater than 48 hours is associated with increased morbidity and mortality. Below are, suggested algorithms for the treatment of NOF. There are some areas of debate/controversy which, are detailed below., , Image sourced from Wikipedia, , * The priority with the young patient is to retain the femoral head if possible, even with a displaced, intracapsular fracture. The risk of avascular necrosis and non-union (and therefore revision surgery), associated with internal fixation needs weighing up against the sequelae of total hip replacement in, the young (wear, dislocation, revision). Discussion is necessary with the patient, on a case by case, basis., ** Undisplaced fractures in the elderly can be treated with internal fixation, often with cannulated, screws. This is appropriate for valgus impacted subcapital fractures which are inherently stable, to, prevent secondary displacement. This does still carry the risk of AVN or non-union, and therefore a, future revision. For this reason, many surgeons advocate arthroplasty as a single surgery., *** NICE guidance - patients who fulfil these criteria should be offered total hip replacement which, conveys better function and prosthetic survivorship, compared with hemiarthroplasty, but at an, increased risk of dislocation.
Page 3761 :
Image sourced from Wikipedia, , * Intertrochanteric fractures vary greatly in their stability. If the trochanter (and therefore lateral wall),, and medial calcar is in tact, then the fracture configuration bears stability. This can be treated with a, DHS, as collapse of the fracture is predictable. Where either or both structures are involved in the, fracture, stability becomes compromised and many surgeons will favour using an intramedullary, device. This is an ongoing debate, and difficult to test in an exam setting., Post operative management, Patients should be mobilised fully weight bearing where possible. Care is multidisciplinary in its, delivery. Elderly patients should have orthogeriatrician assessment of comorbidity, and bone health, with secondary prevention measures if appropriate. There should be early involvement of, physiotherapy and occupational therapy services. For further guidance see sources listed below., NICE clinical guidance on hip fracture: https://www.nice.org.uk/guidance/cg124, Best Practice Tarif:, www.nhfd.co.uk/20/hipfractureR.../Best%20Practice%20Tariff%20User%20Guide.pdf, National Hip Fracture Database: www.nhfd.co.uk/, Next question
Page 3762 :
Of the list below, which is not a cause of avascular necrosis?, , Steroids, , Sickle cell disease, , Radiotherapy, , Myeloma, , Caisson disease, Causes of avascular necrosis, P ancreatitis, L upus, A lcohol, S teroids, T rauma, I diopathic, infection, C aisson disease, collagen vascular disease, R adiation, rheumatoid arthritis, A myloid, G aucher disease, S ickle cell disease, Steroid containing therapy for myeloma may induce avascular necrosis, however the disease itself, does not cause it. Caisson disease as may occur in deep sea divers is a recognised cause., Please rate this question:, , Discuss and give feedback, , Next question, , Avascular necrosis, , , , , , , Cellular death of bone components due to interruption of the blood supply, causing bone, destruction, Main joints affected are hip, scaphoid, lunate and the talus., It is not the same as non union. The fracture has usually united., Radiological evidence is slow to appear., Vascular ingrowth into the affected bone may occur. However, many joints will develop, secondary osteoarthritis.
Page 3763 :
Causes, P ancreatitis, L upus, A lcohol, S teroids, T rauma, I diopathic, infection, C aisson disease, collagen vascular disease, R adiation, rheumatoid arthritis, A myloid, G aucher disease, S ickle cell disease, Presentation, Usually pain. Often despite apparent fracture union., Investigation, MRI scanning will show changes earlier than plain films., Treatment, In fractures at high risk sites anticipation is key. Early prompt and accurate reduction is essential., Non weight bearing may help to facilitate vascular regeneration., Joint replacement may be necessary, or even the preferred option (e.g. Hip in the elderly)., Next question
Page 3764 :
Which of the following is the first radiological change likely to be apparent in a plain radiograph of a, 12 year old presenting with suspected Perthes disease, , Multiple bone cysts, , Sclerosis of the femoral head, , Loss of bone density, , Joint space narrowing, , Collapse of the femoral head, , In Catterall stage I disease there may be no radiological abnormality at all. In Stage II disease there, may be sclerosis of the femoral head., Indication for treatment (aide memoire):Half a dozen, half a head, Those aged greater than 6 years with >50% involvement of the femoral head should almost always, be treated., Please rate this question:, , Discuss and give feedback, , Next question, , Perthes disease, Perthes disease, , , , Idiopathic avascular necrosis of the femoral epiphysis of the femoral head, Impaired blood supply to femoral head, causing bone infarction. New vessels develop and, ossification occurs. The bone either heals or a subchondral fracture occurs., , Clinical features, , , , , , , Males 4x's greater than females, Age between 2-12 years (the younger the age of onset, the better the prognosis), Limp, Hip pain, Bilateral in 20%
Page 3765 :
Diagnosis, Plain x-ray, Technetium bone scan or magnetic resonance imaging if normal x-ray and symptoms, persist., Catterall staging, , Stage, , Features, , Stage 1, , Clinical and histological features only, , Stage 2, , Sclerosis with or without cystic changes and preservation of the articular surface, , Stage 3, , Loss of structural integrity of the femoral head, , Stage 4, , Loss of acetabular integrity, , Management, , , , , , To keep the femoral head within the acetabulum: cast, braces, If less than 6 years: observation, Older: surgical management with moderate results, Operate on severe deformities, , Prognosis, Most cases will resolve with conservative management. Early diagnosis improves outcomes., Next question
Page 3766 :
A footballer is injured in a match and is being assessed in the outpatient department. On, examination he has a positive valgus stress test and minimal joint effusion. What is the most likely, underlying injury?, , Injury to the lateral collateral ligament, , Injury to the medial collateral ligament, , Injury to the anterior cruciate ligament, , Injury to the posterior cruciate ligament, , Injury to the patellar tendon, , Theme from January 2013 Exam, A knee injury in the footballer with a positive valgus stress test is usually associated with MCL injury., Please rate this question:, , Discuss and give feedback, , Next question, , Knee collateral ligament, Anatomy, The tibial collateral ligament is a broad, flat band. Its upper end has an extensive attachment to the, medial epicondyle of the femur with some fibres projecting onto the adductor magnus tendon. The, ligament passes downwards and forwards to the medial side of the tibia. The deepest fibres are, fused with the medial meniscus., The fibular collateral ligament is round and cord like and stands clear of the thin, lateral part of the, fibrous capsule. It is enclosed within the fascia lata. It passes from the lateral epicondyle of the, femur to the head of the fibula in front of its highest point and splits the tendon of biceps femoris. On, the lateral side of the joint the fibres are short and weak and bridge the interval between the femoral, and tibial condyles. The popliteus tendon intervenes between the lateral meniscus and the capsule.
Page 3767 :
The tibial and fibular collateral ligaments prevent disruption of the joint at the sides. They are most, tightly stretched in extension, and then their direction- the fibular ligament downwards and, backwards, the tibial downwards and forwards- prevents rotation of the tibia laterally or the femur, medially. Rotation may be demonstrated in the flexed knee., Injury, The collateral ligaments are commonly injured, the medial is most often affected. It requires a, significant force such as sporting tackle or motor vehicle to strike the side of the leg. Associated, injuries to both the tibial plateau or menisci are not uncommon., Grading and treatment, , Grade of, injury, , Features, , Treatment, , 1, , Minor tearing of ligament fibres, Negative instability tests, , Conservative (analgesia and, physiotherapy), , 2, , Ligament laxity (seen with knee in, 30oflexion), Knee stable when joint extended, , Usually splinting or casting for 4-6 weeks, , 3, , Ligament completely torn, Joint instability, , Surgical ligament reconstruction, , Next question
Page 3768 :
Theme: Upper limb injuries, , A., B., C., D., E., F., G., H., I., , Pulled elbow, Fracture of the coronoid process, Scaphoid fracture, Fracture of the distal humerus, Bennets fracture, Fracture of the shaft of the radius and ulnar, Galeazzi fracture, Fracture of the olecranon, Fracture of the radial head, , Please select the most likely injury for the scenario given. Each option may be used once, more than, once or not at all., , 27., , A 32 year old man presents with a painful swelling over the volar aspect of his hand after, receiving a hard blow to his palm. On examination, he experiences pain on moving the, wrist and on longitudinal compression of the thumb., You answered Pulled elbow, The correct answer is Scaphoid fracture, Scaphoid fractures usually occur as a result of direct hard blow to the palm or following a, fall on the out-stretched hand. The main physical signs are swelling and tenderness in the, anatomical snuff box, and pain on wrist movements and on longitudinal compression of, the thumb, , 28., , A 26 year old man presents to the emergency department with a swelling over his left, elbow after a fall on an outstretched hand. On examination, he has tenderness over the, proximal part of his forearm, and has severely restricted supination and pronation, movements., You answered Pulled elbow, The correct answer is Fracture of the radial head, Fracture of the radial head is common in young adults. It is usually caused by a fall on the, outstretched hand. On examination, there is marked local tenderness over the head of the, radius, impaired movements at the elbow, and a sharp pain at the lateral side of the elbow, at the extremes of rotation (pronation and supination)., , 29., , A 56 year old lady presents with a painful swelling over the lower end of the forearm, following a fall. Imaging reveals a distal radial fracture with disruption of the distal radio-
Page 3769 :
ulnar joint., You answered Pulled elbow, The correct answer is Galeazzi fracture, Galeazzi fractures occur after a fall on the hand with a rotational force superimposed on it., On examination, there is bruising, swelling and tenderness over the lower end of the, forearm. X- Rays reveal a displaced fracture of the radius and a prominent ulnar head due, to dislocation of the inferior radio-ulnar joint., Please rate this question:, , Discuss and give feedback, , Next question, , Upper limb fractures, Colles' fracture, , , , , Fall onto extended outstretched hands, Described as a dinner fork type deformity, Classical Colles' fractures have the following 3 features:, , Features of the injury, 1. Transverse fracture of the radius, 2. 1 inch proximal to the radio-carpal joint, 3. Dorsal displacement and angulation, Smith's fracture (reverse Colles' fracture), , , , Volar angulation of distal radius fragment (Garden spade deformity), Caused by falling backwards onto the palm of an outstretched hand or falling with wrists, flexed, , Bennett's fracture, , , , , Intra-articular fracture of the first carpometacarpal joint, Impact on flexed metacarpal, caused by fist fights, X-ray: triangular fragment at ulnar base of metacarpal
Page 3770 :
Monteggia's fracture, , , , , Dislocation of the proximal radioulnar joint in association with an ulna fracture, Fall on outstretched hand with forced pronation, Needs prompt diagnosis to avoid disability, , Galeazzi fracture, , , , , , Radial shaft fracture with associated dislocation of the distal radioulnar joint, Occur after a fall on the hand with a rotational force superimposed on it., On examination, there is bruising, swelling and tenderness over the lower end of the, forearm., X Rays reveal the displaced fracture of the radius and a prominent ulnar head due to, dislocation of the inferior radio-ulnar joint., , Barton's fracture, , , , Distal radius fracture (Colles'/Smith's) with associated radiocarpal dislocation, Fall onto extended and pronated wrist, , Scaphoid fractures, , , , , , , , , Scaphoid fractures are the commonest carpal fractures., Surface of scaphoid is covered by articular cartilage with small area available for blood, vessels (fracture risks blood supply), Forms floor of anatomical snuffbox, Risk of fracture associated with fall onto outstretched hand (tubercle, waist, or proximal 1/3), The main physical signs are swelling and tenderness in the anatomical snuff box, and pain, on wrist movements and on longitudinal compression of the thumb., Ulnar deviation AP needed for visualization of scaphoid, Immobilization of scaphoid fractures difficult, , Radial head fracture, , , , , Fracture of the radial head is common in young adults., It is usually caused by a fall on the outstretched hand., On examination, there is marked local tenderness over the head of the radius, impaired, movements at the elbow, and a sharp pain at the lateral side of the elbow at the extremes of, rotation (pronation and supination)., Next question
Page 3771 :
Theme: Hand injuries, , A., B., C., D., E., F., G., , Admission and surgical debridement, Application of futura splint and fracture clinic review, Application of tubigrip bandage and fracture clinic review, Admission for open reduction and fixation, Discharge with reassurance, Commence oral prednisolone, Commence oral diclofenac, , Which of the following options is the best management plan? Each option may be used once, more, than once or not at all., , 30., , A 42 year old skier falls and impacts his hand on his ski pole. On examination he is tender, in the anatomical snuffbox and on bimanual palpation. X-rays with scaphoid views show, no evidence of fracture., You answered Admission and surgical debridement, The correct answer is Application of futura splint and fracture clinic review, A fracture may still be present and should be immobilised until repeat imaging can be, performed. If clinical suspicion persists then subsequent imaging should be with MRI, scanning or CT if MRI is contra-indicated., , 31., , A 43 year old man falls over landing on his left hand. Although there was anatomical, snuffbox tenderness no x-rays either at the time or subsequently have shown evidence of, scaphoid fracture. He has been immobilised in a futura splint for two weeks and is now, asymptomatic., You answered Admission and surgical debridement, The correct answer is Discharge with reassurance, This patient is at extremely low risk of having sustained a scaphoid injury and may be, discharged., , 32., , A builder falls from scaffolding and lands on his left hand he suffers a severe laceration to, his palm. An x-ray shows evidence of scaphoid fracture that is minimally displaced., Admission and surgical debridement, This is technically an open fracture and should be debrided prior to attempted fixation
Page 3772 :
(which should occur soon after)., Scaphoid fractures:, 80% of all carpal fractures, 80% occur in men, 80% occur at the waist of the scaphoid, Please rate this question:, , Discuss and give feedback, , Next question, , Scaphoid fractures, , , , , , , , Scaphoid fractures are the commonest carpal fractures., Surface of scaphoid is covered by articular cartilage with small area available for blood, vessels (fracture risks blood supply), Forms floor of anatomical snuffbox, Risk of fracture associated with fall onto outstretched hand (tubercle, waist, or proximal third), Ulnar deviation AP needed for visualization of scaphoid, Immobilization of scaphoid fractures difficult, , Management, , Non-displaced fractures, , - Casts or splints, - Percutaneous scaphoid fixation, , Displaced fracture, , Surgical fixation, usually with a screw, , Complications, , , , , , Non union of scaphoid, Avascular necrosis of the scaphoid, Scapholunate disruption and wrist collapse, Degenerative changes of the adjacent joint, Next question
Page 3773 :
Theme: Paediatric orthopaedics, , A. Musculoskeletal pain, B. Congenital dysplasia of the hip, C. Slipped upper femoral epiphysis, D. Transient synovitis, E. Septic arthritis, F. Perthes disease, G. Tibial fracture, , Please select the most likely diagnosis for the scenario given. Each option may be used once, more, than once or not at all., , 33., , A 4 year boy presents with an abnormal gait. He has a history of recent viral illness. His WCC is 11, and ESR is 30., You answered Musculoskeletal pain, The correct answer is Transient synovitis, Viral illnesses can be associated with transient synovitis. The WCC should ideally be > 12 and the, ESR > 40 to suggest septic arthritis., , 34., , A 6 year old boy presents with groin pain. He is known to be disruptive in class. He reports that he, is bullied for being short. On examination he has an antalgic gait and pain on internal rotation of, the right hip., You answered Musculoskeletal pain, The correct answer is Perthes disease, This child is short, has hyperactivity (disruptive behaviour) and is within the age range for Perthes
Page 3774 :
disease. Hyperactivity and short stature are associated with Perthes disease., , 35., , An obese 12 year old boy is referred with pain in the left knee and hip. On examination he has an, antaglic gait and limitation of internal rotation. His knee has normal range of passive and active, movement., You answered Musculoskeletal pain, The correct answer is Slipped upper femoral epiphysis, Similar theme to September 2012 Exam, Slipped upper femoral epiphysis is commonest in obese adolescent males. The x-ray will show, displacement of the femoral epiphysis inferolaterally. Treatment is usually with rest and non, weight bearing crutches., , Beware of attributing gait disorders to benign processes in young children without careful clinical and, radiological assessment., , Please rate this question:, , Discuss and give feedback, , Next question, , Paediatric orthopaedics, Diagnosis, , Mode of presentation, , Treatment, , Radiology, , Developmental, dysplasia of the, hip, , Usually diagnosed in infancy, by screening tests. May be, bilateral, when disease is, unilateral there may be leg, length inequality. As, disease progresses child, , Splints and harnesses or, traction. In later years, osteotomy and hip, realignment procedures may, be needed. In arthritis a joint, replacement may be needed., , Initially no obvious, change on plain films, and USS gives best, resolution until 3, months of age. On, plain films Shentons
Page 3775 :
may limp and then early, onset arthritis. More, common in extended, breech babies., , However, this is best, deferred if possible as it will, almost certainly require, revision, , line should form a, smooth arc, , Perthes Disease, , Hip pain (may be referred, to the knee) usually, occurring between 5 and 12, years of age. Bilateral, disease in 20%., , Remove pressure from joint, to allow normal, development. Physiotherapy., Usually self-limiting if, diagnosed and treated, promptly., , X-rays will show, flattened femoral, head. Eventually in, untreated cases the, femoral head will, fragment., , Slipped upper, femoral, epiphysis, , Typically seen in obese, male adolescents. Pain is, often referred to the knee., Limitation to internal, rotation is usually seen., Knee pain is usually present, 2 months prior to hip, slipping. Bilateral in 20%., , Bed rest and non-weight, bearing. Aim to avoid, avascular necrosis. If severe, slippage or risk of it occurring, then percutaneous pinning of, the hip may be required., , X-rays will show the, femoral head displaced, and falling, inferolaterally (like a, melting ice cream, cone) The Southwick, angle gives indication, of disease severity, , Next question
Page 3776 :
Theme: Eponymous fractures, , A., B., C., D., E., F., G., , Smith's, Bennett's, Monteggia's, Colles', Galeazzi, Pott's, Barton's, , Link the most appropriate eponymously named fracture to the scenario described. Each scenario, may be used once, more than once or not at all., , 36., , A 28 year old man falls on the back of his hand. On x-ray he has a fractured distal radius, demonstrating volar displacement of the fracture., Smith's, This is a Smith fracture (reverse Colles' fracture); unlike a Colles' this is a high velocity, injury and may require surgical correction. Note that Colles' fractures are usually dorsally, displaced., , 37., , A 38 year old window cleaner falls from his ladder. He lands on his left arm and notices an, obvious injury. An x-ray and clinical examination demonstrate that he has a fracture of the, proximal ulna and associated radial dislocation., You answered Smith's, The correct answer is Monteggia's, This constellation of injuries is referred to as a Monteggia's fracture., , 38., , A 32 year old man falls from scaffolding and sustains an injury to his forearm. Clinical, examination and x-ray shows that he has sustained a radial fracture with dislocation of the, inferior radio-ulna joint., You answered Smith's, The correct answer is Galeazzi, Isolated fracture of the radius alone can occur but is rare. Always check for associated, injury.
Page 3777 :
Please rate this question:, , Discuss and give feedback, , Next question, , Eponymous fractures, Colles' fracture (dinner fork deformity), , , , Fall onto extended outstretched hand, Classical Colles' fractures have the following 3 features:, , 1. Transverse fracture of the radius, 2. 1 inch proximal to the radio-carpal joint, 3. Dorsal displacement and angulation, Smith's fracture (reverse Colles' fracture), , , , Volar angulation of distal radius fragment (Garden spade deformity), Caused by falling backwards onto the palm of an outstretched hand or falling with wrists, flexed, , Bennett's fracture, , , , , Intra-articular fracture of the first carpometacarpal joint, Impact on flexed metacarpal, caused by fist fights, X-ray: triangular fragment at ulnar base of metacarpal
Page 3778 :
Image sourced from Wikipedia, , Monteggia's fracture, , , , , Dislocation of the proximal radioulnar joint in association with an ulna fracture, Fall on outstretched hand with forced pronation, Needs prompt diagnosis to avoid disability
Page 3779 :
Image sourced from Wikipedia, , Galeazzi fracture, , , , Radial shaft fracture with associated dislocation of the distal radioulnar joint, Direct blow, , Pott's fracture, , , , Bimalleolar ankle fracture, Forced foot eversion, , Barton's fracture, , , , , Distal radius fracture (Colles'/Smith's) with associated radiocarpal dislocation, Fall onto extended and pronated wrist, Involvement of the joint is a defining feature, Next question
Page 3780 :
A 54-year-old man presents to the Emergency Department with a 2 day history of a swollen, painful, left knee. You aspirate the joint to avoid admission to the orthopaedic wards. Aspirated joint fluid, shows calcium pyrophosphate crystals. Which of the following blood tests is most useful in revealing, an underlying cause?, , Transferrin saturation, , ACTH, , ANA, , Serum ferritin, , LDH, , This is a typical presentation of pseudogout. An elevated transferrin saturation may indicate, haemochromatosis, a recognised cause of pseudogout., A high ferritin level is also seen in haemochromatosis but can be raised in a variety of infective and, inflammatory processes, including pseudogout, as part of an acute phase response., Please rate this question:, , Discuss and give feedback, , Next question, , Pseudogout, Pseudogout is a form of microcrystal synovitis caused by the deposition of calcium pyrophosphate, dihydrate in the synovium, Risk factors, , , , , , , , hyperparathyroidism, hypothyroidism, haemochromatosis, acromegaly, low magnesium, low phosphate, Wilson's disease
Page 3781 :
Features, , , , , knee, wrist and shoulders most commonly affected, joint aspiration: weakly-positively birefringent rhomboid shaped crystals, x-ray: chondrocalcinosis, , Management, , , , aspiration of joint fluid, to exclude septic arthritis, NSAIDs or intra-articular, intra-muscular or oral steroids as for gout, Next question
Page 3782 :
A 19 year old soldier has just returned from a prolonged marching exercise and presents with a, sudden onset, severe pain, in the forefoot. Clinical examination reveals tenderness along the second, metatarsal. Plain x-rays are taken of the area, these demonstrate callus surrounding the shaft of the, second metatarsal. What is the most likely diagnosis?, , Stress fracture, , Mortons neuroma, , Osteochondroma, , Acute osteomyelitis, , Freiberg's disease, , Theme from 2011 Exam, A short history of pain together with clinical examination and radiological signs affecting the second, metatarsal favour a stress fracture. The fact that callus is present suggests that immobilisation is, unlikely to be beneficial. Freibergs disease is an anterior metatarsalgia affecting the head of the, second metarsal, it typically occurs in the pubertal growth spurt. The initial injury was thought to be, due to stress microfractures at the growth plate. The key feature in the history which distinguishes, the injury as being stress fracture is the radiology. In Freibergs disease the x-ray changes include;, joint space widening, formation of bony spurs, sclerosis and flattening of the metatarsal head., Please rate this question:, , Discuss and give feedback, , Next question, , Stress fractures, Repetitive activity and loading of normal bone may result in small hairline fractures. Whilst these, may be painful they are seldom displaced. Surrounding soft tissue injury is unusual. They may, present late following the injury, in which case callus formation may be identified on radiographs.
Page 3783 :
Such cases may not require formal immobilisation, injuries associated with severe pain and, presenting at an earlier stage may benefit from immobilisation tailored to the site of injury., Next question
Page 3784 :
A 65-year-old Asian female presents with an extracapsular neck of femur fracture. Investigations, show:, Calcium, , 2.07 mmol/l (2.20-2.60 mmol/l), , Phosphate, , 0.66 mmol/l (0.8-1.40 mmol/l), , ALP, , 256 IU/l (44-147 IU/l), , What is the most likely diagnosis?, , Bone tuberculosis, , Hypoparathyroidism, , Myeloma, , Osteomalacia, , Paget's disease, Osteomalacia, , , , low: calcium, phosphate, raised: alkaline phosphatase, , The low calcium and phosphate combined with the raised alkaline phosphatase point towards, osteomalacia., Please rate this question:, , Discuss and give feedback, , Next question, , Osteomalacia, Basics, , , , normal bony tissue but decreased mineral content, rickets if when growing
Page 3785 :
, , osteomalacia if after epiphysis fusion, , Types, , , , , , , vitamin D deficiency e.g. malabsorption, lack of sunlight, diet, renal failure, drug induced e.g. anticonvulsants, vitamin D resistant; inherited, liver disease, e.g. cirrhosis, , Features, , , , rickets: knock-knee, bow leg, features of hypocalcaemia, osteomalacia: bone pain, fractures, muscle tenderness, proximal myopathy, , Investigation, , , , , low calcium, phosphate, 25(OH) vitamin D, raised alkaline phosphatase, x-ray: children - cupped, ragged metaphyseal surfaces; adults - translucent bands (Looser's, zones or pseudofractures), , Treatment, , , calcium with vitamin D tablets, Next question
Page 3786 :
A 78-year-old woman is discharged following a fractured neck of femur. On review she is making, good progress but consideration is given to secondary prevention of further fractures. Unfortunately, the orthogeriatricians are all on annual leave and the consultant has asked you to arrange suitable, management. Which is the best option?, , Alendronate, , Alendronate, calcium and vitamin D supplementation, , Strontium, , Arrange a DEXA scan, , Hormone replacement therapy, , A bisphosphonate, calcium and vitamin D supplementation should be given to all patients aged over, 75 years after having a fracture. A DEXA scan is only needed of the patient is aged below 75 years., Hormone replacement therpay has been shown to reduce vertebral and non vertebral fractures,, however the risks of cardiovascular disease and breast malignancy make this a less favourable, option., Please rate this question:, , Discuss and give feedback, , Next question, , Osteoporosis: secondary prevention, NICE guidelines were updated in 2008 on the secondary prevention of osteoporotic fractures in, postmenopausal women., Key points include, , , , , , Treatment is indicated following osteoporotic fragility fractures in postmenopausal women, who are confirmed to have osteoporosis (a T-score of - 2.5 SD or below)., In women aged 75 years or older, a DEXA scan may not be required 'if the responsible, clinician considers it to be clinically inappropriate or unfeasible', Vitamin D and calcium supplementation should be offered to all women unless the clinician is, confident they have adequate calcium intake and are vitamin D replete, Alendronate is first-line
Page 3787 :
, , , Around 25% of patients cannot tolerate alendronate, usually due to upper gastrointestinal, problems. These patients should be offered risedronate or etidronate (see treatment criteria, below), Strontium ranelate and raloxifene are recommended if patients cannot tolerate, bisphosphonates (see treatment criteria below), , Supplementary notes on treatment, Bisphosphonates, , , , , Alendronate, risedronate and etidronate are all licensed for the prevention and treatment of, post-menopausal and glucocorticoid-induced osteoporosis, All three have been shown to reduce the risk of both vertebral and non-vertebral fractures, although alendronate, risedronate may be superior to etidronate in preventing hip fractures, Ibandronate is a once-monthly oral bisphosphonate, , Vitamin D and calcium, , , Poor evidence base to suggest reduced fracture rates in the general population at risk of, osteoporotic fractures - may reduce rates in frail, housebound patients, , Raloxifene - selective oestrogen receptor modulator (SERM), , , , , , , Has been shown to prevent bone loss and to reduce the risk of vertebral fractures, but has, not yet been shown to reduce the risk of non-vertebral fractures, Has been shown to increase bone density in the spine and proximal femur, May worsen menopausal symptoms, Increased risk of thromboembolic events, May decrease risk of breast cancer, , Strontium ranelate, , , , , 'Dual action bone agent' - increases deposition of new bone by osteoblasts and reduces the, resorption of bone by osteoclasts, Strong evidence base, may be second-line treatment in near future, Increased risk of thromboembolic events, , Next question
Page 3788 :
Which of the following statements relating to avascular necrosis is false?, , When associated with fracture may occur despite the radiological evidence of fracture, union., Pain and stiffness will typically precede radiological evidence of the condition., , Drilling of affected bony fragments may be used to facilitate angiogenesis where, arthroplasty is not warranted., The earliest detectable radiological evidence is a radiolucency of the affected area, coupled with subchondral collapse., It is less likely when prompt anatomical alignment of fracture fragments is achieved., Avascular necrosis- radiological changes occur late., Radiolucency and subchondral collapse are late changes. The earliest evidence on plain films is the, affected area appearing as being more radio-opaque due to hyperaemia and resorption of the, neighboring area. It may be diagnosed earlier using bone scans and MRI., Please rate this question:, , Discuss and give feedback, , Next question, , Avascular necrosis, , , , , , , Cellular death of bone components due to interruption of the blood supply, causing bone, destruction, Main joints affected are hip, scaphoid, lunate and the talus., It is not the same as non union. The fracture has usually united., Radiological evidence is slow to appear., Vascular ingrowth into the affected bone may occur. However, many joints will develop, secondary osteoarthritis., , Causes, P ancreatitis, L upus, A lcohol, S teroids, T rauma, I diopathic, infection
Page 3789 :
C aisson disease, collagen vascular disease, R adiation, rheumatoid arthritis, A myloid, G aucher disease, S ickle cell disease, Presentation, Usually pain. Often despite apparent fracture union., Investigation, MRI scanning will show changes earlier than plain films., Treatment, In fractures at high risk sites anticipation is key. Early prompt and accurate reduction is essential., Non weight bearing may help to facilitate vascular regeneration., Joint replacement may be necessary, or even the preferred option (e.g. Hip in the elderly)., Next question
Page 3790 :
Theme: Diseases affecting the spine, , A., B., C., D., E., F., G., H., I., , Spondylolysis, Spina bifida occulta, Spondylolisthesis, Meningomyelocele, Meningocele, Scoliosis - non structural, Scoliosis, Ankylosing spondylitis, Scheuermann's disease, , Please select the most likely underlying diagnosis for the condition described. Each condition may, be used once, more than once or not at all., , 44., , A 19 year old female is involved in an athletics event. She has just completed the high, jump when she suddenly develops severe back pain and weakness affecting both her legs., on examination she has a prominent sacrum and her lower back is painful., You answered Spondylolysis, The correct answer is Spondylolisthesis, Theme from September 2012 Exam, Young athletic females are the group most frequently affected by spondylolythesis who, have a background of spondylolysis. Whilst the latter condition is a risk factor for, spondylolythesis the former condition is most likely in a young athletic female who, presents with sudden pain., , 45., , A 15 year old boy is brought to the clinic by his mother who is concerned that he has a, mark overlying his lower spine. On examination the boy has a patch of hair overlying his, lower lumbar spine and a birth mark at the same location. Lower limb neurological, examination is normal., You answered Spondylolysis, The correct answer is Spina bifida occulta, Spina bifida occulta is a common condition and may affect up to 10% of the population., The more severe types of spina bifida have more characteristic skin changes. Occasionally, the unwary surgeon is persuaded to operate on these "cutaneous" changes and we would, advocate performing an MRI scan prior to any such surgical procedure in this region., , 46., , A 19 year old female presents to the clinic with progressive pain in her neck and back. The
Page 3791 :
condition has been progressively worsening over the past 6 months. She has not presented, previously because she was an inpatient with a disease flare of ulcerative colitis. On, examination she has a stiff back with limited spinal extension on bending forwards., You answered Spondylolysis, The correct answer is Ankylosing spondylitis, Ankylosing spondylitis is associated with HLA B27, there is a strong association with, ulcerative colitis in such individuals. The clinical findings are usually of a kyphosis, affecting the cervical and thoracic spine. Considerable symptomatic benefit may be, obtained using non steroidal anti inflammatory drugs. These should be used carefully in, patients with inflammatory bowel disease who may be taking steroids., Please rate this question:, , Discuss and give feedback, , Next question, , Diseases affecting the vertebral column, Ankylosing, spondylitis, , , , , , , , Scheuermann's, disease, , , , , , , , , Scoliosis, , , , , Chronic inflammatory disorder affecting the axial skeleton, Sacro-ilitis is a usually visible in plain films, Up to 20% of those who are HLA B27 positive will develop the, condition, Affected articulations develop bony or fibrous changes, Typical spinal features include loss of the lumbar lordosis and, progressive kyphosis of the cervico-thoracic spine, Epiphysitis of the vertebral joints is the main pathological process, Predominantly affects adolescents, Symptoms include back pain and stiffness, X-ray changes include epiphyseal plate disturbance and anterior, wedging, Clinical features include progressive kyphosis (at least 3 vertebrae, must be involved), Minor cases may be managed with physiotherapy and analgesia,, more severe cases may require bracing or surgical stabilisation, Consists of curvature of the spine in the coronal plane, Divisible into structural and non structural, the latter being
Page 3792 :
, , , , , Spina bifida, , , , , , , , , , Spondylolysis, , , , , , , Spondylolisthesis, , , , , , , commonest in adolescent females who develop minor postural, changes only. Postural scoliosis will typically disappear on, manoeuvres such as bending forwards, Structural scoliosis affects > 1 vertebral body and is divisible into, idiopathic, congential and neuromuscular in origin. It is not, correctable by alterations in posture, Within structural scoliosis, idiopathic is the most common type, Severe, or progressive structural disease is often managed surgically, with bilateral rod stabilisation of the spine, Non fusion of the vertebral arches during embryonic development, Three categories; myelomeningocele, spina bifida occulta and, meningocele, Myelomeningocele is the most severe type with associated, neurological defects that may persist in spite of anatomical closure of, the defect, Up to 10% of the population may have spina bifida occulta, in this, condition the skin and tissues (but not not bones) may develop over, the distal cord. The site may be identifiable by a birth mark or hair, patch, The incidence of the condition is reduced by use of folic acid, supplements during pregnancy, Congenital or acquired deficiency of the pars interarticularis of the, neural arch of a particular vertebral body, usually affects L4/ L5, May be asymptomatic and affects up to 5% of the population, Spondylolysis is the commonest cause of spondylolisthesis in, children, Asymptomatic cases do not require treatment, This occurs when one vertebra is displaced relative to its immediate, inferior vertebral body, May occur as a result of stress fracture or spondylolysis, Traumatic cases may show the classic "Scotty Dog" appearance on, plain films, Treatment depends upon the extent of deformity and associated, neurological symptoms, minor cases may be actively monitored., Individuals with radicular symptoms or signs will usually require, spinal decompression and stabilisation, Next question
Page 3793 :
Theme: Management of fractures, , A., B., C., D., E., F., , Discharge home with arm sling and fracture clinic appointment, Discharge home with futura splint and fracture clinic appointment, Admit for open reduction and fixation, Fasciotomy, Active observation for progression of neurovascular compromise, Reduction of fracture in casualty and application of plaster backslab,, followed by discharge home., , Please select the most appropriate immediate management for the fracture scenarios given. Each, option may be used once, more than once or not at all., , 47., , A 22 year old rugby player falls onto an outstretched hand and sustains a fracture of the, distal radius. The x-ray shows a dorsally angulated comminuted fracture., You answered Discharge home with arm sling and fracture clinic appointment, The correct answer is Admit for open reduction and fixation, Unlike an osteoporotic fracture in an elderly lady this is a high velocity injury and will, require surgical fixation., , 48., , A 10 year old boy undergoes a delayed open reduction and fixation of a significantly, displaced supracondylar fracture. On the ward he complains of significant forearm pain, and paraesthesia of the hand. Radial pulse is normal., You answered Discharge home with arm sling and fracture clinic appointment, The correct answer is Fasciotomy, The delay is the significant factor here. These injuries often have neurovascular, compromise and inactivity now places him at risk of developing complications. In, compartment syndrome the loss of arterial pulsation occurs late., , 49., , A 28 year old man falls onto an outstretched hand. On examination there is tenderness of, the anatomical snuffbox. However, forearm and hand x-rays are normal., You answered Discharge home with arm sling and fracture clinic appointment, The correct answer is Discharge home with futura splint and fracture clinic, appointment
Page 3794 :
This could well be a scaphoid fracture and should be temporarily immobilised pending, further review. A futura splint will immobilise better than an arm sling for this problem., Please rate this question:, , Discuss and give feedback, , Next question, , Fracture management, , , , , Bony injury resulting in a fracture may arise from trauma (excessive forces applied to bone),, stress related (repetitive low velocity injury) or pathological (abnormal bone which fractures, during normal use of following minimal trauma), Diagnosis involves not just evaluating the fracture ; such as site and type of injury but also, other associated injuries and distal neurovascular deficits. This may entail not just clinical, examination but radiographs of proximal and distal joints., When assessing x-rays it is important to assess for changes in length of the bone, the, angulation of the distal bone, rotational effects, presence of material such as glass., , Fracture types, , Fracture type, , Description, , Oblique fracture, , Fracture lies obliquely to long axis of bone, , Comminuted fracture, , >2 fragments, , Segmental fracture, , More than one fracture along a bone, , Transverse fracture, , Perpendicular to long axis of bone, , Spiral fracture, , Severe oblique fracture with rotation along long axis of bone, , Open Vs Closed, It is also important to distinguish open from closed injuries. The most common classification system, for open fractures is the Gustilo and Anderson classification system (given below):
Page 3795 :
Grade, , Injury, , 1, , Low energy wound <1cm, , 2, , Greater than 1cm wound with moderate soft tissue damage, , 3, , High energy wound > 1cm with extensive soft tissue damage, , 3 A (sub group of 3), , Adequate soft tissue coverage, , 3 B (sub group of 3), , Inadequate soft tissue coverage, , 3 C (sub group of 3), , Associated arterial injury, , Key points in management of fractures, , , , , , , , Immobilise the fracture including the proximal and distal joints, Carefully monitor and document neurovascular status, particularly following reduction and, immobilisation, Manage infection including tetanus prophylaxis, IV broad spectrum antibiotics for open injuries, As a general principle all open fractures should be thoroughly debrided ( and internal fixation, devices avoided or used with extreme caution), Open fractures constitute an emergency and should be debrided and lavaged within 6 hours, of injury, Next question
Page 3796 :
A 4 year old boy falls and sustains a fracture to the growth plate of his right wrist. Which of the, following systems is used to classify the injury?, , Salter - Harris system, , Weber system, , Gustilo - Anderson system, , Garden system, , None of the above, The mnemonic 'SALTR' can be used to help remember the first five types. This mnemonic requires, the reader to imagine the bones as long bones, with the epiphyses at the base., , , , , , , I "S" = Slip (separated or straight across). Fracture of the cartilage of the physis (growth, plate), II "A" = Above. The fracture lies above the physis, or Away from the joint., III "L" = Lower. The fracture is below the physis in the epiphysis., IV "TE" = Through Everything. The fracture is through the metaphysis, physis, and epiphysis., V "R" = Rammed (crushed). The physis has been crushed, , The Salter - Harris system is most commonly used. The radiological signs in Type 1 and 5 injuries, may be identical. Which is unfortunate as type 5 injuries do not do well (and may be missed!). One, of our users has helpfully supplied a mnemonic for remembering the types (see above)., Please rate this question:, , Discuss and give feedback, , Next question, , Paediatric fractures, Paediatric fracture types, , Type, , Injury pattern, , Complete fracture, , Both sides of cortex are breached
Page 3797 :
Toddlers fracture, , Oblique tibial fracture in infants, , Plastic deformity, , Stress on bone resulting in deformity without cortical disruption, , Greenstick fracture, , Unilateral cortical breach only, , Buckle fracture, , Incomplete cortical disruption resulting in periosteal haematoma only, , Growth plate fractures, In paediatric practice fractures may also involve the growth plate and these injuries are classified, according to the Salter- Harris system (given below):, , Type, , Injury pattern, , I, , Fracture through the physis only (x-ray often normal), , II, , Fracture through the physis and metaphysis, , III, , Fracture through the physis and epiphyisis to include the joint, , IV, , Fracture involving the physis, metaphysis and epiphysis, , V, , Crush injury involving the physis (x-ray may resemble type I, and appear normal), , As a general rule it is safer to assume that growth plate tenderness is indicative of an underlying, fracture even if the x-ray appears normal. Injuries of Types III, IV and V will usually require surgery., Type V injuries are often associated with disruption to growth., Non accidental injury, , , , , , , Delayed presentation, Delay in attaining milestones, Lack of concordance between proposed and actual mechanism of injury, Multiple injuries, Injuries at sites not commonly exposed to trauma
Page 3798 :
, , Children on the at risk register, , Pathological fractures, Genetic conditions, such as osteogenesis imperfecta, may cause pathological fractures., Osteogenesis imperfecta, , , , , Defective osteoid formation due to congenital inability to produce adequate intercellular, substances like osteoid, collagen and dentine., Failure of maturation of collagen in all the connective tissues., Radiology may show translucent bones, multiple fractures, particularly of the long bones,, wormian bones (irregular patches of ossification) and a trefoil pelvis., , Subtypes, , , , , , Type I The collagen is normal quality but insufficient quantity., Type II- Poor collagen quantity and quality., Type III- Collagen poorly formed. Normal quantity., Type IV- Sufficient collagen quantity but poor quality., , Osteopetrosis, , , , , , Bones become harder and more dense., Autosomal recessive condition., It is commonest in young adults., Radiology reveals a lack of differentiation between the cortex and the medulla described as, marble bone., Next question
Page 3799 :
Theme: Bone disease, , A., B., C., D., E., F., , Osteogenesis imperfecta, Osteoporosis, Rickets, Pagets disease, Chondrosarcoma, Metastatic breast cancer, , Please select the most likely diagnosis for the scenario given. Each option may be used once, more, than once or not at all., , 51., , A 66 year old lady presents with pain in her right hip. It has been increasing over the, previous three weeks and waking her from sleep. On examination she is tender on internal, rotation. Blood tests reveal a mildly elevated serum calcium and alkaline phosphatase, levels., You answered Osteogenesis imperfecta, The correct answer is Metastatic breast cancer, Increasing pain at rest, together with increased serum calcium and alkaline phosphatase are, most likely to represent metastatic tumour to bone. Chondrosarcomas do occur in the, pelvis but are not associated with increased serum calcium and typically have a longer, history., , 52., , A 73 year old man presents with pain in the right leg. It is most uncomfortable on walking., On examination he has a deformity of his right femur, which on x-ray is thickened and, sclerotic. His serum alkaline phosphatase is elevated, but calcium is within normal limits., You answered Osteogenesis imperfecta, The correct answer is Pagets disease, This is a typical scenario for Pagets disease., , 53., , A 73 year old lady presents with pain in her left hip. She was walking around the house, when she tripped over a rug and fell over. Apart from temporal arteritis which is well, controlled with prednisolone she is otherwise well. On examination he leg is shorted and, externally rotated.Her serum alkaline phosphatase and calcium are normal., You answered Osteogenesis imperfecta
Page 3800 :
The correct answer is Osteoporosis, The combination of age, female gender and steroids coupled with hip pain on minor, trauma are strongly suggestive of osteoporosis., Please rate this question:, , Discuss and give feedback, , Next question, , Bone disease, Disease, , Pagets, , Features, , , , , , , , Osteoporosis, , , , , , , Secondary bone, tumours, , , , , , , Treatment, , Focal bone resorption followed by, excessive and chaotic bone deposition, Affects (in order): spine, skull, pelvis, and femur, Serum alkaline phosphatase raised, (other parameters normal), Abnormal thickened, sclerotic bone on, x-rays, Risk of cardiac failure with >15%, bony involvement, Small risk of sarcomatous change, , Bisphosphonates, , Excessive bone resorption resulting in, demineralised bone, Commoner in old age, Increased risk of pathological fracture,, otherwise asymptomatic, Alkaline phosphatase normal, calcium, normal, , Bisphosphonates, calcium, and vitamin D, , Bone destruction and tumour, infiltration, Mirel scoring used to predict risk of, fracture, Appearances depend on primary, (e.g.sclerotic - prostate, lytic - breast), Elevated serum calcium and alkaline, , Radiotherapy, prophylactic, fixation and analgesia
Page 3801 :
Disease, , Features, , Treatment, , phosphatase may be seen, Next question
Page 3802 :
Theme: Shoulder pain, , A., B., C., D., E., F., G., , Impingement syndrome, Rotator cuff tear, Adhesive capsulitis, Calcific tendonitis, Biceps tendon rupture, Parsonage - Turner syndrome, Labral tear, , Please select the most likely cause for shoulder pain from the list. Each option may be used once,, more than once or not at all., , 54., , A 63 year old lady undergoes an axillary clearance for breast cancer. She makes steady, progress. However, 8 weeks post operatively she still suffers from severe shoulder pain., On examination she has reduced active movements in all planes and loss of passive, external rotation., You answered Impingement syndrome, The correct answer is Adhesive capsulitis, Theme from January 2016 Exam, Frozen shoulder passes through an initial painful stage followed by a period of joint, stiffness. With physiotherapy the problem will usually resolve although it may take up to 2, years to do so., , 55., , A 78 year old man complains of a long history of shoulder pain and more recently, weakness. On examination active attempts at abduction are impaired. Passive movements, are normal., You answered Impingement syndrome, The correct answer is Rotator cuff tear, Rotator cuff tears are common in elderly people and may occur following minor trauma or, as a result of long standing impingement. Tears greater than 2cm should generally be, repaired surgically. The length of the history in this scenario is suggestive of a tear, complicating impingement., , 56., , A 28 year old man complains of pain and weakness in the shoulder. He has recently been, unwell with glandular fever from which he is fully recovered. On examination there is, some evidence of muscle wasting and a degree of winging of the scapula. Power during, active movements is impaired.
Page 3803 :
You answered Impingement syndrome, The correct answer is Parsonage - Turner syndrome, This is a peripheral neuropathy that may complicate viral illnesses and usually resolves, spontaneously., Deep seated pain in the proximal forearm especially during the night and at rest may be due to, tumour, especially metastatic lesions., Please rate this question:, , Discuss and give feedback, , Next question, , Shoulder disorders, Shoulder fractures and dislocations, Fractures, Proximal humerus, Background, , , , , Third most common fragility fracture in the elderly., Results from low energy fall in predominantly elderly females, or from high energy trauma in, young males., Can be associated with nerve injury (commonly axillary), and fracture-dislocation of the, humeral head. Detailed neurological assessment is essential for all upper limb injuries., , Anatomy, Osteology, Consists of articular head, greater tuberosity, lesser tuberosity, metaphysis and diaphysis. Between, the articular head and the tuberosities is the anatomical neck (previous physis). Between the, tuberosities and the metaphysis is the surgical neck., The supraspinatus, infraspinatus and teres minor muscles attach to the greater tuberosity. The, subscapularis muscle attaches to the lesser tuberosity., Vascular Supply, Humeral head is supplied by the anterior and posterior humeral circumflex arteries. Anatomical neck, fractures are at greatest risk of osteonecrosis., Imaging, Imaging aims to both delineate the fracture pattern, and confirm/exlude the presence of an, associated dislocation., , , Radiographs - True anteroposterior (AP), axillary lateral and/or scapula Y view.
Page 3804 :
, , CT - indicated to better define intra-articular involvement and to aid pre-operative planning., MRI is not useful for fracture imaging., , Classification, Description of the fracture is often more useful than classification. Particular attention should be paid, to humeral alignment, fracture displacement, and greater tuberosity position (rotator cuff will pull the, GT supero-posterioly, which can cause impingement problems with malunion)., - Neer Classification: Most commonly used. Describes fracture as 2,3,or 4 part depending upon the, number main fragments. Also comments on the degree of displacement. Fragments:, -greater tuberosity, -lesser tuberosity, - articular surface, - shaft, Displacement: >1cm or angulation >45 degrees., Treatment, The vast majority of proximal humeral fractures are minimally displaced, and therefore can be, managed conservatively. This involves immobilisation in a polysling, and progressive mobilisation., Pendular exercise can commence at 14 days, and active abduction from 4-6 weeks., Irreducible fracture dislocation is an indication for operative management. Other indications include, large displacement, younger patient, head splitting (intra-articular fractures). However, the recent, PROFHER trial (1) has suggested no benefit to operative intervention on patient outcome (it must be, applied cautiously as majority of patients were elderly with extraarticular fractures). Options available, for surgical management include:, , ORIF, , Most commonly used. Plate and screw fixation. Can reconstruct, complex fractures., , Intramedullary nail, , Suitable for extra-articular configuration, predominantly surgical neck, +/- GT fractures., , Hemiarthroplasty, , Used for un-reconstructable fractures in the older patient who has good, glenoid quality., , Total shoulder, arthroplasty, , Unconstructable fractures where high functioning shoulder is required, (hemiarthroplasty will cause glenoid erosion), , Reverse shoulder, arthroplasty, , Total shoulder arthroplasty that provides better functional outcome than, conventional total shoulder replacement.
Page 3805 :
Scapula, Background, Uncommon fractures usually associated with high energy trauma. Most commonly involve scapula, body or spine (50%), glenoid fossa and glenoid neck. Important to exclude associated life, threatening injury., Imaging, Plain radiographs should include true anteroposterior (AP), axillary lateral and/or scapula Y view. CT, scanning is useful for defining intra-articular involvement, displacement and for three dimensional, reconstruction., Classification, Based on the location of the fracture (coracoid, acromion, glenoid neck, glenoid fossa, scapula, body). Beware of ipsilateral glenoid neck and clavicle fracture -floating shoulder - where limb is, effectively dissociated from axial skeleton., Treatment, The vast majority of scapula fractures are amenable to conservative management, consisting of, sling immobilisation for two weeks followed by early rehabilitation. Floating shoulder will usually, require fixation, and consideration of surgery should also be given to intra-articular and, displaced/angulated glenoid fractures., Dislocations, Types, Dislocations around the shoulder joint include glenohumeral dislocation, acromioclavicular joint, disruption and sternoclavicular dislocation. Only glenohumeral dislocation will be covered here., Glenohumeral dislocation, Diagnosis, classification and management are covered here., Background, Shoulder dislocation is commonly seen in A&E. It has a high recurrence rate that is as high as 80%, in teenagers. Initial management requires emergent reduction to prevent lasting chondral damage., Early assessment and management, Usually a traumatic cause (multi-directional instability in frequent dislocations requires discussion, with orthopaedics and is not covered here). Careful history, examination and documentation of, neurovascular status of the limb, in particular the axillary nerve (regimental badge sensation). This, should be re-assessed post manipulation. Early radiographs to confirm direction of dislocation., Initial management consists of emergent closed reduction under under entanox and analgesia, but, often requires conscious sedation. Arm should then be immobilised in a polysling, and XR to confirm, relocation., Imaging - True anteroposterior (AP), axillary lateral and/or scapula Y view. Reduced humeral head, should lie between acromion and coracoid on lateral/scapula view., Types, , Direction, , Features, , Cause, , Examination, , Reduction, techniques
Page 3806 :
Direction, , Features, , Cause, , Examination, , Reduction, techniques, , Anterior, , Most, Common, >90%, , Usually traumatic - anterior, force on arm when shoulder, is abducted, eternally, rotated, , Loss of shoulder, contour - sulcus sign., Humeral head can be, felt anteriorly., , Hippocratic., Milch., Stimson., Kocher not, advised due to, complication of, fracture, , Posterior, , 50%, missed in, A&E, , 50% traumatic, but, classically post seizure or, electrocution, , Shoulder locked in, internal rotation. XR, may show lightbulb, appearance., , Gentle lateral, traction to, adducted arm., , Inferior, , Rare, , Associated with pectorals, and rotator cuff tears, and, glenoid fracture, , As for primary injury, , Management of, primary injury, , Rare, , Associated with, acrominon/clavicle fracture, , As for primary injury, , Management of, primary injury, , Superior, , Associated injuries, , , , , , , Bankart lesion - avulsion of the anterior glenoid labrum with an anterior shoulder dislocation, (reverse Bankart if poster labrum in posterior dislocation)., Hill Sachs defect - chondral impaction on posteriosuperior humeral head from contact with, gleonoid rim. Can be large enough to lock shoulder, requiring open reduction. (Reverse Hill, Sachs in posterior dislocation)., Rotator cuff tear - increases with age., Greater or lesser tuberosity fracture - increases with age., Humeral neck fracture - shoulder fracture dislocation. More common in high energy trauma, and elderly. Should be discussed with orthopaedics prior to any attempted reduction., , Rotator Cuff Disease
Page 3807 :
Rotator cuff disease is a spectrum of conditions that ranges from subacromial impingement to rotator, cuff tears and eventually to rotator cuff arthropathy (arthritis)., Anatomy, The rotator cuff is a group of four muscles that are important in shoulder movements, and, maintenance of glenohumeral stability., , Scapular, attachment, , Humeral, attachment, , Supraspinatus, , Supraspinatus, fossa, , Infraspinatus, , Muscle, , Action, , Innervation, , Superior facet of, greater tuberosity, , Initiation of, abduction of, humerus, , Suprascapular nerve, , Infraspinatus, fossa, , Posterior facet of, greater tuberosity, , External rotation, of humerus, , Suprascapular nerve, , Teres Minor, , Lateral border, , Inferior facet of, greater tuberosity, , External rotation, of humerus, , Axillary Nerve, , Subscapularis, , Subscapular, fossa, , Lesser tuberosity, , Internal rotation, of humerus, , Upper and lower, subscapular nerve, , , , , The inferior rotator cuff muscles (infraspinatus, teres minor, and subscapularis) balance the, superior pull of the deltoid. Injury/tear results in upward migration of the humeral head on the, glenoid (can be seen on AP radiograph)., Likewise, the anterior muscles (subscapularis) are balanced with the posterior muscles, (infraspinatus, teres minor)., , Subacromial Impingement, , , , , , The most common cause of shoulder pain, which results from impingement of the superior, cuff on the undersurface of the acromion, and an inflammatory bursitis., Associated with certain types of acromial morphology (Bigliani classification)., Presents as insidious pain which is exacerbated by overhead activities., , Rotator Cuff Tear
Page 3808 :
, , , , Often presents as an acute event on the background of chronic subacromial impingement in, the older patient, but can present as an avulsion injury in younger patients., Majority of tears are to the superior cuff (supraspinatus, infraspinatus, teres minor), though a, tear to subscapularis is associated with subcoracoid impingement., Tears present as pain and weakness when using the muscles in question., , Rotator Cuff Arthropathy, , , , , Defined as shoulder arthritis in the setting of rotator cuff dysfunction. Results from superior, migration due to the loss of rotator cuff function and integrity. Unopposed deltoid pulls the, humeral head superiorly., Associated with massive chronic cuff tears., , Imaging, Plain radiographs, , , , AP of the shoulder may show superior migration of the humerus with a cuff tear, and features, of arthritis with arthropathy. Other causes of pain may also be identified (e.g. calcific, tendonitis/fracture), Outlet view is useful for defining the acromial morphology, , USS, , , Allows dynamic imaging of the cuff, and is inexpensive. However, it is very user dependent., , MRI, , , , Best imaging modality for cuff pathology., Also allows imaging of the rest of the shoulder. When intra-articular pathology is suspected,, can be combined with an arthrogram for improved sensitivity and specificity., , Treatment, Subacromial impingement, , , , Physiotherapy, oral anti-inflammatory medication, Subacromial steroid injection can settle inflammation
Page 3809 :
, , Arthroscopic subacromial decompression by shaving away the undersurface of the, acromion, more space is created for the rotator cuff. Cuff integrity is assessed also at time of, surgery, and can be repaired if necessary., , Rotator cuff tear, , , , , When considering repair of a cuff tear, the age and activity of the patient, the nature of the, tear (degenerative vs. acute traumatic), and the size and retraction of the tear should be, considered when making a surgical plan., Mild tears or tears in the elderly can be managed conservatively, as outlined above., Moderate tears can be repaired arthroscopically. Massive or retracted tears will often require, an open repair (occasionally with a tendon transfer). Subacromial decompression is, performed at the same time to reduce impingement, symptoms and recurrence., , Calcific tendonitis, Calcific tendonitis involves calcific deposits within tendons anywhere in the body, but most, commonly in the rotator cuff (specifically the supraspinatus tendon). When present in the shoulder, it, is associated with subacromial impingement and pain., Pathology, , , , More common in women aged 30-60 years., Association with diabetes and hypothyroidism, , There are three stages of calcification, , , , , Formative phase characterized by calcific deposits, Resting phase deposit is stable, but presents with impingement problems, Resorptive phase phagocytic resorption. Most painful stage., , Presentation, , , Similar in presentation to subacromial impingement, with pain especially with over head, activities. Atraumatic in nature., , Imaging, , , Plain radiographs show calcification of the rotator cuff, usually within 1.5cm of its insertion on, the humerus. Supraspinatus outlet views can show level of impingment. Further imaging is, rarely needed.
Page 3810 :
Treatment, , , , Non-operative NSAIDS, steroid injection (controversial, but practiced) and physiotherapy., Approximately 75% will resolve by 6 months with conservative management., Ultrasound guided or surgical needle barbotage can break down deposits and resolve, symptoms. Occasionally surgical excision is required., , Adhesive capsulitis (Frozen Shoulder), , , , , Pain and loss of movement of shoulder joint, which involves fibroplastic proliferation of, capsular tissue, causing soft tissue scarring and contracture. Patients present with a painful, and decreased arc of motion., Associated with prolonged immobilization, previous surgery, thyroid disorders (AI) and, diabetes, Classically three stages which can take up to two years to resolve:, , Stage one the freezing and painful stage, Stage two the frozen and stiff stage, Stage three the thawing stage, where shoulder movement slowly improves, Imaging, , , , Plain radiographs to exclude other causes of a painful shoulder, MRI arthrogram may show capsular contracture, and again may be used to exclude cuff, pathology. However, often not performed as diagnosis is largely clinical., , Treatment, , , , Non-operative NSAIDS, steroid injection and physiotherapy. Patience is required as, condition can take up to 2 years to improve., Operative MUA or arthroscopic adhesiolysis (release of adhesions) can expedite recovery,, followed by intensive physiotherapy., , Glenohumeral Arthritis, Shoulder arthritis presents with the normal symptoms of arthritis, however primary osteoarthritis is, not as commonly the primary cause as seen in other large joints.. A large proportion of shoulder, arthritis is rheumatoid (RA), post traumatic, or secondary to rotator cuff arthropathy (discussed, above)., Treatment
Page 3811 :
, , Surgical options include hemiarthroplasty, total shoulder replacement and reverse geometry, total shoulder replacement (used when rotator cuff function is absent)., , References, 1. JAMA. 2015;313(10):1037-1047. doi:10.1001/jama.2015.1629, Next question
Page 3812 :
Theme: Knee injuries, , A., B., C., D., E., F., G., H., I., , Anterior cruciate ligament rupture, Posterior cruciate ligament rupture, Medial collateral ligament tear, Lateral collateral ligament tear, Torn meniscus, Chondromalacia patellae, Dislocated patella, Fractured patella, Tibial plateau fracture, , What is the most likely injury for scenario given? Each option may be used once, more than once or, not at all., , 57., , A 38 year old man is playing football when he slips over during a tackle. His knee is, painful immediately following the fall. Several hours later he notices that the knee has, become swollen. Following a course of non steroidal anti inflammatory drugs and rest the, situation improves. However, complains of recurrent pain. On assessment in clinic you, notice that it is impossible to fully extend the knee, although the patient is able to do so, when asked., You answered Anterior cruciate ligament rupture, The correct answer is Torn meniscus, Theme from September 2012 Exam, Twisting sporting injuries followed by delayed onset of knee swelling and locking are, strongly suggestive of a menisceal tear. Arthroscopic menisectomy is the usual treatment., , 58., , A 34 year old woman is a passenger in a car during an accident. Her knee hits the, dashboard. On examination the tibia looks posterior compared to the non injured knee., You answered Anterior cruciate ligament rupture, The correct answer is Posterior cruciate ligament rupture, In ruptured posterior cruciate ligament the tibia lies back on the femur and can be drawn, forward during a paradoxical draw test., , 59., , A 28 year old professional footballer is admitted to the emergency department. During a, tackle he is twisted with his knee flexed. He hears a loud crack and his knee rapidly, becomes swollen.
Page 3813 :
Anterior cruciate ligament rupture, This is common in footballers as the football boot studs stick to the ground and high, twisting force is applied to a flexed knee. Rapid joint swelling also supports the diagnosis., Please rate this question:, , Discuss and give feedback, , Next question, , Knee injury, Types of injury, , , , , , , Sport injury, Mechanism: high twisting force applied to a bent knee, Typically presents with: loud crack, pain and RAPID joint, swelling (haemoarthrosis), Poor healing, Management: intense physiotherapy or surgery, , Ruptured posterior, cruciate ligament, , , , , , Mechanism: hyperextension injuries, Tibia lies back on the femur, Paradoxical anterior draw test, , Rupture of medial, collateral ligament, , , , , Mechanism: leg forced into valgus via force outside the leg, Knee unstable when put into valgus position, , Menisceal tear, , , , , , , Rotational sporting injuries, Delayed knee swelling, Joint locking (Patient may develop skills to "unlock" the knee, Recurrent episodes of pain and effusions are common, often, following minor trauma, , Chondromalacia, patellae, , , , Teenage girls, following an injury to knee e.g. Dislocation, patella, Typical history of pain on going downstairs or at rest, Tenderness, quadriceps wasting, , Ruptured anterior, cruciate ligament, , ,
Page 3814 :
, , Dislocation of the, patella, , , , , Most commonly occurs as a traumatic primary event, either, through direct trauma or through severe contraction of, quadriceps with knee stretched in valgus and external rotation, Genu valgum, tibial torsion and high riding patella are risk, factors, Skyline x-ray views of patella are required, although displaced, patella may be clinically obvious, An osteochondral fracture is present in 5%, The condition has a 20% recurrence rate, , , , 2 types:, , , , , Fractured patella, , i. Direct blow to patella causing undisplaced fragments, ii. Avulsion fracture, Tibial plateau fracture, , , , , , , Occur in the elderly (or following significant trauma in young), Mechanism: knee forced into valgus or varus, but the knee, fractures before the ligaments rupture, Varus injury affects medial plateau and if valgus injury, lateral, plateau depressed fracture occurs, Classified using the Schatzker system (see below), , Schatzker Classification system for tibial plateau fractures, , Type, , Anatomical description, , Features, , 1, , Vertical split of lateral, condyle, , Fracture through dense bone, usually in the young. It may be, virtually undisplaced, or the condylar fragment may be, pushed inferiorly and tilted, , 2, , Vertical split of the lateral, condyle combined with an, adjacent load bearing part, of the condyle, , The wedge fragment (which may be of variable size), is, displaced laterally; the joint is widened. Untreated, a valgus, deformity may develop, , 3, , Depression of the articular, surface with intact condylar, rim, , The split does not extend to the edge of the plateau., Depressed fragments may be firmly embedded in, subchondral bone, the joint is stable
Page 3815 :
Type, , Anatomical description, , Features, , 4, , Fragment of the medial, tibial condyle, , Two injuries are seen in this category; (1) a depressed, fracture of osteoporotic bone in the elderly. (2) a high, energy fracture resulting in a condylar split that runs from, the intercondylar eminence to the medial cortex. Associated, ligamentous injury may be severe, , 5, , Fracture of both condyles, , Both condyles fractured but the column of the metaphysis, remains in continuity with the tibial shaft, , 6, , Combined condylar and, subcondylar fractures, , High energy fracture with marked comminution, , Next question
Page 3816 :
A 10 year old boy is referred to the orthopaedic clinic with symptoms of right knee pain. He has, suffered pain for the past 3 months and the pain typically lasts for several hours. On examination he, walks with an antalgic gait and has apparent right leg shortening. The right knee is normal but the, right hip reveals pain on internal and external rotation. Imaging shows flattening of the femoral head., Which of the following is the most likely underlying diagnosis?, , Osteogenesis imperfecta, , Child abuse, , Osteosarcoma, , Osteopetrosis, , Perthes disease, , This is a typical description of Perthes disease. Management involves keeping the femoral head in, the acetabulum by braces, casts or surgery., Please rate this question:, , Discuss and give feedback, , Next question, , Perthes disease, Perthes disease, , , , Idiopathic avascular necrosis of the femoral epiphysis of the femoral head, Impaired blood supply to femoral head, causing bone infarction. New vessels develop and, ossification occurs. The bone either heals or a subchondral fracture occurs., , Clinical features, , , , , , , Males 4x's greater than females, Age between 2-12 years (the younger the age of onset, the better the prognosis), Limp, Hip pain, Bilateral in 20%
Page 3817 :
Diagnosis, Plain x-ray, Technetium bone scan or magnetic resonance imaging if normal x-ray and symptoms, persist., Catterall staging, , Stage, , Features, , Stage 1, , Clinical and histological features only, , Stage 2, , Sclerosis with or without cystic changes and preservation of the articular surface, , Stage 3, , Loss of structural integrity of the femoral head, , Stage 4, , Loss of acetabular integrity, , Management, , , , , , To keep the femoral head within the acetabulum: cast, braces, If less than 6 years: observation, Older: surgical management with moderate results, Operate on severe deformities, , Prognosis, Most cases will resolve with conservative management. Early diagnosis improves outcomes., Next question
Page 3818 :
Which statement relating to talipes equinovarus is untrue?, , It has an annual incidence of around 1 in 1000 in the UK., , The muscles involved in the disorder are intrinsically abnormal., , The cuboid is classically displaced medially., , All cases should be treated with an Ilizarov frame initially unless there is minor, deformity., The talocalcaneal angle is typically less than 20 degrees in club foot., , In most cases of Club Foot conservative measures should be tried first. The Ponsetti method is a, popular approach. Severe cases may benefit from Ilizarov frame re-aligment., Please rate this question:, , Discuss and give feedback, , Next question, , Talipes Equinovarus, Congenital talipes equinovarus., Features:, , , , , Equinus of the hindfoot., Adduction and varus of the midfoot., High arch., , Most cases in developing countries. Incidence in UK is 1 per 1000 live births. It is more common in, males and is bilateral in 50% cases. There is a strong familial link(1). It may also be associated with, other developmental disorders such as Down's syndrome., Key anatomical deformities (2):, , , , , , Adducted and inverted calcaneus, Wedge shaped distal calcaneal articular surface, Severe Tibio-talar plantar flexion., Medial Talar neck inclination
Page 3819 :
, , , , Displacement of the navicular bone (medially), Wedge shaped head of talus, Displacement of the cuboid (medially), , Management, Conservative first, the Ponseti method is best described and gives comparable results to surgery. It, consists of serial casting to mold the foot into correct shape. Following casting around 90% will, require a Achilles tenotomy. This is then followed by a phase of walking braces to maintain the, correction., Surgical correction is reserved for those cases that fail to respond to conservative measures. The, procedures involve multiple tenotomies and lengthening procedures. In patients who fail to respond, surgically an Ilizarov frame reconstruction may be attempted and gives good results., References, 1. Wynne-Davies R, Littlejohn A, Gormley J. Aetiology and interrelationship of some common, skeletal deformities. (Talipes equinovarus and calcaneovalgus, metatarsus varus, congenital, dislocation of the hip, and infantile idiopathic scoliosis). J Med Genet. 1982 Oct;19(5):321-8., 2. Horn BD, Davidson RS. Current treatment of clubfoot in infancy and childhood. Foot Ankle Clin., 2010 Jun;15(2):235-43., 3. Clarke NM, Uglow MG, Valentine KM. Comparison of Ponseti Versus Surgical Treatment in, Congenital Talipes Equinovarus. J Foot Ankle Surg. 2011 Jun 14., Next question
Page 3820 :
Which of the following is least likely to impair bone fracture healing?, , Radiotherapy, , Osteoporosis, , Administration of non steroidal anti inflammatory drugs, , Preservation of periosteum, , Presence of osteomyelitic sequestra, , Periosteal preservation helps fractures to heal., Please rate this question:, , Discuss and give feedback, , Next question, , Fracture healing, Bone fracture, - Bleeding vessels in the bone and periosteum, - Clot and haematoma formation, - The clot organises over a week (improved structure and collagen), - The periosteum contains osteoblasts which produce new bone, - Mesenchymal cells produce cartilage (fibrocartilage and hyaline cartilage) in the soft tissue around, the fracture, - Connective tissue + hyaline cartilage = callus, - As the new bone approaches the new cartilage, endochondral ossification occurs to bridge the gap, - Trabecular bone forms, - Trabecular bone is resorbed by osteoclasts and replaced with compact bone, Factors affecting fracture healing, , , , , , , Age, Malnutrition, Bone disorders: osteoporosis, Systemic disorders: diabetes, Marfan's syndrome and Ehlers-Danlos syndrome cause, abnormal musculoskeletal healing., Drugs: steroids, non steroidal anti inflammatory agents.
Page 3821 :
, , , , , , , , Type of bone: Cancellous (spongy) bone fractures are usually more stable, involve greater, surface areas, and have a better blood supply than cortical (compact) bone fractures., Degree of Trauma: The more extensive the injury to bone and surrounding soft tissue, the, poorer the outcome., Vascular Injury: Especially the femoral head, talus, and scaphoid bones., Degree of Immobilization, Intra-articular Fractures: These fractures communicate with synovial fluid, which contains, collagenases that retard bone healing., Separation of Bone Ends: Normal apposition of fracture fragments is needed for union to, occur. Inadequate reduction, excessive traction, or interposition of soft tissue will prevent, healing., Infection, Next question
Page 3822 :
Theme: Disorders of the hip, , A. Perthes disease, B. Developmental dysplasia of the hip, C. Osteoarthritis, D. Slipped upper femoral epiphysis, E. Septic arthritis, F. Rheumatoid arthritis, G. Intra capsular fracture of the femoral neck, H. Extra capsular fracture of the femoral neck, , Please select the most likely underlying diagnosis for the scenario given. Each option may be used, once, more than once or not at all., , 63., , An obese 14 year old boy presents with difficulty running and mild knee and hip pain. There is no, antecedent history of trauma. On examination internal rotation is restricted but the knee is, normal with full range of passive movement possible and no evidence of effusions. Both the Creactive protein and white cell count are normal., You answered Perthes disease, The correct answer is Slipped upper femoral epiphysis, Slipped upper femoral epiphysis is the commonest adolescent hip disorder. It occurs most, commonly in obese males. It may often present as knee pain which is usually referred from the, ipsilateral hip. The knee itself is normal. The hip often limits internal rotation. The diagnosis is, easily missed. X-rays will show displacement of the femoral epiphysis and the degree of its, displacement may be calculated using the Southwick angle. Treatment is directed at preventing, further slippage which may result in avascular necrosis of the femoral head., , 64., , A 6 year old boy presents with pain in the hip it is present on activity and has been worsening, over the past few weeks. There is no history of trauma. He was born by normal vaginal delivery at, 38 weeks gestation On examination he has an antalgic gait and limitation of active and passive
Page 3823 :
movement of the hip joint in all directions. C-reactive protein is mildly elevated at 10 but the, white cell count is normal., Perthes disease, This is a typical presentation for Perthes disease. X-ray may show flattening of the femoral head, or fragmentation in more advanced cases., , 65., , A 30 year old man presents with severe pain in the left hip it has been present on and off for, many years. He was born at 39 weeks gestation by emergency caesarean section after a long, obstructed breech delivery. He was slow to walk and as a child was noted to have an antalgic gait., He was a frequent attender at the primary care centre and the pains dismissed as growing pains., X-rays show almost complete destruction of the femoral head and a narrow acetabulum., You answered Perthes disease, The correct answer is Developmental dysplasia of the hip, Developmental dysplasia of the hip. Usually diagnosed by Barlow and Ortolani tests in early, childhood. Most Breech deliveries are also routinely subjected to USS of the hip joint. At this, young age an arthrodesis may be preferable to hip replacement., , Early plain x-ray changes in Perthes Disease:, Widening of the joint space., Sub chondral linear lucency., , Please rate this question:, , Discuss and give feedback, , Next question, , Paediatric orthopaedics
Page 3824 :
Diagnosis, , Mode of presentation, , Treatment, , Radiology, , Developmental, dysplasia of the, hip, , Usually diagnosed in infancy, by screening tests. May be, bilateral, when disease is, unilateral there may be leg, length inequality. As, disease progresses child, may limp and then early, onset arthritis. More, common in extended, breech babies., , Splints and harnesses or, traction. In later years, osteotomy and hip, realignment procedures may, be needed. In arthritis a joint, replacement may be needed., However, this is best, deferred if possible as it will, almost certainly require, revision, , Initially no obvious, change on plain films, and USS gives best, resolution until 3, months of age. On, plain films Shentons, line should form a, smooth arc, , Perthes Disease, , Hip pain (may be referred, to the knee) usually, occurring between 5 and 12, years of age. Bilateral, disease in 20%., , Remove pressure from joint, to allow normal, development. Physiotherapy., Usually self-limiting if, diagnosed and treated, promptly., , X-rays will show, flattened femoral, head. Eventually in, untreated cases the, femoral head will, fragment., , Slipped upper, femoral, epiphysis, , Typically seen in obese, male adolescents. Pain is, often referred to the knee., Limitation to internal, rotation is usually seen., Knee pain is usually present, 2 months prior to hip, slipping. Bilateral in 20%., , Bed rest and non-weight, bearing. Aim to avoid, avascular necrosis. If severe, slippage or risk of it occurring, then percutaneous pinning of, the hip may be required., , X-rays will show the, femoral head displaced, and falling, inferolaterally (like a, melting ice cream, cone) The Southwick, angle gives indication, of disease severity, , Next question
Page 3825 :
Theme: Paediatric fractures, , A., B., C., D., E., F., G., H., I., , Non accidental injury, Accidental fracture, Rickets, Metabolic bone disease of prematurity, Hypophosphataemic rickets, Osteopetrosis, Osteogenesis imperfecta, Hypoparathyroidism, Osteoporosis, , Please select the most likely explanation for each of the following injury scenarios. Each option may, be used once, more than once or not at all., , 66., , A toddler aged 3 years presents to the Emergency Department with swelling of his leg and, is found to have a spiral fracture of the tibia. His mother reports that he had tripped and, fallen the previous day but she had not noticed any sign of injury at the time. She is a, single parent with little family support. The child is not on the child protection register., Non accidental injury, Delayed presentation is unusual and should raise concern. In addition spiral fractures are, usually the result of rotational injury which is not compatible with the mechanism, proposed by the parent., , 67., , A 5 month baby boy presents with swelling of his right arm and is found to have a spiral, fracture of the humerus. He had been in the care of her mother's boyfriend who reported, that he had nearly dropped him that day when reaching for his bottle and had inadvertently, pulled on his arm to save him. He was immediately taken to the Emergency Department., You answered Non accidental injury, The correct answer is Accidental fracture, The mechanism fits with the fracture pattern and the presentation is not delayed., , 68., , An infant is admitted with symptoms and signs of respiratory infection and is found to, have several posterior rib fractures on chest radiograph. He was born prematurely at 37, weeks' gestation and was observed overnight on the special care baby unit for tachypnoea, which settled by the following day. On assessment it is also apparent that his head, circumference has increased at an excessive rate and has crossed 3 centiles since birth.
Page 3826 :
Non accidental injury, Posterior rib fractures are extremely unusual in neonates. The change in head size may be, accounted for by hydrocephalus which may occur as a sequelae from head injury., Please rate this question:, , Discuss and give feedback, , Next question, , Paediatric fractures, Paediatric fracture types, , Type, , Injury pattern, , Complete fracture, , Both sides of cortex are breached, , Toddlers fracture, , Oblique tibial fracture in infants, , Plastic deformity, , Stress on bone resulting in deformity without cortical disruption, , Greenstick fracture, , Unilateral cortical breach only, , Buckle fracture, , Incomplete cortical disruption resulting in periosteal haematoma only, , Growth plate fractures, In paediatric practice fractures may also involve the growth plate and these injuries are classified, according to the Salter- Harris system (given below):, , Type, , Injury pattern, , I, , Fracture through the physis only (x-ray often normal), , II, , Fracture through the physis and metaphysis
Page 3827 :
III, , Fracture through the physis and epiphyisis to include the joint, , IV, , Fracture involving the physis, metaphysis and epiphysis, , V, , Crush injury involving the physis (x-ray may resemble type I, and appear normal), , As a general rule it is safer to assume that growth plate tenderness is indicative of an underlying, fracture even if the x-ray appears normal. Injuries of Types III, IV and V will usually require surgery., Type V injuries are often associated with disruption to growth., Non accidental injury, , , , , , , , Delayed presentation, Delay in attaining milestones, Lack of concordance between proposed and actual mechanism of injury, Multiple injuries, Injuries at sites not commonly exposed to trauma, Children on the at risk register, , Pathological fractures, Genetic conditions, such as osteogenesis imperfecta, may cause pathological fractures., Osteogenesis imperfecta, , , , , Defective osteoid formation due to congenital inability to produce adequate intercellular, substances like osteoid, collagen and dentine., Failure of maturation of collagen in all the connective tissues., Radiology may show translucent bones, multiple fractures, particularly of the long bones,, wormian bones (irregular patches of ossification) and a trefoil pelvis., , Subtypes, , , , , , Type I The collagen is normal quality but insufficient quantity., Type II- Poor collagen quantity and quality., Type III- Collagen poorly formed. Normal quantity., Type IV- Sufficient collagen quantity but poor quality., , Osteopetrosis
Page 3828 :
, , , , , Bones become harder and more dense., Autosomal recessive condition., It is commonest in young adults., Radiology reveals a lack of differentiation between the cortex and the medulla described as, marble bone., Next question
Page 3829 :
In paediatric orthopaedic surgery, which of the following does not fulfill the Kocher criteria for septic, arthritis?, , ESR > 40mm/h, , Positive blood culture, , Fever, , White cell count > 12, 000, , Non weight bearing on the affected side, , Kocher criteria, 1. Non weight bearing on affected side, 2. ESR > 40 mm/hr, 3. Fever, 4. WBC count of >12,000 mm 3, - When 4/4 criteria are met, there is a 99% chance that the child has septic arthritis, The Kocher criteria do not consider blood culture results., Please rate this question:, , Discuss and give feedback, , Next question, , Septic arthritis- Paediatric, Septic arthritis, , , , Staph aureus commonest organism, Urgent washout and antibiotics otherwise high risk of joint destruction, , Diagnosis, , , , , Plain x-rays, Consider aspiration, Utilise the Kocher criteria (see below)
Page 3830 :
Kocher criteria:, 1. Non weight bearing on affected side, 2. ESR > 40 mm/hr, 3. Fever, 4. WBC count of >12,000 mm 3, - when 4/4 criteria are met, there is a 99% chance that the child has septic arthritis, Treatment, Surgical drainage of the affected joint is required, this should be done as soon as possible since, permanent damage to the joint may occur. In some cases repeated procedures are necessary., Appropriate intravenous antibiotics should be administered., Next question
Page 3831 :
Theme: Ankle fractures, , A. Surgical fixation, B. Below knee amputation, C. Aircast boot, D. Application of full leg plaster cast to include midfoot, E. Application of below knee plaster cast to include the midfoot, F. Application of external fixation device, G. Application of compression bandage and physiotherapy., , Please select the most appropriate management for the injury type described. Each option may be, used once, more than once or not at all., , 70., , A 24 year old man falls sustaining an inversion injury to his ankle. On examination he is tender, over the lateral malleolus only. On x-ray there is a fibular fracture that is distal to the, syndesmosis., You answered Surgical fixation, The correct answer is Application of below knee plaster cast to include the midfoot, Theme from 2010 Exam, These distal injuries are generally managed conservatively. Conservative management will involve, a below knee cast, this will need to extend to the midfoot. It can be substituted for an aircast boot, once radiological union is achieved., , 71., , An 86 year old lady stumbles and falls whilst opening her front door. On examination her ankle is, swollen with both medial and lateral tenderness. X rays demonstrate a fibular fracture at the level, of the syndesmosis., You answered Surgical fixation, The correct answer is Application of below knee plaster cast to include the midfoot
Page 3832 :
Although, this is a potentially unstable injury operative fixation in this age group generally gives, poor results owing to poor quality bone. A below knee cast should be applied in the first instance., If this fails to provide adequate control it can be extended above the knee., , 72., , A 25 year old man suffers an injury whilst playing rugby involving a violent twist to his left lower, leg. On examination both malleoli are tender and the ankle joint is slightly swollen. On x-ray there, is a spiral fracture of the fibula and widening of the ankle mortise., Surgical fixation, This is a variant of the Weber C fracture in which disruption of the tibio-fibular syndesmosis, occurs leading to joint disruption. Surgical repair is warranted., , Please rate this question:, , Discuss and give feedback, , Next question, , Ankle injuries, An ankle fracture relates to a fracture around the tibio-talar joint. It generally refers to a fracture, involving the lateral, and/or medial and/or posterior malleolus. Pilon and Tillaux fractures are also, considered to be ankle fractures, but are not covered here., Ankle fractures are common. They effect men and women in equal numbers, but men have a higher, rate as young adults (sports and contact injuries), and women a higher rate post-menopausal, (fragility type fracture)., Osseous anatomy, The ankle (or mortise) joint consists of the distal tibia (tibial plafond and posterior malleolus), the, distal fibula (lateral malleolus), and the talus. The main movement at the ankle joint is plantar and, dorsiflexion., Ligamentous anatomy, Medial side: Deltoid ligament. This is divided into superficial and deep portions. It is the primary, restraint to valgus tilting of the talus.
Page 3833 :
Lateral side: Lateral ligament complex consisting from anterior to posterior of the anterior talofibular, ligament (ATFL), calcaneofibular ligament (CFL), and the posterior talofibular ligament (PTFL)., Together they resist valgus stress to the ankle, and are a restraint to anterior translation of the talus, within the mortise joint., Syndesmosis: The syndesmosis is a ligament complex between the distal tibia and fibula, holding, the two bones together. It is fundamental to the integrity of the ankle joint, and its disruption leads to, instability. It consists of (from anterior to posterior) the anterior-inferior tibiofibular ligament (AITFL),, the transverse tibiofibular ligament (TTFL), the interosseous membrane, and the posterior-inferior, tibiofibular ligament (PITFL)., Presentation and initial management, Patients will present following a traumatic event with a painful, swollen ankle, and reluctance/inability, to weight bear. The Ottawa rules can be applied to differentiate between an ankle fracture and, sprain, but can be unreliable., In high energy injuries, management should follow ATLS principles to identify more significant, injuries first. Neurovascular status of the foot should be documented, and open injuries should be, excluded. If an open injury is identified, it should be managed in line with BOAST 4 principles1. If an, obvious deformity exists, it should be reduced as soon as possible with appropriate analgesia or, conscious sedation. Radiographs of clearly deformed or dislocated joints are not necessary, and, removing the pressure on the surrounding soft tissues from the underlying bony deformity is the, priority. If the fracture pattern is not clinically obvious then plain radiographs are appropriate and will, guide the subsequent manipulation during plaster-of-paris below knee backslab application., Imaging, AP, lateral and mortise views (20o internal rotation) are essential to evaluate fracture displacement, and syndesmotic injury. Decreased tibiofibular overlap, medial joint clear space and lateral talar shift, all indicate a syndesmotic injury. (In subtle cases of shift, imaging the uninjured ankle can be helpful, as a proportion of the population have little or no tibiotalar overlap 2.), Where there is suspicion of syndesmosis involvement in the absence of radiographic evidence,, stress radiographs can be diagnostic., Complex fracture patterns (and increasingly posterior malleolar fractures) are best defined using, CT., , Classification, The most commonly used classifications are Lauge-Hansen and Danis-Weber., Lauge-Hansen, Comprises two parts: first part is the foot position, and the second part is the force applied. Useful for, understanding the forces involved and therefore predict the ligamentous or bony injury. Results in, four injury patterns:, Supination - Adduction (SA) - 10-20%
Page 3834 :
Supination - External rotation (SER) - 40-75%, Pronation - Abduction (PA) - 5-20%, Pronation - External rotation (PER) - 5-20%, Not often used in clinical practice but good for understanding the principles of ankle fracture., Danis-Weber, Commonly used. Based on the level of the fibula fracture in relation to the syndesmosis. The more, proximal, the greater the risk of syndesmotic injury and therefore fracture instability., A - fracture below the level of the syndesmosis, B - fracture at the level of the syndesmosis / level of the tibial plafond, C - fracture above the level of the syndesmosis. This includes Maisonneuve fractures (proximal, fibula fracture), which can be associated with ankle instability. Beware the high fibula fracture - it, may be an ankle fracture!, The Weber classification is based purely on the the lateral side. All injuries can include a medial or, posterior bony or ligamentous injury which also dictates fracture stability (bimalleolar and trimalleolar, fractures are more unstable)., Treatment, When deciding upon treatment for an ankle fracture, one must consider both the fracture and the, patient. Diabetic patients and smokers are at greater risk of post-operative complication, especially, wound problems and infection. Likewise, the long term outcome of post-traumatic arthritis from a, malunited ankle fracture is extremely important for a young patient, but not as relevant in the elderly., Therefore, normal surgical decision processes apply as with all fractures., Defining stability of an ankle fracture underpins the treatment decision., Weber A - Unimalleolar Weber A Weber fractures by definition are stable and therefore can be, mobilised fully weight bearing in an ankle boot., Weber C - Fractures tend to include syndesmotic disruption and are usually bimalleolar (either bony, or ligamentous). They are therefore unstable and usually require operative fixation. In addition to the, fracture fixation, the syndesmosis usually requires reconstruction/augmentation with screws to, restore the joint integrity and function., Weber B - B fractures vary greatly. They can be part of a trimalleolar injury and therefore extremely, unstable, requiring fixation. Alternatively, a uni-malleolar Weber B fracture can be a stable injury,, and therefore mobilised immediately in an ankle boot. Defining the stability can be challenging, and, often involves stress radiographs, or a trial of mobilisation and repeat radiographs. Defining stability, is the subject of much ongoing research. However, treating undisplaced ankle fractures in a below, knee plaster, non-weight bearing for six weeks is still widely practised, and a safe approach., When operative fixation is appropriate, it is usually via open reduction and internal fixation using, plates and screws. It must be carried out when soft tissue swelling has settled in order to minimise, the risk of wound problems. This can often take a week to settle.
Page 3835 :
The use of fibula nails is expanding, but is not yet mainstream. Ankle fractures can also be treated, with external fixation, or with a hind foot nail in patients who need fixation but where soft tissue or, bone quality is poor., , Post operative management, Ankle fractures generally take 6 weeks to unite enough to prevent secondary displacement. This is, therefore an appropriate time period to keep a cast on in a conservatively managed patient. Weight, bearing post-operatively depends on the quality of the fixation and bone quality, and preference, varies between surgeons, ranging from aggressive early mobilisation to a period of non-weight, bearing. Return to activities takes approximately three months, and often requires assistance of a, physiotherapist to improve range-of-movement and muscle strengthening., References, 1. http://www.boa.ac.uk/publications/boa-standards-trauma-boasts/, 2. Shah AS, Kadakia AR, Tan GJ, Karadsheh MS, Wolter TD, Sabb B. Radiographic evaluation of, the normal distal tibiofibular syndesmosis. Foot Ankle Int. 2012;33(10):870-6, Next question
Page 3836 :
Theme: Management of hip fractures, , A. MRI scan, B. Hemiarthroplasty, C. Bone scintigraphy, D. Conservative management, E. Total hip replacement, F. Insertion of intra medullary nail, G. Hip arthrodesis, H. Internal fixation, , For each fracture scenario please select the most appropriate management option from the list., Each option may be used once, more than once or not at all., , 73., , An otherwise fit 74 year old man presents with pain in the right hip following minimal trauma. On, examination his leg is shortened and externally rotated. Plain films demonstrate a displaced, intracapsular fracture of the femoral neck., You answered MRI scan, The correct answer is Total hip replacement, In otherwise fit patients aged over 70, the best long term functional outcomes are obtained with, total hip arthroplasty., , 74., , A 72 year old retired teacher is admitted to A&E with a fall and hip pain. He is normally fit and, well. He lives with his son in a detached, 2 storey house. A hip x-ray confirms an subtrochanteric, fracture., You answered MRI scan, The correct answer is Insertion of intra medullary nail
Page 3837 :
Intramedullary devices are normally recommended for reverse oblique, transverse, subtrochanteric fractures., , 75., , A 72 year old lady stumbles and falls. On examination she is tender in the left groin and unable to, weight bear. Attempts at internal rotation produce severe pain. Plain films show of the hip show, no obvious fracture., MRI scan, In those patients who present with a suspected hip fracture, but normal plain films the most, accurate investigation is an MRI or CT scan., , Please rate this question:, , Discuss and give feedback, , Next question, , Hip fractures, Background, Neck of femur (NOF) fracture is a common orthopaedic presentation, with over 65000 fractures in, the UK per year. Like many orthopaedic injuries, there is a bimodal age distribution. It is imperative, to distinguish between the high energy injury in a young patient, and the low energy osteoporotic, fracture in the elderly, as their management aims are very different:, Young patient - Usually high energy trauma (e.g road traffic accident, horse riding) and needs, treating in accordance with Advanced Trauma Life Support (ATLS) principles. Will often have, associated injuries. Aim is to retain the patients own anatomy, and optimise their function., Elderly patient - Predominantly female, fall from standing height (fragility fracture). Often patients, have multiple comorbidities that will ultimately dictate their prognosis. Aim of orthopaedic treatment, is to immediately regain patient mobility so that morbidity (infection, thromboembolic events,, pressure sores etc) and mortality associated with prolonged bed rest is avoided. Left untreated, a, neck of femur fracture can be considered a terminal event. Historically, mortality associated with, elderly hip fracture is 10% at one month, and 30% at one year. However, this has been improved in
Page 3838 :
the UK with the introduction of multidisciplinary, orthogeriatric lead care and the National Hip, Fracture Database and Best Practice Tariff., Pertinent anatomy, Osteology - normal neck-shaft angle is 130 +/- 7 degrees, and 10 +/- 7 degrees of neck anteversion., Vascular supply - The predominant blood supply to the femoral head and neck is from the medial, and lateral femoral circumflex arteries (branches of profunda femoris). These anastomose and, pierce the joint capsule at the base of the neck, mainly posteriorly. There is a small vascular, contribution from the artery of the ligament teres. Understanding the blood supply is fundamental to, the decision making process in treating NOF fractures., Presentation and initial management, Typically, patients present with pain in the hip/groin, a shortened, abducted, externally rotated leg, (due to the unopposed pull of the muscles that act across the hip joint) and the inability to straightleg-raise. With undisplaced fractures, signs are more subtle., High energy injuries should be treated in line with ATLS principles. All patients should be fluid, resuscitated, have adequate pain relief (often with a fascio-iliiaca nerve block), and be optimised for, surgery. In addition, elderly patients should be assessed by an orthogeriatrician., Imaging, Anteroposterior and cross-table lateral plain radiographs are sufficient to diagnose the majority of, NOF fractures. If the fracture extends below the level of the lesser trochanter, or there is any, possibility of pathological fracture, full length femur views are essential to plan surgery., Where there is a high index of suspicion of fracture, but plain radiographs are inconclusive, gold, standard investigation is MRI. However, if unavailable within 24 hours, or if the patient will not, tolerate MRI, CT is appropriate. The majority of fractures can be seen with modern CT techniques,, and so this is becoming first line in many hospitals., Classification, There has been a move away from named classification systems towards descriptive classification, systems., Two main types of NOF exist: Intra-capsular, and extra-capsular. Extra-capsular fractures are further, divided into pertrochanteric or subtrochanteric (within 5cm distal to the lesser trochanter). All, fractures are then described as undisplaced, minimally displaced, or displaced., Femoral neck and head blood supply disruption is common with intracapsular NOF fractures, and, rare with extracapsular fractures. This fundamental principle underpins the practise of arthroplasty, for intracapsular fractures, and fixation for extracapsular fractures., If you wish to use a named classification system, the most commonly used are below:, Elderly intracapsular - Garden Classification, Young intrasapsular - Pauvels Classification, Intertrochanteric - Evans, Subtrochanteric - Russell Taylor, Treatment
Page 3839 :
In general, NOF fractures are treated operatively except if the patient is deemed unlikely to survive, an anaesthetic. Best Practice Tarif (BPT) dictates that surgery should happen within 36 hours, as, delay of greater than 48 hours is associated with increased morbidity and mortality. Below are, suggested algorithms for the treatment of NOF. There are some areas of debate/controversy which, are detailed below., , Image sourced from Wikipedia, , * The priority with the young patient is to retain the femoral head if possible, even with a displaced, intracapsular fracture. The risk of avascular necrosis and non-union (and therefore revision surgery), associated with internal fixation needs weighing up against the sequelae of total hip replacement in, the young (wear, dislocation, revision). Discussion is necessary with the patient, on a case by case, basis., ** Undisplaced fractures in the elderly can be treated with internal fixation, often with cannulated, screws. This is appropriate for valgus impacted subcapital fractures which are inherently stable, to, prevent secondary displacement. This does still carry the risk of AVN or non-union, and therefore a, future revision. For this reason, many surgeons advocate arthroplasty as a single surgery., *** NICE guidance - patients who fulfil these criteria should be offered total hip replacement which, conveys better function and prosthetic survivorship, compared with hemiarthroplasty, but at an, increased risk of dislocation.
Page 3840 :
Image sourced from Wikipedia, , * Intertrochanteric fractures vary greatly in their stability. If the trochanter (and therefore lateral wall),, and medial calcar is in tact, then the fracture configuration bears stability. This can be treated with a, DHS, as collapse of the fracture is predictable. Where either or both structures are involved in the, fracture, stability becomes compromised and many surgeons will favour using an intramedullary, device. This is an ongoing debate, and difficult to test in an exam setting., Post operative management, Patients should be mobilised fully weight bearing where possible. Care is multidisciplinary in its, delivery. Elderly patients should have orthogeriatrician assessment of comorbidity, and bone health, with secondary prevention measures if appropriate. There should be early involvement of, physiotherapy and occupational therapy services. For further guidance see sources listed below., NICE clinical guidance on hip fracture: https://www.nice.org.uk/guidance/cg124, Best Practice Tarif:, www.nhfd.co.uk/20/hipfractureR.../Best%20Practice%20Tariff%20User%20Guide.pdf, National Hip Fracture Database: www.nhfd.co.uk/, Next question
Page 3841 :
Theme: Paediatric orthopaedics, , A. USS hip, B. Hip x-ray, C. Anteroposterior pelvic x-ray, D. CT scan, E. MRI scan, F. Technetium bone scan, G. USS knee, H. X-ray knee, I. Discharge and reassure, , For each of the following scenarios which is the most appropriate investigation? Each option may be, used once, more than once or not at all., , 76., , An obese 12 year old boy presents with knee pain. On examination he has pain on internal, rotation of the hip. His knee is clinically normal., You answered USS hip, The correct answer is Hip x-ray, The main differential diagnosis in a boy over 10 years old is of slipped upper femoral epiphysis., Knee pain is a common presenting feature. An anteroposterior pelvic x-ray may miss a minor slip,, therefore request a hip film., , 77., , A baby is delivered in the breech position. Barlows and Ortolani tests are normal, USS hip, This child is at risk of developmental dysplasia of the hip (up to 20% will have DDH), so should
Page 3842 :
have the hip joints scanned to exclude this., , 78., , A 5 year old boy presents with a painful limp. The symptoms have been present for 8 weeks. Two, hip x-rays have been performed and appear normal., You answered USS hip, The correct answer is Technetium bone scan, Perthes disease should be suspected in boys over 4 years old presenting with a limp. Early disease, can be missed on x-ray, therefore a bone scan should be performed. MRI is less sensitive than the, bone scan., , Please rate this question:, , Discuss and give feedback, , Next question, , Paediatric orthopaedics, Diagnosis, , Mode of presentation, , Treatment, , Radiology, , Developmental, dysplasia of the, hip, , Usually diagnosed in infancy, by screening tests. May be, bilateral, when disease is, unilateral there may be leg, length inequality. As, disease progresses child, may limp and then early, onset arthritis. More, common in extended, breech babies., , Splints and harnesses or, traction. In later years, osteotomy and hip, realignment procedures may, be needed. In arthritis a joint, replacement may be needed., However, this is best, deferred if possible as it will, almost certainly require, revision, , Initially no obvious, change on plain films, and USS gives best, resolution until 3, months of age. On, plain films Shentons, line should form a, smooth arc
Page 3843 :
Perthes Disease, , Hip pain (may be referred, to the knee) usually, occurring between 5 and 12, years of age. Bilateral, disease in 20%., , Remove pressure from joint, to allow normal, development. Physiotherapy., Usually self-limiting if, diagnosed and treated, promptly., , X-rays will show, flattened femoral, head. Eventually in, untreated cases the, femoral head will, fragment., , Slipped upper, femoral, epiphysis, , Typically seen in obese, male adolescents. Pain is, often referred to the knee., Limitation to internal, rotation is usually seen., Knee pain is usually present, 2 months prior to hip, slipping. Bilateral in 20%., , Bed rest and non-weight, bearing. Aim to avoid, avascular necrosis. If severe, slippage or risk of it occurring, then percutaneous pinning of, the hip may be required., , X-rays will show the, femoral head displaced, and falling, inferolaterally (like a, melting ice cream, cone) The Southwick, angle gives indication, of disease severity, , Next question
Page 3844 :
A 5 year old boy is playing in a tree when he falls and lands on his right forearm. He is brought to the, emergency department by his parents. On examination he has bony tenderness and bruising. An Xray is taken and shows unilateral cortical disruption and development of periosteal haematoma., What is the most likely diagnosis?, , Buckle fracture, , Greenstick fracture, , Toddlers fracture, , Complete fracture, , None of the above, , Greenstick fractures are common childhood injuries. Unilateral cortical disruption is the main, radiological feature, since involvement of both cortices makes the injury a complete fracture. Buckle, fractures will show periosteal haematoma formation only., Please rate this question:, , Discuss and give feedback, , Next question, , Paediatric fractures, Paediatric fracture types, , Type, , Injury pattern, , Complete fracture, , Both sides of cortex are breached, , Toddlers fracture, , Oblique tibial fracture in infants, , Plastic deformity, , Stress on bone resulting in deformity without cortical disruption
Page 3845 :
Greenstick fracture, , Unilateral cortical breach only, , Buckle fracture, , Incomplete cortical disruption resulting in periosteal haematoma only, , Growth plate fractures, In paediatric practice fractures may also involve the growth plate and these injuries are classified, according to the Salter- Harris system (given below):, , Type, , Injury pattern, , I, , Fracture through the physis only (x-ray often normal), , II, , Fracture through the physis and metaphysis, , III, , Fracture through the physis and epiphyisis to include the joint, , IV, , Fracture involving the physis, metaphysis and epiphysis, , V, , Crush injury involving the physis (x-ray may resemble type I, and appear normal), , As a general rule it is safer to assume that growth plate tenderness is indicative of an underlying, fracture even if the x-ray appears normal. Injuries of Types III, IV and V will usually require surgery., Type V injuries are often associated with disruption to growth., Non accidental injury, , , , , , , , Delayed presentation, Delay in attaining milestones, Lack of concordance between proposed and actual mechanism of injury, Multiple injuries, Injuries at sites not commonly exposed to trauma, Children on the at risk register, , Pathological fractures, Genetic conditions, such as osteogenesis imperfecta, may cause pathological fractures.
Page 3846 :
Osteogenesis imperfecta, , , , , Defective osteoid formation due to congenital inability to produce adequate intercellular, substances like osteoid, collagen and dentine., Failure of maturation of collagen in all the connective tissues., Radiology may show translucent bones, multiple fractures, particularly of the long bones,, wormian bones (irregular patches of ossification) and a trefoil pelvis., , Subtypes, , , , , , Type I The collagen is normal quality but insufficient quantity., Type II- Poor collagen quantity and quality., Type III- Collagen poorly formed. Normal quantity., Type IV- Sufficient collagen quantity but poor quality., , Osteopetrosis, , , , , , Bones become harder and more dense., Autosomal recessive condition., It is commonest in young adults., Radiology reveals a lack of differentiation between the cortex and the medulla described as, marble bone., Next question
Page 3847 :
Which of the following is not typically seen in patients with a femoral neck fracture?, , Malunion, , Non union, , Avascular necrosis, , Shortening, , External rotation, , Malunion would be unusual with a femoral neck fracture. Because it is a weight bearing joint, if the, fracture is not united then it does not heal at all. It is for this reason that most femoral neck fractures, are fixed. Avascular necrosis is a well recognised complication and a total hip replacement or, hemiarthroplasty is usually considered in the elderly., Please rate this question:, , Discuss and give feedback, , Next question, , Hip fractures, Background, Neck of femur (NOF) fracture is a common orthopaedic presentation, with over 65000 fractures in, the UK per year. Like many orthopaedic injuries, there is a bimodal age distribution. It is imperative, to distinguish between the high energy injury in a young patient, and the low energy osteoporotic, fracture in the elderly, as their management aims are very different:, Young patient - Usually high energy trauma (e.g road traffic accident, horse riding) and needs, treating in accordance with Advanced Trauma Life Support (ATLS) principles. Will often have, associated injuries. Aim is to retain the patients own anatomy, and optimise their function.
Page 3848 :
Elderly patient - Predominantly female, fall from standing height (fragility fracture). Often patients, have multiple comorbidities that will ultimately dictate their prognosis. Aim of orthopaedic treatment, is to immediately regain patient mobility so that morbidity (infection, thromboembolic events,, pressure sores etc) and mortality associated with prolonged bed rest is avoided. Left untreated, a, neck of femur fracture can be considered a terminal event. Historically, mortality associated with, elderly hip fracture is 10% at one month, and 30% at one year. However, this has been improved in, the UK with the introduction of multidisciplinary, orthogeriatric lead care and the National Hip, Fracture Database and Best Practice Tariff., Pertinent anatomy, Osteology - normal neck-shaft angle is 130 +/- 7 degrees, and 10 +/- 7 degrees of neck anteversion., Vascular supply - The predominant blood supply to the femoral head and neck is from the medial, and lateral femoral circumflex arteries (branches of profunda femoris). These anastomose and, pierce the joint capsule at the base of the neck, mainly posteriorly. There is a small vascular, contribution from the artery of the ligament teres. Understanding the blood supply is fundamental to, the decision making process in treating NOF fractures., Presentation and initial management, Typically, patients present with pain in the hip/groin, a shortened, abducted, externally rotated leg, (due to the unopposed pull of the muscles that act across the hip joint) and the inability to straightleg-raise. With undisplaced fractures, signs are more subtle., High energy injuries should be treated in line with ATLS principles. All patients should be fluid, resuscitated, have adequate pain relief (often with a fascio-iliiaca nerve block), and be optimised for, surgery. In addition, elderly patients should be assessed by an orthogeriatrician., Imaging, Anteroposterior and cross-table lateral plain radiographs are sufficient to diagnose the majority of, NOF fractures. If the fracture extends below the level of the lesser trochanter, or there is any, possibility of pathological fracture, full length femur views are essential to plan surgery., Where there is a high index of suspicion of fracture, but plain radiographs are inconclusive, gold, standard investigation is MRI. However, if unavailable within 24 hours, or if the patient will not, tolerate MRI, CT is appropriate. The majority of fractures can be seen with modern CT techniques,, and so this is becoming first line in many hospitals., Classification, There has been a move away from named classification systems towards descriptive classification, systems., Two main types of NOF exist: Intra-capsular, and extra-capsular. Extra-capsular fractures are further, divided into pertrochanteric or subtrochanteric (within 5cm distal to the lesser trochanter). All, fractures are then described as undisplaced, minimally displaced, or displaced., Femoral neck and head blood supply disruption is common with intracapsular NOF fractures, and, rare with extracapsular fractures. This fundamental principle underpins the practise of arthroplasty, for intracapsular fractures, and fixation for extracapsular fractures., If you wish to use a named classification system, the most commonly used are below:
Page 3849 :
Elderly intracapsular - Garden Classification, Young intrasapsular - Pauvels Classification, Intertrochanteric - Evans, Subtrochanteric - Russell Taylor, Treatment, In general, NOF fractures are treated operatively except if the patient is deemed unlikely to survive, an anaesthetic. Best Practice Tarif (BPT) dictates that surgery should happen within 36 hours, as, delay of greater than 48 hours is associated with increased morbidity and mortality. Below are, suggested algorithms for the treatment of NOF. There are some areas of debate/controversy which, are detailed below., , Image sourced from Wikipedia, , * The priority with the young patient is to retain the femoral head if possible, even with a displaced, intracapsular fracture. The risk of avascular necrosis and non-union (and therefore revision surgery), associated with internal fixation needs weighing up against the sequelae of total hip replacement in, the young (wear, dislocation, revision). Discussion is necessary with the patient, on a case by case, basis., ** Undisplaced fractures in the elderly can be treated with internal fixation, often with cannulated, screws. This is appropriate for valgus impacted subcapital fractures which are inherently stable, to, prevent secondary displacement. This does still carry the risk of AVN or non-union, and therefore a, future revision. For this reason, many surgeons advocate arthroplasty as a single surgery., *** NICE guidance - patients who fulfil these criteria should be offered total hip replacement which, conveys better function and prosthetic survivorship, compared with hemiarthroplasty, but at an
Page 3850 :
increased risk of dislocation., , Image sourced from Wikipedia, , * Intertrochanteric fractures vary greatly in their stability. If the trochanter (and therefore lateral wall),, and medial calcar is in tact, then the fracture configuration bears stability. This can be treated with a, DHS, as collapse of the fracture is predictable. Where either or both structures are involved in the, fracture, stability becomes compromised and many surgeons will favour using an intramedullary, device. This is an ongoing debate, and difficult to test in an exam setting., Post operative management, Patients should be mobilised fully weight bearing where possible. Care is multidisciplinary in its, delivery. Elderly patients should have orthogeriatrician assessment of comorbidity, and bone health, with secondary prevention measures if appropriate. There should be early involvement of, physiotherapy and occupational therapy services. For further guidance see sources listed below., NICE clinical guidance on hip fracture: https://www.nice.org.uk/guidance/cg124, Best Practice Tarif:, www.nhfd.co.uk/20/hipfractureR.../Best%20Practice%20Tariff%20User%20Guide.pdf, National Hip Fracture Database: www.nhfd.co.uk/, Next question
Page 3851 :
Theme: Eponymous fractures, , A., B., C., D., E., F., G., , Smith's, Bennett's, Monteggia's, Colle's, Galeazzi, Pott's, Barton's, , Which is the most likely eponymous fracture for the scenario given. Each option may be used once,, more than once or not at all., , 81., , A 14 year old boy jumps off a 10 foot wall and lands on both feet. An x-ray shows a, bimalleolar fracture of the right ankle., You answered Smith's, The correct answer is Pott's, , 82., , A 22 year old drunk man is involved in a fight. He hurts his thumb when he punches his, opponent., You answered Smith's, The correct answer is Bennett's, , 83., , A 63 year nurse falls on an extended and pronated wrist. An x-ray shows a distal radial, fracture with radiocarpal dislocation., You answered Smith's, The correct answer is Barton's, , Please rate this question:, , Discuss and give feedback, , Next question
Page 3852 :
Eponymous fractures, Colles' fracture (dinner fork deformity), , , , Fall onto extended outstretched hand, Classical Colles' fractures have the following 3 features:, , 1. Transverse fracture of the radius, 2. 1 inch proximal to the radio-carpal joint, 3. Dorsal displacement and angulation, Smith's fracture (reverse Colles' fracture), , , , Volar angulation of distal radius fragment (Garden spade deformity), Caused by falling backwards onto the palm of an outstretched hand or falling with wrists, flexed, , Bennett's fracture, , , , , Intra-articular fracture of the first carpometacarpal joint, Impact on flexed metacarpal, caused by fist fights, X-ray: triangular fragment at ulnar base of metacarpal, , Image sourced from Wikipedia
Page 3853 :
Monteggia's fracture, , , , , Dislocation of the proximal radioulnar joint in association with an ulna fracture, Fall on outstretched hand with forced pronation, Needs prompt diagnosis to avoid disability, , Image sourced from Wikipedia, , Galeazzi fracture, , , , Radial shaft fracture with associated dislocation of the distal radioulnar joint, Direct blow, , Pott's fracture, , , , Bimalleolar ankle fracture, Forced foot eversion, , Barton's fracture
Page 3854 :
, , , , Distal radius fracture (Colles'/Smith's) with associated radiocarpal dislocation, Fall onto extended and pronated wrist, Involvement of the joint is a defining feature, Next question
Page 3855 :
Theme: Fracture management, , A., B., C., D., , Application of external fixator, Open reduction and internal fixation, Fasciotomy, Skeletal traction, , For the following upper limb injuries please select the most appropriate initial management. Each, option may be used once, more than once or not at all., , 84., , A 32 year old man falls from a ladder and sustains a fracture of his proximal radius. On, examination, he has severe pain in his forearm and diminished distal sensation. There is a, single puncture wound present at the fracture site., You answered Application of external fixator, The correct answer is Fasciotomy, Theme from April 2012 Exam, Pain and neurological symptoms in a tight fascial compartment coupled with a high, velocity injury carry a high risk of compartment syndrome and prompt fasciotomy should, be performed., , 85., , A 32 year old man falls a sustains a fracture of his distal humerus. The fracture segment is, markedly angulated and unstable. There is a puncture site overlying the fracture site., Application of external fixator, Wide exposure to plate the humerus is generally inadvisable owing to its many important, anatomical relations. Both intramedullary nailing and external fixation are reasonable, treatments. However, in the presence of an open fracture application of an external fixator, and appropriate tissue debridement would be most appropriate., , 86., , A 24 year old man sustains a distal radius fracture during a game of rugby. Imaging shows, a comminuted fracture with involvement of the articular surface., You answered Application of external fixator, The correct answer is Open reduction and internal fixation, Meticulous anatomical alignment of the fracture segments is crucial to avoid the, development of osteoarthritis and risk of malunion.
Page 3856 :
Please rate this question:, , Discuss and give feedback, , Next question, , Fracture management, , , , , Bony injury resulting in a fracture may arise from trauma (excessive forces applied to bone),, stress related (repetitive low velocity injury) or pathological (abnormal bone which fractures, during normal use of following minimal trauma), Diagnosis involves not just evaluating the fracture ; such as site and type of injury but also, other associated injuries and distal neurovascular deficits. This may entail not just clinical, examination but radiographs of proximal and distal joints., When assessing x-rays it is important to assess for changes in length of the bone, the, angulation of the distal bone, rotational effects, presence of material such as glass., , Fracture types, , Fracture type, , Description, , Oblique fracture, , Fracture lies obliquely to long axis of bone, , Comminuted fracture, , >2 fragments, , Segmental fracture, , More than one fracture along a bone, , Transverse fracture, , Perpendicular to long axis of bone, , Spiral fracture, , Severe oblique fracture with rotation along long axis of bone, , Open Vs Closed, It is also important to distinguish open from closed injuries. The most common classification system, for open fractures is the Gustilo and Anderson classification system (given below):, , Grade, , Injury, , 1, , Low energy wound <1cm
Page 3857 :
Grade, , Injury, , 2, , Greater than 1cm wound with moderate soft tissue damage, , 3, , High energy wound > 1cm with extensive soft tissue damage, , 3 A (sub group of 3), , Adequate soft tissue coverage, , 3 B (sub group of 3), , Inadequate soft tissue coverage, , 3 C (sub group of 3), , Associated arterial injury, , Key points in management of fractures, , , , , , , , Immobilise the fracture including the proximal and distal joints, Carefully monitor and document neurovascular status, particularly following reduction and, immobilisation, Manage infection including tetanus prophylaxis, IV broad spectrum antibiotics for open injuries, As a general principle all open fractures should be thoroughly debrided ( and internal fixation, devices avoided or used with extreme caution), Open fractures constitute an emergency and should be debrided and lavaged within 6 hours, of injury, Next question
Page 3858 :
Theme: Fracture management, , A. Copious lavage and generous surgical debridement, followed by, external fixation, B. Intramedullary nail, C. Open reduction and internal fixation, D. Immobilisation in plaster cast, E. External fixation using a frame device, F. Amputation, G. Application of external fixation device, H. Primary closure of wound and application of plaster cast, Please select the most appropriate management for the fractures described. Each option may be, used once, more than once or not at all., , 87., , A 55 year old motorcyclist is involved in a road traffic accident and sustained a Gustilo, and Anderson IIIc type fracture to the distal tibia. He was trapped in the wreckage for 7, hours during which time he bled profusely from the fracture site. He has an established, distal neurovascular deficit., You answered Copious lavage and generous surgical debridement, followed by, external fixation, The correct answer is Amputation, This man is unstable, and at 7 hours after extraction, the limb is not viable. The safest, option is primary amputation., , 88., , A 25 year old ski instructor who falls off a ski lift and sustains a spiral fracture of the mid, shaft of the tibia. Attempts to achieve satisfactory position in plaster have failed., Overlying tissues are healthy., You answered Copious lavage and generous surgical debridement, followed by, external fixation, The correct answer is Intramedullary nail, This would be a good case for intramedullary nailing. Open reduction and external fixation, would strip off otherwise healthy tissues and hence is unsuitable. In some units the injury, may be managed with an Ilizarov frame device but the majority would treat with IM, nailing., , 89., , A 35 year old mechanic is hit by a fork lift truck. He sustains a Gustilo and Anderson type, IIIA fracture of the shaft of the left femur.
Page 3859 :
Copious lavage and generous surgical debridement, followed by external fixation, At the tissues are in better shape than in the first case and as there is no associated vascular, injury the patient may be suitable for debridement of the area and external fixation. If, debridement leaves a tissue defect then plastic surgical repair will be needed at a later, stage., Delayed treatment of open fractures with significant vascular injury may be best treated by primary, amputation., Please rate this question:, , Discuss and give feedback, , Fracture management, , , , , Bony injury resulting in a fracture may arise from trauma (excessive forces applied to bone),, stress related (repetitive low velocity injury) or pathological (abnormal bone which fractures, during normal use of following minimal trauma), Diagnosis involves not just evaluating the fracture ; such as site and type of injury but also, other associated injuries and distal neurovascular deficits. This may entail not just clinical, examination but radiographs of proximal and distal joints., When assessing x-rays it is important to assess for changes in length of the bone, the, angulation of the distal bone, rotational effects, presence of material such as glass., , Fracture types, , Fracture type, , Description, , Oblique fracture, , Fracture lies obliquely to long axis of bone, , Comminuted fracture, , >2 fragments, , Segmental fracture, , More than one fracture along a bone, , Transverse fracture, , Perpendicular to long axis of bone, , Spiral fracture, , Severe oblique fracture with rotation along long axis of bone
Page 3860 :
Open Vs Closed, It is also important to distinguish open from closed injuries. The most common classification system, for open fractures is the Gustilo and Anderson classification system (given below):, , Grade, , Injury, , 1, , Low energy wound <1cm, , 2, , Greater than 1cm wound with moderate soft tissue damage, , 3, , High energy wound > 1cm with extensive soft tissue damage, , 3 A (sub group of 3), , Adequate soft tissue coverage, , 3 B (sub group of 3), , Inadequate soft tissue coverage, , 3 C (sub group of 3), , Associated arterial injury, , Key points in management of fractures, , , , , , , , Immobilise the fracture including the proximal and distal joints, Carefully monitor and document neurovascular status, particularly following reduction and, immobilisation, Manage infection including tetanus prophylaxis, IV broad spectrum antibiotics for open injuries, As a general principle all open fractures should be thoroughly debrided ( and internal fixation, devices avoided or used with extreme caution), Open fractures constitute an emergency and should be debrided and lavaged within 6 hours, of injury
Page 3861 :
Theme: Paediatric gastrointestinal disorders, , A., B., C., D., E., F., G., H., I., J., , Liver transplant, Rectal biopsy, Roux-en-Y portojejunostomy, Ramstedt pyloromyotomy, Abdominal CT scan, Upper GI contrast study, Laparotomy and formation of stoma, Laparotomy, Colonoscopy, Gastroscopy, , What is the best management option for these children? Each option may be used once, more than, once or not at all., , 1., , A male infant, born at term appears well following delivery. Six hours later, he is noted to, have bilious vomiting by the paediatricians. On examination he seems well and his, abdomen is soft and non tender., You answered Liver transplant, The correct answer is Upper GI contrast study, Bilious vomiting in neonates is a surgical emergency and is intestinal malrotation and, volvulus until otherwise proven. It is investigated with an upper GI contrast study. Contrast, should be seen to exit the stomach and the location of the DJ flexure is noted (it lies to the, left of the midline). If this is not the case, or the study is inconclusive, a laparotomy is, performed., , 2., , A 2 month old baby presents with jaundice. He has an elevated conjugated bilirubin level., Diagnosis is confirmed by cholangiography during surgery., You answered Liver transplant, The correct answer is Roux-en-Y portojejunostomy, This child has biliary atresia. The aim is to avoid liver transplantation (however, most will, come to transplant in time)., , 3., , A male infant, born at term by normal vaginal delivery is well. However, 72 hours, following delivery, he has still not passed meconium. On examination, his abdomen is soft, and not particularly distended. He has a normally sited anus.
Page 3862 :
You answered Liver transplant, The correct answer is Rectal biopsy, Delayed passage of meconium is suggestive of Hirschsprung's disease and the investigation, of choice is full thickness suction rectal biopsy. If Hirschprungs is confirmed, then the, correct treatment is laparotomy and stoma formation. At between 9 and 12 months of age,, definitive surgery (usually resection and primary anastomosis) is performed., Please rate this question:, , Discuss and give feedback, , Next question, , Paediatric Gastrointestinal disorders, Pyloric stenosis, , , , , , , , M>F, 5-10% Family history in parents, Projectile non bile stained vomiting at 4-6 weeks of life, Diagnosis is made by test feed or USS, Treatment: Ramstedt pyloromyotomy (open or laparoscopic), , Acute appendicitis, , , , , Uncommon under 3 years, When occurs may present atypically, , Mesenteric, adenitis, , , , , Central abdominal pain and URTI, Conservative management, , Intussusception, , , , , , , Telescoping bowel, Proximal to or at the level of, ileocaecal valve, 6-9 months age, Colicky pain, diarrhoea and vomiting, sausage shaped mass, red jelly, stool., Treatment: reduction with air insufflation, , , , Malrotation, , , , , , High caecum at the midline, Feature in exomphalos, congenital diaphragmatic hernia, intrinsic, duodenal atresia, May be complicated by development of volvulus, infant with
Page 3863 :
, , , volvulus may have bile stained vomiting, Diagnosis is made by upper GI contrast study and USS, Treatment is by laparotomy, if volvulus is present (or at high risk of, occurring then a ladds procedure is performed, , Hirschsprung's, disease, , , , , , , , Absence of ganglion cells from myenteric and submucosal plexuses, Occurs in 1/5000 births, Full thickness rectal biopsy for diagnosis, Delayed passage of meconium and abdominal distension, Treatment is with rectal washouts initially, thereafter an anorectal, pull through procedure, , Oesophageal, atresia, , , , , , Associated with tracheo-oesophageal fistula and polyhydramnios, May present with choking and cyanotic spells following aspiration, VACTERL associations, , Meconium ileus, , , , , , Usually delayed passage of meconium and abdominal distension, Majority have cystic fibrosis, X-Rays may not show a fluid level as the meconium is viscid, (depends upon feeding), PR contrast studies may dislodge meconium, plugs and be therapeutic, Infants who do not respond to PR contrast and NG N-acetyl cysteine, will require surgery to remove the plugs, , , , Biliary atresia, , , , , , Jaundice > 14 days, Increased conjugated bilirubin, Urgent Kasai procedure, , Necrotising, enterocolitis, , , , , Prematurity is the main risk factor, Early features include abdominal distension and passage of bloody, stools, X-Rays may show pneumatosis intestinalis and evidence of free air, Increased risk when empirical antibiotics are given to infants beyond, 5 days, Treatment is with total gut rest and TPN, babies with perforations, will require laparotomy, , , , , , Next question
Page 3864 :
What is the most common abdominal emergency in children under 1 year of age?, , Appendicitis, , Intussusception, , Intestinal malrotation, , Pyloric stenosis, , Mid gut volvulus, , The commonest emergency in this age group is inguinal hernia followed by intussusception., Appendicitis is commoner in those older than 1 year of age., Please rate this question:, , Discuss and give feedback, , Next question, , Paediatric Gastrointestinal disorders, Pyloric stenosis, , , , , , , , M>F, 5-10% Family history in parents, Projectile non bile stained vomiting at 4-6 weeks of life, Diagnosis is made by test feed or USS, Treatment: Ramstedt pyloromyotomy (open or laparoscopic), , Acute appendicitis, , , , , Uncommon under 3 years, When occurs may present atypically, , Mesenteric, adenitis, , , , , Central abdominal pain and URTI, Conservative management, , Intussusception, , , , , , Telescoping bowel, Proximal to or at the level of, ileocaecal valve, 6-9 months age
Page 3865 :
, , , Malrotation, , , , , , , , Colicky pain, diarrhoea and vomiting, sausage shaped mass, red jelly, stool., Treatment: reduction with air insufflation, High caecum at the midline, Feature in exomphalos, congenital diaphragmatic hernia, intrinsic, duodenal atresia, May be complicated by development of volvulus, infant with, volvulus may have bile stained vomiting, Diagnosis is made by upper GI contrast study and USS, Treatment is by laparotomy, if volvulus is present (or at high risk of, occurring then a ladds procedure is performed, , Hirschsprung's, disease, , , , , , , , Absence of ganglion cells from myenteric and submucosal plexuses, Occurs in 1/5000 births, Full thickness rectal biopsy for diagnosis, Delayed passage of meconium and abdominal distension, Treatment is with rectal washouts initially, thereafter an anorectal, pull through procedure, , Oesophageal, atresia, , , , , , Associated with tracheo-oesophageal fistula and polyhydramnios, May present with choking and cyanotic spells following aspiration, VACTERL associations, , Meconium ileus, , , , , , Usually delayed passage of meconium and abdominal distension, Majority have cystic fibrosis, X-Rays may not show a fluid level as the meconium is viscid, (depends upon feeding), PR contrast studies may dislodge meconium, plugs and be therapeutic, Infants who do not respond to PR contrast and NG N-acetyl cysteine, will require surgery to remove the plugs, , , , Biliary atresia, , , , , , Jaundice > 14 days, Increased conjugated bilirubin, Urgent Kasai procedure, , Necrotising, enterocolitis, , , , , Prematurity is the main risk factor, Early features include abdominal distension and passage of bloody, stools, X-Rays may show pneumatosis intestinalis and evidence of free air, ,
Page 3866 :
, , , Increased risk when empirical antibiotics are given to infants beyond, 5 days, Treatment is with total gut rest and TPN, babies with perforations, will require laparotomy, Next question
Page 3867 :
Theme: Paediatric gastrointestinal disorders, , A., B., C., D., E., F., G., H., I., , Duodenal atresia, Hypertrophy of the pyloric sphincter, Budd Chiari Syndrome, Intussceception, Oesophageal atresia, Congenital diaphragmatic hernia, Cystic fibrosis, Intestinal malrotation, Gastroenteritis, , Please select the most likely diagnosis for the scenario given. Each option may be used once, more, than once or not at all., , 5., , A two week old child is brought to the emergency department by his parents. He was slow, to establish on feeds but was discharged home three days following delivery. During the, past 7 hours he has been vomiting and the vomit is largely bile stained. On examination he, has a soft, scaphoid abdomen., You answered Duodenal atresia, The correct answer is Intestinal malrotation, Theme from April 2013 Exam, The combination of scaphoid abdomen and bilious vomiting is highly suggestive of, intestinal malrotation and volvulus. An urgent upper GI contrast study and ultrasound is, required., , 6., , A 4 week old baby is developing well and develops profuse and projectile vomiting after, feeds. He has been losing weight and the vomit is described as being non bilious., You answered Duodenal atresia, The correct answer is Hypertrophy of the pyloric sphincter, A history of projective vomiting and weight loss is a common story suggestive of pyloric, stenosis. The vomit is often not bile stained. Diagnosis is further suggested by, hypochloraemic metabolic alkalosis and a palpable tumour on test feeding., , 7., , A 1 day old child is born by emergency cesarean section for foetal distress. On examination, he has decreased air entry on the left side of his chest and a displaced apex beat. Abdominal, examination demonstrates a scaphoid abdomen but is otherwise unremarkable.
Page 3868 :
You answered Duodenal atresia, The correct answer is Congenital diaphragmatic hernia, Displaced apex beat and decreased air entry are suggestive of diaphragmatic hernia. The, abdomen may well be scaphoid in some cases. The underlying lung may be hypoplastic and, this correlates directly with prognosis., Please rate this question:, , Discuss and give feedback, , Next question, , Paediatric Gastrointestinal disorders, Pyloric stenosis, , , , , , , , M>F, 5-10% Family history in parents, Projectile non bile stained vomiting at 4-6 weeks of life, Diagnosis is made by test feed or USS, Treatment: Ramstedt pyloromyotomy (open or laparoscopic), , Acute appendicitis, , , , , Uncommon under 3 years, When occurs may present atypically, , Mesenteric, adenitis, , , , , Central abdominal pain and URTI, Conservative management, , Intussusception, , , , , , , Telescoping bowel, Proximal to or at the level of, ileocaecal valve, 6-9 months age, Colicky pain, diarrhoea and vomiting, sausage shaped mass, red jelly, stool., Treatment: reduction with air insufflation, , , , Malrotation, , , , , , High caecum at the midline, Feature in exomphalos, congenital diaphragmatic hernia, intrinsic, duodenal atresia, May be complicated by development of volvulus, infant with, volvulus may have bile stained vomiting
Page 3869 :
, , , Diagnosis is made by upper GI contrast study and USS, Treatment is by laparotomy, if volvulus is present (or at high risk of, occurring then a ladds procedure is performed, , Hirschsprung's, disease, , , , , , , , Absence of ganglion cells from myenteric and submucosal plexuses, Occurs in 1/5000 births, Full thickness rectal biopsy for diagnosis, Delayed passage of meconium and abdominal distension, Treatment is with rectal washouts initially, thereafter an anorectal, pull through procedure, , Oesophageal, atresia, , , , , , Associated with tracheo-oesophageal fistula and polyhydramnios, May present with choking and cyanotic spells following aspiration, VACTERL associations, , Meconium ileus, , , , , , Usually delayed passage of meconium and abdominal distension, Majority have cystic fibrosis, X-Rays may not show a fluid level as the meconium is viscid, (depends upon feeding), PR contrast studies may dislodge meconium, plugs and be therapeutic, Infants who do not respond to PR contrast and NG N-acetyl cysteine, will require surgery to remove the plugs, , , , Biliary atresia, , , , , , Jaundice > 14 days, Increased conjugated bilirubin, Urgent Kasai procedure, , Necrotising, enterocolitis, , , , , Prematurity is the main risk factor, Early features include abdominal distension and passage of bloody, stools, X-Rays may show pneumatosis intestinalis and evidence of free air, Increased risk when empirical antibiotics are given to infants beyond, 5 days, Treatment is with total gut rest and TPN, babies with perforations, will require laparotomy, , , , , , Next question
Page 3870 :
A 1-day-old baby girl is noted to become profoundly cyanotic whilst feeding and crying. A diagnosis, of congenital heart disease is suspected. What is the most likely cause?, , Transposition of the great arteries, , Coarctation of the aorta, , Patent ductus arteriosus, , Hypoplastic left heart, , Ventricular septal defect, Congenital heart disease, , , , Cyanotic: TGA most common at birth, Fallot's most common overall, Acyanotic: VSD most common cause, , Theme from April 2011 exam, It is important to be aware of common congenital cardiac abnormalities. The main differentiating, factor is whether the patient is cyanotic or acyanotic. In the neonate, TGA is the most common, condition presenting with profound cyanosis., The other options are causes of acyanotic congenital heart disease, Please rate this question:, , Discuss and give feedback, , Next question, , Congenital heart disease, Acyanotic - most common causes, , , , , , , Ventricular septal defects (VSD) - most common, accounts for 30%, Atrial septal defect (ASD), Patent ductus arteriosus (PDA), Coarctation of the aorta, Aortic valve stenosis
Page 3872 :
A 6 month old boy is brought to the clinic by his mother. She is concerned that his testes are not, located into the scrotum. She has noticed them only when he is in the bath, but not at any other, time. What is the most likely underlying diagnosis?, , Retractile testis, , Ectopic testis, , Undescended testis, , Testicular agenesis, , Intersex child, , Theme from April 2012 Exam, A testis that appears in warm conditions or which can be brought down on clinical examination and, does not immediately retract is usually a retractile testis., Please rate this question:, , Discuss and give feedback, , Next question, , Cryptorchidism, A congenital undescended testis is one that has failed to reach the bottom of the scrotum by 3, months of age. At birth up to 5% of boys will have an undescended testis, post natal descent occurs, in most and by 3 months the incidence of cryptorchidism falls to 1-2%. In the vast majority of cases, the cause of the maldescent is unknown. A proportion may be associated with other congenital, defects including:, Patent processus vaginalis, Abnormal epididymis, Cerebral palsy, Mental retardation, Wilms tumour, Abdominal wall defects (e.g. gastroschisis, prune belly syndrome), Differential diagnosis, These include retractile testes and, in the case of absent bilateral testes the possibility of intersex, conditions. A retractile testis can be brought into the scrotum by the clinician and when released, remains in the scrotum. If the examining clinician notes the testis to return rapidly into the inguinal, canal when released then surgery is probably indicated.
Page 3873 :
Reasons for correction of cryptorchidism, , , , , , Reduce risk of infertility, Allows the testes to be examined for testicular cancer, Avoid testicular torsion, Cosmetic appearance, , Males with undescended testis are 40 times as likely to develop testicular cancer (seminoma) as, males without undescended testis, The location of the undescended testis affects the relative risk of testicular cancer (50% intraabdominal testes), Treatment, , , , , Orchidopexy at 6- 18 months of age. The operation usually consists of inguinal exploration,, mobilisation of the testis and implantation into a dartos pouch., Intra-abdominal testis should be evaluated laparoscopically and mobilised. Whether this is a, single stage or two stage procedure depends upon the exact location., After the age of 2 years in untreated individuals the Sertoli cells will degrade and those, presenting late in teenage years may be better served by orchidectomy than to try and, salvage a non functioning testis with an increased risk of malignancy., Next question
Page 3874 :
Which of the following statements relating to omphalocele is false?, , The herniated organs lie outside the peritoneal sac, , Cardiac abnormalities co-exist in 25%, , The caecum is usually right sided, , The defect occurs through the umbilicus, , Mortality may be as high as 15%, Gastroschisis: Isolated abnormality, bowel lies outside abdominal wall through defect located to right, of umbilicus., Exomphalos: Liver and gut remain covered with membranous sac connected to umbilical cord. It is, associated with other developmental defects., They are contained within the peritoneal sac and therefore do not have the fluid losses seen in, gastroschisis. True malrotation is unusual and minor variants may not result in a requirement for, surgery., Please rate this question:, , Discuss and give feedback, , Next question, , Paediatric Gastrointestinal disorders, Pyloric stenosis, , , , , , , , M>F, 5-10% Family history in parents, Projectile non bile stained vomiting at 4-6 weeks of life, Diagnosis is made by test feed or USS, Treatment: Ramstedt pyloromyotomy (open or laparoscopic), , Acute appendicitis, , , , , Uncommon under 3 years, When occurs may present atypically, , Mesenteric, adenitis, , , , Central abdominal pain and URTI
Page 3875 :
Intussusception, , , , Conservative management, , , , , , , Telescoping bowel, Proximal to or at the level of, ileocaecal valve, 6-9 months age, Colicky pain, diarrhoea and vomiting, sausage shaped mass, red jelly, stool., Treatment: reduction with air insufflation, , , , Malrotation, , , , , , , , High caecum at the midline, Feature in exomphalos, congenital diaphragmatic hernia, intrinsic, duodenal atresia, May be complicated by development of volvulus, infant with, volvulus may have bile stained vomiting, Diagnosis is made by upper GI contrast study and USS, Treatment is by laparotomy, if volvulus is present (or at high risk of, occurring then a ladds procedure is performed, , Hirschsprung's, disease, , , , , , , , Absence of ganglion cells from myenteric and submucosal plexuses, Occurs in 1/5000 births, Full thickness rectal biopsy for diagnosis, Delayed passage of meconium and abdominal distension, Treatment is with rectal washouts initially, thereafter an anorectal, pull through procedure, , Oesophageal, atresia, , , , , , Associated with tracheo-oesophageal fistula and polyhydramnios, May present with choking and cyanotic spells following aspiration, VACTERL associations, , Meconium ileus, , , , , , Usually delayed passage of meconium and abdominal distension, Majority have cystic fibrosis, X-Rays may not show a fluid level as the meconium is viscid, (depends upon feeding), PR contrast studies may dislodge meconium, plugs and be therapeutic, Infants who do not respond to PR contrast and NG N-acetyl cysteine, will require surgery to remove the plugs, , , , Biliary atresia, , , , , Jaundice > 14 days, Increased conjugated bilirubin
Page 3876 :
Necrotising, enterocolitis, , , , Urgent Kasai procedure, , , , , Prematurity is the main risk factor, Early features include abdominal distension and passage of bloody, stools, X-Rays may show pneumatosis intestinalis and evidence of free air, Increased risk when empirical antibiotics are given to infants beyond, 5 days, Treatment is with total gut rest and TPN, babies with perforations, will require laparotomy, , , , , , Next question
Page 3877 :
Theme: Bilious vomiting in neonates, , A. Biliary atresia, B. Intestinal malrotation, C. Ileal atresia, D. Necrotising enterocolitis, E. Duodenal atresia, F. Meconium ileus, G. Viral gastroenteritis, H. Pyloric stenosis, , Please select the most likely underlying cause of bilious vomiting for the situation described. Each, option may be used once, more than once or not at all., , 11., , A male infant is born prematurely at 26 weeks gestation by emergency cesarean section., Following the birth he develops respiratory distress syndrome and is ventilated. He begins to, improve twelve days after birth. Then he becomes unwell and develops abdominal distension and, passes bloody stools and vomits a small quantity of bile stained vomit., You answered Biliary atresia, The correct answer is Necrotising enterocolitis, Necrotising enterocolitis often has a delayed presentation and affected infants will typically pass, bloody stools. Plain films may show air in the intestinal wall (Pneumatosis)., , 12., , A male infant is born by spontaneous vaginal delivery at 39 weeks gestation. He is well after the, birth, established on bottle feeding and discharged home. His parents are concerned because he, subsequently becomes unwell and vomits a large quantity of bile stained vomit approximately 2, days after discharge home. On examination he looks ill and his abdomen is soft and non, distended.
Page 3878 :
You answered Biliary atresia, The correct answer is Intestinal malrotation, Intestinal malrotation with volvulus will typically compromise the vascularisation and lumenal, patency of the gut. This will cause bilious vomiting and the vascular insufficiency will produce a, clinical picture of illness at odds with the lack of overt abdominal signs. Delay in diagnosis and, surgery will result in established necrosis, perforation and peritonitis., , 13., , A female infant is born by cesarean section at 38 weeks gestation for foetal distress. The, attending paediatricians notice that she has a single palmar crease and a mongoloid slant to her, eyes. Soon after the birth the mother tries to feed the child who has a projectile vomit about 10, minutes after feeding. On examination she has a soft, non distended abdomen., You answered Biliary atresia, The correct answer is Duodenal atresia, Proximally sited atresia will produce high volume vomits which may or may not be bile stained., Abdominal distension is characteristically absent. Whilst under resuscitated children may be a, little dehydrated they are seldom severely ill. The presence of Trisomy 21 (palmar and eye signs), increases the likelihood of duodenal atresia., , Please rate this question:, , Discuss and give feedback, , Next question, , Bilious vomiting in neonates, Causes of intestinal obstruction with bilious vomiting in neonates, , Disorder, , Incidence and, , Age at, , Diagnosis, , Treatment
Page 3879 :
causation, , presentation, , Duodenal, atresia, , 1 in 5000 (higher, in Downs, syndrome), , Few hours after, birth, , AXR shows, "double bubble, sign, contrast, study may, confirm, , Duodenoduodenostomy, , Malrotation, with, volvulus, , Usually cause by, incomplete, rotation during, embryogenesis, , Usually 3-7 days, after birth,, volvulus with, compromised, circulation may, result in peritoneal, signs and, haemodynamic, instability, , Upper GI, contrast study, may show DJ, flexure is more, medially placed,, USS may show, abnormal, orientation of, SMA and SMV, , Ladd's procedure, , Jejunal/ ileal, atresia, , Usually caused by, vascular, insufficiency in, utero, usually 1, in 3000, , Usually within 24, hours of birth, , AXR will show, air-fluid levels, , Laparotomy with primary, resection and anastomosis, , Meconium, ileus, , Occurs in, between 15, and20% of those, babies with cystic, fibrosis,, otherwise 1 in, 5000, , Typically in first 2448 hours of life, with abdominal, distension and, bilious vomiting, , Air - fluid levels, on AXR, sweat, test to confirm, cystic fibrosis, , Surgical decompression,, serosal damage may require, segmental resection, , Necrotising, enterocolitis, , Up to 2.4 per, 1000 births, risks, increased in, prematurity and, inter-current, , Usually second, week of life, , Dilated bowel, loops on AXR,, pneumatosis, and portal, , Conservative and, supportive for non, perforated cases,, laparotomy and resection in, cases of perforation of
Page 3880 :
illness, , venous air, , ongoing clinical, deterioration, Next question
Page 3881 :
Theme: Paediatric gastrointestinal disorders, , A., B., C., D., E., F., G., H., , Meconium ileus, Biliary atresia, Oesophageal atresia, Pyloric stenosis, Intussusception, Malrotation, Hirschsprung disease, Mesenteric adenitis., , What is the most likely diagnosis for each scenario given? Each option may be used once, more, than once or not at all., , 14., , A 3 day old baby presents with recurrent episodes of choking and cyanotic episodes. There, is a history of polyhydramnios., You answered Meconium ileus, The correct answer is Oesophageal atresia, Diagnosis is confirmed when an nasogastric tube fails to reach the stomach., , 15., , A 3 day old neonate is developing increasing problems with feeding. On examination she, has a pan systolic murmur and her forearms have not developed properly., You answered Meconium ileus, The correct answer is Oesophageal atresia, This child has VACTERL, which is a combination of Vertebral, Ano-rectal, Cardiac,, Tracheo-oesophageal, Renal and Radial limb anomalies. Half of babies with oesophageal, atresia will have VACTERL., , 16., , A 2 year old child has central abdominal pain. He has had a recent upper respiratory tract, infection., You answered Meconium ileus, The correct answer is Mesenteric adenitis., Mesenteric adenitis may complicate upper respiratory tract infection and clinical exclusion, of appendicitis can be difficult.
Page 3882 :
Please rate this question:, , Discuss and give feedback, , Next question, , Paediatric Gastrointestinal disorders, Pyloric stenosis, , , , , , , , M>F, 5-10% Family history in parents, Projectile non bile stained vomiting at 4-6 weeks of life, Diagnosis is made by test feed or USS, Treatment: Ramstedt pyloromyotomy (open or laparoscopic), , Acute appendicitis, , , , , Uncommon under 3 years, When occurs may present atypically, , Mesenteric, adenitis, , , , , Central abdominal pain and URTI, Conservative management, , Intussusception, , , , , , , Telescoping bowel, Proximal to or at the level of, ileocaecal valve, 6-9 months age, Colicky pain, diarrhoea and vomiting, sausage shaped mass, red jelly, stool., Treatment: reduction with air insufflation, , , , Malrotation, , , , , , , , Hirschsprung's, disease, , , , , , , High caecum at the midline, Feature in exomphalos, congenital diaphragmatic hernia, intrinsic, duodenal atresia, May be complicated by development of volvulus, infant with, volvulus may have bile stained vomiting, Diagnosis is made by upper GI contrast study and USS, Treatment is by laparotomy, if volvulus is present (or at high risk of, occurring then a ladds procedure is performed, Absence of ganglion cells from myenteric and submucosal plexuses, Occurs in 1/5000 births, Full thickness rectal biopsy for diagnosis, Delayed passage of meconium and abdominal distension
Page 3883 :
, , Treatment is with rectal washouts initially, thereafter an anorectal, pull through procedure, , Oesophageal, atresia, , , , , , Associated with tracheo-oesophageal fistula and polyhydramnios, May present with choking and cyanotic spells following aspiration, VACTERL associations, , Meconium ileus, , , , , , Usually delayed passage of meconium and abdominal distension, Majority have cystic fibrosis, X-Rays may not show a fluid level as the meconium is viscid, (depends upon feeding), PR contrast studies may dislodge meconium, plugs and be therapeutic, Infants who do not respond to PR contrast and NG N-acetyl cysteine, will require surgery to remove the plugs, , , , Biliary atresia, , , , , , Jaundice > 14 days, Increased conjugated bilirubin, Urgent Kasai procedure, , Necrotising, enterocolitis, , , , , Prematurity is the main risk factor, Early features include abdominal distension and passage of bloody, stools, X-Rays may show pneumatosis intestinalis and evidence of free air, Increased risk when empirical antibiotics are given to infants beyond, 5 days, Treatment is with total gut rest and TPN, babies with perforations, will require laparotomy, , , , , , Next question
Page 3884 :
Theme: Neonatal gastrointestinal disease, , A., B., C., D., E., F., G., H., I., , Ano-rectal atresia, Pyloric stenosis, Hirschsprungs disease, Duodenal atresia, Meconium ileus, Intussusception, Necrotising enterocolitis, Intestinal volvulus, Tracheo-oesophageal fistula, , Please select the most likely diagnosis to account for the case described. Each option may be used, once, more than once or not at all., , 17., , A newborn baby boy presents with mild abdominal distension and failure to pass, meconium after 24 hours. X- Ray reveals dilated loops of bowel with fluid levels. The, anus appears normally located., You answered Ano-rectal atresia, The correct answer is Hirschsprungs disease, Hirschsprung's disease is an absence of ganglion cells in the neural plexus of the intestinal, wall. It is more common in boys than girls. The delayed passage of meconium together, with distension of abdomen is the usual clinical presentation. A plain abdominal x ray will, demonstrate dilated loops of bowel with fluid levels and a barium enema can be helpful, when it demonstrates a cone with dilated ganglionic proximal colon and the distal, aganglionic bowel failing to distend., , 18., , A premature infant (30-week gestation) presents with distended and tense abdomen. She is, passing blood and mucus per rectum, and she is also manifesting signs of sepsis., You answered Ano-rectal atresia, The correct answer is Necrotising enterocolitis, Necrotising enterocolitis is more common in premature infants. Mesenteric ischemia, causes bacterial invasion of the mucosa leading to sepsis. Terminal ileum, caecum and the, distal colon are commonly affected. The abdomen is distended and tense, and the infant, passes blood and mucus per rectum. X -Ray of the abdomen shows distended loops of, intestine and gas bubbles may be seen in the bowel wall., , 19., , A newborn baby boy presents with gross abdominal distension. He is diagnosed with
Page 3885 :
cystic fibrosis and his abdominal x ray shows distended coils of small bowel, but no fluid, levels., You answered Ano-rectal atresia, The correct answer is Meconium ileus, One in 15,000 newborns will have a distal small bowel obstruction secondary to abnormal, bulky and viscid meconium. Ninety percent of these infants will have cystic fibrosis and, the abnormal meconium is the result of deficient intestinal secretions. This condition, presents during the first days of life with gross abdominal distension and bilious vomiting., x Ray of the abdomen shows distended coils of bowel and typical mottled ground glass, appearance. Fluid levels are scarce as the meconium is viscid., Please rate this question:, , Discuss and give feedback, , Next question, , Paediatric Gastrointestinal disorders, Pyloric stenosis, , , , , , , , M>F, 5-10% Family history in parents, Projectile non bile stained vomiting at 4-6 weeks of life, Diagnosis is made by test feed or USS, Treatment: Ramstedt pyloromyotomy (open or laparoscopic), , Acute appendicitis, , , , , Uncommon under 3 years, When occurs may present atypically, , Mesenteric, adenitis, , , , , Central abdominal pain and URTI, Conservative management, , Intussusception, , , , , , , Telescoping bowel, Proximal to or at the level of, ileocaecal valve, 6-9 months age, Colicky pain, diarrhoea and vomiting, sausage shaped mass, red jelly, stool., Treatment: reduction with air insufflation, ,
Page 3886 :
Malrotation, , , , , , , , High caecum at the midline, Feature in exomphalos, congenital diaphragmatic hernia, intrinsic, duodenal atresia, May be complicated by development of volvulus, infant with, volvulus may have bile stained vomiting, Diagnosis is made by upper GI contrast study and USS, Treatment is by laparotomy, if volvulus is present (or at high risk of, occurring then a ladds procedure is performed, , Hirschsprung's, disease, , , , , , , , Absence of ganglion cells from myenteric and submucosal plexuses, Occurs in 1/5000 births, Full thickness rectal biopsy for diagnosis, Delayed passage of meconium and abdominal distension, Treatment is with rectal washouts initially, thereafter an anorectal, pull through procedure, , Oesophageal, atresia, , , , , , Associated with tracheo-oesophageal fistula and polyhydramnios, May present with choking and cyanotic spells following aspiration, VACTERL associations, , Meconium ileus, , , , , , Usually delayed passage of meconium and abdominal distension, Majority have cystic fibrosis, X-Rays may not show a fluid level as the meconium is viscid, (depends upon feeding), PR contrast studies may dislodge meconium, plugs and be therapeutic, Infants who do not respond to PR contrast and NG N-acetyl cysteine, will require surgery to remove the plugs, , , , Biliary atresia, , , , , , Jaundice > 14 days, Increased conjugated bilirubin, Urgent Kasai procedure, , Necrotising, enterocolitis, , , , , Prematurity is the main risk factor, Early features include abdominal distension and passage of bloody, stools, X-Rays may show pneumatosis intestinalis and evidence of free air, Increased risk when empirical antibiotics are given to infants beyond, 5 days, Treatment is with total gut rest and TPN, babies with perforations, will require laparotomy, , , ,
Page 3887 :
Which of the following statements relating to biliary atresia is untrue?, , It most commonly presents as prolonged conjugated jaundice in the neonatal period., , Evidence of portal hypertension at diagnosis is seldom present in the UK., , It may be confused with Alagille syndrome., , The Kasai procedure is best performed in the first 8 weeks of life., , Survival following a successful Kasai procedure is approximately 45% at 5 years., Alagille syndrome autosomal dominant disorder characterised by presence of paucity of bile ducts, and cardiac defects. Only the embryonic form of biliary atresia is associated with cardiac and other, embryological defects., Biliary atresia usually presents with obstructed jaundice. A Kasai procedure is best performed in the, first 8 weeks of life. If a Kasai procedure is successful most patients will not require liver, transplantation. 45% of patients post Kasai procedure will require transplantation. However, overall, survival following a successful Kasai procedure is 80%., Please rate this question:, , Discuss and give feedback, , Next question, , Biliary atresia, , , , 1 in 17000 affected, Biliary tree lumen is obliterated by an inflammatory cholangiopathy causing progressive liver, damage, , Clinical features, , , , , , , Infant well in 1st few weeks of life, No family history of liver disease, Jaundice in infants > 14 days in term infants (>21 days in pre term infants), Pale stool, yellow urine (colourless in babies), Associated with cardiac malformations, polysplenia, situs inversus
Page 3888 :
Investigation, , , , , Conjugated bilirubin (prolonged physiological jaundice or breast milk jaundice will cause a, rise in unconjugated bilirubin, whereas those with obstructive liver disease will have a rise in, conjugated bilirubin), Ultrasound of the liver (excludes extrahepatic causes, in biliary atresia infant may have tiny, or invisible gallbladder), Hepato-iminodiacetic acid radionuclide scan (good uptake but no excretion usually seen), , Management, , , , , , Early recognition is important to prevent liver transplantation., Nutritional support., Roux-en-Y portojejunostomy (Kasai procedure)., If Kasai procedure fails or late recognition, a liver transplant becomes the only option., Next question
Page 3889 :
Theme: Administration of intravenous fluids, , A., B., C., D., E., F., G., H., I., , 0.9% Saline, 5% Dextrose, 20% Glucose, 0.18% saline/ 4% glucose, 0.45% saline/ 15% glucose, 0.45% saline/ 2.5% glucose, 4.5% albumin, 10% Pentastarch, 10% Dextrose, , For the scenario given please select the most appropriate type of intravenous fluid for the scenario, given. Each option may be used once, more than once or not at all., , 21., , A 4 year old boy is undergoing an elective orchidopexy., 0.9% Saline, Isotonic fluids should be used in this setting and 0.9% saline is the safest option., , 22., , A 2 day old boy is recovering from an inguinal herniotomy he has yet to feed and the, nursing staff would like a prescription for an initial fluid to be given on return to the ward., His potassium is within normal limits., You answered 0.9% Saline, The correct answer is 10% Dextrose, Neonates require 10% dextrose solutions as they are at risk of developing hypoglycaemia., , 23., , A 4 year boy with learning difficulties has developed swallowing problems and is awaiting, a PEG tube. He required maintenance IV fluids and the nursing staff require choice of, fluid for the next bag. He has just been given 250ml of 0.9% saline., You answered 0.9% Saline, The correct answer is 5% Dextrose, 5% Dextrose would the routine choice for water replacement., , Please rate this question:
Page 3890 :
Discuss and give feedback, , Next question, , Paediatric fluid management, Since 2000 there have been at least 4 reported deaths from fluid induced hyponatraemia in children., This led to the National Patient Safety Agency introducing revised guidelines in 2007., Indications for IV fluids include:, , , , , , Resuscitation and circulatory support, Replacing on-going fluid losses, Maintenance fluids for children for whom oral fluids are not appropriate, Correction of electrolyte disturbances, , Fluids to be avoided, Outside the neonatal period saline / glucose solutions should not be given. The greatest risk is with, saline 0.18 / glucose 4% solutions. The report states that 0.45% saline / 5% glucose may be used., But preference should be given to isotonic solutions and few indications exist for this solution either., Fluids to be used, , , , , 0.9% saline, 5% glucose (though only with saline for maintenance and not to replace losses), Hartmann's solution, , Potassium should be added to maintenance fluids according patients plasma potassium levels, (which should be monitored)., Intraoperative fluid management, Neonates should receive glucose 10% during surgery., Other children should receive isotonic crystalloid., Maintenance fluids, , Weight, , Water requirement/kg/day, , Na mmol/kg/day, , K mmol/kg/day, , First 10Kg body weight, , 100ml, , 2-4, , 1.5-2.5, , Second 10Kg body weight, , 50ml, , 1-2, , 0.5-1.5, , Subsequent Kg, , 20ml, , 0.5-1.0, , 0.2-0.7
Page 3891 :
Glucose will need to be given to neonates- usually 10% at a rate of 60ml/Kg/day., Reference, NPSA -reducing risk of hyponatraemia when administering intravenous fluids to children. Issue date, March 2007. Further references included in this document., Next question
Page 3892 :
A 3 day old baby develops dyspneoa. A chest x-ray is performed and shows a radio-opaque shadow, with an air-fluid level in the chest. It is located immediately anterior to the 6th hemivertebra. Which of, the following is the most likely underlying diagnosis?, , Bronchogenic cyst, , Congenital diaphragmatic hernia, , Infection with Staphylococcus aureus, , Oesphageal duplication cyst, , Hiatus hernia, , A midline cystic mass of an infant in this age group is most likely to be a bronchogenic cyst. Hiatus, hernia is unusual in the neonatal period. Oesophageal duplication cysts are very rare and respiratory, symptoms are less common than with bronchogenic cysts. Midline congenital hernias are rare and, would usually not include an air/ fluid level in the rare event that they occur at this site., Please rate this question:, , Discuss and give feedback, , Next question, , Bronchogenic cysts, Overview, Bronchogenic cysts most commonly arise as a result of anomalous development of the ventral, foregut. They are most commonly single, although multiple cysts are described., They often lie near the midline and most frequently occur in the region of the carina. They may be, attached to the tracheobronchial tree, although they are seldom in direct connection with it., Cases may be asymptomatic or present with respiratory symptoms early in the neonatal period.
Page 3893 :
They are the second most common type of foregut cysts (after enterogenous cysts) in the middle, mediastinum. Up to 50% of cases are diagnosed prior to 15 years of age., Investigation, Many cases are diagnosed on antenatal ultrasound. Others may be detected on conventional chest, radiography as a midline spherical mass or cystic structure. Once the diagnosis is suspected a CT, scan should be performed., Treatment, Thorascopic resection is the ideal treatment. Very young babies can be operated on once they reach, six weeks of age., Next question
Page 3894 :
Theme: Paediatric umbilical disorders, , A. Omphalitis, B. Umbilical hernia, C. Umbilical granuloma, D. Paraumbilical hernia, E. Persistent vitello-intestinal duct, F. Persistent urachus, , Please select the most likely underlying disorder for the umbilical condition described. Each option, may be used once, more than once or not at all., , 25., , A 2 week old baby is referred to the surgical team by the paediatricians. They are concerned, because the child has a painful area of macerated tissue at the site of the umbilicus. On, examination a clear- yellowish fluid is seen to be draining from the umbilicus when the baby cries., You answered Omphalitis, The correct answer is Persistent urachus, A patent urachus will present with umbilical urinary discharge. The skin may become macerated if, not properly cared for. The discharge is most likely to be present when intra-abdominal pressure, is raised. It is associated with posterior urethral valves., , 26., , A premature neonate is born by emergency cesarean section at 29 weeks gestation. He initially, seems to be progressing well. However, the team are concerned because he becomes, systemically septic and on examination has a swollen and erythematous umbilicus., Omphalitis, Infection from omphalitis may spread rapidly and cause severe sepsis especially in, immunologically compromised, premature neonates.
Page 3895 :
27., , A baby boy is born by elective cesarean section at 39 weeks gestation. He initially seems to, progress well and is discharged from hospital the following day. The parents bring the child to the, clinic at 10 days of age and are concerned at the presence of a profuse and foul smelling, discharge at the site of the umbilicus. On examination the umbilicus has some prominent, granulation tissue. When the baby cries a small trickle of brownish fluid is seen to pass from the, umbilicus., You answered Omphalitis, The correct answer is Persistent vitello-intestinal duct, A persistent vitello-intestinal duct may allow the persistent and ongoing discharge of small bowel, content from the umbilicus. This fluid may be very irritant to the surrounding skin., , Please rate this question:, , Discuss and give feedback, , Next question, , Paediatric umbilical disorders, Embryology, During development the umbilicus has two umbilical arteries and one umbilical vein. The arteries are, continuous with the internal iliac arteries and the vein is continuous with the falciform ligament, (ductus venosus). After birth the cord dessicates and separates and the umbilical ring closes., Umbilical hernia, Up to 20% of neonates may have an umbilical hernia, it is more common in premature infants. The, majority of these hernias will close spontaneously (may take between 12 months and three years)., Strangulation is rare., Paraumbilical hernia, These are due to defects in the linea alba that are in close proximity to the umbilicus. The edges of a, paraumbilical hernia are more clearly defined than those of an umbilical hernia. They are less likely, to resolve spontaneously than an umbilical hernia., Omphalitis
Page 3896 :
This condition consists of infection of the umbilicus. Infection with Staphylococcus aureus is the, commonest cause. The condition is potentially serious as infection may spread rapidly through the, umbilical vessels in neonates with a risk of portal pyaemia, and portal vein thrombosis. Treatment is, usually with a combination of topical and systemic antibiotics., Umbilical granuloma, These consist of cherry red lesions surrounding the umbilicus, they may bleed on contact and be a, site of seropurulent discharge. Infection is unusual and they will often respond favorably to chemical, cautery with topically applied silver nitrate., Persistent urachus, This is characterised by urinary discharge from the umbilicus. It is caused by persistence of the, urachus which attaches to the bladder. They are associated with other urogenital abnormalities., Persistent vitello-intestinal duct, This will typically present as an umbilical discharge that discharges small bowel content. Complete, persistence of the duct is a rare condition. Much more common is the persistence of part of the duct, (Meckels diverticulum). Persistent vitello-intestinal ducts are best imaged using a contrast study to, delineate the anatomy and are managed by laparotomy and surgical closure., Next question
Page 3897 :
Which one of the following is least associated with Tetralogy of Fallot?, , Right ventricular outflow tract obstruction, , Overriding aorta, , Pan systolic murmur, , Left-to-right shunt, , Right ventricular hypertrophy, , Right-to-left shunting is characteristic of Fallot's. In some patients there can be bidirectional shunting, (if there is mild pulmonary stenosis) and a few patients can even have pink tetralogy when there is a, predominant shunt from left to right due to minimal infundibular stenosis., Please rate this question:, , Discuss and give feedback, , Next question, , Tetralogy of Fallot, Tetralogy of Fallot (TOF) is the most common cause of cyanotic congenital heart disease*. It, typically presents at around 1-2 months, although may not be picked up until the baby is 6 months, old, The four characteristic features are:, , , , , , ventricular septal defect (VSD), right ventricular hypertrophy, right ventricular outflow tract obstruction, pulmonary stenosis, overriding aorta, , The severity of the right ventricular outflow tract obstruction determines the degree of cyanosis and, clinical severity, Other features, , , cyanosis
Page 3898 :
, , , , , causes a right-to-left shunt, ejection systolic murmur due to pulmonary stenosis (the VSD doesn't usually cause a, murmur), a right-sided aortic arch is seen in 25% of patients, chest x-ray shows a 'boot-shaped' heart, ECG shows right ventricular hypertrophy, , Management, , , , surgical repair is often undertaken in two parts, cyanotic episodes may be helped by beta-blockers to reduce infundibular spasm, , *however, at birth transposition of the great arteries is the more common lesion as patients with TOF, generally present at around 1-2 months, Next question
Page 3899 :
A 3 year old boy is brought to the clinic with symptoms of urinary hesitancy and poor stream. Which, of the following is the most likely underlying diagnosis?, , Benign prostatic hypertrophy, , Posterior urethral valves, , Neurogenic bladder, , Urethral calculus, , Hypospadias, , Theme from September 2015 Exam, Posterior urethral valves are one of the commonest causes of poor urinary stream and hesitancy in, children. Prostatic disorders are rare., Hypospadias is associated with urine that is difficult to control, but should not produce hesitancy., Please rate this question:, , Discuss and give feedback, , Next question, , Urethral valves, Posterior urethral valves are the commonest cause of infravesical outflow obstruction in males. They, may be diagnosed on ante natal ultrasonography. Because the bladder has to develop high, emptying pressures in utero, the child may develop renal parenchymal damage. This translates to, renal impairment noted in 70% of boys at presentation. Treatment is with bladder catheterisation., Endoscopic valvotomy is the definitive treatment of choice with cystoscopic and renal follow up., Next question
Page 3900 :
Which of the following is not a feature of oesphageal atresia in neonates?, , High incidence of polyhydramnios, , Risk of recurrence in subsequent pregnancies of 80%, , Distal tracheoesphageal fistula is the commonest variant, , High incidence of associated imperforate anus, , Absence of gastric bubble on antenatal ultrasound, , Most are sporadic and risk in subsequent pregnancies is not increased., Please rate this question:, , Discuss and give feedback, , Next question, , Paediatric Gastrointestinal disorders, Pyloric stenosis, , , , , , , , M>F, 5-10% Family history in parents, Projectile non bile stained vomiting at 4-6 weeks of life, Diagnosis is made by test feed or USS, Treatment: Ramstedt pyloromyotomy (open or laparoscopic), , Acute appendicitis, , , , , Uncommon under 3 years, When occurs may present atypically, , Mesenteric, adenitis, , , , , Central abdominal pain and URTI, Conservative management, , Intussusception, , , , , , , Telescoping bowel, Proximal to or at the level of, ileocaecal valve, 6-9 months age, Colicky pain, diarrhoea and vomiting, sausage shaped mass, red jelly
Page 3901 :
, , Malrotation, , , , , , , , stool., Treatment: reduction with air insufflation, High caecum at the midline, Feature in exomphalos, congenital diaphragmatic hernia, intrinsic, duodenal atresia, May be complicated by development of volvulus, infant with, volvulus may have bile stained vomiting, Diagnosis is made by upper GI contrast study and USS, Treatment is by laparotomy, if volvulus is present (or at high risk of, occurring then a ladds procedure is performed, , Hirschsprung's, disease, , , , , , , , Absence of ganglion cells from myenteric and submucosal plexuses, Occurs in 1/5000 births, Full thickness rectal biopsy for diagnosis, Delayed passage of meconium and abdominal distension, Treatment is with rectal washouts initially, thereafter an anorectal, pull through procedure, , Oesophageal, atresia, , , , , , Associated with tracheo-oesophageal fistula and polyhydramnios, May present with choking and cyanotic spells following aspiration, VACTERL associations, , Meconium ileus, , , , , , Usually delayed passage of meconium and abdominal distension, Majority have cystic fibrosis, X-Rays may not show a fluid level as the meconium is viscid, (depends upon feeding), PR contrast studies may dislodge meconium, plugs and be therapeutic, Infants who do not respond to PR contrast and NG N-acetyl cysteine, will require surgery to remove the plugs, , , , Biliary atresia, , , , , , Jaundice > 14 days, Increased conjugated bilirubin, Urgent Kasai procedure, , Necrotising, enterocolitis, , , , , Prematurity is the main risk factor, Early features include abdominal distension and passage of bloody, stools, X-Rays may show pneumatosis intestinalis and evidence of free air, Increased risk when empirical antibiotics are given to infants beyond, , ,
Page 3902 :
, , 5 days, Treatment is with total gut rest and TPN, babies with perforations, will require laparotomy, Next question
Page 3903 :
A 12 day old infant is brought to the emergency department by his anxious mother who notices that, he has developed a right sided groin swelling. On examination the testes are correctly located but it, is evident that the child has a right sided inguinal hernia. It is soft and easily reduced. What is the, most appropriate management?, , Surgery over the next few days, , Reassure and discharge, , Surgery at 1 year of age, , Surgery once the child is 6 months old, , Application of a hernia truss, Inguinal hernia in infants = Urgent surgery, , The high incidence of strangulation necessitates an urgent herniotomy be performed. In infants with, a reducible hernia this can be performed on a daycase list during the same week. Deferring surgery, on the basis of age is not justified., Please rate this question:, , Discuss and give feedback, , Next question, , Paediatric inguinal hernia, Inguinal hernias are a common disorder in children. They are commoner in males as the testis, migrates from its location on the posterior abdominal wall, down through the inguinal canal. A patent, processus vaginalis may persist and be the site of subsequent hernia development., Children presenting in the first few months of life are at the highest risk of strangulation and the, hernia should be repaired urgently. Children over 1 year of age are at lower risk and surgery may be, performed electively. For paediatric hernias a herniotomy without implantation of mesh is sufficient.
Page 3904 :
Most cases are performed as day cases, neonates and premature infants are kept in hospital, overnight as there is a recognised increased risk of post operative apnoea., Next question
Page 3905 :
Theme: Paediatric gastrointestinal disorders, , A., B., C., D., E., F., G., , Meckel diverticulum, Pyloric stenosis, Acute appendicitis, Mesenteric adenitis, Intussusception, Malrotation, Hirschsprung disease, , What is the most likely diagnosis for each scenario given? Each option may be used once, more, than once or not at all., , 32., , A 48 hour old neonate develops increasing abdominal distension. He had a normal, delivery but has yet to pass any meconium. Following digital rectal examination liquid, stool is released., You answered Meckel diverticulum, The correct answer is Hirschsprung disease, Theme from April 2016, Hirschsprungs may present either with features of bowel obstruction in the neonatal period, or more insidiously during childhood. After the PR there may be an improvement in, symptoms. Diagnosis is by full thickness rectal biopsy., , 33., , A 7 month old girl presents with vomiting and diarrhoea. She is crying and drawing her, legs up. There is a a sausage shaped mass in the abdomen., You answered Meckel diverticulum, The correct answer is Intussusception, Sausage shaped mass (colon shaped) is common in intussusception. The other common, sign is red jelly stool., , 34., , A 1 month old baby girl presents with bile stained vomiting. She has an exomphalos and a, congenital diaphragmatic hernia., You answered Meckel diverticulum, The correct answer is Malrotation
Page 3906 :
Exomphalos and diaphragmatic herniae are commonly associated with malrotation., Please rate this question:, , Discuss and give feedback, , Next question, , Paediatric Gastrointestinal disorders, Pyloric stenosis, , , , , , , , M>F, 5-10% Family history in parents, Projectile non bile stained vomiting at 4-6 weeks of life, Diagnosis is made by test feed or USS, Treatment: Ramstedt pyloromyotomy (open or laparoscopic), , Acute appendicitis, , , , , Uncommon under 3 years, When occurs may present atypically, , Mesenteric, adenitis, , , , , Central abdominal pain and URTI, Conservative management, , Intussusception, , , , , , , Telescoping bowel, Proximal to or at the level of, ileocaecal valve, 6-9 months age, Colicky pain, diarrhoea and vomiting, sausage shaped mass, red jelly, stool., Treatment: reduction with air insufflation, , , , Malrotation, , , , , , , , Hirschsprung's, disease, , , , , High caecum at the midline, Feature in exomphalos, congenital diaphragmatic hernia, intrinsic, duodenal atresia, May be complicated by development of volvulus, infant with, volvulus may have bile stained vomiting, Diagnosis is made by upper GI contrast study and USS, Treatment is by laparotomy, if volvulus is present (or at high risk of, occurring then a ladds procedure is performed, Absence of ganglion cells from myenteric and submucosal plexuses, Occurs in 1/5000 births
Page 3907 :
, , , , Full thickness rectal biopsy for diagnosis, Delayed passage of meconium and abdominal distension, Treatment is with rectal washouts initially, thereafter an anorectal, pull through procedure, , Oesophageal, atresia, , , , , , Associated with tracheo-oesophageal fistula and polyhydramnios, May present with choking and cyanotic spells following aspiration, VACTERL associations, , Meconium ileus, , , , , , Usually delayed passage of meconium and abdominal distension, Majority have cystic fibrosis, X-Rays may not show a fluid level as the meconium is viscid, (depends upon feeding), PR contrast studies may dislodge meconium, plugs and be therapeutic, Infants who do not respond to PR contrast and NG N-acetyl cysteine, will require surgery to remove the plugs, , , , Biliary atresia, , , , , , Jaundice > 14 days, Increased conjugated bilirubin, Urgent Kasai procedure, , Necrotising, enterocolitis, , , , , Prematurity is the main risk factor, Early features include abdominal distension and passage of bloody, stools, X-Rays may show pneumatosis intestinalis and evidence of free air, Increased risk when empirical antibiotics are given to infants beyond, 5 days, Treatment is with total gut rest and TPN, babies with perforations, will require laparotomy, , , , , , Next question
Page 3908 :
A 6 year old child develops ballooning of the foreskin on micturition and is brought to the clinic by his, anxious mother. One examination the foreskin is non retractile but otherwise normal. By which age, are 95% of all foreskins retractile, , 2 years, , 16 years, , 8 years, , 5 years, , 10 years, , By 16 years of age almost all foreskins should be retractile and if they are not circumcision should be, considered at around this time., Please rate this question:, , Discuss and give feedback, , Next question, , Paediatric urology- foreskin disorders, Disorders of the foreskin, At birth and in the neonatal period the normal foreskin is non retractile due to the presence of, adhesions between the foreskin and glans. In most cases these will separate spontaneously. By the, end of puberty 95% of foreskins can be retracted. In some children the non-retractile foreskin may, balloon during micturition. This is a normal variant and requires no specific treatment., , Balanitis, , This is inflammation of the glans penis. It may occur in both circumcised and non-
Page 3909 :
circumcised individuals., , Posthitis, , This is inflammation of the foreskin. It may occur as a result of infections such as, gonorrhoea and other STD's. It may also complicate diabetes. Posthitis may progress, to phimosis and as this may make cleaning of the glans difficult and allow progression, to balanoposthitis., , Paraphimosis, , Prolonged retraction of the foreskin proximal to the glans may allow oedema to occur., This may then make foreskin manipulation difficult. It can usually be managed by, compression to reduce the oedema and replacement of the foreskin. Where this fails a, dorsal slit may be required and this followed by delayed circumcision., , Phimosis, , This is inability to retract the foreskin and may be partial or complete. It may occur, secondary to balanoposthitis or balanitis xerotica obliterans. Depending upon the, severity and symptoms treatment with circumcision may be required., , Balanitis, xerotica, obliterans, , This is a dermatological condition in which scarring of the foreskin occurs leading to, phimosis. It is rare below the age of 5 years. Treatment is usually with circumcision., , Next question
Page 3910 :
A neonate is noted to have colonic obstruction, what is the most likely cause?, , Imperforate anus, , Meconium plugs, , Colonic atresia, , Anal atresia, , Sigmoid volvulus, , Cystic fibrosis is the most common cause of meconium plugs and such cases can be treated with, intestinal lavage, this should be followed by formal testing for CF., Please rate this question:, , Discuss and give feedback, , Next question, , Paediatric Gastrointestinal disorders, Pyloric stenosis, , , , , , , , M>F, 5-10% Family history in parents, Projectile non bile stained vomiting at 4-6 weeks of life, Diagnosis is made by test feed or USS, Treatment: Ramstedt pyloromyotomy (open or laparoscopic), , Acute appendicitis, , , , , Uncommon under 3 years, When occurs may present atypically, , Mesenteric, adenitis, , , , , Central abdominal pain and URTI, Conservative management, , Intussusception, , , , , , Telescoping bowel, Proximal to or at the level of, ileocaecal valve, 6-9 months age
Page 3911 :
, , , Malrotation, , , , , , , , Colicky pain, diarrhoea and vomiting, sausage shaped mass, red jelly, stool., Treatment: reduction with air insufflation, High caecum at the midline, Feature in exomphalos, congenital diaphragmatic hernia, intrinsic, duodenal atresia, May be complicated by development of volvulus, infant with, volvulus may have bile stained vomiting, Diagnosis is made by upper GI contrast study and USS, Treatment is by laparotomy, if volvulus is present (or at high risk of, occurring then a ladds procedure is performed, , Hirschsprung's, disease, , , , , , , , Absence of ganglion cells from myenteric and submucosal plexuses, Occurs in 1/5000 births, Full thickness rectal biopsy for diagnosis, Delayed passage of meconium and abdominal distension, Treatment is with rectal washouts initially, thereafter an anorectal, pull through procedure, , Oesophageal, atresia, , , , , , Associated with tracheo-oesophageal fistula and polyhydramnios, May present with choking and cyanotic spells following aspiration, VACTERL associations, , Meconium ileus, , , , , , Usually delayed passage of meconium and abdominal distension, Majority have cystic fibrosis, X-Rays may not show a fluid level as the meconium is viscid, (depends upon feeding), PR contrast studies may dislodge meconium, plugs and be therapeutic, Infants who do not respond to PR contrast and NG N-acetyl cysteine, will require surgery to remove the plugs, , , , Biliary atresia, , , , , , Jaundice > 14 days, Increased conjugated bilirubin, Urgent Kasai procedure, , Necrotising, enterocolitis, , , , , Prematurity is the main risk factor, Early features include abdominal distension and passage of bloody, stools, X-Rays may show pneumatosis intestinalis and evidence of free air, ,
Page 3912 :
, , , Increased risk when empirical antibiotics are given to infants beyond, 5 days, Treatment is with total gut rest and TPN, babies with perforations, will require laparotomy, Next question
Page 3913 :
An 18 month old boy is brought to the emergency room by his parents. He was found in bed with a, nappy filled with dark red blood. He is haemodynamically unstable and requires a blood transfusion., Prior to this episode he was well with no prior medical history. What is the most likely cause?, , Necrotising enterocolitis, , Anal fissure, , Oesophageal varices, , Meckels diverticulum, , Crohns disease, Meckels diverticulum is the number one cause of painless massive GI bleeding requiring a, transfusion in children between the ages of 1 and 2 years., Other causes of GI bleeding include:, , Older than 2, years, , Site, , Newborn, , 1 month to 1 year, , 1 to 2 years, , Upper, GI tract, , Haemorrhagic disease,, swallowed maternal, blood, , Oesophagitis/, gastritis, , Peptic ulcer, disease, , Varices, , Lower, GI tract, , Anal fissure/ NEC, , Anal fissure/, Intussusception, , Polyps / Meckels, diverticulum, , IBD/ Polyps/, Intussusception, , Please rate this question:, , Discuss and give feedback, , Next question, , Meckel's diverticulum, , , Congenital abnormality resulting in incomplete obliteration of the vitello-intestinal duct
Page 3914 :
, , , , , , , Normally, in the foetus, there is an attachment between the vitello-intestinal duct and the yolk, sac.This disappears at 6 weeks gestation., The tip is free in majority of cases., Associated with enterocystomas, umbilical sinuses, and omphaloileal fistulas., Arterial supply: omphalomesenteric artery., 2% of population, 2 inches long, 2 feet from the ileocaecal valve., Typically lined by ileal mucosa but ectopic gastric mucosa can occur, with the risk of peptic, ulceration. Pancreatic and jejunal mucosa can also occur., , Clinical, , , , , Normally asymptomatic and an incidental finding., Complications are the result of obstruction, ectopic tissue, or inflammation., Removal if narrow neck or symptomatic. Options are between wedge excision or formal, small bowel resection and anastomosis., Next question
Page 3915 :
What is the investigation of choice to look for renal scarring in a child with vesicoureteric reflux?, , Abdominal x-ray, , Ultrasound, , DMSA, , CT KUB, , Micturating cystourethrogram, , Please rate this question:, , Discuss and give feedback, , Next question, , Vesicoureteric reflux, Vesicoureteric reflux (VUR) is the abnormal backflow of urine from the bladder into the ureter and, kidney. It is relatively common abnormality of the urinary tract in children and predisposes to urinary, tract infection (UTI), being found in around 30% of children who present with a UTI. As around 35%, of children develop renal scarring it is important to investigate for VUR in children following a UTI, Pathophysiology of VUR, , , , , ureters are displaced laterally, entering the bladder in a more perpendicular fashion than at, an angle, therefore shortened intramural course of ureter, vesicoureteric junction cannot therefore function adequately, , The table below summarises the grading of VUR, , {Grade}, , I, , Reflux into the ureter only, no dilatation
Page 3916 :
II, , Reflux into the renal pelvis on micturition, no dilatation, , III, , Mild/moderate dilatation of the ureter, renal pelvis and calyces, , IV, , Dilation of the renal pelvis and calyces with moderate ureteral tortuosity, , V, , Gross dilatation of the ureter, pelvis and calyces with ureteral tortuosity, , Investigation, , , , VUR is normally diagnosed following a micturating cystourethrogram, a DMSA scan may also be performed to look for renal scarring, Next question
Page 3917 :
Which of the following statements relating to necrotising enterocolitis is false?, , It has a mortality of 30%, , Most frequently presents in premature neonates less than 32 weeks gestation., , Should be managed by early laparotomy and segmental resections in most cases., , Pneumostosis intestinalis may be visible on plain abdominal x-ray., , May be minimised by use of breast milk over formula feeds., , Most cases will settle with conservative management with NG decompression and appropriate, support. Laparotomy should be undertaken in patients who progress despite conservative, management or in whom compelling indications for surgery exist (eg free air)., Please rate this question:, , Discuss and give feedback, , Next question, , Paediatric Gastrointestinal disorders, Pyloric stenosis, , , , , , , , M>F, 5-10% Family history in parents, Projectile non bile stained vomiting at 4-6 weeks of life, Diagnosis is made by test feed or USS, Treatment: Ramstedt pyloromyotomy (open or laparoscopic), , Acute appendicitis, , , , , Uncommon under 3 years, When occurs may present atypically, , Mesenteric, adenitis, , , , , Central abdominal pain and URTI, Conservative management, , Intussusception, , , , , Telescoping bowel, Proximal to or at the level of, ileocaecal valve
Page 3918 :
, , , , Malrotation, , , , , , , , 6-9 months age, Colicky pain, diarrhoea and vomiting, sausage shaped mass, red jelly, stool., Treatment: reduction with air insufflation, High caecum at the midline, Feature in exomphalos, congenital diaphragmatic hernia, intrinsic, duodenal atresia, May be complicated by development of volvulus, infant with, volvulus may have bile stained vomiting, Diagnosis is made by upper GI contrast study and USS, Treatment is by laparotomy, if volvulus is present (or at high risk of, occurring then a ladds procedure is performed, , Hirschsprung's, disease, , , , , , , , Absence of ganglion cells from myenteric and submucosal plexuses, Occurs in 1/5000 births, Full thickness rectal biopsy for diagnosis, Delayed passage of meconium and abdominal distension, Treatment is with rectal washouts initially, thereafter an anorectal, pull through procedure, , Oesophageal, atresia, , , , , , Associated with tracheo-oesophageal fistula and polyhydramnios, May present with choking and cyanotic spells following aspiration, VACTERL associations, , Meconium ileus, , , , , , Usually delayed passage of meconium and abdominal distension, Majority have cystic fibrosis, X-Rays may not show a fluid level as the meconium is viscid, (depends upon feeding), PR contrast studies may dislodge meconium, plugs and be therapeutic, Infants who do not respond to PR contrast and NG N-acetyl cysteine, will require surgery to remove the plugs, , , , Biliary atresia, , , , , , Jaundice > 14 days, Increased conjugated bilirubin, Urgent Kasai procedure, , Necrotising, enterocolitis, , , , , Prematurity is the main risk factor, Early features include abdominal distension and passage of bloody, stools
Page 3919 :
, , , , X-Rays may show pneumatosis intestinalis and evidence of free air, Increased risk when empirical antibiotics are given to infants beyond, 5 days, Treatment is with total gut rest and TPN, babies with perforations, will require laparotomy, Next question
Page 3920 :
A 6 week old baby boy is brought to the clinic by his mother. She is concerned because although the, left testis is present in the scrotum the right testis is absent. She reports that it is sometimes palpable, when she bathes the child. on examination the right testis is palpable at the level of the superficial, inguinal ring. What is the most appropriate management?, , Discharge, , Re-assess in 5 years, , Laparoscopy, , Re-assess in 6 months, , Orchidopexy, , Undescended testes are not uncommon in young children. They may be present in 4% of term, infants, but only in 1.3% children at 3 months of age. In this scenario the testis is retractile and can, be managed expectantly., Please rate this question:, , Discuss and give feedback, , Next question, , Cryptorchidism, A congenital undescended testis is one that has failed to reach the bottom of the scrotum by 3, months of age. At birth up to 5% of boys will have an undescended testis, post natal descent occurs, in most and by 3 months the incidence of cryptorchidism falls to 1-2%. In the vast majority of cases, the cause of the maldescent is unknown. A proportion may be associated with other congenital, defects including:, Patent processus vaginalis, Abnormal epididymis, Cerebral palsy, Mental retardation, Wilms tumour, Abdominal wall defects (e.g. gastroschisis, prune belly syndrome), Differential diagnosis, These include retractile testes and, in the case of absent bilateral testes the possibility of intersex, conditions. A retractile testis can be brought into the scrotum by the clinician and when released, remains in the scrotum. If the examining clinician notes the testis to return rapidly into the inguinal
Page 3921 :
canal when released then surgery is probably indicated., Reasons for correction of cryptorchidism, , , , , , Reduce risk of infertility, Allows the testes to be examined for testicular cancer, Avoid testicular torsion, Cosmetic appearance, , Males with undescended testis are 40 times as likely to develop testicular cancer (seminoma) as, males without undescended testis, The location of the undescended testis affects the relative risk of testicular cancer (50% intraabdominal testes), Treatment, , , , , Orchidopexy at 6- 18 months of age. The operation usually consists of inguinal exploration,, mobilisation of the testis and implantation into a dartos pouch., Intra-abdominal testis should be evaluated laparoscopically and mobilised. Whether this is a, single stage or two stage procedure depends upon the exact location., After the age of 2 years in untreated individuals the Sertoli cells will degrade and those, presenting late in teenage years may be better served by orchidectomy than to try and, salvage a non functioning testis with an increased risk of malignancy., Next question
Page 3922 :
An 8 week old infant is brought to clinic with a history of 18 days of jaundice. The mother is breast, feeding. He was a full term baby. There is no family history of liver disease. What is the most, appropriate next step?, , Liver USS, , Unconjugated bilirubin measurement, , Conjugated bilirubin measurement, , Reassure and discharge, , ERCP, , This baby is a full term and has > 14 days of jaundice, therefore needs an urgent conjugated bilirubin, check to rule out biliary atresia. If physiological jaundice the unconjugated bilirubin levels will be, increased. Isotope scanning may be used in diagnosis, but a definitive diagnosis is normally made, during a laparotomy., Please rate this question:, , Discuss and give feedback, , Next question, , Biliary atresia, , , , 1 in 17000 affected, Biliary tree lumen is obliterated by an inflammatory cholangiopathy causing progressive liver, damage, , Clinical features, , , , , , , Infant well in 1st few weeks of life, No family history of liver disease, Jaundice in infants > 14 days in term infants (>21 days in pre term infants), Pale stool, yellow urine (colourless in babies), Associated with cardiac malformations, polysplenia, situs inversus, , Investigation
Page 3923 :
, , , , Conjugated bilirubin (prolonged physiological jaundice or breast milk jaundice will cause a, rise in unconjugated bilirubin, whereas those with obstructive liver disease will have a rise in, conjugated bilirubin), Ultrasound of the liver (excludes extrahepatic causes, in biliary atresia infant may have tiny, or invisible gallbladder), Hepato-iminodiacetic acid radionuclide scan (good uptake but no excretion usually seen), , Management, , , , , , Early recognition is important to prevent liver transplantation., Nutritional support., Roux-en-Y portojejunostomy (Kasai procedure)., If Kasai procedure fails or late recognition, a liver transplant becomes the only option., Next question
Page 3924 :
Which of the following statements relating to Hirschsprungs disease is false?, , It is more common in males., , Is typically associated with a dilated aganglionic segment of bowel., , May present with delayed passage of meconium., , Mucosal biopsies are inadequate for diagnosis., , Disease extending beyond 30cm of colon and rectum is unusual., , There is a transition zone from the contracted aganglionic segment (the abnormal area) to dilated, normal bowel on barium enema. Males are more frequently affected than females. Surgery may, involve a pull through procedure. A number of patients will have ongoing evacuatory disturbance., Please rate this question:, , Discuss and give feedback, , Next question, , Paediatric Gastrointestinal disorders, Pyloric stenosis, , , , , , , , M>F, 5-10% Family history in parents, Projectile non bile stained vomiting at 4-6 weeks of life, Diagnosis is made by test feed or USS, Treatment: Ramstedt pyloromyotomy (open or laparoscopic), , Acute appendicitis, , , , , Uncommon under 3 years, When occurs may present atypically, , Mesenteric, adenitis, , , , , Central abdominal pain and URTI, Conservative management, , Intussusception, , , , , Telescoping bowel, Proximal to or at the level of, ileocaecal valve
Page 3925 :
, , , , Malrotation, , , , , , , , 6-9 months age, Colicky pain, diarrhoea and vomiting, sausage shaped mass, red jelly, stool., Treatment: reduction with air insufflation, High caecum at the midline, Feature in exomphalos, congenital diaphragmatic hernia, intrinsic, duodenal atresia, May be complicated by development of volvulus, infant with, volvulus may have bile stained vomiting, Diagnosis is made by upper GI contrast study and USS, Treatment is by laparotomy, if volvulus is present (or at high risk of, occurring then a ladds procedure is performed, , Hirschsprung's, disease, , , , , , , , Absence of ganglion cells from myenteric and submucosal plexuses, Occurs in 1/5000 births, Full thickness rectal biopsy for diagnosis, Delayed passage of meconium and abdominal distension, Treatment is with rectal washouts initially, thereafter an anorectal, pull through procedure, , Oesophageal, atresia, , , , , , Associated with tracheo-oesophageal fistula and polyhydramnios, May present with choking and cyanotic spells following aspiration, VACTERL associations, , Meconium ileus, , , , , , Usually delayed passage of meconium and abdominal distension, Majority have cystic fibrosis, X-Rays may not show a fluid level as the meconium is viscid, (depends upon feeding), PR contrast studies may dislodge meconium, plugs and be therapeutic, Infants who do not respond to PR contrast and NG N-acetyl cysteine, will require surgery to remove the plugs, , , , Biliary atresia, , , , , , Jaundice > 14 days, Increased conjugated bilirubin, Urgent Kasai procedure, , Necrotising, enterocolitis, , , , , Prematurity is the main risk factor, Early features include abdominal distension and passage of bloody, stools
Page 3926 :
, , , , X-Rays may show pneumatosis intestinalis and evidence of free air, Increased risk when empirical antibiotics are given to infants beyond, 5 days, Treatment is with total gut rest and TPN, babies with perforations, will require laparotomy, Next question
Page 3927 :
A 4 year old is admitted with right iliac fossa pain and is due to undergo an appendicectomy. The, nursing staff would like to give the child an infusion of intravenous fluid whilst waiting for theatre., Assuming electrolytes are normal, which of the following is an appropriate fluid for infusion in this, situation?, , 10% Dextrose solution, , 0.9% Saline solution, , 0.45% saline/ 5% glucose solution, , Gelofusin, , None of the above, , 0.45% saline/ 5% glucose solutions carry a risk of hyponatraemia and is contra indicated- see below., Please rate this question:, , Discuss and give feedback, , Next question, , Paediatric fluid management, Since 2000 there have been at least 4 reported deaths from fluid induced hyponatraemia in children., This led to the National Patient Safety Agency introducing revised guidelines in 2007., Indications for IV fluids include:, , , , , , Resuscitation and circulatory support, Replacing on-going fluid losses, Maintenance fluids for children for whom oral fluids are not appropriate, Correction of electrolyte disturbances, , Fluids to be avoided, Outside the neonatal period saline / glucose solutions should not be given. The greatest risk is with, saline 0.18 / glucose 4% solutions. The report states that 0.45% saline / 5% glucose may be used., But preference should be given to isotonic solutions and few indications exist for this solution either., Fluids to be used
Page 3928 :
, , , , 0.9% saline, 5% glucose (though only with saline for maintenance and not to replace losses), Hartmann's solution, , Potassium should be added to maintenance fluids according patients plasma potassium levels, (which should be monitored)., Intraoperative fluid management, Neonates should receive glucose 10% during surgery., Other children should receive isotonic crystalloid., Maintenance fluids, , Weight, , Water requirement/kg/day, , Na mmol/kg/day, , K mmol/kg/day, , First 10Kg body weight, , 100ml, , 2-4, , 1.5-2.5, , Second 10Kg body weight, , 50ml, , 1-2, , 0.5-1.5, , Subsequent Kg, , 20ml, , 0.5-1.0, , 0.2-0.7, , Glucose will need to be given to neonates- usually 10% at a rate of 60ml/Kg/day., Reference, NPSA -reducing risk of hyponatraemia when administering intravenous fluids to children. Issue date, March 2007. Further references included in this document., Next question
Page 3929 :
Theme: Paediatric gastrointestinal disorders, , A., B., C., D., E., F., G., , Appendicectomy, Active observation, Discharge, Ultrasound of the abdomen, Colonoscopy, Pneumatic reduction under fluoroscopic guidance, Laparotomy, , Please select the most appropriate form of management from the list above. Each option may be, used once, more than once or not at all., , 44., , A 5 year old girl has been unwell for 3 days with occasional vomiting and lethargy, she, had one episode of diarrhoea. On examination she has a soft abdomen with tenderness in, the region of the right iliac fossa. Her temperature is 38.1. Urine dipstick shows leucocytes, (+) and protein (+)., Appendicectomy, The most likely diagnosis is appendicitis. This can often present with less robust signs in, paediatric than adult practice., , 45., , A 6 day old baby was born prematurely at 33 weeks. He has been suffering from, respiratory distress syndrome and has been receiving ventilatory support on NICU. He has, developed abdominal distension and is increasingly septic. Ultrasound of the abdomen, shows free fluid and evidence of small bowel dilatation. His blood pressure has remained, labile despite inotropic support, You answered Appendicectomy, The correct answer is Laparotomy, He has necrotising enterocolitis and whilst this is often initially managed medically a, laparotomy is required if the situation deteriorates., , 46., , A 5 year old child has been unwell with a sore throat and fever for several days. He, progresses to develop periumbilical abdominal discomfort and passes diarrhoea. This, becomes blood stained. The paediatricians call you because the ultrasound has shown a, 'target sign'., You answered Appendicectomy
Page 3930 :
The correct answer is Pneumatic reduction under fluoroscopic guidance, This child has an intussusception. The lymphadenopathy will have initiated it. A target, sign is seen on ultrasound and is the side on view of multiple layers of bowel wall., Reduction using fluoroscopy with air is the usual first line management. Ileo-colic, intussceceptions are generally most reliably reduced using this method, long ileo-ileal, intussceceptions usually result in surgery., Please rate this question:, , Discuss and give feedback, , Next question, , Paediatric Gastrointestinal disorders, Pyloric stenosis, , , , , , , , M>F, 5-10% Family history in parents, Projectile non bile stained vomiting at 4-6 weeks of life, Diagnosis is made by test feed or USS, Treatment: Ramstedt pyloromyotomy (open or laparoscopic), , Acute appendicitis, , , , , Uncommon under 3 years, When occurs may present atypically, , Mesenteric, adenitis, , , , , Central abdominal pain and URTI, Conservative management, , Intussusception, , , , , , , Telescoping bowel, Proximal to or at the level of, ileocaecal valve, 6-9 months age, Colicky pain, diarrhoea and vomiting, sausage shaped mass, red jelly, stool., Treatment: reduction with air insufflation, , , , Malrotation, , , , , , , High caecum at the midline, Feature in exomphalos, congenital diaphragmatic hernia, intrinsic, duodenal atresia, May be complicated by development of volvulus, infant with, volvulus may have bile stained vomiting, Diagnosis is made by upper GI contrast study and USS
Page 3931 :
, , Treatment is by laparotomy, if volvulus is present (or at high risk of, occurring then a ladds procedure is performed, , Hirschsprung's, disease, , , , , , , , Absence of ganglion cells from myenteric and submucosal plexuses, Occurs in 1/5000 births, Full thickness rectal biopsy for diagnosis, Delayed passage of meconium and abdominal distension, Treatment is with rectal washouts initially, thereafter an anorectal, pull through procedure, , Oesophageal, atresia, , , , , , Associated with tracheo-oesophageal fistula and polyhydramnios, May present with choking and cyanotic spells following aspiration, VACTERL associations, , Meconium ileus, , , , , , Usually delayed passage of meconium and abdominal distension, Majority have cystic fibrosis, X-Rays may not show a fluid level as the meconium is viscid, (depends upon feeding), PR contrast studies may dislodge meconium, plugs and be therapeutic, Infants who do not respond to PR contrast and NG N-acetyl cysteine, will require surgery to remove the plugs, , , , Biliary atresia, , , , , , Jaundice > 14 days, Increased conjugated bilirubin, Urgent Kasai procedure, , Necrotising, enterocolitis, , , , , Prematurity is the main risk factor, Early features include abdominal distension and passage of bloody, stools, X-Rays may show pneumatosis intestinalis and evidence of free air, Increased risk when empirical antibiotics are given to infants beyond, 5 days, Treatment is with total gut rest and TPN, babies with perforations, will require laparotomy, , , , , , Next question
Page 3932 :
A 4 year old boy presents with symptoms of dysuria and urinary frequency. A urine dipstick is, positive for blood and nitrites. A UTI is suspected. Which of the following follow up strategies is most, appropriate?, , Watchful waiting, , Cystoscopy, , DMSA scan, , CT scan of pelvis, , Renal MRI, , A first presentation of an uncomplicated UTI (even in male children) may be managed expectantly., More than 1 UTI in a six month period should prompt further investigation. NICE guidelines from, 2007 suggest that recurrent UTI and those with a non e-coli UTI should be imaged with USS and, DMSA several months later., Please rate this question:, , Discuss and give feedback, , Urinary tract infection- paediatric, , , , , , UTI's may occur in 5% of young girls and 1-2% males. The incidence is higher in premature, infants., E-Coli accounts for 80% cases., In children with UTI it is important to establish whether there is underlying urinary stasis or, vesico-ureteric reflux (or both)., Pyelonephritis in children carries the risk of renal scarring 10% and this translates into a 10%, risk of developing end stage renal disease., , Diagnosis, , , , , Pyrexia lasting for more than 3 days mandates urine testing., Samples may be taken from mid-stream urine samples or supra pubic aspiration. Urine, collected from nappies usually have faecal contaminants. In samples showing mixed growth, contamination of the sample has usually occurred., As in adults >105 colony forming units of a single organism are usually indicative of a UTI.
Page 3933 :
Management, , , , , , A single isolated UTI (in girls) may be managed expectantly., > 2 UTI's (or 1 in males) in a 6 month period should prompt further testing., Voiding cystourethrograms show the greatest anatomical detail and is the ideal first line test, in males; isotope cystography has a lower radiation dose and is the first line test in girls., USS should also be performed. Renal cortical scintigraphy should be performed when renal, scarring is suspected.
Page 3935 :
Which of the following is not directly affected by warfarin?, , Protein C, , Factor II, , Factor VII, , Factor IX, , Factor VIII, Warfarin affects synthesis of factors II, VII, IX, X and protein C., Theme from September 2013 Exam, Please rate this question:, , Discuss and give feedback, , Next question, , Warfarin, Warfarin is an oral anticoagulant which inhibits the reduction of vitamin K to its active hydroquinone, form, which in turn acts as a cofactor in the formation of clotting factor II, VII, IX and X (mnemonic =, 1972) and protein C, Factors that may potentiate warfarin, , , , , , , Liver disease, P450 enzyme inhibitors, e.g.: amiodarone, ciprofloxacin, Cranberry juice, Drugs which displace warfarin from plasma albumin, e.g. NSAIDs, Inhibit platelet function: NSAIDs, , Side-effects, , , , Haemorrhage, Teratogenic
Page 3936 :
, , Skin necrosis: when warfarin is first started biosynthesis of protein C is reduced. This results, in a temporary procoagulant state after initially starting warfarin, normally avoided by, concurrent heparin administration. Thrombosis may occur in venules leading to skin, necrosis., Next question
Page 3937 :
A 56 year old lady with idiopathic thrombocytopenic purpura has a platelet count of 50. She is due to, undergo a splenectomy. What is the optimal timing of a platelet transfusion in this case?, , 24 hours pre-operatively, , 2 hours pre-operatively, , Whilst making the skin incision, , After ligation of the splenic artery, , On removal of the spleen, , ITP causes splenic sequestration of platelets. Therefore a platelet transfusion should be carefully, timed. Too soon and it will be ineffective. Too late and unnecessary bleeding will occur. The optimal, time is after the splenic artery has been ligated., Please rate this question:, , Discuss and give feedback, , Next question, , Splenectomy, Indications, , , , , , , Trauma: 1/4 are iatrogenic, Spontaneous rupture: EBV, Hypersplenism: hereditary spherocytosis or elliptocytosis etc, Malignancy: lymphoma or leukaemia, Splenic cysts, hydatid cysts, splenic abscesses, , Splenectomy, Technique, Trauma, , , , , GA, Long midline incision, If time permits insert a self retaining retractor (e.g. Balfour/ omnitract)
Page 3938 :
, , , , , , , , , Large amount of free blood is usually present. Pack all 4 quadrants of the abdomen. Allow, the anaesthetist to 'catch up', Remove the packs and assess the viability of the spleen. Hilar injuries and extensive, parenchymal lacerations will usually require splenectomy., Divide the short gastric vessels and ligate them., Clamp the splenic artery and vein. Two clamps on the patient side are better and allow for, double ligation and serve as a safety net if your assistant does not release the clamp, smoothly., Be careful not to damage the tail of the pancreas, if you do then this will need to be formally, removed and the pancreatic duct closed., Wash out the abdomen and place a tube drain to the splenic bed., Some surgeons implant a portion of spleen into the omentum, whether you decide to do this, is a matter of personal choice., Post operatively the patient will require prophylactic penicillin V and pneumococcal vaccine., , Elective, Elective splenectomy is a very different operation from that performed in the emergency setting. The, spleen is often large (sometimes massive). Most cases can be performed laparoscopically. The, spleen will often be macerated inside a specimen bag to facilitate extraction., Complications, , , , , , Haemorrhage (may be early and either from short gastrics or splenic hilar vessels, Pancreatic fistula (from iatrogenic damage to pancreatic tail), Thrombocytosis: prophylactic aspirin, Encapsulated bacteria infection e.g. Strep. pneumoniae, Haemophilus, influenzae and Neisseriameningitidis, , Post splenectomy changes, , , , , , Platelets will rise first (therefore in ITP should be given after splenic artery clamped), Blood film will change over following weeks, Howell Jolly bodies will appear, Other blood film changes include target cells and Pappenheimer bodies, Increased risk of post splenectomy sepsis, therefore prophylactic antibiotics and, pneumococcal vaccine should be given., , Post splenectomy sepsis, , , , Typically occurs with encapsulated organisms, Opsonisation occurs but then not recognised, Next question
Page 3939 :
A 19 year old man has a skin lesion excised from his back. He is reviewed clinically at 4 months post, procedure and the surgeon notes that the scar has begun to contract. Which of the following, facilitates this process?, , Myofibroblasts, , Neutrophils, , Granuloma formation, , Macrophages, , Fibroblasts, , As wounds mature the fibroblast population differentiates into myofibroblasts (usually 6 weeks and, beyond), these have a contractile phenotype and therefore help in contracting the wound. Immature, fibroblasts, though able to adhere to the ECM, do not have this ability., Please rate this question:, , Discuss and give feedback, , Next question, , Wound healing, Surgical wounds are either incisional or excisional and either clean, clean contaminated or dirty., Although the stages of wound healing are broadly similar their contributions will vary according to the, wound type., The main stages of wound healing include:, Haemostasis, , , , Minutes to hours following injury, Vasospasm in adjacent vessels, platelet plug formation and generation of fibrin rich clot., , Inflammation, , , , Typically days 1-5, Neutrophils migrate into wound (function impaired in diabetes).
Page 3940 :
, , , , Growth factors released, including basic fibroblast growth factor and vascular endothelial, growth factor., Fibroblasts replicate within the adjacent matrix and migrate into wound., Macrophages and fibroblasts couple matrix regeneration and clot substitution., , Regeneration, , , , , , Typically days 7 to 56, Platelet derived growth factor and transformation growth factors stimulate fibroblasts and, epithelial cells., Fibroblasts produce a collagen network., Angiogenesis occurs and wound resembles granulation tissue., , Remodeling, , , , , , , From 6 weeks to 1 year, Longest phase of the healing process and may last up to one year (or longer)., During this phase fibroblasts become differentiated (myofibroblasts) and these facilitate, wound contraction., Collagen fibres are remodeled., Microvessels regress leaving a pale scar., , The above description represents an idealised scenario. A number of diseases may distort this, process. Neovascularisation is an important early process. Endothelial cells may proliferate in the, wound bed and recanalise to form a vessel. Vascular disease, shock and sepsis can all compromise, microvascular flow and impair healing., Conditions such as jaundice will impair fibroblast synthetic function and immunity with a detrimental, effect in most parts of the healing process., Problems with scars:, Hypertrophic scars, Excessive amounts of collagen within a scar. Nodules may be present histologically containing, randomly arranged fibrils within and parallel fibres on the surface. The tissue itself is confined to the, extent of the wound itself and is usually the result of a full thickness dermal injury. They may go on, to develop contractures., Image of hypertrophic scarring. Note that it remains confined to the boundaries of the original, wound:
Page 3941 :
Image sourced from Wikipedia, , Keloid scars, Excessive amounts of collagen within a scar. Typically a keloid scar will pass beyond the boundaries, of the original injury. They do not contain nodules and may occur following even trivial injury. They, do not regress over time and may recur following removal., Image of a keloid scar. Note the extension beyond the boundaries of the original incision:, , Image sourced from Wikipedia, , Drugs which impair wound healing:
Page 3942 :
, , , , , Non steroidal anti inflammatory drugs, Steroids, Immunosupressive agents, Anti neoplastic drugs, , Closure, Delayed primary closure is the anatomically precise closure that is delayed for a few days but before, granulation tissue becomes macroscopically evident., Secondary closure refers to either spontaneous closure or to surgical closure after granulation tissue, has formed., Next question
Page 3943 :
Which of the following blood products can be administered to a non ABO matched recipient?, , Whole blood, , Platelets, , Packed red cells, , Stem cells, , Cryoprecipitate, , In the UK, platelets either come from pooling of the platelet component from four units of whole, donated blood, called random donor platelets, or by plasmapharesis from a single donor. The, platelets are suspended in 200-300 ml of plasma and may be stored for up to 4 days in the, transfusion laboratory where they are continually agitated at 22 oC to preserve function. One adult, platelet pool raises the normal platelet count by 30,000 to 60,000 platelets litre. ABO identical or, compatible platelets are preferred but not necessary in adults; but rhesus compatibility is required in, recipients who are children and women of childbearing age to prevent haemolytic disease of the, newborn., Please rate this question:, , Discuss and give feedback, , Next question, , Blood products - cross matching, Whole blood fractions, , Fraction, , Key points, , Packed red cells, , Used for transfusion in chronic anaemia and cases where infusion of large, volumes of fluid may result in cardiovascular compromise. Product obtained, by centrifugation of whole blood., , Platelet rich, , Usually administered to patients who are thrombocytopaenic and are bleeding
Page 3944 :
Fraction, , Key points, , plasma, , or require surgery. It is obtained by low speed centrifugation., , Platelet, concentrate, , Prepared by high speed centrifugation and administered to patients with, thrombocytopaenia., , Fresh frozen, plasma, , , , , , , , , Cryoprecipitate, , SAG-Mannitol, Blood, , , , , , Prepared from single units of blood., Contains clotting factors, albumin and immunoglobulin., Unit is usually 200 to 250ml., Usually used in correcting clotting deficiencies in patients with hepatic, synthetic failure who are due to undergo surgery., Usual dose is 12-15ml/Kg-1., It should not be used as first line therapy for hypovolaemia., Formed from supernatant of FFP., Rich source of Factor VIII and fibrinogen., Allows large concentration of factor VIII to be administered in small, volume., , Removal of all plasma from a blood unit and substitution with:, , , , , , Sodium chloride, Adenine, Anhydrous glucose, Mannitol, , Up to 4 units of SAG M Blood may be administered. Thereafter whole blood, is preferred. After 8 units, clotting factors and platelets should be considered., Cross matching, , Must be cross matched, , Can be ABO incompatible in adults, , Packed red cells, , Platelets, , Whole blood, , FFP
Page 3945 :
Must be cross matched, , Can be ABO incompatible in adults, , Cryoprecipitate, Next question
Page 3946 :
Which of the following would be the optimal fluid management option for a 45 year old man due to, undergo an elective right hemicolectomy?, , Remain "nil by mouth" for at least 6 hours pre-operatively and avoid intra venous fluids, , Remain "nil by mouth" for at least 6 hours pre-operatively and receive supplementary, intravenous 5% dextrose to replace lost calories, Allow him free access to oral fluids only until 30 minutes prior to surgery, , Administer a carbohydrate based loading drink 3 hours pre operatively, and avoid, intravenous fluids, Administer a carbohydrate based loading drink 6 hours pre-operatively and administer 5%, dextrose saline thereafter, , Patients for elective surgery should not have solids for 6 hours pre-operatively. However, clear fluids, may be given up to 2 hours pre-operatively. Enhanced recovery programmes are now the standard, of care in many countries around the world and involve administration of carbohydrate loading, drinks., The routine administration of 5% dextrose in the scenarios given above would convey little in the, way of benefit and increase the risks of electrolyte derangement post operatively., Please rate this question:, , Discuss and give feedback, , Next question, , Pre operative fluid management, Fluid management has been described in the British Consensus guidelines on IV fluid, therapy for Adult Surgical patients (GIFTASUP) and by NICE (CG174 December 2013), The Recommendations include:, , , , , Use Ringer's lactate or Hartmann's when a crystalloid is needed for resuscitation or, replacement of fluids. Avoid 0.9% N. Saline (due to risk of hyperchloraemic acidosis) unless, patient vomiting or has gastric drainage., Use 4%/0.18% dextrose saline or 5% dextrose in maintenance fluids. It should not be used, in resuscitation or as replacement fluids., Adult maintenance fluid requirements are: Na 50-100 mmol/day and K 40-80 mmol/day in, 1.5-2.5L fluid per day.
Page 3947 :
, , , , , , , , , , , , Patients for elective surgery should NOT be nil by mouth for >2 hours (unless has disorder of, gastric emptying)., Patients for elective surgery should be given carbohydrate rich drinks 2-3h before. Ideally, this should form part of a normal pre op plan to facilitate recovery., Avoid mechanical bowel preparation., If bowel prep is used, simultaneous administration of Hartmann's or Ringer's lactate should, be considered., Excessive fluid losses from vomiting should be treated with a crystalloid with potassium, replacement. 0.9% N. Saline should be given if there is hypochloraemia. Otherwise, Hartmann's or Ringer lactate should be given for diarrhoea/ileostomy/ileus/obstruction., Hartmann's should also be given in sodium losses secondary to diuretics., High risk patients should receive fluids and inotropes., An attempt should be made to detect pre or operative hypovolaemia using flow based, measurements. If this is not available, then clinical evaluation is needed i.e. JVP, pulse, volume etc., In Blood loss or infection causing hypovolaemia should be treated with a balanced crystalloid, or colloid (or until blood available in blood loss). A critically ill patient is unable to excrete Na, or H20 leading to a 5% risk of interstitial oedema. Therefore 5% dextrose as well as colloid, should be given., If patients need IV fluid resuscitation, use crystalloids that contain sodium in the range 130154 mmol/l, with a bolus of 500 ml over less than 15 minutes (NICE Guidance CG 174)., Next question
Page 3948 :
A 63 year old man undergoes a laparotomy and small bowel resection. Twelve hours post, operatively he is noted to have a decreased urine output. Which of the hormones listed below is, most likely to be responsible?, , Cortisol, , Atrial natriuretic hormone, , Vasopressin, , Insulin, , Glucagon, , Theme from January 2013 Exam, Vasopressin is released in increased quantities following most operative procedures and will tend to, cause water retention. For this reason, excessive administration of intravenous fluids in an attempt, to force a diuresis may cause fluid overload in post operative patients., Please rate this question:, , Discuss and give feedback, , Next question, , Response to surgery, Sympathetic nervous system, , , , , Noradrenaline from sympathetic nerves and adrenaline from adrenal medulla, Blood diverted from skin and visceral organs; bronchodilatation, reduced intestinal motility,, increased glucagon and glycogenolysis, insulin reduced, Heart rate and myocardial contractility are increased, , Acute phase response, , , , , TNF-α, IL-1, IL-2, IL-6, interferon and prostaglandins are released, Excess cytokines may cause SIRS, Cytokines increase the release of acute phase proteins
Page 3949 :
Endocrine response, , , , Hypothalamus, pituitary, adrenal axis, Increases ACTH and cortisol production:, , increases protein breakdown, increases blood glucose levels, , , , Aldosterone increases sodium re-absorption, Vasopressin increases water re-absorption and causes vasoconstriction, , Vascular endothelium, , , , , Nitric oxide produces vasodilatation, Platelet activating factor enhances the cytokine response, Prostaglandins produce vasodilatation and induce platelet aggregation, Next question
Page 3950 :
A 48 year old lady is being prepared for a Whipples procedure. A right sided subclavian line is, inserted and then anaesthesia is induced. Following intubation the patient becomes progressively, hypoxic and haemodynamically unstable. What is the most likely underlying explanation?, , Drug allergy, , Simple pneumothorax, , Tension pneumothorax, , Halothane toxicity, , Haemothorax, , Theme from September 2014 Exam, Central lines (and particularly subclavian lines) are risk factors for the development of, pneumothorax. In the context of positive pressure ventilation a tension pneumothorax is a strong, possibility and would be associated with haemodynamic instability., Please rate this question:, , Discuss and give feedback, , Next question, , Intravenous access, Venous access, A number of routes for establishing venous access are available., Peripheral venous cannula, Easy to insert with minimal morbidity. Wide lumen cannulae can provide rapid fluid infusions. When, properly managed infections may be promptly identified and the cannula easily re sited. Problems, relate to their peripheral sites and they are unsuitable for the administration of vaso active drugs,, such as inotropes and irritant drugs such as TPN (except in the very short term setting).
Page 3951 :
Central lines, Insertion is more difficult and most operators and NICE advocate the use of ultra sound., Coagulopathies may lead to haemorrhage following iatrogenic arterial injury. Femoral lines are, easier to insert and iatrogenic injuries easier to manage in this site however they are prone to high, infection rates. Internal jugular route is preferred. They have multiple lumens allowing for, administration of multiple infusions. The lumens are relatively narrow and thus they do not allow, particularly rapid rates of infusion., Intraosseous access, This is typically undertaken at the anteromedial aspect of the proximal tibia and provides access to, the marrow cavity and circulatory system. Although traditionally preferred in paediatric practice they, may be used in adults and a wide range of fluids can be infused using these devices., Tunneled lines, Tunneled lines such as Groshong and Hickman lines are popular devices for patients with long term, therapeutic requirements. These devices are usually inserted using ultrasound guidance into the, internal jugular vein and then tunneled under the skin. A cuff of woven material is sited near the end, and helps to anchor the device into the tissues. These cuffs require formal dissection to allow the, device to be removed. Tunneled lines can be linked to injection ports that are located under the skin., These are especially popular in paediatric practice., Peripherally inserted central cannula, Referred to as PICC lines, these are popular methods for establishing central venous access., Because they are inserted peripherally they are less prone to major complications relating to device, insertion than conventional central lines., Next question
Page 3952 :
Theme: Local anaesthetics, , A., B., C., D., E., F., G., H., , 1% xylocaine with 1 in 200,000 adrenaline, 1% Lignocaine, 0.5% Bupivacaine with 1 in 200,000 adrenaline, 0.5% Bupivicaine, Prilocaine 1%, Procaine 1%, Cocaine 25%, Cocaine 10%, , Please select the local anaesthetic formulation most appropriate to the procedure indicated. Each, option may be used once, more than once or not at all., , 8., , A 25 year old male presents with epistaxis, the ENT SpR plans to cauterise the bleeding, point with silver nitrate., 1% xylocaine with 1 in 200,000 adrenaline, Historically cocaine was popular for the management of epistaxis. Some surgeons will still, routinely use cocaine paste for this indication. Its popularity stems from the fact that it, causes vasospasm. However, systemic absorption carries the risk of adverse reactions., Where it is used the correct dose is 4%. Topically applied short acting local anaesthetic, agents with adrenaline may produce similar effects, with lower risks of toxicity., , 9., , An 18 year old boy requires a Zadeks procedure., You answered 1% xylocaine with 1 in 200,000 adrenaline, The correct answer is 1% Lignocaine, This is excision of the toe nail and a fast acting local anaesthetic is indicated. Adrenaline, should be avoided in this setting as it can cause digital ischaemia, , 10., , A 72 year old woman fractured her distal radius. A Biers Block is planned to facilitate, reduction of the fracture., You answered 1% xylocaine with 1 in 200,000 adrenaline, The correct answer is Prilocaine 1%, This is the best local anaesthetic for this. Bupivacaine may cause cardiotoxicity and should, be avoided.
Page 3953 :
Local anaesthetics: avoid use of adrenaline in extremities, Please rate this question:, , Discuss and give feedback, , Next question, , Local anaesthetic agents, Lidocaine, , , , , , , , , An amide, Local anaesthetic and a less commonly used antiarrhythmic (affects Na channels in the, axon), Hepatic metabolism, protein bound, renally excreted, Toxicity: due to IV or excess administration. Increased risk if liver dysfunction or low protein, states. Note acidosis causes lidocaine to detach from protein binding., Drug interactions: Beta blockers, ciprofloxacin, phenytoin, Features of toxicity: Initial CNS over activity then depression as lidocaine initially blocks, inhibitory pathways then blocks both inhibitory and activating pathways. Cardiac arrhythmias., Increased doses may be used when combined with adrenaline to limit systemic absorption., , Cocaine, , , , , , Pure cocaine is a salt, usually cocaine hydrochloride. It is supplied for local anaesthetic, purposes as a paste., It is supplied for clinical use in concentrations of 4 and 10%. It may be applied topically to the, nasal mucosa. It has a rapid onset of action and has the additional advantage of causing, marked vasoconstriction., It is lipophillic and will readily cross the blood brain barrier. Its systemic effects also include, cardiac arrhythmias and tachycardia., Apart from its limited use in ENT surgery it is otherwise used rarely in mainstream surgical, practice., , Bupivacaine, , , , , , Bupivacaine binds to the intracellular portion of sodium channels and blocks sodium influx, into nerve cells, which prevents depolarization., It has a much longer duration of action than lignocaine and this is of use in that it may be, used for topical wound infiltration at the conclusion of surgical procedures with long duration, analgesic effect., It is cardiotoxic and is therefore contra indicated in regional blockage in case the tourniquet, fails., Levobupivicaine (Chirocaine) is less cardiotoxic and causes less vasodilation.
Page 3954 :
Prilocaine, , , Similar mechanism of action to other local anaesthetic agents. However, it is far less, cardiotoxic and is therefore the agent of choice for intravenous regional anaesthesia e.g., Biers Block., , All local anaesthetic agents dissociate in tissues and this contributes to their therapeutic effect. The, dissociation constant shifts in tissues that are acidic e.g. where an abscess is present, and this, reduces the efficacy., Doses of local anaesthetics, , Agent, , Dose plain, , Dose with adrenaline, , Lignocaine, , 3mg/Kg, , 7mg/Kg, , Bupivacaine, , 2mg/Kg, , 2mg/Kg, , Prilocaine, , 6mg/Kg, , 9mg/Kg, , These are a guide only as actual doses depend on site of administration, tissue vascularity and comorbidities., Maximum total local anaesthetic doses, , , , , Lignocaine 1% plain - 3mg/ Kg - 200mg (20ml), Lignocaine 1% with 1 in 200,000 adrenaline - 7mg/Kg - 500mg (50ml), Bupivicaine 0.5% - 2mg/kg- 150mg (30ml), , Maximum doses are based on ideal body weight, Effects of adrenaline, Adrenaline may be added to local anaesthetic drugs. It prolongs the duration of action at the site of, injection and permits usage of higher doses (see above). It is contra indicated in patients taking, MAOI's or tricyclic antidepressants. The toxicity of bupivacaine is related to protein binding and, addition of adrenaline to this drug does not permit increases in the total dose of bupivacaine, in, contrast to the situation with lignocaine., References, An excellent review is provided by:, French J and Sharp L. Local Anaesthetics. Ann R Coll Surg Engl 2012; 94: 76-80., Next question
Page 3955 :
Which statement relating to the peri operative management of patients with diabetes mellitus is, false?, , They should be placed first on the operating list, , An intravenous sliding scale should be used in all cases, , Potassium supplementation is likely to be required in diabetics on a sliding scale, , Electrolyte abnormalities are more common after major visceral resections, , Blood glucose monitoring is required during general anaesthesia, , This is not the case and some type 2 diabetics may be managed using a watch and wait policy with, regular blood glucose monitoring. The cellular shifts of potassium with sliding scales may cause, problems with electrolyte management which should be anticipated., Please rate this question:, , Discuss and give feedback, , Next question, , Preparation for surgery, Elective and emergency patients require different preparation., Elective cases, , , , , , , , Consider pre admission clinic to address medical issues., Blood tests including FBC, U+E, LFT's, Clotting, Group and Save, Urine analysis, Pregnancy test, Sickle cell test, ECG/ Chest x-ray, , Exact tests to be performed will depend upon the proposed procedure and patient fitness., Risk factors for development of deep vein thrombosis should be assessed and a plan for, thromboprophylaxis formulated., Diabetes
Page 3956 :
Diabetic patients have greater risk of complications., Poorly controlled diabetes carries high risk of wound infections., Patients with diet or tablet controlled diabetes may be managed using a policy of omitting medication, and checking blood glucose levels regularly. Diabetics who are poorly controlled or who take insulin, will require a intravenous sliding scale. Potassium supplementation should also be given., Diabetic cases should be operated on first., Emergency cases, Stabilise and resuscitate where needed., Consider whether antibiotics are needed and when and how they should be administered., Inform blood bank if major procedures planned particularly where coagulopathies are present at the, outset or anticipated (e.g. Ruptured AAA repair), Don't forget to consent and inform relatives., Special preparation, Some procedures require special preparation:, , , , , , , , , , Thyroid surgery; vocal cord check., Parathyroid surgery; consider methylene blue to identify gland., Sentinel node biopsy; radioactive marker/ patent blue dye., Surgery involving the thoracic duct; consider administration of cream., Pheochromocytoma surgery; will need alpha and beta blockade., Surgery for carcinoid tumours; will need covering with octreotide., Colorectal cases; bowel preparation (especially left sided surgery), Thyrotoxicosis; lugols iodine/ medical therapy., , References, Management of adults with diabetes undergoing surgery and elective procedures. NHS Diabetes., April 2011., Next question
Page 3957 :
Theme: Surgical complications, , A., B., C., D., E., F., G., , Anastamotic leak, Chyle leak, Air leak, Biliary leak, Deep vein thrombosis, Portal vein thrombosis, Biliary obstruction, , Please select the most likely complication for the scenario given. Each option may be used once,, more than once or not at all., , 12., , A 67 year old female undergoes an oesophagogastrectomy for carcinoma of the distal, oesophagus. She complains of chest pain. The following day there is brisk bubbling into, the chest drain when suction is applied., You answered Anastamotic leak, The correct answer is Air leak, Damage to the lung substance may produce an air leak. Air leaks will manifest themselves, as a persistent pneumothorax that fails to settle despite chest drainage. When suction is, applied to the chest drainage system, active and persistent bubbling may be seen. Although, an anastomotic leak may produce a small pneumothorax, a large volume air leak is more, indicative of lung injury., , 13., , A 20 year old man has a protracted stay on ITU following a difficult appendicectomy for, perforated appendicitis with pelvic and sub phrenic abscesses. He has now deteriorated, further and developed deranged liver function tests., You answered Anastamotic leak, The correct answer is Portal vein thrombosis, Such marked intra-abdominal sepsis may well produce coagulopathy and the risk of portal, vein thrombosis., , 14., , A 63 year old man undergoes an Ivor - Lewis oesophagogastrectomy for carcinoma of the, distal oesophagus. The following day a pale opalescent liquid is noted to be draining from, the right chest drain., You answered Anastamotic leak
Page 3958 :
The correct answer is Chyle leak, Damage to the lymphatic duct may occur during this procedure and some surgeons, administer a lipid rich material immediately prior to surgery to facilitate its identification, in the event of iatrogenic damage., Please rate this question:, , Discuss and give feedback, , Next question, , Surgical complications, Complications occur in all branches of surgery and require vigilance in their detection. In many, cases anticipating the likely complications and appropriate avoidance will minimise their occurrence., For the purposes of the MRCS the important principles to appreciate are:, , , , , , , The anatomical principles that underpin complications, The physiological and biochemical derangements that occur, The most appropriate diagnostic modalities to utilise, The principles which underpin their management, , This is clearly a very broad area and impossible to cover comprehensively. There is considerable, overlap with other topic areas within the website., Avoiding complications, Some points to hopefully avert complications:, , , , , , , , , , , , World Health Organisation checklist- now mandatory prior to all operations, Prophylactic antibiotics - right dose, right drug, right time., Assess DVT/ PE risk and ensure adequate prophylaxis, MARK site of surgery, Use tourniquets with caution and with respect for underlying structures, Remember the danger of end arteries and in situations where they occur avoid using, adrenaline containing solutions and monopolar diathermy., Handle tissues with care- devitalised tissue serves as a nidus for infection, Be very wary of the potential for coupling injuries when using diathermy during laparoscopic, surgery, The inferior epigastric artery is a favorite target for laparoscopic ports and surgical drains!
Page 3959 :
Anatomical principles, Understanding the anatomy of a surgical field will allow appreciation of local and systemic, complications that may occur. For example, nerve injuries may occur following surgery in specific, regions. The table below lists some of the more important nerves to consider and mechanisms of, injury, , Nerve, , Mechanism, , Accessory, , Posterior triangle lymph node biopsy, , Sciatic, , Posterior approach to hip, , Common peroneal, , Legs in Lloyd Davies position, , Long thoracic, , Axillary node clearance, , Pelvic autonomic nerves, , Pelvic cancer surgery, , Recurrent laryngeal nerves, , During thyroid surgery, , Hypoglossal nerve, , During carotid endarterectomy, , Ulnar and median nerves, , During upper limb fracture repairs, , These are just a few. The detailed functional sequelae are particularly important and will often be, tested. In addition to nerve injuries certain procedures carry risks of visceral or structural injury., Again some particular favorites are given below:, , Structure, , Mechanism, , Thoracic duct, , During thoracic surgery e.g. Pneumonectomy, oesphagectomy
Page 3960 :
Structure, , Mechanism, , Parathyroid glands, , During difficult thyroid surgery, , Ureters, , During colonic resections/ gynaecological surgery, , Bowel perforation, , Use of Verres Needle to establish pneumoperitoneum, , Bile duct injury, , Failure to delineate Calots triangle carefully and careless use of diathermy, , Facial nerve, , Always at risk during Parotidectomy, , Tail of pancreas, , When ligating splenic hilum, , Testicular vessels, , During re-do open hernia surgery, , Hepatic veins, , During liver mobilisation, , Again many could be predicted from the anatomy of the procedure., Physiological derangements, A very common complication is bleeding and this is covered under the section of haemorrhagic, shock. Another variant is infection either superficial or deep seated. The organisms are covered, under microbiology and the features of sepsis covered under shock. Do not forget that, immunocompromised and elderly patients may present will atypical physiological parameters., Selected physiological and biochemical issues are given below:, , Complication, , Physiological/ Biochemical Problem, , Arrhythmias following, cardiac surgery, , Susceptibility to hypokalaemia (K+ <4.0 in cardiac patients)
Page 3961 :
Complication, , Physiological/ Biochemical Problem, , Neurosurgical electrolyte, disturbance, , SIADH following cranial surgery causing hyponatraemia, , Ileus following, gastrointestinal surgery, , Fluid sequestration and loss of electrolytes, , Pulmonary oedema following, pneumonectomy, , Loss of lung volume makes these patients very sensitive to fluid, overload, , Anastamotic leak, , Generalised sepsis causing mediastinitis or peritonitis depending, on site of leak, , Myocardial infarct, , May follow any type of surgery and in addition to direct cardiac, effects the decreased cardiac output may well compromise grafts, etc., , Try making a short list of problems and causes specific to your own clinical area., Diagnostic modalities, Depends largely on the suspected complication. In the acutely unwell surgical patient the following, baseline investigations are often helpful:, , , , , , , Full blood count, urea and electrolytes, C- reactive protein (trend rather than absolute value),, serum calcium, liver function tests, clotting (don't forget to repeat if on-going bleeding), Arterial blood gases, ECG (+cardiac enzymes if MI suspected), Chest x-ray to identify collapse/ consolidation, Urine analysis for UTI, , These will often identify the most common complications., Special tests, , , , CT scanning for identification of intra-abdominal abscesses, air and if luminal contrast is, used an anastomotic leak, Doppler USS of leg veins- for identification of DVT
Page 3962 :
, , , , CTPA for PE, Sending peritoneal fluid for U+E (if ureteric injury suspected) or amylase (if pancreatic injury, suspected), Echocardiogram if pericardial effusion suspected post cardiac surgery and no pleural window, made., , Management of complications, The guiding principal should be safe and timely intervention. Patients should be stabilised and if an, operation needs to occur in tandem with resuscitation then generally this should be of a damage, limitation type procedure rather than definitive surgery (which can be more safely undertaken in a, stable patient the following day)., Remember that recent surgery is a contra indication to thrombolysis and that in some patients IV, heparin may be preferable to a low molecular weight heparin (easier to reverse)., As a general rule laparotomies for bleeding should follow the core principle of quadrant packing and, then subsequent pack removal rather than plunging large clamps into pools of blood. The latter, approach invariable worsens the situation is often accompanied by significant visceral injury, particularly when done by the inexperienced. If packing controls a situation it is entirely acceptable, practice to leave packs in situ and return the patient to ITU for pack removal the subsequent day., Next question
Page 3963 :
Theme: Wound closure, , A., B., C., D., E., F., G., , Split thickness skin grafting, Full thickness skin graft, Local flap, Leave wound as it is and apply a simple dressing, Primary closure using interrupted 3/0 silk, Primary closure using 4/0 interrupted nylon, Use of vacuum assisted closure device, , Please select the most appropriate wound closure modality for the scenario given. Each option may, be used once, more than once or not at all., , 15., , A 68 year old man undergoes a wide local excision of a squamous cell carcinoma from the, lateral aspect his nose. At the completion of the operation the alar cartilage is visible., You answered Split thickness skin grafting, The correct answer is Local flap, This type of wound should be managed with a local rotational flap., , 16., , A 68 year old man has a seborrhoiec wart on his left cheek this is removed by use of, curretage leaving a superficial defect approximately 1cm in diameter., You answered Split thickness skin grafting, The correct answer is Leave wound as it is and apply a simple dressing, This type of superficial wound will re-epithelialise satisfactorily without grafting., , 17., , A 72 year old man undergoes a ray amputation for an infection complicating long standing, diabetes., You answered Split thickness skin grafting, The correct answer is Use of vacuum assisted closure device, Ray amputations for diabetic foot infections do not heal well and should never be, primarily closed. The use of vacuum assisted closure devices has been shown to improve, healing rates., , Please rate this question:
Page 3964 :
Discuss and give feedback, , Next question, , Wound healing, Surgical wounds are either incisional or excisional and either clean, clean contaminated or dirty., Although the stages of wound healing are broadly similar their contributions will vary according to the, wound type., The main stages of wound healing include:, Haemostasis, , , , Minutes to hours following injury, Vasospasm in adjacent vessels, platelet plug formation and generation of fibrin rich clot., , Inflammation, , , , , , , Typically days 1-5, Neutrophils migrate into wound (function impaired in diabetes)., Growth factors released, including basic fibroblast growth factor and vascular endothelial, growth factor., Fibroblasts replicate within the adjacent matrix and migrate into wound., Macrophages and fibroblasts couple matrix regeneration and clot substitution., , Regeneration, , , , , , Typically days 7 to 56, Platelet derived growth factor and transformation growth factors stimulate fibroblasts and, epithelial cells., Fibroblasts produce a collagen network., Angiogenesis occurs and wound resembles granulation tissue., , Remodeling, , , , , , , From 6 weeks to 1 year, Longest phase of the healing process and may last up to one year (or longer)., During this phase fibroblasts become differentiated (myofibroblasts) and these facilitate, wound contraction., Collagen fibres are remodeled., Microvessels regress leaving a pale scar.
Page 3965 :
The above description represents an idealised scenario. A number of diseases may distort this, process. Neovascularisation is an important early process. Endothelial cells may proliferate in the, wound bed and recanalise to form a vessel. Vascular disease, shock and sepsis can all compromise, microvascular flow and impair healing., Conditions such as jaundice will impair fibroblast synthetic function and immunity with a detrimental, effect in most parts of the healing process., Problems with scars:, Hypertrophic scars, Excessive amounts of collagen within a scar. Nodules may be present histologically containing, randomly arranged fibrils within and parallel fibres on the surface. The tissue itself is confined to the, extent of the wound itself and is usually the result of a full thickness dermal injury. They may go on, to develop contractures., Image of hypertrophic scarring. Note that it remains confined to the boundaries of the original, wound:, , Image sourced from Wikipedia, , Keloid scars, Excessive amounts of collagen within a scar. Typically a keloid scar will pass beyond the boundaries, of the original injury. They do not contain nodules and may occur following even trivial injury. They, do not regress over time and may recur following removal., Image of a keloid scar. Note the extension beyond the boundaries of the original incision:
Page 3966 :
Image sourced from Wikipedia, , Drugs which impair wound healing:, , , , , , Non steroidal anti inflammatory drugs, Steroids, Immunosupressive agents, Anti neoplastic drugs, , Closure, Delayed primary closure is the anatomically precise closure that is delayed for a few days but before, granulation tissue becomes macroscopically evident., Secondary closure refers to either spontaneous closure or to surgical closure after granulation tissue, has formed., Next question
Page 3967 :
Which of the following statements relating to pre-operative fluid management is false?, , 5% dextrose should be given cautiously in the elderly, , Patients undergoing elective colonic resections may continue to drink water up to 2 hours, prior to surgery, Normal saline increases the risk of hyperchloraemic acidosis, , A 70kg man will need approximately 100mmol of sodium daily, , Carbohydrate rich beverages and loading drinks can cause ileus therefore should be, avoided, , Carbohydrate loading is one of the enhanced recovery principles., Please rate this question:, , Discuss and give feedback, , Next question, , Pre operative fluid management, Fluid management has been described in the British Consensus guidelines on IV fluid, therapy for Adult Surgical patients (GIFTASUP) and by NICE (CG174 December 2013), The Recommendations include:, , , , , , , , , Use Ringer's lactate or Hartmann's when a crystalloid is needed for resuscitation or, replacement of fluids. Avoid 0.9% N. Saline (due to risk of hyperchloraemic acidosis) unless, patient vomiting or has gastric drainage., Use 4%/0.18% dextrose saline or 5% dextrose in maintenance fluids. It should not be used, in resuscitation or as replacement fluids., Adult maintenance fluid requirements are: Na 50-100 mmol/day and K 40-80 mmol/day in, 1.5-2.5L fluid per day., Patients for elective surgery should NOT be nil by mouth for >2 hours (unless has disorder of, gastric emptying)., Patients for elective surgery should be given carbohydrate rich drinks 2-3h before. Ideally, this should form part of a normal pre op plan to facilitate recovery., Avoid mechanical bowel preparation., If bowel prep is used, simultaneous administration of Hartmann's or Ringer's lactate should, be considered.
Page 3968 :
, , , , , , , , Excessive fluid losses from vomiting should be treated with a crystalloid with potassium, replacement. 0.9% N. Saline should be given if there is hypochloraemia. Otherwise, Hartmann's or Ringer lactate should be given for diarrhoea/ileostomy/ileus/obstruction., Hartmann's should also be given in sodium losses secondary to diuretics., High risk patients should receive fluids and inotropes., An attempt should be made to detect pre or operative hypovolaemia using flow based, measurements. If this is not available, then clinical evaluation is needed i.e. JVP, pulse, volume etc., In Blood loss or infection causing hypovolaemia should be treated with a balanced crystalloid, or colloid (or until blood available in blood loss). A critically ill patient is unable to excrete Na, or H20 leading to a 5% risk of interstitial oedema. Therefore 5% dextrose as well as colloid, should be given., If patients need IV fluid resuscitation, use crystalloids that contain sodium in the range 130154 mmol/l, with a bolus of 500 ml over less than 15 minutes (NICE Guidance CG 174)., Next question
Page 3969 :
Theme: ASA scoring, , A. ASA 1, B. ASA 2, C. ASA 3, D. ASA 4, E. ASA 5, , The American society of anaesthesiologists physical status scoring system is a popular method for, stratifying patients physical status. Please select the most appropriate ASA grade for each of the, following scenarios. Each option may be used once, more than once or not at all., , 19., , A 66 year old man is admitted following a collapse whilst waiting for a bus. Clinical examination, confirms a ruptured abdominal aortic aneurysm. He is moribund and hypotensive, You answered ASA 1, The correct answer is ASA 5, Theme from 2009 Exam, Patients who are moribund and will not survive without surgery are graded as ASA 5., , 20., , A 23 year old man with a 4cm lipoma on his flank is due to have this removed as a daycase. He is, otherwise well., ASA 1, Absence of co-morbidities and small procedure with no systemic compromise will equate to an, ASA score of 1., , 21., , A 72 year old man is due to undergo an inguinal hernia repair. He suffers from COPD and has an, exercise tolerance of 10 yards. He also has pitting oedema to the thighs.
Page 3970 :
You answered ASA 1, The correct answer is ASA 4, Severe systemic disease of this nature is a constant threat to life. Especially as he also has, evidence of cardiac failure., , Please rate this question:, , Discuss and give feedback, , Next question, , American Society of anesthesiologists physical status scoring system (ASA), ASA, grade, , Description, , 1, , No organic physiological, biochemical or psychiatric disturbance. The surgical pathology is, localised and has not invoked systemic disturbance, , 2, , Mild or moderate systemic disruption caused either by the surgical disease process or though, underlying pre-existing disease, , 3, , Severe systemic disruption caused either by the surgical pathology or pre-existing disease, , 4, , Patient has severe systemic disease that is a constant threat to life, , 5, , A patient who is moribund and will not survive without surgery, Next question
Page 3971 :
Theme: Wound infections, , A., B., C., D., E., F., , <5%, 5-10%, 15-25%, 25-40%, 0%, 75-100%, , Please select the anticipated risk of surgical site infections for the procedures described. Each, option may be used once, more than once or not at all., , 22., , A patient is undergoing a Hartmans procedure for perforated sigmoid diverticular disease., You answered <5%, The correct answer is 25-40%, This is a 'dirty' procedure and carries an SSI risk of 25-40 %., , 23., , A 23 year old male is undergoing an elective inguinal hernia repair., <5%, This is a clean procedure and carries the lowest risk of SSI., , 24., , A 43 year old women is undergoing a laparoscopic choelcystectomy for uncomplicated, biliary colic., You answered <5%, The correct answer is 5-10%, This is a clean contaminated procedure as the cystic duct is divided. Inadvertent spill of, bile converts the operation to a contaminated one and the risk of infection rises., , Please rate this question:, , Discuss and give feedback, , Next question, , Surgical site infection
Page 3972 :
, , , , , , , , Surgical site infections may occur following a breach in tissue surfaces and allow normal, commensals and other pathogens to initiate infection. They are a major cause of morbidity, and mortality., Surgical site infections (SSI) comprise up to 20% of all healthcare associated infections and, at least 5% of patients undergoing surgery will develop an SSI as a result., In many cases the organisms are derived from the patient's own body. Measures that may, increase the risk of SSI include:, Shaving the wound using a razor (disposable clipper preferred), Using a non iodine impregnated incise drape if one is deemed to be necessary, Tissue hypoxia, Delayed administration of prophylactic antibiotics in tourniquet surgery, , Preoperatively, , , , , Don't remove body hair routinely, If hair needs removal, use electrical clippers with single use head (razors increase infection, risk), Antibiotic prophylaxis if:, , - placement of prosthesis or valve, - clean-contaminated surgery, - contaminated surgery, , , , , Use local formulary, Aim to give single dose IV antibiotic on anaesthesia, If a tourniquet is to be used, give prophylactic antibiotics earlier, , Intraoperatively, , , , , , Prepare the skin with alcoholic chlorhexidine (Lowest incidence of SSI), Cover surgical site with dressing, A recent meta analysis has confirmed that administration of supplementary oxygen does not, reduce the risk of wound infection. In contrast to previous individual RCT's(1), Wound edge protectors do not appear to confer benefit (2), , Post operatively, Tissue viability advice for management of surgical wounds healing by secondary intention, Use of diathermy for skin incisions, In the NICE guidelines the use of diathermy for skin incisions is not advocated(3). Several, randomised controlled trials have been undertaken and demonstrated no increase in risk of SSI, when diathermy is used(4)., References, 1. Brar M et al.. Perioperative supplemental oxygen in colorectal patients: a meta analysis. J Surg
Page 3973 :
A 48 year old lady has a metallic heart valve and requires a paraumbilical hernia repair., Perioperatively she is receiving intra venous unfractionated heparin. To perform the surgery safely a, normal coagulation state is required. Which of the following strategies is routine standard practice?, , Administration of 10 mg of vitamin K the night prior to surgery and stopping the heparin, infusion 6 hours pre operatively, Stopping the heparin infusion 6 hours pre operatively, , Stop the heparin infusion on induction of anaesthesia, , Stopping the heparin infusion 6 hours pre operatively and administration of intravenous, protamine sulphate on commencing the operation, None of the above, , Patients with metallic heart valves will generally stop unfractionated heparin 6 hours pre operatively., Unfractionated heparin is generally cleared from the circulation within 2 hours so this will allow plenty, of time and is the method of choice in the elective setting. Protamine sulphate will reverse heparin, but is associated with risks of anaphylaxis and is thus not generally used unless immediate reversal, of anticoagulation is needed, e.g. coming off bypass., Please rate this question:, , Discuss and give feedback, , Next question, , Heparin, , , Causes the formation of complexes between antithrombin and activated thrombin/factors, 7,9,10,11 & 12, , Advantages of low molecular weight heparin, , , , , , , Better bioavailability, Lower risk of bleeding, Longer half life, Little effect on APTT at prophylactic dosages, Less risk of HIT
Page 3974 :
Complications, , , , , , Bleeding, Osteoporosis, Heparin induced thrombocytopenia (HIT): occurs 5-14 days after 1st exposure, Anaphylaxis, , In surgical patients that may need a rapid return to theatre, administration of unfractionated heparin, is preferred; as low molecular weight heparins have a longer duration of action and are harder to, reverse., Next question
Page 3975 :
Theme: Management of complications, , A., B., C., D., E., F., , Intra venous calcium, Intra venous potassium, Immediate removal of skin clips on ward, Removal of skin clips in theatre, Laryngoscopy, Intravenous thyroxine, , Please select the most appropriate intervention for the scenario given. Each option may be used, once, more than once or not at all., , 26., , A 22 year old lady undergoes a total thyroidectomy for Graves disease. 6 hours post, operatively she develops respiratory stridor and develops a small haematoma in the neck, You answered Intra venous calcium, The correct answer is Immediate removal of skin clips on ward, This is true emergency and evacuation and release of pressure must be performed, immediately, in this case by removal of skin clips on the ward, , 27., , A 44 year old lady undergoes a total thyroidectomy for recurrent multinodular goitre. 3, days post operatively she is still troubled by a hoarse voice., You answered Intra venous calcium, The correct answer is Laryngoscopy, Unfortunately one of the laryngeal nerves may have been injured and this will be best, demonstrated by laryngoscopy., , 28., , A 48 year old lady undergoes a redo thyroidectomy for a multinodular goitre. 24 hours, post operatively she develops oculogyric crises and diffuse muscle spasm., Intra venous calcium, She has most likely developed hypocalcaemic tetany and will require immediate calcium, supplementation., , Please rate this question:
Page 3976 :
Discuss and give feedback, , Next question, , Surgical complications, Complications occur in all branches of surgery and require vigilance in their detection. In many, cases anticipating the likely complications and appropriate avoidance will minimise their occurrence., For the purposes of the MRCS the important principles to appreciate are:, , , , , , , The anatomical principles that underpin complications, The physiological and biochemical derangements that occur, The most appropriate diagnostic modalities to utilise, The principles which underpin their management, , This is clearly a very broad area and impossible to cover comprehensively. There is considerable, overlap with other topic areas within the website., Avoiding complications, Some points to hopefully avert complications:, , , , , , , , , , , , World Health Organisation checklist- now mandatory prior to all operations, Prophylactic antibiotics - right dose, right drug, right time., Assess DVT/ PE risk and ensure adequate prophylaxis, MARK site of surgery, Use tourniquets with caution and with respect for underlying structures, Remember the danger of end arteries and in situations where they occur avoid using, adrenaline containing solutions and monopolar diathermy., Handle tissues with care- devitalised tissue serves as a nidus for infection, Be very wary of the potential for coupling injuries when using diathermy during laparoscopic, surgery, The inferior epigastric artery is a favorite target for laparoscopic ports and surgical drains!, , Anatomical principles, Understanding the anatomy of a surgical field will allow appreciation of local and systemic, complications that may occur. For example, nerve injuries may occur following surgery in specific, regions. The table below lists some of the more important nerves to consider and mechanisms of, injury, , Nerve, , Mechanism
Page 3977 :
Nerve, , Mechanism, , Accessory, , Posterior triangle lymph node biopsy, , Sciatic, , Posterior approach to hip, , Common peroneal, , Legs in Lloyd Davies position, , Long thoracic, , Axillary node clearance, , Pelvic autonomic nerves, , Pelvic cancer surgery, , Recurrent laryngeal nerves, , During thyroid surgery, , Hypoglossal nerve, , During carotid endarterectomy, , Ulnar and median nerves, , During upper limb fracture repairs, , These are just a few. The detailed functional sequelae are particularly important and will often be, tested. In addition to nerve injuries certain procedures carry risks of visceral or structural injury., Again some particular favorites are given below:, , Structure, , Mechanism, , Thoracic duct, , During thoracic surgery e.g. Pneumonectomy, oesphagectomy, , Parathyroid glands, , During difficult thyroid surgery, , Ureters, , During colonic resections/ gynaecological surgery, , Bowel perforation, , Use of Verres Needle to establish pneumoperitoneum
Page 3978 :
Structure, , Mechanism, , Bile duct injury, , Failure to delineate Calots triangle carefully and careless use of diathermy, , Facial nerve, , Always at risk during Parotidectomy, , Tail of pancreas, , When ligating splenic hilum, , Testicular vessels, , During re-do open hernia surgery, , Hepatic veins, , During liver mobilisation, , Again many could be predicted from the anatomy of the procedure., Physiological derangements, A very common complication is bleeding and this is covered under the section of haemorrhagic, shock. Another variant is infection either superficial or deep seated. The organisms are covered, under microbiology and the features of sepsis covered under shock. Do not forget that, immunocompromised and elderly patients may present will atypical physiological parameters., Selected physiological and biochemical issues are given below:, , Complication, , Physiological/ Biochemical Problem, , Arrhythmias following, cardiac surgery, , Susceptibility to hypokalaemia (K+ <4.0 in cardiac patients), , Neurosurgical electrolyte, disturbance, , SIADH following cranial surgery causing hyponatraemia, , Ileus following, gastrointestinal surgery, , Fluid sequestration and loss of electrolytes, , Pulmonary oedema following, , Loss of lung volume makes these patients very sensitive to fluid
Page 3979 :
Complication, , Physiological/ Biochemical Problem, , pneumonectomy, , overload, , Anastamotic leak, , Generalised sepsis causing mediastinitis or peritonitis depending, on site of leak, , Myocardial infarct, , May follow any type of surgery and in addition to direct cardiac, effects the decreased cardiac output may well compromise grafts, etc., , Try making a short list of problems and causes specific to your own clinical area., Diagnostic modalities, Depends largely on the suspected complication. In the acutely unwell surgical patient the following, baseline investigations are often helpful:, , , , , , , Full blood count, urea and electrolytes, C- reactive protein (trend rather than absolute value),, serum calcium, liver function tests, clotting (don't forget to repeat if on-going bleeding), Arterial blood gases, ECG (+cardiac enzymes if MI suspected), Chest x-ray to identify collapse/ consolidation, Urine analysis for UTI, , These will often identify the most common complications., Special tests, , , , , , , CT scanning for identification of intra-abdominal abscesses, air and if luminal contrast is, used an anastomotic leak, Doppler USS of leg veins- for identification of DVT, CTPA for PE, Sending peritoneal fluid for U+E (if ureteric injury suspected) or amylase (if pancreatic injury, suspected), Echocardiogram if pericardial effusion suspected post cardiac surgery and no pleural window, made., , Management of complications, The guiding principal should be safe and timely intervention. Patients should be stabilised and if an, operation needs to occur in tandem with resuscitation then generally this should be of a damage
Page 3980 :
limitation type procedure rather than definitive surgery (which can be more safely undertaken in a, stable patient the following day)., Remember that recent surgery is a contra indication to thrombolysis and that in some patients IV, heparin may be preferable to a low molecular weight heparin (easier to reverse)., As a general rule laparotomies for bleeding should follow the core principle of quadrant packing and, then subsequent pack removal rather than plunging large clamps into pools of blood. The latter, approach invariable worsens the situation is often accompanied by significant visceral injury, particularly when done by the inexperienced. If packing controls a situation it is entirely acceptable, practice to leave packs in situ and return the patient to ITU for pack removal the subsequent day., Next question
Page 3981 :
Theme: Use of blood products in surgery, , A., B., C., D., E., F., G., H., I., , Wait and see, Vitamin K, Fresh frozen plasma, Cryoprecipitate, Platelet cells, Packed red cells, Human Prothrombin Complex, Blood from the cell saver salvaged during surgery, Human Prothrombin Complex and vitamin K, , For each coagulation or bleeding problem please select the most appropriate item. Each item may, be used once, more than once or not at all., , 29., , A 74 year old male is undergoing a revision total hip replacement for aseptic loosening of, the prosthesis. He has lost 1500ml of blood during the procedure. This has been collected, in a cell saver., You answered Wait and see, The correct answer is Blood from the cell saver salvaged during surgery, This blood, which has been correctly collected can then be filtered and re-infused., , 30., , A 74 year old male with colon cancer sustains an iatrogenic splenic injury during surgery., He is bleeding profusely., You answered Wait and see, The correct answer is Packed red cells, The cell saver is inappropriate because the cells will be contaminated with malignant cells, and faecal matter from the open bowel., , 31., , A 53 year old cleaner is admitted with a fall. She is haemodynamically unstable and a CT, has shown a massive retroperitoneal haematoma. She is on warfarin., You answered Wait and see, The correct answer is Human Prothrombin Complex and vitamin K, Each hospital has different protocols and would recommend discussion with a
Page 3982 :
haematologist. However Human Prothrombin Complex with vitamin K is indicated in this, situation, as the condition is life threatening., Please rate this question:, , Discuss and give feedback, , Next question, , Blood products, Whole blood fractions, , Fraction, , Key points, , Packed red cells, , Used for transfusion in chronic anaemia and cases where infusion of large, volumes of fluid may result in cardiovascular compromise. Product obtained, by centrifugation of whole blood., , Platelet rich, plasma, , Usually administered to patients who are thrombocytopaenic and are bleeding, or require surgery. It is obtained by low speed centrifugation., , Platelet, concentrate, , Prepared by high speed centrifugation and administered to patients with, thrombocytopaenia., , Fresh frozen, plasma, , , , , , , , , Cryoprecipitate, , SAG-Mannitol, , , , , , Prepared from single units of blood., Contains clotting factors, albumin and immunoglobulin., Unit is usually 200 to 250ml., Usually used in correcting clotting deficiencies in patients with hepatic, synthetic failure who are due to undergo surgery., Usual dose is 12-15ml/Kg-1., It should not be used as first line therapy for hypovolaemia., Formed from supernatant of FFP., Rich source of Factor VIII and fibrinogen., Allows large concentration of factor VIII to be administered in small, volume., , Removal of all plasma from a blood unit and substitution with:
Page 3983 :
Blood, , , , , , Sodium chloride, Adenine, Anhydrous glucose, Mannitol, , Up to 4 units of SAG M Blood may be administered. Thereafter whole blood, is preferred. After 8 units, clotting factors and platelets should be considered., Cell saver devices, These collect patients own blood lost during surgery and then re-infuse it. There are two main types:, , , , Those which wash the blood cells prior to re-infusion. These are more expensive to purchase, and more complicated to operate. However, they reduce the risk of re-infusing contaminated, blood back into the patient., Those which do not wash the blood prior to re-infusion., , Their main advantage is that they avoid the use of infusion of blood from donors into patients and, this may reduce risk of blood borne infection. It may be acceptable to Jehovah's witnesses. It is, contraindicated in malignant disease for risk of facilitating disease dissemination., Blood products used in warfarin reversal, In some surgical patients the use of warfarin can pose specific problems and may require the use of, specialised blood products, Immediate or urgent surgery in patients taking warfarin(1) (2):, 1. Stop warfarin, 2. Vitamin K (reversal within 4-24 hours), -IV takes 4-6h to work (at least 5mg), -Oral can take 24 hours to be clinically effective, 3. Fresh frozen plasma, Used less commonly now as 1st line warfarin reversal, -30ml/kg-1, -Need to give at least 1L fluid in 70kg person (therefore not appropriate in fluid overload), -Need blood group, -Only use if human prothrombin complex is not available, 4. Human Prothrombin Complex (reversal within 1 hour), -Bereplex 50 u/kg, -Rapid action but factor 6 short half life, therefore give with vitamin K
Page 3984 :
References, 1. Dentali, F., C. Marchesi, et al. (2011). "Safety of prothrombin complex concentrates for rapid, anticoagulation reversal of vitamin K antagonists. A meta-analysis." Thromb Haemost 106(3): 429438., A 22 year old man presents with a peri anal abscess, which is managed by incision and drainage., The perineal wound measures 3cm by 3cm. Which of the following is best management option?, , Primary closure with interrupted mattress sutures, , Delayed primary closure with interrupted mattress sutures, , Allow the wound to heal by secondary intention, , Insert a seton through the cavity into the rectum to allow a mature fistula track to develop, , Perform a V-Y flap 2 weeks later, , Peri anal abscess are typically managed by secondary intention healing. Any attempt at early, closure is at best futile and at worst dangerous. Insertion of a seton may be considered by an, experienced colorectal surgeon, and only if the tract is clearly identifiable with minimal probing., There is seldom a need for flaps, ongoing discharge usually indicates a fistula (managed, separately)., Please rate this question:, , Discuss and give feedback, , Next question, , Wound healing, Surgical wounds are either incisional or excisional and either clean, clean contaminated or dirty., Although the stages of wound healing are broadly similar their contributions will vary according to the, wound type., The main stages of wound healing include:, Haemostasis, , , Minutes to hours following injury
Page 3985 :
, , Vasospasm in adjacent vessels, platelet plug formation and generation of fibrin rich clot., , Inflammation, , , , , , , Typically days 1-5, Neutrophils migrate into wound (function impaired in diabetes)., Growth factors released, including basic fibroblast growth factor and vascular endothelial, growth factor., Fibroblasts replicate within the adjacent matrix and migrate into wound., Macrophages and fibroblasts couple matrix regeneration and clot substitution., , Regeneration, , , , , , Typically days 7 to 56, Platelet derived growth factor and transformation growth factors stimulate fibroblasts and, epithelial cells., Fibroblasts produce a collagen network., Angiogenesis occurs and wound resembles granulation tissue., , Remodeling, , , , , , , From 6 weeks to 1 year, Longest phase of the healing process and may last up to one year (or longer)., During this phase fibroblasts become differentiated (myofibroblasts) and these facilitate, wound contraction., Collagen fibres are remodeled., Microvessels regress leaving a pale scar., , The above description represents an idealised scenario. A number of diseases may distort this, process. Neovascularisation is an important early process. Endothelial cells may proliferate in the, wound bed and recanalise to form a vessel. Vascular disease, shock and sepsis can all compromise, microvascular flow and impair healing., Conditions such as jaundice will impair fibroblast synthetic function and immunity with a detrimental, effect in most parts of the healing process., Problems with scars:, Hypertrophic scars, Excessive amounts of collagen within a scar. Nodules may be present histologically containing, randomly arranged fibrils within and parallel fibres on the surface. The tissue itself is confined to the, extent of the wound itself and is usually the result of a full thickness dermal injury. They may go on, to develop contractures., Image of hypertrophic scarring. Note that it remains confined to the boundaries of the original
Page 3986 :
wound:, , Image sourced from Wikipedia, , Keloid scars, Excessive amounts of collagen within a scar. Typically a keloid scar will pass beyond the boundaries, of the original injury. They do not contain nodules and may occur following even trivial injury. They, do not regress over time and may recur following removal., Image of a keloid scar. Note the extension beyond the boundaries of the original incision:, , Image sourced from Wikipedia
Page 3987 :
Drugs which impair wound healing:, , , , , , Non steroidal anti inflammatory drugs, Steroids, Immunosupressive agents, Anti neoplastic drugs, , Closure, Delayed primary closure is the anatomically precise closure that is delayed for a few days but before, granulation tissue becomes macroscopically evident., Secondary closure refers to either spontaneous closure or to surgical closure after granulation tissue, has formed., Next question
Page 3988 :
A surgeon is considering using lignocaine to provide local anaesthesia for a minor surgical, procedure. Which of the following may attenuate its action?, , Hyperkalaemia, , Administration with adrenaline, , Administration with bupivicaine, , Administration with sodium bicarbonate, , Use in tissues which are infected, Local anaesthetics are relatively ineffective when used in infected tissues., Most anaesthetic agents are amine bases that become ionised due to the relative alkalinity of, tissues. In active infection there may acidosis of the tissues and therefore local anasthetics may be, less effective. Some surgeons mix sodium bicarbonate as it is reported to reduce the pain, experienced by patients during administration., Please rate this question:, , Discuss and give feedback, , Next question, , Local anaesthetic agents, Lidocaine, , , , , , , , , An amide, Local anaesthetic and a less commonly used antiarrhythmic (affects Na channels in the, axon), Hepatic metabolism, protein bound, renally excreted, Toxicity: due to IV or excess administration. Increased risk if liver dysfunction or low protein, states. Note acidosis causes lidocaine to detach from protein binding., Drug interactions: Beta blockers, ciprofloxacin, phenytoin, Features of toxicity: Initial CNS over activity then depression as lidocaine initially blocks, inhibitory pathways then blocks both inhibitory and activating pathways. Cardiac arrhythmias., Increased doses may be used when combined with adrenaline to limit systemic absorption.
Page 3989 :
Cocaine, , , , , , Pure cocaine is a salt, usually cocaine hydrochloride. It is supplied for local anaesthetic, purposes as a paste., It is supplied for clinical use in concentrations of 4 and 10%. It may be applied topically to the, nasal mucosa. It has a rapid onset of action and has the additional advantage of causing, marked vasoconstriction., It is lipophillic and will readily cross the blood brain barrier. Its systemic effects also include, cardiac arrhythmias and tachycardia., Apart from its limited use in ENT surgery it is otherwise used rarely in mainstream surgical, practice., , Bupivacaine, , , , , , Bupivacaine binds to the intracellular portion of sodium channels and blocks sodium influx, into nerve cells, which prevents depolarization., It has a much longer duration of action than lignocaine and this is of use in that it may be, used for topical wound infiltration at the conclusion of surgical procedures with long duration, analgesic effect., It is cardiotoxic and is therefore contra indicated in regional blockage in case the tourniquet, fails., Levobupivicaine (Chirocaine) is less cardiotoxic and causes less vasodilation., , Prilocaine, , , Similar mechanism of action to other local anaesthetic agents. However, it is far less, cardiotoxic and is therefore the agent of choice for intravenous regional anaesthesia e.g., Biers Block., , All local anaesthetic agents dissociate in tissues and this contributes to their therapeutic effect. The, dissociation constant shifts in tissues that are acidic e.g. where an abscess is present, and this, reduces the efficacy., Doses of local anaesthetics, , Agent, , Dose plain, , Dose with adrenaline, , Lignocaine, , 3mg/Kg, , 7mg/Kg, , Bupivacaine, , 2mg/Kg, , 2mg/Kg
Page 3990 :
Agent, , Dose plain, , Dose with adrenaline, , Prilocaine, , 6mg/Kg, , 9mg/Kg, , These are a guide only as actual doses depend on site of administration, tissue vascularity and comorbidities., Maximum total local anaesthetic doses, , , , , Lignocaine 1% plain - 3mg/ Kg - 200mg (20ml), Lignocaine 1% with 1 in 200,000 adrenaline - 7mg/Kg - 500mg (50ml), Bupivicaine 0.5% - 2mg/kg- 150mg (30ml), , Maximum doses are based on ideal body weight, Effects of adrenaline, Adrenaline may be added to local anaesthetic drugs. It prolongs the duration of action at the site of, injection and permits usage of higher doses (see above). It is contra indicated in patients taking, MAOI's or tricyclic antidepressants. The toxicity of bupivacaine is related to protein binding and, addition of adrenaline to this drug does not permit increases in the total dose of bupivacaine, in, contrast to the situation with lignocaine., References, An excellent review is provided by:, French J and Sharp L. Local Anaesthetics. Ann R Coll Surg Engl 2012; 94: 76-80., Next question
Page 3991 :
Which of the following statements relating to use of total parenteral nutrition is untrue?, , It may cause steatosis and derangement of liver function tests, , Administration via a central line or PICC line is preferable to peripheral administration, , It is highly irritant to vessel walls, , It should be administered when a patient has an albumin less than15, , Administration of TPN for periods of less than 1 week is unlikely to produce noticable, benefits, , Albumin is a poor indicator of overall nutrition and the decision to start TPN should not be based on, this parameter alone. Patients should ideally be fed enterally where possible and if this is likely to, occur within 5-7 days then starting TPN is unlikely to confer benefit., Please rate this question:, , Discuss and give feedback, , Next question, , Nutrition Monitoring-NICE guidelines, , , , , , , Weight: daily if fluid balance concerns, otherwise weekly reducing to monthly, BMI: at start of feeding and then monthly, If weight cannot be obtained: monthly mid arm circumference or triceps skin fold thickness, Daily electrolytes until levels stable. Then once or twice a week., Weekly glucose, phosphate, magnesium, LFTs, Ca, albumin, FBC, MCV, , levels if stable, , , , , , 2-4 weekly Zn, Folate, B12 and Cu levels if stable, 3-6 monthly iron and ferritin levels, manganese (if on home parenteral regime), 6 monthly vitamin D, Bone densitometry initially on starting home parenteral nutrition then every 2 years, Next question
Page 3992 :
Which of the following statements relating to use of tourniquets in surgery is false?, , The use of an esmarch bandage tourniquet to exsanguinate the limb reduces the incidence, of neuropraxia., Excessive inflation pressures are amongst the commonest causes of nerve injury related to, tourniquet use., Tourniquet deflation causes a fall in CVP., , Children require lower inflation pressures than adults., , In patients developing neuropraxia related to tourniquets the radial nerve is most, frequently affected., , The use of esmarch bandage tourniquet increases the risk of nerve injury as it increases pressure in, the limb. Limb elevation is safer., Please rate this question:, , Discuss and give feedback, , Next question, , Tourniquets, Tourniquets are used during surgery to minimise blood loss and ensure a clear operative field. They, must be correctly applied and monitored. They are applied to extremities and in most cases are, inflated using a pressure monitoring system., There are a number of systemic effects that can accompany tourniquet use, these can be divided, into those which occur following inflation and those that occur once the tourniquet is deflated., Post inflation, Increased systemic vascular resistance, increased CVP and increased BP, Slower gradual increase in BP over time, Induced hypercoagulable state, Slow increase in core temperature, Post deflation, Fall in CVP, BP and SVR, Increased end tidal carbon dioxide, Enhanced fibrinolysis, Fall in core temperature, Raised serum potassium and lactate levels
Page 3993 :
Contra indications, , Absolute, , Relative, , AV fistula, Severe peripheral vascular disease, Previous vascular surgery, Bone fracture or thrombosis at the site of tourniquet, application, , Sickle cell disease, History of thromboembolic, events, Skin grafts, Localised infection, Lymphoedema, , Local complications, , , , , , Damage to skin, Damage to muscle (rarely compartment syndrome), Damage to vessels, Neuropraxia, Next question
Page 3994 :
In relation to patients with type 1 diabetes mellitus undergoing surgery, which of the following, statements is untrue?, , They should not receive oral carbohydrate loading drinks as part of enhanced recovery, programmes, When a variable rate insulin infusion is required 0.45% sodium chloride with either, 0.15% or 0.3% potassium are the fluids of choice, Hourly intraoperative blood glucose measurements are required, , Insulin infusions are only required in patients who will miss more than two meals or who, are nil by mouth for greater than 12 hours, Blood glucose levels persistently greater than 12 should initiate a change in therapy, Insulin should not be stopped in patients with type 1 diabetes and omission of more than one meal, will usually require a variable rate insulin infusion, Type 1 diabetics who take insulin should have this continued through the perioperative period., Fluid guidelines in diabetics differ and are not well covered in NPSA fluid guidelines., Please rate this question:, , Discuss and give feedback, , Next question, , Preparation for surgery, Elective and emergency patients require different preparation., Elective cases, , , , , , , , Consider pre admission clinic to address medical issues., Blood tests including FBC, U+E, LFT's, Clotting, Group and Save, Urine analysis, Pregnancy test, Sickle cell test, ECG/ Chest x-ray, , Exact tests to be performed will depend upon the proposed procedure and patient fitness.
Page 3995 :
Risk factors for development of deep vein thrombosis should be assessed and a plan for, thromboprophylaxis formulated., Diabetes, Diabetic patients have greater risk of complications., Poorly controlled diabetes carries high risk of wound infections., Patients with diet or tablet controlled diabetes may be managed using a policy of omitting medication, and checking blood glucose levels regularly. Diabetics who are poorly controlled or who take insulin, will require a intravenous sliding scale. Potassium supplementation should also be given., Diabetic cases should be operated on first., Emergency cases, Stabilise and resuscitate where needed., Consider whether antibiotics are needed and when and how they should be administered., Inform blood bank if major procedures planned particularly where coagulopathies are present at the, outset or anticipated (e.g. Ruptured AAA repair), Don't forget to consent and inform relatives., Special preparation, Some procedures require special preparation:, , , , , , , , , , Thyroid surgery; vocal cord check., Parathyroid surgery; consider methylene blue to identify gland., Sentinel node biopsy; radioactive marker/ patent blue dye., Surgery involving the thoracic duct; consider administration of cream., Pheochromocytoma surgery; will need alpha and beta blockade., Surgery for carcinoid tumours; will need covering with octreotide., Colorectal cases; bowel preparation (especially left sided surgery), Thyrotoxicosis; lugols iodine/ medical therapy., , References, Management of adults with diabetes undergoing surgery and elective procedures. NHS Diabetes., April 2011., Next question
Page 3996 :
A 72 year old man is recovering from an inguinal hernia repair when he suffers from an extensive, CVA. He is managed on the rehabilitation unit. However, he is still not able to feed safely and, repeated swallowing assessments have shown that he tends to aspirate. Which of the following is, the best option for long term feeding?, , PEG tube feeding, , Feeding jejunostomy, , Total parenteral nutrition, , Long term naso gastric tube feeding, , Withold feeding and palliate, , Theme from September 2014 exam, A PEG tube is the best long term option although they are associated with a significant degree of, morbidity. A feeding jejunostomy would require a general anaesthetic. TPN is not a good option., Long term naso gastric feeding is usually unsatisfactory., Please rate this question:, , Discuss and give feedback, , Next question, , Enteral Feeding, , , , , , , , , , , , Identify patients as malnourished or at risk (see below), Identify unsafe or inadequate oral intake with functional GI tract, Consider for enteral feeding, Gastric feeding unless upper GI dysfunction (then for duodenal or jejunal tube), Check NG placement using aspiration and pH (check post pyloric tubes with AXR), Gastric feeding > 4 weeks consider long-term gastrostomy, Consider bolus or continuous feeding into the stomach, ITU patients should have continuous feeding for 16-24h (24h if on insulin), Consider motility agent in ITU or acute patients for delayed gastric emptying. If this doesn't, work then try post pyloric feeding or parenteral feeding., PEG can be used 4 hours after insertion, but should not be removed until >2 weeks after, insertion., , Surgical patients due to have major abdominal surgery: if malnourished, unsafe swallow/inadequate, oral intake and functional GI tract then consider pre operative enteral feeding.
Page 3997 :
Patients identified as being malnourished, , , , , BMI < 18.5 kg/m2, unintentional weight loss of > 10% over 3-6/12, BMI < 20 kg/m 2 and unintentional weight loss of > 5% over 3-6/12, , AT RISK of malnutrition, , , , , , Eaten nothing or little > 5 days, who are likely to eat little for a further 5 days, Poor absorptive capacity, High nutrient losses, High metabolism, , Reference, Stroud M et al. Guidelines for enteral feeding in adult hospital patients. Gut 2003; 52(Suppl VII):vii1 vii12., Next question
Page 3998 :
Theme: Anaesthetic agents, , A., B., C., D., E., F., G., H., , Halothane, Propofol, Ketamine, Etomidate, Sodium thiopentone, Flumazenil, Naloxone, Sevoflurane, , Please select the drug which most closely matches the description given. Each option may be used, once, more than once or not at all., , 38., , An agent which reverses the action of midazolam, You answered Halothane, The correct answer is Flumazenil, Flumazenil antagonises the effects of benzodiazepines by competition at GABA binding, sites. Since may benzodiazepines have longer half lives than flumazenil patients still, require close monitoring after receiving the drug., , 39., , An agent which is associated with hepatotoxicity, Halothane, Halothane is hepatotoxic. Despite this it remains in mainstream use. It should be avoided, in patients with hepatic dysfunction, and scavengers should be used in theatres as, accumulation of the drug may be injurious to theatre staff., , 40., , An anaesthetic agent which has anti emetic properties, You answered Halothane, The correct answer is Propofol, Propofol is rapidly metabolised and has mild/ moderate anti emetic properties. It is the, agent of choice in most day case operations for this reason., , Please rate this question:
Page 3999 :
Discuss and give feedback, , Next question, , Anaesthetic agents, The table below summarises some of the more commonly used IV induction agents, , Agent, , Specific features, , Propofol, , , , , , , , , Rapid onset of anaesthesia, Pain on IV injection, Rapidly metabolised with little accumulation of metabolites, Proven anti emetic properties, Moderate myocardial depression, Widely used especially for maintaining sedation on ITU, total IV, anaesthesia and for daycase surgery, , Sodium, thiopentone, , , , Extremely rapid onset of action making it the agent of choice for rapid, sequence of induction, Marked myocardial depression may occur, Metabolites build up quickly, Unsuitable for maintenance infusion, Little analgesic effects, , , , , , , Ketamine, , , , , , , Etomidate, , , , , , , May be used for induction of anaesthesia, Has moderate to strong analgesic properties, Produces little myocardial depression making it a suitable agent for, anaesthesia in those who are haemodynamically unstable, May induce state of dissociative anaesthesia resulting in nightmares, Has favorable cardiac safety profile with very little haemodynamic, instability, No analgesic properties, Unsuitable for maintaining sedation as prolonged (and even brief) use, may result in adrenal suppression, Post operative vomiting is common, Next question
Page 4000 :
A 57 year old man is coming off the cardiac bypass circuit following a successful coronary artery, bypass procedure. Which drug should be administered to normalise the patients clotting prior to, decannulation and chest closure?, , Intravenous vitamin K, , Protamine sulphate, , Aprotinin, , Fresh frozen plasma, , None of the above, , Since cardiac bypass circuits are thrombogenic large doses of intravenous heparin are administered., This is reversed with protamine sulphate. FFP may be effective but would carry a significant risk of, fluid overload., Please rate this question:, , Discuss and give feedback, , Next question, , Heparin, , , Causes the formation of complexes between antithrombin and activated thrombin/factors, 7,9,10,11 & 12, , Advantages of low molecular weight heparin, , , , , , , Better bioavailability, Lower risk of bleeding, Longer half life, Little effect on APTT at prophylactic dosages, Less risk of HIT, , Complications
Page 4001 :
, , , , , Bleeding, Osteoporosis, Heparin induced thrombocytopenia (HIT): occurs 5-14 days after 1st exposure, Anaphylaxis, , In surgical patients that may need a rapid return to theatre, administration of unfractionated heparin, is preferred; as low molecular weight heparins have a longer duration of action and are harder to, reverse., Next question
Page 4002 :
A 34 year old man is suffering from septic shock and receives and infusion of Dextran 70. Which of, the following complications may potentially ensue?, , Anaphylaxis, , Vomiting, , Acute hepatic failure, , Digital necrosis, , Deep vein thrombosis, Dextran 40 and 70 have higher incidence of anaphylaxis than either gelatins or starches., Dextrans are branched polysaccharide molecules. Dextran 40 and 70 are available. The higher, molecular weight dextran 70 may persist for up to 8 hours. They inhibit platelet aggregation and, leucocyte plugging in the microcirculation. Thereby improving flow through the microcirculation,, primarily of use in sepsis., Unlike many other intravenous fluids Dextrans are a recognised cause of anaphylaxis., Please rate this question:, , Discuss and give feedback, , Next question, , Post operative fluid management, Composition of commonly used intravenous fluids mmol-1, , Na, , K, , Cl, , Bicarbonate, , Lactate, , Plasma, , 137-147, , 4-5.5, , 95-105, , 22-25, , -, , 0.9% Saline, , 153, , -, , 153, , -, , -, , Dextrose / saline, , 30.6, , -, , 30.6, , -, , -
Page 4003 :
Hartmans, , 130, , 4, , 110, , -, , 28, , Post operative fluid management, In the UK the GIFTASUP and NICE (CG174 2013) guidelines (see reference below) were devised to, try and provide some consensus guidance as to how intravenous fluids should be administered. A, decade ago it was a commonly held belief that little harm would occur as a result of excessive, administration of normal saline and many oliguric post operative patients received enormous, quantities of IV fluids. As a result they developed hyperchloraemic acidosis. With greater, understanding of this potential complication, the use of electrolyte balanced solutions (Ringers, lactate/ Hartmans) is now favored over normal saline., The other guidance includes:, , , , , , , , Fluids given should be documented clearly and easily available, Assess the patient's fluid status when they leave theatre, If a patient is haemodynamically stable and euvolaemic, aim to restart oral fluid intake as, soon as possible, Review patients whose urinary sodium is < 20, If a patient is oedematous, hypovolaemia if present should be treated first. This should then, be followed by a negative balance of sodium and water, monitored using urine Na excretion, levels, Solutions such as Dextran 70 should be used in caution in patients with sepsis as there is a, risk of developing acute renal injury, , References, NICE guidance CG174. Intravenous fluid therapy in adults. December 2013., British Consensus Guidelines on Intravenous Fluid Therapy for Adult Surgical Patients. GIFTASUP, (2009), Next question
Page 4004 :
In relation to operating in the elderly which statement is false?, , A 30 minute increment in operation length is associated with increase in mortality in, patients over the age of 80, Hypoalbuminaemia is associated with increased mortality, , Statins given preoperatively reduce perioperative cardiac events, , Elevated brain (or B-type) natriuretic peptide (BNP) levels before undergoing non cardiac, surgery is associated with high risk of cardiac mortality and all cause mortality, Beta blockers should be stopped acutely prior to surgery due to risk of perioperative, hypotension, , Beta blockers should not be stopped acutely prior to surgery as there may be a rebound effect, associated with increased complications., Brain natriuretic peptide is a neurohormone synthesized in the cardiac ventricles. Levels have been, used to assess prognosis in heart failure and acute coronary syndromes. Preoperative elevated, brain natriuretic peptide levels identify patients undergoing non cardiac surgery at high risk of, cardiac mortality and all cause mortality., All patients with peripheral vascular disease should take statins prior to vascular surgery as studies, have shown a 50% risk reduction and a reduction in perioperative cardiac events., Reference, 1. Dernellis J, Panaretou M. Assessment of cardiac risk before non-cardiac surgery: brain natriuretic, peptide in 1590 patients. Heart 2006;92:1645-1650, 2. Poldermans, D et al Fluvastatin and Perioperative Events in Patients Undergoing Vascular, Surgery. NEJM 2009; 361:980-989, Please rate this question:, , Discuss and give feedback, , Next question, , Proactive care of older people undergoing surgery (POPS), , , , Comprehensive geriatric assessment, MDT assessment preoperatively
Page 4005 :
, , , , , Main predictors of complications are co-morbidities cardiac disease and reduced functional, capacity - preoperative assessment is the key to preventing adverse postoperative outcomes, Patients screened for risk factors (albumin <30, co morbidities), Management plan made and disseminated to all involved, Patients education: pain relief, post op exercises, nutrition, , Outcomes:, , , , Fewer postoperative medical complications, Reduced length of stay by 4.5 days, , References, Proactive care of older people undergoing surgery (POPS), Danielle Harari et al., Age and Ageing 2007 36(2):190-196, Next question
Page 4006 :
Which of the following intravenous fluid solutions has the greatest chloride content?, , Dextrose / saline, , Normal saline, , Hartmanns solution, , Ringers lactate, , 5% dextrose, , Normal saline has the highest chloride content and excessive administration of normal saline is a, recognised risk factor for the development of hyperchloraemic metabolic acidosis., Please rate this question:, , Discuss and give feedback, , Next question, , Intra operative fluid management, Composition of commonly used intravenous fluids mmol-1, , Na, , K, , Cl, , Bicarbonate, , Lactate, , Plasma, , 137-147, , 4-5.5, , 95-105, , 22-25, , -, , 0.9% Saline, , 153, , -, , 153, , -, , -
Page 4007 :
Dextrose / saline, , 30.6, , -, , 30.6, , -, , -, , Hartmans, , 130, , 4, , 110, , -, , 28, , Recommendations for intra operative fluid management, The latest set of NICE guidelines produced in 2013 relating to intravenous fluids did not specifically, address the requirements of intra operative fluid administration. The reason for this is that, administration of fluids in this specific situation does not lend itself to rigid algorithms., With the introduction of enhanced recovery programmes 10 years ago there was an increasing, emphasis of the concept of fluid restriction. Historically, patients received very large volumes of, saline rich solutions peri-operatively. Clearing the sodium load of a single litre of saline may take up, to 36 hours or more. This can have deleterious effects on the tissues including the development of, oedema. This results in poor perfusion, increased risk of ileus and wound breakdown. A tailored, approach to fluid administration is now practiced and far greater usage is made of cardiac output, monitors in providing goal directed fluid therapy., References, British Consensus Guidelines on Intravenous Fluid Therapy for Adult Surgical Patients, GIFTASUP (2009) Revised May 2011., Frost P. Intravenous fluid therapy in adult inpatients. BMJ 2015 (350): 31-34., Next question
Page 4008 :
A 43 year old lady with a metallic heart valve has just undergone an elective paraumbilical hernia, repair. In view of her metallic valve, she is given unfractionated heparin perioperatively. How should, the therapeutic efficacy be monitored, assuming her renal function is normal?, , Therapeutic monitoring is not required, , Measurement of APTT, , Measurement of INR, , Measurement of Prothromin time, , None of the above, , Unlike low molecular weight heparins that do not require monitoring unfractionated heparin does, require monitoring, this is done by measuring the APTT., Please rate this question:, , Discuss and give feedback, , Next question, , Heparin, , , Causes the formation of complexes between antithrombin and activated thrombin/factors, 7,9,10,11 & 12, , Advantages of low molecular weight heparin, , , , , , , Better bioavailability, Lower risk of bleeding, Longer half life, Little effect on APTT at prophylactic dosages, Less risk of HIT, , Complications
Page 4009 :
, , , , , Bleeding, Osteoporosis, Heparin induced thrombocytopenia (HIT): occurs 5-14 days after 1st exposure, Anaphylaxis, , In surgical patients that may need a rapid return to theatre, administration of unfractionated heparin, is preferred; as low molecular weight heparins have a longer duration of action and are harder to, reverse., Next question
Page 4010 :
A patient receives atropine as pre medication prior to a laparotomy. Which of the following is least, likely to occur?, , Pupillary dilation, , Dry mouth, , Urinary retention, , Bradycardia, , Decreased salivation, , Since it inhibits vagal tone, the use of atropine will typically result in an increased heart rate., Please rate this question:, , Discuss and give feedback, , Next question, , Atropine, Atropine is a muscarinic receptor antagonist (competitive antagonist for the muscarinic acetylcholine, receptor). It therefore inhibits parasympathetic activity.It was traditionally used as a premedication, for anaesthesia because it reduced bronchial secretions, salivary secretions and bradycardia from, increased vagal tone on anaesthetic induction. Modern anaesthetic techniques have reduced the, need for routine use of this drug. Its other effects include urinary retention and pupillary dilatation., Next question
Page 4011 :
Theme: Pre operative preparation, , A., B., C., D., E., F., G., H., I., , Methylene Blue intravenously 1 hour pre-operatively, Lugol's iodine, 100ml single cream given 4 hours prior to surgery, Carbohydrate loading drink 2 hours prior to surgery, Picolax sachet, Fleet enema, Intravenous calcium chloride, 1mg lorazepam orally 30 minutes pre operatively, Patent blue dye intravenously, , For each procedure please select the most appropriate procedure specific preparation required., Each option may be used once, more than once or not at all., , 47., , A 45 year old man is due to undergo an Ivor Lewis oesophagectomy for a carcinoma of the, distal oesophagus., You answered Methylene Blue intravenously 1 hour pre-operatively, The correct answer is 100ml single cream given 4 hours prior to surgery, This will facilitate identification of the thoracic duct if it is inadvertently divided during, the operation., , 48., , A 32 year old man is due to undergo a right hemicolectomy for a large caecal sessile, polyp., You answered Methylene Blue intravenously 1 hour pre-operatively, The correct answer is Carbohydrate loading drink 2 hours prior to surgery, This is now a standard feature of colonic enhanced recovery programmes.The, administration of carbohydrate rich loading drinks results in lower incidence of ileus. The, drink is usually administered 2 hours pre-operatively and is rapidly absorbed from the GI, tract., , 49., , A 67 year old women is due to undergo a parathyroidectomy for a parathyroid adenoma., Methylene Blue intravenously 1 hour pre-operatively, Though not universally adopted, many endocrine surgeons will administer methylene blue, as it will facilitate identification of the parathyroid glands.
Page 4012 :
Please rate this question:, , Discuss and give feedback, , Next question, , Preparation for surgery, Elective and emergency patients require different preparation., Elective cases, , , , , , , , Consider pre admission clinic to address medical issues., Blood tests including FBC, U+E, LFT's, Clotting, Group and Save, Urine analysis, Pregnancy test, Sickle cell test, ECG/ Chest x-ray, , Exact tests to be performed will depend upon the proposed procedure and patient fitness., Risk factors for development of deep vein thrombosis should be assessed and a plan for, thromboprophylaxis formulated., Diabetes, Diabetic patients have greater risk of complications., Poorly controlled diabetes carries high risk of wound infections., Patients with diet or tablet controlled diabetes may be managed using a policy of omitting medication, and checking blood glucose levels regularly. Diabetics who are poorly controlled or who take insulin, will require a intravenous sliding scale. Potassium supplementation should also be given., Diabetic cases should be operated on first., Emergency cases, Stabilise and resuscitate where needed., Consider whether antibiotics are needed and when and how they should be administered., Inform blood bank if major procedures planned particularly where coagulopathies are present at the, outset or anticipated (e.g. Ruptured AAA repair), Don't forget to consent and inform relatives., Special preparation, Some procedures require special preparation:, , , , , , , Thyroid surgery; vocal cord check., Parathyroid surgery; consider methylene blue to identify gland., Sentinel node biopsy; radioactive marker/ patent blue dye., Surgery involving the thoracic duct; consider administration of cream., Pheochromocytoma surgery; will need alpha and beta blockade.
Page 4013 :
, , , , Surgery for carcinoid tumours; will need covering with octreotide., Colorectal cases; bowel preparation (especially left sided surgery), Thyrotoxicosis; lugols iodine/ medical therapy., , References, Management of adults with diabetes undergoing surgery and elective procedures. NHS Diabetes., April 2011., Next question
Page 4014 :
Theme: Local anaesthetics, , A., B., C., D., E., F., G., H., , 1% xylocaine with 1 in 200,000 adrenaline, 1% Lignocaine, 0.5% Bupivacaine with 1 in 200,000 adrenaline, 0.5% Bupivacaine, Prilocaine 1%, Procaine 1%, Cocaine 4%, Cocaine 10%, , Please select the local anaesthetic formulation most appropriate to the procedure indicated. Each, option may be used once, more than once or not at all., , 50., , A 28 year old man has a sebaceous cyst of the scalp that requires excision., 1% xylocaine with 1 in 200,000 adrenaline, As scalp wounds can bleed profusely an adrenaline containing solution is preferred., Xylocaine is similar to lignocaine in its onset and duration of action., , 51., , A 32 year old man has an appendicectomy performed through a Lanz incision, which, anaesthetic would you infiltrate the wound with to provide post operative analgesia., You answered 1% xylocaine with 1 in 200,000 adrenaline, The correct answer is 0.5% Bupivacaine, A long acting local anaesthetic is preferred.There is little advantage to adding a short, acting local anaesthetic agent since by the time the patient has recovered following surgery, the bupivacaine will be active., , 52., , A 43 year old man is due to undergo a vasectomy., You answered 1% xylocaine with 1 in 200,000 adrenaline, The correct answer is 1% Lignocaine, Plain lignocaine will suffice. This will give rapid onset of action. Bupivacaine will take too, long to take effect. There would be little additional benefit derived for adding adrenaline., , Use of adrenaline with local anaesthetic agents prolongs duration of actions and allows, administration of larger doses.
Page 4015 :
Please rate this question:, , Discuss and give feedback, , Next question, , Local anaesthetic agents, Lidocaine, , , , , , , , , An amide, Local anaesthetic and a less commonly used antiarrhythmic (affects Na channels in the, axon), Hepatic metabolism, protein bound, renally excreted, Toxicity: due to IV or excess administration. Increased risk if liver dysfunction or low protein, states. Note acidosis causes lidocaine to detach from protein binding., Drug interactions: Beta blockers, ciprofloxacin, phenytoin, Features of toxicity: Initial CNS over activity then depression as lidocaine initially blocks, inhibitory pathways then blocks both inhibitory and activating pathways. Cardiac arrhythmias., Increased doses may be used when combined with adrenaline to limit systemic absorption., , Cocaine, , , , , , Pure cocaine is a salt, usually cocaine hydrochloride. It is supplied for local anaesthetic, purposes as a paste., It is supplied for clinical use in concentrations of 4 and 10%. It may be applied topically to the, nasal mucosa. It has a rapid onset of action and has the additional advantage of causing, marked vasoconstriction., It is lipophillic and will readily cross the blood brain barrier. Its systemic effects also include, cardiac arrhythmias and tachycardia., Apart from its limited use in ENT surgery it is otherwise used rarely in mainstream surgical, practice., , Bupivacaine, , , , , , Bupivacaine binds to the intracellular portion of sodium channels and blocks sodium influx, into nerve cells, which prevents depolarization., It has a much longer duration of action than lignocaine and this is of use in that it may be, used for topical wound infiltration at the conclusion of surgical procedures with long duration, analgesic effect., It is cardiotoxic and is therefore contra indicated in regional blockage in case the tourniquet, fails., Levobupivicaine (Chirocaine) is less cardiotoxic and causes less vasodilation.
Page 4016 :
Prilocaine, , , Similar mechanism of action to other local anaesthetic agents. However, it is far less, cardiotoxic and is therefore the agent of choice for intravenous regional anaesthesia e.g., Biers Block., , All local anaesthetic agents dissociate in tissues and this contributes to their therapeutic effect. The, dissociation constant shifts in tissues that are acidic e.g. where an abscess is present, and this, reduces the efficacy., Doses of local anaesthetics, , Agent, , Dose plain, , Dose with adrenaline, , Lignocaine, , 3mg/Kg, , 7mg/Kg, , Bupivacaine, , 2mg/Kg, , 2mg/Kg, , Prilocaine, , 6mg/Kg, , 9mg/Kg, , These are a guide only as actual doses depend on site of administration, tissue vascularity and comorbidities., Maximum total local anaesthetic doses, , , , , Lignocaine 1% plain - 3mg/ Kg - 200mg (20ml), Lignocaine 1% with 1 in 200,000 adrenaline - 7mg/Kg - 500mg (50ml), Bupivicaine 0.5% - 2mg/kg- 150mg (30ml), , Maximum doses are based on ideal body weight, Effects of adrenaline, Adrenaline may be added to local anaesthetic drugs. It prolongs the duration of action at the site of, injection and permits usage of higher doses (see above). It is contra indicated in patients taking, MAOI's or tricyclic antidepressants. The toxicity of bupivacaine is related to protein binding and, addition of adrenaline to this drug does not permit increases in the total dose of bupivacaine, in, contrast to the situation with lignocaine., References, An excellent review is provided by:, French J and Sharp L. Local Anaesthetics. Ann R Coll Surg Engl 2012; 94: 76-80., Next question
Page 4017 :
Theme: Acid - base disorders, , A., B., C., D., E., F., , Respiratory alkalosis, Type 1 respiratory failure, Type 2 respiratory failure, Metabolic alkalosis, Metabolic acidosis with normal anion gap, Metabolic acidosis with increased anion gap, , Please match the condition with the blood gas result. Each option may be used once more than, once or not at all., , 53., , pH 7.48, pO2 10.1, Bicarbonate 30, pCO2 4.5, Chloride<10meq, You answered Respiratory alkalosis, The correct answer is Metabolic alkalosis, This would be typical result of prolonged vomiting., , 54., , pH 7.49, pO2 8.5, pCO2 2.4, Bicarbonate 22, Chloride 12meq, Respiratory alkalosis, The hyperventilation results in decreased carbon dioxide levels, causing a respiratory, alkalosis (non compensated)., , 55., , pH 7.20, pO2 7.5, Bicarbonate 22, pCO2 8.1, Chloride 10, You answered Respiratory alkalosis, The correct answer is Type 2 respiratory failure, This is a sign of acute type 2 respiratory failure (non compensated). This is the result of, carbon dioxide retention., , Please rate this question:, , Discuss and give feedback, , Next question, , Disorders of acid - base balance
Page 4018 :
Disorders of acid- base balance are often covered in the MRCS part A, both in the SBA and EMQ, sections., The acid-base normogram below shows how the various disorders may be categorised, , Image sourced from Wikipedia, , Metabolic acidosis, , , , , This is the most common surgical acid - base disorder., Reduction in plasma bicarbonate levels., Two mechanisms:, , 1. Gain of strong acid (e.g. diabetic ketoacidosis), 2. Loss of base (e.g. from bowel in diarrhoea), - Classified according to the anion gap, this can be calculated by:, (Na+ + K+) - (Cl- + HCO3-)., - If a question supplies the chloride level then this is often a clue that the anion gap should be, calculated. The normal range = 10-18 mmol/L, Normal anion gap ( = hyperchloraemic metabolic acidosis), , , , , Gastrointestinal bicarbonate loss: diarrhoea, ureterosigmoidostomy, fistula, Renal tubular acidosis, Drugs: e.g. acetazolamide
Page 4019 :
, , , Ammonium chloride injection, Addison's disease, , Raised anion gap, , , , , , Lactate: shock, hypoxia, Ketones: diabetic ketoacidosis, alcohol, Urate: renal failure, Acid poisoning: salicylates, methanol, , Metabolic acidosis secondary to high lactate levels may be subdivided into two types:, , , , Lactic acidosis type A: (Perfusion disorders e.g.shock, hypoxia, burns), Lactic acidosis type B: (Metabolic e.g. metformin toxicity), , Metabolic alkalosis, , , , , Usually caused by a rise in plasma bicarbonate levels., Rise of bicarbonate above 24 mmol/L will typically result in renal excretion of excess, bicarbonate., Caused by a loss of hydrogen ions or a gain of bicarbonate. It is due mainly to problems of, the kidney or gastrointestinal tract, , Causes, , , , , , , , , , Vomiting / aspiration (e.g. Peptic ulcer leading to pyloric stenosis, nasogastric suction), Diuretics, Liquorice, carbenoxolone, Hypokalaemia, Primary hyperaldosteronism, Cushing's syndrome, Bartter's syndrome, Congenital adrenal hyperplasia, , Mechanism of metabolic alkalosis, , , , Activation of renin-angiotensin II-aldosterone (RAA) system is a key factor, Aldosterone causes reabsorption of Na+ in exchange for H+ in the distal convoluted tubule
Page 4020 :
, , , ECF depletion (vomiting, diuretics) → Na+ and Cl- loss → activation of RAA system → raised, aldosterone levels, In hypokalaemia, K+ shift from cells → ECF, alkalosis is caused by shift of H + into cells to, maintain neutrality, , Respiratory acidosis, , , , Rise in carbon dioxide levels usually as a result of alveolar hypoventilation, Renal compensation may occur leading to Compensated respiratory acidosis, , Causes, , , , , COPD, Decompensation in other respiratory conditions e.g. Life-threatening asthma / pulmonary, oedema, Sedative drugs: benzodiazepines, opiate overdose, , Respiratory alkalosis, , , , Hyperventilation resulting in excess loss of carbon dioxide, This will result in increasing pH, , Causes, , , , , , , Psychogenic: anxiety leading to hyperventilation, Hypoxia causing a subsequent hyperventilation: pulmonary embolism, high altitude, Early salicylate poisoning*, CNS stimulation: stroke, subarachnoid haemorrhage, encephalitis, Pregnancy, , *Salicylate overdose leads to a mixed respiratory alkalosis and metabolic acidosis. Early stimulation, of the respiratory centre leads to a respiratory alkalosis whilst later the direct acid effects of, salicylates (combined with acute renal failure) may lead to an acidosis, Next question
Page 4021 :
Theme: Intravenous fluids, , A., B., C., D., E., F., G., H., I., J., , Gelofusine, Dextran 70, 0.4%/0.18% dextrose saline, 5% dextrose, 1000ml 3% sodium chloride solution, Hartmann's solution, Pentastarch, Fluid restriction 500mls, Fluid restriction 1L, 0.9% sodium chloride with 40mmol potassium chloride per litre, , Which of the following is the best fluid management for the scenario given? Each option may be, used once, more than once or not at all., , 56., , A 53 year old alcoholic male presents with acute pancreatitis. He is clinically dehydrated., His blood results show normal renal function and electrolytes., You answered Gelofusine, The correct answer is Hartmann's solution, This patient needs fluid replacement due to large third space losses. Hartmann's solution is, recommended. N. Saline would put this patient at risk of hyperchloraemic acidosis., , 57., , A 45 year old man with previous laparotomy is admitted with adhesional small bowel, obstruction. He is managed with prolonged nasogastric drainage. His U+E's are as follows:, Sodium, , 129, , Potassium, , 3.4, , Urea, , 8.4, , Creatinine, , 89, , You answered Gelofusine, The correct answer is 0.9% sodium chloride with 40mmol potassium chloride per, litre, The potassium will decline further if this deficiency is not addressed. Remember that, potassium is predominantly an intracellular cation. U+E's measure the serum potassium
Page 4022 :
which is relatively buffered by the intra cellular stores. Therefore a fall in serum potassium, represents a very real intracellular deficiency. This requires supplementary potassium to, correct the defect., A 19 year old lady is admitted with pyelonephritis. She is in septic shock with a blood, pressure of 95/60 and pulse rate of 110. Apart from an allergy to corn she has no other, significant medical history., , 58., , You answered Gelofusine, The correct answer is Hartmann's solution, A 2012 Cochrane review concluded that colloids and crystalloids had the same effects on, outcome. Since crystalloids were more cost effective, these are now the preferred agents., Hypertonic saline (3% sodium chloride) is rarely used in clinical practice and almost never for the, purposes of volume replacement., Please rate this question:, , Discuss and give feedback, , Next question, , Pre operative fluid management, Fluid management has been described in the British Consensus guidelines on IV fluid, therapy for Adult Surgical patients (GIFTASUP) and by NICE (CG174 December 2013), The Recommendations include:, , , , , , , , , Use Ringer's lactate or Hartmann's when a crystalloid is needed for resuscitation or, replacement of fluids. Avoid 0.9% N. Saline (due to risk of hyperchloraemic acidosis) unless, patient vomiting or has gastric drainage., Use 4%/0.18% dextrose saline or 5% dextrose in maintenance fluids. It should not be used, in resuscitation or as replacement fluids., Adult maintenance fluid requirements are: Na 50-100 mmol/day and K 40-80 mmol/day in, 1.5-2.5L fluid per day., Patients for elective surgery should NOT be nil by mouth for >2 hours (unless has disorder of, gastric emptying)., Patients for elective surgery should be given carbohydrate rich drinks 2-3h before. Ideally, this should form part of a normal pre op plan to facilitate recovery., Avoid mechanical bowel preparation., If bowel prep is used, simultaneous administration of Hartmann's or Ringer's lactate should, be considered.
Page 4023 :
, , , , , , , , Excessive fluid losses from vomiting should be treated with a crystalloid with potassium, replacement. 0.9% N. Saline should be given if there is hypochloraemia. Otherwise, Hartmann's or Ringer lactate should be given for diarrhoea/ileostomy/ileus/obstruction., Hartmann's should also be given in sodium losses secondary to diuretics., High risk patients should receive fluids and inotropes., An attempt should be made to detect pre or operative hypovolaemia using flow based, measurements. If this is not available, then clinical evaluation is needed i.e. JVP, pulse, volume etc., In Blood loss or infection causing hypovolaemia should be treated with a balanced crystalloid, or colloid (or until blood available in blood loss). A critically ill patient is unable to excrete Na, or H20 leading to a 5% risk of interstitial oedema. Therefore 5% dextrose as well as colloid, should be given., If patients need IV fluid resuscitationn, use crystalloids that contain sodium in the range 130154 mmol/l, with a bolus of 500 ml over less than 15 minutes (NICE Guidance CG 174)., Next question
Page 4024 :
Theme: Thromboprophylaxis, , A., B., C., D., E., F., G., H., I., J., , Oral dabigatran alone, Oral dabigatran with compression stockings, Low molecular weight heparin and compression stockings, Warfarin, Low molecular weight heparin and pneumatic compression stockings, Low molecular weight heparin alone, No thromboprophylaxis, Unfractionated heparin and compression stockings, Unfractionated heparin alone, Unfractionated heparin and pneumatic compression stockings, , Please select the most appropriate thromboprophylactic regime in the surgical scenarios described, below. Each regime may be used once, more than once or not at all., , 59., , A 30 year old male is admitted electively for a right inguinal hernia repair under local, anaesthesia. He is otherwise well but his grandfather died from a pulmonary embolism., You answered Oral dabigatran alone, The correct answer is No thromboprophylaxis, Inguinal hernia repairs under local anaesthetic have a short operative time and patients are, usually ambulant immediately afterwards. His family history is unlikely to be significant, and he is at very low risk., , 60., , A 5 year old boy undergoes a closure of a loop colostomy., You answered Oral dabigatran alone, The correct answer is No thromboprophylaxis, In paediatric surgical practice the use of heparin type agents is rare. This is because, even, with abdominal surgery, children are ambulant soon after surgery and DVT's vanishingly, rare in this population., , 61., , An 83 year old man is admitted for an abdomino-perineal excision of the colon and rectum, for a distal rectal tumour. His co-mobidities include diabetes and intermittent claudication., His renal function is normal., You answered Oral dabigatran alone
Page 4025 :
The correct answer is Low molecular weight heparin and pneumatic compression, stockings, Pelvic cancer surgery carries a very high risk of development of deep vein thrombosis. In a, patient with normal renal function the use of a low molecular weight heparin is standard., However, many surgeons would only use this in the post operative setting. Intermittent, compression devices in claudicants are not without risk, but on balance probably outweigh, the risk of DVT in this specific case. The perfusion of the feet should be closely monitored, and compression stopped if concerns develop., Please rate this question:, , Discuss and give feedback, , Next question, , Thromboprophylaxis in surgical patients, Deep vein thrombosis may develop insidiously in many surgical patients. Untreated it may progress, to result in pulmonary embolism., The following surgical patients are at increased risk of deep vein thrombosis:, , , , , , , , , , , , Surgery greater than 90 minutes at any site or greater than 60 minutes if the procedure, involves the lower limbs or pelvis, Acute admissions with inflammatory process involving the abdominal cavity, Expected significant reduction in mobility, Age over 60 years, Known malignancy, Thrombophilia, Previous thrombosis, BMI >30, Taking hormone replacement therapy or the contraceptive pill, Varicose veins with phlebitis, , Mechanical thromboprophylaxis, , , , , , Early ambulation after surgery is cheap and is effective, Compression stockings (contra -indicated in peripheral arterial disease), Intermittent pneumatic compression devices, Foot impulse devices, , Therapeutic agents
Page 4026 :
Agent, , Mode of action, , Uses, , Low molecular, weight heparin, , Binds antithrombin, causing inhibition, of factor Xa, , Thromboprophylaxis or treatment of thromboembolic, events in those with normal renal function. It is given as, once daily subcutaneous injection, , Unfractionated, heparin, , Binds antithrombin, III affecting, thrombin and factor, Xa, , Effective anticoagulation, administered intravenously it, has a rapid onset and its therapeutic effects decline, quickly on stopping and infusion. Its activity is, measured using the APTT. If need be it can be reversed, using protamine sulphate, , Dabigatran, , Orally administered, direct thrombin, inhibitor, , Used prophylaxis in hip and knee surgery. It does not, require therapeutic monitoring. It has no known antidote, and should not be used in any patient in whom there is a, risk of active bleeding or imminent likelihood of, surgery, Next question
Page 4027 :
Theme: Management of complications, , A., B., C., D., E., F., G., H., I., , Gastrograffin contrast enema, Barium enema, Oral gastrograffin and CT, Barium meal, Ultrasound of the thorax, Endoanal ultrasound, Anorectal physiology studies, Biofeedback, Abdominal CT scan with IV contrast, , Please select the most appropriate intervention from the list given. Each option may be used once,, more than once or not at all., , 62., , A 65 year old male with carcinoma of the oesophagus undergoes endoscopic dilatation., Following which he develops pleuritic chest pain and sub cutaneous emphysema., You answered Gastrograffin contrast enema, The correct answer is Oral gastrograffin and CT, This is consistent with oesophageal perforation. Gastrograffin and CT will accurately, delineate the site of perforation and guide further therapy. Barium may produce a, mediastinitis and should not be used., , 63., , A frail 73 year old lady is admitted with intractable faecal incontinence. She undergoes a, laparoscopic defunctioning of the rectum with an end colostomy. 48 hours later her stoma, has still not worked and her abdomen is distended and painful., Gastrograffin contrast enema, Occasionally the wrong end of bowel is brought up and fashioned as the end stoma,, effectively leaving the bowel obstructed. A gastrograffin enema will easily demonstrate if, this is the case., , 64., , A 43 year old man develops fast atrial fibrillation 5 days following a low anterior resection, of the rectum for cancer. On examination he has lower abdominal tenderness and a WCC, 19., You answered Gastrograffin contrast enema, The correct answer is Abdominal CT scan with IV contrast
Page 4028 :
An anastomotic leak is the most likely occurrence and may be visualised using CT, scanning. A gastrograffin enema may demonstrate the leak but a CT scan will also provide, information to guide management., Please rate this question:, , Discuss and give feedback, , Next question, , Surgical complications, Complications occur in all branches of surgery and require vigilance in their detection. In many, cases anticipating the likely complications and appropriate avoidance will minimise their occurrence., For the purposes of the MRCS the important principles to appreciate are:, , , , , , , The anatomical principles that underpin complications, The physiological and biochemical derangements that occur, The most appropriate diagnostic modalities to utilise, The principles which underpin their management, , This is clearly a very broad area and impossible to cover comprehensively. There is considerable, overlap with other topic areas within the website., Avoiding complications, Some points to hopefully avert complications:, , , , , , , , , , , , World Health Organisation checklist- now mandatory prior to all operations, Prophylactic antibiotics - right dose, right drug, right time., Assess DVT/ PE risk and ensure adequate prophylaxis, MARK site of surgery, Use tourniquets with caution and with respect for underlying structures, Remember the danger of end arteries and in situations where they occur avoid using, adrenaline containing solutions and monopolar diathermy., Handle tissues with care- devitalised tissue serves as a nidus for infection, Be very wary of the potential for coupling injuries when using diathermy during laparoscopic, surgery, The inferior epigastric artery is a favorite target for laparoscopic ports and surgical drains!, , Anatomical principles
Page 4029 :
Understanding the anatomy of a surgical field will allow appreciation of local and systemic, complications that may occur. For example, nerve injuries may occur following surgery in specific, regions. The table below lists some of the more important nerves to consider and mechanisms of, injury, , Nerve, , Mechanism, , Accessory, , Posterior triangle lymph node biopsy, , Sciatic, , Posterior approach to hip, , Common peroneal, , Legs in Lloyd Davies position, , Long thoracic, , Axillary node clearance, , Pelvic autonomic nerves, , Pelvic cancer surgery, , Recurrent laryngeal nerves, , During thyroid surgery, , Hypoglossal nerve, , During carotid endarterectomy, , Ulnar and median nerves, , During upper limb fracture repairs, , These are just a few. The detailed functional sequelae are particularly important and will often be, tested. In addition to nerve injuries certain procedures carry risks of visceral or structural injury., Again some particular favorites are given below:, , Structure, , Mechanism, , Thoracic duct, , During thoracic surgery e.g. Pneumonectomy, oesphagectomy, , Parathyroid glands, , During difficult thyroid surgery
Page 4030 :
Structure, , Mechanism, , Ureters, , During colonic resections/ gynaecological surgery, , Bowel perforation, , Use of Verres Needle to establish pneumoperitoneum, , Bile duct injury, , Failure to delineate Calots triangle carefully and careless use of diathermy, , Facial nerve, , Always at risk during Parotidectomy, , Tail of pancreas, , When ligating splenic hilum, , Testicular vessels, , During re-do open hernia surgery, , Hepatic veins, , During liver mobilisation, , Again many could be predicted from the anatomy of the procedure., Physiological derangements, A very common complication is bleeding and this is covered under the section of haemorrhagic, shock. Another variant is infection either superficial or deep seated. The organisms are covered, under microbiology and the features of sepsis covered under shock. Do not forget that, immunocompromised and elderly patients may present will atypical physiological parameters., Selected physiological and biochemical issues are given below:, , Complication, , Physiological/ Biochemical Problem, , Arrhythmias following, cardiac surgery, , Susceptibility to hypokalaemia (K+ <4.0 in cardiac patients), , Neurosurgical electrolyte, disturbance, , SIADH following cranial surgery causing hyponatraemia
Page 4031 :
Complication, , Physiological/ Biochemical Problem, , Ileus following, gastrointestinal surgery, , Fluid sequestration and loss of electrolytes, , Pulmonary oedema following, pneumonectomy, , Loss of lung volume makes these patients very sensitive to fluid, overload, , Anastamotic leak, , Generalised sepsis causing mediastinitis or peritonitis depending, on site of leak, , Myocardial infarct, , May follow any type of surgery and in addition to direct cardiac, effects the decreased cardiac output may well compromise grafts, etc., , Try making a short list of problems and causes specific to your own clinical area., Diagnostic modalities, Depends largely on the suspected complication. In the acutely unwell surgical patient the following, baseline investigations are often helpful:, , , , , , , Full blood count, urea and electrolytes, C- reactive protein (trend rather than absolute value),, serum calcium, liver function tests, clotting (don't forget to repeat if on-going bleeding), Arterial blood gases, ECG (+cardiac enzymes if MI suspected), Chest x-ray to identify collapse/ consolidation, Urine analysis for UTI, , These will often identify the most common complications., Special tests, , , , , , , CT scanning for identification of intra-abdominal abscesses, air and if luminal contrast is, used an anastomotic leak, Doppler USS of leg veins- for identification of DVT, CTPA for PE, Sending peritoneal fluid for U+E (if ureteric injury suspected) or amylase (if pancreatic injury, suspected), Echocardiogram if pericardial effusion suspected post cardiac surgery and no pleural window, made.
Page 4032 :
Management of complications, The guiding principal should be safe and timely intervention. Patients should be stabilised and if an, operation needs to occur in tandem with resuscitation then generally this should be of a damage, limitation type procedure rather than definitive surgery (which can be more safely undertaken in a, stable patient the following day)., Remember that recent surgery is a contra indication to thrombolysis and that in some patients IV, heparin may be preferable to a low molecular weight heparin (easier to reverse)., As a general rule laparotomies for bleeding should follow the core principle of quadrant packing and, then subsequent pack removal rather than plunging large clamps into pools of blood. The latter, approach invariable worsens the situation is often accompanied by significant visceral injury, particularly when done by the inexperienced. If packing controls a situation it is entirely acceptable, practice to leave packs in situ and return the patient to ITU for pack removal the subsequent day., Next question
Page 4033 :
A 63 year old man is recovering following an open extended right hemicolectomy for carcinoma of, the colonic splenic flexure. Two days post operatively he develops a persistent pyrexia. What is the, least likely cause?, , Ileus, , Atelectasis, , Anastomotic leak, , Wound infection, , Urinary tract infection, , An ileus in itself is seldom a cause of a pyrexia. It may serve as a proxy marker of other, complications. In this scenario atelectasis would be the most likely underlying cause, as open, extended right hemicolectomies will necessitate a long midline incision. Anastomotic leaks are less, common after right sided colonic surgery and the timeframe for it is rather short (but are possible)., Both wound infections and UTI's ,may complicate major abdominal surgery at any stage. We remind, you to check the wording of the question, it asks for the "least likely" cause of pyrexia., Please rate this question:, , Discuss and give feedback, , Next question, , Pyrexia- post operative, Many surgical patients will develop a pyrexia post operatively. The cause and investigation depends, upon the nature of the infection., The following scenarios may account for post operative pyrexia:, , Cause, , Features, , Anastomotic leak, , , , , , , Swinging pyrexia, Ileus, Increasing abdominal pain, Raised inflammatory markers, , Wound infection, , , , Evidence of superficial erythema, discharge of pus or increasing
Page 4034 :
, , , , pain, Usually mild pyrexia (unless major or deep seated wound infection), May be accompanied by evidence of wound dehisence, Inflammatory markers raised, , Atelectasis, , , , , , , , Usually complicates abdominal surgery, Most common after midline laparotomies (pain impairs ventilation), Pyrexia usually mild and non swinging, Most patients will have chest signs on examination, Inflammatory markers raised, , Central line sepsis, , , , , , , Patients with complex venous access, May have marked pyrexia, Access site may show evidence of erythema, Diagnosis is by blood culture from line, line removal and subsequent, tip culture, Groin lines and those for TPN have the highest risk, Inflammatory markers raised, , , , , Urinary tract, infection, , , , , , , Common in surgical patients, Usually occur in patients with indwelling urinary catheters, Diagnosis is by dipstick and CSU and signs of raised inflammatory, markers, Treatment is with antibiotics (to cover hospital acquired organisms), Next question
Page 4035 :
A 72 year old man is due to undergo an oesophagectomy for malignancy. His BMI is 17.5. What is, the best feeding regime immediately following surgery?, , Total parenteral nutrition., , Feeding jejunostomy., , Feeding duodenostomy., , Liquid diet orally., , Soft solids orally., , Theme from April 2012 Exam, This patient has a condition causing poor absorption, loss of nutrients and high metabolism. Enteral, feeds should be used where possible and many surgeons will site a jejunostomy for this purpose., Oral diet is not permitted following a resection until the anastamosis has had time to heal., Please rate this question:, , Discuss and give feedback, , Next question, , Enteral Feeding, , , , , , , , , , , , Identify patients as malnourished or at risk (see below), Identify unsafe or inadequate oral intake with functional GI tract, Consider for enteral feeding, Gastric feeding unless upper GI dysfunction (then for duodenal or jejunal tube), Check NG placement using aspiration and pH (check post pyloric tubes with AXR), Gastric feeding > 4 weeks consider long-term gastrostomy, Consider bolus or continuous feeding into the stomach, ITU patients should have continuous feeding for 16-24h (24h if on insulin), Consider motility agent in ITU or acute patients for delayed gastric emptying. If this doesn't, work then try post pyloric feeding or parenteral feeding., PEG can be used 4 hours after insertion, but should not be removed until >2 weeks after, insertion., , Surgical patients due to have major abdominal surgery: if malnourished, unsafe swallow/inadequate, oral intake and functional GI tract then consider pre operative enteral feeding.
Page 4036 :
Patients identified as being malnourished, , , , , BMI < 18.5 kg/m2, unintentional weight loss of > 10% over 3-6/12, BMI < 20 kg/m 2 and unintentional weight loss of > 5% over 3-6/12, , AT RISK of malnutrition, , , , , , Eaten nothing or little > 5 days, who are likely to eat little for a further 5 days, Poor absorptive capacity, High nutrient losses, High metabolism, , Reference, Stroud M et al. Guidelines for enteral feeding in adult hospital patients. Gut 2003; 52(Suppl VII):vii1 vii12., Next question
Page 4037 :
A 38 year old lady presents with abdominal pain. On investigation, her serum calcium is found to be, 3.5mmol/L. What is the most appropriate initial management?, , Intravenous bisphosphonates, , Oral bisphosphonates, , Intravenous calcitonin, , Intravenous 0.9% sodium chloride, , Intravenous frusemide, , The immediate treatment of hypercalcaemia involves intravenous fluid resuscitation. This may be, complemented with the use of bisphosphonates and sometimes diuretics. However, fluids are, administered first and because this question asks what the most appropriate initial treatment is,, intravenous fluids are the most appropriate answer. Normal saline is usually preferred for this over, dextrose containing solutions., Please rate this question:, , Discuss and give feedback, , Next question, , Management of hypercalcaemia, , , , , Free Ca is affected by pH (increased in acidosis) and plasma albumin concentration, ECG changes include: Shortening of QTc interval, Urgent management is indicated if:, , Calcium > 3.5 mmol/l, Reduced consciousness, Severe abdominal pain, Pre renal failure, , Management:
Page 4038 :
, , , , , Airway Breathing Circulation, Intravenous fluid resuscitation with 3-6L of 0.9% Normal saline in 24 hours, Concurrent administration of calcitonin will also help lower calcium levels, Medical therapy (usually if Corrected calcium >3.0mmol/l), , Bisphosphonates, , , , , Analogues of pryrophosphate, Prevent osteoclast attachment to bone matrix and interfere with osteoclast activity, Inhibit bone resorption., , Agents, Drug, , Side effects, , Notes, , IV Pamidronate, , pyrexia, leucopaenia, , Most potent agent, , IV Zoledronate, , response lasts 30 days, , Used for malignancy associated hypercalcaemia, , Calcitonin, , , Quickest onset of action however short duration (tachyphylaxis) therefore only given with a, second agent., , Prednisolone, , , May be given in hypercalcaemia related to sarcoidosis, myeloma or vitamin D intoxication., Next question
Page 4039 :
Theme: Bowel preparation, , A., B., C., D., E., F., G., , No preparation required, Phosphate enema, Bowel preparation with oral laxatives (e.g. picolax), Senokot tablets, Oral pergolide, Rectal lavage with saline, 60 ml oral lactulose, , Please select the most appropriate form of bowel preparation for the procedures given. Each agent, may be selected once, more than once or not at all., , 68., , A 56 year old man with a change in bowel habit requires a colonoscopy., You answered No preparation required, The correct answer is Bowel preparation with oral laxatives (e.g. picolax), Endoscopy requires full bowel preparation. In elderly patients, this can cause electrolyte, disturbance and renal compromise and it is important to check the patients urea and, electrolytes beforehand., , 69., , A 44 year old man with carcinoma of the hepatic flexure requires a right hemicolectomy., No preparation required, Formal bowel preparation for right sided colonic resection is unnecessary. The formal, bowel preparation of elective patients for right sided resection results in increased post, operative morbidity and delayed discharge., , 70., , A 34 year old man with rectal bleeding requires a flexible sigmoidoscopy., You answered No preparation required, The correct answer is Phosphate enema, For a limited endoscopy a simple enema will suffice. ., , Please rate this question:, , Discuss and give feedback
Page 4040 :
Next question, , Preparation for surgery, Elective and emergency patients require different preparation., Elective cases, , , , , , , , Consider pre admission clinic to address medical issues., Blood tests including FBC, U+E, LFT's, Clotting, Group and Save, Urine analysis, Pregnancy test, Sickle cell test, ECG/ Chest x-ray, , Exact tests to be performed will depend upon the proposed procedure and patient fitness., Risk factors for development of deep vein thrombosis should be assessed and a plan for, thromboprophylaxis formulated., Diabetes, Diabetic patients have greater risk of complications., Poorly controlled diabetes carries high risk of wound infections., Patients with diet or tablet controlled diabetes may be managed using a policy of omitting medication, and checking blood glucose levels regularly. Diabetics who are poorly controlled or who take insulin, will require a intravenous sliding scale. Potassium supplementation should also be given., Diabetic cases should be operated on first., Emergency cases, Stabilise and resuscitate where needed., Consider whether antibiotics are needed and when and how they should be administered., Inform blood bank if major procedures planned particularly where coagulopathies are present at the, outset or anticipated (e.g. Ruptured AAA repair), Don't forget to consent and inform relatives., Special preparation, Some procedures require special preparation:, , , , , , , , , , Thyroid surgery; vocal cord check., Parathyroid surgery; consider methylene blue to identify gland., Sentinel node biopsy; radioactive marker/ patent blue dye., Surgery involving the thoracic duct; consider administration of cream., Pheochromocytoma surgery; will need alpha and beta blockade., Surgery for carcinoid tumours; will need covering with octreotide., Colorectal cases; bowel preparation (especially left sided surgery), Thyrotoxicosis; lugols iodine/ medical therapy.
Page 4041 :
The following are contra indications to the use of lignocaine for local anaesthesia except:, , Accelerated idioventricular rhythm, , Current treatment with flecainide, , 3rd degree heart block without pacemaker, , Severe sino atrial block, , Protein C deficiency, , Lignocaine is widely used as a local anaesthetic. As a class IB antiarrhythmic it should not be used, in people with unstable disorders of cardiac rhythm and ideally should not be co-administered with, other anti-arhythmics., Please rate this question:, , Discuss and give feedback, , Next question, , Local anaesthetic agents, Lidocaine, , , , , , , , , An amide, Local anaesthetic and a less commonly used antiarrhythmic (affects Na channels in the, axon), Hepatic metabolism, protein bound, renally excreted, Toxicity: due to IV or excess administration. Increased risk if liver dysfunction or low protein, states. Note acidosis causes lidocaine to detach from protein binding., Drug interactions: Beta blockers, ciprofloxacin, phenytoin, Features of toxicity: Initial CNS over activity then depression as lidocaine initially blocks, inhibitory pathways then blocks both inhibitory and activating pathways. Cardiac arrhythmias., Increased doses may be used when combined with adrenaline to limit systemic absorption., , Cocaine, , , Pure cocaine is a salt, usually cocaine hydrochloride. It is supplied for local anaesthetic, purposes as a paste.
Page 4042 :
, , , , It is supplied for clinical use in concentrations of 4 and 10%. It may be applied topically to the, nasal mucosa. It has a rapid onset of action and has the additional advantage of causing, marked vasoconstriction., It is lipophillic and will readily cross the blood brain barrier. Its systemic effects also include, cardiac arrhythmias and tachycardia., Apart from its limited use in ENT surgery it is otherwise used rarely in mainstream surgical, practice., , Bupivacaine, , , , , , Bupivacaine binds to the intracellular portion of sodium channels and blocks sodium influx, into nerve cells, which prevents depolarization., It has a much longer duration of action than lignocaine and this is of use in that it may be, used for topical wound infiltration at the conclusion of surgical procedures with long duration, analgesic effect., It is cardiotoxic and is therefore contra indicated in regional blockage in case the tourniquet, fails., Levobupivicaine (Chirocaine) is less cardiotoxic and causes less vasodilation., , Prilocaine, , , Similar mechanism of action to other local anaesthetic agents. However, it is far less, cardiotoxic and is therefore the agent of choice for intravenous regional anaesthesia e.g., Biers Block., , All local anaesthetic agents dissociate in tissues and this contributes to their therapeutic effect. The, dissociation constant shifts in tissues that are acidic e.g. where an abscess is present, and this, reduces the efficacy., Doses of local anaesthetics, , Agent, , Dose plain, , Dose with adrenaline, , Lignocaine, , 3mg/Kg, , 7mg/Kg, , Bupivacaine, , 2mg/Kg, , 2mg/Kg, , Prilocaine, , 6mg/Kg, , 9mg/Kg, , These are a guide only as actual doses depend on site of administration, tissue vascularity and comorbidities.
Page 4043 :
Maximum total local anaesthetic doses, , , , , Lignocaine 1% plain - 3mg/ Kg - 200mg (20ml), Lignocaine 1% with 1 in 200,000 adrenaline - 7mg/Kg - 500mg (50ml), Bupivicaine 0.5% - 2mg/kg- 150mg (30ml), , Maximum doses are based on ideal body weight, Effects of adrenaline, Adrenaline may be added to local anaesthetic drugs. It prolongs the duration of action at the site of, injection and permits usage of higher doses (see above). It is contra indicated in patients taking, MAOI's or tricyclic antidepressants. The toxicity of bupivacaine is related to protein binding and, addition of adrenaline to this drug does not permit increases in the total dose of bupivacaine, in, contrast to the situation with lignocaine., References, An excellent review is provided by:, French J and Sharp L. Local Anaesthetics. Ann R Coll Surg Engl 2012; 94: 76-80., Next question
Page 4044 :
A 43 year old lady has undergone a total thyroidectomy for multinodular goitre. You are called to see, her because of respiratory distress. On examination she has a marked stridor, her wound seems, healthy but there is a swelling within the operative site. What is the most likely explanation for this, problem?, , Bilateral superior laryngeal nerve injury, , Hypocalcaemic tetany, , Anxiety, , Contained haematoma, , Unilateral recurrent laryngeal nerve injury, , In this setting a contained haematoma is the most likely cause. This will impair venous return, resulting in laryngeal oedema and respiratory compromise., Please rate this question:, , Discuss and give feedback, , Next question, , Thyroid disease, Patients may present with a number of different manifestations of thyroid disease. They can be, broadly sub classified according to whether they are euthyroid or have clinical signs of thyroid, dysfunction. In addition it needs to be established whether they have a mass or not., Assessment, , , , , , History, Examination including USS, If a nodule is identified then it should be sampled ideally via an image guided fine needle, aspiration, Radionucleotide scanning is of limited use, , Thyroid Tumours, , , Papillary carcinoma
Page 4045 :
, , , , , Follicular carcinoma, Anaplastic carcinoma, Medullary carcinoma, Lymphoma's, , Multinodular goitre, , , , , , One of the most common reasons for presentation, Provided the patient is euthyroid and asymptomatic and no discrete nodules are seen, they, can be reassured., In those with compressive symptoms surgery is required and the best operation is a total, thyroidectomy., Sub total resections were practised in the past and simply result in recurrent disease that, requires a difficult revisional resection., , Endocrine dysfunction, , , , , In general these patients are managed by physicians initially., Surgery may be offered alongside radio iodine for patients with Graves disease that fails with, medical management or in patients who would prefer not to be irradiated (e.g. pregnant, women)., Patients with hypothyroidism do not generally get offered a thyroidectomy. Sometimes, people inadvertently get offered resections during the early phase of Hashimotos thyroiditis,, however, with time the toxic phase passes and patients can simply be managed with, thyroxine., , Complications following surgery, , , , , Anatomical such as recurrent laryngeal nerve damage., Bleeding. Owing to the confined space haematoma's may rapidly lead to respiratory, compromise owing to laryngeal oedema., Damage to the parathyroid glands resulting in hypocalcaemia., , Further sources of information, 1. http://www.acb.org.uk/docs/TFTguidelinefinal.pdf- Association of Clinical Biochemistry guidelines, for thyroid function tests., 2. British association of endocrine surgeons website- http://www.baets.org.uk, Next question
Page 4046 :
Which of the following drugs is not positively inotropic?, , Dopamine, , Glucagon, , Theophylline, , Sodium thiopentone, , Dobutamine, , Inotropes are a class of drugs that increase the force or cardiac contractility. This may improve, cardiac output. Increased blood pressure may have direct beneficial effects for the heart in that it, improves myocardial perfusion pressure. Dopamine and dobutamine are both commonly used, inotropes, they should be administered via a central line and in a monitored setting. Glucagon and, theophylline are also positive inotropes (although not commonly used for this purpose). In contrast, sodium thiopentone causes marked myocardial depression., Please rate this question:, , Discuss and give feedback, , Next question, , Inotropes and cardiovascular receptors, Inotropes are a class of drugs which work primarily by increasing cardiac output. They should be, distinguished from vasoconstrictor drugs which are used specifically when the primary problem is, peripheral vasodilatation., Catecholamine type agents are commonly used and work by increasing cAMP levels by adenylate, cyclase stimulation. This in turn intracellular calcium ion mobilisation and thus the force of, contraction. Adrenaline works as a beta adrenergic receptor agonist at lower doses and an alpha, receptor agonist at higher doses. Dopamine causes dopamine receptor mediated renal and
Page 4047 :
mesenteric vascular dilatation and beta 1 receptor agonism at higher doses. This results in, increased cardiac output. Since both heart rate and blood pressure are raised, there is less overall, myocardial ischaemia. Dobutamine is a predominantly beta 1 receptor agonist with weak beta 2 and, alpha receptor agonist properties. Noradrenaline is a catecholamine type agent and predominantly, acts as an alpha receptor agonist and serves as a peripheral vasoconstrictor., Phosphodiesterase inhibitors such as milrinone act specifically on the cardiac phosphodiesterase, and increase cardiac output., , Inotrope, , Cardiovascular receptor action, , Adrenaline, , α-1, α-2, β-1, β-2, , Noradrenaline, , α-1,( α-2), (β-1), (β-2), , Dobutamine, , β-1, (β 2), , Dopamine, , (α-1), (α-2), (β-1), D-1,D-2, , Minor receptor effects in brackets, Effects of receptor binding, , α-1, α-2, , vasoconstriction, , β-1, , increased cardiac contractility and HR, , β-2, , vasodilatation, , D-1, , renal and spleen vasodilatation, , D-2, , inhibits release of noradrenaline, Next question
Page 4048 :
A 28 year old man undergoes a laparotomy for perforated duodenal ulcer and broad spectrum, antibiotics are administered. Post operatively he has hearing impairment. Which of the following, agents is the most likely underlying culprit?, , Gentamicin, , Ciprofloxacin, , Metronidazole, , Ampicillin, , Co-trimoxazole, , Ototoxicity is a recognised adverse reaction with the aminoglycoside antibiotics., Please rate this question:, , Discuss and give feedback, , Next question, , Antibiotics: mechanism of action, The lists below summarise the site of action of the commonly used antibiotics, Inhibit cell wall formation, , , , penicillins, cephalosporins, , Inhibit protein synthesis, , , , , , , aminoglycosides (cause misreading of mRNA), chloramphenicol, macrolides (e.g. erythromycin), tetracyclines, fusidic acid
Page 4050 :
A 62 year old lawyer has a transurethral resection of the prostate which took 1 hour to perform. The, ST2 contacts you as the patient has become agitated. He has a HR 105 bpm and his blood pressure, is 170/100 mmHg. He is fluid overloaded. His blood results reveal a Na of 120mmol/l. What is the, most likely cause?, , Over administration of 0.9% Normal Saline, , Syndrome of inappropriate antidiuretic hormone secretion, , Congestive cardiac failure, , TUR syndrome, , Acute renal failure, Complications of Transurethral Resection: TURP, T ur syndrome, U rethral stricture/UTI, R etrograde ejaculation, P erforation of the prostate, , TUR syndrome occurs when irrigation fluid enters the systemic circulation. The triad of features are:, 1. Hyponatraemia: dilutional, 2. Fluid overload, 3. Glycine toxicity, Management involves fluid restriction and the treatment of the complications associated with the, hyponatraemia., Please rate this question:, , Discuss and give feedback
Page 4051 :
Post prostatectomy syndromes, Transurethral prostatectomy is a common and popular treatment for benign prostatic hyperplasia., The procedure involves insertion of a resectoscope via the penile urethra. The bladder and prostate, are irrigated and strips of prostatic tissue removed using diathermy., , Indications for surgery in patients with BPH, Refractory urinary retention, Recurrent urinary tract infections due to prostatic hypertrophy, Recurrent gross haematuria, Renal insufficiency secondary to bladder outlet obstruction, Permanently damaged or weakened bladders, Large bladder diverticula that do not empty well secondary to an enlarged prostate, , Complications include haemorrhage, urosepsis, retrograde ejaculation and electrolyte disturbances, from the irrigation fluids used during surgery., , Risk factors for increased morbidity following TURP, Glands >45g, Operating time > 90 minutes, Acute urinary retention as presenting feature
Page 4052 :
A 44 year old man undergoes a distal gastrectomy for cancer. He is slightly anaemic and therefore, receives a transfusion of 4 units of packed red cells to cover both the existing anaemia and, associated perioperative blood loss. He is noted to develop ECG changes that are not consistent, with ischaemia. What is the most likely cause?, , Hyponatraemia, , Hyperkalaemia, , Hypercalcaemia, , Metabolic alkalosis, , Hypernatraemia, , The transfusion of packed red cells has been shown to increase serum potassium levels. The risk is, higher with large volume transfusions and with old blood., Please rate this question:, , Discuss and give feedback, , Next question, , Blood transfusion reactions, Acute transfusion reactions present as adverse signs or symptoms during or within 24 hours of a, blood transfusion. The most frequent reactions are fever, chills, pruritus, or urticaria, which typically, resolve promptly without specific treatment or complications. Other signs occurring in temporal, relationship with a blood transfusion, such as severe dyspnoea, pyrexia, or loss of consciousness, may be the first indication of a more severe potentially fatal reaction., The causes of adverse reactions are multi-factorial. Immune mediated reactions, some of the most, feared, occur as a result of component mismatch, the commonest cause of which is clerical error., More common, non immune mediated, complications may occur as a result of product, contamination, this may be bacterial or viral., Transfusion related lung injury is well recognised and there are two proposed mechanisms which, underpin this. One involves the sequestration of primed neutrophils within the recipient pulmonary, capillary bed. The other proposed mechanism suggests that HLA mismatches between donor, neutrophils and recipient lung tissue is to blame., The table below summarises the main types of transfusion reaction., , Immune mediated, , Non immune mediated
Page 4054 :
Which of the following muscle relaxants will tend to incite neuromuscular excitability following, administration?, , Atracurium, , Suxamethonium, , Vecuronium, , Pancuronium, , None of the above, , Suxamethonium may induce generalised muscular contractions following administration. This may, raise serum potassium levels., Please rate this question:, , Discuss and give feedback, , Next question, , Muscle relaxants, Suxamethonium, , , , , , , , , Depolarising neuromuscular blocker, Inhibits action of acetylcholine at the neuromuscular junction, Degraded by plasma cholinesterase and acetylcholinesterase (affected by lack, of acetylcholinesterase), Fastest onset and shortest duration of action of all muscle relaxants, Produces generalised muscular contraction prior to paralysis, Adverse effects include hyperkalaemia, malignant hyperthermia, delayed, recovery
Page 4055 :
, , , , , , Non depolarising neuromuscular blocking drug, Duration of action usually 30-45 minutes, Generalised histamine release on administration may produce facial flushing,, tachycardia and hypotension, Not excreted by liver or kidney, broken down in tissues by hydrolysis, Reversed by neostigmine, , Vecuronium, , , , , , , Non depolarising neuromuscular blocking drug, Duration of action approximately 30 - 40 minutes, Degraded by liver and kidney and effects prolonged in organ dysfunction, Effects may be reversed by neostigmine, , Pancuronium, , , , , , , Non depolarising neuromuscular blocker, Onset of action approximately 2-3 minutes, Duration of action up to 2 hours, Effects may be partially reversed with drugs such as neostigmine, , Atracurium, , Next question
Page 4056 :
A 23 year old man is recovering from an appendicectomy. The operation was complicated by the, presence of perforation. He is now recovering on the ward. However, his urine output is falling and, he has been vomiting. Which of the following intravenous fluids should be initially administered,, pending analysis of his urea and electrolyte levels?, , Hartmans solution, , Dextran 70, , Pentastarch, , Gelofusin, , 5% Dextrose, , Theme from January 2011 Exam, He will have sequestration of electrolyte rich fluids in the abdomen and gut lumen. These are best, replaced by use of Hartmans solution in the first instance., Please rate this question:, , Discuss and give feedback, , Next question, , Post operative fluid management, Composition of commonly used intravenous fluids mmol-1, , Na, , K, , Cl, , Bicarbonate, , Lactate, , Plasma, , 137-147, , 4-5.5, , 95-105, , 22-25, , -, , 0.9% Saline, , 153, , -, , 153, , -, , -, , Dextrose / saline, , 30.6, , -, , 30.6, , -, , -
Page 4057 :
Hartmans, , 130, , 4, , 110, , -, , 28, , Post operative fluid management, In the UK the GIFTASUP and NICE (CG174 2013) guidelines (see reference below) were devised to, try and provide some consensus guidance as to how intravenous fluids should be administered. A, decade ago it was a commonly held belief that little harm would occur as a result of excessive, administration of normal saline and many oliguric post operative patients received enormous, quantities of IV fluids. As a result they developed hyperchloraemic acidosis. With greater, understanding of this potential complication, the use of electrolyte balanced solutions (Ringers, lactate/ Hartmans) is now favored over normal saline., The other guidance includes:, , , , , , , , Fluids given should be documented clearly and easily available, Assess the patient's fluid status when they leave theatre, If a patient is haemodynamically stable and euvolaemic, aim to restart oral fluid intake as, soon as possible, Review patients whose urinary sodium is < 20, If a patient is oedematous, hypovolaemia if present should be treated first. This should then, be followed by a negative balance of sodium and water, monitored using urine Na excretion, levels, Solutions such as Dextran 70 should be used in caution in patients with sepsis as there is a, risk of developing acute renal injury, , References, NICE guidance CG174. Intravenous fluid therapy in adults. December 2013., British Consensus Guidelines on Intravenous Fluid Therapy for Adult Surgical Patients. GIFTASUP, (2009), Next question
Page 4058 :
A 73 year old man develops disseminated intravascular coagulation following an abdominal aortic, aneurysm repair. He receives an infusion of cryoprecipitate. What is the major constituent of this, infusion?, , Factor VIII, , Factor IX, , Protein C, , Protein S, , Factor V, , Please rate this question:, , Discuss and give feedback, , Next question, , Cryoprecipitate, , , , , Blood product made from plasma, Usually transfused as 6 unit pool, Indications include massive haemorrhage and uncontrolled bleeding due to haemophilia, , Composition, , Agent, , Quantity, , Factor VIII, , 100IU, , Fibrinogen, , 250mg, , von Willebrand factor, , Variable
Page 4059 :
Agent, , Quantity, , Factor XIII, , Variable, Next question
Page 4060 :
A 32 year old man presents to the acute surgical unit with acute pancreatitis. Over the next few days, he becomes dyspnoeic and his saturations are 89% on air. A CXR shows bilateral pulmonary, infiltrates. His CVP pressure is 16mmHg. What is the most likely diagnosis?, , Cardiac failure, , Pneumococcal pneumonia, , Staphylococcal pneumonia, , Pneumocystis carinii, , Adult respiratory distress syndrome, , Theme from January 2012 Exam, Theme from September 2013 Exam, Acute pancreatitis is known to precipitate ARDS. ARDS is characterised by bilateral pulmonary, infiltrates and hypoxaemia. Note that pulmonary oedema is excluded by the CVP reading <, 18mmHg., Please rate this question:, , Discuss and give feedback, , Next question, , Adult respiratory distress syndrome, Defined as an acute condition characterized by bilateral pulmonary infiltrates and severe hypoxemia, (PaO2/FiO2 ratio < 200) in the absence of evidence for cardiogenic pulmonary oedema (clinically or, pulmonary capillary wedge pressure of less than 18 mm Hg)., In is subdivided into two stages. Early stages consist of an exudative phase of injury with associated, oedema. The later stage is one of repair and consists of fibroproliferative changes. Subsequent, scarring may result in poor lung function., Causes, , , , , , , Sepsis, Direct lung injury, Trauma, Acute pancreatitis, Long bone fracture or multiple fractures (through fat embolism)
Page 4061 :
, , Head injury (causes sympathetic nervous stimulation which leads to acute pulmonary, hypertension), , Clinical features, , , , , Acute dyspnoea and hypoxaemia hours/days after event, Multi organ failure, Rising ventilatory pressures, , Management, , , , , , , Treat the underlying cause, Antibiotics (if signs of sepsis), Negative fluid balance i.e. Diuretics, Recruitment manoeuvres such as prone ventilation, use of positive end expiratory pressure, Mechanical ventilation strategy using low tidal volumes, as conventional tidal volumes may, cause lung injury (only treatment found to improve survival rates), Next question
Page 4062 :
Which of the anaesthetic agents below is most likely to induce adrenal suppression?, , Sodium thiopentone, , Midazolam, , Propofol, , Etomidate, , Ketamine, , Etomidate is a recognised cause of adrenal suppression, this has been associated with increased, mortality when used as a sedation agent in the critically ill., Please rate this question:, , Discuss and give feedback, , Next question, , Anaesthetic agents, The table below summarises some of the more commonly used IV induction agents, , Agent, , Specific features, , Propofol, , , , , , , , , Rapid onset of anaesthesia, Pain on IV injection, Rapidly metabolised with little accumulation of metabolites, Proven anti emetic properties, Moderate myocardial depression, Widely used especially for maintaining sedation on ITU, total IV, anaesthesia and for daycase surgery, , Sodium, thiopentone, , , , Extremely rapid onset of action making it the agent of choice for rapid, sequence of induction, Marked myocardial depression may occur, Metabolites build up quickly, Unsuitable for maintenance infusion, , , ,
Page 4063 :
Ketamine, , , , Little analgesic effects, , , , , , May be used for induction of anaesthesia, Has moderate to strong analgesic properties, Produces little myocardial depression making it a suitable agent for, anaesthesia in those who are haemodynamically unstable, May induce state of dissociative anaesthesia resulting in nightmares, , , , Etomidate, , , , , , , Has favorable cardiac safety profile with very little haemodynamic, instability, No analgesic properties, Unsuitable for maintaining sedation as prolonged (and even brief) use, may result in adrenal suppression, Post operative vomiting is common, Next question
Page 4064 :
A 63 year old man is commenced on an infusion of packed red cells following a total hip, replacement. Which of the following adverse events is most likely?, , ABO mismatching, , Immune mediated intolerance of rhesus incompatible blood, , Pyrexia, , Jaundice, , Graft versus host disease, , Mild pyrexia during blood transfusion is the most common event and commonly occurs during, transfusion., Please rate this question:, , Discuss and give feedback, , Next question, , Blood transfusion reactions, Acute transfusion reactions present as adverse signs or symptoms during or within 24 hours of a, blood transfusion. The most frequent reactions are fever, chills, pruritus, or urticaria, which typically, resolve promptly without specific treatment or complications. Other signs occurring in temporal, relationship with a blood transfusion, such as severe dyspnoea, pyrexia, or loss of consciousness, may be the first indication of a more severe potentially fatal reaction., The causes of adverse reactions are multi-factorial. Immune mediated reactions, some of the most, feared, occur as a result of component mismatch, the commonest cause of which is clerical error., More common, non immune mediated, complications may occur as a result of product, contamination, this may be bacterial or viral., Transfusion related lung injury is well recognised and there are two proposed mechanisms which, underpin this. One involves the sequestration of primed neutrophils within the recipient pulmonary
Page 4065 :
capillary bed. The other proposed mechanism suggests that HLA mismatches between donor, neutrophils and recipient lung tissue is to blame., The table below summarises the main types of transfusion reaction., , Immune mediated, , Non immune mediated, , Pyrexia, , Hypocalcaemia, , Alloimmunization, , CCF, , Thrombocytopaenia, , Infections, , Transfusion associated lung injury, , Hyperkalaemia, , Graft vs Host disease, , Urticaria, , Acute or delayed haemolysis, , ABO incompatibility, , Rhesus incompatibility, Next question
Page 4066 :
Theme: Diagnosis and management of post operative complications, , A., B., C., D., E., F., G., H., I., J., , Trans anal ultrasound scan, Upper abdominal ultrasound scan, Total abdominal ultrasound scan, PET CT scan, ERCP, Small bowel MRI Scan, Abdominal CT scan with oral and IV contrast, Non contrast abdominal CT scan, Laparotomy, Laparoscopy, , For the following post operative scenarios please select the most appropriate investigation or, management. Each option may be used once, more than once or not at all., , 8., , A 7 year old boy develops a persistent fever following an open appendicectomy for, gangrenous appendicitis. On examination he has erythema of the wound and some, abdominal distension., You answered Trans anal ultrasound scan, The correct answer is Total abdominal ultrasound scan, Theme from September 2013 Exam, This patient has risk factors for a wound infection which is not in itself an indication for, scanning. However, he also had abdominal distension and this, together with the history of, distension would generally attract a recommendation for imaging. A USS will show an, abdominal wall collection and more importantly any phrenic or pelvic collections. Unlike, adult practice, CT scanning is rarely performed in children., , 9., , A 56 year old man is 8 days following a left hemicolectomy. He has developed a swinging, pyrexia over the past 48 hours and has an ileus clinically., You answered Trans anal ultrasound scan, The correct answer is Abdominal CT scan with oral and IV contrast, This would most likely be the result of an anastomotic leak with abscess formation., Detailed imaging is required to allow accurate diagnosis and planning of management., , 10., , A 43 year old lady underwent an acute cholecystectomy for cholecystitis. A drain is left, during the procedure. Over the next 5 days the drain has been accumulating between 100200ml of bile per 24 hour period.
Page 4067 :
You answered Trans anal ultrasound scan, The correct answer is ERCP, The most likely cause of a bile leak in this scenario would be a dislodged clip from the, cystic duct. Whilst it may be tempting to try and plan to manage this surgically the, anatomy is often unfavorable and the duct very difficult to identify. An ERCP has the, advantage of demonstrating the cause of the leak and allowing placement of a stent. This, will usually allow the resolution of most leaks without the need for surgery., Please rate this question:, , Discuss and give feedback, , Next question, , Surgical complications, Complications occur in all branches of surgery and require vigilance in their detection. In many, cases anticipating the likely complications and appropriate avoidance will minimise their occurrence., For the purposes of the MRCS the important principles to appreciate are:, , , , , , , The anatomical principles that underpin complications, The physiological and biochemical derangements that occur, The most appropriate diagnostic modalities to utilise, The principles which underpin their management, , This is clearly a very broad area and impossible to cover comprehensively. There is considerable, overlap with other topic areas within the website., Avoiding complications, Some points to hopefully avert complications:, , , , , , , , , , World Health Organisation checklist- now mandatory prior to all operations, Prophylactic antibiotics - right dose, right drug, right time., Assess DVT/ PE risk and ensure adequate prophylaxis, MARK site of surgery, Use tourniquets with caution and with respect for underlying structures, Remember the danger of end arteries and in situations where they occur avoid using, adrenaline containing solutions and monopolar diathermy., Handle tissues with care- devitalised tissue serves as a nidus for infection
Page 4068 :
, , , Be very wary of the potential for coupling injuries when using diathermy during laparoscopic, surgery, The inferior epigastric artery is a favorite target for laparoscopic ports and surgical drains!, , Anatomical principles, Understanding the anatomy of a surgical field will allow appreciation of local and systemic, complications that may occur. For example, nerve injuries may occur following surgery in specific, regions. The table below lists some of the more important nerves to consider and mechanisms of, injury, , Nerve, , Mechanism, , Accessory, , Posterior triangle lymph node biopsy, , Sciatic, , Posterior approach to hip, , Common peroneal, , Legs in Lloyd Davies position, , Long thoracic, , Axillary node clearance, , Pelvic autonomic nerves, , Pelvic cancer surgery, , Recurrent laryngeal nerves, , During thyroid surgery, , Hypoglossal nerve, , During carotid endarterectomy, , Ulnar and median nerves, , During upper limb fracture repairs, , These are just a few. The detailed functional sequelae are particularly important and will often be, tested. In addition to nerve injuries certain procedures carry risks of visceral or structural injury., Again some particular favorites are given below:, , Structure, , Mechanism
Page 4069 :
Structure, , Mechanism, , Thoracic duct, , During thoracic surgery e.g. Pneumonectomy, oesphagectomy, , Parathyroid glands, , During difficult thyroid surgery, , Ureters, , During colonic resections/ gynaecological surgery, , Bowel perforation, , Use of Verres Needle to establish pneumoperitoneum, , Bile duct injury, , Failure to delineate Calots triangle carefully and careless use of diathermy, , Facial nerve, , Always at risk during Parotidectomy, , Tail of pancreas, , When ligating splenic hilum, , Testicular vessels, , During re-do open hernia surgery, , Hepatic veins, , During liver mobilisation, , Again many could be predicted from the anatomy of the procedure., Physiological derangements, A very common complication is bleeding and this is covered under the section of haemorrhagic, shock. Another variant is infection either superficial or deep seated. The organisms are covered, under microbiology and the features of sepsis covered under shock. Do not forget that, immunocompromised and elderly patients may present will atypical physiological parameters., Selected physiological and biochemical issues are given below:, , Complication, , Physiological/ Biochemical Problem, , Arrhythmias following, , Susceptibility to hypokalaemia (K+ <4.0 in cardiac patients)
Page 4070 :
Complication, , Physiological/ Biochemical Problem, , cardiac surgery, , Neurosurgical electrolyte, disturbance, , SIADH following cranial surgery causing hyponatraemia, , Ileus following, gastrointestinal surgery, , Fluid sequestration and loss of electrolytes, , Pulmonary oedema following, pneumonectomy, , Loss of lung volume makes these patients very sensitive to fluid, overload, , Anastamotic leak, , Generalised sepsis causing mediastinitis or peritonitis depending, on site of leak, , Myocardial infarct, , May follow any type of surgery and in addition to direct cardiac, effects the decreased cardiac output may well compromise grafts, etc., , Try making a short list of problems and causes specific to your own clinical area., Diagnostic modalities, Depends largely on the suspected complication. In the acutely unwell surgical patient the following, baseline investigations are often helpful:, , , , , , , Full blood count, urea and electrolytes, C- reactive protein (trend rather than absolute value),, serum calcium, liver function tests, clotting (don't forget to repeat if on-going bleeding), Arterial blood gases, ECG (+cardiac enzymes if MI suspected), Chest x-ray to identify collapse/ consolidation, Urine analysis for UTI, , These will often identify the most common complications., Special tests
Page 4071 :
, , , , , , CT scanning for identification of intra-abdominal abscesses, air and if luminal contrast is, used an anastomotic leak, Doppler USS of leg veins- for identification of DVT, CTPA for PE, Sending peritoneal fluid for U+E (if ureteric injury suspected) or amylase (if pancreatic injury, suspected), Echocardiogram if pericardial effusion suspected post cardiac surgery and no pleural window, made., , Management of complications, The guiding principal should be safe and timely intervention. Patients should be stabilised and if an, operation needs to occur in tandem with resuscitation then generally this should be of a damage, limitation type procedure rather than definitive surgery (which can be more safely undertaken in a, stable patient the following day)., Remember that recent surgery is a contra indication to thrombolysis and that in some patients IV, heparin may be preferable to a low molecular weight heparin (easier to reverse)., As a general rule laparotomies for bleeding should follow the core principle of quadrant packing and, then subsequent pack removal rather than plunging large clamps into pools of blood. The latter, approach invariable worsens the situation is often accompanied by significant visceral injury, particularly when done by the inexperienced. If packing controls a situation it is entirely acceptable, practice to leave packs in situ and return the patient to ITU for pack removal the subsequent day., Next question
Page 4072 :
A patient with tachycardia and hypotension is to receive vasopressors. Which of the following, conditions are most likely to be treated with vasopressors?, , Hypovolaemic shock, , Septic shock, , Neurogenic shock, , Cardiogenic shock, , None of the above, , Theme from April 2012 Exam, The term septic shock has a precise meaning and refers to refractory systemic arterial hypotension, in spite of fluid resuscitation. Patients will therefore usually require inotropes. Individuals suffering, from neurogenic shock will usually receive intravenous fluids to achieve a mean arterial pressure of, 90mmHg. If this target cannot be achieved then these patients will receive inotropes. Hypovolaemic, shock requires fluids and the management of cardiogenic shock is multifactorial and includes, inotropes, vasodilators and intra-aortic balloon pumps., Please rate this question:, , Discuss and give feedback, , Next question, , Inotropes and cardiovascular receptors, Inotropes are a class of drugs which work primarily by increasing cardiac output. They should be, distinguished from vasoconstrictor drugs which are used specifically when the primary problem is, peripheral vasodilatation., Catecholamine type agents are commonly used and work by increasing cAMP levels by adenylate, cyclase stimulation. This in turn intracellular calcium ion mobilisation and thus the force of
Page 4073 :
contraction. Adrenaline works as a beta adrenergic receptor agonist at lower doses and an alpha, receptor agonist at higher doses. Dopamine causes dopamine receptor mediated renal and, mesenteric vascular dilatation and beta 1 receptor agonism at higher doses. This results in, increased cardiac output. Since both heart rate and blood pressure are raised, there is less overall, myocardial ischaemia. Dobutamine is a predominantly beta 1 receptor agonist with weak beta 2 and, alpha receptor agonist properties. Noradrenaline is a catecholamine type agent and predominantly, acts as an alpha receptor agonist and serves as a peripheral vasoconstrictor., Phosphodiesterase inhibitors such as milrinone act specifically on the cardiac phosphodiesterase, and increase cardiac output., , Inotrope, , Cardiovascular receptor action, , Adrenaline, , α-1, α-2, β-1, β-2, , Noradrenaline, , α-1,( α-2), (β-1), (β-2), , Dobutamine, , β-1, (β 2), , Dopamine, , (α-1), (α-2), (β-1), D-1,D-2, , Minor receptor effects in brackets, Effects of receptor binding, , α-1, α-2, , vasoconstriction, , β-1, , increased cardiac contractility and HR, , β-2, , vasodilatation, , D-1, , renal and spleen vasodilatation, , D-2, , inhibits release of noradrenaline
Page 4074 :
Infusion with which of the following blood products is most likely to result in an urticarial reaction?, , Packed red cells, , Fresh frozen plasma, , Platelets, , Cryoprecipitate, , Factor VIII concentrate, Pyrexia is the most common adverse event in transfusing packed red cells, Urticaria is the most common adverse event following infusion of FFP, , Please rate this question:, , Discuss and give feedback, , Next question, , Blood transfusion reactions, Acute transfusion reactions present as adverse signs or symptoms during or within 24 hours of a, blood transfusion. The most frequent reactions are fever, chills, pruritus, or urticaria, which typically, resolve promptly without specific treatment or complications. Other signs occurring in temporal, relationship with a blood transfusion, such as severe dyspnoea, pyrexia, or loss of consciousness, may be the first indication of a more severe potentially fatal reaction., The causes of adverse reactions are multi-factorial. Immune mediated reactions, some of the most, feared, occur as a result of component mismatch, the commonest cause of which is clerical error., More common, non immune mediated, complications may occur as a result of product, contamination, this may be bacterial or viral., Transfusion related lung injury is well recognised and there are two proposed mechanisms which, underpin this. One involves the sequestration of primed neutrophils within the recipient pulmonary
Page 4075 :
capillary bed. The other proposed mechanism suggests that HLA mismatches between donor, neutrophils and recipient lung tissue is to blame., The table below summarises the main types of transfusion reaction., , Immune mediated, , Non immune mediated, , Pyrexia, , Hypocalcaemia, , Alloimmunization, , CCF, , Thrombocytopaenia, , Infections, , Transfusion associated lung injury, , Hyperkalaemia, , Graft vs Host disease, , Urticaria, , Acute or delayed haemolysis, , ABO incompatibility, , Rhesus incompatibility, Next question
Page 4076 :
Theme: Feeding options, , A., B., C., D., E., F., , Feeding jejunostomy, Percutaneous endoscopic gastrostomy, Total parenteral nutrition, Naso gastric feeding tube, Elemental diet orally, Normal oral intake, , Please select the most appropriate method of delivering nutrition in each of the following scenarios., Each option may be used once, more than once or not at all., , 13., , A 28 year old man is comatose, from head injuries, on the neurosurgical intensive care, unit. Apart from a parietal fracture there is no bony injury. He is recovering well and, should be extubated soon., You answered Feeding jejunostomy, The correct answer is Naso gastric feeding tube, Theme from April 2012 Exam, Theme from January 2013 Exam, The feeding of head injured patients was reviewed in a 2008 Cochrane report. They, concluded that the overall evidence base was poor. However, there was a trend for the, enteral route, with NG feeding in the later stages following injury. This is contra indicated, if there are signs of basal skull fractures., , 14., , A 56 year old man has undergone a potentially curative oesophagectomy for carcinoma., Feeding jejunostomy, Feeding jejunostomy is the standard of care in most centres. Naso jejunal tubes are, preferred by some surgeons. However, if they become displaced the only alternative then, becomes TPN., , 15., , A 43 year old man is recovering from a laparoscopic low anterior resection with loop, ileostomy., You answered Feeding jejunostomy, The correct answer is Normal oral intake, Early feeding in this situation is both safe and will enhance recovery.
Page 4077 :
Please rate this question:, , Discuss and give feedback, , Next question, , Nutrition options in surgical patients, Oral intake, , , , , , Easiest option, May be supplemented by calorie rich dietary supplements, May contra indicated following certain procedures, , Naso gastric feeding, , , , , , , Usually administered via fine bore naso gastric feeding tube, Complications relate to aspiration of feed or misplaced tube, May be safe to use in patients with impaired swallow, Often contra indicated following head injury due to risks, associated with tube insertion, , Naso jejunal feeding, , , , Avoids problems of feed pooling in stomach (and risk of, aspiration), Insertion of feeding tube more technically complicated (easiest, if done intra operatively), Safe to use following oesophagogastric surgery, , , , , Feeding jejunostomy, , , , , , , Percutaneous, endoscopic, gastrostomy, , , , , , Total parenteral, nutrition, , , , , Surgically sited feeding tube, May be used for long term feeding, Low risk of aspiration and thus safe for long term feeding, following upper GI surgery, Main risks are those of tube displacement and peritubal leakage, immediately following insertion, which carries a risk of, peritonitis, Combined endoscopic and percutaneous tube insertion, May not be technically possible in those patients who cannot, undergo successful endoscopy, Risks include aspiration and leakage at the insertion site, The definitive option in those patients in whom enteral feeding, is contra indicated, Individualised prescribing and monitoring needed
Page 4078 :
, , , Should be administered via a central vein as it is strongly, phlebitic, Long term use is associated with fatty liver and deranged LFT's, Next question
Page 4079 :
Theme: Anaesthetic agents, , A., B., C., D., E., F., G., , Etomidate, Ketamine, Propofol, Sodium thiopentone, Methohexitone, Metaraminol, Midazolam, , Please select the most appropriate anaesthetic induction agent for the procedure described. Each, option may be used once, more than once or not at all., , 16., , A 32 year old man is admitted for a trendelenberg procedure for varicose veins. He is, known to have porphyria., You answered Etomidate, The correct answer is Propofol, This is a daycase procedure for which propofol is ideal. Sodium thiopentone and etomidate, are contraindicated in porphyria., , 17., , A 77 year old lady with unstable ischaemic heart disease requires an emergency femoral, hernia repair. She is volume depleted and slightly hypotensive., You answered Etomidate, The correct answer is Ketamine, Ketamine is not negatively inotropic and will not depress cardiac output. Propofol and, Sodium thiopentone will produce myocardial depression. Some doctors may also consider, etomidate. However, it may cause adrenal suppression and post operative vomiting- which, she is at high risk of developing., , 18., , A 22 year old man is brought to theatre for an emergency apppendicectomy for generalised, peritonitis. He is vomiting., You answered Etomidate, The correct answer is Sodium thiopentone, Most anaesthetists would use sodium thiopentone for a rapid sequence induction (which
Page 4080 :
this man will need)., Propofol- Ideal agent for daycase- wears off rapidly, good antiemetic effect., Sodium thiopentone- Fast onset of action- prone to accumulation. Depresses cardiac output., Ketamine- Little haemodynamic instability. Good analgesic properties. Nightmares and restlessness., Please rate this question:, , Discuss and give feedback, , Next question, , Anaesthetic agents, The table below summarises some of the more commonly used IV induction agents, , Agent, , Specific features, , Propofol, , , , , , , , , Rapid onset of anaesthesia, Pain on IV injection, Rapidly metabolised with little accumulation of metabolites, Proven anti emetic properties, Moderate myocardial depression, Widely used especially for maintaining sedation on ITU, total IV, anaesthesia and for daycase surgery, , Sodium, thiopentone, , , , Extremely rapid onset of action making it the agent of choice for rapid, sequence of induction, Marked myocardial depression may occur, Metabolites build up quickly, Unsuitable for maintenance infusion, Little analgesic effects, , , , , , , Ketamine, , , , , , , Etomidate, , , , , May be used for induction of anaesthesia, Has moderate to strong analgesic properties, Produces little myocardial depression making it a suitable agent for, anaesthesia in those who are haemodynamically unstable, May induce state of dissociative anaesthesia resulting in nightmares, Has favorable cardiac safety profile with very little haemodynamic, instability, No analgesic properties
Page 4081 :
, , , Unsuitable for maintaining sedation as prolonged (and even brief) use, may result in adrenal suppression, Post operative vomiting is common, Next question
Page 4082 :
A 54-year-old man is admitted for an elective hip replacement. Three days post operatively you, suspect he has had a pulmonary embolism. He has no past medical history of note. Blood pressure, is 120/80 mmHg with a pulse of 90/min. The chest x-ray is normal. Following treatment with lowmolecular weight heparin, what is the most appropriate initial lung imaging investigation to perform?, , Pulmonary angiography, , Echocardiogram, , MRI thorax, , Ventilation-perfusion scan, , Computed tomographic pulmonary angiography, CTPA is the first line investigation for PE according to current BTS guidelines, This is a difficult question to answer as both computed tomographic pulmonary angiography (CTPA), and ventilation-perfusion scanning are commonly used in UK clinical practice. The 2003 British, Thoracic Society (BTS) guidelines, however, recommended that CTPA is now used as the initial lung, imaging modality of choice. Pulmonary angiography is of course the 'gold standard' but this is not, what the question asks for, Please rate this question:, , Discuss and give feedback, , Next question, , Pulmonary embolism: investigation, The British Thoracic Society (BTS) published guidelines in 2003 on the management of patients with, suspected pulmonary embolism (PE), Key points from the guidelines include:, , , , , , computed tomographic pulmonary angiography (CTPA) is now the recommended initial lungimaging modality for non-massive PE. Advantages compared to V/Q scans include speed,, easier to perform out-of-hours, a reduced need for further imaging and the possibility of, providing an alternative diagnosis if PE is excluded, if the CTPA is negative then patients do not need further investigations or treatment for PE, ventilation-perfusion scanning may be used initially if appropriate facilities exist, the chest xray is normal, and there is no significant symptomatic concurrent cardiopulmonary disease
Page 4083 :
Some other points, Clinical probability scores based on risk factors and history and now widely used to help decide on, further investigation/management, D-dimers, , , sensitivity = 95-98%, but poor specificity, , V/Q scan, , , , , sensitivity = 98%; specificity = 40% - high negative predictive value, i.e. if normal virtually, excludes PE, other causes of mismatch in V/Q include old pulmonary embolisms, AV malformations,, vasculitis, previous radiotherapy, COPD gives matched defects, , CTPA, , , peripheral emboli affecting subsegmental arteries may be missed, , Pulmonary angiography, , , , the gold standard, significant complication rate compared to other investigations, Next question
Page 4084 :
Theme: Surgical analgesia, , A., B., C., D., E., F., G., , Amitriptylline, Pregabalin, Duloxetine, Paracetamol, Diclofenac, Pethidine, Morphine, , Please select the most appropriate analgesic modality for the scenario given. Each option may be, used once, more than once or not at all., , 20., , A 72 year old man attends vascular clinic after having an amputation 2 months ago. He is, having difficulty sleeping at night due to persistent tingling at the amputation site. He is, known to have orthostatic hypotension., You answered Amitriptylline, The correct answer is Pregabalin, This patient has phantom limb pain which is a neuropathic pain. First line management is, with amitriptylline or pregabalin. However this patient has orthostatic hypotension, which, is a side effect of amitriptylline, therefore pregabalin is the treatment of choice., , 21., , A 64 year old type 2 diabetic is referred to vascular clinic with painful foot ulcers. His, ABPI is 0.6. On further questioning the patient reports a burning sensation in both of his, feet., You answered Amitriptylline, The correct answer is Duloxetine, This NICE guidelines state that duloxetine should be used as a 1st line agent in diabetic, neuropathic pain., , 22., , A 24 year old man has had a fracture of the tibia after playing football. He arrives in the, emergency room distressed and in severe pain., You answered Amitriptylline, The correct answer is Morphine
Page 4085 :
This type of injury will require morphine. However, timely fracture splinting will have a, significant analgesic effect., Please rate this question:, , Discuss and give feedback, , Next question, , Management of pain, World Health Organisation Analgesic Ladder, , , , , Initially peripherally acting drugs such as paracetamol or non-steroidal anti-inflammatory, drugs (NSAIDs) are given., If pain control is not achieved, the second part of the ladder is to introduce weak opioid drugs, such as codeine or dextropropoxyphene together with appropriate agents to control and, minimise side effects., The final rung of the ladder is to introduce strong opioid drugs such as morphine. Analgesia, from peripherally acting drugs may be additive to that from centrally-acting opioids and thus,, the two are given together., , The World Federation of Societies of Anaesthesiologists (WFSA) Analgesic Ladder, , , , , , For management of acute pain, Initially, the pain can be expected to be severe and may need controlling with strong, analgesics in combination with local anaesthetic blocks and peripherally acting drugs., The second rung on the postoperative pain ladder is the restoration of the use of the oral, route to deliver analgesia. Strong opioids may no longer be required and adequate analgesia, can be obtained by using combinations of peripherally acting agents and weak opioids., The final step is when the pain can be controlled by peripherally acting agents alone., , Local anaesthetics, , , , , , , , Infiltration of a wound with a long-acting local anaesthetic such as Bupivacaine, Analgesia for several hours, Further pain relief can be obtained with repeat injections or by infusions via a thin catheter, Blockade of plexuses or peripheral nerves will provide selective analgesia in those parts of, the body supplied by the plexus or nerves, Can either be used to provide anaesthesia for the surgery or specifically for postoperative, pain relief, Especially useful where a sympathetic block is needed to improve postoperative blood, supply or where central blockade such as spinal or epidural blockade is contraindicated.
Page 4086 :
Spinal anaesthesia, Provides excellent analgesia for surgery in the lower half of the body and pain relief can last many, hours after completion of the operation if long-acting drugs containing vasoconstrictors are used., - Side effects of spinal anaesthesia include: hypotension, sensory and motor block, nausea and, urinary retention., Epidural anaesthesia, An indwelling epidural catheter inserted. This can then be used to provide a continuous infusion of, analgesic agents. It can provide excellent analgesia. They are still the preferred option following, major open abdominal procedures and help prevent post operative respiratory compromise resulting, from pain., - Disadvantages of epidurals is that they usually confine patients to bed, especially if a motor block is, present. In addition an indwelling urinary catheter is required. Which may not only impair mobility but, also serve as a conduit for infection. They are contraindicated in coagulopathies., Transversus Abdominal Plane block (TAP), In this technique an ultrasound is used to identify the correct muscle plane and local anaesthetic, (usually bupivicaine) is injected. The agent diffuses in the plane and blocks many of the spinal, nerves. It is an attractive technique as it provides a wide field of blockade but does not require the, placement of any indwelling devices. There is no post operative motor impairment. For this reason it, is the preferred technique when extensive laparoscopic abdominal procedures are performed. They, will then provide analgesia immediately following surgery but as they do not confine the patient to, bed, the focus on enhanced recovery can begin sooner., -The main disadvantage is that their duration of action is limited to the half life of the local, anaesthetic agent chosen. In addition some anaesthetists do not have the USS skills required to site, the injections., Patient Controlled Analgesia (PCA), - Patients administer their own intravenous analgesia and titrate the dose to their own end-point of, pain relief using a small microprocessor - controlled pump. Morphine is the most popular drug used., Strong Opioids, Severe pain arising from deep or visceral structures requires the use of strong opioids, Morphine, , , , , , Short half life and poor bioavailability., Metabolised in the liver and clearance is reduced in patients with liver disease, in the elderly, and the debilitated, Side effects include nausea, vomiting, constipation and respiratory depression., Tolerance may occur with repeated dosage, , Pethidine
Page 4087 :
, , , , , Synthetic opioid which is structurally different from morphine but which has similar actions., Has 10% potency of morphine., Short half life and similar bioavailability and clearance to morphine., Short duration of action and may need to be given hourly., Pethidine has a toxic metabolite (norpethidine) which is cleared by the kidney, but which, accumulates in renal failure or following frequent and prolonged doses and may lead to, muscle twitching and convulsions. Extreme caution is advised if pethidine is used over a, prolonged period or in patients with renal failure., , Weak opioids, Codeine: markedly less active than morphine, has predictable effects when given orally and is, effective against mild to moderate pain., Non opioid analgesics, - Mild to moderate pain., Paracetamol, , , , , , Inhibits prostaglandin synthesis., Analgesic and antipyretic properties but little anti-inflammatory effect, It is well absorbed orally and is metabolised almost entirely in the liver, Side effects in normal dosage and is widely used for the treatment of minor pain. It causes, hepatotoxicity in over dosage by overloading the normal metabolic pathways with the, formation of a toxic metabolite., , NSAIDs, , , , , , , Analgesic and anti-inflammatory actions, Inhibition of prostaglandin synthesis by the enzyme Cyclooxygenase which catalyses the, conversion of arachidonic acid to the various prostaglandins that are the chief mediators of, inflammation. All NSAIDs work in the same way and thus there is no point in giving more, than one at a time. ., NSAIDs are, in general, more useful for superficial pain arising from the skin, buccal mucosa,, joint surfaces and bone., Relative contraindications: history of peptic ulceration, gastrointestinal bleeding or bleeding, diathesis; operations associated with high blood loss, asthma, moderate to severe renal, impairment, dehydration and any history of hypersensitivity to NSAIDs or aspirin., , Neuropthic pain, National Institute of Clinical Excellence (UK) guidelines:, , , , , First line: Amitriptyline (Imipramine if cannot tolerate) or pregabalin, Second line: Amitriptyline AND pregabalin, Third line: refer to pain specialist. Give tramadol in the interim (avoid morphine)
Page 4089 :
A 17 year old man undergoes an elective right hemicolectomy. Post operatively he receives a total of, 6 litres of 0.9% sodium chloride solution, over 24 hours. Which of the following complications may, ensue?, , Hyperchloraemiac acidosis., , Hypochloraemic alkalosis, , Hyperchloraemic alkalosis, , Acute renal failure, , None of the above, , Excessive infusions of any intravenous fluid carry the risk of development of tissue oedema and, potentially cardiac failure. Excessive administration of sodium chloride is a recognised cause of, hyperchloraemic acidosis and therefore Hartmans solution may be preferred where large volumes of, fluid are to be administered., Please rate this question:, , Discuss and give feedback, , Next question, , Post operative fluid management, Composition of commonly used intravenous fluids mmol-1, , Na, , K, , Cl, , Bicarbonate, , Lactate, , Plasma, , 137-147, , 4-5.5, , 95-105, , 22-25, , -, , 0.9% Saline, , 153, , -, , 153, , -, , -, , Dextrose / saline, , 30.6, , -, , 30.6, , -, , -
Page 4090 :
Hartmans, , 130, , 4, , 110, , -, , 28, , Post operative fluid management, In the UK the GIFTASUP and NICE (CG174 2013) guidelines (see reference below) were devised to, try and provide some consensus guidance as to how intravenous fluids should be administered. A, decade ago it was a commonly held belief that little harm would occur as a result of excessive, administration of normal saline and many oliguric post operative patients received enormous, quantities of IV fluids. As a result they developed hyperchloraemic acidosis. With greater, understanding of this potential complication, the use of electrolyte balanced solutions (Ringers, lactate/ Hartmans) is now favored over normal saline., The other guidance includes:, , , , , , , , Fluids given should be documented clearly and easily available, Assess the patient's fluid status when they leave theatre, If a patient is haemodynamically stable and euvolaemic, aim to restart oral fluid intake as, soon as possible, Review patients whose urinary sodium is < 20, If a patient is oedematous, hypovolaemia if present should be treated first. This should then, be followed by a negative balance of sodium and water, monitored using urine Na excretion, levels, Solutions such as Dextran 70 should be used in caution in patients with sepsis as there is a, risk of developing acute renal injury, , References, NICE guidance CG174. Intravenous fluid therapy in adults. December 2013., British Consensus Guidelines on Intravenous Fluid Therapy for Adult Surgical Patients. GIFTASUP, (2009), Next question
Page 4091 :
A 28 year old man with Crohn's disease has undergone a number of resections. His BMI is currently, 18 and his albumin is 18. He feels well but does have a small localised perforation of his small, bowel. The gastroenterologists are giving azathioprine. What is the most appropriate advice, regarding feeding?, , Nil by mouth, , Nil by mouth and continuous intra venous fluids until surgery, , Enteral feeding, , Parenteral feeding, , Nutritional supplements, , This man is malnourished, although he is likely to require surgery it is best for him to be nutritionally, optimised first. As he may have reduced surface area for absorption and has a localised perforation, TPN is likely to be the best feeding modality., Please rate this question:, , Discuss and give feedback, , Next question, , Parenteral feeding-NICE guidelines, Parenteral nutrition: NICE guidelines summary, Identify patients as malnourished or at risk, Patients identified as being malnourished, , , , BMI < 18.5 kg/m2, unintentional weight loss of > 10% over 3-6/12, BMI < 20 kg/m 2 and unintentional weight loss of > 5% over 3-6/12, , AT RISK of malnutrition, , , eaten nothing or little > 5 days, who are likely to eat little for a further 5 days, poor absorptive capacity
Page 4092 :
, , , high nutrient losses, high metabolism, , Identify unsafe/inadequate oral intake OR a non functional GI tract/perforation/inaccessible, Consider parenteral nutrition:, , , , , , , for feeding < 14 days consider feeding via a peripheral venous catheter, for feeding > 30 days use a tunneled subclavian line, continuous administration in severely unwell patients, if feed needed > 2 weeks consider changing from continuous to cyclical feeding, don't give > 50% of daily regime to unwell patients in first 24-48 hours, , Surgical patients: if malnourished with unsafe swallow OR a non functional GI, tract/perforation/inaccessible then consider peri operative parenteral feeding., Next question
Page 4093 :
A 51 year old man is shot in the abdomen and sustains a significant intra abdominal injury. A, laparotomy, bowel resection and end colostomy are performed. An associated vascular injury, necessitates a 6 unit blood transfusion. He has a prolonged recovery and is paralysed and ventilated, for 2 weeks on intensive care. He receives total parenteral nutrition and is eventually weaned from, the ventilator and transferred to the ward. On reviewing his routine blood tests the following results, are noted:, Full blood count, Hb, , 11.3 g/dl, , Platelets, , 267 x 109/l, , WBC, , 10.1 x109/l, , Urea and electrolytes, Na+, , 131 mmol/l, , K+, , 4.6 mmol/l, , Urea, , 2.3 mmol/l, , Creatinine, , 78 µmol/l, , Liver function tests, Bilirubin, , 25 µmol/l, , ALP, , 445 u/l, , ALT, , 89 u/l, , γGT, , 103 u/l, , What is the most likely underlying cause for the abnormalities noted?, , Delayed type blood transfusion reaction, , Bile leak, , Anastomotic leak, , Total parenteral nutrition
Page 4094 :
Gallstones, , TPN is known to result in derangement of liver function tests. Although, cholestasis may result from, TPN, it would be very unusual for gallstones to form and result in the picture above. Blood, transfusion reactions typically present earlier and with changes in the haemoglobin and although, they may cause hepatitis this is rare nowadays., Please rate this question:, , Discuss and give feedback, , Next question, , Total parenteral nutrition, , , , , , , Commonly used in nutritionally compromised surgical patients., Bags contain combinations of glucose, lipids and essential electrolytes, the exact, composition is determined by the patients nutritional requirements., Although it may be infused peripherally, this may result in thrombophlebitis., Longer term infusions should be administered into a central vein (preferably via a PICC line)., Complications are related to sepsis, re-feeding syndromes and hepatic dysfunction., Next question
Page 4095 :
Which statement regarding post operative cognitive impairment is true?, , Use of Benzodiazepines preoperatively reduces long-term post operative cognitive, dysfunction, Pain does not cause delirium, , Delirium has no impact on length of hospital stay, , A regional anaesthetic rather than a general anaesthetic is more likely to contribute to post, operative cognitive impairment, Visual hallucinations are not a feature of delirium, , Anaesthetic technique and Post operative cognitive impairment (POCD):, Use of benzodiazepines preoperatively reduces long-term POCD (9.9% vs. 5%), Do not stop drugs for cognitive function, Regional techniques reduce POCD in first week, but no difference at 3 months, References, Fines DP & Severn A. Anaesthesia and cognitive disturbance in the elderly Continuing Education in, Anaesthesia, Critical Care & Pain 2006 6(1):37-40, Please rate this question:, , Discuss and give feedback, , Next question, , Postoperative cognitive dysfunction management, Definition, , , Deterioration in performance in a battery of neuropsychological tests that would be expected, in < 3.5% of controls, , , , Long term, possibly permanent disabling deterioration in cognitive function following surgery, , Or, , Early POCD
Page 4096 :
, , , , , , Increasing age, GA rather than regional, Duration of anaesthesia, Reoperation, Postoperative infection, , Late POCD, , , , , Increasing age, Emboli, Biochemical disturbances, Next question
Page 4097 :
Which statement is false about pethidine?, , Has approximately 10% efficacy of morphine, , Structurally similar to morphine, , Pethidine has a toxic metabolite (norpethidine) which is cleared by the kidney, , Pethidine is metabolized by the liver, , Can be given intramuscularly, , It has a different structure., Please rate this question:, , Discuss and give feedback, , Next question, , Management of pain, World Health Organisation Analgesic Ladder, , , , , Initially peripherally acting drugs such as paracetamol or non-steroidal anti-inflammatory, drugs (NSAIDs) are given., If pain control is not achieved, the second part of the ladder is to introduce weak opioid drugs, such as codeine or dextropropoxyphene together with appropriate agents to control and, minimise side effects., The final rung of the ladder is to introduce strong opioid drugs such as morphine. Analgesia, from peripherally acting drugs may be additive to that from centrally-acting opioids and thus,, the two are given together., , The World Federation of Societies of Anaesthesiologists (WFSA) Analgesic Ladder, , , , , For management of acute pain, Initially, the pain can be expected to be severe and may need controlling with strong, analgesics in combination with local anaesthetic blocks and peripherally acting drugs., The second rung on the postoperative pain ladder is the restoration of the use of the oral, route to deliver analgesia. Strong opioids may no longer be required and adequate analgesia, can be obtained by using combinations of peripherally acting agents and weak opioids.
Page 4098 :
, , The final step is when the pain can be controlled by peripherally acting agents alone., , Local anaesthetics, , , , , , , , Infiltration of a wound with a long-acting local anaesthetic such as Bupivacaine, Analgesia for several hours, Further pain relief can be obtained with repeat injections or by infusions via a thin catheter, Blockade of plexuses or peripheral nerves will provide selective analgesia in those parts of, the body supplied by the plexus or nerves, Can either be used to provide anaesthesia for the surgery or specifically for postoperative, pain relief, Especially useful where a sympathetic block is needed to improve postoperative blood, supply or where central blockade such as spinal or epidural blockade is contraindicated., , Spinal anaesthesia, Provides excellent analgesia for surgery in the lower half of the body and pain relief can last many, hours after completion of the operation if long-acting drugs containing vasoconstrictors are used., - Side effects of spinal anaesthesia include: hypotension, sensory and motor block, nausea and, urinary retention., Epidural anaesthesia, An indwelling epidural catheter inserted. This can then be used to provide a continuous infusion of, analgesic agents. It can provide excellent analgesia. They are still the preferred option following, major open abdominal procedures and help prevent post operative respiratory compromise resulting, from pain., - Disadvantages of epidurals is that they usually confine patients to bed, especially if a motor block is, present. In addition an indwelling urinary catheter is required. Which may not only impair mobility but, also serve as a conduit for infection. They are contraindicated in coagulopathies., Transversus Abdominal Plane block (TAP), In this technique an ultrasound is used to identify the correct muscle plane and local anaesthetic, (usually bupivicaine) is injected. The agent diffuses in the plane and blocks many of the spinal, nerves. It is an attractive technique as it provides a wide field of blockade but does not require the, placement of any indwelling devices. There is no post operative motor impairment. For this reason it, is the preferred technique when extensive laparoscopic abdominal procedures are performed. They, will then provide analgesia immediately following surgery but as they do not confine the patient to, bed, the focus on enhanced recovery can begin sooner., -The main disadvantage is that their duration of action is limited to the half life of the local, anaesthetic agent chosen. In addition some anaesthetists do not have the USS skills required to site, the injections., Patient Controlled Analgesia (PCA), - Patients administer their own intravenous analgesia and titrate the dose to their own end-point of, pain relief using a small microprocessor - controlled pump. Morphine is the most popular drug used.
Page 4099 :
Strong Opioids, Severe pain arising from deep or visceral structures requires the use of strong opioids, Morphine, , , , , , Short half life and poor bioavailability., Metabolised in the liver and clearance is reduced in patients with liver disease, in the elderly, and the debilitated, Side effects include nausea, vomiting, constipation and respiratory depression., Tolerance may occur with repeated dosage, , Pethidine, , , , , , Synthetic opioid which is structurally different from morphine but which has similar actions., Has 10% potency of morphine., Short half life and similar bioavailability and clearance to morphine., Short duration of action and may need to be given hourly., Pethidine has a toxic metabolite (norpethidine) which is cleared by the kidney, but which, accumulates in renal failure or following frequent and prolonged doses and may lead to, muscle twitching and convulsions. Extreme caution is advised if pethidine is used over a, prolonged period or in patients with renal failure., , Weak opioids, Codeine: markedly less active than morphine, has predictable effects when given orally and is, effective against mild to moderate pain., Non opioid analgesics, - Mild to moderate pain., Paracetamol, , , , , , Inhibits prostaglandin synthesis., Analgesic and antipyretic properties but little anti-inflammatory effect, It is well absorbed orally and is metabolised almost entirely in the liver, Side effects in normal dosage and is widely used for the treatment of minor pain. It causes, hepatotoxicity in over dosage by overloading the normal metabolic pathways with the, formation of a toxic metabolite., , NSAIDs, , , , Analgesic and anti-inflammatory actions, Inhibition of prostaglandin synthesis by the enzyme Cyclooxygenase which catalyses the, conversion of arachidonic acid to the various prostaglandins that are the chief mediators of
Page 4100 :
, , , inflammation. All NSAIDs work in the same way and thus there is no point in giving more, than one at a time. ., NSAIDs are, in general, more useful for superficial pain arising from the skin, buccal mucosa,, joint surfaces and bone., Relative contraindications: history of peptic ulceration, gastrointestinal bleeding or bleeding, diathesis; operations associated with high blood loss, asthma, moderate to severe renal, impairment, dehydration and any history of hypersensitivity to NSAIDs or aspirin., , Neuropthic pain, National Institute of Clinical Excellence (UK) guidelines:, , , , , , First line: Amitriptyline (Imipramine if cannot tolerate) or pregabalin, Second line: Amitriptyline AND pregabalin, Third line: refer to pain specialist. Give tramadol in the interim (avoid morphine), If diabetic neuropathic pain: Duloxetine, , References, 1. http://guidance.nice.org.uk/CG96/Guidance/pdf/English, 2. Charlton E. The Management of Postoperative Pain . Update in Anaesthesia. Issue 7 (1997), Next question
Page 4101 :
Which of the following anaesthetic agents is least likely to be associated with depression of, myocardial contractility?, , Propofol, , Etomidate, , Sodium thiopentone, , Ether, , None of the above, , Of the agents mentioned, etomidate has the most favorable cardiac safety profile., Please rate this question:, , Discuss and give feedback, , Next question, , Anaesthetic agents, The table below summarises some of the more commonly used IV induction agents, , Agent, , Specific features, , Propofol, , , , , , , , , Rapid onset of anaesthesia, Pain on IV injection, Rapidly metabolised with little accumulation of metabolites, Proven anti emetic properties, Moderate myocardial depression, Widely used especially for maintaining sedation on ITU, total IV, anaesthesia and for daycase surgery, , Sodium, thiopentone, , , , Extremely rapid onset of action making it the agent of choice for rapid, sequence of induction, Marked myocardial depression may occur, Metabolites build up quickly, Unsuitable for maintenance infusion, , , ,
Page 4102 :
Ketamine, , , , Little analgesic effects, , , , , , May be used for induction of anaesthesia, Has moderate to strong analgesic properties, Produces little myocardial depression making it a suitable agent for, anaesthesia in those who are haemodynamically unstable, May induce state of dissociative anaesthesia resulting in nightmares, , , , Etomidate, , , , , , , Has favorable cardiac safety profile with very little haemodynamic, instability, No analgesic properties, Unsuitable for maintaining sedation as prolonged (and even brief) use, may result in adrenal suppression, Post operative vomiting is common, Next question
Page 4103 :
Theme: Intravenous access, , A. 14 G peripheral cannula, B. Intraosseous infusion, C. Triple lumen central line (internal jugular route), D. Triple lumen central line (femoral vein route), E. Swann Ganz Catheter, F. Swann Ganz Introducer (7G), G. 22 G peripheral cannula, H. Hickman line, , Please select the most appropriate modality of intravenous access for the scenario given. Each, option may be used once, more than once or not at all., , 29., , A 45 year old man with liver cirrhosis is admitted with a brisk upper GI bleed. Multiple infusions, are required and he is peripherally shut down., You answered 14 G peripheral cannula, The correct answer is Triple lumen central line (femoral vein route), A central line is the most sensible option. He is highly likely to be coagulopathic and a femoral, insertion route is safest in these circumstances., Multiple infusions and absence of peripheral veins are the compelling indications for central, access in this case., , 30., , A 3 year old is injured in a road traffic accident and is hypotensive and tachycardic due to a, suspected splenic injury, she is peripherally shut down., You answered 14 G peripheral cannula, The correct answer is Intraosseous infusion
Page 4104 :
Intraosseous infusions are the preferred route in this situation as peripheral cannulation will be, difficult and unreliable., , 31., , A 73 year old man with Dukes C colonic cancer requires a long course of chemotherapy. He has, poor peripheral veins., You answered 14 G peripheral cannula, The correct answer is Hickman line, A Hickman line is the most reliable long term option. Most Hickman lines are inserted under local, anaesthesia with image guidance. They have a cuff that usually becomes integrated with the, surrounding tissues. This requires a brief dissection during line removal., , Please rate this question:, , Discuss and give feedback, , Next question, , Intravenous access, Venous access, A number of routes for establishing venous access are available., Peripheral venous cannula, Easy to insert with minimal morbidity. Wide lumen cannulae can provide rapid fluid infusions. When, properly managed infections may be promptly identified and the cannula easily re sited. Problems, relate to their peripheral sites and they are unsuitable for the administration of vaso active drugs,, such as inotropes and irritant drugs such as TPN (except in the very short term setting)., Central lines, Insertion is more difficult and most operators and NICE advocate the use of ultra sound., Coagulopathies may lead to haemorrhage following iatrogenic arterial injury. Femoral lines are, easier to insert and iatrogenic injuries easier to manage in this site however they are prone to high, infection rates. Internal jugular route is preferred. They have multiple lumens allowing for
Page 4105 :
administration of multiple infusions. The lumens are relatively narrow and thus they do not allow, particularly rapid rates of infusion., Intraosseous access, This is typically undertaken at the anteromedial aspect of the proximal tibia and provides access to, the marrow cavity and circulatory system. Although traditionally preferred in paediatric practice they, may be used in adults and a wide range of fluids can be infused using these devices., Tunneled lines, Tunneled lines such as Groshong and Hickman lines are popular devices for patients with long term, therapeutic requirements. These devices are usually inserted using ultrasound guidance into the, internal jugular vein and then tunneled under the skin. A cuff of woven material is sited near the end, and helps to anchor the device into the tissues. These cuffs require formal dissection to allow the, device to be removed. Tunneled lines can be linked to injection ports that are located under the skin., These are especially popular in paediatric practice., Peripherally inserted central cannula, Referred to as PICC lines, these are popular methods for establishing central venous access., Because they are inserted peripherally they are less prone to major complications relating to device, insertion than conventional central lines., Next question
Page 4106 :
Which of the following is a not a diagnostic criteria for brain death?, , No response to sound, , No corneal reflex, , Absent oculo-vestibular reflexes, , No response to supraorbital pressure, , No cough reflex to bronchial stimulation, , Please rate this question:, , Discuss and give feedback, , Next question, , Brain death, Criteria for brain stem death testing, , , , , , Deep coma of known aetiology., Reversible causes excluded, No sedation, Normal electrolytes, , Testing for brain death, , , , , , , , Fixed pupils which do not respond to sharp changes in the intensity of incident light, No corneal reflex, Absent oculo-vestibular reflexes - no eye movements following the slow injection of at least, 50ml of ice-cold water into each ear in turn (the caloric test), No response to supraorbital pressure, No cough reflex to bronchial stimulation or gagging response to pharyngeal stimulation, No observed respiratory effort in response to disconnection of the ventilator for long enough, (typically 5 minutes) to ensure elevation of the arterial partial pressure of carbon dioxide to at, least 6.0 kPa (6.5 kPa in patients with chronic carbon dioxide retention). Adequate, oxygenation is ensured by pre-oxygenation and diffusion oxygenation during the
Page 4107 :
disconnection (so the brain stem respiratory centre is not challenged by the ultimate, anoxic,, drive stimulus), , The test should be undertaken by two appropriately experienced doctors on two separate occasions., Both should be experienced in performing brain stem death testing and have at least 5 years post, graduate experience. One of them must be a consultant. Neither can be a member of the transplant, team (if organ donation contemplated)., Next question
Page 4108 :
Theme: Airway management, , A., B., C., D., E., , Cricothyroidotomy, Laryngeal mask, Endotracheal intubation, Tracheostomy, Oropharyngeal airway, , Please select the most appropriate method of airway access for the scenario given. Each option may, be used once, more than once or not at all., , 33., , A 63 year old man has been on the intensive care unit for a week with adult respiratory, distress syndrome complicating acute pancreatitis. He has required ventilation and is still, being mechanically ventilated., You answered Cricothyroidotomy, The correct answer is Tracheostomy, Tracheostomy is often used to facilitate long term weaning. The percutaneous devices are, popular. These involve a seldinger type insertion of the tube. A second operator inserts a, bronchoscope to ensure the device is not advanced through the posterior wall of the, trachea. Complications include damage to adjacent structures and bleeding (contra, indication in coagulopathy)., , 34., , A 23 year old man is undergoing an inguinal hernia repair as a daycase procedure and is, being given sevoflurane., You answered Cricothyroidotomy, The correct answer is Laryngeal mask, This procedure will be associated with requirement for swift onset of anaesthesia and, recovery. Muscle paralysis is not required and this would an ideal case for laryngeal mask, airway., , 35., , A 48 year old man is due to undergo a laparotomy for small bowel obstruction., You answered Cricothyroidotomy, The correct answer is Endotracheal intubation, Patients who are due to undergo laparotomies for bowel obstruction have either been
Page 4109 :
vomiting or at high risk of regurgitation of gastric contents on induction of anaesthesia. A, rapid sequence induction with cricothyroid pressure applied to occlude the oesophagus is, performed. A cuffed endotracheal tube is then inserted. Once correct placement of the ET, tube is confirmed the cricothyroid pressure can be removed., Please rate this question:, , Discuss and give feedback, , Next question, , Airway management, Oropharyngeal, airway, , , , , , , Easy to insert and use, No paralysis required, Ideal for very short procedures, Most often used as bridge to more definitive airway, , Laryngeal mask, , , , , , , , , Widely used, Very easy to insert, Device sits in pharynx and aligns to cover the airway, Poor control against reflux of gastric contents, Paralysis not usually required, Commonly used for wide range of anaesthetic uses, especially in, day surgery, Not suitable for high pressure ventilation (small amount of PEEP, often possible), , , , Tracheostomy, , , , , , , Reduces the work of breathing (and dead space), May be useful in slow weaning, Percutaneous tracheostomy widely used in ITU, Dries secretions, humidified air usually required, , Endotracheal tube, , , , , , Provides optimal control of the airway once cuff inflated, May be used for long or short term ventilation, Errors in insertion may result in oesophageal intubation (therefore, end tidal CO2 usually measured), Paralysis often required, Higher ventilation pressures can be used, , , , , Next question
Page 4110 :
You are the cardiothoracic surgical registrar reviewing a patient referred for an aortic valve, replacement. The 40-year-old man is being investigated for progressive breathlessness in a previous, respiratory clinic. The notes show he has smoked for the past 25 years. Pulmonary function tests, reveal the following:, , FEV1, , 1.4 L, , FVC, , 1.7 L, , FEV1/FVC, , 82%, , What is the most likely explanation?, , Asthma, , Bronchiectasis, , Kyphoscoliosis, , Chronic obstructive pulmonary disease, , Laryngeal malignancy, , These results show a restrictive picture, which may result from a number of conditions including, kyphoscoliosis. The other answers cause an obstructive picture., We note that most people have chosen COPD as the answer. In COPD the FEV1/FVC would show, an obstructive picture with the FEV1/FVC value being low (approximately less than 70%). In, restrictive conditions the FEV1/FVC is normal or increased (greater than 70%). With the FEV1/FVC, being over 70% the most likely answer is kyphoscoliosis., , Please rate this question:
Page 4111 :
Discuss and give feedback, , Next question, , Pulmonary function tests, Pulmonary function tests can be used to determine whether a respiratory disease is obstructive or, restrictive. The table below summarises the main findings and gives some example conditions:, , Obstructive lung disease, , Restrictive lung disease, , FEV1 - significantly reduced, FVC - reduced or normal, FEV1% (FEV1/FVC) - reduced (less than approx., 70%), , FEV1 - reduced, FVC - significantly reduced, FEV1% (FEV1/FVC) - normal or increased (over approx., 70%), , Asthma, COPD, Bronchiectasis, Bronchiolitis obliterans, , Pulmonary fibrosis, Asbestosis, Sarcoidosis, Acute respiratory distress syndrome, Infant respiratory distress syndrome, Kyphoscoliosis, Neuromuscular disorders, , If you would like to read more about pulmonary function tests, here is a link that may be useful:, Interpreting pulmonary function tests: Recognize the pattern, and the diagnosis will, followhttp://www.ccjm.org/content/70/10/866.full.pdf, Next question
Page 4112 :
Theme: Management of pain, , A., B., C., D., E., F., G., H., I., , Paracetamol, Non steroidal anti inflammatory drugs, Fentanyl patch, Carbamazepine, Pregabalin, Duloxetine, Radiotherapy, Chemotherapy, Spinal block, , For each scenario please select the most appropriate analgesic modality. Each option may be used, once, more than once or not at all., , 37., , A 52 year old man with prostate cancer is admitted to urology with urinary retention. He, complains of back pain which is not responding to ward analgesia. A lumbar xray, confirms lumbar spine metastases., You answered Paracetamol, The correct answer is Radiotherapy, This patient needs radiotherapy for pain relief. Bisphosphonates may also be effective., , 38., , A 42 year old woman complains of shooting pains in her left arm after a mastectomy., You answered Paracetamol, The correct answer is Pregabalin, Pregabalin is the 1st line treatment described in the NICE guidelines., , 39., , A 2 year old boy is recovering following an uncomplicated appendicectomy., Paracetamol, Paracetamol is an extremely effective analgesic in children., , Please rate this question:, , Discuss and give feedback
Page 4113 :
Next question, , Management of pain, World Health Organisation Analgesic Ladder, , , , , Initially peripherally acting drugs such as paracetamol or non-steroidal anti-inflammatory, drugs (NSAIDs) are given., If pain control is not achieved, the second part of the ladder is to introduce weak opioid drugs, such as codeine or dextropropoxyphene together with appropriate agents to control and, minimise side effects., The final rung of the ladder is to introduce strong opioid drugs such as morphine. Analgesia, from peripherally acting drugs may be additive to that from centrally-acting opioids and thus,, the two are given together., , The World Federation of Societies of Anaesthesiologists (WFSA) Analgesic Ladder, , , , , , For management of acute pain, Initially, the pain can be expected to be severe and may need controlling with strong, analgesics in combination with local anaesthetic blocks and peripherally acting drugs., The second rung on the postoperative pain ladder is the restoration of the use of the oral, route to deliver analgesia. Strong opioids may no longer be required and adequate analgesia, can be obtained by using combinations of peripherally acting agents and weak opioids., The final step is when the pain can be controlled by peripherally acting agents alone., , Local anaesthetics, , , , , , , , Infiltration of a wound with a long-acting local anaesthetic such as Bupivacaine, Analgesia for several hours, Further pain relief can be obtained with repeat injections or by infusions via a thin catheter, Blockade of plexuses or peripheral nerves will provide selective analgesia in those parts of, the body supplied by the plexus or nerves, Can either be used to provide anaesthesia for the surgery or specifically for postoperative, pain relief, Especially useful where a sympathetic block is needed to improve postoperative blood, supply or where central blockade such as spinal or epidural blockade is contraindicated., , Spinal anaesthesia, Provides excellent analgesia for surgery in the lower half of the body and pain relief can last many, hours after completion of the operation if long-acting drugs containing vasoconstrictors are used., - Side effects of spinal anaesthesia include: hypotension, sensory and motor block, nausea and, urinary retention., Epidural anaesthesia, An indwelling epidural catheter inserted. This can then be used to provide a continuous infusion of
Page 4114 :
analgesic agents. It can provide excellent analgesia. They are still the preferred option following, major open abdominal procedures and help prevent post operative respiratory compromise resulting, from pain., - Disadvantages of epidurals is that they usually confine patients to bed, especially if a motor block is, present. In addition an indwelling urinary catheter is required. Which may not only impair mobility but, also serve as a conduit for infection. They are contraindicated in coagulopathies., Transversus Abdominal Plane block (TAP), In this technique an ultrasound is used to identify the correct muscle plane and local anaesthetic, (usually bupivicaine) is injected. The agent diffuses in the plane and blocks many of the spinal, nerves. It is an attractive technique as it provides a wide field of blockade but does not require the, placement of any indwelling devices. There is no post operative motor impairment. For this reason it, is the preferred technique when extensive laparoscopic abdominal procedures are performed. They, will then provide analgesia immediately following surgery but as they do not confine the patient to, bed, the focus on enhanced recovery can begin sooner., -The main disadvantage is that their duration of action is limited to the half life of the local, anaesthetic agent chosen. In addition some anaesthetists do not have the USS skills required to site, the injections., Patient Controlled Analgesia (PCA), - Patients administer their own intravenous analgesia and titrate the dose to their own end-point of, pain relief using a small microprocessor - controlled pump. Morphine is the most popular drug used., Strong Opioids, Severe pain arising from deep or visceral structures requires the use of strong opioids, Morphine, , , , , , Short half life and poor bioavailability., Metabolised in the liver and clearance is reduced in patients with liver disease, in the elderly, and the debilitated, Side effects include nausea, vomiting, constipation and respiratory depression., Tolerance may occur with repeated dosage, , Pethidine, , , , , , Synthetic opioid which is structurally different from morphine but which has similar actions., Has 10% potency of morphine., Short half life and similar bioavailability and clearance to morphine., Short duration of action and may need to be given hourly., Pethidine has a toxic metabolite (norpethidine) which is cleared by the kidney, but which, accumulates in renal failure or following frequent and prolonged doses and may lead to, muscle twitching and convulsions. Extreme caution is advised if pethidine is used over a, prolonged period or in patients with renal failure.
Page 4115 :
Weak opioids, Codeine: markedly less active than morphine, has predictable effects when given orally and is, effective against mild to moderate pain., Non opioid analgesics, - Mild to moderate pain., Paracetamol, , , , , , Inhibits prostaglandin synthesis., Analgesic and antipyretic properties but little anti-inflammatory effect, It is well absorbed orally and is metabolised almost entirely in the liver, Side effects in normal dosage and is widely used for the treatment of minor pain. It causes, hepatotoxicity in over dosage by overloading the normal metabolic pathways with the, formation of a toxic metabolite., , NSAIDs, , , , , , , Analgesic and anti-inflammatory actions, Inhibition of prostaglandin synthesis by the enzyme Cyclooxygenase which catalyses the, conversion of arachidonic acid to the various prostaglandins that are the chief mediators of, inflammation. All NSAIDs work in the same way and thus there is no point in giving more, than one at a time. ., NSAIDs are, in general, more useful for superficial pain arising from the skin, buccal mucosa,, joint surfaces and bone., Relative contraindications: history of peptic ulceration, gastrointestinal bleeding or bleeding, diathesis; operations associated with high blood loss, asthma, moderate to severe renal, impairment, dehydration and any history of hypersensitivity to NSAIDs or aspirin., , Neuropthic pain, National Institute of Clinical Excellence (UK) guidelines:, , , , , , First line: Amitriptyline (Imipramine if cannot tolerate) or pregabalin, Second line: Amitriptyline AND pregabalin, Third line: refer to pain specialist. Give tramadol in the interim (avoid morphine), If diabetic neuropathic pain: Duloxetine, , References, 1. http://guidance.nice.org.uk/CG96/Guidance/pdf/English, 2. Charlton E. The Management of Postoperative Pain . Update in Anaesthesia. Issue 7 (1997), Next question
Page 4116 :
A 78 year old man presents with a ruptured aortic aneurysm. This is repaired but the operation is, difficult as it has a juxtarenal location. A supra renal cross clamp is applied. Post operatively he is, found to be oliguric and acute renal failure is suspected. Which of the following statements relating, to acute post-operative renal failure are untrue?, , Intravenous dopamine does not prevent acute renal failure., , It is more common after emergency surgery., , Use of excessive amounts of intravenous fluids may lead to falsely normal serum, creatinine measurements., Vasopressor drugs have a strong renoprotective effect, , It is minimised by normalisation of haemodynamic status., Key points : Renal injury and acute renal failure: RIFLE Classification., R=Risk (Serum Creatinine x1.5), I=Injury (Serum Creatinine x 2), F=Failure (Serum Creatinine x3), L=Loss (Loss of renal function >4weeks), E=End stage kidney disease, Vasopressor use is linked to renal failure as they are a marker of haemodynamic compromise., Please rate this question:, , Discuss and give feedback, , Next question, , Acute Renal Failure, , , , , , , , Final pathway is tubular cell death., Renal medulla is a relatively hypoxic environment making it susceptible to renal tubular, hypoxia., Renovascular autoregulation maintains renal blood flow across a range of arterial pressures., Estimates of GFR are best indices of level of renal function. Useful clinical estimates can be, obtained by considering serum creatinine, age, race, gender and body size. eGFR, calculations such as the Cockcroft and Gault equation are less reliable in populations with, high GFR's., Nephrotoxic stimuli such as aminoglycosides and radiological contrast media induce, apoptosis. Myoglobinuria and haemolysis result in necrosis. Overlap exists and, proinflammatory cytokines play and important role in potentiating ongoing damage.
Page 4117 :
, , , , Post-operative renal failure is more likely to occur in patients who are elderly, have, peripheral vascular disease, high BMI, have COPD, receive vasopressors, are on, nephrotoxic medication or undergo emergency surgery., Avoiding hypotension will reduce risk of renal tubular damage., There is no evidence that administration of ACE inhibitors or dopamine reduces the, incidence of post-operative renal failure., Next question
Page 4118 :
Which of the following is most suggestive of malnutrition?, , Hypoalbuminaemia, , BMI of 22 kg/m2 and unintentional weight loss of > 5% over 3-6 months, , BMI of 18.5 kg/m2, , Reduced skin turgor, , Unintentional weight loss of > 10% over 3- 6 months in a 60 Kg female who is 1.6m tall, , An unintentional weight loss of >10% in a three to six month period is highly suggestive of, malnutrition. This is particularly true of people with a normal/ low BMI. Hypoalbuminaemia is not, in, itself, a reliable marker of nutrition., Please rate this question:, , Discuss and give feedback, , Next question, , Nutrition Screening-NICE guidelines, NICE Screening for malnutrition: A summary, , , , , To be performed by an appropriate professional., All new hospital admissions, new GP patients, new care home patients and patients, attending their first clinic should be screened. Afterwards hospital in patients should be, screened weekly., The favored screening tool in the UK is the Malnutrition Universal Screening Tool (MUST)., , Nutritional support i.e. oral, enteral or parenteral, , , , , , Given to patients identified as being malnourished:, BMI < 18.5 kg/m2, Unintentional weight loss of > 10% over 3-6 months, BMI < 20 kg/m 2 and unintentional weight loss of > 5% over 3-6 months
Page 4119 :
NB BMI= weight (kg)/height (m2), , , , , , , , Considered in people identified as being AT RISK of malnutrition:, Eaten nothing or little > 5 days, who are likely to eat little for a further 5 days, Poor absorptive capacity, High nutrient losses, High metabolism, , NB if considering feed withdrawal refer to GMC guidance 'withholding and withdrawing life, prolonging treatment'., Next question
Page 4120 :
A 52 year old man is recovering following an elective right hemicolectomy for carcinoma of the, caecum. His surgery is uncomplicated, when should oral intake resume?, , Only once bowels have been opened to stool, , Only once the patient has passed flatus, , Between 24 and 48 hours of surgery, , More than 48 hours after surgery, , Within 24 hours of surgery, , As part of the enhanced recovery principles oral intake in this setting should resume soon after, surgery. Administration of liquid and even light diet does not increase the risk of anastomotic leak., Please rate this question:, , Discuss and give feedback, , Next question, , Oral Nutrition, Oral nutrition: a summary of NICE guidelines, , , , , , , Identify patients who are or at risk of being malnourished (see below for definitions), Check for dysphagia, If safe swallow, provide food and fluid in adequate quantity and quality, Give a balanced diet, Offer multivitamins and minerals, , Surgical patients:, , , If malnourished and safe swallow and post op caesarean, gynaecological or abdominal, surgery, aim for oral intake within 24h, , Patients identified as being malnourished:
Page 4121 :
, , , , BMI < 18.5 kg/m2, unintentional weight loss of > 10% over 3-6/12, BMI < 20 kg/m2 and unintentional weight loss of > 5% over 3-6/12, , AT RISK of malnutrition:, , , , , , eaten nothing or little > 5 days, who are likely to eat little for a further 5 days, poor absorptive capacity, high nutrient losses, high metabolism, Next question
Page 4122 :
Theme: Muscle relaxants, , A., B., C., D., E., , Atracurium, Suxamethonium, Pancuronium, Vecuronium, Curare, , Please select the muscle relaxant that applies to the scenario or description supplied. Each option, may be used once, more than once or not at all., , 43., , An agent that is degraded by hydrolysis and may produce histamine release., Atracurium, Atracurium is degraded by a process of ester hydrolysis. This uses non specific plasma, esterases., , 44., , An agent which should be avoided in a 23 year old man with burns and bilateral tibial, fractures after being trapped in a car accident for 2 hours., Suxamethonium, Suxamethonium may induce hyperkalaemia as it induces generalised muscular, contractions. In patients with likely extensive tissue necrosis this may be sufficient to, produce cardiac arrest., , 45., , An agent with a half life of less than 10 minutes., You answered Atracurium, The correct answer is Suxamethonium, Suxamethonium is extremely rapidly metabolised, acetylcholinesterases degrade the drug, within minutes. In patients who lack this enzyme the drug may last far longer., , Please rate this question:, , Discuss and give feedback, , Next question, , Muscle relaxants
Page 4123 :
Suxamethonium, , , , , , , , , Atracurium, , , , , , , , Vecuronium, , Pancuronium, , , , , , Depolarising neuromuscular blocker, Inhibits action of acetylcholine at the neuromuscular junction, Degraded by plasma cholinesterase and acetylcholinesterase (affected, by lack of acetylcholinesterase), Fastest onset and shortest duration of action of all muscle relaxants, Produces generalised muscular contraction prior to paralysis, Adverse effects include hyperkalaemia, malignant hyperthermia,, delayed recovery, Non depolarising neuromuscular blocking drug, Duration of action usually 30-45 minutes, Generalised histamine release on administration may produce facial, flushing, tachycardia and hypotension, Not excreted by liver or kidney, broken down in tissues by hydrolysis, Reversed by neostigmine, , , , Non depolarising neuromuscular blocking drug, Duration of action approximately 30 - 40 minutes, Degraded by liver and kidney and effects prolonged in organ, dysfunction, Effects may be reversed by neostigmine, , , , , , , Non depolarising neuromuscular blocker, Onset of action approximately 2-3 minutes, Duration of action up to 2 hours, Effects may be partially reversed with drugs such as neostigmine, Next question
Page 4124 :
With which of the following blood products is iatrogenic septicaemia with a gram positive organism, most likely?, , Cryoprecipitate, , Platelets, , Packed red cells, , Factor VIII concentrate, , Factor IX concentrate, , Platelets are stored at room temperature and must be used soon after collection. This places them, at increased risk of culturing gram positive organisms. Iatrogenic infection with gram negative, organisms is more likely with packed red cells as these are stored at 4 degrees., Infections with blood products of this nature are both rare., Please rate this question:, , Discuss and give feedback, , Next question, , Blood products, Whole blood fractions, , Fraction, , Key points, , Packed red cells, , Used for transfusion in chronic anaemia and cases where infusion of large, volumes of fluid may result in cardiovascular compromise. Product obtained, by centrifugation of whole blood., , Platelet rich, plasma, , Usually administered to patients who are thrombocytopaenic and are bleeding, or require surgery. It is obtained by low speed centrifugation., , Platelet, , Prepared by high speed centrifugation and administered to patients with
Page 4125 :
concentrate, , Fresh frozen, plasma, , thrombocytopaenia., , , , , , , , Cryoprecipitate, , SAG-Mannitol, Blood, , , , , , Prepared from single units of blood., Contains clotting factors, albumin and immunoglobulin., Unit is usually 200 to 250ml., Usually used in correcting clotting deficiencies in patients with hepatic, synthetic failure who are due to undergo surgery., Usual dose is 12-15ml/Kg-1., It should not be used as first line therapy for hypovolaemia., Formed from supernatant of FFP., Rich source of Factor VIII and fibrinogen., Allows large concentration of factor VIII to be administered in small, volume., , Removal of all plasma from a blood unit and substitution with:, , , , , , Sodium chloride, Adenine, Anhydrous glucose, Mannitol, , Up to 4 units of SAG M Blood may be administered. Thereafter whole blood, is preferred. After 8 units, clotting factors and platelets should be considered., Cell saver devices, These collect patients own blood lost during surgery and then re-infuse it. There are two main types:, , , , Those which wash the blood cells prior to re-infusion. These are more expensive to purchase, and more complicated to operate. However, they reduce the risk of re-infusing contaminated, blood back into the patient., Those which do not wash the blood prior to re-infusion., , Their main advantage is that they avoid the use of infusion of blood from donors into patients and, this may reduce risk of blood borne infection. It may be acceptable to Jehovah's witnesses. It is, contraindicated in malignant disease for risk of facilitating disease dissemination., Blood products used in warfarin reversal, In some surgical patients the use of warfarin can pose specific problems and may require the use of, specialised blood products, Immediate or urgent surgery in patients taking warfarin(1) (2):
Page 4126 :
1. Stop warfarin, 2. Vitamin K (reversal within 4-24 hours), -IV takes 4-6h to work (at least 5mg), -Oral can take 24 hours to be clinically effective, 3. Fresh frozen plasma, Used less commonly now as 1st line warfarin reversal, -30ml/kg-1, -Need to give at least 1L fluid in 70kg person (therefore not appropriate in fluid overload), -Need blood group, -Only use if human prothrombin complex is not available, 4. Human Prothrombin Complex (reversal within 1 hour), -Bereplex 50 u/kg, -Rapid action but factor 6 short half life, therefore give with vitamin K, References, 1. Dentali, F., C. Marchesi, et al. (2011). "Safety of prothrombin complex concentrates for rapid, anticoagulation reversal of vitamin K antagonists. A meta-analysis." Thromb Haemost 106(3): 429438., 2. http://www.transfusionguidelines.org/docs/pdfs/bbt-03warfarin-reversal-flowchart-2006.pdf, Next question
Page 4127 :
Which of the following is a recognised feature of ketamine when used as an anaesthetic agent?, , Malignant hyperpyrexia, , Adrenal suppression, , Myocardial depression, , Dissociative anaesthesia, , Marked respiratory depression, , Unlike most anaesthetic agents ketamine does not cause myocardial or marked respiratory, depression. It is not associated with the adrenal suppression that may occur with etomidate. It is, however, associated with a state of dissociative anaesthesia which patients may find distressing., Please rate this question:, , Discuss and give feedback, , Next question, , Anaesthetic agents, The table below summarises some of the more commonly used IV induction agents, , Agent, , Specific features, , Propofol, , , , , , , , , Rapid onset of anaesthesia, Pain on IV injection, Rapidly metabolised with little accumulation of metabolites, Proven anti emetic properties, Moderate myocardial depression, Widely used especially for maintaining sedation on ITU, total IV, anaesthesia and for daycase surgery, , Sodium, thiopentone, , , , Extremely rapid onset of action making it the agent of choice for rapid, sequence of induction, Marked myocardial depression may occur, Metabolites build up quickly, , ,
Page 4128 :
Ketamine, , , , , Unsuitable for maintenance infusion, Little analgesic effects, , , , , , May be used for induction of anaesthesia, Has moderate to strong analgesic properties, Produces little myocardial depression making it a suitable agent for, anaesthesia in those who are haemodynamically unstable, May induce state of dissociative anaesthesia resulting in nightmares, , , , Etomidate, , , , , , , Has favorable cardiac safety profile with very little haemodynamic, instability, No analgesic properties, Unsuitable for maintaining sedation as prolonged (and even brief) use, may result in adrenal suppression, Post operative vomiting is common, Next question
Page 4129 :
A 73 year old man undergoes a right below knee amputation for end stage peripheral vascular, disease. He is reviewed in the clinic 8 weeks post operatively and complains of a persistent, burning, discomfort over his amputation site stump. On examination his wound has healed and proximal, pulses have a biphasic signal on doppler ultrasound. What is the post appropriate management?, , Commence amitryptyline, , Commence fentanyl patch, , Arrange duplex scan, , Arrange MRI scan of the stump, , Commence carbamazepine, , This patient has neuropathic pain. Amitryptyline is the treatment of choice. Carbamazepine is mainly, used for trigeminal neuralgia., Please rate this question:, , Discuss and give feedback, , Next question, , Neuropathic pain, Neuropathic pain may be defined as pain which arises following damage or disruption of the nervous, system. It is often difficult to treat and responds poorly to standard analgesia., Examples include:, , , , , , diabetic neuropathy, post-herpetic neuralgia, trigeminal neuralgia, prolapsed intervertebral disc, , NICE issued guidance in 2010 on the management of neuropathic pain:, , , , first-line treatment*: oral amitriptyline or pregabalin, if satisfactory pain reduction is obtained with amitriptyline but the person cannot tolerate the, adverse effects, consider oral imipramine or nortriptyline as an alternative
Page 4130 :
, , second-line treatment: if first-line treatment was with amitriptyline, switch to or combine with, pregabalin. If first-line treatment was with pregabalin, switch to or, , combine with amitriptyline, , , other options: pain management clinic, tramadol (not other strong opioids), topical lidocaine, for localised pain if patients unable to take oral medication, , *please note that for some specific conditions the guidance may vary. For example carbamazepine, is used first-line for trigeminal neuralgia, duloxetine for diabetic neuropathy, Next question
Page 4131 :
A homeless 42 year old male had an emergency inguinal hernia repair 24 hours previously. He has, a BMI of 15. His electrolytes are normal. What is the best initial feeding regime?, , Give 10 kcal/kg/day initially, oral thiamine 200-300mg/day, vitamin B co strong1 tds and, supplements., Give 35 kcal/kg/day initially, oral thiamine 200-300mg/day, vitamin B co strong 1 tds and, supplements., No change to diet needed, , Oral thiamine 200-300mg/day, vitamin B co strong1 tds and supplements., , Give 35 kcal/kg/day initially, , This patient is at high risk of refeeding syndrome., Please rate this question:, , Discuss and give feedback, , Next question, , Nutrition - Refeeding syndrome, Refeeding syndrome describes the metabolic abnormalities which occur on feeding a person, following a period of starvation. The metabolic consequences include:, , , , , , Hypophosphataemia, Hypokalaemia, Hypomagnesaemia, Abnormal fluid balance, , These abnormalities can lead to organ failure., Re-feeding problems, If patient not eaten for > 5 days, aim to re-feed at < 50% energy and protein levels, High risk for re-feeding problems, If one or more of the following:, , , BMI < 16 kg/m 2
Page 4132 :
, , , , Unintentional weight loss >15% over 3-6 months, Little nutritional intake > 10 days, Hypokalaemia, Hypophosphataemia or hypomagnesaemia prior to feeding (unless high), , If two or more of the following:, , , , , , BMI < 18.5 kg/m2, Unintentional weight loss > 10% over 3-6 months, Little nutritional intake > 5 days, History of: alcohol abuse, drug therapy including insulin, chemotherapy, diuretics and, antacids, , Prescription, , , , , Start at up to 10 kcal/kg/day increasing to full needs over 4-7 days, Start immediately before and during feeding: oral thiamine 200-300mg/day, vitamin B co, strong 1 tds and supplements, Give K+ (2-4 mmol/kg/day), phosphate (0.3-0.6 mmol/kg/day), magnesium (0.2-0.4, mmol/kg/day), Next question
Page 4133 :
A 48 year old man is recovering on the high dependency unit following a long and complex, laparotomy. His preoperative medication includes an ACE inhibitor for blood pressure control. For, the past two hours he has been oliguric with a urine output of 10ml/hr-1. What the most appropriate, course of action?, , Stop the ACE inhibitor, , Administer a fluid challenge, , Start an infusion of nor adrenaline, , Administer intravenous frusemide, , Insert a Swann-Ganz Catheter, , Theme from April 2012 Exam, Hypovolaemia is the most likely cause for oliguria and a fluid challenge is the most appropriate, action. Blind administration of inotropes to hypovolaemic patients is unwise, with the possible, exception of cardiac patients., Please rate this question:, , Discuss and give feedback, , Next question, , Hypovolaemia and the surgical patient, Hypovolaemia often represents the end point of multiple pathological processes. It may be divided, into the following categories; overt compensated hypovolaemia, covert compensated hypovolaemia, and decompensated hypovolaemia. Of these three categories the covert compensated subtype of, hypovolaemia remains the commonest and is accounted for by the fact that class I shock will often, produce no overtly discernible clinical signs. This is due, in most cases, to a degree of splanchnic, autotransfusion. The most useful diagnostic test for detection of covert compensated hypovolaemia
Page 4134 :
remains urinanalysis. This often shows increased urinary osmolality and decreased sodium, concentration., In overt compensated hypovolaemia the blood pressure is maintained although other haemodynamic, parameters may be affected. This correlates to class II shock. In most cases assessment can be, determined clinically. Where underlying cardiopulmonary disease may be present the placement of a, CVP line may guide fluid resuscitation. Severe pulmonary disease may produce discrepancies, between right and left atrial filling pressures. This problem was traditionally overcome through the, use of Swann-Ganz catheters., Untreated, hypovolaemia may ultimately become uncompensated with resultant end organ, dysfunction. Microvascular hypoperfusion may result in acidosis with a subsequent myocardial, depressive effect, thereby producing a vicious circle., The treatment of hypovolaemia is with intravenous fluids. In the first instance a fluid challenge such, as the rapid infusion of 250ml of crystalloid will often serve as both a diagnostic and resuscitative, measure. In the event that this fails to produce the desired response the patient will need to be reevaluated clinically. More fluid may be needed. However, it is important not to overlook mechanical, ureteric obstruction in the anuric, normotensive patient., Next question
Page 4135 :
Theme: Muscle relaxants, , A., B., C., D., E., F., G., , Gallamine, Benzquinonium, Tubocurarine, Vecuronium, Pancuronium, Suxamethonium, Decamethonium halides, , Please select the most appropriate neuromuscular blocking drugs for the procedure described. Each, option may be used once, more than once or not at all., , 51., , A 56 year old man is undergoing a distal gastrectomy and just as the surgeon begins to, close the deep abdominal muscle layer the patient develops marked respiratory efforts and, closure cannot continue., You answered Gallamine, The correct answer is Suxamethonium, Suxamethonium has a rapid onset with short duration of action. As this is the final stage of, the procedure only brief muscle relaxation is needed., , 52., , An agent that is associated with a risk of malignant hyperthermia., You answered Gallamine, The correct answer is Suxamethonium, Suxamethonium may cause malignant hyperthermia and 1 in 2800 will have abnormal, cholinesterase enzyme and prolonged clinical effect., , 53., , An agent that may be absorbed from multiple bodily sites and causes histamine release., You answered Gallamine, The correct answer is Tubocurarine, It can be absorbed orally and rectally, though few would choose this route of, administration. It is now rarely used., , Please rate this question:
Page 4136 :
Discuss and give feedback, , Next question, , Muscle relaxants, Suxamethonium, , , , , , , , , Atracurium, , , , , , , , Vecuronium, , Pancuronium, , , , , , Depolarising neuromuscular blocker, Inhibits action of acetylcholine at the neuromuscular junction, Degraded by plasma cholinesterase and acetylcholinesterase (affected, by lack of acetylcholinesterase), Fastest onset and shortest duration of action of all muscle relaxants, Produces generalised muscular contraction prior to paralysis, Adverse effects include hyperkalaemia, malignant hyperthermia,, delayed recovery, Non depolarising neuromuscular blocking drug, Duration of action usually 30-45 minutes, Generalised histamine release on administration may produce facial, flushing, tachycardia and hypotension, Not excreted by liver or kidney, broken down in tissues by hydrolysis, Reversed by neostigmine, , , , Non depolarising neuromuscular blocking drug, Duration of action approximately 30 - 40 minutes, Degraded by liver and kidney and effects prolonged in organ, dysfunction, Effects may be reversed by neostigmine, , , , , , , Non depolarising neuromuscular blocker, Onset of action approximately 2-3 minutes, Duration of action up to 2 hours, Effects may be partially reversed with drugs such as neostigmine, Next question
Page 4137 :
A 45 year old man is involved in a polytrauma and requires a massive transfusion of packed red, cells and fresh frozen plasma. Three hours later he develops marked hypoxia and his CVP is noted, to be 10mm Hg. A chest x-rays shows bilateral diffuse pulmonary infiltrates. What is the most likely, diagnosis?, , Pulmonary embolus, , Myocardial stunning, , Myocardial infarct, , Fluid overload, , Transfusion associated lung injury, The risk of transfusion associated lung injury is greatest with plasma components., , Transfusion lung injury may occur after infusion of plasma components. Microvascular damage, occurs in the lungs leading to diffuse infiltrates on imaging. Mortality is high., Please rate this question:, , Discuss and give feedback, , Next question, , Massive haemorrhage, Definition, This is the loss of one blood volume in a 24 hour period or the loss of 50% of the circulating blood, volume in 3 hours. A blood loss of 150ml/ minute is also included. The normal adult blood volume is, 7% of total adult body weight. The blood volume equates to between 8 and 9% of a child's body, weight., Complications of massive transfusion
Page 4138 :
Complication, , Key points, , Hypothermia, , Blood is refrigerated, Hypothermic blood impairs homeostasis, Shifts Bohr curve to the left, , Hypocalcaemia, , Both FFP and platelets contain citrate anticoagulant, this may chelate, calcium, , Hyperkalaemia, , Plasma of red cells stored for 4-5 weeks contains 5-10 mmol K+, , Delayed type transfusion, reactions, , Due to minor incompatibility issues especially if urgent or non cross, matched blood used, , Transfusion related lung injury, , Acute onset non cardiogenic pulmonary oedema, Leading cause of transfusion related deaths, Greatest risk posed with plasma components, Occurs as a result of leucocyte antibodies in transfused plasma, Aggregation and degranulation of leucocytes in lung tissue accounts for, lung injury, , Coagulopathy, , Anticipate once circulating blood volume transfused, 1 blood volume usually drops platelet count to 100 or less, 1 blood volume will both dilute and not replace clotting factors, Fibrinogen concentration halves per 0.75 blood volume transfused, , References, Stainsby et al. Guidelines on the management of massive blood loss. British Journal of, Haematology2006 (135): 534 641., Next question
Page 4139 :
A 52 year old man undergoes a laparotomy for perforated bowel after a colonoscopy. 2 days after, surgery the nursing staff report there is pink, serous fluid discharging from the wound. What is the, next most appropriate management step?, , IV antibiotics for wound infection, , No further management, , Examine the wound for separation of the rectus fascia, , Insert a drain into the wound, , CT abdomen, , The seepage of pink serosanguineous fluid through a closed abdominal wound is an early sign of, abdominal wound dehiscence with possible evisceration. If this occurs, you should remove one or, two sutures in the skin and explore the wound manually, using a sterile glove. If there is separation, of the rectus fascia, the patient should be taken to the operating room for primary closure., Please rate this question:, , Discuss and give feedback, , Next question, , Abdominal wound dehiscence, , , , This is a significant problem facing all surgeons who undertake abdominal surgery on a, regular basis. Traditionally, it is said to occur when all layers of an abdominal mass closure, fail and the viscera protrude externally (associated with 30% mortality)., It can be subdivided into superficial, in which the skin wound alone fails and complete,, implying failure of all layers., , Factors which increase the risk are:, * Malnutrition, * Vitamin deficiencies, * Jaundice, * Steroid use, * Major wound contamination (e.g. faecal peritonitis), * Poor surgical technique (Mass closure technique is the preferred method-Jenkins Rule), When sudden full dehiscence occurs the management is as follows:, * Analgesia
Page 4140 :
* Intravenous fluids, * Intravenous broad spectrum antibiotics, * Coverage of the wound with saline impregnated gauze (on the ward), * Arrangements made for a return to theatre, Surgical strategy, , , , Correct the underlying cause (e.g. TPN or NG feed if malnourished), Determine the most appropriate strategy for managing the wound, , Options, , Resuturing of the, wound, , This may be an option if the wound edges are healthy and there is enough, tissue for sufficient coverage. Deep tension sutures are traditionally used for, this purpose., , Application of a, wound manager, , This is a clear dressing with removable front. Particularly suitable when some, granulation tissue is present over the viscera or where there is a high output, bowel fistula present in the dehisced wound., , Application of a, 'Bogota bag', , This is a clear plastic bag that is cut and sutured to the wound edges and is, only a temporary measure to be adopted when the wound cannot be closed, and will necessitate a return to theatre for definitive management., , Application of a, VAC dressing, system, , These can be safely used BUT ONLY if the correct layer is interposed, between the suction device and the bowel. Failure to adhere to this absolute, rule will almost invariably result in the development of multiple bowel, fistulae and create an extremely difficult management problem., Next question
Page 4141 :
A 63 year old man undergoes a subtotal colectomy and iatrogenic injury to both ureters is sustained., He develops renal failure and his serum potassium is found to be elevated at 6.9 mmol/L. An ECG is, performed, what is the most likely finding?, , Increased PR interval, , Prominent U waves, , Narrow QRS complexes, , Peaked T waves, , Low ST segments, , Peaked T waves are the first and most common finding in hyperkalaemia., Please rate this question:, , Discuss and give feedback, , Next question, , ECG features in hyperkalaemia, , , , , , Peaking of T waves (occurs first), Loss of P waves, Broad QRS complexes, Ventricullar fibrillation, Next question
Page 4142 :
Theme: Use of vasoactive drugs, , A., B., C., D., E., F., , Metoprolol, Dobutamine, Noradrenaline, Adrenaline, Milrinone, Dopamine, , Please select the most appropriate inotrope for the scenario given. Each option may be used once,, more than once or not at all., , 57., , An inotrope with mixed vaso dilating and vaso constricting properties., You answered Metoprolol, The correct answer is Dopamine, Dopamine is known to have a vasodilator effect in the renal circulation, elsewhere it, typically exerts a vasoconstrictive effect. This led to the previously popular concept of, using "renal dose" dopamine to improve renal function. This is now known to be, ineffective., , 58., , An inotrope that is a phosphodiesterase inhibitor., You answered Metoprolol, The correct answer is Milrinone, Milrinone works by increasing intracellular cAMP concentration., , 59., , A drug that would be useful in a 23 year old female with sepsis secondary to, pyelonephritis. She has an increased cardiac output and decreased systemic vascular, resistance., You answered Metoprolol, The correct answer is Noradrenaline, Theme from September 2011 Exam, In a setting of septic shock with normal or high cardiac output and decreased SVR, a, peripherally acting vasoconstrictor such as noradrenaline would be the primary choice.
Page 4143 :
Please rate this question:, , Discuss and give feedback, , Next question, , Circulatory support of the critically ill, Circulatory support, Impaired tissue oxygenation may occur as a result of circulatory shock. Shock is considered further, under its own topic heading., Patients requiring circulatory support require haemodynamic monitoring. At its simplest level this, may simply be in the form of regular urine output measurements and blood pressure monitoring. In, addition ECG monitoring with allow the identification of cardiac arrhythmias. Pulse oximeter, measurements will allow quick estimation haemoglobin oxygen saturation in arterial blood., Invasive arterial blood pressure monitoring is undertaken by the use of an indwelling arterial line., Most arterial sites can be used although the radial artery is the commonest. It is important not to, cannulate end arteries. The arterial trace can be tracked to ventilation phases and those patients, whose systolic pressure varies with changes in intrathoracic pressure may benefit from further, intravenous fluids., Central venous pressure is measured using a CVP line that is usually sited in the superior vena cava, via the internal jugular route. The CVP will demonstrate right atrial filling pressure and volume status., When adequate intra vascular volume is present a fluid challenge will typically cause a prolonged, rise in CVP (usually greater than 6-8mmHg)., To monitor the cardiac output a Swan-Ganz catheter is traditionally inserted (other devices may be, used and are less invasive). Inflation of the distal balloon will provide the pulmonary artery occlusion, pressure and the pressure distal to the balloon will equate to the left atrial pressure. This gives a, measure of left ventricular preload. Because the Swan-Ganz catheter can measure several variables, it can be used to calculate:, , , , , , Stroke volume, Systemic vascular resistance, Pulmonary artery resistance, Oxygen delivery (and consumption), , Inotropes, In patients with an adequate circulating volume but on-going circulatory compromise a vasoactive, drug may be considered. These should usually be administered via the central venous route., Commonly used inotropes include:, , Agent, , Mode of action, , Effect, , Noradrenaline, , α agonist, , Vasopressor action, minimal effect on cardiac output
Page 4144 :
Agent, , Mode of action, , Effect, , Adrenaline, , α and β receptor, agonist, , Increases cardiac output and peripheral vascular, resistance, , Dopamine, , β1 agonist, , Increases contractility and rate, , Dobutamine, , β1 and β2 agonist, , Increases cardiac output and decreases SVR, , Milrinone, , Phosphodiesterase, inhibitor, , Elevation of cAMP levels improves muscular, contractility, short half life and acts as vasodilator, Next question
Page 4145 :
A 56 year old man with chronic schizophrenia undergoes a cholecystectomy. He receives, metoclopramide for post operative nausea. Twenty minutes later he becomes agitated and develops, marked oculogyric crises and oromandibular dystonia. Which of the following drugs may best, alleviate his symptoms?, , Procyclidine, , Lorazepam, , Chlorpromazine, , Haloperidol, , Sulpiride, , This man has developed an acute dystonic reaction. Administration of further anti dopaminergic, drugs will worsen the situation. Procyclidine will help to reverse the event. This is most likely to have, occurred because the patient is on long term anti psychotics and has then received metoclopramide., Please rate this question:, , Discuss and give feedback, , Next question, , Acute dystonic reaction, The anti dopaminergic drugs (such as antipsychotics) may result in extrapyramidal side effects., These may range from mild parkinsonian symptoms such as resting tremor and bradykinesia., Through to acute dystonic reactions which are characterised by abnormal and involuntary facial and, bodily movements, such as spasmodic torticollis, oculogyric crisis and oromandibular dystonia., Chronic cases are generally only encountered in psychiatric units. In surgical practice the, administration of the anti dopaminergic drug metoclopramide may be sufficient to precipitate an, attack.
Page 4146 :
Treatment may be required if symptoms are sufficiently troublesome; benzhexol and procyclidine are, two drugs which may be used., Next question
Page 4147 :
Theme: Intravenous fluids, , A., B., C., D., E., F., G., H., , Dextran 40, Human albumin solution 4.5%, Dextran 70, Dextrose 4%/ Saline 0.19%, Dextrose 5%, Hartmans solution, Dextrose 10%, Gelofusin, , Please select the most appropriate intravenous fluid for the scenario given. Each option may be, used once, more than once or not at all., , 61., , A 45 year old lady with cirrhosis of the liver is recovering following an emergency para, umbilical hernia repair. She has been slow to resume oral intake and has been receiving, regular boluses of normal saline for oliguria., You answered Dextran 40, The correct answer is Human albumin solution 4.5%, In patients who are hypoalbuminaemic the use of albumin solution may help promote a, diuresis and manage fluid overload., , 62., , A 6 week old preterm neonate is due to have surgery for an inguinal hernia., You answered Dextran 40, The correct answer is Dextrose 10%, Neonates are at considerable risk of hypoglycaemia following surgery and should receive, 10% dextrose., , 63., , A 24 year old man is recovering from a right hemicolectomy for Crohns disease. He is, oliguric and dehydrated owing to a high output ileostomy. His electrolytes are normal., You answered Dextran 40, The correct answer is Hartmans solution, Of the solutions given Hartmans is the most suitable. Consideration should also be given, to potassium supplementation.
Page 4148 :
Starches increase risk of renal failure when used in septic shock., Please rate this question:, , Discuss and give feedback, , Next question, , Post operative fluid management, Composition of commonly used intravenous fluids mmol-1, , Na, , K, , Cl, , Bicarbonate, , Lactate, , Plasma, , 137-147, , 4-5.5, , 95-105, , 22-25, , -, , 0.9% Saline, , 153, , -, , 153, , -, , -, , Dextrose / saline, , 30.6, , -, , 30.6, , -, , -, , Hartmans, , 130, , 4, , 110, , -, , 28, , Post operative fluid management, In the UK the GIFTASUP and NICE (CG174 2013) guidelines (see reference below) were devised to, try and provide some consensus guidance as to how intravenous fluids should be administered. A, decade ago it was a commonly held belief that little harm would occur as a result of excessive, administration of normal saline and many oliguric post operative patients received enormous, quantities of IV fluids. As a result they developed hyperchloraemic acidosis. With greater, understanding of this potential complication, the use of electrolyte balanced solutions (Ringers, lactate/ Hartmans) is now favored over normal saline., The other guidance includes:, , , , , , , Fluids given should be documented clearly and easily available, Assess the patient's fluid status when they leave theatre, If a patient is haemodynamically stable and euvolaemic, aim to restart oral fluid intake as, soon as possible, Review patients whose urinary sodium is < 20, If a patient is oedematous, hypovolaemia if present should be treated first. This should then, be followed by a negative balance of sodium and water, monitored using urine Na excretion, levels
Page 4149 :
, , Solutions such as Dextran 70 should be used in caution in patients with sepsis as there is a, risk of developing acute renal injury, , References, NICE guidance CG174. Intravenous fluid therapy in adults. December 2013., British Consensus Guidelines on Intravenous Fluid Therapy for Adult Surgical Patients. GIFTASUP, (2009), Next question
Page 4150 :
Theme: Surgical analgesia, , A., B., C., D., E., F., G., , TAP block, Epidural, Spinal block, Patient controlled analgesia, Paracetamol and diclofenac, Pethidine as required, Regular nefopam, , Please select the most appropriate analgesic modality for the scenario given. Each option may be, used once, more than once or not at all., , 64., , A 63 year old man with carcinoma of the splenic flexure undergoes an extended right, hemicolectomy through a midline excision. He suffers from COPD., You answered TAP block, The correct answer is Epidural, This man is at high risk of atelectasis, hypoventilation can be avoided by minimising post, operative pain through an epidural. A spinal block is short acting, therefore not, appropriate., , 65., , A 63 year old man with rectal cancer is due to undergo an anterior resection by, laparoscopic approach. He is otherwise well., TAP block, This is a localised infiltration of the abdominal wall with long acting local anaesthetic., This will provide optimal analgesia for the more limited pain that may occur with a, laparoscopic procedure., , 66., , A 52 year old man undergoes an appendicectomy through a lower midline abdominal, incision as the initial laparoscopy shows an appendix mass. He is otherwise well., You answered TAP block, The correct answer is Patient controlled analgesia, This is more painful than a conventional appendicectomy, but conversion to a limited, laparotomy was not anticipated. A PCA is the most effective and practically applicable, modality in this case.
Page 4151 :
Please rate this question:, , Discuss and give feedback, , Next question, , Management of pain, World Health Organisation Analgesic Ladder, , , , , Initially peripherally acting drugs such as paracetamol or non-steroidal anti-inflammatory, drugs (NSAIDs) are given., If pain control is not achieved, the second part of the ladder is to introduce weak opioid drugs, such as codeine or dextropropoxyphene together with appropriate agents to control and, minimise side effects., The final rung of the ladder is to introduce strong opioid drugs such as morphine. Analgesia, from peripherally acting drugs may be additive to that from centrally-acting opioids and thus,, the two are given together., , The World Federation of Societies of Anaesthesiologists (WFSA) Analgesic Ladder, , , , , , For management of acute pain, Initially, the pain can be expected to be severe and may need controlling with strong, analgesics in combination with local anaesthetic blocks and peripherally acting drugs., The second rung on the postoperative pain ladder is the restoration of the use of the oral, route to deliver analgesia. Strong opioids may no longer be required and adequate analgesia, can be obtained by using combinations of peripherally acting agents and weak opioids., The final step is when the pain can be controlled by peripherally acting agents alone., , Local anaesthetics, , , , , , , , Infiltration of a wound with a long-acting local anaesthetic such as Bupivacaine, Analgesia for several hours, Further pain relief can be obtained with repeat injections or by infusions via a thin catheter, Blockade of plexuses or peripheral nerves will provide selective analgesia in those parts of, the body supplied by the plexus or nerves, Can either be used to provide anaesthesia for the surgery or specifically for postoperative, pain relief, Especially useful where a sympathetic block is needed to improve postoperative blood, supply or where central blockade such as spinal or epidural blockade is contraindicated., , Spinal anaesthesia, Provides excellent analgesia for surgery in the lower half of the body and pain relief can last many, hours after completion of the operation if long-acting drugs containing vasoconstrictors are used.
Page 4152 :
- Side effects of spinal anaesthesia include: hypotension, sensory and motor block, nausea and, urinary retention., Epidural anaesthesia, An indwelling epidural catheter inserted. This can then be used to provide a continuous infusion of, analgesic agents. It can provide excellent analgesia. They are still the preferred option following, major open abdominal procedures and help prevent post operative respiratory compromise resulting, from pain., - Disadvantages of epidurals is that they usually confine patients to bed, especially if a motor block is, present. In addition an indwelling urinary catheter is required. Which may not only impair mobility but, also serve as a conduit for infection. They are contraindicated in coagulopathies., Transversus Abdominal Plane block (TAP), In this technique an ultrasound is used to identify the correct muscle plane and local anaesthetic, (usually bupivicaine) is injected. The agent diffuses in the plane and blocks many of the spinal, nerves. It is an attractive technique as it provides a wide field of blockade but does not require the, placement of any indwelling devices. There is no post operative motor impairment. For this reason it, is the preferred technique when extensive laparoscopic abdominal procedures are performed. They, will then provide analgesia immediately following surgery but as they do not confine the patient to, bed, the focus on enhanced recovery can begin sooner., -The main disadvantage is that their duration of action is limited to the half life of the local, anaesthetic agent chosen. In addition some anaesthetists do not have the USS skills required to site, the injections., Patient Controlled Analgesia (PCA), - Patients administer their own intravenous analgesia and titrate the dose to their own end-point of, pain relief using a small microprocessor - controlled pump. Morphine is the most popular drug used., Strong Opioids, Severe pain arising from deep or visceral structures requires the use of strong opioids, Morphine, , , , , , Short half life and poor bioavailability., Metabolised in the liver and clearance is reduced in patients with liver disease, in the elderly, and the debilitated, Side effects include nausea, vomiting, constipation and respiratory depression., Tolerance may occur with repeated dosage, , Pethidine, , , , Synthetic opioid which is structurally different from morphine but which has similar actions., Has 10% potency of morphine., Short half life and similar bioavailability and clearance to morphine.
Page 4153 :
, , , Short duration of action and may need to be given hourly., Pethidine has a toxic metabolite (norpethidine) which is cleared by the kidney, but which, accumulates in renal failure or following frequent and prolonged doses and may lead to, muscle twitching and convulsions. Extreme caution is advised if pethidine is used over a, prolonged period or in patients with renal failure., , Weak opioids, Codeine: markedly less active than morphine, has predictable effects when given orally and is, effective against mild to moderate pain., Non opioid analgesics, - Mild to moderate pain., Paracetamol, , , , , , Inhibits prostaglandin synthesis., Analgesic and antipyretic properties but little anti-inflammatory effect, It is well absorbed orally and is metabolised almost entirely in the liver, Side effects in normal dosage and is widely used for the treatment of minor pain. It causes, hepatotoxicity in over dosage by overloading the normal metabolic pathways with the, formation of a toxic metabolite., , NSAIDs, , , , , , , Analgesic and anti-inflammatory actions, Inhibition of prostaglandin synthesis by the enzyme Cyclooxygenase which catalyses the, conversion of arachidonic acid to the various prostaglandins that are the chief mediators of, inflammation. All NSAIDs work in the same way and thus there is no point in giving more, than one at a time. ., NSAIDs are, in general, more useful for superficial pain arising from the skin, buccal mucosa,, joint surfaces and bone., Relative contraindications: history of peptic ulceration, gastrointestinal bleeding or bleeding, diathesis; operations associated with high blood loss, asthma, moderate to severe renal, impairment, dehydration and any history of hypersensitivity to NSAIDs or aspirin., , Neuropthic pain, National Institute of Clinical Excellence (UK) guidelines:, , , , , , First line: Amitriptyline (Imipramine if cannot tolerate) or pregabalin, Second line: Amitriptyline AND pregabalin, Third line: refer to pain specialist. Give tramadol in the interim (avoid morphine), If diabetic neuropathic pain: Duloxetine
Page 4155 :
Which of the following anaesthetic agents has the strongest analgesic effect?, , Sodium thiopentone, , Ketamine, , Midazolam, , Etomidate, , None of the above, , Ketamine has a moderate to strong analgesic effect. It may be used for emergency procedures, outside the hospital environment to induce anaesthesia for procedures such as emergency, amputation., Please rate this question:, , Discuss and give feedback, , Next question, , Anaesthetic agents, The table below summarises some of the more commonly used IV induction agents, , Agent, , Specific features, , Propofol, , , , , , , , , Rapid onset of anaesthesia, Pain on IV injection, Rapidly metabolised with little accumulation of metabolites, Proven anti emetic properties, Moderate myocardial depression, Widely used especially for maintaining sedation on ITU, total IV, anaesthesia and for daycase surgery, , Sodium, thiopentone, , , , Extremely rapid onset of action making it the agent of choice for rapid, sequence of induction, Marked myocardial depression may occur, Metabolites build up quickly, , ,
Page 4156 :
Ketamine, , , , , Unsuitable for maintenance infusion, Little analgesic effects, , , , , , May be used for induction of anaesthesia, Has moderate to strong analgesic properties, Produces little myocardial depression making it a suitable agent for, anaesthesia in those who are haemodynamically unstable, May induce state of dissociative anaesthesia resulting in nightmares, , , , Etomidate, , , , , , , Has favorable cardiac safety profile with very little haemodynamic, instability, No analgesic properties, Unsuitable for maintaining sedation as prolonged (and even brief) use, may result in adrenal suppression, Post operative vomiting is common, Next question
Page 4157 :
Which statement is true on enteral feeding?, , A PEG can only be used 12 hours after insertion, , A motility agent is avoided for ITU patients with an Nasogastric tube, , A regime of 24 hours continuous feeding is recommended for ITU patients, , It is associated with more hepatic synthetic disruption than use of TPN, , Enteral feeding is not possible in upper GI dysfunction, , Please rate this question:, , Discuss and give feedback, , Next question, , Enteral Feeding, , , , , , , , , , , , Identify patients as malnourished or at risk (see below), Identify unsafe or inadequate oral intake with functional GI tract, Consider for enteral feeding, Gastric feeding unless upper GI dysfunction (then for duodenal or jejunal tube), Check NG placement using aspiration and pH (check post pyloric tubes with AXR), Gastric feeding > 4 weeks consider long-term gastrostomy, Consider bolus or continuous feeding into the stomach, ITU patients should have continuous feeding for 16-24h (24h if on insulin), Consider motility agent in ITU or acute patients for delayed gastric emptying. If this doesn't, work then try post pyloric feeding or parenteral feeding., PEG can be used 4 hours after insertion, but should not be removed until >2 weeks after, insertion., , Surgical patients due to have major abdominal surgery: if malnourished, unsafe swallow/inadequate, oral intake and functional GI tract then consider pre operative enteral feeding., Patients identified as being malnourished, , , , , BMI < 18.5 kg/m2, unintentional weight loss of > 10% over 3-6/12, BMI < 20 kg/m 2 and unintentional weight loss of > 5% over 3-6/12
Page 4158 :
AT RISK of malnutrition, , , , , , Eaten nothing or little > 5 days, who are likely to eat little for a further 5 days, Poor absorptive capacity, High nutrient losses, High metabolism, , Reference, Stroud M et al. Guidelines for enteral feeding in adult hospital patients. Gut 2003; 52(Suppl VII):vii1 vii12., Next question
Page 4159 :
Which of the following does not need monitoring during home parenteral nutritional support?, , Folate levels, , Zinc levels, , Vitamin D, , Thyroid function, , Bone densitometry, , Please rate this question:, , Discuss and give feedback, , Next question, , Nutrition Monitoring-NICE guidelines, , , , , , , Weight: daily if fluid balance concerns, otherwise weekly reducing to monthly, BMI: at start of feeding and then monthly, If weight cannot be obtained: monthly mid arm circumference or triceps skin fold thickness, Daily electrolytes until levels stable. Then once or twice a week., Weekly glucose, phosphate, magnesium, LFTs, Ca, albumin, FBC, MCV, , levels if stable, , , , , , 2-4 weekly Zn, Folate, B12 and Cu levels if stable, 3-6 monthly iron and ferritin levels, manganese (if on home parenteral regime), 6 monthly vitamin D, Bone densitometry initially on starting home parenteral nutrition then every 2 years, Next question
Page 4160 :
Which of the following is not typically included in total parenteral nutritional solutions?, , Fibre, , Lipid, , Potassium, , Glucose, , Magnesium, , There is no indication for inclusion of fibre in solutions of TPN, nor would it be safe to do so., Please rate this question:, , Discuss and give feedback, , Next question, , Total parenteral nutrition, , , , , , , Commonly used in nutritionally compromised surgical patients., Bags contain combinations of glucose, lipids and essential electrolytes, the exact, composition is determined by the patients nutritional requirements., Although it may be infused peripherally, this may result in thrombophlebitis., Longer term infusions should be administered into a central vein (preferably via a PICC line)., Complications are related to sepsis, re-feeding syndromes and hepatic dysfunction., Next question
Page 4161 :
A 28 year old man with poorly controlled Crohns disease is nutritionally compromised. The decision, is made to start TPN, via which of the following routes should it be best administered?, , Internal jugular vein via a central venous catheter, , Internal carotid artery, , Cephalic vein via peripheral cannula, , Basilic vein via peripheral cannula, , Common femoral vein via a central venous catheter, , Since TPN solutions are irritant to veins they are best administered via a central line. The femoral, route has a higher incidence of line associated sepsis and is thus best avoided in this setting., Please rate this question:, , Discuss and give feedback, , Next question, , Parenteral feeding-NICE guidelines, Parenteral nutrition: NICE guidelines summary, Identify patients as malnourished or at risk, Patients identified as being malnourished, , , , BMI < 18.5 kg/m2, unintentional weight loss of > 10% over 3-6/12, BMI < 20 kg/m 2 and unintentional weight loss of > 5% over 3-6/12, , AT RISK of malnutrition, , , , , eaten nothing or little > 5 days, who are likely to eat little for a further 5 days, poor absorptive capacity, high nutrient losses, high metabolism
Page 4162 :
Identify unsafe/inadequate oral intake OR a non functional GI tract/perforation/inaccessible, Consider parenteral nutrition:, , , , , , , for feeding < 14 days consider feeding via a peripheral venous catheter, for feeding > 30 days use a tunneled subclavian line, continuous administration in severely unwell patients, if feed needed > 2 weeks consider changing from continuous to cyclical feeding, don't give > 50% of daily regime to unwell patients in first 24-48 hours, , Surgical patients: if malnourished with unsafe swallow OR a non functional GI, tract/perforation/inaccessible then consider peri operative parenteral feeding., Next question
Page 4163 :
Which of the following statements relating to the use of human albumin solution is false?, , When administered in the peri operative period it does not increase the length of stay in, hospital compared with crystalloid solutions, Concentrated solutions may produce diuresis in patients with liver failure, , It may restore plasma volume in cases of sodium and water overload, , It may be associated with risk of acquiring new variant Creutzfeld-Jacob disease, , Hepatitis C remains a concern when large volumes are infused, , Human albumin solution went out of vogue following the Cochrane review in 2004 that showed it, increased mortality. This view has been challenged and subsequent studies have confirmed it to be, safe for use. Viruses are inactivated during the preparation process. However, theoretical risks, regarding new varient CJD still exist. Outcomes in the peri operative setting are similar whether, colloid, crystalloid or albumin are used., Please rate this question:, , Discuss and give feedback, , Next question, , Post operative fluid management, Composition of commonly used intravenous fluids mmol-1, , Na, , K, , Cl, , Bicarbonate, , Lactate, , Plasma, , 137-147, , 4-5.5, , 95-105, , 22-25, , -, , 0.9% Saline, , 153, , -, , 153, , -, , -, , Dextrose / saline, , 30.6, , -, , 30.6, , -, , -
Page 4164 :
Hartmans, , 130, , 4, , 110, , -, , 28, , Post operative fluid management, In the UK the GIFTASUP and NICE (CG174 2013) guidelines (see reference below) were devised to, try and provide some consensus guidance as to how intravenous fluids should be administered. A, decade ago it was a commonly held belief that little harm would occur as a result of excessive, administration of normal saline and many oliguric post operative patients received enormous, quantities of IV fluids. As a result they developed hyperchloraemic acidosis. With greater, understanding of this potential complication, the use of electrolyte balanced solutions (Ringers, lactate/ Hartmans) is now favored over normal saline., The other guidance includes:, , , , , , , , Fluids given should be documented clearly and easily available, Assess the patient's fluid status when they leave theatre, If a patient is haemodynamically stable and euvolaemic, aim to restart oral fluid intake as, soon as possible, Review patients whose urinary sodium is < 20, If a patient is oedematous, hypovolaemia if present should be treated first. This should then, be followed by a negative balance of sodium and water, monitored using urine Na excretion, levels, Solutions such as Dextran 70 should be used in caution in patients with sepsis as there is a, risk of developing acute renal injury, , References, NICE guidance CG174. Intravenous fluid therapy in adults. December 2013., British Consensus Guidelines on Intravenous Fluid Therapy for Adult Surgical Patients. GIFTASUP, (2009), Next question
Page 4165 :
Theme: Wound management, , A., B., C., D., E., F., G., , VAC Device, Packing with alginate ribbon, Packing with ribbon gauze, Application of silver nitrate, Application of potassium permangenate, Use of iodine soaked gauze, Gauze soaked in proflavin, , For each wound please select the most appropriate management option. Each option may be used, once, more than once, or not at all., , 73., , A 56 year old man has a superficial dehisence of a midline sternotomy wound following, an aortic valve replacement., VAC Device, Provided the sternum is stable a VAC device should promote granulation and healing. It is, not indicated where the sternum has come apart., , 74., , A 72 year old man has discharge from a healed abdomino-perineal resection wound. On, examination, it has almost completely healed but there is prominent granulation tissue at, the apex of the wound. There is no evidence of an underlying collection and he is, otherwise well., You answered VAC Device, The correct answer is Application of silver nitrate, Silver nitrate will cauterise the exuberant granulation tissue and promote healing., , 75., , A 23 year old man has an incision and drainage of an axillary abscess, there is no residual, surrounding tissue infection., You answered VAC Device, The correct answer is Packing with alginate ribbon, Use of gauze is inappropriate and will be painful to redress., , Please rate this question:
Page 4166 :
Discuss and give feedback, , Next question, , Methods of wound closure, Method of, closure, , Indication, , Primary closure, , , , , , Clean wound, usually surgically created or following minor trauma, Standard suturing methods will usually suffice, Wound heals by primary intention, , Delayed primary, closure, , , , , Similar methods of actual closure to primary closure, May be used in situations where primary closure is either not, achievable or not advisable e.g. infection, , Vacuum assisted, closure, , , , , Uses negative pressure therapy to facilitate wound closure, Sponge is inserted into wound cavity and then negative pressure, applied, Advantages include removal of exudate and versatility, Disadvantages include cost and risk of fistulation if used incorrectly, on sites such as bowel, , , , , Split thickness, skin grafts, , , , , , Superficial dermis removed with Watson knife or dermatome, (commonly from thigh), Remaining epithelium regenerates from dermal appendages, Coverage may be increased by meshing, , Full thickness skin, grafts, , , , , , , Whole dermal thickness is removed, Sub dermal fat is then removed and graft placed over donor site, Better cosmesis and flexibility at recipient site, Donor site "cost", , Flaps, , , , , , , Viable tissue with a blood supply, May be pedicled or free, Pedicled flaps are more reliable, but limited in range, Free flaps have greater range but carry greater risk of breakdown as, they require vascular anastomosis, Next question
Page 4167 :
A 22 year old fit and well male undergoes an emergency appendicectomy. He is given, suxamethonium. An inflamed appendix is removed and the patient is returned to recovery. On arrival, in the recovery area; the patient develops a tachycardia of 120 bpm and a temperature of 40 ºC. He, has generalised muscular rigidity. What is the most likely diagnosis?, , Acute dystonic reaction, , Malignant hyperthermia, , Pelvic abscess, , Epilepsy, , Serotonin syndrome, , Anaesthetic agents, such as suxamethonium, can cause malignant hyperthermia in patients with a, genetic defect. Acute dystonic reaction normally is associated with antipsychotics (haloperidol) and, metoclopramide. These lead to marked extrapyramidal effects. Serotonin syndrome is associated, with the antidepressants selective serotonin reuptake inhibitors (SSRIs) and selective, serotonin/norepinephrine reuptake inhibitors (SSNRIs). This causes a syndrome of agitation,, tachycardia, hallucinations and hyper-reflexia., Please rate this question:, , Discuss and give feedback, , Next question, , Malignant hyperthermia, Overview, , , , , , , Condition seen following administration of anaesthetic agents ( rate of 1 in 15,000), Characterised by hyperpyrexia and muscle rigidity, Cause by excessive release of Ca2+ from the sarcoplasmic reticulum of skeletal muscle, Associated with defects in a gene on chromosome 19 encoding the ryanodine receptor,, which controls Ca2+ release from the sarcoplasmic reticulum, Neuroleptic malignant syndrome may have a similar aetiology, , Causative agents
Page 4169 :
A 45 year old man develops acute respiratory distress syndrome during an attack of severe acute, pancreatitis. Which of the following is not a feature of adult respiratory distress syndrome?, , It usually consists of type I respiratory failure., , Patients typically require high ventillatory pressures., , A Swann Ganz Catheter would typically have a reading in excess of 18mmHg., , It may complicate acute pancreatitis., , It may heal with fibrosis., , Right heart pressure should be normal., Please rate this question:, , Discuss and give feedback, , Adult respiratory distress syndrome, Defined as an acute condition characterized by bilateral pulmonary infiltrates and severe hypoxemia, (PaO2/FiO2 ratio < 200) in the absence of evidence for cardiogenic pulmonary oedema (clinically or, pulmonary capillary wedge pressure of less than 18 mm Hg)., In is subdivided into two stages. Early stages consist of an exudative phase of injury with associated, oedema. The later stage is one of repair and consists of fibroproliferative changes. Subsequent, scarring may result in poor lung function., Causes, , , , , , , , Sepsis, Direct lung injury, Trauma, Acute pancreatitis, Long bone fracture or multiple fractures (through fat embolism), Head injury (causes sympathetic nervous stimulation which leads to acute pulmonary, hypertension), , Clinical features
Page 4170 :
, , , , Acute dyspnoea and hypoxaemia hours/days after event, Multi organ failure, Rising ventilatory pressures, , Management, , , , , , , Treat the underlying cause, Antibiotics (if signs of sepsis), Negative fluid balance i.e. Diuretics, Recruitment manoeuvres such as prone ventilation, use of positive end expiratory pressure, Mechanical ventilation strategy using low tidal volumes, as conventional tidal volumes may, cause lung injury (only treatment found to improve survival rates)